
Abstract
Background:
Suction during robotic surgery has traditionally been performed by a bedside assistant. Adequately skilled assistants are not always available. We assessed a purpose-designed robotic surgeon-controlled suction catheter for efficiency and safety by comparing with historic cases of suction controlled by a dedicated bedside assistant using standard rigid laparoscopic suction.
Methods:
Beginning in February 2019, the remotely operated suction irrigation (ROSI) device was used in all robotic prostatectomy procedures, which is a flexible suction catheter manipulated by the surgeon such that a bedside assistant is never required for suction. The initial 300 consecutive cases performed with ROSI were compared with the 300 immediately previous procedures using bedside assistant suction (BAS).
Results:
There were no statistically significant differences between groups in age, body mass index, American Anesthesiologist Association score, prostate specific antigen, or pathologic stage. Lymph node dissection was performed in all 600 patients. All 300 ROSI cases were completed without requiring switching to BAS. Estimated blood loss (102.7 vs 120.2 mL, p = 0.001) and operative time (156.1 vs 149.3 minutes, p < 0.001) were slightly lower in the ROSI group. There was no statistical difference in the 90-day complication rate (Clavien ≥III) between groups, with both having 3% of patients readmitted or seen in the emergency department within 90 days of surgery.
Conclusion:
Surgeon-controlled suction allowed more surgeon autonomy without a negative impact on efficiency or safety issues requiring “bailout” suctioning by the bedside assistant whether urgent or otherwise. Robotic surgeons without access to skilled bedside assistants should consider suctioning for themselves not unlike the norm for many laparoscopic surgeons.
Introduction
Since the advent of robotic surgery over two decades ago, technological advancements both in robotic platforms and in ancillary devices have emerged to perform safer and more efficient procedures with positive impacts on operative and postoperative outcomes. 1,2 Many such improvements, such as the addition of the fourth robotic arm, robot-controlled ultrasound, and robotic stapling, have primarily enhanced surgeon autonomy over the surgical field. 3 –5
Suction and irrigation during robotic surgery have traditionally been performed by the bedside assistant that requires a skilled assistant and synchronization of the surgical team that can take hundreds of cases to develop. 1 Not all surgeons have well trained or consistent bedside assistants such that the ability of the surgeon to suction independently could provide a benefit when resources are limited.
We explored this feasibility by adopting routine use of a purpose-designed robotic surgeon-controlled suction catheter and evaluated potential efficiency and safety issues by comparing with historic cases using traditional laparoscopic rigid suction controlled by a dedicated bedside assistant.
Methods
Beginning in February 2019, the remotely operated suction irrigation (ROSI) device was used in all robotic prostatectomy (RP) procedures performed by a single surgeon (R.A.) (Fig. 1). Bedside assistance was performed by either a physician's assistant associated with our practice or one of three nurses trained in surgical first assisting who work with all surgeons at our hospital across surgical specialties. Bedside assistants were exclusively used to change robotic instruments and introduce and remove sutures such that the surgeon worked autonomously otherwise. Per our routine for several years, all clipping was performed by the surgeon using the robotic clip appliers, all retraction with the fourth robotic arm, and once ROSI was adopted, all suction was performed by the surgeon as well.
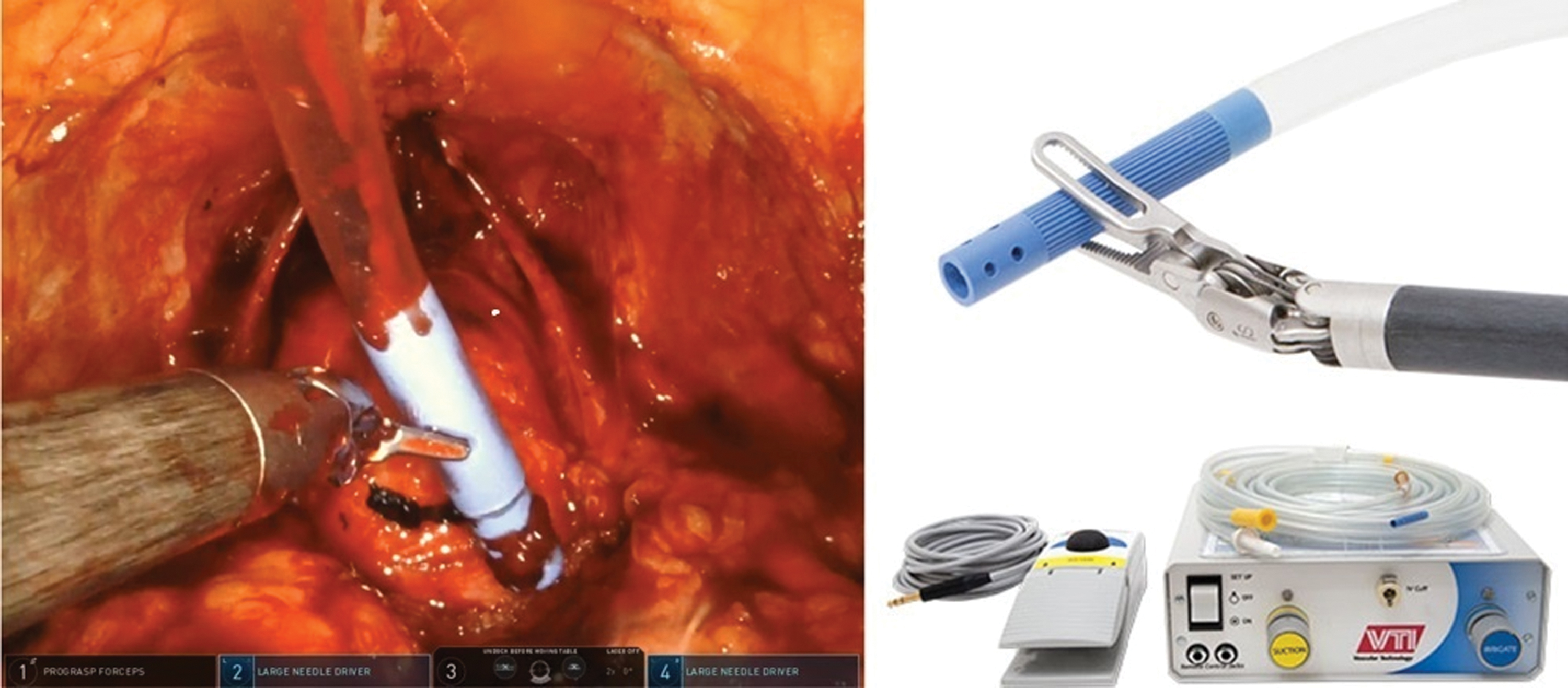
Robotic suction catheter (upper right), control box, and foot pedal for activation of suction/irrigation (lower right), and while in use during robotic prostatectomy procedure (left). Color images are available online.
The ROSI device consists of a flexible suction catheter placed through an assistant port for use by the surgeon when needed such that a bedside assistant is never required for suction. We used an 8 mm Airseal port (Conmed, Inc., Utica, NY) as our single assistant port to house the ROSI catheter so that we could use an ultralow pneumoperitonuem pressure of 6 mm Hg per our routine. 6 The ROSI device includes a foot pedal to activate suction or irrigation, but with Airseal insufflation we set the ROSI catheter to be suctioning at all times (to eliminate the foot pedal) without losing insufflation pressure. This modification was designed to provide constant smoke evacuation for visibility 7 and availability of suctioning of fluids at any time by the surgeon simply by moving the suction catheter to the desired location. The ROSI catheter was only removed when the port was needed to introduce needles or a specimen bag.
We analyzed our prospectively maintained database with IRB approval to determine whether using ROSI during RP had any effect on intra- and postoperative outcomes. The initial 300 consecutive RP cases performed with ROSI were compared with the 300 immediately previous procedures using the traditional rigid laparoscopic suction catheter controlled by the assistant. The traditional suction equipment included a reusable rigid metal suction catheter connected to a widely available disposable battery-powered suction/irrigation tubing set (Stryker, Kalamazoo, MI).
Operative and postoperative outcomes measured included estimated blood loss (EBL), operative time (OT), transfusion rate, length of stay (LOS), and complications.
Differences between groups were calculated using the chi-square or exact Fischer test for categorical data and the Student's t-test for continuous data. Statistical significance was determined based on a two-sided p-value of <0.05 (SAS Enterprise version 7.15, Copyright©2017; SAS Institute, Inc., Cary, NC).
Results
There were no significant differences in preoperative characteristics between groups including age, body mass index, prostate specific antigen, prostate volume, and American Anesthesiologist Association score (Table 1). The mean OT in the ROSI group was shorter than in bedside assistant suction (BAS) group (149 vs 156 minutes, p < 0.001). There were no intraoperative complications in either group, and in no cases was there a need to switch from ROSI suction to BAS. EBL was slightly higher in BAS (120 vs 103 mL, respectively, p < 0.001), but there were only 2 transfusions out of 300 patients in the BAS group (Table 2).
Preoperative Characteristics
ASA = American Anesthesiologist Association; BAS = bedside assistant suction; BMI = body mass index; PSA = prostate specific antigen; ROSI = remotely operated suction irrigation.
Perioperative Outcomes Comparing Remotely Operated Suction Irrigation and Bedside Assistant Suction Groups
EBL = estimated blood loss; LOS = length of stay; OT = operative time.
As per our routine since 2016, all patients were given the option to be discharged the same day as their surgery. 8 Of the 300 patients in each cohort, 227 ROSI and 160 BAS chose to go home the same day of the surgery (76% vs 53%, respectively, p < 0.0001) for a mean LOS of 0.2 vs 0.5 days, respectively. Eight patients in the BAS group (2.7%) and nine patients in the ROSI group (3%) visited the emergency department within 30 days for the following reasons: abdominal pain, shoulder pain, chest pain (noncardiac), cellulitis, constipation, urinary retention, deep venous thrombosis, and infected lymphoceles that were percutaneously drained. Six patients were readmitted in each group. Overall three patients required reoperation during the first 24 hours after RP, one in each group for clot evacuation and one in the BAS group for active bleeding.
Discussion
Robotic surgery has progressively evolved since its inception roughly two decades ago with new technology and devices that have facilitated more precise and safer procedures, and, subsequently, improvements in operative and postoperative outcomes. 2,9 Many of these advances have afforded the surgeon more direct control over the operation with faster execution of required tasks minimizing interruptions to workflow. 1 We had already gravitated toward more surgeon autonomy during RP by surgeon clipping using the robotic clip appliers and all retraction using the robotic fourth arm without relying on the assistant, but with adoption of the ROSI, this was extended even further to almost complete autonomy short of instrument changes and introduction of needles.
The suction–irrigation systems routinely used by most surgeons in robotic surgery are borrowed from laparoscopy and have not changed in decades. Presently, traditional systems use rigid suction cannulas that make access to some narrow spaces difficult while also demanding good communication between surgeon and a skilled bedside assistant. 10,11 An articulating robotic instrument for suction was introduced for the da Vinci Si robot in 2013 with the same instrument also currently available on the Xi robot, but there has not been any significant adoption most likely because this occupies one of the four robotic arms that could be used for other instruments.
Beginning in February 2019, we adopted ROSI as the suction device for all our RPs without exception. The motivation for this initially was to prepare for using ROSI in robotic single-port surgery to avoid need for adding an additional port for the bedside assistant for suction and other tasks. Although we began using ROSI before obtaining the da Vinci SP robot (Intuitive Surgical, Inc., Sunnyvale, CA) and without knowing what to expect, surgeon preference for ROSI over BAS was immediate and became our standard routine.
Although one criticism of using ROSI might be that having the surgeon responsible for suctioning might prolong the operation as compared with a bedside assistant who can suction while the surgeon continues to operate, we did not find this to be the case. In our initial 300 ROSI cases, OT was actually slightly shorter than the previous 300 cases performed using conventional suction. Although counterintuitive, it is possible that this may be related to eliminating the delay between the surgeon's communicated desire for suction and its execution by the assistant. Sexton et al. analyzed assistant anticipation as a measure of efficiency during 12 RPs and found that the mean occupied time in requests was 20% of total OT. The mean anticipated response time was 5.3 seconds while nonanticipated requests took 25.6 seconds. 3
Even if the assistant were perfectly able to anticipate the surgeon's need for suction, the assistant would also need to predict when the surgeon does not want suction so as to prevent interference that can impact the flow of the operation. Allers et al. evaluated workflow during RP and categorized suction as an unavoidable procedure-specific interruption, which occupied 10% of the total interruptions of their procedures. 1
In these ways, ROSI may still match or outperform even the most skilled assistant in efficiency by both eliminating communication delay when suction is desired and removing interference when suctioning is not desired.
During our current patient series, bedside assistance was rendered by a dedicated physician assistant or one of three surgical first assistants in our department (or a robotics fellow on rare occasions), all with extensive experience in robotics, but even with skilled bedside assisting, ROSI was no less efficient and invariably preferred by the surgeon regardless of who was available to assist. Whether surgeon-controlled suction increases surgeon cognitive workload and fatigue was not evaluated in our study, but subjectively, the surgeon involved in this study preferred the autonomy of ROSI and perceived it as less fatiguing such that ROSI was adopted uniformly for all robotic surgeries and continues to be used by the surgeon in all procedures.
An additional potential criticism might be that having the surgeon responsible for suction might lead to more bleeding or inability to address bleeding as quickly as when an assistant can suction sudden or constant bleeding. Once again, we did not find this to be the case as blood loss was slightly lower in ROSI cases. This may either be because surgeon-controlled suctioning facilitated quicker identification and control of bleeding (as subjectively reported by the surgeon) or because of less unnecessary suctioning whereby the surgeon suctioned only the bleeding that was obscuring view rather than the overzealous suctioning that a bedside assistant can be known to do if trying to remove all blood whatsoever from the field.
The introduction of ROSI has been particularly useful during the adoption of the da Vinci SP (single port) robot, since all our SP surgeries are performed without an additional port (+1 technique) for the assistant. As expected, the learning curve of the SP platform has showed longer OT. Despite this, we still noticed an improvement in OT with ROSI such that our improvement in OT is likely underestimated by the confounding additional SP platform that was introduced simultaneously. When we removed the 62 SP RP cases in this consecutive RP series regardless of robot type and considered only 300 consecutive multiport RP cases using ROSI, the mean OT and EBL were even more favorable for ROSI at 152 minutes and 96 mL. Consequently, even surgeons who have no plan to perform SP surgery may consider using ROSI for their standard RPs and particular if they do not have a skilled or consistent bedside assistant.
We routinely offer (not mandate) same-day discharge (SDD) as an option to all patients undergoing RP, and although we found a significantly higher rate of SDD in the ROSI group, we do not intend to suggest that this is due to ROSI. Since beginning to offer SDD in 2016, 8 our rate of SDD has increased over time such that this finding likely reflects the evolution of our surgical pathway for SDD as well as our adoption of SP RP wherein most patients opt for SDD. Since OT and blood loss were not greatly different between groups and complications were similar, it is unlikely in our opinion that ROSI alone would impact LOS.
Since the patient series evaluated in this study, we have more recently leveraged the ROSI and lack of need for an assistant for suctioning to eliminate the assistant port and routinely perform RP with four ports (Fig. 2). With this strategy, we place the ROSI through a 12 mm Airseal port alongside the robotic 8 mm port for the camera where eventually the specimen is extracted. This thereby avoids any ports through the rectus and may reduce the associated pain particularly when patients sit up from reclined position. Once we have a large enough series for review, we intend to investigate this as it may provide even more motivation for use of ROSI in RP.

Representative postoperative image after four-port robotic prostatectomy eliminating assistant port using robot-controlled suction catheter. Color images are available online.
Based on our experience, we have now adopted use of the ROSI not only for all RP procedures, but also in all types of robotic urologic surgery. To our knowledge, this is the largest series investigating ROSI use in urologic procedures and its safety and efficiency. Although our study is limited by its retrospective design and lack of randomization as well as only a single surgeon, this reported experience should warrant additional investigation and potentially adoption of this technology by surgeons willing and able to suction independently. Also, our study did not specifically measure cost, but it is important to note that the cost of the single-use ROSI suction catheters was no more expensive than the commonly used disposable suction–irrigation device we previously used with a reusable rigid metallic tip. Since ROSI did not adversely impact efficiency or safety in this series, it may be an ancillary device that contributes to the growing technology options in robotic surgery particularly for those surgeons or institutions lacking availability of a skilled assistant for every case.
Conclusion
Surgeon-controlled suction allowed more surgeon autonomy without a negative impact on efficiency or safety issues requiring “bailout” suctioning by the bedside assistant whether urgent or otherwise. Outcomes were at least as favorable as historical procedures in which experienced bedside assistants were present. Robotic surgeons and particularly those without access to skilled bedside assistants should consider suctioning for themselves not unlike the norm for many laparoscopic surgeons.
Footnotes
Acknowledgments
The authors thank Deborah Chervin for database maintenance and the OhioHealth Research Institute.
Author Disclosure Statement
Dr. Abaza receives financial support for educational programs from Intuitive Surgical, Inc. and Vascular Technologies, Inc.
Funding Information
The authors report no funding was obtained for this study.