
Abstract
Objectives:
To describe our multi-institutional experience with robotic repair of iatrogenic urogynecologic fistulae (UGF), including vesicovaginal fistulae (VVF) and ureterovaginal fistulae (UVF).
Methods:
We performed a retrospective review identifying patients who underwent robotic repair of VVF and UVF between January 2010 and May 2019. All patients failed conservative management with Foley catheter or upper tract drainage (ureteral stent and/or nephrostomy tube), respectively. Patient demographics and perioperative outcomes were analyzed. Success was defined as no vaginal leakage of urine postoperatively, in the absence of drains, catheters, or stents.
Results:
Of 34 patients, 22/34 (65%) had VVF and 12/34 (35%) had UVF repair. VVF etiology included radiation (1/22, 4.5%) and surgery (21/22, 95.5%). Four of 22 (18%) had undergone prior repair attempt. Median console time was 187 minutes (interquartile range [IQR]: 151–219), estimated blood loss (EBL) was 50 mL (IQR: 50–93), and median length of stay (LOS) was 1 day (IQR: 1–2). Two of 22 (9%) patients had a postoperative complication. At mean follow-up of 28.9 months, 20/22 (91%) VVF cases were clinically effective. UVF etiology was gynecologic surgery in all cases; 8/12 (67%) were left-sided, 4/12 (33%) were right-sided. None was repeat repairs. Two of 12 (17%) underwent ureteroureterostomy, and 10/12 (83%) had reimplant. Median console time was 160 minutes (IQR: 133–196), EBL was 50 mL (IQR: 50–112), and LOS was 1 day (IQR: 1–1). No complications were encountered. At mean follow-up of 29.3 months, 100% of UVF repairs were effective.
Conclusions:
Robotic repair of iatrogenic UGF may be effectively performed with low complication rates by experienced urologic surgeons.
Introduction
Urogynecologic fistulae (UGF), such as vesicovaginal fistulae (VVF) and ureterovaginal fistulae (UVF), are rare but potentially devastating conditions for affected patients. In developed countries, the most common cause of UGF is iatrogenic, most notably after gynecologic surgery. VVF occur after 0.1% to 0.2% of abdominal hysterectomies, while UVF have an incidence of about 0.5% to 2.5% of all major gynecologic surgeries. 1 Iatrogenic UGF can also be radiation-induced, occurring in 0.6% to 2% of women irradiated for cervical cancer. 2 The hallmark symptom of UGF is continuous urinary leakage, which represents a significant psychologic burden, and can also lead to skin breakdown and infection if not addressed. In addition, UVF may cause obstruction leading to eventual renal failure if not identified and repaired. 1 Although VVF and UVF are distinct clinical entities, the management of VVF and UVF is inter-related, as up to 12% of VVF are associated with concomitant UVF. 1
The robotic modality provides three-dimensional magnified visualization, with the ability to work in limited anatomic spaces and suture with precision. This is able to be done while maintaining the advantages of minimally invasive surgery, such as improved cosmesis and decreased estimated blood loss (EBL), postoperative pain, and length of stay (LOS). Furthermore, utilization of intravenous indocyanine green (ICG) with subsequent visualization under near-infrared fluorescence (NIF) may allow for real-time assessment of tissue perfusion during reconstruction. 3 Although there are a handful of reports regarding robotic UGF repair, they are limited by small patient cohorts and limited follow-up. 4 –11 Herein, we report our multi-institutional experience of robotic UGF repair.
Materials and Methods
An institutional review board-approved retrospective review of our multi-institutional UGF database was performed to identify all patients who underwent robotic VVF and UVF repair between January 2010 and May 2019. All patients included in our analysis failed a course of conservative management before surgical repair. For VVF, this involved at least 2 weeks of bladder drainage via the Foley catheter. For UVF, this consisted of urinary drainage via a ureteral stent and/or nephrostomy tube for at least 6 weeks. Our primary outcome was surgical success, which was defined as the absence of vaginal leakage of urine without any catheters, drains, or stents in place. Our secondary outcome was postoperative complications.
Surgical technique
Preoperative and endoscopic evaluation
After a course of conservative management, but before surgical reconstruction, all patients underwent repeat evaluation for the presence of VVF and/or UVF. This included a quality CT scan of the abdomen and pelvis and a preoperative pelvic examination under anesthesia in an attempt to localize the fistulous tract. Thorough cystoscopy was often able to identify the fistula (Fig. 1A).
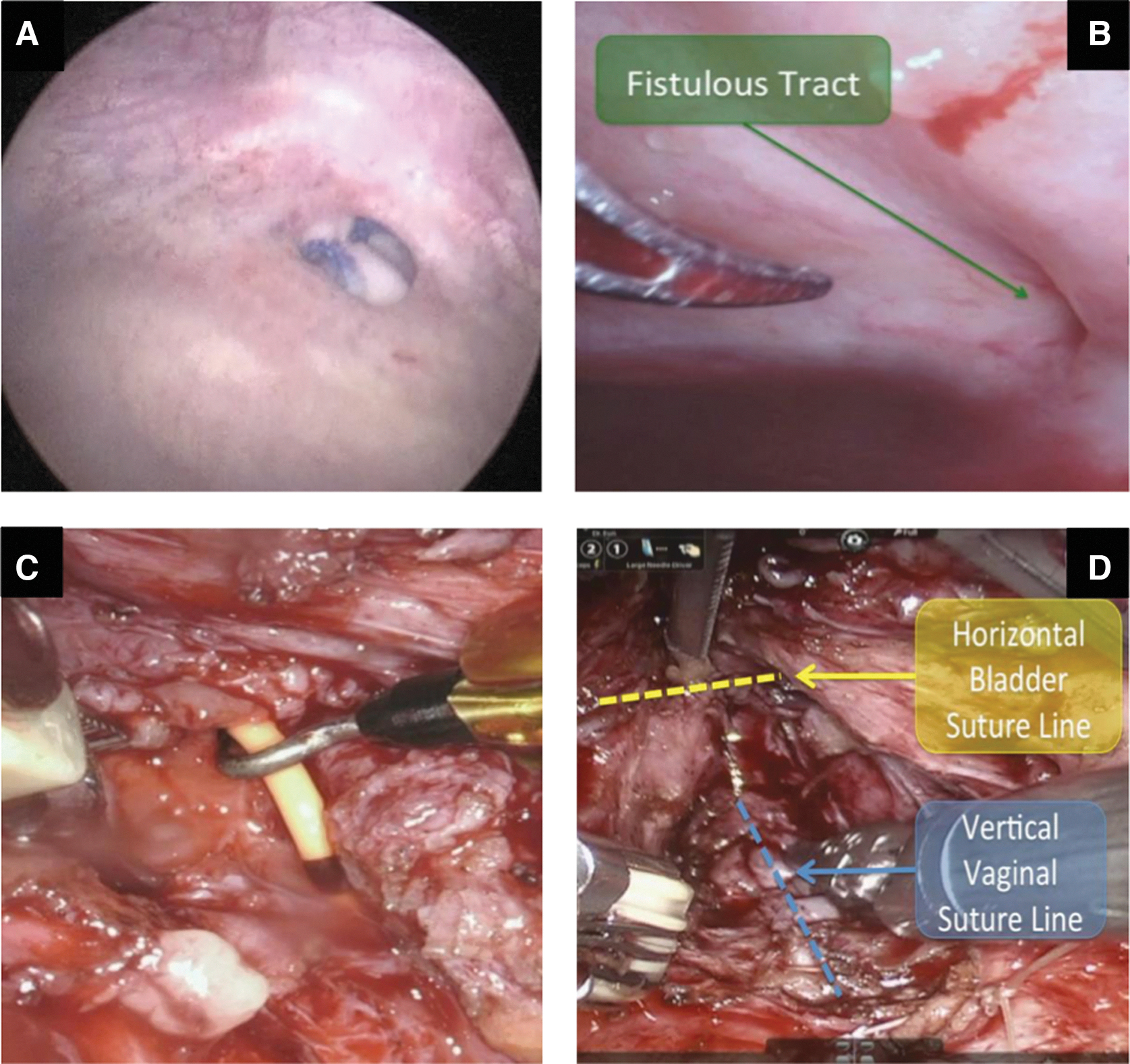
Intraoperative photographs.
In addition, a cystogram was performed under gravity filling via an 18F Foley catheter, and retrograde pyelogram performed under pressure via a 5F ureteral catheter under real-time fluoroscopic visualization. Concomitant antegrade pyelogram was performed in patients with a percutaneous nephrostomy tube. The 12% rate of concurrent ureteral fistula component underscores the importance of comprehensive preoperative imaging and thorough evaluation.
VVF repair
Each patient was prepped and sterilely draped in the dorsal lithotomy position. To begin, a cystogram to evaluate bladder capacity and a cystoscopic evaluation were performed to identify the fistulous tract. If found, an attempt to cannulate the tract was performed with a 5F open-ended catheter. This helped to immediately identify the tract when it was encountered intraoperatively and could even be used to manipulate the tissue and aid in identifying the tract during the dissection (Fig. 1C). Biopsies were taken if there was any suspicion of malignancy.
During the robotic portion of the procedure, a handheld vaginal retractor was manipulated by the bedside assistant to help define the vaginal vault grossly as well as aid in the dissection of the junction between the vaginal cuff, anterior vagina, and bladder. Whenever possible, an extravesical approach was utilized to dissect along the vaginal/bladder border until the fistulous tract was identified. In cases of significant inflammation between the vaginal cuff and bladder, or if this dissection was time-consuming or ineffective, the bladder was typically opened longitudinally, to help isolate the fistula transvesically (Fig. 1B). The fistulous tract was then excised and, when appropriate, sent for pathologic analysis.
An important aspect of the repair was to continue the dissection between the bladder and vaginal wall adjacent to the fistula tract and beyond, to accomplish two goals: (1) to physically separate the bladder and vaginal suture lines from each other to minimize the chance for refistulization and (2) to create a space in between the bladder and vaginal repairs that could accommodate an interposition flap. In cases where tissue quality was of concern (e.g., redo repair or history of radiation), intravenous ICG with NIF was used to assess tissue perfusion in real time. If there was evidence of poor tissue perfusion, the nonviable area was trimmed back to healthy tissue and additional mobilization was performed as needed.
After excision of the fistulous tract, the vaginal defect was closed with barbed absorbable suture in a single layer, and whenever possible, a second imbricating layer over top to bury the underlying closure. Following established principles in UGF repair, the bladder closure was performed in an identical manner, except perpendicular to the suture line used for the vaginal closure to avoid parallel suture lines from overlapping (Fig. 1D).
UVF repair
For UVF repairs, a ureteral catheter was usually placed cystoscopically under fluoroscopic guidance, at the location of the fistula site before the robotic procedure was started. Often, a significant lysis of adhesions and drainage of loculated urinoma was necessary before initiating the fistula repair. The ureter was identified at its crossing of the iliac vessels and ureterolysis was performed caudally with careful dissection to preserve blood supply that usually comes from the internal iliac vessels. Manipulation of the vaginal retractor was critical to help identify the anatomy where the ureter approached the vaginal vault or cuff. Typically, the periureteral dissection planes became noticeably more fibrotic as the fistula site was encountered.
For UVF, the two typical intraoperative findings were as follows: (1) A misplaced lateral vaginal cuff suture that incorporated the ureter or (2) complete or partial wall trauma to the ureter either by transection or electrocautery. In cases where we identified a prior vaginal cuff stitch that incorporated the ureter, we released the stitch and performed any necessary reconstruction of the vaginal cuff to close off the vaginotomy. In cases where the entire ureter was transected or a ureteral wall defect was identified, the vaginal fistulous tract was closed before addressing the ureter. The ureter was then transected proximal to the fistula.
If a psoas hitch was performed, the bladder was mobilized by taking the anterior and lateral attachments and fixed to the psoas fascia with nonabsorbable suture. A prerequisite to placing the psoas fascia stitch was to readily identify and avoid the nearby genitofemoral nerve when placing the bladder tensioning stitch. A small cystotomy was made in the ipsilateral dome and the ureter was spatulated before performing a tension-free anastomosis to the bladder mucosa using running absorbable suture. A stent-over-wire was placed half-way through the anastomosis, which was finished after stent placement.
In two cases, UVF were addressed with a primary ureteral repair and alternatively a ureteroureterostomy was performed instead of a ureteral reimplant. These select cases were performed when the periureteral inflammation was minimal with an extremely short segment of involved ureter. Both ends of the ureter were spatulated and anastomosis was performed using absorbable 5-0 monofilament suture. Again, a stent was placed after one side of the anastomosis was done and the anastomosis was completed after the stent was placed. Similar to VVF repairs, ICG could be utilized in select cases where tissue quality was of concern.
Tissue interposition
The decision to interpose tissue between the reconstructed bladder and vagina, and the reconstructed ureter and vagina, was at the discretion of the primary surgeon based on the patients' specific clinical history and intraoperative findings. Four tissue types were utilized for interposition. For omental flaps, the greater omentum, based on the right or left gastroepiploic artery, was mobilized using a combination of electrocautery and absorbable clips. Peritoneal, sigmoid epiploic appendage and vaginal flaps were also used. Each flap had adequate length to reach the deep pelvis free of tension and was secured to overlie the site of repair.
Postoperative management
Foley catheters were typically left in place for 7 to 10 days following uncomplicated repair. Fourteen days were used for postradiation repairs. Cystograms were performed at the discretion of the operating surgeon.
Results
Of 34 patients, 22/34 (65%) had VVF and 12/34 (35%) had UVF. For VVF, etiology included radiation (1/22, 4.5%) and surgery (21/22, 95.5%). The majority of surgeries were gynecologic (20/21, 95%) followed by colorectal (1/21, 5%). Four of 22 (18%) of patients had undergone prior repair before referral to us (2 transabdominal, 1 transvaginal, and 1 patient had had both types). Table 1 summarizes these demographic data.
Preoperative Demographic Information
UGF = urogynecologic fistulae; UVF = ureterovaginal fistulae; VVF = vesicovaginal fistulae.
Median time from diagnosis of fistula to repair was 55.5 days (interquartile range [IQR]: 25–168). The fistulous tract was preoperatively cannulated effectively in 13/22 patients (59%). Interposition was utilized in 21/22 VVF cases (95%): omentum (62%), peritoneum (14%), sigmoid mesentery/epiploic appendage (14%), vaginal flap (5%), and unspecified (5%). For VVF, median console time was 187 minutes (IQR: 151–219), EBL was 50 mL (IQR: 50–93), and median LOS was 1 day (IQR: 1–2). Two of 22 (9%) patients had a postoperative complication. One patient developed a urinary tract infection requiring antibiotics (Clavien grade 2). The other had exacerbation of underlying restrictive lung disease requiring intensive care (Clavien grade 4). Table 2 summarizes operative interventions and outcomes. Fourteen of the 22 VVF patients underwent cystogram before Foley removal.
Perioperative Outcomes
IQR = interquartile range.
At mean follow-up of 28.9 months, 20/22 (91%) VVF cases were clinically effective. Two failures were encountered. The first patient had a history of bilateral ureteral and bladder injury during a midline total abdominal hysterectomy for fibroids, with bilateral reimplants performed at the time of surgery. She subsequently had a failed transvaginal VVF repair at an outside hospital, followed by our initial robotic repair, which failed 6 months later. She was taken back for repeat robotic repair, which was challenging, although effective. The residual fistula was small and extremely proximal. Methylene blue was instilled into the bladder followed by a speculum examination, which identified its precise location. With great difficulty, the tract was able to be cannulated with a 5F catheter to aid in its dissection. A significant amount of time was also spent on lysis of prior adhesions, to avoid additional injury and to help isolate the fistula for repair.
The second patient also underwent an open hysterectomy for fibroids, with intraoperative left ureteral injury and reimplantation. She developed urinary incontinence 2 years after repair and was diagnosed with recurrent VVF upon examination by her gynecologist. Subsequent transvaginal repair was effective. Neither had received prior pelvic radiotherapy.
For UVF, etiology for all 12 cases was gynecologic surgery. Of these repairs, 8 (67%) were performed on the left side and 4 (33%) on the right. Median time from diagnosis of UVF to repair was 23 days (11–54). Repair was via ureteroureterostomy in 2/12 (17%) and reimplantation in 10/12 (83%) cases, 5 (50%) of which required psoas hitch. Omental interposition was used in 4/12 (33%) cases and peritoneum in 1/12 (8%). Median console time was 160 minutes (IQR: 133–196), EBL was 50 mL (IQR: 50–112), and LOS was 1 day (IQR: 1–1). No complications were encountered. At mean follow-up of 29.3 months, 100% of UVF repairs were effective.
Discussion
In general, for management of UGF, conservative efforts are attempted before progressing to surgical options. For VVF, this involves bladder drainage for 2 to 3 weeks. If able to be isolated, the fistulous tract may also be fulgurated. Fistulae are more likely to close when uncomplicated (e.g., involving nonradiated tissue) and small in size (2–3 mL or less). If no additional complicating factors are present (e.g., infection), immediate repair can be attempted. There is no gold standard approach, rather the operative expertise of the surgeon is the major determinant. 1 In a 2017 systematic review and meta-analysis of 124 articles on VVF repair, only 10 included conservative management. A success rate of 67% to 100% was cited for nonoperative interventions (e.g., fulguration and fibrin glue); 16% of VVF were initially managed with catheter drainage alone, of which 8% resolved and did not require surgery. 12
UVF, in cases where there is a nontransection, or an incomplete injury, can be managed initially with conservative treatment, that is, urinary drainage of the upper tract via stent and/or nephrostomy tube placement. A recent review of UVF repair found an 83% success rate with stenting alone. 13 If there is persistence of the fistula after 4 to 6 weeks of drainage, continued conservative therapy is unlikely to work and definitive repair should be attempted.
The fistula is frequently associated with inflammation and often requires excision and ureteroneocystostomy. 1 It is also important to know that in some cases managed conservatively, the fistula may spontaneously close, but a stricture may then develop at the healed site due to periureteral fibrosis. Therefore, UVF managed conservatively with drainage require extended follow-up to rule out evolution from fistula to stricture.
Most existing literature on UGF management in the developing world is limited and consists mainly of small case series. An exception is a 2018 publication of outcomes from the Danja Fistula Center in Niger. This cohort of 384 women included VVF, UVF, and also urethrovaginal fistulae. All underwent open transvaginal repair. 53.9% of cases were effective and the patient was dry, 16.4% were effective but the patient was incontinent from etiologies other than the repaired fistula, and 29.7% failed initial open repair. 14
The largest published series of robotic VVF repair was by Chandna and colleagues in 2020 and consisted of 33 patients who underwent repair from 2014 to 2019. Hysterectomy was the etiology in 81.8%, and 63.1% were recurrent cases. Similar to the success rate in our series, they found that 31/33 (93.9%) had effective surgical repair. 10 Another publication of 13 patients undergoing robotic VVF repair had an initial success rate of 84.6% (100% after second surgery). Only one patient (7.6%) suffered a Clavien grade 1 complication. 9
Outcomes on redo repair are also optimistic, as evidenced by a 2008 cohort of seven patients undergoing repeat repair after recurrence of their VVF; all cases were effective, 15 similar to the results in our three patients who failed initial repair. Regarding surgical approach, 1 prospective study compared 12 robotically repaired recurrent VVF with 20 openly repaired recurrent VVF and found no difference in success rate but did note lower EBL and LOS in the robotic group. 16
Literature is even more scarce on UVF. A 2014 African single-center retrospective review by Lawal and colleagues evaluated 18 patients with UVF who underwent open repair. All patients were effectively treated, although follow-up duration is not noted. There was one patient who suffered an intraoperative left internal iliac arterial injury requiring vascular surgery consultation and repair. Four of 18 (22.2%) patients suffered low Clavien grade complications. 17
A 2015 multi-institutional review of robotic management of gynecologic surgical injuries included 10 UVF in an overall cohort of 43 patients. 6 This article did not stratify outcomes by type of fistula, rather by the type of repair performed. For example, it included ureterocutaneous fistula and several ureteral ligations in this cohort and, as such, we are unable to elucidate outcomes for UVF patients alone. The only other series of robotic UVF repair was by Menon and colleagues who described three patients who underwent ureteral reimplantation at a single center. They reported 100% success rate after initial repair, with a mean follow-up of 6 months. 5
It is important for the reconstructive urologist to note that despite the absence of a ureteral fistula on imaging studies, ureteral reconstruction may be indicated at the time of surgical repair of a VVF. For example, a two-patient series published in 2010 required ureteroneocystostomy, in addition to vesicovaginal repair, for a VVF located near the ureteral orifice. 18
The results of our study suggest that robotic VVF and UVF repair is safe and effective. With regard to VVF, there was one major complication in our series and our median LOS was 1 day. This compares favorably with the previously cited literature. We had two surgical failures after VVF repair, diagnosed at 6 months and 2 years postoperatively, suggesting that these patients should be monitored long term. With regard to UVF, median LOS was 1 day, and no complications were encountered.
Our report is limited by its small size and retrospective nature, but this must be considered in the context of relative rarity of iatrogenic UGF. Another constraint is our lack of long-term follow-up. In our cohort, 12/34 (35%) patients had >24 months of follow-up. The fact that we had a failure occur at 24 months suggests that long-term follow-up is important. Additional studies with longer term follow-up are necessary. Furthermore, continued multi-institutional collaboration is necessary to generate larger patient cohorts with longer follow-up, and to also include those who have had prior radiation.
Conclusions
Robotic VVF and UVF repair is associated with excellent intermediate-term outcomes. For repairs after surgery, our data suggest that recurrences can occur as late as 2 years after repair, suggesting the importance of long-term follow-up. Additional multi-institutional studies with larger cohorts, longer follow-up, and inclusion of more patients with radiation history are necessary.
Footnotes
Acknowledgments
All authors have made substantial contributions to this work, sufficient to claim formal authorship.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.