
Abstract
Background:
The recent plethora of reports of “free-hand” transperineal prostate biopsy (fTP-Bx) under local anesthesia (LA) demonstrate that many centers consider this technique to be a safer and possibly more accurate approach to prostate biopsy in the clinic setting.
Materials and Methods:
The literature was searched for fTP-Bx, and summary tables were compiled. Studies on the costs of postprostate biopsy sepsis were also researched.
Results:
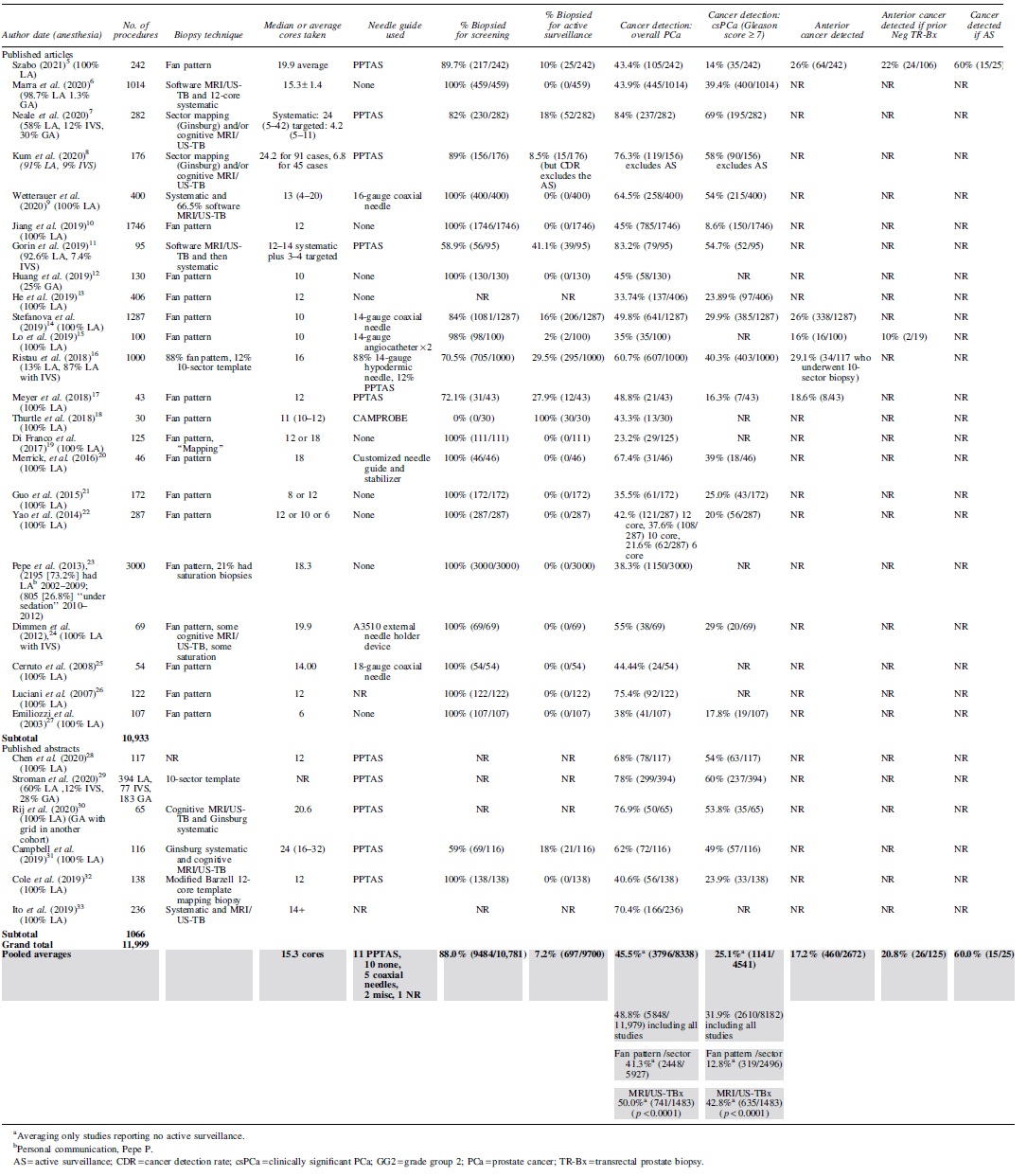
The search found 11,999 cases of fTP-Bx under LA with and without sedation over 29 mutually exclusive studies. Pooled averages calculated for age, prostate-specific antigen (PSA), prostate volume, PSA density, and cores sampled were 67.3 years, 10.4 ng/mL, 47.7 mL, 0.24 ng/mL/cc, and 15.3 cores, respectively. Detection of overall prostate cancer (PCa) and clinically significant (Gleason score ≥7) prostate cancer (csPCa) averaged 45.5% (3796/8338) and 25.1% (1141/4541), respectively. After subgrouping the studies by biopsy technique, studies that used MRI/ultrasound fusion-targeted biopsy in some or all biopsy cases averaged an overall PCa and csPCa detection rate of 50.0% (741/1483) (p < 0.0001) and 42.8% (635/1483) (p < 0.0001), respectively. Visual analog scale pain ratings and procedure times averaged 3.17 and 13.1 minutes, respectively. Averages for complications of sepsis and acute urinary retention were 0.0% (0/7396) and 2.1% (120/5693), respectively. A total of 10.2% (1055/10,334) of cases received no antibiotic prophylaxis. If fTP-Bx under LA replaced transrectal prostate biopsy (TR-Bx) in the United States, the estimated annual savings would be $341,676,800–$752,540,000 through the virtual elimination of admissions for postbiopsy sepsis.
Conclusions:
Many centers around the world have adopted fTP-Bx because it virtually eliminates sepsis, may improve detection rates of csPCa and can be easily integrated into a normal clinic workflow using only LA. If all urologists in the United States abandoned TR-Bx for fTP-Bx, the potential savings in health care costs of complications would be significant.
Introduction
Despite the reduction in incidence of post-transrectal prostate biopsy (TR-Bx) sepsis with the use of targeted and/or augmented antibiotic prophylaxis, life threatening sepsis still occurs at an increasingly unacceptable rate 1,2 for a semielective cancer screening test. Indeed, the increasing difficulty of preventing serious post-TR-Bx infectious complications, stemming from an inherently “transfecal” procedure, has spurred many centers to abandon appropriate antibiotic stewardship as they add antibiotics of last resort (i.e., ertapenem) 3 to their prophylactic regimen.
In response to this challenge, many centers around the world have adopted transperineal prostate biopsy (TP-Bx). 4 Until several years ago, most TP-Bxs were performed with the aid of a perineal grid template (familiar to those experienced in brachytherapy) and required general anesthesia (GA). However, a recent modification of the transperineal technique has allowed it to be easily integrated into a normal clinic workflow using only local anesthesia (LA), with or without the addition of MRI/ultrasound fusion-targeted biopsies (MRI/US-TBx).
This modification, known as “free-hand” transperineal prostate biopsy (fTP-Bx), does away with the bulky perineal grid template and stepper unit in favor of a more flexible technique using one hand for the ultrasound probe and one hand for the biopsy needle instrument. This technique takes advantage of the mobility of the perineal skin and underlying ischiorectal fat through the insertion of a hollow coaxial needle sheath as an introducer for the biopsy needle. The freedom of movement achieved by this method facilitates the biopsy of all areas of the prostate, especially offering easy access to the anterior and apical regions. Many centers have added a proprietary needle guide to more efficiently align the biopsy needle with the ultrasound probe as it is being directed to the intended target.
Materials and Methods
Literature search
The literature search queried PubMed and Embase for “transperineal prostate biopsy,” as well as the terms “free-hand,” “freehand,” and “free hand” transperineal prostate biopsy through June 2020. The search was supplemented through cross references and references found in various articles. The final list was limited to mutually exclusive studies, including recent abstracts, published in English between 2000 and 2020, from which one could clearly extract a series of fTP-Bxs under LA with or without sedation that reported a cancer detection rate (CDR). Updates or subanalyses of previously published series were excluded. Also, to eliminate outlier studies, series with a mean PSA >25 ng/mL, series that included cases of post-treatment prostate cancer (PCa), and series that used spinal or GA in more than 30% of their cases were excluded.
When summing over multiple studies to obtain a denominator for pooled (weighted) averages, studies that did not report the parameter being analyzed were excluded. To obtain a weighted average for a parameter, each reported study average was first multiplied by the study's number of cases, and then, the sum of these products was divided by the total number of cases reporting the specific parameter.
Only the data pertaining to fTP-Bx under LA were extracted, when possible. Important complications were reported both with the exclusion and inclusion of studies that used intravenous sedation (IVS) and/or GA. Classification of the complication of sepsis, acute urinary retention (AUR), gross hematuria (GH), rectal bleeding, and fever relied on the clinical interpretation of the authors of the various articles reviewed. Denominators for different pooled averages vary as not all studies reported every parameter listed in the summary tables.
The literature was also searched for studies on the costs of postprostate biopsy sepsis.
Statistical analyses
Continuous variables were analyzed with paired or unpaired two-tailed Student t-tests based on the sample origins. Nominal variables were analyzed by the chi-square with Yates correction test or Fisher exact test based on sample sizes. Statistical significance was considered at p < 0.05. All statistical analyses were performed with GraphPad Prism 8®.
Results
Our literature search found 11,999 cases among 23 mutually exclusive published articles 5 –27 and 6 published abstracts. 28 –33 Results are summarized from each study in table form and pooled averages gleaned from these reports are listed on the bottom lines.
Demographic and clinical information
The 29 series of fTP-Bxs under LA reviewed in this article, in order of total number of cases reported, come from Italy, the People's Republic of China, the United States, Canada, the United Kingdom, Switzerland, Japan, Taiwan, Singapore, Hong Kong, Norway, and New Zealand (Table 1).
Series of Free-Hand Transperineal Biopsy Under Local Anesthesia (2003-Present) Demographic and Clinical Information
Personal communication, Pepe P.
Calculated by author of this article.
CAMPROBE = CAMbridge PROstate Biopsy; GA = general anesthesia; IVS = intravenous sedation; LA = local anesthesia; MRI/US-TBx = MRI/ultrasound fusion for targeted biopsy; NR = not reported; PPTAS = PrecisionPoint™ Transperineal Access System; PSA = prostate-specific antigen.
Cancer detection rates
Excluding studies that included biopsies for active surveillance (AS), the pooled average CDR was 45.5% (3796/8338) for overall PCa and 25.1% (1141/4541) for clinically significant PCa (csPCa) (Gleason score ≥7) (Table 2). When not excluding studies that included AS, the pooled average CDR was 48.8% (5848/11,979) for overall PCa and 31.9% (2610/8182) for csPCa. After subgrouping the studies analyzed in Table 2 by biopsy technique and excluding studies with AS, the fan pattern/sector techniques yielded an overall PCa and csPCa CDR of 41.3% (2448/5927) and 12.8% (319/2496), respectively, while the studies that used MRI/US-TBx in some or all biopsy cases yielded an overall PCa and csPCa CDR of 50.0% (741/1483) (p < 0.0001) and 42.8% (635/1483) (p < 0.0001), respectively.
Cancer Detection Rate
Patient experience
Pain scores and procedural times were reported as medians, averages, or ranges and not all studies reported these parameters. We used the average of a reported range in calculating the pooled average (Table 3).
Patient Experience
Personal communication, Pepe P.
TMI = testing morbidities index.
Complication rates for fTP-Bx
Most studies and abstracts did not indicate a time frame for complications, but it is assumed that they occurred either immediately after or within a few days of the biopsy except for a case of delayed perianal abscess (Table 4).
Complications
Personal communication, Pepe P.
Excluding IVS and GA.
Including IVS and GA.
Personal Communication, Chen K.
IM = intramuscular; UTI = urinary tract infection.
Postbiopsy sepsis
There were no cases of sepsis among the 7396 cases (0.0% [0/7396]) in studies where fTP-Bx under LA without IVS or GA were clearly delineated. (In a personal communication, Chen and colleagues 28 stated that the initial report of a case of sepsis in their abstract was an error due to a mislabeling of data).
When we included all studies analyzed in Table 4 that reported complications where IVS and GA were also used, Dimmen and colleagues 24 reported one case of post-fTP-Bx sepsis in their series of fTP-Bx with IVS. Their septic patient was reported to have had fever and bacteremia treated effectively with oral ciprofloxacin, but whether this patient had urinary retention was not noted. In addition, Stroman et al. (2020), 29 in an abstract reporting a series containing 28% GA procedures, had 1 case of post-fTP-Bx sepsis in a patient who underwent GA, yielding a pooled average of 0.02% (2/10,386). The GA patient was reported to have gone into urinary retention after the biopsy.
No prophylactic antibiotics were given to 10.2% (1055/10,334) of cases among five studies reporting their prophylaxis protocol and there were no cases of sepsis in these five studies (we excluded two studies that did not specify the exact number of patients who did not receive antibiotic prophylaxis).
Mortality rate
There were no reported mortality rates from fTP-Bxs among the 11,999 cases captured in our literature search.
Acute urinary retention
The pooled average rate of AUR over all studies reporting this complication was 3.1% (276/8982) with a range of 0%–7.1%. This rate fell to 2.1% (120/5693) in the subgroup that excluded studies where LA cases could not be clearly separated from IVS and/or GA cases regarding the rate of AUR (p = 0.0020). AUR decreased further to 1.4% (36/2575) (p < 0.0001) when the subgroup containing only LA cases was limited to those that sampled fewer than 16 cores. The difference between these latter two subgroups was also statistically significant (p = 0.0238).
Gross hematuria
The pooled average incidence of GH was 16.0% (1044/6522). However, the criteria used for reporting GH among the studies varied widely, ranging from observation of red urine to clot retention. Most studies did not distinguish between GH that required intervention (i.e., clot retention) vs self-resolving red urine.
Perianal abscess
Only one case of perianal abscess was reported (Szabo) 5 among the 29 studies in the review, yielding a pooled average of 0.008% (1/11,999).
Fever
The pooled average for fever was 0.5% (25/4745).
Discussion
History of fTP-Bx
Transperineal needle “punch biopsy” of the prostate was first reported in 1942. 34 Although finger-guided TR-Bx was first described in 1937, 35 the transrectal approach to prostate biopsy was not widely adopted until the 1980s with the invention of the 7 MHz transrectal ultrasound probe coupled with the advent of fluoroquinolone antibiotic prophylaxis to prevent postbiopsy sepsis.
In 1981, Holm and Gammelgaard 36 reported on the first fTP-Bx under LA utilizing a biopsy needle holder attached to a transrectal ultrasound probe. They touted the advantage of the transperineal approach in their follow-up publication (Hastak and colleagues), 37 commenting that it was difficult to obtain a tissue specimen from the anterior and periurethral prostate via “conventional posterior approaches.”
However, the transrectal approach to prostate biopsy gained popularity for the next 19 years before Igel and colleagues 38 reported using transperineal saturation biopsy. They used a brachytherapy template device as a biopsy needle guide and noted that the approach provided improved uniform sampling of all prostate regions, especially the anterolateral and midtransition zone regions. They then concluded that the transperineal saturation technique was a reasonable option in patients who were high risk for PCa despite multiple negative transrectal biopsies. Nevertheless, their technique required spinal or GA.
Then, with the quadrupling of post-TR-Bx infectious complications between 1996 and 2005, 39 thought attributable to the increasing incidence of fluoroquinolone resistance in the rectal flora, 40 some centers in Italy, Australia, the United States, Japan, China, the United Kingdom, Norway, and Germany switched from the transrectal to the transperineal approach. 4
The initial prospective, randomized-controlled trials (RCTs) using 8–14 core systematic biopsies compared transperineal and transrectal approaches, with or without a grid template, under general, spinal, or LA. 21,25,27,41,42 Most of these reports and three subsequent meta-analyses 43 –45 of studies using sextant, extensive, and saturation biopsy protocols found no clinically significant difference in CDRs between TP-Bx and TR-Bx. However, a prospective randomized comparison by Takenaka and colleagues 42 did demonstrate that significantly more cores were positive for PCa with TP-Bx, especially in the transition zone, for PSA values between 4 and 10 ng/μL.
Pepe and Aragona, 23 among the early adopters of the transperineal approach, coined the term “freehand” in their 2013 report of 3000 TP-Bxs performed from 2002 to 2012 without the use of a grid template. Since then, reports on series of fTP-Bx under LA have increased in number and frequency, with more than 7000 cases published in the last 3 years.
Evolution of the transperineal biopsy needle guide
In the earlier fTP-Bx series, cores of prostate tissue were taken by direct biopsy needle puncture through the perineal skin. However, as subsequent biopsy protocols increased the number of biopsy cores per procedure, the increasing trauma from the corresponding increase in perineal skin puncture holes required an ever-greater volume of local anesthetic. Then in 2003, Novella and colleagues 43 reported using a 17-gauge coaxial needle as an introducer through a single midline perineal puncture. Besides exploiting the mobility of the perineal skin and the underlying ischiorectal fat, this modification also decreased the volume of anesthetic needed and shortened procedural times.
A further development was the invention of the PrecisionPoint® Transperineal Access System (PPTAS) (Perineologic; Corbin Clinical Resources, LLC, Cumberland, MD) (Fig. 1). This disposable needle guide, approved by the Food and Drug Administration (FDA) in 2016, was used in 11 of the studies found in our literature search. Other proprietary needle guides now also available are usually associated with MRI/US-TBx platforms, including BK Medical, ExactVu™, Koelis Trinity™, and Mindray™/Innofine.

Free-hand transperineal prostate biopsy using a side-fire transrectal ultrasound probe with the PrecisionPoint® Transperineal Access System (Photo Courtesy of Perineologic, Corbin Clinical Resources, LLC, Cumberland, MD).
Biopsy technique effect on CDRs of fTP-Bx vs TR-Bx
Initially, fTP-Bx protocols used a “Fan” pattern for six core systematic biopsies as described by Emiliozzi and colleagues. 27 This pattern, used in conjunction with 8–14 core systematic biopsies in the other previously mentioned RCTs 21,25,41,42 published before 2015, was not associated with a significant difference in overall CDR between fTP-Bx and TR-Bx. Likewise, three later meta-analyses of RCTs and observational studies 44 –46 of sextant, extensive, and saturation biopsy protocols also concluded that there was no statistically significant difference in the overall CDR between the two approaches.
However, in a more recent retrospective study, Jiang and colleagues 10 compared 1216 TR-Bx cases from one hospital to 1746 fTP-Bx cases under LA in another hospital and, after a propensity score adjustment, found that although the overall PCa detection rate between the TR-Bx group and fTP-Bx group was comparable, fTP-Bx detected 13% more patients with Gleason score ≥7 PCa than was detected by TR-Bx. They concluded that TP-Bx has greater diagnostic efficacy than TR-Bx for detecting csPCa.
MRI/US targeting
In 2018, Level 1 evidence from the PRECISION Trial 47 demonstrated that MRI-targeted biopsy (mostly via the transrectal approach) was superior to systematic TR-Bx. Zhang and colleagues 48 presaged this outcome for the transperineal approach when they prospectively compared biopsy outcomes between fTP-Bx with MRI/US-TBx and fTP-Bx with systematic biopsies and found that the former detected a significantly higher rate of csPCa while taking fewer cores. The pooled average CDRs of the studies listed in our literature search also found that the addition of MRI/US-TBx provided a statistically significant advantage in the CDR of overall PCa and csPCa when compared with biopsying with simple fan pattern and/or sector techniques (p < 0.001).
Pepe and colleagues 49 prospectively compared MRI/US-TBx using TP-Bx and MRI/US-TBx using TR-Bx for detection of csPCa. They performed saturation TP-Bx on 200 men, adding 4-core TR-Bx with software-based MRI/US-TBx and 4-core fTP-Bx with cognitive MRI/US-TBx to 95 cases found to have Prostate Imaging–Reporting and Data System ≥4 lesions.
Of the 16 anterior zone cancers among the 60 cases diagnosed with csPCa, the 4-core fTP-Bx with cognitive MRI/US-TBxs found a significantly greater number of csPCas compared with the 4-core TR-Bx with software-based MRI/US-TBx approach (15/16 vs 4/16, p < 0.0001). Peripheral zone cancer detection trended higher with the TP-Bx approach, but the difference was not significant (it must be noted that their definition of csPCa was “Gleason score ≥6 and/or >2 positive cores,” making their findings difficult to compare with other studies of csPCa detection rate).
Then Ber and colleagues 50 offered Level 1 evidence comparing the accuracy of TP-Bx vs TR-Bx in a prospective, noninferiority, within-person trial. Under GA, they targeted the index lesion using software-based TR-Bx MRI/US-TBx and software-based brachytherapy template TP-Bx MRI/US-TBx during the same session. The CDR for csPCa with TP-Bx MRI/US-TBx was significantly higher at 41.6%, compared with 26.0% for TR-Bx MRI/US-TBx (p = 0.029).
A review and meta-analysis by Tu and colleagues 51 pooled 328 cases (including Pepe and colleagues 49 and seven other contemporary studies) of TP-Bx MRI/US-TBxs and 315 cases of TR-Bx MRI/US-TBxs. They found that the transperineal approach detected more csPCa than the transrectal approach, with a pooled CDR of 62.2% (204/328) compared with 41.3% (130/315), respectively (odds ratio = 2.37; 95% confidence interval [CI], 1.71–3.26). After adjusting for differences in cancer prevalence, they concluded that the transperineal route performed better than the transrectal route in MRI-targeted biopsy, especially in detecting csPCa located in the anterior prostate.
Guy's and St Thomas's Hospital in London had already completely converted to fTP-Bx with PPTAS when members of their Urology Center (Neale and colleagues) 7 investigated the need for additional systematic biopsies to avoid missing csPCa when using fTP-Bx with cognitive MRI-TBx. They retrospectively analyzed 282 fTP-Bx patients whose cognitive MRI/US-TBxs were immediately followed by systematic biopsies using a Ginsburg protocol and found that cognitive MRI/US-TBx detected 88% of all the csPCa found, while systematic fTP-Bx found the remaining 12%. After stratifying the results by the MRI Likert score, they concluded that although systematic biopsy was still an important tool, the need for systematic biopsy decreased as suspicion on MRI increased.
Transperineal CDR vs transrectal CDR when using MRI/US-TBx
In analyzing how csPCa is sometimes missed with the transrectal approach, Schouten and colleagues 52 compared transrectal MRI/US-TBx with transrectal 12-core systematic biopsy in 223 patients. They found that both TR-Bx techniques not only had difficulty detecting apical lesions but that the transrectal 12-core systematic biopsies missed cancer in the anterior region 79% of the time, while transrectal MRI/US TBx missed cancer in the dorsolateral region 58% of the time.
Hossack and colleagues 53 analyzed 1132 radical prostatectomy specimens and compared the results of 414 TP-Bxs and 718 TR-Bxs performed preoperatively. TP-Bxs detected proportionally more anterior tumors (16.2% vs 12% [p = 0.046]) and identified them at a smaller size (1.4 vs 2.1 cm3 [p = 0.03]) and stage (extracapsular extension 13% vs 28% [p = 0.03]) compared with TR-Bxs. In explaining the advantage that TP-Bx with MRI/US-TBx has over TR-Bx with MRI/US-TBx in the diagnosis of csPCa, Tu and colleagues 51 observed that the transperineal approach provides easier access to the apex and anterior prostate gland where most of the cancers missed by TR-Bx are located (Fig. 2). fTP-Bx also found anterior cancer in subgroups of patients with prior negative TR-Bx in Szabo 5 and Lo and colleagues's 15 study, 23% and 10% of the time, respectively.

Differences in biopsy needle trajectory (see Schouten et al., 52 Hossack et al., 53 Tu et al., 51 and Vis et al. 54 ). Transrectal: biopsy needle is perpendicular to the thin layer of higher cancer-yielding peripheral zone. Transperineal: biopsy needle is parallel to the horizontally oriented cylinder of peripheral zone and also provides easier access to the apex and anterior prostate gland where most of the cancers missed by transrectal prostate biopsy are located.
Analyzing the influence of biopsy needle trajectory, Vis and colleagues 54 used an ex vivo model to replicate both the transrectal and the transperineal approaches when they biopsied 40 radical prostatectomy specimens. They noted a higher CDR for sextant biopsies simulating the transperineal approach and concluded that when biopsy needles enter the prostate in a longitudinal direction through the apex, the peripheral zone is more efficiently sampled.
Figure 2 illustrates how the trajectory of the TR-Bx needle is relatively perpendicular to the thin layer of higher cancer-yielding peripheral zone, making it easy to overshoot this zone and incorporate a portion of the lower yielding transitional zone. This sampling dilution is even more likely when the peripheral zone layer is compressed by transitional zone hypertrophy. In contrast, TP-Bx needles enter parallel to the horizontally oriented cylinder of the peripheral zone in a trajectory that is more likely to sample only the peripheral zone and avoid the transitional zone.
Patient experience
A key factor determining the acceptability of fTP-Bx under LA in the clinic setting for both patients and urologists is whether the LA provided for fTP-Bx is as good as that provided for TR-Bx. In a prospective RCT comparing fTP-Bx under LA to TR-Bx under LA, Guo and colleagues 21 documented visual analog scale (VAS) pain ratings and found the mean pain rating to be 4.0 (range 1.0–6.0) for 173 fTP-Bx patients and 2.0 (range 0.0–4.0) for 166 TR-Bx patients. In contrast, the weighted average VAS pain rating among the 3868 cases reporting this parameter in our fTP-Bx literature search was 3.17.
Although this pooled average is less than that found in Guo and colleagues's 21 fTP-Bx cohort, it is still higher than what was found in Guo and colleagues's 21 TR-Bx cohort. It is also higher than the pooled average TR-Bx VAS pain rating of 2.6 (p < 0.0001) calculable from a list of 10 studies (comprising 394 cases) in Tiong and colleagues's 55 meta-analysis of LA for TR-Bx.
Smith and colleagues 56 analyzed the differing degrees of discomfort caused by the individual steps of the fTP-Bx procedure and demonstrated that the insertion of the transrectal probe, the injection for anesthesia, and the taking of biopsy cores were associated with VAS pain ratings of 3.08 ± 1.64, 3.29 ± 1.13, and 2.88 ± 1.88, respectively. Although the end-fire transrectal probe used for TR-Bx has an irregular tip and the TR-Bx needle holder augments the thickness of what is inserted through the anus, Guo and colleagues 21 reported that more patients in the fTP-Bx group than in the TR-Bx group claimed that the greatest pain during the procedure occurred during the injection of anesthesia (63.6% vs 17.5%). This is likely because LA for fTP-Bx requires injection of both the perineal skin and pelvic diaphragm, which are often more sensitive than the rectal wall.
In summary, the pooled average VAS pain rating reported in the literature for fTP-Bx under LA is slightly higher than what is reported for TR-Bx under LA. However, efforts to improve LA for fTP-Bx include a recent RCT by Wang and colleagues. 57 They demonstrated a decrease in average VAS pain rating from 3.3 (range 3.1–3.7) for periapical triangle anesthesia to 1.8 (range 1.5–2.2) when they used a novel “branches of perineal nerve” injection. Although their technique seems similar to the techniques described by Emiliozzi and colleagues 27 and Kubo and colleagues, 58 they used double the volume and concentration of lidocaine.
Procedural times are also important in determining the feasibility of fTP-Bx under LA in a clinic setting. The shortest average procedural time reported in the 29 studies reviewed was 7.85 minutes for Ristau and colleagues, 16 but this might be due to the inclusion of a large number of cases that used supplementary IVS, which allows the infiltration of LA to proceed more rapidly.
Excluding cases with IVS or GA, the pooled average for procedural time for fTP-Bx under LA in our review of the literature is longer (19.1 minutes) than that recorded by Guo and colleagues 21 for TR-Bx (14.7 minutes). However, Guo and colleagues 21 took 8–12 cores, whereas the pooled average cores taken for the fTP-Bx studies reporting procedure times in our review were 13.8.
Complications
Postbiopsy sepsis
Our literature search found no cases of sepsis among the 7396 cases (0.0% [0/7396]) of fTP-Bx under LA specifically mentioning whether sepsis occurred. When also including the fTP-Bx studies that used some IVS and/or GA, we found two cases of postbiopsy sepsis, for a pooled incidence of 0.02% (2/10,386). However, even the latter incidence is 50–150 times less than the 1%–3% incidence of sepsis reported after TR-Bx, 40 an incidence that has quadrupled in the last 25 years and is destined to increase in tandem with future increases in antimicrobial resistance. 59 The superiority of fTP-Bx over TR-Bx in avoiding infectious complications is also supported by the fact that 10.2% of the pooled cases from studies reporting antibiotic prophylaxis status in fact received none, yet no cases of sepsis developed even among these patients.
The difference in postbiopsy sepsis between TP-Bx and TR-Bx was studied at a population level when Berry and colleagues 60 reviewed 73,630 patients from the UK National Prostate Cancer Audit from 2014 to 2017. They found that patients who underwent TP-Bx (n = 13,723) were 4.4 times less likely to be admitted for sepsis than those who underwent TR-Bx (n = 59,907) although TP-Bx patients were more likely to be admitted for urinary retention. However, they noted that this higher risk of readmission for urinary retention might have been associated with the widespread use of GA and the larger number of cores taken with TP-Bx during the time period reviewed. They also remarked that after 2017 there had been a shift toward using LA for TP-Bx and toward taking fewer but more targeted tissue cores. They postulated that this change in TP-Bx practice might help reduce subsequent urinary retention and infection rates as well as the need for an overnight admission.
Stroman and colleagues's 29 one case of sepsis was seen in a patient who went into urinary retention following fTP-Bx under GA. Dimmen and colleagues's 24 one case of sepsis had IVS, which may have increased the chance of urinary retention leading to sepsis. Likewise, in 5 of 16 studies reviewed by Grummet and colleagues 4 that reported one case of post-TP-Bx sepsis each (yielding a pooled average of 0.076%), three used GA and one study used IVS (Dimmen and colleagues, 24 also included in our review). These findings suggest that fTP-Bx under LA without IVS or GA is better at avoiding sepsis than fTP-Bx with IVS or GA, although the difference in sepsis rates between these two alternatives is not statistically significant (p = 0.3810).
Recently, a systematic review and meta-analysis 61 of nonantibiotic strategies for the prevention of infectious complications following prostate biopsy found that TP-Bx was associated with significantly reduced infectious complications compared with TR-Bx (risk ratio 0 · 55, 95% CI 0 · 33–0 · 92, p = 0 · 02, I 2 = 0%, participants = 1330, studies = 7) and concluded that TP-Bx should therefore be preferred.
It must be emphasized that post-TR-Bx sepsis is not only life-threatening but can cause devastating permanent disability as illustrated by the case of severe brain injury and peripheral gangrene complicating post-TR-Bx sepsis in our series of 133 TR-Bxs performed before our adoption of fTP-Bx (Szabo). 5 Case reports of the severe consequences of post-TR-Bx sepsis include acute hemorrhagic cerebellar infarction, 62 pressor-induced ischemic gangrene requiring amputation of distal limbs, 63 bacterial meningitis, 64 epidural abscess, 65 bacterial endocarditis, 66 catastrophic hemorrhage due to sepsis-induced thrombocytopenia, 67 diffuse intravascular coagulation, 68 renal failure requiring dialysis, 69 and fatal clostridium ischiorectal abscess. 70
Mortality rate
There were no mortality rates reported in the 11,999 cases reviewed in Table 4 of our literature search. This should be compared with Wei and colleagues's 71 report of a post-TR-Bx sepsis-induced mortality rate of 0.13% in Taiwan and with Johansen and colleagues's 72 estimation of a post-TR-Bx death rate of 10 per year in Norway (average of 8084 biopsies per year, calculated mortality rate: 0.12%).* The latter article was the report of an investigation prompted by the death of a 68-year-old patient from a septic arterial embolus to the brain 6 days after TR-Bx.
Their findings were published the same day an interview and full-page photograph of the bereaved widow and daughter appeared on the front page of Norway's most influential newspaper. The investigation also found that ciprofloxacin resistance increased from 15% in 2013 to about 45% in 2016 and 10% of patients were hospitalized with a diagnosis of infection within the first 60 days after TR-Bx. Shortly afterward, patients in Oslo demanded only transperineal biopsies and the standard of care changed to fTP-Bx under LA.
Earlier studies of large databases 60,73 –75 found it hard to calculate the true incidence of post-TR-Bx mortality rate because of the difficulty of extracting the exact cause of death from the available data within 1–3 months after TR-Bx. However, Loeb and colleagues, 74 in their analysis of 17,472 men from the Surveillance, Epidemiology and End Results (SEER)-Medicare database who underwent prostate biopsy between 1991 and 2007, were able to conclude that men who were hospitalized with an infectious complication had a 12-fold greater 30-day mortality rate compared with those not hospitalized. In any case, because the 1%–3% rate of sepsis after TR-Bx 40,74 is 50–150 times higher than the 0.0%–0.02% rate of sepsis after fTP-Bx demonstrated in our literature search, it follows that the mortality rate from postbiopsy sepsis may also be 50–150 times higher for TR-Bx than for fTP-Bx.
The cost of sepsis
In a systematic review and meta-analysis of 10 studies referencing the cost of post-TR-Bx sepsis, Gross and colleagues 76 reported an inflation-adjusted cost ranging from $8672 to $19,100 per case of sepsis. Length of stay ranged from 1.1 to 14 days and ICU admissions ranged from 1.1% to 25%. Tamhankar and colleagues 77 compared the costs of TR-Bx and TP-Bx complications in their review of 387,879 TR-Bx cases and 98,588 TP-Bx cases performed in the United Kingdom between 2008 and 2019. After noting that the rates of sepsis had nearly tripled for the transrectal route in 2017–2019 compared with 2012–2016, they estimated that the cost for nonelective readmissions for the decade studied was £33,589,527 ($41,395,000) and £7,179,926 ($8,848,000) for the TR-Bx and TP-Bx cohorts, respectively (p < 0.001). Estimated costs per readmission were £2225.00 ($2746) and £1758.00 ($2169) in the TR-Bx and TP-Bx groups, respectively (p < 0.001). They found that infection complications were the main reason for nonelective admission in the TR-Bx cohort, whereas urinary retention was the predominant cause for nonelective admission in the TP-Bx cohort.
Extrapolating the costs of post-TR-Bx sepsis admissions in the United States estimated by Gross and colleagues 76 and assuming a 2% incidence of these admissions among an estimated 1.97 million TR-Bxs per year in the United States, 72 the annual bill for 39,400 admissions for post-TR-Bx sepsis comes to between $341,676,800 and $752,540,000. This represents an added cost to Medicare and insurance companies of $173-$382 for every TR-Bx performed. This extra financial burden does not include emergency room visits for rectal bleeding requiring intervention (2.5%), 40 a complication that is virtually nonexistent after fTP-Bx under LA. The huge cost of post-TR-Bx sepsis also grossly overshadows the cost of the 2.1% incidence of AUR after fTP-Bx under LA that we found in our subgroup analysis.
Acute urinary retention
AUR has often been reported as one of the disadvantages of TP-Bx after several earlier studies reported a higher incidence of this complication after TP-Bx (4%–6%) 4 than that seen after TR-Bx (0.2%–2.6%). 40 However, this may have been due to the use of GA and the larger number of cores taken with saturation biopsy protocols in earlier reports of TP-Bx.
Supporting this observation, Stroman and colleagues 29 found a statistically significant difference in AUR following fTP-Bx under GA (3.3% [6/183]) compared with fTP-Bx under LA (0.25% [1/394]) (p = 0.03) but not under IVS (1.3% [1/77]) (p = 0.30). Although the pooled average rate of AUR in our literature review was 3.1% (276/8982) (Table 4), when we then limited our analysis to the subgroup of fTP-Bx under LA utilizing fewer than 16 cores, the average rate of AUR fell to 1.4% (36/2575) (p < 0.0001). This lower incidence is comparable with the incidence of AUR after routine TR-Bx under LA (0.2–2.6%). 40
Perianal abscess
The patient who developed a Bacteroides fragilis perianal abscess (Szabo) 5 was one of the 88% of patients in that series who did not receive prophylactic antibiotics. Although we have not come across another report of a similar post-TP-Bx complication in the literature, four cases of perineal abscess after injection of the SpaceOAR Hydrogel System were reported to the Manufacturer and User Facility Device Experience Database. 78 It is therefore likely that either a puncture of the rectum or contamination of the perineum by rectal bacteria was responsible for this complication.
Should we use antibiotic prophylaxis for fTP-Bx?
American Urological Association Guidelines 79 state that surgical antimicrobial prophylaxis is recommended only when the potential benefit exceeds the risks and anticipated costs. In considering the risks, the rate of allergic reactions to antibiotics ranges from 0.52% for quinolones to 2.23% for sulfa drugs, 80 and these allergic reactions vary from minor rashes to anaphylaxis. Also, as highlighted in the guidelines, antibiotics suppress normal bacterial flora, which can lead to Clostridium difficile colitis or colonization/infection with resistant organisms. Thus, the relative risks from routine antibiotic prophylaxis for fTP-Bx might outweigh the negligible incidence of sepsis or abscess seen in our literature review.
However, the pooled averages for febrile urinary tract infection (0.7%) and fever (0.5%) found in our literature review are not negligible and argue in favor of the use of antibiotic prophylaxis. In addition, the guidelines 79 remind us that decisions about antibiotic prophylaxis also require comprehensive evaluation of the patients' specific circumstances (i.e., recent history of urinary tract infections, indwelling catheters, and immunocompromise). The answer to this question about antibiotic prophylaxis for fTP-Bx will likely require a large prospective study.
Gross hematuria
The incidence of GH after fTP-Bx varied widely in our literature review, likely because GH is reported for any red urine in some studies, while other studies only reported GH needing intervention. Pooling cases where GH was reported, we found an average incidence of 16.0% (1044/6522). However, eliminating studies averaging >16 biopsy cores brought the rate down to 0.8% (11/1398) (p < 0.0001), an incidence comparable with that seen after TR-Bx (<1% needing intervention 40 ). In any case, it is advisable to avoid puncturing the urethral mucosa in the low-yield paraurethral transitional zone or overshooting into the bladder when biopsying the base of the prostate.
Rectal bleeding
This complication was rarely mentioned in the fTP-Bx studies reviewed, yet it is seen in over 20% of TR-Bxs where it requires intervention in 2.5%. 40 With emergency room visits costing an average of $1096, 81 this exclusively post-TR-Bx complication extrapolates to almost $54,000,000 annually, not including the costs of the subsequent interventions (i.e., rectal balloon tamponade, sclerosis, endoclipping, and blood transfusion).
Limitations of our review of the literature on fTP-Bx under LA
Among the limitations of this review was the inclusion of studies where some IVS and GA cases could not be completely separated from LA cases. Also, there was an absence of standardization of fTP-Bx techniques across different institutions, with variations in biopsy patterns, numbers of cores sampled, and use or omission of antibiotic prophylaxis. Some studies reported a small number of post-fTP-Bx fevers along with a sepsis rate of zero but did not clarify why these fevers were not classified as sepsis. Lastly, six of the studies included were recently published abstracts.
Conclusion
Almost 12,000 cases of fTP-Bx under LA from around the world have been reported in the literature in the last several years, reflecting increasing acknowledgment of the superiority of this approach compared with TR-Bx in both safety, through the virtual elimination of postbiopsy sepsis, and accuracy, through a higher CDR of csPCa when coupled with MRI/US-TBx. Although our literature search suggests that fTP-Bx under LA procedural times are slightly longer and the pain scores are slightly higher than for TR-Bx, they are still comparable. Likewise, the average rate of AUR is also comparable when fTP-Bx under LA utilizes fewer than 16 cores.
The increasing popularity of fTP-Bx under LA confirms the feasibility of incorporating it into the regular clinic workflow for both systematic and MRI/US-TBxs. Moreover, there is now ample evidence that a change in standard of care from TR-Bx to fTP-Bx under LA would save our national health systems hundreds of millions of dollars annually through the near elimination of hospital admissions for post-TR-Bx sepsis. Most importantly, the adoption of fTP-Bx under LA will save lives.
Footnotes
Acknowledgments
Ingrid Rosenthal developed the clarity report spreadsheets from the Kaiser Permanente HealthConnect™ database and Jiaxiao M. Shi, PhD, provided statistical analysis advice.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Southern California Kaiser Permanente provided database service and statistical advice.