
Abstract
Background:
Robot-assisted kidney transplantation (
Materials and Methods:
All consecutive cases performed at our center from April 2016 to March 2020 were reviewed. LC was analyzed by using the cumulative summation method for total anastomosis time (technical outcome) and serum creatinine at days 7 and 30 (functional outcome). Patient safety was assessed by using Shewhart control charts, and a comparison of safety outcomes before and after achieving LC was done by using Chi-square or Fischer exact test as appropriate. A descriptive review of technical modifications made during our experience was conducted.
Results:
Ninety patients underwent robot-assisted renal transplant during the study period. LC was crossed at 24 cases (total anastomosis time) and 15 to 25 cases (serum creatinine). Shewhart control charts showed that total anastomosis time remained below alert/alarm line in 94.4%/98.9% cases, with the alert line being crossed a significantly greater number of times before the LC. Serum creatinine values remained below alert/alarm line in 85.5%/90% cases at day 7 and 92.2%/96.7% cases at day 30, with no difference made due to LC. Key technical modifications included arterial and ureteric spatulation at bench, use of polypropylene 5 to 0 holding stitch in graft vessels to facilitate intraoperative handling, keeping anterior arterial wall smaller to visualize posterior arterial wall anastomosis, and leaving a small amount of fatty tissue on the supero-lateral surface of the kidney for handling after jacket removal.
Conclusion:
Our LC of
Introduction
Robot-assisted kidney transplant (RAKT) is a recent technical advancement in renal transplantation since its inception six decades ago. 1 Undoubtedly, this is a technically challenging procedure involving intra-corporeal vascular anastomosis performed within a restricted timeframe. 2 Moreover, renal transplants in many centers are still being performed by dedicated transplant surgeons, who are not routinely involved in robot-assisted surgeries. This could be a reason why RAKT has still not been widely adopted worldwide. Previous series show that it is easier for surgeons already doing robotic urologic surgery to convert from open renal transplant to RAKT compared with open renal transplant surgeons who are not proficient in robot-assisted surgeries. 3
Learning curve (LC) calculation is helpful in determining when the surgeon becomes proficient in any procedure and the amount of training required to achieve optimum surgical outcomes. In addition, LC calculation is essential as it gives a threshold about the number of cases to be performed under either mentorship or supervision while establishing any new surgical program. Nonetheless, patient safety and functional outcomes are uncompromisable even during LC. This is even more important for a sensitive procedure such as renal transplant, which has an established gold standard in the form of an open technique. Unfortunately, there has been limited reporting of LC for RAKT. All except one of these reports have come from a single working group. 3,4 Further, there is wide variation in reported LC, ranging from 9 to more than 40 cases in different publications. 2,4 Therefore, it is essential to perform an independent analysis of LC and of patient safety, especially before the procedure may be considered generalizable.
Continued performance of any surgical procedure also generates modifications in the established initial procedure, which helps in making it technically sounder, easier to perform, more feasible, and more reproducible. Therefore, we analyzed our prospectively maintained database to calculate LC and detail surgical tips and tricks that we learned during our experience with RAKT over the past 4 years.
Materials and Methods
The study was conducted in a single tertiary care center in India. Our team is highly experienced in open renal transplant, with more than 3500 transplants done till date. We started our RAKT program in April 2016 by using da Vinci Xi® Surgical System (Intuitive Surgicals, Sunnyvale, CA). Since then, perioperative details of all cases are recorded in a prospectively maintained database. All consecutive live donor RAKT cases from April 2016 till March 2020 were included and their data were analyzed. The recipients undergoing second or third renal transplant were not offered RAKT and were, therefore, excluded. There were no other exclusion criteria. At the same time, all open live donor renal transplant data were also prospectively maintained. All RAKT procedures were conducted by a single surgeon, who had reasonable experience in robot-assisted urological procedures and large experience in open renal transplants.
The primary objective was calculation of LC by using cumulative summation (CUSUM) analysis of anastomosis time and recipient serum creatinine at postoperative days 7 and 30. Anastomosis time was defined as time starting from placement of venous clamps till declamping of renal artery and vein (incorporating both venous and arterial anastomosis time). Patient safety during and beyond LC was assessed by using Shewhart control charts for technical and functional outcomes and compared before and after LC, as calculated by CUSUM analysis. The secondary objective of the study was to describe technical tips and tricks learnt from our RAKT experience.
Preoperative data collected included demographic details of the recipients, donor kidney retrieval side and number of vessels, preoperative recipient hemoglobin, and duration of maintenance dialysis. Intraoperative details included assessment of total anastomosis time, use of GelPOINT® (Applied Medicals, Rancho Santa Margarita, CA) or Pfannenstiel incision for kidney insertion, and intraoperative complications. Postoperatively, all recipients underwent daily monitoring of hematological parameters and renal function till discharge and were thereafter monitored twice weekly for 1 month. Later on, monitoring interval was gradually increased. Recipient serum creatinine at days 7 and 30 was used to estimate LC. Thirty-day postoperative complications were noted and graded according to the Clavien–Dindo (CD) scale. In case any patient had more than one complication, the highest applicable CD grade was assigned.
Institutional review board approval was taken for the study. All patients had given written informed consent before their surgery. The study was conducted according to the principles of Helsinki Declaration, 1964 (amended in 2013). All original data reported in the study are available and accessible by the authors.
Statistical analysis
CUSUM analysis was used for the assessment of LC. 5 For CUSUM analysis, a target value is chosen and the difference of observed value for each successive case from the target value is cumulatively added and plotted. The initial LC is said to be overcome when the curve reaches a plateau, suggestive of attainment of target value. With the achievement of continued skill, the observed value may be a better target value, in which case the CUSUM curve shows a downward trend. Since open renal transplant is considered the gold standard technique for renal transplant, we used data from our open renal transplant done at the same timeframe, to set the target values. 6 We used three parameters for the calculation of LC. Technical competence was assessed by using total anastomosis time. This was compared against rewarm ischemia time (reWIT) during open renal transplant, which is equivalent to anastomosis time, as no extra reWIT is spent in open renal transplant for placement of graft kidney. The target value for anastomosis time was set at 45.26 minutes. Functional competence was assessed by using recipient serum creatinine values at days 7 and 30, compared with results of our open transplant series at these time points (1.17 mg/dL at day 7 and 1.19 mg/dL at day 30).
We also assessed technical and functional safety of our procedures performed throughout the study period by using Shewhart control charts for technical (anastomosis time) and functional outcomes (recipient serum creatinine at days 7 and 30). 7,8 For the creation of Shewhart control charts, a target value was defined as above, followed by determination of upper and lower alert (set at ± two times the standard deviation) and alarm (set at ± three times the standard deviation) lines. 4 The target values and alert/alarm lines are detailed in Table 1. Further, after the calculation of LC by using CUSUM analysis, the number of cases crossing the alert/alarm line before and after attainment of LC were compared for analyzing the possible adverse effect of LC on patient safety by using Chi-square or Fischer exact test as appropriate.
Control Line (Mean), Upper Alert Line (Mean +2 Standard Deviation), and Upper Alarm Line (Mean +3 Standard Deviation)
SD = standard deviation.
For the analysis of postoperative complications, the patients were divided into three groups (first 30 cases, middle 30 cases, and last 30 cases) and the number and severity of complications were analyzed among the groups by using Chi-square test. Statistical analysis was done by using STATA version 12.0 (2011).
Results
Baseline characteristics
During the study period, a total of 90 RAKT cases were performed. The baseline characteristics of all recipients are detailed in Table 2. Most grafts had a single renal artery. For grafts with two renal arteries, reconstruction using either Pantaloon technique or end-to-side anastomosis of smaller artery to main renal artery was performed during bench preparation, so that single arterial anastomosis could be done. All recipients had an American Society of Anesthesiologists score of 3. Ten (11.1%) recipients underwent a preemptive renal transplant.
Baseline Recipient Characteristics
ABO = ABO blood groups; BMI = body mass index; CIN = contrast induced nephropathy; CKD = chronic kidney disease; FSGS = focal segmental glomerulosclerosis; GN = glomerulonephritis; Hb = hemoglobin; HD = hemodialysis; MG = membranous glomerulopathy; MPGN = membranoproliferative glomerulonephritis; SLE = systemic lupus erythematosis.
Calculation of LC and patient safety monitoring
CUSUM analysis of total anastomosis time showed attainment of initial LC at 24 cases (Fig. 1). For recipient serum creatinine at day 7, the LC was overcome at 25 cases and the same was achieved at 15 cases for serum creatinine at day 30, suggestive of an LC of 15 to 25 cases for adequate functional outcome (Fig. 1).

CUSUM analysis graphs of—
Using Shewhart control charts, we found that the anastomosis time was below the upper alert/alarm line in 94.4%/98.9% cases (Fig. 2). A significantly higher number of cases crossed the alert line before the LC at 24 cases compared with the post-LC cohort (16.7% vs 1.5%, Fischer exact p-value 0.0169). There was no difference in the proportion of cases crossing the alarm line before and after the LC. Recipient serum creatinine at day 7 remained below the upper alert/alarm line in 85.5%/90% cases, with no difference before and after the LC cutoff in 25 cases (Fig. 2). Recipient serum creatinine at day 30 was found to be below the upper alert/alarm line in 92.2%/96.7% cases, with no difference before and after the LC in 15 cases (Fig. 2).
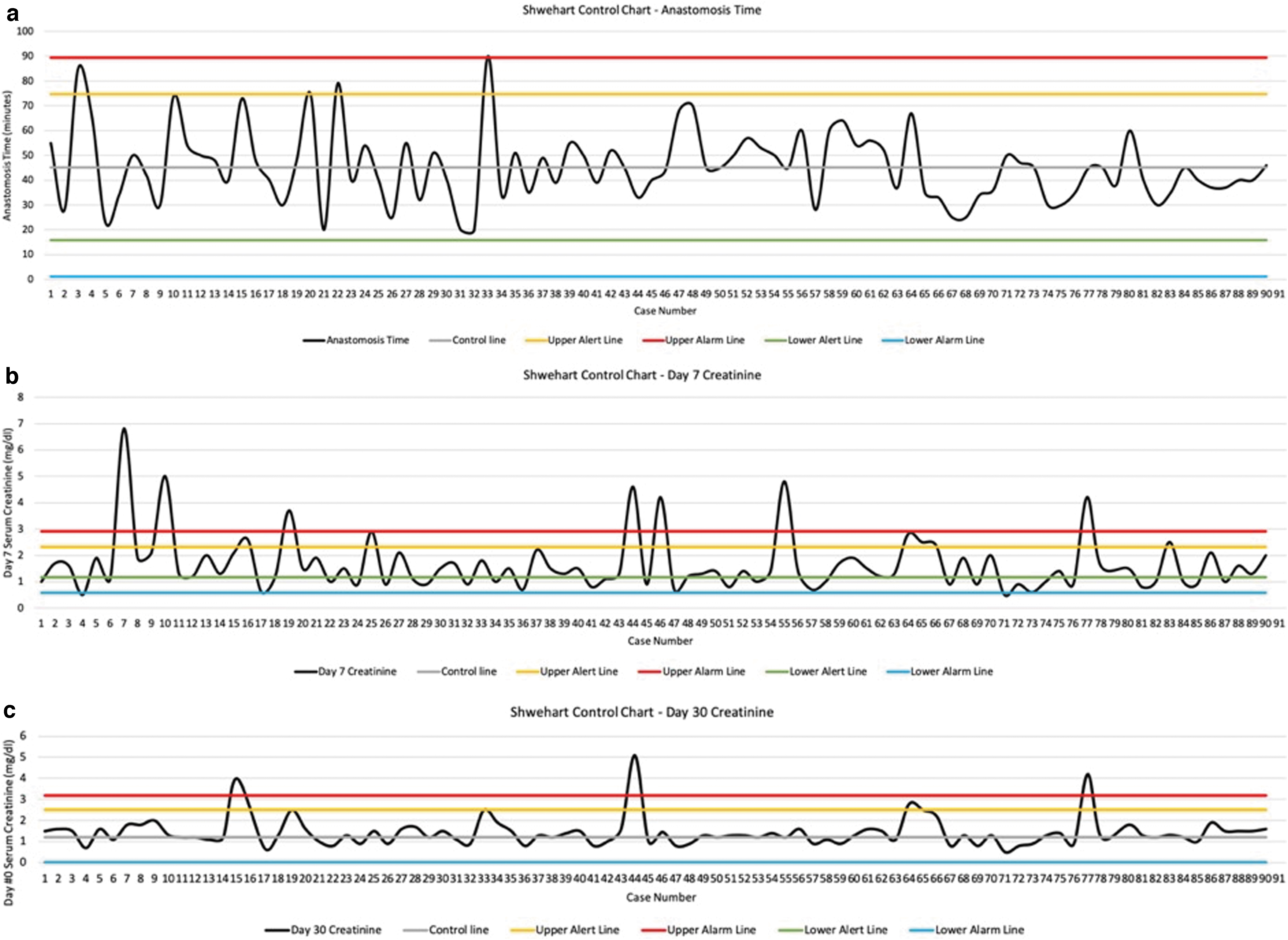
Shewhart control charts of—
Surgical tips and tricks
We adapted the Vattikuti Urology Institute-Medanta technique of RAKT with regional hypothermia. 9,10 However, during our experience, we incorporated several technical modifications to improve intra-corporeal renal, vascular, and ureteric handling. Apart from technical modifications resulting from the ongoing RAKT experience of the operative surgeon, some lessons were also learnt due to intraoperative complications (Table 3; Fig. 3).

Technical modifications in the surgical technique of robot-assisted renal transplant—
Problems and Learnings from Our Experience with Robot-Assisted Kidney Transplant
OKT = open kidney transplant; RAKT = robot assisted kidney transplant.
Intra- and postoperative complications
The intra- and postoperative complications are detailed in Table 4. The complication rates compared among first, middle, and last 30 cases (Table 4) were not significantly different. However, there were two patients with CD grade 4b complication and one mortality (CD grade 5) in the first 30 cases, whereas there were none in the middle and last 30 cases.
Description of Intra- and Postoperative Complications and Comparison of Complications Graded According to the Clavien–Dindo Scale Among First, Middle, and Last 30 Cases
Discussion
RAKT is the latest technical innovation in renal transplantation. However, its significance lags behind other advancements such as modern immunosuppression, laparoscopic donor nephrectomy, and use of expanded criteria donors including non-heart-beating donors. Compared with open renal transplant, RAKT has shown similar, non-inferior short-term graft outcomes in published research. 6,11 However, with increasing surgical experience and improvement in graft outcomes, RAKT is likely to be more widely adopted in future due to decreased wound complications, earlier postoperative recovery, and improved cosmetic results. Its minimally invasive nature is more appealing in females, obese recipients, and children. Knowledge of LC of any new procedure guides the surgeon and helps in self-assessment and improvement in patient outcomes. Therefore, deducing LC assumes center stage before initiating the RAKT program.
The LC analysis may be performed by various methods, such as CUSUM analysis, calculation of moving average, multimode LC, Cartesian method, and mean operative time of every few consecutive cases. 12 We chose to conduct CUSUM analysis for calculation of LC as this is one of the most widely used methods, 13 and it has been performed in the few published series on RAKT LC, which makes our results comparable to published literature.
We found that our initial LC for performing vascular anastomosis was completed after 24 cases. Compared with LC of the pioneer group in current RAKT technique, our result suggests a more modest case number needed to achieve LC. 4 We believe that this is more representative of a real-world scenario, especially for independent transplant centers looking to initiate the RAKT program. We used total anastomosis time as an assessment variable, as this was likely to have a direct impact on total renal reWIT. We could not analyze the time required for kidney insertion for calculation of LC, as we used either GelPOINT or Pfannensteil insertion for the same, depending on patient body habitus; this variation in insertion time (∼5 minutes in GelPOINT and 10 minutes in Pfannensteil incision) was due to the use of differing techniques that precluded the use of this parameter for the calculation of LC. Calculation of ureteroneocystostomy time for calculation of LC was not considered, as the operating surgeon was already reasonably experienced in doing robot-assisted urological procedures, including ureteroneocystostomies, and the duration of this step does not directly affect kidney function.
Although the reference for anastomotic time was taken as reWIT in open renal transplant, during both anastomosis and RAKT, some additional time is spent for rearranging vascular clamps after venous anastomosis and application of Bulldog clamps over external iliac artery. This leads to an increase in total anastomotic time during RAKT. Thus, anastomosis time of RAKT may not exactly match open surgery even after completion of LC.
We found similar results for the calculation of LC by using anastomosis time and serum creatinine at day 7. LC as calculated by recipient serum creatinine at day 30 was achieved earlier. This is logical, as serum creatinine at day 7 is more likely to reflect the influence of surgical parameters as compared with day 30 creatinine values, which may be confounded by medical complications such as rejection, infection, and calcineurin inhibitor toxicity.
Our Shewhart control charts showed that our technical and functional outcomes remained in control limits in the majority of cases, similar to what has been reported in published literature. 2 We found that anastomosis time exceeded upper alert limit in a significantly higher proportion of cases before LC. However, this did not adversely affect renal functional outcomes. This is reassuring for surgeons starting the RAKT program, as functional outcomes are unlikely to be adversely affected even if anastomosis time may be exceeded in a few cases during LC. 14 Our anastomosis time remained within alarm line in all but one case (90 minutes). That patient was discharged on day 7 with a serum creatinine level of 1.8 mg/dL (below upper alert line).
We made several modifications in our initial surgical technique during our RAKT program. A few other modifications have similarly been suggested by other authors recently as well, which suggests a rational evolution of any surgical technique. 2,15,16 One case developed subcapsular hematoma due to trauma during kidney placement in iliac fossa and had to be re-explored laparoscopically to drain it by capsulotomy. We found that leaving a small amount of perinephric fat on the lateral and upper aspect of the kidney was very helpful in atraumatically manipulating the kidney to the extraperitoneal pocket after removal of the ice jacket. Similarly, the use of Prolene® loop on each graft vessel helps in vessel manipulation without risk of intimal injury. Ureteric orientation was confusing initially if the kidney was not making urine immediately. So, we started ureteric spatulation on a bench; this made orientation easier during ureteroneocystostomy. We consider Pfannensteil incision for graft insertion more cost-effective and cosmetically better than the use of GelPOINT system. As assessed from functional Shewhart control charts, addition of a few minutes to close Pfannensteil incision does not adversely affect graft outcome.
Due to its retrospective nature, there are inherent limitations in our study. Our surgical technique continuously evolved during LC by incorporating modifications as detailed earlier, which might, in itself, have affected the LC. We could not control for case complexity and demographic features, which might have had an impact on our LC. The experience of the operative surgeon with robot-assisted surgery and open renal transplant helped in overcoming LC in our series after a modest number of cases. In such cases, the surgeon may be considered as a pre-trained novice. The LC may be longer for novice surgeons (not well versed with robotic surgery) and shorter for expert surgeons (having done robotic surgery and a few RAKT as well). Establishment of a new surgical program in the presence of a proctor may further smoothen the LC. Low LC will stimulate other surgeons to venture into such programs.
Conclusion
We provides an independent analysis of LC of RAKT and found that LC is crossed in 24 cases (technical outcome) and 15 to 25 cases (functional outcome). We also detail many technical modifications. These are helpful to urologists and transplant surgeons who are planning to initiate an RAKT program at their center.
Footnotes
Authors' Contributions
D.B.: study design, data collection, article preparation, and literature search. S.C., R.M., and A.B.: study design, data collection, and article editing. A.K.: study design, data collection, article editing, and review.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.