
Abstract
Objective:
To determine patterns of kidney and retroperitoneal organ movement during positional change between the supine and prone positions as seen on CT scans.
Methods:
Axial CT scans of 75 subjects who underwent supine and prone positions were retrospectively analyzed. A total of 1650 measurements were taken for anterior/posterior, medial/lateral, cranial/caudal, skin-to-calix distance, kidney-to-liver distance, and kidney-to-colon distance in both positions.
Results:
Pronation shortens the distance from the skin to renal calix for both the right (99.62 mm vs 85.14 mm; p < 0.00001) and left (96.67 mm vs 90.80 mm; p < 0.00001) sides. The reduction in left-side tract length for obese patients is significantly greater than that of normal weight patients (11.88 mm vs −5.02 mm; p = 0.001). The left kidney displaces ventrally (11.12 mm vs 18.59 mm; p < 0.00001), while the right kidney does not (14.26 mm vs 15.30 mm; p = 0.30). The right kidney displaces cranially (62.76 mm vs 79.51 mm; p < 0.00001), while the left kidney does not (64.35 mm vs 66.52 mm; p = 0.14). The left kidney in females moves medially, while no change is seen in males (4.22 mm vs −0.48 mm; p = 0.0004). The left kidney in females displaces toward the descending colon, while it moves farther away in males (2.73 mm vs −2.01 mm; p = 0.011).
Conclusions:
Both sex and body mass index had effects on the movement of the kidneys upon pronation. The differences can be clinically useful to help pre- and intraoperative planning.
Introduction
Kidney stones affect an estimated 7% of adults worldwide, with some estimates ranging up to 15%. 1 The procedure of percutaneous nephrolithotomy (PCNL) was developed in the late 1970s and 1980s to remove renal stones larger than 2 cm. Historically, PCNL has been performed in a prone position. The prone positioning gives the surgeon better access to the retroperitoneum while avoiding intraperitoneal structures. 2 –4
CT imaging is most commonly performed with the patient in supine position, with eventual prone positioning in most cases during PCNL surgery. Due to the mobility of the kidneys and surrounding retroperitoneal structures, it is vital to know how these structures move on position change based on gender and body mass index (BMI). These factors have not been studied before in a standardized manner. This knowledge can be of clinical importance to help plan the procedure, limit fluoroscopic exposure, and prevent intraoperative complications. Therefore, the purpose of this study is to examine the movement of the kidneys and surrounding organs upon supine to prone position change.
Methods
Internal review board approval for data collection was obtained. Axial CT urograms at a single institution for any clinical indication were retrospectively analyzed. Facility-standard protocol involved repositioning patients from supine to prone for the excretory phase as the prone position fills the ureters better. Kidneys naturally move in the cranial/caudal (C-C) axis during a normal breathing cycle, so therefore, patients were instructed to hold their breath during inspiration. A single investigator measured distances in both positions for a total of 75 patients. These distances were then subtracted to calculate the differential movement of the kidneys when transitioning from the supine to prone position.
Measurements
Distance from skin to calix and subcutaneous fat thickness
The distance from the skin to the posterior calix of the inferior pole of the kidney was measured. This was evaluated as the straight-line distance from the posterior calix to the skin edge in line with the infundibulum of the calix (Fig. 1A). Also, the thickness of the subcutaneous fat was measured along this same line from the skin edge to the muscle (Fig. 1A). Posterior calix was used because this is the most common site used for access during PCNL. This led to a total of 600 renal measurements: 75 patients (150 renal units), 2 measurements per renal unit (supine and prone), and 2 variables measured (skin-to-calix and subcutaneous fat thickness).
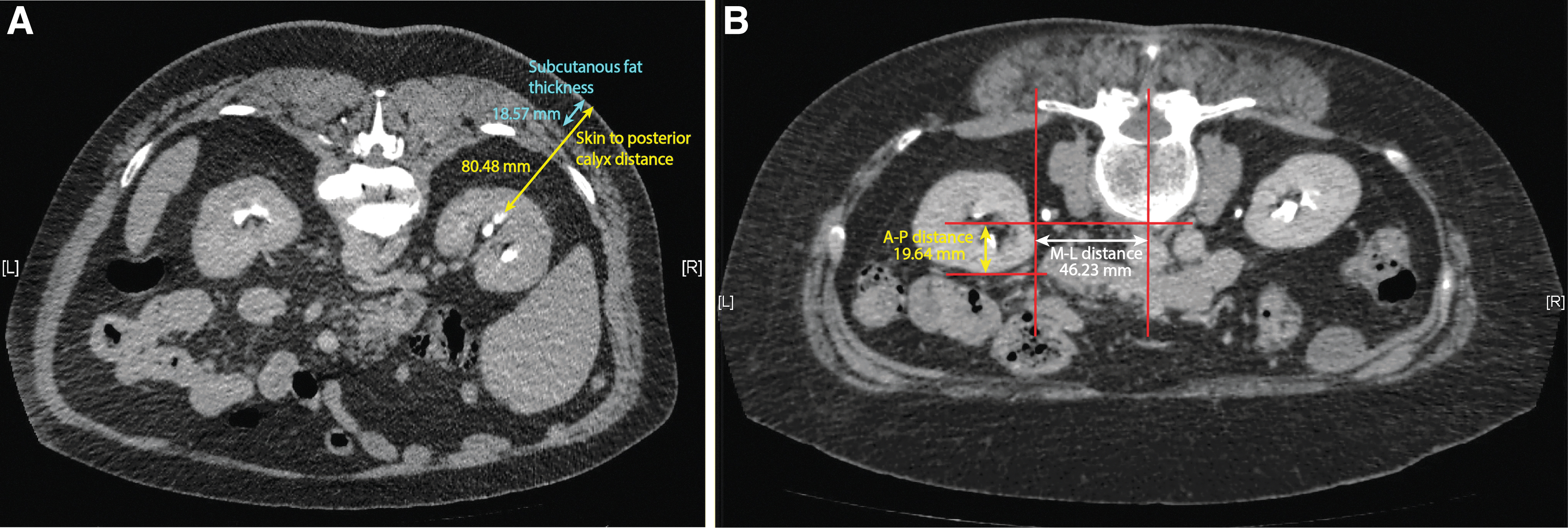
Kidney movement along three axes
The kidneys can move in three directions: anterior/posterior (A-P), medial/lateral (M-L), and C-C. The A-P measurement of the kidneys was defined as the distance from the anterior aspect of the kidney to the anterior aspect of the vertebral body (Fig. 1B). A more anterior kidney is ventral and closer to the anterior abdominal wall. We will use the terms anterior and ventral interchanged. The M-L measurement of the kidneys was defined as the distance from the medial border of the kidney to the midline of the vertebral body (Fig. 1B). A-P and M-L measurements were taken at level of inferior pole which was defined as the first CT cross-sectional image where hilum ended. The C-C measurement of the kidney was determined as the distance from the superior tip of the kidney to the tip of the 12th rib. This led to a total of 900 renal measurements: 75 patients (150 renal units), 3 axes, and 2 measurements per unit.
Distance from organs to kidney
Kidney movement was determined relative to other retroperitoneal structures at the level of the inferior pole. These included the distances from the right kidney to the ascending colon and liver, and the left kidney to the descending colon (Fig. 2A, B). This led to a total of 300 kidney/colon and 150 kidney/liver measurements.

Subjects were stratified based on sex and BMI. Statistical analysis was performed using GraphPad Prism version 8.4.2 for Windows, GraphPad Software, San Diego, CA,
Results
Pooled data
CT urograms of 75 patients were used for the study. Patient urograms were performed in the supine and prone positions.
We observed a significant reduction in right-side tract length when going from the supine-to-prone position (99.62 mm vs 85.14 mm; p < 0.00001). A less drastic change was seen on the left side but was still significant (96.67 mm vs 90.80 mm; p < 0.00001) (Table 1). The thickness of the subcutaneous fat was shorter in the prone position for both left and right kidneys (right: 43.76 mm vs 29.43 mm; p < 0.00001. left: 42.11 mm vs 31.52 mm; p < 0.00001).
Measurements of Right and Left Kidney Movement and Position
*Indicates statistical significance
A-P = anterior/posterior; C-C = cranial/caudal; M-L = medial/lateral.
The left kidney displaced ventrally (11.12 mm vs 18.59 mm; p < 0.00001) after pronation, while no difference was noted for the right kidney (14.26 vs 15.30 mm; p = 0.30). Movement of the kidneys along the M-L axis showed statistically significant movement bilaterally. However, the right kidney moved laterally (47.44 mm vs 48.97 mm; p = 0.033), while the left kidney moved medially (51.01 mm vs 49.62 mm; p = 0.042). The right kidney moved cranially (62.76 mm vs 79.51 mm; p < 0.00001), while there was no difference for the left kidney (51.01 mm vs 49.62 mm; p = 0.14) (Table 1).
The right kidney moved farther away from the liver in the prone position (35.31 mm vs 48.52 mm; p < 0.00001) and closer to the ascending colon (34.39 mm vs 39.74 mm; p < 0.00001). The left kidney remained a similar distance from the descending colon after positional change (45.04 mm vs 45.15 mm; p = 0.90) (Table 1).
Sex
Patients were separated into male (n = 45) and female (n = 30).
Right kidney movement on pronation
In both males and females, pronation shortened the right-side tract length. Also, the right kidney displaced cranially was farther from the liver edge and moved closer to the ascending colon (Table 2). The only difference, in females the right kidney displaced ventrally and in males it moved laterally (Table 2).
Effect of Gender on Movement and Position of Right Kidney
*Indicates statistical significance
Left kidney movement on pronation
Upon pronation, the left-side tract length shortened, and the left kidney displaced ventrally in both genders. However, in females there was significant medial movement after position change (Table 3).
Effect of Gender on Movement and Position of Left Kidney
*Indicates statistical significance
Magnitude of change males vs females
Next, we compared the magnitude of change between males and females. The right kidney did not show any significant findings.
There was a statistically significant difference in magnitude of movement along the M-L axis for the left kidney. In females it moved medially, while in males it did not. Also, in females the left kidney moved closer to the descending colon upon pronation, while in males it moved farther away (Table 3).
Body mass index
Patients were separated based on BMI: normal weight (18.5–24.9; n = 7), overweight (25.0–29.9; n = 25), and obese (30 and above; n = 35). BMI data were unavailable for eight patients.
Right kidney movement on pronation based on BMI categories
In patients of all three categories (normal weight, overweight, and obese), the right kidney had a shorter tract length, was more cranial, and the liver edge was displaced more laterally in the prone position. In overweight and obese patients, the right kidney was closer to the ascending colon in the prone position (Table 4). We observed a positive correlation between BMI and tract length in both the supine (R 2 = 0.46) and prone (R 2 = 0.54) positions for the right-side tract (Fig. 3A, B).

Effect of Body Mass Index on Movement and Position of Right Kidney
Indicates the statistical significance between the normal and overweight groups.
Indicates the statistical significance between the normal and obese groups.
Indicates the statistical significance between the overweight and obese groups.
*Indicates statistical significance
BMI = body mass index; ns = not significant.
Left kidney movement on pronation based on BMI categories
The only finding similar across all three groups was the left kidney displaced ventrally upon pronation. Obese patients had cranial displacement and shortening of the left-side tract length upon position change. There was a positive correlation between BMI and tract length in both the supine (R 2 = 0.58) and prone (R 2 = 0.48) positions (Fig. 3A, B, and Table 5).
Effect of Body Mass Index on Movement and Position of Left Kidney
Indicates the statistical significance between the normal and overweight groups.
Indicates the statistical significance between the normal and obese groups.
Indicates the statistical significance between the overweight and obese groups.
*Indicates statistical significance
Magnitude of change across BMI categories
There was a larger reduction in the left-side tract length in obese patients compared with nonobese patients. Also, the left kidney in obese patents displaced significantly less ventrally compared with nonobese patients (Table 5).
Discussion
To our knowledge, this is one of the largest studies (75 subjects) documenting relative and absolute renal displacement utilizing axial CT scans in supine and prone positioning of patients.
In this study, the tract length was statistically shorter in the prone position for both the kidneys, indicating dorsal (posterior) movement of the kidneys. Shorter tract length is important because it decreases torque on the kidney during rigid instrumentation, which can potentially lead to inadvertent fracture and bleeding. 5 –7
The reduction in tract length is most likely due to the less deformable nature of the posterior body wall compared with the anterior abdominal wall. 6 While prone, the backpressure exerted by intra-abdominal contents pushes the kidneys dorsally closer to the skin edge and pulls the subcutaneous adipose tissue toward the anterior body wall. We were able to show that subcutaneous fat thickness along the hypothetical PCNL tract is shorter in the prone position. However, when measured in relation to the anterior border of the vertebral body, both kidneys (statistically significant only for the left kidney) moved ventrally, that is, farther away from the skin edge. Prior studies also noticed this contradictory finding but were unable to reconcile it. 6,8 We hypothesize that upon pronation, compression of the kidney alters its morphology and relation to the skin. Compression laterally displaces the outer edge of the kidney and brings the calix closer to the skin edge, hence reducing the tract length. Also, lateral movement of the right kidney upon pronation brings it closer to the skin edge and confers a larger reduction in tract length (14 mm vs 5.8 mm) compared with the left kidney, which moves medial. Therefore, in the prone position, the kidneys are closer to the skin edge due to the synergistic effects of compression of the kidney (moving the lateral edge closer), movement of subcutaneous fat toward anterior body wall due to gravity, and lateral movement.
Previously reported reductions in length range from 13.7 to 31.7 mm for the right side and from 7.4 to 25.4 mm for the left side. 5 –9 The smaller reduction on the left side may be due to the attachment of the splenorenal and phrenicocolic ligaments to the left kidney, hindering its mobility. 10 We have shown that the prone position shortens the distance from the skin edge to renal calix. An interesting study by Yazici and colleagues observed that when the thickness of the subcutaneous fat was subtracted from the tract length, there was no difference in length when comparing the supine and prone positions. 7 We observed similar findings with shorter subcutaneous fat in the prone position. This indicates that the main factor in differences in tract length is the amount of subcutaneous fat. This might be an explanation for greater tract lengths in obese patients and a positive correlation between BMI and tract length.
The next key finding was the movement along the A-P axis. We observed the left kidney shifted anterior (ventrally) upon prone positioning, while the right kidney did not displace. Possible explanation could be less room to move due to the presence of the liver on the right side. Prior studies observed significant bilateral anterior displacement (3.5–7 mm for right kidney and 4.3–13 mm for left kidney), while we found this only for the left kidney. 6,8,11 However, in 2 of these studies, only 19 and 20 subjects were included, while we analyzed scans for 75 patients. A smaller number of patients included in those studies might have impacted their findings. Also, Lusch and coworkers measured from the posterior aspect of the vertebral body, while this study used the anterior aspect of the vertebral body. Difference in measurement technique could lead to discrepancies. One study conducted by Ball and coworkers reported more drastic changes, with displacement anywhere from 10 to 50 mm. 12 While our study showed statistically significant differences in A-P movement for the kidneys, the differences are minimal and do not need to factor into presurgical planning.
In our study, we found that the right kidney moved laterally upon pronation, while the left kidney moved medially. This differs from previously reported studies that showed no significant M-L movement of the hilum of the kidney for both sides. 7,8 The presence of vessels and lymphatics at the hilum hinders its mobility. 7 We hypothesize that upon pronation, the liver compresses and laterally displaces the right kidney. In females, the left kidney moved medially, but not in males. The right kidney moved lateral in males, with no displacement in females. We hypothesize that these differences might be due to a narrow costal angle in females affording less room for lateral displacement. 13 While there was a statistically significant movement in the M-L axis, there was minimal magnitude of displacement.
One of the most salient findings was cranial movement of the right kidney upon pronation (16.75 mm). Cranial displacement was observed in both genders and all BMI groups. However, there was no significant cranial movement of the left kidney (2.17 mm). Prior studies have reported cranial movement of the kidneys upon pronation with magnitudes of 22 to 29.8 mm for the right kidney, and 4 to 19.6 mm for the left kidney. 8,10,11 Guzzetta et al. reported similar findings with significant movement for the right kidney (22 mm), but insignificant movement of the left (5 mm). 11 This is important because access to the upper pole of the right kidney can be tricky with the patient in the prone position. This may potentially change a planned upper calix access from the subcostal to supracostal tract endangering the liver, lung, and diaphragm. These patients may benefit from preoperative imaging done in prone position.
An important finding was the increase in distance between the right kidney and liver edge in the prone position. A study by Pombo et al. reported similar findings, with a 2 cm increase in the distance from the kidney to liver edge after pronation at the level of the inferior hepatorenal space. 14 This is due to the liver displacing toward the left hypochondrium. We additionally hypothesize that pronation moves the liver edge away from the kidney by virtue of increased intra-abdominal pressure. At the same time, pronation displaced the right kidney closer to the ascending colon. This was seen across both sexes and all BMI groups. Therefore, the prone position potentially increases the risk for colonic perforation. However, meta-analyses of colonic complications show similar rates between the two positions: 0% to 3.3% for supine and 0.2% to 3.4% for prone. 15 –18
Gaining safe access to the kidneys during surgical procedures is important for effective outcomes and avoidance of complications. Prone positioning gives the urologist the best access to the retroperitoneum while avoiding intraperitoneal structures, and is most commonly used specifically for PCNL. 2 Some advantages of the prone position include better exposure of the lumbar area, easier access to the upper pole, and better endoscope mobility. 3,4 However, the supine position addresses many of the disadvantages of the prone position: better respiratory control, easier management for obese and heart failure patients, not needing to flip the patient over under anesthesia (which requires great care), and shorter operation times compared with prone-positioned PCNL. 19
One strength of this study is the number of patients included with 75 patients and 1650 total renal measurements; this study is one of the largest. Another strength is the standardized protocol of image acquisition (breath holding, slice thickness, etc.). This prevents inaccuracies in measurements between patients. Another strength is the use of a single investigator for taking measurements as this prevents interevaluator variability. One final strength is the use of bony landmarks wherever possible as they are incompressible and therefore optimal for measuring displacement. There are also some limitations to this study. These include varied indications for CT. This may impact the anatomy of the patient due to prior surgeries, infections, and so on. Lastly, these findings cannot be completely translated to the PCNL setting because during PCNL, patients are positioned with chest bolsters, table flexion, and so on, which might alter organ mobility seen in a purely radiologic setting.
Conclusion
In this study, comparison of kidney position and movement in the supine and prone positions showed potential clinically relevant findings. Knowledge of these anatomical changes between males and females as well as in BMI can be useful for surgical planning to achieve the best patient outcomes and limit intraoperative complications. While there are general trends, preoperative imaging in both the supine and prone positions might be helpful in pre- and intraoperative planning.
Footnotes
Authors' Contributions
A.D.: Study design, data collection, statistics and data analysis, writing and editing of the article. Z.C.: Data collection. D.G.: Study design and writing and editing of the article. B.S.: Statistics and data analysis. P.S.: Study design and writing and editing of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.