
Abstract
Background:
Relative value units (RVUs) are the measure of value used in US Medicare reimbursement. Medicare determines physician work RVUs (wRVUs) from the Relative Value Update Committee (RUC) for a procedure based on operative time, technical skill and effort, mental effort and judgment, and stress. In theory, work RVUs should account for the complexity and operative time involved in a procedure. The aim of this study was to assess whether major procedures for treatment of benign prostatic enlargement (BPE) are fairly compensated based on complexity and operative time in the RVU system and compare them with the intended reimbursement.
Methods:
The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database and the Centers for Medicare and Medicaid Services (CMS) Medicare Physician Fee Schedule were queried from 2015 to 2017. Single, current, procedural terminology codes associated with BPE treatments were included: transurethral resection of the prostate (TURP), photovaporization of the prostate (PVP), holmium laser enucleation of the prostate (HoLEP), retropubic simple prostatectomy (RSP), and suprapubic simple prostatectomy (SSP). The CMS operative times and the NSQIP real data were used in turn to calculate separate values for wRVUs per hour (wRVUs/hr) of operative time. The wRVUs/hr derived from CMS operative times represent RUC-estimated wRVUs/hr and wRVUs/hr derived from NSQIP represent actual wRVUs/hr.
Results:
A total of 27,664 cases were included from the NSQIP dataset. Median wRVU was 15.3 (interquartile range [IQR] 12.2–15.3), median operative time 50 minutes (IQR 33–74), and median wRVUs/hr 17.0 (IQR 11.6–26.2). RUC-estimated wRVUs/hr were TURP 12.2, PVP 12.2, RSP 9, SSP 9.3, and HoLEP 7.3. The actual wRVUs/hr were TURP 19.1, PVP 15.5, RSP 10.2, HoLEP 9.4, and SSP 7.6.
Conclusions:
Laser enucleation and simple prostatectomy are highly complex and efficacious procedures for treating BPE, yet the current payment schedule assigns these procedures the least amount of wRVUs/hr. Financial incentives for performing BPE surgeries are clearly misaligned.
Introduction
Multiple payment models currently determine physician reimbursement in the United States. Although alternative strategies such as bundled payments and capitation are gaining momentum, fee-for-service remains the most dominant payment, accounting for the majority of private and public spending on physician services. 1 The resource-based relative value scale is the system by which the Centers for Medicare and Medicaid Services (CMS) reimburses physicians, and physician work relative value units (wRVUs) comprise the largest component of this value scale. 2,3 The Relative Value Update Committee (RUC) responsible for updating wRVUs for surgical procedures considers several parameters in determining these values, including operative time, technical skill and effort, mental effort and judgment, and intensity. 4 –6
However, often these wRVUs do not accurately reflect objective measures of these parameters and this has been shown to be true across multiple specialties, including urology. 7 –9
Procedures for benign prostatic enlargement (BPE) are among the most commonly performed by practicing urologists. The primary aim of this study was to assess whether operative time and complexity are adequately accounted for by the current wRVU assignments for BPE procedures and compare these values with the reimbursement as intended by the RUC.
Methods
NSQIP data set
The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database was reviewed from 2015 to 2017. NSQIP is a validated, outcome-based clinical registry of postoperative complications for patients who undergo surgery at over 700 participating hospitals. NSQIP collects data on a representative sample of patients undergoing major surgery at member hospitals. Highly trained abstractors collect patient demographics, preoperative risk factors, surgical variables, and morbidity and mortality rates. The reproducibility of this data abstraction is periodically checked by repeat abstraction of a sample. The operative time utilized from this data set was the median intraoperative time per current procedural terminology (CPT) code, which does not include perioperative or anesthesia time. The NSQIP intraoperative time is directly measured in the operating room and will be referred to as the actual operative time.
CMS Medicare Physician Fee Schedule data set
The CMS Medicare Physician Fee Schedule, reviewed from 2015 to 2017, 10 is an annually released data set that includes the official median intraservice time. In the case of surgical procedures, this is explicitly meant to represent skin-to-skin or scope-in-scope-out operative time, excluding perioperative or anesthesia time. The median intraservice time is derived from RUC recommendations that are based on survey-generated operative time estimates. Thus, the CMS intraservice time will be referred to as the RUC-estimated operative time.
Study population
This study is exempt by the local Institutional Review Board. The consort diagram is shown in Figure 1. Procedures coded using the CPT codes for transurethral resection of the prostate (TURP), laser ablation of the prostate photovaporization of the prostate (PVP), holmium laser enucleation of the prostate (HoLEP), and simple prostatectomy (suprapubic and retropubic) were included in the analysis (CPT 52601, 52648, 52649, 55821, and 55831). Of note, the CPT code for HoLEP, 52649, also includes other modalities of laser such as thulium enucleation of prostate. We excluded procedures that were missing data on operative time, or wRVUs, or were coded with multiple CPT codes. We excluded cases with operative times of <10 minutes or >600 minutes as these were likely major outliers or miscoded entries.
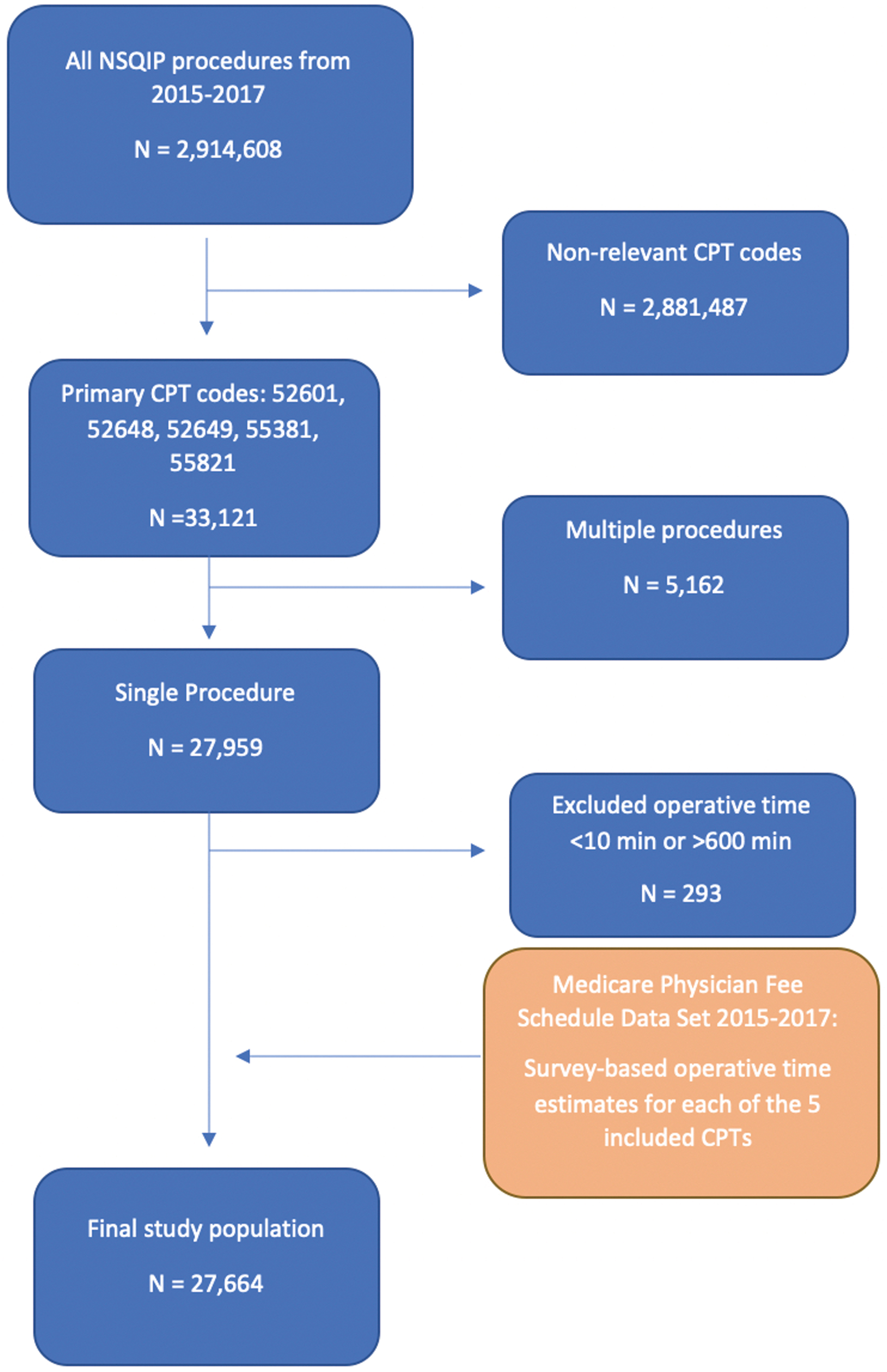
Consort diagram for the NSQIP data set. We identified 33,121 relevant CPT codes (52601, 52648, 52649, 55381, and 55821). After applying the exclusion criteria, we identified 27,664 for our final study population. This was compared with the Medicare Physician Fee Schedule data. CPT = current procedural terminology; NSQIP = National Surgical Quality Improvement Program. Color images are available online.
Statistical analyses
The primary outcome was wRVUs per hour (wRVUs/hr) of operative time. wRVUs/hr were determined for the included procedures using both the actual (from NSQIP) and RUC-estimated operative times (from CMS-estimated median intraservice time) and will be referred to as the actual wRVUs/hr and RUC-estimated wRVUs/hr. Analysis of variance was used to determine statistically significant differences in wRVUs/hr between the five different procedures.
Statistical significance for all analyses was defined as a two-tailed alpha risk of 0.01 or less. Statistical analysis was performed using Stata (version 16.1; StataCorp, College Station, TX).
Results
After applying the inclusion and exclusion criteria, 27,664 cases were obtained from NSQIP for analysis. Median total wRVU was 15.3 (interquartile range [IQR] 12.2–15.3), median actual operative time 48 minutes (IQR 47–48), and median actual wRVUs/hr 19.1 (IQR 15.5–19.1). Values from the highest to the lowest actual wRVUs/hr were TURP 19.1, PVP 15.5, retropubic simple prostatectomy (RSP) 10.2, HoLEP 9.4, and suprapubic simple prostatectomy (SSP) 7.6. These wRVUs/hr were statistically significantly different (p < 0.01) on analysis of variance. These results are shown in Table 1.
Benign Prostatic Enlargement Operations Ranked by Work Relative Value Units per Hour
wRVUs/hr are statistically significantly different on ANOVA (p < 0.01).
ANOVA = analysis of variance; CPT = current procedural terminology; IQR = interquartile range; NSQIP = National Surgical Quality Improvement Program; RUC = Relative Value Update Committee; TURP = transurethral resection of the prostate; wRVU = work relative value unit; wRVUs/hr = work RVUs per hour.
Data from the CMS Medicare Physician Fee Schedule as well as NSQIP confirmed total assigned wRVUs to be 15.26 for TURP, 12.15 for PVP, 14.56 for HoLEP, 15.76 for SSP, and 17.19 for RSP. Global periods were equivalent at 90 days. The median intraservice times for the five procedures did not change during the study period and are displayed in Table 1. RUC-estimated wRVUs/hr were highest for TURP and PVP and lowest for HoLEP (TURP 12.2 RVUs/hr, PVP 12.2 RVUs/hr, RSP 9 RVUs/hr, SSP 9.3 RVUs/hr, and HoLEP 7.3 RVUs/hr). The RUC-estimated operative times for TURP and HoLEP were overestimated when compared with NSQIP data and underestimated for SSP. The discrepancy between RUC-estimated and actual wRVUs/hr was largest for TURP and smallest for RSP (Fig. 2).
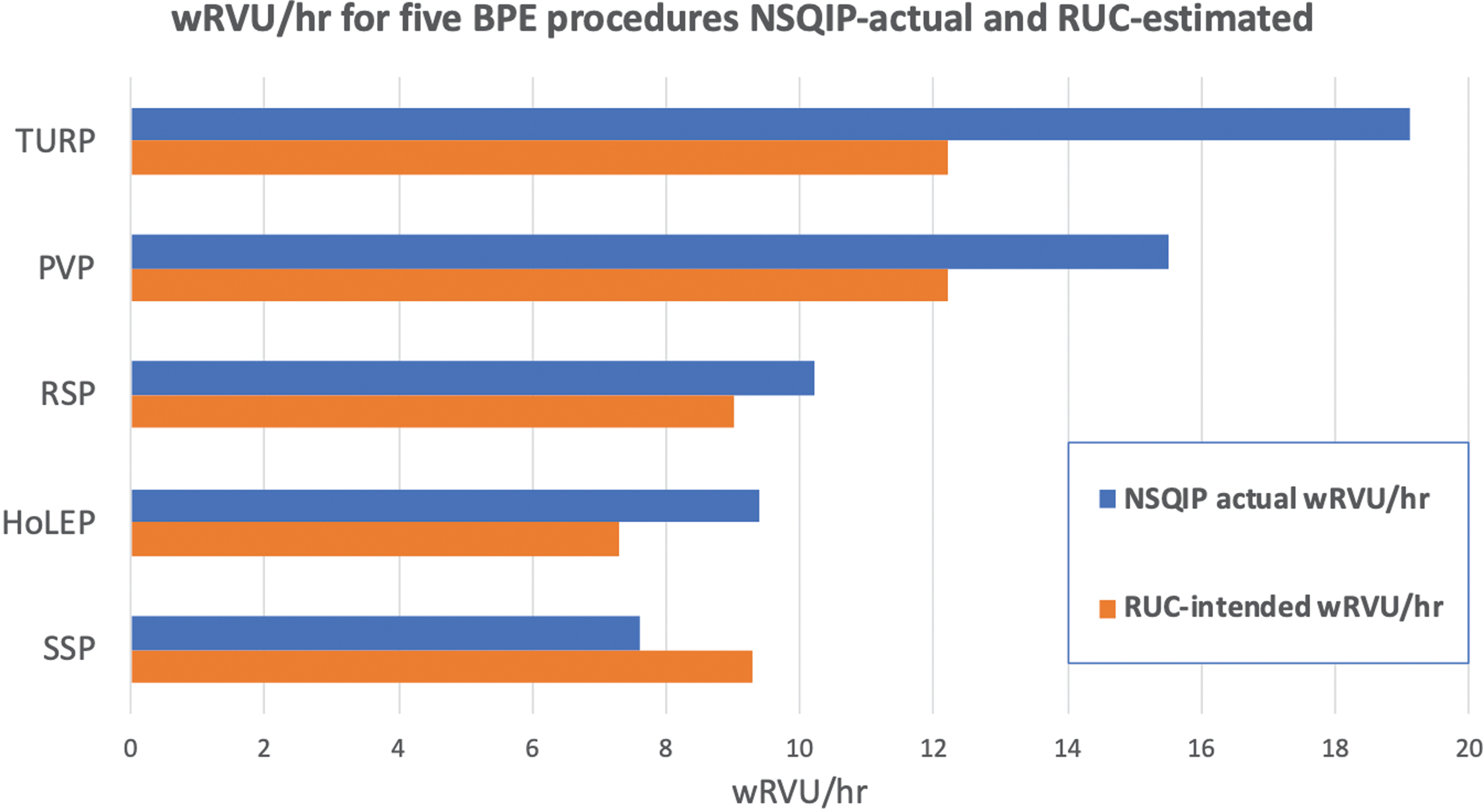
wRVUs/hr for the five different BPE procedures analyzed. The top blue line shows the NSQIP actual wRVUs/hr, and the RUC-estimated wRVUs/hr are shown in orange below. BPE = benign prostatic enlargement; HoLEP = holmium laser enucleation of the prostate; PVP = photovaporization of the prostate; RSP = retropubic simple prostatectomy; RUC = Relative Value Update Committee; SSP = suprapubic simple prostatectomy; TURP = transurethral resection of the prostate; wRVUs/hr = work relative value units per hour. Color images are available online.
Discussion
Surgical therapies for BPE are among the most commonly performed procedures in urology, and the procedures discussed herein are the most frequently performed procedures for BPE. RUC determines wRVUs for each procedure based on four indices: operative time, technical skill and effort, mental effort and judgment, and intensity. 4 –6 We compared the reimbursement rates, measured by wRVUs/hr, from actual cases from the NSQIP database with RUC estimates. Our analysis reveals substantially higher wRVUs/hr for TURP and PVP compared with laser enucleation (i.e., holmium or thulium) and simple prostatectomy using both actual and RUC-estimated operative times.
The unit, wRVUs/hr, adjusts for the discrepancy in operative times and therefore should reflect the remaining components of wRVUs; namely, technical skill, mental and physical effort, physician judgment, and stress. However, available data do not support the assertion that TURP is over twice as effortful or stressful as HoLEP or SSP or requires significantly more skill. In fact, HoLEP has a well-described, lengthy learning curve due to significant technical challenges, leading many centers to abandon the technique. 11,12 By comparison, TURP is one of the most commonly performed urologic procedures, for which almost every urologist has received extensive training during residency.
These results highlight obviously misaligned incentives in surgical BPE treatment. Although the outcomes for HoLEP appear to be superior to TURP for patients with large prostates, the reimbursement schedule does not reward physicians who have undergone the additional training required to become proficient in this procedure. Randomized controlled trials (RCTs) comparing HoLEP with TURP have shown HoLEP to be associated with shorter hospital stay, shorter catheter time, increased amount of prostate tissue removed, and superior 6-month urodynamic outcomes, with equivalent 24-month urodynamic outcomes. 13
RCTs comparing HoLEP with SSP have shown equivalent improvement in AUA symptom scores, with less blood loss, shorter hospitalization, and shorter catheter time for HoLEP. 14 Additionally, HoLEP has been shown to be associated with decreased overall complications and cost than TURP. 15,16 When HoLEP is not an option, the financial incentive is misplaced for urologists to perform TURP over simple prostatectomy. The actual operative times suggest that on average, two TURPs can be performed in less time than it takes to perform one SSP, with these procedures earning very similar total wRVUs.
The RUC-estimated operative times for BPE procedures in this analysis differed from NSQIP operative times; however, despite the difference in operative times, the RUC-estimated wRVUs/hr were no more equitable than the actual wRVUs/hr. The intended reimbursement for HoLEP was only 7.3 wRVUs/hr compared with 12.2 wRVUs/hr for TURP and PVP. Simple prostatectomy was only intended to be reimbursed at ∼9 wRVUs/hr. Although the RUC-estimated operative times are inaccurate, the root cause for the poor reimbursement of simple prostatectomy needs to be addressed with a reevaluation of wRVU assignment.
BPE is estimated to affect almost 70% of US men between the ages of 60 and 69 and nearly 80% of men aged >70 years. 17 It is unsurprising that many companies invest capital to gain a share of the BPE treatment market. Novel therapies are rapidly emerging. Therapies such as Aquablation, UroLift, and Rezum are unfortunately not well captured in the NSQIP and could not be studied in our analysis. CMS has, however, assigned wRVUs for UroLift (CPT 52441 and 52442) at 4.0 wRVUs for the first implant and 1.0 wRVU for every additional implant. The estimated intraservice time for UroLift is 25 minutes for the first implant and 15 minutes for each subsequent implant. 10 Even under the assumption that these time estimates are accurate, if one were to only place two UroLift implants, the RUC-estimated reimbursement is 7.5 wRVUs/hr, which is still more than HoLEP at 7.3 wRVUs/hr.
Rezum (CPT 53854) is reimbursed at 5.93 wRVUs with an estimated intraservice time of 25 minutes, 10 which comes to an RUC-estimated reimbursement rate of 14.2 wRVUs/hr, almost double the rate of reimbursement for HoLEP. These newer modalities are promising with decreased sexual side effects and may even be performed in the outpatient setting, but long-term outcomes are not as robust. 18 Aquablation does not currently have a wRVU reimbursement assignment yet.
With the current wRVU assignments and novel BPE treatments, there is very little incentive encouraging physicians to adopt HoLEP or simple prostatectomy into their practice despite being the most durable treatment for BPE. The reason for poor adoption is widely believed to be a steep learning curve. 19,20 However, we argue that if the reimbursement for HoLEP is increased to an appropriate level, urologists will naturally learn it. Urologists have overcome steep learning curves to widely adopt any number of novel procedures, including various robotic and laparoscopic surgeries and laser TURP. These procedures were readily adopted, despite their learning curves, because wRVU assignments adequately incentivized clinicians to put in the effort to adopt them.
The RUC is responsible for updating wRVUs and it comprises 31 volunteer physicians, most of whom have been appointed by a major physician specialty society. 21 The remainder of the seats are designated for the RUC chairperson, at least 1 primary care representative, a representative from the American Medical Association, and additional seats for various health policy committee representatives. Congress mandates CMS to review the RVUs no less than every 5 years and it is also responsible to develop RVUs for new services. Outside of the 5-year reviews, CMS may examine the RVUs for services that it or physician specialty societies identify as being misvalued and possibly needing modification. 21 For services selected for review, relevant specialty societies field surveys of their members to gather data on physician time and effort and the practice expenses required to provide the service. The RUC reviews these data and makes comparisons with similar services to develop its recommendations, and CMS reviews the RUC recommendations and the underlying data.
There are limitations to this analysis. CMS median intraservice time was used to obtain a direct comparison with the NSQIP operative time; however, we did not include other times estimated by CMS—pre-evaluation time, prepositioning time, preservice scrub dress wait time, and immediate postservice time—in reimbursement calculations. These additional times are not recorded in the NSQIP data set. Procedures coded with concurrent CPTs were excluded to create a less heterogeneous data set for statistical analysis; however, majority of procedures for BPE are likely single procedures.
Our analysis cannot separate simple prostatectomy by approach: robot assisted vs open. NSQIP does not capture BPE-specific factors, such as gland size and symptom score, which are critical factors in determining treatment modality. Additionally, NSQIP collects data on a selection of procedures and does not track every procedure performed by participating hospitals, resulting in a distribution of procedures in the database that may not reflect the actual distribution of procedures nationally. Finally, the available data in NSQIP are not adequate for a direct objective assessment of the other inputs used in formulating wRVUs, such as technical skill, mental effort, and stress.
Conclusions
Laser enucleation of the prostate and simple prostatectomy are more challenging and efficacious procedures for BPE, yet these procedures are significantly undervalued by wRVU reimbursement. This effect persisted with both actual and RUC-estimated wRVUs/hr metrics. wRVU assignments for laser enucleation of the prostate and simple prostatectomy should be raised to an appropriate level that reflects their level of complexity.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.