
Abstract
Background:
Previous randomized-controlled trials have demonstrated that intraoperative intravenous mannitol administration shows no added value on renal functional preservation after partial nephrectomy (PN) in patients with normal renal function. However, the renoprotective effect of mannitol has not been fully evaluated in patients with preoperative chronic kidney disease (CKD).
Materials and Methods:
This was a retrospective cohort study with propensity score matching. Patients with a preoperative estimated glomerular filtration rate (eGFR) of <60 mL/minute/1.73 m2 undergoing PN were enrolled in the study between January 2012 and December 2019 in Peking University First Hospital. Participants were divided into two groups: patients who received 25 g of mannitol (group M+) or not (group M−). The primary endpoint was the decreased rate of eGFR at the 6-month follow-up.
Results:
A total of 244 patients were included in the analysis. After propensity score matching, 80 patients remained in each group. The percentage of decrease from baseline eGFR at postoperative 6-month follow-up showed no difference between the two patient groups (median 11.1 [interquartile range 5.3–25.3] in group M+ vs 12.2 [4.7–21.3] in group M
Conclusions:
A 25 g dose of mannitol administration during PN failed to provide added value on renal functional preservation in CKD patients.
Introduction
Partial nephrectomy (PN) is an established approach for the management of localized renal tumors. 1 Traditionally, mannitol has been administered before removal of renal artery occlusion to attenuate ischemia/reperfusion injury as an oxygen-free radical scavenger 2,3 and an osmotic diuretic. 4 In recent years, two double-blinded randomized trials by Spaliviero and colleagues 5 and Choi and colleagues 6 have provided solid evidence that intraoperative intravenous mannitol administration during PN had no demonstrable clinical benefit compared with standardized fluid hydration in patients with normal preoperative renal function.
However, some experts in this field suggested that these previous findings failed to discourage the routine use of mannitol. 7,8 First, high-risk patient populations, such as those with low preoperative estimated glomerular filtration rate (eGFR), were not included in the previous studies and these patients were most likely to benefit from renal functional preservation strategies. Second, the doses of mannitol applied in the randomized trials 5,6 were 12.5 and 12.0 g, respectively, which are considered low doses. It is recommended to administer the most utilized dose of 25 g in contemporary practice. 9
Before now, the renoprotective effect of mannitol has not been well evaluated in patients with preoperative chronic kidney disease (CKD). Since CKD patients undergoing PN are uncommon, it is difficult to recruit participants and carry out a randomized-controlled trial. We conducted a retrospective cohort study in a tertiary high caseload center to assess the effect of a 25 g dose of mannitol on postoperative renal function in patients with preoperative eGFR <60 mL/minute/1.73 m2 undergoing PN.
Materials and Methods
Study design and ethics
The present study was a retrospective cohort study. The study protocol was approved by the Clinical Research Ethics Committee of Peking University First Hospital, Beijing, China, on December 2, 2020 [approval number: 2020(394), Chairperson Prof. Bao-Wei Zhang]. Written informed consent was waived because of the retrospective nature of our study. All data were maintained with confidentiality. The study was conducted according to the guidelines of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE).
Participants
Potential participants who underwent PN at Peking University First Hospital were screened using the electronic medical records system from January 2012 to December 2019. This series included all cases of open and laparoscopic PN performed during this period. Exclusion criteria for patients were as follows: (1) younger than 18 years; (2) baseline eGFR ≥60 mL/minute/1.73 m2; (3) combined surgery; (4) bilateral PN at the same time; (5) no renal artery clamp; (6) multiple tumors; (7) renal surgery within 6 months after PN; and (8) unavailable postoperative 6 months serum creatinine measurements. In the present study, CKD was defined as preoperative eGFR <60 mL/minute/1.73 m2.
Patients were divided into two groups according to whether they received mannitol (group M+) or not (group M−). In group M+, patients were administered mannitol at 25 g (125 mL of a 20% mannitol solution).
Perioperative management and follow-up
All patients underwent a routine history and physical examination, as well as an abdominal and pelvic computed tomography scan and/or a renal ultrasound within 2 months of surgery, electrocardiogram and chest X-ray within 30 days of surgery, and preoperative laboratory investigations, including baseline eGFR.
The choice of approach was at the discretion of the patient and the treating surgeon. In general, tumor diameter >7 cm or a R.E.N.A.L. score of 10 and higher was an indication for an open approach. Cold ischemia was performed in most open surgeries, whereas warm ischemia was routine for laparoscopic surgery. The choice of mannitol was at the discretion of the treating urologist and anesthesiologist. If mannitol was chosen, a standard dose of 25 g (125 mL of a 20% mannitol solution) was completely administered intravenously within 20 minutes before vascular occlusion of the renal artery.
All patients were intubated under general anesthesia. Propofol or/and etomidate were used for anesthesia induction. Propofol, sevoflurane, or/and nitrous oxide were used for anesthesia maintenance. Remifentanil was continuously pumped and sufentanil was intermittently given for analgesia. Rocuronium and cisatracurium were given for muscle relaxation. All patients were monitored by routine electrocardiogram, pulse oximetry, invasive arterial blood, capnography, bispectral index, temperature, and urine output.
When discharged from the hospital, patients would be advised to complete a reexamination 6 months following surgery; thereby, the postoperative 6-month (between 4 and 8 months after surgery) serum creatinine and eGFR measurements were obtained from the Laboratory Information Management System of our hospital. However, a small proportion of patients (18%) chose to be reexamined in other medical centers and a follow-up call was performed to obtain their serum creatinine and eGFR measurements.
Data collection
Data were collected using electronic medical records, anesthesia information system, and electronic image management system. The following patient information was collected: (1) demographic data, including age, sex, and body mass index (BMI); (2) preoperative data, including comorbidity, premedication, laboratory investigations (baseline serum creatinine, baseline eGFR, hemoglobin, and albumin), imaging information (tumor size and location), and solitary kidney; (3) intraoperative data, including the type of surgery (open or laparoscopic), type of ischemia (warm or cold), clamp time, surgical duration, fluids, urinary output, and estimated blood loss; and (4) postoperative data, including complications, renal replacement therapy, serum creatinine within 48 hours, and eGFR at the 6-month follow-up.
Endpoints of the study
The primary endpoint was the decreased rate of eGFR at postoperative 6-month intermediate-term follow-up, calculated by the following:
Statistical analysis
A logistic regression model was used for the propensity score match (PSM) using SPSS version 22 (IBM, Armonk, NY), and the free software package “R” version 2.15.3, including the “SPSS Statistics Essentials for R 22.0” and “psmatching 3.04” plugin, was used. Patients were matched in a 1:1 ratio using the nearest-neighbor matching with caliper widths equal to 0.2 of the standard deviation of the logit of the propensity score. The odds ratio (OR) was used to represent the probability that a patient received mannitol administration.
We selected matching variables a priori if they were relevant to postoperative kidney function. The following variables were used for matching: age, sex, BMI, hypertension, diabetes mellitus, baseline eGFR, hemoglobin, albumin, maximal tumor diameter, tumor location, tumor contact with renal sinus, solitary kidney, surgical approach (open or laparoscopic), clamp time, type of ischemia (cold or warm), and estimated blood loss. Continuous variables were presented as mean ± standard deviation for normal distribution or as median (lower and upper quartiles) for skewness distribution. Categorical variables were presented as numbers (%). Between-group differences for propensity score matching were compared using the standardized differences (SDs). An absolute SD ≥0.255 (i.e.,  ) was considered imbalanced.
13
There were no missing variables for PSM in all patients.
) was considered imbalanced.
13
There were no missing variables for PSM in all patients.
For endpoints, continuous variables were compared using the Student t-test for normal distribution and Mann–Whitney U test for skewness distribution. Categorical variables were analyzed using the χ 2 test. The median difference (and 95% confidence interval [CI]) between the two groups was calculated with the Hodges–Lehmann estimator. To evaluate the interaction effect of subgroups on the association between the choice of mannitol and % change from baseline eGFR at 6 months postoperatively, we used the Z test to compare the difference between the two regression coefficients from subgroup analysis by using the following equation:
To further confirm the effect of mannitol on postoperative renal function, we applied a logistic regression model adjusting for covariates, which were considered clinically relevant to postoperative renal function, to examine the association between intraoperative mannitol infusion and postoperative AKI and 6-month eGFR >20% decrease from baseline eGFR in the matched patients. First, univariate logistic regression analysis was used to screen predictors that might be associated with postoperative renal function (p < 0.10).
The presence of multicollinearity between related parameters was determined using a variance inflation factor of >10. If multicollinearity was observed between parameters, one parameter was left for analysis that considered the p-value and clinical usefulness. Then, these selected predictors and mannitol were included in the multivariate logistic regression model to determine whether mannitol was the independent predictor of AKI and 6-month eGFR >20% decrease from baseline eGFR with the forward method. A p value of <0.05 (two sided) was considered statistically significant.
Results
Patient recruitment
A total of 4054 PN cases were obtained from the anesthesia information system from January 2012 to December 2019. Two hundred seventy-six cases with a baseline eGFR <60 mL/minute/1.73 m2 were eligible for the study. Among them, 32 cases were excluded, including 4 for multiple tumors, 3 for combined surgeries, 3 without renal artery clamp, 1 for bilateral PN, 1 for nephrectomy within 6 months after PN, 20 for post-6-month eGFR measurements missing. Of the remaining 244 patient cases, 100 cases received 25 g of mannitol and 144 cases did not. After PSM, 80 patients remained in each group for further evaluation (Fig. 1).
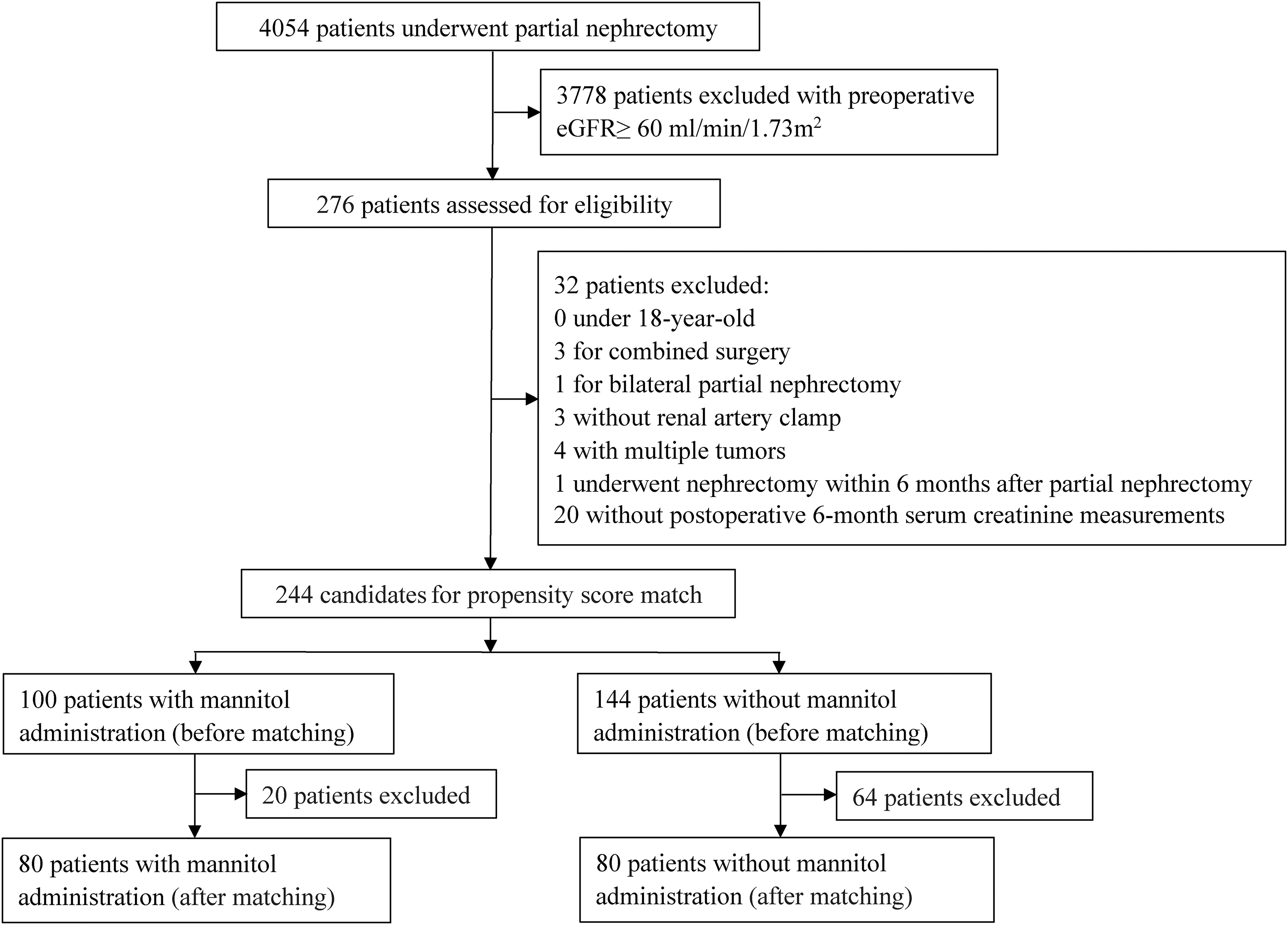
Flowchart of the present study.
Baseline, preoperative, and intraoperative data before and after PSM
Before matching, proportions of patients who had complications such as diabetes mellitus (37.0% vs 23.6%, SD = 0.276) and who received cold ischemia (22.0% vs 7.6%, SD = 0.345) were different between the two groups. Renal artery clamp time (median 25 minutes [interquartile range, IQR 20–30] vs 20 [15–25], SD = 0.492) was different between the two groups as well. After matching, all confounding variables were well balanced (Table 1).
Variables Used for Propensity Score Matching
Data are presented as mean ± standardized deviation, number of patients (percentage), or median (interquartile range). SDs in bold indicate those with an absolute value of ≥0.255.
eGFR = estimated glomerular filtration rate; SD = standardized difference.
Renal function and adverse event outcome in the matched cohort
Percentage of decrease from baseline eGFR in postoperative 6-month follow-up was not different between the two groups (median 11.1 [IQR 5.3–25.3] in group M+ vs 12.2 [4.7–21.3] in group M−, median difference
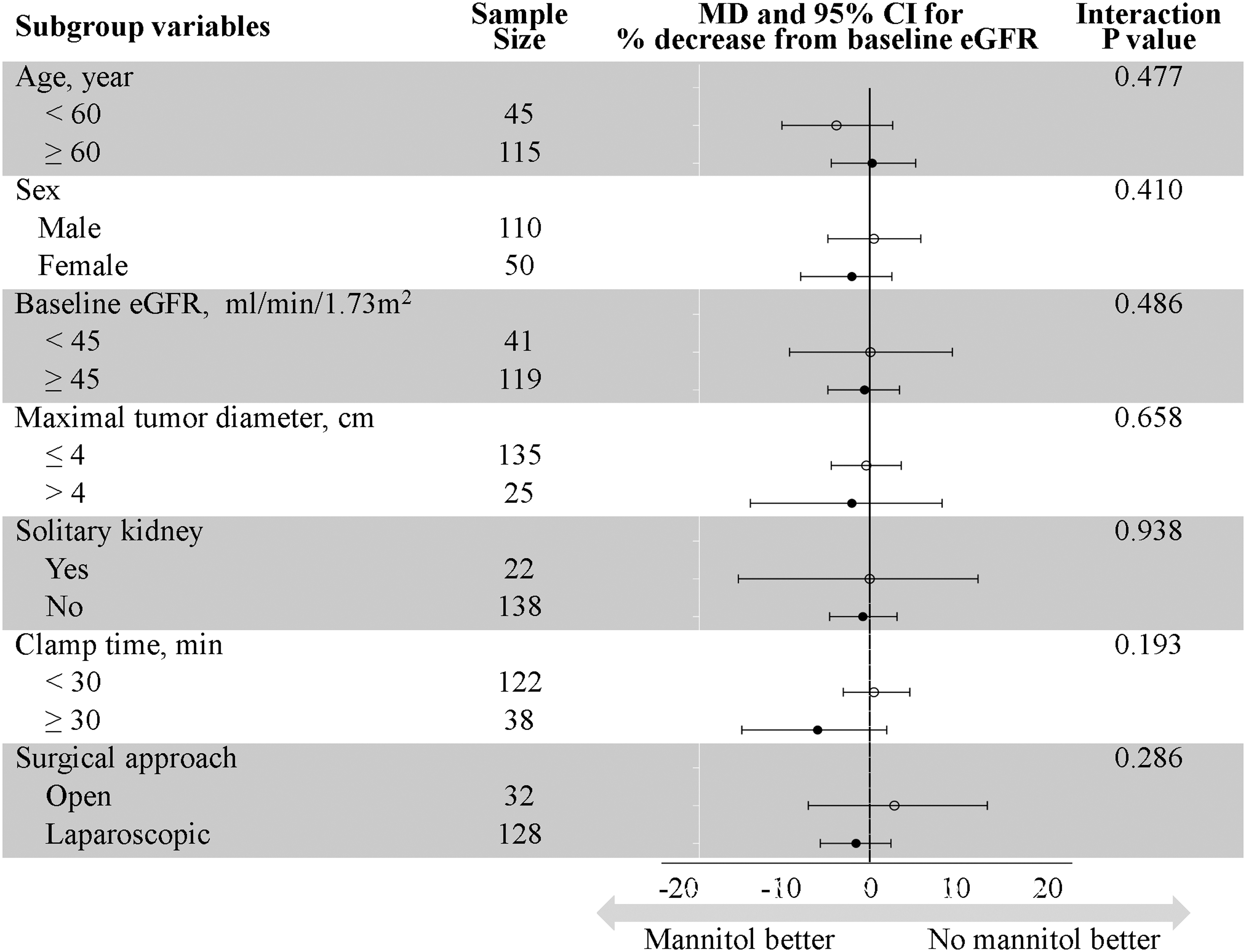
Interactions of the subgroups on the association between intraoperative intravenous mannitol administration and percent decreased from baseline eGFR at 6-month follow-up in the propensity score-matched cohort. eGFR = estimated glomerular filtration rate; MD = median difference.
Endpoints of the Matched Cohort
Data are presented as mean ± standardized deviation, number of patients (percentage), or median (interquartile range).
Defined as Clavien–Dindo classification Grade ≥II.
CI = confidence interval.
Thirty-two patients had complicated AKI in both group M+ and group M− (p > 0.999). Two patients in group M+ needed renal replacement therapy during hospitalization and both recovered when discharged. Patients with postoperative complications (three cases vs four cases, p > 0.999), incidence of >20% decrease from baseline eGFR at the 6-month follow-up (31.3% vs 30.0%, p = 0.864), and dialysis at 6-month follow-up (three cases vs two cases, p > 0.999) were similar between the two groups.
Independent predictors for postoperative renal function
Male gender, low baseline eGFR, large maximal tumor diameter, solitary kidney, long clamp time, open approach, and cold ischemia were associated with postoperative AKI in the univariate logistic regression analysis. These factors and mannitol were entered for multivariate logistic regression, and male gender, low baseline eGFR, large maximal tumor diameter, solitary kidney, and long clamp time remained as the independent predictors of AKI. Mannitol was not associated with AKI both in univariate (OR 1.000, 95% CI 0.531 to 1.882, p > 0.999) and multivariate (OR 1.223, 95% CI 0.529 to 2.828, p = 0.638) logistic regression analyses (Table 3).
Logistic Regression Analysis on Possible Predictors for Postoperative Acute Kidney Injury Within 48 Hours
p Values in bold indicate <0.05.
OR = odds ratio.
Male gender, low baseline eGFR, large maximal tumor diameter, solitary kidney, long clamp time, and open approach were associated with a >20% decrease from baseline eGFR at the 6-month follow-up in univariate logistic regression analysis. These factors and mannitol were entered for multivariate logistic regression, and low baseline eGFR and long clamp time remained as independent predictors. Mannitol was not associated with a >20% decrease from baseline eGFR at 6-month follow-up both in univariate (OR 1.061, 95% CI 0.541 to 2.078, p = 0.864) and multivariate (OR 1.145, 95% CI 0.546 to 2.401, p = 0.719) logistic regression analyses (Table 4).
Logistic Regression Analysis on Possible Predictors for >20% Decreased Estimated Glomerular Filtration Rate from Baseline at 6-Month Follow-Up
p Values in bold indicate <0.05.
Discussion
In the present study, neither the decreased postoperative 6-month eGFR nor the incidence of postoperative AKI was mitigated by intraoperative intravenous mannitol administration. We demonstrated that mannitol failed to create renoprotective properties during PN in CKD patients. The narrow CI suggested that any plausible effects of mannitol on early- and intermediate-term renal function would not be clinically meaningful.
Several previous studies 5,6,15,16 have investigated the renoprotective effect of mannitol in patients with normal renal function undergoing PN. A double-blinded randomized trial by Spaliviero and colleagues 5 studied the potential effects of mannitol in nephron-sparing surgery in 199 patients with a preoperative eGFR >45 mL/minute/1.73 m2 and demonstrated no significant differences in eGFR at the 6-week or 6-month follow-up or on split renal function at 6-month follow-up; long-term value on renal functional preservation was not identified at the 3-year (±6 months) follow-up. 17
A previous randomized-controlled, double-blinded trial by Choi and colleagues 6 focused on robot-assisted PN and no differences of eGFR at 24 hours, 1 week, and 30 days between individuals receiving mannitol vs controls were observed. Two retrospective studies adopting a multivariate model found that mannitol was not significantly associated with improved renal function at postoperative 6 months. 15,16 These results were consistent and provided ample evidence of discontinuing routine use of mannitol during PN in patients with normal renal function.
However, many authors 7,8 insisted on the possible renoprotective effect of mannitol on high-risk patients, namely, patients with low preoperative eGFR, large tumor diameter, or solitary kidney, who were much more likely to progress to an advanced stage of CKD. They believed that compared with patients with renal dysfunction, healthy patients were much more likely to be able to withstand physiologic perturbations intraoperatively and postoperatively. 7 Preoperative renal function was one of the most important predictors of renal function recovery after surgery. Small changes of renal function after PN in the healthy kidney may create the renoprotective effect of mannitol invisible, thus biasing the study toward null hypothesis.
However, Omae and coworkers 18 analyzed the effect of mannitol during open nephrectomy for renal cancer on postoperative renal function in a high-risk population and found that a solitary kidney showed no advantage from mannitol administration. In the present study, we determined that mannitol had no protective effect on renal function in our high-risk population (i.e., patients with preoperative eGFR <60 mL/minute/1.73 m2). In the subgroup analysis, mannitol failed to prevent eGFR decline in patients with larger tumor size (>4 cm), solitary kidney, or reduced renal function (eGFR <45 mL/minute/1.73 m2), indicating that the effect of mannitol was not modified by renal function and tumor characteristics. However, due to the limited sample size in each subgroup, the interaction results are only hypothesis-generating because confounders have not been controlled for within the subgroups.
Several studies have evaluated the renoprotective effect of mannitol in patients with CKD. In a previous randomized-controlled trial 19 that included 50 patients undergoing cardiac surgery with established renal dysfunction (serum creatinine levels between 130 and 250 μmol/L), 0.5 g/kg of mannitol failed to improve renal function in the first 3 postoperative days. Solomon and coworkers 20 assessed patients with chronic renal insufficiency who were undergoing cardiac angiography and demonstrated that 25 g of mannitol failed to show a functional benefit within 48 hours after the injection of the radiocontrast medium. Another randomized-controlled trial 21 found forced euvolemic diuresis with saline, 25 g of mannitol, and 100 mg of furosemide compared with saline hydration controls that doubled the risk of contrast-induced nephropathy within 48 hours in patients with CKD undergoing coronary angiography.
Thus, the above previous studies showed no potential benefit to postoperative early renal function of mannitol in CKD patients, which is similar to the present study results. Furthermore, intermediate term added value to renal functional preservation, not observed in our study either.
The optimal dose of mannitol for renoprotection was equivocal due to the paucity of evidence. An international survey 9 investigated 47 high-volume tertiary centers and the dose utilized during PN was highly variable. Mannitol has been used in 37 centers (78.7%), of which 14 centers (29.8%) used 12.5 g, 23 centers (48.9%) used 25 g, and 10 centers (21.3%) used other different dosages; our regimen was consistent with most of the centers.
Several limitations should be highlighted in the present study. First, we applied PSM to minimize imbalance; however, unrecognized confounding factors might bias the conclusions. Second, even though the largest tumor diameter was matched, tumor size could not definitively reflect the volume loss of the kidney. The data of excisional volume loss were missing in the present study, and the actual loss of nephrons may not be exactly matched between the two groups. Third, the prevalence of AKI might be underestimated, due to the absence of urine output criteria in the diagnosis of AKI. Fourth, we only carried out a 6-month intermediate follow-up, the long-term effect of mannitol on renal function was not assessed. Nonetheless, a relatively large sample size for a rare population was investigated. Further studies are warranted to validate our results.
Conclusion
The results of our study provided evidence that mannitol infusion during PN failed to provide added value on renal functional preservation in CKD patients, similar to patients with normal renal function. Therefore, the present study supports discontinuing routine use of mannitol in individuals with renal insufficiency. Further randomized-controlled trials are required for the critical evaluation of mannitol as a renal protective agent.
Footnotes
Authors’ Contributions
H.K.: designed the study, analyzed the data, and drafted and revised the article. Y.-X.Z. and P.-C.Y.: designed the study, collected and analyzed the data, and drafted the article. J. Guan and J. Gao: helped collect and analyzed the data. J.-H.M.: helped with statistical analysis. All authors read the article and approved the final version.
Acknowledgments
The authors gratefully acknowledge Dr. Zhong-Yuan Zhang, MD (Department of Urology, Peking University First Hospital, Beijing, China), for his help in study design and Ms. Xue-Ying Li (Department of Biostatistics, Peking University First Hospital, Beijing, China) for her help in statistical analysis.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.