
Abstract
Objective:
To evaluate the association between preoperative statin use with changes in estimated glomerular filtration rate (eGFR) after robot-assisted partial nephrectomy (RAPN).
Methods:
Three hundred eighty-nine consecutive patients undergoing RAPN were evaluated. Associations of preoperative statin use with change in eGFR from pre-RAPN to postoperative day 1 (POD1), 1, 6, and 12 months after RAPN were evaluated using longitudinal mixed-effects regression models with random patient-specific intercepts and slopes while accounting for imbalance of preoperative patient and tumor characteristics between groups with stabilized inverse propensity score weighting. Postoperative eGFR change from baseline was measured as total change, maintaining eGFR within 10% of baseline, and as going from eGFR >60 mL/min/1.73 m2 to <60 mL/min/1.73 m2.
Results:
One hundred sixty-seven (43.0%) of 389 patients were on statin therapy preoperatively. Statin patients were older (66 vs 58 years) and had higher rates of comorbidities, including diabetes mellitus (31.7% vs 14.9%) and hypertension (82.6% vs 45%). Statin patients tended to have lower preoperative eGFR (mean ± standard deviation, 71.1 ± 17.6 vs 77.4 ± 19.4 mL/min/1.73 m2). There was no evidence of an association of preoperative statin use with changes in eGFR at any time point after RAPN (p = 0.66).
Conclusion:
Patients on preoperative statins undergoing RAPN had lower eGFR preoperatively compared with those not taking those medications. There was no evidence of an association between preoperative statin use and change in post-RAPN eGFR in the immediate postoperative period or at 1 year after surgery.
Introduction
Robot-assisted partial nephrectomy (RAPN) has become a common treatment for small renal masses. 1 Statins are lipid lowering agents that are commonly used and have been shown to have vasodilatory, anti-inflammatory, antioxidant, and antithrombotic effects, which could be beneficial for postoperative renal function after partial nephrectomy. 2
Multiple studies have attempted to study the effect of perioperative statin use on renal function in patients undergoing noncardiac surgery, resulting in conflicting evidence. 3 Studies performed in patients undergoing partial nephrectomy (PN) have failed to demonstrate an association with perioperative statin use and changes in renal function. 2,4 Because of this conflicting evidence we elected to analyze the association between the use of statins preoperatively and changes in estimated glomerular filtration rate (eGFR) post-RAPN. We hypothesized that preoperative statin use would be protective for postoperative eGFR after RAPN.
Materials and Methods
Robotic partial nephrectomy and perioperative statin management
Institutional Review Board approval was acquired to complete this analysis (IRB-12-004921). RAPN was performed by a single surgeon as previously described. 5 A 12-mm assistant port was placed in the supraumbilical midline in all patients and a 5-mm assistant port was placed in the midline below the xiphoid for liver retraction in right-sided tumors. The renal hilum was controlled using bulldog clamps when necessary for tumor resection. Gerota's fascia was incised and the perirenal fat was dissected to the renal capsule allowing adequate exposure of the renal tumor. Disruptions in the collecting system were closed with a running absorbable suture and renorraphy was completed using the sliding-clip technique. 6 All patients were instructed to take their statin up until the morning of surgery. The statin was held on the morning of surgery. The statin was started in all patients on the morning of postoperative day number one.
Study subjects and data collection
We included all patients who underwent RAPN at our institution from February 2008 through April 2019. Patients who were started on statins greater than a month before surgery were included in the statin group. Patients with caliceal diverticulum, conversion to nephrectomy, bilateral renal cell carcinoma, and patients with more than one renal mass were excluded. Preoperative data included age, gender, body mass index (BMI), history of hypertension, history of diabetes mellitus, history of smoking, treatment of comorbidities with angiotensin converting enzyme inhibitors and angiotensin receptor blockers (ARBs), American Society of Anesthesiologists [ASA] score, 7 Mayo Adhesive Probability [MAP] score, 5 Radius, Exophytic, Nearness to collecting system, Anterior/Posterior, Location near polar lines (RENAL) nephrometry score, 8 renal mass size, and preoperative hemoglobin. In addition, we collected creatinine preoperatively and postoperatively. eGFR was calculated with the MDRD 2006 equation as described by Levey et al. 9 Intraoperative data, including warm ischemia time (WIT) and estimated blood loss (EBL), were also collected.
Statistical analysis
Age and eGFR were summarized with the sample mean and standard deviation (SD). The median and interquartile range were used to summarize WIT, operative time, and EBL. Categorical variables were summarized with the number and percentage of patients. For the primary analysis, associations of preoperative statin use with change in eGFR from pre-RAPN to postoperative day 1 (POD1), 1, 6, and 12 months after RAPN were evaluated using a longitudinal mixed-effects regression model with random patient-specific intercepts and slopes. The models included data from all five time points (baseline, POD1, 1, 6, and 12 months). A fixed effect for statin use was included to model eGFR at baseline. The mean change in eGFR from baseline to each of the postoperative time points (our primary outcome) was modeled with fixed effects for statin use, WIT (continuous), operative time continuous, and EBL >300 mL. A likelihood ratio test (LRT) was used to evaluate the overall association of statin use with changes in eGFR after RAPN. Owing to considerable imbalance in baseline patient and tumor characteristics between groups, we used propensity score methods to improve balance between groups for purposes of evaluating the association of statin use on changes in eGFR after RAPN. The propensity score (Pi ) for each patient (i) was calculated as the expected probability of preoperative statin use from a multivariable logistic regression model using preoperative patient and tumor characteristics (Table 1). Stabilized inverse probability weights (wi ) were calculated as wi = P*/Pi for those with preoperative statin use and wi = (1 − P*)/(1 − Pi ) for those without preoperative statin use where P* is the proportion of patients with preoperative statin use in our cohort. Standardized mean differences (SMDs) were used to assess balance between groups where we considered SMDs >0.10 to indicate imbalance between groups. Among patients with an expected probability of statin use <5%, wi = 0. Weighted N was calculated as the sum of the weights separately for each group. As a secondary analysis, we used two-sample t-tests with and without propensity score weights to compare preoperative eGFR between statin users and nonusers. Two-sided p < 0.05 was considered statistically significant. SAS (version 9.4; SAS Institute, Inc., Cary, NC) was used for all statistical analyses.
Standardized Mean Differences Between Preoperative Statin Use and No Preoperative Statin Use Before and After Propensity Score Weighting
SMDs >0.10 were considered to indicate imbalance between groups.
BMI was not available for seven patients. The most frequent category was imputed for purposes of propensity score estimation.
MAP score was not available for six patients. The most frequent category was imputed for purposes of propensity score estimation.
Intraoperative variables were not included in the propensity score model; therefore, SMDs and weighted summaries were not estimated.
ACE = angiotensin converting enzyme; ARB = angiotensin receptor blockers; ASA = American Society of Anesthesiologists; BMI = body mass index; EBL = estimated blood loss; IQR = interquartile range; MAP = Mayo Adhesive Probability; RENAL = Radius, Exophytic, Nearness to collecting system, Anterior/Posterior, Location near polar lines; SD = standard deviation; SMD = standardized mean difference; WIT = warm ischemia time; wt = weighted.
Results
Among the 389 patients who had RAPN between February 2008 and April 2019, 167 (43.0%) were using a preoperative statin. In the statin group, 31 (18.6%) had a benign tumor, and 136 (81.4%) had a malignant tumor, 165 (98.8%) had follow-up eGFR available at POD1, 135 (80.8%) patients at 1 month postoperative, 110 (65.9%) patients at 6 months postoperative, and 81 (48.5%) patients at 12 months postoperative. Table 1 shows a comparison of patient and tumor characteristics between those who used statins and those who did not use statins before and after propensity score weighting. Preoperative statin use was associated with older age (median age: 66 vs 58 years, SMD = 0.85), male gender (68.9% vs 56.8%, SMD = 0.25), black race (13.2% vs 7.7%, SMD = 0.18), overweight (BMI 25.0–29.9 kg/m2: 41.1% vs 34.2%, SMD = 0.13), obesity (BMI 30.0–39.9 kg/m2: 42.9% vs 36.1%, SMD = 0.15), hypertension (82.6% vs 45.0%, SMD = 0.85), diabetes (31.7% vs 14.9%, SMD = 0.41), cardiovascular disease (37.7% vs 8.1%, SMD = 0.75), angiotensin converting enzyme inhibitor use (53.9% vs 26.6%, SMD = 0.59), ARB use (25.1% vs 12.6%, SMD = 0.32), higher chronic kidney disease (CKD) stage (CKD stage 3–5: 23.4% vs 14.%, SMD = 0.23), higher ASA score (ASA 3–4: 85.6% vs 51.4%, SMD = 0.79), high MAP score (MAP 4–5: 37.8% vs 21.0%, SMD = 0.37), larger renal mass size (size >4 cm: 22.8% vs 16.2%, SMD = 0.17), and RENAL scores of moderate complexity (56.9% vs 49.1%, SMD = 0.16). There was no indication of imbalance in smoking history between those who used statins and those who did not (SMD = 0.06). After propensity score weighting, all differences in patient and tumor characteristics between those who used statins and those who did not were considered negligible (SMD ≤0.10, Table 1). Although not included in propensity score estimation, unweighted summaries of intraoperative information are also summarized in Table 1. The median operative time was 10 minutes longer among statin users (median: 202 vs 192 minutes).
A descriptive unweighted summary of preoperative and postoperative renal function is shown in Supplementary Table S1. Statin users had an unadjusted mean preoperative eGFR that was 6.36 mL/min/1.73 m2 lower (95% confidence interval [CI] 2.61 to 10.11, p < 0.001) compared with nonusers (mean ± SD, 71.1 ± 17.6 mL/min/1.73 m2 vs 77.4 ± 19.4 mL/min/1.73 m2). However, this was no longer statistically significant in a PS-weighted two-sample t-test where the weighted mean pre-RAPN eGFR was 1.28 mL/min/1.73 m2 (95% CI −2.66 to 5.22 mL/min/1.73 m2, p = 0.52) lower for statin users compared with nonusers.
The primary analysis with propensity score weighting to evaluate associations of preoperative statin use with changes in eGFR after RAPN is shown in Table 2. There was no evidence of an association with preoperative statin use with changes in eGFR after RAPN (LRT p = 0.66). The estimated mean change in eGFR from pre-RAPN to 12 months after RAPN was −11.4 mL/min/1.73 m2 (95% CI −15.0 to −7.8 mL/min/1.73 m2) among statin users and −12.4 mL/min/1.73 m2 (95% CI −15.3 to −9.6 mL/min/1.73 m2) among those not using statins preoperatively in our propensity score-weighted analysis. The estimated difference in mean change in eGFR from pre-RAPN to 12 months after RAPN adjusting for WIT, operative time, and EBL was 1.00 mL/min/1.73 m2 (95% CI −2.90 to 4.90 mL/min/1.73 m2, p = 0.62). Fitted estimates of eGFR at each timepoint are shown in Figure 1.
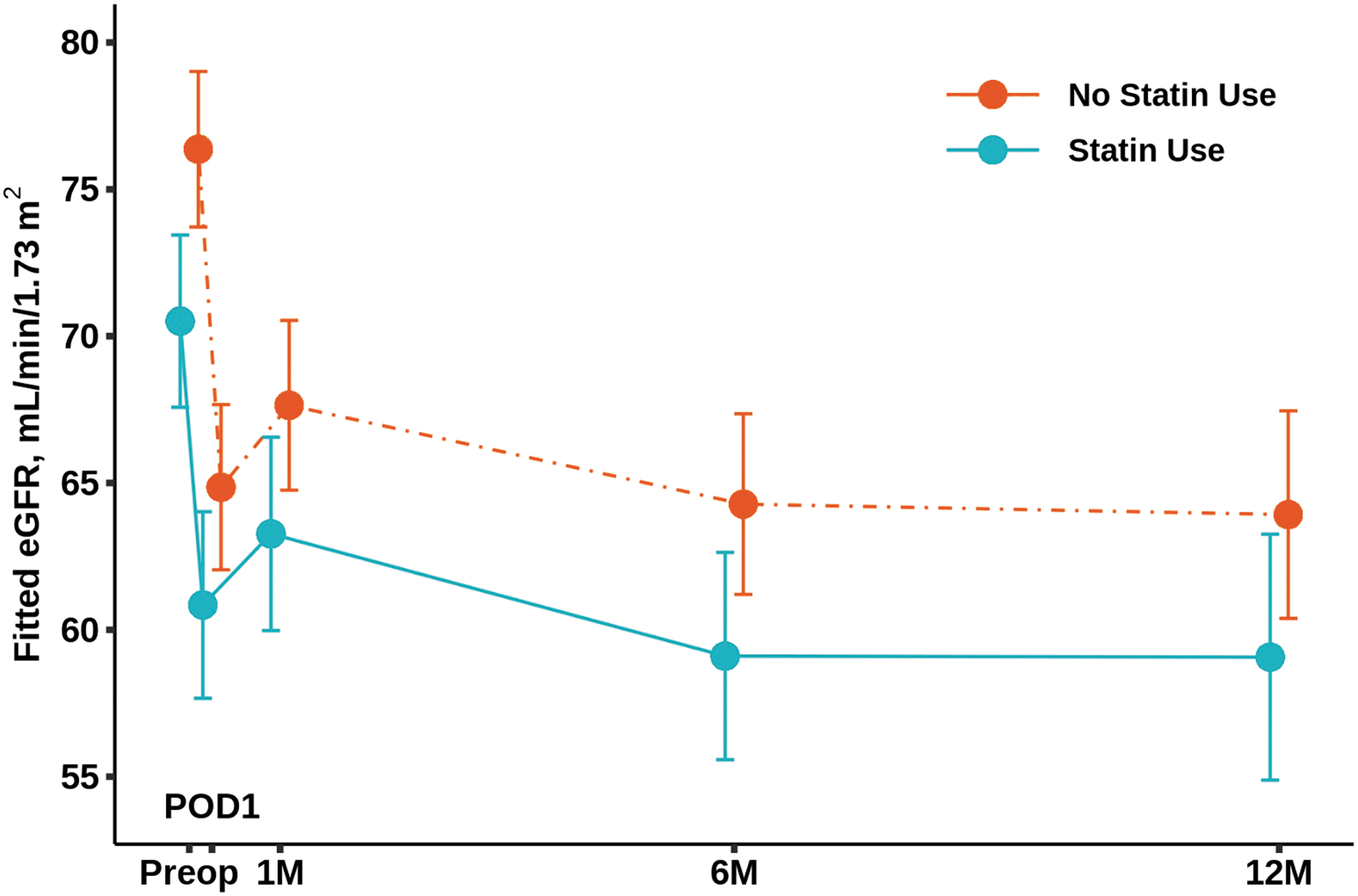
Fitted eGFR before and after robot-assisted partial nephrectomy according to preoperative statin use. The fitted eGFR was estimated from a longitudinal mixed effects linear regression model with random patient-specific intercepts and slopes. Stabilized inverse propensity score weighting was used to improve balance between those who did use statins preoperatively and those who did not use statins preoperatively. Fitted estimates at POD1, 1 month (1M), 6 months (6M), and 12 months (12M) assume a warm ischemia time of 18 minutes, operative time of 195 minutes, and estimated blood loss 300 mL or less. Vertical bars represent 95% confidence intervals for the fitted estimates. eGFR = estimated glomerular filtration rate; POD1 = postoperative day 1.
Association of Preoperative Statin Use with Change in Renal Function After Robot-Assisted Partial Nephrectomy: A Propensity Score-Weighted Analysis
CI = confidence interval; eGFR = estimated glomerular filtration rate; PS = propensity score; RAPN = robot-assisted partial nephrectomy.
Preoperative eGFR of 60 or higher was observed in 76.6% (128/167) of statin users and 85.6% (190/222) of patients who did not use the medication preoperatively. Among the 128 statin users with normal preoperative eGFR, postoperative eGFR remained ≥60 mL/min/1.73 m2 for 61.1% (77/126) at POD1, 69.5% (73/105) at 1 month, 66.7% (58/87) at 6 months, and 67.2% (39/58) at 12 months after RAPN. Among the 190 patients with normal preoperative eGFR who did not use statins preoperatively, postoperative eGFR remained ≥60 mL/min/1.73 m2 for 71.1% (135/190) at POD1, 75.8% (119/157) at 1 month, 71.4% (85/119) at 6 months, and 66.3% (59/89) at 12 months post-RAPN.
Discussion
Acute kidney injury (AKI) is a common postoperative complication for patients undergoing major surgery. The incidence of patients with postoperative AKI fluctuates depending on the type of surgery. The incidence of AKI after cardiac surgery has been estimated between 7.7% and 40%, 10 whereas in patients undergoing major abdominal surgery, the overall incidence is estimated to be 6.8% to 13.4%. 11 Statins are the preferred treatment for lowering lipid levels to prevent coronary atherosclerotic events. In addition, statins have a vasodilatory, anti-inflammatory, antioxidant, and antithrombotic effect, which may assist in endothelial recovery and improved oncologic outcomes. 12
Current guidelines recommend continuation of statins in the perioperative period in noncardiac surgery. 13,14 Multiple studies have shown contradictory evidence regarding the postoperative effect of statins in renal function in patients undergoing elective surgery. 11,12,15 –17 Siyang and colleagues conducted a meta-analysis looking for the effect of perioperative statin use on postoperative renal outcomes in patients undergoing cardiac surgery. 18 This group concluded that the use of perioperative statins in patients undergoing cardiac surgery was associated with an increased occurrence of postoperative renal complications. 18 Putzu et al. conducted a meta-analysis looking for the association between perioperative statin use and postoperative outcomes in adult cardiac and noncardiac surgery. 19 This meta-analysis showed that patients undergoing cardiac surgery pretreated with statins had a higher incidence of AKI. However, in noncardiac surgery patients this association was not present. 19 In contrast, Brunelli and colleagues found a decreased risk of postoperative AKI in statin users undergoing elective surgery. 20 Molnar et al. reported an association between perioperative statin and a reduced risk of AKI in patients undergoing major elective surgery. 3 Argalious and coworkers examined the incidence of postoperative AKI change in patients taking statin prior a noncardiac surgery. 17 They found no association between the use of perioperative statins and postoperative AKI. 20 Our study findings revealed that those patients who underwent RAPN with a history of perioperative statin consumption were older men with a lower preoperative eGFR. Statin use did not show any difference on renal function after RAPN.
There is limited evidence on the effects on continuation or discontinuation of statins in patients undergoing RAPN. Schmid et al. analyzed the National Surgical Quality Improvement Program data set, finding that 1.8% of patients developed AKI 5.4 days after partial or radical nephrectomy. 21 A later study by the same group evaluated a database of >200,000 patients that underwent a partial or radical nephrectomy. This study found an incidence of AKI in 5% of patients after the procedure. 22 Krane and coworkers prospectively studied the impact of statins on renal function in 104 patients undergoing RAPN. 2 This group determined that statins do not have an influence in perioperative renal function after RAPN. 2 Joshi et al. described a prospective study of 1056 patients undergoing partial nephrectomy to evaluate the effect of perioperative statin use on AKI rates. 4 This group concluded that there was no association between perioperative statin use and the rate of postoperative AKI. 4
The strength of this study is that it is a single surgeon series that eliminates operative technique as a variable in the analysis. The main limitation to this study is its retrospective nature. This limits the ability to accurately account for all possible factors influencing the change in post-RAPN eGFR. Other limitations include small sample size, short follow-up and no identification of the indication, type, duration, and dosage of statins within the statin group. Another weakness of our analysis is that it does not include perioperative lipid values. This information may have proved useful for evaluating its impact on postoperative renal function. In this study, there was not an observed effect on post-RAPN eGFR between the statin group and nonstatin group.
Conclusions
Patients on statins had lower preoperative eGFR compared with those not taking statins. Perioperative statin use does not appear to be associated with change in eGFR after RAPN in the immediate postoperative period or at 1 year follow-up.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.