
Abstract
Objectives:
To evaluate learning curves in pediatric flexible ureteroscopy (FURS) and pediatric prone percutaneous nephrolithotomy (PCNL) by a single surgeon with experience in adult endourologic procedures.
Materials and Methods:
Children who were found to have nephrolithiasis and treated with PCNL or FURS from June 2014 to April 2019 were analyzed. Patient demographics, stone characteristics, stone-free rate (SFR), and complication rate (CR) were reported. Learning curves were generated to estimate the effect of a surgeon's experience on outcomes.
Results:
Seventy-three children underwent PCNL on 86 sides in 77 operations and 275 children underwent FURS on 320 sides in 288 operations. The SFRs were 88.1% (282/320) for FURS procedures and 89.5% (77/86) for PCNL procedures. CRs were 19.8% (57/288) and 35.1% (27/77), respectively. Learning curves showed that the SFRs of the two procedures increased with the accumulation of cases. There was an apparent improvement of SFR for PCNL procedures after ∼60 surgeries. A favorable SFR of FURS could be achieved at the start of learning. No apparently decreased CRs were observed for either PCNL or FURS.
Conclusions:
Both PCNL and FURS could achieve satisfactory SFRs and accepted CRs in pediatric stones. Increased surgical experience was associated with improved SFRs of both PCNL and FURS procedures, and the surgeon's experience of adult FURS translating to that of pediatric FURS was better than adult PCNL translating to pediatric PCNL. A surgeon needs ∼60 cases of PCNL to achieve competence. For FURS, a favorable SFR could be achieved at the start of learning.
Introduction
The incidence of pediatric urolithiasis has increased dramatically in the past few years, mainly because of a rising incidence in adolescents. 1 The endourologic managements of pediatric urolithiasis mainly include flexible ureteroscopy (FURS) and percutaneous nephrolithotomy (PCNL), which are minimally invasive. The development of endoscopic equipment and techniques has promoted the progress of endourologic procedures and has led to an improved stone-free rate (SFR) and a decreased complication rate (CR) in children. 2 However, the case volume necessary for a surgeon to become competent in performing these two procedures remains unknown.
The learning curve is a graphical presentation of the progress in learning skills and experience. Previous studies 3,4 have investigated the learning curves in the training of PCNL for adults. However, less research investigated the role of learning curves in the training of FURS or PCNL for children. In this study, we aimed to evaluate the learning curves of pediatric FURS and prone PCNL by a single surgeon with experience in adult endourologic procedures, showing how a surgeon learned to transition for treating adult stone disease to treating pediatric stone disease. We hypothesized that the outcomes of both FURS and prone PCNL for children could be improved over the accumulation of cases and that the transition effect differed between FURS and prone PCNL.
Materials and Methods
Study population and design
This study was approved by the ethics committee of our institution. All children and their parents signed the informed consent for the study. Data were collected for all children who received endourologic procedures by one surgeon (J.L.) for nephrolithiasis at our institution from June 2014 to April 2019. All data were obtained through Beijing Municipal Administration of Hospitals Clinical Medicine Development of special support project, which provided the database containing all pediatric patients with the first stone episode. Three hundred sixty-eight children <14 years old who underwent FURS or prone PCNL met the inclusion criteria.
The exclusion criteria were as follows: (1) 16 children lacking clinical data (images), (2) 2 children with hemorrhagic disease that affects the assessment of postoperative complications, and (3) 2 children with completely spontaneous passage of stones just before the surgery. Finally, a total of 348 children were included in the study cohort.
According to our study protocol, we first examined variables such as demographic characteristics, diagnostic data, and surgical information. If a child received more than one operation at our center, we analyzed the surgical information effectively. Next, we aimed to show how the surgical outcomes changed as the cases accumulated by drawing learning curves. At our institution, all the pediatric endourologic procedures were performed by the same surgeon (J.L.) who had no previous experience in pediatric FURS or PCNL. But he had experience in >500 cases of PCNL and FURS for adults.
Procedures and definitions
Flexible ureteroscopy
At our institution, all FURS procedures required preoperative stenting (4.7F/12 cm) for at least 2 weeks. In lithotomy position, the ureter stents were first removed through 8/9.8F ureteroscopes under general anesthesia. The bladder was maintained at low pressure with a 14-Gauge transurethral angiocatheter in girls; for boys, a 14-Gauge suprapubic angiocatheter was placed. The ureteral access sheaths were routinely inserted under the guidance of 0.035-inch (0.889-mm) ultrastiff guidewires except for children whose urethras were too narrow to pass through.
A flexible ureteroscope (8F/30–42 cm) combined with holmium-YAG laser (272 μm fiber) was used for lithotripsy. The laser was used with high frequency (20–30 Hz) and low energy (0.6–0.8 J), so that the stones were preferentially dusted and not fragmented. We placed postoperative ureteral stents for protection of ureters if visible mucosal trauma or edema occurred.
Percutaneous nephrolithotomy
Children first received the placement of open-ended 5F ureteral catheters in lithotomy position under general anesthesia. Saline infusion through retrograde catheterization was performed by an assistant if artificial hydronephrosis was needed. Children were then put in prone position. Microperc procedures were the prior consideration for children with low-burden stones. Renal access was performed in a single step using a 4.85F all-seeing needle in Microperc procedures; then, the inner puncture shaft was removed and a three-way connector was applied to the outer tip of the shaft, allowing the insertion of a flexible micro-optic and a laser fiber.
The irrigation fluid was injected manually with a syringe by the assistant. As for minipercutaneous nephrolithotomy (miniPCNL) procedures, we still used the all-seeing needle to puncture the target calix followed by tract dilatation up to 16F or 18F according to the stone burden and location. The irrigation fluid was pumped into the pelvis. The 272-μm holmium–YAG laser fiber was also used in PCNL procedures. The ureteral catheters were retained in both procedures for 12 or 24 hours before removal. The nephrostomy tubes were placed to reduce the bleeding in some cases after miniPCNL. The Microperc procedures were terminated without nephrostomy tubes.
Indications for FURS procedures were as follows: (1) stones <20 mm in the pelvis and upper pole/mid region calix, (2) stones <10 mm in the lower pole calix, and (3) failed treatment of stones with extracorporeal shockwave lithotripsy (SWL). Indications for PCNL procedures were as follows: (1) stones >20 mm in the pelvis and upper pole/middle region calix, (2) stones >10 mm in the lower pole calix, (3) failed treatment of stones with SWL or FURS, and (4) comorbid ureteropelvic junction obstruction or stenotic infundibulum.
Stone clearance was defined as no remaining stone fragments or stone fragments <2 mm in diameter on low-dose CT scan (slice width of 1.25 mm) at 1 month after surgery. 5 Complications were graded according to the modified Clavien–Dindo classification system. 6 In our study, we did not include urinary tract infection (UTI) in the assessment of complications, because most children had elevated urinary leukocytes because of the surgery.
Instead, we regarded the presence of postoperative fever and positive urine culture as the sign of UTI to assess the probability of infection caused by the surgery. Fever was defined as a body temperature ≥38°C. We also did not include postoperative pain in the complication analysis, because children had lower pain tolerance and thus most had symptoms. Besides, it may be helpful to differentiate pain vs stent irritation. Ureter injury was defined according to the classification of ureter wall injuries. 7 Hydronephrosis was evaluated by the Society for Fetal Urology grading system. 8 The stone burden was calculated according to the formula (stone burden = stone length × stone width × stone depth × 3.14 × 0.167). 9
Statistical analysis
A prespecified statistical analysis plan was developed at the start of the study. Baseline characteristics were shown for both categoric variables and continuous variables. Measurement data and enumeration data were analyzed using Wilcoxon rank sum tests and chi-square tests, respectively. All tests were two sided, and the significance level was set at p < 0.05.
In addition to SFR and CR, operation duration was also considered in the learning curve analysis. Surgical experience (SFR, CR, or operation duration) was entered as a continuous variable, using restricted cubic splines with knots at the tertiles to allow a nonlinear relationship between experience and the number of cases. The intersurgeon heterogeneity could be ignored because all the surgeries were performed by the same surgeon.
All statistical tests were performed by SPSS version 25.0 (IBM, Armonk, NY, USA) and the R statistics package version 3.5.1 (R Project for Statistical Computing;
Results
Baseline characteristics
Seventy-three children who underwent PCNL on 86 sides in 77 operations and 275 children who underwent FURS on 320 sides in 288 operations were enrolled in our study cohort.
The median ages of the FURS group and PCNL group were 2 years (interquartile range [IQR], 1.4–4.0) and 2 years (1.8–4.0), respectively. The median stone burdens were 0.79 cm3 (IQR 0.28–3.20) and 4.91 cm3 (IQR 1.77–11.10), respectively. The median operation durations were 35 minutes (IQR 30–40) and 45 minutes (IQR 35–60), respectively. The median intrarenal irrigations were 300 mL (IQR 200–600) and 1300 mL (IQR 250–3000), respectively. The SFR and auxiliary treatment rate were 88.1% (282/320) and 1.6% (5/320) for FURS procedures, and for PCNL procedures, the rates were 89.5% (77/86) and 0.0% (0/86).
CRs for FURS and PCNL were 19.8% (57/288) and 35.1% (27/77), respectively. Ureter injury (Clavien–Dindo grade 3) occurred in two children after FURS who recovered after Double-J stenting. No perforation occurred at our institution. Steinstrasse (Clavien–Dindo grade 3) occurred in two children that improved after the ureteroscopic treatment and Double-J stenting. Hemostatic agents were used in eight children with hematuria (Clavien–Dindo grade 2) after PCNL and none of them needed blood transfusion. Fever occurred in 40 (14.5%) and 21 (27.3%) children in the FURS group and the PCNL group, respectively. Other demographic data and stone characteristics are summarized in Table 1.
Demographic and Stone Characteristics of Pediatric Patients (N = 348)
CR = complication rate; FURS = flexible ureteroscopy; IQR = interquartile range; PCNL = percutaneous nephrolithotomy; PUC = positive urine culture; SFR = stone-free rate.
Learning curves for the FURS and PCNL procedures
Table 2 gives both the clinical outcomes and several characteristics of stones and demographics that were all stratified by surgeon experience (i.e., number of cases). To better demonstrate the changes between surgical data and surgeon experience, we divided all cases of FURS procedures into three groups of consecutive cases (1 to 106, 107 to 213, and 214 to 320). We applied the same method to divide cases of PCNL (1 to 29, 30 to 58, and 59 to 86). We could observe a decreasing tendency of intrarenal irrigation as cases accumulated in both FURS groups and PCNL groups.
Patient and Stone Characteristics As Well As Surgical Outcomes by Surgical Experience
BMI = body mass index.
Figure 1 shows surgical outcomes plotted against surgical experience and provided the learning curves. PCNL is more difficult or complex than FURS, so the SFR was lower (41.4% vs 86.8%) and the CR was higher (34.5% vs 17.9%) at the start of PCNL learning. However, the learning or transition effect (SFR) of PCNL was more obvious than that of FURS. There was an apparent improvement of SFR for PCNL procedures after ∼60 surgeries (Fig. 1A). A favorable SFR of FURS could be achieved at the start of learning and could still improve as the cases accumulated (Fig. 1B).
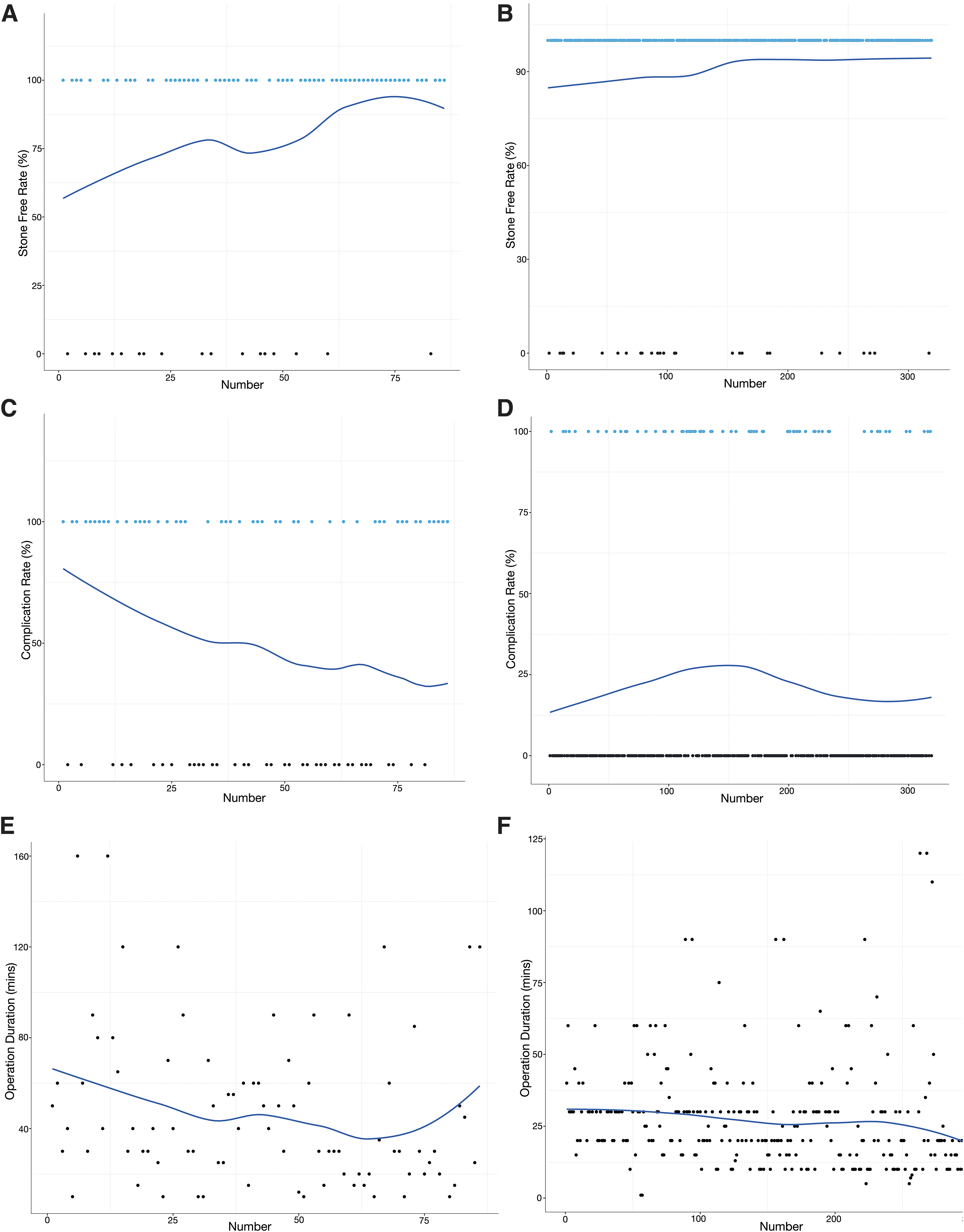
Learning curves for surgical outcomes of PCNL and FURS.
We did not observe an apparently decreased CR for either PCNL procedures or FURS procedures (Fig. 1C, D). As the cases accumulated, we shortened the operation duration for FURS procedures (Fig. 1F). However, we did not find a decreasing trend of operation duration for the PCNL procedures. We observed that the CR curve of PCNL changed with that of operation duration, whereas the CR of FURS was not related to operation duration.
Discussion
Understanding the number of procedures that a surgeon needs to gain surgical competence in treating pediatric stones and how to learn to transition from adult procedures to pediatric procedures is critically important. Our study enabled us to report the learning curves of prone PCNL as well as FURS and to estimate the association between surgeon experience and outcomes.
We found that increased surgical experience was associated with significantly improved SFR in PCNL (from ∼60% to >90%) and slightly improved SFR in FURS (from ∼88% to 92%). It seems that the surgeon's experience of adult FURS translating to that of pediatric FURS was better than adult PCNL translating to pediatric PCNL, as both SFR and CR were more favorable at the start of learning and nearly stable across all the cases in FURS.
Previous studies have shown that PCNL can be a good treatment option for nephrolithiasis in children. 10,11 Çıtamak et al. 10 reported an SFR of 84.4% and a CR of 22.6% for PCNL procedures in 294 children. Bhageria and coworkers 11 found a similar SFR of 83% and a higher CR of 32% in 95 patients with a mean age of 12 years. Our findings confirmed their conclusions in SFR. However, in our study, the CR of PCNL (35.1%, 27/77) was higher that could be attributed to the higher stone burdens. A previous study showed that surgical competence for adult PCNL could be achieved after ∼60 cases. 4 Although this number was consistent with ours, the competence was based on experience in adult procedures, which demonstrated that performing PCNL in children was a new challenge despite adult PCNL experience.
Sahan et al. 3 reported that a satisfactory SFR of supine PCNL could be reached after only 45 cases. Supine PCNL was proved to have a comparable SFR compared with prone PCNL and maintained the advantages of anesthesia. 12,13 Whether supine PCNL has a shorter learning curve than prone PCNL in children or not needs to be further explored. We could not observe an apparent decreasing trend of CR in PCNL procedures, which might be correlated with increased stone burden as case volume increased. Another possible reason was that the high CRs of PCNL were mainly caused by the invasive nature of such a procedure, which might be only diminished by reducing the caliber of the sheath and the number of tracts. 14,15
Our study demonstrated that an SFR of FURS could be achieved at the start of learning and could still improve slightly as the cases accumulated. A previous prospective investigation 16 showed that complications of ureteroscopy for adults started to decrease when case volume reached ∼200. Surgeon experience has been shown to be predictive for CRs in ureterolithotripsy. 17 However, our CR in FURS did not appear to have an association with increasing surgeon case volume. Taken together, these observations supported that the surgeon's adult FURS experience translated well to pediatric FURS. These results could help guide surgical teams to train surgeons, guide urologists to participate in the treatment of pediatric stones and guide the rational planning of costs associated with training.
We applied the operation duration as another assessment index to plot learning curves, because operation duration combined with the surgical outcomes could help better assess learning curves. 18 The reduction in the operation duration can be partially explained by the increased familiarity to the endourologic instruments and better understanding of urologic anatomy from two-dimension images. For PCNL procedures, the changing trend of CR was paralleled to that of operation duration. This could be explained by the fact that long operation duration was proven to be an independent risk factor for CR in PCNL procedures. 19
Dogan and coworkers 20 found that operation duration was an independent predictor for CR in children treated by semirigid ureteroscopy. However, the CR of FURS was not found to be associated with operation duration in our study. The discrepancy was difficult to explain and needed to be further explored.
There are several strengths of our study. First, the effects of surgeon experience on surgical outcomes in pediatric stones have not been evaluated in previous studies. To the best of our knowledge, we were the first to report the learning curves of both FURS and prone PCNL in children. Second, the study cohort was composed of pediatric patients from 27 provinces in China, which could eliminate geographical variations to some extent.
However, our study has some limitations as well. One limitation in evaluating the pediatric learning curve is that the surgeon had a degree of baseline adult surgical experience that may limit generalizability of the learning curve results to other surgeons or centers. However, with rising nephrolithiasis rates and limited pediatric treatment centers in some countries, some surgeons and centers with adult experience may likewise transition to treating pediatric stone patients. This study may provide a reference for surgeons undergoing that transition.
Further studies are necessitated to determine the learning curves of pediatric endourologic procedures by novice surgeons. Moreover, our study was limited to the retrospective nature, though the database was constructed prospectively. Last but not least, the number of children who underwent PCNL was relatively small. We might generate better learning curves of PCNL after the accumulation of adequate cases.
Conclusions
Both PCNL and FURS could achieve satisfactory SFRs and accepted CRs in pediatric stones. PCNL is more difficult or complex than FURS at first, so the SFR was lower and the CR was higher for PCNL. Increased surgical experience was associated with improved SFRs of both PCNL and FURS procedures, and the surgeon's experience of adult FURS translating to that of pediatric FURS was better than adult PCNL translating to pediatric PCNL. The learning effect of PCNL was more obvious than that of FURS. A surgeon needs ∼60 cases for PCNL procedures to achieve competence. For FURS procedures, a favorable SFR could be achieved at the start of learning.
Footnotes
Authors' Contributions
X.W. contributed to project development, data analysis, article writing, and revision; Y.Z. carried out data collection, project development, data analysis, and article revision; F.Z. was involved in project development and article revision; and J.L. and Y.T. were in charge of project development and critical revision. We confirm that the article has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed.
Acknowledgments
We thank all the staff of department of urology in the Capital Medical University affiliated Beijing Friendship Hospital.
Compliance with Ethical Standards
Ethical approval: This article does not contain any studies with human participants or animals performed by any of the authors, and it receives ethics approval from Capital Medical University affiliated Beijing Friendship Hospital Ethics Committee; all patients signed the informed consent for the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project was sponsored by Beijing Municipal Administration of Hospitals Clinical Medicine Development of special funding support (XMLX201826) and Capital Health Research and Development of special funding (2018-2-1101).