
Abstract
Background:
The creation and dilatation of the nephrostomy tract is a fundamental step in percutaneous nephrolithotomy (PCNL). In one-shot dilatation (OSD), we used a single Amplatz dilator over a central Alken rod. PCNL in the supine position is as effective and safe as in the prone position. The Barts flank-free modified supine position sums several advantages of the different supine positions. We evaluated the efficacy and safety of OSD compared with metal telescopic dilator (MTD) during PCNL while the patient was in Barts flank-free modified supine position.
Materials and Methods:
Within 2.5 years, 150 patients with kidney stone candidates for PCNL were randomized into two equal groups according to the dilatation technique. In the OSD group, dilatation was performed using a single Amplatz dilator (30F) and in the MTD group dilatation was performed by sequential MTD (9–30F). All PCNL procedures were done with patients in Barts flank-free modified supine position. Patient characteristics, operative data, and results were collected for statistical analysis.
Results:
There are no statistically significant differences between both groups regarding patients' characters. The tracts were effectively dilated in all patients. Statistical analyses show a significant difference (p ˂ 0.05) between both groups regarding the time of dilatation (seconds; 68 ± 15 vs 147 ± 18), time of X-ray exposure (seconds; during dilatation; 36 ± 10 vs 61 ± 15 and the total; 157 ± 16 vs 181 ± 20), hemoglobin loss (mg/dL; 0.7 ± 0.2 vs 1.2 ± 0.3), and hospital stay (days; 3 ± 0.6 vs 3.7 ± 0.7) with favorable results to OSD. Complication rates were comparable between the two groups.
Conclusions:
OSD is efficient as MTD during PCNL while patients are in Barts flank-free modified supine position, with less dilatation time, X-ray exposure, blood loss, and hospital stay than MTD.
Introduction
Currently, percutaneous nephrolithotomy (PCNL) is the treatment of choice for managing large renal stones measuring ≥2 cm. 1
Dilatation of the percutaneous tract and insertion of the access sheath is a crucial step in this operation and is performed using two different techniques. First, the multiple incremental dilators, either Amplatz sequential facial dilators or Alken metal telescopic dilator (MTD), with the hazards of a longer access time, longer duration of X-ray exposure, and increased incidence of tract displacement. MTD is reusable and thus more economical, and it maintains a tamponed effect throughout the dilatation. Second, the balloon dilator has the advantages of shorter dilatation time and less fluoroscopy time, but it is expensive, especially in developing countries. 2,3 Each technique has its own advantages and disadvantages. 3,4
Frattini published his new technique, one-shot dilatation (OSD), for tract dilatation by using a single Amplatz dilator (30F) over a central Alken rod, which combines the advantages of all previous techniques for dilatation. 5 Later, several investigators reported on the efficacy and safety of this technique (even in patients with a history of previous open kidney surgery) with a significantly shorter access time, less X-ray exposure time, and less blood loss than the gradual dilator. 4,6 –10
For several years, the prone position was the only position used for PCNL. It was initially considered by many to be the safest approach to the kidney. However, this position has some disadvantages for patients, anesthesiologists, and surgeons. The necessity for position changes during the procedure is another disadvantage of this position. The rising number of PCNL procedures combined with increasing confidence and surgical experience has encouraged researchers to modify the prone position for PCNL to improve results and overcome prone position-related obstacles. 11 –14
Since 1998, Valdivia and colleagues presented their first clinical experience for PCNL in the supine position, with several advantages for patients, surgeons, and anesthesia-related complications. Many meta-analyses have reported that supine PCNL is comparable with prone regarding stone-free rate, blood transfusion rate, and complication rate, with shorter operative time, less X-ray exposure, and performed while the surgeon is sitting. 13 –17
Later, several modifications were made for this technique, to improve its effectiveness and allow for simultaneous ante- and retrograde renal access without changing the patient's position. There is no consensus on the ideal supine position. 12,18 –20
This study aimed to compare the OSD technique and Alken metal telescopic dilator for PCNL tract dilatation regarding efficacy and safety while the patient is in Barts flank-free modified supine position.
Materials and Methods
Our ethics committee board approved this study (Number 53; 8/10/2017), and all patients provided written informed consent. Between December 2017 and March 2020, 150 patients with renal stone candidates for PCNL were prospectively enrolled and randomized by 1:1 allocation using random block sizes of 2, 4, and 6, to two equal groups, depending on the technique used for PCNL tract dilatation. In group 1 dilatation was performed using OSD, whereas in group 2 we used Alken MTD.
Inclusion criteria were renal stones ≥2 cm eligible for PCNL, whereas exclusion criteria included upper caliceal stones, staghorn stones, presence of associated ipsilateral ureteral calculi, kidney anomalies, and patients ˂18 years or body mass index >40 kg/m2.
Preoperative evaluation
Baseline data included medical and surgical history, physical examination, and laboratory and radiologic investigations. These include complete blood count (CBC), serum creatinine, urine analysis, urine culture/sensitivity, abdominal plain film (kidney, ureter, and bladder radiograph [KUB]), abdominal ultrasonography, intravenous urography, and/or noncontrast urinary tract computed tomography (NCCT). We measured the longest diameter of stone from KUB or NCCT for the stone size and in multiple stones, taking the sum of the longest diameter for all stones.
These parameters were collected for each operation, total operative time (from induction of anesthesia until insertion of the nephrostomy tube), time of tract dilatation (by seconds from the insertion of the safety guidewire until insertion of the Amplatz sheath 5 ), and X-ray time during tract dilatation, and time of X-ray exposure for the entire operation.
We assessed the success of tract dilatation (when we see the pelvicaliceal system [PCS] by the nephroscope through the access sheath), number of tracts used, success rate, hospital stay, and postoperative complications.
All operations were performed by two urologists with endourology experience of >8 years.
Operative technique
Before the start of the operation, we marked the last two ribs, the posterior axillary line (PAL), and the iliac crest when the patient was in a standing position. Under general anesthesia, all patients were placed in Barts flank-free modified supine position by placing the patient in a supine position with two suitable cushions for the affected side one under the ipsilateral rib cage and the other under the buttocks (to provide 15° inclination) aligning this flank to the edge of the operating table. The ipsilateral arm was placed over the chest, directed to the other side. The legs were placed in lithotomy position, with the ipsilateral leg relatively extended whereas the other leg was abducted. 19 This position permits a wider surface area for a renal puncture, with simultaneous ante- and retrograde manipulation of the kidney, Figures 1 –3.

Patient in Barts flank-free modified supine position. Color images are available online.

Retrograde ureteral catheter insertion. Color images are available online.
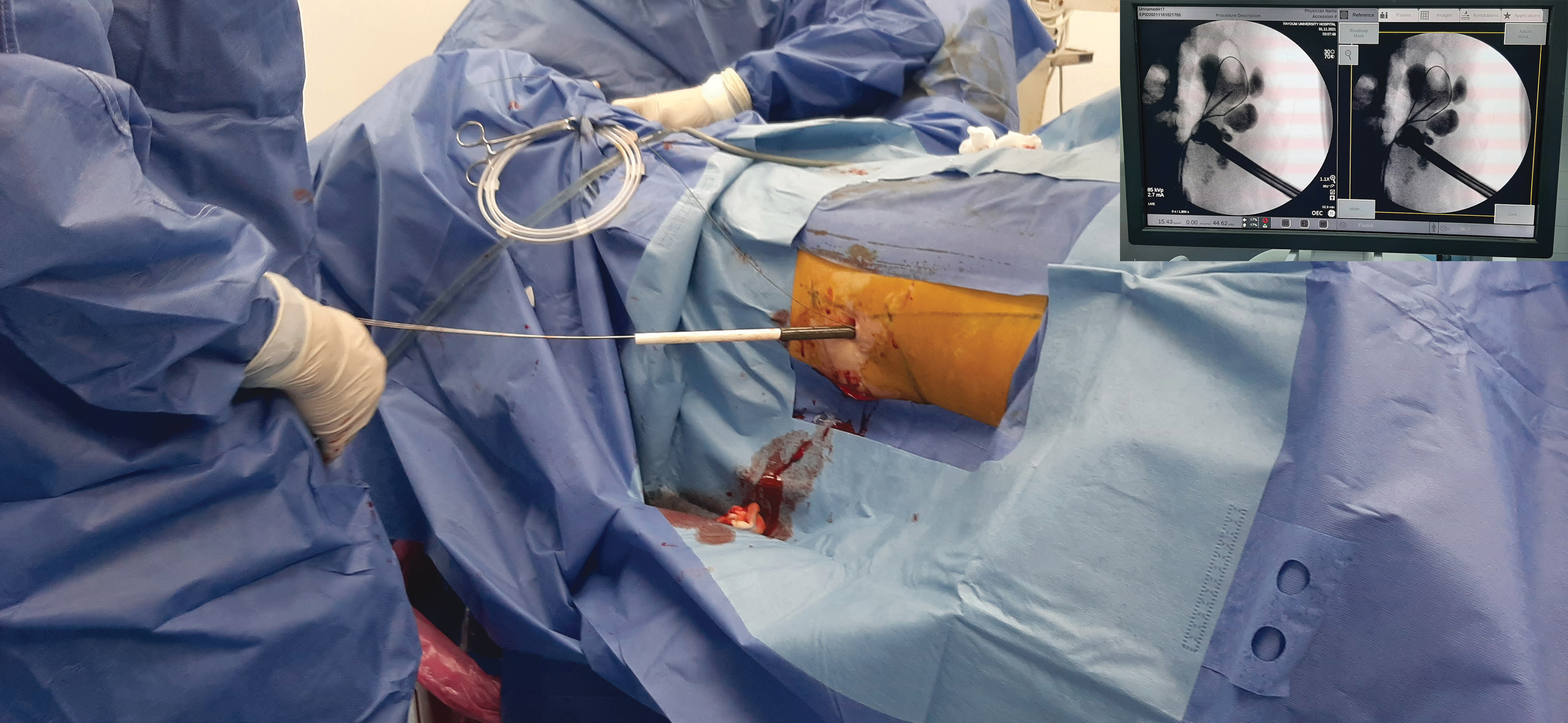
Tract dilatation by OSD. OSD, one-shot dilatation. Color images are available online.
After retrograde insertion of the open-tip ureteral catheter, we interred the kidney from the PAL through subcostal puncture using an 18-G access needle to the targeted calix under fluoroscopic guidance with horizontal or slightly inclined anterior direction. After efflux of urine, a guidewire was passed to PCS, and dilatation of the tract was performed using a fascial 8F polyurethane dilator, followed by insertion of safety guidewire. The lumbodorsal fascia was punctured and split using a long straight hemostat under fluoroscopy. 8 These steps were performed in all patients.
In group 1, the Alken rod advanced to PCS, with the advancement of single Amplatz dilator (30F; single use) increment on it, as we advance the dilator in a coaxial manner using gentle steady rotating movements, and the assistant inflated the PCS by injecting saline from the ureteral catheter to ensure dilatation of the chosen calix. Then, we introduce 30F Amplatz sheath.
In group 2, we used the Alken MTD (9–30F) with its rod over the guidewire for dilatation of the tract, followed by insertion of a 30F Amplatz sheath.
All dilatation steps for both groups were performed under fluoroscopic control. If the guidewire was kinked, we replaced it with a new one.
We used a 26-F nephroscope and pneumatic lithoclast device for the disintegration of stones and then extracted using forceps while the surgeon was sitting. We did a second tract when needed.
We inserted a nephrostomy tube at the end of the operation. The success of the operation was defined as stone free or patients with residual stones ˂4 mm, whereas residual stones >4 mm were arranged for extracorporeal shockwave lithotripsy (SWL) or second-look PCNL.
Second CBC collected 24 hours postoperative to assess the hemoglobin (Hb) loss.
We removed the nephrostomy tube on the first postoperative day (in successful cases) followed by the ureteral catheter 24 hours later.
Statistical analysis
Data were analyzed using the statistical package SPSS version 20 for Windows (SPSS, Inc., Chicago, IL). Variables were represented using numbers and percentages for qualitative variables and mean ± standard deviation for quantitative data. Quantitative variables between groups were compared using the independent t-test and chi-square test for other parameters. For all statistical analyses, p-values ≤0.05 were considered statistically significant.
Results
One hundred fifty patients underwent PCNL in Barts flank-free modified supine position. They were divided into two equal groups according to tract dilatation techniques used (Group 1: OSD and Group 2: Alken MTD). The baseline characteristics of all patients were comparable between the two groups (Table 1).
Represents Patients' Demographical Data for Both Groups
Data presented as mean (±SD), or number (%).
Independent t-test.
Chi-square test.
BMI = body mass index; DM = diabetes mellitus; Hb, hemoglobin; PCNL = percutaneous nephrolithotomy; SD = standard deviation; SWL = extracorporeal shockwave lithotripsy.
We effectively dilated the PCNL tract in all cases and entered the targeted calix even in patients with a history of previous renal surgery with a success rate of 100% in both groups.
There is a statistically significant difference between both groups regarding time of dilatation (seconds) 68.5 (±15) vs 147.2 (±18), X-ray time (seconds) during dilatation 36.3 (±10) vs 61.8 (±15), and total X-ray time (seconds) for whole operation 157.7 (±16) vs 181 (±20), with favorable results to OSD.
The Hb loss (mg/dL) was significantly lower in OSD, 0.75 (±0.29) vs 1.21 (±0.35). The success rate was comparable between the two groups (92% vs 89.3%). The hospital stay (days) was significantly lower in OSD than MTD, 3 (±0.6) vs 3.7 (±0.7) (Table 2).
Represents Intra- and Postoperative Data for Both Groups
Data presented as mean (±SD), or number (%).
Independent t-test.
Chi-square test.
We classified the operative complications according to the Dindo-modified Clavien system. 21
Two (2.7%) patients received one unit of blood in OSD and 3 (4%) patients in MTD. Three patients in each group developed acute pyelonephritis and all responded well to parenteral antibiotics. Three patients underwent DJ insertion for persistent leakage. Two patients were admitted to ICU for one organ failure. There were no organ injuries or deaths. There is no statistically significant difference between both groups (p = 0.965) regarding the complications rate (Table 3).
Complication According to Dindo-Modified Clavien System
Chi-square test.
Discussion
In PCNL, percutaneous tract dilatation is an essential step, as inadequate tract dilatation can prevent access sheath insertion into PCS and induce bleeding. 3
In Barts flank-free modified supine position, there is no loin support allowing wide space for renal puncture and allowing for simultaneous ante- and retrograde kidney access without changing the position. In this position the kidney lies in its normal position, it becomes less mobile, making the puncture and tract dilatation easier than other supine position modifications and the tract is more lateral, making surgeon X-ray exposure less. Because of the nearly horizontal lye of the tract, this facilitates stone fragment washout and lower intrarenal pressure. 18,19
We entered all targeted calix (100% success rate), even in cases with previous renal surgery in both groups [as in this position the kidney is less mobile with less incidence for the risk of tract displacement]. In different studies on OSD, the success rate for dilation ranges from 92.6% to 100%; this is comparable with other gradual dilatation techniques, although the lowest rate in patients with a history of previous surgery. 4,6,8,9,22 We overcome the perirenal scar tissue by disrupting it by inserting a long straight hemostat under fluoroscopy before dilatation and applying gradual rotational advancement movement for the Amplatz dilator and sheath. 8,23 El Harrech assessed OSD in the supine position with a success rate for tract dilatation was 97.8%. 7
In OSD the time needed (68.5 seconds ±15) for tract dilation is statistically significantly less than in MTD 147.2 seconds (±18). Also the X-ray time, 36.3 seconds (±10) for dilatation and the total X-ray time 157.7 seconds (±16) for the whole operation in OSD are statistically significantly less than in MTD 61.8 (±15) and 181 (±20), respectively, as a single dilator is less time-consuming than multiple incremental dilators. 3,6,24 These results are inconsistent with meta-analysis data 3,6,24 and other comparative studies. In these studies, the dilatation time and X-ray time for dilatation ranged from 5.7 to 6.3 minutes and 20 to 46 seconds in OSD and were significantly less than MTD, 7 to 10.4 minutes and 60 to 81 seconds, respectively. 3 –6,9,21 –25
Two studies presented the total X-ray time (262 vs 310 seconds and 10.5 vs 11.8 minutes), which is also significantly less in OSD. 5,8
In the El Harrech study (supine position) the dilatation time was 2.1 minutes [0.7–6.2], X-ray time for dilatation was 25 seconds (±17), and total X-ray time was 142 seconds (±54), and these data correlate with our data. 7
We should consider the variation in definitions used for the assessed parameters in the different studies for example, timing of X-ray and operative time. 6
Our operative time (minutes; 71.1 [±10] vs 73.1 [±9]) was comparable in both groups. It is less than Nour and colleagues 8 study (100.9 vs 124) when they compared OSD vs MTD in prone position as in supine position no need to change patients' position, and also less than Bach 19 study (74.4 minutes) when they performed PCNL in Barts flank-free supine position; however, in this study they used an incremental dilator.
Our operative time in OSD is more than El Harrech's and colleauges 7 study (54.8 minutes) but within his range [25–137]; in this study, there is no operative time definition.
There is an agreement that the Hb loss in OSD is less than that in MTD and varies from statistically significant to not statistically significant. 3 –6,8,9,17,21,24 In this study, the Hb loss (mg/dL) is significantly less in OSD, 0.75 (±0.29) vs 1.21 (±0.35), and it is in the range of different studies [0.8–1.6 vs 1.1–2] for both groups, respectively.
We used 161 guidewires in OSD and 169 in MTD without significant differences, although we did 83 tracts in OSD and 81 in MTD. Ziaee and colleagues stated that in OSD, there is less risk of tract displacement, with fewer incidences of guidewire kinking. 23
The operative success rate was 92% (OSD) vs 89.3% (MTD), which was not statistically significant. This is inconsistent with many studies comparing either OSD vs MTD or even comparing prone vs supine positions. 2,3,6,12,14 All patients with significant fragments >4 mm underwent SWL.
Our hospital stay (days) was significantly lower in OSD than in MTD, 3 (±0.6) vs 3.7 (±0.7). Different studies in prone positions present the same result, but without a significant difference. 4,8 Our hospital stay (3.6 days) is comparable with El Harrech and colleagues 7 study.
One of the best measures to decrease complications is proper access tact creation. 26 The low-grade complication (grade 1 and 2) rate according to the modified Clavien system for all patients was 24.6%. Fever and pain were the main complaints. Our OSD complication rate in the supine position is comparable with that in different studies either assessing OSD or supine position or combining both techniques as in the Harresh study. 2,7,8,26
Despite being a prospective controlled study, and these encouraging results, we recommend further analysis and comparative studies to confirm these data. Another limitation of this study is that we excluded upper caliceal stones and staghorn stones.
Conclusion
Patients and doctors can obtain more benefits by combining the advantages of OSD and Barts flank-free modified supine position during PCNL, as it is simple, safe, and efficient as MTD, with shorter dilatation time, X-ray exposure time, hospital stay, and less blood loss.
Authors' Confirmation Statement
All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the study to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the article. All authors certify that this article represents valid and original study. If requested the authors will provide raw data on which the article is based for examination by the editors and reviewers. Furthermore, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication before its appearance in Journal of Endourology.
Footnotes
Authors' Contributions
This paragraph delineates each specific contributions made by each author.
Category 1: Conception and design of study by Khaled Mohyelden and Amro Mostafa. Acquisition of data by Mohamed Dogha and Ahmed Kadry. Analysis and/or interpretation of data by Mohammed Abdel-Rassoul.
Category 2: Drafting the article by Khaled Mohyelden and Amro Mostafa. Revising the article critically for important intellectual content by Mohammed Abdel-Rassoul, Mohamed Dogha, and Ahmed Kadry.
Category 3: Statistical analysis by Khaled Mohyelden and Mohammed Abdel-Rassoul. Supervision by Amro Mostafa, Mohamed Dogha, and Ahmed Kadry. We approve this version of the article to be published.
Author Disclosure Statement
We declare there are no financial and nonfinancial relationships and activities, and conflicts of interest.
Funding Information
No funding agreement limits my ability to complete and publish this study.