
Abstract
Background:
Robot-assisted ureteral reimplantation (RAUR) is a relatively new minimally invasive procedure. As such, research is lacking, and the largest adult cohort studies include fewer than 30 patients. Our aim was to be the first population-based study to report on national utilization trends, factors associated with patient selection, inpatient outcomes, and the relative cost of RAUR for adults with benign ureteral disease (BUD).
Materials and Methods:
The National Inpatient Sample (2010–2015) was queried to identify all elective, nontransplant-related, open and robot-assisted reimplants for adult BUD. Survey-weighted logistic regression using Akaike Information Criterion identified patient-/hospital-level factors associated with robotic procedure. Survey-weighted regression models examined the association of robotic procedure with outcomes and charges.
Results:
A weighted total of 9088 cases were included: 1688 (18.6%) robot assisted and 7400 (81.4%) open. There were significantly increased odds of RAUR across consecutive years (odds ratio [OR] = 3.0, p < 0.001) and among patients operated on at private for-profit hospitals (OR: 2.1; p = 0.01), but significantly decreased odds among older patients (OR = 0.98, p < 0.001), those with Medicaid (OR = 0.5, p = 0.02), those with 2+ comorbidities (OR = 0.6, p = 0.009), and those operated on in western (OR = 0.5; p = 0.005) states. RAUR was significantly associated with a reduced length-of-stay (incidence rate ratio: 0.60; p < 0.001), decreased odds of blood transfusion (OR = 0.40; p < 0.001), and a lower mean ratio of total hospital charges (ratio: 0.71; p = 0.006).
Conclusions:
This is the first population-based study to report on the utilization and clinical benefits of RAUR for adult BUD. Open reimplantation remains the most common surgical technique utilized, despite the potential benefits of RAUR. Future research is needed to explore the mechanisms behind patient-/hospital-level factors and surgical selection. Work to investigate potential barriers in access to robotic procedure can help us provide equitable care across patient populations.
Introduction
Ureteral reimplantation is the definitive treatment for distal ureteral strictures in adult patients. 1 Although ureteral strictures can be idiopathic, most result from iatrogenic injury from endoscopic stone procedures, radiation therapy, retroperitoneal fibrosis after vascular bypass grafting, or most commonly, injury or devascularization during pelvic procedure. 1 –3 The distal ureter is the most common site of iatrogenic injury during pelvic procedure. 4,5 Gynecologic surgeries are estimated to account for 52% to 82% of injuries, whereas colorectal surgeries account for 9%. 6 Open ureteral reimplantation is historically the gold standard for repairing distal strictures and creating a tension-free anastomosis. With over 50 years of data, reported success rates are as high as 97% at 4.5 years of follow-up. 7
The first robot-assisted ureteral reimplantation (RAUR) was described by Yohannes and colleagues. 8 Robotic assistance offers improved visualization, 3D magnification, and precise intracorporeal suturing. 9 Although previous single-center studies have suggested that open and robotic reimplantation have at least equivalent success rates, 9 –11 no studies have used population-level data to compare clinical outcomes or financial costs associated with each technique.
The largest published studies of RAUR are restricted to single-center series of up to 30 adult patients, all of whom were operated on at tertiary-care academic centers or by surgeons with extensive experience in minimally invasive surgery (MIS). 12 –15 To date, there is no published information on national trends in the utilization of RAUR for adult benign ureteral disease (BUD) or factors associated with patient selection.
In this study, we utilize national data to investigate clinical outcomes, hospital charges, and both patient- and hospital-level factors associated with RAUR in adults with BUD. Our objective was to demonstrate patterns in utilization, disparities in access, and postoperative inpatient outcomes.
Materials and Methods
The National Inpatient Sample
The National Inpatient Sample (NIS) is the largest all-payer inpatient care database in the United States. It includes a 20% stratified sample of hospitalization data obtained from 46 states, equating to ∼8 million discharge records per year from more than 1000 hospitals. 16 Each record includes ICD-9 (International Classification of Disease, 9th Edition) diagnosis and procedure codes, patient demographics, insurance status, median household income (based on zip code), hospital characteristics (bed number, teaching status, region, and ownership), Elixhauser comorbidity index, and inpatient outcomes (length of stay [LOS], mortality rate, and total hospital charges). IRB approval was obtained for this study.
Study cohort and covariates
We identified all records of adult (≥18 years old) inpatient hospitalizations for elective ureteral reimplantation from 2010 to 2015. “Ureteral reimplantation” was defined using ICD-9 procedure code 56.74 alongside common indications for reimplantation (ICD-9 codes: 591, 593.3, 593.4, 593.5, 593.82, and 593.89). The robotic modifier (ICD-9 code: 17.42) was used to identify cases of RAUR. We excluded patients with any documented history of end-stage renal disease, ureteral cancer-related reimplant, kidney transplant-related reimplant, and laparoscopic reimplant (ICD-9 codes in Supplementary Table S1). These cases were excluded as they were deemed to be clinically and/or technically distinct from cases that occur for BUD.
Clinical outcomes of interest included inpatient mortality rate, LOS, red blood cell (RBC) transfusion, and total hospital charges.
Statistical analysis
Patient and hospital-level covariates were summarized using descriptive statistics. Categorical variables were analyzed using Rao–Scott chi-square tests and continuous variables using Student's t-test. Skewed continuous variables were analyzed using Wilcoxon rank sum tests.
Univariable and multivariable logistic regression were used to identify predictors of RAUR. Given the paucity of known predictive factors to RAUR, a multivariable model was first generated using variables of interest, and backwards elimination by Akaike Information Criteria was used to identify the best-fitting model.
Additional regression models were used to compare the association of RAUR to outcomes. Univariable and multivariable logistic regression were used to compare RBC transfusion. A negative binomial regression model was used to model the over-dispersed distribution of LOS. A generalized linear model with a logarithmic transformation was used to model the positively skewed distribution of total hospital charges. All models assessing these outcomes were adjusted for age, insurance, race, income, Elixhauser comorbidity index, hospital region, teaching status, urban vs rural, bed size, and ownership.
All data were survey weighted and clustered by hospital strata to account for NIS sampling weights in adherence to best practices as outlined by the Agency of Health care Quality and Research. 17 All statistical tests were two sided. Alpha <0.05 was considered statistically significant. All statistical analysis was performed on R version 4.00 (R Foundation for Statistical Computing, Vienna, Austria).
Results
A weighted total of 9088 cases were identified: 7400 (81.4%) performed open and 1688 (18.6%) performed robotically. Utilization of robotic assistance increased from 9% of cases in 2010 to 22% in 2015 (Fig. 1).
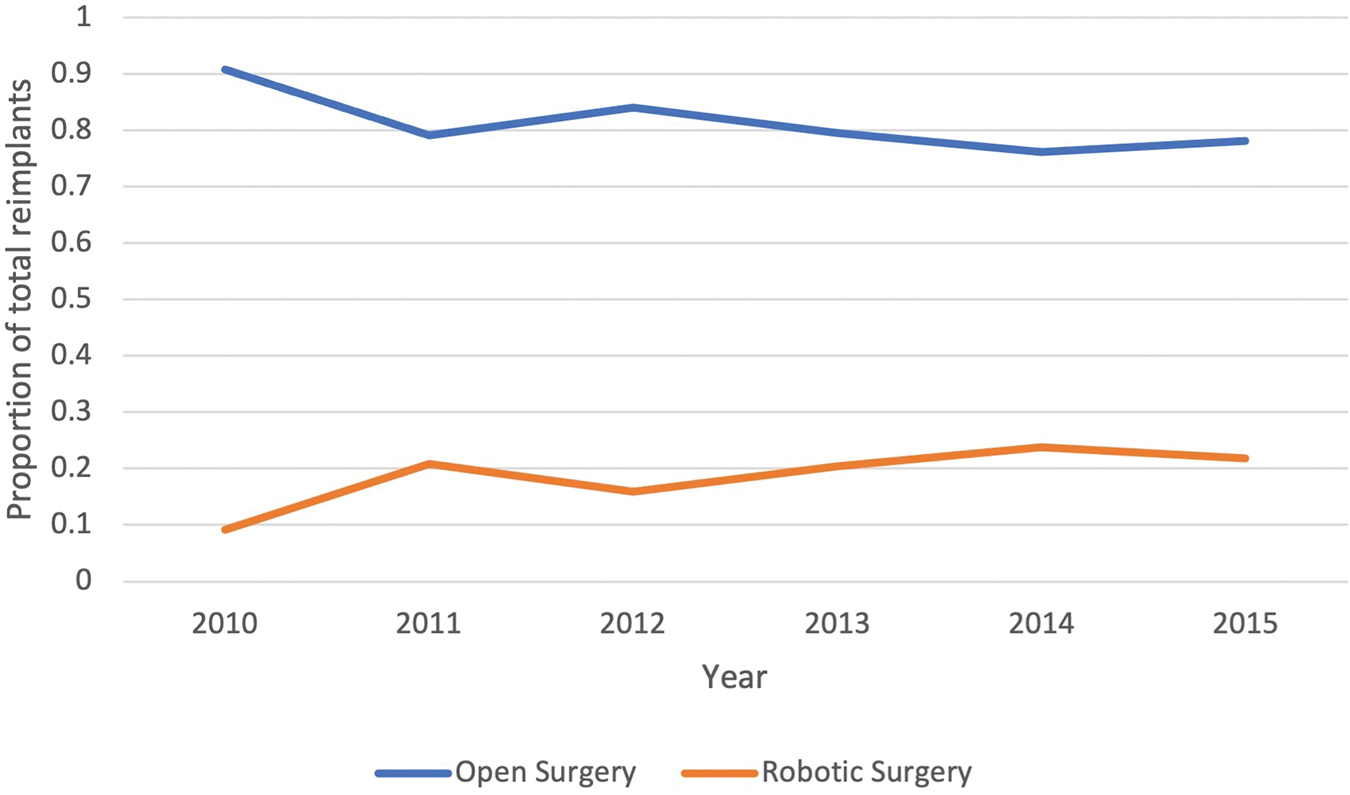
National utilization of operative approach for ureteral reimplantation for benign disease: 2010 to 2015. Color images are available online.
Table 1 provides the baseline characteristics of the entire cohort stratified by surgical approach. Patients who underwent RAUR were significantly younger, with a mean age of 51 (standard deviation [SD] = 14.8), than those who underwent an open approach, with a mean age of 53.6 (SD = 14.5), p < 0.001. They were also more likely to be covered by private insurance (62.1%; p = 0.009), operated on at a private for-profit institution (14.2%; p = 0.01), and have a lower Elixhauser comorbidity score (p = 0.01).
Cohort Characteristics
IQR = interquartile range; RBC = red blood cell; SD = standard deviation; USD = U.S. dollars.
Less than 1% of open cases (0.3%, n = 20) resulted in inpatient mortality rate compared with 0% (n = 0) of RAUR cases (p = 0.34). Median LOS for RAUR was 2 days (interquartile range [IQR] = 2–3), compared with 4 days (IQR = 3–7) for open procedure (p < 0.001). Ninety-two percent of all RBC transfusions were for open cases (p < 0.001). Total mean hospital charges were significantly higher for open procedure, $70,546, than RAUR, $60,113 (p = 0.01).
Figure 2 provides the results of the multivariable logistic regression. We demonstrated significantly increasing odds of RAUR across consecutive years from 2010 to 2015 (e.g., 2011 vs 2010: odds ratio [OR] = 2.58, p = 0.001; Supplementary Table S2). Increasing age and comorbidity was significantly associated with lower odds of RAUR (OR = 0.98, p < 0.001 and OR = 0.60, p = 0.009, respectively). Patients with Medicaid (OR = 0.54, p = 0.002) or other insurance, for example, self-pay (OR = 0.50, p = 0.029) were significantly less likely to undergo RAUR compared with patients with Medicare or private insurance. However, patients operated on at private, for-profit hospitals were significantly more likely to undergo a robotic approach (OR = 2.09, p = 0.014). Patients treated in Western states were significantly less likely to undergo RAUR (OR = 0.52, p = 0.005).
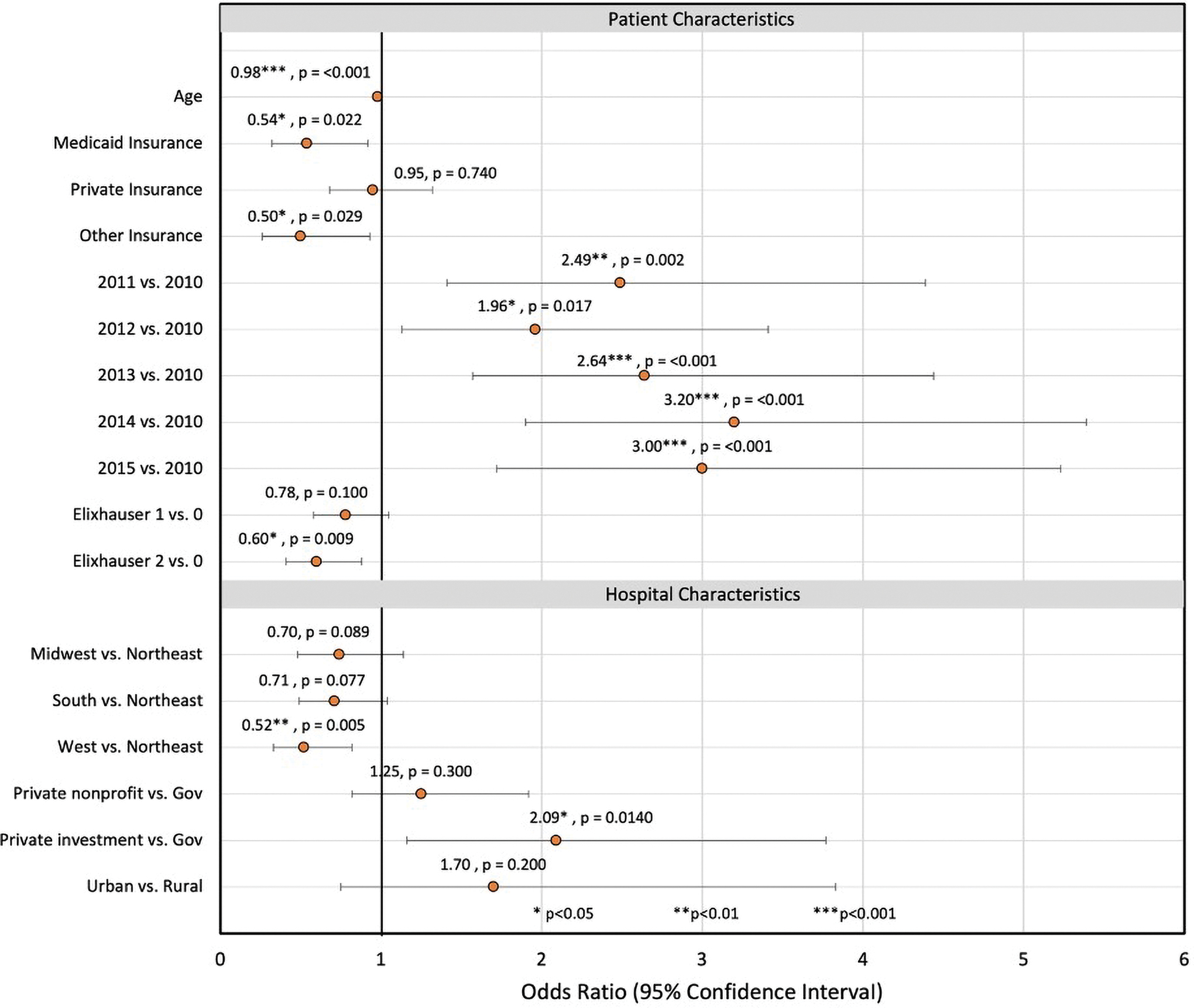
Multivariable model of patient and hospital factors associated with robotic procedure for elective ureteral reimplant. Color images are available online.
Multivariable analyses of clinical outcomes are given in Table 2. After adjustment, RAUR was associated with a significantly shorter LOS (incidence rate ratio = 0.56; 95% confidence interval [CI] = 0.50–0.63; p < 0.001), significantly decreased odds of receiving an RBC transfusion (OR = 0.39; 95% CI = 0.22–0.67; p < 0.001) and a significantly lower mean ratio of total hospital charges (ratio: 0.71; 95% CI = 0.56–0.91; p = 0.006).
Association of Robotic Approach to Ureteral Reimplantation to Outcomes
Adjusted for age, insurance status, race, income quartiles, Elixhauser comorbidity index, hospital region, teaching status, urban vs rural, bed size, and ownership.
Additional adjustment for pRBC transfusion.
Reflects the ratio of mean hospital charges.
CI = confidence interval; IRR = incidence rate ratio; OR = odds ratio; pRBC = packed red blood cell.
Discussion
This is the first population-based analysis of elective, nontransplant ureteral reimplantation for adults with BUD in the United States. We found that ∼1110 to 1700 persons a year required reconstructive procedure for BUD. With an estimated mean total hospital charge of ∼$69,000 per procedure, this amounts to ∼$75 to $117 million per year. Although RAUR is on the rise since 2010, it appears to remain underutilized for BUD, despite its potential benefits. We found that RAUR is associated with significantly decreased LOS, need for RBC transfusion, and total hospital charges.
Before this study, only two single-center studies, both from Europe, have reported on postoperative outcomes after RAUR for patients with BUD. 14,15 Buffi and coworkers reported on a total of 21 RAUR patients and Schiavina and associates reported on 26. 14,15 For these patients, both studies reported a mean hospital stay of 8 days, substantially higher than our reported mean of 2 days. Buffi and colleagues, reported a 4.8% rate of Clavien–Dindo II postoperative complications (including RBC transfusion), and Schiavina and colleagues reported a 0% rate of blood transfusion. 14,15 Although the authors reported on preoperative patient characteristics and long-term postoperative success, they did not compare patient outcomes or selection criteria to the classic open approach. Most importantly, these results are difficult to generalize to most U.S. community hospitals, as these studies included data from tertiary care centers or institutions with “long-term experience in MIS.” 15
Several single-center, U.S.-based cohort studies have also reported on outcomes after minimally invasive reimplantation; however, they have similarly been limited by cohort size and hospital setting. The largest single-center study comparing open, laparoscopic, and robotic reimplant was published in 2014, and included 20 cases of RAUR and 25 cases of open reimplant from one high-volume academic hospital. 12 Unlike our study, 30% of robotic cases and 36% of open cases were for malignant ureteral disease. The authors reported a significantly decreased risk of blood transfusion and a decreased LOS (mean of 2 days) in patients who underwent MIS reimplantation; the findings corroborate our results.
The issue of financial cost associated with robotic procedure is hotly debated across surgical fields. Early criticisms of robotic procedure have focused on the high initial cost of buying a robot ($1–2.5 million per unit) as well as the maintenance costs/purchases and use of disposable equipment.
Several studies outside of urology have demonstrated that procedural costs for robotic procedure are generally higher than open or laparoscopic procedure. However, when the overall hospitalization cost is considered, the cost of robotic procedure may be justifiable. 18 For instance, shorter hospital stays associated with robotic procedure can translate into savings on inpatient costs, as well as societal costs by enabling patients to return to work faster. Given our findings of reduced hospital charges, transfusion rates, and LOS with RAUR, we surmise that the additional costs of robotic procedure may be offset, at least in part, by lower complication rates, fewer intensive care unit stays, and shorter operative times. 18 Furthermore, dedicated research is needed to corroborate these hypotheses.
As robotic procedure for ureteral reconstruction becomes more common, patient selection is increasingly important. Our study is the first to investigate factors that could influence patient selection for RAUR in adult patients with BUD. We demonstrated that hospital ownership, geographic region, patient age, comorbidities, and insurance status appear play a role.
Unlike previous studies of robotic procedure for urologic conditions, we did not demonstrate an association among race, income, and access to robotic procedure. In a population-based study from 1998 to 2009, Sukumar and colleagues found that African Americans had less access to MIS pyeloplasty for adult ureteropelvic junction obstruction. 19 Likewise, Xia and colleagues found that between 2010 and 2015, non-Hispanic black and Hispanic patients were less likely to receive MIS for treatment of localized renal cancer. 20 Given our discrepant findings, further research to investigate the association between race and robotic surgical access for benign urologic pathology analysis in recent years will be necessary.
Both Sukumar and Xia also found significant geographic disparities in access to MIS. Sukumar and coworkers showed highest odds of MIS pyeloplasty in the Midwest, 19 whereas Xia and colleagues demonstrated lowest odds of MIS renal cancer operation in the South. 20 We found access to RAUR to be most limited in the West. This discrepancy in geographic access suggests a complex interplay between incidence of BUD, access to robotic systems, and perhaps access to reconstructive surgeons with robotic surgical proficiency. Although these differences are difficult to clarify with administrative data alone, additional work is needed to elucidate this finding.
Our findings also suggest that insurance status may impact choice of surgical modality in patients with BUD. Specifically, patients with Medicaid or “other” insurance (including self-pay) were less likely to undergo RAUR than those with private or Medicare insurance. Similar associations have been reported in other urologic conditions, including ureteropelvic junction obstruction and cancer surgeries, and in gynecologic operation, for which robotic assistance is an option. 19 –21
We hypothesize these patients may be less likely to undergo RAUR because of compromised access to robotic surgeons and/or hospitals with robotic systems. Alternatively, this disparity may stem from delays in access to specialty care, a consequence commonly reported among patients of lower socioeconomic status, resulting in disease progression and/or complexity that may be best managed best with traditional open procedure. Finally, it may also reflect surgeon or hospital selection bias.
There are several limitations to this study. First, we utilized a large, administrative database that lacks detailed clinical findings such as laboratory results and radiographic imaging. In addition, although we demonstrated a relatively high annual incidence of ureteral reimplantation for BUD, we could not assess the etiology of disease (gynecologic operation, stone operation, etc.). The absence of such details may restrict the interpretability of the findings, as detailed clinical information can provide additional insight into surgical selection. Furthermore, beyond distinguishing between open and robotic procedure, we could not assess differences in operative approach and/or technique. Second, our analysis of the relative cost of robotic vs open reimplant relies on billed hospital charges, which may be different from the actual amount paid. Charges and payments can significantly differ, because most insurers pay based on fee schedules or diagnosis-related groups formulas and not on the basis of charges. 22 Third, studies reliant on large, administrative data are subject to misclassification bias; however, prior research utilizing such databases have demonstrated accuracy rates exceeding 80%. 23
In addition, the NIS lacks the ability to longitudinally track patients, which restricts our analyses of costs and clinical outcomes to within the postoperative admission. As such, we could not assess the rate of postoperative ureteral patency, and therefore could not draw conclusions on differences regarding success rates in open vs robotic reimplantation. In addition, because patients are not tracked across encounters, we cannot account for patients who underwent reoperation for stricture recurrence after an initial ureteral reimplant. Moreover, because the NIS only captures inpatient data, it is possible that patients who underwent same day, outpatient procedure for BUD were not accounted for in our study. Despite these limitations, our findings are first to provide national estimates for the incidence of disease and trends in access to care for an uncommon urologic condition.
Conclusions
This is the first population-based study in the literature to report on national utilization, clinical outcomes, and the approximate cost of RAUR for treating BUD in the United States. Open ureteral reimplantation remains the most common surgical technique, despite the potential benefits of RAUR. Future research is needed to explore the associations that we identified between patient and hospital-level factors and surgical selection. Dedicated studies should focus on why patients operated on at private for-profit hospitals are more likely to undergo RAUR and why patients insured with Medicaid are less likely. Investigating these relationships could help expose gaps and barriers in access to robotic procedure, and ideally help ensure equitable care and outcomes across patient populations.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.