
Abstract
Purpose:
To compare preoperative midstream urine cultures (PMUC) and renal pelvic urine culture (RPUC) or stone culture (SC) in predicting systemic inflammatory response syndrome (SIRS) and urosepsis after percutaneous nephrolithotomy (PCNL).
Methods:
We searched the PubMed, Web of Science, and EMBASE databases up to September 1, 2020, for relevant published studies. Two authors independently confirmed whether the literatures met the inclusion criteria and collected the data from the selected literatures. A meta-analysis was performed with Review Manager Software 5.4.1. A total of 14 studies with 3540 patients were selected and analyzed in the meta-analysis.
Results:
Pooled data showed that SC was associated with a higher sensitivity (odds ratios [OR] 2.36, confidence interval [95% CI] 1.31–4.25; p < 0.00001), positive predictive value (PPV) (OR 1.54, 95% CI 1.18–2.01; p = 0.16) and negative predictive values (OR 1.17, 95% CI 1.01–1.37; p = 0.06) in the diagnosis of SIRS and urosepsis after PCNL, and RPUC provided a significantly higher specificity (OR 2.70, 95% CI 2.16–3.38; p = 0.07) and PPV (OR 2.17, 95% CI 1.49–3.15; p = 0.48) than PMUC in the diagnosis of SIRS and urosepsis after PCNL.
Conclusion:
Intraoperative SC and RPUC are more reliable than PMUC in predicting postoperative SIRS and urosepsis, identifying causative organisms, and directing antibiotic therapy for patients who underwent PCNL. PMUC, SC, and RPUC should be routinely collected for the diagnosis and management of SIRS and urosepsis after PCNL.
Introduction
Percutaneous nephrolithotomy (PCNL) has been the first-line therapy for patients with large renal stones (≥20 mm) since 1976. 1 Despite ensuring sterile preoperative midstream urine cultures (PMUC) and providing preoperative antibiotic prophylaxis, postoperative infectious complications may often occur, including systemic inflammatory response syndrome (SIRS) and urosepsis. 2
Urosepsis often evolves from SIRS, which occasionally progresses to septic shock with a devastating mortality rate of 50% to 66%. 3,4 It was reported that the incidence of SIRS and urosepsis in patients who underwent PCNL was 10% to 35% and 0.3% to 4.7% respectively. 1,5 Infected stones, obstructed kidneys, difficult access, prolonged manipulation, and comorbidity are responsible for these complications, often decreasing patient comfort, prolonging hospitalization, and escalating health care costs. 5 Therefore, there is a need to identify the patients at risk for SIRS and urosepsis after PCNL.
In the past, it was not reliable for clinicians to rely on blood culture to diagnose sepsis, because blood culture was often not positive for urinary tract infection (UTI), and, more importantly, has a certain time delay. 6 Now, instead of blood cultures, PMUC, renal pelvic urine culture (RPUC), and stone culture (SC) are suggested as the important factors to predict the occurrence of postoperative SIRS and urosepsis.
Several studies have shown that PMUC, RPUC, and SC results can predict postoperative SIRS or urosepsis, and that SC and RPUC were more accurate than PMUC in this regard. 3,7 –10,11,12 However, other studies suggested that PMUC, RPUC, and SC are not associated with postoperative SIRS or urosepsis. 13 –15 Considering the inconsistence among published studies, the current meta-analysis was conducted to identify the differences between PMUC and RPUC or SC in predicting postoperative infectious complications after PCNL.
Methods
The ethical approval was waived due to the design of meta-analysis in the current study.
Data sources and search
A literature review of articles that compared the differences between urine culture and SC in predicting infection after PCNL was performed. We conducted a systematic literature search in the PubMed, Web of Science, and EMBASE databases to identify relevant studies until September 1, 2020. The following search algorithm was used by two of the authors independently: (percutaneous nephrolithotomy OR PCNL OR PNL OR micro-percutaneous nephrolithotomy OR percutaneous lithotripsy OR mini-PCNL) AND (preoperative midstream urine cultures OR urine cultures) AND (stone cultures). The reference lists from the relevant studies were also conducted to identify additional eligible studies.
Study selection and quality assessment
The article selection was carried out independently based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 16 The included studies fulfilled the following criteria: (1) literature language limited to English; (2) the patients were adults and diagnosed with complex renal or upper ureteral stones; (3) the patient underwent PCNL; and (4) the study compared the differences between PMUC and SC in predicting postoperative SIRS or urosepsis. The studies meeting any of the following criteria were excluded: (1) failure to meet all of the inclusion criteria; and (2) publication type as letters, conference articles, reviews, and comments. The methodologic quality of those cohort studies was evaluated by the Newcastle/Ottawa Scale (NOS), 17 which comprised three factors: (1) selection of patients; (2) comparability of the study cohorts; and (3) outcome. The levels of evidence were rated for each selected study based on the criteria provided by the Oxford Centre for Evidence-based Medicine. 18
Data extraction and analysis
Two authors independently confirmed whether the literatures met the inclusion criteria and collected the data from the selected literatures. Any disagreements were documented and resolved by consensus among all the authors. Data from each included literature were extracted, including the first author, study country, year of publication, sample size, the number of positive PMUC and SC, and related postoperative SIRS and urosepsis outcomes.
In the meta-analysis, the sensitivity, specificity, positive predictive values (PPV), and negative predictive values (NPV) of PMSU, RPUC, and SC were calculated. Odds ratios (ORs) with confidence interval (95% CI) were calculated to assess the differences between PMUC and SC in predicting postoperative SIRS or urosepsis. Mean differences (MDs) and standardized mean difference (SMD) were used for the continuous parameters according to the scales among studies. We assessed the statistical heterogeneity of the included studies with the inconsistency (I 2 ) and Cochrane chi-square (χ 2 ) test. A p-value <0.10 or I 2 value >50% indicated the existence of significant heterogeneity. 19 A random-effects model (DerSimonian–Laird method) was assessed for low heterogeneity, and a fixed-effects model (Mantel–Haenszel method) was used for high heterogeneity among studies. 20,21 A sensitivity analysis was carried out by using a leave-one-out approach. A subgroup analysis was carried out by PMUC and SC to predict postoperative SIRS or urosepsis. A funnel plot was used to assess potential publication bias. 22 The meta-analysis was performed with Review Manager Software (RevMan v.5.4.1; Cochrane Collaboration, Oxford, United Kingdom) and STATA 12.0 (Stata Corp LP, College Station, TX).
Results
Characteristics of included studies
A total of 617 potentially relevant studies were identified, 357 of which were duplicates. After screening title and abstract, 231 studies were excluded, leaving 29 articles for full article review. Finally, 14 studies published between 2005 and 2019 that met the inclusion criteria were selected and analyzed (Fig. 1). No additional records were identified through reference lists. The included studies reflected modern clinical practice, the data of which were available for analysis on 3540 patients. The baseline characteristics of the 14 studies are shown in Table 1 and they consisted of 11 prospective comparative studies (PCS) 3,9,10,11,13 –15,23 –26 and 3 retrospective comparative studies. 8,12,27 The occurrence of at least two or more of the following criteria during the inpatient stay was diagnostic of SIRS: (1) leukocyte count, <4000 or >12,000 cells/μL; (2) fever, >38°C or <36°C; (3) respiratory rate, >20 breaths/min; (4) heart rate, >90 beats/min. 28 Urosepsis was defined as the presence of UTI together with SIRS or at least two criteria of the quick sepsis-related organ failure assessment (q-SOFA): (1) respiratory rate of ≥22 breaths/min; (2) systolic blood pressure of ≤100 mm Hg; (3) altered consciousness (Glasgow Coma Scale score of <13). 29 In addition, inconsistencies were noted among included studies regarding the definition of SIRS and urosepsis. The duration and dose of antibiotic prophylaxis received by patients with UC− (negative urine culture), UC+ (positive urine culture) in the included studies are also listed in Table 1. According to the quality assessment of cohort studies of NOS, a total of nine high-quality studies and five medium-quality study were assessed in this meta-analysis and the procedures of quality assessment are illustrated in Table 2.

Flow diagram of studies identified, included, and excluded during the selection process. PCNL, percutaneous nephrolithotomy; SIRS, system inflammatory reaction syndrome.
Characteristics of Included Studies
NE = not evaluated; NR = not reported; LE = level of evidence; PCS = prospective comparative study; RCS = retrospective study; SD = systemic inflammatory response syndrome was defined as at least two of the following criteria: (1) leukocyte count, <4000 or >12,000; (2) fever, >38°C or <36°C; (3) heart rate, >90 beats/min; (4) respiratory rate, >20 breaths/min; UD1 = urosepsis was defined as two or more criteria of quick sepsis-related organ failure assessment: (1) respiratory rate of ≥22 breaths/min; (2) altered consciousness (Glasgow Coma Scale score of <13); (3) systolic blood pressure of ≤100 mm Hg; UD2 = urosepsis was defined as the presence of a source of infection together with systemic inflammatory response syndrome; UN = treat until a negative urine culture.
Risk-of-Bias Assessment for Included Cohort Studies
a = representativeness of the exposed cohort; b = selection of the nonexposed cohort; c = ascertainment of exposure to implants; d = demonstration that outcome of interest was not present at start of study; e = study controls for the most important factor; f = study controls for any additional factor; g = assessment of outcome; h = was follow-up long enough for outcomes to occur; and i = adequacy of follow-up of cohorts. A study was considered low quality with 0 to 3 points, moderate quality with 4 to 5 points, and high quality with 6 to 9 points.
As shown in Supplementary Figure S1, the baseline characteristics were evaluated and compared among the included studies. No significant statistical differences were identified for age (MD −1.24 years, 95% CI −3.03 to 0.54; p = 0.17, I 2 = 60%), female (OR 1.10, 95% CI 0.67–1.81; p = 0.71, I 2 = 72%), body mass index (MD −0.61, 95% CI −1.51 to 0.29; p = 0.18, I 2 = 92%), surgery history (OR 1.23, 95% CI 0.99–1.54; p = 0.07, I 2 = 47%), serum creatinine (MD −0.06 mg/dL, 95% CI −0.12 to 0.01; p = 0.10, I 2 = 94%), hypertension (OR 1.11, 95% CI 0.79–1.57; p = 0.62, I 2 = 0%), and stone burden (SMD 0.65, 95% CI −0.25 to 1.55; p = 0.16, I 2 = 98%). Of note, there were significant statistical differences for stone-free rate (OR 0.55, 95% CI 0.44–0.69; p < 0.00001, I 2 = 25%).
Meta-analysis results
PMUC vs SC
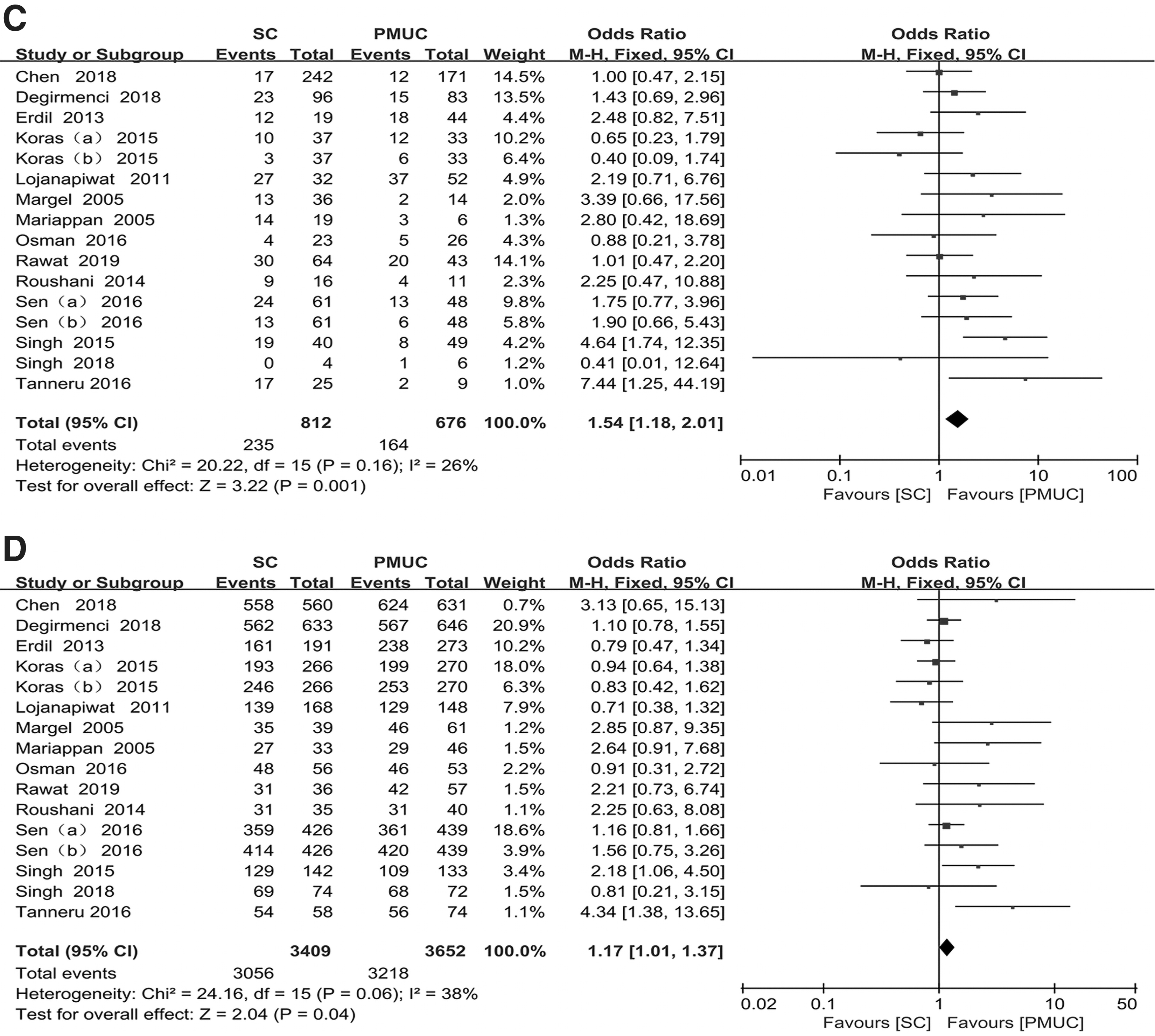
Fourteen studies compared the differences between PMUC and SC in predicting postoperative SIRS and urosepsis, of which two studies summarized the data of both SIRS and urosepsis; so, we analyzed twice each of them. Figure 2 lists the sensitivity, specificity, PPV, and NPV for SIRS and urosepsis between PMUC and SC. Also, compared with PMUC, SC provided a significantly higher sensitivity (OR 2.36, 95% CI 1.31–4.25; p < 0.00001, I 2 = 74%, Fig. 2A), PPV (OR 1.54, 95% CI 1.18–2.01; p = 0.16, I 2 = 26%, Fig. 2C), and NPV (OR 1.17, 95% CI 1.01–1.37; p = 0.06, I 2 = 38%, Fig. 2D) in the diagnosis of SIRS and urosepsis after PCNL. The pooled result showed that there were no significant statistical differences for specificity between PMUC and SC in predicting postoperative SIRS and urosepsis (OR 1.04, 95% CI 0.80–1.36; p = 0.0001, I 2 = 65%, Fig. 2B).

Forest plots for
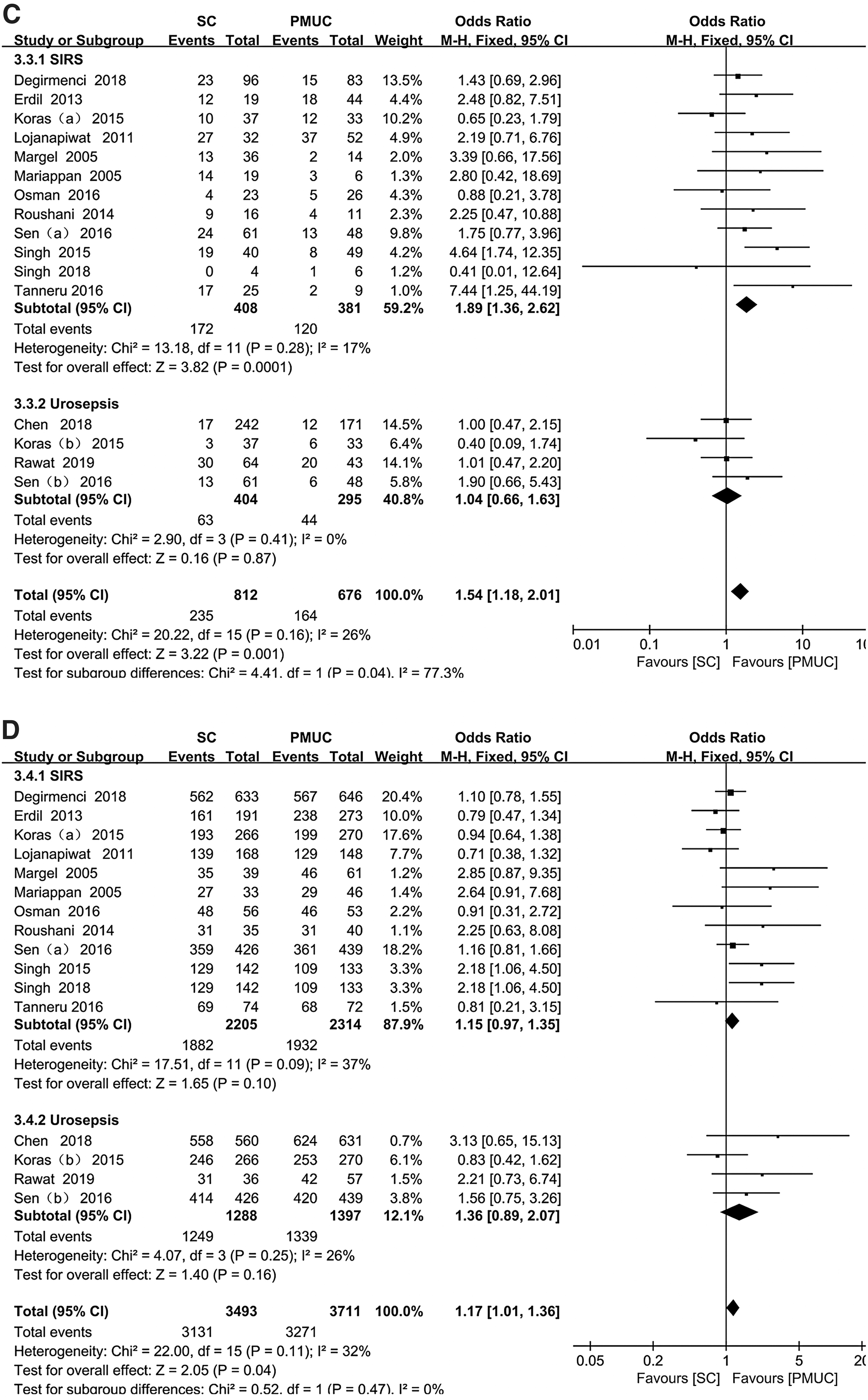
Subgroup analyses were also, respectively, conducted to identify whether PMUC and SC are risk factors for SIRS or urosepsis. Twelve included studies were used for SIRS 3,8 –15,24,25,27 and the remaining four were for urosepsis. 12,13,23,26 The pooled result showed that SC was associated with a higher sensitivity (OR 2.35, 95% CI 1.16–4.76; p < 0.00001, I 2 = 78%, Fig. 3A) and PPV (OR 1.89, 95% CI 1.36–2.62; p = 0.28, I 2 = 17%, Fig. 3C) than PMUC in assessing post-PCNL SIRS. No significant statistical differences were discovered for specificity (OR 0.88, 95% CI 0.62–1.24; p = 0.003, I 2 = 61%, Fig. 3B) and NPV (OR 1.15, 95% CI 0.97–1.35; p = 0.09, I 2 = 37%, Fig. 3D) in the diagnosis of post-PCNL SIRS. However, subgroup analysis indicated that PMUC provided a higher specificity than SC for post-PCNL urosepsis (OR 1.48, 95% CI 1.23–1.79; p = 0.48, I 2 = 0%, Fig. 3B). No significant statistical differences were identified for sensitivity (OR 2.47, 95% CI 0.86–7.11; p = 0.07, I 2 = 57%, Fig. 3A), PPV (OR 1.04, 95% CI 0.66–1.63; p = 0.41, I 2 = 0%, Fig. 3C), and NPV (OR 1.36, 95% CI 0.89–2.07; p = 0.25, I 2 = 26%, Fig. 3D) between PMUC and SC in the diagnosis of urosepsis.

Forest plots for
PMUC vs RPUC
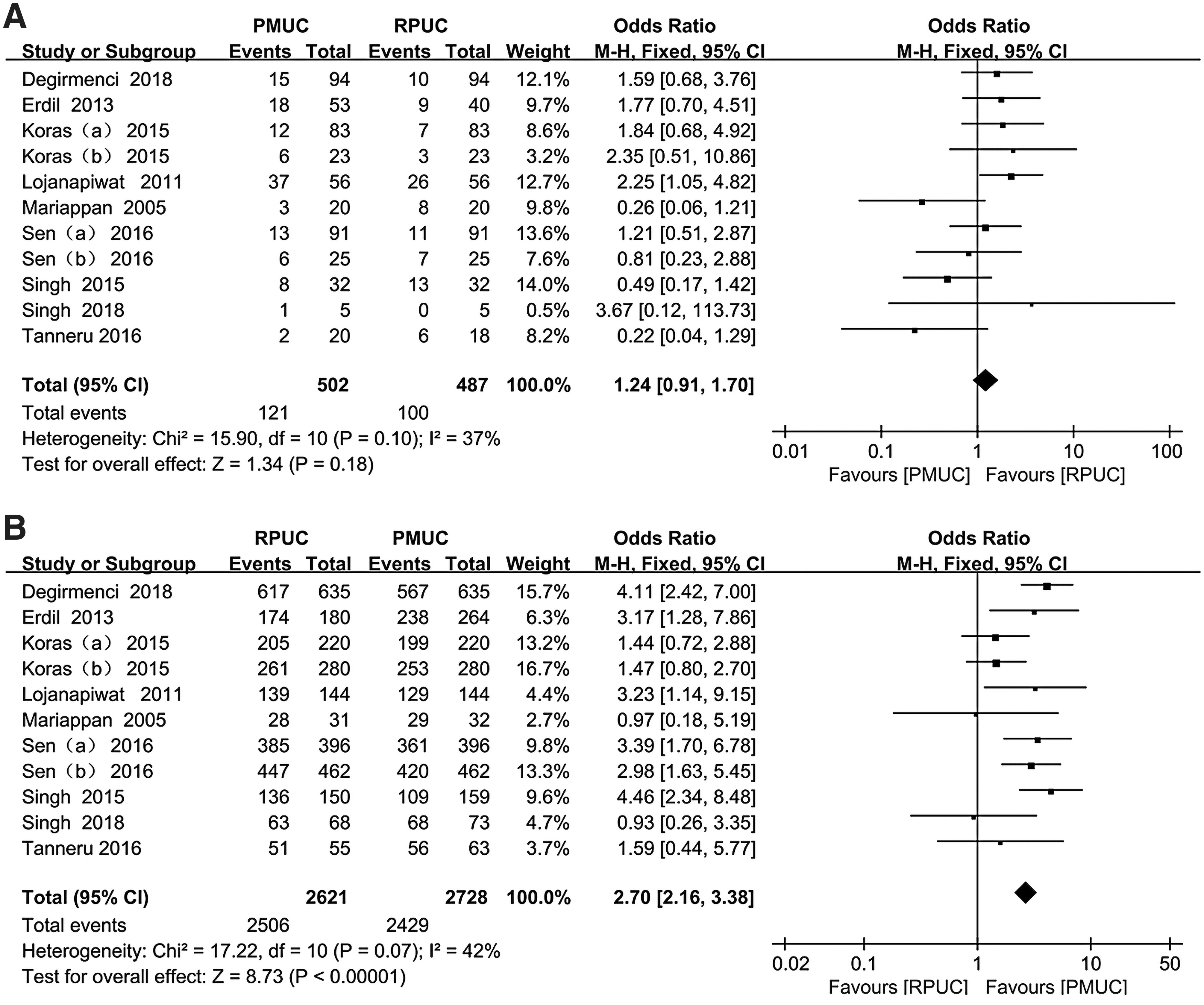
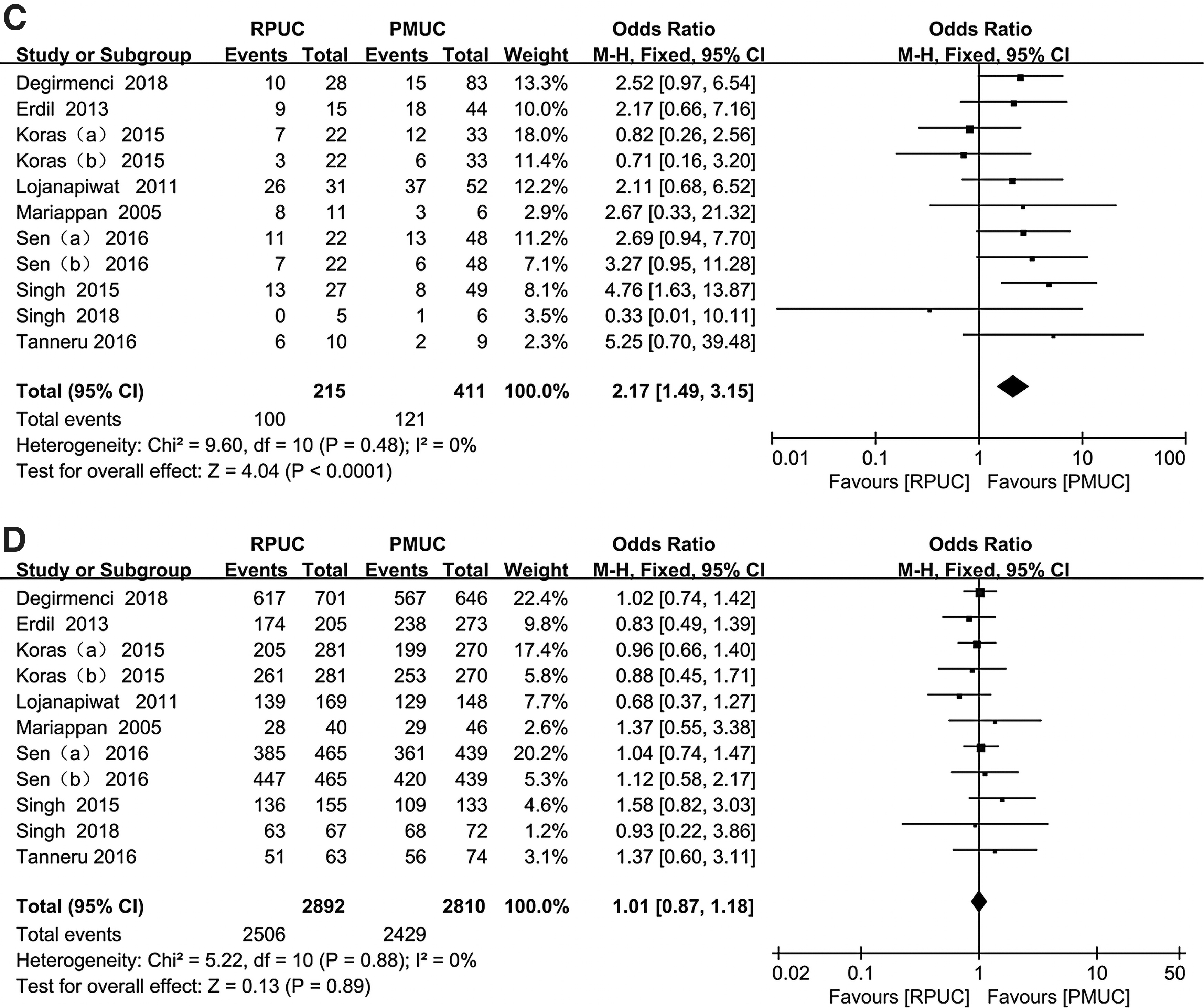
Nine studies compared the differences between PMUC and RPUC in assessing the risk factors for postoperative SIRS and urosepsis, and two studies were analyzed twice, each of them, for SIRS or urosepsis. The pooled results showed that RPUC provided a significantly higher specificity (OR 2.70, 95% CI 2.16–3.38; p = 0.07, I 2 = 42%, Fig. 4B) and PPV (OR 2.17, 95% CI 1.49–3.15; p = 0.48, I 2 = 0%, Fig. 4C) than PMUC in the diagnosis of SIRS and urosepsis after PCNL. There were no significant statistical differences for sensitivity (OR 1.24, 95% CI 0.91–1.70; p = 0.10, I 2 = 37%, Fig. 4A) and NPV (OR 1.01, 95% CI 0.87–1.18; p = 0.88, I 2 = 0%, Fig. 4D) between PMUC and RPUC in predicting post-PCNL SIRS and urosepsis. Due to the lack of concerned studies, we failed to conduct a subgroup analysis of the difference between PMUC and RPUC in identifying postoperative urosepsis.
Forest plots for
Publication bias and sensitivity analysis
Funnel plots were used to assess potential publication bias (Supplementary Figs. S2 and S3). The result was vertical and symmetrical, indicating no evident publication bias. A sensitivity analysis was carried out by using a leave-one-out approach to assess the stability of our meta-analysis results. When the study of Chen and colleagues 23 was removed, there was no significant effect in predicting postoperative SIRS and urosepsis, as shown in Supplementary Figure S4. However, the OR and 95% CI results were consistent with the previous result, which confirmed that the results of this meta-analysis were reliable.
Discussion
Due attention should be paid to the life-threatening urosepsis. The mechanism responsible for post-PCNL urosepsis most likely involves two major components. The first is a lot of stone-colonizing bacteria and a certain concentration of bacterial endotoxins that are released during the fragmentation of renal stones and washing out the fragments with the irrigating solution. 30,31 The second is the significant absorption of irrigating fluid containing bacteria and endotoxins via multiple small venous and lymphatic systems due to the positive irrigation pressure through the nephroscope during PCNL. 9 The incidence of postoperative infectious complications can be reduced by diminishing the irrigation pressure of renal pelvis, shortening the operation time, avoiding multiple access tract operation, and using sensitive antibiotics obtained from bacterial culture results. The most noteworthy is that the bacterial culture is the only way to identify the microbiology of stone diseases and thus direct perioperative antimicrobial therapy. However, SIRS and urosepsis after PCNL may still occur despite the presence of a sterile PMUC and a preoperative proper regimen of antibiotic prophylaxis.
Several studies reported that a sterile PMUC is not always consistent with upper UTI. Mariappan and colleagues conducted a prospective clinical study in 54 patients undergoing PCNL, and a negative PMUC was reported in 46 patients and 17 of them were diagnosed with SIRS, but only 6 of the 33 patients with negative SC and 12 of the 41 patients with negative RPUC developed SIRS. 10 Dogan et al. conducted a retrospective study in 338 patients undergoing PCNL and discovered that 54 patients (66%) in the study had SIRS despite negative preoperative PMUC. 32 Eswara et al. found that 3% (11/328) developed postoperative urosepsis, 8 of whom had positive SCs, but none had a positive PMUC. 33 These data showed that a significant number of potential SIRS patients may be missed due to the poor predictive value of PMUC, which may be explained by the potential stone obstruction of the urinary tract. Thus, in this situation, pelvic urine and stones may still be infected despite the sterile PMUC. As the first meta-analysis to compare PMUC with RPUC or SC in predicting postoperative SIRS and urosepsis for patients who underwent PCNL, it clearly demonstrated that SC provided a significantly better sensitivity, PPV, and NPV in the diagnosis of SIRS and urosepsis than PMUC, and RPUC shows a higher specificity and PPV than PMUC. All in all, SC and RPUC are better predictors of potential postoperative SIRS and urosepsis than PMUC.
In most hospitals it is common means to culture midstream bladder urine preoperatively to identify potential bacteria in the upper tract for patients with upper urinary stones. However, PMUC does not always associate with RPUC or SC and the uropathogens detected by PMUC do not necessarily correlate with those of SC and RPUC. Margel and coworkers reported on 75 patients who underwent PCNL for upper urinary tract stones. Positive SC was associated with negative PMUC in 19 of 75 patients (25%). Also, the sensitivity of PMUC for the detection of SC was only 30%. They also discovered among 17 patients with post-PCNL SIRS, the antibiotic treatment was altered in 13 patients according to the results of the SC, of which 8 patients had a positive SC and negative PMUC, and 5 patients had a positive SC and positive PMUC, but with different pathogens. 24 These data indicated that it was not accurate to predict the causative organisms detected by SC and RPUC from the results of PMUC. SC and RPUC seem to be the best guide for antibiotic therapy due to their high predictive value of pathogens. Similarly, Korets and coworkers reported that, among their 204 patients of PCNL, 5 of 14 (35.7%) had discordant culture results between PMUC and RPUC, and 5 of 17 (29.4%) had discordant culture results between PMUC and SC. 5 Some studies showed that the most common bacteria of PMUC, RPUC, and SC are not always identical, 10,24 and other studies demonstrated that the most common uropathogens in urine and stone are the same, but the bacterial spectrum was different. 23,34 Either way, the bacterial spectra in both urine and stone should be routinely identified for the adequate treatment of postoperative infectious complications.
A recent study demonstrated that PMUC still played an important role in predicting SIRS following PCNL, but it failed to prevent the happening of SIRS even with antibiotic prophylaxis, based on PMUC results. 35 PMUC must combine with other indicators because of its low predictive value, and several risk factors for infectious complications after PCNL have been identified. Preoperative urine tests with both positive white blood cells and positive nitrite were early and rapid predictors of postoperative urosepsis. 23 Despite baseline negative PMUC, urine test with positive white blood cells and leukocyte esterase and nitrite was considered an efficient prediction of urosepsis and can early predict the bacterial status of RPUC and SC. 36 Procalcitonin seems to be an early marker to diagnosis urosepsis following PCNL and a valuable tool to monitor antibiotic therapy in urosepsis. 37 Low CT value of stone and CT localization puncture can shorten the operation time and reduce postoperative infectious complications. Renal pelvis urine Gram staining (RPUGS) had a high sensitivity, specificity, PPV, and NPV in predicting SC positivity, and was as effective as SC in predicting fever for patients who underwent PCNL. As a simple, inexpensive and easy-to-use tool with rapid results, RPUGS was recommended for broad-spectrum antibiotic therapy before the SC and RPUC results are obtained in patients with postoperative fever. 38 Accurate preoperative prediction and isolation of uropathogens remain an important and challenging task. Timely acquisition of causative bacterial spectra and early and rapid prediction of postoperative infection can effectively reduce the incidence of SIRS and urosepsis.
Besides, two of the included studies summarized the data that compared the differences between PMUC and SC in predicting postoperative SIRS and urosepsis. 12,13 Similar with our results, Sen and associates showed that SC was associated with a higher sensitivity than PMUC and that RPUC provided a higher specificity than PMUC in the diagnosis of SIRS and urosepsis after PCNL, while Koras and associates indicated that PMUC provided a higher sensitivity than SC in assessing post-PCNL SIRS and urosepsis. Moreover, both the studies showed that PMUC, RPUC, and SC provided a higher sensitivity and a lower specificity in predicting urosepsis than SIRS. Further studies with a more rigorous study design and a larger sample size are required to support the findings of our meta-analysis. The incidence of SIRS after PCNL ranged from 10% to 35% and for urosepsis from 0.97% to 4.9%, 23,27 and the difference may be associated with the following reasons: demographic characteristics of patients, 27,39 stone types and burden, 5,40 UTI, 23,36 duration of antibiotic prophylaxis, intrapelvic pressure during PCNL, operating time, 3 stone-free rate, and so on. Female patients have a higher tendency for UTI, which may be the main reason for the higher incidence of postoperative infection. Large stones might require multiple tracts to be removed, and struvite stones are more likely harbor stone-colonizing bacteria that contain endotoxins. 40 Operating time is affected by stone size and is closely associated with a longer duration of high irrigation pressure and significant absorption of irrigating fluid containing bacteria and endotoxins. Lower stone-free rate is common in patients with large stones, who tend to be at greater risk of infection. Yu and colleagues performed a meta-analysis and discovered that preoperative prophylactic antibiotics can lower the risk of postoperative infection. 41 The EAU and AUA guidelines recommend a single-dose antibiotic for patients prior PCNL with UC−. Zeng et al. reported that antibiotic prophylaxis according to sensitivity profile should be administered for at least 7 days in patients with UC+. 42 In 13 of the included studies, patients with UC− received at least a single dose of antibiotic prophylaxis preoperatively or intraoperatively. Also, most of patients with UC+ were treated with appropriate antibiotics based on the sensitivity profile for a different duration ranging from 2 to 14 days.
There are several limitations to the present meta-analysis. First, no randomized-controlled trial was available for inclusion and three studies were retrospective analysis. Second, heterogeneity of >50% was found on several parameters in meta-analysis and some relevant subgroup analyses could not be carried out due to the lack of concerned studies. Third, the definitions of urosepsis were not completely consistent in the included studies. Sepsis 3 conference definition indicated that the updated clinical criteria of q-SOFA and SOFA should replace SIRS, but a systematic review and meta-analysis showed that SIRS was significantly superior to the q-SOFA for sepsis diagnosis. 43 It is premature to have a conclusion, and further well-designed studies are still required. Fourth, other confounding factors such as diabetes mellitus, perioperative bleeding, and duration of prophylactic antibiotics for UTI could also influence the incidence of postoperative infection. Fifth, sensitivity analysis suggested that some of the results may be unstable. Finally, the included studies covered a long period of time, from 2005 to 2018, during which the efficacy of antibiotics and PCNL technology developed rapidly.
Conclusion
Intraoperative SC and RPUC are more reliable than PMUC in predicting postoperative SIRS and urosepsis, identifying causative organisms, and directing antibiotic therapy for patients who underwent PCNL. As a simple, inexpensive and valuable practice, PMUC, SC, and RPUC should be routinely collected for the diagnosis and management of SIRS and urosepsis after PCNL.
Footnotes
Authors' Contributions
M.L.: Project development, data analysis, and article writing. J.C.: Data collection and analysis. M.G.: Data collection. H.Z.: Data collection. Y.C.: Data analysis. Z.Z.: Project development. H.C.: Project development.
Compliance with Ethical Standards
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was mainly funded by the National Natural Science Foundation of China (NO. 81770705).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.