
Abstract
Introduction and Objective:
Robot-assisted radical nephrectomy (RRN) is increasingly utilized as an alternative to laparoscopic radical nephrectomy (LRN), but there are concerns over costs and objective benefit. In the setting of very large renal masses (>10 cm), comparison between techniques is limited and it is unclear whether a robotic approach confers any perioperative benefit over LRN or open radical nephrectomy (ORN). In this study, perioperative outcomes of RRN, LRN, and ORN for very large renal masses are compared.
Methods:
Using the National Cancer Database, patients were identified who underwent radical nephrectomy for kidney tumors >10 cm diagnosed from 2010 to 2015. Patients were analyzed according to surgical approach. Perioperative outcomes, including conversion to open, length of stay, readmission rates, positive surgical margins, and 30- and 90-day mortality were compared among cohorts.
Results:
A total of 9288 patients met inclusion criteria (RRN = 842, LRN = 2326, ORN = 6120). Compared with ORN, recipients of RRN or LRN had similar rates of 30-day readmission and 30- and 90-day mortality. Length of hospital stay was significantly shorter in RRN (−1.73 days ±0.19; p < 0.0001) and LRN (−1.40 days ±0.12; p < 0.0001) compared with ORN. LRN had a higher rate of conversion to open compared with RRN (odds ratio 1.48; 95% confidence interval 1.10–1.98; p = 0.0087). Conversion to open from RRN or LRN added 1.3 additional days of inpatient stay. Over the study period, RRN use increased from 4.1% to 14.8%, LRN from 20.9% to 25.6%, whereas ORN use decreased from 75% to 59.6%.
Conclusions:
Minimally invasive approaches are increasingly utilized in very large renal masses. RRN has lower rates of conversion to open but produces comparable perioperative outcomes to LRN. Minimally invasive approaches have a shorter length of inpatient stay but otherwise report similar surgical margin status, readmission rates, and mortality rates compared with ORN.
Introduction
Since being introduced nearly 30
There are few studies investigating trends and outcomes with minimally invasive techniques for very large renal masses >10 cm. ORN has remained the preferred approach for these very large masses given the surgical complexity and association with locally advanced or venous extension. 7 However, given increasing utilization and comfort with laparoscopic and robotic surgery for many urologic procedures, including radical nephrectomy, we sought to determine the role of minimally invasive approaches in these large renal masses. In this study, we use the National Cancer Data Base (NCDB) to compare the perioperative outcomes of ORN, LRN, and RRN for large renal masses greater than 10 cm.
Methods
Data source
The NCDB is a facility-based, comprehensive cancer registry, established in 1989 that captures ∼70% of all new cancer diagnoses across the United States. The NCDB draws data from over 1500 commission-accredited cancer programs in the United States and Puerto Rico. The database is a joint project of the American Cancer Society and the Commission on Cancer (CoC) of the American College of Surgeons. No Internal Review Board approval was required for this study.
Study population
We identified 20,790 patients ages 18 to 80 diagnosed with renal cancer from 2010 to 2015 with renal masses >10 cm. We sequentially excluded 8765 patients with stage cT3b-4 disease, 2152 patients who did not undergo radical nephrectomy, and 585 patients without defined surgical approach. The final study population included 9288 patients (Fig. 1).
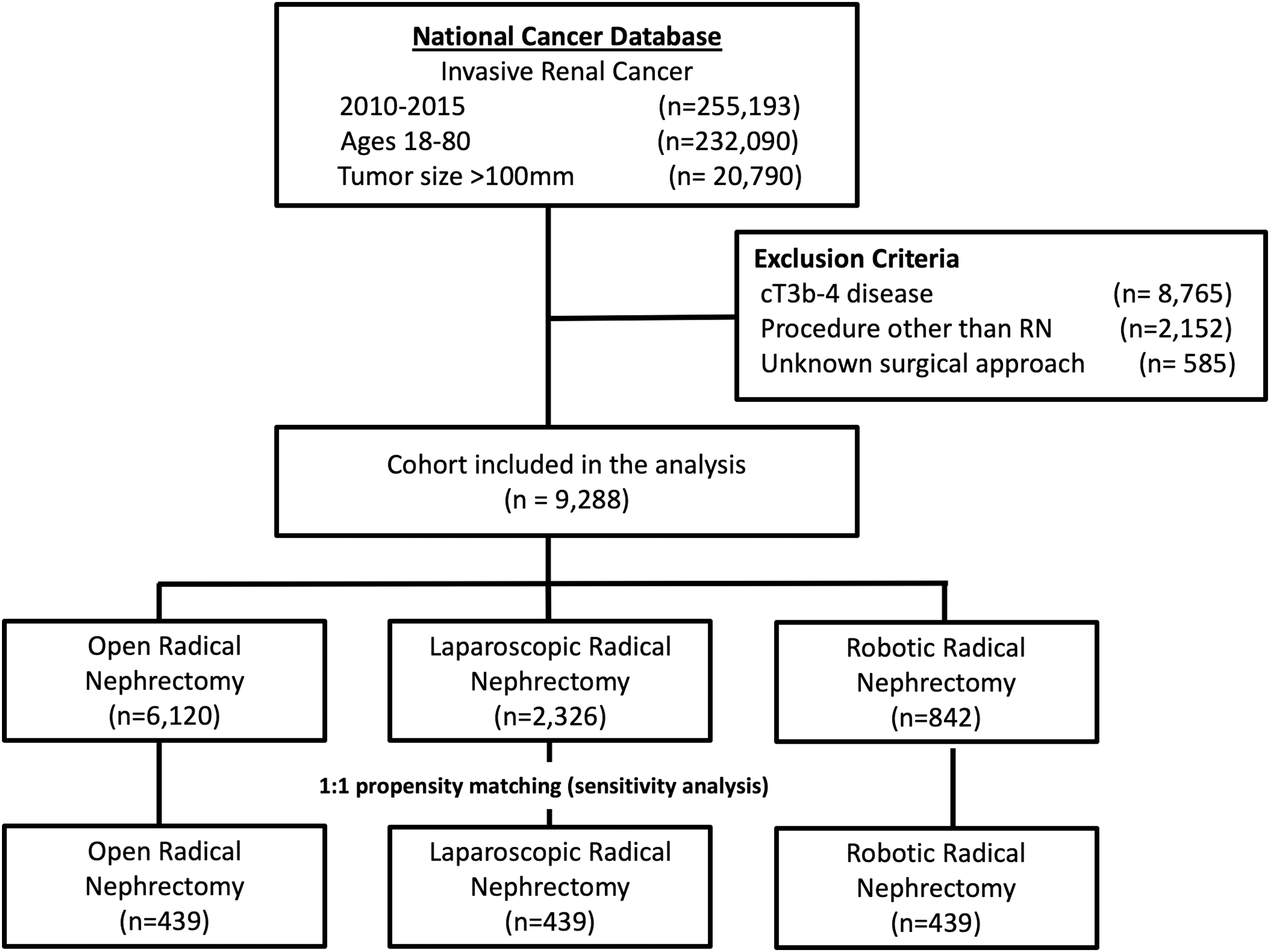
Consort flow diagram.
Patient characteristics
Demographic and clinical characteristics such as age at diagnosis, sex, race/ethnicity, insurance status, facility type, and comorbidity were extracted from NCDB data. Tumor characteristics, including clinical and pathologic T stage, tumor grade, histology, and tumor size were recorded. Patient comorbidity was categorized as 0, 1, ≥2 according to NCDB Charlson/Deyo comorbidity score. Pathologic stage was determined using the American Joint Committee on Cancer Staging Manual edition in use at the time of diagnosis. Patient's surgery approach was categorized as RRN, LRN, and ORN.
Statistical analyses
Patient's demographic and clinical characteristics by surgical approach category were compared using the Chi-squared test. Adjusted odds ratios (OR), their 95% confidence intervals (CI), and p-values were calculated from multivariable logistic regression models to compare perioperative outcomes, such as, risk of conversion to open, surgical margin status, 30-day readmission, and 30- and 90-day mortality. A multivariate linear regression model was fitted for continuous outcome of length of inpatient stay in days. Multivariate analyses included all patient demographics, clinical, and tumor characteristics. Subset analyses within the RRN and LRN cohort were conducted in a similar manner to identify significant predictors of receipt of each surgical modality. As a sensitivity analysis, patients in each cohort were propensity score matched on a 1:1 basis, based on the previously described demographic-, clinical-, and tumor-level characteristics. Outcomes were compared using the matched sample. All statistical analyses were performed on SAS 9.4 (SAS Institute Cary, NC). Statistical significance was set at p < 0.05, using two-tailed tests.
Results
Patient characteristics
A total of 9288 patients met inclusion criteria (RRN = 842, LRN = 2326, ORN = 6120). Of the included masses, 52.0% measured 10.1 to 12.4 cm, 26.3% measured 12.5—to 14.9 cm, and 21.7% measured >15.0 cm. The majority of masses were clear cell renal cell carcinoma (53.3%) (Table 1).
Distribution of Patient and Tumor Characteristics by Surgical Approach
p-Value from chi-squared test to test the difference of characteristics among three approach categories.
Trends in surgical approach
Over the 6-year study period, RRN use increased from 4.1% to 14.8%, LRN from 20.9% to 25.6%, whereas ORN use decreased from 75% to 59.6%. The percentage of nephrectomies performed open was higher at community cancer programs than at academic programs, comprehensive community cancer programs, or integrated network cancer programs (71.2% vs 67.6%, 63.8%, 62.3%, respectively). ORN use increased from 59.9% to 78% with increasing tumor size (10–12.5, 12.5–15, ≥15 cm), whereas RRN decreased from 10.9% to 6.2% and LRN decreased from 29.2% to 15.7% (Fig. 2).
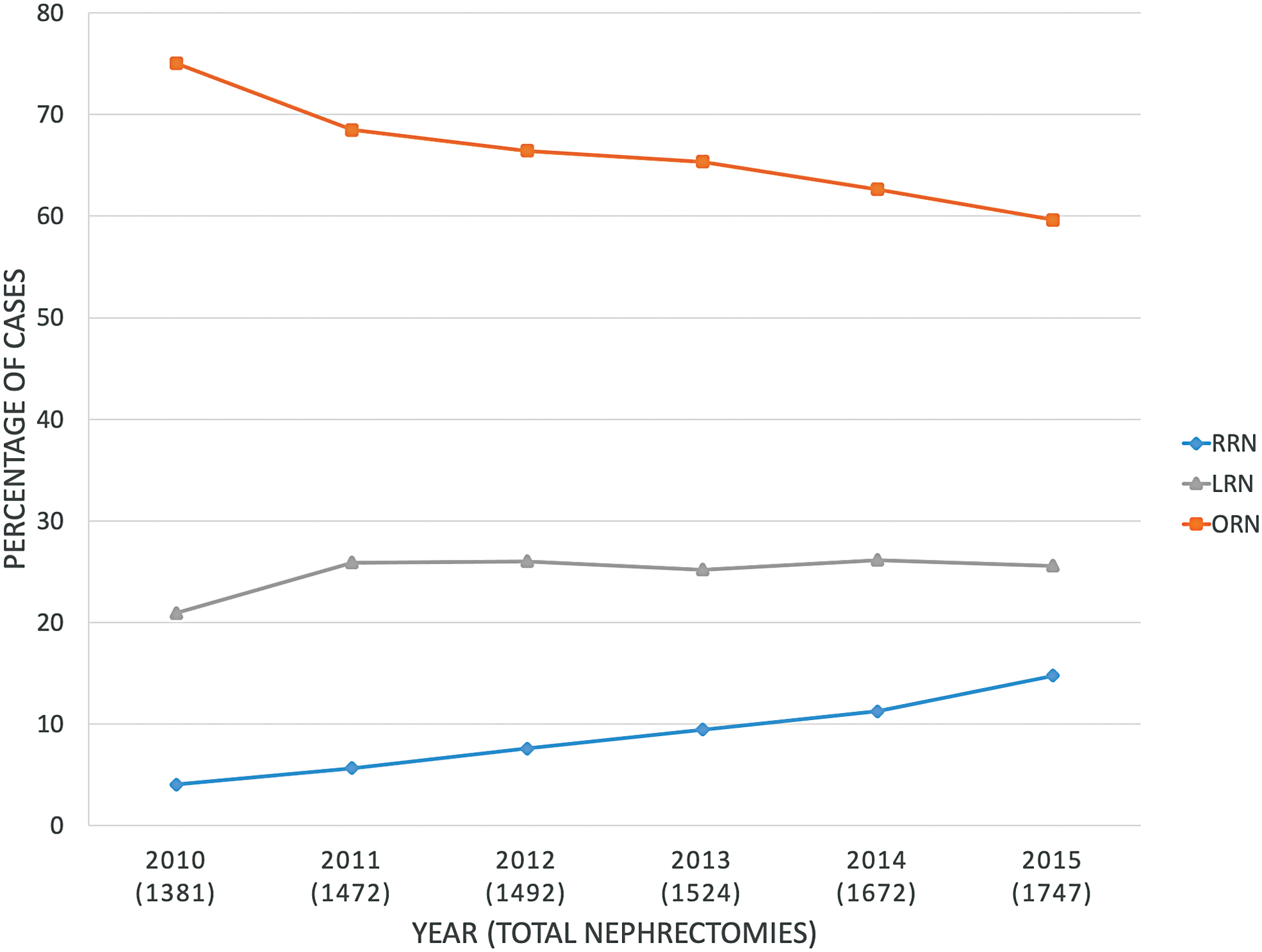
Trends in surgical approach 2010–2015. LRN = laparoscopic radical nephrectomy; ORN = open radical nephrectomy; RRN = robot-assisted radical nephrectomy. Color images are available online.
In the subset of RRN and LRN, compared with 2010, there was an increasing likelihood to utilize RRN with each year with significance being reached from 2012 to 2015 (OR 1.57 vs 2.04 vs 2.30 vs 3.10 [2012–2015]; p < 0.013). Compared with community care programs, patients at integrated network cancer programs were significantly more likely to undergo RRN (OR 1.68; 95% CI 1.08–2.63). Compared with patients with comorbidity score of 0, patients with comorbidity score ≥2 were significantly more likely to receive RRN (OR 1.35; 95% CI 1.01–1.80). There was no difference with respect to age at diagnosis, race/ethnicity, or insurance type (Results not shown).
Conversion to open
LRN had a higher risk of conversion compared with RRN (11.4% vs 7.7%; p = 0.0025) (Table 2). Compared with non-Hispanic whites, non-Hispanic blacks were more likely to covert to open (OR 1.66; 95% CI 1.19–2.32). There was no significant difference between cohorts with respect to insurance type, facility type, or comorbidity score. When compared with tumor sizes 101 to 124 mm, patients with tumor size >150 mm were more likely to convert to open (OR 1.65; 95% CI 1.21–2.26). There was no significant difference with respect to tumor grade or histology (Results not shown). Overall, LRN was more likely to convert to open when compared with RRN (OR 1.48; 95% CI 1.10–1.98) on multivariate analysis, which was confirmed with the sensitivity analysis (Table 3).
Distribution of Outcomes by Surgical Approach
p-Value from chi-squared test or analysis of variance test to test the difference of distribution of outcome among three approach categories.
A small percentage of missing due to unknown information.
SD = standard deviation.
Comparison of Perioperative Outcomes
p-Value from logistic regression or linear regression models for the odds ratio or parameter estimate. Analysis for multivariate cohort adjusted for all demographic and clinical characteristics in Table 1.
Among subset of robot-assisted or laparoscopic approaches.
Perioperative outcomes
On multivariate analysis, there was a significantly lower positive margin rate in RRN and LRN when compared with ORN (RRN: OR 0.75; 95% CI 0.56–0.99, LRN: OR 0.64; 95% CI 0.52–0.78). However, the difference in positive surgical margin rates between cohorts did not reach statistical significance on sensitivity analysis with propensity matching. When compared with ORN, RRN and LRN had no significant difference in 30-day mortality (RRN: OR 0.86; 95% CI 0.43–1.75, LRN: OR 0.95; 95% CI 0.61–1.47) or 90-day mortality (RRN: OR 0.89; 95% CI 0.58–1.37, LRN: OR 0.81; 95% CI 0.61–1.08). There was also no difference in 30-day readmission rates when RRN and LRN were compared with ORN (RRN: OR 0.91; 95% CI 0.60–1.37, LRN: OR 0.81; 95% CI 0.61–1.07). On multivariate analysis, length of hospital stay was significantly shorter in RRN (−1.73 days ±0.19; p < 0.0001) and LRN (−1.40 days ±0.12; p < 0.0001) compared with ORN. Conversion to open from RRN or LRN added 1.3 additional days of inpatient stay (Table 3).
Sensitivity analysis
Following 1:1 propensity matching, 439 patients remained in each cohort. Statistical analysis with propensity matching supported the multivariate linear regression results of the study cohort for associations in conversion to open, readmission, length of stay, and mortality. Positive surgical margins did not reach significance between open and minimally invasive approaches (Table 3).
Discussion
Minimally invasive approaches for radical nephrectomy continue to grow in popularity. 5,8,9 The cohort examined in this study not only corroborates these data, but also demonstrates a similar trend in radical nephrectomies for very large renal masses.
Few studies have specifically focused on the application of minimally invasive techniques for removal of large masses, and those exclusively investigating masses >10 cm have been limited by small cohorts. 10 A recent multi-institutional retrospective analysis conducted by the ROSULA collaborative group compared the perioperative outcomes between RRN and LRN for ≥cT2 renal masses. This was the first study to compare LRN to RRN for large masses on a large scale, however, the masses observed ranged in size from 7.4 to 10.2 cm. 11 Despite the increasing utilization of LRN and RRN for renal masses measuring >10 cm, perioperative outcomes have yet to be reported on the scale that they are within this study.
Between 2010 and 2015, use of LRN gradually decreased, RRN increased, and ORN remained relatively stable for renal masses of all sizes. 5 In contrast, for masses >10 cm over the same period, LRN was still increasingly utilized. Over the study period, the proportion of large mass radical nephrectomies completed with LRN increased by 4.7%. The proportion of radical nephrectomies using RRN more than tripled during the same period, increasing by 10.7%. This may demonstrate a growing preference for RRN over LRN despite higher cost. 5
A well-documented barrier to wide implementation of minimally invasive radical nephrectomy for larger tumors is its perceived technical difficulty, particularly by surgeons who have not received extensive training in minimally invasive techniques. 12,13 However, robotic surgery is known to have a less significant learning curve, provide better visualization, offer superior mechanical stabilization and allow for improved ergonomics when compared with laparoscopic techniques. 14,15
Features unique to the robotic platform, including the use of the fourth arm and the articulation of endowrist instruments may also help with more challenging nephrectomies. These advantages may be a primary factor leading surgeons to increasingly prefer RRN over LRN when choosing a minimally invasive technique, particularly for large masses, which are often more technically complex to remove. 16 Additional possible contributing factors include growing emphasis on robotic surgery in urology residency/fellowship curriculum and patient demand. 17 –20
Within this cohort, it is evident that ORN remains the preferred method for very large, operatively complicated masses. ORN was used with increased frequency as renal mass size increased, with 78% of masses >15 cm being removed with an open approach. While the advantages of robotic surgery may ultimately have some benefit for large, surgically complex masses, RRN for very large renal masses has only recently become more common. 21 Possible explanations for this trend include continued advancement in robotic technology and the comfort level of robotic surgeons to perform more complex procedures. 22 This may explain why academic and integrated network cancer programs were more likely to use RRN than community cancer programs.
On meta-analysis, LRN has demonstrated superiority to ORN in both overall mortality and postoperative complications, but only for masses <7 cm. 23 Similarly, in more limited studies, RRN has been shown to have equivalent perioperative outcomes and postoperative complication rates to LRN. 6,24 In our study of large masses, LRN and RRN were statistically equivalent to ORN for all observed perioperative outcomes with the exception of length of hospital stay, which was significantly shorter for both LRN and RRN. Length of stay for LRN and RRN was comparable. These results suggest that both LRN and RRN can be successfully employed for selected renal masses >10 cm, while allotting the patient shorter recovery times.
The cost of procedures is often discussed as a shortcoming of RRN when compared with LRN, given otherwise similar perioperative results. However, conversion to ORN from a minimally invasive radical nephrectomy has rarely been analyzed on a significant scale. 5,25 Helmers and colleagues found that in a single institution cohort of 319 patients, with masses of a median diameter of 5.5 cm, in years 2010 to 2014, conversion to another approach was significantly higher for RRN than LRN (11.1% vs 1.0%, p < 0.001), although the authors noted that the majority of RRN conversions occurred early in the surgeon's robotic surgery experience. 6
A recent meta-analysis of perioperative outcomes for radical nephrectomy from Li and colleagues (mass median diameter 5.6–8.7 cm) demonstrated similar rates of conversion when comparing RRN and LRN (3.88% vs 1.60%, p = 0.16). 26 In this study, a contradictory observation was made that conversion to open was more likely for LRN than RRN (11.4% vs 7.7%; p = 0.0025). The cohort of surgeons reported in this study may have been adequately robust and diverse to account for a small number of RRN conversions attributable to novice robotic surgeons overcoming the learning curve of robotic surgery. It is also possible that surgeons choosing LRN may be more prone to elect to convert to ORN than those with a robotic setup. However, with advancing robotic technology, RRN may offer particular benefit for large masses, leading to the trend observed in this study and explaining the difference in results from studies of masses of smaller median diameter. In other surgical fields, laparoscopic surgery has also been shown to have a greater risk of conversion than robotic surgery and conversion has been shown to substantially increase the cost of surgery. 27,28 Increased cost associated with conversion is partially due to the associated increased length of hospital stay. 29 On average, conversion to open resulted in an additional 1.3-day hospital stay, which was similar to the average length of stay for ORN. There is evidence to suggest that the cost discrepancy between RRN and LRN may not be as significant as previously thought. 6,26 Future cost analysis could further justify these findings by determining if the discrepancy in conversion rate between LRN and RRN in large renal masses specifically is considerable enough to offset the higher base cost of RRN.
Limitations
Retrospective studies that utilize large national databases offer robust sets of real-world data but are inherently limited in several ways. 30 While randomized study designs would be more ideal to limit selection bias, it is technically difficult and expensive to conduct studies for relatively rare, high-stakes treatments. In this study, several specific shortcomings should be appreciated. First, no cost-based analysis was conducted as a part of this study, which has been one of the key points of differentiation when comparing LRN to RRN in recent literature. 5,6 Additionally, the NCDB did not allow for the analysis of certain parameters that have been reported by other studies comparing radical nephrectomy approaches, including nephrometry scores, reason for conversion, blood loss volumes, and operation times. 6,11 The NCDB also lacks granular details about tumor complexity. Ideally, information on specific surgical technique (e.g., hand-assisted laparoscopy), tumor characteristics beyond basic staging, and long-term oncologic outcomes would allow surgical approaches to be compared with a more complete clinical picture. Due to the inherent limitations of this study, all statistically derived conclusions require further study for confirmation. Despite these clear limitations, the study offers valuable insight into the perioperative outcomes of a rarely examined subset of renal masses.
Conclusion
Minimally invasive approaches are increasingly utilized for very large renal masses. In selected patients, LRN and RRN can be performed as safely as ORN for renal masses >10 cm. After adjusting for covariates, RRN has lower rates of conversion to open but produces comparable perioperative outcomes to LRN. LRN and RRN both resulted in significantly shorter length of inpatient hospital stay but are otherwise equivalent to ORN for all other perioperative outcomes. RRN may offer technical advantages that allow it to be more easily implemented for very large, technically complex, renal masses than LRN, while still offering the benefits of minimally invasive surgery.
Footnotes
Authors' Contributions
F.V.C., J.C., A.Zr., H.A.-C., and G.E.G collected initial data from NCDB. L.W.G., F.V.C., J.C., E.M.U., J.P.S., K.K.B., and G.E.G., collaborated on study design. J.C., A.Z., and H.A.-C. completed statistical analysis. L.W.G., F.V.C., J.C., A.Z., H.A.-C., E.M.U., J.P.S., K.K.B, and G.E.G. interpreted final data. L.W.G., F.V.C., J.C., and G.E.G. created tables and figures. L.W.G., F.V.C., J.C., and G.E.G. drafted article. L.W.G., J.C., and G.E.G edited/revised article. All authors approved the final article.
Acknowledgments
The data used in the study are derived from a deidentified NCDB file. The American College of Surgeons and the Commission on Cancer have not verified and are not responsible for the analytic or statistical methodology employed, or the conclusions drawn from these data by the investigator.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.