
Abstract
Introduction:
With an increase in the prevalence of kidney stone disease (KSD), there has been a universal drive to develop reliable and user-friendly tools such as grading systems and predictive nomograms. An atlas of scoring systems (SS), grading tools, and nomograms in Endourology is provided in this article.
Methods:
A comprehensive search of world literature was performed to identify nomograms, grading systems, and classification tools in endourology related to KSD. Each of these was reviewed by the authors and has been evaluated in a narrative format with details on those that are externally validated and their respective citation count on google scholar.
Results:
A total of 54 endourological tools have been described in our atlas of endourological SS, grading tools, and nomograms. Of the tools, 23 (43%) have been published in the past 3 years showing an increasing interest in this area. This includes five for percutaneous nephrolithotomy, six for flexible ureteroscopy, three for semi-rigid ureteroscopy (URS), nine for extracorporeal shockwave lithotripsy, two for stent encrustations, three for intraoperative appearance at the time of URS, and three to classify intraoperative ureteric injury. There were three tools for renal colic assessment, one each for prediction of future stone event, stone classification, and stone impaction and two for need of emergency intervention in ureteral stone. Two tools are related to stone recurrence, whereas six are related to postprocedural complications. There are now two tools for simulation in endourology and five for patient-reported outcome measures.
Conclusions:
A number of reliable and established tools currently exist in endourology. Each of these offers their own respective advantages and disadvantages. Although nomograms and SS can help in the decision making, these must be tailored to individual patients based on their specific clinical scenarios, expectations, and informed consent.
Introduction
In recent years, there has been a rise in the prevalence of kidney stone disease (KSD) as well as an expansion in the range of endourological interventions available. 1,2 Alongside modifications and advancements in equipment, for example, laser, digital systems, and miniaturization, there has been a universal drive to develop reliable and user-friendly tools such as grading systems and predictive nomograms. 3 –5 These can allow for more refined operative planning and improved procedural efficacy and safety. This befits better preoperative counseling and patient expectation and experience accordingly. It brings the clinician closer to providing a tailored approach as well as better resource allocation in a financially restricted environment.
Instruments such as the R.E.N.A.L. nephrometry scoring system (SS), which provides standardized reporting of renal tumor size, location, and depth, serve as an example of such a validated tool, and has achieved widespread dissemination. 4 Within the subspecialty of endourology, there has been a plethora of new instruments that have been recently developed and are now available at the clinician's disposal. At the same time, review and awareness of these tools remains underreported. To date, there exists no reference that provides a summary of these in one document. This article serves to provide the clinician with such a resource. An atlas of SS, grading tools, and nomograms in Endourology is provided in this article.
Methods
A comprehensive search of world literature was performed to identify nomograms, grading systems, and classification tools in endourology related to KSD. Each of these was reviewed by all the authors and has been evaluated in a narrative format. A selection of the key instruments is outlined next. All the identified tools are listed in Table 1. Table 2 provides further information on those tools, which have been externally validated.
All Endourological Scoring Systems, Grading Tools, and Nomograms Included in the Paper
In English Language.
ARC = acute renal colic; CReSP = Cambridge Renal Stone PROM; CROES = Clinical Research Office of the Endourologic Society; CUSP = Cambridge Ureteral Stone PROM; DACA-KS = diagnostic acute care algorithm–kidney stones; ED = emergency department; FECal = forgotten, encrusted, calcified; fURS = flexible ureteroscopy; GAUES = Global assessment tool for endourological skills; GSS = Guy's Stone Score; HFMEA = healthcare failure mode effects analysis; IPA = infundibulopelvic angle; ISF = impacted stone formula; KSD = kidney stone disease; KUB = kidney, ureter, and bladder radiograph; PCNL = percutaneous nephrolithotomy; PPLA = plugging, pitting, loss of contour, and amount of Randall's plaque; PROMS = patient-reported outcome measures; PULS = postureteroscopic lesion scale; QoL = quality of life; RIRS = retrograde intra-renal surgery; ROKS = recurrence of kidney stone; RUSS = Resorlu-Unsal stone score; SFR = stone-free rate; S-ReSC = Seoul National University renal stone complexity; STEP = Stone Episode Prediction; STONE = stone size, tract length, obstruction, number of involved calices, and essence/stone density; SWL = extracorporeal shockwave lithotripsy; TOHO = tallness, occupied lesion, hounsfield units; Triple D = density, distance, diameter; UAS = ureteral access sheath; URS = ureteroscopy; USIQoL = urinary stones and intervention quality of life; USSQ = ureteral stent symptom questionnaire; WISQoL = Wisconsin stone quality of life questionnaire.
Externally Validated Tools with Citation Count
According to Google Scholar (as of January 18, 2021).
Results
A total of 54 endourological tools have been described in our atlas of endourological SS, grading tools, and nomograms (Fig. 1). Of the tools, 23 (43%) have been published in the past 3 years, showing an increasing interest in this area. This includes five for percutaneous nephrolithotomy (PCNL), six for flexible ureteroscopy (fURS), three for semi-rigid URS, nine for extracorporeal shockwave lithotripsy (SWL), two for stent encrustations, three for intraoperative appearance at the time of URS, and three to classify intraoperative ureteric injury. There were three tools for renal colic assessment, one each for prediction of future stone event, stone classification, and stone impaction, and two for need of emergency intervention in ureteral stone. Two tools are related to stone recurrence, whereas six are related to postprocedural complications. There are now two tools for simulation in endourology and five for patient-reported outcome measures (PROMS).
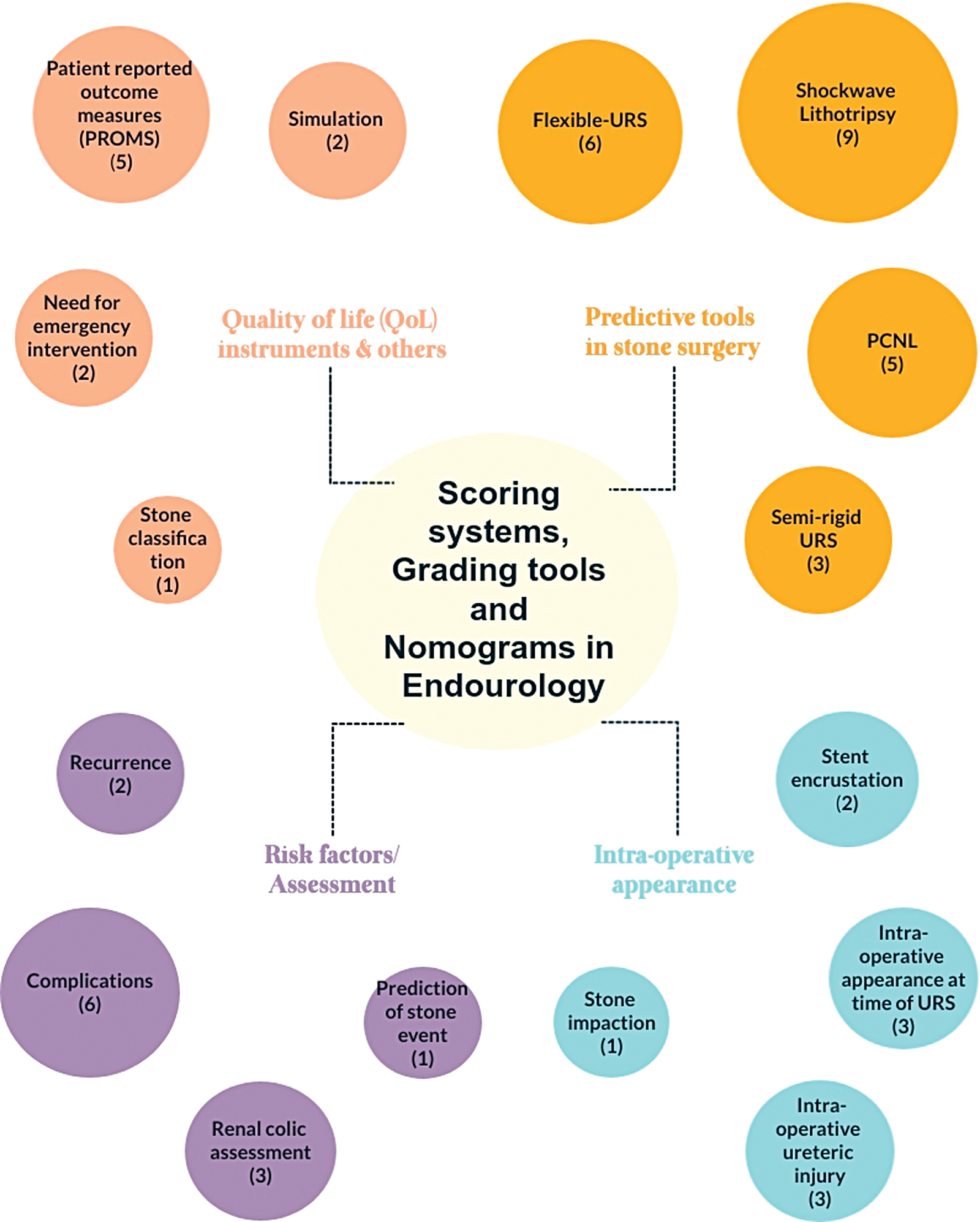
Infographics of all included studies. Color images are available online.
Discussion
Predictive tools in stone surgery
Percutaneous nephrolithotomy
There are multiple quantitative SS in use for PCNL that have been externally validated. Four main tools of this kind exist, which are the most commonly used in clinical practice as well as in the research setting. 5 –8 The principal goal of this particular tool is prediction of outcomes after PCNL.
Guys Stone Score
Developed in 2011, this was the first of its kind for use in PCNL. 5 The need for such a tool was triggered at the time of national audit of PCNL in the United Kingdom, where it became evident that stratifying procedural complexity was difficult. The initial form comprised five grades, but the final version consolidated this to four. It was devised based on expert opinion and published reports. At the time of conception, it was based on CT, plain X-ray, or intravenous urography. The two key parameters are stone location and renal anatomy. 9 The assessment incorporates all stones identified at imaging and, therefore, not just the stone targeted for treatment. Reproducibility was determined through evaluation of preoperative images of 40 cases by a panel of 3 clinicians. Internal validation was then carried out over 100 consecutive cases at their tertiary referral center.
STONE nephrolithometry score
This SS is based on the five variables that give its name: stone size (S), tract length (T), obstruction (O), number of involved calices (N), and essence or stone density (E). 6 The assessment is made based on noncontrast CT imaging. Each variable is graded and allocated a score. The total score can range from 5 to 13. The latter indicates the most complex scenario. It was devised based on a literature review of outcome variables affecting PCNL and then tested on a cohort of 117 adult patients. The overall accuracy of this SS to predict stone-free rate (SFR) was 83.1% at the time of its conception.
Clinical Research Office of the Endourologic Society nephrolithometric nomogram
This was developed by using data from the Clinical Research Office of the Endourologic Society (CROES) prospective patient registry from 97 centers globally. 7 A total of 2806 patients were included in the multiple logistic regression analysis, and exclusions had been made where patients were <14 years of age, in centers performing <10 PCNL cases per annum, and where plain X Ray had not been used to evaluate treatment success. It has been externally validated by a number of studies confirming the suitability of applying CT scans.
Seoul National University renal stone complexity
This tool is quite different in that the system is wholly based on the complexity of stone distribution. 8 In this respect, it is unique because it does not evaluate parameters such as size and number of stones. It is also, therefore, arguably the simplest tool. The authors determined this was the most important outcome to determine PCNL outcomes and derived a schematic diagram of nine areas that the stone can occupy, and a point given for each area. A cumulative score is calculated by the user out of a maximum score of 9. Of note, this system was designed for single-tract PCNL. Patients can be then categorized into three groups based on complexity: low (1 and 2), medium (3 and 4), and high (≥5). The risk of complications was 18.7%, 28.6%, and 34.2% for low, medium, and high Seoul National University renal stone complexity (S-ReSC) score groups, respectively. The SFRs were 96.0%, 69.0%, and 28.9% in these groups. A modified version has been successfully designed for application in URS and has since also been externally validated. 10
Ureteroscopy
Resorlu-Unsal stone score
Developed in 2012, it was the first tool specifically designed for prediction of SFR after URS. 11 It was achieved after a retrospective evaluation of 207 cases at their institution. Variables that were significantly associated with SFR were stone size, stone composition, number of stones, lower infundibulopelvic angle (IPA), and anatomical abnormalities, for example, horseshoe kidney. These were all incorporated into the SS with the exception of stone composition, as this is not known preoperatively. The clinician scores the case based on each of these four variables. It is a simple system, as each variable is either scored zero or one based on a yes or no answer. Scoring points are given for abnormal anatomy, IPA <45°, stone positioned in more than one calix, and if the stone size is >2 cm. Additional points can also be given in this variable. One extra point can be given for every centimeter in size where the stone is larger than 2 cm. There was a significant correlation between final RUS score and final SFR. For example, SFR was 84.4% and 27.2% for RUS score 1 and ≥3, respectively.
Ito's score
In 2015, Ito and colleagues developed a tool for fURS based on five independent predictors for the stone-free status that they identified. 12 These were stone volume (SV), lower pole calculi, hydronephrosis, stone number, and operator experience (>50 fURS). In contrast to other SS, a higher score correlates with high treatment success where the maximum possible score is 25.
Shockwave lithotripsy
Triple D score
Tran and colleagues carried out a retrospective analysis of 235 patients undergoing SWL and used this evaluation to create a CT-based, 3-metric system, incorporating stone density in HU, ellipsoid SV, and skin-to-stone distance. 13 Cutoff values for each of these parameters were generated from receiver operator characteristic curves. If a stone under evaluation has a value less than the cutoff for one of the parameters, they are given a score of 1. The Triple D scores of 0, 1, 2, and 3 are consistent with successful stone clearance rates of 21.4%, 41.3%, 78.7%, and 96.1%, respectively. An advantage is that it can be calculated by the radiologist even at time of reporting, which could provide early assistance in clinical decision making.
S3HoCKwave score system
This new tool is the result of a multi-center retrospective cohort study carried out over a 10-year period. 14 Analysis of 2271 patients allowed for eventual creation of a clinical prediction model based on six variables. These are sex, skin-to-stone distance, size, HU, colic, and location (kidney or ureter). This tool primarily addresses the risk of SWL failure. This was the primary outcome of interest for this study and was defined as a lack of stone clearance after three SWL sessions. It has yet to be externally validated.
Stent encrustation
Stents represent an integral tool in the endourologist's toolkit, and the global market is estimated to exceed $560 million by 2025. 15 Despite advances related to design since first described in a urological setting in 1967, adverse effects related to them include pain, infection, and stent encrustation. 16 Kawahara and colleagues, reported stent encrustation to occur to some extent in up to 47% of cases, and length of indwelling time is regarded as the greatest risk factor for encrustation. 17 Careful surgical planning is required to achieve clearance and minimize morbidity. Two validated tools now exist to assist the clinician in achieving this.
Forgotten, encrusted, calcified Double-J ureteral stents
The authors devised a five-level grading system based on stone size, location, and degree of encrustation. 18 Grade 1 refers to minimal encrustation at one of the stent's coils, grade 2 encrustation completely encompasses one of the stent coils, grade 3 involves complete encrustation of one of the coils as well as the linear portion of the stent along the course of the ureter, grade 4 refers to complete encrustation of coils at both ends of the stent, and grade 5 involves diffuse encrustation affecting the entirety of the stent. Each grade of encrustation is accompanied by a pictorial schematic to show clinicians the morphology to expect. It was developed by using a retrospective analysis of cases presenting with this clinical problem between 2000 and 2007. It is accompanied by a useful algorithm to help guide potential management based on imaging gained with the CT stone protocol. This allows for recommendation for a single or multimodality treatment. It has already achieved widespread dissemination owing to its ease of application and novelty in addressing a challenging scenario. However, it was established on a review of only nine patients, which is acknowledged as a limitation.
Kidney, ureter, and bladder radiograph system
This tool holds an overlap with forgotten, encrusted, calcified (FECal); however, it was designed more with the aim of aiding the clinician determine the nature of patients with stent encrustation that may require multimodal surgery, multiple surgeries, and a prolonged operative time. 19 A retrospective review of 110 cases was carried out to find associations with these variables as well as SFR. The final system created gives a separate score for each third of the stent affected by encrustation: proximal coil in the kidney (K), portion of the stent in the ureter (U), and distal coil in the bladder (B). Each portion is attributed a score (1–5) based on the degree of calcification present. These can be summated to provide an overall score (3–15). The authors were able to correlate scores to likelihood of different operative outcomes. For example, K score ≥3 was determined to be matched to longer operative time (>180 minutes), need for multi-modal surgery, and poorer stone-free status. This study was only devised based on retrospective observations of a single surgeon, and, therefore, inter-rater reliability was not measured at time.
Renal papillary appearance
Plugging, pitting, loss of contour, and amount of Randall's plaques
This novel grading scale was developed to aid surgeons in describing the appearance of renal papilla at the time of endoscopy. 20 This research was borne out of the finding that at a histological level, different stone-forming pathologies render varying papillary morphologies, for example, calcium oxalate stones do not result in intratubular crystals or interstitial fibrosis. Further, a macroscopic view of papilla at time of surgery can also be indicative of stone type. For example, calcium phosphate stones result in greater flattening and erosion of papilla compared with idiopathic calcium stone formers. 21
It contains four domains and includes: plugging, pitting, loss of contour, and amount of Randall's plaque (mild, moderate or severe). Assessment can be made once an overlying stone has been cleared. A completely healthy appearance receives a final score of 0(a) in contrast to the most diseased appearance, which is given the maximum score of 6(a). Each renal papilla is given a separate score and at the end of the procedure a mean score can be calculated. This was developed in a cohort of 342 patients who had been prospectively enrolled in the project and had undergone digital video mapping at the time of surgery. This tool was made possible as a result of the high-definition scopes, which are available nowadays. This is the first study of its kind to create a standardized assessment method for this purpose.
Endoscopic description of renal papillary abnormalities in stone disease by fURS
Almeras et al. developed a tool to describe and classify papillary abnormalities seen at fURS. 22 Findings were formulated by using 164 sequential cases. The result is a system, inspired by the oncological TNM classification, which allows the surgeon to outline findings according to a stone description (Sx), for example, anchored, subepithelial, or intraductal, the number of abnormal papilla (n), and description of its abnormality (Px), for example, tip erosion or extrophic papilla and the amount of Randall's plaque (Rx). The authors also generated a simple algorithm, which groups the most important abnormalities. After systematic use, the authors gave an update in 2020, which provides improvements to address previous limitations such as for mixed stones. 23
Intraoperative ureteric injury (iatrogenic)
Postureteroscopic lesion scale
This tool was developed in 2012 with the principle aim of creating a way for surgeons to intraoperatively grade injury due to URS to determine whether a Double-J stent should be inserted at the end of the procedure and establish standardized recommendations accordingly. 24 The authors highlighted ambiguity in the definition of studies referring to URS as “complicated” or “uncomplicated.” The only existing tool prior to this was the generic American Association for the Surgery of Trauma (AAST) classification of ureteric injuries, which holds limited value in its application for endourological scenarios. 25 The Clavien-Dindo classification also exists, but this is intended for use postoperatively. 26 This new tool was developed through use on 435 patients before evaluation on a further 112 patients to confirm inter-rater reliability. The result is a 0 to 5 level grading system, which is assessed by the surgeon at the time of the final endoscopic passage in the ureter. Postureteroscopic lesion scale (PULS) grade 0 indicates no lesions and therefore an uncomplicated URS, which does not warrant stent insertion. Grade 5 refers to a complete transection with formal reconstruction indicated. Grade 1 to 4 ranges from a superficial mucosal lesion only to a >50% partial transection, which required stent insertion. The authors then provide recommendations for duration of stent insertion. This ranged from 2 days for a grade 1 injury to 6 to 8 weeks for a grade 4 injury.
Although the follow-up period in this study was <1 year only, in 2014 the authors published findings from a multi-center international study, which further supported the high inter-rater reliability (Kendall's W = 0.69, p < 0.001) among urologists. 27 This involved participant viewing video sequences from the final endoscopic passage of URS procedures in 100 cases and grading them accordingly.
Injury secondary to ureteral access sheath
Although the PULS grading system has been validated for use in the assessment of ureteral access sheath (UAS) injuries as well, Traxer and Thomas designed a tool specifically for this purpose rather than after a generic URS. 28 Again, limitations of the AAST scale were cited as the key reasons for the clinical need for such a tool. Advantages related to UAS are numerous and include facilitation of access of the collecting system, lowering intra-renal pressures, and scope protection. 28 However, ureteric injuries can occur and systematic evaluation of ureteral integrity at the end of the procedure is therefore of paramount importance. This classification system was made through an iterative process carried out prospectively over 359 consecutive patients. A five-level grading system (0–4) was the end result. Overall, 46.5% of the study group was identified to have had some degree of ureteric injury. Grade 0 refers to no identifiable lesion, and grade 4 corresponds with total avulsion. High-grade injuries (≥2) were recommended by the authors to have a ureteral stent left in for 3 to 6 weeks followed by ultrasound follow-up 1 to 3 months after stent removal.
KSD recurrence
Up to 50% of patients with KSD are estimated to experience recurrence within 10 years after their first episode. 1 Any means of identifying patients who will go on to experience a further symptomatic stone episode holds immeasurable value and offers the ability to tailor prevention measures accordingly.
Recurrence of kidney stone
The recurrence of kidney stone (ROKS) tool aimed at achieving this. 29 It was developed through the identification of first-time symptomatic stone formers in a longitudinal study based in Olmsted County, USA which had been led by the Rochester Epidemiology Project. Between 1984 and 2003, a total of 2239 patients had follow-up carried out until 2012. The end result is a tool including variables such as gender, race, visible hematuria, stone location, and nature of presentation. A revised version was developed in 2019 and was made by using a longer follow-up. 30 This model is applicable to patients with any previous episode(s) and not just after their first episode.
Renal colic assessment tools
Real-world studies have shown that more than 50% of patients with acute flank pain and suspected renal/ureteral stone who have a CT are found to have an alternative diagnosis. 31 Largely driven by need, therefore, of clinicians in the emergency department to help identify and triage those patients most in need of up-front CT imaging based on the likelihood of having a ureteral stone, nomograms have been developed to help this process.
STONE
This is the most well-known tool of its kind. 32 The nomenclature can be confusing, as it shares its name with one of the nomograms used to predict PCNL success. The name of this nomogram is not based on an acronym. Released in 2014, it was derived by using the medical records from ∼1000 patients who had been managed under the CT “renal colic pathway.” The advantage of such an objective SS is that it relies less on clinician experience during the triage process. The tool is based on five prognostic factors: gender, race, nausea/vomiting, timing of onset, and nonvisible hematuria. Patients are attributed a total score (0–13 point scale) and can be categorized into three groups of risk, which correlates with the probability of having a ureteral stone. In the internal validation phase, low (0–5), moderate (6–9), and high (10–13) correspond to 9.2%, 51.3%, and 88.6% risk, respectively. Two separate revisions to this STONE nomogram now exist.
The “modified STONE” nomogram was created in 2016 to improve the diagnostic performance. 33 The main adjustment is the replacement of nausea/vomiting and racial origin with C reactive protein and previous stone history, respectively. The other revision to this nomogram is called “STONE point of care limited ultrasonography,” which uses ultrasound imaging to check for hydronephrosis. 34 Interestingly, the authors of that study did not find the addition of hydronephrosis to increase the detection of ureteral stones in high-risk patients, but they put forward that it holds relevance and application in deciding the patients who require urgent surgical intervention.
Quality-of-life instruments
Another development within endourology over the past two decades has been the development of multiple PROMS to assess the impact on quality of life (QoL) as a result of KSD and treatment related to it. 35
Ureteral stent symptom questionnaire
In 2003, Joshi and colleagues developed this tool to assess symptoms and impact on QoL caused by ureteral stents. 36 With six domains covering urinary symptoms, body pain, general health, work performance, sexual matters, and any additional problems, it has become well used and now established in endourology. It is the most commonly used validated stent symptom questionnaire in the literature. 37
Wisconsin stone quality-of-life questionnaire
Penniston and Nakada established the first PROM specific for use in patients with KSD. 38 It has since achieved validation in many different languages worldwide. 39 It comprises 28 question items, which cover multiple domains, including fatigue, sleep disturbance, urinary symptoms, pain, employment, and emotional well-being. Although other QoL questionnaires have been applied in the setting of KSD, at present it serves as the only stone-specific tool for QoL that has achieved external validation.
Other resources and future directions
There exists a range of other tools in addition to those mentioned earlier (Table 1). The majority have been published recently and have therefore yet to gain recognition and external validation. Many have not achieved dissemination, and this is most likely through a lack of simple application. The latter is one explanation for why multiple nomograms appear to exist on the same topic. Another possible reason why there have been challenges in producing a universally agreeable tool is that they are constructed by using different patient populations and, therefore, the results are less generalizable to a worldwide population. For example, the ROKS tool was developed by using a predominantly Caucasian sample. On a similar note, one of the reasons for generation of the CHOKAI tool was to deliver a tool more specific for their patient population in Japan, in contrast to the STONE nomogram, which was made in the United States. The “ideal” nomogram should be easy to utilize in daily clinical practice and achieve reproducible results with minimal subjectivity or inter-observer variability. Newly published tools should be followed by external validation and head-to-head comparison with any previous similar tools, with standardized outcome measures. Findings from this review would suggest that the most widely disseminated tools use simple systems that do not rely on special software, for example, for radiomics, and where parameters can be easily obtained. For example, albumin-globulin ratio may not be readily available as a part of routine work-up. 40 Limiting the tool to only a few parameters is also likely to make it more user-friendly and promote its uptake. The maximum number of parameters in one study included was 25. 41
Currently, machine-learning software applications exist, which represent advancements in artificial intelligence (AI) within endourology. 42 Aminsharifi et al. reported validation of outputs from a software, which is an intelligible interface for predicting PCNL outcomes. 43 It is anticipated that such research will expand in the future. Development of a nomogram specific for miniaturized PCNL is still awaited. Given the expanded role of URS, for example, a nomogram, which could highlight chances of success through different interventions could be of great clinical use to aid decision making for stone cases. Similarly, a nomogram to give clinicians information regarding whether a case is better suited to miniaturized PCNL or standard PCNL would also be valuable. 44 Penniston and colleagues are currently developing a stone dietary assessment tool. 47 More recent advancements in endourology include simultaneous bilateral endoscopic surgery and endoscopic combined intra-renal surgery. 45,46 Nomograms for use within these surgeries is also eagerly anticipated, including to help predict patients most suited for these particular interventions. An ideal nomogram would take into account patient demographics and stone factors, cost, and equipment availability balanced with morbidity and outcomes. Perhaps, AI with big data should be able to help with this dilemma and make the predictive tools better.
Limitations
Although we have covered the most commonly used SS and nomograms in the article, there are others that are either relatively new or that have not been clinically used or externally validated; we have included them in Table 1. 39,40,47 –81 Of the included tools, 23 (43%) have been published in the past 3 years. We presume that the use of these helpful clinical tools is going to increase in the future. A limitation of many of the available nomograms in stone surgery is that they only provide predictions related to a limited number of outcomes such as stone clearance. They do not, therefore, necessarily aid the tailored intervention as much as one might hope. Future tools should also aim at guiding the surgeon on themes such as the context of URS, for example, whether a UAS or postoperative ureteral stent is recommended and the cost comparison of these interventions. 82,83 A further limitation of this review is the lack of appraisal beyond description of advantages and disadvantages. There are a number of studies that do this for a particular surgery, for example, for PCNL. 84 However, to our knowledge, this review is the first to provide an overview of all those available collectively. Although images could have been used for the explanation of SS, we would need copyright permission for individual studies, and this was beyond the scope of our review.
Conclusions
A number of reliable and established tools already exist in endourology. Each of these offers their own respective advantages and disadvantages. Although nomograms and SS can help in the decision making, these must be tailored to individual patients based on their specific clinical scenarios, expectations, and informed consent.
Footnotes
Acknowledgment
The authors acknowledge the Team of Worldwide Endourological Researchers (TOWER) Endourological society research group.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.