
Abstract
Introduction:
We present perioperative outcomes of a single-center experience with robot-assisted antegrade colonic enema (ACE) channel creation for the treatment of chronic constipation refractory to medical therapy and compare it to the traditional open surgical approach. We also demonstrate a step-by-step video presentation of the robotic approach for cecal flap ACE performed as part of a dual continence procedure in patients with short length of appendix.
Methods:
A retrospective chart review of pediatric patients who underwent ACE channel creation between 2008 and 2020 was performed. We compared demographics and intraoperative and postoperative variables of the open vs robotic approach.
Results:
Among 28 patients, 15 were open and 13 robotic. To construct the ACE channel, a cecal flap was utilized in 36%, split appendix in 50%, full-length appendix in 11%, and sigmoid colon in 3% of patients. Both approaches showed equivalent estimated blood loss (50 mL [interquartile range; IQR = 20–100]), median length of hospital stay (7 days vs 8 days, p = 0.7), and median time to return to regular diet (4 days vs 5 days, p = 0.5) (Table 1). Patients in the open group were more likely to have a history of prior abdominal surgeries than those in the robotic group (80% vs 38.5%, p = 0.02). The risk of Clavien-Dindo grade 3 or more complications (40% vs 23.1%, p = 0.04) and the rate of ACE channel stenosis (46.7% vs 7.7%, p = 0.02) were significantly higher in the open approach. Channel stenosis was significantly higher in patients with an appendix ACE channel (87.5% vs 12.5%, p < 0.05) compared to those with cecal flap ACE.
Demographic, Operative Characteristics, and Complications Among Patients Undergoing Antegrade Colonic Enema and Comparison Between Open Approach and Robotic Approach
Total
Open
Robotic
p
Patients
28
15
53.60%
13
46.40%
0.027
Age, median (IQR)
9 (6–14)
6
(5–11.5)
12
(9–14)
Preoperative diagnosis
Spinal dysraphism
26
14
93.30%
12
92.30%
0.92
Cerebral palsy
2
1
6.70%
1
7.70%
Prior abdominal procedure
17
12
80.00%
5
38.50%
0.025
Procedures
ACE
28
15
100.00%
13
100.00%
APV
19
8
53.30%
11
84.60%
0.077
Monti
5
5
33.30%
0
0.00%
0.044
BA
16
7
46.70%
9
69.20%
0.25
Bladder neck reconstruction
8
6
40.00%
2
15.40%
0.15
Bladder neck closure
2
0
0.00%
2
15.40%
0.22
ACE channel technique
Appendix
3
1
6.70%
2
15.40%
0.53
Split appendix
14
7
46.70%
7
53.80%
0.71
Cecal flap
10
6
40.00%
4
30.80%
0.62
Sigmoid colon
1
1
6.70%
0
0.00%
0.96
Estimated blood loss (mL), median (IQR)
50 (20–100)
50
(35–75)
50
(20–100)
0.93
Return to diet, median (IQR)
4 (3–7)
5
(3–7)
4
(3–4)
0.5
Length of hospital stay, median (IQR)
7 (6–10)
8
(7–11)
7
(6–10)
0.74
Complications
ACE suprafascial stomal stenosis
4
4
26.70%
0
0.00%
0.11
ACE subfascial stomal stenosis
4
3
20.00%
1
7.70%
0.45
Total ACE channel stenosis
8
7
46.70%
1
7.70%
0.023
ACE channel-related Clavien grade 3 or more complication (0: No, 1: Yes)
9
6
40.00%
3
23.10%
0.037
Conclusion:
Robot-assisted ACE channel creation is a safe and acceptable alternative with a significantly lower rate of channel stenosis and other clavien dindo grade 3 complications compared to the traditional open approach. Cecal flaps are also at a lower risk of stomal stenosis than appendix.
Introduction
In pediatric urology, the most challenging patients are those who display urologic manifestations of primary neurologic diseases, such as spina bifida, myelomeningocele, sacral agenesis, and cerebral palsy, among others. In addition to speech and learning difficulties as well as physical challenges, these patients often present with urinary incontinence and severe fecal constipation/incontinence. 1,2
When conservative medical therapies like dietary modifications, laxatives, and enemas fail to alleviate their symptoms, patients and their caregivers seek surgical alternatives to achieve social urinary and fecal continence. 3 The antegrade colonic enema “ACE” channel is an option for the treatment of chronic constipation refractory to medical therapy. First described by Malone and colleagues in 1990, this catheterizable channel allows the administration of an enema in an antegrade manner to allow washout of impacted stool. 4,5
With the advent of surgical technology and innovation, the Da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA, USA) allows urologists to explore minimally invasive techniques to treat pediatric patients and achieve outcomes comparable to the traditional open approach. We report our single-center experience with 13 consecutive robot-assisted catheterizable ACE channel creations and compare their outcomes to 15 patients treated by the traditional open approach. We aim to describe the procedure's intraoperative nuances, highlight its advantages, and report potential postoperative complications and functional outcomes. We also compare the utility of the appendix vs cecal flap to make the ACE channel. We demonstrate a step-by-step video presentation of the robotic approach for cecal flap ACE performed as part of a dual continence procedure. To our knowledge, this is the first series of its kind to be reported in the literature.
Methods
After obtaining institutional review board approval, we performed a retrospective database review of pediatric patients who underwent catheterizable channel creations at our institution between April 2008 and April 2020. The inclusion criterion was patients ≤18 years of age, who underwent ACE channel creation as the primary procedure. Patient information included patient age (years), sex (male/female), ethnicity (White, Hispanic, and African American), body mass index (BMI), history of prior abdominal surgeries, preoperative primary neurologic diagnosis, and the specific indication for ACE channel creation. Procedure-related information included estimated blood loss (EBL in mL), time to return to full diet (days), length of hospital stay (LOS) (days), type of surgical procedure (patients often undergo more than one intervention simultaneously, in addition to ACE channel creation (e.g., appendicovesicostomy [APV], bladder neck reconstruction or closure, etc.), and the segment of bowel used (full-length appendix vs split appendix vs cecum).
Surgical complications were analyzed, including bowel obstruction, recurrent fecal incontinence, stomal leak, stomal stenosis/stricture formation, and spontaneous closure of the ACE channel. Suprafascial stenosis was defined as extrinsic compression at the skin level caused by granulomas or keloids, whereas subfascial stenosis as intrinsic obstruction in the channel attributable to ischemia, acute angulation of the channel, or false passage. Moreover, complications were graded according to the Clavien-Dindo classification. 6
Surgical technique of robotic ACE channel creation
With the patient under general anesthesia and in the lithotomy position, all pressure points are appropriately padded. No bowel prep is routinely given pre-operatively even in cases of cecal flaps. The camera port is inserted through a 12 mm trocar just below the umbilicus, two 8 mm ports at 6–8 cm on either side of the umbilicus, and a 5 mm assistant port cephalad and lateral to the camera (Fig. 1). This port configuration is necessary not only for construction of the ACE channel but also for additional simultaneous reconstructive procedures as well. If a concomitant APV is to be performed and the length of appendix is short, a cecal flap from the anterior wall of the cecum can be used for creation of the ACE channel, as portrayed in the Supplementary Video S1.
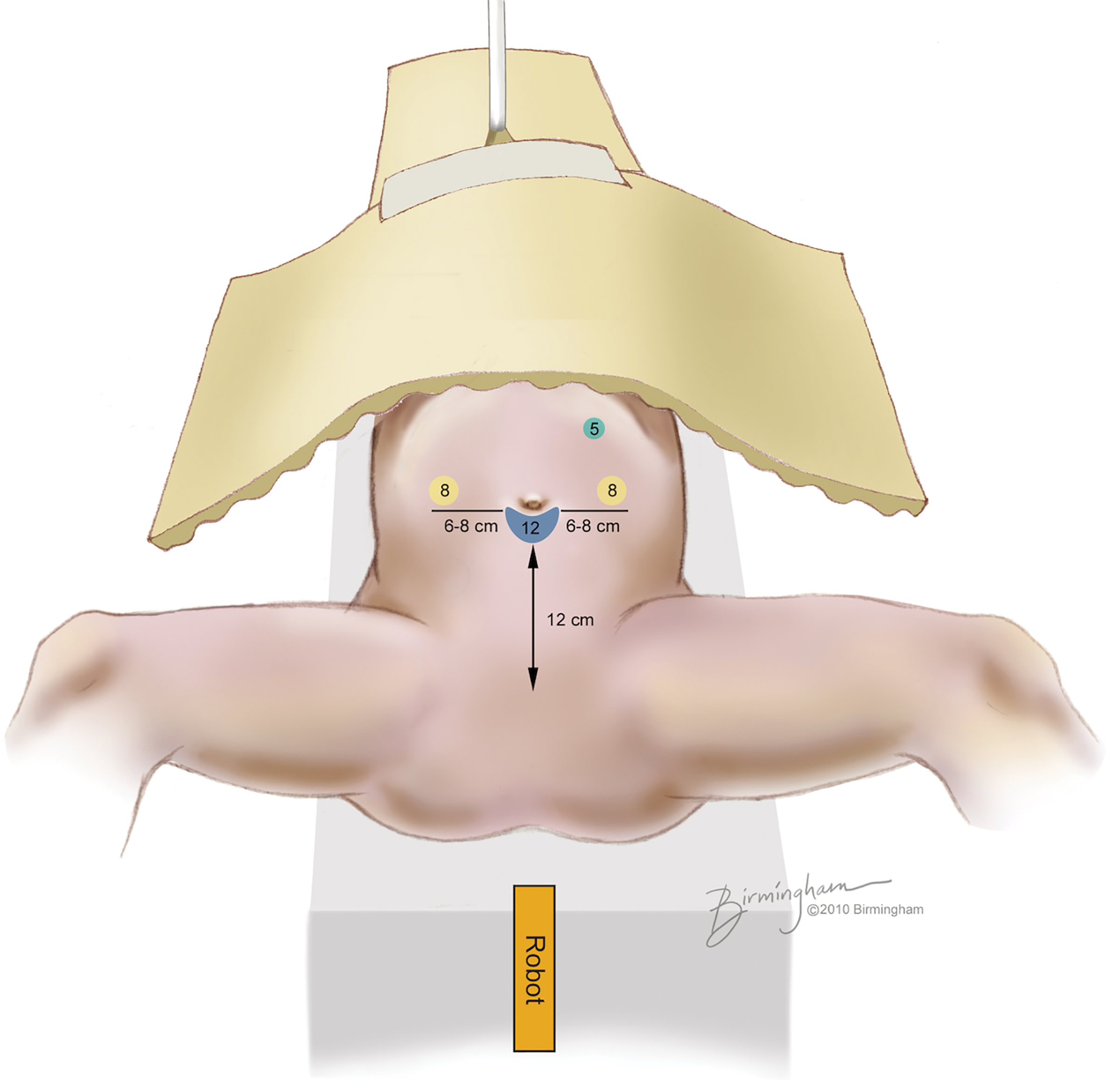
Trocar placement for robot-assisted ACE channel creation (please note that all patients in our cohort are undergoing concomitant augmentation cystoplasty/APV and/or BNR). ACE
Once the appendix is identified, a stay suture is placed at its tip for easier handling. It is traced down its mesentery toward the cecum and 1 cm of cecum is incised along with the proximal end of appendix to augment the length of the channel and avoid future stomal stenosis. When a cecal flap is the channel of choice, a 4 cm in length × 2 cm in width flap is created by incising the anterior wall of the cecum using monopolar scissors. The cecal flap is then tubularized around an 8F feeding tube using single layer 4-0 or 5-0 PDS® (polydioxanone) suture. The cecal defect is closed in two layers using 4-0 PDS. To complete the procedure, the tubularized cecal flap is brought to the skin of the right lower quadrant using a grasper.
The ACE channel is matured with a “V” or “VQ” shaped skin flap of the abdominal wall to cover the stoma with skin. Alternatively, in patients who require a dual continence procedure, and the length of appendix is deemed satisfactory for creation of both channels, a split appendix technique is utilized. The proximal end of the appendix can be used for ACE channel formation depending on abdominal wall thickness, whereas the remaining distal end is used for the APV, taking care to preserve the mesentery. The adequate appendiceal length for the reimplantation into bladder should be about 4 cm to obtain continence, but this can vary based on age and BMI. The addition of umbilical skin flap at skin level helps to bridge the short length.
In regard to the ACE with split technique, another 3–4 cm is adequate and mobilization of the cecum and colon is done as needed, and the creation of cutaneous skin flap helps to bridge the shortness.
Results
A total of 28 patients in our cohort were identified, 15 underwent an open procedure and 13 underwent a robotic reconstructive procedure (ACE channel combined with APV, bladder neck reconstruction, etc.) The median age was 6 years in the open group, and 12 years in the robotic group (p = 0.027). The primary neurologic pathology in two patients (7.1%) was cerebral palsy, whereas 26 (92.9%) suffered from spinal dysraphism and presented with spina bifida, myelomeningocele, or sacral agenesis. The median time of follow-up for patients in the open group was 81 months (interquartile range [IQR] = 2–132), compared to 66.5 months (IQR = 12–137) in the robotic group. Among patients who required an open approach, 80% had a history of prior surgical interventions compared to only 38.5% of the robotic group (p = 0.02) (Table 1).
In addition to chronic constipation, most patients present with urinary incontinence caused by neurogenic bladder or an incompetent bladder neck. In our cohort, every patient who underwent ACE channel creation, did so in combination with one or more necessary procedures (i.e., 68% required APV, 57% augmentation cystoplasty [bladder augmentation; BA], and 36% bladder neck procedures [BNR]). Such procedures require a prolonged operative time. Consequently, operative time was not assessed for either cohort as it does not reflect the true time required to construct an ACE channel alone. However, both approaches showed equivalent EBL (50 mL [20–100]), median LOS (7 [6–10] days vs 8 [7–11] days, p = 0.74), and time to return to regular diet (4 [3–4] days vs 5 [3–7] days, p = 0.5) for the robotic and open approaches, respectively.
A split appendix was used to form the ACE channel in 14 patients, tubularized cecal flap in 10 patients, full length of appendix in 3 patients, and a tubularized sigmoid flap in one patient.
Patients in the open group were at a significantly higher risk of postoperative Clavien-Dindo grade 3 or more complications (40% vs 23.1%, p = 0.04) compared to the robotic group. Among those who underwent open ACE channel, four patients (26.7%) presented with suprafascial stomal stenosis and a difficulty passing the catheter compared to none (0%) in the robotic group.
Three patients (20%) in the open group also presented with subfascial stomal stenosis compared to 1 patient (7.7%) in the robotic group (Fig. 2). Among seven patients with stomal stenosis in the open group, five patients required surgical revision of the native ACE channel and insertion of a MIC-KEY button gastrostomy tube for easier access, one patient required creation of a new cecal flap ACE, and one patient with an existing sigmoid ACE required takedown of a colonic fistula and subsequently underwent a loop colostomy for bowel management. Among seven patients with stenosis, three were Hispanic, three African American, and one Caucasian. Overall, there was a significantly higher risk of stomal stenosis in the open approach compared to the robotic approach (46.7% vs 7.7%, respectively, p = 0.023).

Distribution of patients with stomal stenosis in the robotic vs open groups. Color images are available online.
Stenosis was significantly higher in patients with an appendix ACE channel (87.5% vs 12.5%, p < 0.05) compared to those with tubularized cecal flap ACE. On last follow-up, the proportion of functional channels was comparable between both groups, as 87% of ACE channels in the open group and 84.6% in the robotic group (p = 0.9) were still utilized by the patient.
Discussion
The Malone antegrade continence enema (MACE) procedure, first described by Malone and coworkers in 1990, 4 has revolutionized the management and improved the quality of life (QOL) of patients with spinal dysraphism, who suffer from constipation and fecal incontinence refractory to medical therapy. 7,8 It is a surgical technique that uses the appendix (4) or tubularized cecal flap 9 to create a continent access channel between the skin and colon, through which an enema can be administered. 5,10 We have previously reported on our experience with robot-assisted continent catheterizable channels 10 ; however, to our knowledge, this is the first study comparing outcomes in robotic vs open ACE channels.
In our cohort, the robotic approach was more often utilized in patients without a history of prior abdominal surgeries. Even though adhesiolysis is feasible using the robotic platform, 11 pediatric patients with spinal dysraphism often have a complex surgical history (e.g., multiple ventriculoperitoneal [VP] shunt insertions) with hostile abdomens that may preclude seamless completion of the procedure. In our experience, those children with VP shunts often have a scarred, poor appendiceal mesentery and the shunt is often situated in a difficult intra-abdominal location (e.g., the subhepatic space). Even though abdominal access and appendix localization and mobilization can be more challenging because of intra-abdominal adhesions, we have previously reported on the technique and its reproducibility in such challenging patients. 12
The robotic approach might also offer an added advantage by decreasing the exposure of the intraperitoneal portion of the shunt to the external environment and probably decrease infectious complications. 13,14 Moreover, these procedures can be challenging if the patient had a previous appendectomy; in the beginning of our experience, patients without appendices were converted to open for Monti channel procedures.
The robotic approach to ACE channel does not offer an advantage regarding operative time, LOS, and time to return to regular diet. This is because all patients in our cohort underwent ACE along with a concomitant procedure (e.g., APV, BA, and BNR), which tend to be complex and time consuming. This justifies the extended operative time, and consequently postoperative recovery of bowel function and discharge from the hospital. However, from a technical standpoint, the robotic approach offers easier intracorporeal suturing and bowel handling compared to traditional laparoscopy.
In our series, only two patients experienced leak from the ACE channel, one had undergone robotic ACE and the other underwent ACE creation with the traditional open approach. Several variations in technique have been described for construction of the ACE channel and prevention of stomal leak. Some authors imbricate the appendicocecostomy, by wrapping the base of the appendix with cecum similar to the technique used for Nissen fundoplication. 2 Others place a stomal MIC-KEY button to prevent both leak and stomal stenosis 15 ; the latter is the most commonly reported complication of MACE. 8,16,17 Saikaly and associates showed that the placement of a stomal button without imbrication can increase the risk of leak of bowel contents and infection. 2
Others describe use of a silicon plug across the stoma between catheterizations to prevent stomal stenosis and reduce the risk of leakage. 18,19 Our preference in both robotic and open approaches is not to imbricate the appendicostomy or tubularized cecal flap. However, we do emphasize the placement of silicone plug (ACE stopper) to prevent stenosis. We also advocate use of a perioperative bowel regimen to prevent stomal leak and resultant soiling. In patients who later present with fecal incontinence attributable to absence of compliance and poor bowel washout, a MIC-KEY button is used to plug the stoma and prevent soiling. It is also helpful in patients who are predisposed to keloid formation and stomal scarring to prevent stomal stenosis. 14
In this cohort, the risk of ACE channel stenosis was significantly higher in the open approach. Known etiologies for stomal stenosis include weight gain after stoma formation, and a short length of exteriorized bowel segment, especially in obese patients, where the thickness of the abdominal wall makes exteriorization difficult. 20,21 Other causes include individual variability in hyperplasia, presence of adhesions, hyperkeratosis, and compromised vascularity. 22,23
Maintaining the integrity of the bowel segment and preserving its blood supply are crucial to ensure a healthy channel and stoma. Patient ethnicity, for example, did not predispose patients to stenosis more than others, even though scarring and keloid formation are more common in certain races/ethnicities than others. Another more common cause is absence of compliance by patients' caregivers who are instructed to catheterize the ACE channel at least once daily along with administration of the enema for bowel evacuation. 5 Failure to repeatedly catheterize the channel may lead to channel stenosis, as well. This requires surgical repair and revision of the stoma or dilation using a MIC-KEY button. We were unable to discern the reasons for stomal stenosis in our cohort as BMI, changes in weight, as well as compliance of the groups were not analyzed.
The risk of Clavien-Dindo grade 3 or more complications (40% vs 23.1%, p = 0.04) was higher in the open approach. Among six patients who required surgical intervention in the open group (40%), one patient with a sigmoid flap ACE had a necrotic channel with the formation of colonic fistula, treated with sigmoid colostomy formation. Another patient suffered complete blockage of the appendix ACE requiring exploratory laparotomy and replacement with a cecal flap ACE. The rest of the patients had stomal stenosis requiring revision and placement of a MIC-KEY button. In the robotic group, one patient with an underlying intrinsic bowel disorder had a failed ACE channel resulting in severe colonic dilation and eventually diversion through a loop ileostomy, another patient with severe stomal stenosis requiring surgical revision, and a third patient with spontaneous closure of the channel because of poor compliance.
The risk of ACE channel stenosis appeared to be higher in patients with an appendix ACE channel compared to those with cecal flap ACE. This is in concordance with outcomes in the literature. In a study comparing appendix ACE (MACE) to cecostomy channels, the risk of complications requiring operative intervention was higher in patients who underwent MACE. The main complication requiring surgical intervention was stomal stenosis (11%). 17 In a meta-analysis of 40 studies assessing a total of 2086 patients, the overall rate of complications in the appendicostomy group was higher than the cecostomy group (42.3% vs 16.6%, respectively). 24
On the other hand, Halleran and coworkers reported a lower overall complication rate of appendix channels when compared to cecostomy creation. 25 However, both procedures were deemed reliable and effective with high success rates 17 and comparable rates of patient satisfaction and impact on QOL. 24 We speculate that the larger caliber stoma of the tubularized cecal flap, in addition to a better vascular supply compared to the native appendix, explains the lower chance of stomal stenosis.
Eighty-five percent of ACE channels in both the open and robotic groups remained functional and utilized by the patients on consequent follow-up, which is in concordance with values reported in the literature (60%–100% functionality). 26 On longer-term follow-up, 20% of patients are eventually able to defecate without an ACE channel enema, whereas 60% will continue to require the channel for bowel evacuation. 27
The limitations of this study include its retrospective nature, small sample size, and the fact that it is a single surgeon experience. Although the median time of follow-up was more than 5 years in both groups, complications often happen during adolescence, possibly necessitating a longer follow-up time in patients who underwent operation in childhood. Another important limitation is the difference in follow-up time between the robotic approach and traditional open approach group, which can partly explain the slightly higher complication rates with the traditional approach such as stomal stenosis. Moreover, suboptimal outcomes and absence of timely management of complications in our cohort can be attributed to noncompliance by the patient and/or their caregivers. This is often difficult to account for, especially in a morbid and complex patient population.
Conclusion
In pediatric neuropathic patients with constipation refractory to medical therapy, robot-assisted ACE channel creation is a safe and acceptable alternative with possibly a significantly lower rate of channel stenosis compared to the traditional open approach. Even though both types of ACE channels are effective, reliable, and significantly improve QOL, cecal flap tubularized ACE channels are at a lower risk of stomal stenosis on the long term.
Footnotes
Authors' Contributions
The authors confirm contribution to the article as follows: study conception and design: M.S.G. Data collection: C.A. and R.S. Analysis and interpretation of results: N.A.H and R.S. Draft article preparation: R.S. and N.A.H. Article revision: M.S.G. All authors reviewed the results and approved the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Video S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.