
Abstract
Introduction:
We present our initial experience using the Moses 2.0 system for flexible-ureteroscopy (f-URS) high-frequency renal stone dusting, including a step-by-step video guide of our clinical principles for dusting technique.
Materials and Methods:
Twelve consecutive patients undergoing f-URS with Moses 2.0 (Lumenis) for a single renal stone by a single surgeon at an ambulatory center were reviewed. Stone-free rates (SFRs) and Clavien grade complications were assessed. Operative steps with illustrative examples are provided in an accompanying video.
Results:
Mean (range) stone size and lithotripsy time were 10.4 (5.3–17.2) mm and 15.0 (5–26) minutes, respectively. Complete SFR and <2 mm residual fragments were 82% and 18%, respectively. One patient had a Clavien Grade 1 complication. Operative steps reviewed include instrumentation, stone control, laser settings, and stent omission criteria. The preferred laser settings for renal stone dusting were 0.2–0.3 J and 100–120 Hz. Limitation of this early experience study is the small sample size. Larger studies are needed to confirm our initial findings.
Conclusions:
Early experience of Moses 2.0 for f-URS renal stone dusting demonstrated effective and efficient laser lithotripsy in patients with renal stones <2 cm.
Introduction
The ability of the holmium: yttrium-aluminum-garnet (Ho:YAG) laser to treat stones of all compositions in all locations of the urinary tract safely via ureteroscopy (URS) positioned it to become the standard for laser lithotripsy. 1,2 However, initial Ho:YAG lasers were low-power systems (≤20 W) that had a limited range of pulse energy (0.6–1.4 J) and frequency (4–15 Hz) settings. 3 This made it well suited for the technique of stone fragmentation with basket retrieval. Over the last two decades, advances in laser technology and the development of high-power systems have resulted in holmium lasers that provide low pulse energies and higher frequencies. This has increased the adoption of a “dusting” technique, through which the stone is disintegrated into very small fragments for spontaneous passage by the patient. 4,5
The foundation of low pulse energy and high frequency for a URS dusting technique is built upon evidence from the laboratory. In vitro studies have demonstrated that low pulse energy settings result in the smallest fragment sizes. 2,6 –8 Similarly, studies have shown that higher pulse frequencies increase fragmentation. 9,10 Recently, a new advance for laser lithotripsy has been pulse modulation with Moses technology (Lumenis), through which a multipulse is delivered compared with the traditional short or long pulse. 11 In this mode, the first pulse serves to form a vapor channel for a second pulse to travel through. Benefits are enhanced energy transfer to the stone with reduced retropulsion and improved fragmentation. 11 –13 An important feature is the ability to work at a distance from the stone, with significantly increased fragmentation at 1–2 mm distance compared with nonmodulated single short pulse. 12,13 A recent study using light reflectance demonstrated that during the dusting technique with long pulse mode, 48% of pulses are delivered with the fiber >1 mm away from the stone, while 23% are delivered <0.5 mm from the stone. 14 Since the technique for renal stones consist of chipping, dancing, and painting movements, 15 the constant laser fiber movement occurring during URS makes pulse modulation well-suited for dusting.
In 2020, Lumenis released the Moses 2.0 system with an optimized Moses pulse for frequencies >80–120 Hz. Considering these advances, we present our early experience with Moses 2.0 for treating renal stones with flexible URS (f-URS) using a high-frequency dusting technique. The technology and its application are explained, including our clinical principles for performing f-URS dusting. An accompanying video highlights the operative steps with illustrative examples.
Discussion of Technology
Pulse modulation with Moses technology provides a split-pulse mechanism for optical energy delivery. For frequencies 5–80 Hz, there are two modes the user can select: Moses contact (MC) and Moses distance (MD). The major difference between MC and MD is in their unique split-pulse dynamics. When the optical pulse profiles were assessed at 1 J, MC mode delivered 25% of the total optical energy in the initial pulse, and 75% in the second pulse. In contrast, MD mode divided the total optical energy evenly with ∼50% delivered for each pulse. 13 These differences are appreciated in the size of the initial and secondary vapor bubbles (Fig. 1).
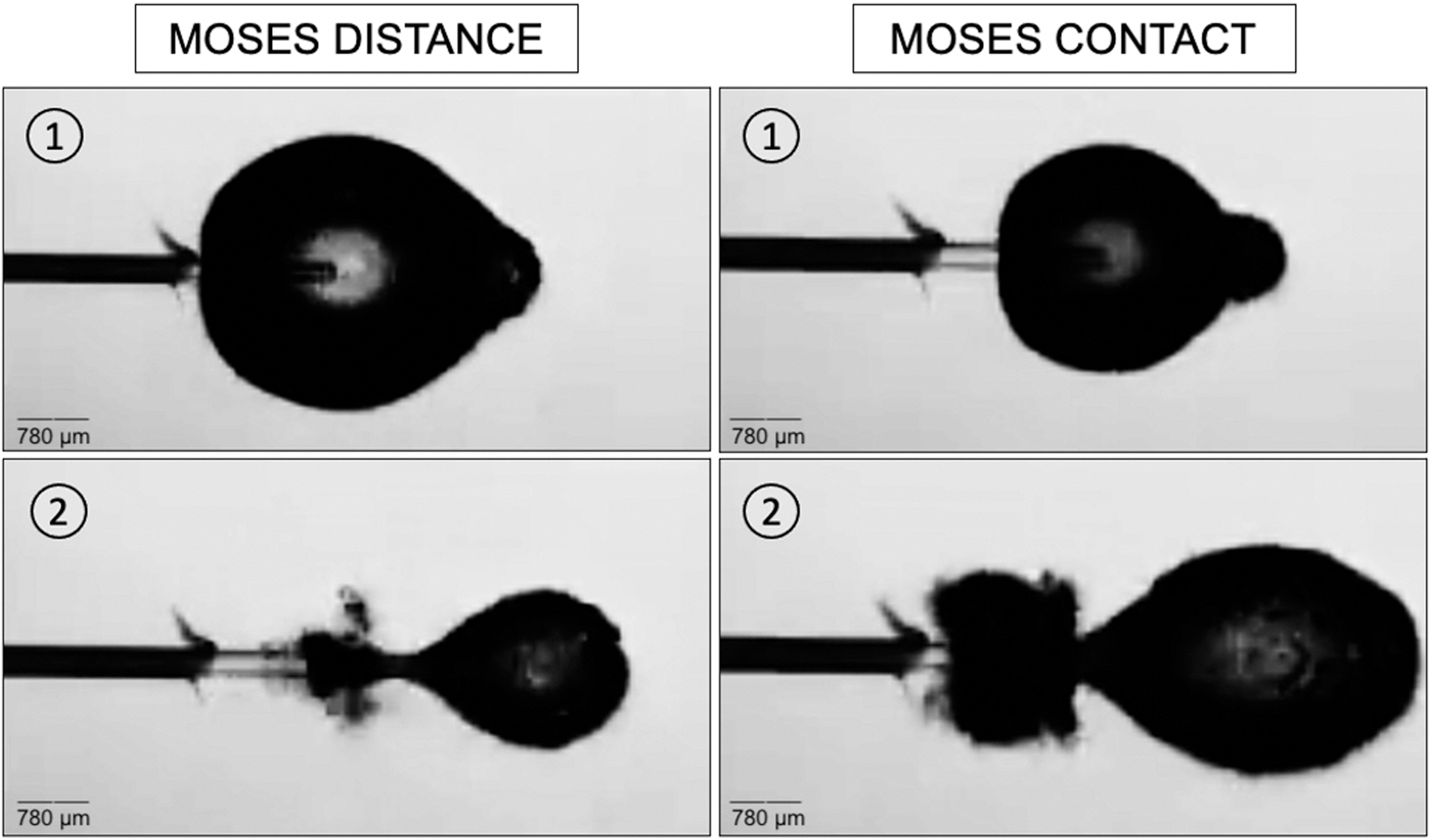
Still images of 1 J pulse energy of the MC and MD mode initial (1) and secondary (2) vapor bubbles at maximum expansion. MC = Moses contact; MD = Moses distance.
Moses 2.0 is the first Ho:YAG laser that provides pulse frequencies >100 Hz (Fig. 2). Table 1 provides the maximum frequency, pulse modulation mode, and power achievable for pulse energies between 0.2 and 1.0 J. The system has a dual pedal footswitch for the surgeon to alternate between two preset laser settings without needing to place the laser on standby. Surgeons can save individual preset settings to maximize operative room (OR) efficiency. If utilizing >80 Hz, the option to select MD or MC modes is replaced with a system-provided optimized Moses mode, using rapid pulse sequence. This mechanism of energy delivery, paired with the Moses 200 D/F/L ball-tip laser fiber, allows efficient energy delivery through a small core that is easily passed through a deflected ureteroscope.

System touch screen for Moses 2.0 demonstrating pulse frequencies of 90–120 Hz with pulse energies of 0.3–0.4 J.
Maximum Pulse Frequency (Hz), Pulse Modulation Mode, and Total Power (W) Available for Pulse Energies 0.2–1.0 (J) on the Moses 2.0 System
MC = Moses contact; MD = Moses distance; Optimized = optimized Moses mode for pulse frequencies >80 Hz.
Initial Case Series
We reviewed all consecutive cases of a unilateral single renal stone treated with f-URS and the Moses 2.0 in a single stage by one surgeon (K.R.G.) at Brighton Center for Specialty Care, Michigan Medicine, from July 2020 to March 2021. All cases were retrospectively reviewed (IRB approval) and assessed for multiple parameters, including stone size (largest maximum dimension in single plane), renal location, stone density (HU) in patients with preoperative CT, use of ureteral access sheath (UAS), and postoperative stenting. f-URS was performed using an Olympus URF-P6 ureteroscope, an Olympus V3 digital ureteroscope, or a LithoVue (Boston Scientific) single-use ureteroscope. A 230-μm ball-tip fiber (Moses 200 D/F/L) was used for all cases. All patients had documented urine cultures before surgery. Patients with urine infection were treated with culture-directed antibiotics with documented negative culture before surgery, and all patients received perioperative intravenous prophylaxis. Laser settings and outputs were recorded within the system and collated for this evaluation. Lithotripsy time was defined as the time from first laser activation to the end of last laser activation, including pedal on and off times. Lasing time was the summative time of when the pedal is depressed with laser activity. All patients were prescribed alpha-adrenergic blocker and nonsteroidal anti-inflammatory drugs for pain relief. Stented patients were prescribed anticholinergic medication. Stone clearance was determined on postoperative imaging with either radiography (kidney, ureter, and bladder radiograph [KUB]) or CT. Complications were classified using the Clavien–Dindo grade. Postoperative encounters were assessed, including ambulatory health care utilization, emergency department (ED) visits, or hospitalization.
Step-by-Step Technique
An accompanying video (Supplementary Video S1) highlights the operative steps summarized below:
1. Overall strategy: Communicating the surgical plan and equipment needs with the OR team before the patient arriving in the room helps improve surgical efficiency.
2. Anesthesia: For renal stones, endotracheal intubation is requested so that ventilation parameters such as respiratory rate and tidal volume can be controlled to mitigate excessive renal movement that can hinder accurate laser lithotripsy. Occasionally apnea may be needed to improve stone targeting and prevent bleeding, which is important if the goal is to provide stentless URS.
3. Guidewires: Placement of a safety guidewire during URS is recommended unless the wire cannot pass a ureteral stone or stricture, or if using a UAS where it can act as a safety wire.
16
If the plan is to place a ureteral stent, a safety wire maintains access to the collecting system and facilitates rapid stent placement. For select cases, an experienced urologist might choose to save a step and time, by doing the procedure wireless as long as they are experienced enough to regain access should it be lost. Wireless technique should only be performed by surgeons with experience to reduce the risk of complications, especially if using larger caliber ureteroscopes. In our schema, we use a wireless technique if the patient is prestented because the ureter is dilated in this scenario. Typically, a hybrid wire is used as a working wire for f-URS access into the kidney.
4. Ureteral access sheath: Indications for using a UAS for renal stone dusting are as follows: large stones (>1 cm), hard stones, history of infection, or if the kidney is hydronephrotic. In general, we use a 10F/12F or 11F/13F, and reserve larger sheaths for prestented patients. In cases where we do not use a UAS, a 12F bladder catheter is placed to promote lower urinary tract pressure.
5. Ureteroscope selection: If a stentless technique is the goal, a small-caliber fiberoptic scope (e.g., Olympus P6 or P7) is preferred. If using a UAS, or in those who are prestented, a larger caliber reusable digital ureteroscope can be considered. For patients with challenging lower pole stones, a single-use ureteroscope is preferred. For a difficult lower pole stone in the left kidney, a LithoVue may be preferred as the working channel is at 3 o'clock camera position. The laser fiber may therefore be better aligned to target the stone and not mucosa. For right-sided lower pole stone, the Olympus ureteroscope can be considered as the working channel is at the 9 o'clock camera position. Such differences can make laser-to-stone targeting easier.
17
Laser fiber selection: 200–230 μm core fibers provide smaller stone “chips,” which is advantageous for a dusting technique. The Moses system has fibers with a ball-tip that can be inserted through a deflected scope, which is helpful for lower pole lithotripsy.
7. Irrigation: Gravity-based irrigation is used during URS without laser lithotripsy. Pressurized irrigation with higher flow rates is used when dusting laser lithotripsy is performed to permit a clear visual field. Evacuation of fragments by injection of a bolus of saline with a syringe can be performed at the end of the procedure.
8. Patient and stone positioning: The patient is placed in the Trendelenburg position at the beginning of the case to prevent fragment migration into the lower pole. For stones in the renal pelvis, the ureteroscope is used to nudge the stone to an upper or interpolar location for subsequent noncontact laser lithotripsy or “pop-dusting.”
9. Laser settings: With Moses 2.0, contact laser lithotripsy is begun utilizing settings of 0.2–0.3 J and 100–120 Hz, depending on the hardness of the stone. The goal is to shave and debulk the stone systematically without fracturing it. Once the stone crumbles into midsized fragments, higher power settings for a pop-dusting technique are used with intraoperative adjustments to 0.5 J and 80 Hz using the MD mode. It is also feasible to use 0.3 J and 120 Hz throughout the entirety of the case. The goal is to get fragments <0.5–1 mm for optimal spontaneous passage. If larger fragments persist after pop-dusting, they can be extracted with a basket (hybrid technique).
10. Stents and exit strategy: All patients are placed on alpha-adrenergic blockers 7 days before URS to facilitate ureteral dilation. If a UAS is not used and the stone is <1 cm, a stent can be avoided if there has been no ureteral trauma, excessive bleeding, and the ureter is not tight or been dilated. Prestented patients, who have a UAS placed, are also eligible for stent omission. Figure 3 provides a schematic of our step-by-step technique.
Results
Over a 9-month period, f-URS with Moses 2.0 was performed on 12 patients with a solitary renal stone treated in a single procedure. One patient had a large lower pole stone treated with a staged procedure and excluded from this series. Table 2 provides patient characteristics, including stone size, density (HU), and outcomes. Mean stone size was 10.4 mm. Mean OR, lithotripsy, and lasing times were 36, 15, and 6.9 minutes, respectively. Mean energy used was 11985.8 J. Baskets were used to extract fragments for stone composition in six patients (50%). Postoperative stenting was performed in 2 (18%) patients. One patient failed to have follow-up imaging. Stone clearance in the remaining patients was determined using CT or KUB in 3/11 (27%), and 8/11 (73%), respectively. The complete stone-free rate (SFR) was 82%. One patient had a Clavien Grade 1 complication; the patient called the clinic for stent-related pain and was recommended increased analgesia and supportive therapy. No patients had an ED visit, hospitalization, or required an unplanned surgical intervention.
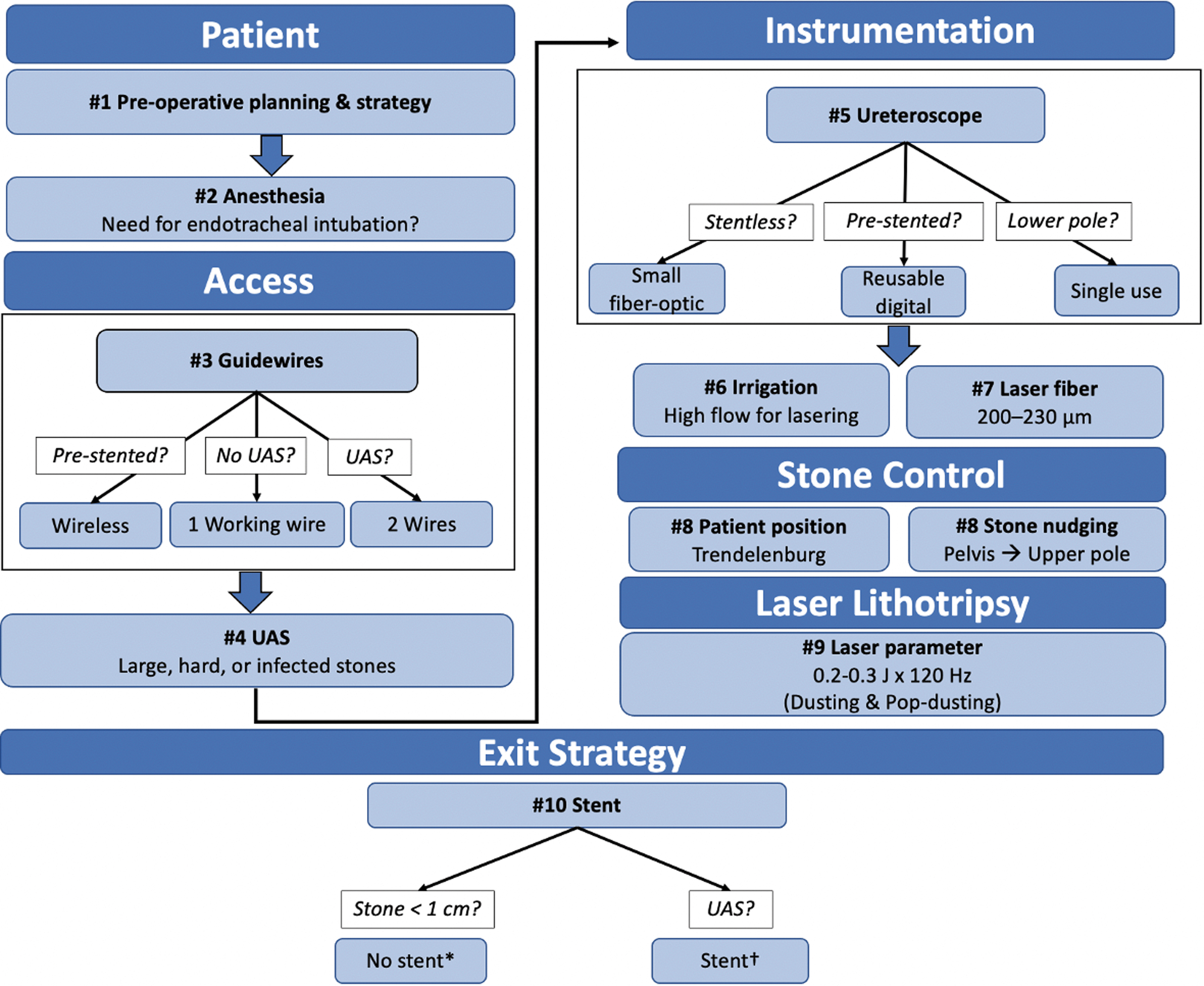
Step-by-step schematic of the operative steps for high-frequency f-URS dusting technique with Moses 2.0. A stent can be avoided if there has been no ureteral trauma, excessive bleeding, or ureteral dilation. Prestented patients who receive UAS may be eligible for stent omission. f-URS = flexible ureteroscopy; UAS = ureteral access sheath.
Patient Characteristics and Outcomes for 12 Patients Undergoing Flexible-Ureteroscopy High-Frequency Dusting Technique for Solitary Renal Stones with Moses 2.0
BMI = body mass index; COD = calcium oxalate dihydrate; COM = calcium oxalate monohydrate; CP = calcium phosphate; OR = operative room; SD = standard deviation; UA = uric acid.
Discussion
We present our early experience of using Moses 2.0 for high-frequency URS renal stone dusting. Our preferred setting for dusting renal stones was 0.2–0.3 J and 100–120 Hz. Review of operative data and outcomes on patients undergoing URS for solitary renal stones of <2 cm demonstrated that short lithotripsy times and excellent SFRs are achievable with minimal complications. Postoperative stenting was avoided in most patients. In the accompanying video, we illustrated our principles for f-URS with a step-by-step technique.
Pulse modulation with Moses technology can improve fragmentation. When stimulating “painting” motions with the laser fiber tip in contact with a flat BegoStone, use of MD mode resulted in 28% and 39% greater ablation compared with all pulse modes at 0 and 1 mm distance from the stone, respectively. 13 Laser fiber-to-stone distance is a critical factor for fragmentation efficacy. Regardless of pulse mode, contact laser lithotripsy achieves the greatest efficiency of fragmentation. However, the dusting technique utilizes constant fiber movement during URS, which can result in fragmentation at a distance from the stone during parts of the lithotripsy. Since Moses technology demonstrated superior fragmentation at a distance compared with traditional pulse modes, this mode is helpful for the dusting technique. 14 Furthermore, use of Moses mode has been shown to reduce stone retropulsion compared with the short pulse mode in an in vitro study. 11 A randomized-controlled trial comparing short pulse to Moses mode in patients undergoing URS and laser lithotripsy demonstrated 20% lower procedural times. 18
Studies of high-frequency URS dusting have reported complete SFRs of 62%–93%. 19 –22 Tracey and colleagues described 71 patients undergoing high-frequency (80 Hz) dusting of both renal and ureteral stones (mean size 12.5 mm), and demonstrated a complete SFR of 62%, while the ≤2 mm residual fragment (RF) rate was 74%. 19 Postoperative outcomes were comparable with other techniques described in the literature. 23,24 Pietropaolo and colleagues investigated dusting and pop-dusting in 50 patients using laser settings of 0.3–0.6 J and 20–50Hz with a 100 W system, on large renal stones (≥15 mm), and reported an SFR of 93% after a single procedure. 21 Mekayten et al. found a 50% faster lasing time with high-power (120 W) lasers compared with low-power (20 W) lasers when treating renal and ureteral stones with URS. However, there was no significant difference in the SFRs or postoperative complications. 20 We report on a small sample of patients, and while the data are not exhaustive, an early report of the efficacy of this new laser demonstrates acceptable SFRs and OR times with minimal complications.
Our study has a number of limitations. We report on a small sample of patients, and so, the data are not exhaustive, but an early report of the efficacy of this new laser. We did not compare this to the Moses 1.0 system, and a larger study to assess this would be beneficial. The patient populations are only those with single renal stones <2 cm, which are considered less complex. Surgeries were in patients with low comorbidity who are eligible to be operated at a free-standing ambulatory center. Furthermore, we report on only a single surgeon's experience. However, the homogeneity of a single surgeon allowed for analysis of Moses 2.0 without surgeon technique as a confounding variable. Also, variable imaging modalities were used and the SFR may differ if all patients received CT. However, our imaging is pragmatic clinical practice where the motivation is to use CT judiciously in patients at risk of a lifetime of radiation. A total of 11/12 of our patients presented for imaging, which is high in comparison with the average in the United States, where ∼50% of patients receive postoperative imaging after URS. 25 Furthermore, we recognize that high-power laser settings in conjunction with low irrigation rates may lead to thermal injury. 26 It is important to note that we used high flow irrigation for laser lithotripsy. We do not recommend renal stone dusting settings in the ureter, where we advocate low-power (<10 W) settings for lithotripsy.
Studies detailing techniques or outcomes of high-frequency URS dusting technique are limited. Our study serves to provide early experience on Moses 2.0 for renal stone dusting. Our work has helped to develop a video technique teaching guide. We found that postoperative stents can be avoided in select patients with stones <1 cm because of the improved dusting capabilities. However, larger studies are needed to validate these findings. Similarly, laboratory studies to understand the optical pulse profile and ablative effects of the optimized Moses pulse for >80–120 Hz are needed. This is the focus of our future efforts in the laboratory.
Conclusions
Early experience of Moses 2.0 for f-URS renal stone dusting demonstrated effective and efficient laser lithotripsy in patients with renal stones <2 cm. The limited number of patients in this series prevents comparison of Moses 2.0 with Moses 1.0, or with other nonpulse-modulated holmium systems, and larger studies are needed to assess this rigorously.
Footnotes
Authors' Contributions
N.R.K., S.E.M., and K.R.G. collected and analyzed the data. N.R.K. and K.R.G. wrote the article. S.E.M. provided critical revisions. K.R.G. conceived and managed the study. All authors reviewed the final article.
Author Disclosure Statement
N.R.K. and S.E.M. have no disclosures. K.R.G. has consulting relationships with Boston Scientific, Lumenis, Olympus, Coloplast, and Karl Storz.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Video S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.