
Abstract
Introduction:
High-power lasers (100–120 W) have widely expanded the available settings for laser lithotripsy and facilitated tailoring of treatment for individual cases. Previous in vitro and in vivo studies have demonstrated that a toxic thermal dose to tissue can result from treatment within a renal calix. The objective of this in vitro study was to compare thermal dose and time with tissue injury threshold when using chilled (CH) irrigation and room temperature (RT) irrigation.
Materials and Methods:
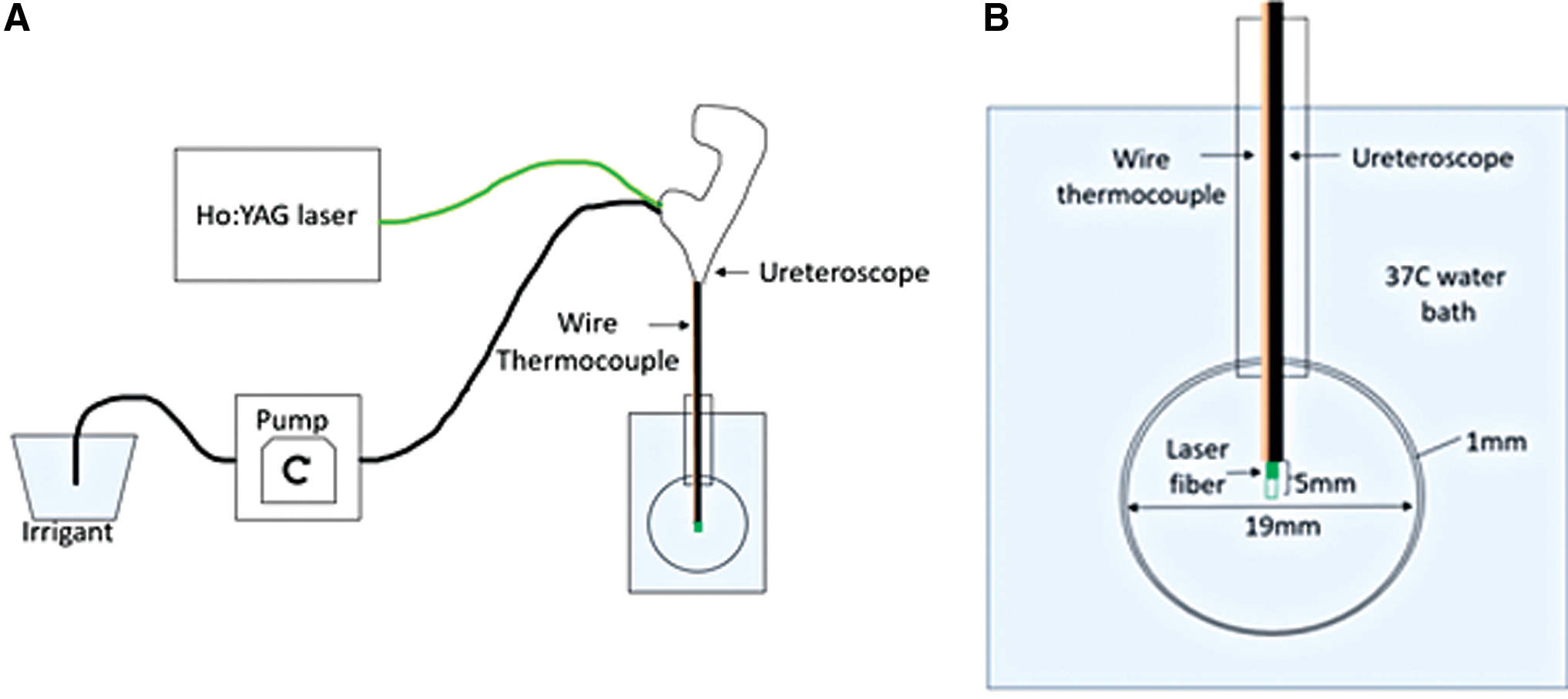
A glass tube attached to a 19 mm diameter bulb simulating a renal calix was placed in a 37°C water bath. A 242 μm laser fiber was passed through a ureteroscope with its tip in the center of the glass bulb. A wire thermocouple was placed 3 mm proximal to the ureteroscope tip to measure caliceal fluid temperature. RT at 19°C or CH at 1°C irrigation was delivered at 0, 8, 12, 15, or 40 mL/minute. The laser was activated at 0.5 J × 80 Hz (40 W) for 60 seconds. Thermal dose was calculated using the Sapareto and Dewey t43 methodology with thermal dose = 120 equivalent minutes considered the threshold for thermal tissue injury.
Results:
At each irrigation rate, CH irrigation produced a lower starting temperature, a lower plateau temperature, and less thermal dose compared with RT irrigation. The threshold of thermal injury was reached after 13 seconds of laser activation without irrigation. With 12 mL/minute irrigation, the threshold was reached in 46 seconds with RT irrigation but was not reached with CH irrigation.
Conclusion:
As higher power laser lithotripsy techniques become further refined, methods to mitigate and control thermal dose are necessary to enhance efficiency. CH irrigation slows temperature rise, decreases plateau temperature, and lowers thermal dose during high-power laser lithotripsy.
Introduction
High-power lasers (100–120
Many in vitro and in vivo studies, as well as computer simulations, have shown that high power equates to greater heating of the fluid within the collecting system. 3 –11 An in vitro study revealed temperatures reaching 60°C after only 10 seconds of laser activation at 40 W power, producing a thermal dose at which tissue damage would occur. 4 These results were validated in an in vivo porcine model where gross pathologic changes consistent with thermal injury were observed after 60 seconds of laser activation in the collecting system. 9
In vitro bench studies have concluded that high irrigation rates can control thermal dose experimentally. 3 –8,12 In many cases, however, these high irrigation rates may only be achievable with placement of an access sheath. An in vivo porcine study found that access sheath use can reduce intrarenal temperatures under certain irrigation conditions. 13 However, even use of an access sheath can result in the undesirable elevation of intrarenal pressure with resultant risks of pyelovenous backflow, infection, sepsis, and organ injury. 14 –17 In many clinical circumstances, placement of an access sheath may not be possible or desirable.
As such, there is value in developing additional techniques for mitigating thermal dose to be used in place of or in conjunction with increased irrigation rates. In this study, we sought to quantify and characterize the magnitude of benefit from using chilled (CH) irrigation during ureteroscopy with laser lithotripsy in a standardized in vitro caliceal model. We hypothesized that the resultant thermal dose would be lower and the time of laser activation to reach the threshold of thermal injury would be increased for CH vs room temperature (RT) irrigation.
Materials and Methods
A cylindrical glass tube (inner diameter 6 mm, length 55 mm) with a glass bulb (19 mm inner diameter) at its distal end simulated a ureter and small renal pelvis or calix (total volume 5.8 mL), respectively, for this experiment. This tube was positioned upright in a water bath maintained at 37°C ± 1°C by an immersion heater (Ulanet, CT) with its opening 1 cm above the water surface. A flexible ureteroscope (LithoVue; Boston Scientific) was introduced into the glass tube through the upper opening and positioned so that its distal end was centered within the glass bulb. A 242 μm laser fiber (Flexiva; Boston Scientific) was then passed through the working channel of the ureteroscope, extending 5 mm beyond its distal tip. A wire thermocouple (Omega, CT) was secured adjacent to the ureteroscope 3 mm proximal to its tip (Fig. 1).
Deionized water irrigation was delivered to the ureteroscope from a peristaltic pump (Masterflex; Cole Parmer, IL) through a 133 cm tube (0.32 cm inner diameter) (Masterflex Tygon tubing; Cole Parmer) to minimize fluid volume in the tubing and reduce warming of the CH irrigant. Needle thermocouples (Physitemp, NJ) were used to record temperature every second within the irrigation reservoir and “body temperature tank.”
The irrigation reservoir was maintained at 19°C ± 1°C RT or 1°C ± 1°C CH. Steady-state bulb temperatures were determined for RT and CH irrigation by delivering the irrigant at each rate for 5 minutes. For laser trials, irrigation was first delivered at the specified rate until the bulb temperature had stabilized and was within 1°C of steady-state temperature. At this point, the 120 W holmium:YAG laser (pulse120; Lumenis, CA) was activated at 0.5 J × 80 Hz (40 W) in short pulse mode for 60 seconds. Three trials were performed for RT irrigation and CH irrigation at irrigation rates of 0, 8, 12, 15, and 40 mL/minute.
The mean and standard deviation of the fluid temperatures were calculated using Microsoft Excel (Redmond, WA) for each set of trials. Thermal dose was then calculated using the Sapareto and Dewey t43 methodology. 18 A thermal dose of 120 equivalent minutes at 43°C was considered the threshold for thermal tissue injury.
Results
Irrigation with CH fluid, 1°C ± 1°C at the source, produced steady-state temperatures in the model calix ranging from 9.9°C ± 0.2°C at 40 mL/minute irrigation rate to 23.6°C ± 0.5°C at 8 mL/minute irrigation (Table 1). Similarly, for RT irrigation that was 19°C ± 1°C at the source, the steady-state temperature in the model calix ranged from 22.7°C ± 0.4°C at 40 mL/minute irrigation rate to 26.9°C ± 0.4°C at 8 mL/minute irrigation (Table 1).
Steady-State Bulb Temperatures After 5 Minutes of Irrigation
CH = chilled; RT = room temperature; SD = standard deviation.
Once the laser was activated, an immediate rise in fluid temperature was noted in all trials. Temperatures reached a maximum of 68.5°C ± 0.3°C without irrigation. For trials using RT irrigation, average peak temperatures were 58.6°C ± 0.4°C, 53.1°C ± 0.4°C, 48.5°C ± 0.2°C, and 32.9°C ± 0.2°C at irrigation rates of 8, 12, 15, and 40 mL/minute, respectively (Fig. 2A). For trials using CH irrigation, maximum temperatures were 56.4°C ± 0.4°C, 48.0°C ± 0.2°C, 43.0°C ± 0.5°C, and 20.7°C ± 0.2°C at irrigation rates of 8, 12, 15, and 40 mL/minute, respectively (Fig. 2B). Increasing irrigation rate resulted in a lower starting temperature and a lower plateau temperature at the end of 1 minute of laser activation. At fixed irrigation rates, CH irrigation produced a lower starting temperature and a lower plateau temperature compared with RT irrigation (Fig. 3).
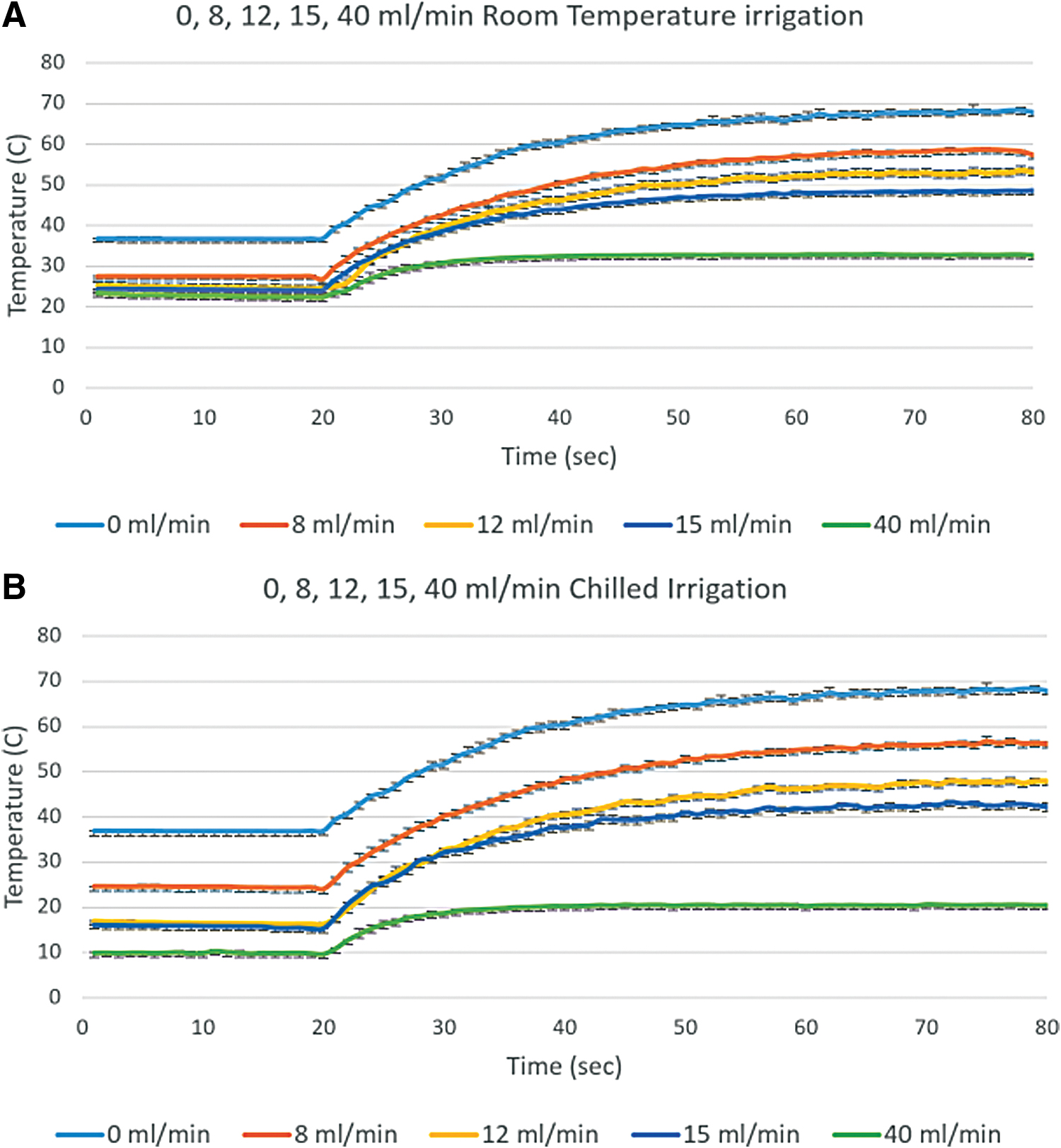
Temperature curves for RT and CH irrigation at various irrigation rates during 1 minute of laser activation (40 W). Error bars represent SD. CH, chilled; RT, room temperature; SD, standard deviation. Color images are available online.

The threshold of thermal injury, defined as t43 = 120 equivalent minutes, was reached after 13 seconds of laser activation without irrigation. With 8 mL/minute irrigation, the threshold was reached in 28 and 33 seconds with RT and CH irrigation, respectively. With 12 mL/minute irrigation, the threshold was reached in 46 seconds with RT irrigation but was not reached with CH irrigation (Table 2). In the absence of irrigation, total thermal dose was 1.53 × 107 equivalent minutes. At 8 mL/minute, thermal dose was 1.48 × 104 and 3.77 × 103 equivalent minutes using RT and CH irrigation, respectively. With 12 mL/minute irrigation, thermal dose was 433 equivalent minutes for RT irrigation. Thermal dose was below the threshold for tissue injury with irrigation rates of 12, 15, and 40 mL/minute using CH irrigation and with rates of 15 and 40 mL/minute using RT irrigation (Table 2).
Time to Thermal Injury and t43 Thermal Dose During 60 Seconds Laser Activation (40 W) Using Room Temperature and Chilled Irrigation at Irrigation Rates of 0, 8, 12, 15, and 40 mL/Minute
Discussion
Results from this study demonstrate that CH irrigation can lower thermal dose and lengthen the time until the threshold of tissue injury is reached during laser lithotripsy, compared with RT or no irrigation. Although this seems intuitive at one level, it has important implications for clinical laser lithotripsy techniques. Currently, there is no guidance from industry, professional groups, or regulatory bodies on selection of safe laser settings and irrigation rates to prevent thermal (and pressure) injury during ureteroscopy. Furthermore, the presence and extent of tissue injury after ureteroscopy is unknown as imaging modalities capable of discerning tissue damage or histologic assessment are rarely if ever performed. To what extent elevated fluid temperatures and pressures during ureteroscopy result in tissue injury and inflammation that could contribute to pain and high emergency department visit/readmission rates after ureteroscopy is an area of active investigation.
Water has a specific heat capacity of 4.18 J/g/°C; in other words, 4.18 J of energy will increase the temperature of 1 mL of water 1°C. When one considers that the volume of a calix may be only 1–2 mL and that the energy delivered with a typical 40 W laser setting is 40 J/second, the importance of irrigation becomes clear. In a perfectly insulated calix of 2 mL volume, 5 seconds of energy delivery without irrigation will elevate the fluid temperature 24°C (from 37°C to 61°C). Under physiologic conditions, vascular perfusion has a heat sink effect, but is quickly overwhelmed by this rate of energy delivery from the laser. 9
Results from this study suggest that RT irrigation is adequate to protect the kidney from thermal injury at rates of 15 mL/minute or greater. However, these rates can be difficult to maintain even with use of an access sheath, without exceeding acceptable intrarenal pressures. Consider the scenario of pop-dusting using 40 W settings in a calix with a narrow infundibulum. With the ureteroscope passed through the infundibulum, resistance to fluid flow from the calix to the renal pelvis will be high resulting in diminished rate of irrigation from bags hung above the patient or producing overpressure of the calix in cases where continuous irrigation pumps are used.
Use of CH irrigation can provide thermal protection in these difficult irrigation scenarios or when low-pressure strategies, such as use of ureteral access sheaths, are not possible or practical. CH irrigation lowers the starting temperature of the fluid within the calix and collecting system, which increases the energy that can be safely applied without reaching threshold of thermal injury. Furthermore, the continuous inflow of lower temperature irrigation blunts the temperature elevation from laser energy deposition.
When considering temperature elevation within biologic systems, it is not adequate to simply define a threshold temperature for tissue injury and cellular death. Thermal tissue injury is dependent on both the degree of temperature elevation and the duration of exposure to elevated temperatures. 18 To standardize this concept for varying time–temperature curves, Dewey and Sapareto developed the concept of t43 equivalence. Using this methodology, any temperature curve can be converted into “equivalent minutes” at 43°C. One minute of exposure to 43°C = 1 equivalent minute, at 44°C = 2 equivalent minutes, at 45°C = 4 equivalent minutes and so forth.
The threshold for tissue injury and cell death ranges between 120 and 240 equivalent minutes for most tissues. 19 In this study, 120 equivalent minutes was used as the thermal injury threshold. Understanding these concepts, one quickly sees that higher temperatures have a disproportionate effect on tissue toxicity. For example, tissue exposed for 1 minute at 49°C experiences a thermal dose of 64 equivalent minutes, whereas 1 minute of exposure to 56°C = 10,192 equivalent minutes. 18
In this study, in the absence of irrigation, 1 minute of laser activation at 40 W resulted in a temperature curve with maximum temperature of 66.9°C ± 0.5°C. Calculation of the thermal dose from this curve was 3.1 × 106 equivalent minutes at 43°C, far beyond the threshold of cell death. By delivering 12 mL/minute RT irrigation, the thermal dose was decreased to 433 equivalent minutes—although still above the threshold for thermal injury. Using 12 mL/minute CH irrigation, the thermal dose was only 11 equivalent minutes—below the threshold for thermal injury.
Considering this concept in another way, it is possible to determine the maximal safe exposure time during a defined temperature curve. In the three trials just described, without irrigation, injury threshold was reached in 13 seconds. With 12 mL/minute RT irrigation, the injury threshold was crossed at 46 seconds and with CH irrigation, this threshold was not reached during the 60 seconds of continuous laser activation. We previously published a framework to determine safe laser parameters across various laser power and RT irrigation rates in a model ureter, renal pelvis, and renal calix. 12 Use of CH rather than RT irrigation will shift these safety boundaries in a favorable direction, and safely allow use of higher laser power settings at any selected irrigation rate.
It is important to realize that the steady-state model calix/bulb temperatures were higher than the irrigation reservoir temperatures. In the case of RT irrigation this is caused by heat diffusion from the 37°C water bath through the wall of the glass bulb. In the case of CH irrigation, there is also a component of heating as the irrigation fluid transits through the 133 cm irrigation tube (capacity 10.5 mL fluid volume) and the working channel of the ureteroscope (1.5 mL fluid volume with laser fiber in place). These effects will hold true in the clinical scenario as well and may be amplified by longer and more capacious irrigation tubing and a greater length of the ureteroscope shaft within the 37°C environment of the patient's body.
Use of CH irrigation with ureteroscopy may raise theoretical concerns for depression of core body temperature, which is associated with increased perioperative complication rates. Avoidance of CH irrigation in procedures such as percutaneous nephrolithotomy (PCNL), where large volumes of irrigation fluid are used is a reasonable approach to minimize this risk. 20 However, fluid volumes used in ureteroscopic procedures are much smaller. For example, at an irrigation rate of 12 mL/minute for a 1-hour operating time, 720 mL of irrigation fluid would be administered. This volume is probably not sufficient to cause systemic body cooling compared with the 14–16 L of irrigation administered during PCNL. 20
This study was performed in vitro and as such several limitations are worth mentioning. A range of clinically applicable irrigation rates were utilized in this study to demonstrate the relationships between irrigation temperature and irrigation rate. However, this is not a complete sampling of the parameter space. Laser activation was standardized to be 40 W power applied for 1 minute. Although this methodology is consistent with previous publications evaluating thermal effects from laser lithotripsy, it is not directly applicable to clinical patterns of laser activation. Thermal diffusion across the glass bulb (model calix) to the 37°C may not accurately replicate the physical characteristics of the tissues of the collecting system.
In light of the results from this research and the limitations noted, additional in vivo studies are planned to validate these findings and better understand the sensitivity of core body temperature to CH irrigation during ureteroscopy. Additional evaluation with warmed irrigation is also planned to more fully sample the clinical parameter space and represent the diversity of clinical practice. Once the safety of a CH irrigation strategy has been validated, irrigation temperature will be incorporated into thermal modeling and predictive models that guide safe selection of laser and irrigation parameters.
Conclusions
As higher power laser lithotripsy techniques become further refined, methods to mitigate and control thermal dose are necessary to further enhance efficiency and patient safety. High irrigation rates have been shown to control thermal dose experimentally but carry risks associated with increased intrarenal pressures. In scenarios where lower pressure strategies such as ureteral access sheath placement are inefficient or not practical, the use of CH irrigation can augment or replace these strategies. CH irrigation slows temperature rise, decreases plateau temperature, and lowers thermal dose during laser lithotripsy while also allowing for lower irrigation rates, making the prevention of thermal injury a multifaceted approach and reducing dependence on high irrigation rates alone.
Footnotes
Authors' Contributions
J.J.D. collected the data. J.J.D. and W.W.R. analyzed the data and wrote the article. T.L.H., A.D.M., K.R.G., and W.W.R. provided critical revisions. W.W.R. conceived and managed the study. All authors reviewed the final article.
Author Disclosure Statement
A.D.M. has equity and consulting relationships with SonoMotion and a consulting relationship with Boston Scientific. K.R.G. has consulting relationships with Boston Scientific, Lumenis, Olympus, and Coloplast. W.W.R. has a consulting relationship with Boston Scientific. J.J.D. and T.L.H. have no disclosures.
Funding Information
Funding for this research was provided through a research grant from Boston Scientific.