
Abstract
Introduction:
Urinary tract infection (UTI) should be treated before percutaneous nephrolithotomy (PCNL). However, the most appropriate treatment strategy in patients with negative urine culture but positive urine dipstick infection test (positive urinary leukocyte or nitrite reaction) remains unclear.
Materials and Methods:
From August 2016 to February 2018, 806 consecutive patients who had undergone the first-stage PCNL with negative urine culture were included. Preoperative urinalysis, antibiotic treatment, intraoperative stone culture, and postoperative systemic inflammatory response syndrome (SIRS) were prospectively recorded. The primary outcome was SIRS. The impact of preoperative antibiotics on preoperative UTI, stone culture, and postoperative SIRS was studied.
Results:
Among the 806 participants, the rate of positive urine dipstick infection test and SIRS were 26.8% and 7.2%, respectively. In univariable analysis, positive urinary nitrite (p < 0.001), positive urinary leukocytes (p < 0.001), positive urine dipstick infection test (p < 0.001), longer duration of pre-PCNL antibiotics (p = 0.001), higher level of pre-PCNL antibiotics (p = 0.010), infection stones (p = 0.001), and positive stone culture (p < 0.001) were risk factors for SIRS. However, multivariable analysis showed that positive stone culture (p = 0.004) and prolonged preoperative treatment with antibiotics (p = 0.021) were independent risk factors for SIRS. Although preoperative antibiotics reduced the incidence of positive urine leukocyte (p < 0.001) or nitrite reactions (p < 0.001), prolonged or upgraded preoperative antibiotics did not affect the incidence of positive stone culture. Whether stone culture was positive (p = 0.023) or negative (p = 0.025), prolonged preoperative treatment with antibiotics was associated with a higher incidence of SIRS.
Conclusions:
Enhanced preoperative antibiotic treatment based on positive urine dipstick infection tests was insufficient to reduce the incidence of positive stone culture but increased the risk of SIRS after PCNL in patients with negative urine cultures.
Introduction
Percutaneous nephrolithotomy (PCNL) is the standard minimally invasive procedure for the removal of renal stones >2 cm. 1 However, postoperative infection is the most dangerous complication after PCNL. 2,3 The 2020 European Association of Urology (EAU) guidelines established that preoperative urinary tract infection (UTI) is a major risk factor for urosepsis, 1 and it was emphasized that once observed, preoperative UTIs should be controlled whenever stone removal is planned. 1 Meanwhile, a positive urine dipstick infection test (either positive urinary leukocyte or nitrite reactions) reflects the presence of UTIs. 2 The literature has shown that positive urinary infection tests are associated with a high risk of postoperative infections, such as systemic inflammatory response syndrome (SIRS) and urosepsis. 1,2,4 –8 Our recent results also showed that preoperative positive urinary infection tests are associated with positive stone culture, which independently increases the risk of postoperative infection 3 to 10 times. 1 Therefore, patients with positive urine dipstick infection test should be treated preoperatively. Currently, 21% to 39% of urologists in North and South America, Asia, and Europe empirically give prolonged antibiotics to those patients. 9,10 However, prolonged preoperative treatment with antibiotics associated with considerable side effects. 9,11 Precedentedly, no guidelines or literature notes are addressing the strategy of preoperative antibiotics to patients with positive urine dipstick infection tests and negative urine culture. Therefore, we conducted this study to fill that knowledge gap by analyzing the quantitative effects of different levels and durations of pre-PCNL antibiotic therapy on perioperative infections in those patients.
Patients and Methods
Type of study and participants
This retrospective cohort study was approved by the Institutional Review Board of the First Affiliated Hospital of Guangzhou Medical University. From August 2016 to February 2018, consecutive patients with negative urine cultures who had undergone the first-stage PCNL were included. They were found to have nephrolithiasis in the outpatient department and had not received stone-removal procedures in this episode of renal stone disease. Patients with preoperative SIRS, fever, or antibiotics within the last month preceding admission to the inpatient department were excluded.
Protocol
All patients were examined preoperatively with midstream urine cultures, urine routine dipstick test, blood routine analysis, and noncontrast CT on the day when they were admitted to the inpatient department. As antibiotics should be given before PCNL, the choice of preoperative antibiotic agent and duration were empirically decided by the surgeons according to local general hospital recommendations. For the lack of consensus, patients with negative or positive urine dipstick infection tests may receive single- or multidose antibiotics. If a patient was given multidose preoperative antibiotic therapy, a re-examination of urine dipstick would be carried out preoperatively. Multidose preoperative antibiotics therapy started on days before PCNL, whereas single-dose were used within 30 minutes before anesthesia of PCNL surgery. All patients were operated in the prone position with the access acquisition technique of stepwise facial dilatation to 18F to 20F. Stone specimens were collected and ground aseptically for bacteria culture. 4
Outcomes and measurements
Perioperative data of the participants were prospectively registered and retrospectively reviewed. The primary outcome was the development of postoperative SIRS. The diagnosis of SIRS was established if at least two of the following criteria were met within 6 days after PCNL: axillary temperature >38°C or <36°C, heart rate >90/min, respiration >20/min or PaCO2 <32 mm Hg, and blood leukocytes >12 × 109 or <4 × 109/L. 8 Blood routine analysis was repeated in all patients within 24 hours postoperatively. Positive urine and stone cultures were defined as bacterial colonies ≥105 CFU/mL. The number of urinary leukocytes in the resuspended urine sediment after centrifugation was quantified by counting cells in high-power (10 × 40) microscopic fields. 4 The average occurrence of urinary leukocytes per high-power field was graded as follows: 0–5 (score 0), 6–10 (score 1), 11–15 (score 2), 16–20 (score 3) and >20 (score 4). According to antibiotic generation and antimicrobial effect, three levels were defined: I, II, and III. The I level included: second-generation cephalosporin (cefuroxime) and third-generation quinolone (ciprofloxacin and levofloxacin). The II level included third-generation cephalosporin (cefoperazone sulbactam), cefoperazone and sulbactam, and fourth-generation quinolone (moxifloxacin). The III of antibiotics was carbapenem (imipenem and meropenem). The compositions of all stone specimens were identified by the infrared absorption technique. The patient was considered to have an infection stone when a major part of the stone specimen was composed of carbonate apatite, magnesium ammonium phosphate, or ammonium urate, 1 instead of stones with a positive bacteria culture.
Data analysis
SPSS Software 20.0 (IBM, USA) was used for statistical analysis. The strategy of analysis consisted of two parts. The first part was the univariable and multivariable analysis of risk factors for SIRS. The second part was to elucidate the detailed thorough effect of different durations and levels of preoperative antibiotics on preoperative urine dipstick infection tests, intraoperative stone culture, and postoperative SIRS. To test the results rigorously, stratified analysis and multivariable analysis were carried out. The patients were stratified by an independent risk factor for SIRS so that major bias was controlled and every member inside one same subgroup had a comparable baseline value. And subgroup analysis was only conducted inside each subgroup, in which way the results would be more valid. Continuous variables were described by mean (standard deviation) or median (quartile). Categorical values were reported as frequency (rate/ratio). Urine leukocyte score and level of antibiotic treatment were ordinal variables and analyzed by the Spearman Mann–Whitney U test. p Values were calculated by Student's t-test or Mann–Whitney U test for continuous variables and chi-square test for categorical variables. Logistic regression was utilized for univariable and multivariable analysis. Two-tailed p-value ≤0.05 was defined as statistically significant.
Results
Among the 806 participants, preoperative positive urine dipstick infection tests were recorded in 216 (26.8%) patients. Patients who received multidose preoperative antibiotics in urine dipstick infection test negative and positive subgroups took 60.8% (359/590) and 92.6% (200/216), respectively (Fig. 1). Overall, postoperative SIRS developed in 58 (7.2%) patients. The incidence of SIRS was 3.9% and 5.6% in patients with negative urine dipstick infection tests treated by single- and multidose preoperative antibiotics, respectively. And postoperative SIRS develop in 6.3% and 14.0% of patients with positive urine dipstick infection test treated with single- and multidose of preoperative antibiotics. No death was reported.
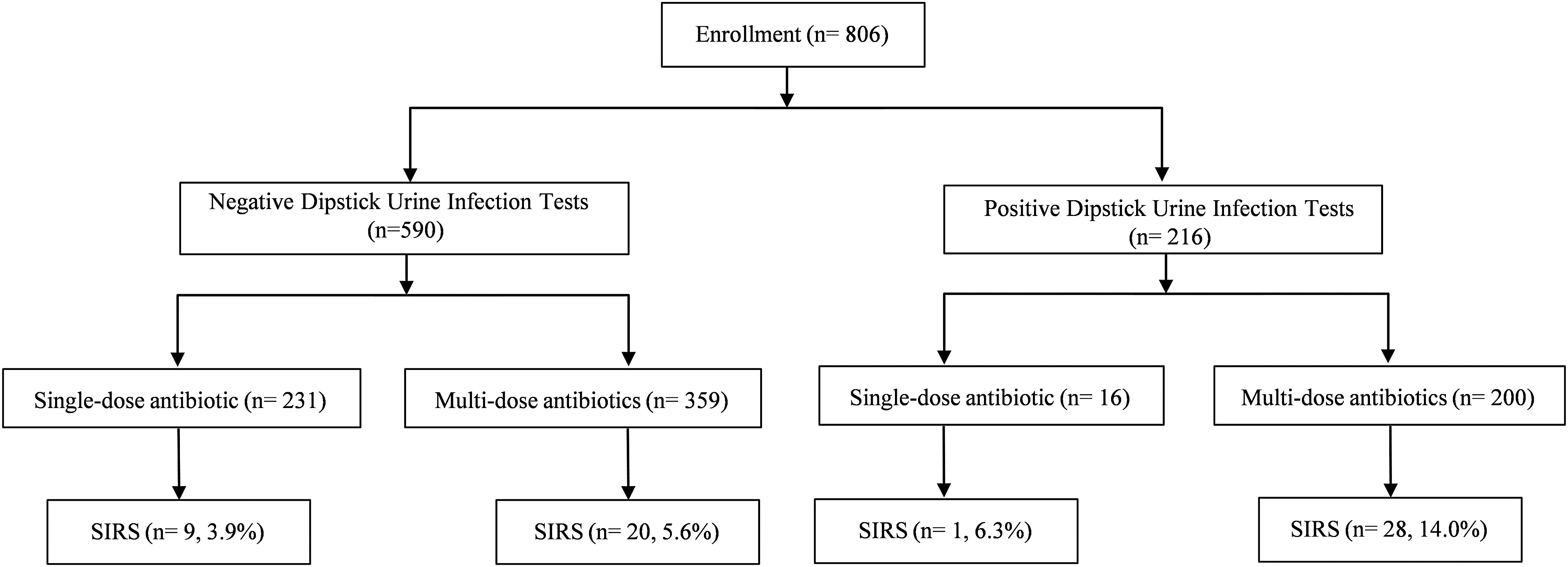
Flowchart of this study.
In univariable analysis (Table 1), positive urine leukocyte test (p < 0.001), high urine leukocyte score (p < 0.001), positive urine nitrite test (p < 0.001), higher levels of pre-PCNL antibiotic therapy (p = 0.010), presence of infection stones (p = 0.001), and positive stone cultures (p < 0.001) were all risk factors for postoperative SIRS. Compared with patients without SIRS, those who developed postoperative SIRS received a longer duration of preoperative antibiotic therapy (3 days vs 2 days, p = 0.001). Further multivariate logistic regression analysis showed that only positive stone culture (p = 0.004, odds ratio [OR] = 2.938, 95% confidence interval [CI] 1.587–5.438) and elongated duration of pre-PCNL antibiotic therapy (p = 0.021, OR = 1.139, 95% CI 1.020–1.272) were independent risk factors for postoperative SIRS (Table 2). The risk of postoperative SIRS increased to 1.139 times with every 1-day elongation of preoperative antibiotics duration.
Univariable Analysis of Postoperative Systemic Inflammatory Response Syndrome
p with # were tested by Mann–Whitney U test. p values in bold are statistically significant (p ≤ 0.05).
SIRS = systemic inflammatory response syndrome.
Multivariable Logistic Regression Analysis for Postoperative Systemic Inflammatory Response Syndrome
CI = confidence interval; OR = odds ratio.
After preoperative antibiotic therapy, the frequency of positive urine nitrite (p < 0.001) and leukocyte (p < 0.001) decreased significantly (Fig. 2). The urine leukocyte score was also reduced significantly (p < 0.001).
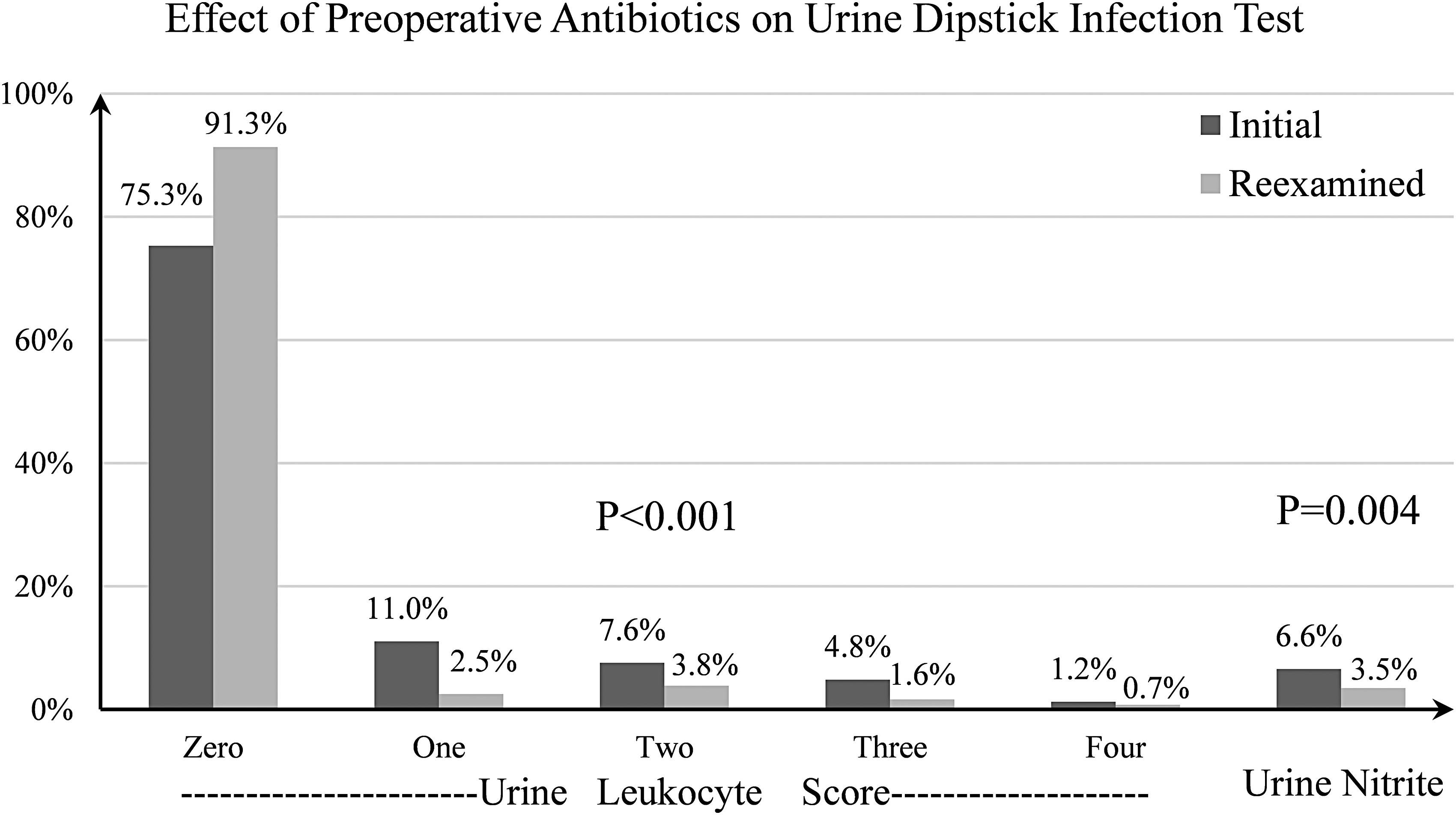
The effect of pre-PCNL antibiotics on urine dipstick infection test in patients with initial positive urine dipstick infection test. The data of urine leukocyte score were analyzed by paired Mann–Whitney U test. The data of urine nitrite were analyzed by paired chi-square test. PCNL = percutaneous nephrolithotomy
Both positive urine leukocyte and nitrite were associated with positive stone culture (p < 0.001; Fig. 3). Therefore, to test whether preoperative antibiotic therapy can eradicate the bacteria inside stones, the patients were stratified into two groups: positive urine dipstick infection test subgroup and negative urine dipstick infection test subgroup to make the intra-subgroup baseline of positive stone culture rate comparable. The effect of different periods and levels of preoperative antibiotic therapy on the stone culture positivity was only tested inside each subgroup. However, inside each subgroup with positive or negative urine dipstick infection tests, there was no difference in the rate of positive stone cultures between patients who received different durations or different levels of preoperative antibiotic therapy (Fig. 4).

The predictive value of pre-PCNL urine dipstick infection test on positive stone culture and postoperative SIRS. *p < 0.001. SIRS = systemic inflammatory response syndrome.
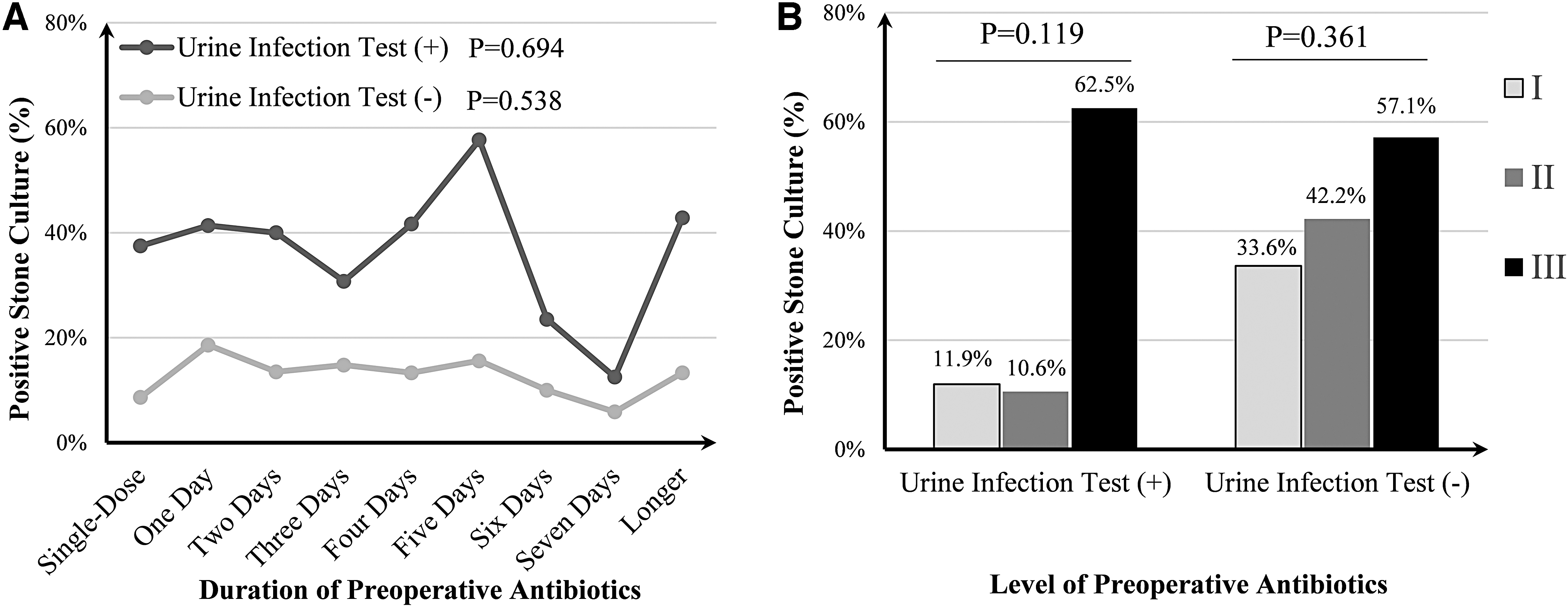
The effect of preoperative antibiotic therapy on the incidence of positive stone culture. The number of the patients who received pre-PCNL treatment with antibiotics as single-dose, or treatment 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 12, and 13 days were 247, 131, 109, 93, 81, 58, 37, 25, 12, 3, 4, 4, and 2, respectively. Because the number of patients who received antibiotics ≥8 days was so small, they were combined as “longer.” The data in
Since positive stone culture was a major independent risk factor for SIRS, to balance its impact, the patients were stratified into stone culture-positive subgroup and stone culture-negative subgroup. Irrespective of negative (p = 0.025) or positive stone culture (p = 0.023), a longer duration of preoperative antibiotic treatment was associated with a higher risk of postoperative SIRS (Fig. 5).

The impact of duration of preoperative antibiotics on postoperative SIRS stratified by positive and negative stone culture. The data were analyzed by univariable logistic regression.
Discussion
The original intention of this study was to fill the knowledge gap of how patients with pre-PCNL positive urine dipstick infection tests should be treated when the urine culture was negative. It turned out that positive stone culture and prolonged duration of preoperative antibiotic therapy were independent risk factors for SIRS.
In patients with positive stone culture, the uropathogens determined the outcome of urine dipstick infection tests and triggered postoperative infection in patients with a negative urine culture. Since PCNL causes renal bleeding trauma, bacteria released from stones can enter the blood circulation intraoperatively to trigger infectious complications. 2 Other factors such as female gender, increased pressure in the renal collecting system, high urine leukocyte score, positive urine nitrite, hydronephrosis, and infection stones all exert an influence on postoperative SIRS by affecting the number of bacteria and endotoxins leaking into the blood circulation. Our results showed that preoperative therapeutic antibiotics alleviated the rate of urine nitrite and leukocyte scores possibly because antibiotics reduced the burden of bacteria in the urine. However, preoperative antibiotics did not reduce the incidence of positive stone culture, neither by longer treatment duration nor by choosing antibiotics of higher levels. Accordingly, preoperative antibiotics cannot prevent the release of bacteria and endotoxins from stones during operation, and thus fail to prevent postoperative SIRS.
Some reports have claimed that 7 days of pre-PCNL antibiotics reduced the rate of positive stone culture. 8,12 –14 Such an effect was, however, not consistent with results by others or us. 15 –17 A probable explanation for our finding is that protective stone layers hinder antibiotics from reaching sufficient concentrations inside the stones. Accordingly, without sufficient concentrations of antibiotics, the interior of the stones cannot be sterilized. 18 In fact, it has been shown that even the mere bacteria biofilm, which is much thinner than stones, can protect the bacteria inside by preventing the diffusion of antibiotics. 19 UTIs associated with catheter encrustations cannot be cured unless the catheters are removed because of the biomineralization in bacterial biofilms. 20 A similar mechanism might be valid for the resistance of stones against diffusion of antibiotics. It is of fundamental clinical interest to further examine rigorously whether bacteria in urinary stones can be treated effectively by preoperative antibiotics.
Interestingly, a longer duration of preoperative antibiotic treatment was independently associated with a higher risk of SIRS. Those results are consistent with the report by Gupta et al. 11 They found that preoperative antibiotic treatment not only failed to reduce the risk for postoperative UTIs but also increased the risk of Bacillus fragilis diarrhea in patients with negative urine culture but positive urine pyocytes. 11 Prolonged preoperative antibiotic treatment may also cause drug resistance in bacteria. 9 Because of the barrier effect of stone layers, 18 the antibiotics not only failed to eradicate bacteria inside stones but also induced the development of drug resistance. 21 Since enhanced preoperative antibiotics cannot reduce positive stone culture rate and were associated with a higher rate of postoperative SIRS, a single-dose preoperative antibiotic was recommended.
To our knowledge, this is the first report of a preoperative antibiotic strategy specifically for patients with positive urine dipstick infection tests and with a negative urine culture. Our results suggest the term “stone-related antibiotic-refractory UTIs,” which cannot be controlled unless the stones are removed. Therefore, it is necessary to distinguish between the predictive and treatment values of preoperative positive urine dipstick infection tests. It is also novel and notable information that postoperative SIRS was possible to predict by urine dipstick infection tests but impossible to prevent by preoperative antibiotic treatment when urine was sterile. Because of the predictive value, urine routine analysis is recommended preoperatively.
This report is a single-center experience with a relatively small number of patients. Also, the study was a little complex so that multivariable and stratified analysis were used.
Conclusion
Positive stone culture and elongated duration of preoperative treatment with antibiotics were independent risk factors for postoperative SIRS when the urine culture was negative. Although pre-PCNL antibiotics alleviated positive urine dipstick infection tests, they did not reduce the incidence of positive stone cultures. Consequently, enhanced treatment was even associated with an increased risk of developing SIRS after PCNL in patients with a negative urine culture. Accordingly, a single-dose antibiotic should be recommended for patients with negative urine culture, regardless of the result of the urine dipstick infection test.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Guangdong Provincial Natural Science Project [2020A151501198], Key Project Of Guangdong Provincial Department Of Education [2018KZDXM056], and Guangzhou Medical University High-level Construction Project [201716007].