
Abstract
Objective:
To evaluate the knowledge and current radiation safety practice among health care professionals undertaking fluoroscopic procedures in urology.
Materials and Methods:
A 14-question survey was disseminated to multidisciplinary urology theater staff. Questions included demographic data, usual radiation safety practice, and knowledge. The questions were selected based on guidelines from the International Commission of Radiological Protection and Health and Safety Executive. The survey was disseminated through regional collaborators and social media.
Results:
The survey received a total of 309 completed responses, including 272 from the United Kingdom. Responses from the United Kingdom multidisciplinary team included 164 (60.3%) urologic surgeons, 68 (25.0%) theater nurses, 27 (9.9%) from the anesthetic team, and 13 (4.7%) radiographers. Results from the United Kingdom demonstrated use of lead aprons and thyroid shields as 99.3% and 52.2%, respectively. Lead glasses and lead glove use were 7.4% and 0.7%, respectively. Lack of availability was cited as a reason for noncompliance with shielding guidelines in 208 (76.5%) of the respondents. No form of training in radiation safety was reported by 120 (44.1%) respondents. However, there was no association between answering knowledge questions correctly and having completed some form of radiation safety training (p = 0.41). There was an association between dosimeter use and those who had received radiation safety training (p = 0.02). Consultant urologists were also more likely to use a dosimeter than training grade urologists (p = 0.035).
Conclusion:
Suboptimal compliance with radiation safety guidelines is prevalent in contemporary urologic practice, and presents a significant occupational health concern. Availability of protective equipment needs to be urgently addressed.
Introduction
The rising prevalence of stone disease has led to an increase in the number of endourologic interventions performed. 1,2 Interaction of radiation with the patient's body during shockwave lithotripsy, ureteroscopy, and percutaneous nephrolithotomy (PCNL) produces scatter, which poses an occupational health hazard for all urology theater staff.
Radiation exposure can cause serious short- and long-term effects on health, including solid organ and hematologic malignancy. There is a linear relationship between ionizing radiation exposure and development of solid cancers in humans. 3 However, stochastic effects occurring by chance and without a threshold dose also occur. This results in genetic defects and posing cancer risk at even low exposure levels and may take decades to manifest. 4
Studies by Lee et al. and Zielinski and coworkers showed that medical workers exposed to low-dose radiation have an increased lifetime risk of bladder and thyroid cancers. 5,6 Despite some studies showing that urologic procedures do not exceed the maximum recommended radiation exposure limit, there is no data to show that the lifetime attributable risk from cumulative low-dose exposure is negligible. 7,8
Guidelines from the International Commission of Radiological Protection (ICRP) recommend a maximum exposure limit of 20 mSv per year to limit occupational risk. Specific dose limitations for lens of eyes, thyroid, and limbs are also reported. 9 Health and Safety Executive (HSE) guidelines recommended that employees who spend a significant amount of time in ionizing radiation controlled areas should be provided with personal dose monitoring, that is, with a dosimeter. 10 In the authors' experience, training grade urologists who rotate through departments frequently are rarely provided with dosimeters.
The principle “As Low As Reasonably Achievable” (ALARA) was introduced to protect staff from both linear and stochastic effects of radiation exposure. 11 The ALARA principle takes into account three factors: time of exposure, distance from radiation, and shielding from radiation. Shielding can be in the form of a lead apron, thyroid guard, lead eyeglasses, and lead gloves. A lead apron reduces radiation exposure by >90%. 12 An orthopedic study of radiation exposure during intramedullary nailing found that radiation exposure without thyroid shielding was 70 times higher than with thyroid protection. 13
Current radiation safety practice in the United Kingdom is not known. The primary aim of this study was to report the radiation safety practice of the urology multidisciplinary theater team in the United Kingdom. The secondary aim was to identify training and knowledge of radiation safety, and barriers to the use of shields and dosimeters in those with occupational exposure.
Materials and Methods
A 14-question survey was disseminated to multidisciplinary urology theater staff through local representatives at each participating center, and online through social media (Twitter®, Facebook®, and WhatsApp®) to a urology-based audience through Google Forms™. The questionnaire was self-administered and not validated.
All members of the endourology theater team were invited to participate, including urologists (consultants, training urologists, and medical students), the anesthetic team (consultants, training anesthetists, and anesthetic assistants), nurses (scrub team and support workers), and radiographers (fluoroscopy technicians).
Questions included demographic data such as professional role, age group, and number of cases involving radiation exposure per week. Radiation safety practice such as use of protective equipment and dosimeters was recorded. Reasons that affected the use of personal protective equipment (PPE) were also explored. Radiation exposure knowledge questions were developed from the ICRP and HSE guidelines.
To evaluate the primary outcome of radiation safety practice in the United Kingdom, responses from outside the United Kingdom were excluded from the primary analysis.
A chi-squared test was used to evaluate the association between radiation safety training, dosimeter, and PPE use, as well as whether consultant urologists were more likely to use a dosimeter than training grade urologists. Dosimeter and radiation shield use in a higher risk subgroup of respondents involved with >10 fluoroscopy cases per week were compared with those undertaking <10 cases per week using a chi-squared test. All statistical analyses were performed using STATA v15.1, and p-value <0.05 was considered statistically significant.
Results
The study collated a total of 309 completed responses, 272 from U.K. centers and 37 from non-U.K. centers. Of the U.K. respondents, 58.5% worked in a university teaching hospital and 41.5% in district general hospitals. Table 1 illustrates respondents' demographics.
Participant Demographics
Radiation exposure practice
Respondents reported their average frequency of exposure to fluoroscopic procedures with 173 (63.6%) involved in 1–5 cases per week, 77 (28.3%) in 6–10 cases per week, and 22 (8.1%) in >10 cases per week.
A total of 34 (12.5%) respondents answered “yes” to using a dosimeter in their practice, whereas 238 (87.5%) answered “no” or “I don't know.” Consultant urologists were more likely to use a dosimeter than training grade urologists (p = 0.035). With regard to PPE use, 270 (99.3%) of respondents reported shielding with a lead apron and 142 (52.2%) of respondents reported shielding with a thyroid guard. Lead eyeglasses and gloves were used by 26 (9.6%) and 2 (0.7%), respectively. Two (0.7%) respondents wore the full protective equipment (lead apron, thyroid guard, gloves, and eyeglasses). PPE use across the multidisciplinary theater team is depicted in Table 2.
Use of Personal Protective Equipment in the Multidisciplinary Urology Theater Teams
Respondents were invited to provide reasons for not using a full set of PPE, with multiple answers permitted. Selectable options included “availability,” “affects work ability,” “did not think it was necessary,” “personal preference,” “discomfort,” and “other.” The distribution of reasons is illustrated in Figure 1. A total of 208 (76.5%) respondents selected “availability” as a reason for not using a full set of PPE. “Availability” was stated as a reason for not using PPE in 77.4% of respondents from university teaching hospitals and 71.7% from district hospitals.
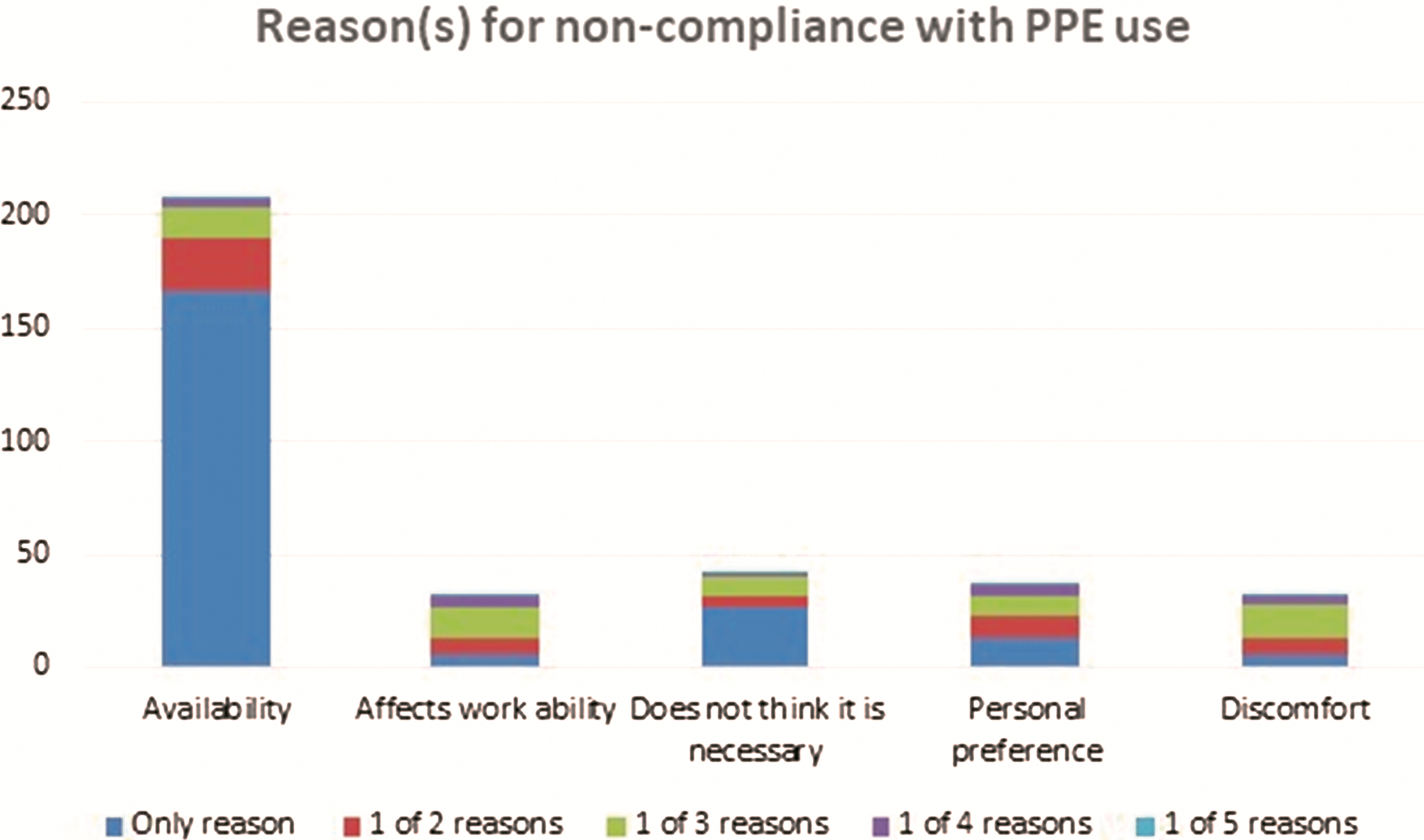
Reason (s) for noncompliance of personal protective equipment use. Color images are available online.
In the subgroup of respondents with higher radiation exposure with >10 cases per week, 36.4% used a dosimeter compared with 12% in the <10 cases per week group (p < 0.01). Lead apron use was 100% vs 99% (p = 0.67), thyroid guard 59.0% vs 55% (p = 0.74), lead eyeglasses 9.2% vs 9.1% (p = 0.99), and lead gloves 0% vs 0.8% (p = 0.67). In the >10 cases per week subgroup, 81.8% of the respondents stated availability was their single contributing factor for noncompliance with full PPE use.
Training
A total of 152 (45.9%) respondents received some form of radiation safety training, of whom 70 (46.1%) received e-learning, 71 (46.7%) attended a course, and 13 (8.6%) had both. Other forms of training included informal hospital teaching, part of examination curriculum, and formal teaching in conferences or lectures. Table 3 illustrates rates of training by profession. The percentage of respondents who had no form of radiation safety training in district and teaching hospitals was 46.9% and 41.5%, respectively.
Training on Radiation Safety Received by Each Theater Team
Use of a lead apron, thyroid shield, eyeglasses, or gloves was not associated with completion of radiation safety training (p = 0.87, p = 0.34, p = 0.64, and p = 0.20, respectively). There was, however, an association between dosimeter use and completion of some form of radiation safety training (p = 0.02).
A survey question assessing respondents' confidence in radiation safety knowledge showed that 100 respondents (36.8%) were confident they had received adequate training. The anesthetic team members were least confident in adequacy of radiation safety training, with 16 (59.3%) respondents stating that they did not feel adequately trained. This was closely followed by 21 (30.9%) nurses.
Knowledge
A total of 43 (15.8%) respondents correctly answered the question regarding maximum radiation exposure per year as per ICRP guidelines. There was no association between answering knowledge questions correctly and having completed any form of radiation safety training (p = 0.41).
Discussion
This multicenter collaborative study received ∼300 nationwide responses demonstrating that training on radiation safety and utilization of protective shielding is suboptimal among urology theater staff in the United Kingdom. In our study, although lead aprons were near-universally used, other forms of shielding wear were less frequently utilized. This observation is comparable with that of other studies conducted in Europe, Brazil, and the United States that demonstrated 84%–99% lead apron use and 54%–84% thyroid guard use. 14 –16
Occupational radiation exposure is associated with higher incidence of thyroid cancer. 17 Given this, we would compel all clinicians with occupational exposure to ionization radiation to use thyroid shields. Lead aprons with integrated thyroid guards are commercially available and may be one way to increase uptake and ensure availability of both is equal.
Reported use of lead gloves and eyeglasses in this study was low. A prospective study that measured radiation exposure with dosimeters for 12 urologists performing fluoroscopic procedures found that the annual exposure of the lens of the eye and extremities was 200 times lower than the regulatory ICRP limit without shielding. 18 Another study demonstrated the lens of the eye of screening urologists was exposed to an average of 2 μSv per procedure, indicating that urologists could perform 1000 procedures per year before reaching the ICRP regulatory limit of 20 mSv. 19 Although not in keeping with the ALARA principle, the low radiation exposure of lenses along with the impact on dexterity and comfort may explain the poor utilization of eye shields.
Our U.K. study revealed availability as the primary reason for urology theater staff not shielding from ionizing radiation in the workplace. In a similar survey in the United States, the use of protective equipment and dose monitoring among residents was low, with availability being the main reported reason. 15 In a survey of 321 French urology residents, 90% identified a lack of protective equipment in the operating room. 18 Our survey did not breakdown availability by item, nor did it further explore the detail of “availability,” for example, institutions not possessing the relevant equipment or it being stored in an inconvenient place. These limitations restricted our ability to suggest solutions that could be applied to other centers. We would, therefore, encourage readers to explore availability of radiation shields in their institution and identify local barriers to use.
An additional barrier identified in our study was that 13.9% of respondents “did not think it was necessary” to wear radiation protection equipment. As no follow-on question was asked, it is not known whether these respondents believed no radiation protection was necessary, or just certain elements of the protective equipment. Borges and associates similarly reported that 16% of 332 Brazilian urologist surveyed did not believe in the efficacy of PPE. 20
According to U.K. law, it is an employer's responsibility to provide appropriate safety training for individuals with occupational exposure to ionizing radiation. 21 Our survey suggests training is not comprehensively provided in the United Kingdom, which leaves employers exposed to risk of litigation. In our study, fewer than half of respondents had received formal radiation safety training. This is in keeping with the data from studies worldwide that reported radiation training provision ranged between 17% and 55.6%. 15,22 There was no association between completion of training and use of radiation shields, reflecting poorly on the quality of any training that was received.
It is our belief that recall of annual radiation dose limits and the physics of ionizing radiation are less important than understanding the risks of inadequate radiation protection. We advocate development of engaging and relevant training to ensure staff members are motivated to utilize PPE and to encourage colleagues to do so too. This may also positively impact the institution's safety culture. Informed demand for adequate provision of shielding equipment will put pressure on employers to make this vital equipment available. In the authors' personal experience, knowledge of our employer's duty to provide adequate radiation shielding facilitated procurement of additional shielding equipment.
Although not a specific questionnaire item, concerns over hygiene of shared equipment may also be a barrier to use, particularly in the COVID-19 era. Personal items, or maintenance of radiation shields with cleaning between each user, are necessary.
HSE guidelines state that individuals with regular occupational exposure to ionizing radiation should monitor their exposure with a dosimeter. However, our study showed that dosimeters were largely not adhered to, with only 12.5% of respondents reporting dosimeter use. Dosimeter use was low for each professional role, but more so for trainee urologists than consultants. This may be due to frequent rotation of trainees with employers failing to prioritize this need. We would advocate a personal dosimeter being part of an “induction pack,” delivered alongside radiation safety education for incoming trainees, particularly in endourology.
Simson et al. showed that PCNL has the highest radiation exposure and the longest fluoroscopy time compared with other endourologic procedures. 23 We did not collect information on the type or length of endourologic procedure our respondents performed, but looked at average number of cases per week instead. Hence, respondents who performed <10 PCNL cases per week may not have been classified as high risk. Respondents who reported more frequent radiation exposure did not have more training than the remainder of the respondents, nor were they found to be any more compliant with shielding despite being exposed to radiation more routinely.
A strength of our study is the inclusion of the multidisciplinary urology theater team, whereas previous studies have reported practice among operating surgeons or interventionists.
Limitations of this study included unequal distribution of respondents from the multidisciplinary theater teams. The questionnaire (provided in the Supplementary Data) on current knowledge was limited to familiarity with guidelines and not on the consequences of radiation exposure, which is arguably more important. The questionnaire that we developed has not been validated. The reasons for noncompliance were not specific to each type of PPE and reasons for nonavailability were not explored. No Welsh or northern Irish centers contributed to the data, so the findings may not be generalizable to these nations.
Conclusion
This is the first U.K. report of radiation safety practice and knowledge among the urology multidisciplinary theater team. Lead apron use was high, but use of other shielding equipment was poor, with lack of availability being the most common reason for nonuse. Radiation safety training and knowledge among urology theater staff were limited. Employers are obliged to provide adequate radiation safety training and protective equipment, and this is a need that must be urgently addressed.
Footnotes
Authors' Contributions
K.O. and H.W. contributed to the conception and design of the study. K.O. developed the protocol and survey. K.O. and H.W. contributed to representative recruitment and data analysis. K.O. drafted the article. S.N., H.W., and J.M. contributed to the revision of the article. All authors contributed to acquisition of data. All authors contributed to interpretation and drafting the article and critically revising it for important intellectual content and approved the final version of the article. J.M. supervised the study.
Informed Consent
Informed consent was obtained from all individual respondents included in the study.
Acknowledgments
Many thanks to all respondents and all who helped disseminate this survey.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.