
Abstract
Background:
Percutaneous nephrolithotomy (PCNL) is the first-choice treatment of renal stones larger than 2 cm. We aimed to evaluate if lasers perform as equal as non-laser devices in patients with kidney stones candidate to PCNL.
Materials and Methods:
A comprehensive literature search was performed in MEDLINE through PubMed, Scopus, and Cochrane Central Register of Controlled Trials (CENTRAL) to assess differences in the perioperative course, incidence of postoperative complications, and stone-free rate (SFR) in patients with kidney stones undergoing laser vs non-laser PCNL in randomized studies. The incidences of complications were pooled using the Cochran–Mantel–Haenszel Method with the random effect model and expressed as risk ratios (RRs), 95% confidence intervals (CIs), and p-values. Surgical time and length of stay were pooled using the inverse variance of the mean difference (MD) with a random effect, 95% CI, and p-values. Analyses were two tailed, with a significance set at p ≤ 0.05.
Results:
Six articles, including 732 patients (311 patients undergoing holmium laser and 421 non-laser PCNL), were included in meta-analysis. Surgical time and postoperative stay were shorter in the non-laser group (MD: 11.14, 95% CI: 2.32 to 19.96, p = 0.002; MD: −0.81, 95% CI: −2.18 to 0.57, p = 0.25, respectively). SFR was significantly higher in the non-laser group (RR: 1.08, 95% CI: 1.01 to 1.15, p = 0.03). Patients undergoing laser PCNL had a nonsignificant higher risk of postoperative fever >38°C (RR: 0.64, 95% CI: 0.31 to 1.30, p = 0.22). Transfusion rate did not differ between the two groups (RR: 1.02, 95% CI: 0.50 to 2.11, p = 0.95). The need for stent positioning because of urine extravasation was higher risk in the laser group, but the difference did not reach significance (RR: 0.49, 95% CI: 0.17 to 1.41, p = 0.19).
Conclusions:
Non-laser PCNL showed better perioperative outcomes and SFR compared to holmium laser PCNL.
Introduction
Percutaneous nephrolithotomy (PCNL) is the first-choice treatment of renal stones larger than 2 cm according to the European Association of Urology and American Urological Association owing to the increased stone-free rate (SFR) and reduced need for a second procedure. 1,2 Since its first description in 1976 by Fernström and Johansson, 3 PCNL has evolved extraordinarily in all aspects, including advances in energy devices to make it a faster procedure, with the hope of improving stone clearance and reducing the morbidity. 4,5
According to the Clinical Research Office of the Endourological Society global study on PCNL, energy devices used for lithotripsy were pneumatic lithotripsy (41.6%), ultrasound (24%), combined pneumatic/ultrasound (18.3%), laser (7%), and shockwave (1.0%). At the 30-day follow-up, SFR was 75.7%, but 15.5% of patients required additional treatment. 6 Currently, lasers are becoming a relevant energy source, particularly in miniaturized PCNL, but it is not fully understood if they could replace traditional energy devices.
This review aims to evaluate if lasers perform as equal as non-laser devices in terms of operative time, postoperative course, and SFR in patients with kidney stones candidate to PCNL.
Materials and Methods
Aim of the review and literature search
This systematic review aimed to assess the differences in the incidence of perioperative course, postoperative complications, and SFR in patients with kidney stones undergoing laser vs non-laser PCNL. The primary outcome was to assess whether outcomes were different in the two groups. This systematic review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework. A comprehensive literature search was performed on April 20, 2021, in MEDLINE through PubMed, Scopus, and Cochrane Central Register of Controlled Trials (CENTRAL), using the following Medical Subject Heading (MeSH) terms and keywords: (energy device OR lithotripsy OR shock pulse OR laser OR trilogy OR pneumatic OR ultrasonic) AND (stone free rate OR SFR OR renal calculi) AND (nephrolithotomy OR PCNL OR PNL) AND (complication OR outcomes). No date limit was imposed.
Selection criteria
The Patient Intervention Comparison Outcome Study type (PICOS) model was used to frame and answer the clinical question. P: adult Patients with kidney stones; Intervention: PCNL with laser; Comparison: PCNL with non-laser (pneumatic/ultrasonic/combination/shock pulse/trilogy); Outcome: complications and SFR; and Study type: randomized clinical trials (RCTs). Patients were allocated in two groups regardless of the energy device used for lithotripsy (laser vs non-laser). We gathered the following operative and perioperative data: surgical time, length of stay, blood transfusion, fever >38°C, and urine extravasation requiring stent positioning. We sought the following outcome: SFR at the last follow-up visit after a single session of PCNL.
Study screening and selection
Two independent authors screened all retrieved studies. Articles were included once agreed on by two reviewers independently. A third author solved discrepancies. Studies were included based on PICOS eligibility criteria. Only RCTs were accepted. Meeting abstracts, retrospective and prospective non-randomized studies, case reports, non-English, animal, and pediatric studies were excluded. The full text of the screened articles was selected if found relevant to the topic of this review. The research was further implemented by the manual search based on the references of the full-text relevant articles.
Data synthesis and statistical analysis
We aimed to perform a meta-analysis comparing the outcomes after PCNL using laser for kidney stones compared to PCNL using non-laser devices. Meta-analyses were performed when studies were reporting the same outcomes. The incidences of complications were pooled using the Cochran–Mantel–Haenszel Method with the random effect model and expressed as risk ratios (RRs), 95% confidence intervals (CIs), and p-values. RRs of more than one (1) indicate an increased risk of complications after non-laser procedures. Surgical time and length of stay were pooled using the inverse variance of the mean difference (MD) with a random effect, 95% CIs, and p-values. Analyses were two tailed, with a significance set at p ≤ 0.05 and a 95% CI. Study heterogeneity was assessed utilizing the I2 statistics. Substantial heterogeneity was defined as an I2 value >50%. Meta-analysis and risk of bias assessment were performed using Review Manager (RevMan) 5.4 software by Cochrane Collaboration. The quality assessment of the included studies was performed using the Cochrane Risk of Bias tool, using RoB 2. 7
Results
The literature search retrieved 2225 articles. Two hundred sixteen duplicates were removed. Two thousand nine articles were screened against title and abstract. One thousand nine hundred fifty-seven articles were excluded because the content was irrelevant for the purpose of this review. The full texts of the remaining 52 studies were assessed for eligibility and 46 articles were excluded because the content was irrelevant to this review. Finally, 6 articles were identified for meta-analysis. 8 –13 Figure 1 shows the PRISMA flow diagram of the study.
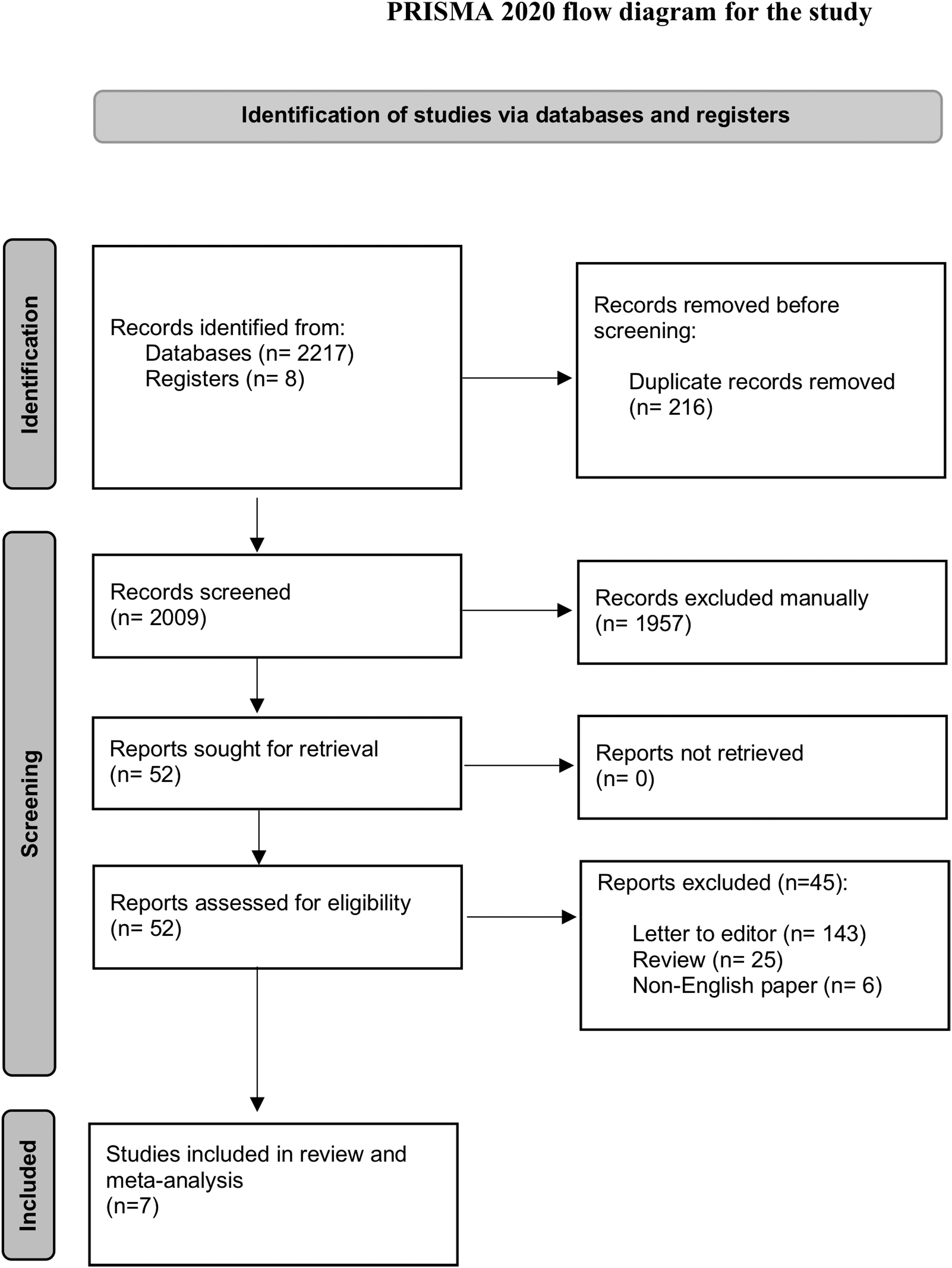
PRISMA 2020 flow diagram for the study. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study characteristics
There were 732 patients involved in 6 studies: 311 and 421 patients underwent laser and non-laser PCNL, respectively. Supplementary Table S1 shows the characteristics of the 6 studies included in this meta-analysis. 8 –13
Quality assessment
Supplementary Figure SF1 demonstrates the details of quality assessment for RCTs. Five studies showed a low overall risk of bias. 8,9,11,13 The remaining two studies showed some concerns about possible risks of bias, one attributable to missing outcome data 12 and one attributable to measurement of the outcome. 10
Surgical time, length of stay, and SFR
Data from five studies of 432 patients showed a significantly shorter surgical time in the non-laser group (MD: 11.14, 95% CI: 2.32 to 19.96, p = 0.002). Data from four studies of 372 patients showed a shorter postoperative stay in the laser group, but the difference did not reach statistical significance (MD: −0.81, 95% CI: −2.18 to 0.57, p = 0.25). Data from six studies, including 732 patients, showed a significantly higher SFR in the non-laser group (RR: 1.08, 95% CI: 1.01 to 1.15, p = 0.03). Study heterogeneity was substantial in surgical time (I 2 67%) and considerable in the length of stay (I 2 94%). However, heterogeneity was not important in SFR (I 2 0%). Figure 2 displays meta-analyses.

Meta-analysis of
Postoperative complications
Data from five studies, including 432 patients, showed a higher risk of postoperative fever >38°C in the laser group, but the difference did not reach significance (RR: 0.64, 95% CI: 0.31 to 1.30, p = 0.22). Data from five studies of 672 patients compared the need for blood transfusion and showed no difference between the two groups (RR: 1.02, 95% CI: 0.50 to 2.11, p = 0.95). Data from five studies, including 532 patients, compared the need for stent positioning because of urine extravasation and showed a higher risk in the laser group, but the difference did not reach significance (RR: 0.49, 95% CI: 0.17 to 1.41, p = 0.19). Heterogeneity was not important in blood transfusion (I 2 8%), postoperative fever >38°C (I 2 8%), and urine extravasation requiring ureteral stent positioning (I 2 0%). Figure 3 displays meta-analyses.
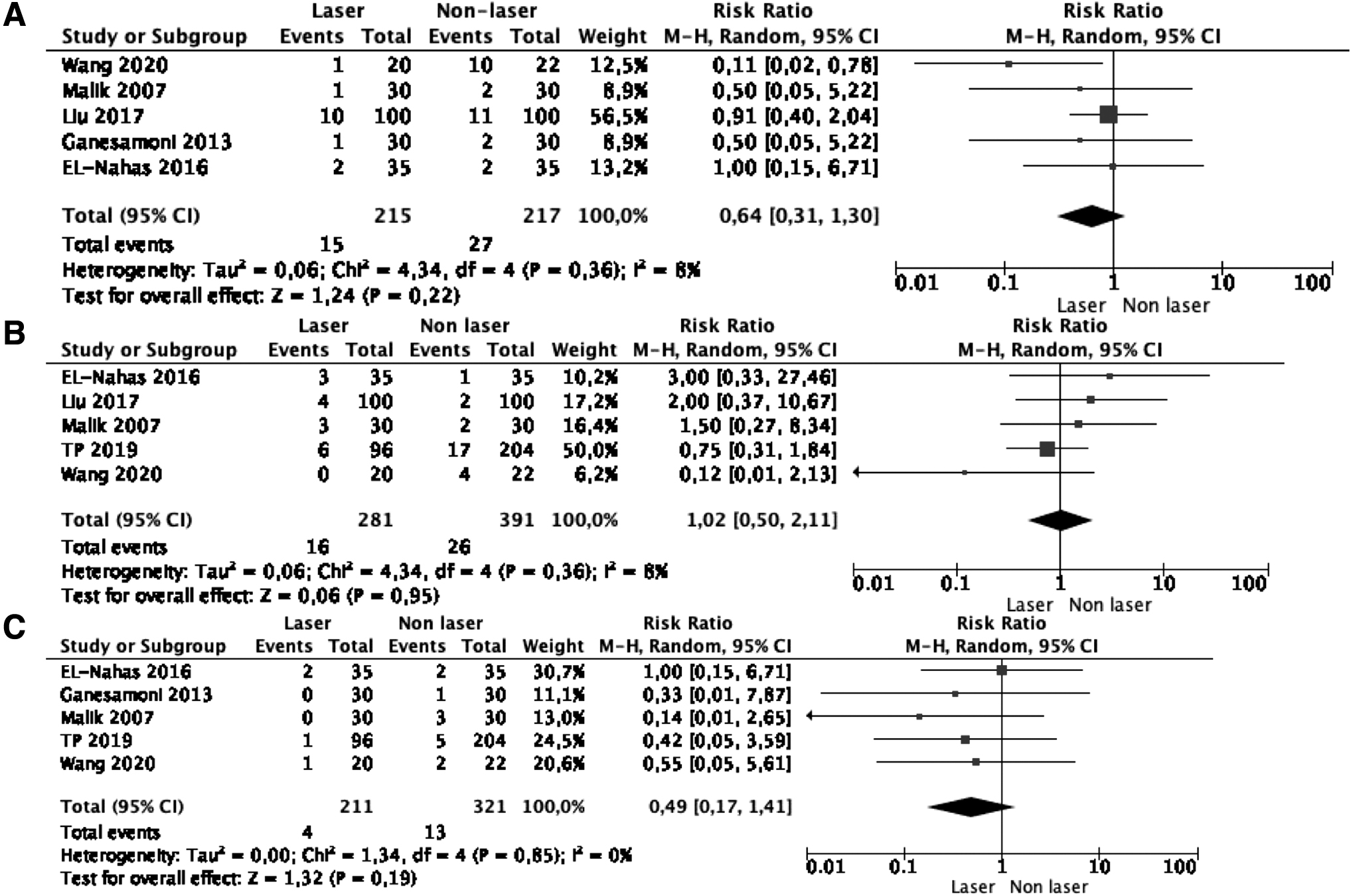
Meta-analysis of
Discussion
Ultrasonic lithotripsy was first introduced in 1970 and has been for decades the energy source of choice for PCNL, allowing a single-stage stone clearance in most cases. 4 Since then, a variety of intracorporeal lithotripter and suction devices (pneumatic, ultrasonic, and a combination of them) have been developed and made available for clinical use to improve the efficiency of stone clearance. The advancements in endoscopic instrument miniaturization and the introduction of holmium:yttrium aluminum garnet (Ho:YAG) lasers have made miniaturized PCNL a feasible option for upper tract stones. Furthermore, Ho:YAG lasers can be used in endoscopic prostate/urothelial tumor procedure, making lasers a single and appealing source of energy for different urological procedures.
Ho:YAG is a solid-state pulsed-wave laser that fragments stones by utilizing the photothermal ablation properties of the vaporization bubble, leading to destabilization and decomposition of the stone. 14 Still, Ho:YAG laser can fragment stones of any composition and hardness. 14 The introduction of high-powered Ho:YAG lasers with variable pulse energies and frequencies has enabled the ability to “dust” stones faster and more efficiently. 15 “Dust” can be easily aspirated or washed out, avoiding, probably, the need for fragment extraction and minimizing the operative time and residual stone fragments. Dusting is considered the correct way to follow in flexible ureteroscopy, but probably not in PCNL. Indeed, our results show that non-laser devices still demonstrated a significantly shorter operative time (MD: 11.14, 95% CI: 2.32 to 19.96, p = 0.002) and higher SFR (RR: 1.08, 95% CI: 1.01 to 1.15, p = 0.03) compared to Ho:YAG laser. EL-Nahas and colleagues randomized 70 complete staghorn stones patients to standard PCNL using VersaPulse PowerSuit 100 W Ho:YAG laser (Lumenis Inc., Dreieich-Dreieichenhain, Germany) or Calcuson ultrasonic lithotripter plus Endomat suction device (Karl Storz, Tuttlingen, Germany). 13 The laser power setting was 40 W (2 J and 20–30 Hz) and lithotripsy was attempted to achieve very small fragments that could pass through the Amplatz sheath with the irrigation fluid. The laser power was increased as much as 60 W for harder stone. Interestingly, the authors found that 60 W power was not a favorable setting for softer stones because it produced many large fragments, significantly increasing the operative time. This was confirmed in a study published by Kronenberg and Traxer. 16 They demonstrated that in vitro the ablation volume of artificial stones increases with the rising of laser energy (i.e., higher disintegration speed), whereas pulse frequency and total power play a less important role. 16 Thus, the laser energy of 2 J with a “painting technique” over the stone surface allowed EL-Nahas and colleagues to achieve comparable 3-month SFR between Ho:YAG laser (60%) and ultrasound lithotripsy (57%), but with a significantly shorter surgical time in the latter group (130 ± 34 vs 148.7 ± 35 minutes, p = 0.028). 13
Concerning Ho:YAG laser vs pneumatic lithotripsy, Ganesamoni and coworkers randomized 60 patients undergoing mini-PCNL (16.5F) for 15 to 30 mm renal stones. 8 Laser fragmentation started with low energy and high frequency (0.5 J, 20 Hz) and changed to high energy (1.5 J) and low frequency (6 Hz) for final fragmentation. Pneumatic lithotripsy was performed using a 1.0 mm lithoclast probe in single-pulse mode. In both arms, fragments were flushed out of the kidney through the sheath with saline irrigation. The authors showed that both lithotripsy devices were equally efficient stone fragmentation modalities in terms of fragmentation and surgical time, and SFR. Remarkably, stone migration was lower in the laser group (1.3–0.5 vs 1.7–0.8, p = 0.043), and fragment removal was easier with the laser (1.1–0.3 vs 1.7–1.1, p = 0.011). Selecting the most efficient lithotripter is of utmost importance in mini-PCNL because operative time has been shown to be prolonged owing to smaller instruments and sheath size, and proper fragmentation is key for procedure success. 17 Despite similar operative time and SFR, Ganesamoni and coworkers pointed out that pneumatic lithotripsy was fast at the beginning, but further fragmentation of the fragments became more difficult and time-consuming. Conversely, the laser approach of low energy and high frequency for the whole stone and high energy and low frequency for its fragments permitted a nearly uniform and efficient fragmentation throughout the procedure. 8 The ability of Ho:YAG laser to modify the settings to enhance lithotripsy and reduce fragment migration in inaccessible calices could be an important benefit, particularly in inexperienced hands.
A temporary renal function deterioration has been demonstrated to be associated with the high intrarenal pressure reached during endoscopic stone operation by irrigating fluid, which may result in pyelosinus, pyelovenous, and/or pyelolymphatic backflow. 18 The reported intrarenal pressure range during standard PCNL and mini-PCNL was 3 to 40.8 and 10 to 45 cm H2O, respectively. 19 Pyelovenous backflow may occur already at a pressure range of 13.6 to 27.2 cm H2O. 18 Theoretically, a higher intrarenal pressure may be necessary for a better view and stone removal with some energy devices. Liu and associates demonstrated in a randomized study of 200 patients undergoing laser vs pneumatic PCNL that serum creatinine increased in both groups 2 to 24 hours after the operation and decreased to a normal level 1 to 4 days after operation. Split renal function in diuresis renography was also similar in both groups 1 year after the procedure. 9 We found that patients undergoing laser PCNL had a nonsignificant higher risk of postoperative fever >38°C (RR: 0.64, 95% CI: 0.31 to 1.30, p = 0.22). Thus, we argue that the intrarenal pressure during laser PCNL was not higher, despite its longer surgical time, even if one attempts dusting.
The need for transfusion did not differ between the two groups in our study (RR: 1.02, 95% CI: 0.50 to 2.11, p = 0.95). Therefore, energy devices showed no different effect in bleeding during operation (i.e., damage to urothelium), which was be probably correlated to tract dilatation.
We showed that surgical time was significantly shorter in the non-laser group (MD: 11.14, 95% CI: 2.32 to 19.296, p = 0.002), and non-laser devices demonstrated higher SFR compared to Ho:YAG lasers (RR: 1.08, 95% CI: 1.01 to 1.15, p = 0.03). This result points out that current Ho:YAG lasers are probably still not efficient enough in lithotripsy than traditional devices in PCNL and advancements are required to compete with pneumatic and ultrasonic devices. We recently witnessed the introduction of the Moses technology that allows the so-called “Moses effect.” By adjusting the pulse regime, the laser pulse is modulated into two consecutive parts. The first part separates the water by creating a small vapor bubble (“the Moses effect”), and then the remaining energy is transmitted by the vapor bubble toward the target, with a decrease in energy loss and greater lithotripsy efficiency. 20 Leotsakos and associates reported a preliminary study on 12 patients with a mean stone diameter of 30.1 ± 11.1 mm undergoing ultra-mini PCNL (14F sheath) with the new 120-watt laser, with the Moses technology (Lumenis MOSES Pulse 120H). They showed excellent results with 11 patients out of 12 being completely free of any residual stone, with a mean surgical time of 86.4 ± 36.8 minutes. Remarkably, the mean laser time was very low at 755.7 ± 954.7 seconds. 21
Thulium-fiber laser technology has been recently introduced in clinical practice to challenge the Ho:YAG lithotripsy domination, showing multiple potential advantages. Thulium fiber laser has shown to be as much as fourfold faster without additional heat increase and less retropulsion in comparison to Ho:YAG laser. 22 Furthermore, thulium fiber laser promotes the development of novel miniature fiber optic delivery systems, including tapered, ball tip, hollow steel tip fibers, and muzzle brake fiber-optic tips, which can reduce both fiber burn back or degradation and stone retropulsion without sacrificing laser ablation rates. 23 Enikeev and coworkers reported the first clinical experience of thulium fiber laser “FiberLase” (NTO IRE-Polus, Russia) PCNL in 120 patients with renal stones as much as 30 mm (size tract 16.5F–17.5F). Laser settings were 6 to 40 W, 7 to 300 Hz, and 0.1 to 4.0 J with a 200 mcm laser fiber. Mean operative time (without puncture time) was 23.4 ± 17.9 minutes. SFR at 3-month follow-up was 85%, with a further residual stone size equal to or smaller than 3 mm in 7% and larger than 4 mm in the remaining 8% patients. 24 One of the main advantages of this laser was the insignificant retropulsion. Indeed, surgeons reported stone retropulsion with lithotripsy interference only in 1.7% of the cases. Gao and colleagues showed in a recent review in 13 small prospective cohort studies and one case series that thulium fiber laser had comparable SFR to Ho:YAG laser, but it was superior in operating time. 25
Our review is not devoid of limitations. First, we were able to find seven studies comparing Ho:YAG laser vs other lithotripsy devices in PCNL, including only 835 patients. Despite the low number of patients included, the quality of evidence of those studies was high because they were randomized prospective studies. Second, study heterogeneity was substantial in surgical time, but it was not important in SFR, allowing reasonable comparative results. Third, tract size ranged from 12F to 25F, and of course any non-laser device might not work as well in 20F to 24F accesses when applied in miniaturized settings. Finally, information on postoperative complications was inhomogeneous and allowed us to gather data only for blood transfusion, postoperative fever >38°C, and urine extravasation requiring ureteral stent positioning. Despite these limitations, this study provides a valuable synthesis of the current literature regarding comparative studies of Ho:YAG laser performance in PCNL compared to other energy sources.
Conclusions
Ho:YAG laser PCNL was associated with longer operative time and lower SFR. Postoperative fever, blood transfusion rate, length of stay, and the need for postoperative stenting did not differ between Ho:YAG laser compared to non-laser PCNL. The introduction in clinical practice of the Moses technology and thulium fiber laser raises the need for RCTs in the future comparing them to non-laser devices, particularly in miniaturized PCNL.
Footnotes
Authors' Contributions
V.G. conceptualization. V.G., M.C., E.J.L., and D.C. article writing. D.C. methodology and statistics. C.C. and C.M.S. data analysis. J.Y.C.T. and O.T. supervision.
Author Disclosure Statement
The authors have nothing to disclose.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Figure S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.