
Abstract
Background:
To develop an efficient and stable canine model of inferior vena cava (IVC) progressive obstruction at the renal hilus level.
Methods:
The model was established in two beagles by encircling an ameroid constrictor (AC) on the IVC at the renal hilus level. Abdominal wall varicosity and animal weight variations were observed weekly after operation. Ultrasound examination was performed weekly after surgery to observe the AC position, the diameter, and the velocity in the IVC. Six weeks after surgery, IVC angiography and CT scan were performed to observe the collateral circulation establishment and internal organ variation. Blood samples were taken regularly to monitor for variation in critical biochemical parameters. Renal biopsy was performed at 0, 2, 4, and 6 weeks after surgery.
Results:
Superficial varicose veins were observed on the abdominal wall at 2 weeks after surgery. Four weeks after operation, the IVC diameter increased by ∼30%, whereas the IVC velocity decreased by more than 50%. Collateral circulation was observed by IVC angiography at 6 weeks through multiple dilated veins along with neovascularization. CT scan showed congestive alteration in the kidney. The body weight, kidney, and liver function were not significantly affected. Chronic congestive renal injury was detected in the renal tubular epithelium by kidney biopsy after surgery.
Conclusions:
A canine model of IVC progressive obstruction at the renal hilus level was stably and safely established for the first time by using an AC, which may be helpful for preserving pivotal collateral circulation and nontumor-side kidney function in the IVC thrombus surgery.
Introduction
We have previously reported a series of surgical techniques and strategies in inferior vena cava (IVC) thrombus (IVCT). 1 –3 One of the most challenging problems during the surgery involves the decision of IVC thrombectomy or cavectomy, 4,5 which is strongly associated with the extensive establishment of collateral vessels. Based on our previous clinic experience, venous return was identified through various collateralization, including the caudal IVC, lumbar vein, and lumbar ascending vein to the hemiazygos and azygos vein systems. 6,7 Shirodkar and colleagues 8 believed that significant collateralization, which allowed venous drainage of the lower extremity veins and prevented lower extremity edema, was vital to the successful resection of IVC.
Gonzalez and colleagues 9 recommended to preserve the retroperitoneal, mesenteric, gonadal, and pelvic collateral vessels to the greatest extent when performing suprarenal IVC en bloc resection. However, the key events and factors in the process of collateral circulation establishment cannot be well understood. Thus, in the present study, we introduced a novel experimental canine model of IVC progressive obstruction at the renal hilus level using ameroid constrictor (AC), unveiling the hemodynamic and compensatory patterns of tumor thrombus formation, which may be helpful in designing a surgical strategy for IVCT operation.
Materials and Methods
The study was approved by the Institutional Animal Care and Use Committe of the PLA General Hospital under ethical code of 2018-D14-17.
Subjects
Two healthy adult male beagles weighing 15.1 and 14.4 kg were provided by the Chinese PLA General Hospital Experimental Animal Center. This study was approved by the Institutional Animal Care and Use Committee of the PLA General Hospital under ethical code of 2018-D14-17. The dogs were housed under standard conditions and fed a regular diet.
Permanent IVC obstruction procedures
The dogs were fixed on a board in the supine position, shaved of fur on the abdomen, and anesthetized with 3% pentobarbital sodium (30 mg/kg, intravenously). The operational region was exposed and sterilized. A 20 cm midline incision was made in the upper abdomen, followed by the mobilization and exposure of the left renal vein and IVC (Fig. 1A). An AC (Research Instruments NW, Inc.) with the inner diameter of 7.5 mm was encircled on the IVC at the level of 2 cm above the entrance of the left renal vein (Fig. 1B), downsizing the transverse area of IVC to at least 50%. 10 Internal bleeding and bowel movement were carefully examined before closing the incision. Penicillin (3.2 million U per day) was injected intramuscularly for three successive days to prevent any in vivo or incision infection.
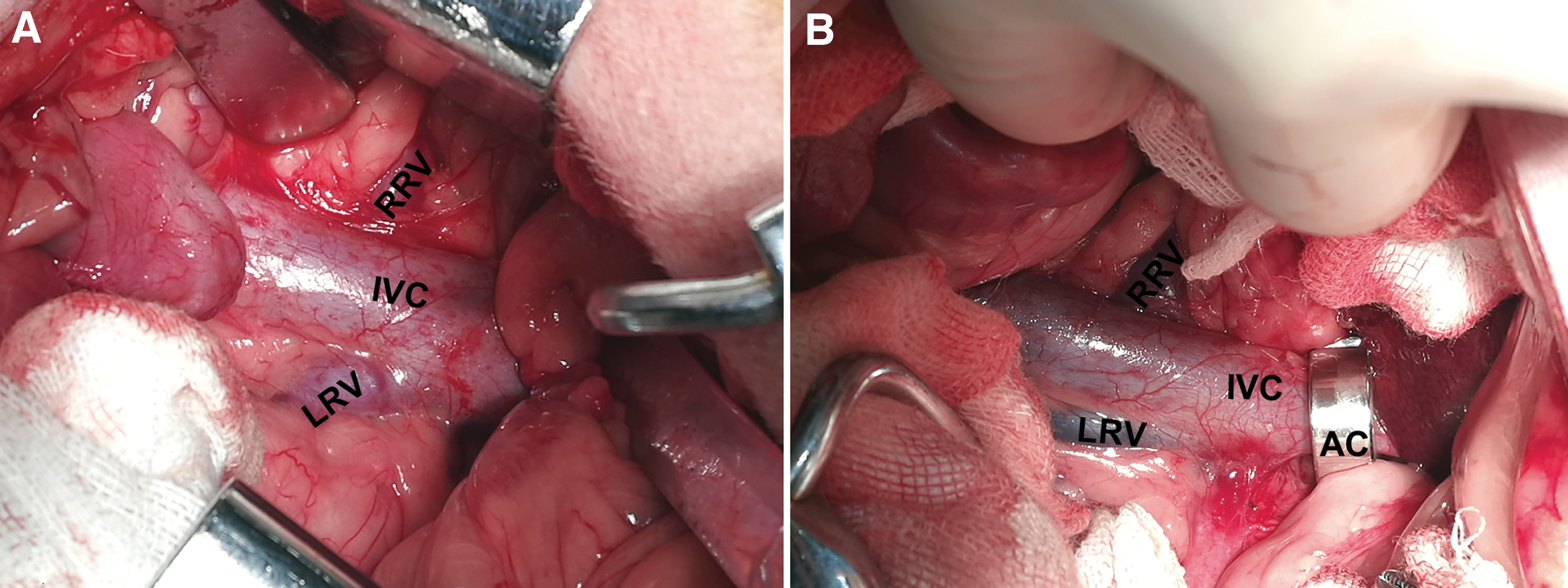
Mobilization and exposure of the IVC
Evaluation of animal models
General observation. Abdominal wall varicose veins and animal weight variation were observed weekly after operation.
Ultrasound examination. It was performed weekly after surgery to observe the position of the AC, the diameter, and the blood flow velocity in the IVC.
CT scan. Six weeks after operation, the experimental dogs were given multi-row spiral CT examination under general anesthesia to observe AC position and internal organ variation by AC obstruction.
IVC angiography. Six weeks after surgery, the experimental dogs were anesthetized. Then, they were fixed on a board in the supine position and venous access was established on one side of the upper limb. The right groin area was sterilized. Modified Seldinger technique was used. 11 Specifically, the right femoral vein was punctured to leave a 4F catheter sheath, and a pigtail catheter was placed through the sheath to accomplish IVC angiogram (20 mL of Iohexol through a quick push). The catheter sheath was removed after angiography and the puncture point was pressed for 5 minutes to prevent bleeding.
Liver and renal function assessment. Blood samples were taken before and weekly after the surgery. Critical biochemical parameters such as alanine aminotransferase (ALT), aspartate transaminase (AST), blood urea nitrogen (BUN), and serum creatinine (SCR) were monitored.
Renal biopsy. It was performed before AC placement and at 2, 4, and 6 weeks after IVC obstruction.
Statistical analyses
Results for diameter and flow rate of IVC before and after AC occlusion were analyzed by t-test. All statistical analyses were performed with PASW Statistics software 18.0 (IBM Corp., Armonk, NY), with p < 0.05 considered statistically significant.
Results
Varicosity on the abdominal wall
Superficial varicose veins were observed on the abdominal wall of both dogs at 2 weeks after AC placement. As time went by, 4–6 dendritic or tortuous varicose veins were detected with diameter up to 6 mm (Fig. 2). However, the number of superficial varicose veins on the abdominal wall no longer increased at 4 weeks after the surgery.

Superficial varicose veins on the abdominal wall.
Increasing diameter and reducing flow rate of IVC after AC obstruction
Doppler ultrasound examination was performed regularly before and after operation. As shown in Figure 3A, the diameter of the IVC after AC obstruction increased by ∼30% at 4 weeks compared with the preoperational size (dog 1, from 11 to 14.1 mm; dog 2, from 10.4 to 13.5 mm). Meanwhile, the IVC flow rate decreased by more than 50% at 4 weeks after operation (dog 1, from 7 to 2.4 cm/s; dog 2 from 7.3 to 3.4 cm/s). Significant differences were noted for IVC diameter (p = 0.0182, Fig. 3B) and IVC flow rate (p = 0.0148 Fig. 3C) before and 4 weeks after AC occlusion. Interestingly, the peak diameter and bottom flow rate of the IVC were both documented at 4 weeks after AC placement, which may indicate the mature establishment of collateral circulation by IVC occlusion at that time point (Supplementary Fig. S1). No evidence of thrombosis was noted in the IVC at all time points after AC placement.
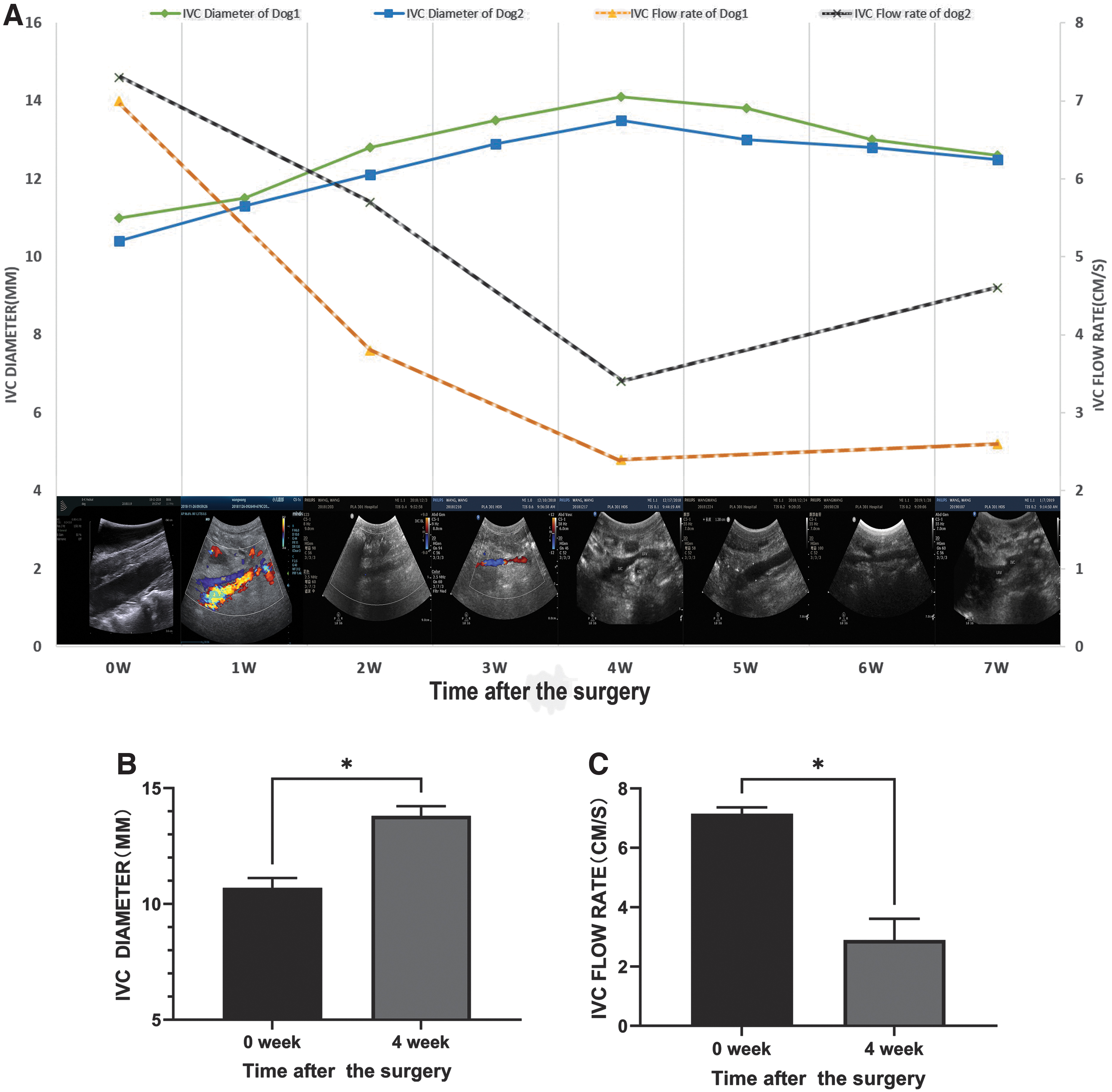
IVC diameter and flow rate variation by ultrasound examination.
Extensive establishment of the collateral circulation and kidney congestive alteration by AC obstruction
Six weeks after surgery, IVC angiography was performed. After injecting the contrast agent, the angiography results indicated total occlusion of the IVC in the location where the AC was placed. Venous return blood made a diversion through the dilated lumbar vein, azygos vein, hemiazygos vein, and inferior phrenic vein back to the right atrium. Meanwhile, neovascularization was also observed by IVC angiography. More collateral circulation establishment was found on the right side than on the left side of the IVC (Fig. 4A).
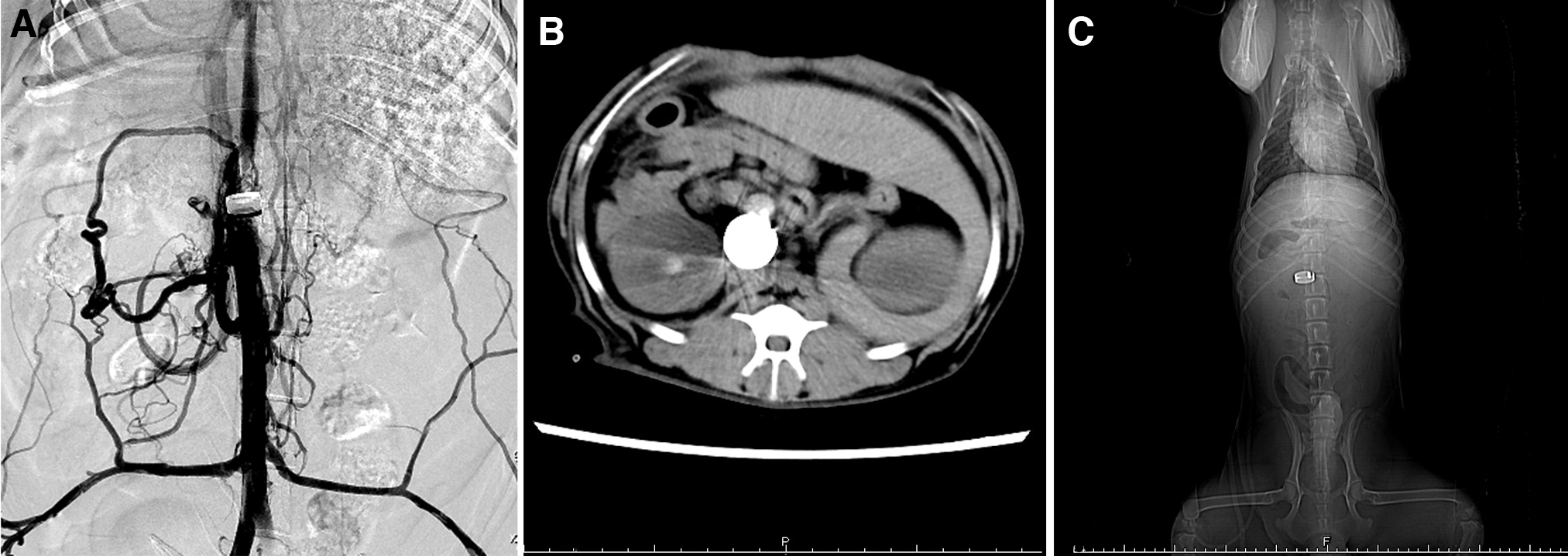
IVC angiography and CT scan after AC obstruction.
As shown in Figure 4C, stable placement of the AC was confirmed by CT scan 6 weeks after surgery. Although congestive alteration was observed in the kidney, no evidence of seroperitoneum or edema in the bowel system was observed (Fig. 4B).
Modeling is safe and stable
The vital signs and mental state of experimental dogs were in stable condition after surgery. In terms of preoperative body weight, one dog slightly lost its weight (from 15.15 to 14.4 kg, dog 1), whereas the weight of the other dog remained unchanged after surgery (from 14.4 to 14.5 kg, dog 2) (Fig. 5A). Kidney function parameters such as SCR and BUN were affected 2 weeks after IVC obstruction and then returned to normal level. Similar variation was observed for liver function parameters (ALT and AST) (Fig. 5B, C). Both dogs experienced mild depression and loss of appetite. No obvious complications, such as infections, ascites, or renal insufficiency, were detected after modeling. The perioperative outcomes of experimental dogs are listed in Table 1.
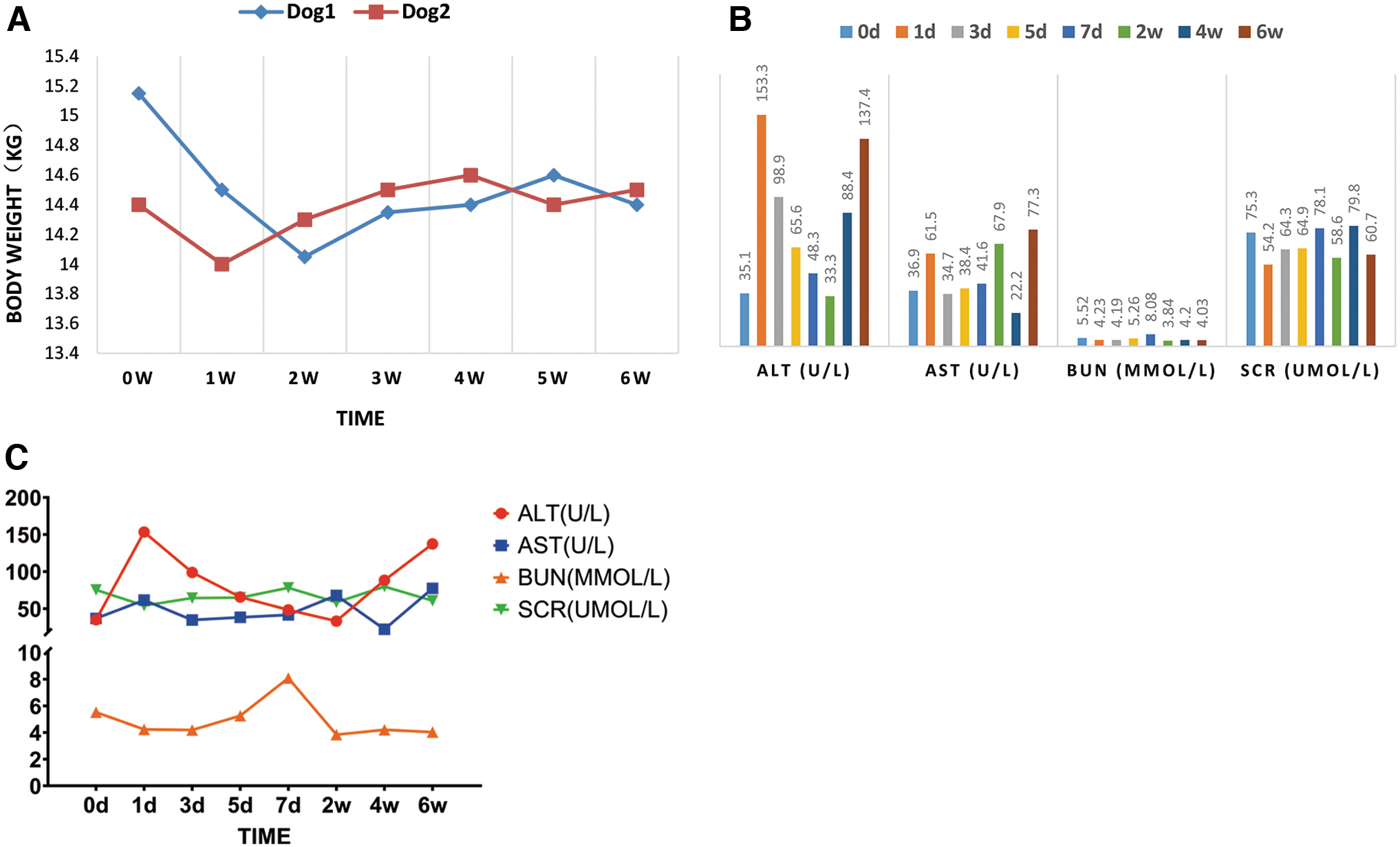
Body weight and liver and kidney function variation.
Perioperative Outcomes of Experimental Dogs
Chronic congestive damage in the kidney
As shown in Figure 6, after placing the AC ring, the biopsy slice showed vacuolation, brush border detachment, epithelial cell deformation, and transparent renal tubular epithelial cells. Mild edema was observed in the stroma with inflammatory cell infiltration. Chronic congestive renal injury was mainly seen in the renal tubular epithelium.

Chronic congestive damage in the kidney. After placing the AC, the biopsy slice showed vacuolation, brush border detachment (red arrows), epithelial cell deformation, and transparent renal tubular epithelial cells (black arrows). Mild edema was observed in the stroma with inflammatory cell infiltration.
Discussion
To date, the key events and factors in the process of progressive IVC obstruction remain unclear. The first key event is the pattern and timing of vessel collateralization. Generally, there are two types of compensatory collateralization: neovascularization and dilatation of the existing vessels. 12 In our study, as a result of IVC progressive obstruction by the AC ring, dendritic or tortuous superficial varicose veins were observed on the abdominal wall. Furthermore, venous return blood made a diversion through a series of dilated vessels, including the lumbar vein, azygos vein, hemiazygos vein, and inferior phrenic vein back to the right atrium. These results indicated the vessel dilation pattern in the collateral circulation establishment process. Meanwhile, IVC angiography showed evidence of neovascularization. Therefore, the two patterns of collateral circulation establishment played an important role in the IVC obstruction process.
The timing of the steady formation of collateral circulation vessels is another key factor. IVCT surgery, including IVC thrombectomy or cavectomy, is determined to remove or resect IVC tumor thrombus while retaining normal venous return function. Thus, in our clinical practice, the optimal timing for surgery should be after the extensive establishment of collateral vessels. In this study, the peak IVC diameter and bottom IVC flow rate were both documented at 4 weeks after AC obstruction, indicating the mature establishment of collateral circulation at that time point. This finding could be favorable for designing the operation timing of IVCT surgery clinically.
The second key event is the thrombosis in IVC progressive obstruction. Previous studies have suggested that reduced venous blood flow can lead to thrombosis. 13 In our clinical experience, thrombosis in the IVC of patients is often accompanied by the formation of tumor thrombus. Interestingly, no evidence of thrombosis in the IVC was observed at all time points after AC placement, which was beyond our expectations and previous reports. 14 The underlying explanation may include the lack of tumor microenvironment, because the IVC was only mechanically obstructed by the ring in our experiment. Therefore, we speculate that the presence of decreased venous flow rate in the tumor microenvironment is a key factor in thrombosis, which needs to be further confirmed by combining the tumor microenvironment with IVC mechanical obstruction in large-scale animal experiments.
The rate of AC closure is known to be nonlinear. In a study by Besancon and colleagues, 10 AC was positioned around the left common iliac vein in six adult dogs to establish the portosystemic shunt animal model. By the time of 8 days after surgery, all dogs had reduction (>50%) in blood flow and three dogs had complete blood flow cessation. Blood flow dropped on an average of ∼10%/day for the first 2–3 days; flow then sharply dropped in all dogs over a period of 24–48 hours. Since one of the major limitations of AC is the variable closure rates from one device to the next, Elzinga, W.E found out by careful fabrication of the device and by drying of the ameroid material, uniform closure rates are obtainable. 15
The AC ring has been widely used in establishing animal models of chronic myocardial ischemia, 16 chronic myocardial infarction, 17 portal hypertension, 10 and treating congenital extrahepatic portal body shunt in animals. 18 Moreover, the AC ring can also be utilized for studying Budd–Chiari syndrome, which is characterized by hepatic venous outflow obstruction at any level from the small hepatic veins to the cavoatrial junction. In a study by Ingles and colleagues 19 using cats, in seven of the animals, portal stenosis was produced by applying an AC. This led to portal hypertension in all animals in the fourth week. In another study by Orloff and colleagues 20 using rat, hepatic venous outflow occlusion has been induced by occluding the IVC cranially to the hepatic veins. Unfortunately, both studies failed to report the variation of IVC flow rates and degree of obstruction. However, none of these animal models are appropriate for studying the tumor thrombus by renal cell carcinoma (RCC) in humans, especially when dealing with the strategy of IVC thrombectomy or cavectomy.
In this study, the IVC was completely obstructed by AC at 6 weeks, which simulated the process of tumor thrombus in humans. Extensive establishment of collateral circulation and stable condition of the experimental animals after AC occlusion could provide solid evidence for the feasibility of IVC resection without large vessel replacement in human IVCT operations.
Conclusions
This study successfully established a canine model of IVC progressive obstruction at the renal hilus level by using an AC ring. This model will be beneficial for studying the pathogenesis and progression of RCC-induced IVC obstruction and can be used to evaluate the efficacy of intervention measures related to IVC obstruction. In addition, it can also provide a research basis for studying more complex circumstances such as the RCC-related IVC obstruction below the hepatic segment in the future.
Footnotes
Authors' Contributions
Conception and design: X.M. and B.W. Administrative support: X.Z. Provision of study materials or patients: Y.Y., S.W., and Q.H. Collection and assembly of data: Q.A. and C.C. Data analysis and interpretation: X.L., H.W., and Q.L. Article writing: all authors. Final approval of article: all authors.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Beijing Natural Science Foundation (no.7194319) and Chinese National Natural Science Foundation (no. 81970594).
Supplementary Material
Supplementary Figure S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.