
Abstract
Objective:
The aim of this study is to validate the efficacy and reliability of two predictive models for postoperative fever after retrograde intrarenal surgery (RIRS) in pediatric patients
Materials and Methods:
A total of 124 children who were treated with RIRS between August 2014 and August 2020 in our center were included. All the predictors were obtained by preoperative routine examinations. Receiver operative curve (ROC) and area under curve (AUC) were showed to compare the predictive power of the two models.
Results:
One hundred twenty-four children included of 94 boys and 30 girls, with median ages of 2.1 (1.3, 7.0) years and median body mass index of 17.3 (15.6, 20.6) kg/m2. The total points of the two nomograms were 81.0 (67.3, 90.3) and 45.5 (20.4, 94.0). Eventually, 21 children (16.9%) suffered from postoperative fever. With the exception of C-reactive protein values (25.0 mg/L vs 5.0 mg/L, p = 0.015), irrigation volumes (800 mL vs 500 mL, p = 0.01), and total points of the two predictive models (Nomogram 1: 88.0 vs 76.0, p < 0.001; Nomogram 2: 76.0 vs 39.0, p = 0.016), there was no statistical difference detected between the fever and nonfever groups. ROCs showed that Nomogram 1 presented with better predictive accuracy and efficacy with excellent AUC values of 0.805 in comparison with Nomogram 2 (0.805 vs 0.664, p = 0.025).
Conclusion:
We reported a sample of 124 children undergoing RIRS with a final stone-free rate of 87.1%. Twenty-one pediatric patients (16.9%) suffered from postoperative fever. Nomogram 1 presented with better predictive power for postoperative fever after RIRS in pediatric patients.
Introduction
The incidence of pediatric urolithiasis is increasing rapidly in the past decade. 1 With the advances of endourologic techniques and devices, retrograde intrarenal surgery (RIRS) is gradually recognized as an effective and safe procedure, especially for children. 2 However, postoperative infection after RIRS is still a common and intractable complication, which may progress to fever, systemic inflammatory response syndrome (SIRS), or urosepsis. 3 Compared with adults, the progress of postoperative fever and infection may be more dangerous in children due to their developing immunity and poor tolerance. Therefore, timely and effective interventions are more needed for pediatric patients.
Fever (>38°C within postoperative 3 days) is one of the simplest markers to support the evidence of postoperative infectious complications in clinical practice. To resolve these problems, two predictive models (nomograms) consisting of multiple risk factors were developed. 4,5 To the best of our knowledge, there is no one article exploring whether these two nomograms are also suitable to pediatric patients. Thus, we hypothesize that the two models can be applicable to children, and the aim of our study is to investigate and validate the efficacy and accuracy of the two predictive models for postoperative fever after RIRS in children.
Methods
Patients and data
A total of 124 children who were treated with RIRS between August 2014 and August 2020 in Beijing Friendship Hospital were retrospectively included. The included and excluded criteria were as follows: (1) children younger than 14 years; (2) preoperative data and surgical information were available; (3) patients who received bilateral surgeries were ruled out; and (4) informed consents were obtained from their parents. Clinical data including routine blood and urine test, blood biochemistry, urine culture, and CT were collected. Both the models adopted the same multivariable logistic regression method to identify the independent risk factors and construct the nomograms based on regression coefficients. The involved parameters of Nomogram 1 were as follows: surgical duration, urine culture, urine nitrite (NIT), and albumin/globulin ratio (A/G). The associated variables of Nomogram 2 were as follows: the status of diabetes mellitus, surgical time, stone burden, stone culture, and C-reactive protein (CRP). Total points were the sum of all scores corresponding with their variables (Supplementary Table S1). The study was approved by our institutional review board and written informed consents were obtained from their parents.
Retrograde intrarenal surgery
Five French Double-J stents were placed for patients at least 2 weeks before RIRS. All patients were in the lithotomy position under general anesthesia. The usage of 9/11.5F ureteral access sheath (UAS) depended on the age and situation of patients. After removing the ureteral stent and/or placing the UAS, an 8F flexible ureteroscope in combination with 200 μm holmium:yttrium-aluminum-garnet lasers was inserted along the ureter and fragmented the stones. The laser energy was maintained between 0.6 and 0.8 J (power: 18–32 W; frequency: 30–40 Hz). An assisted manually injected irrigation fluid was adopted to maintain the pelvic pressure during the procedure. Finally, a ureteral stent and urethral catheter were placed to keep the continuous drainage. All procedures were limited to be performed within 60 minutes. All patients were administered with third-generation cephalosporins at least 3 days before and after RIRS. For patients with preoperative fever, the procedures were performed after defervescence. Stone-free rate (SFR) was assessed by kidney, ureter, and bladder radiography or ultrasound postoperative day 1 and 1 month. SFR was defined as no residual fragments or less than 4 mm. Postoperative complications were graded according to the Clavien classification system. Temperature >38°C was defined as postoperative fever. All procedures were performed by two surgeons (J.L. and W.-Y.W.).
Statistical analysis
SPSS Version 22.0 and MedCalc Version 19.5 were used for statistical analysis in our study. All continuous variables were presented as median (interquartile distance) due to the non-normal distributions. The indexes between the fever and nonfever groups were compared with Mann–Whitney U test. Chi-square test was performed for categorical variables. Receiver operative curve (ROC) and area under curve (AUC) were shown to compare the predictive potency of the nomograms. p < 0.05 was considered statistically significant.
Results
One hundred twenty-four children included of 94 boys and 30 girls, with median ages of 2.1 (1.3, 7.0) years and median body mass index of 17.3 (15.6, 20.6) kg/m2. Fifty-eight children (46.8%) were accompanied by hydronephrosis. Preoperative fever, positive urine culture, and positive NIT were diagnosed in 17 (13.7%), 38 (30.6%), and 3 (2.4%) patients, respectively. The median CT, CRP and A/G values were 632.0 (450.5, 850.5) HU, 8.0 (4.0, 15.0) mg/L, and 1.6 (1.4, 1.9), respectively. All baseline data are shown in Table 1. Stone characteristics and treatment-related information are given in Table 2. The median cumulative stone diameters, stone burden, surgical duration, and irrigation volumes were 15.0 (10.0, 20.0) mm, 226.9 (133.5, 1067.6) mm2, 30.0 (20.0, 40.0) minutes, and 500 (300, 1000) mL, respectively. For stone complexity, 106 patients (85.5%) were diagnosed with solitary stones and the rest were multiple or staghorn stones. All staghorn stones were partial and between 10 and 20 mm. UAS was used for 48 children (38.7%), and 108 patients were rendered stone free (87.1%). The total points of the two nomograms were 81.0 (67.3, 90.3) and 45.5 (20.4, 94.0). Eventually, 21 children (16.9%) suffered from postoperative fever. With the exception of CRP values (25.0 mg/L vs 5.0 mg/L, p = 0.015), irrigation volumes (800 mL vs 500 mL, p = 0.01), and total points of two predictive models (Nomogram 1: 88.0 vs 76.0, p < 0.001; Nomogram 2: 76.0 vs 39.0, p = 0.016), there was no statistical difference detected between the fever and nonfever groups. ROCs showed that Nomogram 1 presented with better predictive accuracy and efficacy with excellent AUC values of 0.805 in comparison with Nomogram 2 (0.805 vs 0.664, p = 0.025) (Fig. 1).
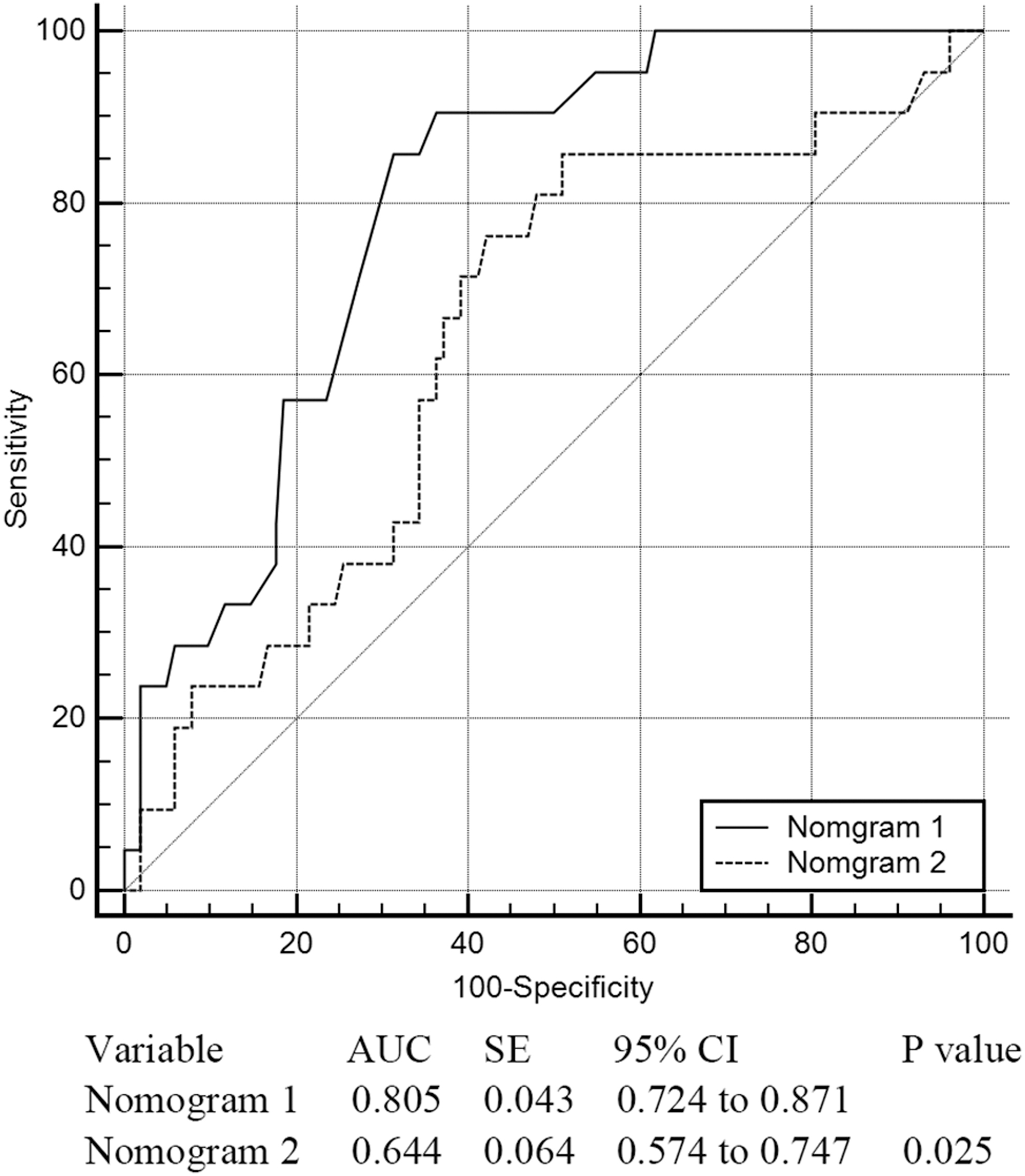
ROC of two predictive nomograms for 124 pediatric patients. AUC = area under curve; CI = confidence interval; ROC = receiver operative curve; SE = standard error.
Baseline Data and Preoperative Examinations of 124 Pediatric Patients
Chi-square test.
Mann–Whitney U test.
A/G = albumin/globulin ratio; BMI = body mass index; CRP = C-reactive protein; NIT = urine nitrite.
Stone Characteristics and Treatment-Related Information of 124 Pediatric Patients
Chi-square test.
Mann–Whitney U test.
SFR = stone-free rate; UAS = ureteral access sheath.
Discussion
Postoperative infectious complications of RIRS have always been a hot issue without being well resolved up to now. At present, in addition to perioperative management, including adequate antibiotic prophylaxis and close observation, evaluation of high-risk factors and prediction of targeted events have been a key part of comprehensive treatment. Li and colleagues 5 designed the first predictive model of postoperative fever and SIRS after RIRS by univariate and multivariate logistic regression (Nomogram 2 in our study), and their model demonstrated an acceptable outcome with a c-statistic of 0.766. Jian and coworkers 4 developed another predictive model (Nomogram 1 in our study) based on the same method and larger sample size, and they showed good agreement between observation and prediction in their model. Pediatric patients are the special population of stone formers, and surgical tolerance and short- or long-term effects on their growth should also be taken into account. In the previous studies, the incidence of postoperative fever after RIRS in children varied from 0% to 18.2%, and most of them could recover under the conservative treatments. 6 –10 However, postoperative infectious complications in children are prone to progress to SIRS or urosepsis. Thus, early prediction and diagnosis of postoperative fever after RIRS contribute to better management. In our study, we reported baseline and surgical information of 124 pediatric renal stone formers, and came to the conclusions that the predictive power of Nomogram 1 was superior to Nomogram 2 for children.
Surgical time and urine culture are both the common parameters in the two models. Similar with their results, Sorokin and colleagues 11 showed that the complication rate after RIRS could increase with prolonged operative time. Ito and coworkers 12 revealed that four independent factors (stone volume, surgical experience, maximum CT values, and preoperative stents) influenced total surgical duration. Sorokin and colleagues 11 reported a simple formula to predict operative time by roughly adding 2 min/100 mm3 increase in volume. In our study, we could not get the statistical significance in terms of stone burden, urine culture, maximum CT values, and the usage of ureteral stents between the fever and nonfever groups, which implied that other potential factors may affect the complications together. In addition, longer operative time reflects larger irrigation volume to flush the optic field and stone fragments. With the increase of irrigation volume, the pressure of collecting system elevates, which leads to the vascular and lymphatic backflow of bacteria and endotoxin, and this is certainly one of the reasons of infectious complications after RIRS. 5,13 In our study, the utilization rate of UAS in nonfever group was higher than the fever group (74.6% vs 23.5%), and UAS was regarded as the key tool to drain continuously and maintain the intrarenal pressure (IRP) without any long-term sequelae, especially for children weighing <20 kg. 8,14 Cai and colleagues 15 demonstrated a latest outcome that postoperative infection after RIRS was not correlated with the spreading of stone-contained bacteria into the irrigation fluid, but the usage of preoperative antibiotic regimens. These results highlighted IRP and bacterial load, both influenced infectious pathogens to enter the blood and cause systemic inflammation reaction.
Stone burden and CRP were also the parameters in Nomogram 2. As discussed above, stone burden was associated with stone clearance, operative time, and irrigation volume. Notably, stone burden was also an independent factor of surgical duration. 11 Thus, the two risk factors did not produce a synergistic effect and improve the predictive accuracy of Nomogram 2, and this might be the reason why Nomogram 2 was inferior to Nomogram 1. CRP is one of the sensitive markers of systemic inflammation reaction and innate immunity. 16 From our results, preoperative CRP values were higher in the fever group in comparison with the nonfever group and a significant difference was also detected between the two groups. A/G ratio and NIT are the remaining two variables of Nomogram 2. A/G represents the liver synthetic function and nutritional and immune status. It was reported that albumin-containing solutions could be applied for the resuscitation of patients with sepsis, and A/G had been confirmed as an independent predictive factor of mortality rate for chronic heart failure, cancer, and other diseases. 17,18 Although a significant difference was not detected between the fever and nonfever groups, the potential predictive value of A/G should be further verified. NIT is one of the routine indexes of urine test and produced by urinary nitrate-metabolizing pathogens, which can instruct the application of preoperative antibiotics. 19 In consideration of the delayed outcome of urine culture, NIT plays a pivotal role in the timely diagnosis of urinary tract infection in children of any age. In our study, positive NIT was relatively low and its practical value could not be embodied. In general, all these routine inflammatory and nutritional indicators should be further confirmed in a prospective randomized trial.
In summary, the role of the two models is to predict the risk rate of postoperative fever (>38°C within postoperative 72 hours) before RIRS in clinical practice. For high-risk patients, to prevent postoperative infectious complications occurring and progressing, perioperative antibiotic administration should be prolonged, and the pressure of irrigation should be limited. This is the first study to investigate preoperative prediction of fever after RIRS in children. Also, our preliminary results show that between the two models, Nomogram 1 may be more applicable for pediatric patients.
There are some limitations in our research. First, it was a retrospective investigation with a small sample size; also, other important factors such as the usage of UAS, irrigation volume, and residual stones were not included in the two models. What is more, the two nomograms were developed based on adults, and a novel predictive model could not be designed due to the small sample size. Finally, our results may not be generalizable at other institutions in consideration of surgical experience for children.
Conclusion
We reported a sample of 124 children undergoing RIRS with the final SFR of 87.1%. Twenty-one pediatric patients (16.9%) suffered from postoperative fever. Nomogram 1 presented with better predictive power for postoperative fever after RIRS in pediatric patients.
Footnotes
Ethical Approval
All procedures performed in the studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Authors' Contributions
All authors contributed to the study design. Material preparation, data collection, and analysis were performed by F.-Z.Z., L.T., C.-M.L., W.-Y.W., and C.N. The first draft of the article was written by F.-Z.Z. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by Beijing Municipal Administration of Hospitals Clinical Medicine Development of special funding support, code: XMLX201826 and Beijing Health Commission, Capital Health Development Research Project, code: 2018-2-1101.
Supplementary Material
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.