
Abstract
Objectives:
To evaluate the outcomes of robot-assisted partial nephrectomy (RAPN) in cystic renal tumors.
Materials and Methods:
We retrospectively analyzed patients who underwent RAPN for either cystic (n = 46) or solid (n = 271) renal tumors at Fujita Health University between 2010 and 2019. Cystic renal tumors were diagnosed using cross-sectional imaging. Perioperative, oncologic, and functional outcomes were assessed.
Results:
The median follow-up periods were 38, 41, and 37 months in the total, cystic, and solid groups, respectively. Most patient characteristics were similar among both groups, while the median age of the cystic group was significantly lower than that of the solid group (p = 0.02). Most perioperative variables and complications were comparable between the two groups. There was no significant difference between the groups in perioperative renal function. The estimated glomerular filtration rate preservation rates were 93.1% and 89.2% in the cystic and solid groups, respectively (p = 0.17). The cystic group showed a higher benign histology rate (19.6% vs 7%) and lower Fuhrman grade than the solid group (24.3% vs 15.1% in grade 1, and 73% vs 81.3% in grade 2), although there was no statistically significant difference between the two groups. In the solid group, 10 patients (3.7%) experienced recurrence, and 2 patients (0.7%) died of renal-cell carcinoma, while none of the patients with cystic tumors experienced recurrence. There was no statistically significant difference between the cystic and solid tumors with respect to 5-year recurrence-free survival (p = 0.18), cancer-specific survival (p = 0.55), and overall survival (p = 0.35).
Conclusions:
RAPN for cystic renal tumors appears to be safe and feasible with perioperative, long-term functional and oncologic outcomes comparable with those in solid tumors. RAPN can be a safe and effective surgical option for cystic renal tumors.
Introduction
Partial nephrectomy (PN) is considered the established treatment for small renal tumors, including cystic renal tumors. 1,2 The frequency of cystic renal tumors in the PN series has been reported to range from 2.5% to 18%. 3 –7 Although the feasibility of laparoscopic nephron-sparing surgery for cystic renal tumors has been previously reported, 3 the standard surgical approach has not yet been established.
Recently, robot-assisted partial nephrectomy (RAPN) has gained popularity for the management of small renal tumors with convincing outcomes. 8,9 However, the available literature on RAPN for cystic renal tumors is insufficient. Two previous studies reported comparable outcomes for RAPN in cystic and solid renal tumors 5,6 ; subsequently, the evidence of long-term oncologic safety and renal function was confirmed. 7
The present study aimed to validate the previous findings and to report our experience with RAPN for cystic renal tumors.
Materials and Methods
Patients
We conducted a retrospective cohort study of 317 patients with cystic and solid renal tumors who underwent RAPN at the Fujita Health University between 2010 and 2019. Patients' demographic, renal function, surgical parameters, pathologic parameters, and survival data were recorded in our database. RAPN was considered imperative in patients with the absence of a normal contralateral kidney or estimated glomerular filtration rate (eGFR) <50 mL/min/1.73 m2. The present study was approved by the local institutional review board (approval number: HM20-216).
Imaging
Cystic renal tumors were diagnosed on cross-sectional imaging (CT, MRI, or both). All cystic renal tumors were graded according to the most recent Bosniak classification system 10 by a radiologist specialized in urology. Tumor complexity was stratified using the RENAL (Radius, Exophytic/Endophytic, Nearness, Anterior/Posterior, Location) nephrometry scoring system. 11 Decision for surgical intervention was based on Bosniak classification and radiologic changes during the period of surveillance.
Surgical procedure
RAPN procedures were performed transperitoneally or retroperitoneally according to the tumor location and the complexity of renal vessels. To localize the tumor, the kidney was defatted, and a laparoscopic ultrasound was used to assess tumor depth and margin. After administration of mannitol, the renal artery or its branches were clamped with a bulldog clamp. The tumor was resected with an adequate safety margin. For the inner renorrhaphy layer, the collecting system and large vessels were closed with 3 to 0 V-Loc sutures, and, if needed, parenchymal sutures were made with 2 to 0 V-Loc. Surgery was performed by eight surgeons who completed the da Vinci certification program approved in Japan.
Baseline and perioperative variables
Age, body mass index (BMI), sex, American Society of Anesthesiologists (ASA) classification, tumor size, and RENAL nephrometry score were extracted from the database. Preoperative renal function was assessed by calculating the eGFR using the Modification of Diet in Renal Disease formula. Operative time (OT), warm ischemia time (WIT), estimated blood loss (EBL), and length of stay (LOS) were evaluated and compared between the groups. Postoperative complications were classified according to the Clavien–Dindo classification. Trifecta achievement, defined as WIT <25 minutes, negative surgical margins, and no intraoperative and postoperative complications, was considered the key surrogate for success of RAPN.
Pathologic evaluation
All surgical specimens were processed according to standard pathologic procedures and assessed by several expert pathologists in a standard manner. Tumors were staged according to the 2009 American Joint Committee on Cancer-Union Internationale Contre le Cancer Tumor-Node-Metastasis classification. 12 Histologic subtype was evaluated according to the Heidelberg classification. 13 Tumor grading was defined according to the Fuhrman system. 14 Positive surgical margin (PSM) status was defined as the presence of malignant tissue on the inked surface of the tumor on final pathologic assessment.
Follow-up
Regarding the follow-up regimen, patients were evaluated every 3 to 6 months by performing a blood and serum test, urine test, and CT to detect tumor recurrence. Recurrence was defined as tumor relapse in the operative field and presence of lymph node or distant metastasis. Postoperative renal function was assessed by serial measurement of eGFR. The eGFR preservation rate was estimated using the following equation: latest eGFR/preoperative eGFR × 100.
Statistical analyses
Categorical variables were compared using the Fisher's exact test or chi-squared test. Quantitative variables were evaluated using the Student's t-test for normal distribution or the Mann–Whitney U-test for non-normal distribution. Recurrence-free survival (RFS), cancer-specific survival (CSS), and overall survival (OS) were estimated using the Kaplan–Meier method and log-rank test. Two-sided p-values <0.05 were considered statistically significant. All statistical analyses were performed using GraphPad Prism 7.04 (GraphPad software, San Diego, CA) and EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria). 15
Results
Baseline characteristics
We identified 317 patients with cN0M0 renal tumors who underwent RAPN. The cystic group comprised 46 (14.5%) patients, and the solid group comprised 271 (85.5%) patients. The median follow-up periods were 38, 41, and 37 months in the total, cystic, and solid groups, respectively. There were no significant differences in BMI, sex, ASA classification, tumor size, clinical T stage, and RENAL complexity between the groups. The median age of the cystic group was significantly lower than that of the solid group (p = 0.02; Table 1). There was no imperative indication to RAPN in the cystic group. Bosniak distributions in the cystic group were 7 (15.2%), 11 (23.9%), and 28 (60.9%) in Bosniak IIF, III, and IV, respectively (Table 1).
Baseline Characteristics
ASA = American Society of Anesthesiologists; BMI = body mass index; IQR = interquartile range; RAPN = robot-assisted partial nephrectomy; RENAL = Radius, Exophytic/Endophytic, Nearness, Anterior/Posterior, Location.
Perioperative variables
Most perioperative variables were comparable between the groups in terms of OT, WIT, EBL, clamp type, LOS, and trifecta achievement. Overall, intraoperative complications were not statistically significant between the two groups (p = 0.7; Table 2). Intraoperative conversion to RN was performed in two patients with solid tumors, while no RN conversion was observed in the cystic group. Intraoperative cyst rupture was observed in four patients (8.7%).
Perioperative Characteristics
Comparison between the cystic and solid groups in grade 3 or greater.
EBL = estimated blood loss; eGFR = estimated glomerular filtration rate; LOS = length of stay; WIT = warm ischemia time.
Postoperative complications of any grade were recorded in nine cystic (19.5%) and 33 solid (12.2%) tumors (p = 0.3). Grade 3 or greater postoperative complications were observed in 4 cystic (8.7%) and 10 solid (3.6%) tumors (p = 0.13). There were no grade 4 or grade 5 postoperative complications in either the cystic or solid group (Table 2).
Regarding renal function, there was no significant difference between the groups in preoperative, postoperative (1 month), and latest eGFR. The eGFR preservation rates were 93.1% and 89.2% in the cystic and solid groups, respectively (p = 0.17; Table 2).
Oncologic outcomes
Histologically, clear cell renal-cell carcinoma (RCC) was the most common variant of RCC in both groups (71.7% in the cystic RCC and 75.6% in the solid). The cystic group showed a higher benign histology rate than the solid group (19.6% in the cystic vs 7% in the solid), although there was no statistically significant difference in the prevalence of the histologic subtypes (p = 0.06; Table 3). The cystic group had a lower Fuhrman grade than the solid group (24.3% vs 15.1% in grade 1, 73% vs 81.3% in grade 2, respectively), although there was no statistically significant difference between the groups (p = 0.05; Table 3). PSM was observed in one (0.4%) solid tumor but not in the cystic tumors. The rates of malignancy for Bosniak IIF, III, and IV were 42.9%, 63.6%, and 96.4%, respectively (Table 3).
Oncologic Outcomes
PSM = positive surgical margin; RCC = renal-cell carcinoma.
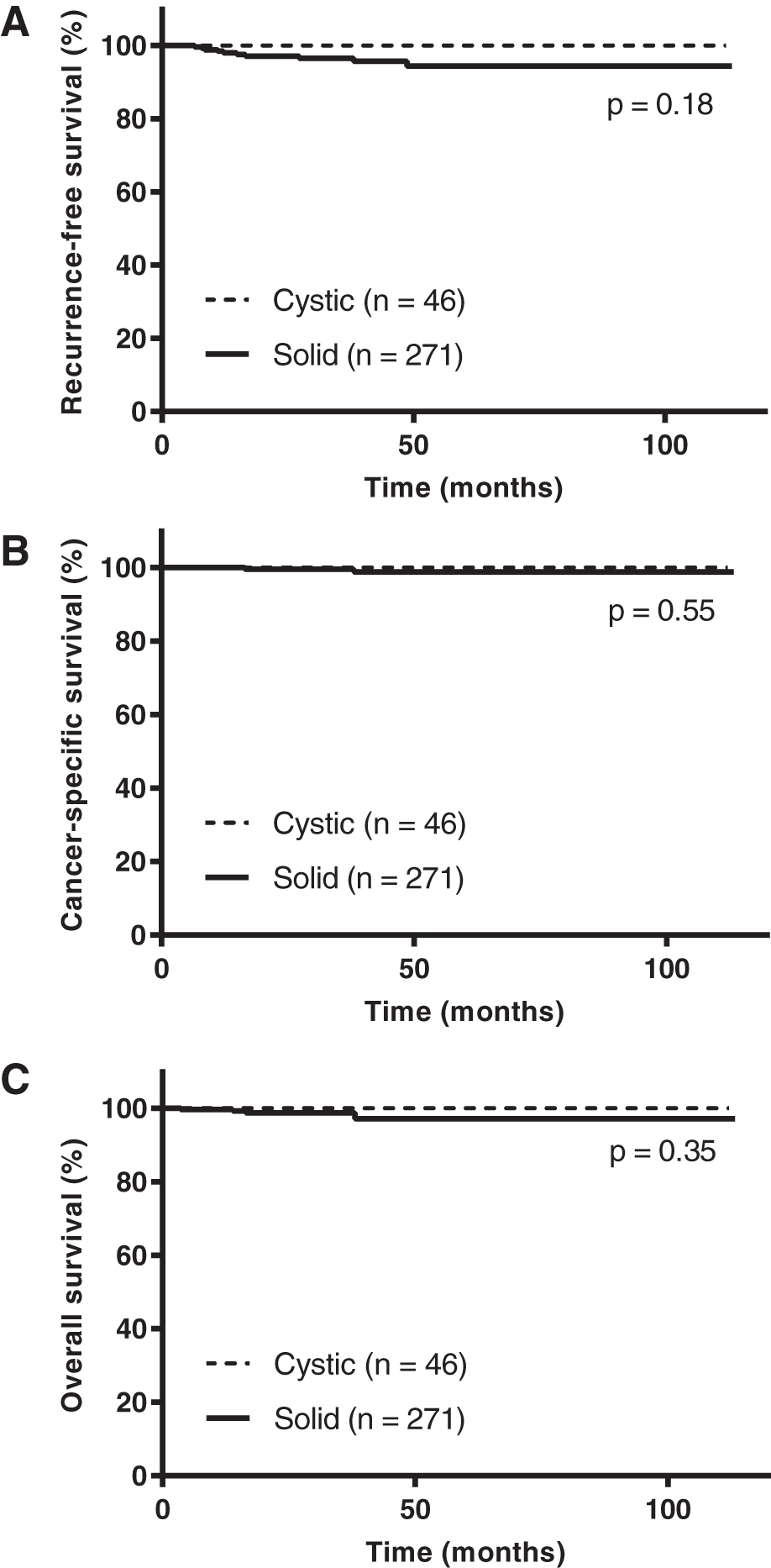
During the follow-up period, we identified 10 recurrences and two cancer-associated deaths in the solid group, while none of the patients with cystic tumors experienced recurrence, including the four patients who experienced intraoperative cyst rupture (Table 3). The 5-year RFS, 5-year CSS, and 5-year OS in the cystic and solid groups were 100% and 94.4%, 100% and 98.7%, and 100% and 97.1%, respectively. There was no statistically significant difference between the cystic and solid tumors with regard to RFS (p = 0.18), CSS (p = 0.55), and OS (p = 0.35; Fig. 1).
Discussion
PN is considered a standard treatment option for small renal tumors and is strongly recommended in the major guidelines. 1,2 In the last decade, RAPN has been widely used in the management of small renal tumors, showing favorable outcomes. 8,9
Cystic renal lesions should be classified according to the most updated Bosniak classification system, 10 and decision-making for surgical intervention is determined based on the risk of malignancy. However, the optimal therapeutic management, specifically for Bosniak IIF and III in cystic renal tumors, still remains challenging and controversial. 10,16,17 Moreover, since the feasibility and safety of RAPN for cystic renal tumors have not been fully elucidated, it is more difficult to consider surgical intervention. Recently, several retrospective studies reported comparable perioperative, functional, and oncologic outcomes of RAPN for cystic renal tumors compared with solid renal tumors (Table 4). 5 –7 We conducted the present study assessing the perioperative, long-term functional, and oncologic outcomes to validate the previous literature and enrich the evidence of optimal management of cystic renal tumors.
Comparison of Reports on Robot-Assisted Partial Nephrectomy for Cystic Renal Tumors in Oncologic and Functional Outcomes
CSS = cancer-specific survival; MFS = metastasis-free survival; OS = overall survival; RFS = recurrence-free survival.
To date, few studies on RAPN for cystic renal tumors have been reported. Akca and colleagues 5 first demonstrated the feasibility of a robotic approach for cystic renal tumors by comparing 55 cystic masses with matched 55 solid masses. There were no significant differences between the groups in terms of eGFR preservation rates (85% vs 86%; p = 0.94) and overall complications (p = 0.3), while RCC prevalence in the cystic group was significantly lower than in the solid group (54.5% vs 85.5%; p = 0.001). Novara and colleagues 6 also reported data from 465 patients who underwent RAPN extracted from the Vattikuti Global Quality Initiative in Robotic Urologic Surgery database. A total of 54 (12%) tumors were cystic, and the cystic group showed significantly lower OT than the solid group (p < 0.001), whereas EBL, WIT, postoperative complications, prevalence of cancer histology, and postoperative eGFR were comparable between the groups. However, these two studies had a short median follow-up period (10 months) and did not evaluate the long-term oncologic safety and renal functional preservations. Subsequently, Raheem and colleagues reported excellent long-term outcomes for the treatment of complex cystic renal tumors with a median follow-up of 58 months. 7 Cystic masses were more likely to have a low Fuhrman grade (p = 0.03) and shorter OT (p = 0.04) than solid masses. Notably, the solid group experienced 4.1% of recurrence and 2% of cancer-associated deaths, while no recurrence or metastasis was observed in the cystic group even after a long follow-up period.
Previous studies have demonstrated the lower malignant potential of cystic RCCs than solid RCCs. 18,19 Cystic RCCs appear to have a low malignancy rate, low Fuhrman grade, and favorable oncologic outcomes. Consistent with three previous RAPN series, 5 –7 cystic renal tumors in the present study also demonstrated lower Fuhrman grade and higher benign histology than the solid tumors, although there was no statistically significant difference between the tumors.
In contrast, there is a technical challenge regarding the prevention of intraoperative cyst rupture, which could cause tumor spillage. The frequency of cyst rupture during RAPN and its actual impact have rarely been addressed, although fluid spillage theoretically may increase the risk of local recurrence. Recently, a retrospective multicenter study was conducted to assess the prevalence of intraoperative cyst rupture and its impact on oncologic outcomes. Surprisingly, there were no local or distant recurrences, including peritoneal carcinomatosis and port site recurrence, despite 50 (18.7%) cyst ruptures in 268 patients. 20 Consistent with this report, there were no recurrence and metastasis, although we found four intraoperative cyst ruptures (8.7%) in the cystic group. Although cyst rupture appears to have a small oncologic impact, further studies are required to address this issue, and we should pay special attention to the manipulation of cystic renal tumors during surgical procedures.
Regarding the prevalence of PSM in cystic renal tumors, Novara and colleagues 6 reported 7.4% and Raheem and colleagues 7 reported 3.1% of PSM, while PSM was not observed in the cystic group of Akca and colleagues 5 and our study. Despite the presence of PSM, two studies showed excellent oncologic outcomes. A previous study that examined the prevalence and impact on survival of PSM in RAPN for RCCs showed little to no impact on 5-year survival rates. 21 Taken together, PSM in RAPN for solid and cystic renal tumors appears to have little impact on survival rates.
Trifecta achievement can provide data on the quality and efficiency of the surgical procedure, although it does not affect the long-term functional or oncologic outcomes. The study by Raheem and colleagues 7 was the first to assess the trifecta achievement rate (59.4%) in cystic tumors, which was similar to that seen in previous studies of RAPN. The present study showed a satisfactory Trifecta achievement rate in the cystic and solid groups (76.1% and 79.7%, respectively).
The long-term functional outcomes in the present study demonstrated a favorable eGFR preservation rates in cystic and solid tumors (93% vs 84%), which are similar to those of previous RAPN series. We typically perform tumor excision with an adequate margin to minimize the risk of tumor spillage and to avoid significant renal parenchymal resection to preserve renal function. Other RAPN series and our data suggested a comparable renal function preservation rate with solid tumors. In addition, Raheem and colleagues 7 and the current study present long-term functional safety.
In the current study, we found that RAPN for cystic renal tumors showed comparable outcomes with those of solid tumors and excellent long-term survival and renal functional preservation. Our findings are consistent with those of previous studies that support the safety and feasibility of RAPN as a treatment option for cystic renal tumors.
Our study has several limitations. First, this was a single-center retrospective study with a relatively small sample size, which might result in selection bias and unmeasured confounders. Second, the population in the present study underwent RAPN by multiple surgeons, which may have reduced the generalizability of the surgical procedure and quality. Third, Bosniak classification in our cohort was mostly determined by CT, which is less sensitive and specific, although some patients were diagnosed using MRI, and an expert radiologist reviewed all the imaging findings. Regardless of the aforementioned limitations, our study suggests that RAPN can be a useful treatment option for cystic renal tumors. Further studies are required to address the feasibility of RAPN for the optimal management of cystic renal tumors.
Conclusions
RAPN for cystic renal tumors appears to be safe and feasible, with perioperative, long-term functional, and oncologic outcomes comparable with those in solid tumors. RAPN can be a safe and effective surgical option for cystic renal tumors.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.