
Abstract
Objectives:
The current study aimed to evaluate the long-term outcomes of TURED (transurethral resection of the ejaculatory duct) in treating male infertility due to ejaculatory duct obstruction (EDO) to the short-term follow-up.
Methods:
From 2000 to 2010, we retrospectively reviewed 30 men with infertility resulting from EDO who underwent TURED. Information on preoperative evaluation of patients was collected from the medical records. Standardized semen analysis was performed 6 weeks, 3 months, and 12 months postoperatively, as well as after a 7-year follow-up.
Results:
The average age of patients was 35.5 ± 2.6. All patients had low ejaculate volume and normal range of the mean serum hormone levels (gonadotropins and testosterone). Transrectal ultrasonography (TRUS) assessment revealed midline cysts in 46.7% (n = 14 cases), a seminal vesicle dilatation in 83.3% (25/30 cases), and ejaculatory duct dilatation in 76.7% (23/30 patients). In addition, two patients (6.6%) underwent MRI pelvis to confirm equivocal EDO by TRUS. After short-term and long-term follow-up, semen parameters improved significantly in 90% of cases vs 63.3% of cases, respectively, with statistically insignificant differences in all parameters (p ≥ 0.1). Based on subgroup analysis, semen parameters improved in all partial EDO and cystic EDO cases vs complete EDO and noncystic EDO, respectively. Spontaneous pregnancies were achieved in 10 (33.3%) vs 8 (26.6%) cases after short and long term, respectively. Regarding post-TURED complications, we reported 23.3% (n = 7).
Conclusion:
TURED is an effective treatment for EDO. It significantly improves all semen parameters and improves the symptoms related to EDO after short and long-term follow-up.
Introduction
Infertility accounts for 15% of couples worldwide, with male factor infertility accounting for 50% of cases. 1 In addition, ejaculatory duct obstruction (EDO) represents a percentage ranging from 1% to 5% in infertile men. 2
Cysts and strictures are congenital causes of EDO, while infections, trauma, and stones are acquired causes. 2,3
EDO can be accompanied by some symptoms, such as low ejaculate volume, postejaculatory pain, hematospermia, or infertility. It has pathognomonic semen parameters that include low-volume azoospermia or severe oligozoospermia, low potential of hydrogen (PH), low or absent fructose with normal secondary sex characteristics, testes, and hormonal profile.
Vasography is the most accurate diagnosis in these cases; nonetheless, it may lead to severe vasal injury or stricture. 3 Radiology to confirm the diagnosis includes high-resolution transrectal ultrasonography (TRUS) and/or MRI showing dilated seminal vesicles (>1.5 cm) or dilatation of ejaculatory duct (ED) diameter (>2.3 mm), midline cyst, or calcifications. 4
The main treatment cornerstone for these conditions is transurethral resection of the ejaculatory duct (TURED), 2 as recommended by the European Association of Urology. 5 Farley and Barnes described this procedure for the first time in 1973. 6
Many studies have discussed the short-term outcome of TURED as a treatment for EDO and demonstrated its success and effectiveness, but the long-term effect has yet to be defined. To our knowledge, this is the first study to address the long-term follow-up for 7 years after TURED.
We aimed to study the long-term follow-up results of the TURED in terms of symptoms, semen parameters improvement, and occurrence of the pregnancy. In addition, we investigated success predictors. Therefore, the wife's age must be in the fertility stage during the follow-up period.
Methods
The current retrospective study included 36 patients who underwent TURED for EDO at Banha and Al-Azhar University hospitals between January 2000 and December 2010. Patients' data were obtained from the medical records after bioethical approval by local ethical committee of the author's institutional review board and obtaining informed consent from participants. Patients were contacted by phone and email for long-term follow-up. However, only 30 patients responded, and they were scheduled for the urology clinic and laboratory visits.
All patients were evaluated by taking a complete history that focuses on symptoms related to EDO, such as decreased orgasmic sensation, nonprojectile ejaculation, and painful ejaculation. Also, the physical examination included normal external genitalia and a standard hormonal profile (follicle-stimulating hormone [FSH], luteinizing hormone [LH], testosterone, and prolactin. All patients had an active and healthy sexual life.
Semen analysis was performed twice before TURED, and it was characterized by low ejaculate volume (<1.5 mL). All patients underwent TRUS (6–10-MHz 3D endorectal probe) to determine the cause of EDO, which was suggested by seminal vesicle dilatation (>15 mm) with or without ED dilatation (>2.3 mm). For an equivocal diagnosis, an MRI with the endorectal coil was performed.
In all patients who had postejaculate urine analysis, the diagnosis of retrograde ejaculation was ruled out. In addition, the patients' wives were in the fertility age and had no female impediment to pregnancy conception.
Surgical procedure
The procedures were performed under spinal anesthesia and in the lithotomy position, with a single prophylactic dose of 1 gm intravenous (IV) of ceftriaxone 1 hour before the induction of anesthesia, and oral antibiotics for 1 week postoperatively.
Cystourethroscopy was performed to rule out any urethral abnormality and delineate verumontanum anatomy status and any abnormalities such as calcifications.
A standard 24-French transurethral resectoscope loop (30_ optical device) was used to perform resection. The TURED procedure was performed as follows:
According to the operation described by Farley and Barnes, (1) transurethral resection of the proximal verumontanum was carried out. 6 In cases diagnosed with midline cyst, deroofing was done (Fig. 1).
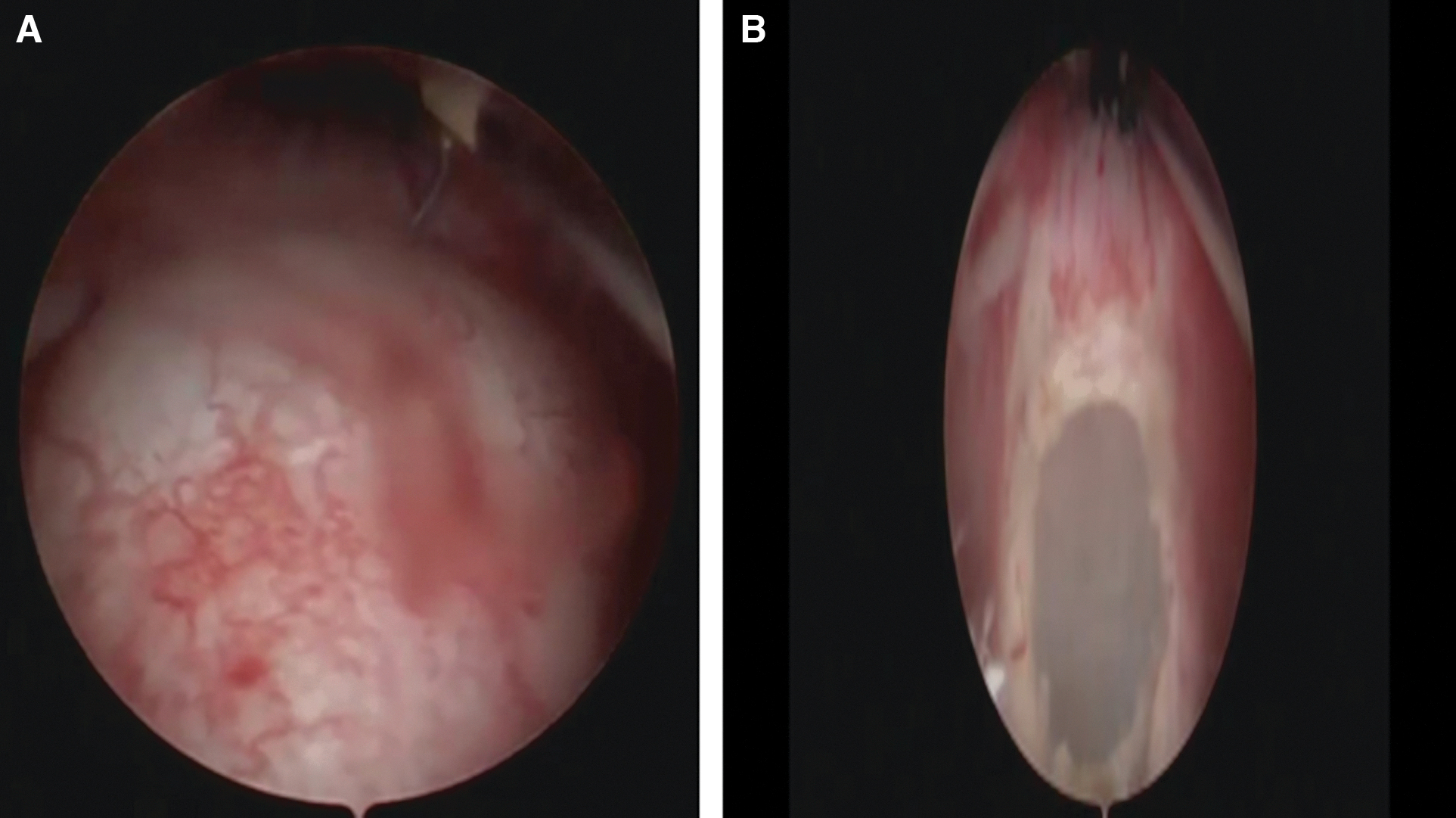
(2) In patients with noncystic obstruction, the procedure's success was determined by visualizing the two openings of the EDs and the efflux of copious, cloudy material. If not, digital rectal prostatic massage was performed until efflux was detected (Fig. 2). In addition, retrograde vasography was done in two patients after completion of resection to document patency of vas.

Electrocauterization was avoided or gently done if needed to prevent iatrogenic obstruction.
The urethral catheter was fixed over a floppy-tip straight guidewire to facilitate insertion after resection. A urethral catheter was left postoperative for 24 hours, whereas abstinence of ejaculation was advised for 1 week postoperatively.
Follow-up
In some patients, a follow-up evaluation was performed to assess the improvement of symptoms present before the operation. Standardized semen analysis was performed 6 weeks postoperatively and at 3-month, then at 12-month follow-up, and finally after 7 years according to World Health Organization standards 2010. 13
Statistical analysis
We analyzed the collected data using SPSS (IPSS Statistics for Windows, version 27.0; IBM, Armonk, NY). Descriptive statistics were performed to evaluate the whole population and both subgroups. Non-normally distributed data were presented as median and range, and the Wilcoxon signed-rank test was used to compare non-normally distributed continuous variables in one group. Chi-square was used to assess categorical variables. The level of significance was determined at p < 0.005.
Results
Thirty patients met the criteria and were included in our study, with a mean age ± standard deviation of 35.5 ± 2.6, a mean patient's wife age of 28 ± 4.4, and the average duration of infertility was 4.33 ± 1.9 years. External genitalia were normal in all patients, as was the digital rectal examination. In addition, the mean serum hormone levels (FSH, LH, testosterone, and prolactin) were within the normal range in all patients. Infertility was primary in 90% (n = 27) and secondary in 10% (n = 3).
On TRUS assessment, 46.7% (n = 14 cases) had midline cysts, a seminal vesicle dilatation in 83.3% (25/30 patients) with a mean diameter of 15.9 ± 1.9 mm, and ED dilatation was reported in 76.7% (23/30 patients) with a mean diameter of 2.57 ± 0.18 mm. In addition, two patients (6.6%) underwent an MRI pelvis to confirm equivocal EDO by TRUS, which revealed dilated EDs.
Congenital midline cysts were the cause of EDO in 46.7% (n = 14 cases) and postinflammatory in 53.3% (n = 16), including patients with a history of STDs in 13 patients, and bilharziasis in three patients.
Complete EDO was considered in 66.7% (n = 20) with azoospermia, while partial EDO in 33% (n = 10) with severe oligozoospermia (<1 million/mL) and all those patients had low-volume ejaculate (<1.5 mL) and asthenozoospermia (motility <30%). Semen fructose was low in all cases with a mean of 2.27 ± 3.67 and low PH.
The mean operative time of TURED was 27.50 ± 9.45, post-TURED, semen parameters significantly improved in 90% of cases after short-term follow-up (1 year follow-up with mean (10.5 ± 3.5 months) (p < 0.001), semen volume increased from 0.5/(0.4–0.8) mL to 2.25/(0.4–4.2) mL, sperm concentration improved from 0/(0–5) × 106/mL to 16.2/(0–64) × 106/mL, and sperm motility increased from 0/(0–28) % to 40/(0–65) (median/range) (Table 1).
Comparison Between Preoperative Semen Parameters and Postoperative Early and Late Follow-up
Statistics: non-normally distributed data presented as median and range, Wilcoxon signed-rank test was used.
On subgroup analysis, semen parameters improved in all cases of partial EDO compared with 85% for complete EDO cases. Similarly, they improved in all patients with cystic EDO compared with 81.3% for noncystic EDO, with an insignificant p-value (Table 2).
Comparison Between Subgroups of EDO (Cystic vs Noncystic and Partial vs Complete Obstruction) as Regard Post-TURED Semen Parameters Improvement After Early and Late Follow-up
Chi square test was used.
EDO = ejaculatory duct obstruction; TURED = transurethral resection of the ejaculatory duct.
Long-term follow-up (7 years with a mean of 90.87 ± 4) months post-TURED, semen parameters improved in 63.3% of cases (p < 0.001), 30% of the patients had normal semen parameters that can impregnate their wives, median/range of the semen volume was 2.5/(0.3–4) mL, sperm concentration and motility was 12/(0–62) × 106/mL and 38/(0–60) %, respectively. On subgroup analysis, semen parameters improved in 80% of partial EDO compared with 55% for complete EDO cases. Similarly, with an insignificant p-value, they improved in 71.4% cystic EDO compared with 56.3% for noncystic EDO (Table 2).
Spontaneous pregnancy occurred in ten cases (33.3%) vs eight cases (26.6%) after a mean post-TURED time of 10.5 ± 3.5 months vs 90.87 ± 4 months, respectively. It predominates in partial and cystic EDO cases compared with complete EDO and noncystic cases.
Regarding post-TURED complications, we reported 23.3% (n = 7), including epididymitis in two patients who improved after 3 weeks of antibiotics and analgesics, watery ejaculate in two patients, hematospermia in one patient, which was self-limited after 1 month, postvoid dribbling in one patient, and one patient had oligozoospermia converted to azoospermia after 7 years, which might be testicular dysgenesis.
After 7 years, we detected a statistically insignificant decline in all semen parameters compared with early post-TURED parameters. However, it was more pronounced for sperm motility and concentration, as depicted in Table 1.
After short and long-term follow-up, we reported 90% post-TURED symptom relief; the prevalent symptoms were perineal pain, hematospermia, and testicular and periejaculatory pain.
Discussion
EDO is a rare and correctable cause of male infertility. 7 It can be accompanied by azoospermia in complete obstruction and oligozoospermia, low ejaculate volume, hematospermia, or periejaculatory pain. 8
TRUS is considered the first choice for evaluating patients with suspicious EDO, as reported in more than 85% of the published studies. 9 For equivocal TRUS evaluation results, a pelvic MRI can be considered. However, as Purohit et al. 10 reported, both diagnostic tools rely on static anatomical assessments, misdiagnosing functional EDO, and indicating false-positive results.
In a prospective study including 25 patients, Purohit and colleagues 10 compared three diagnostic tools with TRUS for EDO diagnosis. They found that obstruction diagnosed on TRUS was confirmed in only 36%, 48%, and 52% of cases by duct chromotubation, seminal vesicle aspiration, and vesiculography, respectively. They concluded that duct chromotubation is more accurate in diagnosing EDO.
In our study, EDO diagnosis depended on TRUS assessment. In addition, we requested pelvic MRI assessment in two patients for equivocal results on TRUS and showed dilated ED.
Some modifications in the EDO diagnostic techniques, including TRUS-guided aspiration of the seminal vesicle, proceeded with ejaculation in the last 24 hours. The presence of three sperms/high-power field in the aspirate is a clue for EDO diagnosis. 11,12
Seminovesiculography depends on TRUS-guided injection of nonionic contrast media into the seminal vesicle followed by fluoroscopy or plain pelvic X-ray. 13 Seminal vesicle chromotubation depends on TRUS-guided injection of Methylene Blue or Indigo Carmine inside the seminal vesicle combined with cystoscopic assessment for ED patency. 14
Although TURED is the standard treatment for EDO, new surgical techniques include dilatating the ED using a balloon or F9 seminal vesiculoscopy 15 and drilling of the ED with LASER. 16 Holmium LASER is used for TURED with a short depth (0.4 mm) to alleviate the incidence of rectal injury. Still, there is a risk for postoperative azoospermia secondary due to the closure of ED, and thus several studies are needed to confirm its use in reproductive urology. 17
One year after TURED, we detected an improvement in all semen parameters in 90% of cases. In addition, on subgroup analysis, semen parameters improved in 100% of partial EDO cases compared with 85% for complete EDO cases. Furthermore, they improved in 100% of cystic EDO compared with 81.3% for noncystic EDO, with a statistically insignificant difference.
Some authors discussed subgroup analysis and the predictors of improvement post-TURED; El-Assmy and others 7 reported semen parameters improved in 100% of cases with partial EDO compared with 23.5% for those patients with complete obstruction. In addition, 71.5% of patients with cystic EDO improved compared with 31% of patients with noncystic EDO. Similarly, Kadioělu et al. 18 found that 94% of cases with partial EDO improved compared with 59% for complete EDO and 85% of patients with cystic EDO improved in semen parameters compared with 45% of noncystic EDO. Also, Netto and associates 19 reported improvement for all patients with congenital EDO compared with 37.5% for acquired causes.
Previous research on the post-TURED outcome revealed improvement in at least one semen parameter. Semen volume improved in 83% of patients, while sperm concentration and motility improved in 62.5% and 63% of patients, respectively. 9
In our study, one patient was low-volume oligozoospermia transformed to normal volume azoospermia after 7 years. In addition, some studies reported a post-TURED transformation from low-volume azoospermia state to normal-volume azoospermia that can be illustrated with secondary epididymal obstruction, which was confirmed and treated. 7,18,20,21
This obstruction can be attributed to the longer and more proximal EDs or even extracapsular in patients with the acquired causes, making the operation more complex, or there is difficulty and an inability to reach the level of stenosis. 22,23
However, one study showed significant improvements in patients with stenosis due to infection-causing EDO. 24 Consequently, the cause is still being debated.
According to previous research, post-TURED natural pregnancy rates ranged between 0% and 67%, with a median of 25% with no findings regarding live birth percent outcome, as reported by 23 studies.
The short-term and long-term pregnancy rates were 33.3% and 26.6%, respectively; all had a live birth. The best pregnancy rates were observed for partial EDO (90%) and congenital EDO (92.9%), which coincides with other reports, such as El-Assmy and others, 7 who reported two of the three pregnancies in partial obstruction. Similarly, Kadioělu et al. 18 found that three of five pregnancies occurred in patients with partial obstruction. Netto and associates 19 discovered that patients with congenital obstruction had a higher pregnancy rate (four of five pregnancies). By improving semen parameters, TURED also allows for the utilization of ARTS if intrauterine insemination (IUI) criteria were not met and the natural pregnancy was not possible. 9,25
A surgical alternative to TURED for men with EDO to conceive naturally is to retrieve sperm for in vitro fertilization/intracytoplasmic sperm injection (IVF/ICSI). In men with obstructive azoospermia, sperm retrieval rates were ∼100%. Also, live birth rates were documented in 32%–36% of the cases. 26,27 Although it may enable the couple to conceive at a higher rate and faster than TURED and normal pregnancy, this approach is significantly more expensive. It requires interventions from both partners: sperm retrieval from the man and egg extraction and transfer for the woman. IVF/ICSI may be necessary after TURED, but the use of ejaculated sperm becomes an option for patients who have experienced azoospermia. 28
In our study, we had eight patients qualified for IVF/ICSI with ejaculated sperm (26.6%).
IUI is often offered to patients with a total motile sperm count (TMC) greater than 5 × 106. 9 For example, in the study of Mekhaimar et al., 9 25%–40% of patients had a TMC of more than 5 × 106, making IUI eligible instead of In vitro fertilization (IVF) and the pregnancy rate for those patients ranged between 7%–8%. Our study reported two patients who were transferred from IVF to IUI eligibility state, where (TMC) was greater than 5 × 106 but no pregnancy (Table 3).
Qualified Patients for IUI and for IVF/ICSI with Ejaculated Sperm Post-TURED
Chi square test was used.
IUI = intrauterine insemination; IVF/ICSI = in vitro fertilization/intracytoplasmic sperm injection; TMC = total motile sperm count.
Complications following the TURED procedure were reported in a range between 0% and 36% with a median of 10% of the patients, commonly epididymo-orchitis (26% of the reported complications), hematuria (22%), and watery ejaculate that can be explained with urine reflux into the seminal vesicles accounting for 20% of the reported complications. 9 In the current study, the complication rate was 23.3%, commonly epididymo-orchitis (28.5%), watery ejaculate (28.5%), hematospermia (14.3%), postvoid dribbling (14.3%), and one (14.2%) patient had oligozoospermia converted to azoospermia after 7 years.
Our study revealed symptom relief for 90% of the patients. The most common EDO-related symptoms were epididymitis, watery ejaculate, and hematospermia, coinciding with other reports. 3,18,22,25 In contrast, other series reported 50%–100% symptom improvement. 9
In the current study, long-term follow-up after a mean period of 90.8 ± 4 months post-TURED showed improvement in all semen parameters for 63.3% of our patients; 30% of the patients had normal semen parameters that can impregnate their wives. The follow-up time was detailed in most studies, ranging from 2 to 78 months, with a median of 12 months postoperatively. 9 In the current study, we discussed two follow-up terms: the short term after 1 year with a mean of 10.3 ± 3.5 months and the longer one after 7 years with an average of 90.87 ± 4 months.
Limitations
First, our study is a retrospective study with small sample size. Retrospective studies may be a potential source of selection bias, and hence outcomes across different variables could be inaccurate. Furthermore, the predictor of success and causes of lower efficacy of TURED after long term need further prospective studies to delineate.
Conclusion
TURED is effective and durable in infertile males with EDO by permanent removal of the cause of the obstruction in the long term. However, there is a decrease in all semen parameters in the long term than short term, but statistically insignificant and long term allows the result of pregnancy to be judged better, considering the age of the wife in the fertile stage.
Key Points
TURED has been shown to improve semen parameters in 100% of partial EDO cases compared with 85% for complete EDO cases. Similarly, they have been improved in all patients with cystic EDO compared with 81.3% for noncystic EDO.
Around 33.3% vs 26.6% of patients achieved natural pregnancy post-TURED on short- and long-term follow-up, respectively.
Partial EDO and congenital causes of EDO (cysts) were associated with more significant improvements in semen parameters and higher natural pregnancy rates.
The median complication rate post-TURED was 23.3%, with the most common complications being epididymitis and watery ejaculate.
TURED is an effective and durable treatment option for EDO on long-term follow-up.
Informed Consent for Participation and Publication
Informed written consent was obtained from all patients before the study for the involvement and publication.
Ethics Approval
Patients' data were obtained from the medical records after bioethical approval by local Ethical Committee of the author's institutional review board.
Availability of Data and Materials
The data that support the findings of this study are available from the corresponding author upon request.
Footnotes
Authors' Contributions
All listed authors (I.A, A.E., G.M.H., and T.M.G.) have performed all four points specified below: (1) Made substantial contributions to conception and design, methodology, acquisition of data, or analysis, review, and interpretation of data. (2) Involved in drafting the article or revising it critically for important intellectual content. (3) Provided final approval of the version to be published. Each author should have participated sufficiently to take public responsibility for appropriate portions of the content. (4) Agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors read and approved the final article and confirmed that all methods were carried out in accordance with relevant guidelines and regulation.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.