
Abstract
Background:
In the absence of overt infection signs, clinical criteria for early intervention in patients with ureteral stones are poorly defined. We aimed to develop a model that can identify patients who are at risk for developing sepsis if discharged home from the emergency department (ED).
Materials and Methods:
We retrospectively reviewed patients between January 2010 and December 2019 who were discharged from the ED after diagnosis of ureteral stones. The primary outcome was sepsis requiring urgent surgical decompression. We used multivariable logistic regression to identify predictors of sepsis. We refined the model using backward stepwise regression with a threshold p-value of 0.05.
Results:
We identified 1331 patients who were discharged from the ED with ureteral stones. Of these patients, 22 (2%) subsequently developed sepsis requiring urgent decompression. In the initial multivariable model, female gender (odds ratio [OR]: 2.82, p = 0.039) and urine white blood cells (WBCs) (OR: 1.02 per cell count, p < 0.001) were predictive of sepsis. After performing backward stepwise regression, female gender, urine WBCs, and leukocytosis (WBCs >15,000/mm3) met criteria for inclusion in the model. A logistic model including these variables predicted sepsis with an internally cross-validated area under the curve (AUC) of 0.79. Among patients with urine cultures completed in the ED, rates of sepsis were 9% in patients with positive cultures and 1% in patients with negative cultures (p < 0.001). Antibiotic usage was not protective against developing sepsis.
Conclusions:
Sepsis is a rare complication among patients with ureteral stones selected for conservative management. The presence of elevated urine WBCs and female gender can help identify patients who are at risk of developing sepsis. Patients with risk factors should be managed with an increased index of suspicion for infection and may benefit from early intervention to reduce the risk of sepsis. Sepsis is more common in patients with positive urine cultures.
Introduction
Renal colic due to obstructing ureteral stones is a common cause for emergency department (ED) visits. 1 Although many patients with obstructing stones can be discharged from the ED without intervention, the presence of suspected urinary tract infection in the setting of an obstructing stone is recognized as an indication for urgent decompression with either a ureteral stent or nephrostomy tube. 2 –4
However, in the absence of sepsis or overt infection signs, it is often challenging to determine whether an infection is present. Furthermore, urine culture results to definitively diagnose an infection are not typically available in the ED setting or can be falsely negative in the setting of high-grade ureteral obstruction and thus cannot be used in the acute decision-making process.
These factors present a clinical challenge for ED providers and urologists. Discharging patients with unrecognized infections would put them at risk of progression to obstructive pyelonephritis and sepsis, with delayed diagnosis potentially leading to severe illness and death. 4 –6 Conversely, admitting noninfected patients for decompression would result in unnecessary surgical morbidity and excess costs. 7 –10 Thus, the ability to detect patients who are at risk of developing sepsis would enable physicians to more effectively select patients for early urinary decompression vs trial of stone passage.
Prior studies aiming to detect infection in the ED setting have been limited by small samples and they have not distinguished between patients with and without clinical evidence of infection. 11 –14 Therefore, the criteria for early intervention in patients without clear infection signs are poorly defined, potentially contributing to wide variability in intervention rates and antibiotic usage. 15 –17 In this study, we aim to use demographic, laboratory, and radiographic characteristics to identify which patients with ureteral stones are at risk of developing sepsis.
Materials and Methods
Data collection
This study was approved by our Institutional Review Board (AAAS6647). We conducted a retrospective review of patients between January 2010 and December 2019 who were diagnosed as having ureteral stones on CT in the ED and discharged from that index encounter without surgical intervention.
We searched radiology reports using the M*Modal Catalyst application (MModal, Inc., Franklin, TN) to identify patients who had a CT report in the ED containing at least one of the following phrases: “ureteral stone(s),” “ureteral calculus/calculi,” “forniceal rupture,” “impacted stone(s),” “impacted calculus/calculi,” “obstructing stone(s),” “obstructing calculus/calculi,” or “obstructive pyelonephritis.”
These reports were individually reviewed to determine whether a ureteral stone was present. We excluded patients who were admitted from the ED, had bilateral ureteral obstruction, were below 18 years of age, or did not have a complete blood count and urinalysis during their ED visit. Patients with renal stones in addition to ureteral stones were eligible for inclusion.
We reviewed each patient's medical record for demographic characteristics, laboratory results, CT reports, antibiotic usage, and subsequent procedures within 30 days of the index encounter. For patients who underwent subsequent procedures, we reviewed inpatient notes and operative reports to determine the indication for these procedures.
Primary outcome
The primary outcome was sepsis requiring decompression with a ureteral stent or nephrostomy within 30 days of the index encounter. Sepsis was defined as temperature ≥38°C or <36°C with at least one of the following additional features: heart rate ≥90 beats per minute, leukocytosis >12,000/mm3, or leukopenia <4000/mm3.
Patients with tachycardia and leukocytosis/leukopenia, but no fever, were not considered to have sepsis as these signs are common and often attributable to noninfectious causes in patients with stones.
Statistical methods and variable selection
Chi-square and Wilcoxon rank-sum tests were used to compare demographic, laboratory, and radiographic characteristics from the index visit between patients with and without subsequent sepsis. We used multivariable logistic regression to identify variables associated with sepsis. We selected variables to include in the analysis based on existing literature and data that were readily available in this patient population.
The demographic factors selected were age, gender, and diabetes mellitus, which are recognized risk factors for urinary tract infection. 11,12,18 –20 The radiographic variables selected were hydronephrosis, perinephric fat stranding, stone size, and location, all of which have been found to be associated with infection. 13,18,21 Hydronephrosis was graded as mild, moderate, or severe. In cases where no hydronephrosis grade was reported, the images were graded by an attending radiologist (H.S.).
The laboratory variables included were urine white blood cells (WBCs), urine nitrite, and leukocytosis, all of which have been shown to be associated with infection in patients with stones. 12 –14,18,22 Urine culture was not included in the model because culture results are not typically available in the ED setting, but rates of sepsis were compared between patients with positive and negative urine cultures. Positive urine culture was defined as growth of ≥10,000 colony-forming units per milliliter.
After constructing an initial multivariable model to predict sepsis, we performed backward stepwise regression using a t-statistic criterion with a threshold p-value of 0.05, resulting in the final model. We then calculated the area under the curve (AUC) using 10-fold internal cross-validation. After developing the final model, we used the variables to develop a predictive nomogram based on coefficients of the logistic function 23 ; p-values <0.05 were considered statistically significant. Stata 12.1 (StataCorp, College Station, TX) was used for the analysis.
Results
Patient characteristics and infection rates
We identified 3254 patients to assess for eligibility based on CT reports (Fig. 1). Of these, we identified 1331 patients with ureteral stones who met criteria for inclusion. Demographic information, laboratory results, and radiographic findings are displayed in Table 1. Sepsis requiring urgent decompression was identified in 22 patients (2%) and 2 patients required transfer to the intensive care unit.
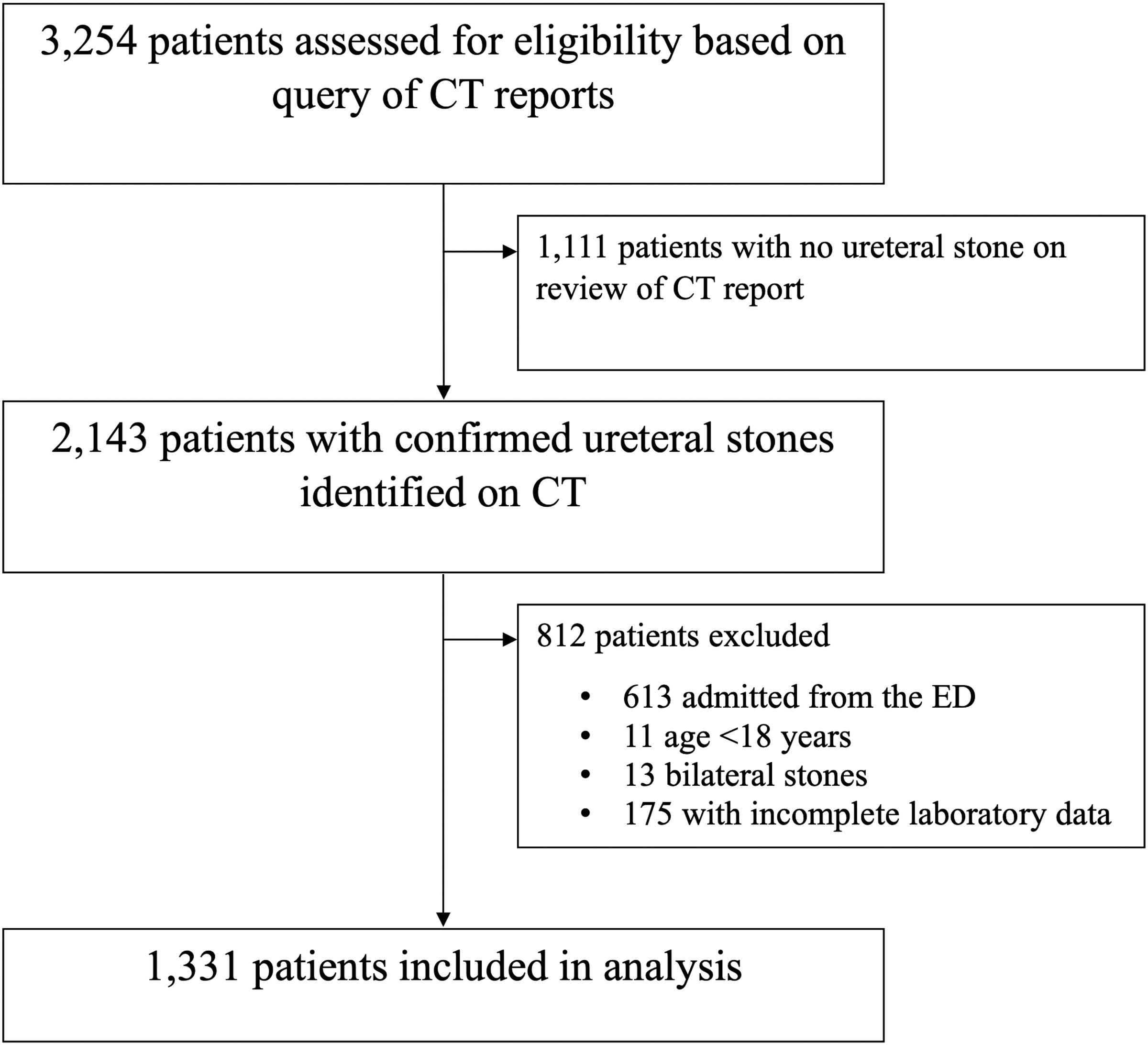
Flowchart of patients assessed for eligibility.
Demographic, Laboratory, and Imaging Characteristics
Statistical testing between sepsis and no sepsis groups using Wilcoxon rank-sum tests for continuous variables and chi-square tests for categorical variables.
HPF = high-power field; IQR = interquartile ratio; WBCs = white blood cells.
Multivariable logistic regression
The initial multivariable logistic regression model showed that female gender (odds ratio [OR]: 2.82, 95% confidence interval [CI]: 1.05–7.57, p = 0.039) and urine WBCs (OR: 1.02 per cell count, 95% CI: 1.01–1.04, p < 0.001) were independently associated with subsequent sepsis (Table 2). The initial model predicted sepsis with an AUC of 0.77.
Multivariable Logistic Regression Models for Predicting Sepsis and Positive Urine Culture
The initial model includes all variables listed. The final model was reached by performing backward stepwise regression on the initial model using a p-value threshold of 0.05. CIs and p-values are only reported for the initial model as they are not reliably interpretable following stepwise regression.
CI = confidence interval; OR = odds ratio.
Backward stepwise regression resulted in the final model, with three variables associated with infection: female gender (OR: 3.06), urine WBCs (OR: 1.02 per cell count), and leukocytosis (OR: 3.54). The final model predicted sepsis with an AUC of 0.79.
Applying the model
The sensitivity and specificity when retroactively applying the model with different thresholds are shown in Table 3. Using the coefficients from the final logistic model, we created a predictive nomogram to evaluate the risk of sepsis (Fig. 2). Each variable in the nomogram is given a score, and the probability of developing sepsis is calculated based on the sum of scores for each variable.

Predictive nomogram for estimating the probability of sepsis. Each variable in the nomogram is given a score, and the probability of sepsis is calculated based on the sum of scores for each variable. WBCs = white blood cells.
Predictive Ability of the Final Model When Retroactively Applied to the Study Sample, Using Different Thresholds for Determining Intervention Based on the Probability of Sepsis
Sensitivity and specificity are reported for each specified threshold.
A decision tree analysis for early intervention vs no intervention based on this nomogram, using a 5% threshold probability of sepsis as a criterion for early intervention, is shown in Figure 3. Urologic consultation during the index encounter was obtained for 23 (31%) of the 75 patients with at least 5% probability of sepsis.
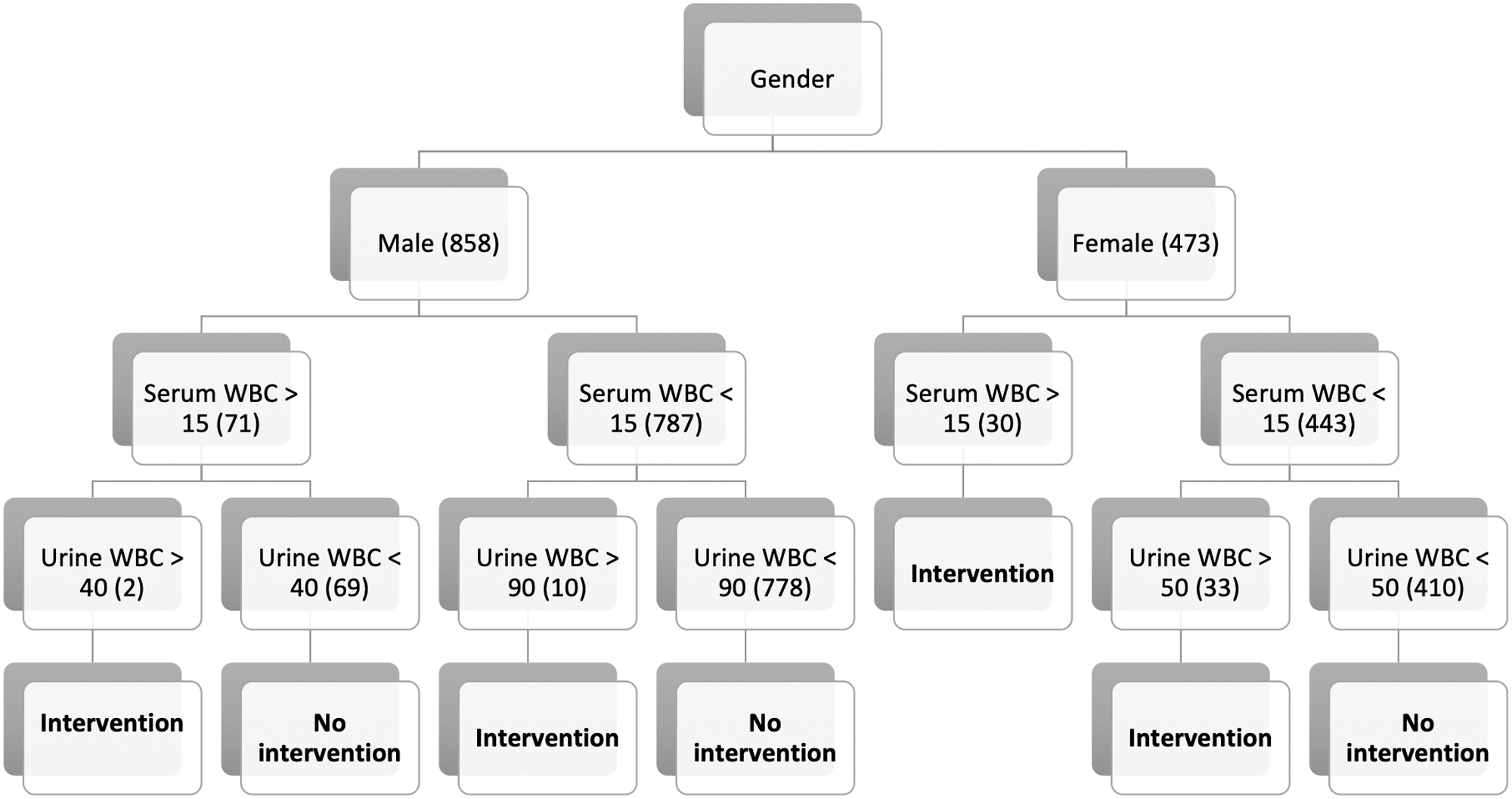
Decision tree analysis for intervention vs no intervention, using the logistic model with a 5% threshold for intervention based on probability of sepsis. Urine WBC thresholds are rounded to the nearest 10 cells/HPF for simplicity in interpretation. Numbers in parentheses represent the number of patients in our study sample who corresponded to each step in the pathway. HPF = high-power field.
Urine culture
Of the 810 patients with urine cultures sent from the ED, 66 (8%) had positive urine cultures (Table 4). Of patients with positive cultures, 6/66 (9%) developed sepsis, compared with 5/744 patients (1%) with negative cultures and 11/521 patients (2%) with no culture results (p < 0.001). The most common organism seen in the patients who developed sepsis was Escherichia coli (four patients).
Urine Culture Results Among the 66 Patients with Positive Cultures and the Subset of 6 Patients with Positive Cultures Who Developed Sepsis
Antibiotic usage
Data on antibiotic usage were available for all patients starting in December 2010 (n = 1188). Of these patients, 35 (3%) were prescribed antibiotics before the index ED encounter and 133 (11%) were discharged from the ED with antibiotics. The median duration of antibiotics prescribed in the ED was 7 days (range 3–14), and the majority received cephalosporins (72 patients) or fluoroquinolones (44 patients).
After controlling for gender, urine WBCs, and leukocytosis, antibiotic usage was not protective against sepsis in the overall cohort (OR: 1.66, 95% CI: 0.59–4.61, p = 0.335) or in the subgroup of 63 patients with positive urine cultures (OR: 0.82, 95% CI: 0.14–5.01, p = 0.833).
Discussion
In our cohort of patients discharged from the ED after diagnosis of an obstructing ureteral stone, we found that female gender and elevated urine WBCs are independent predictors of subsequent sepsis requiring urgent decompression. We did not find any radiologic characteristics predictive of sepsis in this cohort. Sepsis was a rare complication, and antibiotic usage was not protective against sepsis.
Our nomogram is easy to use and can provide useful clinical guidance for physicians and patients regarding the choice between early intervention and trial of stone passage. Using the nomogram with a 5% threshold probability of sepsis as a criterion for intervention would have led to early intervention for over one-third of the septic patients in our cohort, while also intervening on a modest 5% of noninfected patients. We should note that these estimates are optimistic given that the nomogram is being retroactively applied to the data from which they were derived. However, the model had a fairly high internally cross-validated AUC, suggesting its validity across the entire data set. Certainly, this would benefit from future external validation, but it nonetheless provides a useful clinical framework.
We found that female gender and elevated urine WBCs are independently associated with sepsis. These factors have been shown in prior studies to be predictive of infection in patients with ureteral stones, although they have not previously been integrated into a single predictive model. 11 –14,18 As demonstrated by the nomogram and decision tree analysis, we would recommend a lower urine WBC threshold for considering intervention in women, compared with men.
The other variable in our predictive model was leukocytosis, which met the p-value threshold for inclusion. Leukocytosis can be a useful clinical marker, particularly in cases with high-grade ureteral obstruction where the urinalysis may be falsely negative. Although it did not meet statistical significance in the initial multivariable model, leukocytosis should be incorporated into the clinical algorithm when evaluating patients with ureteral stones.
Nitrite is a widely recognized marker for infection, but we did not find a strong association in this study. This can likely be attributed to the low rate of nitrite positivity, resulting in a wide CI in the model. Most patients with urine nitrite and ureteral stones at our institution are admitted to the hospital and were thus excluded from this study. Additionally, patients with stones have a high prevalence of gross hematuria, which may cause nitrite to be falsely positive, reducing its predictive value. Despite the lack of statistical significance, we would recommend caution when discharging a patient with urine nitrite in the setting of a ureteral stone.
Urine culture was not included in our model because the results are typically not available in the ED setting, so it cannot be incorporated into decision-making algorithms. However, we did find that patients with positive urine cultures had a significantly higher risk of developing sepsis (9%) than those who had negative urine cultures (1%). In cases where patients do have urine culture results available in the ED, we would consider early intervention to mitigate the risk of sepsis, particularly when E. coli is the offending organism.
Implications
This is the largest study to examine risk factors for sepsis in patients with obstructing ureteral stones and it is the first study to do so in patients undergoing trial of passage. The largest previously published studies of infection risk in this patient population included fewer than 400 patients; these studies included patients with overt infection at their index visit, representing a higher-risk cohort than our study. 12,14
Larger studies investigating early stone intervention did not focus on infection risk. 24,25 Thus, in the absence of absolute indications for decompression, the choice between trial of passage and early intervention has been poorly defined. This study offers specific criteria to help physicians identify higher-risk patients to improve clinical decision-making.
While our model can help identify patients at risk of sepsis, it does not offer clear guidance on how to manage the higher-risk patients. Management options for these patients include early decompression, inpatient observation, close outpatient monitoring, and antibiotic treatment. Early decompression would likely prevent sepsis in some patients, potentially averting severe illness and death, but it would cause unnecessary morbidity in others. As there is currently no strong evidence on the best management strategy for these patients, we encourage shared decision-making based on risk factors and risk tolerance.
Certainly, higher-risk patients who do not undergo early decompression should be managed with an increased index of suspicion for worsening infection. This predictive model is best used as a tool to inform shared decision-making regarding these risks. It can also be used to help refine criteria for urologic consultation in the ED; only 31% of higher-risk patients in our cohort received urologic consultation, which is a prerequisite for informed decisions about stone management.
There are a few points worth emphasizing regarding the utilization of this model. The first is that it is designed for use in patients without clinical evidence of infection. This should not supersede clinical judgment, and patients with signs of infection warrant early decompression regardless of laboratory findings. The second point is that this model is intended as a clinical aid to guide management decisions and patient counseling; it is not a definitive diagnostic tool and is limited in its predictive capacity. Third, the model is intended for use in the ED; its applicability to the outpatient setting is unclear as these patients are often seen several days following urine collection, allowing additional time for infection signs to present.
Limitations
This study has several limitations, the first being its single-institution retrospective design without external validation. Second, the low rate of sepsis leaves the model susceptible to overfitting and potentially overly reactive to minor fluctuations in data. Third, we defined sepsis using the systemic inflammatory response syndrome criteria rather than the more contemporary Sequential Organ Failure Assessment score; although the latter score is generally preferred, it requires data that were not consistently available in the medical record, prohibiting its use in this study. 26,27
Additionally, we chose to identify patients using radiology reports rather than diagnosis codes to avoid biases associated with inconsistent coding practices in the ED; however, this method likely resulted in missing patients whose radiology reports did not include one of the specified phrases. Finally, we limited the study to patients who underwent CT to evaluate radiographic variables; as such, we excluded patients whose disease was diagnosed using other imaging modalities.
Despite these limitations, our findings offer a practical guide for clinicians to assess the risk of sepsis among patients with ureteral stones undergoing trial of stone passage. We use readily available data to help select patients for early intervention vs conservative management. Future research should attempt to externally validate these findings to optimize clinical protocols.
Conclusions
Sepsis is a rare complication among patients with ureteral stones selected for conservative management. The presence of elevated urine WBCs and female gender can help identify patients who are at risk of developing sepsis. Patients with risk factors should be managed with an increased index of suspicion for infection and may benefit from early intervention to reduce the risk of sepsis. Sepsis is more common in patients with positive urine cultures.
Footnotes
Authors' Contributions
E.J.M. was involved in conception of the study, acquisition of data, analysis of data, drafting the manuscript, and revising the manuscript. B.K.W. and M.M. were involved in acquisition of data, analysis of data, and revising the manuscript. C.H.M. was involved in analysis of data and revising the manuscript. H.S., R.G., C.B.A., and O.S. were involved in conception of the study and revising the manuscript. M.J.K. was involved in conception of the study, acquisition of data, and revising the manuscript. All authors have given final approval of the version to be published and agree to be accountable for all aspects of the work.
Acknowledgment
The authors would like to acknowledge Jussara Barone for her help with data acquisition for this study.
Author Disclosure Statement
E.J.M., B.K.W., M.M., C.H.M., H.S., R.G., M.J.K., and C.B.A. have no disclosures to declare. O.S. has worked for Boston Scientific (advisory board and lecturer), Coloplast (advisory board and lecturer), and Ambu (advisory board).
Funding Information
No funding was received for this article.