
Abstract
Objective:
The aim of the study is to propose a visual classification for encrusted stents (ESs) to help choose the appropriate endourologic treatment.
Materials and Methods:
A multicenter, retrospective, and descriptive study was performed. A total of 140 patients with encrusted Double-J stents were enrolled from 5 different institutions. The novel visual grading for ureteral encrusted stent (V-GUES) classification system ranges from A to D, increasing with severity of encrustation.
Results:
ESs could be removed with a single intervention in 112 patients (86.8%). Type A and B ESs could be removed in all patients (100% success). Type D stents had minor retrieval and stone-free rates (p = 0.006 and p < 0.0001, respectively). Flexible ureteroscopy had a low success rate (77.7%) for type C stents (odds ratio [OR]: 0.21). Combined access had a 100% success rate for retrieval of type C ESs and a 92.9% success rate for type D ESs (OR: 9.18). Type D stents were associated with patients requiring more than one session to retrieve the stent (OR: 0.11) and stones (OR: 0.21).
Conclusions:
The V-GUES system is associated with treatment success rates of ES retrieval and stone-free status. It is also associated with the complication rate and the number of sessions needed for patients to be stent and stone free. The V-GUES classification could help counsel patients about the best treatment options and their outcomes. Further prospective studies will be needed to provide external validation.
Introduction
Double-J stents are essential tools for urologists today, especially in the field of endourology. Since their introduction into urology, Double-J ureteral stents have been widely used worldwide. Some current indications for use of a Double-J stent include acute obstructive uropathy, ureteral strictures, congenital anomalies, pelvic oncological processes, and at the end of urological procedures for drainage of the upper urinary tract. 1 –5 It has been described that the ideal stent is one that is biocompatible, radio-opaque, avoids encrustation and infection, causes little discomfort, has a reasonable cost, and is effective in resolving urinary tract obstruction. 1 However, despite recent efforts to find the ideal stent, even with recent technological advances, the problems of stents have not yet been solved. 2 –4
Encrustation is one of the most critical problems seen with Double-J stents, leading to high morbidity rates in patients. An encrusted stent (ES) is one that cannot be removed simply by cystoscopy due to calcification or stone formation around the stent. 1 Therefore, an ES, by definition, will require an ancillary procedure for its removal.
Currently, there is no consensus about the optimal surgical management of ESs. ES removal depends on the severity of calcification and represents one of the most significant surgical challenges for urologists. 5 –14
In 2009, a simplified approach based on a ureteral stent grading system (the FECal grading system) was proposed to gauge ESs. 1 The FECal (forgotten, encrusted, and calcified) grading system has been widely mentioned and used by urologists; however, this grading system based on just nine patients does not recommend a specific treatment modality concerning each grading and is not related to the ES treatment outcomes. Additionally, time-consuming and complex scores for ESs have been developed, but unfortunately they have not been accepted worldwide. 15 Therefore, a simple, fast, and trustworthy grading system that helps choose an ES's treatment and patient's counseling is necessary for the present era. Thus, this study's main objective is to propose an easy, fast, and effective classification for ESs, which could be helpful in the complicated decision-making process of the treatment required for ESs and their associated urinary stones.
Methodology
A multicenter, retrospective, and descriptive study was performed. A total of 140 patients with encrusted Double-J stents were enrolled from 5 different institutions. We included all patients with available information and with an encrusted Double-J ureteral stent from each participating center from April 2014 to July 2020. We excluded patients who were able to remove the stent without resistance with simple cystoscopy or had incomplete information. All grades of stent calcification severity were evaluated by the senior surgeon of each center using a preoperative noncontrast CT (NCCT) scan to develop the novel visual grading for ureteral encrusted stent (V-GUES) classification system. We grouped each ES based on the shape and location of calcifications in a preliminary alphabetical classification (a–q); after that to simplify the grading system, we grouped all calcified stents (a–q) into four more wide categories (A, B, C, and D) that give birth to the new V-GUES classification based on NCCT (Fig. 1). ESs with distal calcifications, sparing the ureter portion and proximal tail of the stent, were included in group A. Group B included ESs with distal tail calcification, sparing the proximal tail, but not the ureteral portion. Group C included ESs with calcification on the stent's proximal tail and could have distal tail calcification while sparing the ureter stent's portion. Finally, group D included all stents with calcification on the stent's proximal tail and ureter portion and, additionally, could have calcification on the distal tail (Fig. 1). Importantly, of note, type A and C ESs do not have ureteral calcifications.
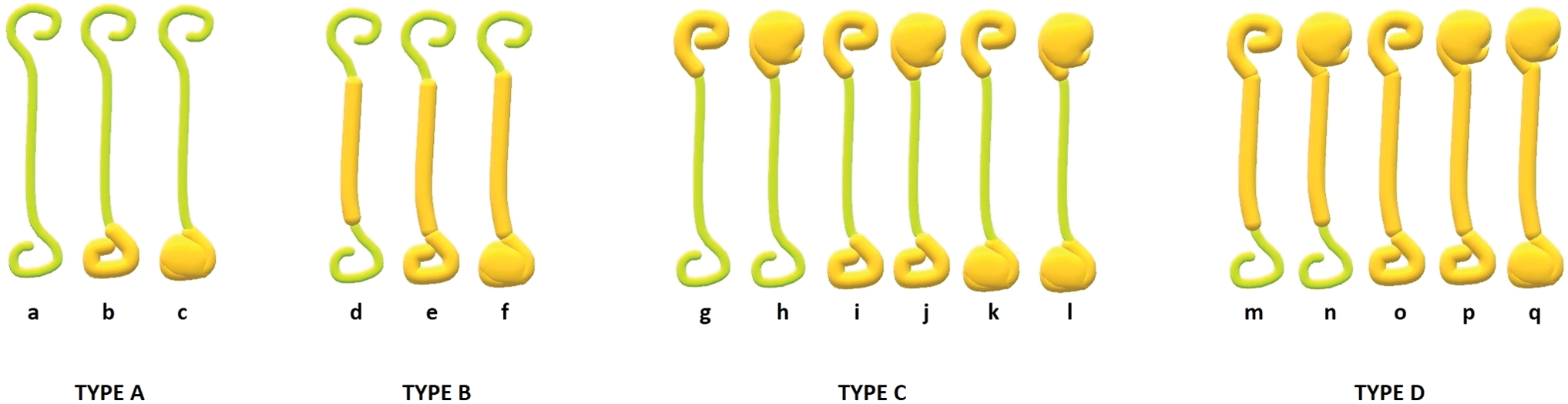
Type A: linear or nonlinear calcification in the distal stent's tail, susceptible to being retrieved with cystolithotripsy; type B: linear or nonlinear calcification in the distal stent's tail associated with calcification of the stent's ureteral portion, susceptible to being removed with semirigid ureteroscopy; type C: linear or nonlinear calcification of the stent's proximal portion, which could also be associated with distal stent's tail calcification without compromising the ureteral stent's portion, susceptible to being removed with combined access; and type D: linear or nonlinear calcification of the proximal stent's portion associated with calcification of the ureteral stent's portion, which could also be calcification of the distal stent's tail, susceptible to removal with combined access. Please check the supplementary video to see a non-enhanced CT scan with a Type C encrusted stent. Color images are available online.
The data collected retrospectively were age, sex, affected side, hydronephrosis, body mass index (BMI), and initial and final creatinine levels. To analyze treatment outcomes, we evaluated the first treatment each center had offered for the encrusted stent, the success of the first and subsequent treatment sessions, and the number of procedures required for the patient to be stent and stone free. Finally, we evaluated the postoperative complications. Stone-free status was defined as the absence of any fragments in the postoperative NCCT.
The statistical program SPSS 25 for Windows® was used for descriptive statistics. Qualitative variables were reported as frequency and percentage. The Kolmogorov–Smirnov normality test with Lilliefors correction was performed on quantitative variables. If they fulfilled the normality assumptions, they were reported as mean and standard deviation; if the variables did not fulfill the normality criteria, they were reported as median and 25th to 75th percentile. Four groups were formed for the new proposed classification: A, B, C, and D. Comparisons between groups and dependent variables were performed using the chi-squared test. Any p-value <0.05 was reported as statistically significant. Additionally, we performed association tests by odds ratio (OR) calculation with a confidence interval of 95%. This study was approved by the Institutional Review Board (CI/HRAEB/052/2020).
Results
Data of 140 patients were obtained and just 129 patients were included, 73 (56.6%) were women, while 56 were men (43.4%). The right side was affected in 77 (59.7%) patients and the left side in 52 (40.3%) patients. The mean age was 49.9 years. Hydronephrosis was present in 72 patients (55.8%). The mean BMI was 29.4, mean preoperative creatinine level was 1 mg/dL, and postoperative level was 0.91 mg/dL. Type C and D ESs were the most common ESs. The frequency of all types of ESs (A, B, C, and D) is described in Table 1.
Demographic Data and Complications
Mean (percentile 25–75).
BMI = body mass index; fURS = flexible ureteroscopy; PCNL = percutaneous nephrolithotomy; V-GUES = visual grading for ureteral encrusted stent.
Cystolithotripsy, semirigid ureteroscopy, flexible ureteroscopy (fURS), percutaneous nephrolithotomy (PCNL), mini-PCNL, and combined access (endoscopic combined intrarenal surgery and PCNL plus cystolithotripsy or semirigid ureteroscopy) were the endourology treatments used for all the reported ESs (Table 1). The first procedure performed on each patient to treat the ES is described in Table 1.
ESs could be removed with a single intervention in 112 patients (86.8%). Type A and B ESs could be removed in all patients (100% OR: ND). On the other hand, type D stents had minor retrieval success compared with the rest of the ESs (p = 0.006) (Table 2).
Overall Success Rates of Surgical Procedures Regarding the Visual Grading for Ureteral Encrusted Stent Classification
Chi-square test. A statistically significant value was considered at p = <0.005.
Stone-free status was achieved after the first procedure in 89 patients (69%). Patients with type C and D ESs had a lower stone-free status rate (Table 2). Outcomes of the surgical procedures for overall stent retrieval and stone clearance rates are summarized in Table 2.
Type A stents were predominantly treated with cystolithotripsy, type B with semirigid ureteroscopy, type C with combined access, and finally, type D stents were predominantly treated with semirigid ureteroscopy and combined access (Table 3). Each treatment's success rate of stent retrieval and stone-free status based on the V-GUES classification is summarized in Table 4. For stent retrieval, cystolithotripsy had a 100% (OR: ND) success rate for type A and B ESs (Table 4) in contrast to the success rate seen for type C (33% OR: 0.025) and D (0%) stents. Semirigid ureteroscopy had a low rate of success (56% OR: 0.37) in type D stents. fURS had a low success rate (77.7% OR: 0.21) in type C stents. Combined access had a 100% (OR: ND) success rate for type C ES retrieval and a 92.9% (OR: 9.18) success rate for type D ESs (Table 4).
Summary of Surgical Procedure Types with Respect to the Visual Grading for Ureteral Encrusted Stent Classification
Success Rates and Complications by Treatment Based on the Visual Grading for Ureteral Encrusted Stent Classification
Odds ratio 95% confidence interval.
ND, (not determinable): because these patients were all stent-free and stone-free with the first surgical intervention (100% success rate).
The number of procedures that patients needed to be stent and stone free is detailed in Table 5. Type D stents were associated with patients requiring more than one session to retrieve the stent (OR: 0.11) and stones (OR: 0.21).
Treatment Sessions Needed for Patients to Be Stent and Stone Free Based on the Visual Grading for Ureteral Encrusted Stent Scale
Odds ratio (95% confidence interval).
ND, not determinable: these patients were all stent free and stone free with the first intervention.
There were 29 complications reported at the end of the treatment for ESs and urinary calculi (Table 2). Patients with the type A ESs had a lower complication rate (OR: 0.22), and patients with type D stents had a higher complication rate (OR: 2.29). The summary of complications based on the V-GUES classification is summarized in Table 1.
Discussion
The ES is defined as an indwelling stent that cannot be retrieved with simple cystoscopy in an ambulatory setting. 1 Based on this definition, accompanying renal, ureteral, and bladder stones should also be considered in addition to calcium deposition inside the stent. Therefore, before treating an ES, urologists should know the different treatment modalities' success rates for each type of stent to best counsel their patients. Moreover, an ES is not necessarily a forgotten one, but it could be a stent that due to external causes could not be retrieved in a timely manner. Currently, a significant reason for leaving stents in patients could be by far the COVID-19 pandemic. 16 Therefore, we believe that the novel V-GUES system will help urologists manage the rising problem of ESs.
In 2009, a grading system for forgotten stents (FECal) was described based on only nine patients. 1 In the FECal system, the amount of encrustation is evaluated in five grades concerning the calcification sites. A scoring system has recently been published to identify ESs that will require multimodal therapy and multiple surgeries. 15 Multimodal treatment mentioned in this study is a broad concept that includes shockwave lithotripsy and endoscopic combined intrarenal surgery, therefore urologists do not have enough information to choose the right treatment for each patient based on this score. Of notable concern for the KUB scoring system is that individually, calcifications inside the kidney (K score) showed higher associations with the analyzed variables than the total score obtained from the sum of the individual calcifications (K+U+B). Therefore, the whole KUB score loses its strength to adequately counsel patients. A significant advantage of the V-GUES classification over the KUB score is that it is easier and faster. It just needs a visual evaluation of the NCCT scan without the need for calculations in outpatient daily care. Additionally, the KUB score did not show the score's association with complications as the V-GUES did. 15
Besides, evaluating the encrustation with an NCCT scan is another advantage over the previously defined grading systems. NCCT is accepted as the gold standard for renal stone diagnosis and preoperative planning, taking into account the radiation risk and costs (main disadvantages of the NCCT scan). Furthermore, as reported by Adanur and Ozkaya, the simple KUB film could fail to detect the exact amount and site of calcification of an ES. 5
For stent retrieval, a patient with an ES may need more than one surgical procedure. The novel V-GUES classification is associated with the number of procedures required for the patient to be stent free. Patients with type D stents had a higher risk of needing more than one procedure to be stent free (OR: 0.11) than the rest of the ESs.
To our knowledge, this is the most extensive case series of ESs reported, collecting data from four different countries in two different continents. Interestingly, our results show that the most severely calcified stents were the most prevalent of all the ESs evaluated based on the new V-GUES classification (type C and D stents). Some case series have found similar data, with most stents being complex calcified ESs. 3,8 At the same time, other authors have reported the opposite, with the most frequent ESs being the simplest calcified stents (some classified as FECal grades I and II). 5,6
Weedin and colleagues reported that the proximal stone burden (proximal calcification of the stent) is the most critical factor, and not the FECal classification, in predicting whether multiple surgeries will be necesary. 6 The new V-GUES classification is associated with the treatment outcomes based on the ES severity (Fig. 1).
Data show that the success rate decreased, while the severity of encrustation increased (Table 2). Therefore, the V-GUES classification could be useful in clinical practice because it is a quick calculation scale. The severity of encrustation proposed in the V-GUES scale is associated with the stent retrieval rate depending on the endourologic treatment chosen. Therefore, patients' counseling could be more precise and more straightforward using the V-GUES scale.
It has been described that the type of treatment employed for the ES influences the success rate of stent retrieval. 17 Based on the V-GUES classification, cystolithotripsy has shown a high success rate for type A stents (100% OR: ND). It is crucial to note that some type A ESs were reported to be treated by fURS. This issue is explained because some centers reported that they had performed ureteroscopy for a type A ES because there was a ureteral or renal stone beside the ES.
Semirigid lithotripsy has shown the worst success rate (OR: 0.37) of stent retrieval in type D stents. PCNL and combined access were associated with the best stent and stone retrieval success rates for type C and D stents (Table 4). Knowing the success rate for stent retrieval related to the type of treatment selected based on the V-GUES scale would help physicians counsel patients in daily patient care practice.
Stone clearance is an essential factor that must be considered because most patients need ancillary surgeries to get rid of the stones and for stent retrieval. The V-GUES classification is associated with the stone-free rate because the higher the ES grade, the lower the stone-free rate. Cystolithotripsy was 100% effective in achieving stone-free status for patients with type A stents, but, at the same time, had the worst efficacy for patients with type D ESs. Therefore, cystolithotripsy could be recommended as the treatment of choice for patients with type A ESs (Table 4). With semirigid ureteroscopy, the best success rate (100% OR: ND) for stone-free status is for patients with type B stents, and fURS is effective for types A and B. Combined intrarenal access has a high success rate in rendering patients stone free, especially for type C (75% OR: 2.25) and D (64.3% OR: 2.95) ESs (Table 4). Based on the above data, classifying ESs with the new V-GUES classification will allow urologists to choose the most reliable intervention and counsel the patient about the treatment and outcomes.
Some case reports describe that ES retrieval is possible in one single session. 10 –14,17 Combined access was associated with a high success rate of retrieval of type C and D ESs in one session. The number of sessions needed to render a patient stent and stone free is also essential. Patients with type C and D ESs have a higher risk of undergoing ancillary procedures to reach the stent- and stone-free status (Table 5).
Complications secondary to ESs, such as sepsis, can be lethal for patients. 18 Additionally, complications related to the surgical extraction of ESs increase morbidity rates. 19 The FECal classification does not predict complications related to active surgical treatment. The new V-GUES classification showed an association with complications with the ES's severity (Table 2). Therefore, the complication rate was directly proportional to the severity of encrustation on the V-GUES classification. For example, type D ESs show a higher complication rate after active treatment for stent retrieval than type A ESs (Table 2).
Although this is the most extensive case series evaluating ESs, we recognize our study's retrospective design. Based on this, it is of great relevance that the type of treatment was not chosen based on the scale, therefore we only collected data of all patients who were already operated on by each center's senior surgeon. Our study's retrospective nature could also explain how a notable percentage of patients were operated on using semirigid ureteroscopy. Different circumstances, including economic reasons (such as not having all the endourologic tools), influenced each center's treatment choice.
However, a randomized study would not be feasible for these cases that are uncommon and would also be potentially unethical given the potential severity of the consequences.
Additionally, the number of events with complications was low and may not be sufficient to detect a significant difference in complications.
In addition, as this is an international multicenter study, surgical procedures and surgical equipment vary, affecting the outcomes.
Conclusions
The novel V-GUES system is associated with treatment success rates of ES retrieval and stone-free status. It is also associated with complications and the number of sessions needed for patients to be stent and stone free. The new V-GUES classification helps in counseling patients about the best treatment options and their outcomes. Endoscopic combined access was associated with the best stent- and stone-free rates when treating type C and D stents. Further prospective studies will be needed to provide external validation to corroborate our results.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Video S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.