
Abstract
Background:
Comparative outcome studies investigating internal Double-J (DJ) and externalized stents have primarily been performed for open and laparoscopic pyeloplasty, with a paucity of literature surrounding outcomes in robot-assisted laparoscopic pyeloplasty (RALP). Furthermore, outcomes of a modified external stent inserted into the renal pelvis, termed cutaneous pyeloureteral (CPU) stent, remain unexamined. This study investigates outcomes of DJ and CPU stents as methods of trans-anastomotic drainage.
Materials and Methods:
A retrospective analysis identified pediatric patients who underwent RALP between December 2007 and January 2020 at a single tertiary center, where CPU stents were introduced in June 2012. Operative success was defined as improved or stable hydronephrosis without subsequent redo pyeloplasty. Secondary outcomes included stent reinsertion, anesthesia requirements, opioid administration, urinary tract infection (UTI), and bladder spasms.
Results:
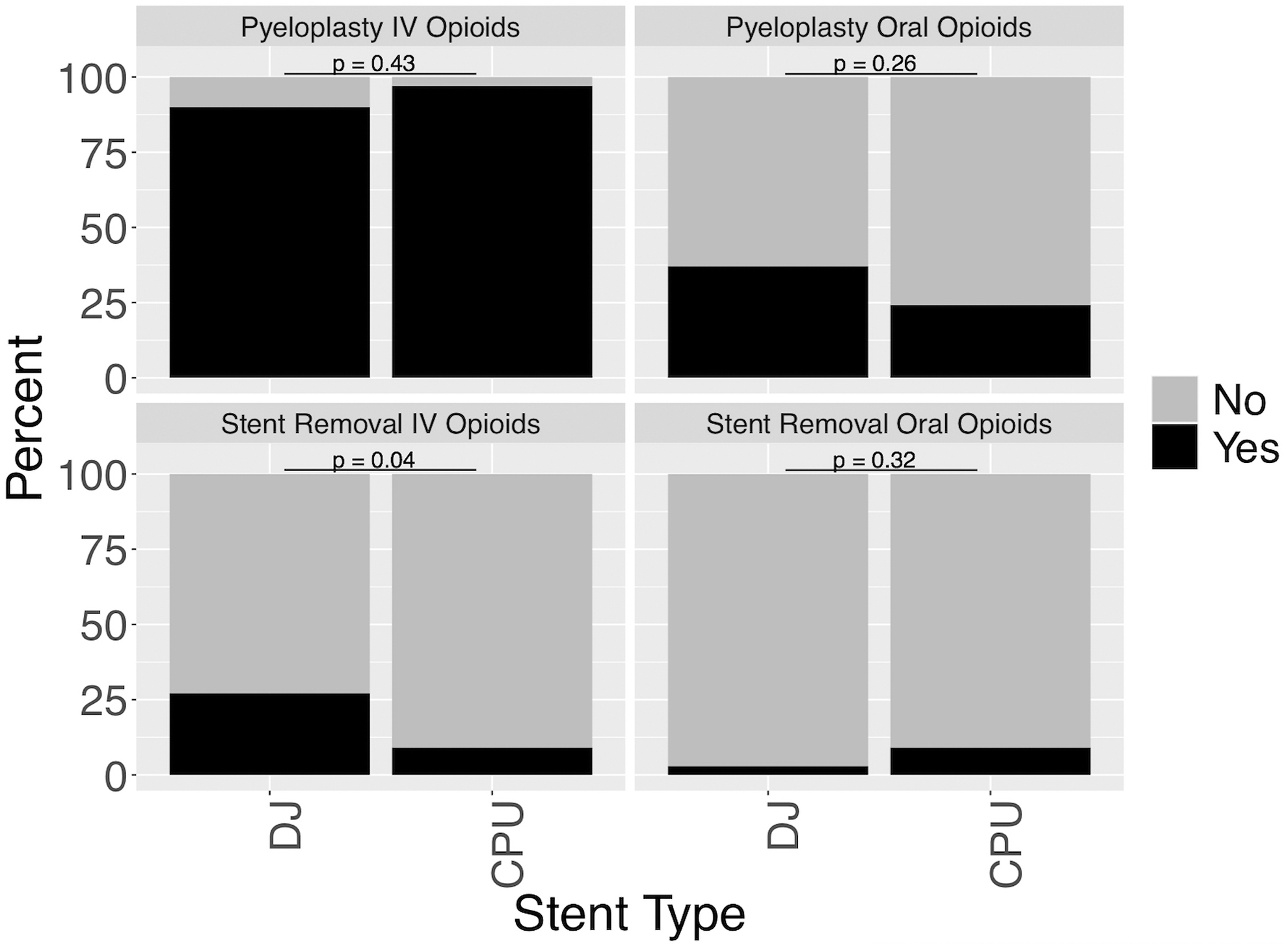
A total of 103 pediatric RALP procedures were analyzed (DJ = 70, CPU = 33). Operative success (DJ = 95.7%, CPU = 100%, p = 0.55), Society for Fetal Urology (SFU) grade improvement, and length of stay were comparable. Accidental stent expulsion was only seen with CPU stents (9%; p = 0.03). Intracorporeal stent migration also occurred more frequently in CPU stents (DJ = 3%, CPU = 15%, p = 0.03). Stent reinsertion, when needed, used a DJ stent with rates of 4% and 9% for DJ and CPU stents, respectively (p = 0.38). DJ stents were removed at a later postoperative day (DJ = 45.2 ± 25.0, CPU = 8.3 ± 4.2; p < 0.001) with increased general anesthesia (DJ = 99%, CPU = 3%; p < 0.001) and intravenous (IV) opioid (DJ = 27%, CPU = 9%; p = 0.04) requirements. Finally, DJ stents had nonsignificant increased rates of UTI (DJ = 17%, CPU = 3%, p = 0.06) and bladder spasms necessitating postoperative medication (DJ = 26%, CPU = 9%, p = 0.07).
Conclusions:
DJ and CPU stents display equivalent success rates in pediatric RALP and similar stent reinsertion rates. Appreciable differences can inform stent selection, including higher general anesthesia requirements and IV opioid administration among DJ stents and a higher incidence of accidental stent expulsion among CPU stents. In addition, DJ stents were associated with nonsignificant increased rates of UTI and bladder spasm necessitating medication.
Introduction
The most common pathologic cause of antenatally detected hydronephrosis is ureteropelvic junction (UPJ) obstruction, which is estimated to affect 1 in 500 live-births. 1 For cases necessitating surgical correction, the Anderson–Hynes dismembered pyeloplasty is the gold standard. 2 Techniques for trans-anastomosis drainage remain controversial and include no stent, internal Double-J (DJ) stent, and various iterations of extracorporeal stents, including “trans-parenchymal” and “trans-renal pelvic.” 3 –6 Adequate comparison of such extracorporeal stents with the more traditional internal DJ stent is critical for appropriate stent selection. 7 Although comparative analyses have been well described for open and laparoscopic pyeloplasty, outcomes are largely unexplored for robot-assisted laparoscopic pyeloplasty (RALP), 8 –11 a technique that continues to gain popularity among pediatric urologists for its shorter hospital stays and fewer reported complications. 12 –15 The objective of this study was to compare the outcomes of DJ internal stent and cutaneous pyeloureteral (CPU) internal–external stent in a large cohort of pediatric patients undergoing primary RALP. The primary outcome was operative success, defined as improved or stable hydronephrosis without subsequent redo pyeloplasty. Secondary outcomes included stent reinsertion, anesthesia requirements, opioid administration, urinary tract infection (UTI), and bladder spasms. It was hypothesized that RALP success rates would be similar between the stent types but that CPU stents would minimize opioid and anesthesia exposure by capitalizing on its ability to be removed in an outpatient setting and would be associated with fewer lower urinary tract symptoms (e.g., bladder spasms and UTI), as it does not reside in the bladder.
Materials and Methods
Operative technique
All RALP procedures were executed using the Anderson–Hynes technique. The CPU stent consisted of a previously described modified Salle nephroureteral stent (Cook Medical, Inc., Bloomington, IN), trimmed at the proximal end, and placed percutaneously to transverse the anterior renal pelvis to the mid-ureter and secured to the skin using 4-0 nylon. 16 An additional stitch to the renal pelvis using 6-0 polydioxanone suture (PDS) in a “purse-string” manner was added during technique optimization. The DJ stent is typically placed in an antegrade manner and courses from the renal pelvis through the UPJ and ureterovesical junction (UVJ), into the bladder. 17
Study sample and inclusion criteria
Primary RALP procedures completed between December 2007 and January 2020 at a single tertiary center were included in this study. Redo pyeloplasty procedures, all of which received DJ stents, were excluded for absence of CPU comparisons. CPU stents were introduced in June 2012. For bilateral operations, each side was counted as an individual data point.
Two stent types were investigated: an internal DJ stent and an internal–external CPU stent. Stent selection was determined by the renal pelvis anatomy and patient preference. Procedures with no stent or other alternatives to the CPU and DJ stent were excluded. Furthermore, patients with UVJ obstruction ipsilateral to the UPJ obstruction were excluded to limit confounding effects on postoperative hydronephrosis and kidney function. Finally, patients with an inaccessible postoperative ultrasound scan after stent removal that precluded determination of operative success were excluded.
Variables
Patient demographic data included sex, age, body mass index, history of operation necessitating anesthesia, and presence of duplex collecting system or solitary kidney. Although some stents were inserted preprocedurally to manage acute obstruction, “stent duration” was defined as the time from pyeloplasty until stent removal. Patients who required a second stent after migration, expulsion, or routine removal of the first stent were grouped according to the original stent that was placed. The primary outcome of operative success was defined as stable or decreased postoperative hydronephrosis on the latest ultrasound scan without subsequent redo pyeloplasty. Hydronephrosis grade was assigned perioperatively by the operating urologist according to the Society for Fetal Urology (SFU) system, which was substituted with resident and radiologist reports if undocumented. 18 Secondary outcomes included stent migration, accidental stent expulsion, stent reinsertion, anesthesia during stent removal, opioid administration, bladder spasm necessitating postoperative medication, infection rate, and postoperative complications. The term “stent migration” was classified as incorrect location of the proximal or distal end of the stent. For all complications, the assumption was made that they would be recorded in the electronic health care record system and/or communicated to the operating urologist. In patients who experienced a postoperative complication, the Clavien–Dindo classification system was utilized with the highest grade reported if multiple complications occurred. 19
Statistical analyses
Fisher's exact tests were used to compare categorical variables and Student's t-tests were used for continuous data. Statistical analysis was conducted with R software (RStudio, Inc., Boston, MA, 2018). Institutional review board approval was received (IRB17-1059).
Results
Over the 12-year period, 132 primary RALP procedures were performed, of which 103 (79%) met the inclusion criteria: 3 had no stent, 8 had ipsilateral UVJ obstruction, and 18 had inaccessible follow-up information. DJ stents were placed in 70 ureters and CPU stents were placed in 33 ureters. Preoperative and demographic data are summarized in Table 1. In both groups, majority of the patients were male (DJ = 71%, CPU = 88%, p = 0.08) and around one-fourth of patients had experienced anesthesia exposure before pyeloplasty. Patients who received DJ stents were older with a mean age of 7.6 ± 6.4 years compared with 3.9 ± 4.9 years for CPU patients (p = 0.002). Preoperatively, the mean SFU grade was comparable between groups (DJ = 3.7 ± 0.7, CPU = 3.6 ± 0.7, p = 0.58).
Preoperative and Demographic Information
CPU = cutaneous pyeloureteral; DJ = Double-J; SD = standard deviation; SFU = Society for Fetal Urology.
Table 2 details the hospital course, which differed significantly regarding operative time, direction of stent placement, intraoperative blood loss, stent duration, and anesthesia and opioid requirement for stent removal. Operative time in minutes for RALP with DJ stents were longer (DJ = 174 ± 53.8, CPU = 149 ± 31.5; p = 0.003) with increased blood loss in mL (DJ = 10.6 ± 6.1, CPU = 8.0 ± 4.5; p = 0.02). On average, DJ stent duration was longer in days (DJ = 45.2 ± 25.0, CPU = 8.3 ± 4.2; p < 0.001). Removal of DJ stents necessitated use of general anesthesia (DJ = 99%, CPU = 3%; p < 0.001) and were associated with higher rates of IV opioid administration (DJ = 27%, CPU = 9%; p = 0.04). Mean length of hospital stay was similar between stent types (DJ = 2.3 ± 1.5, CPU = 1.9 ± 1.3, p = 0.11).
Hospital Course
IV = intravenous.
Finally, Table 3 characterizes the success rate and major complications. The mean length of follow-up by the operating surgeon was 23.4 ± 23.7 months among DJ stents and 21.2 ± 18.3 months among CPU stents (p = 0.61). Patients with DJ and CPU stents experienced comparable reduction in hydronephrosis SFU grades (DJ = 1.6 ± 1.1, CPU = 1.3 ± 1.1; p = 0.13). The success rate was 95.7% for RALP with DJ placement and 100% for RALP with CPU placement (p = 0.55). The distribution of Clavien–Dindo surgical complications was similar among the two groups (p = 0.27) and were as follows: Grade I (DJ = 7%, CPU = 9%), Grade II (DJ = 16%, CPU = 3%), Grade IIIb (DJ = 13%, CPU = 18%), and none (DJ = 64%, CPU = 70%). The rate of postoperative UTI (DJ = 17%, CPU = 3%, p = 0.06) and postoperative oral antispasmatic for bladder spasms (DJ = 26%, CPU = 9%, p = 0.07) were nonsignificantly increased in DJ stents. Intracorporeal stent migration occurred with 2 (3%) DJ stents and 5 (15%) CPU stents (p = 0.03), of which 2 DJ and 2 CPU stents required stent reinsertion or replacement. Accidental stent expulsion did not occur in DJ stents (0%) but did occur in 3 (9%) CPU stents (p = 0.03), with one necessitating replacement. One additional DJ stent required stent reinsertion after stricture development in the postoperative period. All replacement stents were DJ stents.
Operative Success and Complications
Change in SFU grade was calculated as the difference between the preoperative assigned grade and latest postoperative ultrasound grade.
Clavien–Dindo grades were assigned according to the most severe complication that occurred.
UTI = urinary tract infection.
Discussion
This comparative analysis of externalized CPU and internalized DJ stents demonstrates equivocal success rates in the setting of pediatric UPJ obstruction repair by RALP. Our success rates for DJ and CPU RALP were 95.7% and 100%, respectively, which are similar to rates reported by studies of DJ (88%–95%) and other externalized stents (86%–94.7%). 3 All failures in the DJ group had procedures performed in early 2009 suggesting the surgeon's “learning curve” and technique optimization of robot-assisted pyeloplasty may be confounding factors. In 2009, 47% of pyeloplasty procedures were performed robotically, whereas by 2019, 89% were robot assisted. Outcomes of RALP with CPU placement as an alternative to DJ placement are multifaceted and cannot be well-illustrated by success rate alone. Critical examination of the potential advantages and disadvantages of the CPU stent can better inform which patient populations will benefit most from its utilization.
Opioid utilization.
In 2016, the U.S. Food and Drug Administration released a warning regarding anesthetics in young children, especially those less than 3 years of age and those who experience repeated anesthesia exposure. 21 The mechanistic association between early anesthetic exposure and neurotoxicity remains unclear. 20,22 In an effort to minimize exposure in patients with complex medical conditions and histories, the CPU stent can be advantageous. Of all 103 cases included in the study, 25 (24%) had a history of operation necessitating anesthesia. In this regard, use of a CPU stent is advantageous as it can be removed in clinic without anesthesia, unlike DJ stents that require an additional operation for removal. Among 33 cases with a CPU stent, 3 (9%) required additional episodes of anesthesia postpyeloplasty for stent replacement of an expulsed or migrated CPU stent and subsequent removal of the replacement stent. For DJ stents, 69 of 70 (99%) cases required one additional episode of postpyeloplasty general anesthesia, with the exception of one patient who underwent stent removal using incomplete induction to achieve conscious sedation in the operating room. Furthermore, in patients with DJ stents, anesthesia associated with removal was often compounded by utilization of IV opioid analgesics intraoperatively and postoperatively (p = 0.04). When appropriate, placing a CPU stent instead of a DJ stent can generate a multifold impact on risk reduction by reducing subsequent exposures, which is of particular importance given the current opioid epidemic.
Previously, in an effort to minimize anesthesia exposure, a nephroureteral stent was implemented in open pyeloplasty procedures. 16 Unfortunately, the adoption of minimally invasive techniques limited the amount of pressure control that could be applied to stop puncture bleeding as the stent coursed through the renal cortex. In the setting of this dilemma, CPU stents that course transrenal pelvic rather than transparenchymal were introduced as this trajectory limits puncture bleeding to allow for complete visualization of the anastomosis intraoperatively. 16 Alternatively, a modified DJ stent with distal strings would provide benefit in terms of removal without anesthesia, but was not utilized in this study because of evidence of increased expulsion risk and discomfort in toilet-trained children. 22,23 Recently described DJ stents with a magnetic tip (mDJS) provide a novel method for removal in the outpatient setting and may be considered for future use. 24
Although the CPU stent does offer the advantage of reduced anesthesia and opioid exposures, it is important to recognize its limitations. Both stent migration and accidental stent expulsion occurred at higher rates in the CPU stents. Not all cases required stent replacement and the need for intervention was determined by imaging and clinical signs of urine leak or inadequate drainage. Among the three CPU stents that were completely expulsed, one required replacement with a DJ stent. Two CPU stents that migrated intracorporeally required intervention with DJ stent placement. CPU stent expulsion or intracorporeal dislodgement occurred exclusively at the beginning of stent introduction (four in 2013, three in 2014, and one in 2015). Following this pattern, the CPU technique was modified with an additional 6-0 PDS suture that secured the stent to the renal pelvis with a purse string stitch, thereby preventing this complication. In the original methodology, the stitch was not placed because of fear that it would complicate removal, but this has not proved to be the case upon implementation. Of note, reinsertion rates were comparable between DJ and CPU stents because a few DJ stents migrated and required intervention. CPU expulsion and migration rates may also be influenced by the rigid material of the Salle stent, which was designed for intravesical placement and modified for the renal pelvis in accordance with the current technique. A customized stent with increased flexibility may help to further abate these issues in the future.
One key point in maximizing the benefits of the CPU stent as an alternative to a DJ stent is identification of appropriate patient populations. Although patients with concomitant UVJ obstruction were excluded, DJ stents are particularly difficult to navigate across said stricture and CPU stents may provide additional advantage in such cases. Conversely, CPU placement can be difficult in patients with an intrarenal or small renal pelvis, wherein a DJ stent is of higher utility. Age may also play a role and multiple considerations may offer insight into why younger patients tended to receive CPU stents. First, lessening the anesthetic burden, opioid administration and potential neurotoxicity is particularly important in this vulnerable patient group. Second, in a younger pediatric patient population, the CPU stent may offer convenience when monitoring stent output, as the external portion of the stent can be drained into the outer diaper in a “double diaper” apparatus. 25 Finally, it was hypothesized that increased activity level in older patients would increase risk of CPU expulsion, but within the patient cohort, this does not seem to be the case.
Finally, indwelling ureteral stents offer an ideal surface substrate for biofilm formation that may be associated with subsequent UTI with or without clinical symtomatology. 26 Significantly increased DJ stent duration and surface area may explain nonsignificantly increased rates of UTI and bladder spasm necessitating oral postoperative antispasmatic medications. It is possible that our study was underpowered to demonstrate statistical significance in these parameters.
Limitations
Presented findings should be interpreted considering several limitations. First, the generalizability of the results is limited to pediatric patients who underwent primary RALP. Second, confounding bias is possible given the retrospective nature of the study. Third, postoperative diuretic renography could not be used for success determination because it was performed only in a subset of patients exhibiting signs of severe or recurrent hydronephrosis. Finally, earlier cases may have suffered from inadequate documentation owing to lack of widespread use of the electronic medical system. Patients who transferred care were similarly subject to suboptimal documentation.
Conclusion
In summary, DJ and CPU stents display equivocal success as methods of trans-anastomosis drainage in pediatric RALP with similar stent reinsertion rates. However, noting appreciable differences can better inform stent selection, which includes a higher incidence of general anesthesia and IV opioid administration among DJ stents and a higher incidence of accidental stent expulsion and migration among CPU stents. Although DJ stents were associated with higher rates of UTI and bladder spasm necessitating postoperative antispasmatic medication compared with CPU stents, rates were not significantly increased. Appropriate stent selection should consider the factors and outcomes explored above as it pertains to each patient.
Footnotes
Authors' Contributions
A.L., T.T., and C.A.: Collected the data, performed the analysis, and wrote the article. M.S.G.: Conceived and designed the analysis, contributed data, and analysis tools and wrote the article.
Acknowledgment
The authors thank Diboro Kanabolo, MD for contributions to the database.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.