
Abstract
Introduction:
To compare complication rates in radical nephrectomy (RN) for renal cell carcinoma (RCC) across different age groups.
Methods:
Retrospective analysis of the British Association of Urological Surgeons Nephrectomy audit database between January 1, 2012, and December 31, 2017, was performed. Comparisons were made between different age groups (<60, 60–79, and ≥80) in patients undergoing RN for RCC.
Results:
Eighteen thousand four hundred thirty-eight patients with RCC underwent RN: 6128 (33.2%) <60 years of age, 10,785 (58.5%) 60–79 years of age, and 1525 (8.3%) ≥80 years of age. There was a significantly lower preoperative hemoglobin and estimated glomerular filtration rate with advancing age (p < 0.001). Patients ≥80 had a higher Charlson comorbidity index and World Health Organization (WHO) performance status (p < 0.001). There was also significant variability in the approach to RN (p < 0.001): laparoscopy was most commonly performed (68.8% vs 69.3% vs 75.0%). Patients ≥80 years of age were found to have the shortest operating time (p < 0.001). There were significant differences in T stage between groups with patients ≥80 years of age having a higher T stage (p < 0.001). The incidence of intraoperative complications did not significantly differ between age groups (p = 0.18). The incidence of postoperative complications was 15.7%, 18.2%, and 20.5% and major postoperative complications was 1.4%, 2.1%, and 2.8% in patients <60, 60–79, and ≥80 years of age, respectively (p < 0.001). The most common complication in all age groups was blood transfusion (7.6% <60, 8.6% 60–79, and 9.1% ≥ 80 years of age). Stepwise logistic regression analysis adjusting for additional variables found the odds of a postoperative complication increased with age with an odds ratio of 1.25 in patients ≥80 years of age and an odds ratio of 1.09 in patients 60–70 years of age compared with <60 years of age.
Conclusion:
Overall complications in all age groups are low, but advancing age should be considered an independent risk factor for postoperative complications after RN and should be appropriately considered when counseling elderly patients before treatment.
Introduction
Renal cell carcinoma (RCC) has an increasing incidence with age, with a peak incidence between 70 and 74 years. 1 In United Kingdom, between 2013 and 2015, 36% of all new diagnoses occurred in patients ≥75 years of age. 2 This is, in part, contributed to by the increasing number of RCC being incidentally detected on imaging. 3
With the number of people in United Kingdom older than 85 years projected to double in the next 25 years, we would anticipate a significant increase in the number of elderly patients being diagnosed with RCC. 4 Furthermore, the Berlin aging study has demonstrated that older adults now have higher levels of cognitive function and well-being than those 20 years ago. 5 If this continues, then we are likely to see an increase in the number of older adults undergoing curative treatment such as radical nephrectomy (RN) for their RCC. Therefore, to appropriately counsel these patients, there is a need to understand the outcomes of RN in older adults and how that compares to the younger population.
The aim of this project was to compare complication rates in RN for RCC across different age groups.
Methods
Data collection
Consultant members of the British Association of Urological Surgeons (BAUS) from England, Scotland, Wales, and Northern Ireland were invited to recruit all patients undergoing nephrectomy between January 1, 2012, and December 31, 2017. Data were submitted to a membership-based password-protected central database. A retrospective analysis of all adult patients undergoing RN with RCC confirmed on pathological assessment was performed. Three subgroups were identified according to age: 18–60, 60–79, and 80 years of age and older.
Data were collected on patient demographics and baseline preoperative characteristics, including age, sex, Charlson comorbidity index, WHO performance status, hemoglobin, and estimated glomerular filtration rate (eGFR). Perioperative data were collected on surgical technique, operative time, estimated blood loss, length of stay (LOS), intraoperative and postoperative complications, and tumor characteristics according to the TNM staging.
Statistical analysis
Categorical variables were summarized by the number and percentage of patients in each group. Continuous variables were summarized by median and interquartile range for nonparametric data and mean and standard deviation for parametric data. Categorical variables were compared using the Chi-square test. Continuous variables were compared using Kruskal–Wallis and one-way analysis of variance (ANOVA) tests. Logistic regression analysis was performed to compare differences between groups. Statistical significance was defined as p < 0.05.
Results
Forty-five thousand nine hundred ninety-nine patients were reported by the BAUS nephrectomy audit database by 511 urology consultants from 171 institutions between January 1, 2012, and December 31, 2017. A total of 18,438 patients with RCC underwent RN: 6128 (33.2%) <60 years, 10,785 (58.5%) 60–79 years, and 1525 (8.3%) 80 years of age and older.
Patient characteristics
Patient demographics and preoperative variables are shown in Table 1, separated according to age group; < 60, 60–79, and ≥80 years of age. The median age of each group was 52, 69, and 82 years. The proportion of male patients significantly decreased with increasing age. There was also a statistically significant decrease in preoperative hemoglobin and eGFR with advancing age. The presence or absence of metastatic disease was poorly reported in less than half of all cases (n = 2693 < 60, n = 4631 60–79, n = 634 ≥ 80). In those where it was reported, there were significantly fewer patients ≥80 years of age with metastatic disease (6.0%) undergoing RN (cytoreductive nephrectomy) compared to those younger than 60 years (10.0%) and 60–79 years of age (10.3%).
Patient Demographics and Preoperative Variables
Statistically significant result.
Data from 2693 (43.9%) <60-year, 4631 (42.9%) 60–79-year, and 634 (41.6%) ≥80-year patients.
eGFR = estimated glomerular filtration rate; WHO = World Health Organization.
The Charlson comorbidity index showed expected significant variation between age groups with those <60 years of age having the highest proportion of patients scoring 0 (65.7% vs 45.2% in 60–79 years of age and 35.5% in ≥80 years of age). Similarly, the WHO performance status was higher in the older age groups.
In all age groups, the clinical presentation of RCC was most commonly an incidental finding (Table 2). The proportion of patients with incidentally diagnosed RCC increased with age from 42.5% in patients younger than 60 years to 51.7% in those ≥80 years of age. Hematuria and pain were the next most common presentations in all age groups.
Reported Clinical Presentation for Patients Undergoing Radical Nephrectomy
Statistically significant result.
LUTS = lower urinary tract symptoms; UTI = urinary tract infection.
Perioperative outcomes
Alongside the RN, additional procedures were performed in 311 (5.1%) patients younger than 60 years, 656 (6.1%) patients 60–79 years, and 87 (5.7%) patients ≥80 years of age. Table 3 shows the additional procedures performed in each age group.
Additional Procedures Performed at the Time of Radical Nephrectomy
IVC = inferior vena cava; TURBT = transurethral resection of bladder tumour.
Perioperative outcomes are shown in Table 4. In all age groups, the RN was most frequently performed by a consultant urologist. There was significant variability in the approach used to perform RN with all groups most commonly undergoing laparoscopic RN followed by open, hand-assisted, and then robotic approaches. In cases using minimally invasive surgery (MIS), the conversion to open rate was not significantly different between groups. Within the database, operating time and blood loss were reported in ranges. A higher proportion of patients ≥80 years of age had shorter operations (<2 hours). There were no statistically significant differences in estimated blood loss or blood transfusion rates between the different age groups. Median LOS was 4 days in those <60 and 60–79 years of age and 5 days in those ≥80 years of age.
Perioperative Outcomes
Statistically significant result.
LOS = length of stay; MIS = minimally invasive surgery.
Tumor characteristics are shown in Table 5. Clear cell was the most common histological subtype across all age groups. There were statistically significant differences in T stage and nodal status across age groups. Patients ≥80 years of age had higher T stages and a lower incidence of nodal disease compared to the younger age groups.
Tumor Characteristics
Statistically significant result.
Intraoperative and postoperative complications
Over 90% of all age groups reported whether an intraoperative complication had occurred (n = 5845 < 60; n = 10,280 60–79; and n = 1437 ≥ 80). There was no significant difference in the overall rate of intraoperative complications across age groups; reported as 4.8% in patients younger than 60 years, 5.4% in patients 60–79 years of age, and 5.4% in patients ≥80 years of age (p = 0.18).
Specific intraoperative complications are shown in Figure 1. The most common intraoperative complication across all age groups was hemorrhage. There were 3 (0.05%) intraoperative mortalities reported in those younger than 60 years: 2 because of hemorrhage and 1 because of pulmonary embolism (PE). There were 5 (0.05%) intraoperative mortalities in those 60–79 years of age: 2 because of hemorrhage, 1 because of PE, and the additional 2 did not specify. There were no intraoperative mortalities in patients ≥80 years of age.
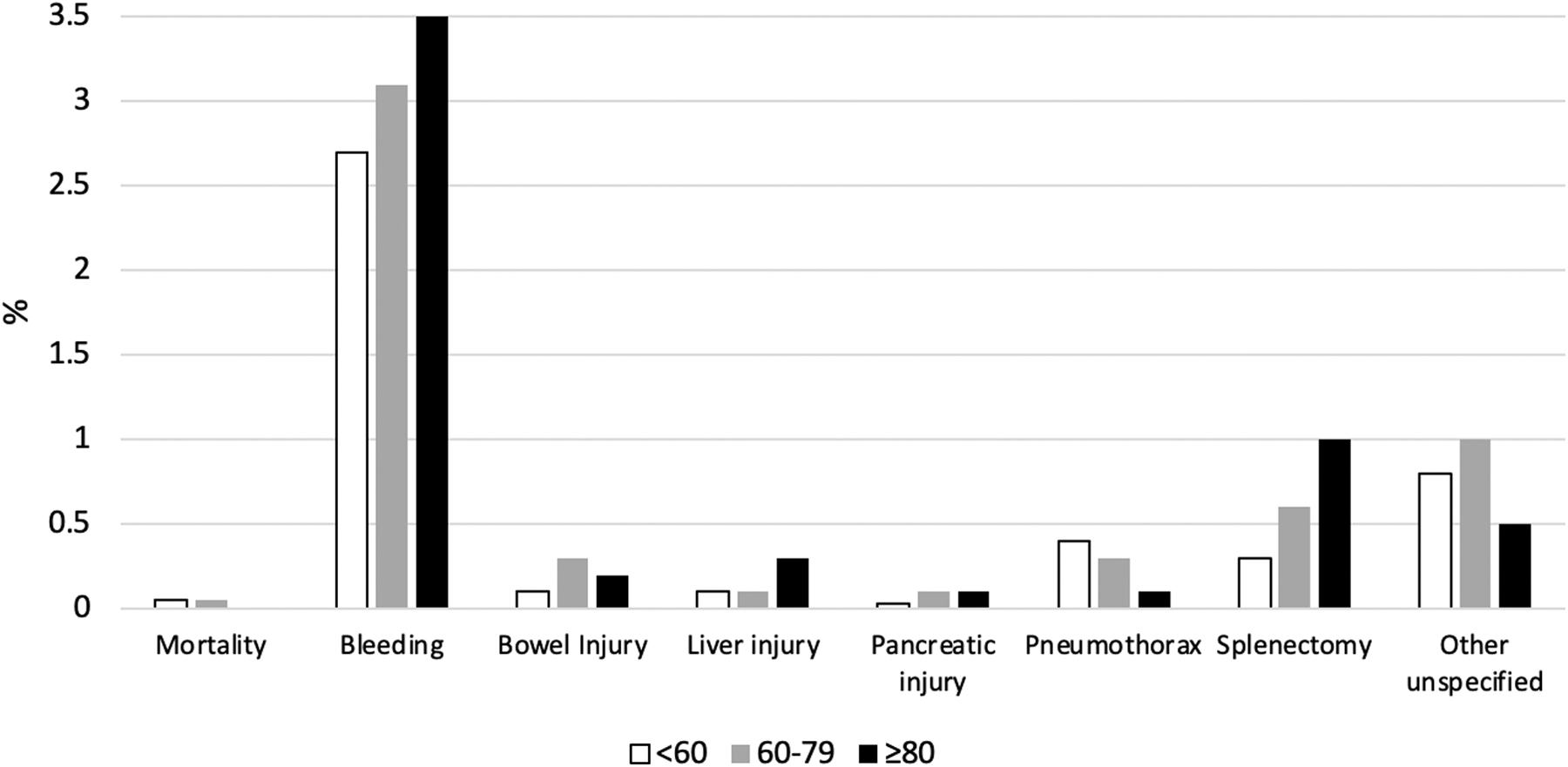
Intraoperative complications displayed according to age range.
The overall incidence of postoperative complications was 15.7% in patients younger than 60 years, 18.2% in patients 60–79 years of age, and 20.5% in patients ≥80 years of age. The incidence of major postoperative complications (Clavien >2) was 1.4% in patients younger than 60 years, 2.1% in patients 60–79 years of age, and 2.8% in patients ≥80 years of age. There was a statistically significant increase in postoperative complications with advancing age (p < 0.001). Figure 2 illustrates postoperative complications according to the Clavien-Dindo classification system and their nature with a further comparison of minimally invasive and open surgery in Figure 3. The most common complication in all age groups was blood transfusion, with a significantly higher rate of blood transfusions in open compared to MIS in all age groups.

Postoperative complications displayed according to age range.

Postoperative complications according to age comparing minimally invasive (hand assisted, laparoscopic, and robotic) to open surgery.
There were 13 (0.2%) postoperative mortalities within 30 days of operation in those <60 years of age, with only three giving a cause: one cardiac and two because of metastatic disease. There were 42 (0.4%) postoperative mortalities in those 60–79 years; 4 cardiac, 3 chest sepsis, 2 cerebrovascular accident, 2 metastatic disease, 2 multiorgan failure, 1 anastomotic leak, 1 pancreatitis, 1 PE, 1 perforated diverticulitis, 1 postoperative hemorrhage, and 24 causes were unspecified. There were 12 (0.8%) postoperative mortalities in patients ≥80 years of age: 2 multiorgan failure, 2 chest sepsis, 1 cardiac, 1 gastrointestinal bleeding, 1 sepsis (unspecified), and 5 with no reported cause of death.
Stepwise logistic regression analysis was performed adjusting for gender, T stage, technique, preoperative hemoglobin, WHO performance status, operating time, blood loss, nodal status, Charlson comorbidity index, and eGFR (Table 6). There was no significant difference in intraoperative complication rates between the three age groups. Postoperative complications rates were found to differ between age groups, although the final analysis did not reach statistical significance. All analyses showed the ≥80 years of age group had the highest rate of postoperative complications. In the ≥80 years of age group, the odds of a postoperative complication were around 25% higher than the <60 years of age group. Similarly, the 60–79 years of age group demonstrated around 10%–20% higher odds of postoperative complications than the <60 years of age group.
Regression Analyses Comparing Complication Rates Across Age Groups
OR represent the odds of the outcome in each age group relative to the <60 age group and p-value indicates the overall significance between three age groups.
Statistically significant result.
OR = odds ratio.
Discussion
With the increasing incidence of RCC, an increase in the proportion of patients presenting with more advanced disease and improvements in life expectancy, as well as functional status of older adults, we are likely to see a growth in the number of RN being performed in older patients. 1,4,5 In this study, we have performed a large multicenter comparison of perioperative outcomes in patients undergoing RN for RCC, comparing three different age groups (<60, 60–79, ≥80 years of age). We have demonstrated an increase in postoperative complications with advancing age even when accounting for a number of potentially confounding variables. This suggests that age alone has an independent importance in predicting the risk of postoperative complications.
The baseline preoperative data in our study showed some expected variations between the groups. With advancing age, there was a decrease in the proportion of male patients. This is likely attributable to the differences between life expectancy, estimated at 79.3 years for males and 82.9 years for females. 6 The authors do not believe it reflects an increase in incidence of female patients undergoing RN. The older age groups also had more comorbidities and a worse baseline performance status as demonstrated by the differences in the Charlson comorbidity index and WHO performance status. These findings are consistent with other studies comparing different age groups undergoing RN. 7 –9
Our results have demonstrated some variation in clinical presentation across the age groups. The youngest age group was more likely than the older age groups to present with symptoms, most commonly hematuria and pain, whereas over half of those ≥80 years of age were detected as an incidental finding on imaging. These findings are consistent with other studies. 10,11 However, typically, the rates of incidental presentations reported in the literature are much higher than we have found in this study, with rates as much as 70%. 11 –13 This difference is most likely because our results only include those patients undergoing RN; we would anticipate more patients being managed with active surveillance or partial nephrectomy (PN) to have incidental presentations.
In all age groups, we found robotic surgery was reported as the least common approach, which is representative of UK practice during the analyzed period (2012–2017). A recent study exploring trends in UK renal oncology practice between 2008 and 2017 also demonstrated a lower proportion of robotic surgeries in the earlier years. However, the study found the most significant change in approach was with robotic, where there was a >200% annual increase corresponding to a decrease in open and hand assisted. 14 We would anticipate this trend to continue as robotic surgery becomes more widespread.
In our data, patients ≥80 years of age were found to have a statistically significant higher rate of MIS rather than open. The surgical approach is determined by tumor characteristics, including size and location, patient factors such as previous abdominal operation, and the surgeon's expertise. It is not possible to account for all these factors to explain differences between the age groups.
The advantages of minimally invasive over open surgery are well documented and include reduced blood loss, decreased analgesia requirement, shorter hospital stay, and a quicker return to normal activity. 15 All of these factors are clearly advantageous to older patients who have a poorer preoperative performance status and more comorbidities. It is therefore possible that age contributes to decision making for surgical approach. However, even once these differences in approach are taken into consideration with the regression analyses, there remains an increase in postoperative complications with age. This demonstrates that technique alone is not the only responsible factor for increased postoperative complication rates.
There have been limited reported comparisons in the literature for RN outcomes according to age. In general, unlike our study, the few that exist suggest that there is no difference in postoperative complications with advancing age. 7,8,16,17 However, it is impossible to draw conclusion from these studies as they are based on a single-center experience with low patient numbers (range 33–158). In addition, the age groups vary between the studies with one defining their older population as ≥65 years. 8
With increasing age, patients are known to have a decreased physiological reserve and reduced ability to accommodate metabolic challenges. 18 Functional impairment is, in part, contributed to by sarcopenia, a loss of muscle mass and strength, which has been shown to continuously decline with advancing age. 19 Therefore, when making age comparisons, it is important to divide up older populations further as we did in this study.
Because of the absence of reported oncological outcomes within the BAUS nephrectomy audit database, it was not possible to compare these between age groups. Gao et al. retrospectively reviewed 672 patients who underwent PN or RN with a median follow-up of 50.8 months. 9 Their study demonstrated that patients ≥75 years, as might be expected, had a decreased overall survival compared to younger age groups, but no difference in cancer-specific survival. More research would be required to better understand whether the oncological outcomes in the older age groups are equivalent to younger populations. However, the risks of operation and a patient's anticipated life expectancy must be taken into consideration when planning treatment or considering active surveillance in small renal masses.
In this study, we have only looked at the outcomes of RN and not made any comparison with PN. However, several recent propensity score-matched analyses have extensively explored this. Veccia et al. compared RN and PN in patients ≥65 years of age with large renal masses (cT1b or ≥cT2) and Mir et al. explored an older age group looking at patients ≥75 years of age with cT1/2 renal masses. 20,21 Both studies found no significant difference in the rate of major complications or survival outcomes.
A larger propensity score-matched analysis from the surveillance, epidemiology, and end result database looking only at T1a RCC in patients ≥75 years of age suggested PN resulted in a lower 5-year other-cause mortality without impacting cancer-specific mortality or 30-day mortality rates. 22 This would suggest that in the appropriately selected renal masses, PN is not only a safe and suitable alternative to RN in the older age group but also shows that the benefits of nephron sparing surgery apply to the older age group.
The strengths of our study include its multicenter nature and large patient number. In addition, we have taken into consideration multiple potential confounding factors to reach our conclusions. The BAUS nephrectomy audit database is an invaluable resource for understanding nephrectomy outcomes. It is open to all urological surgeons performing nephrectomy within United Kingdom. Based on hospital episode statistics, it is estimated to have captured over 90% of patients undergoing nephrectomy in the time period during this study (2012–2017). It therefore enables analysis of a large volume of patients, which would accurately reflect UK outcomes, essentially benchmarking the outcome of RN for an entire nation. Furthermore, it would be applicable to other countries with similar operative strategies.
However, there are limitations to the data. The data is all self-reported, which is open to reporting bias. Although many of the demographics, and operative and perioperative details are well reported within the database, there is poor reporting of some variable, for example, baseline characteristics such as body mass index and frailty assessments, which arguably could affect perioperative outcomes, and as already discussed poor reporting of oncological outcomes.
Conclusion
In this multicenter study of over 18,000 patients, we have demonstrated that advancing age should be considered an independent risk factor for postoperative complications after RN. Age alone should not be considered a contraindication to curative treatment with RN for RCC. However, patients should be appropriately counseled about the increased risk of complications with advancing age.
Footnotes
Authors' Contributions
All authors have sufficiently contributed to meet the authorship criteria.
Acknowledgments
We thank Paul Bassett for assistance with statistical analyses. On behalf of BAUS, we thank all surgeons who have contributed to the nephrectomy database.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.