
Abstract
Introduction:
Ureteral access sheaths (UASs) are frequently used during ureteroscopy (URS), but their use is not without potential risk. We investigated patterns of UAS use and associated outcomes across practices in Michigan within a quality improvement collaborative.
Methods:
The Michigan Urological Surgery Improvement Collaborative (MUSIC) Reducing Operative Complications from Kidney Stones (ROCKS) initiative maintains a web-based, prospective clinical registry of patients undergoing URS for urinary stone disease (USD). We analyzed all patients undergoing primary URS for renal and ureteral stones from June 2016 to July 2018 in the ROCKS registry. We determined rates of UAS usage across practices and associated outcomes, including 30-day emergency department (ED) visits and hospitalization, as well as stone-free rates. Using multivariate logistical regression, we determined the predictors of UAS use as well as outcomes, including stone-free rates, ED visits, and hospitalizations, associated with UAS use.
Results:
Of the 5316 URS procedures identified, UASs were used in 1969 (37.7%) cases. Stones were significantly larger and more likely to be located in the kidney in cases with UAS use. UAS use during URS varied greatly across practices (1.9%–96%, p < 0.05). After adjusting for clinical and surgical risk factors, UAS use significantly increased the odds of postoperative ED visits (odds ratio [OR] = 1.50, 95% confidence interval [CI] 1.17–1.93, p < 0.05) and hospitalization (OR = 1.77, 95% CI 1.22–2.56, p < 0.05) as well as decreased the odds of being stone free (OR = 0.75, 95% CI 0.57–0.99, p < 0.05).
Conclusions:
In the current study, UAS use during URS for USD was not associated with an increased likelihood of being stone free; moreover, it increased the odds of a postoperative ED visit and or hospitalization. Our findings demonstrate that UAS use is not without risk and should be employed judiciously.
Introduction
Survey data estimate that 11% of Americans will experience a stone episode during their lifetime. 1 Ureteroscopy (URS) is the most frequently performed surgical procedure to treat urinary stone disease (USD) in the United States. 2 Ureteral access sheaths (UASs) facilitate repeated entry into the collecting system, with several potential benefits, including improved operative visibility, the ability to extract stone fragments, a diminished infection risk owing to decreased intrarenal pressures, and potentially increased longevity of reusable ureteroscopes. 3 –5 These benefits likely explain the widespread adoption of UAS use during URS. 6,7
While there is little debate surrounding the benefits of UAS use, intraoperative insertion can result in unintended consequences with reported rates of significant ureteral injury in 13% of cases. 8 The late consequences of ureteral injury at the time of UAS placement are poorly defined. Although several small series, 9,10 including one prospective trial, 11 indicate that ureteral stricture rates are low following injury related to UAS placement, when a stricture does occur, this results in substantial morbidity for patients. 12 Less is known regarding the impact of UAS use on patient outcomes, namely unplanned health care encounters, which occur in as many as 15% of patients following URS. 13
In this context, we evaluated the impact of UAS use on health services utilization following URS. In particular, we assessed the frequency and predictors of UAS use within a surgical collaborative in addition to defining the relationship between UAS use and unplanned health care utilization following URS for USD. This information will allow for improved patient counseling regarding UAS use and help guide surgical decision-making with the aim to improve the quality of stone surgery.
Methods
Data source: Michigan Urological Surgery Improvement Collaborative
Michigan Urological Surgery Improvement Collaborative (MUSIC) was established in 2011 in partnership with Blue Cross Blue Shield of Michigan with the goal of improving the care of patients with prostate cancer. The Reducing Operative Complications from Kidney Stones (ROCKS) initiative was launched as a pilot in August 2016 with the aim to reduce emergency department (ED) visits following ambulatory stone surgery. The prospectively maintained ROCKS clinical registry includes 22 diverse academic and community urology practices representing more than 90% of practicing urologists in the state of Michigan. Each practice has a clinical champion who implements local quality improvement activities, with oversight provided by a centralized coordinating center. Detailed demographic, clinical, and operative data for patients undergoing shockwave lithotripsy and URS are entered into a web-based clinical registry by trained abstractors at each practice location. To ensure data quality, the coordinating center performs on-site data audits on a regular basis.
Study population
In this IRB approved study (no. IRB 2019-056), all patients over the age of 18 who underwent a primary URS for USD between June 2016 and July 2018 were eligible to be included in this analysis. We exclude bilateral procedures as well as staged procedures (ipsilateral procedure within 4 weeks of the initial surgery). For reliability purposes, we only included practices that performed at least 10 URS procedures during the study period.
Outcome measures
Our primary outcomes of interest were the associations between UAS use and unplanned health care encounters in the form of unplanned ED visits or hospitalizations within 30 days of the index URS surgery. We also assessed variation in the use of UASs at a practice level and the impact of UAS use on the stone-free rate (SFR) following URS. Stone free was defined as the absence of stone in the treated region on relevant postop imaging (Abdominal x-ray [AXR], renal ultrasound [US], or CT) within 60 days of the procedure.
Statistical analyses
Clinical and demographic characteristics of patients as well as postoperative outcomes were compared by UAS usage (yes vs no), using the chi-squared test for categorical measures and Wilcoxon rank-sum test for continuous variables. Among MUSIC practices with at least 10 URS procedures during the study period, practice-level variation in UAS use was assessed. To identify factors associated with the utilization of UASs, a mixed-effects logistic regression model was used. The model included, as predictors, patient's age, insurance type, comorbidity, body mass index (BMI), and gender, along with clinical characteristics such as urine culture, preoperative alpha-blocker usage, preoperative anticoagulation usage, preoperative antiplatelet medication usage, stone location/size, prestenting status, and the use of ureteral dilation. The model also included random intercepts for each MUSIC practice to account for within-practice correlation. To further evaluate the impact of UASs on unplanned health care encounters following URS and the SFR, separate mixed-effects logistic regression models were performed. Each model included an indicator for the usage of UASs as the primary predictor variable, along with all the aforementioned demographic and clinical factors as covariates. Each model also included practice-specific random intercepts to account for within-practice correlation. All the statistical analyses were performed using SAS 9.4, and statistical significance was set at 0.05.
Results
We identified a total of 5316 primary URS cases conducted during the study period. UASs were used in 1969 (37.7%) of these cases. Patient characteristics differed with respect to UAS utilization (Table 1). UAS use was significantly more common in older patients, those with more substantial comorbidity (Charlson comorbidity index [CCI] ≥2) and BMI >30, and those with public insurance. Additionally, rates of UAS use were higher if the patient had a positive preoperative urine culture. Patients taking any alpha-blocker at the time of surgery had lower rates of UAS use.
Patient Demographics and Clinical Characteristics of Patients Undergoing Primary Ureteroscopy With or Without Ureteral Access Sheaths
BMI = body mass index; CCI, Charlson comorbidity index; ED = emergency department; SD = standard deviation.
Of the 22 practices included in this analysis, there was substantial variation in UAS use across practices (1.9%–96%, p < 0.05; Fig. 1). This variation in UAS use persisted regardless of stone location (Fig. 2). Access sheath use by ureteral and renal stone location is listed in Supplementary Tables S1 and S2, respectively. Regarding renal stones, we found that increasing stone size was directly correlated with increased likelihood of UAS use, p < 0.05 (Supplementary Table S3).
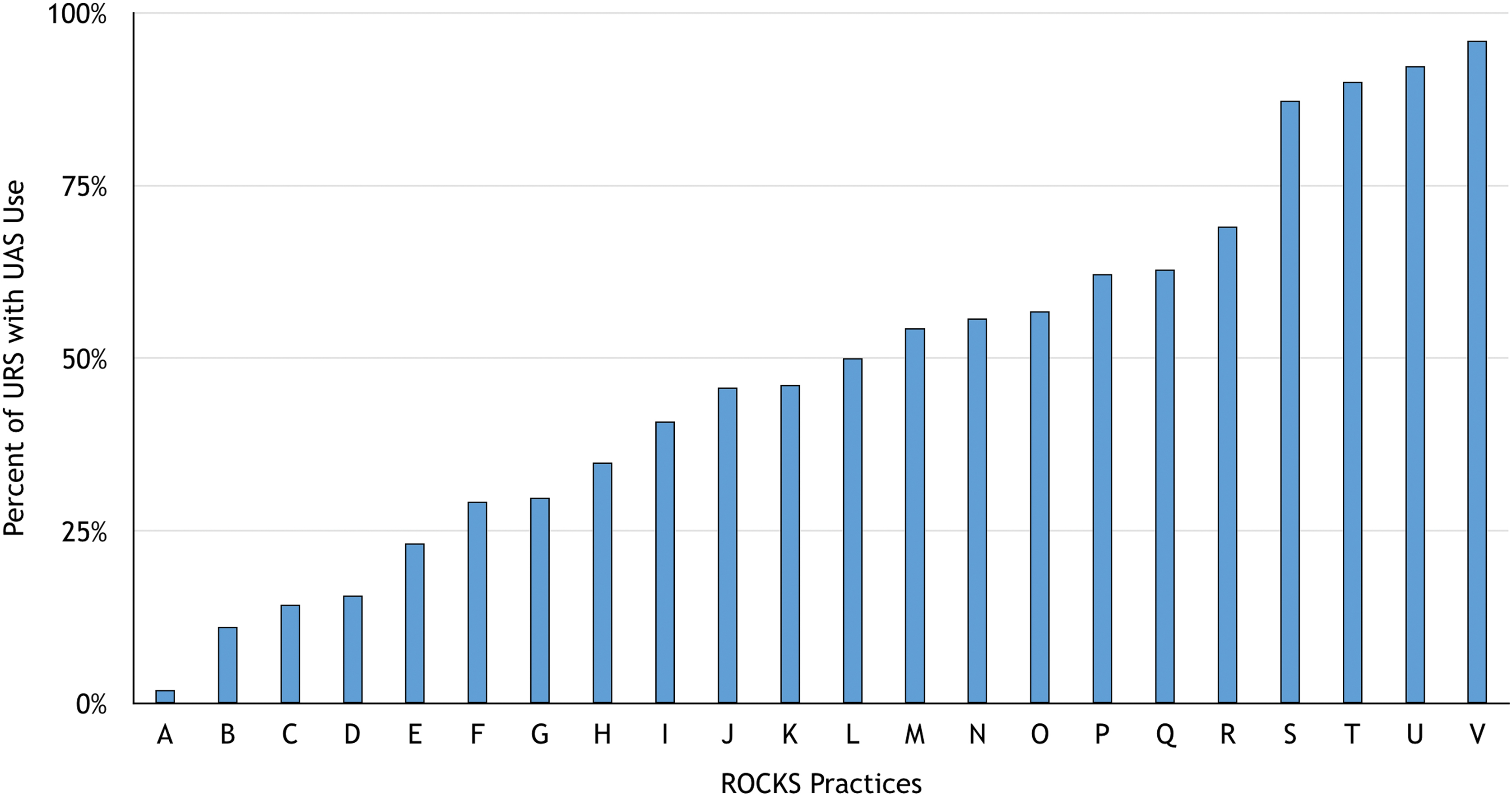
Practice variation in the frequency of ureteral access sheath use during ureteroscopy. Color images are available online.
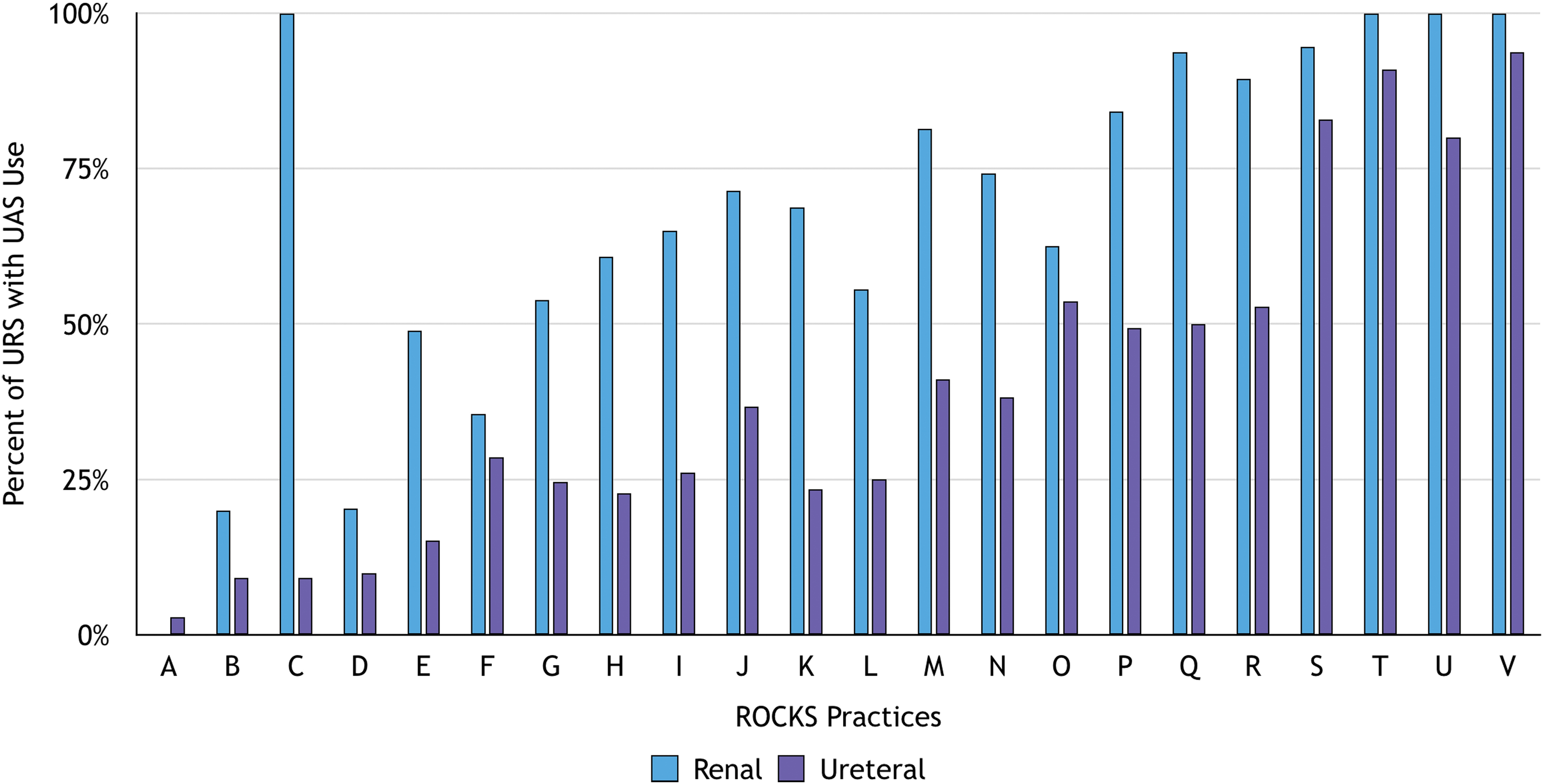
Practice variation in the frequency of ureteral access sheath use by stone location. Color images are available online.
On multivariable analysis, controlling for practice variation, several factors increased the odds of UAS use, including increased comorbidity, male gender, increased stone size, renal stone location, presence of ureteral stent before URS, and ureteral dilation during URS (Table 2).
Multivariable Model Assessing Odds of Ureteral Access Sheath Use
CI = confidence interval; OR = odds ratio.
Unadjusted rates of ED visits (10.2% vs 8.0%, p < 0.05) and hospitalization (4.7% vs 3.3%, p < 0.05) differed between those patients in whom a UAS was and was not used, respectively. After controlling for patient- and practice-level differences, those in whom a UAS was used had increased odds of an ED visit (odds ratio [OR] = 1.50, 95% confidence interval [CI] 1.17–1.93, p < 0.05) and hospitalization (OR = 1.77, 95% CI 1.22–2.56, p < 0.05) relative to those without UAS use. Using this multivariable model, we did find that prestenting decreased the odds of an ED visit (adjusted OR = 0.68, 95% CI 0.52–0.88, p < 0.05). Stent placement at the time of surgery was not found to be significantly associated with ED visits (adjusted OR = 1.14, 95% CI 0.87–1.50, p = 0.3) (Table 3).
Multivariable Analyses Assessing Odds of Emergency Department Visit, Hospitalization, and Stone-Free Status in Patients Undergoing Ureteroscopy With or Without Ureteral Access Sheath Use
UAS = ureteral access sheath.
Regarding time to ED visit or hospitalization, ED visit rates differed between UAS and non-UAS groups. Median ED visit in patients with UASs was observed on postop day 3 (interquartile range [IQR] = 2–7) vs postop day 5 (IQR = 2–11), p < 0.05, for patients without UASs. Those whose surgery did not include UASs were hospitalized on median day 4 (IQR = 2–7) and those with UASs were hospitalized on postop day 5 (IQR = 2–9), p = 0.4041. The most common reasons for ED visits were pain (48%), followed by “other” (38.0%), and urinary tract infection/hematuria (21.5% each) (Supplementary Table S4). It is worth noting that some patients may have more than one reason recorded for the ED visit.
Postoperative imaging was available for 47.6% of patients to assess SFRs. Abdominal X-ray was the most common modality used (55.0% of patients), followed by US (21.9%) and CT (11.1%). On multivariable analysis, UAS use was associated with lower odds of being stone free (OR = 0.75, 95% CI 0.57–0.99, p < 0.05) relative to those where a UAS was not used.
Discussion
In this pragmatic evaluation of practice patterns within the state of Michigan, we report several interesting findings. First, access sheaths are commonly used (37.7% overall), with a surprising degree of variation in the frequency of UAS use depending upon the practice. Factors associated with UAS use included increased comorbidity, male gender, increased stone size, renal stone location, and presence of ureteral stent before URS, as well as ureteral dilation during URS. After controlling for risk factors, we found that UAS use increased the odds of unplanned health care utilization and decreased the likelihood of being stone free compared with cases where no UAS was used. Collectively, these findings suggest that UAS usage is not without risk to the patient and can potentially increase the burden on the health care system.
Using this multivariable model, we did find that prestenting decreased the odds of an ED visit when UASs were used (adjusted OR = 0.68, 95% CI 0.52–0.88, p < 0.05) (Table 3). Stent placement at the time of surgery was not found to be significantly associated with ED visits in UAS patients (adjusted OR = 1.14, 95% CI 0.87–1.50, p = 0.3) (Table 3); however, it must be taken into account that these two variables were covariates and not primary predictors. They were not the primary outcome of focus in this study, so conclusions drawn from this particular analysis must be interpreted carefully and necessitate further research.
We chose to exclude staged procedures from this particular analysis because they typically represent the highest risk and highest complexity patients. Often, staged procedures are for patients with large stones who may not be percutaneous nephrolithotomy (PCNL) candidates or have especially complex factors that preclude them from treatment in a single setting. There were a total of 303 staged procedures that were excluded, encompassing 5.4% of all URS procedures. This was a small proportion of overall cases and we felt it was worthwhile to exclude them as they could skew the results. Furthermore, we also chose to exclude centers with <10 cases. There were only 3 centers that treated <10 patients, and the number of patients treated at these three centers only added up to 10. We chose to exclude them to minimize variation due to low case volume or potential lack of proficiency. We felt that they may not be comparable with the rest of the group.
Previous investigators have shown that UAS use is frequent, in as many as two-thirds of URS procedures for renal stones. 7 International survey data indicate that 58% of urologists report UAS use in every URS case. 6 Interestingly, our data suggest a much lower frequency of UAS use across all stone locations. This likely exists because of our large variety of group practice types and settings. Prior studies have suggested using UASs in cases with concern for infection due to decreased intrarenal pressure 3 as well as in patients with coagulopathy or antiplatelet use because of decreased trauma from multiple passes of the ureteroscope. 14 In line with this, in our series, we found that patients with a prior positive urine culture and those on antiplatelet agents had higher rates of UAS use during their URS.
While up-front UAS use is suggested to improve visibility in addition to decreasing postoperative infection and bleeding risk, little is known regarding downstream consequences of UAS use such as unplanned health care encounters. Previous investigations into UAS use have focused on their association with SFRs and complications; however, ED visit rates and hospitalization rates after URS are not infrequent. Specifically, their association with UAS use has been poorly defined. In an administrative claims analysis of 93,523 procedures to treat USD, 15% of patients had either an unplanned ED visit or hospital admission within 30 days, resulting in an adjusted incremental expenditure of $23,436 per episode. 13 One of the novel findings from the current study was that UAS use was associated with increased odds of both an ED visit and hospitalization within 30 days of URS. Although questions have been raised if this is related to stent status, we found that even after controlling for this in our multivariable models, which used both preop stenting and stenting at the time of surgery as predictors, UAS use was still associated with increased odds of both ED visits and hospitalization. This highlights the importance of judicious usage of UASs; omitting UASs in select patients may help reduce the frequency of postoperative ED visits and, in turn, decrease the overall costs of stone surgery.
UASs have been proposed to enhance fragment removal, but results regarding their association with SFRs are inconsistent. Early retrospective data suggested a significant improvement in the SFR when a UAS was used. 15 However, more recent data from 2239 patients with renal stones treated with flexible URS found no difference in the SFR when a UAS was used, but there was an increased risk of complications. 7 It should be noted that significant variability in the definition of stone free between studies on the subject can preclude direct comparison. Nevertheless, recent meta-analysis data again suggest that UAS use does not improve the SFR, 16 consistent with our findings. Our study did not show better SFRs with UASs even after controlling for stone size, stone location, and other factors.
Our study does have several limitations. Although we capture a wide range of demographic, clinical, and operative data in the registry, our variable library is not exhaustive, thus the potential for unmeasured factors leading to confounding exists. The data set records numerous variables, but it does not have the granularity to look at every specific detail such as stent presence at the time of ED visit or hospitalization, although this may represent an area of future research. In addition, our overall rate of postoperative imaging is low, 17 so conclusions about the SFR must be drawn cautiously. That said, our rate of postoperative imaging is consistent with national claims-based data suggesting that imaging is performed in less than 50% of patients undergoing URS. As with any retrospective study, it is difficult to retroactively control for all variables through stats; the retrospective nature is an inherent limitation. Finally, we report data from a statewide clinical registry, thus our findings may not be generalizable to the broader urological community. However, the inclusion of a diverse group of academic centers as well as small and large private urology practices does mitigate this limitation to an extent.
Despite these limitations, this study is among the largest series to date to look at UAS use outcomes, which gives weight to the findings. Although UAS use is likely beneficial in patients at high risk for infection or in those with coagulopathy or taking anticoagulation or antiplatelet medications, our study indicates that the choice to use a UAS is not without potential consequences. Future work is needed to understand provider factors that may drive the variation in UAS use seen across the state. Potential next steps include leveraging the collaborative nature of MUSIC to define appropriateness criteria for UAS use.
Conclusions
UASs are employed in approximately one-third of URS procedures performed in the state of Michigan and we observed wide variation in use across participating urology practices. In our study, we found that UAS use was associated with increased odds of requiring a postoperative ED visit or hospitalization relative to patients in whom a UAS was not used. Based on these findings, future efforts are underway to understand appropriate use criteria for UASs in Michigan.
Footnotes
Acknowledgments
The authors would like to acknowledge the significant contributions of the MUSIC urologists, administrators, and data abstractors in each participating practice. In addition, they would like to acknowledge the support provided by the Value Partnerships program at Blue Cross Blue Shield of Michigan.
Author Disclosure Statement
All authors involved in this work made meaningful contributions. There are no competing interests or disclosures to report.
Funding Information
This study was financially supported by Blue Cross Blue Shield of Michigan.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.