
Abstract
The mini percutaneous nephrolithotomy (mini-PCNL) has become a versatile tool to remove kidney stones >2 cm, lower pole stones >1 cm, renal stones previously unresponsive to shockwave therapy or inaccessible by ureteroscopy (within a caliceal diverticulum), stones within complex urinary tracts (urinary diversions, transplanted kidney, and horseshoe kidneys), and large impacted proximal ureteral stones. After positioning in either the supine or prone position, a cystoscopy is performed to place an open-ended catheter, occlusion balloon, or Accordian device into the collecting system. A foley catheter is placed in the bladder. An ultrasound with a curvilinear probe is used to survey the kidney and guide access into the collecting system with an 18 g percutaneous needle. Once access is obtained, a small 0.5 cm skin incision is made and the percutaneous tract is dilated over a wire. A 16.5F metallic or self-dilating suctioning access sheath is positioned with fluoroscopic guidance. A 12F rigid mini-PCNL nephroscope is used to evaluate the collecting system. Once a calculus is observed, options for stone fragmentation include a lithotripter with ultrasonic and ballistic energy, or laser lithotripsy using holmium or thulium laser fibers. Flexible ureteroscopy can be considered to ensure clearance of the collecting system. A 6F ureteral stent can be placed in either a retrograde or antegrade approach for drainage. The tract is sealed using Surgiflo hemostatic matrix with thrombin. Guidelines for postoperative care and troubleshooting techniques for mini-PCNL are reviewed along with the surgical steps in the accompanying video (Supplementary Video S1). There are few randomized trials comparing mini-PCNL with standard PCNL and ureteroscopy. There is some evidence to suggest a difference in transfusion rates comparing mini- and standard PCNL, as well as differences in stone-free rates when comparing mini-PCNL with ureteroscopy for the treatment of lower pole stones.
Featured Video
https://stream.cadmore.media/player/8b0d5be5-e4f7-4959-9329-b511d1f89fae
Indications
Mini percutaneous nephrolithotomy (mini-PCNL) has become a useful tool in an armamentarium of minimally invasive techniques for the treatment of renal calculi. A mini-PCNL traditionally uses a tract size of 14F to 22F, compared with standard PCNL (>22F), ultra-mini-PCNL (11F–13F), and micro-PCNL (4F–10F). 1 Indications for mini-PCNL include kidney stones >2 cm, lower pole stones >1 cm, renal stones previously unresponsive to shockwave therapy or inaccessible by ureteroscopy (e.g., within a caliceal diverticulum), stones within complex urinary tracts (e.g., urinary diversions, transplanted kidney, and horseshoe kidneys), and, finally, large impacted proximal ureteral stones. 2 –4 Relative contraindications to surgery include coagulopathy, active urinary tract infection, tumor along tract, pregnancy, and inability to tolerate surgical position. 5
Preoperative Preparation
Before surgical intervention, a complete history and physical examination should be completed including review of prior urologic procedures, history of anticoagulation use, and contraindications to surgical positioning. Based on the 2016 American Urologic Association and Endourological Society Guidelines, a urinalysis should be obtained and those with suspected infection should have a urine culture obtained. 4 Antimicrobial prophylaxis is indicated in all patients undergoing percutaneous surgery; however, in a patient with active urinary tract infection, one must treat infection preoperatively in an attempt to sterilize the urine. 4,6,7 In addition, if the infection is associated with obstruction of the kidney, a percutaneous nephrostomy or ureteral stent should be placed in addition to treatment of the infection before PCNL. It is recommended that a complete blood count and platelet count should be obtained on patients with risk of hemorrhage and a metabolic panel and creatinine should be obtained on those with suspicion of renal dysfunction. 4 A noncontrast CT scan should be obtained for preoperative planning to assess anatomy that may determine operative approach including retrorenal colon, hepatomegaly, splenomegaly, level of pleura, and rotation of kidneys. 4 In those with collecting system anomalies, a CT scan with contrast can be obtained to delineated anatomy further. 4 In patients with suspected loss of renal function, functional renal imaging can be obtained. 4 It is our standard practice to also perform office renal ultrasonography in the simulated position for PCNL in patients where there are anatomical abnormalities to assure a safe access can be obtained.
Patient Positioning
Patients can be positioned prone or supine. Our preferred positions are the prone split leg position using spreader bars (Fig. 1) or our modification of the Barts Flank-free position (Fig. 2). 8,9 In the prone split leg position, the patient's arms are outstretched with 90° angles at the shoulder and elbow joints. Two gel bolsters are placed in a horizontal manner supporting the xiphoid process and pubic bones. Foam pads are used to support pressure points around knees and ankles. The split leg position allows for easy access to the urethra during the procedure. The modified Barts Flank-free position uses gel bolsters to lift and support the ipsilateral hip and shoulder, with a 10 to 15° tilt to provide exposure to the flank. The ipsilateral leg is straight and the contralateral leg is gently flexed at the knee. The ipsilateral arm is placed across the chest and supported by foam. Foam pads are also used to support pressure points around knees and ankles.

Prone split leg position.

Modified Barts Flank-free supine position.
Surgical Steps
Step 1
The surgical steps are reviewed in the accompanying video (Supplementary Video S1).
After induction of spinal or general anesthesia, the patient is positioned as already mentioned. We prefer general anesthesia with intubation for prone cases and general anesthesia with a laryngeal mask airway for supine cases. Sequential compression devices are placed and preprocedural antibiotics are administered. The flank and genitalia are prepped. The patient is draped allowing for simultaneous access to the flank and urethra. A cystoscopy is performed in either the prone or supine position. A 5F open-ended ureteral catheter, a balloon occlusion balloon, or an Accordion device can be placed for retrograde access to the collecting system. A 16F foley catheter is placed for maximal drainage during the procedure.
Step 2
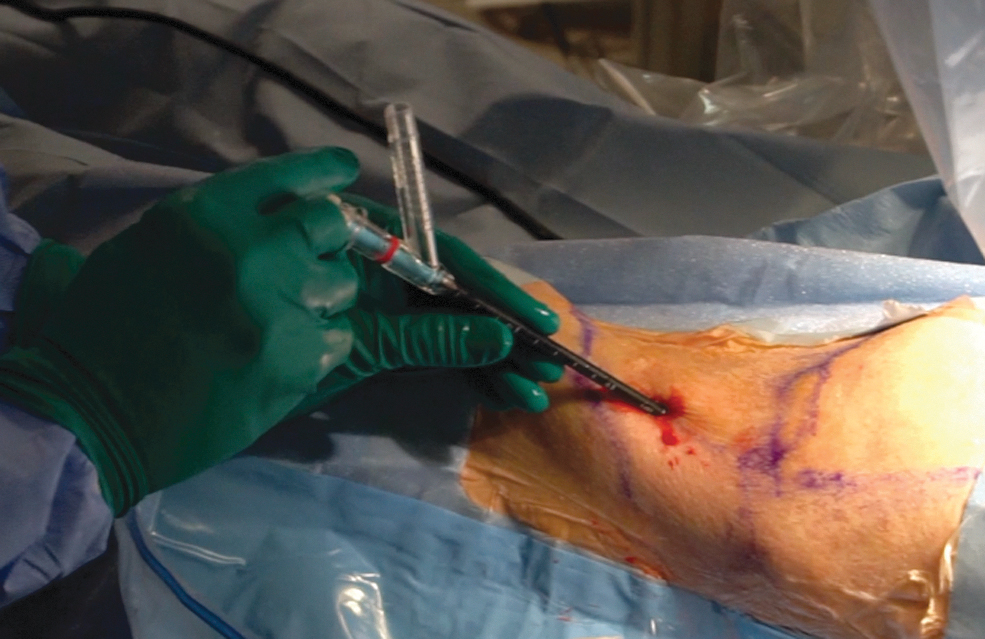
An ultrasound with a convex curvilinear probe with a frequency between 3.5 and 5.0 mHz focused at 7 to 9 cm is used to survey the flank. The kidney is identified and any other identifying surrounding structures including liver, spleen, pleura, and bowel are observed in real time. Stones are identified as a hyperechoic foci with posterior acoustic shadowing (Fig. 3). On color flow Doppler, a twinkle artifact can be seen. An appropriate calix of entry is identified with the ultrasound. The most posterior calices are usually seen closest to the ultrasound probe. Filling the collecting system with saline through the open-ended catheter or occlusion balloon can aid in making calices more prominent on ultrasound imaging. An ultrasound needle guide is placed on the probe through which an 18 g percutaneous access needle is positioned (Fig. 4). The needle is advanced in real time under direct vision into the calix. The ultrasound guide and probe are detached from the needle. Urine flowing through the needle confirms placement into the collecting system. A 0.038 angled tipped Nitinol wire is passed into the collecting system confirming positioning with fluoroscopy. In some cases, it may be desired to have through and through access, however, it is not imperative to complete the procedure.

Renal ultrasonography demonstrating calculus with posterior acoustic shadow.

Ultrasound probe with needle guide and percutaneous needle.
Step 3
A 0.5 cm incision is made on the skin. The access needle is removed maintaining access into the collecting system with the Nitinol wire. We prefer to use a 10F fascial dilator to perform the initial dilatation, and this can be with ultrasonic or fluoroscopic guidance. A 16.5F metallic dilator or a 16F self-dilating suctioning sheath then is advanced over the wire into the collecting system (Fig. 5). This can also be done with ultrasound or fluoroscopic guidance. Several metallic dilators ranging from 8.5F to 24F can be used. A metallic sheath is placed over the dilator into the collecting system (Fig. 6). Alternatively, various access sheaths can be used, including those that connect to suction and irrigation, allowing for continuous flow irrigation during the procedure (Fig. 7). Final position of the access sheath is confirmed on fluoroscopy.

Placement of metallic dilator.

Placement of metallic sheath over dilator.
Placement of continuous flow access sheath.
Step 4
A rigid 12F mini nephroscope is used to identify all calculi. A lithotripter using a combination of ballistic and ultrasonic energy can be used to fragment the stone (Fig. 8). Alternatively, a holmium or thulium fiber laser fiber can be used to fragment the stone. A vortex effect created within the sheath allows for easy removal of the fragmented stones through the sheath. The safety wire can be removed to allow for better vortexing ability. After all fragments are removed, final nephroscopy is performed. A flexible ureteroscope can also be used to reach calices inaccessible with the rigid nephroscope. Alternatively, a second or several additional mini percutaneous access sites can be used to reach such stones. The collecting system is cleared of any clots and inspected for perforation. This complete nephroscopy ensures stone-free status.
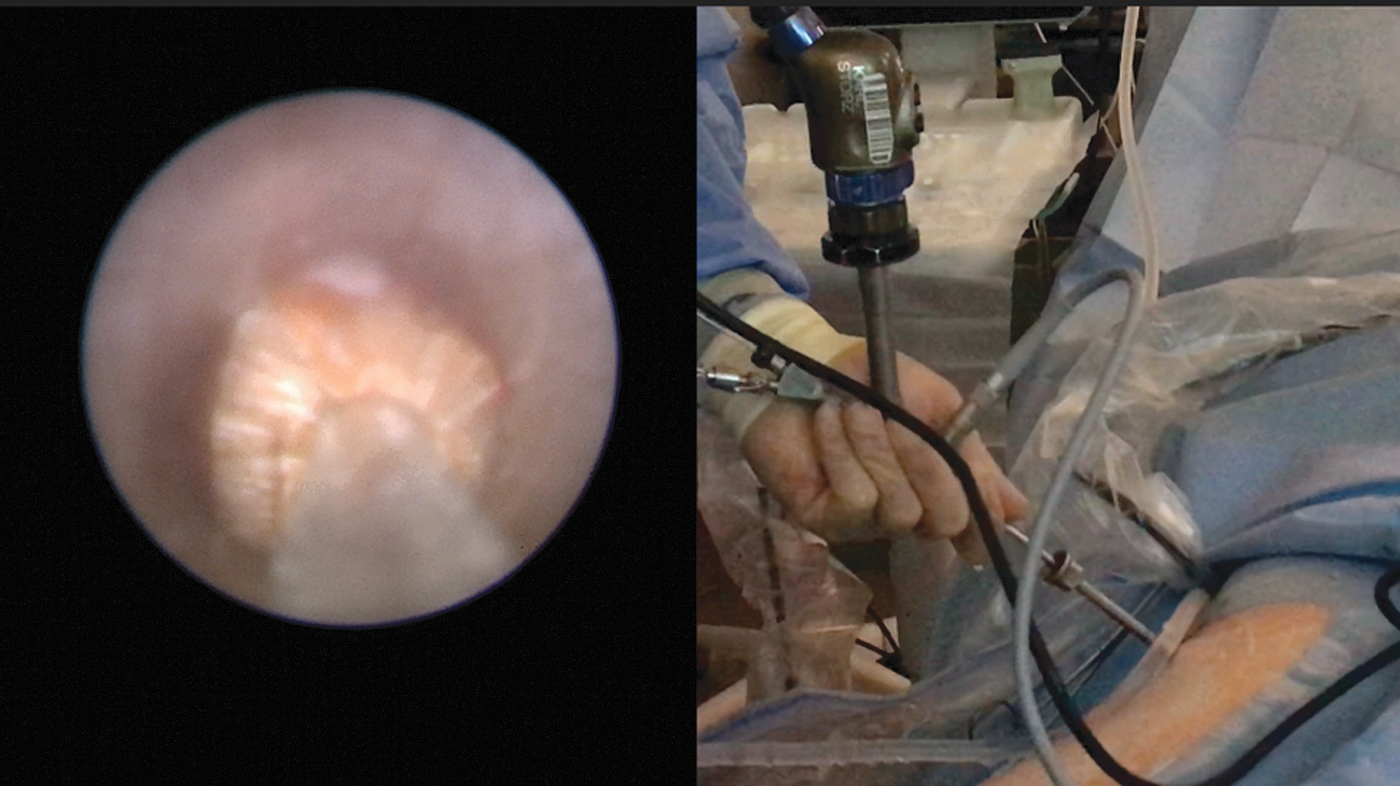
Nephroscopy and lithotripsy using ultrasonic and ballistic energy.
Step 5
In cases wherein longer term renal drainage is necessary, a 6F double pigtail ureteral stent can be placed through a retrograde or antegrade approach using fluoroscopic guidance, especially in cases where ureteral or ureteropelvic junction (UPJ) edema may cause postoperative obstruction (Fig. 9). In most routine cases where there is minimal manipulation of the ureter, UPJ, or the collecting system, a totally tubeless procedure can be performed. In cases where short-term drainage is desired, we leave a 5F open-end catheter connected to a foley catheter, which are simultaneously removed in the recovery room before discharge.

Ureteral stent placement via antegrade approach.
Step 6
Tract closure if desired is performed by injecting Surgiflo hemostatic matrix with thrombin into the tract (Fig. 10). Other gel- or foam-based hemostatic agents can also be used. Slight pressure is applied at the insertion site. A skin glue can be applied to the incision site or it can be simply dressed with sterile dressing in the absence of significant bleeding. The stones collected during the procedure are sent for stone composition analysis and culture. If in the prone position, the patient is then flipped into the supine position.
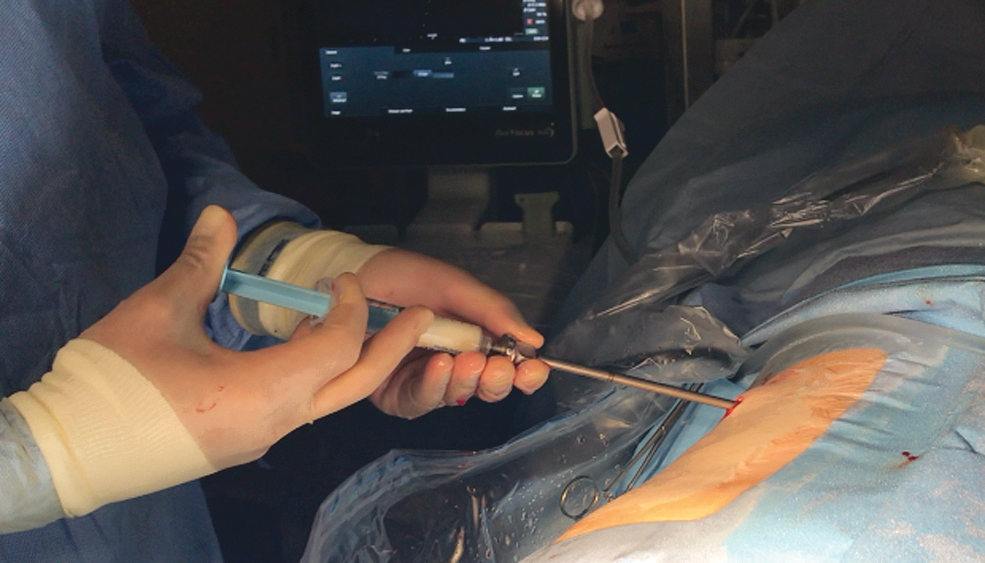
Injection of Surgiflo into tract.
Postoperative Care
Patients are routinely discharged from the recovery room after foley catheter removal. Patients with open-end catheters have it removed simultaneously with the foley catheter. For those with indwelling stents, routine cystoscopy with stent removal can be performed in the office 3 to 10 days postoperatively. If supracostal access is obtained, a chest radiograph is obtained to rule out pneumothorax, hemothorax, or hydrothorax. During postoperative office visits, a metabolic work-up including a 24-hour urine test can be offered to patients. A renal ultrasonography and/or abdominal X-ray is obtained as an outpatient to assess stone-free status. In some practices, a low dose CT scan may be obtained.
Troubleshooting
Obese patients or inability to tolerate prone
The supine position is an acceptable alternative for patients who cannot tolerate prone position because of medical conditions or obesity. Obese patients are noted to have elevated peak inspiratory airway pressures regardless of prone or supine position. 10
No urine seen through percutaneous needle on entry
Using the open-end or occlusion balloon catheter, saline can be injected in a retrograde manner to distend the collecting system in an attempt to create outflow through the needle. If urine is still not observed, a retrograde pyelogram can be performed. If the needle appears to be outside of the collecting system, ultrasound or traditional methods of fluoroscopic guidance can be used to advance or reinsert the needle.
No space in calix to pass wire because of impacted stone
In the event a stone is impacted within the targeted calix, when attempting to pass a wire through the needle, only a small amount of wire may be noted to be coiled in the vicinity of the stone. This may lead to doubts as to whether the wire is still within the collecting system. To avoid this situation, the percutaneous needle can be used under ultrasound guidance to tap the stone and push it to create further space within the calix. If the stone is soft enough, the stone can be impaled with the needle, and the wire fed “through” the stone allowing one to position a dilator and access sheath right up to the stone. Alternatively, a flexible ureteroscope can be used in a retrograde manner to target the calix of interest and visually confirm wire passage or to select an alternative access site.
Percutaneous needle with blood return
If a slow drip of blood is noted, one can use ultrasound or fluoroscopy to assess location of needle tip and its proximity to the collecting system. At times, slowly withdrawing the needle can lead to ultimate positioning within the collecting system. This can be aided by simultaneously distending the collecting system through retrograde access. If there is no urine return at all, completely withdraw needle and attempt another access.
Prior scars
In patients with prior open lithotomy incisions or prior PCNL incisions, there can be some scar tissue encountered making dilatation difficult. Sequential dilators may be useful to allow access into the tract or using an 11-blade and running it parallel along the access needle to incise fibrotic tissue to the fascia can allow easier access with a dilator.
Horseshoe kidney
Although a more medial and posterior approach in access may favor prone positioning, in selected patients who cannot tolerate prone position, an ultrasonography can be performed before start of the procedure to assess whether the kidney can be easily accessed through a supine position.
Duplicated collecting system
Large stones found within different parts of a duplicated system can utilize two or more mini percutaneous access sites. A retrograde pyelogram is imperative to delineate this anatomy intraoperatively, however, ultrasound guidance for access can still be employed.
Caliceal diverticulum
After stone removal from a caliceal diverticulum, if the narrowed infundibulum is identified, it can be laser incised to widen entry to remainder of the collecting system. Methylene blue can be used in a retrograde or antegrade manner to help identify infundibulum. The caliceal diverticulum can also be fulgurated. 11
Kidney ptosis
An abnormal lie of the kidney can sometimes be corrected by placing an occlusion balloon into the renal pelvis and providing gentle downward traction to straighten the kidney along a more linear axis. This can theoretically also be done to aid to achieve a higher access site.
Hypermobile kidney
The surgeon or assistant can place abdominal pressure to keep the kidney from moving during ultrasound-guided access and also during tract dilatation.
Tract dilated but cannot observe the collecting system
If the collecting system is not observed after dilatation, however, the needle did have urine return before dilatation, the access sheath is likely too deep or not deep enough. Fluoroscopy in different planes can help make this determination. If too deep, gentle withdrawal of the sheath usually will reveal the stone or the collecting system. If shallow, following the path of the wire can lead to the collecting system, while gently dilating the prerenal tissues or parenchyma with peanut graspers. Alternatively, the tract can be redilated. Gently injecting saline or methylene blue from the retrograde catheter may allow aid in identifying the intended calix.
Stone in parallel calix
If retroflexion of a flexible ureteroscope is still not enough to gain access to a stone in a parallel calix as that of the dilation tract, decision can be made to use a second percutaneous access site to gain access to stone or to use a flexible ureteroscope retrograde to grasp the stone and deliver it to the nephroscope (“pass the ball” technique).
Stone fragment migration into inaccessible calix
During lithotripsy, stone fragments that are broken may migrate to a difficult-to-access calix of the kidney. The use of continuous flow access sheath that uses both suction and irrigation can prevent some migration as the suction acts to remove pieces as soon as they are broken up. 12 We also liberally use patient position to prevent this. Airplaning the patient away from the operative side and in reverse Trendelenburg position can keep fragments in the renal pelvis and toward the UPJ. At the end of the procedure, flexible ureteroscopy antegrade and/or retrograde can be used to inspect all calices to ensure the collecting system is stone free.
Bleeding during procedure
If excessive bleeding is encountered during the procedure, then, along with a ureteral stent, a 10F nephrostomy tube can be placed through the access site and used to tamponade or drain the collecting system as needed.
Bleeding after sheath removal
After access sheath removal, if excessive bleeding is encountered, pressure can be held at the access point to tamponade.
Postoperative sepsis
In the event the patient demonstrates signs of sepsis postoperatively including fevers, hypotension, profound leukocytosis, or lactic acidosis, antibiotic coverage should be broadened and fluid resuscitation should be initiated. Results of the stone culture can ultimately guide antimicrobial coverage. 13
Colon perforation
If a retroperitoneal colonic perforation is recognized intraoperatively, a ureteral stent and foley catheter are placed for maximal urinary drainage. A nephrostomy tube is placed into the lumen of the colon allowing for the medial aspect of the bowel to heal. After 1 week, the nephrostomy tube is withdrawn out of the colon, and repositioning in the pericolonic space to allow for the lateral wall to heal. After another week, the tube is removed completely. In the event an intraperitoneal injury has occurred with sepsis or peritonitis, surgical intervention is necessary. 14
Hydrothorax, pneumothorax, or hemothorax
This is best detected intraoperatively by surveying the chest with fluoroscopy. Sharp diaphragmatic angles should be seen. Asking the anethesiologist to perform a deep ventilation and hold in that position can aid in detection. A small pigtail catheter or a chest tube is placed for decompression. A ureteral stent and foley catheter should be placed for maximal urinary decompression.
Splenic or hepatic injury
At times small injuries identified on CT scan can be managed conservatively especially in a setting where a hemostatic agent was used to plug tract. However, if not effective, surgical intervention may be needed.
List of Instruments
Table 1 lists the most commonly used instruments and materials needed to perform the mini-PCNL.
Comprehensive List of Instruments
Clinical Outcomes
There are a few randomized controlled trials comparing mini-PCNL with retrograde ureteroscopy and trials comparing mini-PCNL with standard PCNL. Cheng and colleagues demonstrated a significant difference in rate of transfusions comparing mini- and standard PCNL (1.4% vs 10.4%, p < 0.05). 15 Although stone-free rates were not significantly different, the operative time was longer for mini-PCNL than for standard PCNL (89 minutes vs 77 minutes, p < 0.5). 15 Kukreja demonstrated similarly no difference in stone-free rates between the groups, however, also demonstrated no significant differences in operative time or complications. 16 Mini-PCNL, however, was more likely to be a tubeless procedure (no nephrostomy tube) than standard PCNL (95% vs 77%). 16 Yavuz et al. demonstrated high stone-free rates when treating lower pole stones when performing mini-PCNL and standard PCNL compared with when performing ureteroscopy (94% vs 94% vs 76%). 17 Although two trials—Zeng and colleagues 18 and Lee et al. 19 —demonstrate differences in stone-free rates between mini-PCNL and ureteroscopy, they are not consistent with one another. Lee shows higher stone-free rates in ureteroscopy whereas Zeng et al. demonstrate higher stone-free rates for mini-PCNL. 18,19 These differences may be related to different operative techniques including types of sheaths used (i.e., standard sheath vs continuous flow irrigation sheaths) or differences in postprocedural imaging used to verify stone-free status. Tables 2 and 3 summarize some key features of the randomized controlled trials.
Summary of Randomized Controlled Trials Comparing Mini Percutaneous Nephrolithotomy and Ureteroscopy
m
Summary of Randomized Controlled Trials Comparing Mini Percutaneous Nephrolithotomy and Standard Percutaneous Nephrolithotomy
PCNL = percutaneous nephrolithotomy
Conclusions
Mini-PCNL has developed into a versatile tool to remove large renal and proximal ureteral stones. It can be applied to patients with complex urologic anatomy and can be adapted for patients in the prone or supine position. With the propensity of mini-PCNL to be an outpatient tubeless (no nephrostomy tube) or totally tubeless (neither nephrostomy tube nor ureteral stent) procedure, it is attractive as an efficient way to treat relatively large stones safely while keeping complications low and pain and discomfort at a minimum. Although a smaller working channel may be related to longer operative times, there are ways to improve efficiency including considering various lithotripters (combination of ultrasound and ballistic energy) and lasers (holmium and thulium) as well as different access sheaths (continuous flow sheath with suction and irrigation) that can both fragment and remove stones efficiently, maintaining high stone-free rates. The accompanying video demonstrates a step-by-step approach to performing mini-PCNL.
Footnotes
Patient Consent Statement
The author(s) have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Recommended Videos from Videourology
1. Videourology 2020 Vol. 34, No. 5.
Mini-Percutaneous Nephrolithotomy Technique of Percutaneous Nephrolithotomy with Thulium Fiber Laser.
Sida Niu, Raphael Carrera, and Wilson Molina.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.