
Abstract
Objectives:
Mixed reality (MR) technology has emerged in recent years and allows three-dimensional visualization, multiangle observation, remote vision, and virtual–real interaction. This study aims to explore the influence of MR technology on the outcomes and strategy planning of robotic surgery for complex renal tumors.
Patients and Methods:
A total of 92 patients with complex renal tumors were enrolled in this study from June 2018 to June 2020. All patients were found to have tumors by magnetic resonance imaging (MRI) in our department. This trial follows CONSORT guidelines and adopts a single-blind parallel design and randomizes patients with a random number table. The study was approved by the institutional review board, and written informed consent was obtained from each participant. All surgeries were performed by three experienced and high-volume surgeons. The demographic indicators, intraoperative and postoperative complications, renal function outcomes, pathological results, and surgical strategies were recorded. Student's t-test and Wilcoxon rank-sum test were used to compare continuous variables, and Pearson's chi-squared and Fisher's exact tests were used to compare categorical variables.
Results:
Warm ischemia time (WIT) mainly comprises tumor resection time and reconstruction time, and the reconstruction time accounts for a larger proportion. For urologists treating complex renal tumors, MR technology can help them reduce the warm ischemia time (21.3 ± 4.0 vs 23.6 ± 5.9 minutes, p = 0.031), reconstruction time (15.4 ± 3.8 vs 17.2 ± 4.2 minutes, p = 0.034), estimated blood loss (p = 0.044), operation time (125.7 ± 26.3 vs 144.6 ± 27.9 minutes, p = 0.001), and intraoperative complications (p = 0.030).
Conclusions:
MR-assisted surgery can reduce the incidence of intraoperative complications and improve perioperative outcomes, and MR may be a good preoperative tool for planning complex renal tumor surgery.
Introduction
Renal-cell carcinoma (RCC) is a common malignant tumor of the urinary system accounting for 3% of adult malignant tumors. 1 –3 Complex renal tumor mainly refers to a localized tumor with a RENAL score 4,5 ≥ 7 points or an anatomically or functionally isolated kidney with no local or distant metastasis. 6 Technical difficulties during surgery include a shorter warm ischemia time (WIT), 7,8 avoiding positive margins while preserving renal function as much as possible, and reducing complications, which are key for safe and effective partial nephrectomy for complex renal tumors. 9
Mixed reality (MR) technology has emerged in recent years 10 and allows three-dimensional (3D) visualization, multiangle observation, remote vision, and virtual–real interaction. 11 MR technology is being gradually applied in the medical field, but its application to minimally invasive surgery is still in its infancy. 12 In this study, we compared the effectiveness of MR technology-assisted surgery and traditional robotic surgery for complex renal tumors.
Patients and Methods
Patients
Ninety-two patients (59 males and 33 females; mean age 51.6 years; range: 15–86 years) diagnosed as having complex renal tumors based on magnetic resonance imaging (MRI) in our department from June 2018 to June 2020 and who underwent robot-assisted partial nephrectomy (RAPN) were prospectively reviewed in the study. This study was approved by the institutional review board, and written informed consent was obtained from each participant (ethics number: S2017-100-10).
Inclusion and exclusion criteria
Patients with localized tumors with a RENAL score ≥7 points were included in the study. The renal scores of all patients were evaluated by a single senior doctor. The exclusion criteria were bilateral renal tumors, acute heart failure, cardiogenic shock, major organ diseases, previous radical nephrectomy or open or laparoscopic nephron-sparing surgery, and extraordinary complex operation needing hypothermic renal perfusion. 13
Implementation process of the MR model
The patient underwent enhanced MRI examination in our hospital, and the scanning slice thickness was 0.625 mm. The researchers copied the original MRI DICOM-format image data and used the 3D reconstruction system to segment, collect the images, and obtain the mask data for blood vessels and bones. If the images of adjacent structures were not obvious, as the software may not be able to recognize them, manual operation was needed. The kidney, collecting system, arteriovenous system, liver, spleen, and adjacent organs were segmented and then noise reduction and refinement of the model were realized through registration. Finally, the kidney and surrounding tissue structures were constructed. Before operation, the surgeon observed the MR image with the help of handheld devices and HoloLens glasses. The 3D image constructed by MR technology can provide functions such as splitting, transparency, scaling, and rotation to realize immersive deep interaction. At the same time, as a special type of renal tumor, the complex renal tumor presents high technical difficulty in operation because of its difficult location, complex anatomical relationship, and many variations. MR can enable doctors to more intuitively observe the anatomical adjacent relationship between the tumor and artery, vein, and ureter. During the operation, the operator can place the MR images parallel to the console at any time so as to facilitate more rapid resection of the focus and reduce the operation risk and side injury. The depth of the tumor bed was simulated before the operation, and the suture method was performed according to the simulated wound condition. At present, the technology is being routinely used in our department and can be realized by software by ourselves, free of charge for patients. Now there are many technology companies providing MR technical support in our country and the cost for patients is reasonable.
Patient groups and parameters of interest
To understand the impact of MR technology on the clinical efficacy of RAPN for complex renal tumors, the following single-blind research protocol was followed. First, 92 consecutive patients who were diagnosed as having complex renal tumors in our department based on MRI and planned to undergo RAPN were randomly divided into the MR group and control group. This trial adopts a parallel design and randomizes patients with a random number table. For the former group, in addition to referring to MRI, the surgeons formulated the surgical strategy for each patient using 3D images obtained using MR technology before the operation. Only MRI was referred to in the control group. Each patient's demographic indicators (gender, age, body mass index [BMI], RENAL score, and preoperative clinical stage), perioperative parameters (operation time, intraoperative bleeding, WIT, tumor bed reconstruction time, intraoperative blood transfusion, positive resection margin status, postoperative hospital stay, postoperative drainage [the first 24 hours after the operation], and postoperative blood transfusion), intraoperative complications, postoperative complications (based on the Clavien-Dindo classification), pathological results, and surgical strategy, among other parameters, were recorded. The mean follow-up for the MR group and control group was 14.6 and 15.5 months, respectively.
Imaging results of a representative patient
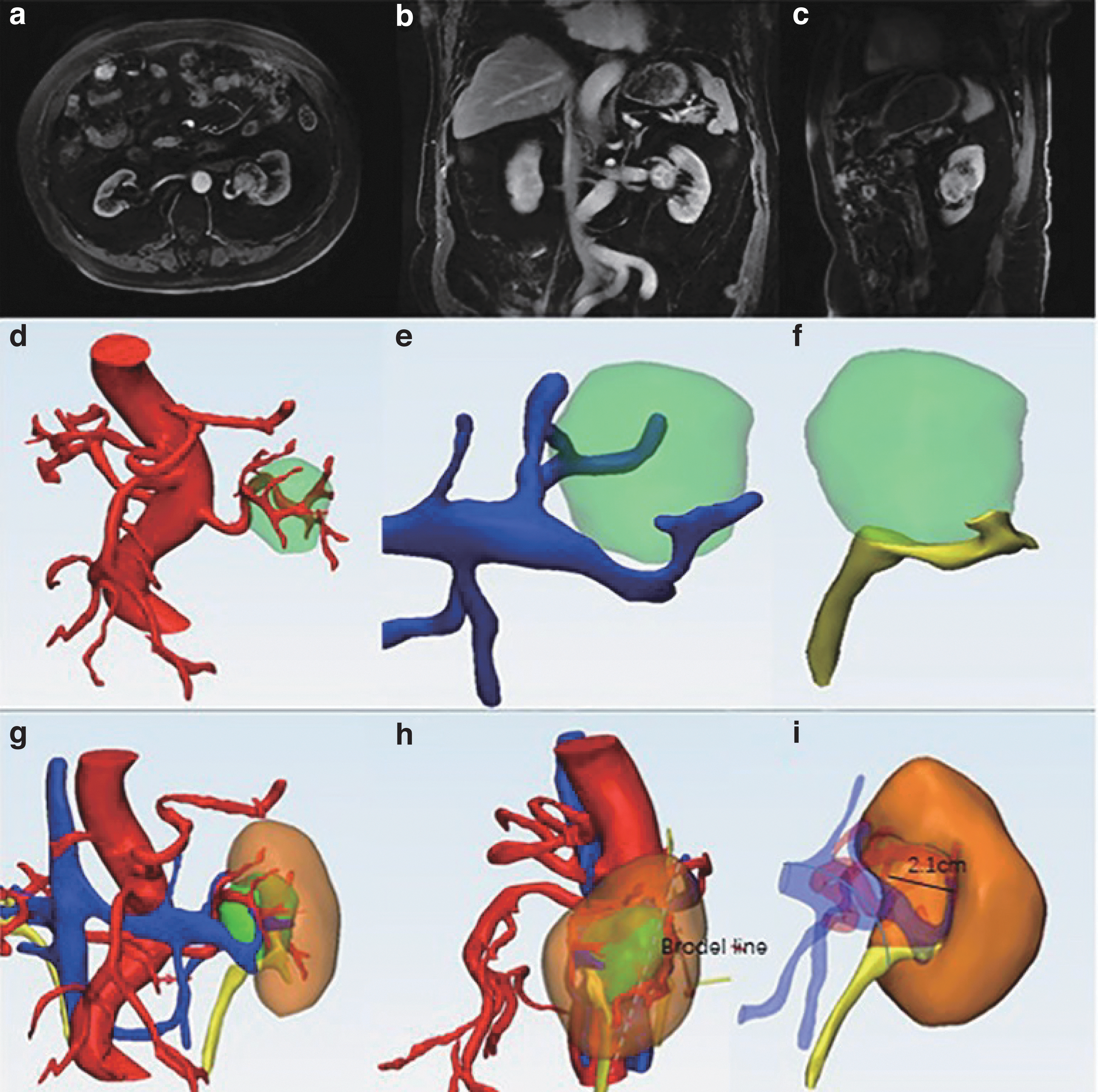
MR results showed that the renal arteriovenous and collecting systems were compressed, and the tumor was completely surrounded by the arteriovenous and collecting systems. The depth of the tumor bed was 2.1 cm after simulated tumor resection (Fig. 1).
Imaging results of a representative patient.
Surgical procedure of the representative patient
Due to the accuracy, predictability, and good visualization of the MR model, the patient's tumor was located; the tumor “squeezed” the vessels and the collecting system. Considering the adjacent relationship of the tumor, the arteriovenous and collecting systems mostly surround the tumor on the ventral side, so we chose the retroperitoneal approach to remove the tumor. The operator resected the renal parenchyma from the dorsal side of the tumor close to the Brodel line, then found the tumor capsule, and completely enucleated the tumor along the capsule. This approach was used in a similar proportion between the two groups. To balance the postoperative bleeding probability and WIT, in our department, if the depth of the tumor bed is <1.5 cm, a single-layer suture is adopted, otherwise a double-layer suture is adopted. If the collecting system is damaged, another single-layer suture is used to close the collecting system. According to the depth of the tumor bed, the surgeon used a single-layer suture to close the collection system and double-layer contraposition suture to close the incision. The operation was successful (Fig. 2); no significant vascular injury or postoperative urine leakage was observed.

Surgical procedure.
Statistical analysis
SPSS 19.0 statistical software (SPSS, Inc., Chicago, IL) was used for the analysis. For statistical analysis, Student's t-test and Wilcoxon rank-sum test were used to compare continuous variables and Pearson's chi-squared and Fisher's exact tests were used to compare categorical variables. A two-sided p-value <0.05 was considered significant.
Results
Comparison of demographic indicators between the two groups
All 92 operations were completed, and in no case was the surgery converted to open surgery. All operations were performed by three experienced and high-volume surgeons (at least 200 RAPN operations). No significant differences in gender, BMI, RENAL score, preoperative clinical stage, or any demographic indicators were observed between the two groups (p > 0.05) (Table 1).
Comparison of Demographic Indicators Between the Two Groups
BMI = body mass index; MR = mixed reality.
Group comparison of parameters of interest in the perioperative period
In the MR group, one patient had intraoperative blood transfusion and one patient had a mild ureter injury. In the control group, five patients had intraoperative blood transfusion, three patients had a mild ureter injury, and two patients had minor spleen tearing. In this trial, we defined mild ureter injury as injury of the ureteral tube wall by electrocoagulation during the operation. To prevent ureter stenosis, Double-J ureteral stents were implanted and removed after 1 month.
All margins were negative. The estimated blood loss (EBL), operation time, WIT, tumor bed reconstruction time, and ratio of intraoperative complications in the MR group were lower/shorter than those of the control group (p < 0.05). There were no significant group differences in the ratio of the single-layer suture or postoperative hospital stay (p > 0.05) (Tables 1 –3).
Nonparametric Test of Estimated Blood Loss and Drainage
EBL = estimated blood loss.
Comparison of Perioperative Indicators Between the Two Groups
WIT = warm ischemia time.
One patient in the MR group had postoperative urine leakage (Clavien-Dindo grade III). One patient in the control group underwent radical nephrectomy on the day of the surgery due to postoperative hemorrhagic shock and was transferred to the intensive care unit (Clavien-Dindo grade IV). One patient received a 4-unit blood transfusion (Clavien-Dindo grade II) due to a continuous decline in the postoperative hemoglobin level (Table 4).
Comparison of Complications Between the Two Groups
Regarding functional outcome, the levels of the estimated glomerular filtration rate (eGFR) after 1 day (p = 0.380) and 6 months (p = 0.894) are similar after surgery between the two groups (Table 5).
Renal Function Outcomes (Estimated Glomerular Filtration Rate, mL/Minute per 1.73 m2)
The postoperative pathological diagnoses in the MR group were clear cell carcinoma (n = 35), eosinophilia (n = 4), chromophobe tumor (n = 1), synovial sarcoma (n = 2), angiomyolipoma (n = 3), and renal perivascular epithelioid cell tumor (n = 1). In the control group, there were 39 cases of clear cell carcinoma, 3 cases of reninoma, and 4 cases of renal vascular-like perivascular tumors. None of the patients developed recurrence or distant metastasis. As of the end of the follow-up period, all patients had no tumor recurrence.
Discussion
Due to the development of technical innovation, more and more patients with complex renal tumors can be treated by nephron-sparing surgery. However, the lack of hand tactile feedback, a narrowed operating space, and limited visual field and visual angle of an endoscope have put forward higher requirements for surgical assistance technology. 14
In 2001, Prof. Cohen proposed the concept of digital medicine. During the past 20 years, the utility of digital medicine has been continuously enhanced. 15 Digital imaging technology can convert two-dimensional images into 3D images. 16 MR technology can be used to accurately reconstruct and display relationships between a tumor and adjacent structures, such as arteries, veins, and the ureter (Fig. 1d–i). Based on these properties, MR technology has broad clinical applications. 17,18 Visualizing the position, anatomical relationships, and variations of complex renal tumors is technically demanding. 19 Due to improvements in surgical equipment and the technical ability of urological surgeons, the postoperative quality of life and survival rate of patients with complex renal tumors have significantly improved. 20,21 In the past, during laparotomy, surgeons were required to shift between the direct vision and the fusion images. MR-assisted surgery has the following advantages: it implements the plane of preoperative virtual nephrectomy into surgery; surgeons can focus on the same monitor without being distracted by changing the field of vision; and if necessary, according to the 3D model of overlapping images, the positional relationship between the tumor and blood vessels can be well understood in real time, which can guide resection of the renal parenchyma and reduce the damage to important blood vessels. 22 –25
Since 2018, our center has taken the lead in development of MR-assisted robotic surgery to treat complex renal tumors and has experience with dozens of cases. Therefore, we are well placed to explore the clinical efficacy of MR-assisted robotic surgery in treating complex renal tumors and its suitability for wide application.
In our original research, improvement of perioperative outcomes and a lower complication rate may be because surgeons formulate more detailed and reasonable resection and suture strategies through MR images before the operation, which can better predict possible adjacent anatomical structure damage so as to avoid some complications and reduce the operation time. In addition to the MR guidance factors, it may also be related to intra-abdominal adhesion, previous abdominal surgery history, and adherent perinephric fat. 26 –28
Previous studies have also reported that the WIT is the most important factor affecting short- and long-term renal functions. 29 WIT >15 minutes is an independent predictor of decline in long-term renal function. 30 WIT mainly comprises tumor resection time and reconstruction time, and the reconstruction time accounts for a larger proportion. Through the comparative analysis of the two groups, we found that the reconstruction time of patients in the MR group was significantly reduced. This result may be due to the lower decision-making time during the operation, and the conjecture is also verified by our research data. MR technology reduces the average operation time by 19 minutes. The reason for this advantage may be that with the help of MR technology, the surgeon can participate in the interaction between the virtual world and the real world and can obtain more tumor anatomical information before the operation. It is helpful for the operator to find the tumor, separate the renal artery faster, select a more appropriate location to remove the tumor, and avoid side injury. Although there were no statistical differences in the preoperative or postoperative eGFRs between the MR group and control group, the main reason for concern is that there is no early method to monitor split renal function, and the compensatory effects of the residual nephron and healthy kidney offset the difference in eGFR values between the two groups.
According to the representative case in this study, the left kidney tumor is located at the hilum, which is completely endogenous and difficult to operate (Fig. 1a–c). The reconstructed MR images before the operation obviously indicate that the tumor compresses the blood vessels and collecting system of the kidney (Fig. 1d–f). An incision close to the Brodel line is a reasonable surgical method (Fig. 1h). According to the depth of the tumor bed, the surgeon used a single-layer suture to close the collection system and double-layer contraposition suture to reconstruct the tumor bed. Compared with the intraoperative situation, the preoperative MR reconstructed images provide accurate and important information such as the location and adjacent relationship of the tumor.
This study further demonstrated that due to the unique advantages of MR technology in displaying anatomical structures, MR technology can guide urologists to develop more effective surgical strategies for treating complex renal tumors.
In addition, there are some limitations in our trial: (1) intraoperative application of the MR model requires manual registration and there is no real-time registration; and (2) this is a small series and further study is required. We will improve the above defects in the next step.
Conclusions
MR-assisted surgery can reduce the incidence of intraoperative complications and improve perioperative outcomes, and MR can be a good preoperative tool for planning complex renal tumor surgery.
Footnotes
Authors' Contributions
Y.Y., Y.G., and X.Z. contributed to testing, statistical analysis, and article writing and editing. B.W., J.Z., and X.Z. contributed to project design and article writing and editing.
Acknowledgment
This study was supported by the Beijing Visual 3D Medical Science and Technology Development Co., LLC, for technical support.
Ethical Approval
Our study was approved by the local ethics committee and performed in accordance with the ethical standards of the institutional research committee. This article does not contain any studies with animals performed by any of the authors.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was financially supported by the Artificial Intelligence Project of PLA General Hospital: 2019MBD-033.