
Abstract
Background:
Stone prevention is dependent on high fluid intake, with evidence that low urine volume (LUV) can promote nephrolithiasis in the absence of other metabolic abnormalities. Herein, we investigate patient-related factors associated with LUV on initial 24-hour urine collection in an underserved population.
Materials and Methods:
A retrospective chart review was performed of patients treated by a single surgeon for nephrolithiasis from August 2014 to January 2019. Patients who submitted 24-hour urine samples were divided into two groups based on whether their initial collection was >2 L or not. Factors associated with 24-hour urine volume were analyzed using bivariate and multivariate analyses. As a secondary outcome, we investigated factors associated with corrected 24-hour urine volume on repeat 24-hour urine collection.
Results:
Two hundred eight patients (45.1%) submitted 24-hour urine collections, 63.9% (133/208) of which demonstrated a urine volume of <2 L. LUV was more common in female patients (77.1% vs 49.5%; p = 0.001) and patients with no insurance and Medicaid (no insurance [100%] vs Medicaid [74.1%] vs Medicare/private [58.6%]; p = 0.02). Female gender and insurance status were independent predictors of LUV in the multivariable analysis. Seventeen of 43 patients (39.5%) with LUV who provided a subsequent collection were able to correct their urine volume. Patients who improved their LUV were older (58.5 vs 45.9 years, p = 0.0149) and more likely to have surgical intervention for their kidney stones (94.1% vs 53.8%, p = 0.006). In our multivariable analysis, surgical intervention was associated with correcting urine volume.
Conclusions:
Female patients and those with no insurance or Medicaid were more likely to have LUV on an initial 24-hour urine collection. Further research into barriers to fluid intake is important for these two groups, along with directed patient education on strategies for increasing fluid intake.
Introduction
Nephrolithiasis is a complex metabolic condition affecting ∼5%–10% of the adult population in the United States. 1 According to the most recent analysis of data from the 2007 to 2010 National Health and Nutrition Examination Survey (NHANES) sample, there is a growing prevalence of nephrolithiasis across male and female patients of all age groups and particularly in minority groups. 2 Furthermore, nephrolithiasis is a condition that can recur, with research showing more than 50% of patients having a relapse within 10 years. 3
Dietary and lifestyle recommendations have shown benefit in reducing kidney stone recurrence in a cost-effective manner. 4 Optimization of fluid volume is no exception and is often the first recommendation that is made in our practice. One limitation in the literature regarding the prevalence of low urine volume (LUV) is the lack of investigation of LUV in underserved medical communities. This raises the question of how prevalent LUV is in our patient population, which is a designated health enterprise zone of north Philadelphia. 5
Herein, we sought to describe the current prevalence of LUV in 24-hour urine collection results in our underserved patient population. Factors that help to predict urine volume correction on subsequent collections were also investigated.
Materials and Methods
Approval for studying the metabolic evaluation and compliance among our kidney stone population was obtained from our institutional review board. A retrospective chart review of 461 patients between August 2014 and January 2019 was performed. Patients who had a complete 24-hour urine collection were included in the study. Patients with incomplete 24-hour urine collections or previous metabolic evaluations by another provider were excluded from the study.
In our clinical practice, we routinely request 24-hour urine collections for patients who are recurrent stone formers and of younger age (<40 years old), with a positive family history of kidney stones, and with medical comorbidities that predispose them to forming stones. Results of the 24-hour urine collection prompt recommendations for dietary and lifestyle modifications and, if needed, pharmacological therapy. For patients with LUV (<2.0 L), we typically recommend that they drink at least 100 ounces of water per day. A follow-up 24-hour urine collection is then requested at a minimum of 6 months after the interventions to assess whether any improvements in the analysis have been observed.
Patient demographics, pertinent medical history, family history of stone disease, stone composition, stone burden, and 24-hour urine collection data were all obtained from the electronic medical record. Patient demographics included age, sex, race/ethnicity, weight (kg), and insurance status (no insurance vs Medicaid vs Medicare/private). The prevalence of LUV as well as other 24-hour urine abnormalities was defined within our patient population.
Patients were divided into two groups, those with urine volume ≥2 L/24 hours vs those with urine volume <2 L/24 hours on initial 24-hour urine submission. A bivariate analysis using Fisher's exact test (for binary variables) and unpaired t-tests (for continuous variables) were used to identify patient characteristics that made LUV (volume <2 L/day) more likely on initial 24-hour urine collection. A multivariable logistic regression was performed following the bivariate analysis to identify individual predictors for LUV while adjusting for age, sex, race, weight (kg), presence of lower urinary tract symptoms (LUTS), type of health insurance, family history of kidney stones, personal history of kidney stones, and stone burden.
Patients with LUV (<2 L) on their initial 24-hour urine collections and who also provided a subsequent collection at a 6-month interval were identified. A bivariate analysis using Fisher's exact test (for binary variables) and unpaired t-tests (for continuous variables) were used to identify patient characteristics that made correction of urine volume to >2 L more likely on the subsequent collection. We compared patient demographics, the presence of LUTS, personal stone history, family history of stone disease, and surgical intervention. A multivariable logistic regression was performed to compare age, sex, body mass index, LUTS, presence of first stone, and recent surgery data between the two groups. All statistical analyses were performed using Stata, version 15 (College Station, TX); p < 0.05 was considered to indicate statistical significance.
Results
Of the 461 patients identified in our kidney stone database, 208 (45.1%) patients met inclusion criteria. When comparing groups, 63.9% (133/208) of patients had LUV (<2 L/day) on initial 24-hour urine collection. Information regarding patient demographics and stone history based on volume status on initial 24-hour urine submission can be found in Table 1. A total of nine patients in each group had a history of inflammatory bowel disease (n = 4), small bowel resection (n = 3), gastric bypass (n = 8), or colon resection (n = 3). There was no statistical difference between groups regarding history of bowel-related diseases (12% vs 6.7%; p = 0.197).
Patient Demographics and Baseline Stone History
Value is calculated across categories “Urine volume <2L/day” vs “Urine volume ≥2L/day” in regard to patient demographics and stone history using a two-sampled t-test or Fisher's exact test for continuous and categorical variables, respectively.
AA = African American; Other = Asian/Pacific Indian and Middle Eastern; SD = standard deviation.
The frequencies of abnormalities that exist on initial 24-hour urine collection were assessed. LUV was the most prevalent 24-hour urine abnormality (133/208, 63.9%). The second most common 24-hour urine abnormality was low urine citrate in female patients (68/109, 62.4%). The third most common 24-hour urine abnormality was elevated supersaturation of uric acid (91/208, 43.8%). Figure 1 demonstrates the prevalence of 24-hour urine abnormalities within our patient population.
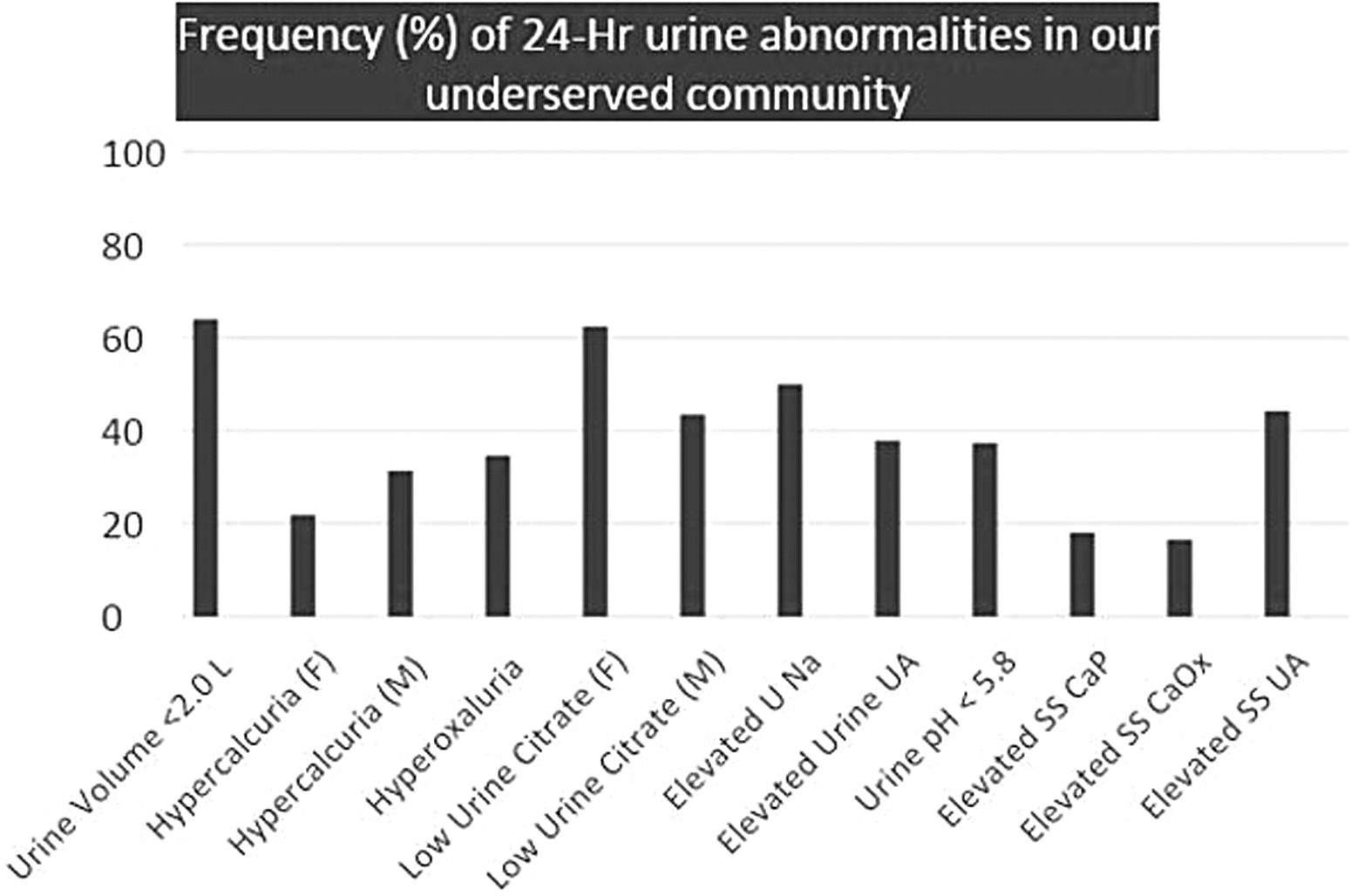
Frequency (%) of 24-hour urine abnormalities in our underserved community. Units: please refer to Table 2 for unit values and definitions for each 24-hour urine variable. F = female; M = male; Na = sodium; SS CaOx = supersaturation calcium oxalate; SS CaP = supersaturation calcium phosphate; SS UA = supersaturation uric acid; UA = uric acid.
On bivariate analysis, female patients were more likely to have LUV on initial 24-hour urine collection compared with men (77.1% vs 49.5%; p = 0.001). Patients with Medicaid were more likely to have LUV when compared with patients with Medicare or private insurance (74.1% vs 58.6%; p = 0.027). When comparing weights (kg) between groups, the LUV group had a lower average body weight compared with the group with urine volume ≥2 L/24 hours (85.1 vs 93.9 kg; p = 0.022).
A multivariate logistic regression was then performed, adjusting for age, sex, type of health insurance, race, weight (kg), personal history of kidney stones, family history of kidney stones, and stone burden. Gender (odds ratio [OR]: 3.11, 95% confidence interval [CI]: 1.61–5.98; p = 0.001) and type of insurance (2.75, 95% CI: 1.31–5.80; p = 0.008) remained independent predictors of LUV on initial 24-hour urine collection.
Parameters across the 24-hour urine analysis were compared between patients with no insurance/Medicaid vs Medicare/private insurance (Table 2). Patients with Medicare/private insurance were found to have a higher 24-hour urine volume (1.82 vs 1.56 L, p = 0.025) and a lower supersaturation of calcium oxalate (6.60 vs 7.58, p = 0.033).
Comparison of 24-Hour Urine Parameters by Insurance Status
SS CaOx = supersaturation calcium oxalate; SS CaP = supersaturation calcium phosphate; SS UA = supersaturation uric acid.
Forty-three patients (43/133 = 33.1%) with LUV on initial 24-hour urine collection also submitted a 6-month follow-up 24-hour urine collection. Seventeen (39.5%) of these patients were able to correct their urine volume on the repeat collection (Table 3). Patients who were able to improve their urine volume were older (58.5 vs 45.8 years; p = 0.0149) and more likely to have undergone recent surgical intervention for their kidney stones (94.1% vs 53.8%; p = 0.006). In our multivariable analysis, undergoing surgery remained an independent predictor of correcting urine volume (OR: 11.69, CI 1.16–118.10; p = 0.037).
Comparison of Characteristics Between Patients Who Were Successful and Unsuccessful in Correcting Their Urine Volume
Previous surgery: ureteroscopy (n = 8), percutaneous nephrolithotomy (n = 4), and SWL (n = 4).
BMI = body mass index; SWL = extracorporeal shockwave lithotripsy.
Discussion
Increasing fluid intake for prevention of kidney stones is a common first-line recommendation in combination with other lifestyle and dietary recommendations. This strategy is well accepted as early studies demonstrated that urine dilution has a protective effect on crystallization of calcium salts. 6 Prospective studies have shown an inverse relationship between fluid intake and relative risk of kidney stones, 7 making it imperative to understand risk factors for LUV. In our patient population, LUV was the most prevalent 24-hour urine abnormality as the urine volume in 63.9% patients did not exceed 2 L on initial 24-hour urine collection. Factors associated with LUV on initial 24-hour urine collection were female gender and having Medicaid for health insurance (Table 1).
In this study, we focused on patient demographics and past stone-related medical history. Disparities in urine volume related to gender have previously been identified. In one retrospective study, 1737 kidney stone formers submitted a single 24-hour urine collection to identify metabolic risk factors for nephrolithiasis. 8 LUV was defined as <15 mL/kg on 24-hour urine collection. The frequency of LUV was higher in women when compared with men, which was statistically significant (20.5% vs 15.5%, p = 0.049). 8 Another retrospective study, which reviewed metabolic risk factors for nephrolithiasis in obesity, also suggested lower urine volumes in women. 9 Although the results were not significant, women had lower mean urine volumes (cc/day) within the obese (1820 vs 2052, p = 0.281) and nonobese (1597 vs 1721, p = 0.534) groups. 9
There are potential explanations for why women can have lower urine volumes on 24-hour urine collection compared with men. LUTS, including stress and urge urinary incontinence, are more common in women compared with men. 10 Furthermore, undercollection on 24-hour urine has been described in women due to their physical and anatomical constraints. 11 Both factors leading to inaccurate quantification of urine volumes on 24-hour urine collection can ultimately lead to patient frustration. Women may feel they drink plenty of water throughout the day, but if not reflected on testing, their doctor may not believe them, potentially straining the doctor–patient relationship.
When looking specifically at patients with adequate 24-hour urine collection based on 24-hour urine creatinine/kg (women: 15–20 mg/kg and men: 20–25 mg/kg), female patients still had a higher frequency of LUV compared with male patients (84.1% vs 50.8%, p < 0.001). This finding suggests that there may be additional factors contributing to LUV in female patients, which are poorly understood.
Socioeconomic factors related to fluid volume on 24-hour urine collection are not well understood. Furthermore, it is difficult to study urine volume on 24-hour urine collection in the underserved community. The most important barrier is access to metabolic testing for patients without insurance. Patients without insurance would have to pay for a 24-hour urine collection out of pocket. Ultimately, this leads to this patient population being underrepresented. Only five patients without health insurance in our cohort submitted a 24-hour urine collection during this study period. All five of these patients had LUV on initial 24-hour urine collection. Two of these patients were able to correct their fluid volume on subsequent 24-hour urine collections. Further study should be focused on this patient population to better understand and appreciate their barriers to fluid intake.
For the purposes of this study, patients were divided into separate groups by insurance: no insurance, Medicaid, and private/Medicare. To qualify for Medicaid, the household income needs to be under a certain threshold, which is why we thought it was appropriate to compare this group with patients with Medicare and private insurance. In our study, patients with no insurance or Medicaid were less likely to reach the 2 L/24-hour mark when compared with patients with Medicare and those who had private insurance (p = 0.027).
We believe that low-income patients and those without insurance would be at higher risk for LUV on 24-hour urine collection as their ability to drink enough fluids throughout the day is limited by financial and lifestyle constraints. These explanations have support as multiple studies have confirmed that Medicaid insurance status is a predictor of food insecurity in regions across the United States. 12,13
Another demographic factor that has been linked to LUV is race. Zisman et al. showed that African American stone formers were more likely to have LUV compared with Caucasian stone formers (1.4 ± 0.8 vs 2.0 ± 0.8 L/day, p < 0.001). 14 A limitation of this finding is that insurance status was not included in the analysis. When controlling for insurance in our study, African Americans, Caucasians, and Hispanics with no insurance or Medicaid had high percentages of LUV (88.2% vs 83.3% vs 71.4%, p = 0.093). When controlling for insurance status and gender in our patient population, female patients were still more likely to have a higher rate of LUV compared with male patients. Specifically, 84.6% of women with no insurance or Medicaid had LUV compared with 62.5% of men (p = 0.045).
Factors that predict improved fluid volume on subsequent 24-hour urine collection have only been investigated in a handful of studies. Khambati et al. evaluated 363 patients who had <2.5 L on their initial urine collection and performed a repeat collection after 6 months. 15 They found that factors associated with improved compliance included male gender (OR: 3.27), percutaneous nephrolithotomy (OR: 3.48), and ureteroscopy (OR: 2.31), and age over 58 (OR: 0.39) and LUTS (OR: 0.50) were associated with decreased compliance. 15 In Khambati's study, elevated age and the presence of LUTS were thought to be deterrents of compliance with fluid recommendations as older patients are more likely to have an overactive bladder and bladder outlet obstruction, as well as other cardiovascular morbidities, which may be exacerbated by fluid intake. 15
Age was one factor associated with fluid volume correction to >2 L on subsequent 24-hour urine collection. Older age has been identified as a predictor for patient compliance specifically with 24-hour urine collection. 16,17 Better compliance with treatment recommendations in our older population could explain the improvement in fluid intake. Patients who were able to improve their urine volume were more likely to have undergone ureteroscopy, percutaneous nephrolithotomy, or extracorporeal shockwave lithotripsy (OR: 11.69, 95% CI: 1.16–118.10; p = 0.037) for their kidney stones. We hypothesize that the morbidity of undergoing surgical intervention may serve as a motivating factor for patients to adhere more closely to dietary recommendations.
There are many limitations to this study. We understand that there are many factors that can contribute to LUV on 24-hour urine collection and these factors extend outside the scope of patient-related factors. Specifically, 24-hour urine collection can often be inadequate based on 24-hour urine creatinine clearance. 11,18 The incidence of undercollection and overcollection based on gender was not quantified for the purposes of this study. Our study was limited by the number of patients as patients typically have poor compliance with providing both initial and subsequent 24-hour urine collections.
Although our study was able to show that the type of health insurance was associated with LUV on 24-hour urine submission, other socioeconomic factors that are poorly understood among underserved medical communities likely contribute to this finding. These factors encompass a wide variety of hardships that exist on a day-to-day basis, which are simply not captured in a patient's medical record. Since our study is retrospective in design, additional limitations include inherent biases that exist within retrospective studies.
Conclusions
In this retrospective review, the type of health insurance and female gender were both independent predictors of LUV on initial 24-hour urine submission. Undergoing surgery was associated with improved 24-hour urine volume in short-term follow-up. Further research is required to explore the barriers to fluid intake, which underserved medical communities face, along with directed patient education on strategies for increasing fluid intake.
Footnotes
Authors' Contributions
An equal contribution of time and efforts was provided by each author involved with this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.