
Abstract
Purpose:
Lower urinary tract symptoms among adult men can significantly impact quality of life. We evaluated complications based on prostate size following plasmakinetic enucleation of the prostate.
Materials and Methods:
Patients were grouped into the small prostate group (SPG, <75 g) and large prostate group (LPG, >75 g) based on preoperative imaging. Patient data on demographics, comorbidities, preoperative international prostate symptom score (IPSS), bother index (BI), prostate-specific antigen (PSA) if indicated, postvoid residual volume (PVR), indwelling catheter or self-catheterization status, and any prior surgical intervention were evaluated. Postoperative IPSS, BI, and PVR values were assessed at 6 weeks, 4 months, and yearly. Postoperative urge urinary incontinence (UUI), stress urinary incontinence (SUI), and pad use were assessed.
Results:
Between September 2015 and December 2020, 296 patients who underwent bipolar enucleation with minimum follow-up of 4 months were evaluated. Postoperative IPSS, BI, PVR, and PSA values at all time points were significantly decreased compared with preoperative values (p < 0.05). There was no significant difference in the complications between groups. Univariable and multivariable analysis found that size <75 g was predictive of stricture formation and bladder neck contracture (BNC). UUI was more common at 6 weeks in the SPG, and SUI was more common at 6 weeks in the LPG, but no difference was noted at the 4-month and 1-year time points. Pad use was equal between the two groups at all time points.
Conclusions:
Plasmakinetic enucleation of the prostate provides an effective treatment option for prostates of all sizes; however, prostates <75 g have a higher rate of BNC and urethral strictures compared with those >75 g.
Introduction
Lower urinary tract symptoms (LUTS) are common among adult men and can significantly impact quality of life. 1 Most guidelines recommend medical therapy for first-line management, reserving surgery for refractory cases or contraindications to medical management. 2 For larger prostates, transurethral resection of the prostate (TURP) and open simple prostatectomy (OSP) have long been mainstays of surgical therapy, with robot simple prostatectomy gaining popularity. 2
Anatomic endoscopic enucleation of the prostate (AEEP) has gained popularity in the treatment of enlarged prostates. The concept is to take advantage of the surgical plane that exists between an enlarged obstructing adenoma and the capsule of the prostate and remove 100% of the obstructing tissue as in OSP. Compared with OSP, AEEP has lower transfusion rates, shorter hospitalization times, and shorter catheterization times. 3 The first report on AEEP was by Hiraoka and Akimoto, who documented 200 cases of transurethral enucleation of the prostate in 1989. 4 Despite clear advantages of AEEP over OSP, this technique was not widely adopted. Ten years later, holmium laser enucleation of the prostate (HoLEP) was introduced. The principles of dissection were similar to those first described using monopolar energy, instead of using a laser to develop the surgical plane. 5,6 While HoLEP was widely admired, the need for special equipment and a steep learning curve limited widespread adoption. 7 –9 Nevertheless, HoLEP proponents now view it as the new gold standard. 10
In 2006, Neil and colleagues proposed the first use of transurethral plasmakinetic enucleation of the prostate (PKEP) as an alternative to HoLEP for prostates greater than 30 mL. 6 PKEP boasts a shorter learning curve than HoLEP and the ability to convert to a traditional TURP if needed. Additional advantages include ubiquitous availability of necessary equipment and surgeon familiarity with the instrumentation. Efficacy and efficiency of PKEP have been well established compared with OSP, HoLEP, and TURP. 11 –14 While morbidities appear to be similar for PKEP compared with TURP 14 and HoLEP, 13 less is known regarding patient factors influencing complications for PKEP. Because PKEP is indicated for prostates of any size, we need a better understanding of how prostate size affects PKEP complication rates. In this study, we evaluate the complications of PKEP based on prostate size in our single-institution experience. We hypothesize that bladder neck contracture (BNC) will be higher in patients with smaller prostates and stress urinary incontinence (SUI) will be higher in patients with larger prostates.
Materials and Methods
An IRB-approved retrospective review was performed on a database for patients undergoing PKEP by a single surgeon. Patients with a minimum follow-up of 4 months were included in the analysis. Patients were grouped into the small prostate group (SPG, <75 g) and large prostate group (LPG, ≥75 g) based on preoperative imaging. Patient data on demographics, comorbidities, preoperative international prostate symptom score (IPSS), bother index (BI), prostate-specific antigen (PSA) if indicated, postvoid residual volume (PVR), indwelling catheter or self-catheterization status, and any prior surgical intervention were evaluated. All patients underwent preoperative size assessment by ultrasound. All patients had a preoperative cystoscopy unless they had recently had a catheter placed without issue. Operative time, blood loss, pathology weight, cancer incidence, <90-day complications, and ≥90-day complications were assessed.
The surgical technique has been previously described. 15 In the immediate postoperative course, patients had their catheters removed on day 1 after the surgery; if the catheter had to be left in for more than one day, this was included as a grade 1 complication. Postoperatively, IPSS, BI, and PVR were assessed at 6 weeks, 4 months, and yearly. In addition, at each postoperative time point, patients were asked “Do you have any degree of leakage associated with physical activity?” (SUI); “Do you leak urine with a strong urge to urinate or leak urine on the way to the bathroom?” (urge urinary incontinence, UUI); and finally, “Are you currently using any pads or diapers because of urinary leakage?” PSA was assessed at 4 months and then yearly.
Statistical methods
Patient demographics and operative findings are summarized using frequency and percentage for categorical data and median and interquartile range for continuous fields. Results were compared across the SPG and LPG, using the chi-square test for discrete variables and the Wilcoxon rank-sum test for continuous data. Univariable and multivariable logistic regression models were used to identify clinical and surgical parameters predictive of stricture. A threshold of 0.05 was used for significance. SAS 9.4 (SAS Institute, Cary, NC) was used to conduct analyses and to generate figures.
Results
Between September 2015 and December 2020, 320 patients underwent bipolar enucleation. Of that population, 296 had minimum follow-up of 4 months and were included in the evaluation. Eighty patients in the SPG and 50 patients in the LPG were seen at 1 year.
Table 1 summarizes patient demographics and operative findings. Figures 1 and 2 demonstrate the IPSS, BI, and PVR at all time points. At all postoperative time points, IPSS, BI, PVR, and PSA values were significantly decreased compared with preoperative values (p < 0.05). PSA level was 2.9 ng/dL and 6.3 (p < 0.01) preoperatively, 0.88 and 1.2 (p 0.1) at 4 months, and 1.5 and 1.5 (p = 0.88) at 1 year in the SPG and LPG, respectively. At the 4-month and 1-year follow-ups, IPSSs and BIs were significantly higher in the SPG compared with LPG (p < 0.05). Preoperative retention rates were equal between the two groups, and no patients remained in retention at last follow-up. Cancer was more commonly identified in the SPG.

International prostate symptom score and bother index over time. Color images are available online.
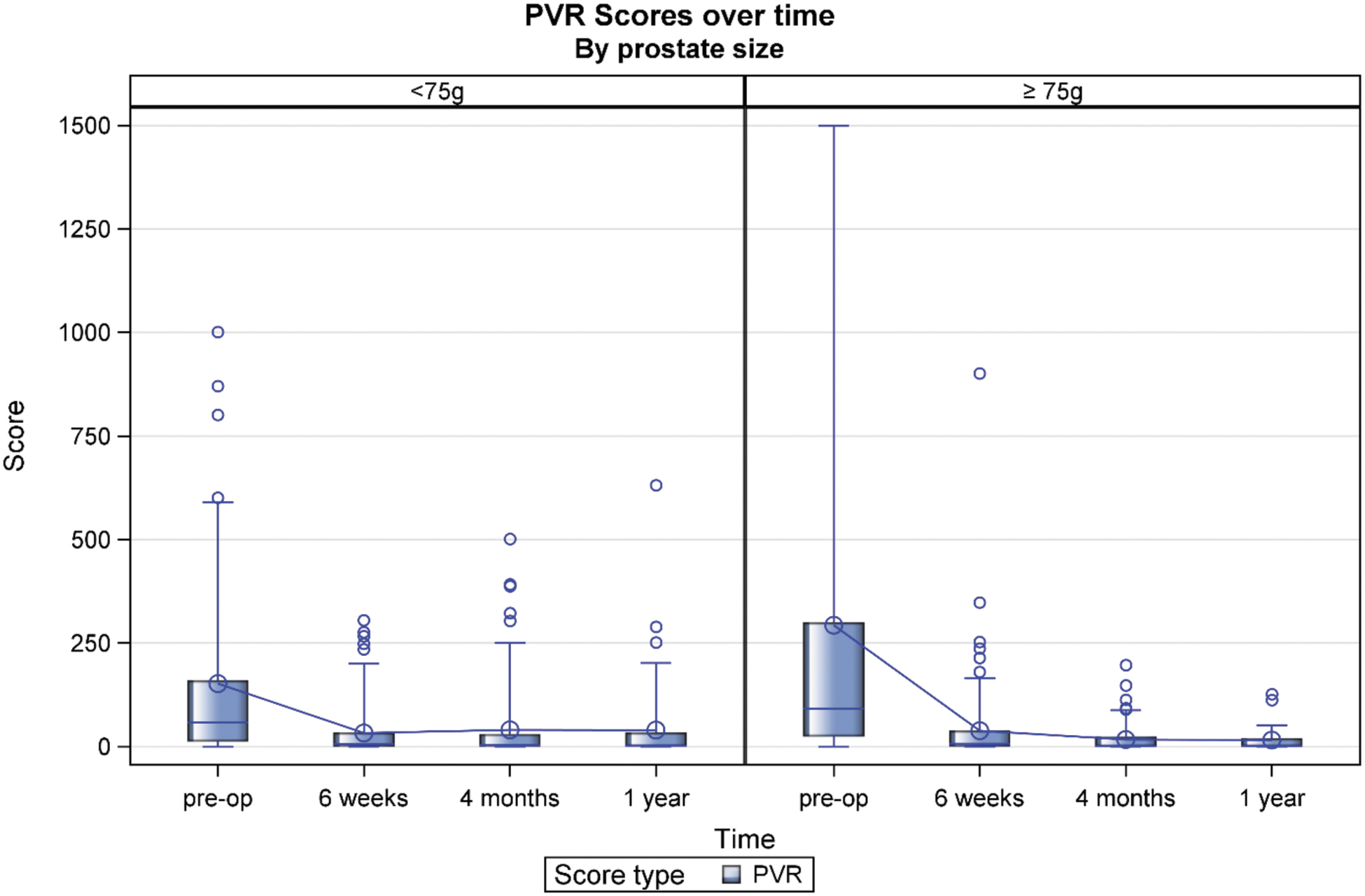
Postvoid residual volume over time. Color images are available online.
Patient Demographics and Operative Findings Based on Prostate Size
The bold values indicate statistical significance.
PSA = prostate-specific antigen.
Table 2 summarizes the incontinence and pad use data. Self-reported episodes of UUI were higher in the SPG, but only at the 6-week time point (p < 0.5), and the rate of SUI was significantly higher in the LPG. By 4 months, there was no significant difference in rates of SUI or UUI. Pad use was equal at all time points. At 1 year, 5/130 (3.8%) patients had pad use. One patient had undergone an anti-incontinence procedure.
Incontinence and Pad Use
Table 3 summarizes the complications. Two patients in the LPG died of myocardial infarction within the 90-day postoperative period and were not included in the final evaluation. There was no significant difference in Clavien-Dindo complication rates between the groups. BNC only occurred in the SPG, and strictures were more common in the SPG. On multivariable analysis, including age, diabetes, body mass index (BMI), prior surgery, and transrectal ultrasound (TRUS) volume, only TRUS volume <75 g was predictive of stricture formation; OR 10.6 (1.35, 84.3). Meanwhile, BMI (≥30), prior prostate surgery, and TRUS volume <75 g were predictive of BNC; ORs 8.40 (2.32, 30.4), 4.64 (1.17, 18.5), and >999.9 (<0.01, 999.9), respectively. Odds ratio for TRUS volume was inestimable as all the BNC occurred in the SPG.
Complications
BNC = bladder neck contracture.
Table 4 shows changes in IPSS, BI, PVR, and PSA levels. Univariate analysis and multivariate analysis for prediction of incidence of stricture and BNC can be seen in Tables 5 and 6, respectively.
Changes in International Prostate Symptom Score, Bother Index, Postvoid Residual Volume, and Prostate-Specific Antigen Level
Bold values indicate statistical significance.
Univariable and Multivariable Logistic Regression for Prediction of Incidence of Stricture
CL = confidence level; TRUS = transrectal ultrasound.
Univariable and Multivariable Logistic Regression for Prediction of Incidence of Bladder Neck Contracture
NC = not calculable.
Discussion
In this study, we have examined bipolar enucleation of the prostate as a function of size. In our series, all BNC and most urethral strictures occurred in patients with smaller (<75 g) prostates (SPG). The SPG patients also have worse postoperative symptoms, reporting higher postoperative IPSSs and BIs at the 4-month and 1-year postop time points. While SUI rates are higher in patients with larger prostates, UUI is higher in patients with smaller prostates, with differences equilibrating by the 4-month and 1-year time points.
Bladder neck contracture
BNC occurred exclusively in the SPG. Similar BNC rates have been reported for HoLEP in patients with smaller prostates. 16,17 Multivariate analysis demonstrated that prior surgery was an additional risk factor for BNC in our series. We have adapted in several ways to this finding. First, if someone has significant LUTS and failed medical therapy, we will offer a minimally invasive option rather than an enucleation. We have adopted the adage “small prostates deserve small operations.” The exception is for patients with a high preoperative PVR (>500 mL) or who are in retention preoperatively. We accept that patients with small prostates in retention may experience a higher rate of BNC after PKEP, but have a higher chance of being able to urinate after PKEP compared with minimally invasive therapies. All of our patients in retention were able to urinate at last follow-up, which is similar to the HoLEP experience. 18,19 This is notably superior to outcomes for patients in retention when compared with other modalities used to treat small prostates, including prostatic urethral lift and vapor therapy, which boast 86% and 70% respective rates of voiding. 20,21
We have developed a few strategies to optimize bladder neck integrity. For instance, in a reoperative field, we pay close attention to the bladder neck. If the bladder neck is widely patent and has a normal mucosal appearance, we will avoid any resection at the bladder neck and focus on the apex and mid-section of the adenoma. If there is any suggestion of bladder neck narrowing, we will perform full enucleation and endoscopic bladder neck advancement with good outcomes. 22
Why the smaller prostates tend to develop more BNC has not been well studied. In our opinion, the large prostate tends to stretch the bladder neck fibers to a wider caliber. We suspect that even a large bladder neck will have some degree of scar formation, but will not become so narrow that it limits flow as it will in a smaller prostate with a smaller caliber bladder neck. In the HoLEP literature, there have been studies that evaluated the rate of BNC based on prostate size and saw no difference. 23 It is possible that with the laser, there is less thermal effect on the bladder neck, and the overall scar rates are lower. However, several authors have found a correlation between smaller prostate size and increased rates of BNC in HoLEP. 16,24 Krambeck and colleagues favor bladder neck-relaxing incisions in smaller prostates in an effort to prevent BNC (23234620). We too have adopted this into practice, yet the rates of BNC remain higher in smaller prostates.
Strictures
Anecdotally, men with smaller urethras will have onset of LUTS despite smaller prostatic size. In this series, the rate of urethral strictures is also higher in men with smaller prostates, 6.8% vs 0.7%. We have made several attempts to minimize the risk of strictures. As stated previously, using minimally invasive therapies, such as Rezum or urethral lifts, for smaller prostates is one way to avoid larger resectoscopes. Most of these minimally invasive therapies use a narrowed sheath. If we perform enucleation, we use intermittent flow, 24F resectoscope, and leave an 18F three-way catheter postoperatively. Some studies have speculated that longer operative times and bigger prostates lead to more risk of strictures. 25 This is thought to be due to the excess energy required during the resection of larger prostates. However, in enucleation, similar overall energy rates applied to the capsule despite the size of the prostate as the majority of the enucleation procedure is mechanical and not with energy.
Incontinence
We observed a high rate of SUI at 6 weeks; the high rate of SUI reflects the strict inclusion of any degree of leakage with activity. The corresponding pad or diaper use was relatively low at 10.8% and this fell to 5% by 4 months. Nearly 100 patients were lost to follow-up at 1 year in the LPG. We speculate that this is because our patients who are doing well at 4 months are offered follow-up as needed. Nevertheless, in patients who completed the 1-year follow-up, overall pad use was 3.8%. Large prostates have previously been shown to increase the risk of SUI in bipolar enucleation. 26 These values are comparable with HoLEP. In a series of 1476 patients, SUI occurred in 3.8% of patients after HoLEP. 27 In our entire series, only one patient has undergone an anti-incontinence procedure postoperatively. The significant improvement in BI in our entire cohort is further indication of patient satisfaction.
Urgency incontinence is less frequently reported upon, and in our anecdotal experience, patients in the LPG and SPG were more likely to wear a pad due to UUI rather than for the minimal drops of urine they experienced. In the SPG, IPSSs did not improve beyond the 4-month follow-up visit, and IPSSs were higher than in the LPG at all but the 6-week postoperative time point. It has thus now become our recommendation to initiate early dual bladder medical therapy, onabotulinum toxin injection, or sacral neuromodulation in the SPG population if the IPSS remains elevated at the 4-month follow-up. In these cases, we also rule out secondary BNC as a cause for persistent symptoms using cystoscopy.
International prostate symptom score
Prior studies have used urodynamic evaluation to show patients who are at risk for persistent storage symptoms after TURP. For example, Choi and colleagues demonstrated that poor contraction, small storage capacity, and high preoperative storage scores were associated with persistent elevation in storage symptoms postoperatively. 28 Meanwhile, Park and colleagues have shown that with HoLEP, patients with smaller prostates do not show improvement in the storage component of IPSS in the short-term follow-up. 16 We did not differentiate the IPSS into storage and voiding scores. However, anecdotally, strength of stream, intermittency, and incomplete emptying improve routinely, corroborated by improved PVR. Meanwhile, high frequency, urgency, and nocturia scores tend to be the last symptoms to improve. As mentioned above, we are now favoring minimally invasive therapies to minimize side effects in patients with smaller prostates and aggressively treating them with early bladder-targeted interventions.
Limitations
This is a retrospective review. We have a high dropout rate of patients after the 4-month follow-up, especially in the LPG, which likely falsely elevates the SUI rates at the 1-year time point. We do not divide IPSSs into storage and voiding scores. However, these data represent the largest analysis of bipolar enucleation cases, looking at complications specifically for prostate size. We anticipate subsequent follow-up to determine whether using smaller resectoscopes and ensuring mucosal advancement in reoperative cases will reduce the rate of BNC and urethral strictures. In addition, future analysis will incorporate pad use and type of incontinence to offer clarity on this association as well as focus on IPSSs divided by storage and voiding.
Conclusions
We report our single-surgeon series on complications of PKEP by prostate size. We identified that prostates <75 g have a higher rate of BNC and urethral strictures compared with those ≥75 g. At the 4-month and 1-year time points, the SPG had higher IPSSs and BIs compared with the LPG. SUI is higher in the early 6-week postoperative period in the LPG, but this difference disappears by the 4-month follow-up. Further studies will focus on the best means of prevention of strictures, BNC, and SUI during PKEP.
Footnotes
Authors' Contributions
J.N.W. conceived of the presented idea and supervised the project at all stages. N.H.R., M.P., and A.-P.S. performed the data collection as well as statistical analysis. A.M. and F.L.B. wrote the manuscript. All authors discussed and contributed to the final manuscript.
Ethical Approval
This study had IRB approval with associated ethics consent through the City of Hope Medical Center. This study was performed in accordance with the Declaration of Helsinki.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.