
Abstract
Background:
Holmium laser enucleation of the prostate (HoLEP) is a highly effective and durable minimally invasive surgery for benign prostatic hyperplasia. Historically, alternative treatments for large glands (≥175 cc) are associated with prolonged length of stay (LOS) and postoperative catheterization. However, advances in laser technology combined with surgical technique optimization have early evidence supporting same-day discharge. We look to examine contemporary same-day discharge outcomes for large glands.
Materials and Methods:
With Institutional Review Board (IRB) approval we queried our electronic medical record and retrospective clinical registry to examine perioperative outcomes of large gland (≥175 cc) prostates that underwent HoLEP with consideration for same-day discharge.
Results:
From December 10, 2019 to September 29, 2020 we identified 55 patients with a preoperative prostate size ≥175 cc (39 CT, 12 MRI, 4 transrectal ultrasound), of which 45 were scheduled for same-day discharge and 10 for admission. Mean preoperative prostate size was 229.9 cc (range 175–535 cc) and 36 (65.5%) were in urinary retention. Mean preoperative prostate-specific antigen (PSA) was 8.58 ng/mL, American Urological Association Symptom Score (AUASS) 22.3, and Qmax 8.8 mL/second. At 3 months postoperative follow-up mean AUASS was 6.7, PSA 0.87 ng/mL and Qmax 20.4 mL/second. All comer same-day discharge rate was 70% (38/55). Of patients planned for same-day discharge 38/45 (84%) were effective. Average LOS for all patients was 11.8 hours with catheterization of 21.2 hours. When compared with 2010 published large gland outcomes, our current LOS represents a 220% reduction. Looking specifically at patients planned for same-day discharge, average LOS and catheter duration was 8.8 and 17.0 hours, whereas LOS and catheter duration for patients planned for admission was 25.7 and 39.4 hours, respectively.
Conclusions:
We report the first outcomes of preoperatively planned same-day discharge for HoLEP in large glands (≥175 cc). A combination of technologic advances and optimization of technique have allowed for a safe adoption of same-day discharge, providing additional advantages over alternative large gland treatments.
Introduction
Holmium laser enucleation of the prostate (HoLEP) is a highly effective and durable minimally invasive surgery for benign prostatic hyperplasia. 1,2 Alternative treatments (open or robot-assisted simple prostatectomy [RASP]) for large glands (≥175 cc) are associated with prolonged length of stay (LOS) and postoperative catheterization. 3 Despite technology (robotic platform) and technique advances (retropubic, transvesical, and single-port) in the management of large gland simple prostatectomy, the majority remain overnight with average LOS ranging 1.05–5 days and catheterization 3.5–8.1 days. 4 –7
The safety of transitioning HoLEP management to day-surgery was first published in 2003 by Larner et al. in 38 men with gland size <60 cc. 8 Since then, a small number of studies have examined same-day discharge in selective patients, typically with smaller glands. 9 –14 Abdul-Muhsin et al. (2020) attempted to find objective measures to predict safe same-day discharge cases; however, the major barrier identified was degree of hematuria. At our center, advances in pulsed modulated laser technology for improved hemostasis, combined with surgical technique optimization within a health system familiar with perioperative HoLEP care have demonstrated early evidence for same-day discharge and same-day trial of void (TOV). 9,15
Locally, we transition toward same-day discharge consideration for initially select HoLEP cases in 2019 with provider education and care pathway handouts provided to our postanesthetic care units (PACUs). As our center optimized our care pathway and gained confidence in our outcomes, we expanded patient eligibility for same-day discharge. Anecdotally, with the use of the Moses 2.0 optimized for benign prostatic hyperplasia (BPH) we have minimal hematuria concerns immediately postoperatively, irrespective of gland size. We look to examine contemporary same-day discharge outcomes specifically in patients assessed to have large glands defined as ≥175 cc.
Materials and Methods
After Institutional Review Board (IRB) approval, we queried our electronic medical record and retrospective clinical registry for specifically large gland prostates (≥175 cc) that underwent HoLEP with consideration for same-day discharge from December 10, 2019 to September 29, 2020. Before the study period, our three endourologists adopted a practice of considering all HoLEP patients for same-day discharge and same-day catheter removal. 9 Preoperative reasons to exclude same-day discharge consideration included lack of a caregiver or significant comorbidities (including American Society of Anesthesiology (ASA) ≥4, inability to hold therapeutic anticoagulation, or dual antiplatelet therapy). 16
Per our revised local practice, the entire surgical care team and PACU received education and are familiar with our post-HoLEP procedures, including avoidance/limiting postinduction narcotics. 9 It is important to acknowledge that we have >20 years of HoLEP care at our center, which results in a system familiar with the perioperative course. Our HoLEP technique has evolved over the past decade with the investigation and adoption of high-power laser technology (550 μm D/F/L fiber with Moses 2.0 optimized for BPH—Lumenis Ltd., Yoknaem, Israel). Bi- or trilobar enucleation depends on the presence or absence of a median lobe with a bottom-up technique. Laser settings for enucleation include 2 J and 40–60 Hz on primary and 1 J and 20 Hz on secondary foot-pedal for intermittent vessel hemostasis. We previously showed Moses 2.0 improves hemostasis vs conventional techniques. 15 We adapted our previously published technique by moving away from predominately peeling (blunt scope dissection) toward an increased use of noncontact lasering with Moses facilitated bubble dissection. The Piranha Wolf morcellator was used in all cases.
Postoperatively, 3 L continuous bladder irrigation (CBI) using 0.9% saline (NS) was ran through 20–22 F three-way Foley catheter with 40–60 mL sterile water in the balloon. At the completion of 3 L, the PACU team clamps CBI and assess hematuria. If the urine output (to the tubing) was ketchup colored (by visual hematuria scale 9,14 ) or blood clots block the tubing, an additional 3 L bag was run full speed. If the urine was not ketchup colored upon initial clamping, then the nursing teams monitored outputs >30 minutes with ambulating. If the urine remained less than ketchup colored, and the patient met day surgery discharge criteria then they were sent home from PACU. If the urine remained ketchup colored after a second 3 L NS bag, the urology service assessed the patient. Although we implemented the use of an objective visual scale for hematuria there remains a subjective component to evaluating these patients postoperatively. For any borderline cases, the urology team was contacted at which point the decision for admission vs discharge was made by the surgeons.
All patients who failed same-day TOV receive 18 F Coude-tip catheter overnight with a repeat TOV on postoperative day 1 (POD1). Patients admitted to hospital had a TOV on POD1 at 06:00. All HoLEP patients receive patient-reported outcomes (PROs) surveys (American Urological Association Symptom Score [AUASS], BPH Index, Michigan Incontinence Symptoms Index, Sexual Health Inventory for Men, generalized Anxiety Disorder-7, Male Sexual Health Questionnaire Ejaculatory Function Short Form) preoperative and before their 3-month follow-up. We have a preference for in person 3-month follow-up appointments; however, because of the COVID-19 pandemic some of our patient follow-ups were conducted through virtual visit.
Baseline demographics, medical history, past urologic surgeries, intraoperative and postoperative variables along with follow-up and Clavien–Dindo complications were acquired. All comorbid patients or those on dual antiplatelet therapy or therapeutic anticoagulation received medical clearance with medication recommendations perioperatively. None of our patients required therapeutic anticoagulation bridging. Our primary outcomes of interest were hospital LOS (recorded in minutes from surgical procedure conclusion to patient discharge) and postoperative duration of catheterization (recorded in minutes from surgical procedure conclusion to the TOV).
Statistical analysis was performed using IBM SPSS software (version 25, Armonk, NY). Continuous variables were expressed as mean and range, whereas proportions were used for categorical variables. Statistical analysis included two-tailed homoscedastic and heteroscedastic t-tests as well as chi-squared or Fisher's exact test (when individual group sizes <10) with significance set at p < 0.05.
Results
There were 55 patients with preoperative prostate size ≥175 cc (39 CT, 12 MRI, 4 transrectal ultrasound [TRUS]) scheduled for HoLEP between December 10, 2019 and September 29, 2020. There were 45/55 (82%) patients scheduled for same-day discharge, whereas 10 patients were scheduled for overnight admission based on comorbidities. Patient and perioperative demographics are outlined in Table 1. Of patients undergoing concurrent stone surgeries, 2/8 (25%) had an unplanned hospital admission (vs 5/37 (14%) unplanned admission for HoLEP without concurrent stone surgery, p = 0.59). Five (9%) patients had prostate surgery before their HoLEP consult (two transurethral resection of the prostate [TURP], two Greenlight laser vaporization of the prostate [GLVP], one Rezum) with one patient undergoing two separate GLVP before consultation. Of the 10 patients planned for admission, 2 (20%) utilized antiplatelet or anticoagulation medications beyond ASA 81 mg daily (one clopidogrel and one rivaroxaban). Of the 45 patients planned for same-day discharge, 8 (18%) utilized antiplatelet or anticoagulation beyond ASA 81 mg daily (one ASA 325 mg, one clopidogrel, two Coumadin, two apixaban, and two rivaroxaban).
Patient and Perioperative Demographics for All Holmium Laser Enucleation of the Prostate in Glands ≥175 cc After Transition to Same-Day Discharge Consideration
ASA = American Society of Anesthesiology; HoLEP = holmium laser enucleation of the prostate; n = number of patients.
Mean preoperative prostate size was 229.9 cc (range 175–535 cc) obtained by CT, MRI, or TRUS imaging modalities (Table 2). Mean rate of tissue enucleation was 2.34 g/minute (range 1.11–4.55 g/minute), and morcellation was 8.56 g/minute (range 3.41–22.5 g/minute). One patient required a perineal urethrostomy (preoperative prostate size 535 cc) to reach the prostate.
Comparison of Preoperative Prostate Size Estimation (CT, MRI, or TRUS) with Intraoperative Specimen and Postoperative Pathologic Dry Weight
TRUS = transrectal ultrasound.
A comparison of preoperative and 3-month postoperative follow-up investigations and PROs is outlined in Table 3. Overall, mean preoperative prostate-specific antigen (PSA) was 8.58 ng/mL (range 2.70–15.66 ng/mL), AUASS 22.3 (range 2–35), and Qmax 8.8 mL/second (range 2.7–19.5 mL/second). At 3 months postoperative follow-up the mean AUASS improved to 6.7 (2–12), PSA 0.87 ng/mL (0.082–3.25 ng/mL) and Qmax 20.4 mL/second (10.9–29.9 mL/second) (all p < 0.05).
Comparison of Preoperative Serum PSA, Validated Symptom Scores (AUASS, QOL, BPH Index, SHIM, MISI, GAD-7, and EjD), Postvoid Residuals and Urinary Flow to 3 Months Follow-Up
AUASS = American Urological Association Symptom Score; BPH = benign prostatic hyperplasia; EjD = Male Sexual Health Questionnaire Ejaculatory Function Short Form; GAD-7 = Generalized Anxiety Disorder-7; MISI = Michigan Incontinence Symptoms Index; PSA = prostate-specific antigen; Qavg = average urinary flow; Qmax = peak urinary flow; SHIM = Sexual Health Inventory for Men.
All comer same-day discharge rate was 70% (38/55). Of patients planned for same-day discharge 38/45 (84%) were effective. Average LOS for all large gland patients (n = 55) was 11.8 hours with catheterization of 21.2 hours (Fig. 1). Looking specifically at patients planned for same-day discharge (n = 45), average LOS and catheter duration were 8.8 and 17.0 hours, whereas LOS and catheter duration for patients planned for admission (n = 10) were 25.7 and 39.4 hours, respectively (LOS p = 0.0052. Catheterization p = 0.23) (Fig. 2). The average LOS and catheterization for patients actually discharged on the same day as their HoLEP (n = 38) were 2.7 and 16.7 hours, respectively.

Comparison of mean LOS and postoperative catheter duration for patients assessed to have large gland prostates (≥175 cc) undergoing holmium laser enucleation of the prostate between historical cohort 17 (Krambeck et al., 2010) and modern cohort after adoption of same-day discharge consideration. LOS, length of stay. Color images are available online.
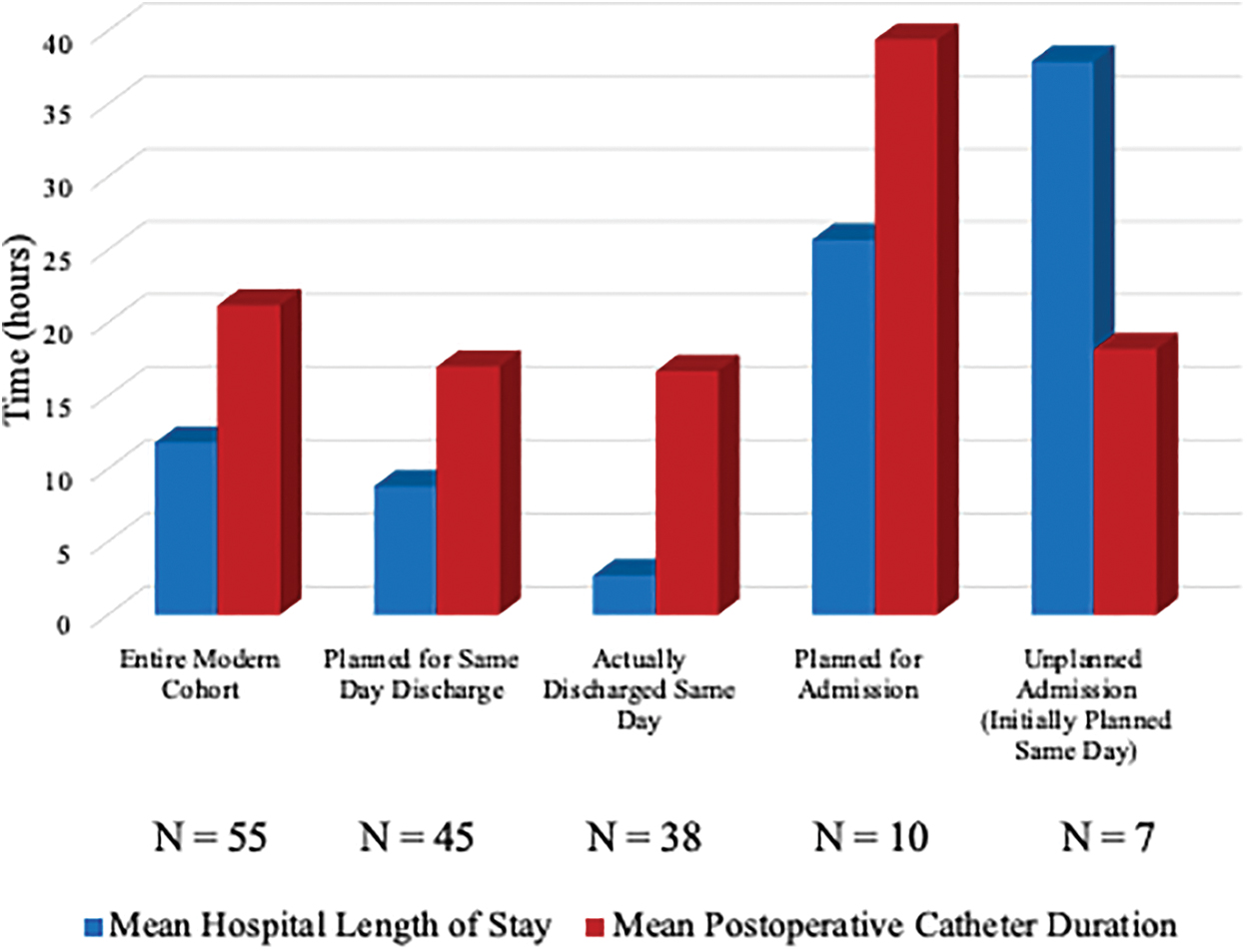
LOS and postoperative catheter duration for patients assessed to have large gland prostates ((≥175 cc) undergoing holmium laser enucleation of the prostate with consideration for same-day discharge broken down by clinical course. Color images are available online.
Reasons for unplanned admission in our seven patients included four genitourinary (GU) reasons (postoperative hematuria) and three non-GU system reasons (one atrial fibrillation requiring cardiology, one bradycardia requiring cardiology, and one vocal cord mass on intubation requiring intraoperative laryngoscopy/biopsy and postoperative observation).
Postoperatively, unplanned medication encounters occurred in 3/55 (5.5%) patients before their 3-month follow-up (two Emergency Department [ED], one Urology Office). The two patients presenting to the ED after discharge had infectious complications (one urinary tract infection—Clavien–Dindo II, one urosepsis with acute kidney injury [AKI] requiring temporary [<14 days] dialysis—Clavien–Dindo IVa). Overall complication rate was 13/55 (23.6%) with only 1/55 patient having a Clavien–Dindo grade 3 or higher complication (Grade: I[5], II[7], III[0], IV[1], V[0]). The single IVa complication was a 74-year-old man with preoperative urinary retention and indwelling catheter who underwent same-day discharge and TOV with success (postvoid residual = 20 mL) followed by increased hematuria/clots and fever starting >24 hours postoperatively. He subsequently presented to ED with clot retention, fever, and urosepsis (Sequential Organ Failure Assessment score ≥2) leading to a transient AKI requiring short-term dialysis (<14 days). After antibiotic therapy his 3-month follow-up renal function was at baseline with complete emptying. No patients had bladder neck contractures or required subsequent genitourinary tract surgery.
Discussion
We report the safety and efficacy of same-day discharge considerations in specifically large gland prostates undergoing HoLEP. The overall average LOS was 11.8 hours with catheter duration of 21.2 hours. When compared with large gland outcomes at our center in 2010, our current LOS represents a 220% reduction. 17 For all large gland patients, we achieved >70% rate of same-day discharge with a 3.6% re-presentation to ED and <2% readmission rate before scheduled follow-up. For patients specifically planned for same-day discharge our success rate was 84%. Transitioning to same-day discharge consideration and same-day TOV has not compromised clinical outcomes. Compared with the current literature, we included a wider range of patients who were eligible for same-day discharge and provide evidence to support the inclusion of large glands.
As one of the recurring barriers for same-day discharge in large gland HoLEPs is the immediate postoperative degree of hematuria, the utilization of Moses 2.0 technology has proven valuable in its improved hemostasis along with adopting a surgical technique that uses less blunt dissection as well as implementing a system for monitoring patient's eligibility for discharge postoperatively. 14,15 As technologies and techniques have improved, morcellation efficiency has also improved when comparing with our own center's rates reported 10 years ago. 17 We feel that transitioning to the Wolf Piranha morcellator as well as the use of Lumenis Moses 2.0 and subsequent improved hemostatic surgical technique all play a factor in allowing continuous morcellation because of improved observation.
There is minimal difference in length of catheterization compared with large gland HoLEPs performed at our center 10 years ago or between subcohorts in our study. 17 This catheter duration (<24 hours) remains significantly shorter than either robotic or open simple prostatectomy for large gland BPH management. 4 –7 Factors contributing to the unchanged catheter duration include access to our urology clinic for same-day TOV occurring later in the day or provider comfort. Ultimately, we believe that if having the TOV effectively passed the following morning allows for >70% of large gland HoLEPs to be safely performed as same-day discharge, then this is a positive outcome in the setting of transitioning large glands to same-day discharge.
Examining the unplanned admission cohort (Fig. 2) is interesting as the duration of their catheterization is not different than the entire cohort, planned same-day cohort or actually discharged same-day cohort. This finding points toward the nonurologic etiology of unplanned admissions and shows that ongoing hematuria, CBI, or failed TOV is likely not contributing to their longer LOS (>24 hours) as most had effective TOVs in the morning of POD1.
In our study, 14.5% of patients had concurrent urolithiasis intervention without a significant difference in LOS, catheter duration, or unplanned admission. Our results support the previous few studies that examined same-day discharge feasibility in patients who utilize antiplatelet/anticoagulation medications. 12,14 Changing our operative technique to improve hemostasis is reflected in our lower rate of unplanned admissions for hematuria (6.7%) compared with other literature for same-day discharge (31.9%). 14 Our findings that large gland size itself is not a contraindication to same-day discharge is supported by Abdul-Muhsin H et al. who showed effective same-day discharge was associated with larger glands (88.4 vs 69.0 cc p = 0.033); however, primarily because of degree of postoperative hematuria they concluded that it would be safer to consider admitting these patients. 14
Only 3.6% presented to the ED postoperatively with one requiring readmission. This is lower than the current literature on same-day discharge post-HoLEP, which reports a range of ED presentation 28%–36.7% and 3.4%–28.9% readmission. 8,10 –12,14 We believe this difference is a combination of the improved operative hemostasis, thorough discussion with patients regarding healing expectations, and a strong clinic support staff who have worked within a system familiar with perioperative HoLEP care for >20 years at our center. It is important to acknowledge one patient had a grade Iva complication and was fortunate to return to his baseline. It is unclear if his clinical course would have changed by admitting overnight or POD1 TOV, as the onset of hematuria/clots and fever occurred >24 hours after surgery. Even for the 10 comorbid high-risk patients planned for admission, half were discharged within 24 hours and may have had the same resultant postdischarge complication. Despite ongoing efforts to minimize infectious complications with preoperative urine cultures and targeted preoperative antibiotics we consent all patients that we are unable to completely remove infectious complications from surgical intervention of the urinary tract.
There are few specific situations (e.g., bladder diverticula) where RASP may be advantageous; however, HoLEP has shorter operative time, less transfusions, catheterization, and LOS. 18,19 Transitioning to same-day discharge and TOV further adds to the advantages of HoLEP. GLVP for prostates >100 cc show increased conversion to electrocautery TURP (7.3%–16%) for hemostasis along with increased retreatment (1.2%–16% at 12%–36 months). 20 –22 Similarly, novel use of transurethral bipolar plasmakinetic enucleation/resection is associated with longer LOS and catheterization vs HoLEP. 22,23 Further prospective randomized studies are required to identify the role of alternative treatments compared with safe and durable large gland HoLEP outcomes.
A limitation is the generalizability of our surgical outcomes and implementation of a same-day discharge protocol within this large gland prostate cohort, particularly for low volume centers or surgeons starting to perform HoLEP. The challenge of the HoLEP learning curve have been well documented and the effect of surgeon expertise on effective management in these large gland prostates and ability to safely transition to same-day discharge is important. 24 Also, as our high-volume center has provided HoLEP for >20 years our patients interact with a system (operative team, nursing, PACU, and anesthesia) that is familiar with the typical perioperative course.
Conclusions
We report the first outcomes of same-day discharge for HoLEP in specifically large glands (≥175 cc). A combination of technologic advances and technique optimization at our high-volume center have allowed for a safe adoption of same-day discharge, providing additional advantages over alternative large gland treatments.
Footnotes
Author Disclosure Statement
T.L. and M.E.R. are consultants for Boston Scientific and Lumenis. A.E.K. is consultant for Boston Scientific, Lumenis, Ambu and Virtuoso, and is on the data safety monitoring board for Sonomotion. M.A.A., M.S.L., and D.K.A. have none.
Funding Information
No funding was received for this article.