
Abstract
Introduction:
Appropriate risk stratification and complete tumor ablation are the key factors to optimize the oncologic outcomes of patients undertaking endoscopic management for upper urinary tract urothelial carcinoma (UTUC). We aimed to identify risk factors associated to tumor recurrence and progression in a contemporary cohort of patients diagnosed and treated with the latest endourologic technologies.
Patients and Methods:
Forty-seven patients were selected between January-2015 and March-2019 for an endoscopic management of UTUC. Last generation of digital ureteroscopes with image-enhancing technologies were used for the detection of the lesions. The retrograde approach was the most frequent access (n = 45/47). The confocal laser endomicroscopy and multiple biopsy devices were variably used according to site and tumor presentation for their characterization. Holmium and Thulium lasers were variably used, with their combination being the preferred approach in case of larger lesions. Primary endpoints included the identification of factors associated with UTUC recurrence and progression, and bladder tumor recurrence.
Results:
Median follow-up (FU) was 24 months (interquartile range 17–44). On multivariate analysis, bladder cancer (BC) recurrence was associated to previous contralateral UTUC (hazard ratios: 5.08 confidence interval [95% CI: 1.35–18.94], p < 0.05) and tumor size (hazard ratios: 1.07 [95% CI: 1.00–1.14], p < 0.05). UTUC recurrence was associated to incomplete clearance after primary treatment (hazard ratios: 4.99 [95% CI: 1.15–21.62], p < 0.05), while UTUC progression was significantly related to the number of UTUC recurrences (hazard ratios: 3.10 [95% CI: 1.27–7.53], p < 0.05). No significant survival differences in BC/UTUC recurrence, as well as in UTUC progression, were detected between risk groups. No Clavien-Dindo grade >2 were detected; one patient developed ureteric stricture at 7-month FU. Limitations involve retrospective nature of the study and relatively small number of patients.
Conclusions:
The appropriate use of latest technology may enhance the oncologic outcomes of the endoscopic management of UTUC without compromising the safety of the approach. Among the prognostic factors identified in our series, UTUC recurrence seems to be associated to disease progression.
Introduction
Upper urinary tract urothelial carcinoma (UTUC) is an uncommon urologic neoplasm, accounting for a minority of all urothelial carcinomas (UC) (5%–10%). Even though it is generally regarded as a rare cancer, its estimated annual incidence in western countries is reportedly rising as a result of improved survival in patients with lower tract UC. 1
Radical nephroureterectomy (RNU) is the gold standard treatment option in patients with UTUC; nevertheless, kidney-sparing endoscopic management is an alternative treatment option in highly selected patients, providing comparable oncologic outcomes as well as optimizing renal function preservation. 2,3 The conservative approach, initially restricted to imperative cases, has been extended as an elective treatment option for low-risk (LR) tumors in the latest editions of the European Association of Urology (EAU) guidelines. 1 Currently, mounting evidence is pushing the boundaries for its indication, with bigger and/or multifocal low-grade lesions also treated electively. 4,5
The rapid technologic advancement is helping the practitioners in improving the technique, especially in terms of accurate identification, characterization, and ablation of the tumors. 6 We aimed to identify the prognostic factors associated to the oncologic outcomes of patients selected for the endoscopic management of UTUC as optimized by the application of the latest technologies.
Patients and Methods
Study population and study design
We retrospectively reviewed institutional records of all consecutive patients who were selected for an endoscopic management of UTUC with curative intent at our center between January 2015 and March 2019. IRB approval number was FP2014/17.
Preoperative data included patients' demographics and comorbidities. History of UC was assessed, including bladder cancer (BC), contralateral UTUC, and previous homolateral distal ureterectomy; none of the patients underwent previous homolateral endoscopic management of the disease. A preoperative workout, including contrast-enhanced CT urography, white-light flexible cystoscopy, urine cytology, and standard blood test, was undertaken in all the patients.
Patients were classified as harboring LR or high-risk (HR) disease according to current EAU guidelines criteria. 1 Endoscopic management was offered as an elective indication to patients having LR disease and in selected cases of HR disease (e.g., >2 cm lesion and/or multifocal low-grade neoplasm, in which complete ablation was deemed feasible), or as an imperative indication to patients with HR disease and solitary kidney, chronic kidney disease (stage ≥III), bilateral involvement, genetic predisposition (e.g., Lynch syndrome) or in case of patients unfit or unwilling to undergo radical surgery. Nevertheless, the indication to an endoscopic approach was always agreed at the multidisciplinary team meetings. Otherwise, patients were selected directly for undertaking a RNU. All patients were informed about the risks and benefits of the procedure, including the possibility of a multistep treatment, the risk of recurrence and progression, and the need of a strict follow-up (FU); this latter included CT scan+flexible cystoscopy+urine cytology and endoscopic revision in the operating theater alternated every 6 months.
Operative time was defined as the time between cystoscopic examination and exit strategy deployment. Intraoperative and postoperative complications were scored according to the modified Satava 7 and Clavien-Dindo classifications, 8 respectively. The 8th edition of the TNM classification 9 and the 2016 World Health Organization classification system 10 were applied for tumor staging and grading, respectively. Postoperative data included length of hospitalization and renal function. In case of high-burden disease (>2 cm in size or multifocal) or uncertain complete treatment, patients were submitted to second-look ureteroscopy (URS) within 60 days to ensure treatment radicality; the eventual second-look procedure was considered as an integral part of the treatment session.
The primary endpoints consisted in finding factors eventually associated with BC and UTUC recurrence, and UTUC progression. UTUC progression was defined in LR patients as the progression to HR UTUC, while in the HR group, it was defined as the need for RNU for lesions not any more manageable endoscopically or as the appearance of high-grade disease in case of initial low-grade HR disease (Fig. 1). Overall, RNU not necessarily was indicated after progression of disease: in the LR group, this could be the case of progression to HR for the presence of multiple recurrent lesions that still were deemed approachable endoscopically (either electively or imperatively); in the HR group, this could have been the case of patients unfit to surgery. The secondary endpoints included the assessment of the overall survival (OS), the cancer-specific survival (CSS), and the postoperative complication rate.
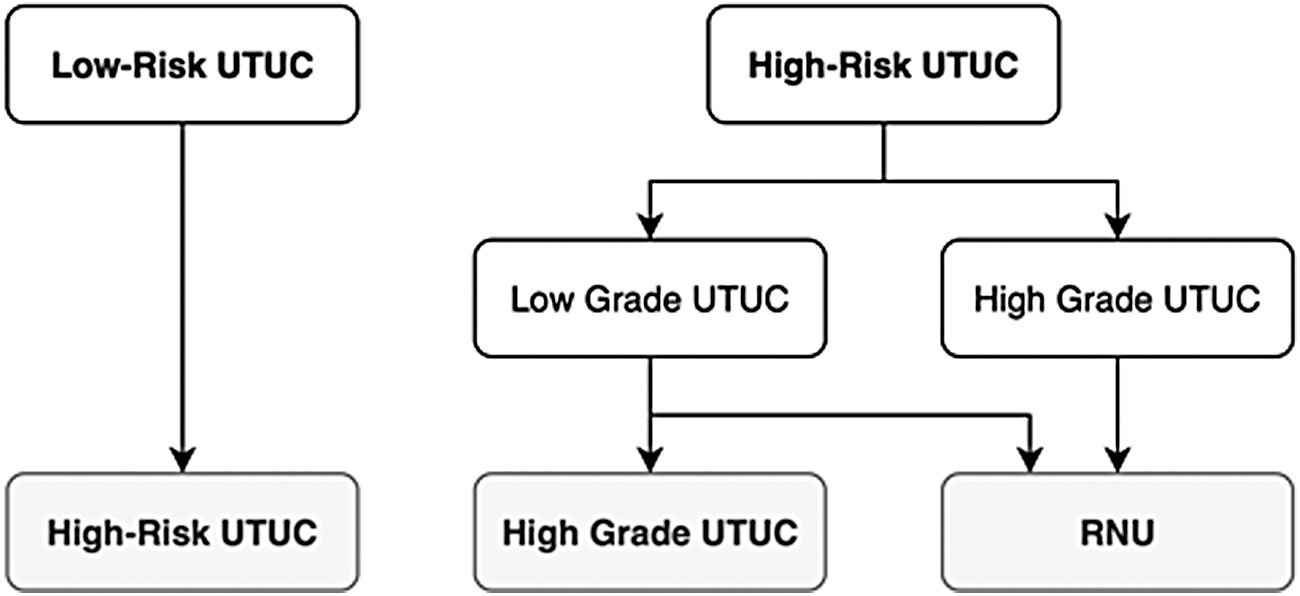
Definition of UTUC progression based on EAU classes of risks. EAU = European Association of Urology; UTUC = upper urinary tract urothelial carcinoma.
Exclusion criteria included the ineligibility to a conservative management protocol after the first endoscopic intervention (e.g., patients with HG tumors at biopsy histology and normal renal function), so that radical surgery was promptly expedited. Patients with medical history of UTUC in the same lateral site were also excluded to reduce confounding factors.
Absolute frequencies and percentages were used to describe the qualitative variables, while median and interquartile range (IQR) were used for quantitative variables. The Kolmogorov–Smirnov test was used to assess the normality of distributions. A univariate Cox proportional hazards regression was performed for each explanatory variable. According to Mickey and Greenland selection criteria recommendations, 11 variables with p-value <0.2 were selected for a multivariate stepwise regression model to identify variables associated to the relevant outcomes. The results have been described as hazard ratios with a confidence interval (95% CI); for all the tests, p-values <0.05 were considered statistically significant. The RStudio (version 2.5.1; RStudio, Boston) package was used for statistical analysis.
The principles of the Declaration of Helsinki (version of 2013) have been scrupulously followed in full respect of the patients' privacy and confidentiality.
Pre-op setting and endoscopic evaluation of the urinary tract
All the patients underwent general anesthesia and received antibiotic prophylaxis 60 minutes before the surgery. Operating theater set up is illustrated in Figure 2.
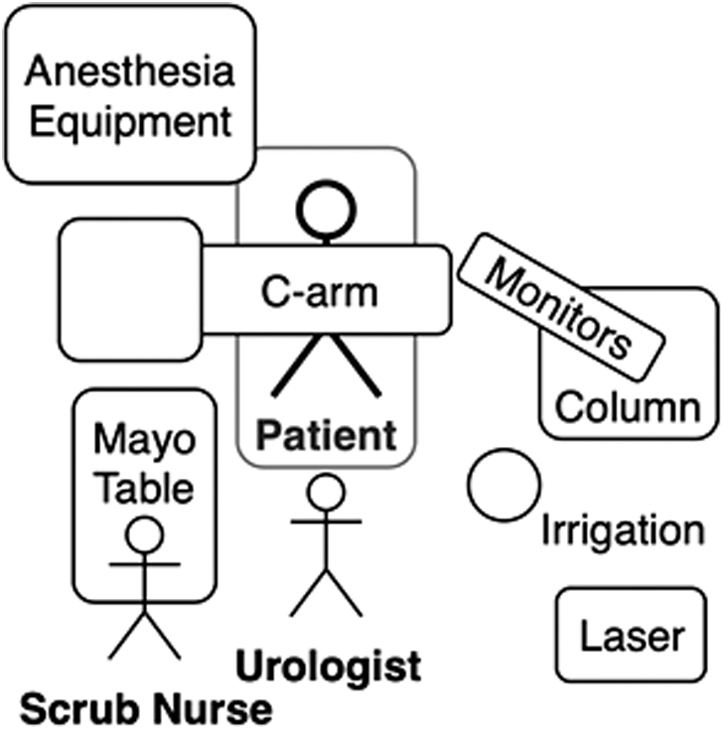
Operating theater setting, for left UTUC lesions.
A cystoscopy and semirigid URS were systematically carried out to rule out synchronous bladder tumors and to inspect and/or dilate the ureter. Urine samples for cytologic examination were selectively collected. 12 Whenever feasible, a “no touch technique” without guidewire placement was used to prevent potential mucosal injury and bleeding that could compromise the appropriate identification of all the lesions, especially Carcinoma In Situ. 13 Alternatively, a working guidewire was inserted to eventually negotiate the ureteric orifice. A safety guidewire, if necessary, was put in either through a dual-lumen catheter or during semirigid URS. A flexible URS was attempted in some cases since the beginning of the procedure, especially in case of dilated or prestented ureters.
As soon as the manipulation of the lesion was foreseen (ablation and/or multiple biopsies), a 10F to 12F ureteral access sheath (UAS) was put in with its upper tip below the target lesion or caudally to the lowest tumor in case of multifocal UTUC. The rational for the UAS placement are similar to those described for the endoscopic treatment of urinary stone (multiple accesses, better visibility, and lower intrarenal pressure). Furthermore, the UAS enables the use of back-loading forceps (BIGopsy; Cook Medical) and may help to avoid potential tumor seeding to the ureter and the bladder by allowing for direct outflow of saline. 14
Since the endoscopic findings may significantly differ from those of CT urography, 15 a thorough exploration of the pelvis and of the collecting system was systematically undertaken by means of a digital flexible ureteroscope (Flex XC; Karl Storz, Germany, URF-V; Olympus, Japan), that with the aid of image-enhancing modalities (Image1S; Karl Storz, Narrow Band Imaging; Olympus) provided better image quality and diagnostic accuracy. 16 –18 The macroscopic characteristics of the tumor were recorded, including the number of lesions, their architectural presentation (papillary, sessile, and solid), and the estimated endoscopic size.
Whenever feasible, an intraoperative tumor grade characterization was performed through confocal laser endomicroscopy (CLE) (Cellvizio®; Mauna Kea Technologies, France) that provided a dynamic evaluation of the cellular morphology and microarchitecture of the lesions in support of the surgeon's decision-making. 19
In the case of tumors that could not be reached or safely treated by a pure retrograde access (e.g., lower calyx with a steep infundibulopelvic angle, patients with urinary diversions or ureteric stricture, and so on), a percutaneous approach was performed by using a biplanar 0° to 90° supine technique. 20 Depending on the site and size of the lesions, either a 24F Amplatz sheath or a 10F to 12F UAS was placed percutaneously to ease the passage of a flexible scope.
Bioptic sampling and laser ablation
According to lesion size and morphologic features, different devices were used for biopsy, including 3F ureteroscopic forceps, 6F back-loading forceps (BIGopsy; Cook Medical), and a 2.2F nitinol basket (N-Circle; Cook Medical). The ureteroscopic or the back-loading forceps were preferred for the sampling of sessile, flat, or nonpapillary tumors, while the nitinol basket was used to avulse larger papillary lesions by gently trapping and pulling the lesion within the basket wires. The use of a basket allows for bigger specimen retrieval and tumor mechanical de-bulking; on the contrary, the back-loading forceps provides bigger specimen with less cytoarchitectural distortion than the 3F forceps, at the cost of a reduced visibility, irrigation, and instrument manoeuvrability. 21,22
Tumor ablation was initially performed with the aid of holmium-YAG laser (HL) only (standard setting: 0.8–1.2 J and 8–12 mHz), even though its disruptive effect on tissues was not ideal for tumor ablation. Thulium-YAG laser (TL) has become more recently the new standard because of its better fiber tip stability, inferior tissue penetration, smaller cavitation bubbles generation, and a distinct photothermic coagulative effect (standard setting: 10–15 W). 23 Its main disadvantage consists in the generation of a layer of coagulative necrosis at the tumor base, which may hide residual tumor, especially in case of larger lesions. The possibility to switch to HL may help to overcome this issue, as it can be used to swiftly cut and dislodge the necrotic tissue to eventually uncover residual neoplastic tissue to be targeted with TL for complete ablation.
Accordingly, in the case of larger lesions, the combination of the two lasers was the preferred approach to combine their advantages. 24
Exit strategy
At the end of the procedure, the UAS was removed under visual control to identify any ureteric injuries, 25 and a final retrograde pyelogram was obtained to detect any possible leakage. A 6F to 7F double-J or mono-J ureteral stent was left in place for either 14 days or 24 to 48 hours, respectively.
Postoperative instillation of Mitomycin C was attempted either intravesically or in the upper tract (via a mono-J stent; off-label indication) whenever possible.
Results
A total of 47 consecutive, highly selected patients were included in our analysis. Baseline clinical characteristics and perioperative data are detailed in Table 1. Median operative time was 90 minutes (IQR 60–120). Two patients (4.3%) required a percutaneous/antegrade access. Tumor ablation was performed by means of either HL or TL in 34 (72.3%) and 5 (10.6%) patients, respectively, while both lasers were used in eight (17%) cases. One patient experienced a Satava grade I intraoperative complication (bleeding), while a total of five (10.6%) patients developed a postoperative complication, including one Clavien-Dindo grade I (self-limiting bleeding) and four (8.5%) grade II complications (three infectious complications and one major bleeding requiring blood transfusion). One patient developed a ureteric stricture in the lumbar tract at 7 months post-op, which required a ureteric segmental resection with an end-to-end anastomosis. No further grade ≥III or late complications were observed. Median hospital stay was 3 days (IQR 2–4). Histopathologic diagnosis and grading of the lesions were obtained in all the patients, while T stage could not be determined in 35 (74.5%) cases. The real-time tumor grading characterization with CLE could be performed in seven cases, with a concordance with the histology at biopsy of 71.4% (n = 5/7); sensitivity for HG lesions was 100%, while specificity accounted for 57.1%.
Baseline Clinical Characteristics and Perioperative Data
ASA = American Society of Anesthesiologists; BC = bladder cancer; BMI = body mass index; CCI = Charlson Comorbidity Index; eGFR = estimated glomerular filtration rate; IQR = interquartile range; MMC = mitomycin C; UTUC = upper urinary tract urothelial carcinoma.
According to intraoperative and histopathologic findings, 29 (61.7%) and 18 (38.3%) patients were classified as having HR and LR disease (Table 2).
Risk Stratification According to Tumor Characteristics
HG = high grade; LG = low grade.
UTUC clearance was deemed macroscopically complete in 41 patients (87.2%) after primary procedure. Nevertheless, 23 (48.9%) patients were submitted to a second-look procedure: no residual disease was detected in the majority of them (n = 15; 65.2%), while a persistence (i.e., residual tumor on the site of former ablation) of disease was identified and treated in 8 patients (24.8% of the second-look subgroup; 12.8% of the overall cohort).
Median FU was of 24 months (IQR 17–44). Median OS and CSS were 24 (IQR 17–44) and 24.5 months (IQR 17–44), with 4 patients dying in the FU, 2 of them because of the UTUC progression. A bladder recurrence was detected in 11 (23.4%) patients at a median FU time of 15 months (IQR 8–17). An UTUC recurrence developed in 13 (28.3%) patients at a median FU time of 7 months (IQR 5–31). Nine patients (n = 3 and n = 6 in the LR and HR group, respectively; overall 19.1%) experienced tumor progression at a median FU time of 9 months (IQR 6–37). All except one of these patients (n = 2 and n = 6 in the LR and HR group, respectively; overall 17%) eventually underwent RNU, with a kidney-preservation rate of 82.9% at last FU; grade-concordance rate between RNU histology and former biopsy was 87.5%.
Results of the univariate analysis are shown in the Supplementary Data. On multivariate analysis (MVA), bladder recurrence was associated to previous contralateral UTUC (hazard ratios: 5.08 [95% CI: 1.35–18.94], p < 0.05) and tumor size (hazard ratios: 1.07 [95% CI: 1.00–1.14], p < 0.05). UTUC recurrence was associated to incomplete clearance after primary endourologic treatment (hazard ratios: 4.99 [95% CI: 1.15–21.62], p < 0.05), while UTUC progression was significantly related to the number of UTUC recurrences (hazard ratios: 3.10 [95% CI: 1.27–7.53], p < 0.05) (Table 3). Due to the low number of events recorded, no statistical analysis was undertaken for the OS and CSS. According to Kaplan–Meier analysis, no significant differences in BC/UTUC recurrence, as well as in UTUC progression, were detected between LR and HR groups in the survival curves (Fig. 3).

Kaplan–Meier survival curves.
Multivariate Models
Discussion
Tumor detection, appropriate risk stratification, and complete ablative treatment are the cornerstones of an effective endoscopic therapeutic strategy.
The introduction of last-generation digital scopes, together with the application of image-enhancing technologies and a no-touch technique, contributed to better detection of neoplastic lesions. 13,16 –18
The key factor in patient selection is the correct grading characterization, as low-grade disease has been widely associated with effective endoscopic management. 2,3,26 In the present series, histopathologic and grading characterization at biopsy was achievable in the totality of the patients, with an 87.5% grade-concordance in those that ultimately underwent RNU. This finding underlines the effectiveness of using the best biopsy device according to the tumor site and presentation. 21,22 The concomitant use of CLE provides additional information on this matter, helping to intraoperatively identify those patients more suitable for conservative treatment, with a high sensitivity for ruling-in potential high-grade tumors; nevertheless, more robust data are warranted on this regard, especially for what concerns its lower specificity. 19
The introduction of TL set a new standard in the endoscopic treatment of the disease, providing a more effective and precise ablation. 23,27,28 The possibility to integrate different laser generator in one device (Revolix Duo; LisaLaser, Katlenburg-Lindau, Germany) has resulted effective in our experience. Overall, we reached macroscopic radicality in 87.2% of cases with an overall rate of 12.8% of residual disease at the second-look URS, as opposed to the 51.2% rate described in the literature in routinely performed second-look procedures. 29 Defidio et al. 23 has recently reported the outcomes of a series of endoscopic UTUC cases treated by means of the same combination of laser energies, with a 49.5% recurrence rate at 3 months. However, this series included cases treated in the span of 13 years with different generations of devices used, which might have undermined the outcomes.
Our rate of recurrence (28.3%), progression (19.6%), and renal function preservation (82.9%) are comparable to other case-series with similar FU, 23,27,28 even though we reported a much higher proportion of imperative and HR cases. Furthermore, we reported the association on MVA between incomplete clearance of the tumor at initial URS and UTUC recurrence, underscoring the importance of obtaining treatment radicality.
Tumor burden (defined by the combination of size and focality) seems to play a minor role if macroscopic complete ablation can be achieved, 4,5 as in our series, it was not a factor associated to UTUC recurrence or progression. However, tumor size was associated to bladder recurrence: intuitively, this circumstance could be attributable to a higher risk of tumor seeding as a consequence of prolonged tumor manipulation and urine drainage to the bladder. The theoretic utility of UAS to prevent tumor seeding cannot be confirmed based on our experience; future investigations may involve the perioperative use of mitomycin C in the urinary tract, as some preliminary reports have shown a benefit from it. 30
Interestingly, we found a significant association between the number of recurrences and UTUC progression: this could be an important finding, as it mirrors the role of tumor recurrence in the risk classification of the nonmuscle invasive BC. 31 Accordingly, we believe that UTUC recurrence should be considered and included among the risk stratification criteria of UTUC, although more robust data will be necessary to confirm our outcome.
Finally, we observed a low rate of minor complications with only one long-term complication (ureteric stricture), confirming the safety of endoscopic management of UTUC. 23 Conversely, older series showed a ureteral stricture rate of 16.4%, 26 suggesting that endourologic advancements may have played a role on this matter.
Our work is not devoid of limitations. The retrospective nature of the study, the low number of patients included, the lack of a comparative group (e.g., historical series of patients treated without the aid of the latest technologies), and the lack of long-term outcomes limited the possibility to reach more definite conclusions, so that further studies are warranted to assess the long-term outcomes of an advanced endourologic approach to UTUC.
Conclusions
The appropriate use of latest technology may enhance the oncologic outcomes of the endoscopic management of UTUC without compromising the safety of the approach. Tumor size seems to be associated to BC recurrence, while the number of recurrences to UTUC progression. Longer FU data and larger series are needed with the application of the latest generation of technologies.
Footnotes
Acknowledgments
To C. Esquina Lopez—Professor of Statistics at Vall d'Hebron Research Institute, Universitat Autonoma de Barcelona-has realized the statistical analysis. crise4@hotmail.com
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was not funded.
Supplementary Material
Supplementary Data
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.