
Abstract
Management options for small renal masses include active surveillance, partial nephrectomy, radical nephrectomy, and thermal ablation. For tumors typically ≤3 cm in size, thermal ablation is a good option for those desiring an alternative to surgery or active surveillance, especially in patients who are considered high surgical risk. We favor microwave ablation because of the more rapid heating, higher temperatures that overcome the heat sink effect of vessels, reproducible cell kill, and a highly visible ablation zone formed by water vapor that corresponds well to the zone of necrosis. For central tumors, we favor cryoablation because of the slower formation of the ablation zone and less likelihood of damage to the collecting system. With microwaves, it is important to monitor the ablation zone in real time (ultrasound is the best modality for this purpose), avoid direct punctures of the collecting system, and to place probes tangential to the collecting system to avoid burning open a persistent tract between the urothelium and extrarenal spaces or causing strictures. The surgical steps described in this video cover our use of high-frequency jet ventilation with general anesthesia to minimize organ motion, initial imaging and targeting, probe insertion, hydrodissection (a technique that enables displacement of adjacent structures), the ablation itself, and finally our dressing. Postoperative cares typically consist of observation with a same-day discharge or an overnight stay. Follow-up includes a magnetic resonance imaging abdomen with and without contrast, chest X-ray, and laboratories (basic metabolic panel, complete blood count, and C-reactive protein) 6 months postablation. Overall, percutaneous microwave ablation is an effective and safe treatment option for renal cell carcinoma in both T1a and T1b tumors in selected patients with multiple studies showing excellent oncologic outcomes when compared with partial and radical nephrectomy.
Featured Video
https://stream.cadmore.media/player/004a2cf8-c08c-4ad7-9187-13ee991d95e3
Indications
All patients with small renal masses are seen in urology clinic for counseling. For patients who are considering thermal ablation, biopsy is obtained before the ablation procedure so that a pathologic diagnosis is available for shared treatment decision-making.
1
When counseling patients about treatment options, the following points are discussed in detail: Surgery is preferred in younger patients, especially those with larger and more aggressive tumors. Percutaneous microwave ablation offers an alternative treatment to surgery and may be utilized in patients who are older, more comorbid, and have smaller tumors. Percutaneous ablation has a low risk of procedural complications and minimal recovery. General anesthesia or conscious sedation is used for ablation. Patients may leave the hospital on the same day or be kept overnight for observation. Most patients do not require pain medications after percutaneous ablation. Rare complications that are discussed include risk of damage to adjacent structures, pain, bleeding, or nerve injury. Local recurrence rates are slightly higher with ablation vs surgery
2
but may be salvaged with a second ablation procedure in most patients. Metastatic recurrence and cancer-specific mortality rate are not significantly different between surgery and ablation.
2,3
Cryoablation, radiofrequency ablation, and microwave ablation have all been used effectively to ablate renal cell carcinoma (RCC). Cryoablation freezes tissue and requires temperatures below −20°C to −40°C for consistent tumor kill. Radiofrequency and microwave ablation heat tissue to temperatures >60°C at which point tissue is destroyed in seconds.
For tumors that are amenable to ablation, we prefer microwave ablation because of the more rapid heating, higher temperatures that overcome the heat sink effect of vessels, reproducible cell kill, and a highly visible ablation zone formed by water vapor that corresponds well to the zone of necrosis. For selected central tumors, we use cryoablation because of the slower formation of the ablation zone and less likelihood of damage to the collecting system. With microwave ablation, it is important to monitor the ablation zone in real time (ultrasound is the best modality for this purpose), avoid direct punctures of the collecting system, and to place probes tangential to the collecting system to avoid burning open a persistent tract between the urothelium and extrarenal spaces or causing strictures. Patients who are considering ablation are discussed at a weekly conference of urologists and radiologists who are experienced with thermal ablation. 4
The ablation primarily demonstrated in this video is that of an 81-year-old man with hyperlipidemia, prediabetes, and an incidental right-sided 1 cm exophytic, interpolar renal mass with ultrasound-guided biopsy identifying chromophobe RCC. He was initially followed but decided to be treated with percutaneous ablation after 1 year of active surveillance.
Preoperative Preparation
All patients undergo a history and physical examination to determine any pertinent comorbidities that could affect their ability to undergo this procedure. We have a standardized preoperative planning sheet to ensure all pertinent information is obtained. Of note, it is important to obtain the patient's creatinine before the procedure given iodinated contrast will be used in their immediate postablation scan to evaluate for complete treatment. Ultrasound-based contrast agents may be used in patients with allergies or chronic kidney disease. The patient will also have a preoperative planning ultrasound to determine which position allows for best observation of the tumor.
Patient Positioning and Anesthesia
Patients are most often placed in the lateral decubitus position with the affected side facing up toward the ceiling. For example, if we are treating a right-sided mass, the patient would be in a left lateral decubitus position (or left side down). The patient's arms are in a prayer position with all bony prominences protected and pillows placed between the knees and ankles. For anesthesia purposes, an axillary roll is placed at the breast to protect the brachial plexus. We also use a flank roll to prop the patient up and to push the kidney closer to the skin.
We most often use general anesthesia combined with a technique called jet ventilation. This allows the anesthesiologist to significantly minimize kidney motion throughout the case, leading to safer more accurate targeting. A Monsoon™ jet ventilator machine is employed with typical settings turned to a frequency of 120 breaths per minute allowing for fast, but small tidal volumes. In the past, jet ventilation was accomplished using a manual technique, but the use of modern jet ventilators is far less laborious (particularly for prolonged procedures) and associated with a low incidence of complications.
Surgical Steps
Initial imaging and targeting (Fig. 1) Marking probe insertion site on patient. 
After the patient is positioned, we use ultrasound guidance to observe the mass and mark the target site for probe insertion. The patient is then prepped and draped.
Probe insertion (Fig. 2) Computed tomography of probe insertion.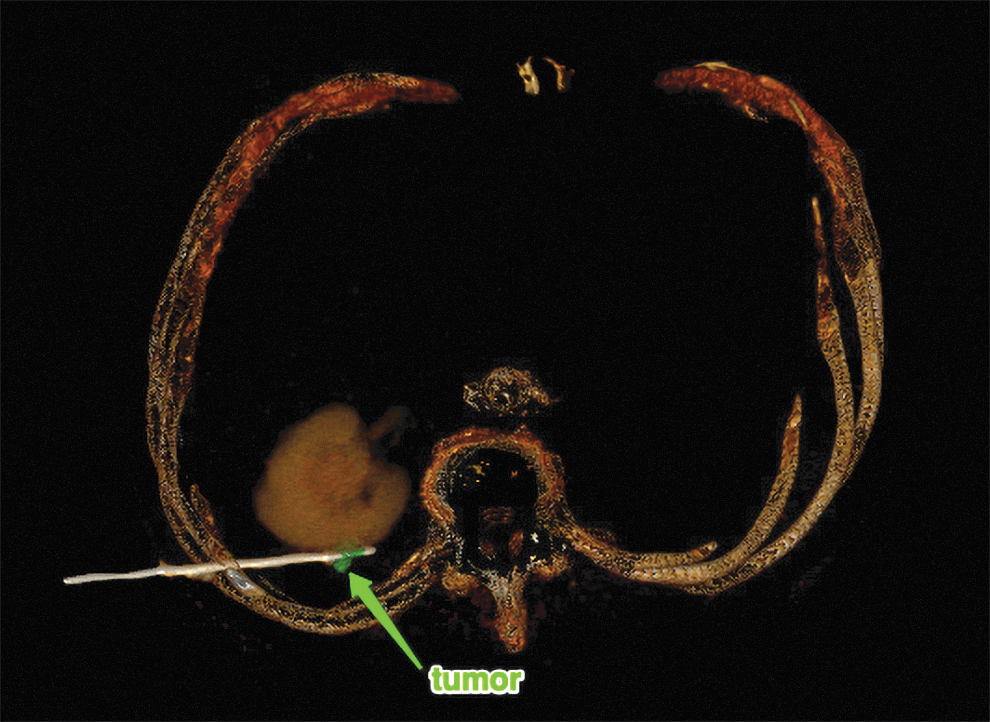
The probe is first tested by placing it in physiologic saline and ensuring a good seal is intact with no air bubbles observed. A skin incision is made with an 11-blade at our previously marked site and ultrasound guidance is used to insert the probe to the desired location. CT guidance is then used to confirm the probe is in the appropriate position.
Hydrodissection (Fig. 3) Computed tomography of hydrodissection. 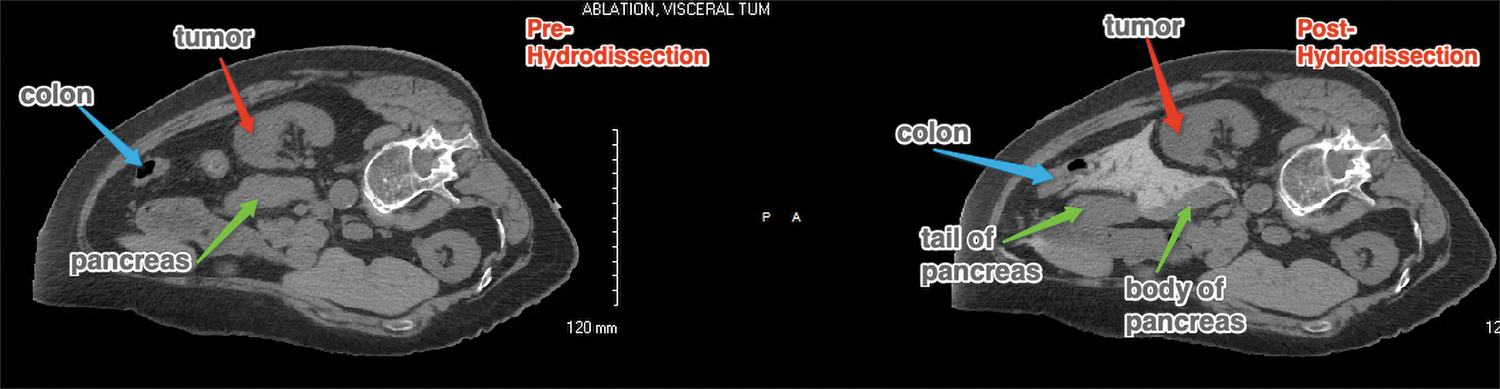
This technique can be employed to displace critical structures away from the tumor to prevent thermal damage and enable treatment in difficult locations. 5 A spinal needle is inserted into the proper plane between the tumor and critical structure using either ultrasound or CT fluoroscopic guidance. A mixture of physiologic saline and 2% ioversol contrast is then injected through a spinal or Chiba needle using a 60-cc syringe and three-way stopcock. The use of contrast allows hydrodissection to be performed under CT fluoroscopic guidance, ensuring adequate separation of the mass from the critical structure in question (generally colon, small bowel, and pancreas). This creates a safer ablation zone and prevents serious complications from occurring.
Ablation of renal mass (Fig. 4) Computed tomography of renal mass pre and post ablation.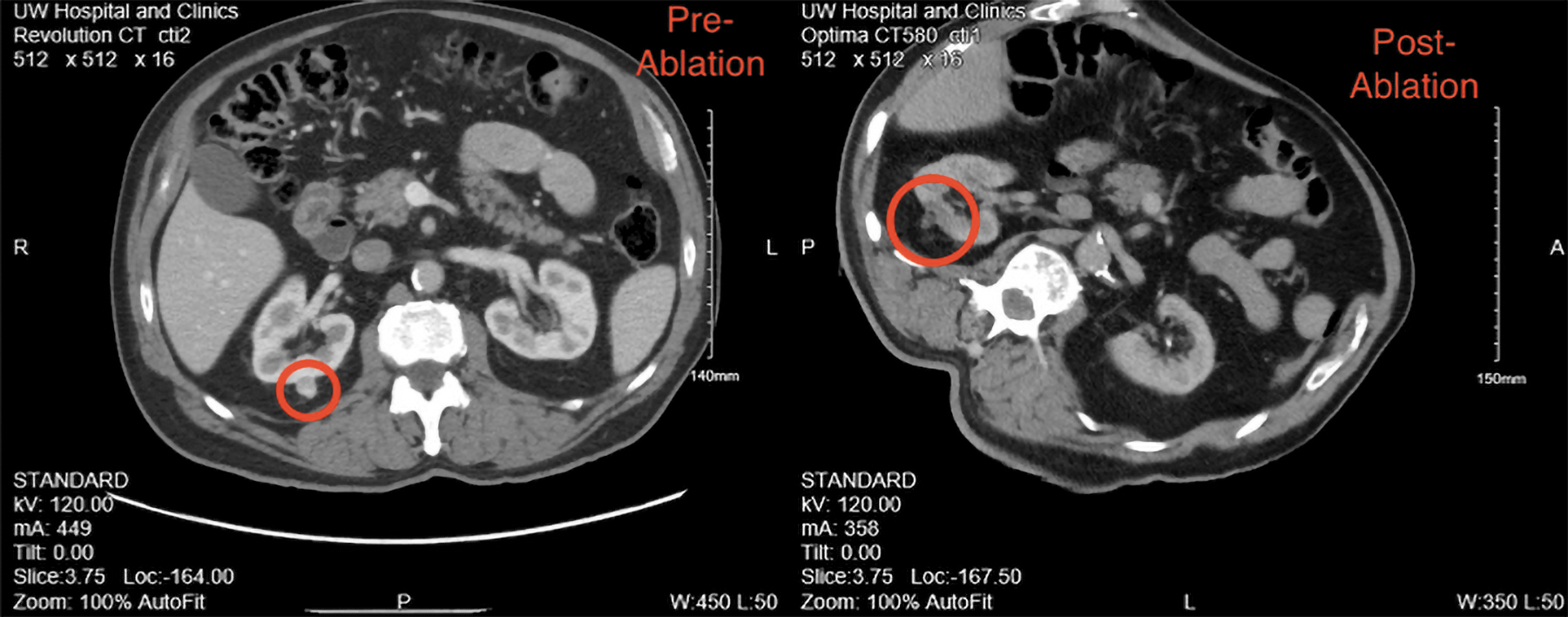
Standard ablation settings are at a power of 65W for 5 minutes. The probe temperatures and ablation zone are closely watched throughout the duration of the ablation. The number of probes used depends on the size of the mass. Typically, tumors ≤2.5 cm are treated with one probe, tumors 2.5 to 3.5 cm are treated with two probes, and tumors at least 3.5 cm are treated with three probes. After ablation, the probes are removed and a CT with IV contrast is performed to observe the ablation zone and ensure complete ablation of the tumor. The advantage of this contrasted scan is to identify any residual enhancing tumor that can be immediately treated if necessary.
Wound care/dressing (Fig. 5) Dermabond being applied to probe insertion site.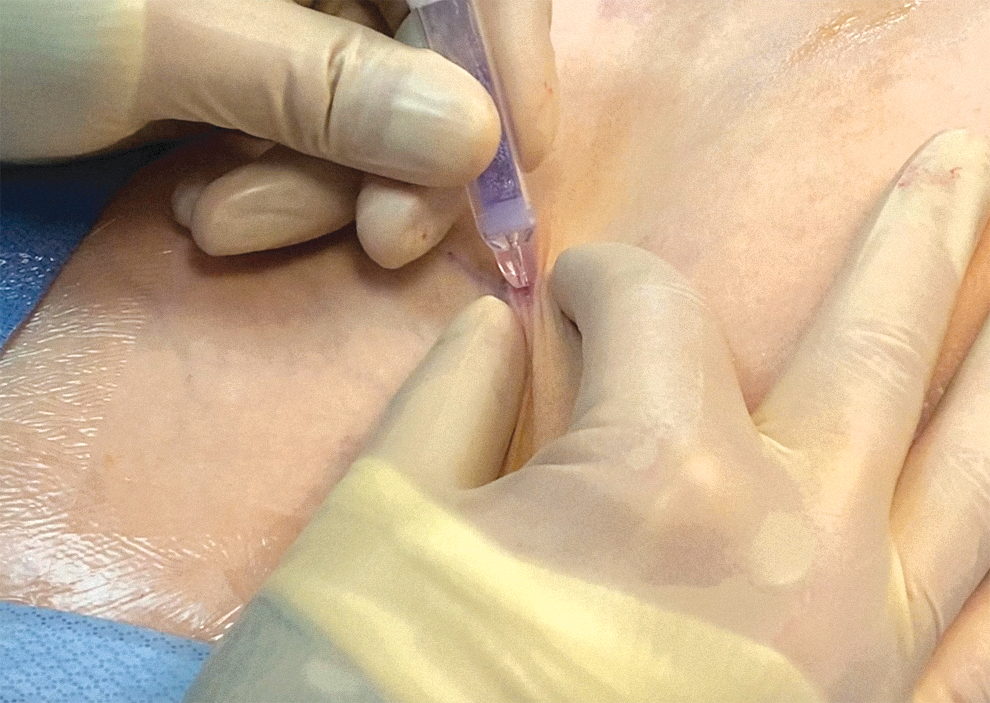
The site is cleaned and dried. Dermabond is then applied over the puncture site. The patient is woken up, extubated, and taken back to the post-anesthesia care unit.
Postoperative Care
Patients are discharged on the same day or admitted for observation overnight. We generally admit patients with >3 cm tumors, a solitary kidney, or concern for hematoma. A hematocrit is obtained 4 hours postprocedure. Patients are given a general diet postoperative day 0 and analgesics as needed. Follow-up consists of an magnetic resonance imaging of the abdomen w/and w/o contrast (or a CT if contraindicated), chest X-ray, and laboratories, including basic metabolic panel, complete blood count, and C-reactive protein in 6 months. 6 Patients are subsequently followed with imaging surveillance according to a risk-stratified approach. 7
Troubleshooting: Anatomical Anomalies, Obesity, Previous Surgeries, and so on
Complications increase with centrally located tumors, tumors near the collecting system, or tumors near critical organs such as the pancreas and spleen. These adverse events include perinephric hematoma, urinoma, transient hematuria, and injury to surrounding structures. 8 As described earlier, hydrodissection is sometimes employed to create a safer ablation zone. For tumors located directly adjacent to the collecting system, ureteral stents are sometimes placed immediately before ablation to protect the collecting system. These are placed by the urologist cystoscopically in the operating room under general anesthesia. The patient is then transported to the ablation suite. Stents are typically removed 1 month after ablation.
List of instruments
Please include generic terms when possible. When specific proprietary instruments, products, disposables are required please include the name of the company.
Microwave ablation system: Certus 140, NeuWave™ Medical
Jet Ventilator Machine: Monsoon, Vyaire Medical
Ultrasound: GE Logiq E10
CT: GE 580 Widebore 16 detector row
Imactis CT-Navigation for targeting
Alternate or modification of technique if applicable
Not applicable.
Clinical Outcomes
When choosing ablation as a treatment modality for RCC, an important factor to consider is local tumor progression (LTP) (Table 1). A meta-analysis of 107 studies showed that local recurrence-free survival for thermal ablation was inferior compared with partial and radical nephrectomy with one treatment but reached equivalence with subsequent treatments. Cancer-specific survival was excellent among all modalities with a median 5-year survival of 95% for cT1a tumors. 2
Large Patient Series
LTP = local tumor progression; MW = microwave ablation; PN = partial nephrectomy; RCC = renal cell carcinoma; RN = radical nephrectomy.
One study of 171 cT1a RCC tumors evaluated LTP based on the influence of specific factors such as age, gender, longest tumor diameter, tumor location, number and pathology type, and ablation power and time. LTP only occurred in five patients with tumor location found to be the only independent predictor of LTP. Of these patients, three underwent additional ablation and the other two underwent nephrectomy because of refusal of additional ablation. There were no instances of LTP-related deaths. 9
Data for single-session treatment efficacy in the first 100 T1a RCC tumors were evaluated at our institution. 10 For tumors between 2.5 and 3.5 cm two ablation probes were used, whereas three probes were used for tumors >3.5 cm. One case of LTP was identified where the patient was lost to follow-up for an extended period of time but eventually treated with radical nephrectomy and no subsequent recurrence. Three-year cancer-specific survival and overall survival were 100% and 91%, respectively.
Selected clinical stage T1b (cT1b) RCC tumors may also be treated with microwave ablation. In a study of perioperative and oncologic outcomes for 325 patients with cT1b RCC (40 of whom underwent microwave ablation, 74 partial nephrectomies, and 211 radical nephrectomies), the estimated 5-year local recurrence-free survival was 94% for ablation, 98% for partial nephrectomy, and 99% for radical nephrectomy. The two patients (5%) who recurred after initial ablation were subsequently treated with a second ablation without further recurrence. There were no differences in 5-year metastasis-free survival or cancer-specific survival among ablation, partial, or radical nephrectomy patients. 11
Conclusion
Overall, percutaneous microwave ablation is a safe and efficacious treatment option for RCC in both T1a and selected T1b tumors in selected patients with multiple studies showing excellent oncologic outcomes when compared with partial and radical nephrectomy.
Footnotes
Patient Consent Statement
The author(s) have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Author Disclosure Statement
F.T.L.: consultant: Ethicon, Inc.; stockholder and board of directors: Histosonics, Inc.; patents and royalties: Medtronic, Inc. T.J.Z.: consultant and research funding: Neuwave Medical; consultant, shareholder, and research funding: Histosonics. J.L.H.: consultant: Neuwave Medical; Spouse: cofounder of Accure Medical; stockholder: Elucent Medical. S.A.W: consultant: Ethicon, Inc. P.E.L. consultant: Johnson & Johnson/Ethicon, Inc.; consultant and shareholder: HistoSonics; consultant and shareholder: Elucent Medical; shareholder: McGinley Orthopedic Innovation; member and shareholder: Blueprint Life Science Advisors. S.Y.N.: consultant: Boston Scientific.
Funding Information
No funding was received for this article.