
Abstract
Background:
There is lack of evaluation of the effect of the treated area on the urinary function after focal therapy. The objectives of the study is to evaluate the effects of focal therapy on urinary function in the anterior portion of the transition zone (TZ) with transrectal high-intensity focused ultrasound (HIFU) for localized prostate cancer (PCa).
Methods:
From 2016 to 2018, patients who were diagnosed as having localized PCa and treated with focal therapy with HIFU, were included prospectively. The urinary function and complications were evaluated separately in the treated regions of the anterior TZ (TZ group) and other portions (other group) for 12 months. Before and after the treatment, the International Prostate Symptom Score (IPSS), IPSS Quality Of Life (QOL), Overactive Bladder Symptom Score (OABSS), and uroflowmetry were evaluated to assess the urinary function.
Results:
Ninety patients were included in the study. There was no significant differences in the patients' characteristics between the two groups. At 1 month after the treatment, IPSS (p = 0.011), IPSS QOL (p = 0.002), OABSS (p = 0.002), maximum flow rates (p = 0.011), and residual urine volume (p = 0.011) in TZ group were significantly deteriorated compared with the other group. Multivariate logistic regression analysis revealed that anterior TZ treatment (odds ratio, 3.386; p = 0.029) was an independent risk factor for the deterioration with ≥32% of preoperative status of maximum flow rates. Concerning complication, the rates of Grade 2 urinary retention and Grade 3 urethral stricture were 15.4% and 11.5% in the TZ group and 0% and 0% in the other group, respectively.
Conclusions:
There was a greater risk of urinary dysfunction with treatment in the anterior TZ portion than in the other portion at 1 month after focal therapy with HIFU.
Introduction
Although radical treatment, such as radical prostatectomy and radiation therapy, is an effective treatment option for localized prostate cancer (PCa), it is associated with considerable morbidity in some cases and efforts are made to provide minimally invasive alternatives with equal efficacy but fewer side effects. 1 Focal therapy is a diagnosis-based investigational treatment option for localized PCa that effectively controls the clinically significant PCa while preserving the anatomical structures related to urinary and sexual function. 2 High-intensity focused ultrasound (HIFU) has been used as representative modalities for focal therapy based on oncological and functional outcomes confirmed in long-term follow-up after whole-gland treatment. 2
HIFU is a noninvasive technique for the thermal ablation of tissue and induces a complete coagulation necrosis of a target tumor, without requiring surgical exposure. 3 With the development of HIFU technology, 4 HIFU has been the most frequently used technique in recently reported clinical trials of focal therapy. 2,5 In the previous reports of whole-gland therapy with HIFU for localized PCa, bladder outlet obstruction occurred in 13% to 19.7% of the patients after the treatment, 4,6 which was due to the prostatic swelling and/or urethral stricture. 7,8 On the other hand, urinary retention (1.2% to 15%) and urethral stricture (2% to 5%) were lower in the patients after focal therapy with HIFU, 9 rather than in patients after whole-gland therapy. Although the adverse effects were decreased in focal therapy compared with those in whole-gland therapy with HIFU, there are some reports in the literature that show urinary disorders such as urinary retention (5%–13%) and urethral stenosis (0.03%) in patients after focal therapy. 9,10 In a previous report, urinary dysfunction was significantly preserved after the HIFU in patients who were treated with urethra-sparing ablation compared with that in patients who were treated with whole-gland ablation, including the urethra. 8
To date, there is lack of evaluation on the effect of the treated area on the urinary function after focal therapy. The prediction of the effect would provide detailed information and ameliorate the medical approach to patients with localized PCa before and after treatment. We hypothesized that the treatment of the anterior transition zone (TZ) has more risks of causing urinary dysfunction compared with that of other portions in focal therapy, because prostate swelling is more likely to occur in TZ than in PZ (18% vs 9%) after HIFU, 7 and urethral stricture and urinary retention easily occur in nonsparing urethral treatment with HIFU. 8 In this study, the urinary effect of the treated area was prospectively evaluated in patients who were treated by focal therapy with HIFU.
Patients and Methods
Patients
From 2016 to 2018, the patients who were scheduled to be treated with focal therapy using HIFU received informed consent after receiving Institutional Review Board approval (15R-212). The focal therapy was performed for the patients who had serum PSA levels ≤20 ng/mL, significant PCa that had been located using MRI/transrectal ultrasound elastic fusion image-guided transperineal prostate biopsy using BioJet® system (D&K Technologies GmbH, Barum, Germany) and 12-cores transperineal systematic biopsy, life expectancies longer than 10 years, no metastasis, no bilateral cancers with Gleason scores ≥7, no severe anal strictures, and no previous history of treatment for PCa. The patients were informed of this procedure as an optional treatment, in addition to the standard treatment; those who underwent this procedure provided informed consent.
Treatment protocol
The details of our protocol of the focal therapy were described in the previous report. 11 HIFU produces ultrasound waves generated by a spherical transducer, delivering ultrasonic energy to pinpoint the focal area of only millimeters in diameter (3 × 3 × 12 mm or 3 × 3 × 10 mm) and the focal area moves the treatment-planned area (Fig. 1). A day after the treatment, the patients were discharged after the removal of the urethral catheter. Before the discharge, self-catheter guidance was done for all patients in case of urinary retention. The status of self-catheterization was confirmed by the urologist at an outpatient clinic during follow-up.

HIFU for the anterior TZ portion in the apex and base sides of the prostate/HIFU produces ultrasound waves generated by a spherical transducer, delivering ultrasonic energy to pinpoint the focal area of only millimeters in diameter (3 × 3 × 12 mm or 3 × 3 × 10 mm). The focal area moves the treatment-planned area, and the thermal and mechanical effects of HIFU destroy PCa within the prostate tissue. The gray zone is the anterior TZ. The figure shows that the focal area moves from the center to the lateral position in the anterior TZ portion, and the ultrasonic energy in the focusing process goes through the urethra during the treatment of the anterior TZ portion. HIFU = high-intensity focused ultrasound; PCa = prostate cancer; TZ = transition zone. Color images are available online.
Evaluation of urinary functional outcomes and complications by the location of the treatment
The urinary function and complications were evaluated separately in the anterior TZ portion (Fig. 1) and the other portion without TZ. The anterior TZ portion is above the urethra and does not include the urethra. Ultrasonic energy in the focusing process passes through the urethra during the treatment of the anterior TZ portion. Follow-up periods were 12 months after treatment in all cases in this study. Before and after the treatment, the following scores were assessed: the International Prostate Symptom Score (IPSS), IPSS Quality Of Life (QOL), Overactive Bladder Symptom Score (OABSS), and uroflowmetry to assess urinary function by the location of the treatment, which included the anterior TZ portion or not. Scores for all these indices were taken before treatment and at 1, 3, 6, 9, and 12 months after. Complications were evaluated at 1, 3, 6, 9, and 12 months after treatment with the Common Terminology Criteria for Adverse Events (CTCAE) version 4.0.
Statistical analyses
All statistical analyses were performed using IBM SPSS® Statistics version 26 (IBM, Armonk, NY). The longitudinal changes in urinary function in the follow-up period were analyzed using the one-way analysis of variance. The differences in the characteristics of the patients whose maximum flow rates after treatment deteriorated, improved, or remained the same, as well biochemical failure were analyzed using Mann–Whitney U test for quantitative data and chi-square test for categorical variables, such as D'Amico Risk classification and the location of treatment area. Univariate and multivariate analyzes using logistic regression identified significant risk factors of the worsening the urination status. A p < 0.05 was considered statistically significant.
Results
Ninety patients were included in this study, and their characteristics are shown in Table 1. Of the patients, 26 patients (29%) were treated in the anterior TZ. Between the patients who were treated in the anterior TZ and the other portion, there was no significant difference in age, serum PSA value, prostate volume, PSA density, and percentage of the patients within the risk group. The perioperative data are detailed in Table 2. Between the patients who were treated in the anterior TZ portion and the other portion, there was no significant difference in procedural and HIFU ablation time, treated volume, and HIFU energy for each case. There was no intraprocedural complication in the cases. Catheterization and hospitalization times were within 24 hours after treatment in all patients. Of the 90 patients, 6 (6.7%) experienced the self-catheterization within 1 month after the treatment. Of the six patients, five were treated in the anterior TZ portion.
Patients' Characteristics
D'Amico risk classification.
PSA = prostate-specific antigen; PZ = peripheral zone; TZ = transition zone.
Perioperative Data
HIFU = high-intensity focused ultrasound.
Longitudinal changes of IPSS, IPSS QOL, OABSS, maximum flow rate, and residual urine in the patients 12 months after the treatment (anterior TZ portion, n = 26 vs without the anterior TZ portion, n = 64), are shown in Table 3 and Figure 2. In the patients who were treated in the anterior TZ portion and in the other portion, urinary function was significantly impaired at 1 month after treatment compared with pretreatment values. They improved to baseline, and did not significantly differ 3 months after the treatment. At 1 month after the treatment, IPSS (p = 0.011), IPSS QOL (p = 0.002), OABSS (p = 0.002), maximum flow rates (p = 0.011), and residual urine volume (p = 0.011) in TZ group were significantly deteriorated compared with the other group. In 90 patients, median deterioration rates of maximum flow rates was 32% at 1 month after the treatment. In the evaluation of characteristics of the patients who had deterioration with ≥32% and <32% of preoperative status of maximum flow rates (Table 4), there was a significant difference between the maximum flow rate in the pretreatment (p = 0.009) and the location of treatment area (p = 0.008). The multivariate logistic regression analysis showed that maximum flow rate in pretreatment (odds ratio, 1.083; p = 0.023) and the location of treatment area (odds ratio, 3.386; p = 0.029) were significant risk factors of the deterioration with ≥32% of preoperative status of maximum flow rates (Table 5).
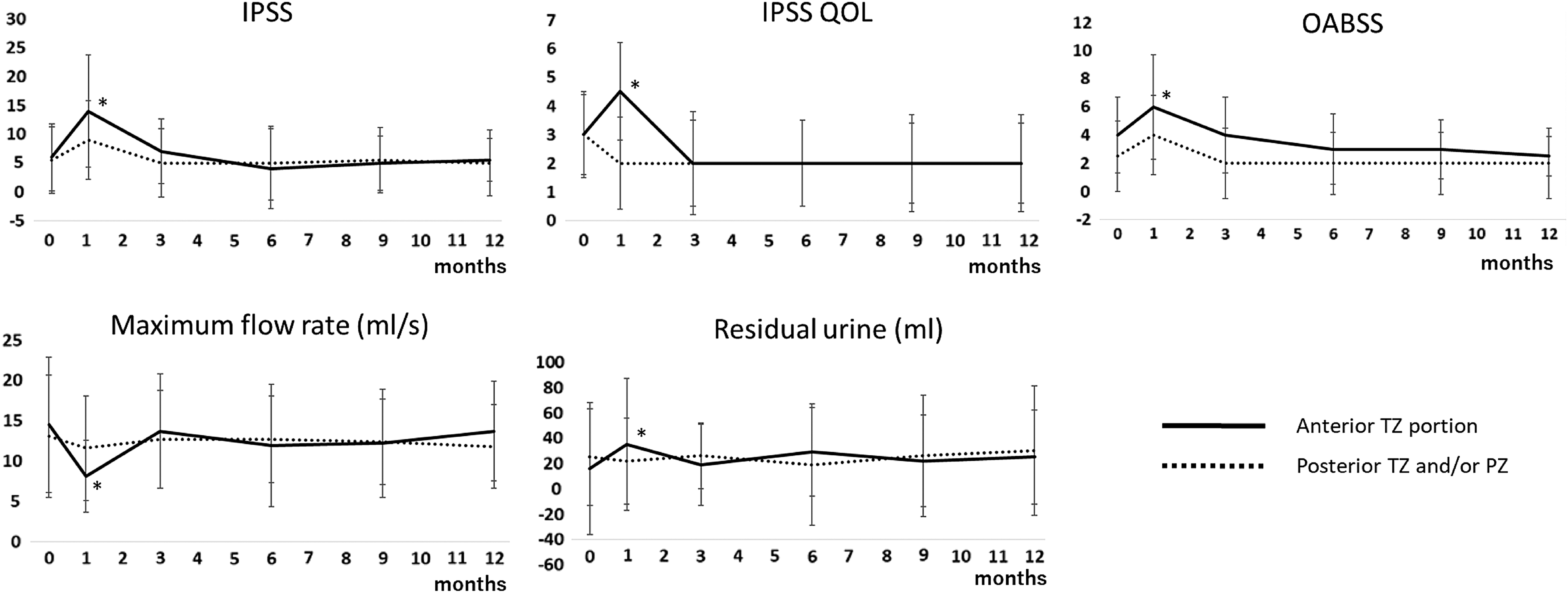
Longitudinal changes of IPSS, IPSS QOL, OABSS, maximum flow rate, and residual urine in the patients during 12 months after the treatment of the treatment area (anterior TZ portion, n = 26 vs posterior TZ and/or PZ, n = 64)/Solid and dotted lines show the longitudinal changes in the patients who were treated in the anterior TZ and in the other portion, respectively. In the patients who were treated in the anterior TZ portion and in the other portion, urinary function was significantly impaired at 1 month after treatment compared with pretreatment values, they improved to baseline, and did not significantly differ 3 months after the treatment. There was a significant difference in IPSS (p = 0.011), IPSS QOL (p = 0.002), OABSS (p = 0.002), maximum flow rates (p = 0.011), and residual urine volume (p = 0.011) between the patients who were treated with and without the anterior TZ portion at 1 month after the treatment. *IPSS = International Prostate Symptom Score; OABSS = Overactive Bladder Symptom Score; PZ = peripheral zone; QOL = quality of life.
Longitudinal Changes of IPSS, IPSS QOL, OABSS, Maximum Flow Rate, and Residual Urine in the Patients During 12 Months After the Treatment of the Treatment Area (Anterior TZ Portion, n = 26 vs Posterior TZ and/or PZ, n = 64)
p < 0.05.
IPSS = International Prostate Symptom Score; OABSS = Overactive Bladder Symptom Score; QOL = quality of life; SD = standard deviation.
Characteristics of the Patients Who Had Deterioration with ≥32% and <32% of Preoperative Status of Maximum Flow Rates
p < 0.05.
PSA = prostate-specific antigen.
Univariate and Multivariate Logistic Regression Analyzes to Predict the Deterioration with ≥32% of Preoperative Status of Maximum Flow Rates
p < 0.005.
Among the urinary function-associated complications, Grade 2 urinary retention occurred within 1 month after treatment in four patients (4.4%), which was caused by transient prostatic swelling. After self-catheterization for urination in four patients, three patients (3.3%) developed grade 3 urethral stricture within 3 months after the treatment. Two patients showed improved urethral stricture by the bougie dilator, and one patient showed improved urethral stricture by the transurethral incision of the urethral stricture. No patient suffered from incontinence and rectourethral fistulae. Self-catheterization was used within 1 month after the treatment for six patients who experienced difficulty urinating after the treatment, which included the four patients who suffered from urinary retention. Of the six patients, four were treated in the anterior TZ.
Discussion
In terms of functional outcomes in recent prospective studies of focal therapy with HIFU, the leak- and pad-free continence rate ranged from 80% to 100%, 10 –15 and erectile function was preserved in 50% to 90% of patients. 10 –12,15 Concerning complication, urinary retention and urethral stricture occurred in 5.6% to 9.8% at 1 month, 10,13 and 1.9% to 3.3% at 3 months after the focal therapy with HIFU. 10,15 However, the previous studies did not report the relation between the treated area and these complications. In this study, the leak- and pad-free continence rate was 100%, and the rate of Grade 2 urinary retention and Grade 3 urethral stricture were 15.4% and 11.5% in the patients who were treated in the anterior TZ, and 0% and 0% in the patients who were treated out of the anterior TZ. The rates of self-catheterization were 15.4% in the patients who were treated in the anterior TZ, and 3.1% in the patients who were treated in the other portion (p = 0.002). These findings show that the anterior TZ portion treatment has a higher risk of leading to the urinary retention and urethral stricture compared with the patients who were treated in the other portions.
In this study, there were significant differences in IPSS, IPSS QOL, OABSS, maximum flow rates, and residual urine volume between the patients who were treated with and without the anterior TZ portion at 1 month after the treatment. In the evaluation of the characteristics of the patients who had a deterioration, an improvement, or a stationary maximum flow rate, there was a significant difference between the maximum flow rate (mL/s) in the pretreatment and the location of the treatment area. Considering the patients with a preprocedural maximum flow rate ≥10 mL/s (n = 65), IPSS, IPSS QOL, OABSS, and maximum urinary flow rate were significantly impaired at 1 month after treatment compared with pretreatment values, they improved to baseline, and OABSS and maximum flow rate did not significantly differ after 3 months after the treatment in both the patients who were treated with (n = 19) and without (n = 46) the anterior TZ portion. However, there was a significant difference in the IPSS at 1 month and 3 months and IPSS QOL at 1 and 3 months after the treatment between the patients who were treated with and without the anterior TZ portion (Table 6 and Fig. 3). In the evaluation of the characteristics of the patients whose maximum flow rate was higher than 10 mL/s, median deterioration rates of maximum flow rates was 30% at 1 month after the treatment. The location of the treatment area was significantly different between the patients who had a deterioration of ≥30% and <30% of the preoperative status of maximum flow rates (Table 7). Multivariate logistic regression analysis showed that the location of treatment area was significant risk factors for the deterioration with ≥30% of preoperative status of maximum flow rates (odds ratio, 10.906; p = 0.003) (Table 8). These results showed that the anterior TZ treatment may has risk of worsening the urination status compared with the treatment of the other portion, and this result was consistent with our hypothesis that anterior TZ treatment could predispose to urinary dysfunction due to the prostatic swelling 7 and urinary stricture 8 after the focal therapy with HIFU.

Longitudinal changes of IPSS, IPSS QOL, OABSS, maximum flow rate, and residual urine in the patients with preprocedural maximum flow rate ≥10 mL/s during 12 months after the treatment of the treatment area (anterior TZ portion, n = 19 vs posterior TZ and/or PZ, n = 46)/Solid and dotted lines show the longitudinal changes in the patients who were treated in the anterior TZ and in the other portion, respectively. In the patients with preprocedural maximum flow rate ≥10 mL/s (n = 65), IPSS, IPSS QOL, OABSS, and maximum urinary flow rate were significantly impaired at 1 month after treatment compared with pretreatment values, they improved to baseline, and OABSS and maximum flow rate did not significantly differ after 3 months after the treatment in both of the patients who were treated with (n = 19) and without (n = 46) the anterior TZ portion. However, there was a significant difference in IPSS at 1 (p = 0.003) and 3 (p = 0.047) months after the treatment, and *IPSS QOL at 1 (p = 0.001) and 3 (p = 0.035) months after the treatment between the patients who were treated with and without the anterior TZ portion.
Longitudinal Changes of IPSS, IPSS QOL, OABSS, Maximum Flow Rate, and Residual Urine in the Patients with Preprocedural Maximum Flow Rate ≥10 mL/s During 12 Months After the Treatment by the Treatment Area (Anterior TZ Portion, n = 19 vs Posterior TZ and/or PZ, n = 46)
p < 0.05.
Characteristics of the Patients Who Had Deterioration and Improvement or Non-Change of Maximum Flow Rates in the Patients with Preprocedural Qmax >10 mL/s
p < 0.05.
Univariate and Multivariate Logistic Regression Analyzes to Predict the Deterioration with ≥30% of Preoperative Status of Maximum Flow Rates in the Patients with Preprocedural Qmax >10 mL/s
p < 0.05.
Although the characteristics make HIFU an attractive therapeutic modality for focal therapy of PCa, it has been known that negative effects on urination occurred in the prostate tissue after the treatment. Just after the HIFU ablation, prostatic swelling is caused due to diffuse stromal edema of the prostate for 1 to 2 months. 7 In the previous report, the median percent volume increase of the TZ was 18% during the anterior TZ treatment. 7 The transient prostatic swelling would be considered as the reason for the pressure of the urethra and difficulty in urination. However, the prostatic swelling is known to resolve within 2 month after the treatment. 16 Indeed, the transient deterioration of urinary function improved within 3 months in this study, and this duration was similar to that of the prostatic swelling. 17 Ultrasonic propagation through tissues can also produce another negative effect on urinary function. An ultrasound wave emanating from a transducer outside the body must travel through multiple tissue layers including the rectal wall, fat, and prostate capsule, before reaching the target area within the prostate. With the exception of fat, air and bone, most tissues in the human body have acoustic properties similar to those of water. Aqueous media are therefore optimal for transmitting ultrasonic energy from the transducer into the body, and reflections at tissue interfaces are generally weak. 18 At each tissue interface, part of the energy carried by the sound wave will be reflected, while the remaining energy is transmitted. 18 In the commercially available transrectal HIFU device, the energy was set based on the reflection of ultrasonic waves in the prostate tissue. 19,20 Furthermore, when ultrasound propagates through a tissue layer, the pressure fluctuations induced lead to a shearing motion of tissue at a microscopic level, which results in frictional heating. 18 Urethral fibrosis is thought to be a reason of the urethral stricture after the HIFU for the localized PCa. 8 Urethral fibrosis is regarded as due to the direct ablation of HIFU to the urethra. 8 Actually, urethral stricture occurred in the three patients who were treated in the anterior TZ anterior zone, but in no patient who was treated in the other portion. Based on the characteristics of HIFU, shearing motion of tissue and heating effect occur in the urethra during the anterior TZ portion treatment due to the ultrasonic propagation, and fibrosis was induced in the urethra after the treatment.
This study had some limitations. It was a non-randomized controlled trial for the analysis. In addition, 26 patients were treated in the anterior TZ. However, significant differences were found in the longitudinal changes of IPSS, IPSS QOL, OABSS, and maximum flow rate, as well as complications in this study. These findings support the hypothesis that the treatment of the anterior TZ portion treatment has more risks of leading to urinary dysfunction compared with that of the other portion in focal therapy. Multi-institutional studies with large sample sizes will be needed to analyze the functional outcomes in patients with localized PCa. Further, this study was conducted for 12 months. To clarify the effect to the urinary function after the focal therapy, longer periods of follow up would be required.
Conclusions
The treatment of the anterior TZ portion has more risks of causing urinary dysfunction compared with the treatment of the other portion in focal therapy, which was thought to be due to the transient prostatic swelling and urethral stricture post-HIFU. The present results should include the informed consent for the patients who had the significant cancer in the anterior TZ portion. In addition, extension of scheduled catheterization, such as suprapubic catheter and urethral catheter, might be considered for the patients. Multi-institutional studies with large sample sizes will be needed to analyze the functional outcomes in patients with localized PCa.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this work.