
Abstract
Purpose:
To establish the first comprehensive nomogram for prediction of infection stones before treatment for better perioperative treatment and postoperative prevention of infection stones.
Methods:
A total number of 461 patients with kidney stones who underwent mini-percutaneous nephrolithotomy and flexible ureteroscopy between January 2019 and March 2021 were retrospectively analyzed. Univariable analysis and multivariable logistic regression analysis were conducted to identify the predictors for infection stones. Furthermore, the nomogram was established as a predicted model for infection stones.
Results:
Among 461 patients with infrared spectroscopy stone analysis, 100 (21.70%) had infection stones and 361 (78.31%) had noninfection stones. Multivariate logistic regression analysis indicated that female (odds ratio [OR] 2.816, 95% confidence interval [CI] 1.148–6.909, p = 0.024), recurrent kidney stones (OR 8.263, 95% CI 2.295–29.745, p = 0.001), stone burden (OR 6.872, 95% CI 2.973–15.885, p < 0.001), HU (OR 15.208, 95% CI 6.635–34.860, p < 0.001), positive preoperative bladder urine culture (PBUC; OR 4.899, 95% CI 1.911–12.560, p = 0.001), positive urine leukocyte esterase (ULE; OR 3.144, 95% CI 1.114–8.870, p = 0.030), urine pH (OR 2.692, 95% CI 1.573–4.608, p < 0.001), and positive urine turbidity (OR 3.295, 95% CI 1.207–8.998, p = 0.020) were predictors for infection stone.
Conclusions:
For patients with kidney stones, female, recurrent kidney stones, stone burden (>601 mm2), HU (750–1000), positive PBUC, positive ULE, urine pH, and positive urine turbidity were predictors for infection stone. We established the first comprehensive model for identifying infection stones in vivo, which is extremely useful for the management of infection stones.
Introduction
Infection stones are a particular type of urinary stones with mineral composition of struvite stones (magnesium ammonium phosphate) and/or carbonate apatite. They are associated with urinary tract infections (UTI) caused by urease-producing organisms such as Proteus, Pseudomonas Klebsiella, and Staphylococcus. 1,2
Infection stones are one of the most intractable diseases for urologists owing to the complexity of the stone and the high risk of regrowth. 1 Infection stones can grow rapidly into large staghorn stones in 4 to 6 weeks and even fill the whole intrarenal collecting system. If left untreated, they may lead to life-threatening complications such as kidney failure, kidney loss, and even death. 3,4 Gao et al. reported that struvite patients were associated with a significantly high rate of calculi recurrence and urosepsis after surgery. 5 Effective treatment of infection stones should involve the use of antibiotics, stone removal as completely as possible and followed by medical therapy to prevent stone recurrence. 6
The management of infection stones should start with an early and correct identification. However, accurate detection of stone composition can now only be performed in vitro. The aim of the clinical study was to establish the first comprehensive nomogram for prediction of infection stones before treatment for better perioperative treatment and postoperative prevention of infection stones.
Materials and Methods
Patients
The study was approved by the Ethics Committee of XiangYa Hospital and the number is 202108163, Central South University, Hunan province, China. We retrospectively reviewed 461 consecutive patients with renal stones who underwent mini-percutaneous nephrolithotomy (mPCNL) or flexible ureteroscopy (FURS) between January 2019 and March 2021. Patients with ureteral stone and those without infrared spectroscopy stone analysis were excluded.
All patients preoperatively underwent a urinary noncontrast CT and plain film radiography of kidney, ureter, and bladder (KUB). Bladder urine culture, blood and urine routine tests, and laboratory examination of kidney and liver function were performed preoperatively. Midstream urine specimens from the patients' bladders were collected for the preoperative bladder urine culture (PBUC) and urine routine tests after perineal cleaning within 1 week before surgery. The isolated bacteria or fungi with a count ≥105 cfu/mL was regarded as positive PBUC. Urine pH referred to the first value of admission to our department.
Patients with recurrent kidney stones were those who were found to have ipsilateral kidney stones more than two times. For patients undergoing mPCNL the stone was broken by laser lithotripsy under nephroscope vision, and the fragments were flushed out with saline perfusion, whereas for FURS the stones were broken into smaller pieces and the larger portions were removed with a disposable nitinol stone basket. We routinely collected all stone fragments after the operation and selected randomly different size, shape, and color stones for infrared spectroscopy stone analysis.
Data collection and outcome assessment
Demographic and perioperative data were recorded from the institution's electronic medical record management system. According to the results of stone composition analysis, infection stones were classified into two main categories according to their composition: (1) pure infection stones, consisting entirely of magnesium ammonium phosphate and/or carbonate apatite; (2) predominantly infection stones, where magnesium ammonium phosphate and/or carbonate apatite was identified by infrared spectroscopy as the major component (>50%) of the stones.
Stone burden was routinely estimated by two specialized surgeons independently according to the formula: Σ(0.785 × Widthmax × Lengthmax). 7 The cutoff value of stone burden was obtained by receiver operating characteristic (ROC) curve. HU value of renal stone was repeatedly measured three times and took the average, and for complex stones, whose different positions were repeatedly measured to get the average value. Renal stones filling the renal pelvis and at least two calices were considered as partial staghorn, and stones occupying the entire collecting system (>80%) was defined as complete staghorn stones. 8
Statistical analysis
The analysis of all data was performed using the Statistical Package for the Social Sciences (SPSS) version 22.0.0.0 for Windows (Chicago, IL). The continuous variables were described as the mean ± standard deviations and analyzed using Student's t-test for normal distribution or Mann–Whitney U test for non-normal distribution. The categorical variables were described as the percentages (%) and analyzed using chi-squared (χ 2 ) test or Fisher's exact probability test. Multivariate stepwise logistic regression analysis was used to identify the independent risk factors for infection stones. Two-tailed p-values <0.05 was regarded as statistically significant difference. The parameters with statistically significant differences in multivariate logistic regression analysis could be incorporated in the nomogram predicting infection stones. The nomogram was established using R software version 4.0 for Windows.
Results
Stone composition
We included 461 patients with infrared spectroscopy stone analysis after mPCNL or FURS in this study, including 100 (21.70%) infection stones and 361 (78.31%) noninfection stones. Calcium oxalate were the predominant type of kidney stones, which accounted for 63.56%, followed by carbapatite (13.88%) and uric acid (13.45%). The main stone composition confirmed was struvite in 36 (7.81%) cases and carbapatite in 64 (17.73%) cases among the infection stones. Detailed data of stone composition distribution are shown in Table 1. The cutoff value of stone burden was 601 mm2 that is calculated by ROC curve.
Composition Distribution of Kidney Stones
Univariate analysis
Demographic and clinical data of included population are presented as two groups in Table 2. The univariate analysis revealed that people with infection stones was associated with several parameters, such as female gender (p < 0.001), hypertension (p = 0.009), recurrent kidney stones (p < 0.001), stone burden (p < 0.001), HU (p < 0.001), staghorn stones (p < 0.001), history of mPCNL (p < 0.001), open surgery (p = 0.002), positive PBUC (p < 0.001), urine white blood cells (WBC; p < 0.001), urine bacteria (p = 0.016), positive urine protein (p < 0.001), positive urine nitrite (p < 0.001), positive urine leukocyte esterase (ULE; p < 0.001), urine pH (p < 0.001), positive urine turbidity (p < 0.001), urine specific gravity (p < 0.001), serum uric acid (p = 0.024), serum phosphorus (p = 0.019), and serum magnesium (p = 0.008).
Demographic and Clinical Data of Included Population
The bold numbers are less than 0.05, meaning statistical difference.
BMI = body mass index; BUN = blood urea nitrogen; mPCNL = mini-percutaneous nephrolithotomy; PBUC = preoperative bladder urine culture; PTH = parathyroid hormone; RBC = red blood cells; RIRS = retrograde intrarenal surgery; Scr = serum creatinine; SD = standard deviation; SWL = extracorporeal shockwave lithotripsy; ULE = urine leukocyte esterase; WBC = white blood cells.
However, there were no significant statistical differences in some previously reported factors, such as age, body mass index, diabetes mellitus, and serum creatinine (Scr; all p-values >0.05). 9 As shown in Table 3, for patients with infection stones, 65% presented with flank or abdominal pain, 14% present with fever, 9% with gross hematuria, and 2% can present with urosepsis, all of which were higher than those with noninfection stones.
Details of Preoperative Clinical Symptoms
Bacteria spectrum
Positive PBUC was present in 56 (56.0%) cases with infection stones and 59 (16.3%) patients with noninfection stones. preoperatively, including 18 (16.3%) cases. As shown in Figure 1, Escherichia coli were the predominant bacteria in both infection-stone group and noninfection-stone group, with 24 and 33 cases, respectively. However, the proportion of urease-producing bacteria in patients with infection stones was higher, such as Proteus (10 vs 2), Klebsiella (9 vs 6), Staphylococcus (4 vs 2), and Pseudomonas (1 vs 1).

Analysis of bacterial spectra of urine cultures in infection-stone group and noninfection-stone group. Color images are available online.
Multivariate analysis
Multivariate binary logistic regression analysis indicated that female (odds ratio [OR] 2.816, 95% confidence interval [CI] 1.148–6.909, p = 0.024), recurrent kidney stones (OR 8.263, 95% CI 2.295–29.745, p = 0.001), stone burden >601 mm2 (OR 6.872, 95% CI 2.973–15.885, p < 0.001), HU (OR 15.208, 95% CI 6.635–34.860, p < 0.001), positive PBUC (OR 4.899, 95% CI 1.911–12.560, p = 0.001), positive ULE (OR 3.144, 95% CI 1.114–8.870, p = 0.030), urine pH (OR 2.692, 95% CI 1.573–4.608, p < 0.001), and positive urine turbidity (OR 3.295, 95% CI 1.207–8.998, p = 0.020) were predictors for infection stone (Table 4). There were no significant statistical differences with regard to the remaining factors.
Multivariate Logistic Regression Analysis for Predictors of Infection Stones
The bold numbers are less than 0.05, meaning statistical difference.
CI = confidence interval; OR = odds ratio.
Nomogram
The nomogram was established by eight predictors described in multivariate logistic analysis to calculate the probability of infection stones (Fig. 2). Each horizontal line was assigned a numerical score by drawing a vertical line from it to the point scale. The sum of the eight factors constitutes the total scores, which indicated the final probability of an infection stone for a given patient. It should be noted that the c-index was 0.903, indicating a high discriminative ability of the nomogram.
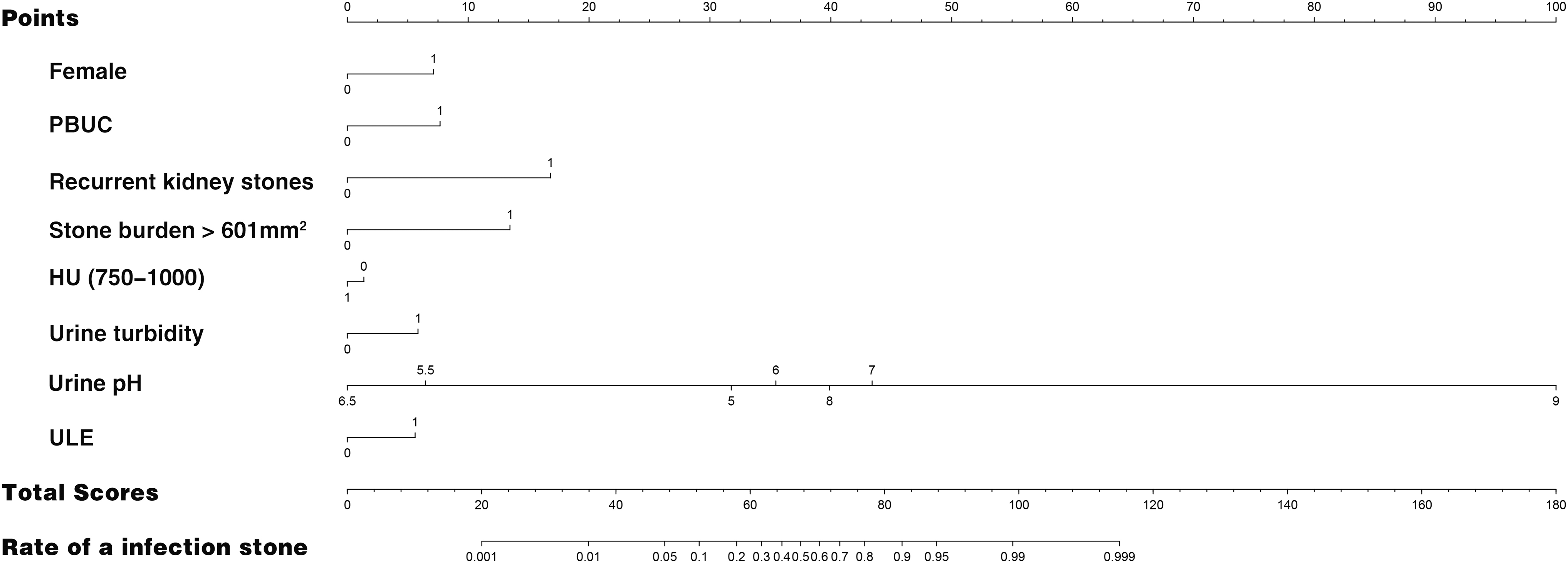
Nomogram to predict infection stones.
Discussion
Patients with infection stones, with or without treatments, are more likely to have higher rates of infectious complications and mortality. 10,11 The mean serum endotoxin concentration in patients with infection stones was 35 times higher than those with noninfection stones. 12 Some studies have not only demonstrated that positive preoperative PBUC was an independent risk predictor of postoperative infectious complications, 13 but also that positive rate of PBUC in patients with infection stones was much higher than that in patients with noninfectious stones. 5 Infection stone accounts for nearly a quarter of staghorn stones, 14 which are at risk of developing obstructive symptoms that can lead to renal failure, urosepsis, and even death. 15
The management of infection stones can be determined by their size, location, and stage of development, and generally involves surgical and pharmacologic treatment. Surgery is currently the first-line treatment for infection stones. Percutaneous nephrolithotomy is the gold-standard approach of larger infection stone (>2 cm). Ureteroscopy and extracorporeal shockwave lithotripsy (SWL) can be considered for patients with infection stones <2 cm. For those patients who cannot tolerate surgical stone removal or who have not been cured by surgical therapy, dissolution therapy can be considered as a second-line treatment and is currently approved by U.S. Food and Drug Administration (FDA). 9,15
And chemolysis for infection stones through ureteral stents, percutaneous nephrostomy tube, and access sheaths is considered safe and effective. 16 The use of antibiotics before and after surgery is clearly essential for the adjunctive treatment of infectious stones, but the duration and administration mode of antibiotic therapy are not mentioned in the available clinical guidelines. 17 Urease inhibitors, which directly interfere with growth processes of infection stones precursors, are recommended to those patients with surgical contraindications or recurrent infections even after infection stones removal. 17,18 Urine acidification, complementary to antibiotic treatment and urease inhibitors, is used to alter urine pH to avoid infection stones precipitation. 19
However, early and correct detection of infection stone is crucial regardless of the earlier methods. At present, accurate identification of stone composition can only be carried out in vitro, such as the common use—infrared spectroscopy stone analysis. Marchini et al. reported that HU on CT alone cannot accurately predict the struvite stone composition. 20 Therefore, we established the first comprehensive model for identifying infection stones in vivo before treatment, which is extremely useful for the management of infection stones.
The formation of infection stones is always associated with urease-producing bacterial pathogens, such as Proteus, P. Klebsiella, and Staphylococcus, 1 which accounted for 42.9% (24/56) and 18.6% (11/59) in infection-stone group and noninfection-stone group in our study, respectively. In this study, positive preoperative PBUC was a predictor of infection stones even though E. coli was still the common bacteria. This may be explained by the presence of unsuccessfully cultured urease-producing bacteria during the crystallization of stones. 9
In addition, the urine tests with higher pH, positive ULE (++ and +++), or positive urine turbidity were confirmed as predictors in our study. When these urease-producing organisms infect the urinary tract, urea is hydrolyzed by ammonia and carbon dioxide in the presence of urease, which elevates urine pH and increases the concentration of NH4 +, CO3 2−, and PO4 3−. These ions combine with Mg2+ and Ca2+ present in urine to form magnesium ammonium phosphate and carbonate apatite. 21,22 Most importantly, crystallization of carbonate apatite starts at a pH >6.8 and that of struvite occurs at a pH >7.2, 1,23 which can be to some extent reflected in our nomogram (pH = 7 scored higher than pH = 8). Urine turbidity, which can reflect the number of WBC, proteins, crystals, and microorganisms, has been reported to be the best predictor of UTI. 24
The unique formation process of infection stones distinguishes them from other types of kidney stones in terms of density, size, shape, and recurrence rate. This study showed that recurrent kidney stones, stone burden, and HU (750–1000) were predictors for infection stones. Infection stones are characterized by the rapid growth in the body (form within 4–6 weeks), the tendency to aggregate into larger stones or staghorn stones and the high recurrence rates. Our overall HU average value was 888.7, which is consistent with previously reported data. 20,25 However, there were significant overlap between infection stones and other stone types (such as uric acid, calcium oxalate, and mixed stones), resulting in limited value of HU in predicting infection stones 20 (Fig. 2).
In addition, our results suggested that the risk of infection stone in women was ∼3 times than men, which attributes to a higher frequency of UTI in women. 26 In this study, staghorn stone was not a predictor for infection stone, possibly because staghorn stones can present as mixed stones. They may occur when calcium oxalate stones harbor urease-producing bacteria and trigger secondary struvite deposition. 27 And urine WBC also do not predict infection stones, which can be explained by the patients with complex kidney stones that our center receives from all over the country. UTI may be caused by urinary stasis secondary to obstruction by any type of stone and previous study reported the incidence rate of UTI was up to 7% to 28% during renal colic episodes. 28 And 211 (58.4%) patients with noninfection stones had flank or abdominal pain before admission.
There are some limitations in this study. First of all, it is a retrospective study in a single institution with a small sample size. In addition, we failed to perform subgroup analysis for pure infection stones and predominantly infection stones because of the limited cases. Finally, renal stones may not be obtained for analysis for some patients under FURS, leading to a higher proportion of infection stones and a higher average stone burden. Therefore, further large, prospective, and multicenter studies are needed to confirm our nomogram.
Conclusion
For patients with kidney stones, female, recurrent kidney stones, stone burden, HU (750–1000), positive PBUC, positive ULE, urine pH, and positive urine turbidity were predictors for infection stone. And we established the first comprehensive model for identifying infection stones in vivo, which is extremely useful for the management of infection stones.
Ethical Approval
All procedures performed in the study were in accordance with the ethical standards of the local research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Informed consent was obtained from all the individual participants included in the study.
Footnotes
Authors' Contributions
Project development, data analysis, and article writing by M.L. Data collection and analysis by Z.Z. and J.C. Data collection by Z.C. Article editing by F.Z. and Z.C. Project development and article editing by C.H. and H.C.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Funding was provided by the National Natural Science Foundation of China (81770705 to H.C.).