
Abstract
Objectives:
To evaluate the safety and efficacy of ultrasound (US) and primary ureteroscopy (URS) in the management of symptomatic obstructive ureteric stones during pregnancy.
Patients and Methods:
A prospective multicenter study was performed between June 2013 and December 2019, including all consecutive pregnant patients admitted to three urology centers with intractable renal colic with obstructed ureter secondary to obstructive ureteral calculi. Color Doppler ultrasound was used to evaluate renal Resistive Index (RI) and ureter jet. Primary URS was performed to remove the blocking stones. The safety and effectiveness of the procedures were assessed, as well as the stone-free rate (SFR) and the condition of the upper tract after delivery.
Results:
A total of 111 pregnant patients were included with a mean age of 27.4 ± 4.4 years and a mean renal RI of 0.78 ± 0.02. US diagnosed stones in 46.8% of patients, while 100 (90%) patients had altered lower ureter urinary jet, including 86.5% who had URS-confirmed ureteric stones; SFR was 95.8% with no serious urologic, fetal, or obstetric complications. Nine percent of patients had premature delivery, which was significantly correlated with postoperative urinary tract infection and premature uterine contraction (p ˂ 0.0001). In the third-month follow-up of US, all patients showed no residual hydronephrosis. Postoperative follow-up procedures were required in 15.3% of patients.
Conclusion:
Obstructive ureteral stones during pregnancy can be detected safely and appropriately with a combined elevated renal RI and absent ureteral jet detected by Doppler US. Definitive URS is an efficient and safe alternative option for those who fail in conservative management.
Introduction
Renal colic secondary to urolithiasis during pregnancy is the main cause of nonobstetric hospitalization after urinary tract infection (UTI). Complicated renal colic may be associated with an increased risk of spontaneous abortion and an increased risk of premature labor, in particular, with UTI and pyelonephritis. 1,2 Despite being critical for the baby and the pregnant women, the correct diagnosis of obstructive uropathy is not usually straightforward due to such physiologic changes of the upper urinary tract secondary to pregnancy. Gestational hydronephrosis (HN) is more frequent on the right side and can promote the passage of renal stones, thus increasing the incidence of ureteric stones during pregnancy. 3
Ultrasound (US) remains the best imaging modality to diagnose urolithiasis during pregnancy; especially, all imaging studies with hazardous ionizing radiation have teratogenic effects on the fetus. 4 However, the US has a low sensitivity and specificity of 34% and 86%, respectively, in the detection of obstruction as a cause of HN. The absence of a ureteric urinary jet and elevated renal resistive index (RI) detected in renal Doppler imaging can increase the expected rate of obstructed ureteral stones. 5 Change in RI has a sensitivity of 77% and specificity of 83% for the diagnosis of acute unilateral ureteral obstruction in pregnant women. 6
Conservative management considered the first line of treatment for noncomplicated cases of urolithiasis during pregnancy, with a success rate of 50% to 80%. 7,8 However, the use of nonsteroidal anti-inflammatory drugs during pregnancy was linked to fetal pulmonary hypertension and increased the risk to premature closure of the ductus arteriosus. 9,10 Twenty percent to 30% of patients are indicated for aggressive intervention: progressive renal obstruction, single renal obstruction, sepsis, colic persistence refractory to analgesia, and/or obstetric complication (i.e., presence of uterine contraction, premature labor, or preeclampsia), 11 and therefore there should be active management, including percutaneous nephrostomy (PCN), ureteral stent, or definitive management with ureteroscopy (URS). 12
PCN and ureteric stents may be poorly tolerated, subject to bacterial colonization and persistent infection, migration and entrustment of the stent, and subsequent altered drainage and worsening of the obstruction. 9,13 With continued advances in endoscopic equipment, the small caliber URS provides a definitive, safe and less invasive treatment option, especially for patients who fail conservative treatment. 12 –15
Therefore, the aim of the current study was to evaluate the efficacy of renal US assisted by color Doppler ureteric jet and renal RI for the diagnosis of obstructive uropathy during pregnancy and the outcomes of definitive URS for management of obstructing ureteric stones not responding to conservative options during pregnancy.
Patients and Methods
Study design
This prospective multicenter study was conducted in pregnant women who were admitted to the emergency departments of three urology centers (Zagazig university hospital, El-Mina university hospital, and Ismailia insurance hospital) between June 2013 and December 2019. Patients eligible for the study were those who presented with persistent renal colic secondary to obstructing stones, which were not responding to conservative management within 2 weeks, presence of progressive HN, renal colic-induced premature uterine contractions (PUCs) unresponsive to tocolytics, and unilateral obstructive ureteral stones in single kidney. Exclusion criteria included patients with severe renal impairment, uncontrolled UTI or sepsis, bilateral obstruction, congenital renal and ureteric anomalies, history of ureteral stricture, and/or a history of ureteral open surgery.
The diagnosis was based on the clinical manifestations, transabdominal US, and renal Doppler ultrasound to assess the renal RI of the obstructed kidney and change in the ureteric jet of urine within the urinary bladder. Demographic and preoperative data were collected, including patient age, clinical presentation, gestational age, complete obstetric history, previous procedures, and passage of stone, as well as physical examination and a comprehensive laboratory workup. On admission, all patients underwent a transabdominal US examination to assess fetal and urinary tract obstruction status and the degree of HN. Mild, moderate, and severe HN was defined as a renal pelvis diameter of <15, 15–20, and >20 mm, respectively.
Doppler ultrasound of the urinary bladder was performed for all patients to assess the change of the ureteric jet of urine for 5-minute, which was confirmed in the contralateral decubitus position. In addition, the renal RI measured, and defined as the peak diastolic velocity subtracted from the peak systolic velocity, divided by the peak systolic velocity. An abnormally elevated RI was defined as ≥0.70 and a _significant ΔRI (interrenal difference in RI) as ≥0.08, or a difference of more than 0.04 between the obstructed and the contralateral kidney. The length of hospital stay, perioperative adverse events, and long-term complications were recorded.
Surgical procedure
All patients who met the inclusion criteria and confirmed obstruction by US evaluation were admitted after obstetric consultations for assessment of the maternal and fetal conditions, while anesthetic assessment was performed just before the intervention. The procedure was performed under spinal anesthesia and prophylactic antibiotics 1-hour before the procedure. Cystoscopy was performed with identification of the ureteral orifice of the affected renoureteral unit. A sensor guide wire was introduced into the ureteric orifice and advanced under direct vision through a small caliber 7.5–8F semirigid ureteroscope up to obstruction site. The sensor guidewire was then advanced to bypass the obstructed site to the kidney. A ureteroscopy forceps or zero tip Dormia basket was used to remove the obstructive calculus, with or without active disintegration of the stone by the pneumatic lithoclast or the holmium laser. A ureteral Double-J stent was then placed with its string fixed outside, unless there was a ureteral stricture, ipsilateral renal stones, significant residual stones, or iatrogenic ureteral trauma (long-term Double-J stents were fixed). The entire procedure was monitored by real-time US to ensure the appropriate positioning of the guidewire and ureteral stents.
All patients were followed regularly during the pregnancy period, including an obstetric and urologic assessment with monthly urinalysis and culture. The primary endpoints were the safety of the procedure on the mother and fetus and the stone-free rate (SFR), defined as the total absence of stone fragments during the URS. Secondary endpoints included perioperative adverse events such as UTI or sepsis, hematuria, stone migration, and ureteral stent migration.
Ethical Standards
All procedures performed in studies were in accordance with the ethical standards of the institution and/or National Research Committee and with the code of ethics of the World Medical Association Declaration of Helsinki (1964) and its later amendments. The study was approved by the Institutional Ethics Committee (4165) with the informed consent of all patients who participated in the study.
Statistical analyses
Statistical analyses were performed using the Statistical Package of Social Science (SPSS) software, version 20.0 (IBM Corp, NY). Data were presented in terms of numbers and percentages for categorical variables and mean (SD) or medians and interquartile ranges for continuous variables, depending on the normality of data distribution. The Fisher's exact test was used to compare categorical variables, while the t-test of an independent-sample was used to compare the quantitative variables. A p-value of below 0.05 was considered as an indicator of statistically significant differences.
Results
A total of 111 pregnant patients with unilateral ureteric obstruction were included in the study (Fig. 1), with a mean age ± SD (range) of 27.4 ± 4.4 (19–39) years, mean gestational age of 23.2 ± 5.9 (10–37) weeks, and a mean serum creatinine of 1.03 ± 0.36 (0.4–2.3 mg/dL).
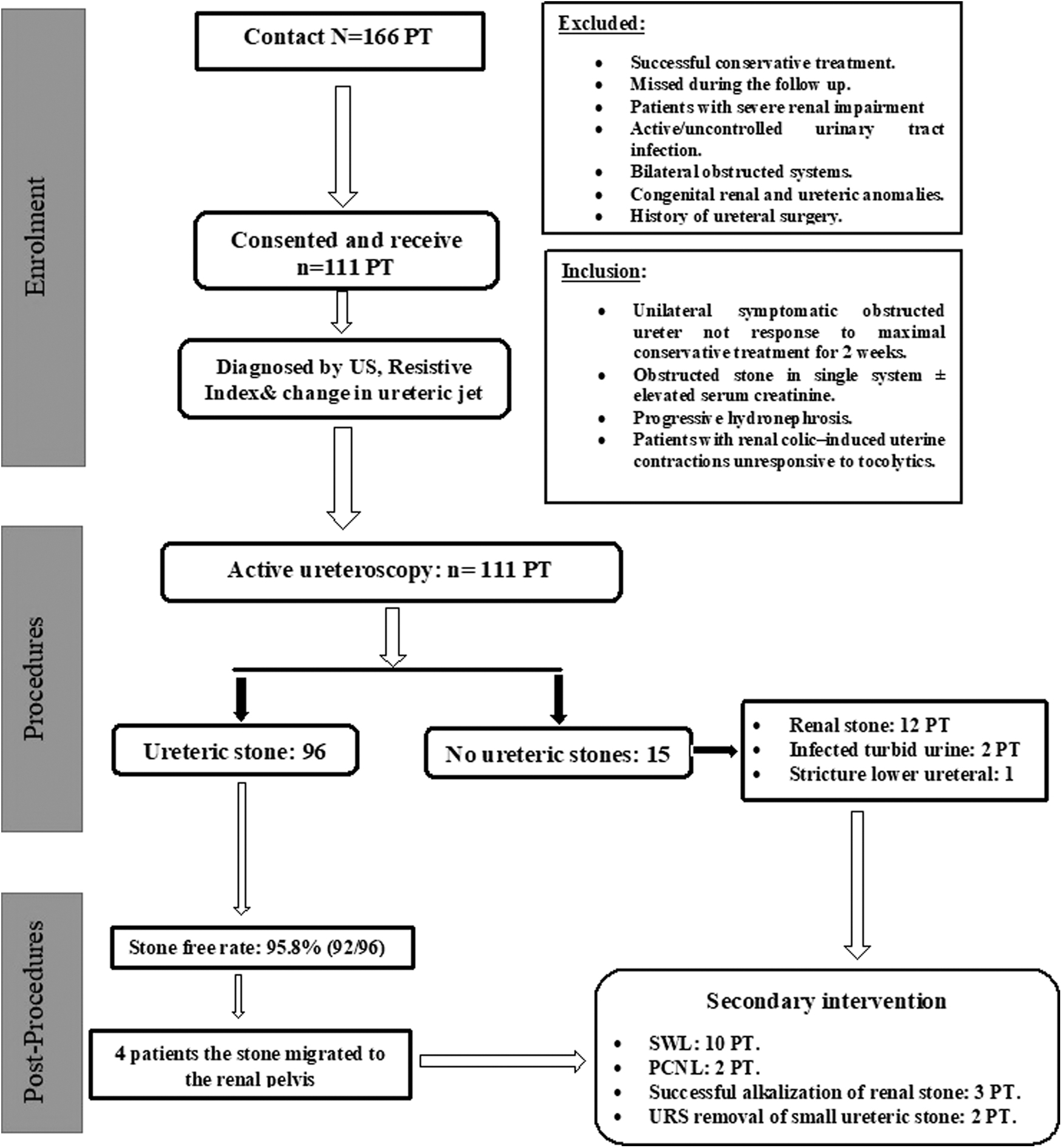
Flowchart of the study population.
Five (4.5%), 80 (72.1%), and 26 (23.4%) patients were admitted during the first, second, and third trimesters of pregnancy, respectively. The main presenting symptoms were renal colic in 107 (96.4%) patients associated with irritative voiding symptoms in 67 (60.4%), hematuria ± pyuria in 52 (46.8%), fever in 24 (21.6%), and PUC in 29 (26.1%) patients. Thirty-nine patients (35.1%) reported positive urine culture. Obstruction in the only functioning kidney was detected in 10 patients (9%), including 7 (6.3%) of whom had elevated serum creatinine levels above the normal range. Otherwise, all other patients had average serum creatinine. Right renal obstruction was found in 72 patients (64.87%) (Table 1). Mild, moderate, and severe ipsilateral HN was reported in 14 (12.6%), 75 (67.6%), and 19.8 (19.8%) of patients, respectively. Preliminary color Doppler US diagnosed stones in 52 (46.8%) patients, with a mean stone size of 9.4 mm (7–15 mm). A hundred patients (90%) showed absent or low frequency ureteral urinary jet, which was confirmed with contralateral decubitus position, including 96 (86.49%) patients with ureteric stones confirmed by URS. Eighteen (16.21%), 30 (27.02%), and 48 (43.2%) patients had upper, middle, and lower ureteral stones, respectively. Renal RI was measured in 97 (87.3%), with a mean RI of 0.78 ± 0.02 (0.73–0.87), including 85 (88.5%) patients with RI >0.70 and were confirmed to have ureteral stones (Table 2).
Demographic and Clinical Data of the Pregnant Women with Obstructive Uropathy
Data presented as mean ± SD (range) or frequency (%).
The Diagnostic Ultrasonography Results in the Study
RI = resistive index; US = ultrasound.
Primary URS was effective in all patients with a mean operating time of 33.0 ± 8.7 (12–55) minutes and a SFR of 95.8% (92/96 patients). Fifteen (13.5%) patients reported no ureteral stones during diagnostic URS. Ureteral calculi were removed without fragmentation in 12 (12.5%) patients, while pneumatic and laser lithotripsy were used in 68 (70.8%) and 16 (19.7%) patients, respectively, with a mean intracorporeal lithotripsy time of 15.2 ± 0.8 minutes. All patients had a ureteral stent inserted at the end of the procedure. Ureteral stents were removed after 2-week in 92 (82.9%) patients without anesthesia, while 19 (17.1%) patients needed long-term stenting, including four with migrated stones, 12 associated with renal stones, 2 with impacted stones in single systems, and 1 patient had stricture in lower ureter that required transureteroscopy ureteral balloon dilatation. Eight patients had minor intraoperative adverse events, including ureteral edema, minimal mucosal laceration, and minimal bleeding without further intervention. No serious perioperative urologic, fetal, or obstetrical complications were observed. The mean time of hospitalization was 72.2 ± 5.5 hours (Table 3). Post-URS UTI was found in 15 patients (13.5%) and was safely managed with antibiotics. Twenty-two patients reported persistent irritative voiding symptoms, of which 19 had long-term ureteral stents, while renal colic was observed in eight patients, responded to acetaminophen-based medications.
The Results of Ureteroscopy During Pregnancy
Data presented as mean ± SD (range) or frequency (%).
LUTS = lower urinary tract symptoms; PUC = premature uterine contraction; URS = ureteroscopy.
Sixteen patients (14.4%) had postoperative PUCs, of which 10 responded to tocolytics, while the remaining 6 had premature deliveries. Full-term delivery occurred in 101 patients (90.9), while 10 patients (9.1%) experienced premature delivery from 35 to 37 weeks. Premature delivery was significantly related to postoperative UTI (p < 0.001) and PUC (p 0.001) (Table 4).
Procedures and Clinical Outcome in Patients With and Without Preterm Labor
Statistically significant differences; **highly statistically significant differences.
RR = relative risk.
HN was alleviated in all patients within 3 months of childbirth. Postdelivery additional radiologic studies was required in 19 patients with long-term ureteral stenting, with additional adjunctive therapy in 17 patients; including extracorporeal shockwave lithotripsy (SWL) in 10 patients with renal pelvic stones, percutaneous nephron-lithotomy (PNL) in 2 patients, alkalization in three patients with renal stone, and another URS for removal of small ureteric stones in 2 patients (Table 4). Stone analysis was carried out in 78/111 patients, where calcium oxalate was the principle component in 39, calcium phosphate in 36, and uric acid stone in 3 patients.
Discussion
The diagnosis and management of obstructive uropathy during pregnancy is complex and critical to urologists and obstetricians. This may be influenced by the physiologic HN, which may be detected during pregnancy. A complicated and persistent renal colic would increase the risk of PUC, premature membrane rupture, and premature delivery. 1 This condition may be critically aggravated by sepsis or increased serum creatinine secondary to a single obstructed system. Therefore, an optimal diagnosis and management are warranted, taking into account all possible risks and benefits to minimize harm to the fetus and mother. 16
Although noncontrast CT is the standard radiologic assessment of the stone disease in nonpregnant women with high sensitivity and specificity, the available guidelines recommend the need to weigh the risks of exposure to ionizing radiation with the risk and benefit for accurate diagnosis, worsening of disease, and better to avoid routine imaging with ionizing radiation in pregnant women. 17 Recent advances in the US machine technology have increased its sensitivity in the diagnosis of obstructive urolithiasis during pregnancy. Therefore, US is the safest, noninvasive, timely, and cost-effective first-step tool for the diagnostic assessment of the pregnant patients with renal colic. However, US cannot easily differentiate calcular-obstructed ureter from the physiologic HN associated with pregnancy. 18
In this study, most patients were admitted during the second and third trimesters of pregnancy and renal colic was the major symptoms. US showed different degrees of HN and 47% of patients had stones documented with US, which was comparable to what had been reported previously. 19,20 When ultrasound results are inconclusive in diagnosis of obstructed stone, alternative diagnostic modalities should be considered. Interestingly, the color Doppler US showed an abnormal ureteral urinary jet in 90% of our patients and was confirmed in the contralateral decubitus position, 21 including 86% with URS-confirmed ureteric stones. Andreoiu and MacMahon reported that the absence of a ureteric jet improved the accuracy of US in predicting ureteral stones from 56% to 72%. 5 However, this finding should be interpreted with caution since compression of the ureter by the gravid during later pregnancy may affect the symmetry of the ureteral jet. 22 Therefore, the absence of ureteral jets should be confirmed in the contralateral decubitus position as suggested earlier, 18 and was conducted in the present study.
Increased renal vascular resistance during acute ureteral obstruction reduces the diastolic blood flow and increases the renal RI, which can be measured by the renal Doppler. Renal RI remains unchanged throughout the course of pregnancy and unaffected by the physiologic HN of pregnancy, 23 with a sensitivity of 95% and a specificity of 100% in detecting obstructing ureteral calculi. 6 In our study, 88.5% of patients with obstructed ureteral stones had a renal RI above the normal value (0.7). Moreover, the combining of the ureteric urinary jet with renal RI increased the detection rate of obstructing calculi in comparison with US alone during pregnancy, as confirmed by URS.
When conservative measures fail in pregnant patients to control renal colic and obstructive uropathy, the definitive management of stone should be considered, especially with the availability of flexible and small caliber ureteroscopes. 24 Deters and coworkers recommended ultrasound-guided URS as a viable option for the gravid patient with suspected urolithiasis, as it allows intraoperative monitoring of wire positioning, ureteroscope location, and stent placement. 25 Wymer and colleague, concluded that the URS was ultimately more cost-effective than serial stents every 4 weeks. 14 Furthermore, the recent AUA guidelines support URS as a definitive alternative option to temporizing stent or nephrostomy in pregnant women who fail the trial of observation for ureteral stones. 12
URS can be safely performed during the second trimester of pregnancy in higher institutes with advanced neonatal and obstetric services to minimize the risk of PUCs and spontaneous abortion. 24 In the current study, semirigid URS was used for diagnostic purposes, accessing all aspect of the ureter in all patients without difficulty using follow-the-wire technique 26 and active stone management without exposure to ionizing radiation. Under US monitoring, the guidewires and ureteral stents were introduced into the renal pelvis at the end of URS, which is consistent with what had been done previously. 25 Despite the relaxing effect of progesterone on the ureteral orifices, 12.6% of our patients required ureteric balloon dilatation, which is consistent with the previous reports. 20,27,28 In our study, the SFR was 95.8%, stones were effectively fragmented in 87.5% with the use of pneumatic and laser lithotripsy and no serious peroperative urologic, fetal, or obstetric complications were detected, which is comparable to similar studies. 20,27,28,30,31
Several studies have approved the safety and efficacy of pneumatic lithotripsy and holmium laser during pregnancy 15,20,28 ; especially, the latter produce low shock waves with minimal tissue penetration, limiting the risk of fetal injury, with less probability of stone migration. Post-URS UTI was identified in 13.5% of our patients and was treated safely with antibiotics, without major adverse events, ureteral perforation, or obstetrical complications. A systemic review showed comparable complication rates for pregnant women undergoing URS, compared to the stone guidelines for nonpregnant ladies. 13 Furthermore, Wymer and colleagues found that the definitive URS during pregnancy was ultimately less costly and more effective. 14 This approach was endorsed by the American guidelines as a definitive alternative option for those who failed the observational approach for ureteral stones.
In the current study, 16 (14.4%) patients had postoperative PUC, including six patients who showed preterm delivery with significant correlation to postureteroscopy UTI, which was comparable to the findings of Butticè and his colleagues. 18 Three months after delivery, preexisting HN was relieved for all patients. Adjunctive postoperative procedures for stone clearance were needed in 19 patients; most of them had associated nephrolithiasis, including SWL, PNL, and chemolysis, where URS was only required in two patients for removal of small ureteric stones. Johnson et al., reported an overall obstetric complication rate of 4.3% in 46 gravid patients undergoing URS at five institutions. 31
The main limitation of the present study resides in its retrospective nature without control, which may inevitably be affected by selection bias. However, the sample size is appropriate to validate the study conclusions, especially with the multicenter nature and long-term experience, indicating its reproducibility. Despite that this is not the scope of the present study, the lack of patient stratification by the gestational age may represent another limitation.
Conclusion
Obstructive ureteral stones during pregnancy can be detected safely and adequately with a combined high renal RI and absent ureteral jet detected by Doppler US. Renal RI may be affected by the concomitant nephrolithiasis or ureteric compression by gravid uterus, therefore, altered ureteric jet of urine detected in the contralateral decubitus position may increase the diagnostic accuracy for obstructing ureteral stones. The definitive URS with pneumatic or holmium laser lithotripsy is an effective and safe alternative option for those who fail to the conservative management of ureteral stones during pregnancy.
Footnotes
Authors' Contributions
Study concept: E.A.S., A.A.R, and E.R.T. Conducted, managing, and follow-up of the cases: E.A.S., A.A.R., and E.R.T. Methodology, data analyzing, and article drafting: E.A.S., A.A.R., E.R.T., and M.F.R. Article and last revision: E.A.S., A.A.R., E.R.T., and M.F.R.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.