
Abstract
Background:
We aimed to compare the oncologic outcomes of intracorporeal urinary diversion (ICUD) and extracorporeal urinary diversion (ECUD) following robot-assisted radical cystectomy (RARC) in patients diagnosed with bladder cancer.
Materials and Methods:
Medical records of 730 patients who underwent RARC between April 2007 and May 2019 in 11 tertiary referral centers were retrospectively reviewed. We assessed recurrence-free survival (RFS), cancer-specific survival (CSS), and overall survival (OS) in the two groups using the Kaplan–Meier method. Cox regression models were used to identify factors associated with RFS, CSS, and OS.
Results:
Among 591 patients, neobladder diversion was performed more frequently in the ICUD group (70.8% vs 52.5%, p = 0.001). The median follow-up duration was shorter in the ICUD group than in the ECUD group (16 vs 26 months, p < 0.001). The rates of overall recurrence (36.5% vs 25.5%, p = 0.013) and pelvic recurrence (12.1% vs 5.9%, p = 0.031) were higher in the ECUD group. However, no differences in 5-year RFS (43.2% vs 58.4%, p = 0.516), CSS (79.3% vs 89.7%, p = 0.392), and OS (74.3% vs 81.4%, p = 0.411) were noted between the two groups. Multivariable analysis revealed that when compared to ICUD, ECUD was not associated with RFS (hazard ratio [HR], 0.982; p = 0.920), CSS (HR, 0.568; p = 0.126), and OS (HR, 0.642; p = 0.124).
Conclusion:
Although there was a difference in recurrence rate between the two groups, multivariable analysis indicated that the diversion technique after RARC did not affect the oncologic outcomes. Large prospective studies with long-term follow-up are warranted to verify the oncologic outcomes of ICUD and ECUD following RARC.
Introduction
Radical cystectomy with pelvic lymph node (LN) dissection and urinary diversion has become the standard treatment for both muscle-invasive bladder cancer and high-risk nonmuscle-invasive bladder cancer. 1,2 Open radical cystectomy (ORC) is considered an effective locoregional option for controlling high-risk bladder cancer. 3,4 Nonetheless, owing to the complexity of this surgical procedure, 13% to 67% of patients undergoing ORC have been reported to experience considerable perioperative and postoperative complications. 5,6 Robotic surgery has been introduced in an effort to decrease the complications and substantial morbidity of diverse surgeries. Previous studies reported that robot-assisted radical cystectomy (RARC) was associated with a reduction in estimated blood loss (EBL), risk of perioperative blood transfusion, and bowel complications. 7,8
During the early application of RARC, majority of surgeons preferred the hybrid approach of RARC with extracorporeal urinary diversion (ECUD) because intracorporeal urinary diversion (ICUD) has a steep learning curve and is a challenging technique, particularly orthotopic neobladder diversion. 9,10 Several surgeons have attempted to continuously refine and standardize the ICUD procedure because it is a completely minimally invasive technique and provides benefits such as a smaller incision, decreased pain, and reduced risk of fluid. The feasibility of RARC with intracorporeal ileal conduit has been shown relatively earlier. 11,12 Furthermore, several intracorporeal neobladder techniques with promising outcomes have recently been introduced. 13,14 Consequently, the proportion of ICUD performed has dramatically increased in the last years. 15
Diverse studies have compared the oncologic outcomes of ORC and RARC and reported the absence of significant difference between these two radical cystectomy approaches. 9,16,17 However, few studies have compared the oncologic outcomes of ICUD and ECUD. 15 During the ICUD procedure after RARC, the specimens are placed into an impermeable retrieval bag, which is left in the abdominal cavity until the operation is completed. 18,19 Leaving the pouch containing the specimens in the abdominal cavity for a long period of time increases the probability of tumor seeding, and this may serve as a reason to compare the oncologic outcomes of ICUD and ECUD. Hence, this multi-institutional study aimed to compare the oncologic outcomes of ICUD and ECUD following RARC in patients diagnosed with bladder cancer.
Patients and Methods
Medical records of 730 patients who underwent RARC between April 2007 and May 2019 in 11 tertiary referral centers were retrospectively reviewed; for these patients, RARC was performed by 21 surgeons included in the Korean Robot-Assisted Radical Cystectomy (KORARC) Study Group. The KORARC database is a planned web-based electronic database originating from the Korean Society of Endourology and Robotics (KSER). After generating this database in 2019, a single dedicated database manager retrospectively collected the data of 730 patients. Since then, the database was maintained prospectively.
This study was conducted under internationally accepted ethical standards after relevant ethical review. After receiving approval from the Institutional Review Board (2019AN0102), all analyses were performed following the tenets of the Declaration of Helsinki. The requirement for acquisition of informed consent was waived owing to the retrospective nature of the study.
Patients with distant metastasis, missing data, and short-term follow-up duration as well as those who underwent RARC only without urinary diversion due to end-stage renal disease were excluded. We analyzed the following data: age, sex, body mass index, American Society of Anesthesiologists (ASA) score, smoking history, previous history of abdominal surgery and radiation, clinical stage, neoadjuvant chemotherapy, operative time EBL, type of urinary diversion, pathologic T stage, LN invasion, and surgical margin. The indications for ICUD after RARC were different for each urologist. In general, the decision was made according to the patient's characteristics such as age, surgical and radiation history, and the stage before surgery, but there is no absolute standard, and the criteria also vary from surgeon to surgeon. Likewise, intracorporeal neobladder was performed in various methods according to the preference of the surgeons such as U-shape, Studer, or modified Hautmann. Figure 1 shows the surgical procedure of the U-shape orthotopic neobladder.

Surgical procedure of U-shape neobladder.
Patients' characteristics were compared between the two groups using the Mann–Whitney U-test for continuous data and the chi-squared test for dichotomous variables. Categorical variables are presented as frequency and percentages, whereas continuous variables are expressed as medians and interquartile range. Kaplan–Meier curves and the log-rank test were used to depict and compare recurrence-free survival (RFS), cancer-specific survival (CSS), and overall survival (OS) between the two groups. Multivariable Cox regression models were constructed to determine the variables associated with RFS, DSS, and OS. All tests were two-sided, with statistical significance considered at p < 0.05. All statistical analyses were performed using STATA® version 15.1 (StataCorp, LLC, College Station, TX).
Results
Table 1 shows the patients' clinical, perioperative, and pathologic characteristics. Of 591 patients, 153 (25.9%) underwent ICUD. The ICUD group had fewer patients with an ASA score of ≥2 (54.9% vs 75.6%, p < 0.001) as well as fewer current or former smokers (41.8% vs 51.8%, p = 0.033) than the ECUD group. Patients treated with ICUD had a longer operative time (495 vs 410 minutes, p < 0.001); however, no significant difference in EBL was observed (480 vs 410 mL, p = 0.252). Orthotopic neobladder diversion was performed more frequently in the ICUD group (70.8% vs 52.5%, p = 0.001). The two groups had comparable ≥pT3 disease rate (32.7% vs 37.9%, p = 0.284), urothelial carcinoma rate (95.4% vs 96.1%, p = 0.845), and regional LN invasion rate (19.0% vs 21.0%, p = 0.104); nevertheless, the ICUD group had a higher positive surgical margin rate (5.9% vs 2.1%, p = 0.027). The follow-up duration was much longer in the ECUD group (26 vs 16 months, p < 0.001).
Clinical Characteristics and Pathologic Results of Patients Who Underwent Robot-Assisted Radical Cystectomy
ASA = American Society of Anesthesiologists; BMI = body mass index; ECUD = extracorporeal urinary diversion; ICUD = intracorporeal urinary diversion; IQR = interquartile range; LN = lymph node; PLND = pelvic lymph node dissection.
At a median follow-up of 23 months, recurrence occurred in 199 patients and 79 patients died (47 due to disease). Patients in the ECUD group more frequently experienced recurrence (36.5% vs 25.5%, p < 0.013) than those in the ICUD group. In addition, patients in the ECUD group exhibited a trend toward higher rates of neobladder or conduit recurrence (5.0% vs 2.6%, p = 0.211), urinary tract recurrence (3.2% vs 2.0%, p = 0.579), and distant recurrence (23.1% vs 17.0%, p = 0.116); however, the difference was not statistically significant. Pelvic recurrence was observed more frequently in the ECUD group than in the ICUD group (12.1% vs 5.9%, p = 0.031) (Table 2).
Site of Disease Recurrence After Robot-Assisted Radical Cystectomy
Although the rate of overall disease recurrence was higher in the ECUD group, no difference in 5-year RFS was noted between the ICUD and ECUD groups (43.2% vs 58.4%, p = 0.516) (Fig. 2A). Furthermore, the two groups had comparable 5-year CSS (79.3% vs 89.7%, p = 0.392) (Fig. 2B) and OS (74.3% vs 81.4%, p = 0.411) (Fig. 2C).
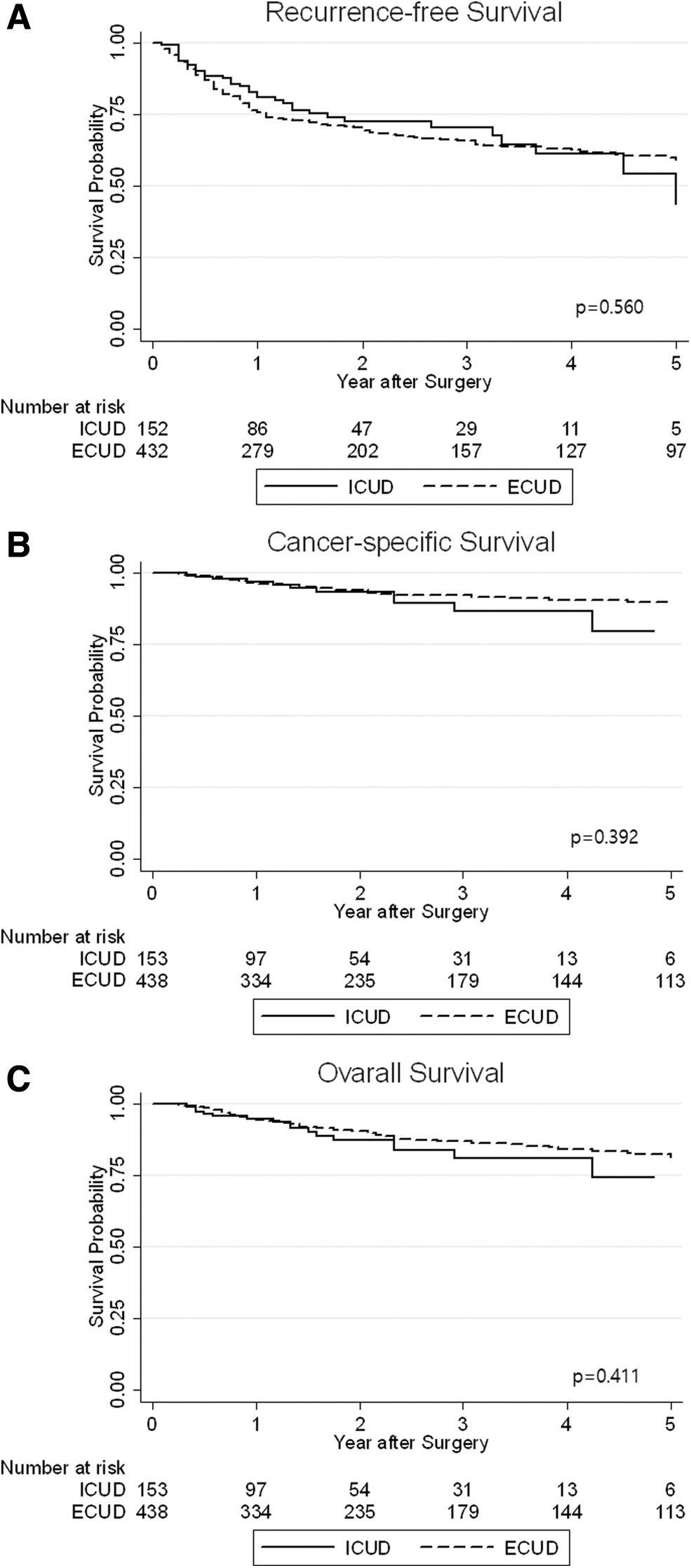
Kaplan–Meier curves for recurrence-free survival
Multivariable Cox regression analysis revealed that higher pathologic T stage (hazard ratio [HR], 2.438; 95% confidence interval [CI], 1.704–3.488; p < 0.001), and LN invasion (HR, 2.741; 95% CI, 1.998–3.760; p < 0.001) were related to RFS (Table 3). Both higher pathologic T stage (HR, 4.258; 95% CI, 1.742–9.404; p < 0.001) and LN invasion (HR, 3.865; 95% CI, 2.077–7.193; p < 0.001) were also associated with worse CSS. In the context of OS, old age (HR, 1.024; 95% CI, 1.002–1.047; p = 0.030), higher pathologic T stage (HR, 2.941; 95% CI, 1.625–5.323; p < 0.001), and LN invasion (HR, 2.874; 95% CI, 1.766–4.679; p < 0.001) were correlated with worse OS. However, ECUD was not a prognostic factor for RFS (HR, 0.982; 95% CI, 0.681–1.415; p = 0.920), CSS (HR, 0.568; 95% CI, 0.276–1.172; p = 0.126), and OS (HR, 0.642; 95% CI, 0.364–1.130; p = 0.124).
Multivariable Analyses of Factors Associated with Recurrence-Free Survival, Cancer-Specific Survival, and Overall Survival
CI = confidence interval; HR = hazard ratio.
Discussion
Robotic surgery has been proposed to meet the expectations for a minimally invasive surgery and improve perioperative outcomes without compromising oncologic outcomes. This procedure has been actively applied to urologic surgery and has become the most widely used surgical approach, especially in radical prostatectomy. 20,21 RARC has also been introduced in an effort to reduce the perioperative complications of ORC. Actually, several studies reported that RARC was associated with favorable perioperative outcomes when compared to ORC. 7 In addition, recent studies have shown that the oncologic outcomes and recurrent pattern of RARC were similar to those of ORC. 9 From this point of view, RARC is a technique suitable for the purpose of robotic surgery.
Although ICUD is a challenging and time-consuming procedure, expertise and continuous refinement of the technique have led to an increase in the proportion of ICUD performed. 15,22 Results of recent studies from the International Robotic Cystectomy Consortium (IRCC) have indicated that the proportion of ICUD performed has dramatically increased from 9% in 2005 to 97% in 2016 from their cohorts. They also reported that patients who underwent ICUD had shorter operative time (357 vs 400 minutes, p < 0.001) and less blood loss (300 vs 350 mL, p < 0.001) than those treated with ECUD. 15 However, our study showed different results. While there was no difference in EBL between the two groups (480 vs 410 mL, p = 0.252), the operative time was much longer in the ICUD group (495 vs 410 minutes, p < 0.001). The reason for such difference in operative time is the difference in urinary diversion type. Intracorporeal neobladder diversion has a steep learning curve and is an extremely challenging procedure, thus requiring a longer time to complete than ileal conduit diversion. In the IRCC group, the majority of urinary diversions was ileal conduit, and they reported that ileal conduit was a significant predictor of ICUD being performed. Of patients from the IRCC, 21% and 23% were received neobladder diversion in ICUD and ECUD, respectively. However, continent urinary diversion was performed more frequently (57.2%) by our study group, and the proportion of patients treated with neobladder diversion was higher in the ICUD group than in the ECUD group. This difference would have made the operative time of ICUD longer.
In the context of oncologic outcomes, prior studies on ORC reported an overall recurrence rate of 30% to 43%. 4,23 There have been concerns about the increased risk of recurrence because pneumoperitoneum might contribute to tumor dissemination via fluctuations in pressure, inhibition of the immune response due to CO2, or surgical technique causing tumor spillage from the bladder. 24,25 However, many studies showed that there was no significant difference in the recurrence rate between ORC and RARC. Nguyen and colleagues 16 reported an overall recurrence rate of 42% for the ORC group and 36% for the RARC group, although the difference was insignificant. They also reported that there was no large difference in local recurrence rates within 2 years between ORC and RARC (23% vs 18%). Furthermore, a randomized clinical trial obtained similar results. Bochner and coworkers 9 reported an overall recurrence rate of 33.3% for the RARC group and 43.1% for the ORC group, and the difference in local recurrence rates did not meet conventional levels of significance.
In performing ICUD after RARC, compared to ECUD, there is a problem to consider that may be related to oncologic outcomes, especially local recurrence or intra-abdominal recurrence. After bladder extraction is completed, the specimens contained in an impermeable retrieval bag from RARC and pelvic LN dissection is taken out just before performing ECUD. However, during the ICUD procedure, the specimens are placed into a retrieval bag, which is positioned in the upper abdominal cavity for a long period of time. 18,19 Because it is difficult to completely tighten the opening of the bag, there exists the possibility that the contents of the bag may come out due to fluctuations in pressure or other causes. Therefore, if the bag is left in the abdominal cavity for a long time, the possibility of tumor spillage may increase.
Studies comparing the oncologic outcomes between ICUD and ECUD are rare. Previous studies from the IRCC reported an overall recurrence rate of 19% and showed that the ICUD group had a lower recurrence rate than the ECUD group. 15 However, there was no significant difference in the local recurrence rate between the two groups. In recent studies that compared the perioperative outcomes of ICUD and ECUD using propensity score-matched analysis, overall recurrence, local recurrence, and distant recurrence were similar between the two approaches of urinary diversion. 22
In our study, 33.6% of patients experienced disease recurrence, which is similar to the rate reported by prior studies on ORC. The overall recurrence rate was higher with ECUD than with ICUD. In addition, in our study, patients in the ECUD group exhibited a trend toward slightly higher rates of neobladder or conduit recurrence, urinary tract recurrence, and distant recurrence; abdominal recurrence was observed more frequently in the ICUD group. However, these results were not statistically significant. Only the pelvic recurrence rate was significantly higher in the ECUD group, unlike in previous studies. The most important reason for this result seems to be the difference in follow-up duration between the two groups. The median follow-up duration was much longer in the ECUD group than in the ICUD group (26 vs 16 months, p < 0.001). If the follow-up duration in the ICUD group was as long as that in the ECUD group, it is possible that the recurrence rate in the ICUD group might not differ from that in the ECUD group. This result suggests that tumor spillage might not be a concerning problem during ICUD. In fact, it has been reported that preexisting micrometastatic tumor clones play a greater role in local recurrence than tumor spillage during RARC with intracorporeal ileal conduit. 26
Although a difference in recurrence rate was observed, the Kaplan–Meier curves indicated that there was no difference in 5-year RFS between the two groups. The 5-year CSS and OS of the ICUD group were also similar to those of the ECUD group. Previous studies obtained slightly different results. Hussein and colleagues 15 reported that the two groups showed similar RFS and CSS. However, OS at 1, 3, and 5 years was worse in the ICUD group than in the ECUD group. They explained that this result was attributable to a higher complication rate associated with ICUD, especially early in the ICUD experience. Furthermore, they showed that corporeal type was not a predictor of RFS, CSS, and OS in the multivariable Cox regression analysis. In that study, cystectomy era, pT stage, and pN stage were associated with RFS, whereas LN yield, surgical margin, pT stage, and pN stage were related to CSS. The predictors of OS were body mass index, high-grade complications, ASA score, diversion type, surgical margin status, pT stage, and pN stage. Our study showed that higher pathologic T stage and LN invasion were significant predictors of RFS and CSS. Along with these two parameters, older age was associated with worse OS in the multivariable Cox regression analysis. However, corporeal type was not associated with RFS, CSS, and OS.
Our study has some limitations inherent to a retrospective analysis. We were unable to control patient and disease status, including the ASA score, smoking status, diversion type, and surgical margin. In addition, this study includes many of the early experiences of RARC, and it is expected that this will be included in the ECUD group. This fact is also likely to confuse the results. There is also a drawback of this study derived from being a multicenter study. It is difficult to equally apply various variables such as surgical procedure, follow-up protocol, and pathology reporting. The number of patients included in our study is relatively small when compared to that in previous studies. In addition, there was a lack of information about the purpose of surgery (i.e., curative, salvage, or palliative) and adjuvant chemotherapy. Another factor that may bias the results is that ICUD has not been performed by some urologists. Considering that the surgeon who has performed ICUD even once tends to do it more than ECUD, it seems that one of the important factors in doing ICUD is the operator's experience. Finally, the short follow-up duration with significant difference in follow-up duration between the ICUD and ECUD groups is the main drawback.
Conclusion
Our analysis showed that the overall and local recurrence rates were higher in the ECUD group than in the ICUD group; however, this might be due to the long follow-up duration. Multivariable analysis indicated that the diversion technique after RARC did not affect the oncologic outcomes. Large prospective studies with long-term follow-up are warranted to verify the oncologic outcomes of ICUD and ECUD following RARC.
Footnotes
Author Disclosure Statement
The authors declared that there was no competing of interest.
Funding Information
This research was supported by a Korean Society of Endourology and Robotics (KSER) Grant.