
Abstract
Introduction:
One of the most important problems in the supine percutaneous approach to the kidney is the narrow surgical surface area (SSA) in the lumbar region. Herein, the spatial and angular geometric advantages of the U-shaped lumbar pad (U-Pad) used as a new positioning tool for safety and ergonomics in the supine percutaneous approach have been revealed.
Materials and Methods:
Data of patients who underwent endoscopic combined intrarenal surgery (ECIRS) using the U-Pad for kidney stones between March and September 2021 were prospectively collected. The demographic, preoperative, operative, and postoperative data of patients have been saved. The patients were positioned first with the standard gel pad (group 1) and then with the U-Pad (group 2). Both SSA (X and X+Y, cm2) and angular degree (α and β,°) calculations were compared. Fluoroscopy images with the same settings (97 kV/3.00 mA) were visually compared. In geometric data, trapezoidal area formula [(upper base + lower base) × height/2] and goniometer were used to compare with paired t-test.
Results:
ECIRS was performed on 17 patients, 13 men and 4 women, with a median age of 39 (range 32–47). The median body mass index was 26.2 (23.5–29.1). Stone localization and features were recorded. The median SSA was calculated as 35.7 cm2 in group 1 and 97.3 cm2 in group 2, and it was calculated that the total SSA increased to 272.5% with a median of 61.6 cm2 extra surgical area. Similarly, the downward manipulation angle was 32° (α°) in group 1, whereas it was 60.6° (β°) in group 2, and the median extra motion angle was calculated as 28.6° (89.3%).
Conclusion:
The U-Pad is a safe and rapid tool in the supine percutaneous approach to the kidney, providing at least two times the extra SSA and manipulation angle.
Introduction
The position and angle of the area to be operated have great importance and can decide whether an operation is easy and/or effective in endourology. There have been many trials and improvement efforts for safety and ergonomics in the supine percutaneous approach to the kidney. In the process starting with Valdavia, various angles (0°–45°) were tried for patient flank elevation to enter the calix more accurately and to reduce visceral injury. 1 –6 In addition to these developments in flank positioning, the Valdavia position has been made suitable for retrograde interventions by Galdakao and the Galdakao-modified supine Valdivia (GMSV) position, which is routinely used in our clinic, has emerged. 7
To prevent bowel injury in supine percutaneous interventions, it is necessary to stay behind the posterior axillary line. The major disadvantage of the supine position is not only the limited flank surgical surface area (SSA) for kidney puncture but also the limitation of manipulation during the operation and the increased possibility of surgical failure and/or complication. Although it has been shown that stone-free and calix access is higher in the supine position than prone, manipulation is limited when looking at technical details and current practice. 8 Various manipulations and positionings have been made to reduce this relative limitation. 9 –11
In current practice, gel pads or 3 L of the saline bag placed in the dorsolumbar region provide the desired angle, but they limit manipulation. Although the patients are tried to be fixed with various adhesive tapes, patients or equipment can be moved across during the operation. These shifts make manipulation and surgery even more difficult in the relatively narrow supine lumbar SSA. To eliminate this problem, the U-shaped lumbar pad (U-Pad) is designed to expand the SSA in the flank region and to increase the manipulation and angles of surgical instruments. In this study, the spatial and angular advantages of the U-Pad were tried to be revealed with geometric data.
Materials and Methods
Data of patients who underwent endoscopic combined intrarenal surgery (ECIRS) using the U-Pad for kidney stones between March and September 2021 were prospectively collected. The study was approved by the local ethics committee (IRB approval number: 2021/169) and informed consent was obtained from all individual participants. The demographic, preoperative, operative, and postoperative data of patients have been saved. Kidney, ureter, and bladder radiograph was used to evaluate the stone-free rate (SFR) in the first month after surgery.
The SFR was defined as no residual stones of diameter >3 mm. Patients with any anatomical anomalies, comorbidities (American Society of Anesthesiologists [ASA] score >1), and obesity (body mass index [BMI] >30) were excluded from the study. The patients were positioned first with the standard gel pad (group 1) and then with the U-Pad (group 2) (Fig. 1A, B). The efficacy of the standard gel pad and the U-Pad was evaluated and compared preoperatively for the SSA and manipulation angles.
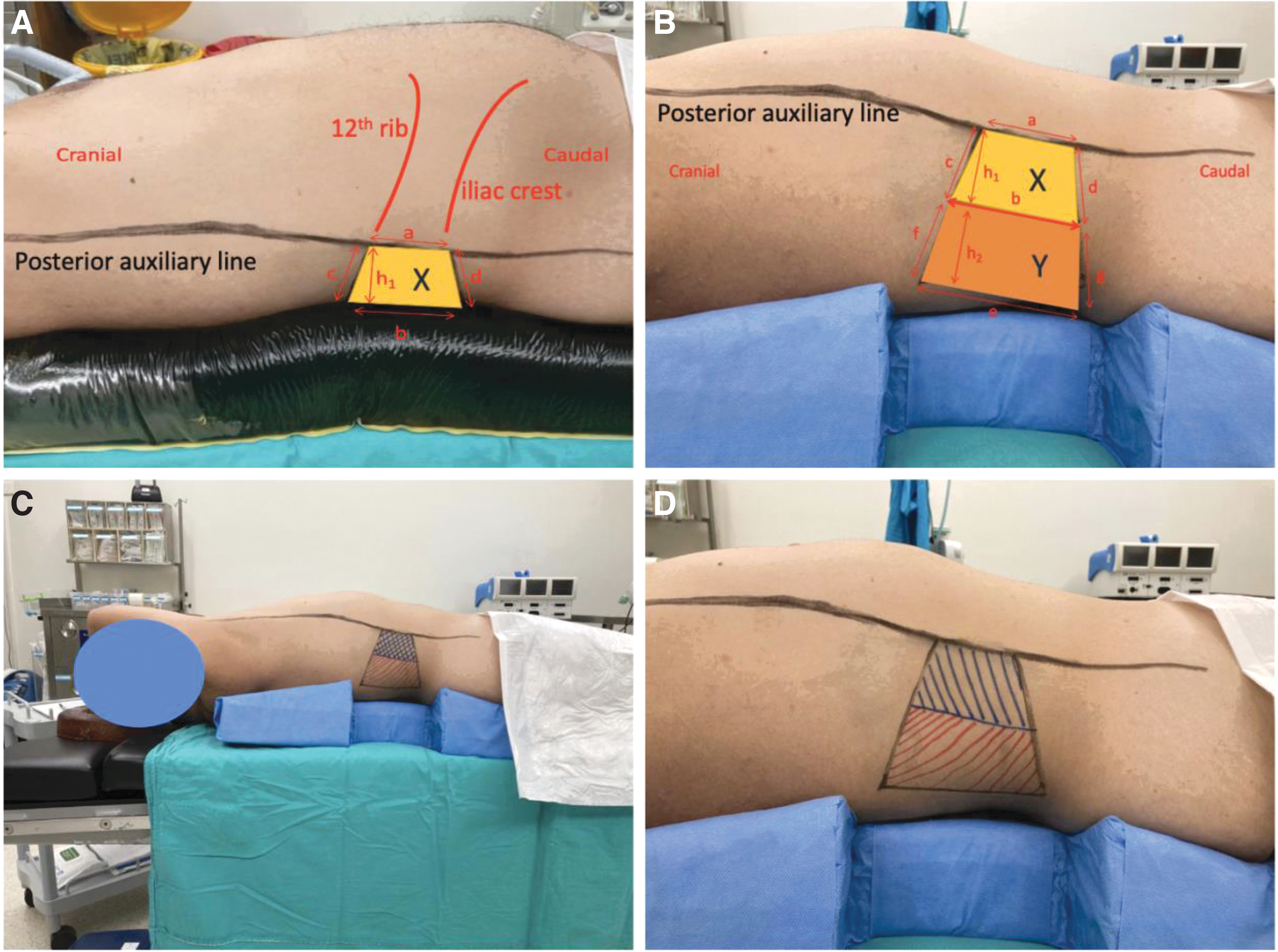
Patient position.
The U-Pad was designed to be suitable for the thoracolumbar and gluteal anatomy of the patients. It is made of rubber sponge material. It was cut in a vertical plane resembling a triangular prism (with an acute angle of 30°) and the middle part planned to come to the lumbar region was removed (Fig. 2A, B). Thus, a U shape is formed when viewed from above (Fig. 2C). The top and bottom sides were cut in a way that they gradually became thinner compared with the middle. In this way, the thoracic and sacrogluteal areas were less supported. In the supine position, the desired sub-concave space for the lumbar region was created safely and immobile without the need for any other equipment or fixation with tape (Fig. 1C, D). Subsequently, the possibility of getting wet and causing infection was eliminated by being wrapped with a waterproof operation cover.
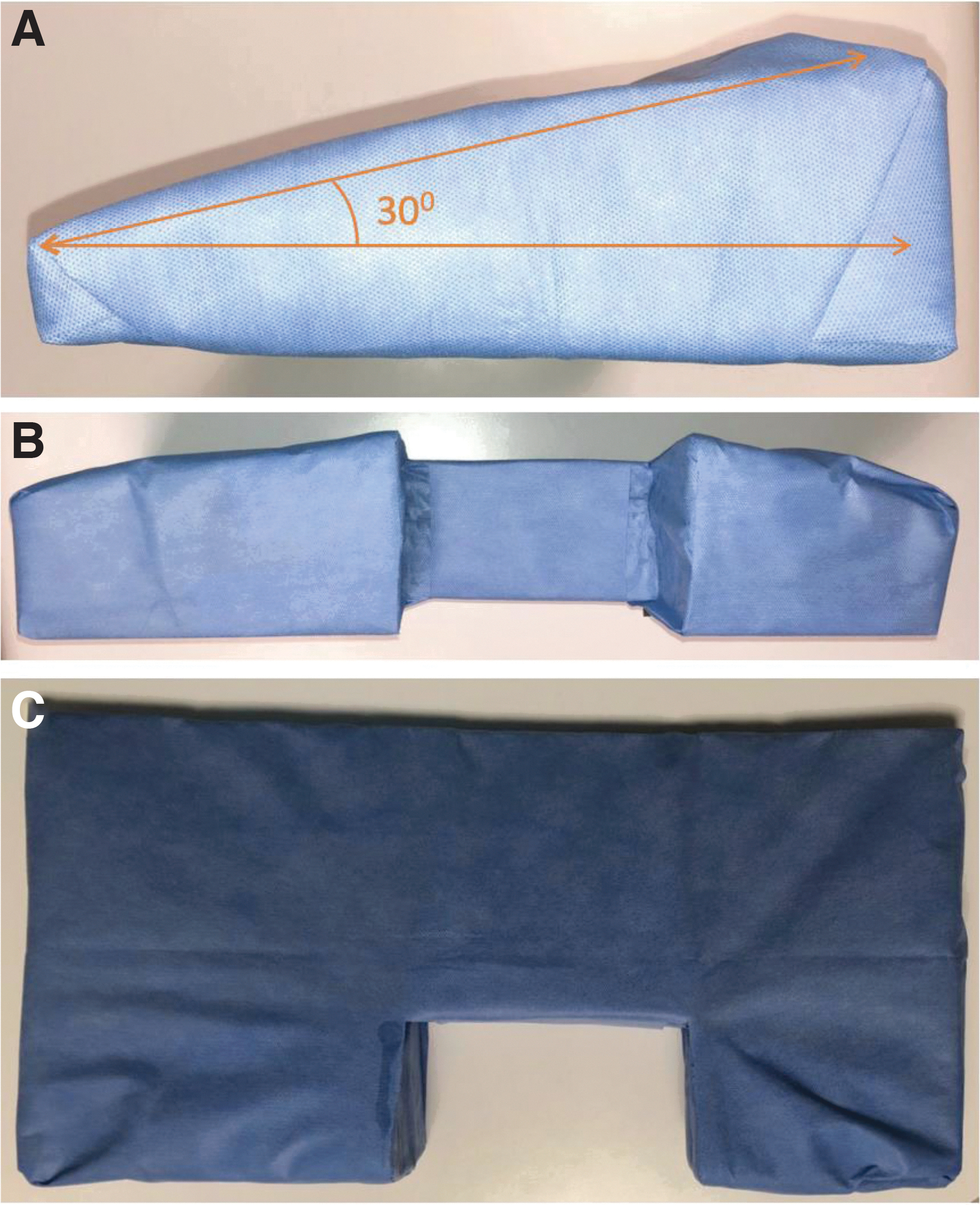
View of the U-Pad from various sides.
The trapezoidal access and manipulation area were defined as the safe area for supine percutaneous nephrolithotomy (PNL)/ECIRS in the lumbar region, between the posterior axillary line anteriorly, the 12th rib above, the iliac bone below, and the upper anterior surface of the pads used in the posterior (Fig. 1). Both SSA (X and X+Y, cm2) and angular degree (α and β,°) calculations were compared in group 1 and 2, respectively (Figs. 1 and 3) (Table 2). Fluoroscopy images of the standard gel pad and the U-Pad with the same settings (97 kV/3.00 mA) were visually compared (Fig. 3C, D).
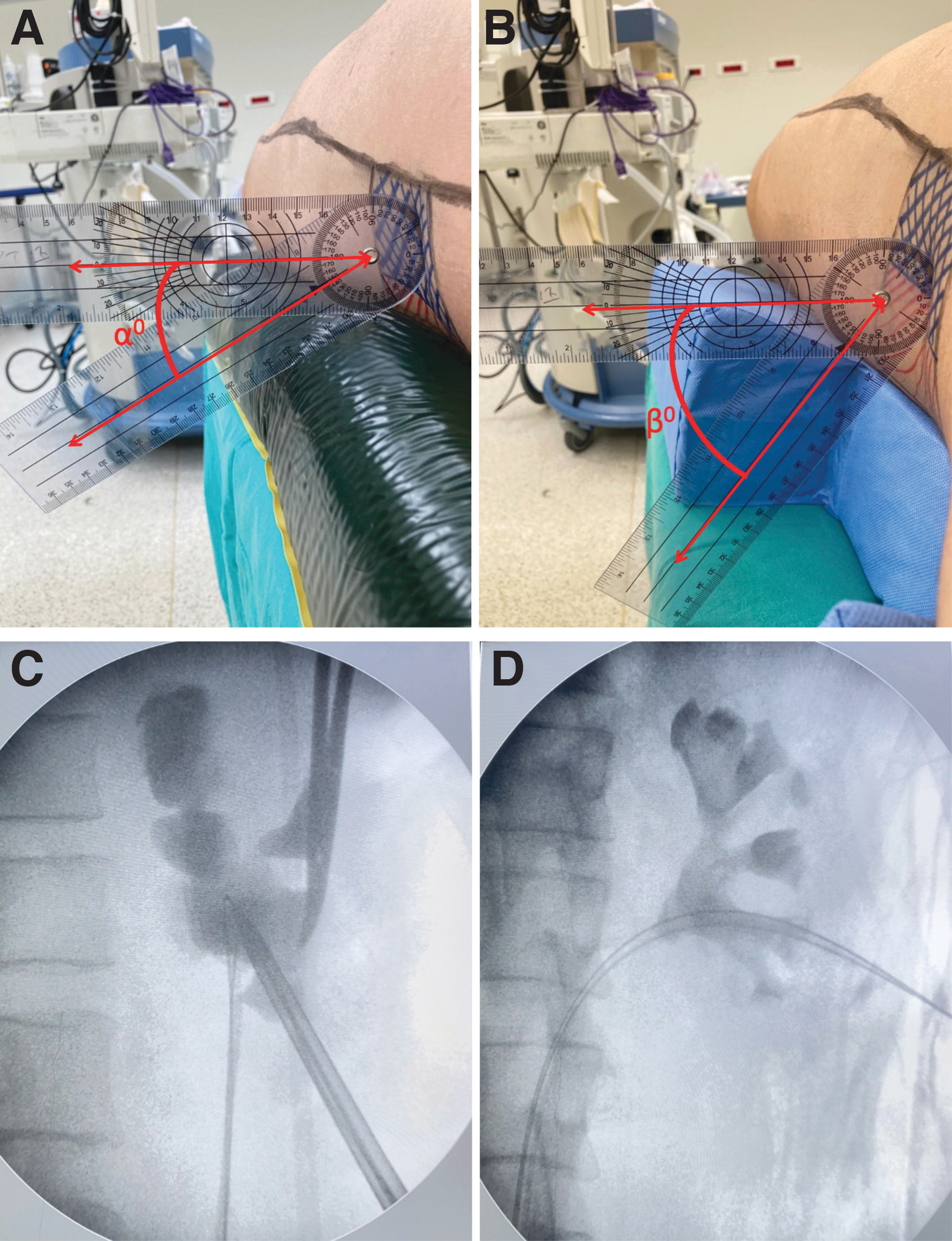
Downward manipulation angles (α° and β°) and fluoroscopy images with the same settings (97 kV/3.00 mA).
The data of the patients were measured demographically and geometrically. Microsoft Excel Office 2010 (Microsoft Corp., Washington) was used for demographic data. In geometric data, trapezoidal area formula [(upper base + lower base) × height/2] and goniometer were used. Paired t-test was used with SPSS version 22 (IBM, Armonk, NY) to compare in group 1 and 2.
Results
The demographic, preoperative, operative, and postoperative data of patients are shown in Table 1. ECIRS was performed on 17 patients, 13 men and 4 women, with a median age of 39 (range 32–47). General anesthesia was applied to all patients. The median BMI was 26.2 (23.5–29.1). The median stone size, volume, and density were 36 mm (20–60), 7320 mm3 (1150–17,987), and 1150 HU (910–1403), respectively. Two caliceal access was required in 2 patients. The median operation and fluoroscopy time, median hospital stay, and hemoglobin decrease were recorded as 96 minutes, 83 seconds, 4 days, and 1.6 g/dL, respectively. Transient postoperative fever was recorded in 1 patient, and SFR was calculated as 84.2%.
Demographic, Preoperative, Operative, and Postoperative Data of Patients Who Underwent Endoscopic Combined Intrarenal Surgery
The geometric and comparative data of group 1 and 2 are shown in Table 2. The median SSA was calculated as 35.7 cm2 in group 1 and 97.3 cm2 in group 2, and it was calculated that the total SSA increased to 272.5% with a median of 61.6 cm2 extra surgical area increase. Similarly, the downward manipulation angle was 32° (α°) in group 1, whereas it was 60.6° (β°) in group 2, and the median extra motion angle was calculated as 28.6° (89.3%). Visually, the U-Pad has a better fluoroscopy clearance than the standard gel pad (Fig. 3C, D).
Geometric and Comparative Data of Standard Gel Pad and U-Pad Group
∗p < 0.05 between standard gel pad and U-Pad in each group (paired t test).
Standard gel pad group is the reference group.
U-Pad = U-shaped lumbar pad.
Discussion
Considering the innovative developments in urology, as expected, the greatest advances have been experienced in endourology parallel with the technological developments in the past decades. The currently recommended modality for the treatment of large and complex kidney stones is PNL, and it has undergone various modifications over the years to both increase SFRs and minimize complications. 12
One of the most important of these changes was the miniaturization of tools and equipment. In this way, the trauma created in the kidney was minimized. Another development was the transition to the supine position. 1,13 This new position brought with it serious advantages in terms of being ideal for anesthesia, not wasting time and complication caused by repositioning and allowing simultaneous retrograde intervention. However, as expected, this new position caused certain hesitations among urologists and was not immediately accepted. The most feared of these hesitations was the risk of bowel injury.
Complication analysis and CT studies have shown that the supine position is at least as safe as the prone. 1,14 Although limited access to the upper pole, narrow space for multiple tracts, and a long learning curve is presented as other problems. Studies have shown that these concerns are unreasonable fears and surgeons with prone training can easily achieve supine PNL. 15 –17 Although there are other problems such as failure to perform simultaneous bilateral PNL, kidney hypermobility, longer percutaneous tract, and low intrarenal pressure. These deficiencies have been minimized with various maneuvers and modified equipment. 3,18
The supine approach allowed simultaneous bilateral endoscopic surgery (SBES) as well as ECIRS. Efforts to provide the ideal position have continued, both for the development of new techniques (ECIRS and SBES) and for solving the aforementioned problems. Confusion in the lower extremity position seems to be resolved with the GMSV position. However, the narrowness of the safe SSA behind the posterior axillary line in the lumbar region and the patient's shift to the opposite side makes it difficult to access the kidney (especially ultrasonic access), nephroscopic manipulation, and stone extraction. It is precisely because of this problem that the search for many positions has continued and has been tried.
The U-Pad has been designed for the supine percutaneous approach to minimize these restrictions in accordance with human dorsolumbar anatomy. One of the first positions used to remove these restrictions in the lumbar region is “The Barts Technique.” 10 Considering the details of this position, although sufficient space is obtained in the lumbar region, the patient is positioned relatively far from the surgeon toward the middle of the operating table. Renal anatomy becomes unusual because of the patient's torso being placed in a 90° position, and percutaneous access may be difficult. In addition, because the hemipelvis is positioned at 45°, it becomes more difficult to enter the ureter and retrograde flexible ureterorenoscopy.
Although the Barts flank-free-modified supine position aims to support the gluteus and chest, as in the U-Pad, the area in between collapses downward because of the lack of resistance of the saline or soft gel equipment used, the kidney becomes more mobile and, therefore, both angle loss (∼15°) also causes loss of space. 19 In the complete or modified complete supine position, the lower part of the patient is not supported by any equipment. Although these techniques seem safe and feasible, the narrow SSA and the difficulty in manipulation caused by angle loss are the limitations of these positions. 20,21 All these restrictions have been removed in the U-Pad. Extra-large SSA and angle of manipulation are achieved. Patients remain fixed in their current position. With its relatively high-concave segment in its middle part, the kidney and patient remain more stable than other positions.
Another physiologic manipulation in the supine approach is the “Double S” position. 9 A large dorsolumbar SSA was obtained, similar to the U-Pad. The effectiveness of the Double-S position and the experience of the surgical team revealed high success and low complications. 22 In this position, the patient's gluteal region is adjacent to the table. The ipsilateral thoracic region is supported by thick gel pads through a metal bar to position ∼35°. The patient's torso is relatively torsioned compared with the supine position, resembling the semiflank position.
The Montreal mattress and Proneview™ protective helmet system is inventive equipment designed for Prone PNL to minimize skeletal and anesthetic complications. 23 Although the search for new positions continues in the supine approach, no inventive equipment has been encountered except for routine equipment (gel pads, support tools, adhesive tapes, 3 L of the saline bags, etc.). In Giusti's supine position, a height of about 7 cm and an angle of 20° were obtained by using swim noodles. 18,24 However, no extra SSA increase was observed in the lumbar region. The U-Pad has increased this area ∼2.5 times. The 30° angle created in the horizontal plane provided the most appropriate angle for the kidney anatomy. In this way, both fluoroscopic and ultrasonic renal access can be performed easily and safely. Posteriorly, nephroscope and stone extraction were facilitated by the approximately twofold increased angle of manipulation.
Although preparations and planning are made for possible situations before the operation, some surprises are encountered in endourology. Migrated or encrusted stents, pelviureteral junction, or ureteral strictures are some of these, and a simultaneous antegrade approach may be required for the patient in the lithotomy position. In such difficult situations, the U-Pad can make the patient suitable for percutaneous intervention in a short time of about 5 minutes, safely and without difficulty in terms of anesthesia. In this respect, it seems much more feasible than routinely applied techniques. The extra-large SSA gained may not require the ipsilateral arm to be turned to the opposite side and a more controlled and safe position is obtained in terms of anesthesia and the airway.
In supine PNL, multiple renal access, upper pole access or reaching the upper calix through lower pole access was initially met with hesitation. Clinical and angle studies have shown that this concern is unfounded. 15,25 The extra SSA obtained with the U-Pad can also provide convenience in terms of upper pole and/or multiple access. The U-Pad provides this with the posterior extra surface area.
The area that is most exposed to pressure during the operations is the sacral region, and the others are the scapula and heels. 26 The U-Pad was designed in accordance with the thoracic and sacrogluteal anatomy of the patients, and in this way, the pressure on the sacral region was tried to be minimized. The stable and nonslip structure of the U-Pad allows the patient to be taken out of the operating table safely (5–10 cm) and the manipulation is made easier, almost as in the prone position. The U-Pad is designed from sponge material and the gel version is in the patent and production process.
Considering the operative and postoperative data, stone-free and complication results almost were compatible with the literature despite the small number of patients in this study. 27 In 2 patients, upper and lower calix access was required in addition to the lower and middle calix access. These extra calix accesses and manipulations were easily done using the U-Pad. In the routine 1-month evaluation, the SFR was determined as 84.2% and was interpreted as satisfactory. Although women gender seems to be at risk for sepsis and postoperative fever in PNL and other endoscopic stone surgeries, a postoperative transient fever was observed in 1 male patient in this study. 28,29 This complication can also be evaluated more objectively by increasing the number of patients with using the U-Pad.
Although PNL operations have been performed with fluoroscopy compatible operating tables in recent years, it is known that dense standard gel pads reduce the fluoroscopy image quality in practice. In this study, visual comparison of fluoroscopy images with the same settings (97 kV/3.00 mA) (Fig. 3C, D) showed that the image of the U-Pad was clearer than the standard gel pad. This difference can be attributed to the fact that it is made of foam material and does not reduce the X-ray beam transmission compared with the standard gel pad.
There are many studies in endourology that measure angles and lengths. However, as far as the literature can be evaluated, this is the first study in which SSA and manipulation were evaluated geometrically in supine PNL. One of the limitations of the study is the small number of patients. Results need to be confirmed by including more patients. Another limitation is that in addition to geometric measurements, patients are operated with existing U-Pad and the geometric superiority should be checked with operative data such as accessibility, SFR, and less complications.
Conclusion
In the supine approach, The U-Pad is one of the most suitable equipment for the patient's topographic and renal anatomy, and it provides at least two times relief and range of motion with both the extra SSA and the angle. Despite its limited usage experience, it seems ideal both anesthetically and urologically. Its effectiveness needs to be improved with more patient numbers and clinical data.
Ethical Approval
The study was approved by the Ethic Committee of Istanbul Medipol University (Approval No. 2021/169, Date: February 18, 2021). The study protocol conformed to the ethical guidelines of the Helsinki Declaration.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.