
Abstract
Background:
Robot-assisted simple prostatectomy (RASP) has emerged as a safe surgical treatment for patients with benign prostatic hyperplasia with large glands (>80 mL). Several studies reported on perioperative outcomes of RASP by the standard multiport (MP) da Vinci® robotic system approach. Studies conducted on RASP utilizing the novel single-port (SP) da Vinci SP robotic platform (Intuitive Surgical, Sunnyvale, CA) are scarce. We aimed to compare intraoperative and short-term postoperative outcomes between the da Vinci MP and SP robots for patients undergoing RASP in a referral center.
Methods:
In this retrospective study, we reviewed all patients who underwent RASP using MP or SP robot from September 2016 to March 2021. Intraoperative data, overall 30-day complications, complications by Clavien–Dindo classification, and 90-day readmission and reoperation rates were assessed and compared between the two groups using appropriate statistical methods.
Results:
Seventy-five patients who underwent RASP were identified. Of these, 47 were in the MP group and 28 were in the SP. Compared with SP, mean operative time in MP group was 216.6 vs 232.4 minutes (p = 0.39), estimated blood loss was 195.7 vs 227.1 mL (p = 0.43), and length of stay was 2 vs 2.5 days (p = 0.45). There was a trend toward higher overall complication rate in SP group vs MP (42.86% vs 21.28%, p = 0.09). There were no significant differences in the readmission (17.02% vs 10.71%, p = 0.52) and reoperation (2.1% vs 7.14%, p = 0.34) rates between MP vs SP group.
Conclusion:
SP-RASP is safe and shows equivalent perioperative outcomes when compared with the MP robotic system. A marginal increase of complication rate was recorded in the SP group; however, this did not demonstrate statistical significance.
Introduction
Lower urinary tracts symptoms (LUTS) attributed to benign prostatic hyperplasia (BPH) can significantly affect quality of life in aging men. 1 In the setting of prostate size >80 mL, open simple prostatectomy has been recommended as option for surgical treatment. 2,3 However, it has been shown that open approach is associated with higher estimated blood loss (EBL) and longer length of stay (LOS) compared with other alternatives such as holmium laser enucleation of the prostate and laparoscopic prostatectomy. 4,5 Hence, robot-assisted simple prostatectomy (RASP) has increasingly been pursued with emerging evidence of promising results. 6,7 Several reports have demonstrated that RASP is a safe and effective modality for treatment of large glands. In addition, it is currently recommended as an alternative option to the open surgical approach. 8,9
In an effort to further reduce the morbidity, simple prostatectomy using the novel single-port (SP) da Vinci® SP robotic platform (Intuitive Surgical, Sunnyvale, CA) was initially described in 2012. 10 The SP-RASP provides several merits such as robot docking inside the bladder with better adenoma visualization and avoidance of bowel manipulation. 11 Nevertheless, there has been absence of evidence comparing the perioperative outcomes between the traditional multiport (MP) and the SP robotic systems in the setting of simple prostatectomy. Hence, we sought to investigate the intraoperative and short-term postoperative outcomes between the MP- vs SP-RASP in our tertiary referral center.
Materials and Methods
Patient cohort
We conducted a retrospective review of all patients with BPH who underwent RASP using MP or SP robotic system from September 2016 to March 2021 from our institutional database after Institutional Review Board approval. All procedures were equally performed by two surgeons (A.G. and J.V.J.) and da Vinci Xi robot was used as the MP robot. Prostate volume was determined using prostate image studies such as transrectal ultrasonography, prostate MRI, and CT scan. Other workup included digital rectal examination, serum creatinine, prostate-specific antigen (PSA), and urine analysis reflex to culture. Patients' demographics, perioperative data, and postoperative outcomes were collected. A total of 75 patients who underwent RASP for different indications were identified. Of these, 47 were in the MP-RASP group and 28 were in the SP-RASP. Within the MP-RASP group, 26 (55.3%) patients received transperitoneal transvesical approach and 21 (44.7%) received extraperitoneal transcapsular approach. All patients in SP-RASP group underwent the operation using the extraperitoneal transvesical approach.
Surgical technique
Our technique includes two different approaches for MP-RASP, either traditional transperitoneal or extraperitoneal. For SP-RASP, we utilize the extraperitoneal transvesical approach. Transperitoneal transvesical MP-RASP approach has been described in several reports. 12,13
Extraperitoneal transcapsular MP-RASP approach
We described this technique in a cases series of 33 patients. 14 Procedure starts with a 3 cm infraumbilical incision, which is carried down to the anterior rectus sheath. A 1-cm incision is made in the fascia and the midline is developed. The rectus muscle is swept laterally to create the extraperitoneal space. A balloon dilator is passed and manually inflated, gradually expanding the space of Retzius.
Port placement configuration is given in Figure 1. Mild Trendelenburg (around 10°–15°) is usually sufficient during this approach. The robot is then docked. The anterior prostate capsule is exposed. A transverse capsulotomy, 2 cm from the bladder neck, is performed as described by Millin. 15 Prostate adenoma is resected circumferentially after which the urethra is incised (Fig. 2). The posterior bladder wall is sutured to the prostatic fossa and continued circumferentially. After Foley catheter placement, closure of the anterior capsulotomy is performed.
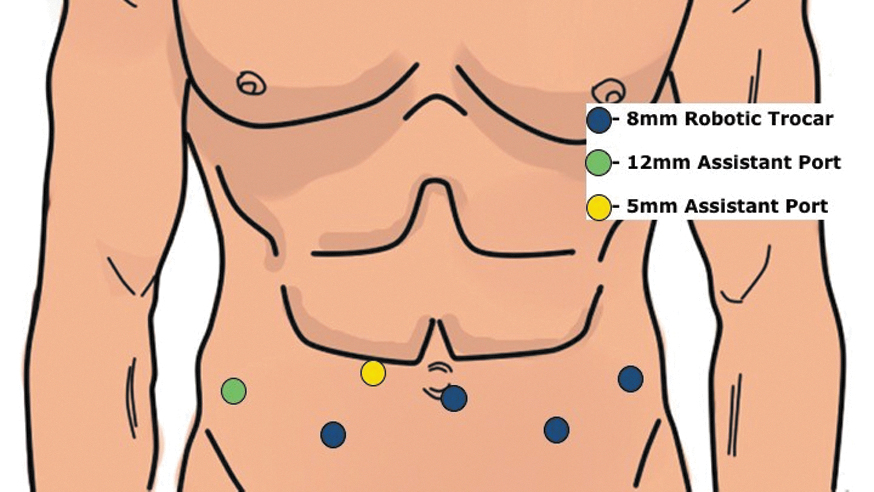
Diagrammatic representation of port placement sites. Color images are available online.
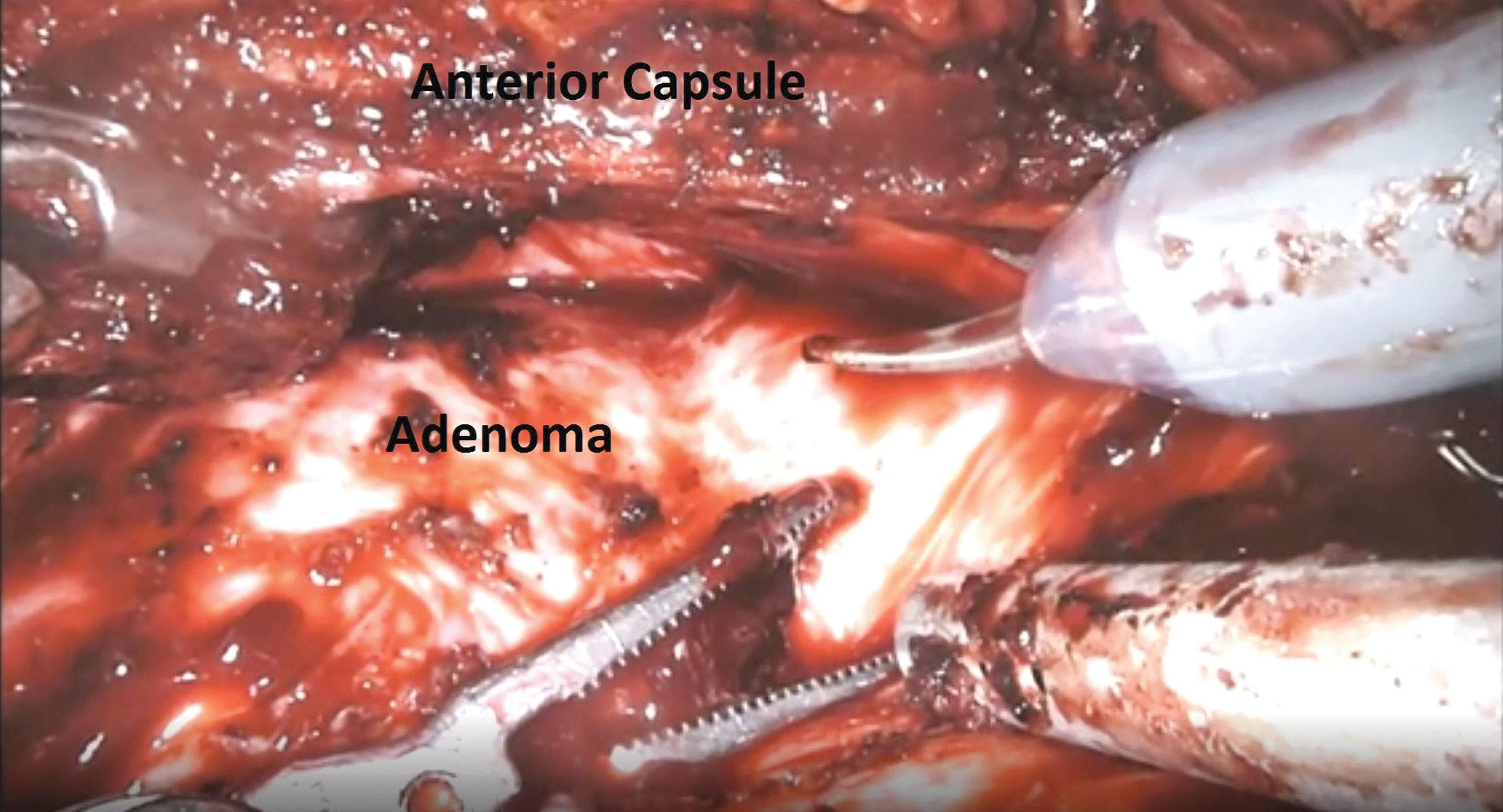
Transcapsular resection of the adenoma. Color images are available online.
Extraperitoneal transvesical SP-RASP approach
The patient is placed in the supine position. A 20F Foley catheter is inserted, and the bladder is filled with sterile water. A 3 cm infraumbilical incision is carried out. This is carried down to the fascia that was then opened separately. The muscle is swept laterally using index finger. The transversalis fascia is divided and the distended bladder is then identified after instillation of saline. The anterior bladder wall is opened in the same longitudinal incision ∼2.5 inches in length. A GelPOINT mini-system (Applied Medical, Rancho Santa Margarita, CA) is used for ports placement. The 25 mm SP cannula with a multichannel guide port as well as a 5 mm port and 10 mm AirSeal (ConMed, Largo, FL) trocar were inserted into the GelSeal cap. The 5 mm port is used for insertion of suction tubing, which is manipulated by the surgeon and kept accessible in the operative field. The 10 mm AirSeal port is used by the assistant for passage of sutures, and the specimen retrieval bag. The SP robot is then docked. We place the camera in 12 o'clock position for all cases. In select cases with enormous glands, we transiently switch the camera in the 6 o'clock position so we can use the fenestrated forceps to retract the adenoma anteriorly to facilitate posterior deep dissection. After dissecting the adenoma circumferentially and incising the urethra, the adenoma is placed in the bladder for later extraction. The urethrovesical anastomosis is performed (Fig. 3). A 20F three-way Foley catheter is inserted, then a 10 cm bag is inserted through the assistant trocar for retrieval. The bladder is closed in two-layer manner using 2-0 Vicryl sutures and checked for water tightness. The fascia is then closed followed by the skin subcuticular closure.

Vesicourethral anastomosis completed. Color images are available online.
Postoperative care
In our practice, we tend to insert a 19F Blake pelvic drain only if extraperitoneal transcapsular MP approach is utilized. In other approaches, watertight closure of the bladder allows for minimizing the risk of leak and subsequently the necessity of drain insertion.
Postoperatively, continuous bladder irrigation is started if concern for significant gross hematuria or clotting is present. Typically, patients are discharged within 1 to 2 days with the catheter in place after removal of the drain if present. The catheter is removed 7 to 10 days later without prior imaging.
Data collection
Patients' demographics and clinical characteristics collected were age, body mass index (BMI), American Society of Anesthesiologists (ASA) score, preoperative PSA level, prostate volume, prior prostate surgeries, indication for RASP, and concomitant procedures. Intraoperative data included operative time, EBL, and intraoperative complications. Postoperative data included LOS, catheterization time, postoperative voiding status, specimen weight, histopathological findings, 30-day complications, and mortality rate, as well as 90-day reoperation and readmission rates. Complications were recorded according to the Clavien–Dindo classification system (grade <3 vs ≥3).
Statistical analysis
The mean values and standard deviations were calculated for continuous outcomes in each group. Two-sample t-test was used to compare the mean values between two groups. Pearson's chi-square test or Fisher's exact test were used to compare frequencies for categorical outcomes between two groups. The significance level was set to 0.05 for all analyses. The statistical analyses were implemented with SAS 9.4 (SAS Institute Inc., Cary, NC).
Results
There was no significant difference between both groups regarding age, BMI, preoperative prostate volume (Fig. 4), ASA class, preoperative PSA, and indications for operation (Table 1). Severe obstructive urinary symptoms or failed medical treatment was the most common indication in both groups (48.94% in MP vs 53.58% in SP). Seven patients (14.89%) in the MP group received prior prostate procedure such as transurethral resection of prostate and prostate fulguration vs no patients in the SP group (p = 0.041).
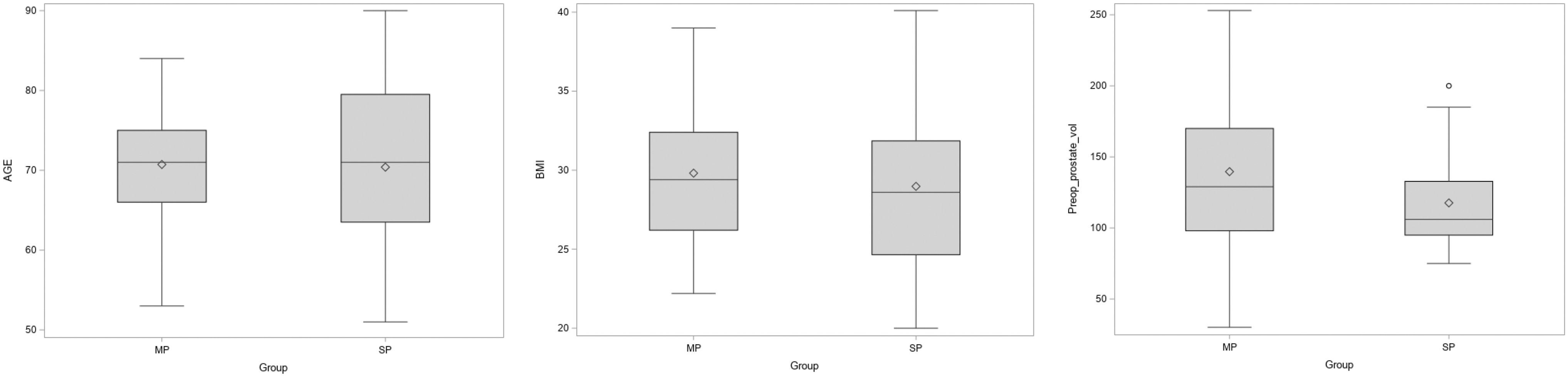
Boxplot for age, BMI, and preoperative prostate volume for MP- vs SP-RASP groups. BMI = body mass index; MP = multiport; RASP = robot-assisted simple prostatectomy; SP = single port.
Preoperative Characteristics of Patients Undergoing Multiport- vs Single-Port Robot-Assisted Simple Prostatectomy
ASA = American Society of Anesthesiologists; LUTs = lower urinary tract symptoms; m = missing; MP = multiport; RASP = robot-assisted simple prostatectomy; SP = single-port.
Both groups showed comparable perioperative outcomes as given in Table 2. However, there was a trend toward longer mean operative time (232 ± 86 minutes vs 217 ± 59 minutes, p = 0.39) and LOS (2.5 ± 3.3 days vs 2 ± 1.3 days, p = 0.45) in SP-RASP vs MP-RASP. Similarly, there was no significant difference in EBL (mL) between both groups (227 ± 197 in SP vs 196 ± 103 in MP, p = 0.44). No patient required blood transfusion in both groups.
Perioperative Outcomes of Multiport- vs Single-Port Robot-Assisted Simple Prostatectomy
SD = standard deviation.
Recorded concomitant surgeries were bladder stone extraction, umbilical hernia repair, and excision of bladder diverticulum. There was no significant difference in proportion of patients who received concomitant surgeries between groups (p = 0.55). Mean catheterization time was 10.2 to 10.5 days in both groups. All patients in both groups voided spontaneously after urethral catheter removal. The mean retrieved adenoma weight was greater in the MP group (98.5 ± 58.3 g) vs SP group (67.9 ± 45.3 g, p = 0.01). Only 3 (4%) patients in both groups had evidence of prostate cancer (Gleason score 3 + 3 and 3 + 4) in histopathological analysis.
With regard to postoperative complications (Table 3), there was a trend toward higher 30-day complication rate in SP group (42.86%) vs MP (21.28%); however, it lacked statistical significance (p = 0.098). Rate of major complications (Clavien–Dindo classification ≥III) was 4.26% in MP vs 7.14% in SP group (p = 0.21).
The 30- and 90-Day Postoperative Outcomes
A majority (87%) of the recorded complications were minor (Clavien–Dindo classification of I, II) such as epididymitis, epididymo-orchitis, mild hematuria, urinary tract infections, later onset urinary retention, atrial fibrillation, and prerenal azotemia. All patients were managed conservatively by appropriate medical therapy without serious consequences. Recorded major complications were urethral stricture, severe hematuria, pulmonary embolism, intraoperative air embolus, and respiratory arrest on the way to postanesthesia care unit (PACU). All critical patients were resuscitated in intensive care unit and responded appropriately.
Rates of 90-day readmission and reoperation were not significantly different between groups. One patient required visual internal urethrotomy for anterior urethral stricture in MP group and two patients underwent clot evacuation with fulguration for severe gross hematuria in SP group (p = 0.34). Readmissions occurred for urosepsis, urinary tract infections complicated by delirium, prerenal azotemia, need for endoscopic intervention for urethral stricture, and gross hematuria. No 30-day mortality was recorded in both groups.
Discussion
In the setting of large prostate glands (≥80 g), open simple prostatectomy provides effective and durable relief of LUTS with minimal rate of reoperation; however, it is associated with some morbidtiy. 16 RASP has been utilized broadly with evidence of lower rate of postoperative complications with shorter LOS. 8 With the increasing adoption of the SP robotic system, several reports have shown its safety and efficacy as a surgical treatment for patients with BPH. 11,17
Our cohort of patients was identified during a span of 4.5 years. Both MP and SP groups were similar with regard to demographics and preoperative characteristics. At our institution, we started performing SP-RASP as soon as the SP robot became available and active. Of note, they only differed in the patient proportion who received prior prostate procedure, with MP group being higher (p = 0.041).
In our practice, we utilize diverse approaches for RASP, which is accustomed to several factors such as patients' prior abdominal surgeries and associated bladder pathology report, that is, stone and diverticulum. We tend to favor extraperitoneal approach in patients with extensive previous surgeries where intraperitoneal access might be problematic. We found several merits of transvesical approach when using SP-RASP as reported in several articles such as fast and direct access of the adenoma, and exclusive insufflation of the bladder with carbon dioxide (CO2) gas with lower pressures (pneumovesicum). 10,11 Extraperitoneal SP-RASP was also described with satisfactory results. 17 The authors used a separate assistant port in the left lateral quadrant for suction and suture passage. 17
In our study, the operative time was recorded from the skin incision to closure. The mean operative time was longer in the SP-RASP, but without reaching statistical significance (232.4 ± 86.2 vs 216.6 ± 59.1 minutes, p = 0.395). Mean operative time in our MP-RASP group was similar to Leslie and colleagues series of patients with operative time of 214 minutes (range: 165–345). 18 The median operative time in our SP-RASP was 216.5 minutes, which is slightly longer than what was reported in Kaouk and others study (190 minutes) of 10 patients. It is noteworthy to mention that our SP group is larger with 21.43% of patients receiving concomitant procedures such as extraction of bladder stones in three patients, bladder diverticulectomy in two and umbilical hernia repair in one.
For MP-RASP group, our mean EBL was 195.7 mL, which is lower than what was reported in several reports. Mourmouris and colleagues reported 274 mL in a series of 7 patients and Simone and coworkers reported 250 mL in series of 12 patients. 19,20 However, Steinberg and others reported mean EBL of 141 mL in 10 patients. 17 We believe that the best EBL outcomes depend on the fine definition of the plane between the adenoma and surgical capsule and the judicious use of electrocautery during circumferential dissection. Mean EBL in our SP-RASP group was 227.1 mL, which is lower than the first SP-RASP report of Fareed and others (425 mL) and higher than that of the latest Kaouk and associates report in 2020 with median EBL of 100 (interquartile range, 68–175) mL. 11
The reported mean LOS in several reports of MP-RASP was widely varied from 1 to 8.8 days. 21 –23 Our mean LOS in the MP group was 2 ± 1.3 days. This was not significantly different from the SP group (2.5 ± 3.3 days, p = 0.452). Our practice is keeping the patient overnight with or without continuous bladder irrigation and removal of the pelvic drain if present before discharge. A few patients might need an extra day to ensure tolerance to regular diet and adequate pain control.
In our study, the mean weight of adenoma was significantly greater in the MP group compared with SP (98.5 ± 58.3 g vs 67.9 ± 45.3 g, p = 0.013). Possible explanation is the higher preoperative mean prostate volume in the MP group, which was marginal to statistical difference compared with SP (139.6 ± 54.7 g vs 117.6 ± 34.5 g, p = 0.0548).
With regard to postoperative outcomes, there was no significant difference in the rate of 30-day complications, and 90-day readmissions and reoperations between both groups. However, there was a trend toward higher complication rate in the SP group (42.86% vs 21.28%, p = 0.098). A majority of complications (87%) were low grade. High-grade complications were recorded in the MP group in two patients, one because of respiratory arrest on arrival to PACU. The patient was resuscitated and was admitted to surgical intensive care unit (SICU) with return of ventilations and consciousness after 90 seconds. The second patient started having obstructive symptoms 3 to 4 weeks from operation and was found to have bulbar urethral stricture and underwent direct visual internal urethrotomy.
In the SP group, high-grade complications were recorded in two patients. One patient was 80 years old, who developed intraoperative air embolism, manifested by hypotension with drop of end-tidal CO2 to <10. Instantly, the pneumovesicum was dropped down from 12 to 8 mm Hg. Intraoperative transesophageal echocardiogram was performed, which showed air embolus in the right atrium. Anesthesia team decided to continue the procedure and supportive management was given until the case is completed. The patient remained intubated postoperatively and was transferred to SICU for further management. He eventually stabilized and was transferred to the floor after 10 days of SICU admission. The second patient was 79 years old who presented with syncope and dyspnea on postoperative day 14 and was found to have extensive bilateral pulmonary embolism. The patient was started on anticoagulation, which was complicated by extensive hematuria necessitating transfusions and return to operating room for clot evacuation and fulguration. On discharge, the patient was ambulating with assistance and had no additional hematuria.
In the first SP-RASP of Fareed et al., high-grade complications were reported in 3 of 9 patients. 10 In Kaouk and others' report of 10 patients, only 1 patient developed epididymitis managed with oral antibiotics. For MP-RASP, our complication rate (21.28%) was similar to Johnson and others study on 120 cases with complication rate of 18.3%. 21 Chavali and colleagues reported the same rate (22.2%) in 28 patients. 24 Mourmouris and colleagues 19 reported lower rate of 3.8% in 26 patients, whereas Umari and others 25 reported a higher rate of 31% in 81 patients.
To the best of our knowledge, our study represents the first report that performs a head to head comparison between the MP- and SP-RASP with focus on the perioperative outcomes; however, it is not without limitations. First, it comprised a relatively small sample size and the inherent selection bias owing to its retrospective nature. Second, a proportion of patients in both groups had concomitant surgeries; despite being relatively minor procedures, they might have affected some intraoperative characteristics. Third, as surgeries were performed by two surgeons, differences in the individual experience and intraoperative strategies could have affected our results. Fourth, postoperative functional metrics such as pain control and uroflowmetry were not recorded. Nevertheless, the fact that the majority of patients were discharged within 1 to 2 days and voided spontaneously after catheter removal would provide a clue about these perspectives postoperatively.
Conclusion
SP-RASP is safe and offers comparable intraoperative and postoperative outcomes when compared with the standard MP system. There was a trend toward a higher complication rate in the SP group; however, this failed to demonstrate statistical significance. Safety and efficacy of SP-RASP should be further investigated in the context of long-term randomized trials to set its rank within the armamentarium of BPH treatment strategies.
Footnotes
Authors' Contributions
M.I.K.: Conceptualization, data curation, resources, writing—original draft. A.C.: Conceptualization, data collection. J.V.J.: Conceptualization, writing—review and editing. A.G.: Conceptualization, supervision, validation, writing—review and editing.
Author Disclosure Statement
A.G.: Grant from intuitive surgical and Coloplast. Consultant for Medtronic, J & J, Ollympus and virtuoso. J.V.J.: consultant with Boston scientific. All other coauthors report no conflicts of interest.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.