
Abstract
Purpose:
Extracorporeal shockwave lithotripsy (SWL) results in a lower stone-free rate (SFR) for ectopic kidneys when using the standard technique, directing the shock wave from the same side of the stone; however, this may not be the optimal approach when the ectopic kidney is located more medial and anterior than the normally positioned kidney. Thus, contralateral coupling where waves come from the opposite direction may result in a better outcome. We tested the feasibility and outcome of contralateral coupling during SWL for stone in ectopic kidney.
Materials and Methods:
We prospectively recruited 20 patients with simple renal ectopia, who presented with renal stones that were amenable for SWL in the period between 2014 and 2018 at outpatient clinic of urology department, Minia University. Patients received SWL in Private Nile SWL Center were included to benefit from the ability of the electromagnetic SWL lithotripter. We did SWL in a supine position, and then contralateral coupling was performed from the opposite side of the affected kidney, rather than using the standard ipsilateral coupling approach. The SFR and various pre-, intra-, and postprocedural SWL variables were assessed, including stone characteristics, body habitus, shock wave numbers, and auxiliary measures. Count and percentages were calculated.
Results:
The mean stone radius was 14.7 mm with a mean S.T.O.N.E. (size, topography, obstructions, number of stones, and evaluation of HUs) of 9.6 points. Effective SWL was achieved in 80% of cases, 65% of them were stone free with effective single SWL session in 56% of cases. Hematuria, infection, and obstruction occurred in 50%, 20%, and 15% cases, respectively. One case required ureteral stent insertion.
Conclusions:
SWL applied through contralateral coupling is feasible, with comparable safety profile to the standard ipsilateral approach. Better SFR was achieved with the contralateral approach, in fewer sessions. However, the recruitment of more cases is necessary.
Introduction
Published data regarding the optimal management of kidney stones in patients with ectopic kidneys remain limited. 1 Data concerning the stone-free rate (SFR) after extracorporeal shockwave lithotripsy (SWL) applied to ectopic kidneys have demonstrated a good SFR that remains inferior to that for normal kidneys. 2,3 This difference is likely caused by variations in the anatomic perspective associated with the treatment of ectopic kidney, which represents a substantial challenge for SWL. Various modifications have been applied to focus the shock waves, either through anterior or posterior coupling, using different positions, ranging from the straight prone position, a semiprone position, lateral positions, and the pure supine position. 1,3 –7 However, versatile innovations made to the SWL machine, including the ability to change the direction of focus by rotating the cushion head, have advanced the available coupling mechanisms during SWL. 8 Previous studies examining SWL in ectopic renal stones have described using the standard SWL technique, applied from the ipsilateral side of the affected ectopic kidney, with limited exploration of different focus directions. 9 Based on a review of ectopic renal anatomy, we found that the ectopic kidney tends to be positioned more anteriorly and medially than normal kidneys, and the related pelvicaliceal system tends to project more toward the contralateral side. 10 Thus, we may benefit from the anterior rotation of the cushion, to focus the shock wave from the contralateral side. In this study, we attempted to determine the safety and feasibility of applying SWL from the contralateral side, to enhance the SWL outcomes for the ectopic kidney.
Patients and Methods
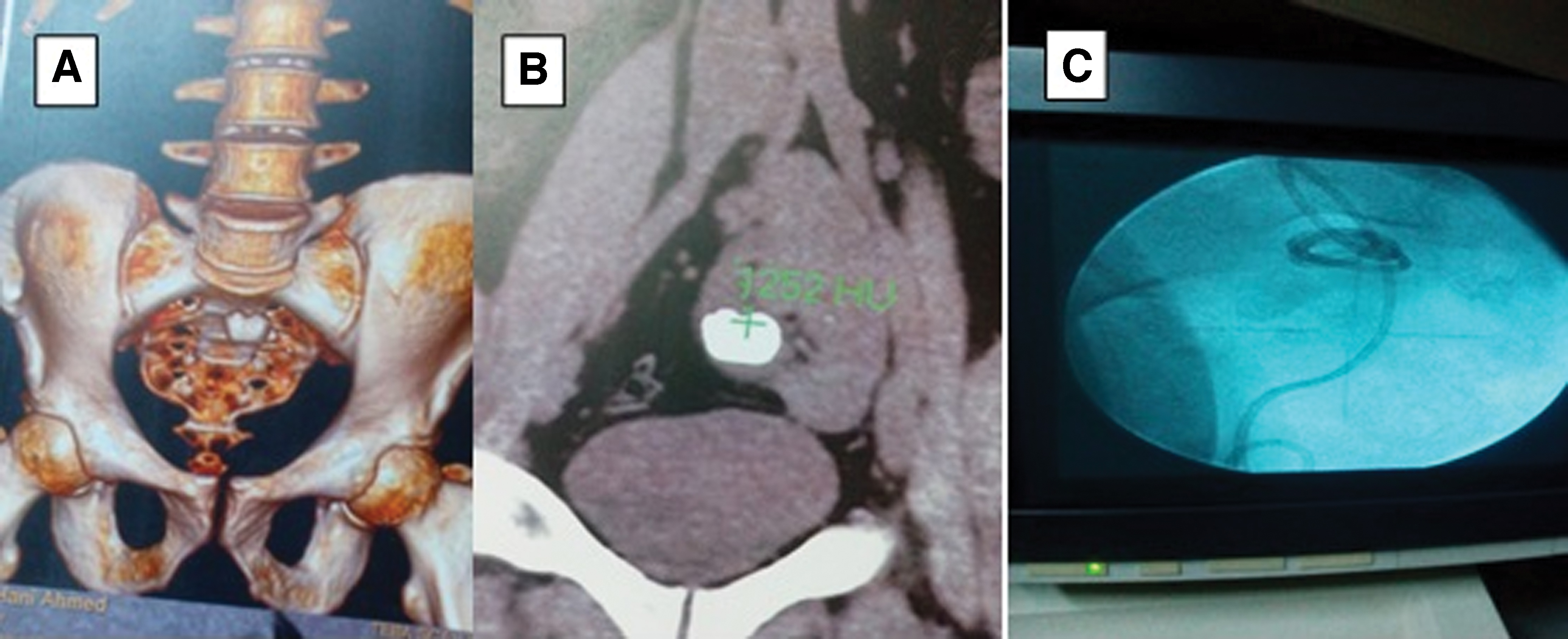
We prospectively included 20 patients with renal stone disease attendant at the outpatient clinic of urology department of Minia Urology and Nephrology University Hospital, between 2014 and 2018. Patients were assigned for SWL as the definitive management strategy for stones located in their anomalous kidneys. In this study, we included only patients with simple ectopic kidney, in either the iliac or sacral/pelvic region, based on positioning in preliminary CT scans. Patients with stone diameters >2.5 cm and/or radiolucent stones were excluded from this study. We excluded kidneys that previously underwent operation or stenting or with a history of bilateral obstruction or only functioning kidney. Patients received a full clinical examination, to exclude the presence of diffuse abdominal distention, waist obesity, or organomegaly. Laboratory tests included complete blood count, prothrombin time and concentration, liver enzymes, and viral hepatitis C marker. Patients' abdomens were screened for the presence of organomegaly, using ultrasonography. Stone and kidney status were detailed through plain kidney, ureter, and bladder radiograph (KUB). Noncontrast CT was performed after preliminary examinations to determine the number of stones, the largest stone diameter, stone radius, and HU density. Patients received SWL in Private Nile SWL Center after well-informed consent about the procedure and the change of the direction of shock wave as a part of study. The day before SWL, patients were instructed to have a fluids and soft palatable carbohydrate only. To adsorb colonic gases, two activated charcoal tablets every 4 hours with cathartic drops (sodium picosulfate 7.5 mg) to allow for better observation, decrease intestinal distention and consequently potential injury. Patients were allowed fluid till 6 hours and water 2–4 hours before start of session. SWL was done under intravenous IV Midazolam. Session started with slow IV infusion over 2–3 minutes at a dose 150–350 mcg/Kg then maintenance was injected every 5 minutes at a 25% of the intial dose on signs of reawakening (maximally repeated twice). Stones were focused using a combination of 0° and 30° fluoroscopic planes. Power was gradually increased until the maximal tolerable voltage was achieved to adequately prime the stone for the shock wave, which was applied by an electromagnetic shock generator (Medipuls, Dornier Med Tech Systems; Dornier compact sigma modulator). The patients underwent SWL sessions in the supine position, with the cushion coming from the side contralateral to the stone that in case of a right-sided stone, the patient left side is the nearest to the arm of the cushion. The cushion was rotated to face the anterior surface of the patients' abdomen. An adequate amount of sonar jell was used as a coupling medium, and the patient was adequately coupled by filling the cushion. The stone was further localized by manipulating the table movement in different directions through different fluoroscopic planes (Fig. 1).

Male patient (32 years) with renal stone in ectopic right kidney.
Each session was limited to 3500 shock waves per session, at the maximum tolerable power. Then, the patient was transferred to the recovery room. Patients were allowed to return home after regaining full consciousness. All patients were prescribed an nonsteroidal anti-inflammatory drugs analgesic (Lornoxicam, 8 mg, twice daily) and an alpha-blocker (Tamsulosin, 0.4 mg caps, once daily). Patients were asked to continue ciprofloxacin 500 mg, twice daily. Patients were asked to return for follow-up weekly, at which time the response to SWL was determined using serial, digital, plain KUB imaging. Patients were advised to drink plenty of fluids and to expect mild (resolved within 48 hours) to moderate (resolved after >48 hours) hematuria and post-SWL pain episodes. Data collection was performed by a blinded investigator, who revised the patient's data, including age, date, number of sessions, body mass index, and stone characteristics, including S.T.O.N.E. (size, topography, obstructions, number of stones, evaluation of HUs) score and the calculation of stone burden, using Ackermann's formula. 11 Success was defined when complete clearance of stone occurs or residual fragment of <4 mm, 2 weeks after the third session. Complications, including post-SWL pain episodes, visual analog pain (VAP) score, urinary tract infections (classified as mild when resolved by oral antibiotics, moderate, necessitating IV antibiotics, or severe, if associated with hospitalization), hematuria, steinstrasse occurrence, obstructions, and auxiliary measures, were documented. The time to stone expulsion was defined as the time from the first session to the last change on follow imaging, in effective cases. The average time was determined by dividing the number of days by the number of sessions.
Statistical analysis
Data are reported as the mean ± standard deviation, median and range, or frequencies (number of cases) and percentages, where appropriate. To compare categorical data, the chi-square (χ 2 ) test was performed. Fisher's exact test was used when the expected frequency was fewer than five counts. Comparisons of numerical variables between the study groups were performed using the Mann–Whitney U test for independent samples, when comparing two groups, and the Kruskal Wallis test, when comparing more than two groups. All statistical calculations, except for calculating the power of the study, were performed using the computer program SPSS (Statistical Package for the Social Science; SPSS, Inc., Chicago, IL, USA), version 15, for Microsoft Windows.
Results
Our study included 20 patients with kidney stones in a single ectopic renal unit, of which 85% were men. The average age of our patients was 36 years (Table 1). A single stone was identified in 80% of cases, 70% of stones were on the right side, and the mean stone radius was 14.7 mm, with most stones (65%) between 5 and 10 mm, whereas the remaining 35% were >10 mm. The mean stone density was 954 HU, and most stones were between 750 and 1000 HU (60%). The stones were located in the pelvis in 35% of cases, followed by the upper calix in 30% of cases, with only two cases presenting a solitary lower caliceal stone. In 60% of cases, no backpressure changes were observed, whereas five cases presented Grade I–II hydronephrosis. The mean S.T.O.N.E. score was 9.6 after calculation of the stone burden, according to Ackermann's formula. In total, we performed 34 SWL sessions, with a mean number of 3400 shocks per session (Table 2). The mean VAP score was 4.6, for the most painful episode after any SWL session (Table 3). Severe obstruction in one patient was managed by ureteral stent placement then had a third SWL session but with significant residual fragment (Fig. 2). The mean number of days to stone expulsion was 33 days in the 16 cases with effective SWL in 80% of cases. First session success was achieved in 56% of cases (Table 4). Failure occurred in four cases, including one case with no response and three cases with clinically significant residual fragments (Table 4). When comparing the different patient and stone variables, we found that the stone burden, based on Ackermann's formula and the S.T.O.N.E. score, was significantly lower for effective cases than for failed cases (Table 5).
The only case with post-SWL obstruction and infection was treated with ureteral Double-J stent insertion and third SWL session was done but with significant residual fragment.
Patients Demographics
SD = standard deviation; SWL = extracorporeal shockwave lithotripsy.
Stone Characters, Measurement, and Shock Wave Criteria
S.T.O.N.E. = size, topography, obstructions, number of stones, evaluation of HU.
Complications
VAP = visual analog pain.
Stone-Free Rate and Time to Stone Expulsion
CIRF = clinically insignificant residual fragments; CSRF = clinically significant residual fragments.
Factors Affecting Outcome
On bivariate analysis, we found that stone burden and S.T.O.N.E. score were significantly lower in effective cases.
Statistically significant difference (p-value <0.05).
Discussion
Ectopic kidneys continue to present a challenge for all aspects of stone disease management, including percutaneous nephrolithotripsy (PCNL) and SWL, because of the more central renal position and abnormal relationships with other organs, intestines, and overlapping bone. 12 Thus, shock waves applied to ectopic kidneys were applied from in prone position when using older lithotripters. 13 Advancements in the technical properties of newly designed lithotripters have facilitated an anterior coupling, with the cushion in the supine position, usually from the ipsilateral side of the affected kidney. 14 However, the utility of new lithotripters, which allow the rotation of the cushion, enabled the focus of the shock wave to be directed from the contralateral side. This utility met our need to enhance SWL outcomes, particularly in cases of more anteriorly and centrally located ectopic kidneys. Thus, we conducted this study on 20 cases with simple renal ectopia, to determine the feasibility, safety and outcome of anterior coupling, while focusing shock waves from the contralateral side. Our findings provide a basis for further studies exploring the application of this new technique to more cases and various renal anomalies. Many modifications have been attempted to manage stones, including those in anomalous kidneys; SWL in a horse-shoe-shaped kidney was performed in the prone position. 9 A modified lateral position has been used for the management of cases with lumbar/iliac ectopic kidney. 2 Also, twin head SWL prototype that targeted stone from both direction was tested experimentally; one head targets stone from the posterior and the other one from the anterior surface but from the ipsilateral side. 15 Recently, an anterior approach was described for the management of upper ureteral stones while in the supine position, despite the absence of traditional bony obstacles. 16 Thus, positional modifications and the use of different directions for the shock wave appear to be key elements for the application of the SWL technique, which should be managed to suit different renal and stone topographies. 2 Contradictory reports exist regarding the frequency of anterior vs posterior coupling, in the prone or supine position, in cases of anomalous ectopic or low lying kidneys. The positioning above or below the sacroiliac joint was the only determining factor that could be used to focus shock waves through anterior or posterior approaches, despite the presence of broad iliac wings, which may block some, if not all, shock waves. 1 The presence of a stone just above the sacroiliac joint did not justify merely complete absence of bony obstacles that may hinder shock waves, such as the transverse process and related vertebrae. 17 The described disadvantages of anterior coupling include the presence of intestinal gas, which may hinder shock waves, theoretically, and the risk of intestinal injuries, although these are rarely reported. 18 In our study, we attempted to avoid these potential disadvantages through the adequate preparation of the intestines before SWL, good coupling, and precise focusing. None of our cases reported gastroIntestinal tract (GIT) bleeding or documented to have GIT complications.
In a previous study, effective outcomes after the application of SWL to anomalous kidneys were simply described as the absence of residual fragments. 19 SFR was documented in 82% when success was defined as the presence of clinically insignificant residual fragments (CIRF) <4 mm, 3 months after SWL, in 11 cases of stones (mean burden 3.2 cm) in ectopic pelvic kidneys. 4 In another series, SWL applied to ectopic kidneys resulted in a 57.2% complete SFR and a 35.7% CIRF rate, with a mean stone size of 2.35 cm. 1 Only one out of four cases subjected to SWL for stones in ectopic kidneys had a completely stone-free outcome, although two additional cases had residual fragment <5 mm. 20 In a retrospective review of 68 cases in which SWL was applied to anomalous kidneys, eight cases with ectopic kidneys presented a 37.5% SFR, and 50% had CIRF, whereas failure occurred in only one case, with a mean stone load of 2.1 cm. 6 The SFR in one of the largest ectopic kidney series (with a mean stone burden of 22 m), which included 29 renal units, reached 77% after SWL, with the presence of <10% stone burden in 10% of cases. 7 In our series, the SFR was 80%, including those with CIRF (three cases), which coincided with previous results. However, on further analysis, our results showed more stone-free cases (80% of effective cases) in fewer numbers of sessions. An SFR of 100% after SWL was documented in a study performed on 10 ectopic kidneys, but this study used more frequent sessions (mean number of sessions per case was 4.4, vs 1.7 in our series). Other studies described a minimum mean number of two sessions or more per renal unit. 1,3,4,6,7 Only one study, performed on two pelvic kidneys, reported an average of 1.5 sessions per patient, resulting in a 100% SFR. 21 The numbers of shock waves that are delivered to each patient are not constant and may be affected by many factors, including body configuration, power, and stone and kidney characteristics. 22 However, most shock wave frequencies per session ranged from 2000 to 3500 for most renal stones. 23 The mean number of shock waves in a single session was 3400 in our series, at an average power of 21.2 kV. Our results were similar to those described in other series, which reported 2850–3770 shock waves at powers ranging from 18.4 to 20 kV. 1,20,21
Excluding those patients in which SWL failed or required retreatment, CIRF were reported in 2 of 14 patients with renal ectopia, 4 6 of 13 ectopic renal units, 3 and 6 of 14 pelvic kidney cases. 1,7 The discrepancies among these results are caused by different endpoints for success, different follow-up imaging, and differences in the clinical impacts of residual fragments. However, the effects of these fragments on both short- and long-term regrowth rates were likely insignificant, as no recurrence was reported in seven cases with residual fragment after SWL. 7 Similarly, in our cases, residual fragment <4 mm were deemed clinically insignificant and did not result in near regrowth or require auxiliary measures.
Hematuria post-SWL was described as being transient or instant in almost all patients. 4,7 Similarly, 50% of our cases had mild-to-moderate transient hematuria; however, one case in our series experienced severe (not resolving) hematuria after SWL, accompanied by obstruction and infection. Obstruction and infection by steinstrasse occurred in three cases in our study, two of whom were managed actively, one by focal SWL and the other by Double-J stent insertion. Similar to our findings, no cases of obstruction/infection were reported in a previous study of ectopic kidneys, except for one case who underwent ureterorenoscopy for a ureteral stone fragment after SWL. 20 In another study, 2 of 14 patients with ectopic renal units developed post-SWL steinstrasse, which was managed with focal SWL, although one of them proceeded to the ureteroscopic removal of fragments. 2,4 In other studies involving renal ectopia, lower incidence of obstruction/infection and the need for post-SWL drainage were described; however, these studies only reported the total burden of complications and did not describe the numbers for each type of renal anomalies. 1,3,7 Only one patient with a large stone in a pelvic kidney, who developed large residual fragments and obstruction, required PCNL 6 similar to only one case of our series.
Our technique was found to be satisfactory, with a good success rate compared with standard SWL techniques, no major differences in post-SWL complications, auxiliary events, or retreatments. No intestinal or other abdominal organ injuries noticed. The recruitment of additional cases is ongoing, and we are examining additional types of renal anomalies, such as horse-shoe-shaped kidneys, to explore the utility of the contralateral SWL technique for other conditions.
Conclusions
The contralateral SWL approach is feasible in selected renal anomalies, particularly simple renal ectopia with amenable stones, with no additional adverse consequences compared with the standard ipsilateral SWL approach. In addition, contralateral SWL achieved a better SFR with reduced SWL session frequency. The further recruitment of both similar and different renal anomalies with stones remains necessary to continue evaluating this technique.
Ethical Considerations and Declarations
Our study was done on human participant after well-informed written consent at every step of management and at study inclusion, which is a basic requirement of the institutional review board either in governmental or private health care facilities, patients refused the study were announced for alternative choices and excluded from the study. Study was done according to ethical consideration of Helsinki declaration and the following declarations. Study done with commitment to local ethical committee namely Research Ethics Committee of Ministry of Health (IRB No. 0000687).
Consent for Publication
All patients who receive any medical service at our institute or specialized center sign in informed consent for publication of their data conditioned with the privacy and coding of their data. Also, any pictures or videos were taken after well-informed consent of the participant and used for research purposes and may be published online or in periodicals.
Availability of Data and Material
Data are available and ready to be shared.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.