
Abstract
Abstract Objectives:
To compare the perioperative hemodynamic consequences and oncology outcomes of robotic retroperitoneal vs transperitoneal inferior vena cava (IVC) thrombectomy (IVCT) for right renal cell carcinoma (RCC) with IVC tumor thrombus (IVCTT) that located below the first porta hepatis.
Patients and Methods:
Between January 2018 and June 2019, 35 patients of right RCC with IVCTT that located below the first porta hepatis underwent robotic retroperitoneal IVCT (16 patients) or transperitoneal IVCT (19 patients). We have described the procedures of transperitoneal IVCT earlier. The main procedure of robotic retroperitoneal IVCT include circumferential dissection of the IVC, sequentially clamping subhepatic IVC, the left renal vein and the caudal IVC with vessel loops, IVCT, IVC repair, and radical nephrectomy (RN). The following parameters were compared between the two groups: baselines characteristic, perioperative consequences, and hemodynamic changes.
Results:
Retroperitoneal and transperitoneal cohorts were comparable in terms of IVC thrombus length (3.2 vs 4.0 cm), IVC block time (18 vs 16 minutes, p = 0.64), postoperative hospital stay (6 vs 6 days, p = 0.67), postoperative complications (0 vs 0), and recurrence or metastasis rate (0 vs 0) for patients with similar baseline characteristic. The retroperitoneal cohort tended to less blood loss (160 vs 240 mL, p = 0.024), shorter operative time (130 vs 145 minutes, p = 0.003), lower central venous pressure (p < 0.05), and smaller diameter of IVC (p < 0.05).
Conclusions:
Robotic retroperitoneal RN and IVCT is feasible for patients of right RCC with IVCTT located below the first porta hepatis and is superior to transperitoneal IVCT in terms of bleeding control and operation time for skilled surgeons.
Introduction
Radical nephrectomy (RN) combined with inferior vena cava (IVC) thrombectomy (IVCT), representing the only potential curative treatment for patients of renal cell carcinoma (RCC) with IVC tumor thrombus (IVCTT), is a challenging surgery in urologic oncology. 1,2 Laparoscopic or robotic transperitoneal RN combined with IVCT is a common surgery for level I–II tumor thrombus, 1,3 –8 and there have also been some reports that discussed the safety and feasibility of this surgery for level III–IV IVCTT. 9 –12 Reconstructive kidney surgery and pyeloplasty can be performed feasibly using the robotic retroperitoneal technique, 13,14 which combines the advantages of robotic surgeries and the retroperitoneal approach, thus allowing for a more precise operation and reducing the risk of irritation to the bowel and less blood loss. 15 Moreover, hemodynamic consequences for transperitoneal and retroperitoneal laparoscopic surgeries are different. 16 –18 However, research on robotic retroperitoneal IVCT is limited, and there are no studies comparing the treatment outcomes and hemodynamic changes between the robotic retroperitoneal and transperitoneal IVCT for level I–II IVCTT.
Therefore, we aimed to compare the perioperative outcomes and hemodynamic consequences between robotic retroperitoneal and transperitoneal IVCT for patients with right RCC and level I–II IVCTT.
Patients and Methods
Participants and study design
A retrospective serial case–control study was performed. From January 2018 to June 2019, 35 patients with right RCC and level I–II IVCTT underwent robotic IVCT by three experienced surgeons at our institution. Sixteen of them underwent robotic retroperitoneal IVCT, and their treatment outcomes and perioperative hemodynamic consequences were compared with those of remaining 19 patients who underwent robotic transperitoneal IVCT. This study was approved by the medical ethics committee of our hospital.
We retrospectively reviewed and analyzed the baseline characteristics (including age, gender, body mass index [BMI], tumor size, IVC thrombus length and classification, and neoadjuvant therapy) (Table 1), perioperative data (including operative time, estimated blood loss, IVC blocking time, postoperative hospital stay, perioperative complications, pre- and postoperative serum creatinine levels) and follow-up data (Table 2) of the two groups. We also recorded and analyzed perioperative hemodynamic changes of eight patients in both groups.
Baseline Characteristics of Two Groups
BMI = body mass index; IQR = interquartile range; IVC = inferior vena cava; RCC = renal cell carcinoma.
Perioperative and Follow-up Data of Two Groups
Cr = creatinine; EBL = estimate blood loss.
Surgical techniques and data collection
Robotic transperitoneal IVCT
The surgical techniques of robotic transperitoneal IVCT were the same as those reported in our previous study on a robotic technique for level I–II IVCT for RCC. 6 A 12-mm port for the camera was placed ∼2–3 cm to the upper right of the umbilicus. Three 8-mm ports were placed at ∼3 cm medial to the right midclavicular line under the costal margin, ∼3 cm lateral to the right midclavicular line near McBurney's point, and 6–8 cm lateral to the second robot port for the first, second, and third robotic arm, respectively. The main aspects of this surgical procedure include separation and ligation of IVC tributaries (including lumbar, right adrenal, gonadal, and short hepatic veins), sequentially clamping the subhepatic IVC, the left renal vein, and the caudal IVC with vessel loops, and performing IVCT, IVC repair, and RN.
Robotic retroperitoneal IVCT
The retroperitoneal IVCT was performed using the Da Vinci Si robotic surgical system. After general anesthesia induction and Foley catheter placement, patients were placed in a 90° left lateral decubitus position with overextension (Supplementary Fig. S1), which maximized the space between the iliac crest and the 12th rib. First, we made a 2-cm incision at ∼5 cm above the intersection of the iliac crest and mid-axillary line. The muscle layer and lumbodorsal fascia was divided with a Kelly clamp, and the retroperitoneal space was bluntly separated with a finger. Then, a homemade balloon dilator was inserted and inflated to establish the retroperitoneal space.
A 12-mm port for the camera was placed ∼8 cm above the iliac crest along the mid-axillary line. Three 8-mm ports for the first, second, and third robot arms were placed under the intersection of anterior axillary line and costal margin, under the costal margin on the posterior axillary line, and at 6 cm ventral to the first robot port, respectively. An assistant port for dissecting and clamping the left renal vein was placed ∼5 cm below the midpoint of the first and third robotic arms. After positioning all the trocars, the robotic arms were docked to the ports. Then, the working space was created by CO2 inflation to maintain the pneumoretroperitoneum (pressure range 13–15 mm Hg).
A monopolar scissor (first robot arm), bipolar Maryland (second robot arm), and noninvasive forceps (third robot arm) were used, and a 30° robotic camera was inserted.
First, the retroperitoneal fat tissue present outside the Gerota's fascia was dissected downward until the fascia was exposed up to the iliac fossa. Then, dissection along the posterior renal fascia and the anterior surface of the psoas muscle to fully expose the renal pedicle was performed. It is often faster to isolate the renal artery by identifying the medial arcuate ligament as an anatomical landmark in this step. 19 Using the third robot arm to push the kidney toward the ventral side, the renal artery was fully mobilized and clamped with Hem-o-lok clips. Then, the arteries were transected. After the lower pole of the kidney was separated, the ureter was ligated and transected with Hem-o-lok clips. Then, the tributaries of the IVC (including the lumbar, right adrenal, gonadal, and short hepatic veins) were ligated and disconnected. Then, circumferential dissection of the IVC, left, and right renal veins was performed at the location of the tumor thrombus. Under the guidance of an intraoperative ultrasonography probe, the surgeon could confirm the extent of the thrombus, and tourniquets were applied twice, both above and below the thrombus. Then, the caudal and cephalic IVC, and the left renal vein were sequentially clamped. As the left renal vein was relatively far away from the camera port, during the process of dissecting the left renal vein, we used the third robotic arm to expose the surgical field by fending off the peritoneum and the kidney. As a result, the surgeon could dissect and clamp the left renal vein effectively.
Subsequently, the IVC wall was cut, and the thrombus was removed. A 5-0 polypropylene suture was used to close the IVC lumen after irrigating the lumen with heparinized saline. Then, the vessel loops around the cephalic and caudal IVC and the left renal vein were sequentially released. In the same position, the right RN was performed (Fig. 1).
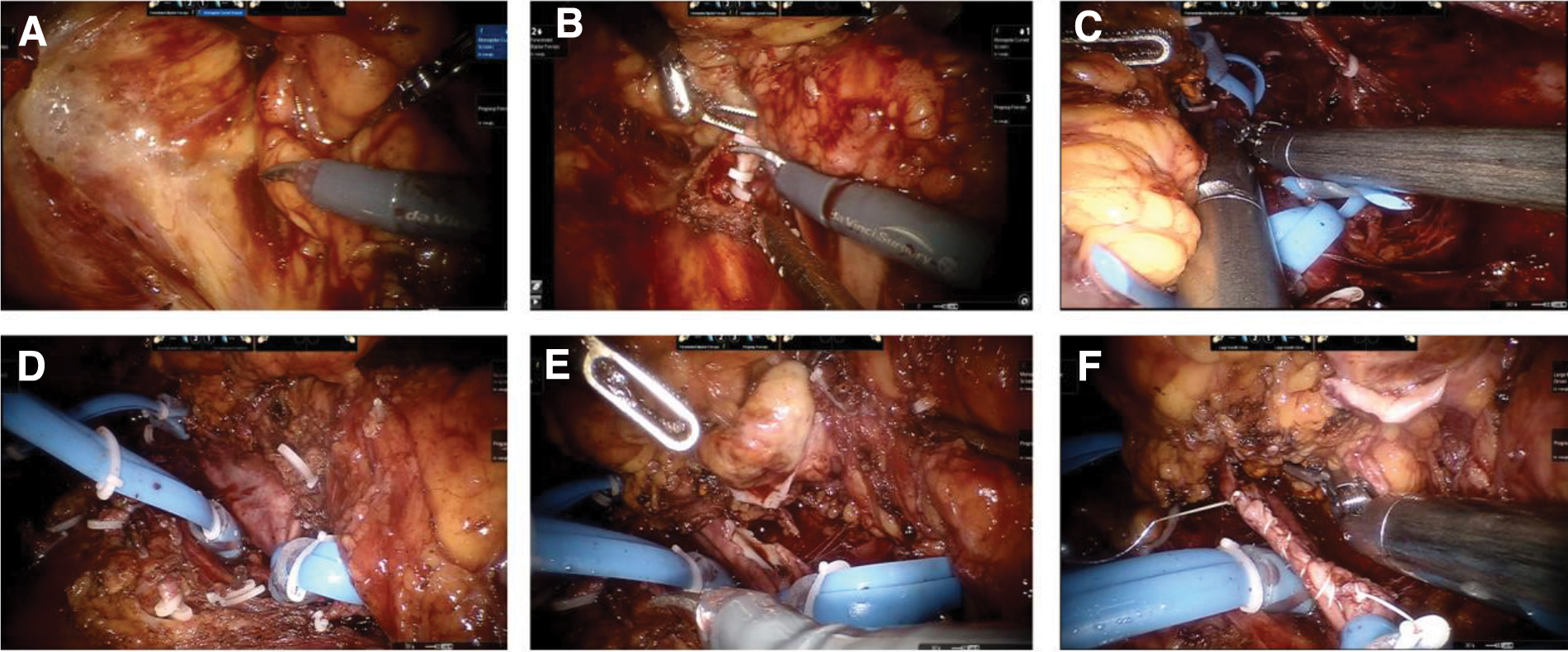
Robotic retroperitoneal thrombectomy in patients with right RCC and level I–II IVCTT.
To record the hemodynamic changes, a Swan–Ganz catheter was inserted through the right internal jugular vein to measure the central venous pressure (CVP), and transesophageal echocardiography was used to measure the diameter of the IVC.
Follow-up
Basic physical examination, contrast-enhanced computerized tomography, or magnetic resonance imaging for abdomen and pelvis was performed at follow-up after every 3–6 months.
Statistical analysis
Continuous variables are presented as median and interquartile range and were compared with one-way analysis of variance. Categorical variables are presented as frequencies and percentages, and the chi-square test was applied for comparisons. Statistical analysis was performed using Statistical Package for Social Sciences (SPSS) v. 19.0 (SPSS, Inc., Chicago). Statistical significance was set at two-sided p < 0.05.
Results
The baseline characteristics were comparable between the retroperitoneal and transperitoneal cohorts in terms of age, gender, BMI, tumor size, IVC thrombus length and classification, and preoperative angioembolization (Table 1).
All patients were treated with robotic IVCT without converting to open surgery, and no patient required blood transfusion. Table 2 shows the perioperative, pathologic, and follow-up data of robotic retroperitoneal and transperitoneal IVCT. Compared with the robotic transperitoneal cohort, the retroperitoneal cohort tended to have less blood loss (160 vs 240 mL, p = 0.024), shorter operative time (130 vs 145 minutes, p = 0.003), lower CVP (p < 0.05), and a smaller diameter of IVC during surgeries (p < 0.05) (Fig. 2). There were no significant differences in IVC thrombus length (3.2 vs 4.0 cm), IVC blocking time (18 vs 16 minutes; p = 0.64), and postoperative hospital stay (6 days for each group; p = 0.67). No perioperative bleeding, pulmonary embolism, or other serious complications occurred. No patient was found to have tumor recurrence or metastasis during the follow-up period in either group.
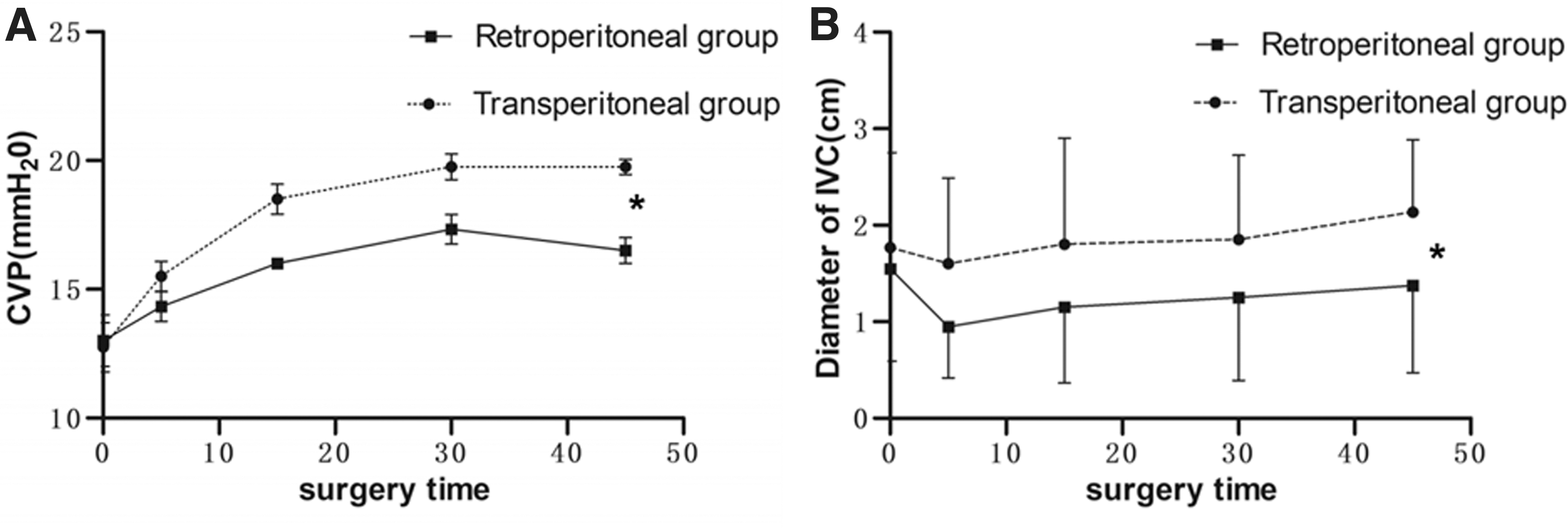
The hemodynamic changes during robotic retroperitoneal IVCT and transperitoneal IVCT.
Discussion
The study showed that robotic retroperitoneal RN and IVCT are feasible and safe for the patients with right RCC and level I–II IVCTT. Patients undergoing robotic retroperitoneal IVCT tended to have less blood loss and shorter operative time than those undergoing transperitoneal IVCT. In 2005, Disanto et al. described the application of laparoscopic surgery through a retroperitoneal approach combined with open surgery for right RCC and IVCTT reaching infrahepatic veins. The author considered the retroperitoneal laparoscopic approach safe from a surgical and oncologic perspective, as it is the most reliable method for protecting the IVC in the right RCC with IVCTT. 20 Wang et al. demonstrated the safety and feasibility of pure retroperitoneal laparoscopic surgeries in selected patients with left RCC and different levels of renal vein tumor thrombus extension and right RCC with minimal IVCTT. 21,22
In our opinion, as we are familiar with the procedures of retroperitoneal operations and the anatomy, the surgeon could expose and control the renal artery directly before mobilization of the renal vein and IVC, and early blockage of the renal artery can reduce the blood supply to the tumor and lower the risk of bleeding. Our previous study indicated that the medial arcuate ligament could be used as an anatomical landmark for the location of the renal artery in retroperitoneal laparoscopic renal surgery. 19 Rose et al. and Vuong et al. also performed robotic IVCT with principle as ligation the renal artery first. 7,8 Furthermore, it may be difficult to ligate the lumbar veins located on the dorsal or external side of IVC during transperitoneal IVCT, whereas it would be easier for the surgeon to perform the procedure during retroperitoneal IVCT. Besides, compared with robotic transperitoneal IVCT, robotic retroperitoneal IVCT has little effect on abdominal organs, for which it does not require the gastric tube. Thus, the patient's gastrointestinal function will recover rapidly after surgery. While performing retroperitoneal IVCT for patients with right RCC and IVCTT, Disanto et al. and Wang et al. suggested that retroperitoneal laparoscopic approach provides a more direct and earlier access to the vena cava than the transperitoneal approach without mobilizing the colon and duodenum or rotating the liver. 20 –22
However, there are also some limitations of robotic retroperitoneal IVCT. First, the dissection and ligation of short hepatic veins may be more difficult through the retroperitoneal approach than the transperitoneal laparoscopic approach, which may increase the risk of vascular complications. Second, it may be difficult to perform robotic retroperitoneal IVCT for patients with right RCC and IVCTT located in or above the retrohepatic IVC because of the liver obstructing the pathway. Therefore, further studies are warranted to examine the safety and feasibility of robotic retroperitoneal IVCT for patients with right RCC and IVCTT located at or above the porta hepatis. Third, as the operating space of the retroperitoneal IVCT is narrower than that of transperitoneal IVCT, it may be difficult for surgeons who are not proficient in robotic surgery to perform robotic retroperitoneal IVCT.
In our opinion, the key features of robotic retroperitoneal IVCT for patients with right RCC and level I–II IVCTT include preparation of the retroperitoneal operating space and ligation of the left renal vein. Although there was a narrower operating space through the retroperitoneal approach, the surgical procedures were feasible with the five-port technique. Furthermore, robotic retroperitoneal IVCT was performed with the da Vinci Si surgical system in this study. As the robotic arms of the Xi surgical system are smaller than those of the Si system, robotic surgeries using the Xi system would be more flexible with a relatively sufficient operating space. Besides, the Xi system might confer some advantages during robotic retroperitoneal procedures, especially in terms of the use of the fourth arm. Aghazadeh and Goh reported their experience with a novel supine single-dock approach for robotic IVCT for a left-sided RCC with level II IVCTT using the Xi surgical system. 23
In this study, the right renal artery was located quickly and mobilized safely when the patients were placed in a left lateral decubitus position during the retroperitoneal surgeries. However, the left renal vein was relatively far away from the camera port; thus, safe dissection of the left renal vein and prevention of damage to the peritoneum became difficult. During the process of dissecting the left renal vein, the third robotic arm can be used to expose the surgical field by fending off the peritoneum and the kidney to the opposite side, and the surgeon can isolate and dissect the left renal vein effectively. In addition, as the right central adrenal vein drains vertically into the IVC through its right posterior wall, the surgeon should be careful not to damage the right central adrenal vein when dissociating it from the upper pole of the right kidney and the adrenal gland.
In this study, the retroperitoneal robotic IVCT group tended to have less blood loss compared with robotic transperitoneal group. The amount of bleeding from the IVC during laparoscopic surgery depends on the pressure gradient between the pneumoperitoneum pressure and CVP. We found that the degree of vascular filling of the IVC was much higher in robotic transperitoneal than in retroperitoneal IVCT. In our opinion, pneumoperitoneum pressure may cause an upward movement of the liver and diaphragm during transperitoneal IVCT, which can exert additional pressure on the mediastinum and right atrium. Thus, the resistance to blood flow from the IVC to the right atrium would increase. However, pneumoperitoneum pressure has little effect on the liver and diaphragm during retroperitoneal laparoscopic surgeries, because of which the upward movement of the liver and diaphragm is reduced, less pressure is exerted on the right atrium and mediastinum, and resistance to blood flow from the IVC to the atrium is much lower during retroperitoneal laparoscopic surgeries.
The indications for robotic transperitoneal and retroperitoneal IVCT are different. First, we have shared our experience on robotic transperitoneal IVCT for level I–IV IVCTT. 6,12,24 In our experience, it is feasible to perform robotic retroperitoneal IVCT for patients with right RCC and level I–II IVCTT. However, because of limitations in terms of the operating space, it is difficult for a surgeon to perform retroperitoneal IVCT for patients with level III–IV IVCTT. Besides, it will be difficult to perform robotic retroperitoneal IVCT for left RCC patients with level I–II IVCTT, as the left renal vein traverses anterior to aorta and superior mesenteric artery. Furthermore, we performed IVCT using the retroperitoneal approach for patients with a history of abdominal surgery and adhesions.
Conclusions
Despite the technical challenges, it is safe and feasible to perform robotic retroperitoneal IVCT for patients with right RCC and level I–II IVCTT. Patients undergoing retroperitoneal IVCT tended to have less blood loss and shorter operative time than those undergoing transperitoneal IVCT. Future studies should include larger sample size and analyze long-term follow-up data to evaluate the efficacy of these surgical procedures.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Natural Science Foundation of China (Grants Nos. 81970594 and 81970665).
Supplementary Material
Supplementary Figure S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.