
Abstract
Purpose:
Large meta-analyses demonstrate the noninferiority of laser enucleation to transurethral resection of the prostate (TURP) with regard to long-term efficacy and reoperation rate. Although the 1470 nm diode laser enucleation of the prostate (DiLEP) is superior in hemostasis and surgical visibility, its complexity and associated longer operative time limit its widespread usage. The objective of this study was to generate long-term cost estimates for bipolar TURP and DiLEP, taking into account perioperative and adverse event costs.
Materials and Methods:
This is a retrospective review of patients who underwent DiLEP (n = 114; November 2016 to February 2020) or TURP (n = 194; January 2016 to December 2018). A decision analysis model was constructed to compare costs of the primary procedure and subsequent complications taking into account disposable costs, operating room time, length of stay, reoperation rates, and readmissions. Costs were estimated from internal data, published literature and Medicare procedure costs. Markov modeling was used to create cost projections up to 10 years.
Results:
DiLEP was associated with shorter length of stay and fewer total complications, but longer operative times and greater initial costs. Cost were recuperated at 8 years postoperatively. At 10 years postoperatively, DiLEP represented approximately $664 cost savings per patient over TURP.
Conclusions:
DiLEP is a cost-effective alternative to TURP for the treatment of benign prostatic hyperplasia in the properly selected patient. DiLEP has greater initial costs due to longer operative times. Costs are recuperated by 10 years postoperatively due to higher rate of same-day discharges, and lower complication and reoperation rates, incurring a $664 cost savings per patient treated by DiLEP relative to TURP.
Introduction
For refractory benign prostatic hyperplasia (BPH), transurethral resection of the prostate (TURP) has been the gold standard of treatment since the 1930s, and remains so today. 1,2 A prominent alternative is laser enucleation: a size-independent option, effective for large prostates (>100 g), and recommended by the American Urological Association (AUA) for medically complex patients on anticoagulants due to its decreased risk of blood transfusion. 2 –4
The diode laser differs from the popular holmium laser in that it utilizes a semiconductor bar to generate laser radiation. 5 The 1470 nm wavelength can seal a wide range of blood vessel sizes with superior seal pressures, decreased charring, and maximal power output compared with other diode wavelengths. 6 There is no evidence that diode laser enucleation of the prostates (DiLEPs) depth of penetration contributes to a higher rate of dysuria or otherwise negative impact on the quality of life compared with other laser modalities or TURP 2,7 . Because it does not require a masked cooling system and has only small fans, the footprint is smaller. This portable design makes 1470 nm DiLEP an attractive laser fiber for the outpatient setting.
Large meta-analyses demonstrate the noninferiority of laser enucleation of the prostate (LEP) to TURP with regard to long-term efficacy and reoperation rate. 8 –13 These findings were replicated in our institution's own retrospective review of bipolar TURP and a 100 W DiLEP examining max flow rate (Qmax) and postvoid residual (PVR) up to 1 year, postoperatively (SHB Monfared, 2020 internal data). DiLEP is associated with a shorter length of stay in select patients and fewer long-term complications relative to TURP. 14 However, DiLEP is associated with greater costs, largely due to longer operative time. Of note, in their DiLEP vs holmium laser enucleation of the prostate (HoLEP) head-to-head study, Das and colleagues found no difference in operative time. 15
Although LEP is noninferior, and even superior in hemostasis and surgical visibility, the high cost is often cited in preference for TURP. 16,17 A study from 2001 by Fraundorfer and colleagues comparing the clinical outcomes and costs of HoLEP found a nearly 25% cost savings at 1 year postoperatively with HoLEP due to a lower complication rate and shorter inpatient stay. 18 There is a paucity of data examining the relative costs of TURP and DiLEP over an extended postoperative period. The objective of this study was to generate long-term cost estimates based on perioperative and complication-associated costs for bipolar TURP and DiLEP to compare cost effectiveness.
Methods
Patient population
After obtaining Institutional Review Board (IRB) approval (BUMC IRB protocol H-39406), we conducted a single-center, retrospective review of patients who underwent DiLEP between November 2016 to February 2020, or who underwent TURP between January 2016 and December 2018. Time frames were selected to capture a study population large enough to compare and power the analysis. DiLEP was performed by a single surgeon using a 1470 nm laser. TURP was performed by five surgeons. Patients were excluded from the analysis if they had a history of prostate cancer or prior surgery for BPH. Outcomes were recorded for up to 1 year follow-up.
Cost estimates
Hospital-associated costs were derived from internal data, published literature, and Medicare costs (Supplementary Table S1). Costs included: primary procedure billing, equipment costs, operating room (OR) time, outpatient cystoscopy, length of stay, level of care (inpatient, intensive care), emergency room presentations, readmissions, and reoperation. Apart from postoperative diagnostic cystoscopy, all outpatient and postanesthesia care unit (PACU) visits were considered equivalent between the two groups and thus, negligible. Direct primary procedure costs included supplier prices for disposable equipment. Costs related to installation and maintenance were not included, nor were physician fees. The complication rate and associated costs of blood transfusions were negligibly low in both groups and thus excluded. All surgeries, primary procedure and reoperation, included an institution-specific OR rate of $62/min. To equalize, only OR times for prostate volumes 80 to 100 cc were used to calculate the average OR time for each primary procedure (Supplementary Table S2).
Statistical methods
A decision analysis model was constructed to compare costs over a 1-year period using observed frequencies of complications from our dataset. Long-term cost estimates were extrapolated over a 10-year period using a Markov model and using a reoperation rate of 12.3% for TURP patients and 2.6% for LEP based on reported rates in the literature. 19,20 Decision tree and Markov model were performed with TreeAge 3.5 (TreeAge Software, Williamstown, MA). Student's t-test and Wilcoxon signed-rank test were used to compare the central tendency of continuous variables for normal and non-normal distribution, respectively. Fisher's exact test was used to compare the distribution of categorical variables. A p-value <0.05 was considered statistically significant. All statistical tests were two sided.
Results
Our dataset included a total of 308 patients (194 TURP; 114 DiLEP). Twenty-one patients were excluded from the dataset due to prior prostate cancer diagnosis or BPH surgery. Data were collected at 1, 3, 6, and 12-month follow-up periods. Twelve-month follow-up data were available for 119 patients. Table 1 shows demographic and clinical information of the patients in both groups. Compared with the TURP group, the DiLEP group had significantly larger initial median prostate sizes [92 IQR (65.2–115) vs 65 IQR (48–88); p < 0.0001] and more elevated prostate-specific antigen [4.0 IQR (1.9–5.6) vs 2.7 IQR (1.2–5.4)]. DiLEP patients were more likely to have a median lobe (77% vs 57%, p = 0.001).
Demographic and Preoperative Characteristics of the Study Cohort
Unpaired t-test (for normally distributed variables).
Fisher's exact analysis.
Wilcoxon rank-sum test (for non-normally distributed variables).
ASA = American Society of Anesthesiology (Physical Status Classification System); BMI = body mass index; CIC = clean intermittent catheterization; DiLEP = diode laser enucleation of the prostate; IPSS = international prostate symptom score; IQR = interquartile range; PSA = prostate-specific antigen; PVR = postvoid residual; Qmax = max velocity flow rate; SD = standard deviation; TURP = transurethral resection of the prostate.
Initial DiLEP operative costs were greater than TURP, approximately $13,242 vs $10,071, respectively (Supplementary Table S3). For patients with 80 to 100 cc initial prostate volumes, the median DiLEP operative time was nearly double the median TURP operative time (128 minutes vs 63.5 minutes; p < 0.0001). However, DiLEP patients had more same-day discharges than TURP patients (46% vs 0%; p < 0.0001).
Tables 2 and 3 show complications rates and frequency-weighted costs for DiLEP and TURP, respectively. Over a 1-year period, DiLEP patients had a lower rate of emergency department presentations [5 (4.4%) vs 17 (8.8%); p = 0.17] and significantly lower rate of reoperations [1 (0.9%) vs 11 (5.7%); p = 0.036]. These findings are consistent with the literature examining the long-term reoperation rates for TURP vs laser enucleation.
Diode Laser Enucleation Of The Prostate Complications
Includes inpatient admission for treatment of acute urinary retention, urinary tract infection, blood transfusion.
Includes longer initial admission due to additional clot and fulguration procedure.
Reoperation under general anesthesia for late-onset postoperative urethral stricture.
LOS, length of stay; SDD, same-day discharge.
Transurethral Resection of the Prostate Complications
Includes inpatient admission for treatment of acute urinary retention, urinary tract infection, urosepsis (non-ICU management).
Includes longer initial admission due to arrhythmias, blood transfusions, vasovagal episode.
Reoperation under general anesthesia for late-onset postoperative urethral stricture and bladder neck contractur.
Figure 1 shows the decision analysis for 1 year postoperatively. On a per-patient basis, DiLEP and TURP had average costs of $13,665 and $11,777, respectively. This represents an estimated savings of $1,888 per patient receiving TURP after 1 year. Figure 2 shows the 5-year Markov model extrapolation, assuming a reoperation rate of 12.3% for TURP patients and 2.6% for LEP patients. Reoperations include any corrective procedures requiring general anesthesia. Figure 3 shows the absolute and relative costs of DiLEP relative to TURP initially and extrapolated up to 10 years postoperatively. TURP and DiLEP have nearly equivalent costs at 8 years postoperatively. By 10 years, DiLEP has approximately $664 savings over TURP on a per-patient basis.
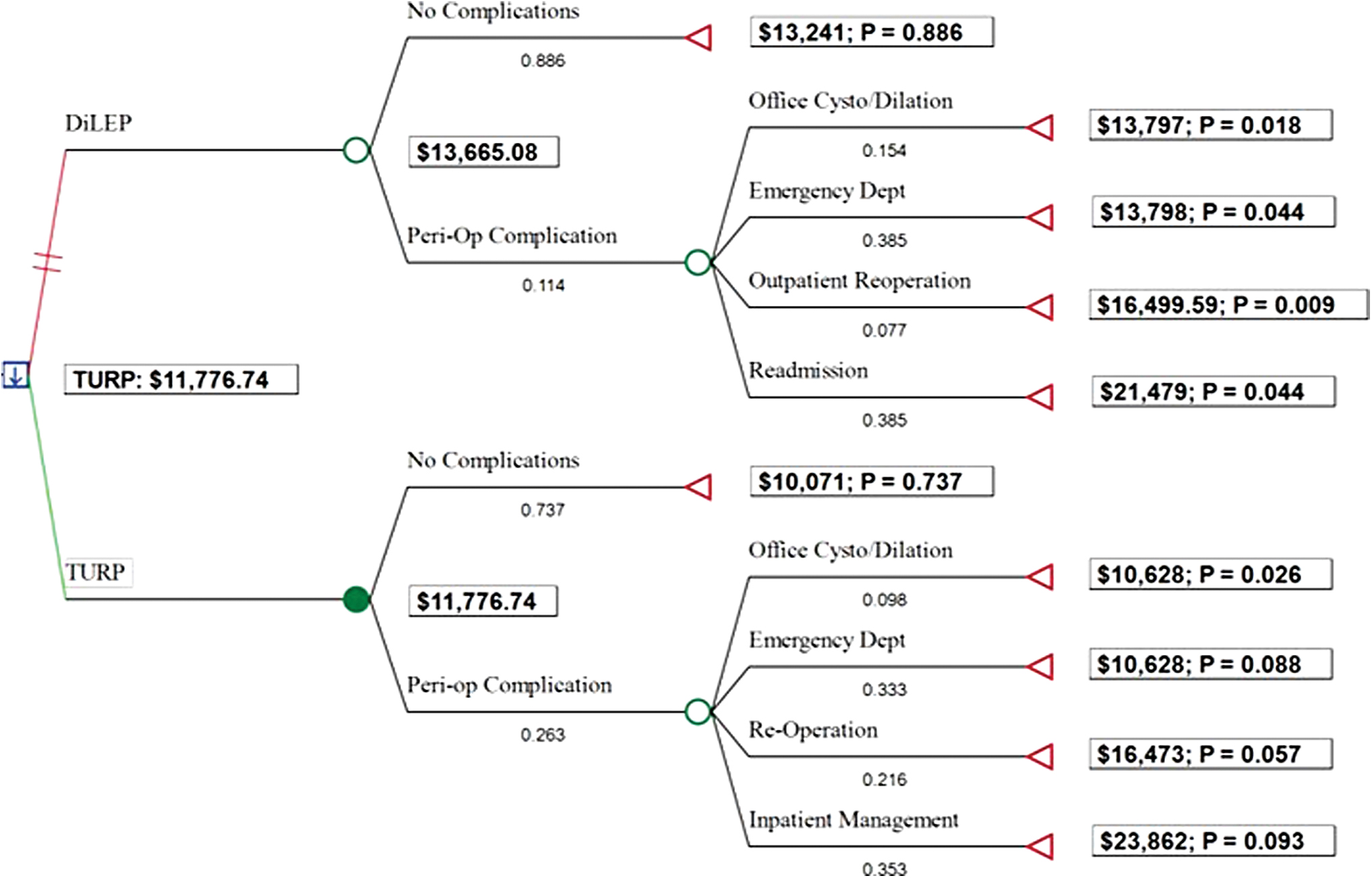
One-year Decision Tree Analysis for Surgical Management of BPH. Frequency of complications (p) observed in our institution's retrospective review were used to calculate weighted costs of complications in the 1-year postoperative period. BPH, benign prostatic hyperplasia. Color images are available online.

Five-year Decision Tree Analysis for Surgical Management of BPH. Markov analysis used to generate extrapolation of costs over 5 years based on 5-year reoperation rates reported in the literature (TURP 12.3%; LEP 2.6%). LEP, laser enucleation of the prostate; TURP, transurethral resection of the prostate. Color images are available online.
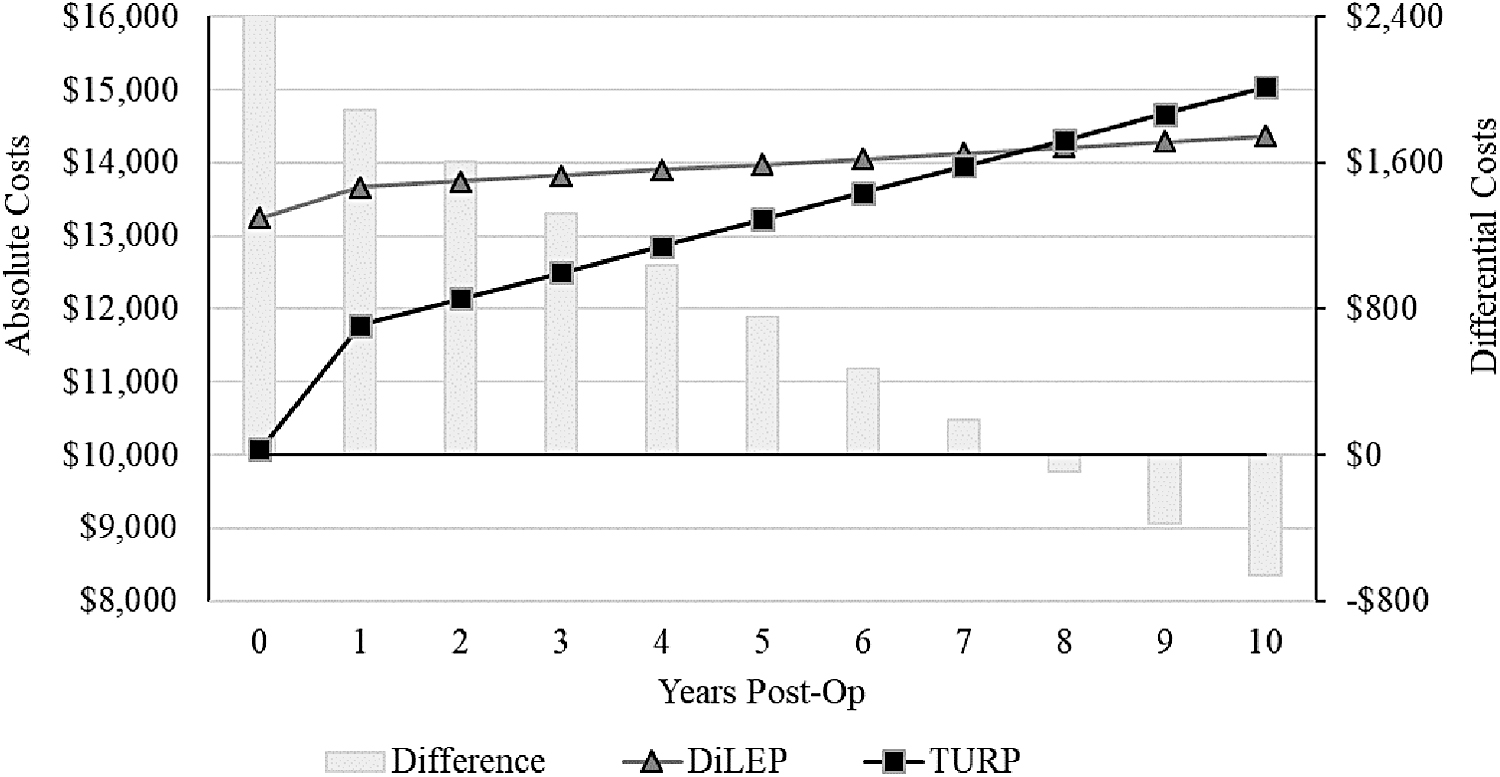
Extrapolated absolute and differential costs for DiLEP and TURP over 10 years. Markov analysis used to generate extrapolation of costs over 10 years based on 5-year reoperation rates reported in the literature (TURP 12.3%; LEP 2.6%). The blue horizontal line represents cost equivalency (cost of DiLEP − cost of TURP = 0). Negative values on the secondary y-axis indicate a per-patient cost savings for DiLEP relative to TURP. DiLEP, diode laser enucleation of the prostate.
Discussion
DiLEP is noninferior to TURP for surgical treatment of BPH. DiLEP is a viable option for all initial prostate sizes, has a higher rate of same-day discharges, and a lower risk of bleeding. 3,21 However, the technical complexity and associated learning curve, as well as the additional morcellation step, drive longer operative time. These longer operative times and possible loss of productivity (i.e., fewer procedures performed overall), in addition to greater upfront costs related to the purchase and installation of equipment for DiLEP, contribute to the expense which is often cited as a reason to prefer TURP as the gold standard. 7,22 Previous studies examining the cost effectiveness of TURP to LEP are mixed: some favor TURP, whereas others report a recuperation of initial operative costs with LEP owing to lower reoperation rates. 16,17,23 The multiplicity of laser modalities—including holmium, thulium, KTP/Nd:YAG, Nd:YAG, diode, and green light—contribute to a scant literature base that specifically examines novel forms of laser, such as DiLEP. 24 Finally, many of these studies have small sample sizes and short follow-up periods, failing to capture late-onset complications requiring reoperation. 16
Early complications following surgery for BPH include acute urinary retention, urinary tract infection, and bleeding. Long-term complications include reoperation for urethral strictures or bladder neck contractures, or a regrowth of prostatic tissue requiring a repeat resection. In the literature, 5-year reoperation rates post-TURP range from 3% to 15.5%. 19,25,26 Five-year reoperation rates post-LEP range from 0% to 5.3%. 7,27 A large study by Madersbacher and colleagues of 20,671 men who underwent TURP in Austria between 1992 and 1996 found a 5-year reoperation rate of 12.3%. 28 The surgical retreatment rate at 5-year follow-up for BPH regrowth, specifically, ranges from 5% to 17.7% for TURP and laser photovaporization of the prostate, but 0% to 1.4% following HoLEP. 14
The current study examined the tradeoffs between DiLEP and TURP. Similar to previous studies, we observed a significantly longer operating time for DiLEP (Supplementary Table S2). However, we also observed a higher rate of same-day discharges and a lower complication rate. The lower complication rate among the DiLEP group compared with the TURP group included approximately half the rate of emergency department visits in the acute follow-up period, and a significantly lower rate of reoperation at 1-year follow-up.
Strengths of this study include a large number of patients from a diverse population treated with a novel modality, DiLEP, for which there is little preexisting evidence. Moreover, 1-year follow-up data points were available for nearly 40% of patients, and 5-year projections were calculated using Markov modeling. These data further inform the tradeoffs among TURP, DiLEP, and patient selection based on initial prostate size to minimize additional OR time. Our findings may encourage urologists to perform prostate resection with the underutilized 1470 nm diode laser, enabling them perform resection of the prostate as an outpatient procedure, offering a cost-effective, portable alternative to holmium laser.
Limitations include those inherent to retrospective reviews and nonrandomized studies. A number of assumptions are built into the cost estimates, including a negligible difference in costs incurred in outpatient and PACU. This study did not track costs from drug therapy, nor outcomes related to if, and when, patients needed to resume drug therapy for lower urinary tract symptoms. Costs related to equipment installation and maintenance were not included, nor were estimated costs from lost productivity (i.e., fewer total procedures performed in an OR) secondary to longer procedure times with DiLEP. The fragmented nature of a multipayer system in the United States presents inherent challenges in generating accurate and generalizable cost estimates. Cost data were generated from multiple sources and may not reflect exact costs billed by our institution. Lastly, TURP was performed by multiple surgeons and DiLEP was performed by one surgeon. We did not control for the degree of experience among surgeons. Future studies would benefit from economic analyses that include cost estimates for lost productivity and prospective pre- and postoperative prostate sizing to compare the degree of resection and possible correlations with the length of the procedure.
With regard to cost analysis, while the short-term costs suggest superior cost effectiveness with TURP, long-term economic projections favor DiLEP. However, financial modeling is only one small, simplified consideration in the larger scheme of clinical decision making, and based on the aforementioned clinical data, DiLEP shows superior short-term outcomes.
Conclusions
Our study demonstrates that despite greater upfront costs and longer operating times, DiLEP is a more cost-effective option than TURP at 10 years postoperatively in properly selected patients, resulting in $664 savings per patient. This effect is chiefly due to a higher rate of same-day discharges and a lower rate of complications and reoperations. Further large sample studies tracking prospective costs, complications, and outcomes over longer periods are needed. As the technology and expertise of urologists offering DiLEP improves, it is likely that shorter operative times and better outcomes will continue to drive the cost effectiveness of this procedure, resulting in earlier recuperation of costs.
Footnotes
Author Contributions
All authors listed below have reviewed and approved of this article before submission. This article has been submitted solely to this journal and is not published, in press, or submitted elsewhere.
A.I.: Conducted data collection from electronic medical records to build patient database used for the project. Contributed to study concept and design. Collected primary cost information. Drafted article, designed Tables and Figures.
S.H.B.M.: Conducted data collection from electronic medical records to build patient database used for project. Contributed to study concept and design. Performed statistical analyses for clinical information.
M.U.: Contributed to study concept and design. Conducted economic analysis and produced relevant Figures. Provided study and editorial feedback.
M.K., D.W., and R.B.: Performed surgeries. Provided study feedback.
S.W.: Performed surgeries. Contributed to study concept and design. Provided study and editorial feedback. Oversaw project.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.