
Abstract
Background:
We performed a retrospective comparison of surgical, oncologic, and functional outcomes after robot-assisted radical prostatectomy between patients who have undergone prior transurethral resection of prostate (TURP) to TURP-naive patients.
Methods:
Past robotic prostatectomy hospital data were scrutinized to form two matched groups of patients: those who have undergone prior TURP and TURP-naive patients. The perioperative and pathologic data along with functional and oncologic outcomes for a period of 3 years were compared between groups.
Results:
Compared with TURP-naive patients, prior TURP patients experienced longer robot-assisted laparoscopic prostatectomy times (p < 0.001), increased incidence of bladder neck reconstruction (p = 0.03), greater blood loss (p = 0.0001), and lesser nerve sparing (p < 0.01). Complication rates (p = 0.3), positive surgical margin (p = 0.4), extracapsular disease (p = 0.3), or seminal vesicle invasion (p = 0.1) were comparable between groups. Continence (p = 0.5) and potency (p = 0.1) at 1 year were not different between groups. Biochemical recurrence rates were not different at 3 years (p = 0.9). Diabetes slowed recovery of continence in patients with prior TURP compared with TURP-naive patients until 6 months after surgery.
Conclusion:
Although prior TURP makes subsequent robotic prostatectomy more technically demanding, it can be safely performed by experienced surgeons without compromising long-term functional or oncologic outcomes.
Introduction
Benign enlargement and malignant transformation of the prostate are sometimes synchronously present. Incidental prostate cancer (PCa) is found in 3% to 16% of specimens from transurethral resection of prostate (TURP). 1,2 Alternatively, 4% to 6.4% of patients who have undergone TURP are found with PCa within 7 years. 3,4 Prior TURP can potentially affect surgical, pathologic, functional, and oncologic outcomes after robot-assisted laparoscopic prostatectomy (RALP) caused by periprostatic fibrosis, scarring, and inflammation. 4 –6 Specifically, higher percentage of capsular violation, bladder neck stenosis, and morbidity are documented. 7,8 However, use of the da Vinci robot® has been shown to deliver superior outcomes in such patients. 9,10
There exists paucity of published data comparing outcomes for patients undergoing RALP with and without prior history of TURP. We hypothesize that the impact of prior TURP on overall difficulty of RALP, biochemical recurrence (BCR)-free rates, and functional outcomes is negligible when performed by experienced surgeons. The purpose of this study was to examine the experience of a single-center single high-volume surgeon to determine impact of prior TURP on operative difficulty and clinicopathologic and oncologic outcomes.
Materials and Methods
Study design and protocol
We conducted this retrospective cohort study, which is being reported as per STROBE guidelines. 11 Hospital review board approved (Protocol No. LCH-3-092020) us to query prospectively collected RALP data of 2892 patients for the past 12 years. These were evaluated for demographic, perioperative, pathologic, functional (potency and continence level 1 year after RALP), and oncologic outcomes (BCR within 3 years of RALP). A case–control design formulated two groups of patients. Each of the 150 patients with prior TURP (Group T) was matched in a 1:3 ratio to the remaining cohort that was TURP-naive (Group NoT). Patients were matched for age, body mass index (BMI), clinical stage, prostate-specific antigen (PSA), biopsy Gleason score, D'Amico score, prostate weight, and sexual health inventory for men (SHIM) score (Table 1). The only difference between the groups was the study variable (prior TURP).
Preoperative Characteristics of the Two Groups
Categorical variables by chi-square test and nonparametric continuous data by Mann–Whitney test.
Group T = with prior TURP; Group NoT = TURP-naive group; BMI = body mass index; PSA = prostate-specific antigen; SD = standard deviation; SHIM = sexual health inventory for men; TURP = transurethral resection of prostate.
Exclusion criteria
Patients were excluded from the study if they underwent salvage RALP/neoadjuvant therapy (8), non-TURP surgical benign prostatic hyperplasia treatment (22), had a SHIM score <17 (31), had a urethral stricture (9), were lost to follow-up within 3 years of RALP (16), or had PSA >10 ng/mL (39).
Surgical procedure
All RALPs underwent standard six-port transperitoneal technique using the da Vinci surgical system Si ® (Intuitive Surgical, Sunnyvale, CA, USA) by a single high-volume surgeon. All patients underwent maximum urethral length preservation (MULP) technique as described by Razdan and colleagues. 12,13 Van Velthoven technique was utilized for all. Patients with Biopsy Gleason grade group (BGGG) ≥2 received lymphadenectomy limited to the external iliac nodes. No ureteral stent was placed before RALP. Estimated blood loss (EBL) was defined by the anesthesiologist as the amount of blood in the suction canister minus irrigation.
Patients were discharged after drain removal on postoperative day 1. Foley catheter was removed after 7 days. All patients were initiated on a penile rehabilitation program consisting of 5 mg Tadalafil daily with a vacuum erection device and had regular follow-up visits every 3 months. Perioperative complications over 180 days were graded as per Clavien–Dindo classification system. 14
Data collection
Compliance with the rehabilitative program was confirmed during each visit and by a monthly telephone call by a nurse for 1 year. Functional outcome data were collected at each visit and PSA was monitored regularly. The data were collected in a secured customized database.
Definitions
Console time (CT): Total time surgeon was on the console.
BGGG: Biopsy Gleason grade group. 15
Positive margin: Cancer reaching the inked surface.
Extracapsular disease: Disease outside prostatic capsule.
BCR: Two consecutive PSA ≥0.2 ng/mL after achieving a nadir value of <0.01 ng/mL.
Continence: Pad-free status.
Potency: Penetrative intercourse with/without phosphodiesterase type 5 (PDE-5) inhibitors >50% of times.
Statistical analysis
Age, PSA, BMI, CT, EBL, and prostate weight were tested for normality and homogeneity of variance by Shapiro–Wilk test and two-tailed Mann–Whitney U test, since all showed significant departure from normality (each with p < 0.05). Chi-square test was used for nominal variables. We used multivariable linear regression to assess CT and EBL adjusting for confounders. Binomial logistic regression was performed to predict if prior TURP was an independent predictor of margin positivity, functional recovery, and BCR. Two patients in Group T and four in Group NoT had positive lymph nodes on final histopathology and were eliminated while calculating results of BCR.
All statistical analyses were performed using SPSS v.22.0 software (IMB, Chicago, IL, USA) and Jamovi. 16 p-Value of <0.05 was considered significant.
Results
Group T consisted of 150 patients and Group NoT had 450 patients. In Group T, PCa was diagnosed on TURP chips (n = 2, 1.3%), by delayed detection of elevated PSA (n = 145, 96.6%), or by isolated abnormal DRE (n = 3, 2%). Minimum time between TURP and RALP was 3 months. 17
Perioperative outcomes
Console time
CT was significantly increased in Group T compared with Group NoT (Group T median 70 minutes, interquartile range [IQR] 9 vs Group NoT median 60 minutes, IQR 12 [z = −9.2, p < 0.001]). On multiple regression analysis, longer CT was significantly and independently predicted by prior TURP (p = 0.001), prostate weight (p < 0.001), and EBL (p = 0.04). However, no patients required blood transfusion. Age, BMI, and nerve sparing (NS) status were not predictive of CT (all p > 0.05) (Table 2).
Perioperative Data and Complications As Per Clavien–Dindo Classification
Grade I included additional analgesics, hematuria, and antipyretics. Grade II included UTI's needing antibiotics, and hypnotics. Grade IIIa had Foley reinsertion after catheter removal caused by mucosal edema or lymphocele aspiration. Grade IIIb had bladder neck contractures needing surgical correction.
BNR = bladder neck reconstruction; BPLND = bilateral pelvic lymph node dissection; IQR = interquartile range; UTI = urinary tract infection.
Estimated blood loss
Prior TURP was associated with significantly increased EBL compared with TURP-naive patients (Group T median EBL 110 mL, IQR 20; Group NoT median 90 mL, IQR 40) (z = −7.2, p < 0.01). On multiple regression analysis, EBL was significantly and independently predicted by prior TURP (p = 0.001), prostate weight (p = 0.01) and CT (p = 0.02). Age, BMI, and NS status had no predictive value for EBL (all p > 0.05).
Nerve sparing, pelvic lymph node dissection, and bladder neck reconstruction
We performed significantly less NS on patients in Group T (n = 15) as compared with Group NoT (n = 11) patients (p = 0.002) (Table 2). No significant difference was observed in the prevalence of unilateral (p = 0.07) or bilateral NS (p = 0.5). The positive surgical margins (PSM) rates when stratified by the NS status showed no difference between the two groups (p = 0.7 for non-NS, p = 0.07 for unilateral NS and p = 0.7 for bilateral NS).
Eighty-three patients (55%) in Group T and 253 patients from Group NoT (56.2%) underwent pelvic lymph node dissection (p = 0.8).
The need for bladder neck reconstruction (BNR) was significantly greater in Group T (8%) than in Group NoT (3.7%) [χ 2 (1, 600) = 4.3, p = 0.03].
Length of hospitalization
Two patients in Group T and five in Group NoT were discharged on second postoperative day, whereas remaining patients were discharged on postoperative day 1 with no difference in the duration of hospital stay between the two groups [χ 2 (1, 600) = 0.04, p = 0.8].
Postoperative complications
Differences in the rate of complications between the two groups was insignificant, 21 patients in Group T vs 50 patients in Group NoT [χ 2 (1, 600) = 0.8, p = 0.3]. All complications were Clavien ≤IIIb. Bladder neck contracture occurred in three patients in Group T and six in Group NoT [ χ 2 (1, 600) = 0.3, p = 0.5] (Table 2).
Pathologic data
Margins, capsular breach, seminal vesicle invasion, and lymph node status
Group T had 16 solitary and 5 multifocal PSM. Group NoT had 34 solitary and 19 multifocal PSM with the overall incidence of PSM between groups not significant [14% and 12%, respectively, χ 2 (1, 600) = 0.5, p = 0.4]. We found significantly increased incidence of PSM at the bladder neck in Group T (n = 22, 59.5%) vs Group NoT (n = 21, 33%) [χ 2 (1, 101) = 6.8, p = 0.01], and significantly decreased incidence of PSM at the apex in Group T (n = 5, 13%) vs Group NoT (n = 20, 31%) [χ 2 (1,101) = 3.9, p = 0.04].
For pathologically organ confined disease (pT2a-c), 10 patients in Group T and 34 patients in Group NoT had PSM [χ 2 (1, 538) = 0.04, p = 0.8]. pT3a disease was present in similar proportions in both groups: Group T (n = 11, 7.3%) vs Group NoT (n = 23, 5.1%) [χ 2 (1, 600) = 1, p = 0.3]. Among patients with pT3a disease, we noted PSM in n = 2 (18%) in Group T and n = 15 (65%) in Group NoT, the difference not being significant [χ 2 (1, 34) = 2.5, p = 0.1]. The difference in numbers of seminal vesicle invasion (pT3b) between the two groups was insignificant, Group T (n = 10, 6.6%) vs Group NoT (n = 18, 4%) [χ 2 (1, 600) = 1.7, p = 0.1]. Difference in PSM in pT3b patients was not statistically significant either [χ 2 (1, 28) = 3.5, p = 0.06] (Table 3).
Pathologic and Functional Results
When multiple sites were involved in a single specimen, each site was considered as one site.
Group T (n = 148) and Group NoT (n = 446) as patients with metastatic nodes on specimen received adjuvant treatment and hence removed from analysis.
BCR = biochemical recurrence.
Binomial logistic regression to analyze effect of prior TURP on margin positivity did not show prior TURP to be an independent predictor of PSM status (p = 0.2). PSA, BMI, BGGG, clinical stage, and degree of NS were found to be independent predictors of margin positivity such that higher values of these had a higher margin positivity rate. Higher degree of NS predicted more PSM (Table 4).
Binomial Logistic Regression for Margin Positivity
Estimates represent the log odds of “Margins = Involved (1)” vs “Margins = Not involved (0).” SE of estimate, which measures the accuracy of predictions. A smaller SE means more accurate predictions.
BGGG = Biopsy Gleason grade group; CI = confidence interval; SE = standard error.
There was no statistical difference in the lymph node yield between the groups (p = 0.4). Lymph node involvement was higher in Group T vs Group NoT, although not statistically so (1.3% vs 0.8%, p = 0.6).
Functional outcomes
Continence
There was no statistical difference in the proportion of continent patients at 1 month between the two groups, Group T (n = 122, 82%) and Group NoT (n = 378, 85%) [χ 2 (1, 594) = 0.4, p = 0.5] (Table 3).
At 3 months, significantly different proportions of patients were continent between the groups [χ 2 (1, 594) = 19.2, p = 0.00001] (Table 3). Continence recovery was slower in Group T than in Group NoT (log-rank test p < 0.001 at 3 months). Nevertheless, 9 months after surgery all patients in both groups were continent (Fig. 1).
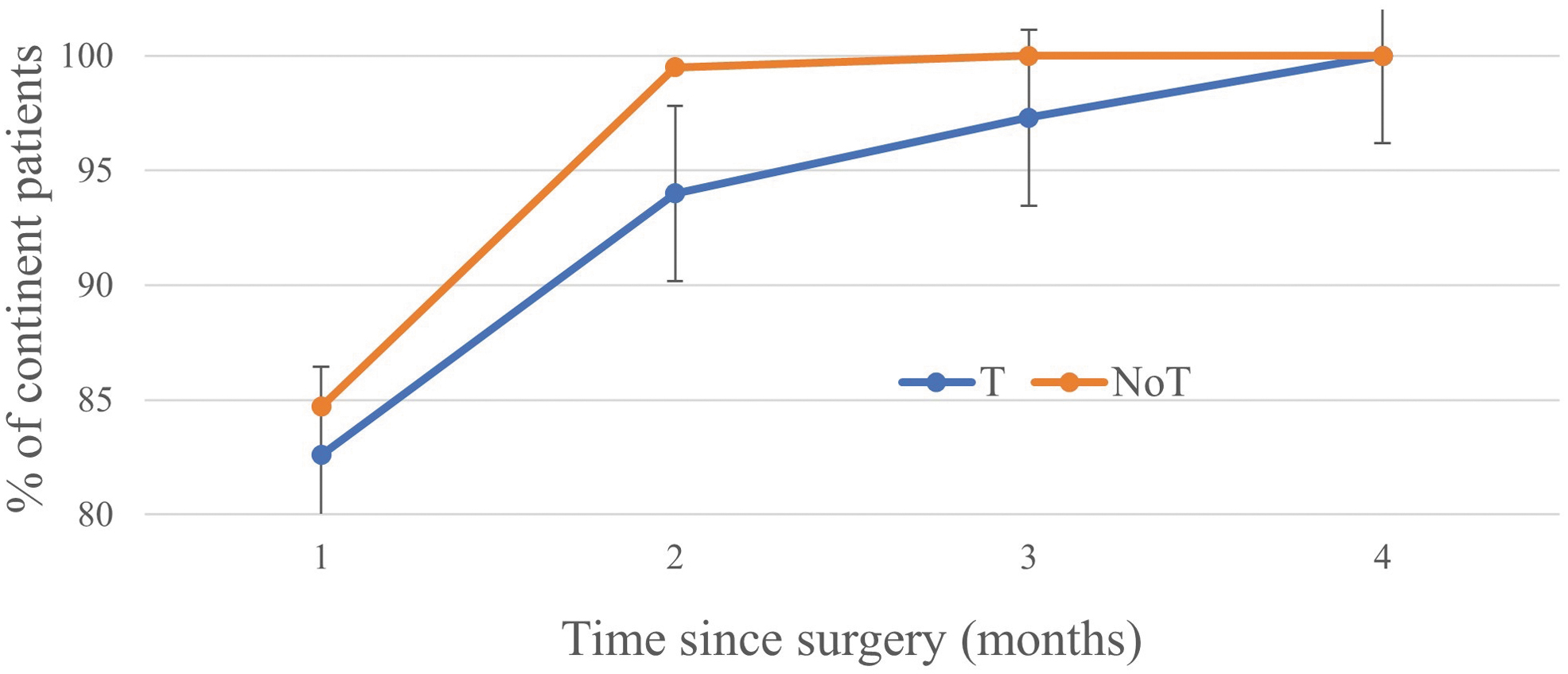
Continence attainment over time for all patients. T = group with prior TURP (blue); NoT = TURP-naive group (red); TURP = transurethral resection of prostate. Color images are available online.
Diabetes mellitus (DM) significantly delayed return of continence in Group T (log-rank test, p = 0.04), and in Group NoT it approached statistical significance (log-rank test, p = 0.05) (Table 5). A log-rank subgroup analysis of nondiabetics from both groups was performed to eliminate the confounding effects of diabetes. 18 No significant difference was observed in the rate of continence at the end of 6 months in this subgroup (log-rank test, p = 0.6) (Fig. 2).

Continence attainment over time in nondiabetics. T = group with prior TURP (blue); NoT = TURP-naive group (red); TURP = transurethral resection of prostate. Color images are available online.
Continence Achievement in Diabetics Vs Nondiabetics in Both Groups
Binomial logistic regression looked for predictors of continence recovery at 3 and 6 months. At 3 months, BNR, DM, and prior TURP were significant independent predictors of continence return. At 6 months none of the parameters analyzed were significant except DM (Table 6). That difference was lost by 9 months, as all patients in both groups were continent by then.
Binomial Logistic Regression for Predictors of Continence at 3 and 6 Months
Estimates represent the log odds of “Continence at 3 and 6 months = 1” vs “Continence at 3 and 6 months = 0”. SE of estimate, which measures the accuracy of predictions.
DM, diabetes mellitus.
Potency
At 1 year, 129 patients in Group T (88%) vs 405 patients (90%) in Group NoT were potent [χ 2 (1, 594) = 2, p = 0.14]. There was no difference in the rate at which these patients gained potency, log-rank test p = 0.2. Binomial logistic regression did not reveal prior TURP to be an independent significant predictor of potency return (p = 0.3). Age, BMI, and NS type were significantly related to return of potency at 1 year, such that advanced age, higher BMI, and lesser grade of NS was associated with poor return. Diabetes and clinical stage were not predictive (Table 7).
Binomial Logistic Regression for Predictors of Potency
SE of estimate, which measures the accuracy of predictions. A smaller SE means more accurate predictions.
Oncologic control
Biochemical recurrence
PSA was <0.01 ng/mL in both groups until the end of 1 year. Three patients in Group T and nine patients in Group NoT had BCR within 3 years of RALP (p = 0.9). BCR was found in two patients with PSM in Group T and in five patients with PSM in Group NoT (p = 0.9). The risk of having BCR did not differ between groups (relative risk [RR] 1, 95% confidence interval 0.2–3.6, p = 0.8).
Binomial logistic regression for BCR showed PSM (p = 0.01) and clinical stage (p < 0.001) to be independently predictive of BCR. Prior TURP was not a significant predictor (p = 0.8).
Discussion
TURP alters tissue layers making subsequent RALP difficult. 7,19,20 Literature compares outcomes of open, laparoscopic, and robotic prostatectomies after TURP with conflicting outcomes. 4,6,10,17,21 Noticeably, robotics has drastically improved the results in terms of functional outcomes post-TURP. 9,10
The goal of this study was to compare perioperative RALP experience with long-term outcomes in matched patients with and without history of TURP. The results show that histopathologic, functional, and oncologic outcomes are not altered by prior TURP.
We report longer operative times for patients with prior TURP, probably accounted for by increased incidence of BNR in these patients. Although our results corroborate data reported by many, Zugor and coworkers had conflicting results. 9,10,22 –25 Despite matching patients like us, their patients had delayed functional recovery. Their subjects came from multiple centers with different surgeons, possibly explaining the delay. Continence recovery in patients post-RALP, with prior TURP is presumed to be difficult because of fibrosis and periprostatic adhesions making salvage of enough urethral length to perform a good anastomosis challenging. MULP enabled us to perform a better anastomosis resulting in superior continence rates as compared with other published studies. 7,10,13
Mustafa and colleagues also reported PSM in men with prior TURP and in TURP-naive patients. 6,23 We report prior TURP results in an overall incidence of PSM like TURP-naive patients, but with a higher risk of PSM at bladder neck and lower risk at apex, which has also been described in the literature. 26,27 The mechanism for these findings is that TURP makes the bladder neck open and thinned out. Therefore, during RALP the margins of the bladder neck incision shifts deep into the prostate base with increased risk of PSM. Meanwhile, the fibrosis at the apex compels the surgeon to put forward the point of apical resection distally consequently decreasing the risk of PSM.
Our study demonstrates that DM delays continence recovery, and its effect is especially pronounced in patients with prior TURP.
Limitations
This retrospective study has its inherent disadvantage of lacking randomization. Role of parenchymal tumor location and its volume on PSM was not assessed. The location and not the length of PSM sites was assessed, which can potentially impact BCR. We did not have the pre-TURP details such as PSA, prior biopsies, resected volume of prostate, which could have been valuable components in the analysis. Improved generalizability would need multicenter prospective randomized studies.
Conclusion
Prior TURP does not impair functional or oncologic outcomes at 1 or 3 years after RALP. Prior TURP may result in longer operative time, increased need for BNR, and greater blood loss. The degree of NS also declines with prior TURP, which should be considered a risk factor for delayed recovery of continence and possibly potency. Prior TURP does not increase the overall risk of PSM but enhances the risk of PSM at the bladder neck.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.