
Abstract
Introduction:
Office cystoscopy is one of the most frequently performed procedures by a urologist. However, single-use cystoscopes remain quite undeveloped. Ambu® has developed single-use broncoscopes, rhinolaryngoscopes, and duodenoscopes. Recently, they released a single-use cystoscope. In this study, we performed a benchtop and an initial clinical assessment of the Ambu aScope™ (4) Cysto (aS4C) single-use cystoscope.
Materials and Methods:
Ten new, never-used aS4C single-use cystoscopes were assessed for optical performance, maximal tip flexion, and irrigation flow rate with empty working channel, 365 μm laser fiber, 0.035 in hydrophilic-tipped wire, 1.9F nitinol basket, and a 1.8 mm flexible stent grasper. All cystoscopes were then fully flexed 25 times in each direction, and maximal flexion angles were remeasured with and without instruments. Optical resolution, distortion, and depth of field were measured and compared with our reusable digital flexible cystoscopes. Assessment of clinical use was performed for inpatient bedside procedures using a Likert feedback survey and the NASA Task Load Index.
Results:
Maximal upward flexion exceeded 200° and 160° for all working instruments in upward and downward flexion. Downward flexion demonstrated different flexion between instrument groups in pre- and postcycling (p < 0.001). There was no clinical difference between the pre- and postcycling flexion. Flow rate decreased with increasing working instrument size (p < 0.001). The Olympus HD cystoscope resolution was superior at 3 and 5 mm distance, but not at other distances. The Ambu scope was superior to the Olympus SD scope at all distances except 3 mm. The aS4C had higher Likert scale survey scores for clinical use.
Conclusions:
The new Ambu single-use cystoscope demonstrates good flexion across instruments and comparable optics with reusable cystoscopes. In addition, initial inpatient bedside use of the aS4C and Monitor system compares favorably with the Olympus reusable cystoscope. Further testing in clinical scenarios such as hematuria, urothelial carcinoma, and operative endoscopy is warranted.
Introduction
Cystoscopy is one of the most commonly performed procedures by urologists. Over time, cystoscopy has undergone several improvements in technology with flexible cystoscopes, evolution from standard-definition (SD) to high-definition (HD) video and advanced optics such as narrow-band imaging (NBI) and blue-light cystoscopy, and expansion beyond office diagnostics alone. 1,2 Cystoscopy is used to evaluate hematuria and lower tract voiding dysfunction, remove ureteral stents, and perform complex urethral catheter placement. 1 In addition, it remains a critical operative tool for surgical treatment of prostate and bladder pathology and calculus disease. However, drawbacks of reusable endoscopes include significant initial capital investment and repair costs, 3 –5 time and skilled labor resources for processing and cleaning, 6 as well as reports of multidrug-resistant infections through biofilm and other cleaning difficulties. 7,8
There are multiple commercially available and highly used single-use ureteroscopes. 9 Although there are single-use flexible cystoscopes available, 10,11 none has gained widespread traction. Ambu® (Ballerup, Denmark) has released and upgraded several versions of a single-use bronchoscope, rhinolaryngoscope, and duodenoscope, which have demonstrated comparable efficacy to reusable endoscopes. 12 –15 Ambu has recently released a single-use cystoscope called the aScope™ (4) Cysto 16 (aS4C), designed to perform all tasks of reusable flexible cystoscopes. We performed benchtop physical and optical testing with comparative optical testing to our office and operating room flexible cystoscopes. In addition, we report our initial inpatient clinical use for urology consults at an academic tertiary-care center.
Materials and Methods
An Internal Review Board waiver was provided for this study. Ten new, never-used, single-use Ambu aS4C cystoscopes were assessed for physical, functional, and optical performance. Maximal upward and downward flexion was measured with an empty working channel and with insertion of a 365 micron (μm) Moses™ laser fiber (Lumenis, Yokneam, Israel), a 1.9F Zero Tip™ nitinol basket (Boston Scientific, Marlborough, MA), 0.035 inch (in) straight-tipped Sensor™ wire (Boston Scientific), and a 1.8 millimeter (mm) flexible stent grasper (Advanced Endoscopic Devices, Canoga Park, CA). In addition, our current inpatient HD (CYF-VH) and SD (CYF-V2) Olympus (Tokyo, Japan) digital flexible cystoscopes were tested for maximal upward and downward flexion with an empty channel for comparison. Irrigation flow rate with an empty working channel and insertion of the same instruments in the aS4C was measured using the Thermedx® FluidSmart® (Thermedx LLC, Solon, OH) Fluid Management System with inflow pressure set at 100 millimeters Mercury (mm Hg) with 0.9% saline. In addition, a single Olympus HD CYF-VH cystoscope was measured for flow rate with an empty channel at the same pressure settings. Flow into a graduated cylinder was measured after 30 seconds and normalized to a rate in milliliters (mL) per second. For each flow rate measured, the system was allowed to equilibrate for 30 seconds before measuring the flow rate. All Ambu cystoscopes were then fully deflected 25 times in each direction without any instruments in the working channel (50 total flexions), and maximal upward and downward flexion was remeasured with the same working instruments. The distance for a 365 μm Moses™ laser fiber to exit the tip of the cystoscope and become visible on the monitor was measured for both the aS4C and the Olympus digital flexible cystoscopes.
In vitro optical testing was then performed with the Ambu aS4C and the Olympus SD (CYF-V2) and HD (CYF-VH) outpatient clinic digital flexible cystoscopes. Resolution testing was performed with a 1951 United States Air Force (USAF) test pattern card (Edmund Optics, Barrington, NJ) at 3, 5, 10, 30, and 50 mm. Testing was completed using the manufacturers' respective proprietary monitors in a dark room to remove ambient light. Distortion was measured with a multifrequency grid distortion target where: Distortion = (Actual distance−Theoretical distance)/Theoretical distance × 100. Depth of field was determined using the Edmund Optics depth-of-field test target.
The aS4C was implemented as the cystoscope for inpatient bedside procedures during the severe acute respiratory syndrome coronavirus 2 (SARS-CoV2) pandemic 17 to reduce potential viral spread. Survey feedback was obtained from urology residents performing the procedure immediately before, and after the implementation of the aS4C. The prior bedside procedure cystoscope was the Olympus SD (CYF-V2) flexible cystoscope and a portable cart with mounted monitor. The Likert survey was scored from 1–5 (5 being best) on Visibility, Handling, Flexion, and Desire to Use Again. Summated Overall Score was also assessed. In addition, the NASA Task Load Index (TLX) 18 was taken after each inpatient bedside procedure. Scope usage was nonrandomized. The surveys were obtained with the final uses of the Olympus scope and the initial uses of the aS4C. Procedural and resident-specific details were obtained. The postgraduate year was converted to number of training days completed using a July 1st start date as the implementation of the Ambu aS4C was in the June-July academic year transition.
Statistical analyses using paired Wilcoxon rank-sum tests was performed for pre- and postcycling upward and downward flexion within the same working channel instrument; for optical resolution, distortion and depth of field comparing the aS4C with the HD and SD reusable cystoscopes, and for the Likert score and NASA TLX, between the aS4C and the reusable cystoscope surveys. One-way repeated-measures analysis of variance (ANOVA) with post hoc analysis was performed across the different working channel instruments for both upward and downward flexion in both pre- and postcycling groups and for the flow rates with working channel instruments. Analysis was completed in SPSS version 27 (IBM, Chicago, IL). Threshold for significance set at p < 0.05.
Results
The Ambu aS4C produced median flexion >200° in upward flexion and >160° in downward flexion while empty and with all instruments in the channel (Table 1 and Fig. 1). By comparison, the inpatient Olympus digital flexible cystoscopes had a median maximal upward flexion of 185.5° [183.2°–191.1°] and downward flexion of 105.7° [103.9°–106.8°]. The aS4C empty, Sensor™ wire, and 1.9F Nitinol basket all allow for downward flexion >170°. For the aS4C upward flexion precycling, there was no difference between working channel instruments [F(1.204–10.836) = 1.747, p = 0.217]. For downward flexion precycling, there was a difference among working channel instruments [F(2.628–23.656) = 135.470, p < 0.001]. On post hoc analysis, the 1.8 mm flexible grasper and 365 μm laser fiber had less downward flexion than the empty channel, Sensor wire, and 1.9F basket (all p < 0.001, respectively). In addition, the empty channel had greater downward flexion than the Sensor wire (p = 0.009).

Ambu ® aS4C cystoscope upward and downward median flexion pre- and postcycling. Error bars = IQR. *p < 0.05 for pre- and postcycling comparison within the same working instrument. aS4C = aScope™ (4) Cysto; IQR = interquartile range. Color images are available online.
Pre- and Postcycling Upward and Downward Average Flexion of Ambu aScope (4) Cysto Single-Use Cystoscope
Flow rate with various working channel instruments before flexion cycling. * p = 0.009; α = p = 0.009 on post hoc analysis relative to empty channel within precycling downward flexion; β = p < 0.001 on post hoc analysis relative to empty channel, 0.035 mm Sensor wire, and 1.9F basket within precycling, downward flexion; γ = p < 0.001 on post hoc analysis relative to empty channel, 0.035 mm Sensor wire, and 1.9F basket within postcycling downward flexion.
ANOVA = analysis of variance; IQR = interquartile range.
After 50 total deflections (25 cycles), there was only a statistical difference between the pre-/postcycling instruments in the downward flexion with the 1.9F basket (172.5° [170°–178°] vs 173.5° [171.25°–179.25°], p = 0.009), although this is of questionable clinical relevance. However, the empty channel and each instrument failed to meet the manufacturer's claim of >210° upward flexion. The median upward flexion for the empty channel and all instruments was ≥205°. All downward flexion exceeded the manufacturer's claim of >120° as the lowest median downward flexion was 163.0°. No scope failures were observed during flexion testing.
For upward flexion postcycling, there was no difference between working channel instruments [F(2.780–25.016) = 1.789, p = 0.178]. For downward flexion postcycling, there was a difference between working channel instruments [F(2.304–20.740) = 56.121, p < 0.001]. On post hoc analysis, the 1.8 mm flexible grasper and 365 μm laser fiber had less downward flexion than the empty channel, Sensor wire, and 1.9F basket (all p < 0.001, respectively).
The irrigation flow rate (Table 1) was highest with an empty channel and decreased with introduction of various instruments through the channel [F(4–36) = 4263.385, p < 0.001]. On post hoc analysis, flow decrease was greater with larger sized instruments with the flexible stent grasper having the largest negative impact (all p < 0.001, respectively). Flow with the empty channel in the aS4C was 5.4 mL/s [5.3–5.4]. Flow from the tested Olympus HD cystoscope was 5.8 mL/s [5.8–5.9]. Flow rates in the aS4C were 4.1 [4.1–4.2], 3.2 [3.1–3.2], 3.1 [3.0–3.1], and 0.9 [0.8–0.9] mL/s for the 365 μm laser fiber, Sensor wire, 1.9F basket, and flexible stent grasper, respectively.
The Olympus HD flexible cystoscope demonstrated superior resolution at 3 and 5 mm distance, however, this was no longer evident at 10 and 30 mm distance (Fig. 2 and Table 2). Representative optical testing images of the aS4C are shown in Figure 3. The aS4C showed higher resolution to the HD cystoscope at 50 mm. The aS4C was superior to the Olympus SD flexible cystoscope at 5, 10, 30 and 50 mm. There was no difference at 3 mm. The aS4C and Olympus HD cystoscopes had similar depth of field. The aS4C had a superior depth of field compared with the Olympus SD cystoscope. There was no difference in the distortion between the Ambu aS4C and the Olympus HD or SD flexible cystoscopes.
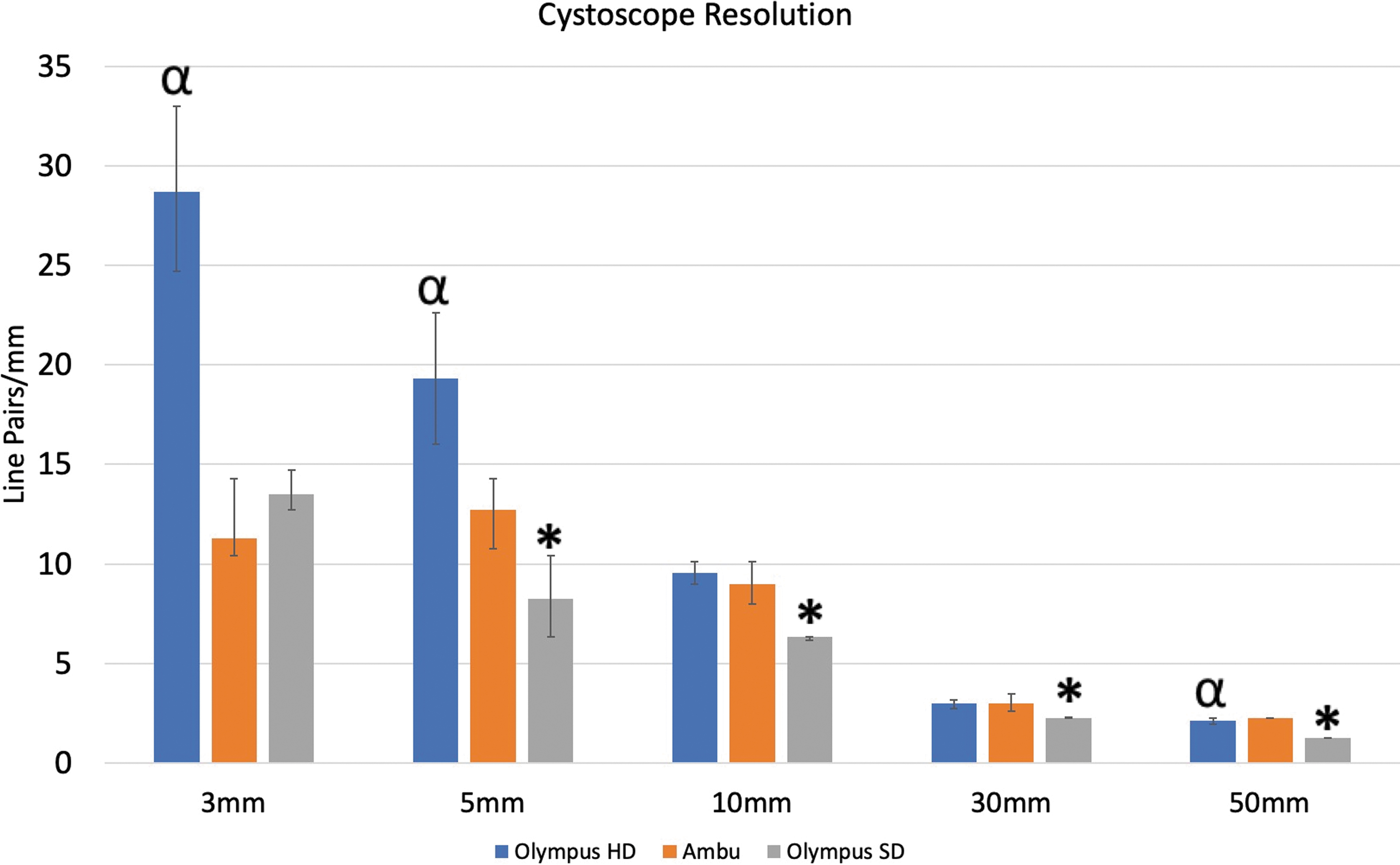
Ambu aS4C, Olympus SD and HD flexible cystoscope median resolution. Error bars = IQR. α = p < 0.05 for HD vs aS4C, *p < 0.05 for SD vs aS4C. HD = high-definition; SD = standard-definition. Color images are available online.

Single-Use Cystoscope Optical Resolution, Distortion, and Depth-of-Field Comparison
p < 0.05.
aS4C = aScope™ (4) Cysto; HD = high-definition; LP = line pairs; SD = standard-definition.
The distance measured for the 365 μm laser fiber to exit the scope and be visible on the screen was 5 [5–5] mm for the four measured Olympus cystoscopes and 4 [4–5] mm for the aS4C.
Survey data were recorded for 17 inpatient bedside procedures (n = 10 Ambu & n = 7 Olympus). The aS4C was rated higher on Visibility, Flexion, Desire to Use Again, and Overall Summated Score (Table 3) for inpatient bedside procedures. There was no need to convert to the reusable cystoscope for procedures and there were no reported complications related to the scopes. Procedure types were similar between groups (Table 4). Within the NASA TLX, the aS4C had a lower Frustration score (Table 3). A lower score in the NASA TLX indicates favorable scoring to each domain. There was no difference between any of the other domains or the overall score. There was no difference in the help from assistants, procedure type, urine appearance, or the number of completed postgraduate training days of the residents completing the procedures between the reusable and single-use cystoscopes.
Likert Scale User Feedback and NASA Task Load Index Comparison
* p < 0.05.
TLX = Task Load Index.
Inpatient Bedside Cystoscopy Indications of Ambu Single-Use and Olympus Reusable Cystoscopes
Discussion
The Ambu aS4C performs well in flexion, durability, and optical performance in this benchtop study. As per manufacturer specifications, aS4C is a single-use cystoscope with 210° upward and 120° downward flexion with 120° field of view. It has an outer diameter of 16.2F and a working channel size of 6.6F that exits at the 9-o'clock position on the tapered scope tip. 19 The camera is located at the tip with two light emitting diodes as the light source. The scope itself has an attached cord that plugs directly into the Ambu aView™ 2 Advance HD 20 (1920 × 1080p), touch screen monitor with battery or wall-outlet power capability. The system is capable of taking still images and video with high-definition multimedia interface or 3G-Serial-Digital-Interface digital video outputs, Universal Serial Bus ports, and WiFi capabilities. 21 Our testing demonstrated that downward flexion exceeds the manufacturer's specifications, although did not quite meet the upward flexion as per product specification (5° less). This may be due to inherent differences between flexion measurement techniques between our testing and Ambu internal measurement as the total flexion range (maximum upward to downward) exceeded the manufacturer's specifications. However, there was no clinically appreciable difference in pre- and postcycling flexion capabilities within the same working channel instrument and no scope failures. Flexion did decrease about 10° with use of a 365 μm fiber and 1.8 mm flexible stent grasper in pre and postcycling measurements, although this is not unexpected given the stiffness and width of each instrument. The aS4C exceeded our current operating room flexible cystoscopes by about 20° and 70° in upward and downward flexion with an empty channel, respectively. Although none of the Olympus scopes was brand new, it is notable as reusable scopes likely lose flexion over time despite not being marked as necessary for repair. 22 We attempted to obtain the number of operative uses each flexible cystoscope had undergone since purchase, however, were unsuccessful due to lack of complete granular data. The tested reusable cystoscopes were purchased at least 5 years ago. One cystoscope had required seven repairs, however, the remaining cystoscopes only two or fewer repairs within the past 5 years. In most clinical scenarios, a brand new reusable scope is not available and the urologists must use what is at their disposal. This may raise the potential benefit of a “brand new” scope for each procedure that a single-use scope provides. 23 However, whether it translates from ureteroscopy to cystoscopy remains to be determined.
Flow in the aS4C decreased as expected with increasing instrument size. The aS4C had a slightly lower flow rate with an empty channel compared with the single tested Olympus HD cystoscope, despite an equivalent reported working channel size at 6.6F, although was not tested for statistical significance. This may be clinically insignificant in many scenarios. However, in difficult visualization due to hematuria or small working space, even the slightest of greater flow rates may prove useful. However, this study was not designed to capture that difference. Although the Olympus HD cystoscope outperformed the aS4C resolution at 3 and 5 mm, this was no longer evident at >10 mm. How much of clinical benefit at 3 and 5 mm standoff distance during cystoscopy remains unknown. Compared with a ureteroscope, where short standoff distances are more common, the cystoscope benefit would intuitively be less, however, must be further evaluated. The aS4C had superior resolution compared with the SD scope at all distances except 3 mm. Again, this benefit in benchtop testing remains unproven to clinical use. The depth of field was similar between the aS4C and the HD cystoscopes. The aS4C showed superior depth of field compared with the SD cystoscope. The distance for an instrument to exit the tip of the cystoscope and become visible on the monitor was similar between the aS4C and the Olympus scopes. Broadly speaking, the optical characteristics appear to be comparable with currently commercially available reusable flexible cystoscopes, although additional clinical testing is necessary to confirm this.
The aS4C compares similarly with recent benchtop testing of the Coloplast Isiris stent-grasper Cystoscope (Humlebaek, Denmark), Vision Science (Orangeburg, NY) CST 5000 EndoSheath single-use cystoscopes, the Olympus CYF-VH, CYF5, and Karl-Storz (Tuttlingen, Germany) 11272C1 reusable cystoscopes, where upward and downward flexion with an empty channel ranged from 100.41° to 218.10° and from 101.50° to 166.32°, respectively. 11 With insertion of a flexible stent grasper, this decreased to 100.81°–155.40° and 76.43°–113.11° for upward and downward flexion, respectively. 11 In our study, the aS4C demonstrated upward and downward flexion >200° and >160°, respectively.
In a benchtop study of the NeoFlex single-use cystoscope (NeoScope, Inc., Watsonville, CA), flexion was reported to be 285° and 270° for upward and downward flexion, respectively. 10 With a 365 μm laser fiber and 3F flexible stent grasper, upward and downward flexion decreased to 205° and 215°, and 75° and 70°, respectively. 10 The aS4C appears to have less flexion with an empty channel, however, comparable flexion with the tested working instruments in our study. Optical resolution was measured at 5.5 line pairs/mm at 10 mm, 10 while our testing of the aS4C demonstrated a superior resolution at this distance. Although conclusions across studies between single-use cystoscopes have inherent flaws, the aS4C appears at least comparable with other commercially available single-use cystoscopes.
Our initial inpatient clinical use for bedside procedures indicates that the aS4C may be a viable alternative to a reusable cystoscope system. On the physician feedback survey, the aS4C rated higher on each domain and the overall score of the survey. However, differences in rating were only noted in the Frustration index of the NASA TLX. Notably, our survey is not validated. Potential factors that are unaccounted for include the perception of equipment upgrade, the movement of the equipment necessary for a reusable scope, and tower setup vs the peel-pack of the aS4C, which may be independent of the physical function of the cystoscopes. In addition, it is possible that the technical feedback of the aS4C translated into the Frustration index, but not any of the remaining indices. Larger sample sizes are needed. In the clinical evaluation of the NeoScope (n = 25), scope passage, flexion, and color image were rated as “successful,” although three scopes reported poor light distribution and bright spots in one cystoscope. 10 One of the reported cases required switching to a reusable cystoscope. None of the procedures performed with the aS4C required conversion to the reusable cystoscope system, although it was a small procedural volume reported. The aS4C continues to be the primary flexible cystoscope used for inpatient bedside procedures at our institution and overall continues to gain positive feedback. Although not measured by any metric in our data, we have not received feedback that the aS4C results in additional pain or difficulty completing procedures due to material type, irrigation flow rates, stiffness, or flexion capabilities.
What remains to be known is the use of the aS4C for detection of urothelial malignancy and its use in bloody fields. To our knowledge, no comparative testing of urothelial malignancy evaluation with single-use cystoscopes has been performed. Given the advent of blue-light cystoscopy and NBI, further investigations into the appropriateness for urothelial malignancy surveillance are warranted. Historically, reports of poor vision in bloody fluid have been a complaint with single-use ureteroscopes 24 due to the use of complementary metal oxide semiconductor (CMOS) chips in single-use ureteroscopes vs charge-couple device imaging chips present in reusable digital ureteroscopes. CMOS are known to be more sensitive to red light, which affects the image in bloody fields. Color-checkered card testing in this study was felt to be limited without a blood-tinged fluid simulation and thus was not performed. No complaints of color artifact have been reported from clinical use. In addition, usage and reporting of bloody or simulated bloody aqueous environments should be performed.
The development of even the best physical and optical performing single-use cystoscope will always have the challenge of adopting widespread market use. Incorporation of single-use ureteroscopes has gained much larger acceptance than single-use cystoscopes. This fact is likely due to the high repair costs and relatively short usage period between initial purchase and first repair of a flexible ureteroscope. 5 However, flexible cystoscopy rarely requires the degree of torquing or manipulation that is asked of a ureteroscope. Prior study has demonstrated 134–495 office cystoscopies per failure depending on the processing and system management. 25 That is roughly 10- to 40-fold more procedures completed before first ureteroscope repair. 5 However, many institutions have now transitioned to high-level disinfection 26 requiring central instrument processing, which can increase costs and, at times, the availability of a flexible cystoscope. In addition, the flexible cystoscopy cart for inpatient procedures can be cumbersome to move depending on the setup. The Ambu aS4C flexible cystoscope and built-in cord plug directly into the Ambu aView 2 Advance HD Monitor (12 inches; can be battery operated). The Monitor has its own “kick-stand,” which can be placed on many flat surfaces. The setup may allow for easier inpatient use when navigating multiple cords or lines in a patient room compared with a wheeled tower system.
Costs, financial efficiency, and even environmental impact are continuously scrutinized in health care systems. Each individual health care system, hospital, and practice are unique and have their own challenges to overcome. 3 Single-use vs reusable flexible ureteroscopes have been the most well studied in urology, with differing outcomes depending on procedural volumes, reprocessing time, and delay costs. 3,5,27,28 A recent microcost analysis was performed using the Isiris single-use flexible cystoscope and grasper stent removal system. Using the Olympus HD flexible cystoscope, annual servicing contract, reprocessing and labor costs, and sterilization contract and costs at a tertiary care center, a cost of $161.85 per office cystoscopic ureteral stent removal was calculated compared with the purchasing cost of the Isiris device at $200.00. 29 The break-even point number of procedures was determined to be 705 stent removals. 29 Fewer than this per year would favor the Isiris system as potentially being more cost effective. 29 Another microcost study of the Isiris system from the United Kingdom showed the Isiris to be £252.62 vs £267.20 for the reusable flexible cystoscope. 30 However, as the Isiris system is only used for stent removal, the effect of a single-use, single-procedure device on the overall impact of office cystoscopy device longevity, repair, and efficiency is yet to be studied. Prior studies have shown that the distal deflection tip is the most common area of required repair (28%), which can cost up to $1370 per type of repair needed. 31 A single-use cystoscope avoids the need for repairs. However, in an ever increasing environmentally conscious world, practitioners and providers alike may be concerned with the increased waste created with each single-use device. In a study evaluating carbon-footprint per flexible ureteroscopic case, the Boston Scientific LithoVue (Marlborough, MA) and Olympus Flexible Video Ureteroscope (URV-F) compared favorably with 4.43 kg CO2 vs 4.47 kg CO2 per endourologic case, respectively. 32 However, given that office cystoscopy is more commonly performed than flexible ureteroscopy, the environmental impact may be different for cystoscopic procedures. To our knowledge, no known environmental impact of single-use cystoscopes has been performed.
Our current study is limited by its benchtop assessment as clinical scenarios were not recreated. Much of what was tested was applicable for office cystoscopy. The inpatient bedside procedures were limited to a small volume and no operative procedures were performed. It is unknown if certain difficulties will arise in more complicated bedside or operative procedures. At times, these procedures can be in bloody environments, require more manual torquing, and involve use of a laser, which can create image interference. In our study, the scopes were flexed in free space rather than torqued against resistance, were not tested in an aqueous or bloody environment, and lasers were not used; we therefore cannot conclude how different clinical scenarios would affect the aS4C function. Nonetheless, it appears that the Ambu aS4C performs well in benchtop testing and in limited inpatient bedside cystoscopic procedures. Although benchtop testing serves as an initial evaluation of a recently introduced device, it does not replace a well-conducted clinical study. We hope that with multiple single-use cystoscopes now available, direct clinical comparison of these products can be performed. Further clinical testing and economic and environmental analysis are warranted to determine the depth to the ability of the Ambu aS4C single-use cystoscope to emerge as a viable cystoscope.
Conclusions
The Ambu aS4C is a new single-use flexible cystoscope that demonstrates sufficient benchtop flexion capability and durability with comparable optics to commercially available HD and SD flexible cystoscopes. Further clinical and economic study should be performed.
Footnotes
Authors' Contributions
P.W., C.K., and C.T. contributed to the project design, testing, statistical analysis, and article writing and editing. G.M.P. and M.E.L. contributed to project design, article writing and editing, and final approval.
Author Disclosure Statement
P.W., C.K., and C.T. have no conflicts of interest to disclose. G.M.P. is a consultant for Boston Scientific, Auris Health, and Kalera Medical. M.E.L. is a consultant for Boston Scientific and Lumenis.
Funding Information
Ambu® provided the single-use Ambu® aScope™ (4) Cysto flexible cystoscopes and Ambu® aView™ 2 Advance HD Monitor for completion of this study.