Seasonal and COVID Pandemic‐Related Variations in Patients' Self‐Reported Adherence to Nutrition Recommendations for Stone Prevention Suggest Temporal Increases in Stone Recurrence Risk
KL Penniston, K Schobert, RJ Medenwald
University of Wisconsin School of Medicine and Public Health
MP01‐02
Withdrawn
MP01‐03
Percutaneous nephrostomy in Ureteropelvic junction obstruction with poorly functioning kidney: Is it still pertinent in adults
A Srivastava, S Kakoti, Z Tamboli, SK Sureka, UP Singh
Sanjay Gandhi Post Graduate institute of medical sciences
MP01‐04
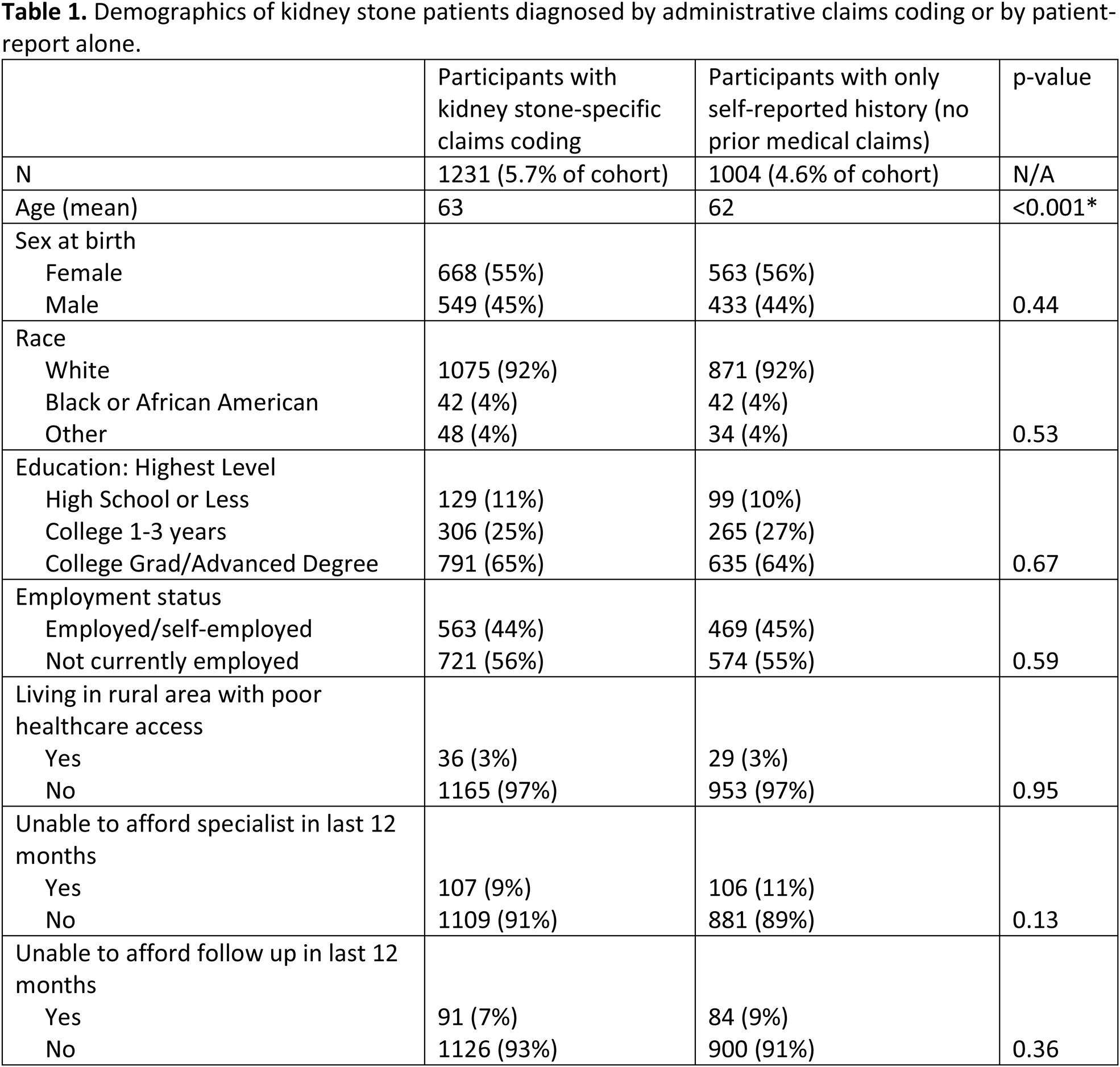
Kidney stone disease prevalence from administrative coding compared to self‐report: a report from the All of Us Research Program
CM Forbes, N Nimmagadda, NL Kavoussi, NL Miller, R Hsi
Vanderbilt University Medical Center, Department of Urology
MP01‐05
A Delphi Process Consensus Statement on Urinary Stone Treatment During COVID‐19: A World Endourological Society TOWER Research Initiative
R Smith, T Tailly, BH Chew, N Bhojani, KB Scotland
Institute of Urology, University College London Hospitals NHS Foundation Trust
MP01‐06
Prospective non‐randomized comparison of transperitoneal transvesical versus extravesical laparoscopic supratrigonal vesico‐vaginal fistula repair: A single centre experience
V Singh, RJ Sinha, G Singh
Dept of urology, King George Medical University
MP01‐07
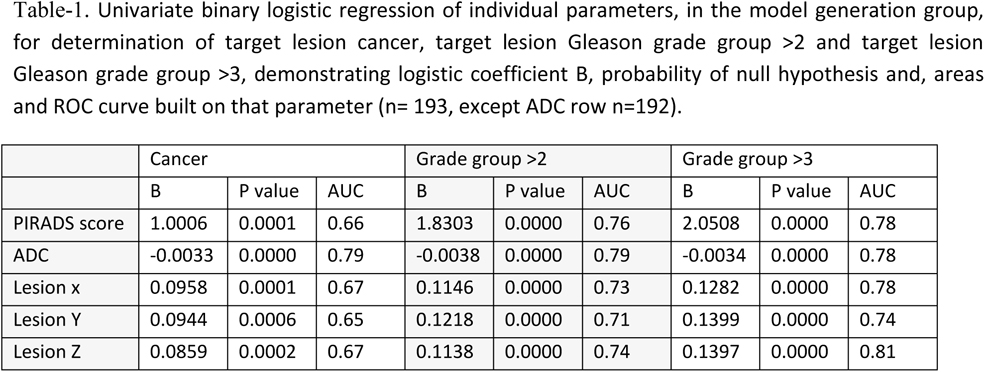
Identifying patients who will benefit from extended pelvic lymph‐node dissection during radical prostatectomy: a novel nomogram based on target biopsy only
E Checcucci, C Fiori, I Stura, D Amparore, S De Cillis, A Pecoraro, P Alessio, A Piana, F Piramide, G Volpi, P Verri, S Granato, B Carbonaro, D Zamengo, A De Pascale, D Gned, M Manfredi, G Migliaretti, F Porpiglia
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
MP01‐08
Clinical significance of markers of acute renal injury in predicting adverse outcomes in patients with coronavirus infection
V Pavlov, I Kabirov, A Alekseev, A Tarasenko, R Abdrakhimov, AO Papoyan
Bashkir State Medical University
MP01‐09
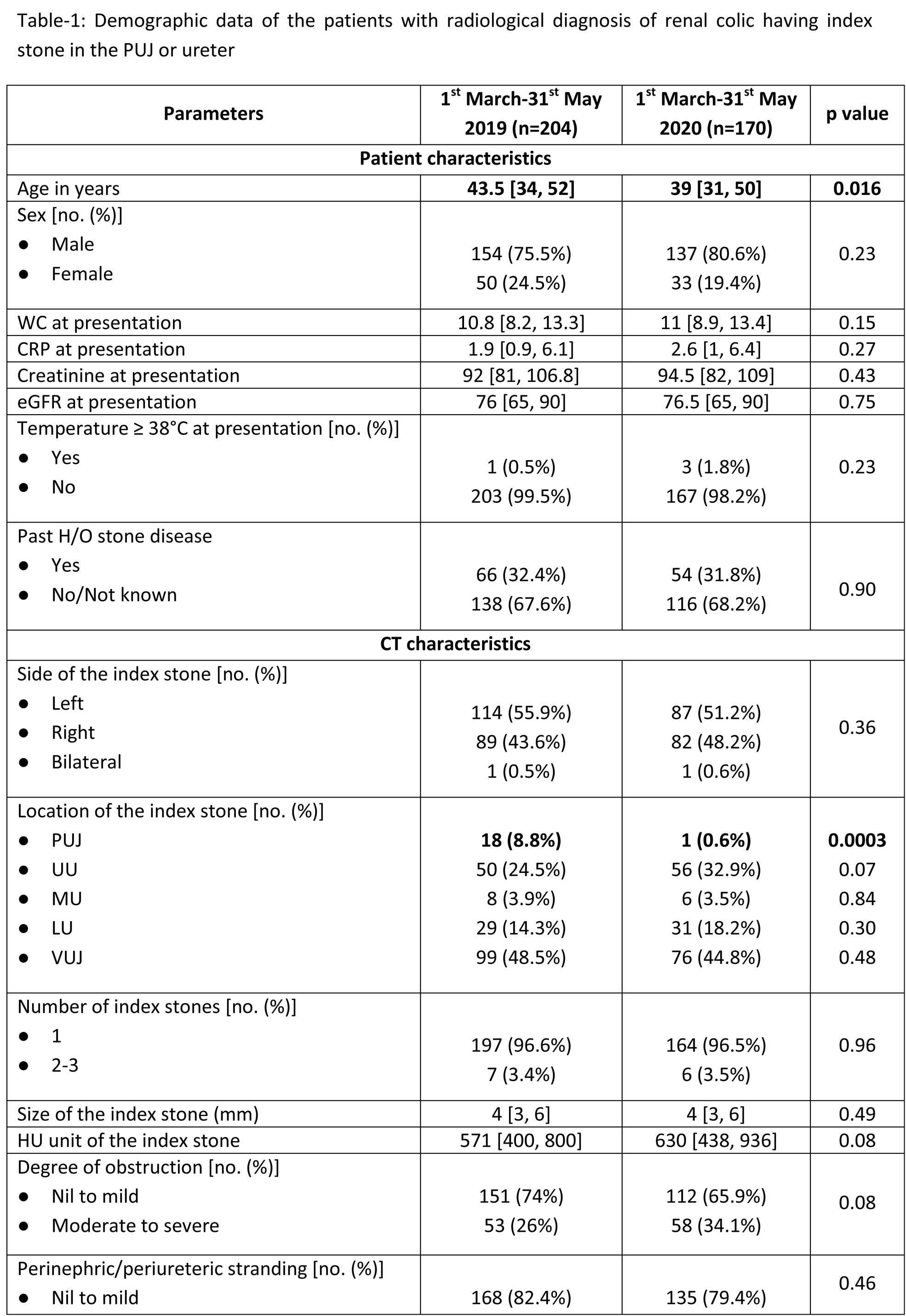
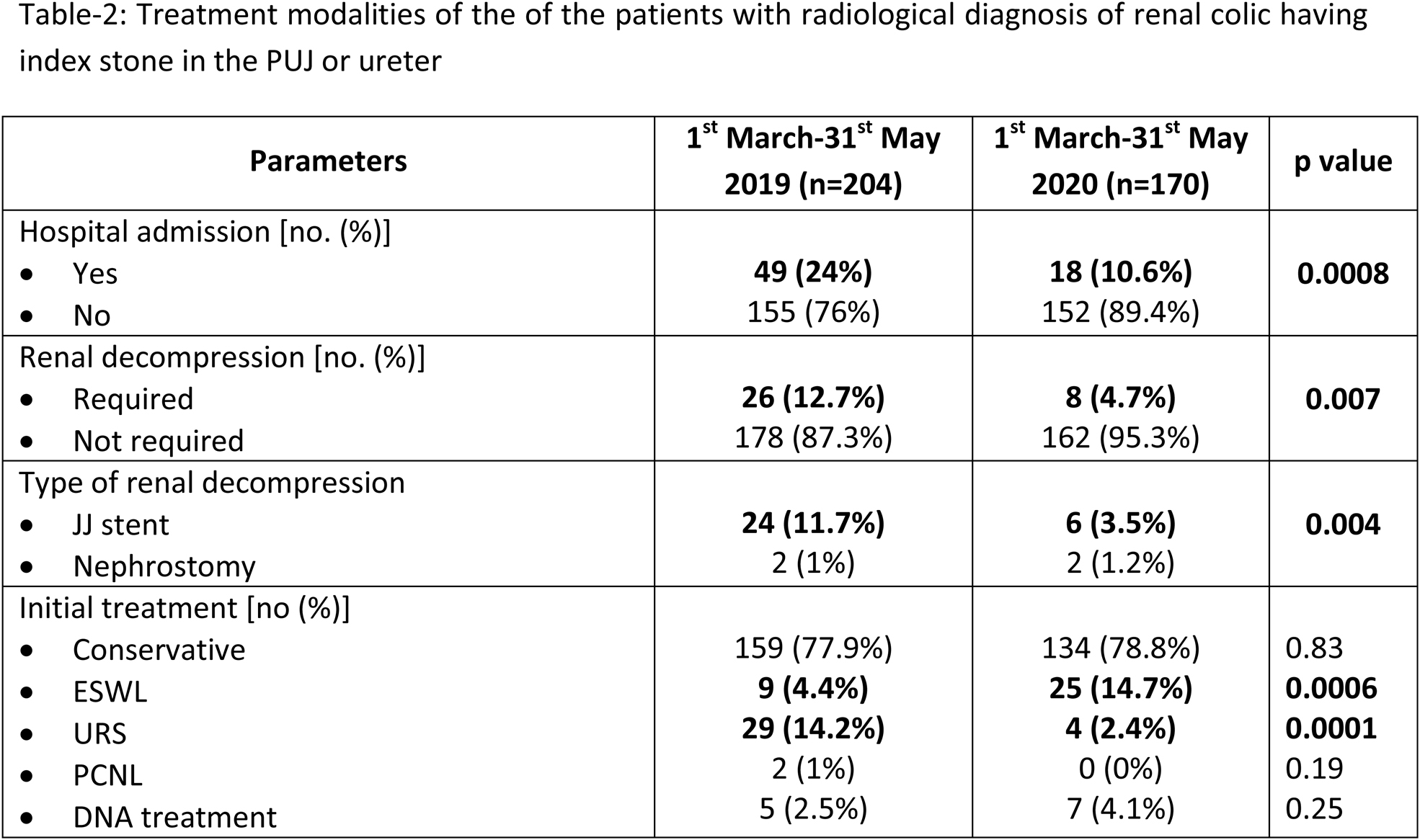
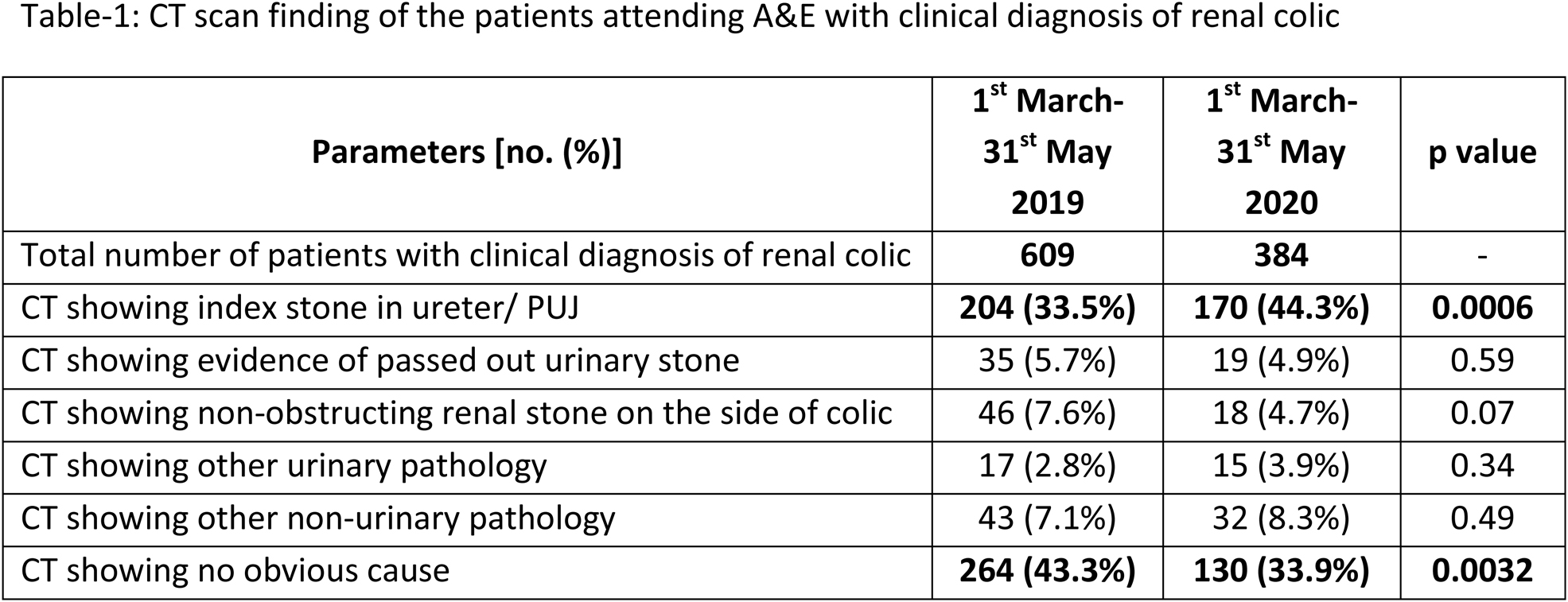
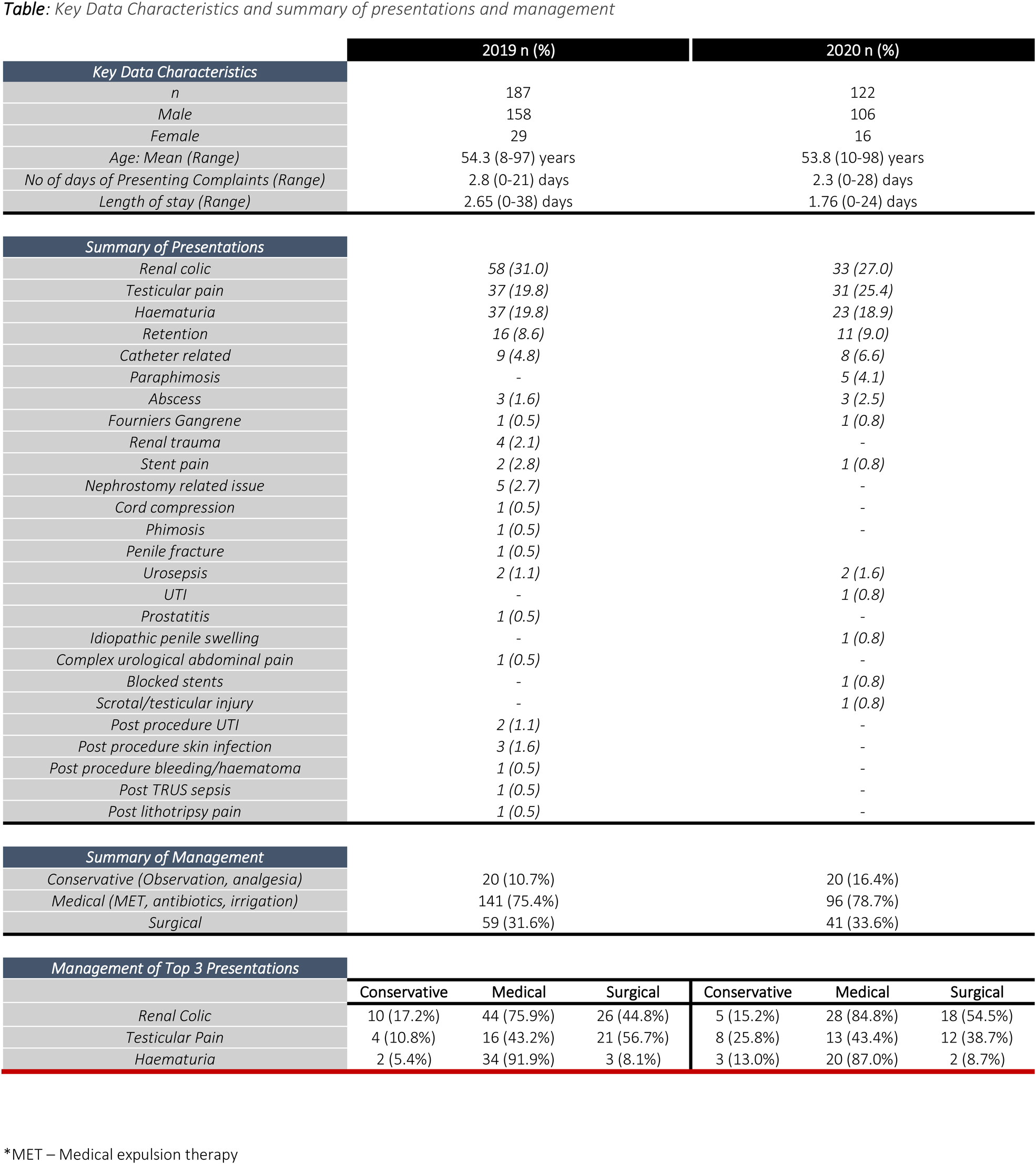
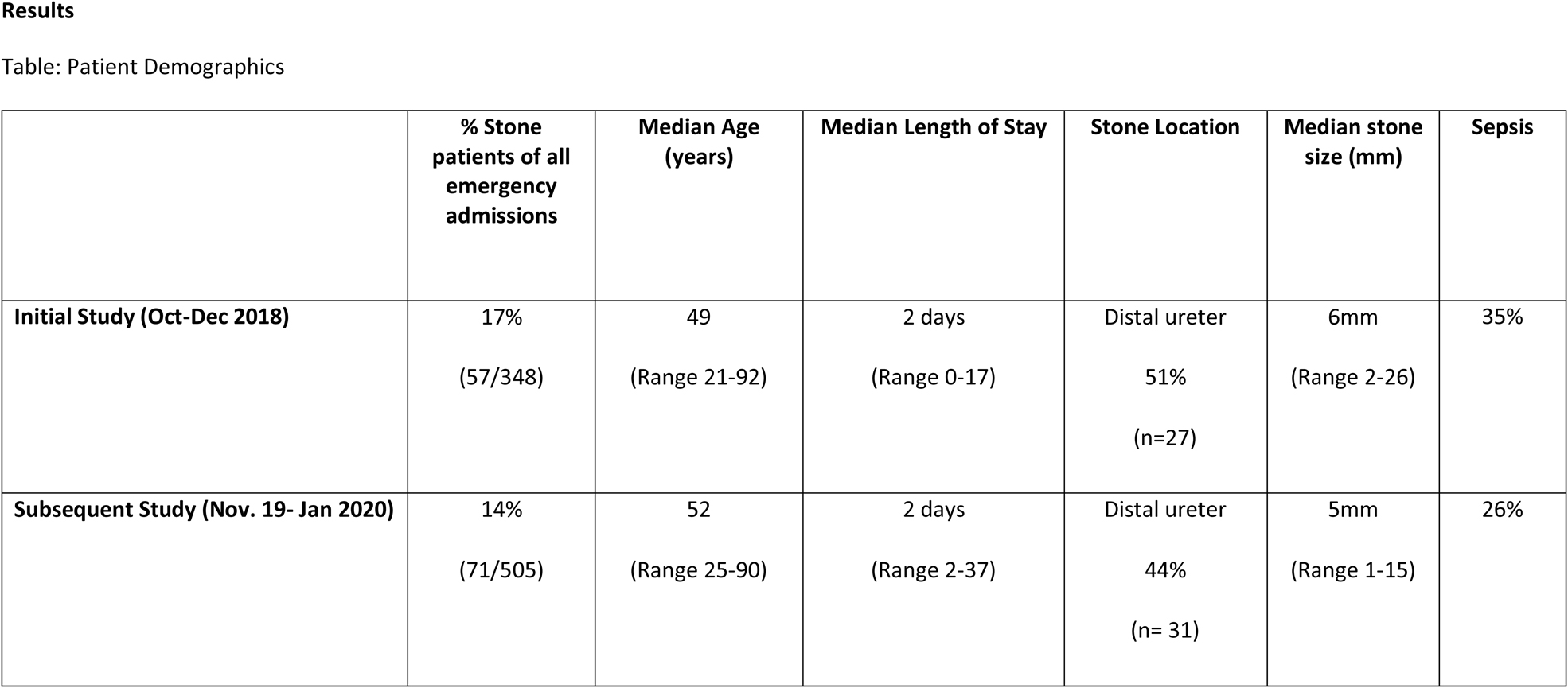
The impact of the COVID‐19 pandemic on the presentation and management of renal colic patients
S Mukherjee, H Kadhim, I Sahibzada, D Feflea, L Goldsmith, C Popanes, A Raza
London North West University Healthcare NHS Trust
MP01‐10
“Pseudo‐renal colic”–a neglected common entity with significant impact on health service providers' resources during both pre‐ and peri ‐ COVID‐19 pandemic
S Mukherjee
London North West University Healthcare NHS Trust
MP01‐11
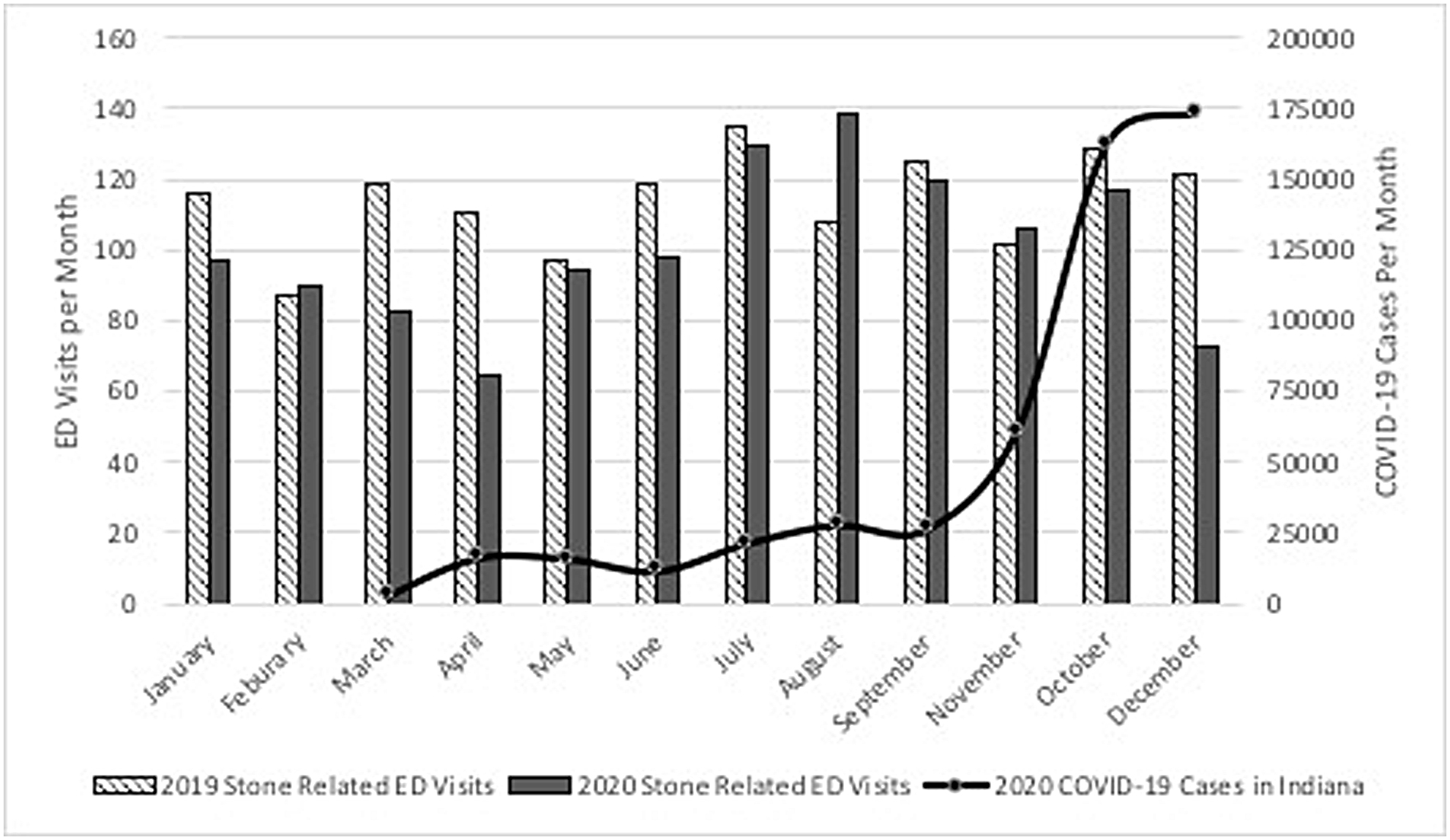
Assessment of Emergency Department Urolithiasis Presentations During the COVID‐19 Pandemic
DK Agarwal, T Large, M Assmus, ME Rivera
Indiana University Department of Urology
MP01‐12
Are patients' fears of catching COVID‐19 during an emergency hospital admission with an acute urological problem justified?–A UK epicentre experience
O Gbolahan, V Bonatsos, A Raza
London North West University Healthcare NHS Trust
MP01‐13
The effect of the COVID‐19 pandemic on management of urological emergencies including risk of contracting COVID‐19–a UK epicentre experience
O Gbolahan, V Bonatsos, A Raza
London North West University Healthcare NHS Trust
MP01‐14
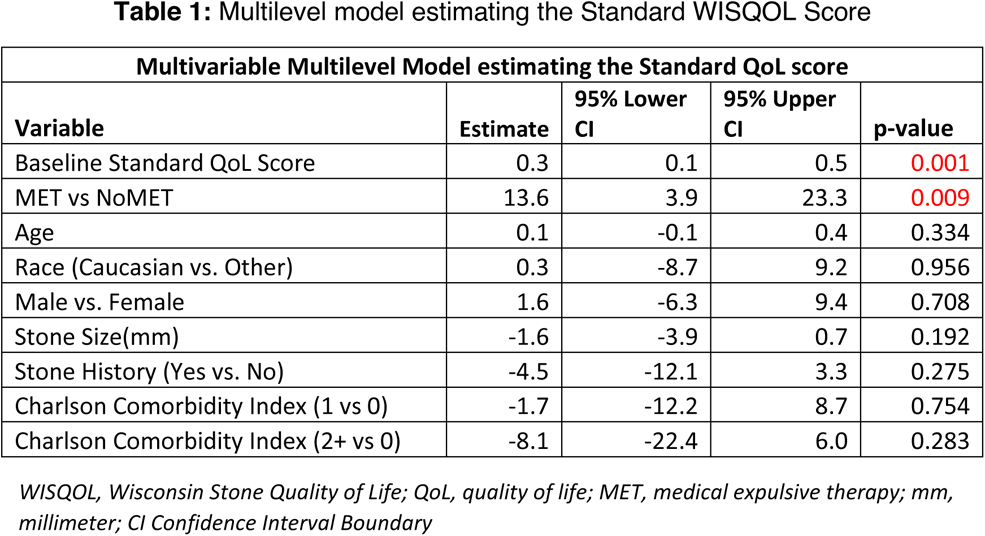
Quality of Life of Urolithiasis Patients During the COVID‐19 Pandemic: A Wisconsin Stone Quality of Life (WISQOL) Research Consortium Cross‐Sectional Study
VK Wong, BH Chew, KL Penniston, VG Bird, NM Streeper, SY Nakada, N Bhojani
University of Montreal Hospital Center (CHUM)
MP01‐15
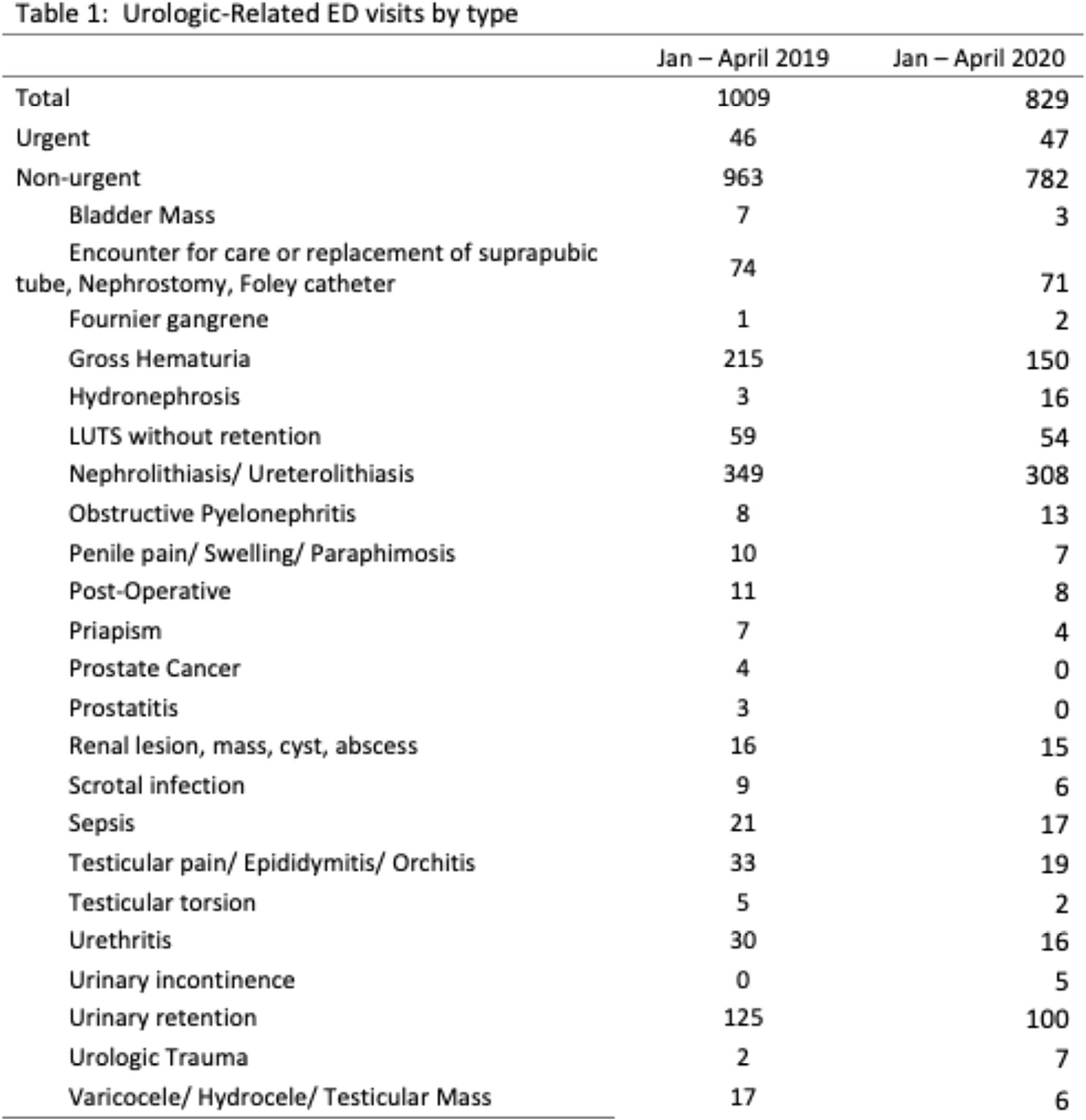
COVID‐19 Pandemic Results in Decreased Non‐Urgent Urologic‐Related Presentations to the ED
A Balen, J Molino, C Tucci, G Pareek, DW Sobel
Warren Alpert Medical School of Brown University
MP01‐16
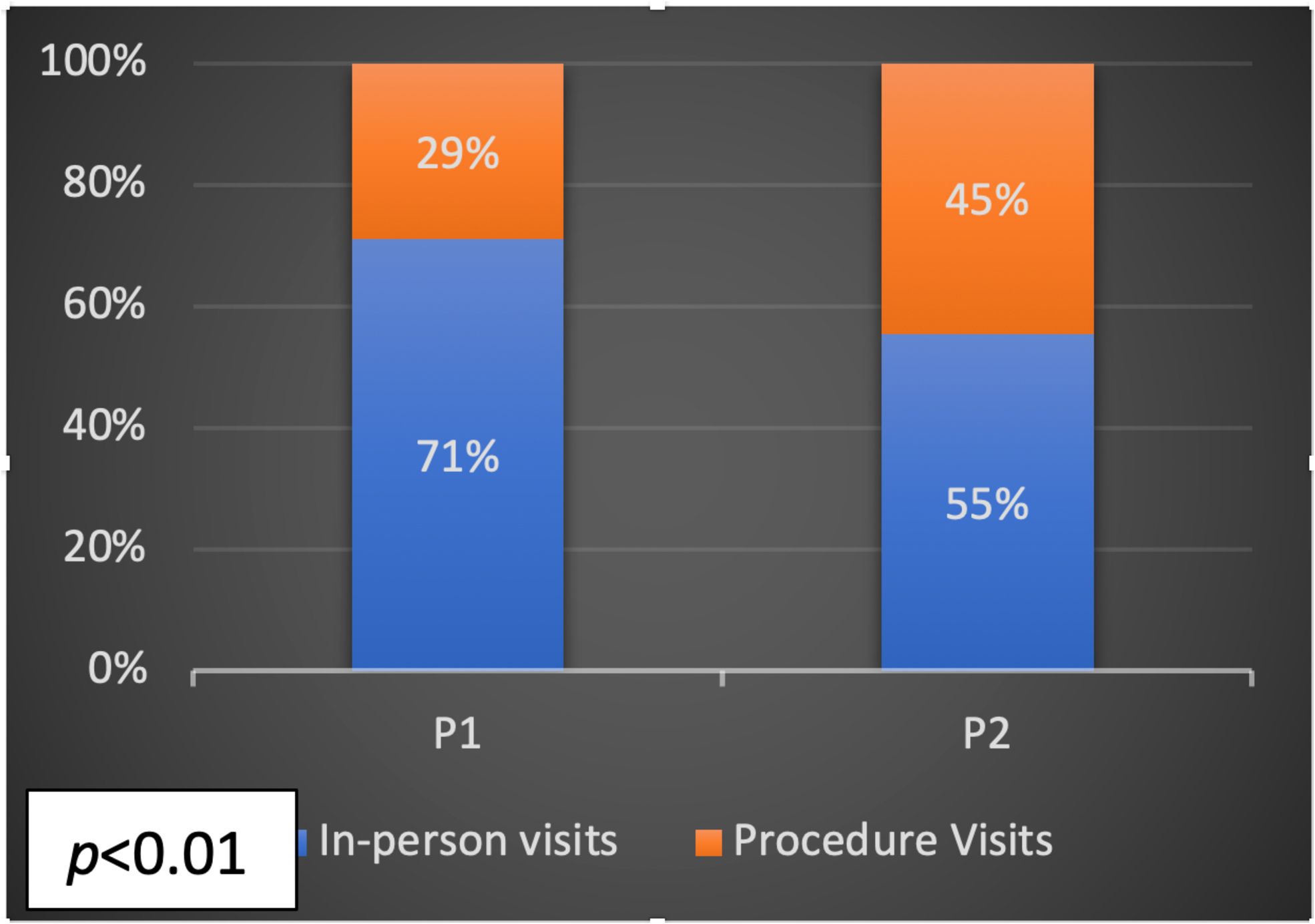
Transforming the Urology clinic to a procedure‐oriented center improves the quality of urological care and patient experience
F Hamouche, R Unno, J Ahn, D Bayne, H Yang, M Stoller, E Finlayson, s smith, R Pruthi, J Smith, T Chi
UCSF
MP01‐17
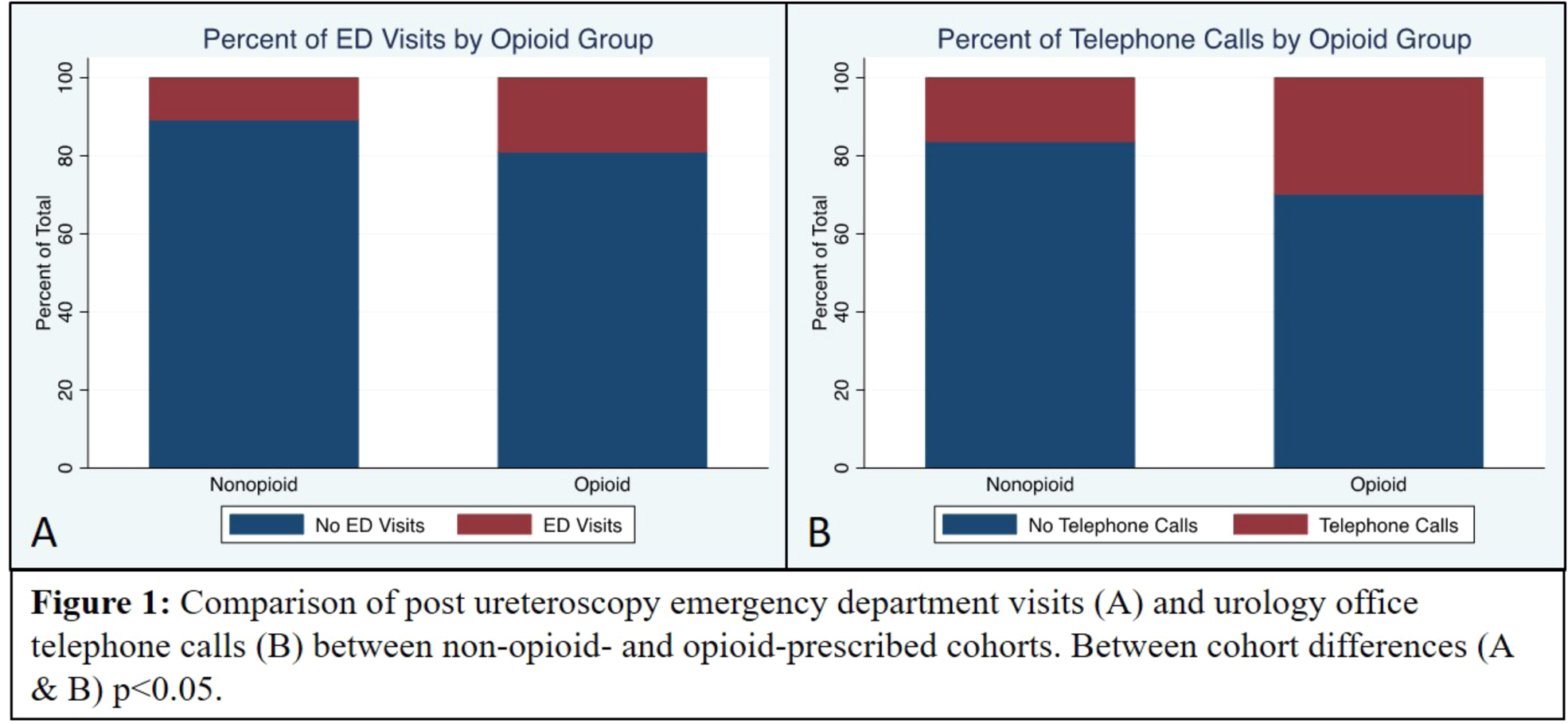
Quality Improvement for Quality of Life: Low‐Dose Buprenorphine Decreased Opioid Utilization Protocol in Robot‐Assisted Radical Cystectomy
LJ Smith, TC Peak, HE Moreland, DB Rukstalis
University of South Carolina School of Medicine
MP01‐18
Theatre utilisation in the era of COVID‐19
A Brodie, A Pai
Northampton General Hospital
MP01‐19
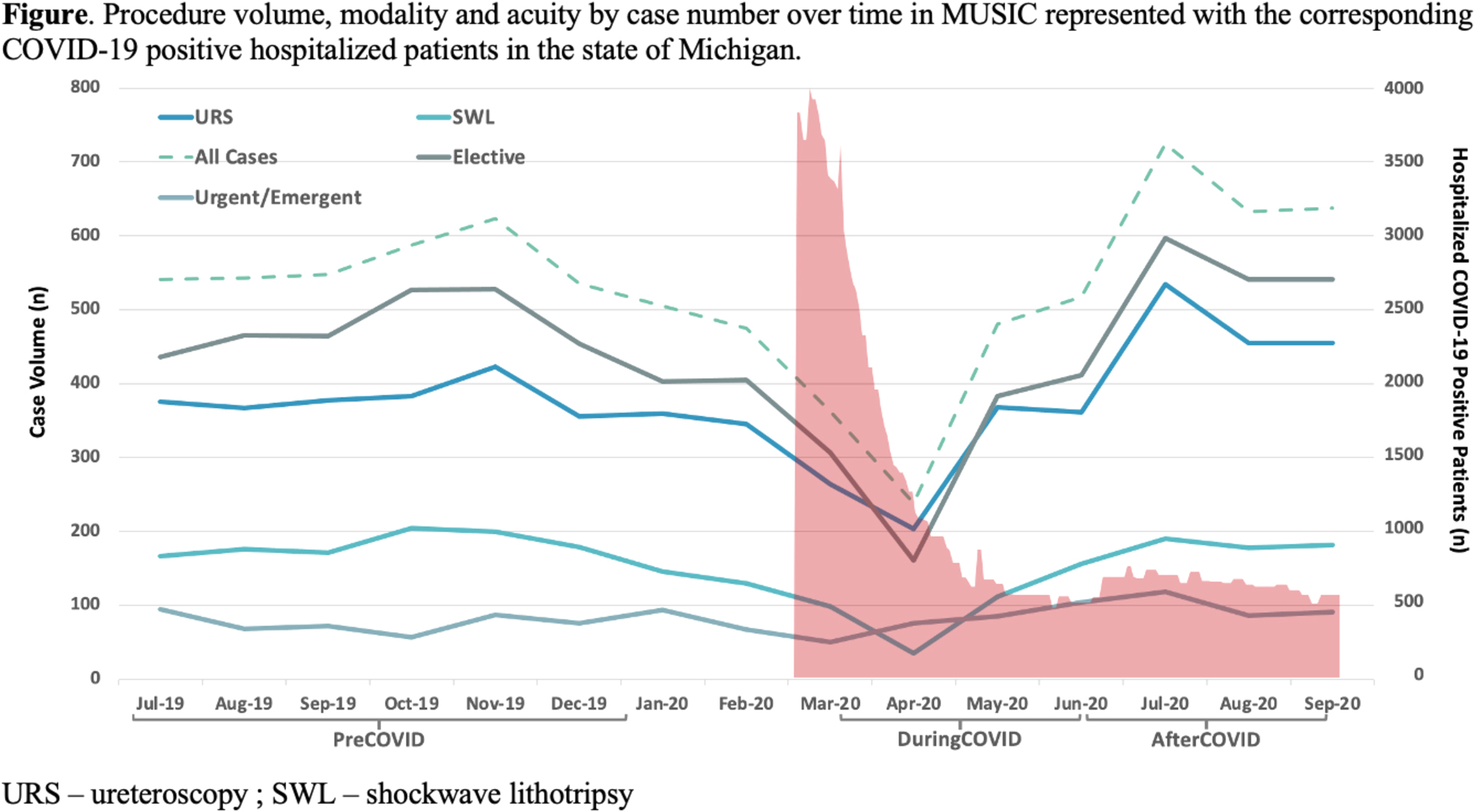
The impact of COVID‐19 on surgical care delivery for patients with urinary stones
J DiBianco, S Daignault‐Newton, J Ludlow, J Phelps, E Ratchford, M Cotant, KR Ghani, CA Dauw, f Urological Surgery Improvement Collaborative
Department of Urology, University of Michigan
MP01‐20
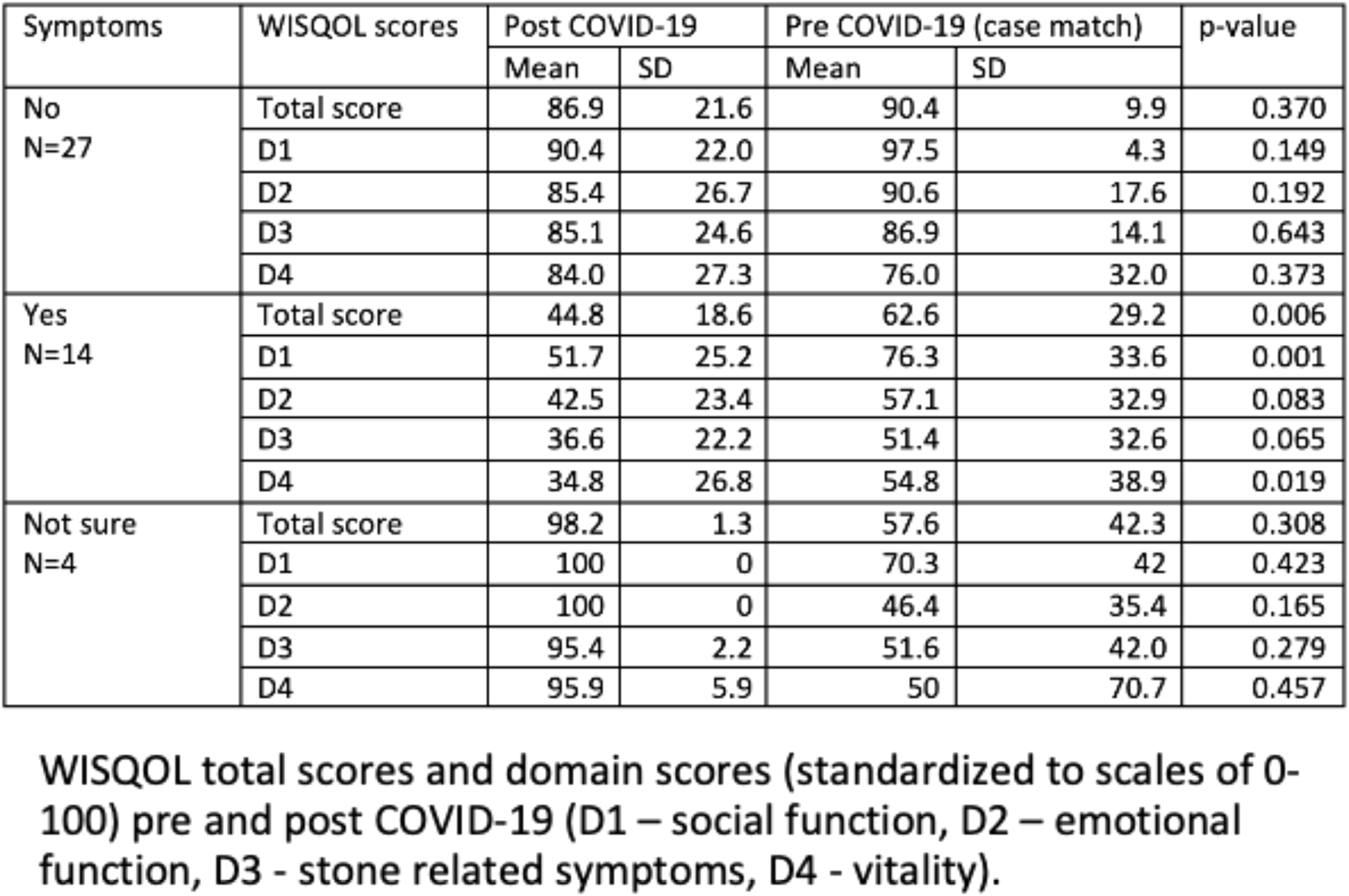
Health Related Quality of Life for Stone Patients During COVID‐19 Pandemic is Significantly Lower than Pre‐Pandemic
MA Knoedler, S Li, SL Best, SP Hedican, KL Penniston, SY Nakada
University of Wisconsin, Department of Urology
MP01‐21
COVID‐19 pandemic and its effect on supra‐regional extracorporeal shock wave lithotripsy (ESWL) service
M Kay, J Lau, F Jarral, S Rajpal, N Boucher, J Patterson
Royal Hallamshire Hospital
MP01‐22
#AUAMatch: The Impact of COVID‐19 on Social Media Use in the Urology Residency Match
P Ho, EJ Margolin, E Sebesta, A Small, GM Badalato
Columbia University Vagelos College of Physicians and Surgeons
Moderated Poster Session 02: Epidemiology
MP02‐01
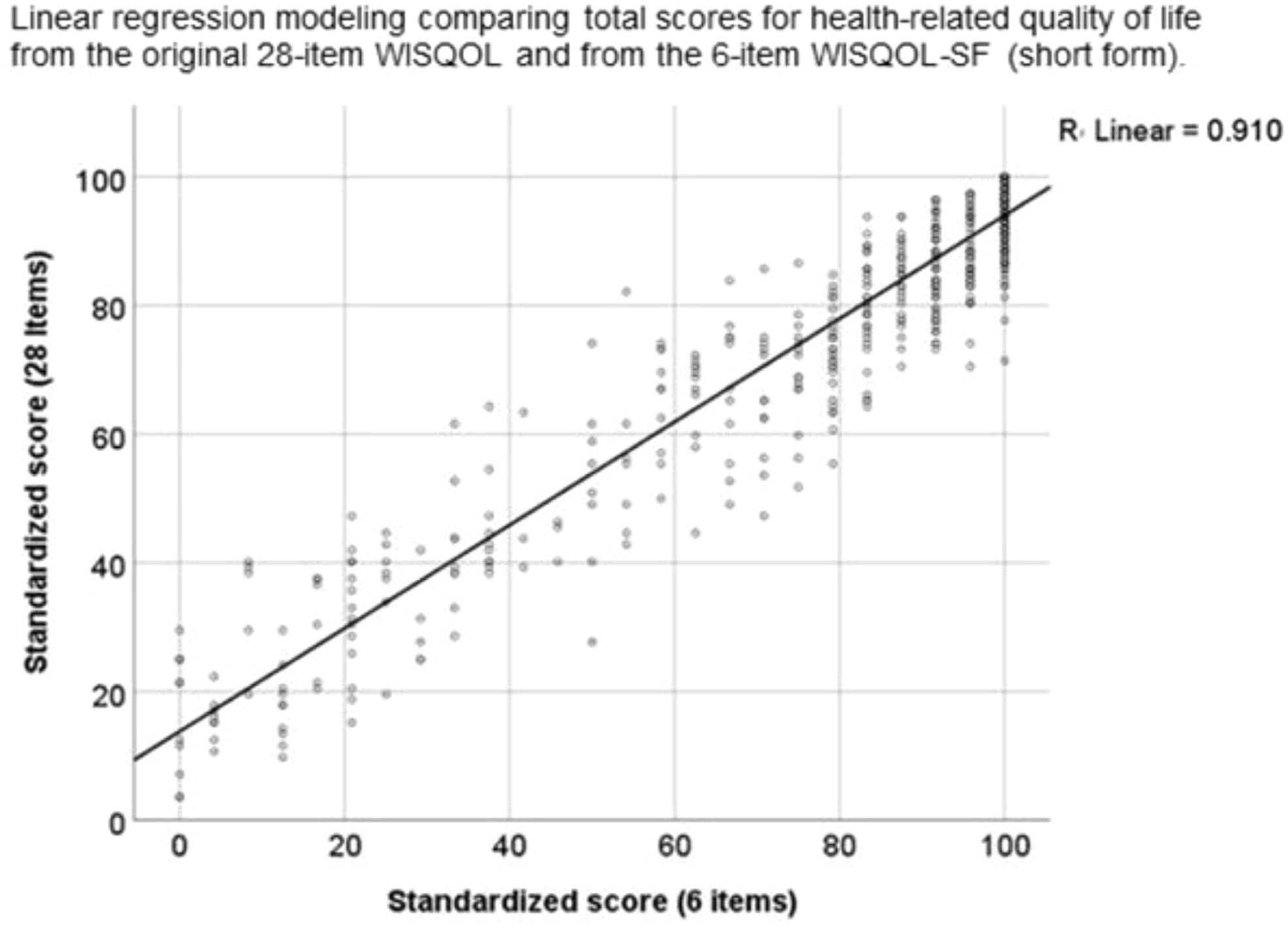
Development of the Short Form of the Wisconsin Stone Quality of Life (WISQOL) Questionnaire for Assessing the Health‐Related Quality of Life of Patients with Urolithiasis
KL Penniston, S Li, SY Nakada
University of Wisconsin School of Medicine and Public Health
MP02‐02
Where do you practice? And its effect on equipment, technique, and more
T Aro, A Smith, A Rai, D Mikhail, D Hoenig, AD Smith, Z Okeke
The Smith Institute for Urology
MP02‐03
Withdrawn
MP02‐04
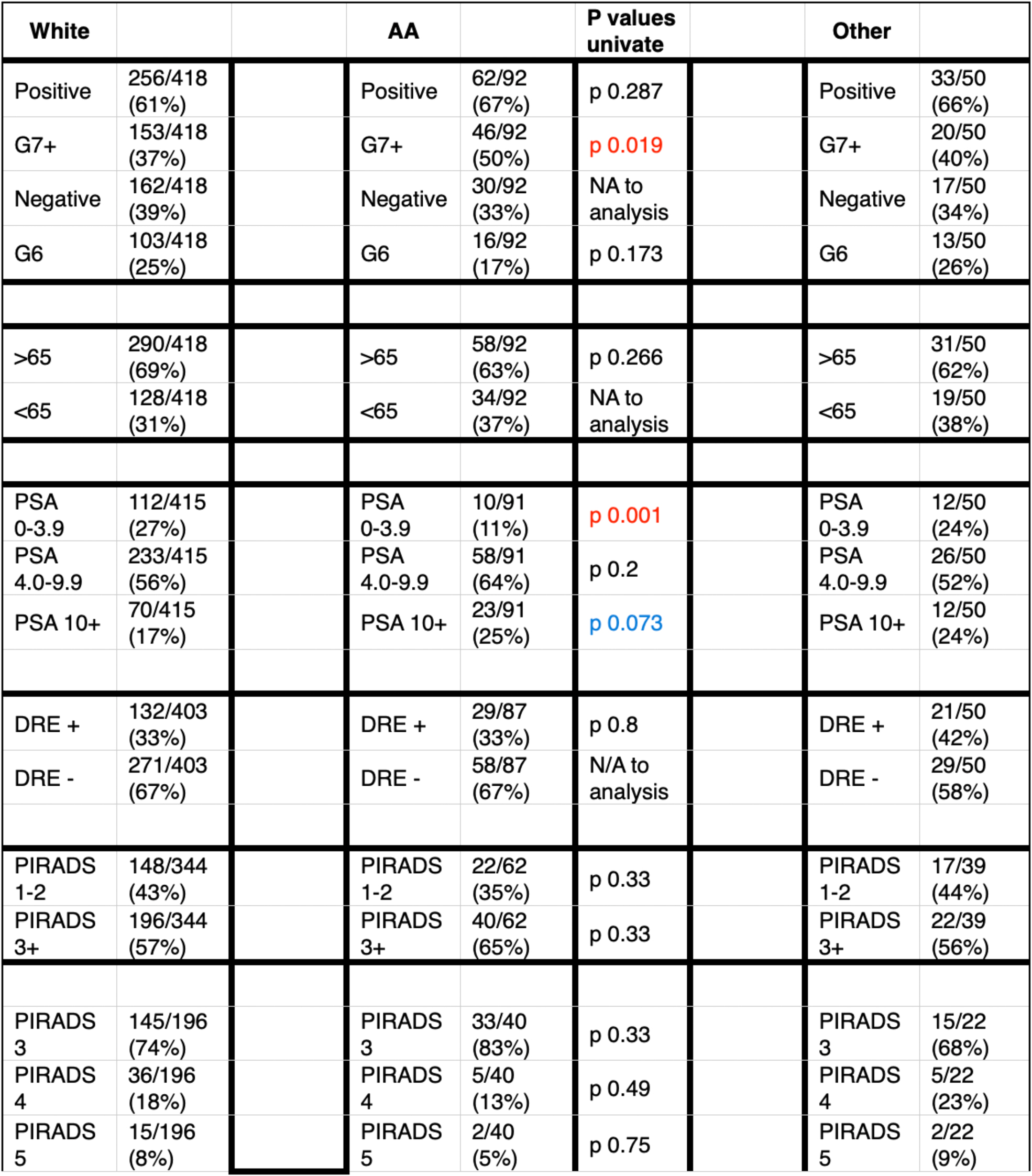
Racial Disparity in Prostate Cancer Diagnosis: A Comparison of Prostate Biopsy Results in African American and White Men using an MRI based Biopsy Strategy
A Kasraeian, M Alcantara, K Mola Alcantara, J Cesaretti, A Kasraeian
Kasraeian Urology
MP02‐05
Economic Burden of Complicated Ureteral Stent Removal in Patients with Kidney Stone in the United States
KR Ghani, S Rojanasarot, B Cutone, S Bhattacharya, AE Krambeck
Northwestern University
MP02‐06
Cost‐Effectiveness of Retrograde Intrarenal Surgery, Standard and Mini Percutaneous Nephrolithotomy, and Extracorporeal Shock Wave Lithotripsy for the Management of 1‐2cm Renal Stones
KM Wymer, T Juvet, V Sharma, K Koo, MR Humphreys, AM Potretzke
Mayo Clinic
MP02‐07
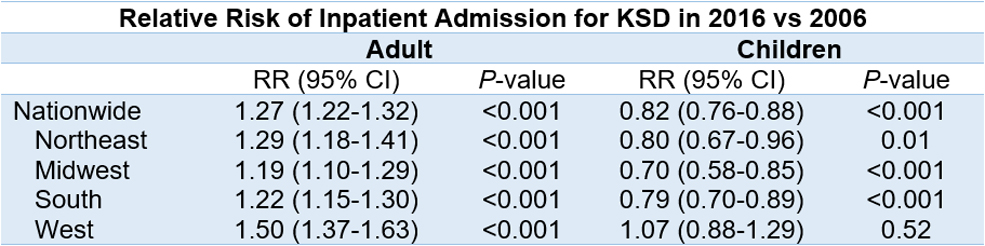
Seasonal Variations in Inpatient Pediatric Admissions for Urolithiasis
R Alam, W Wu, BR Matlaga, JS Winoker
Johns Hopkins University School of Medicine
MP02‐08
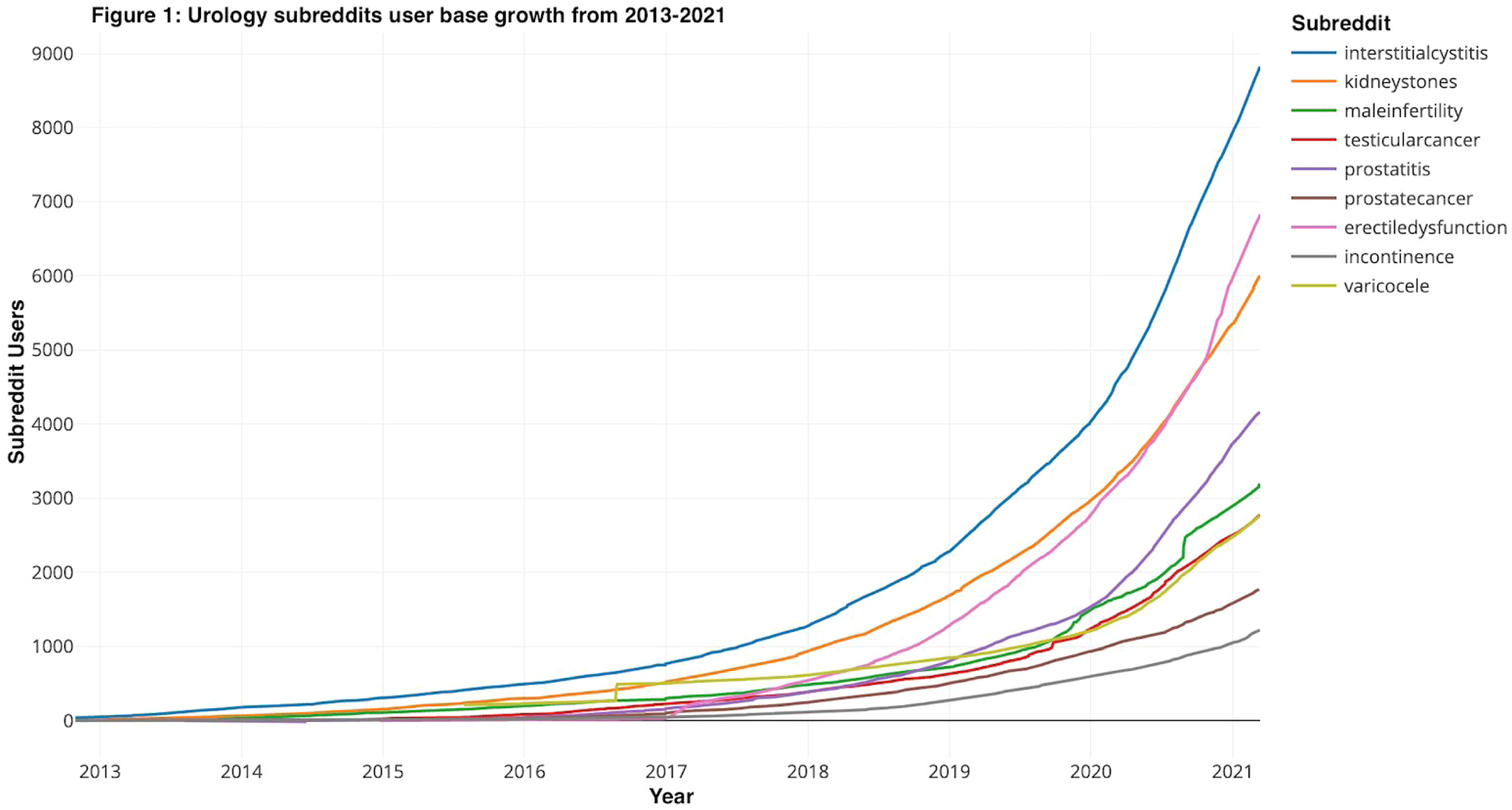
Analysis of urological discussions on Reddit: an emerging platform for patient‐to‐patient information, advice and support
KT Ravivarapu, EB Garden, A Small, O Al‐Alao, MA Palese
Icahn School of Medicine at Mount Sinai
MP02‐09
Understanding patients' concerns regarding kidney stones using quantitative thematic analysis of social media
KT Ravivarapu, A Small, EB Garden, M Levy, O Al‐Alao, MA Palese
Icahn School of Medicine at Mount Sinai
MP02‐10
Thulium laser enucleation of the prostate versus open prostatectomy: A prospective cost analysis
M Maltagliati, L Berti, U Besana, A Calori, C Buizza, S Micali, BC Rocco, M Sighinolfi, G Bozzini
ASST Valle Olona
MP02‐11
Seasonal variation in the incidence of acute renal colic
A Alkhayal, O Alfraidi, T Almudlaj, A Nazer, N Alboqami, K Alrabeeah, AH Alathel
Schulich School of Medicine & Dentistry, Western University
MP02‐12
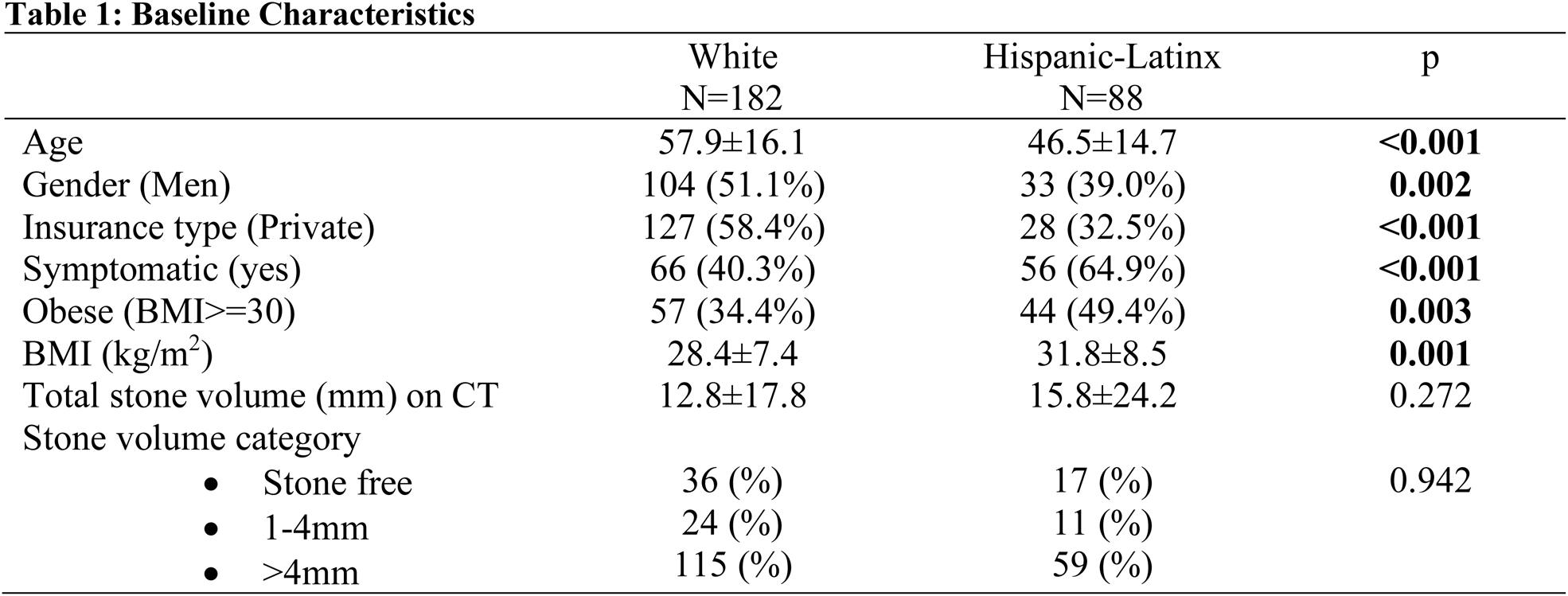
Health‐Related Quality of Life Disparities among Hispanic/Latinx Patients with Nephrolithiasis
AR Flores, G abedi, C Girgiss, KL Penniston, S Li, D Norena, DF Friedlander, SK Bechis, RL Sur
MP02‐13
What is the kidney stone related nephrectomy prevalence in an emerging country?
V Dall'Aqua, R Borges, A Rodrigues, A Lopes Neto
MP02‐14
Withdrawn
MP02‐15
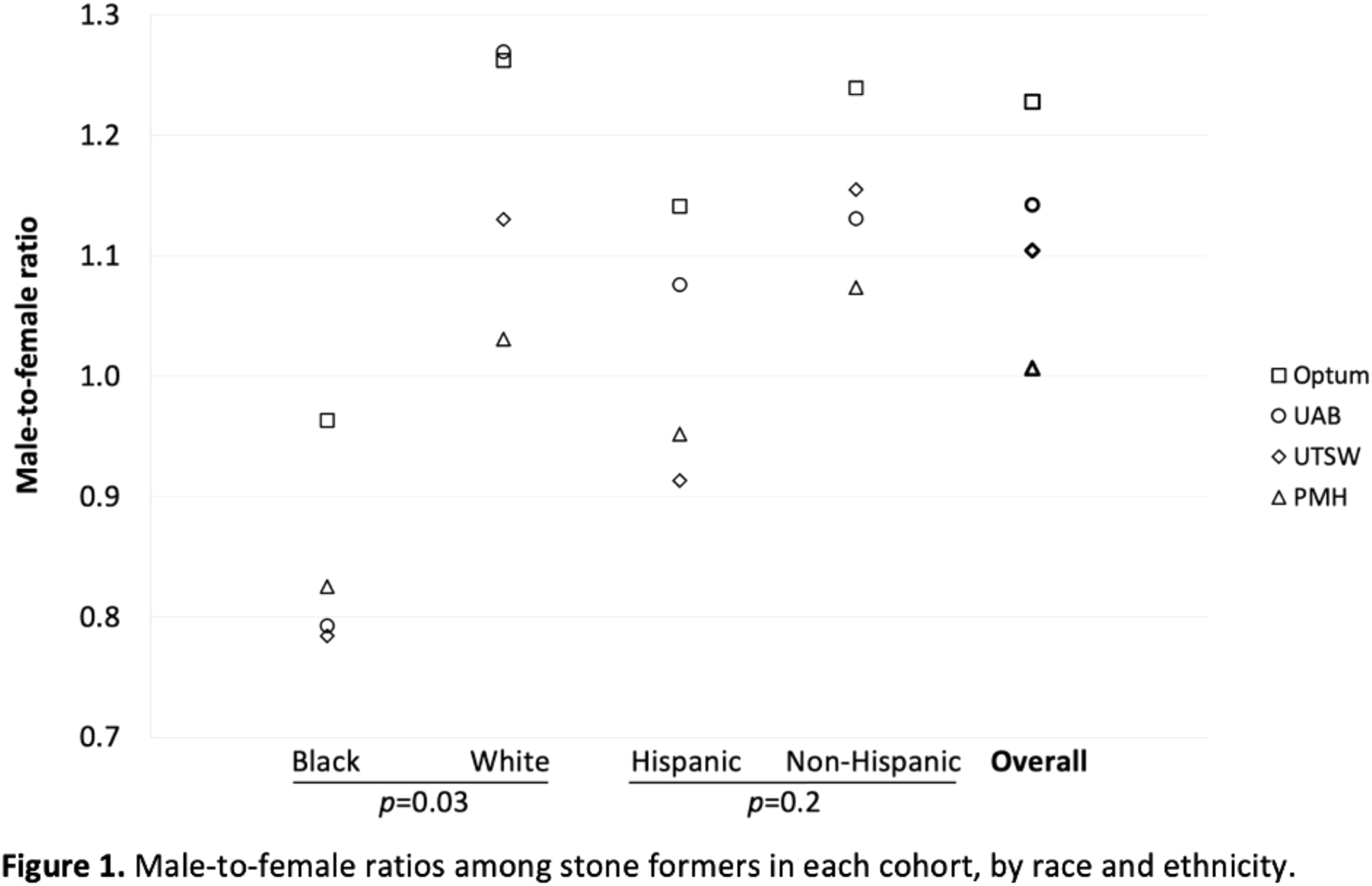
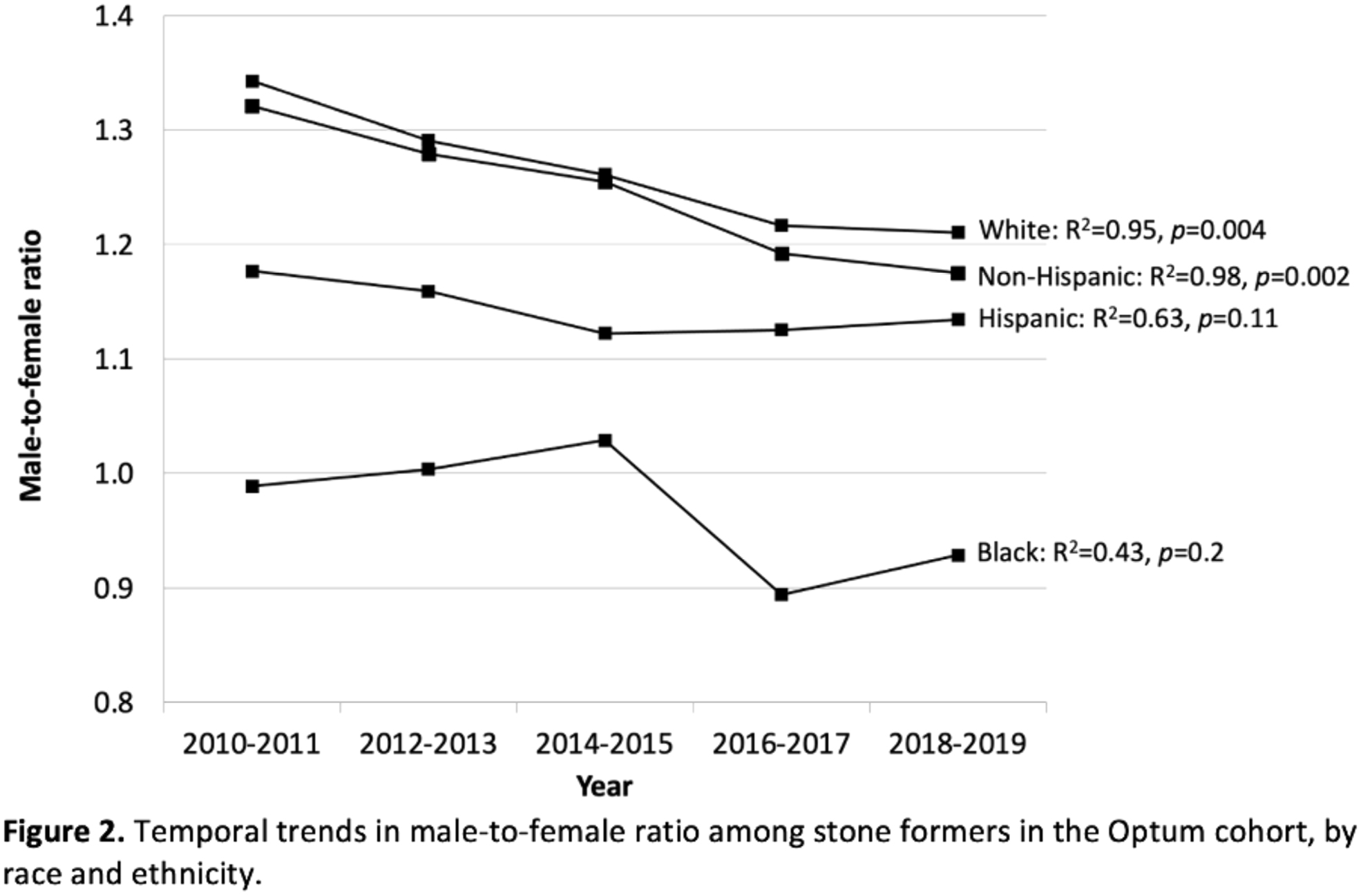
Trends in the Influence of Gender, Race, and Ethnicity on the Prevalence of Kidney Stones: A Multi‐Institutional and Claims Analysis
J Crivelli, N Maalouf, P Yan, A Hughes, R Hsi, NE Canvasser, N Kachroo, D Leavitt, K Wood, G Oates, JM Hollingsworth, DG Assimos
The University of Alabama
MP02‐16
Withdrawn
MP02‐17
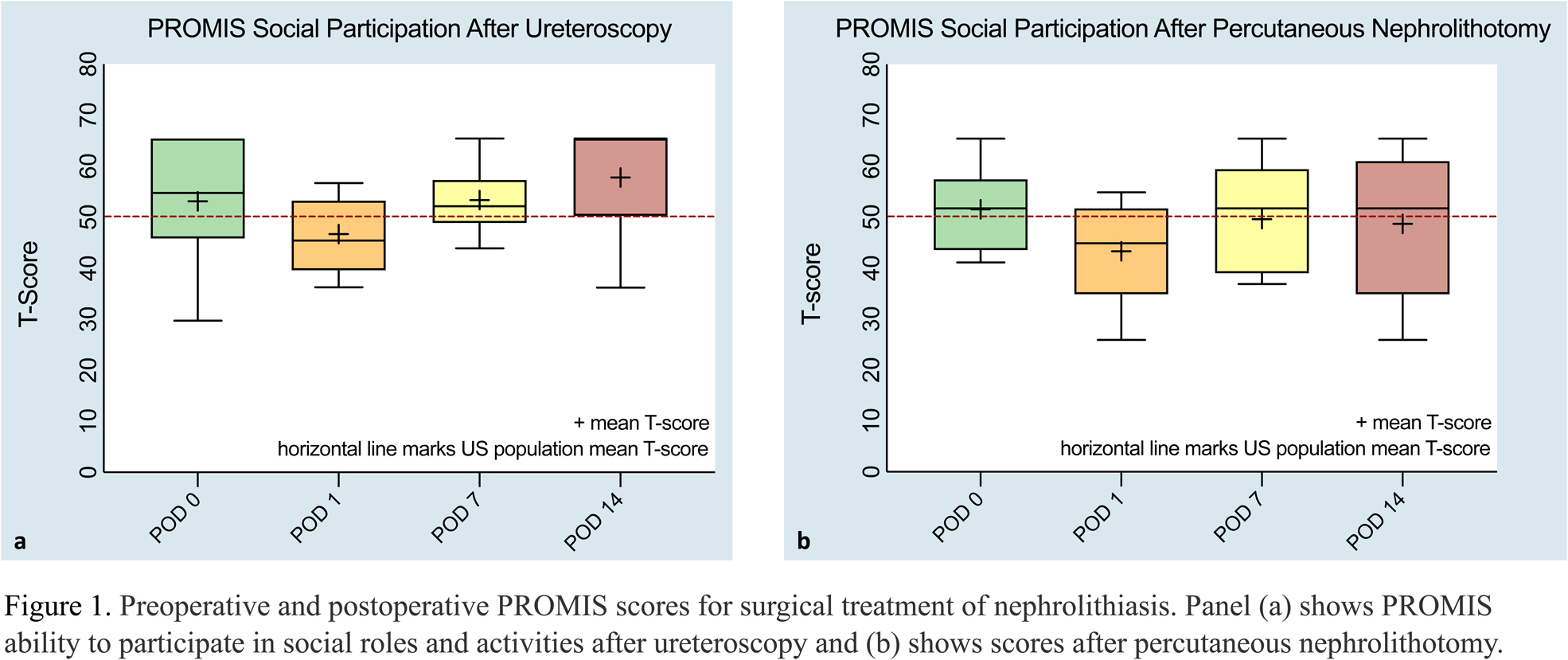
The Social Impact of Surgery for Nephrolithiasis: Results from the Endourological Society TOWER Research Collaborative
AE Jones, G Lin, H Stambakio, BH Chew, JM Stern, JB Ziemba
University of Pennsylvania Perelman School of Medicine
MP02‐18
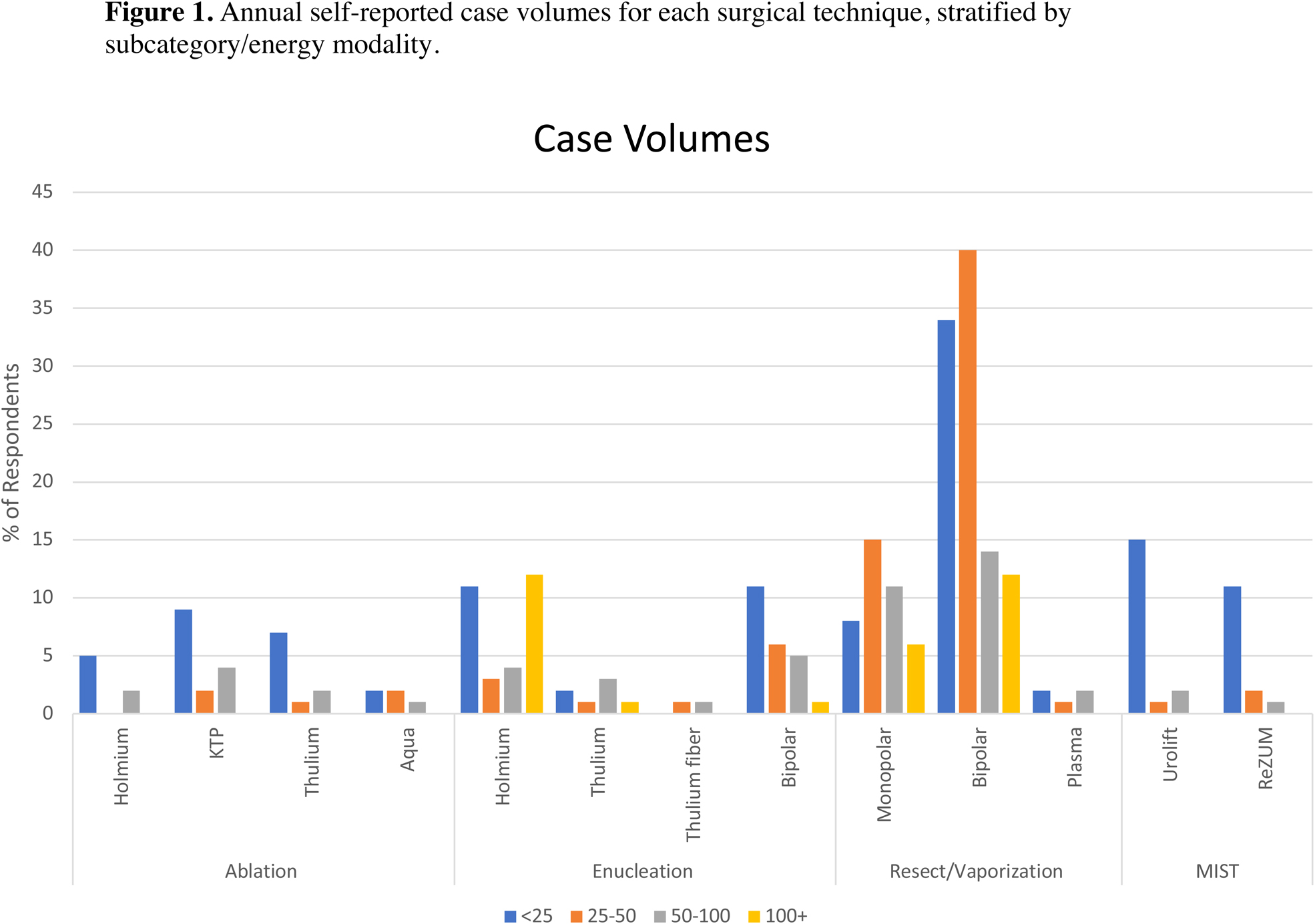
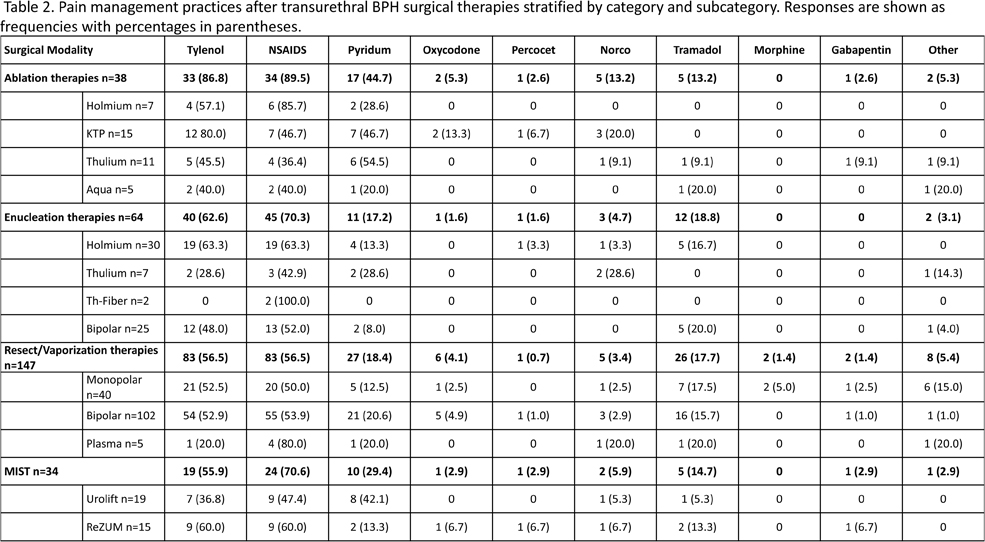
Contemporary practice patterns of transurethral therapies for benign prostate hypertrophy: Results of a worldwide survey
MS Lee, M Assmus, DK Agarwal, T Large, AE Krambeck
Northwestern University Feinberg School of Medicine
MP02‐19
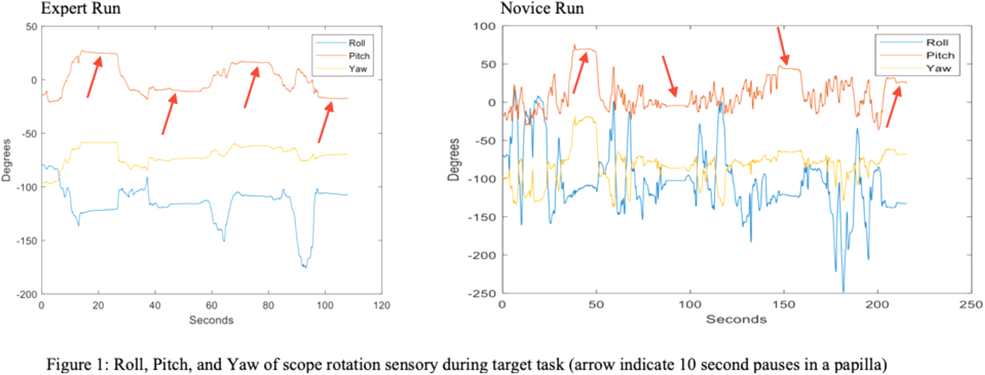
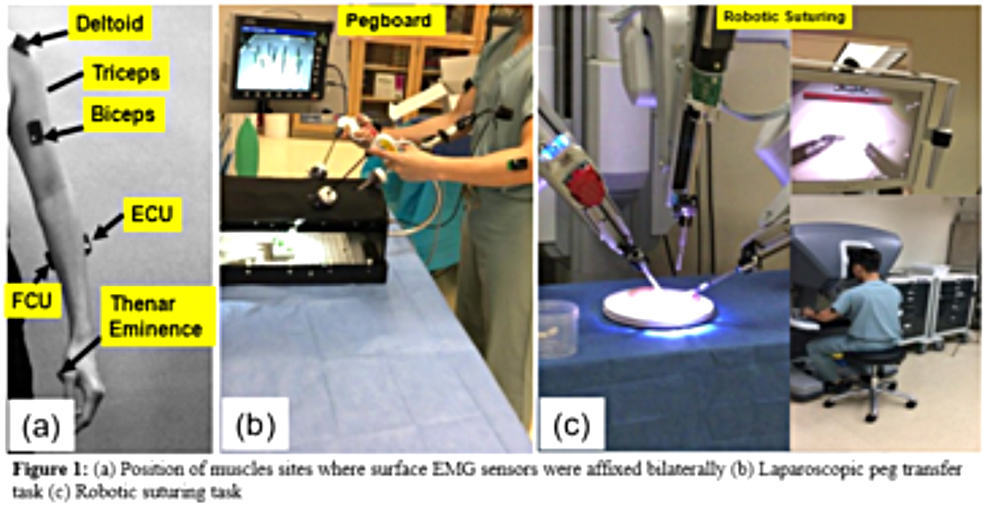
Impact of flow disruptions on mental workload and performance during Percutaneous Nephrolithotomy
S Hussain, SM Nazim, M Ather, N Zahid, M Ather
Aga Khan University
MP02‐20
Racial Differences in Utilization of Cytoreductive Surgery among Metastatic Renal Cell Carcinoma Patients Receiving Systemic Therapy
A Becerra, D Cao, N Buac, M Greydanus, M Sturgis, C Feng, C Coogan, E Cherullo, S Vourganti, A Stephenson, AK Chow
Rush University Medical Center
MP02‐21
Withdrawn
MP02‐22
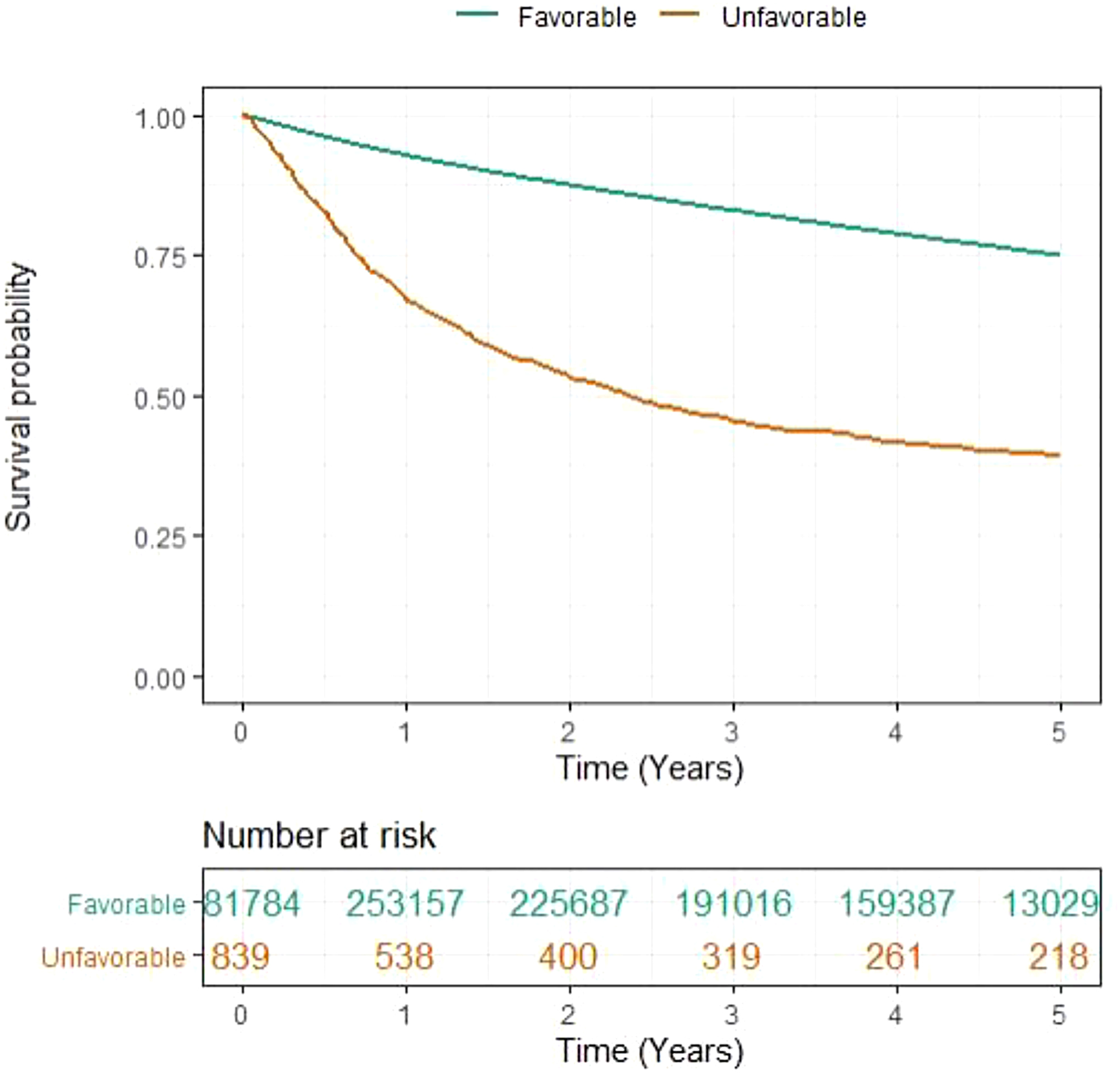
Five Year Survival Outcome Comparison amongst Patients with Unfavorable vs. Favorable Renal Cell Carcinoma Subtypes
D Roadman, A Becerra, N Buac, M Greydanus, M Sturgis, D Cao, C Coogan, E Cherullo, S Vourganti, A Stephenson, AK Chow
Rush University Medical Center
Moderated Poster Session 03: BPH I
MP03‐01
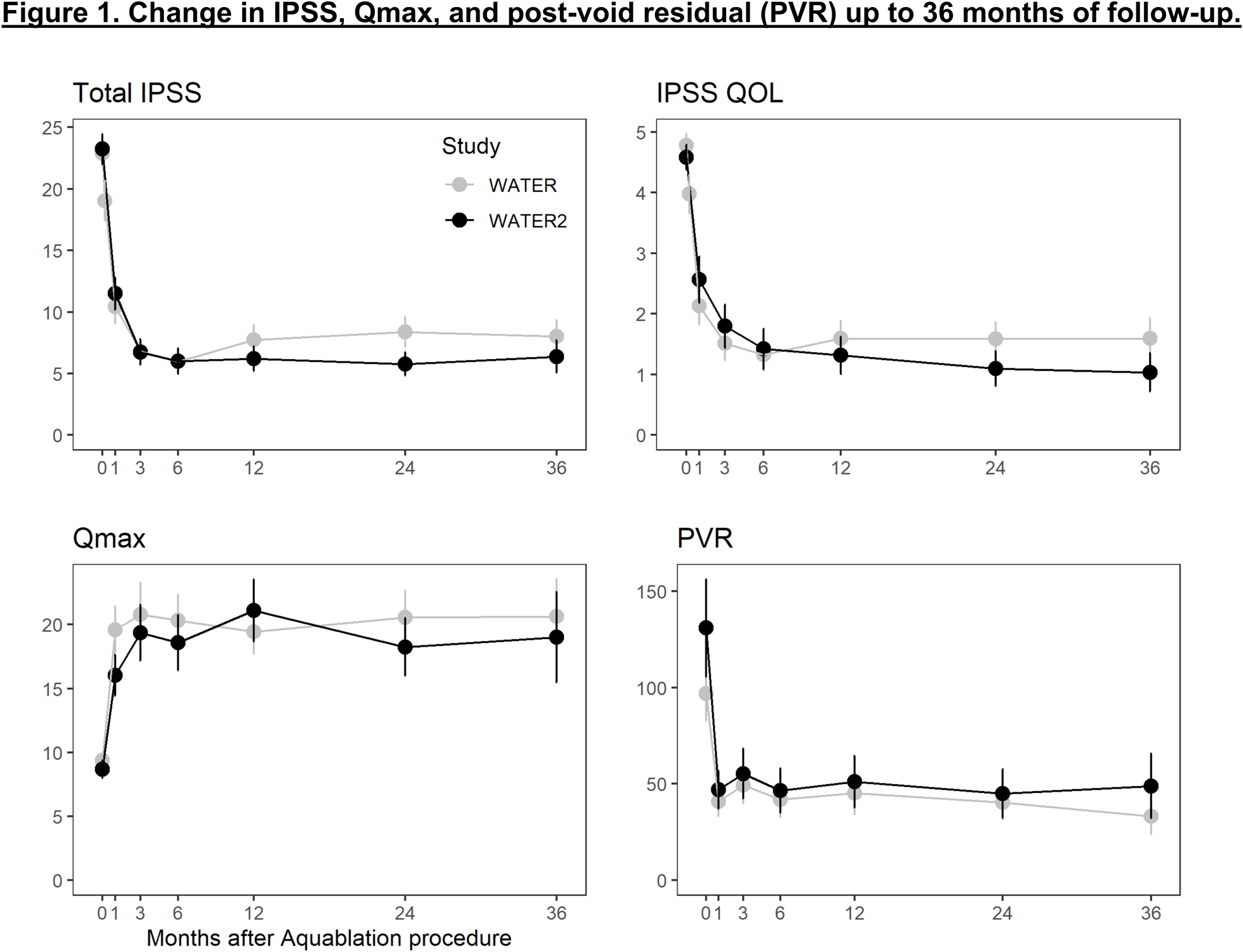
Three‐Year Outcomes after Aquablation Compared to TURP: Efficacy and Ejaculatory Improvements Sustained
PJ Gilling
Urology Bay of Plenty
MP03‐02
The OPEN WATER trial: Aquablation in a real‐world setting 1 year follow‐up
PJ Gilling
Urology Bay of Plenty
MP03‐03
Pulsed thulium laser enucleation of the prostate (ThuLEP) utilizing a novel pulsed Thulium:YAG laser: first clinical results
C Netsch, B Becker, CM Rosenbaum, AJ Gross
Department of Urology, Asklepios Hospital Barmbek, Hamburg, Germany
MP03‐04
Aquablation vs. thulium laser enucleation of the prostate (ThuLEP): early functional results of a matched‐paired analysis
B Becker, K Vogt, AJ Gross, CM Rosenbaum, C Netsch
Department of Urology, Asklepios Hospital Barmbek, Hamburg, Germany
MP03‐05
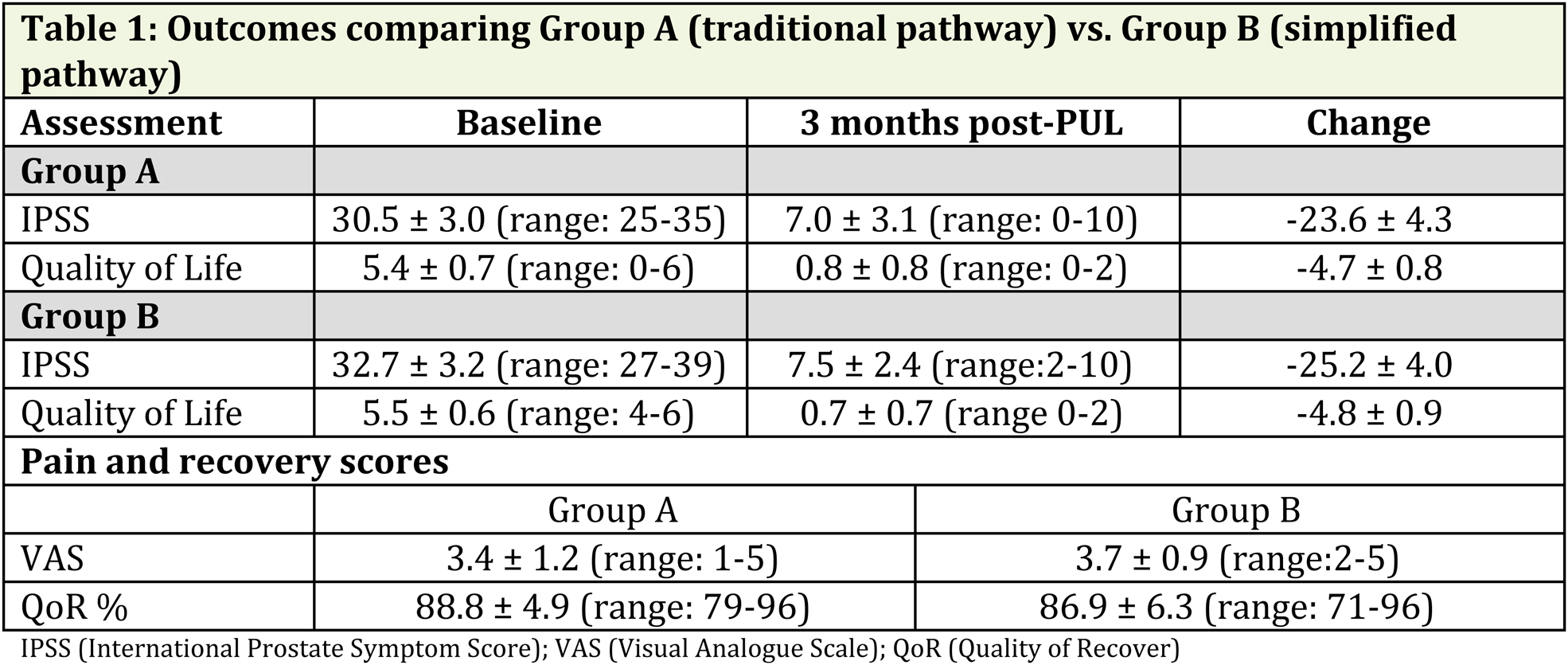
Prostatic Urethral Lift (PUL) demonstrates real world effectiveness in subjects with obstructive median lobes
NJ Barber, KL Ng, G Eure, D Grier, M Rochester, D Rukstalis
Frimley Park Hospital
MP03‐06
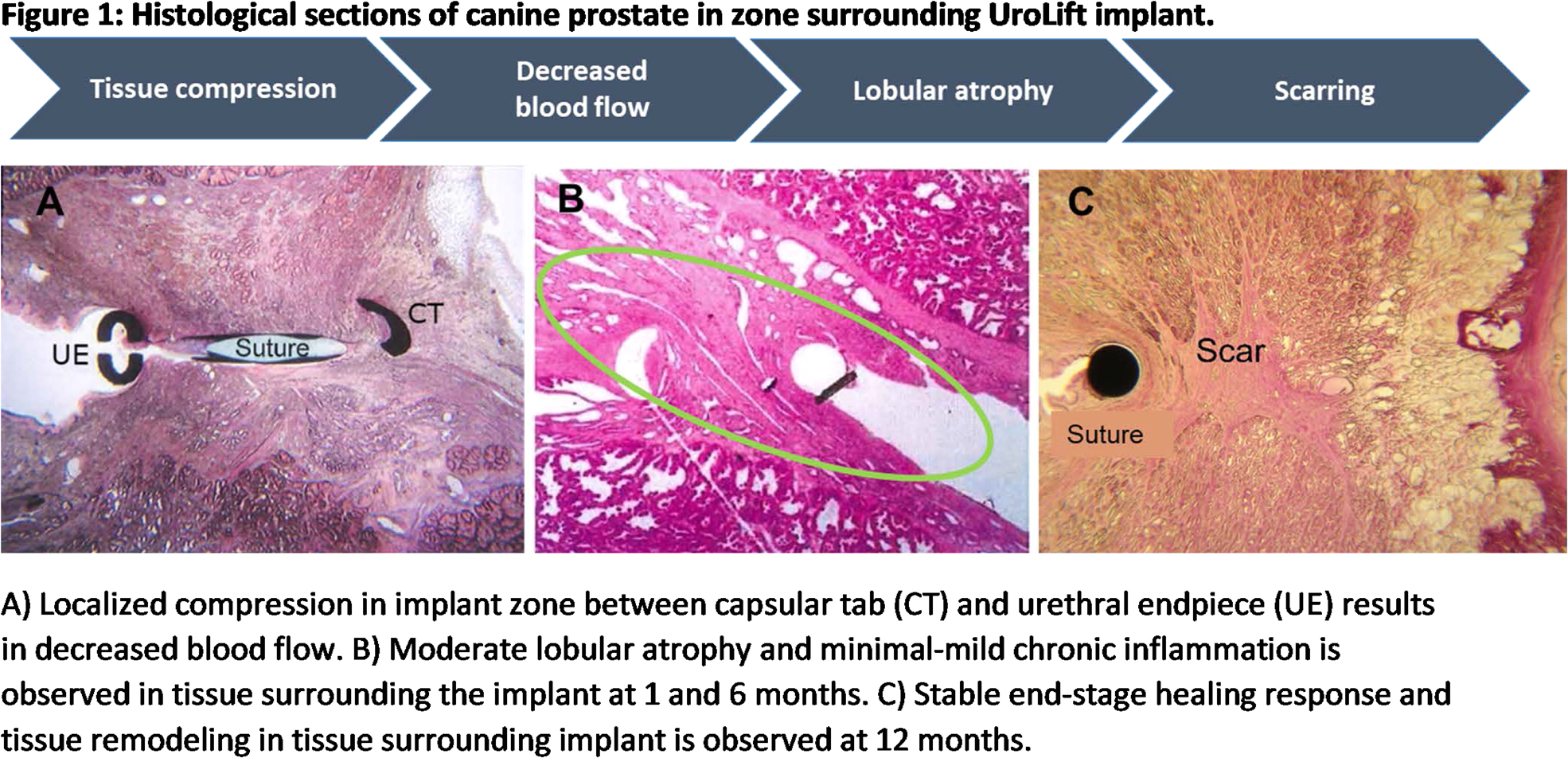
The UroLift® Implant Long‐Term Biological Mechanism Behind Relief from Prostatic Obstruction
CG Roehrborn, P Chin, H Woo
UT Southwestern
MP03‐07
Aquablation Outcomes in Superlarge Prostates
A Kasraeian, M Alcantara, K Mola Alcantara, S Sterious, N Patel, R Gonzalez, D Elterman, B Helfand, B Chughtai, L Kriteman, A Te
Kasraeian Urology
MP03‐08
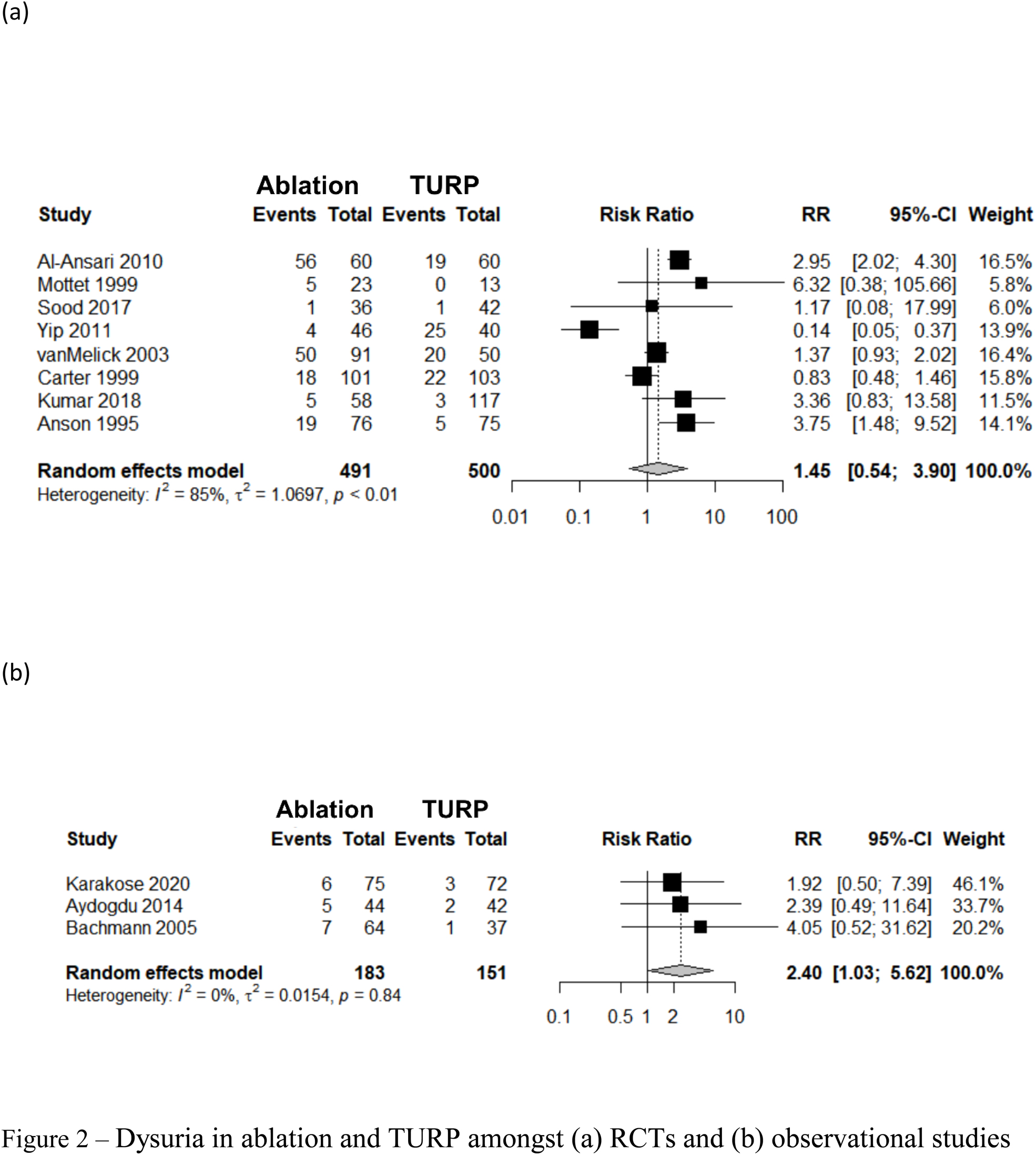
Post‐operative pelvic pain after prostate enlargement transurethral procedures: A systematic review and meta‐analysis
ML Wroclawski, D Castellani, F Heldwein, SB Teles, JD Cha, H Zhao, T Herrmann, V Vinson, J Teoh
School of Medicine, Faculty of Medicine and Health, University of Leeds, Leeds Department of Targeted Intervention, Division of Surgery and Interventional Science, University College London, London
MP03‐09
WATER vs WATER II: Three Year Comparison of Aquablation Therapy for Benign Prostatic Hyperplasia
D Nguyen, KC Zorn, N Bhojani
University of Montreal Hospital Center (CHUM)
MP03‐10
Withdrawn
MP03‐11
Withdrawn
MP03‐12
Prostatic Urethral Lift ‐ Influence of advanced techniques on benign prostatic enlargement patient pathway
A Dhanasekaran
Sandwell And West Birmingham NHS Trust
MP03‐13
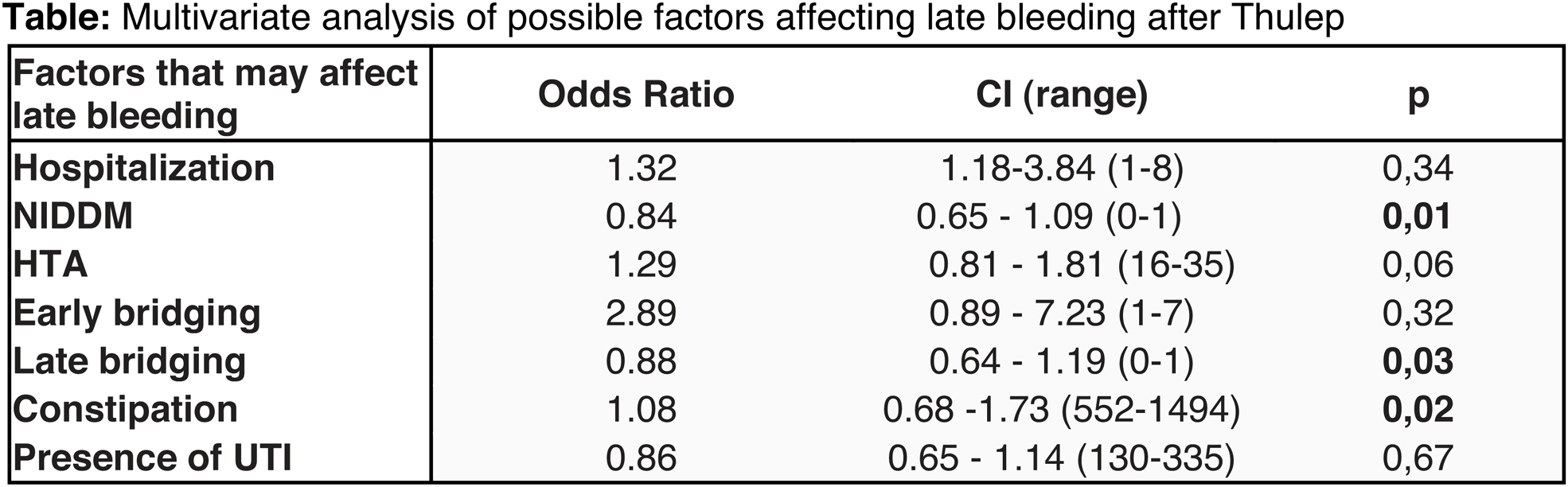
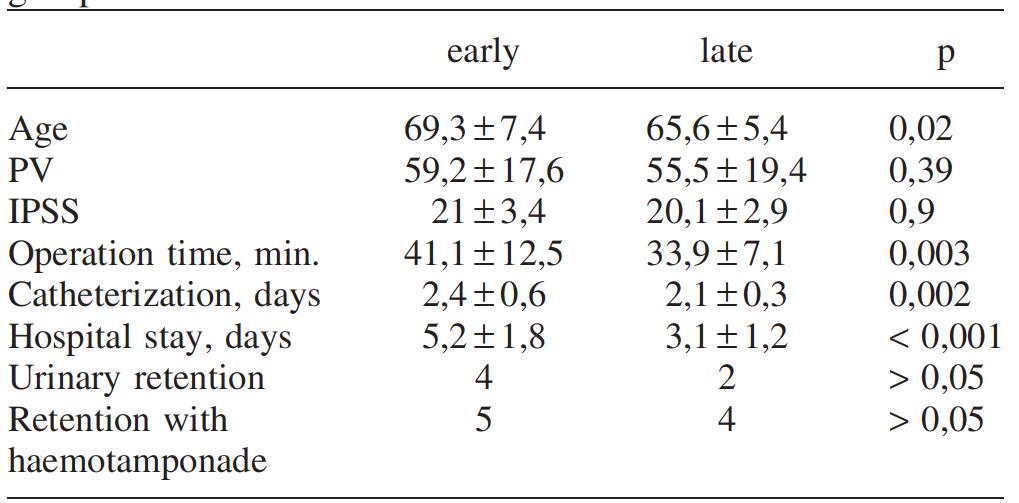
Prognostic factors predicting late bleeding after ThuLEP
M Maltagliati, L Berti, U Besana, A Calori, C Buizza, BC Rocco, S Micali, M Sighinolfi, G Bozzini
ASST Valle Olona
MP03‐14
Post Enucleation Morcellation procedure: Lights and Shadows
L Berti, M Maltagliati, P Marcangeli, A Calori, U Besana, C Buizza, M Sighinolfi, S Micali, BC Rocco, G Bozzini
ASST Valle Olona
MP03‐15
The Gold Standard Technique for Robotic‐Assisted Simple Prostatectomy: A Multi‐Institutional Assessment of Postoperative Urinary Function Outcomes
CU Okoro, M Lee, JY Lee, S Shekar, G Reyes, M Loecher, N Krishnan, AC Harbin, DD Eun
Department of Urology, Lewis Katz School of Medicine at Temple University
MP03‐16
Outcomes and Complications of bipolar enucleation by prostate size
JN Warner
City of Hope
MP03‐17
Outcomes Following Surgical Treatment of BPH in Patients with Neurologic Diseases
M Wahba, J Vetter, A Paradis, C Nottingham
Washington University School of Medicine
MP03‐18
Identifying Predictors of Antispasmodic use Following Robotic Assisted Simple Prostatectomy
JC Dai, TN Morgan, A Garbens, S Kusin, H Trivedi, H Kominsky, CG Roehrborn, JC Gahan
UT Southwestern
MP03‐19
Surgical Treatment of Large Gland BPH : A Comparison Between ThuLEP and Single Port Transvesical Robotic Simple Prostatectomy
S Talamini, HT Vigneswaran, MJ Zuberek, S Crivellaro
University of Illinois at Chicago
MP03‐20
Pivotal roles of macrophage recruitment and polarization in bladder outlet obstruction
W Wang, K Xiao, H Chen, L Zhou
MP03‐21
Minimally Invasive Surgical Treatment of Benign Prostatic Hyperplasia: A Systematic Review
A Ting, N Shanmugathas, C Khoo, T El‐Husseiny, H Abboudi
Imperial College Healthcare NHS Trust
MP03‐22
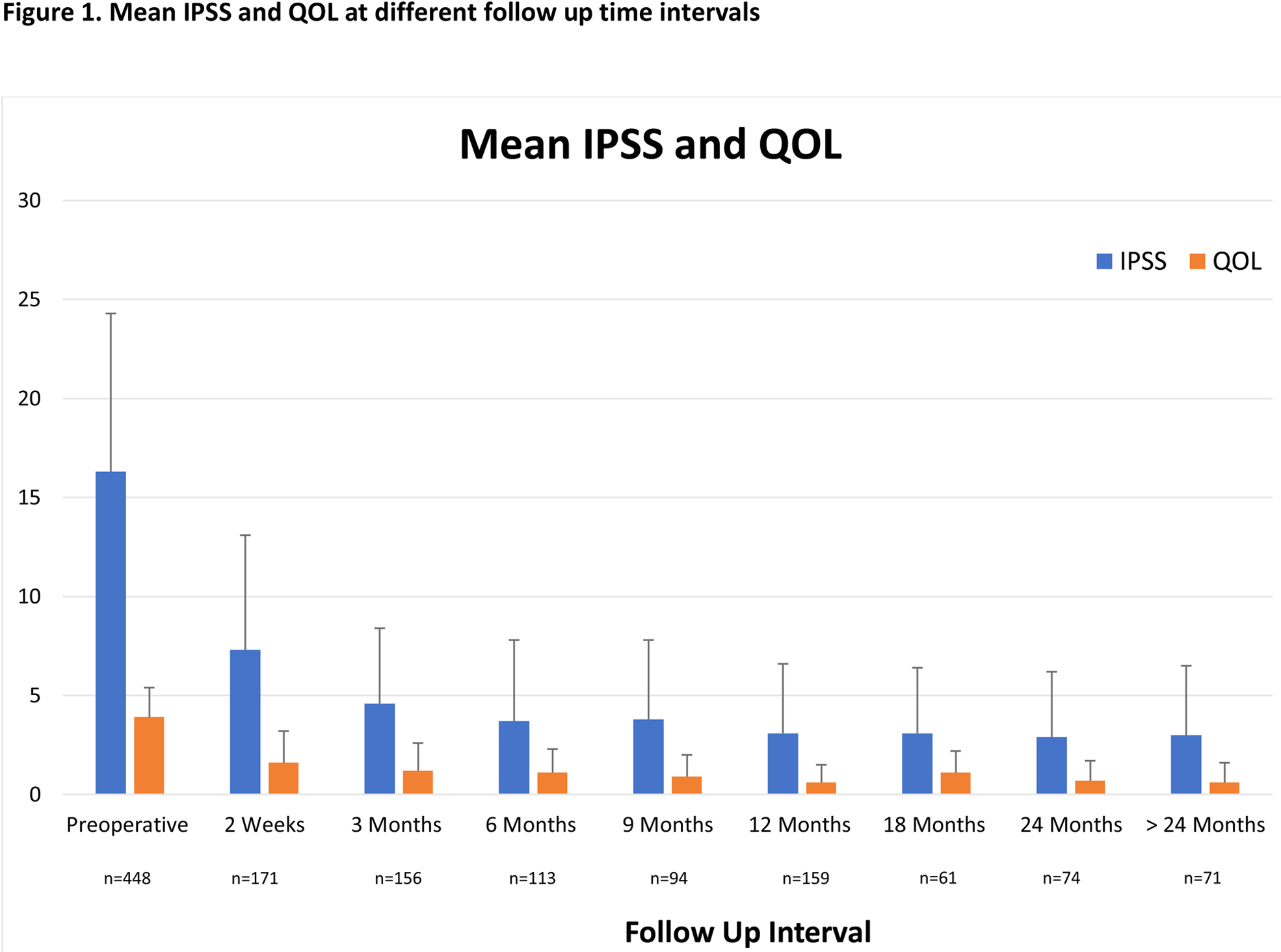
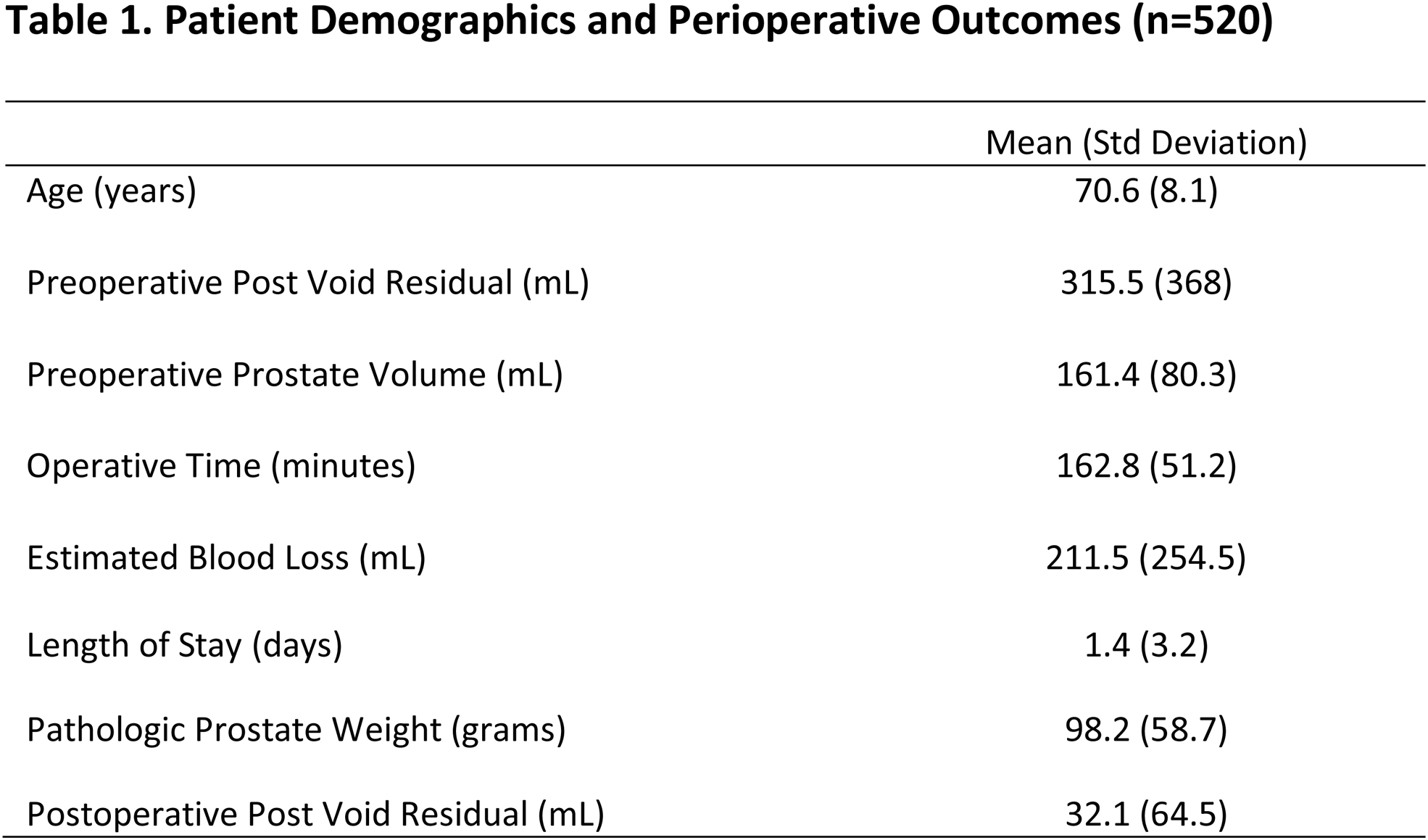
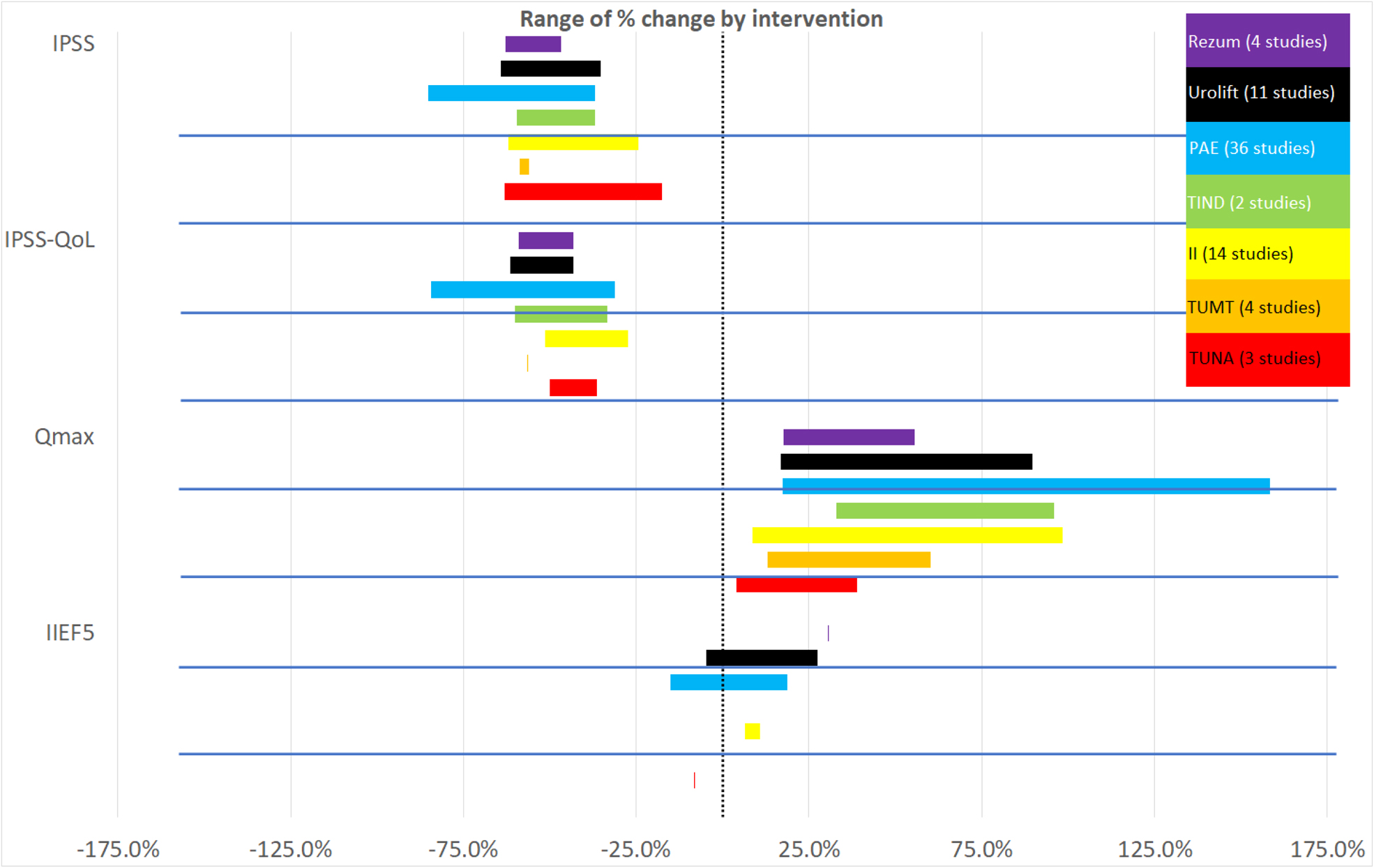
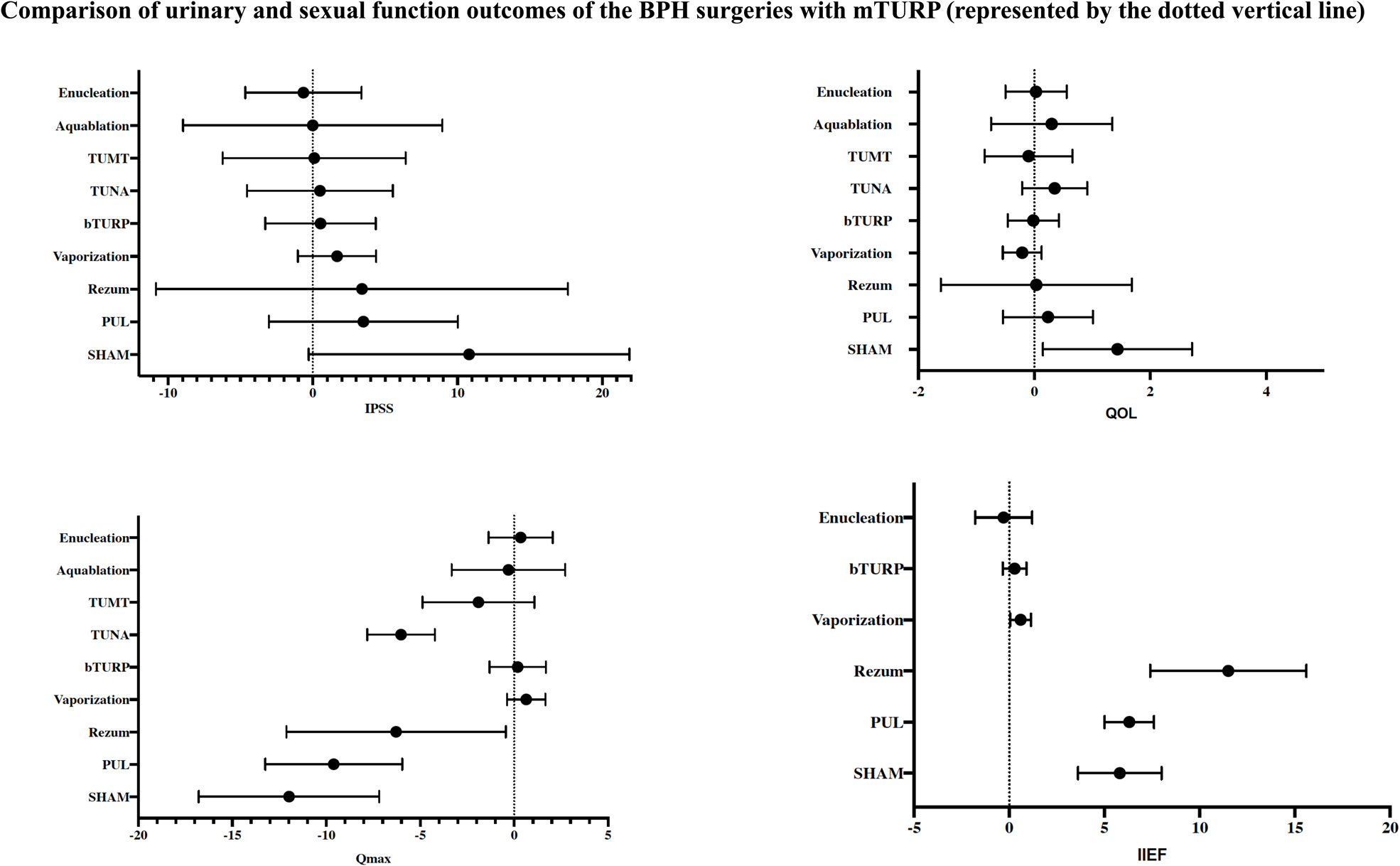
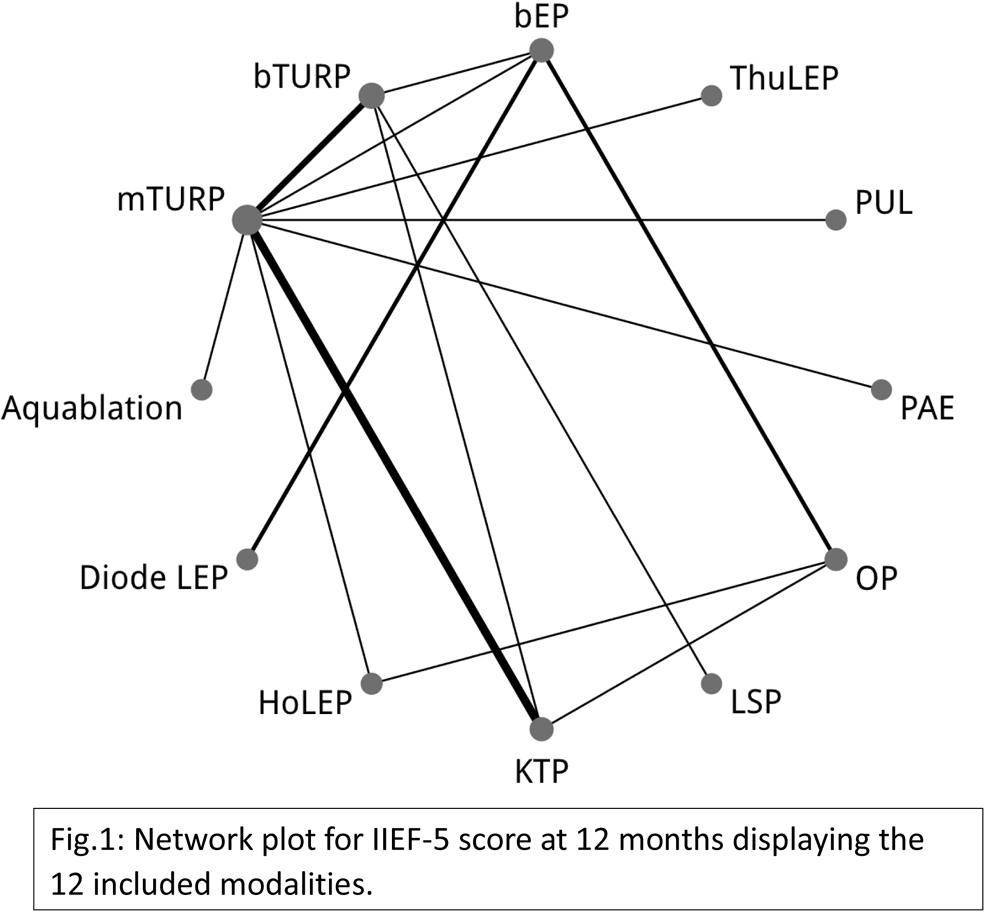
Minimally Invasive and Endoscopic Therapies of Benign Prostatic Hyperplasia (BPH): Head‐to‐Head Comparison of Short‐Term outcomes by Multiple Treatments (Network) Meta‐Analysis
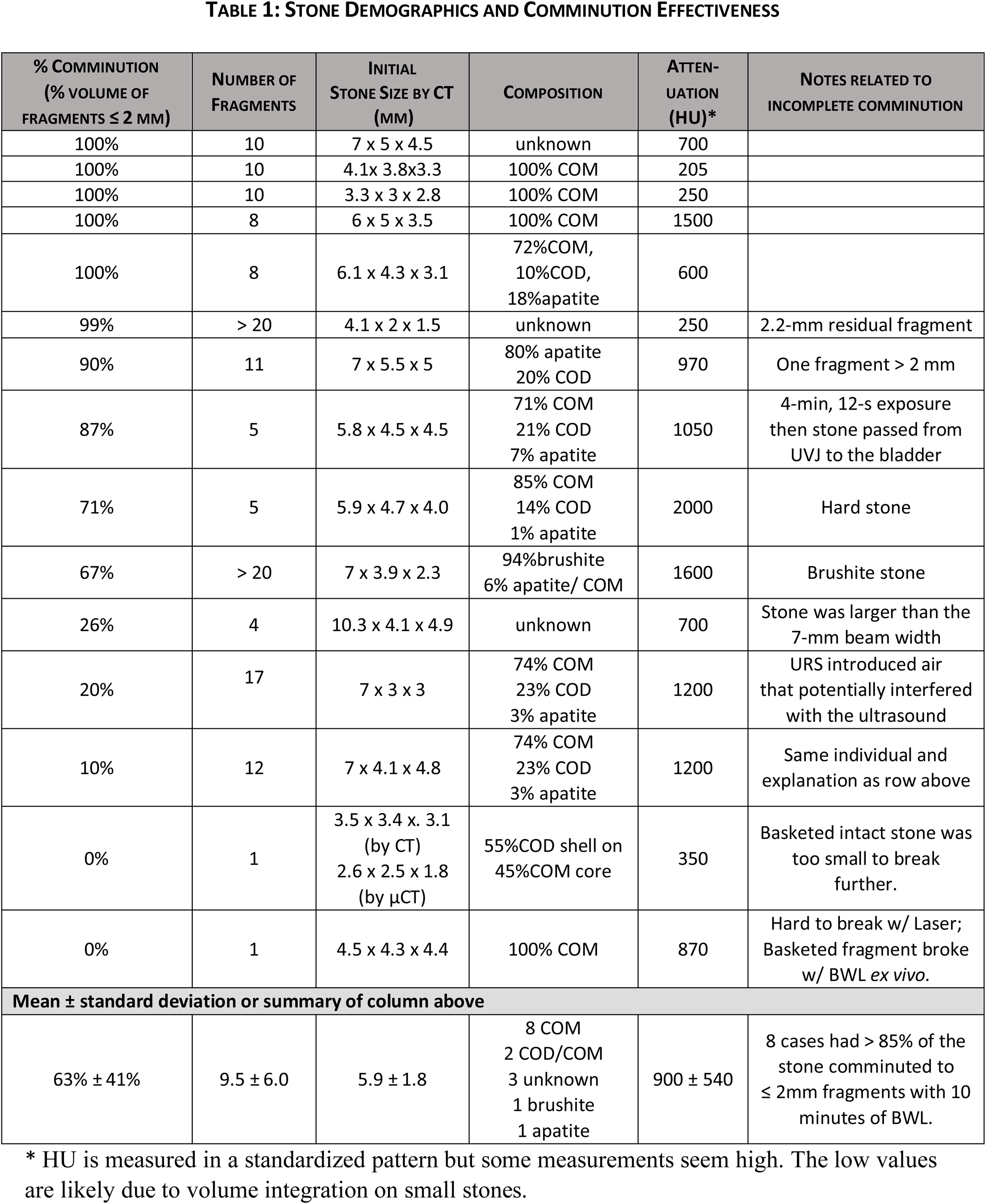
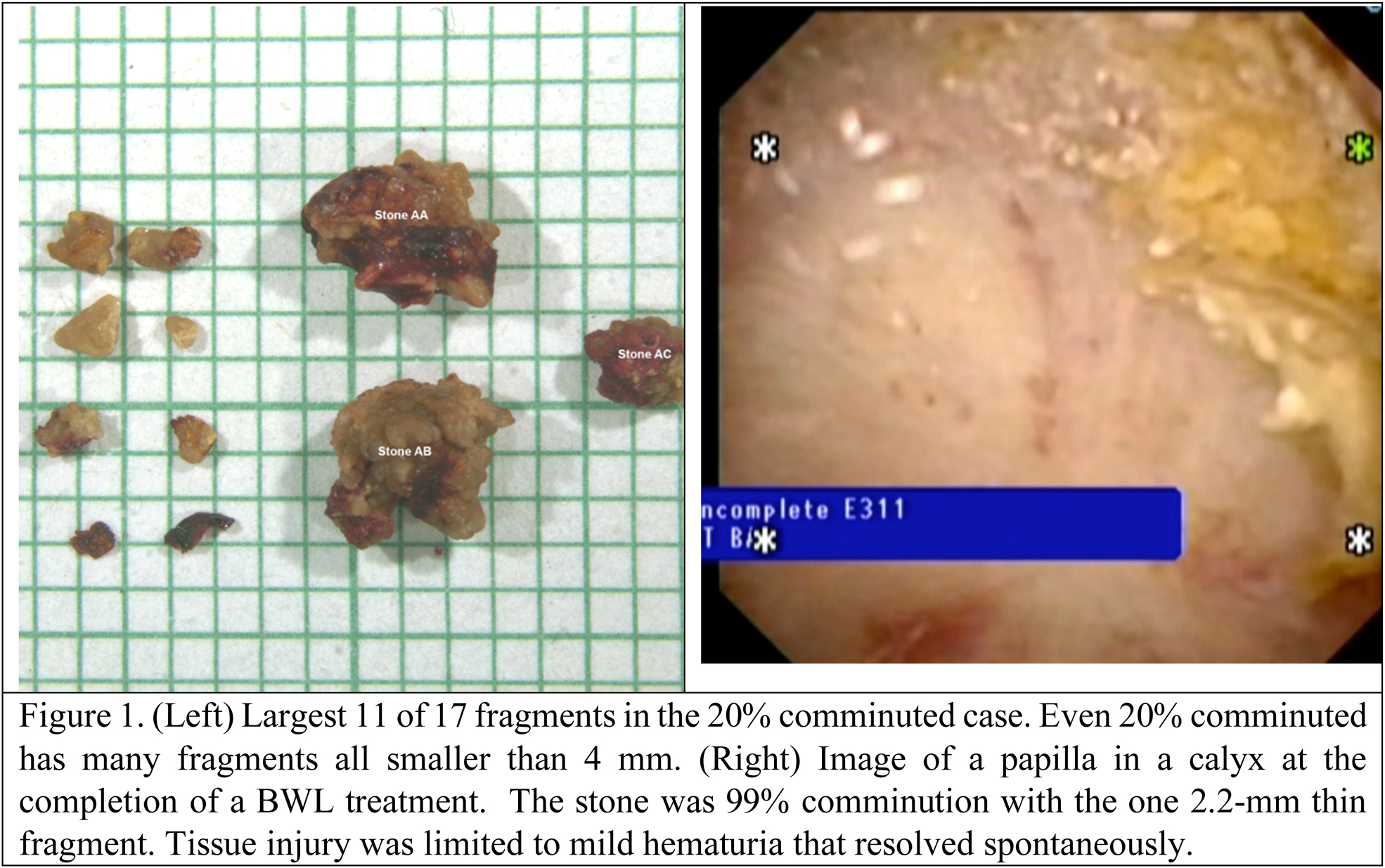
First comminution of stones in humans by burst wave lithotripsy
JD Harper, JE Lingeman, I Metzler, RM Sweet, P Sunaryo, JC Williams, AD Maxwell, J Thiel, B Cunitz, B Dunmire, MR Bailey, M Sorensen
University of Washington School of Medicine
MP04‐03
Comparison of Laparoscopic Pyelolithotomy versus Percutaneous Nephrolithotomy for the Treatment of patients with Staghorn Kidney Stones referred to Labbafinezhad hospital in 2019; a randomized clinical trial
M Soltani, S Farshid, R Valizadeh, N Ahmadian
MP04‐04
Complications after 4,500 flexible ureteroscopy (academic single center experience)
BF Geavlete, R Multescu, C Ene, C Bulai, PA Geavlete
“Saint John” Emergency Clinical Hospital, Department of Urology
MP04‐05
Role of stone size, stone density, and skin‐to‐stone distance by non‐ contrast computed tomography abdomen in predicting success of shock‐wave lithotripsy for kidney stones
A Hamid, A Ahmad, N Choh, S Malik, R Khawaja, M Wani
Department of Urology, SKIMS, Srinagar, Kashmir, India
MP04‐06
Upper Urinary Tract Stones: Evolution of Surgical Management Trends in Germany, France and England over the Past Decade
BW Turney, C Demaire, S Klöcker, H Sommerfeld, O Traxer
University of Oxford, Nuffield Department of Surgical Science, Department of Urology, Churchill Hospital
MP04‐07
The effect of smaller residual stones after minimal invasive endourology procedures for renal stones: prospective study
N Iqbal, A Hasan, S Imtiaz Ali, S Akhter
PKLI, Lahore, Pakistan
MP04‐08
Total Power is the Most Important Factor Determining Efficiency in Treatment of Large Bladder Stones
M Hajiha, AS Amasyali, M Keheila, J Groegler, A Goyne, D Baldwin, JD Belle, DD Baldwin
Loma Linda University, Department of Urology
MP04‐09
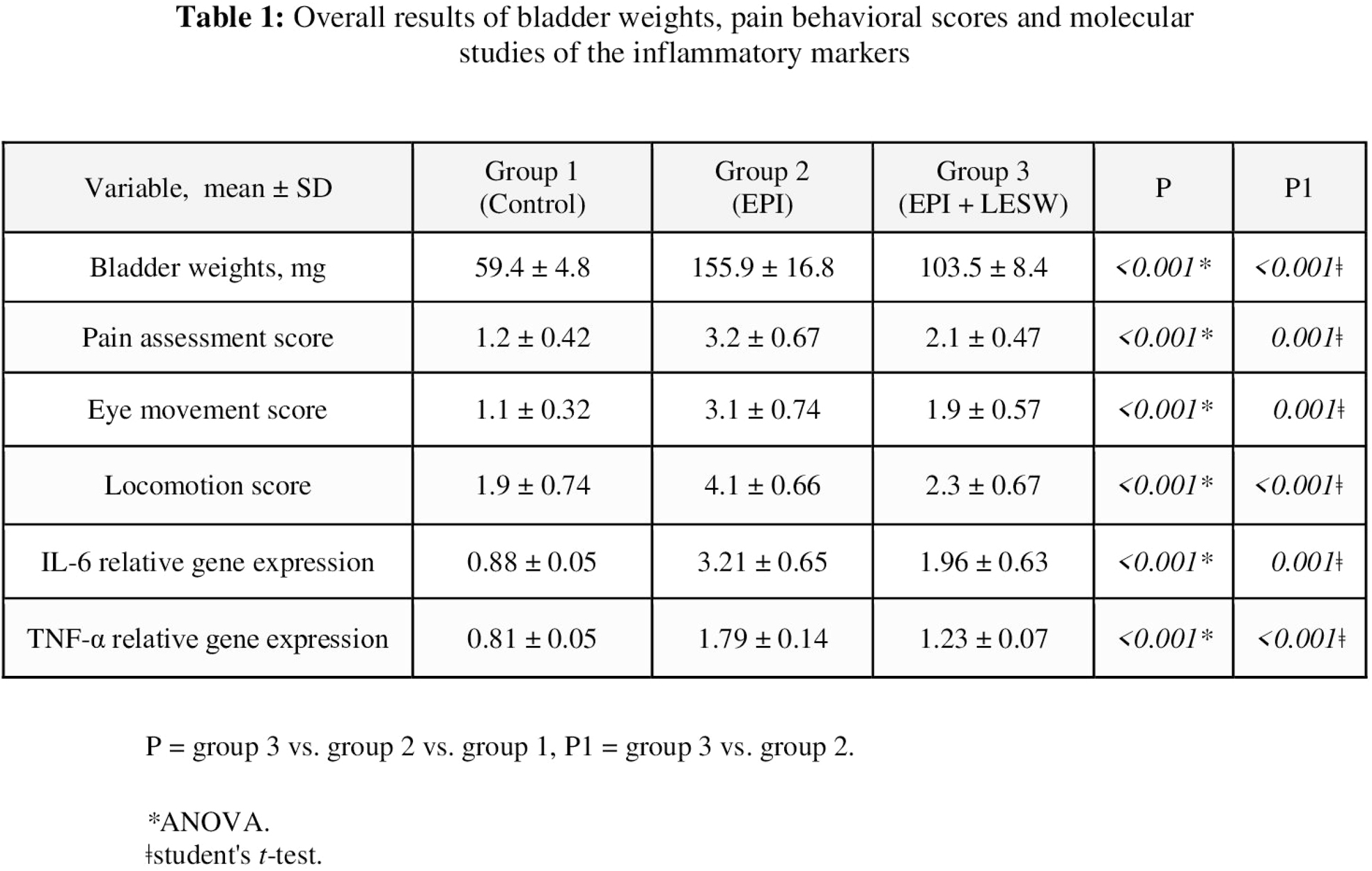
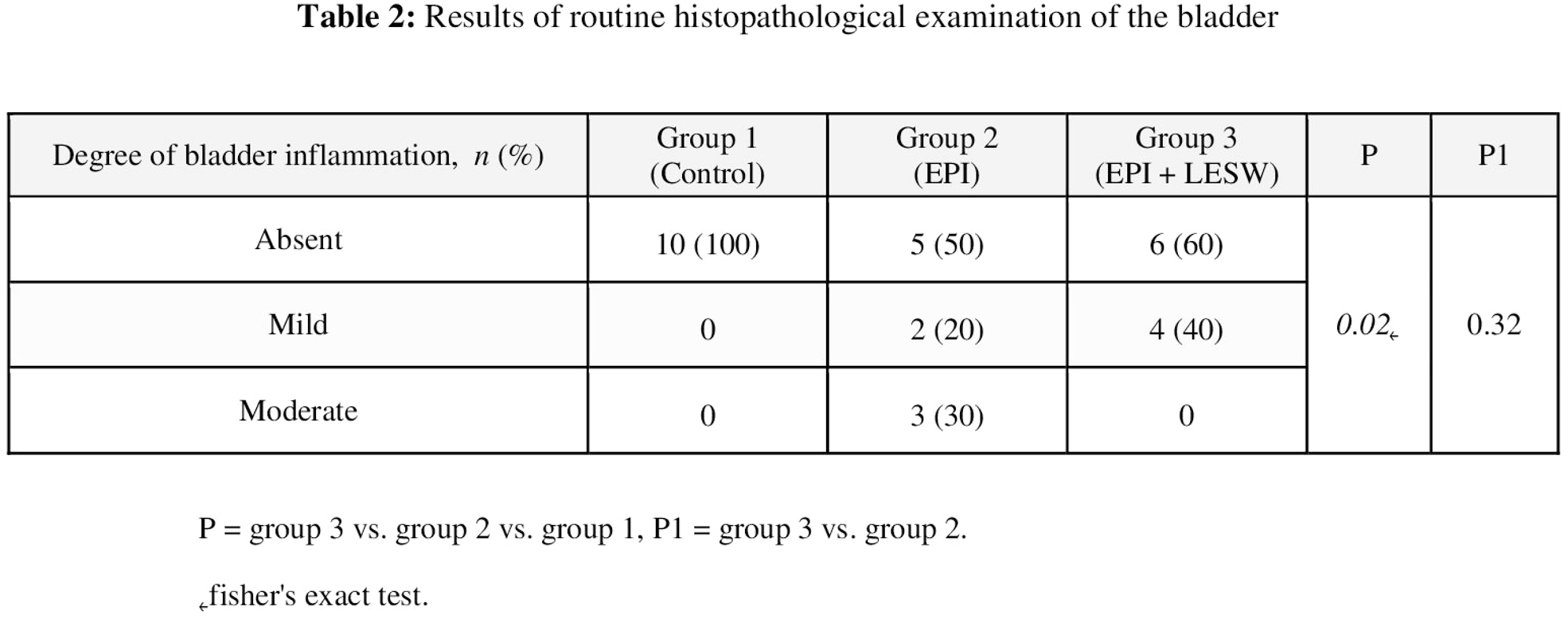
Effect of Low‐Energy Shock Wave Therapy on Behavioral, Histopathological and Molecular Changes in a Rat Model of Epirubicin‐Induced Cystitis
AH Elkashef, N Barakat, S Khater, A Awadalla, M El‐Ghar, A El‐assmy, K Sheir, A Shokeir
Department of Urology, Urology and Nephrology Center, Mansoura University, Egypt
MP04‐10
Short chain fatty acids reduce renal calcium oxalate stones by regulating oxalate transporters SLC26A3/6 in intestine
Y Liu, X Jin, Y Ma, Z Jian, L Zhou, L Xiang, Q Sun, H Li, K Wang
MP04‐11
Extracorporeal shockwave lithotripsy: a good option for treating distal ureteric stones
G Celentano, M Creta, G Cancelmo, F Mangiapia, M Marsicano, M Capece, R La Rocca, G Califano, C Collà Ruvolo, L Napolitano, S Morra, C Turco, C Imbimbo, V Mirone, N Longo
University of Naples Federico II
MP04‐12
External shockwaves lithotripsy a multi‐institutional international study
M Sighinolfi, M Benedetti, T Calcagnile, A Cassani, M Amato, G Saraceni, N Ferrari, G Bozzini, Z ahmed, E Ahmed, E Ahmed, D Cosimo, A Nacchia, P Fedelini, F Chiancone, S Ferretti, P Curti, G Bianchi, BC Rocco, S Micali
Azienda ospedaliero‐universitaria di Modena e Reggio Emilia, Modena, Italy
MP04‐13
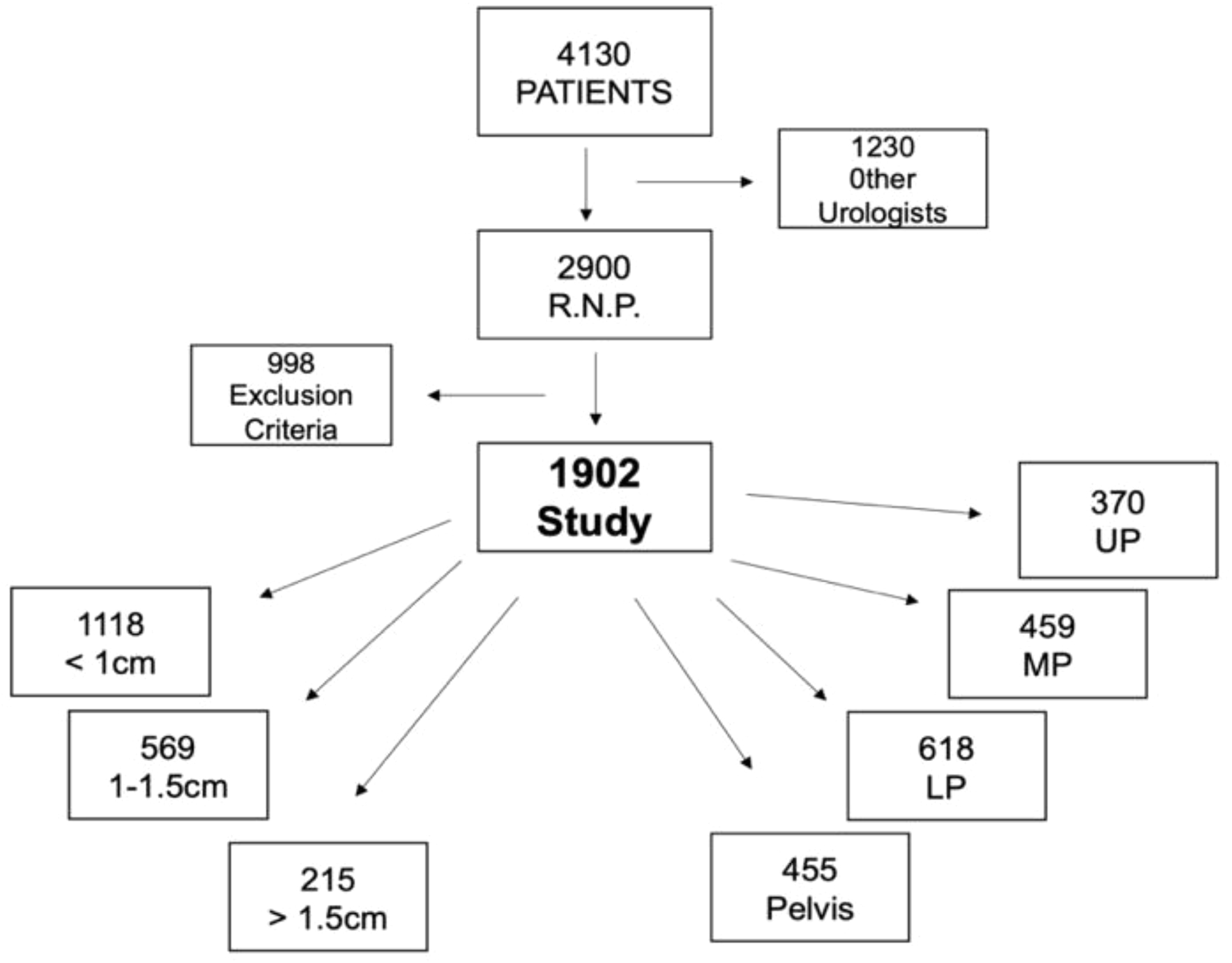
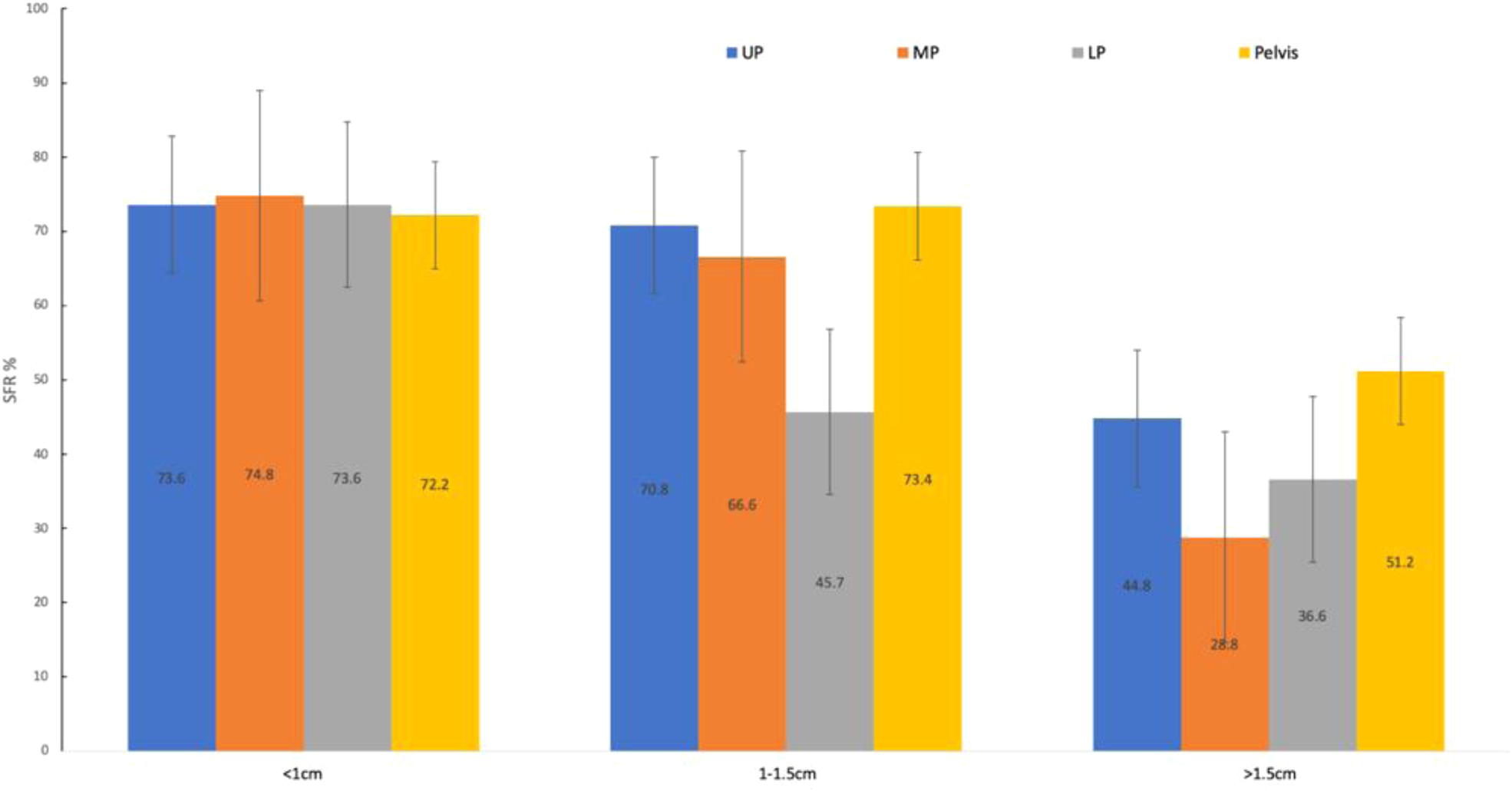
Is extracorporeal shock wave lithotripsy (ESWL) still suitable for >1.5cm intrarenal stones? Data Analysis of 1902 ESWLs
M Pachecco, E Soares Morales, R Nardi Pedro, L O. Reis, W Azal Neto, L Castro Santos
Endourology Staff UNICAMP, AME/SBO Lithotripsy Center Coordinator, Professor Faculdade São Leopoldo Mandic, Medicine
MP04‐14
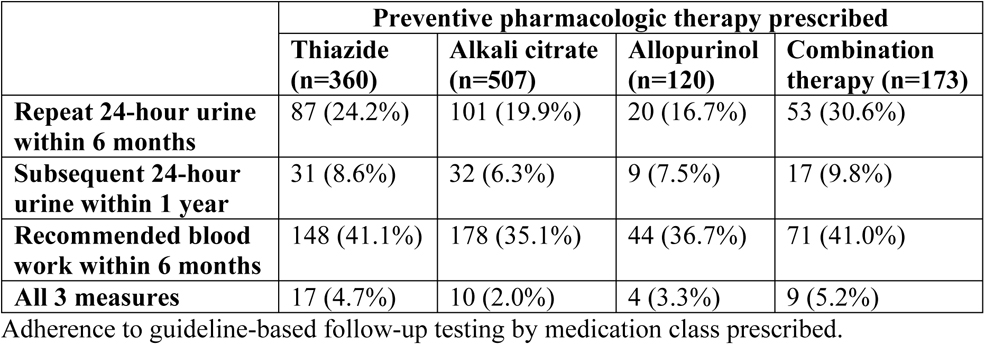
The benefit of obtaining 24‐hour urine testing before prescribing preventive pharmacological therapy to patients with high‐risk urinary stone disease
R Hsi, P Yan, J Crivelli, V Shahinian, JM Hollingsworth
Vanderbilt University School of Medicine
MP04‐15
Shockwave Lithotripsy for Distal Ureteric Stones ‐ Results from the Endourological Society T.O.W.E.R. Research Initiative
F Gabrigna Berto, H Razvi, J Bjazevic, VK Wong, L Nott, M Hossny, R Dasgupta, PJ Osther, BW Turney, BH Chew
Western University
MP04‐16
How Necessary is Post‐Operative Ultrasound Imaging for Ureteroscopic Stone Procedures?
N O'Connell, C Ashley, Z Yasen, R Peggs, J Stephenson, T Tien, R Oliver, P Pal, S Graham
Barts Health NHS Trust
MP04‐17
Using Artificial Intelligence to Identify Stones on SWL Intra‐Operative Fluoroscopic Images
RG Seltzer, D Soetemans, I Okwuchi, BD Hamilton, SY Nakada
Translational Analytics and Statistics
MP04‐18
Medical Impulsive Therapy: Early results from a Randomized Controlled Trial to evaluate tamsulosin use before ureteral access sheath deployment
V Dall'Aqua, A Lopes Neto, A Rodrigues, M Mattos, L Costa, S Glina
MP04‐19
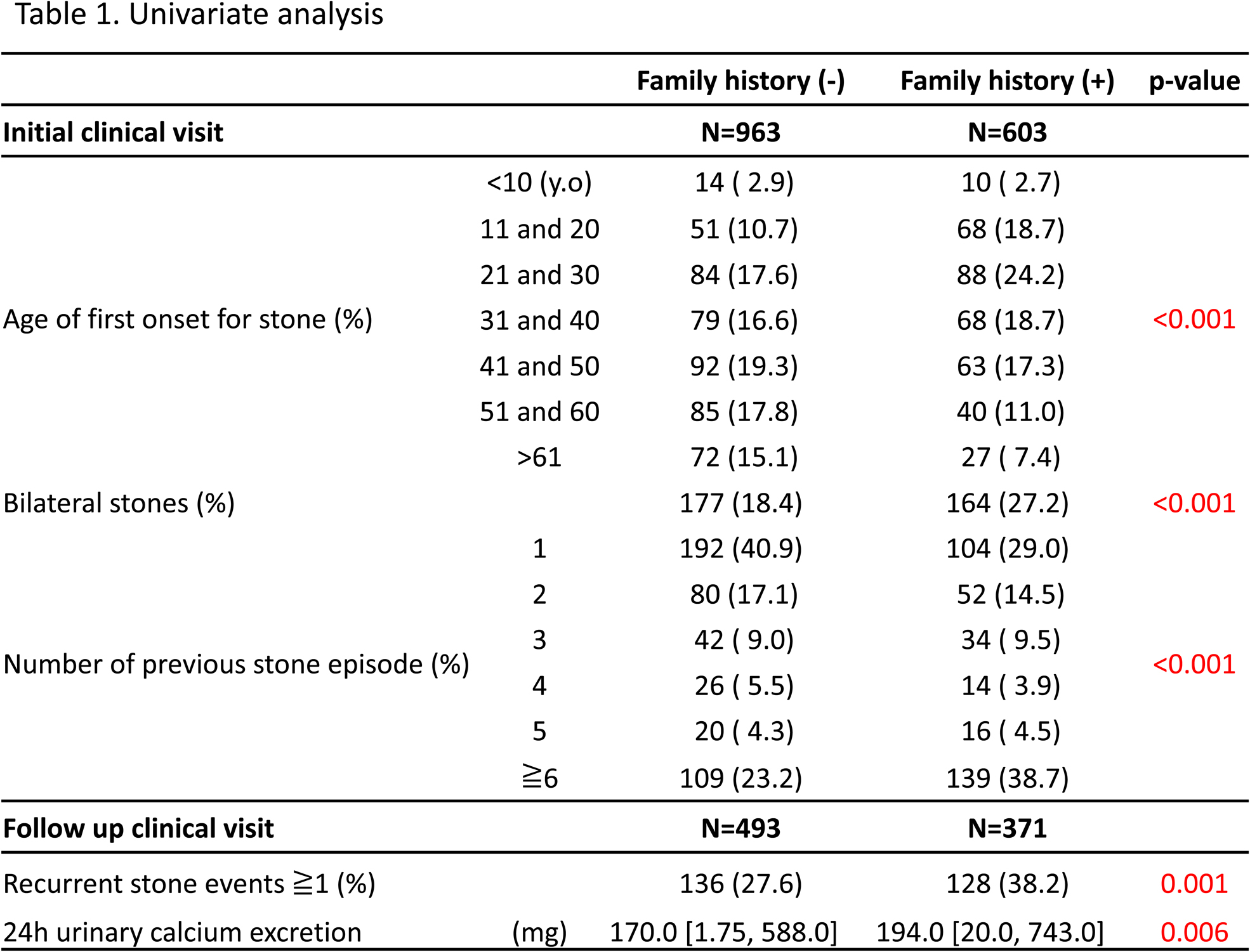
Maternal family history of urolithiasis is associated with earlier onset of urinary stone disease: results from ReSKU
R Unno, K Taguchi, M Usawachintachit, H Yang, F Hamouche, J Ahn, D Bayne, M Stoller, T Chi
University of California San Francisco
MP04‐20
Extracorporeal shock wave lithotripsy in patients with spinal cord injury: have contemporary outcomes improved?
MS Yassin, BW Turney, JS Reynard
Oxford University Hospitals NHS Foundation Trust
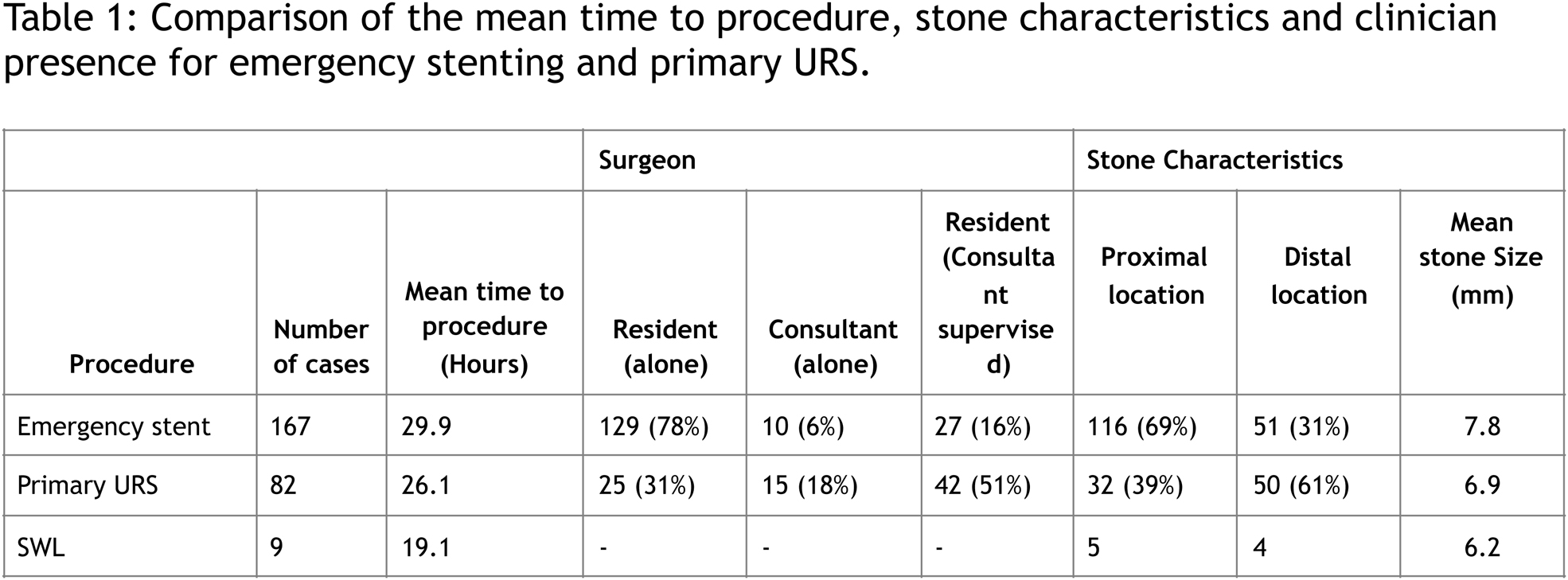
MP04‐21
Emergency Ureteroscopy Service Reduces Patient morbidity and need for secondary procedures in Acute Stone Patients
A Jha, C Ho, S Lee, S Albuheissi, F Keeley, A Timoney, J Philip
Bristol Urology Institute
MP04‐22
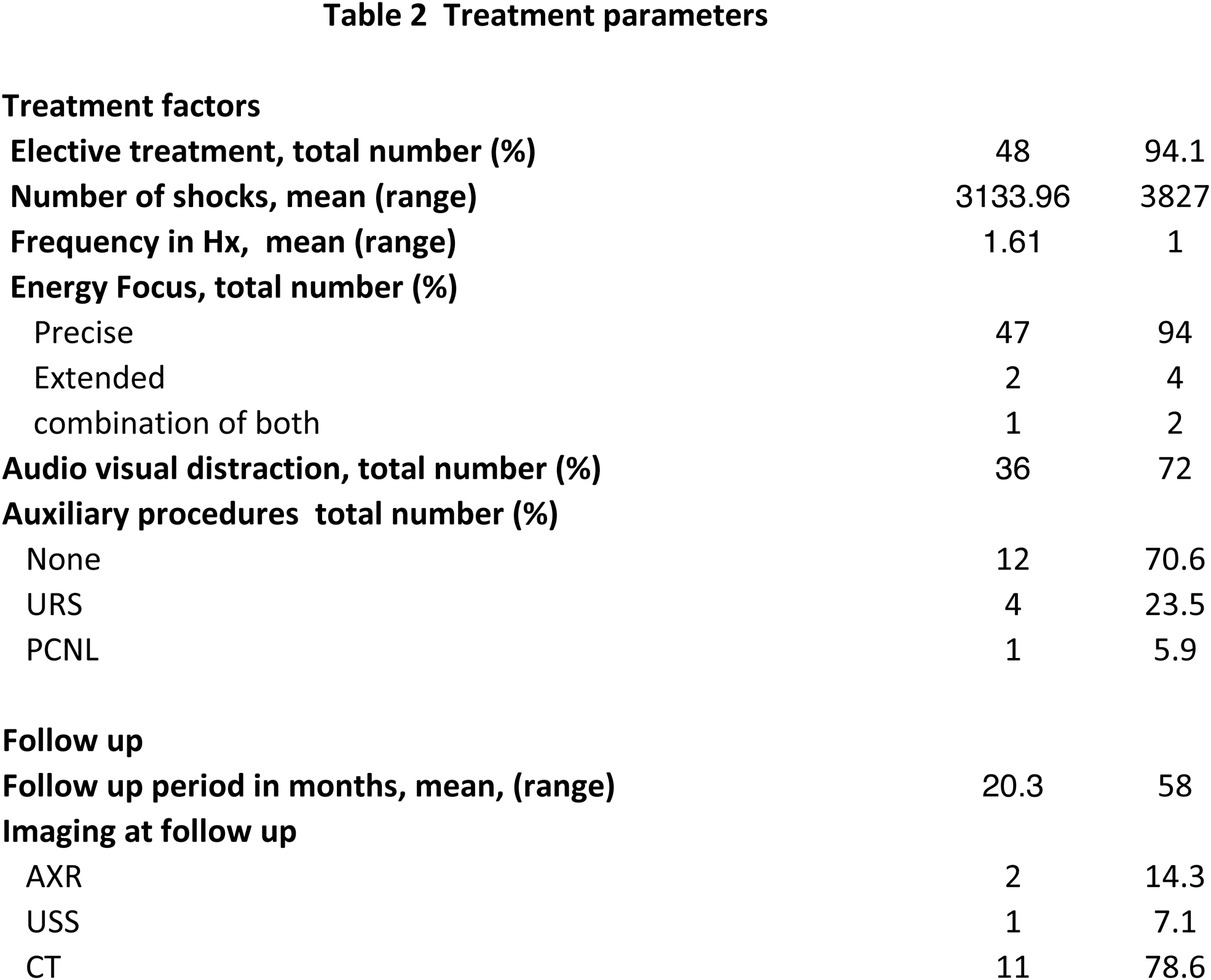
Matched Pair Analysis of Extended versus Precise Focus Shockwave Lithotripsy for Urolithiasis
AJ Sharp, CE Lovegrove, R Sreekumar, M Spencer, BW Turney, SA Howles
Suction Assisted Mini Percutaneous Nephrolithotomy as a day care procedure for medium sized renal stones
MS Agrawal, D Mishra
Global Rainbow Hospital, Agra, India
MP05‐02
Comparison of pain scores and recovery after Percutaneous Nephrolithotomy in patients with and without regional anesthesia block. Prospective Randomized controlled study
N Iqbal, A Hasan, S Imtiaz Ali, J Rahim, S Akhter
PKLI, Lahore, Pakistan
MP05‐03
Withdrawn
MP05‐04
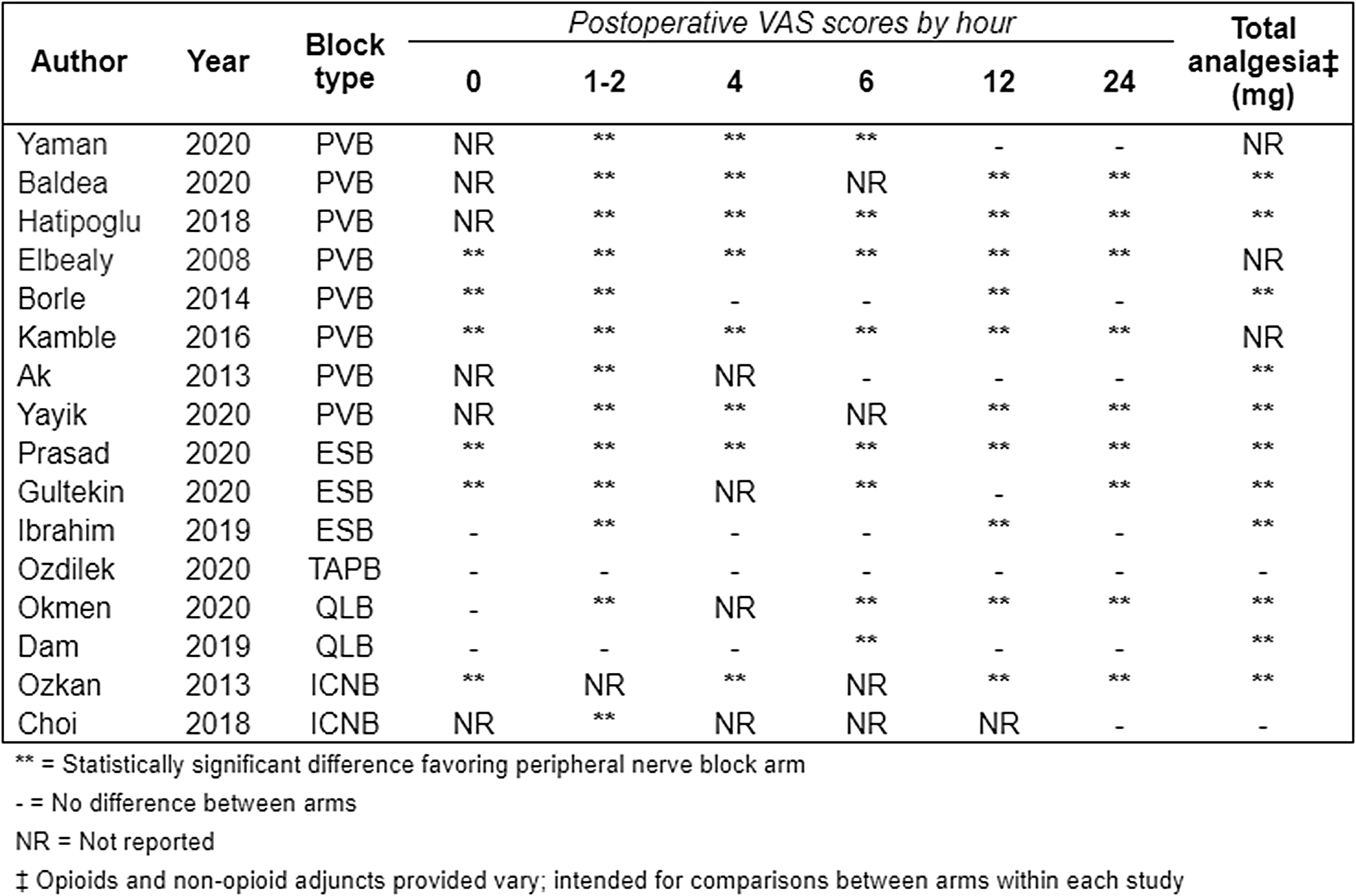
The Use of Peripheral Nerve Blocks Provides a Significant Opioid‐Sparing Analgesic Effect for Percutaneous Nephrolithotomy: A Systematic Review
R Alam, K Koo, BR Matlaga, JS Winoker
Johns Hopkins University School of Medicine
MP05‐05
Withdrawn
MP05‐06
Feasibility of a Non‐opioid Pathway Post Ureteroscopy: Joint Analysis from Two Academic Centers
M Awad, M Assmus, a Berg, M Lee, L Hallgarth, AE Krambeck, K Sternberg
Northwestern University, Department of Urology
MP05‐07
The effect of topical tranexamic acid on postoperative hemoglobin level in patients undergoing PCNL
S Farshid, V Rezvankhah, N Ahmadian, M Sadri
MP05‐08
Safety and feasibility of intraoperative real‐time digital stone fragment measurement during ureteroscopy
R Becker, K Koo, T Aro, JS Winoker, S Lim, D Petrisor, D Stoianovici, BR Matlaga
James Buchanan Brady Urological Institute, The Johns Hopkins Medical Institutions
MP05‐09
In‐Vivo Porcine Evaluation of the Thermal Effects of the Superpulse Thulium Laser Lithotripsy during Ureteral Stone Laser Lithotripsy
P Jiang, A Peta, M Ayad, A Brevik, K Larson, Z Okhunov, RM Patel, T Farzaneh, J Landman, RV Clayman
Department of Urology, University of California, Irvine
MP05‐10
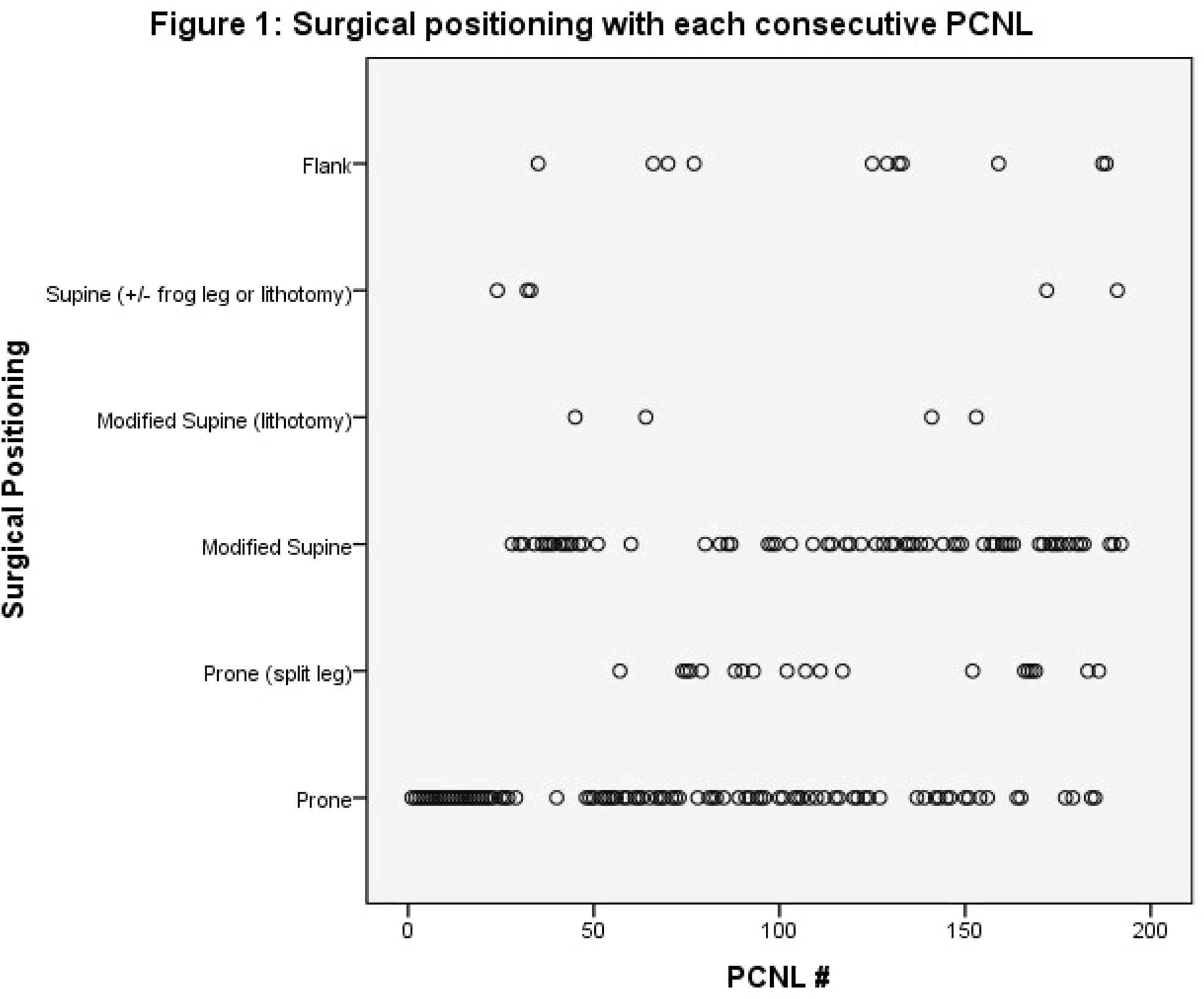
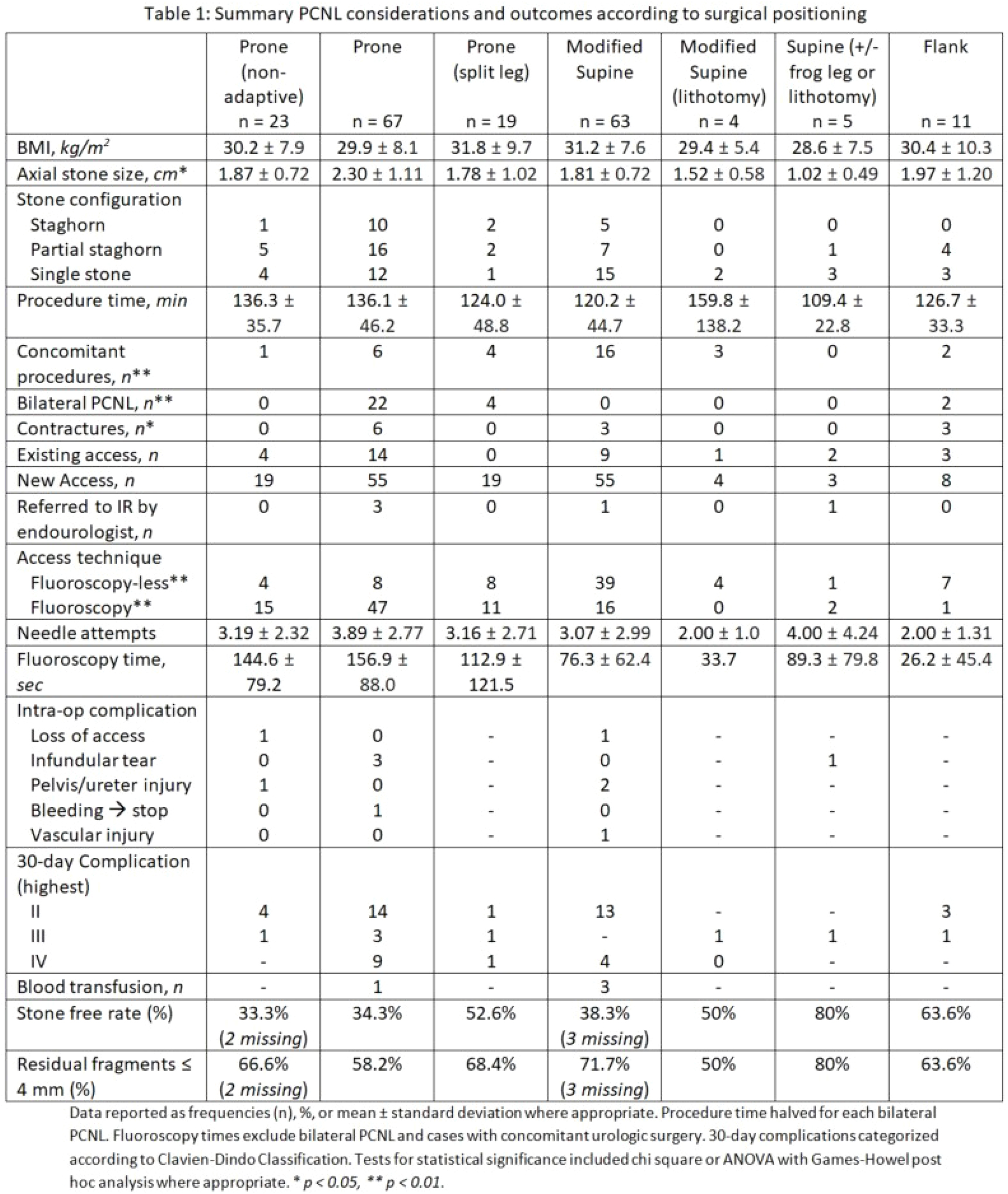
Adaptive Percutaneous Nephrolithotomy: Modifying Positioning & Access for Each Patient
N Nimmagadda, CM Forbes, NL Kavoussi, R Hsi
Vanderbilt University Medical Center, Department of Urology
MP05‐11
Holmium laser lithotripsy with Moses™ Technology in percutaneous nephrolithotomy: preliminary results from a comparative study
E Lievore, S Zanetti, M Turetti, L Boeri, M Fontana, A Gallioli, F Longo, E De Lorenzis, G Albo, E Montanari
Dept. of Urology, Foundation IRCCS Ca' Granda Ospedale Maggiore Policlinico, Milan
MP05‐12
Factors affecting the ability to offer emergency primary ureteroscopy in a tertiary teaching hospital
C Fontaine, R Sehgal, Y Abu‐Ghanem, L Forster, G Ellis, P Singh, R Kucheria, A Goyal, D Allen, L Ajayi
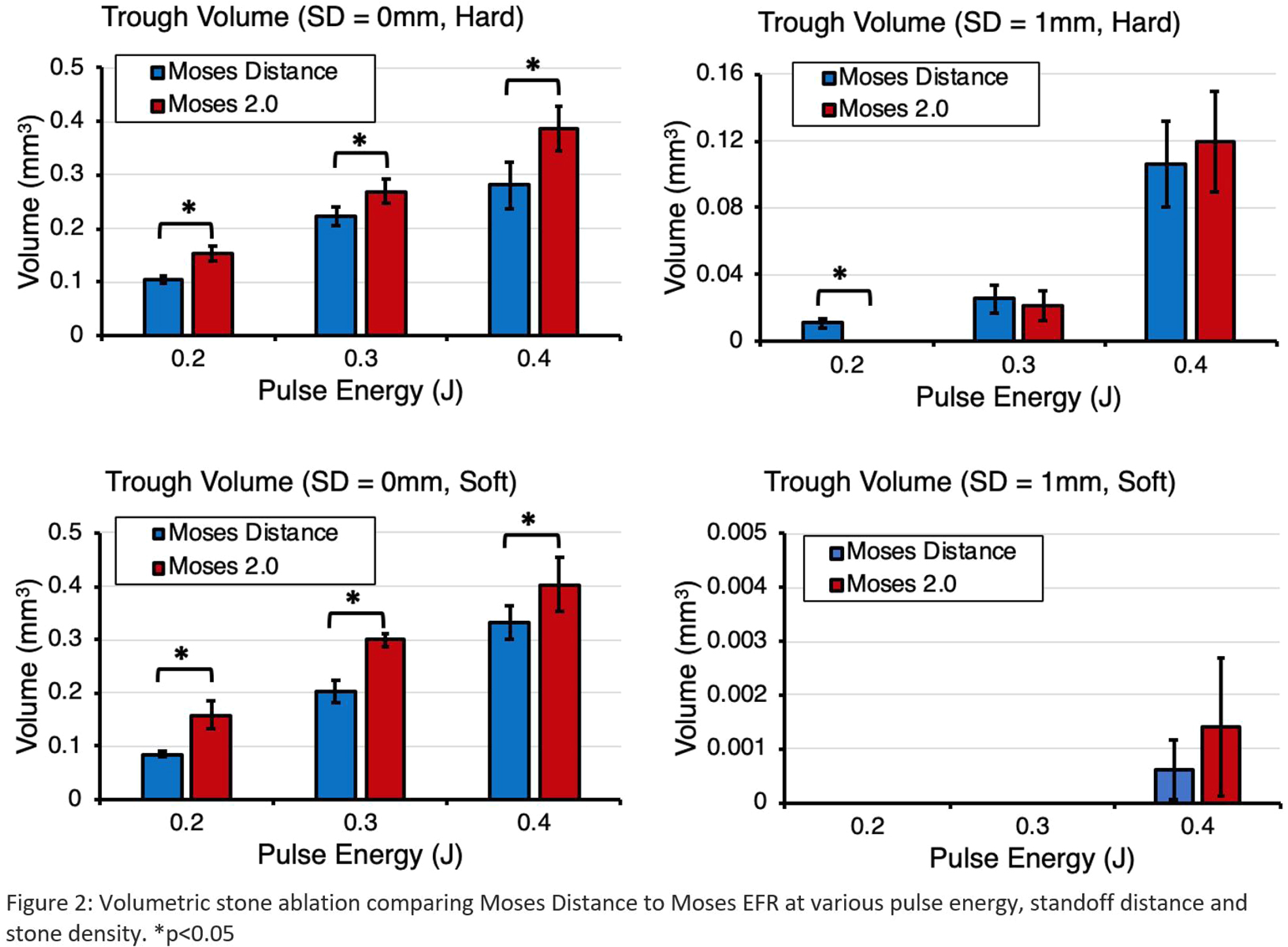
MP05‐13
Dusting Efficiency of the Moses Pulse 120H 2.0 Laser System: An In vitro Assessment
P Whelan, CJ Kim, D Ho, C Tabib, F Soto‐Paulo, J Chen, P Zhong, GM Preminger, M Lipkin
Duke University
MP05‐14
Reducing the rate of negative ureteroscopy: predictive factors and the role of pre‐ureteroscopy imaging
AC Brodie, TJ Johnston, P Lloyd, L Hemsworth, S Keoghane, M Barabas
MP05‐15
Risk of unplanned postoperative re‐admissions in children undergoing ureteroscopy: a post‐hoc analysis of the pediatric National Surgical Quality Improvement Program database
Y Ding, J Davidson, EP Chan, J Bjazevic, G Filler, S Dave, Z Wang
Western University
MP05‐16
Mini percutaneous nephrolithotomy using SuperPulse Thulium Fiber Laser: Evaluation of clinical efficacy and safety
DA Sytnik, S Popov, I Orlov, I Pazin, M Suleymanov, A Kulikov
St. Luke's Clinical Hospital
MP05‐17
Micro‐ureteroscopy for treatment of mid and upper ureteral stones and kidney stones in pediatric patients younger than 3 years
R Zhan, Y Ge, W Wang
beijing friendship hospital
MP05‐18
Ambulatory Percutaneous Nephrolithotomy Performed in a Free‐Standing Surgery Center: Outcomes of 1000 Cases
MM Dunne, N Ariasvillela, JE Abbott, J Davalos
Chesapeake Urology, Univeristy of Maryland Baltimore Washington Medical Center
MP05‐19
Cost‐Analysis of Mini‐Percutaneous Nephrolithotomy (PCNL) and Standard Tract PCNL for Stone Burden Greater/Less Than 20 mm in an Ambulatory Setting
MM Dunne, J Chong, B Magnan, J Davalos
Chesapeake Urology, Univeristy of Maryland Baltimore Washington Medical Center
MP05‐20
Ambulatory PCNL may be cost‐effective compared to Standard PCNL
MS Lee, M Assmus, DK Agarwal, ME Rivera, T Large, AE Krambeck
Northwestern University Feinberg School of Medicine
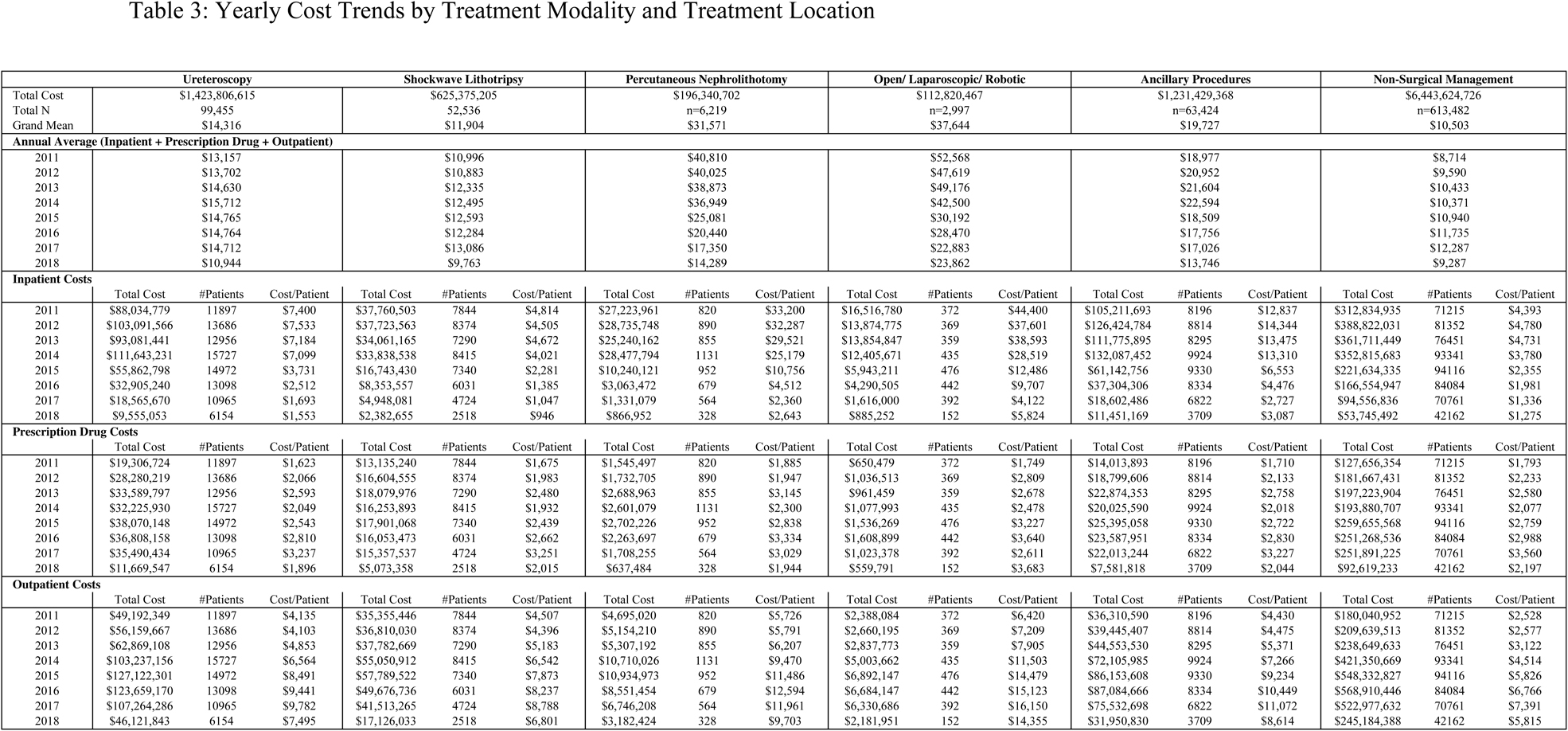
MP05‐21
Economic Burden of Urolithiasis Management in United States Adults 2011‐2018: Analysis of Surgical vs. Non‐Surgical Interventions
E Olweny, A Becerra, JA Khusid, M Sturgis, L Fink, M Gupta, B Konety
Rush University Medical Center
MP05‐22
Determinants of ureteral patency after percutaneous nephrolithotomy
H Lee, H Yang, R Unno, F Hamouche, J Ahn, D Bayne, M Stoller, T Chi
Moderated Poster Session 06: Stones III: New Technology/Outcomes
MP06‐01
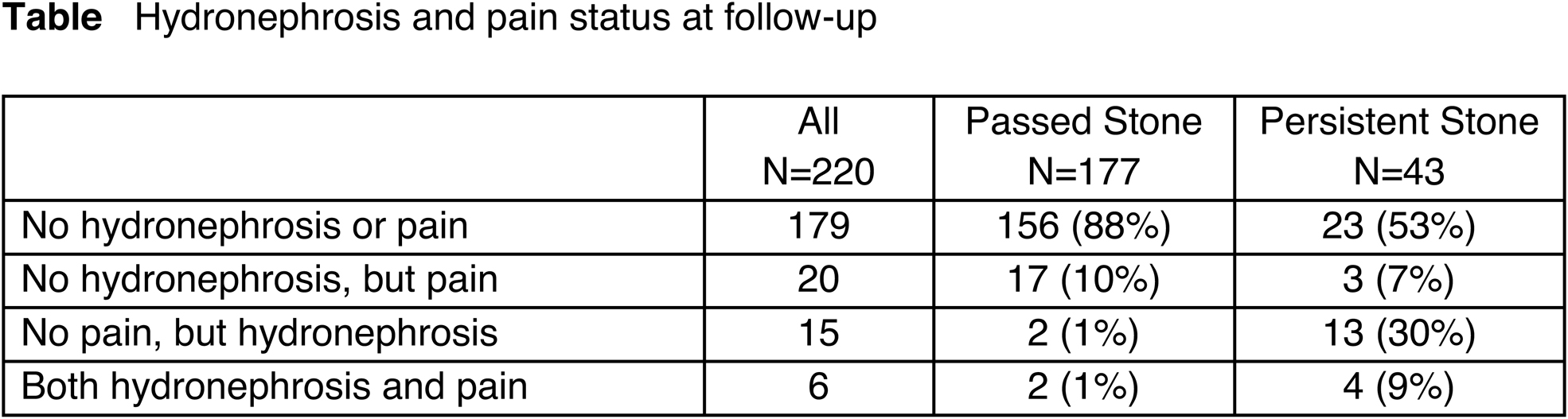
Resolution of Hydronephrosis and Pain to Predict Stone Passage for Patients with Acute Renal Colic: Analysis from the STONE trial
S Jackman, A Maganty, A Wolfson, P Burrows, C MacPherson, N Montano, Z Kirkali, A Meltzer
UPMC
MP06‐02
Visual clarity of irrigants used during flexible ureterorenoscopy: an in vitro comparison
V Ulker, Z Gulerce, O Celik, C Yucel, E Can, B Turna
Department of Urology, University of Health Sciences Izmir Tepecik Training and Research Hospital
MP06‐03
Chloroquine attenuates hyperoxaluria‐induced renal oxidative injury and calcium oxalate crystal depositions via inhibiting NADPH oxidases
X Duan, S Yin, Y Liu, G Zeng
MP06‐04
Automatic computer‐aided in‐situ recognition of morphological features of pure and mixed urinary stones using intraoperative endoscopic images
V Estrade, M Daudon, F Bladou, J Bernhard, G Robert, B Denis De Senneville
Chu Pellegrin
MP06‐05
Postoperative Urinary Tract Infections After Flexible Ureteroscopy Using High‐Level Disinfection With 2 % Glutaraldehide for Flexible Scopes
P Alarcon, E Flores, EE Lozada, S Hector, BO Manzo
Hospital Regional de Alta Especialidad del Bajío
MP06‐06
A critical assessment of digital single‐use flexible ureteroscopes in a porcine model
SK Bechis, B Eisner, BR Matlaga, O Shah
University of California ‐ San Diego, Department of Urology
MP06‐07
Predictive factors for ureteric stricture formation after ureteroscopic treatment of impacted ureteric stones
M Ramachandra, Z Al‐Nabulsi, Y Phan, P Osborn, A Auer, C Rowbotham, M Ismail
University Hospital Southampton, UK
MP06‐08
Prospective randomized comparison of classical retroperitoneoscopic pyelolithotomy versus percutaneous nephrolithotomy for solitary large pelvic kidney stones
V Singh, RJ Sinha, G Singh
Dept of urology, King George Medical University
MP06‐09
Endoscopic Combined Intrarenal Surgery (ECIRS)–The new standard in the treatment of complex stone disease?
J Correia, M Madanelo, B Teixeira, G Mendes, S Mesquita, A Fraga, M Silva‐Ramos, V Cavadas
Department of Urology, Centro Hospitalar Universitário do Porto
MP06‐10
A preoperative predictive score for uric acid kidney stones
MJ Basulto‐Martínez, S Proietti, M Pavia, L Rico, Y Yeow, J Flores‐Tapia, A Esqueda‐Mendoza, F Gaboardi, G Giusti
Dept. of Urology, Hospital Regional de Alta Especialidad de la Península de Yucatán
MP06‐11
Pattern of key opinion leaders talks at major international urological meetings reflect the main differences in flexible ureteroscopy and PCNL diffusion
E Ventimiglia, F Quadrini, F Pauchard, H Kamkoum, S Doizi, O Traxer
Division of Experimental Oncology/Unit of Urology; URI; IRCCS Ospedale San Raffaele
MP06‐12
Withdrawn
MP06‐13
Natural history of small asymptomatic kidney and residual stones over a long‐term follow‐up: Systematic review over 25 years
CE Lovegrove, R Geraghty, B Yang, E Brain, SA Howles, BW Turney, BK Somani
Department of Urology, Oxford University Hospitals NHS Foundation Trust; Nuffield Department of Surgical Sciences, University of Oxford
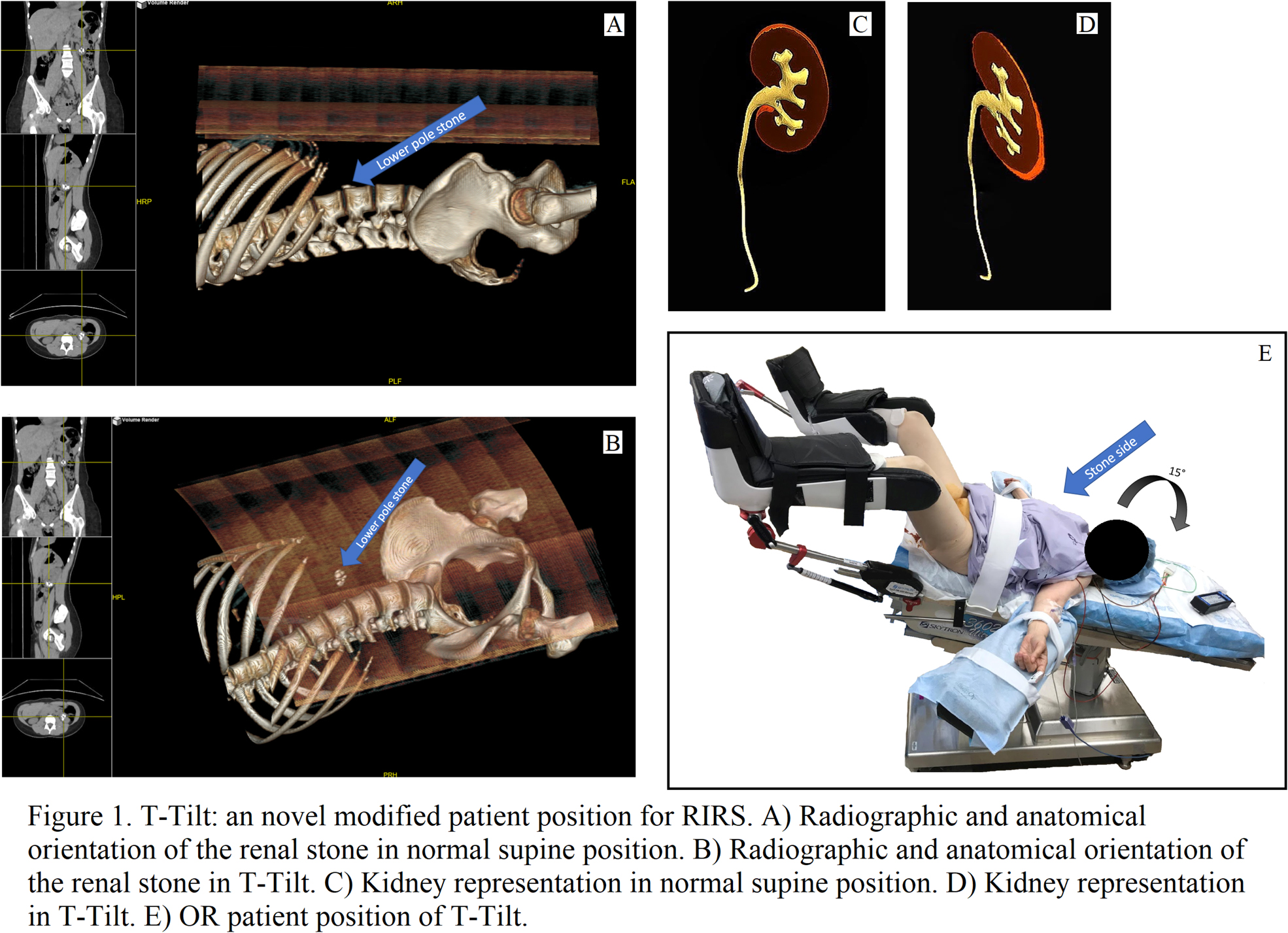
MP06‐14
The T‐Tilt Position: a Novel Modified Patient Position to Improve Stone‐Free Rates in Retrograde Intrarenal Surgery
C Liaw, JA Khusid, B Gallante, JN Bamberger, WM Atallah, M Gupta
Icahn School of Medicine at Mount Sinai
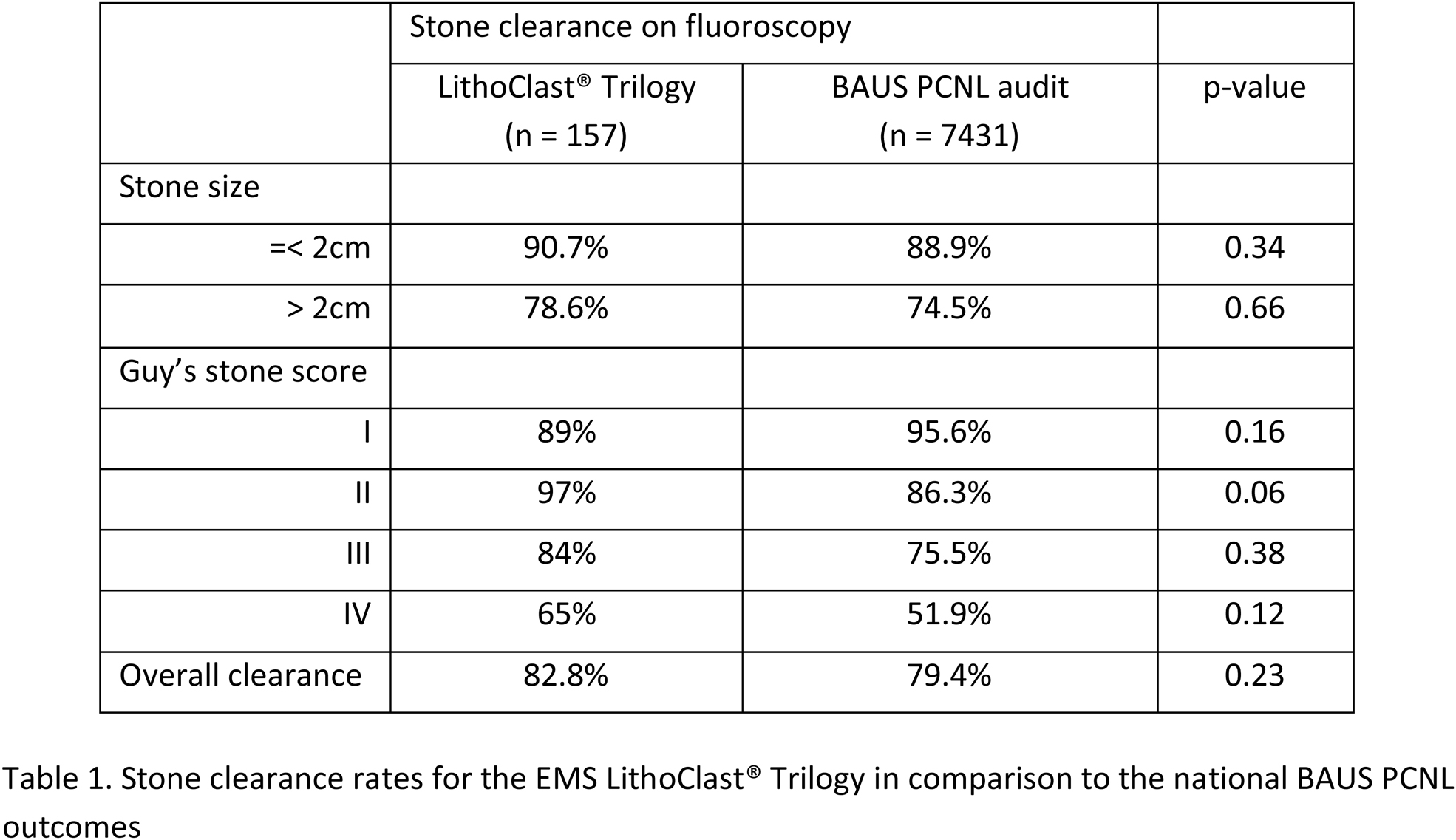
MP06‐15
Stone clearance using the EMS Swiss LithoClast® Trilogy: results of the European multicentre prospective study in comparison to the BAUS national PCNL outcomes on behalf of the European Society of UroTechnology
N Thakare, F Tanse, K Saeb‐Parsy, N Atassi, R Endriss, G Kamphuis, D Perez‐Fentes, M Hasan, M Brehmer, PJ Osther, HU Jung, BW Turney, W Finch, N Burgess, S Irving, L Dragos, E Liatsikos, T Knoll, V Cauni, O Wiseman
Cambridge University Hospitals Nhs Trust
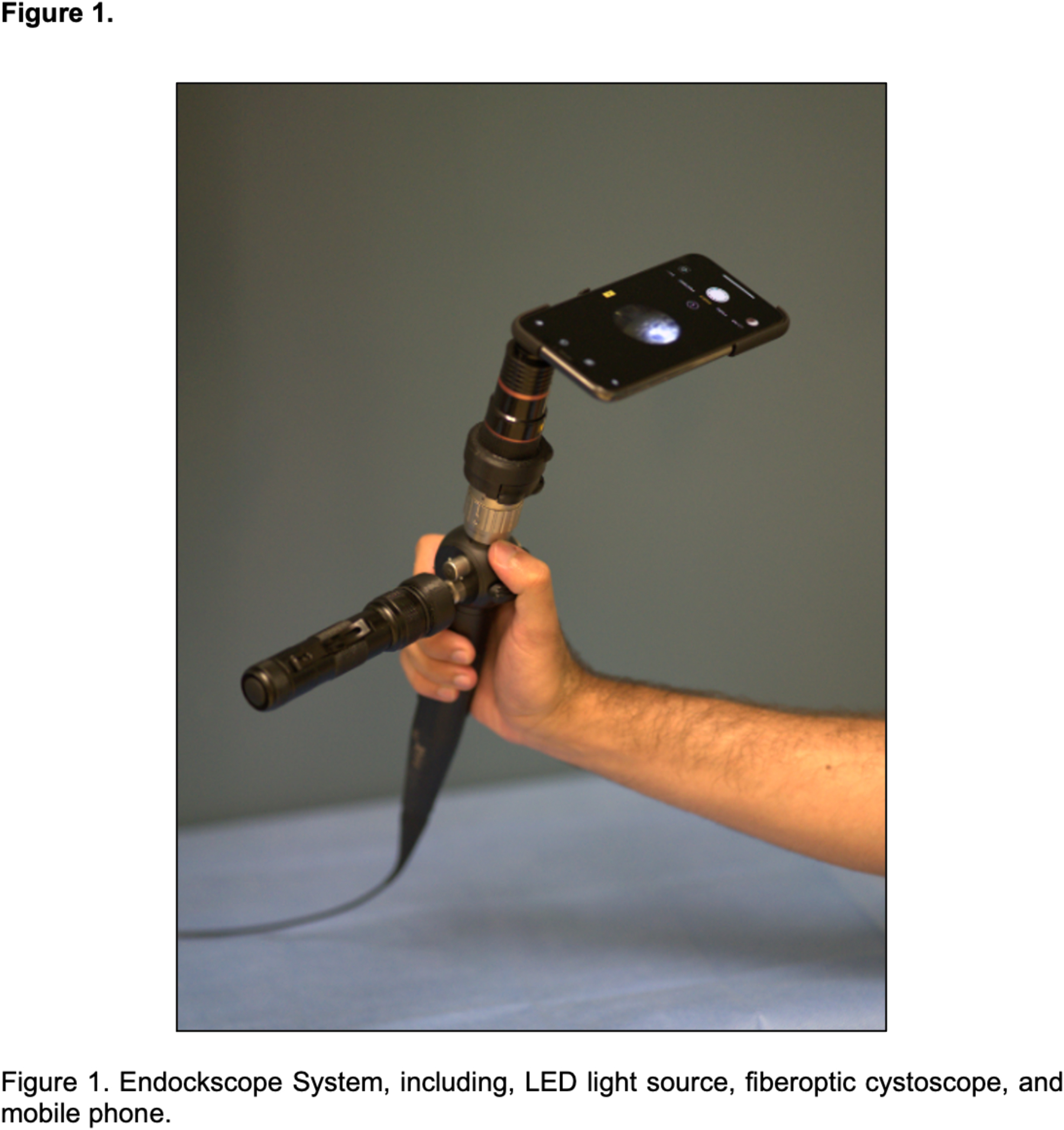
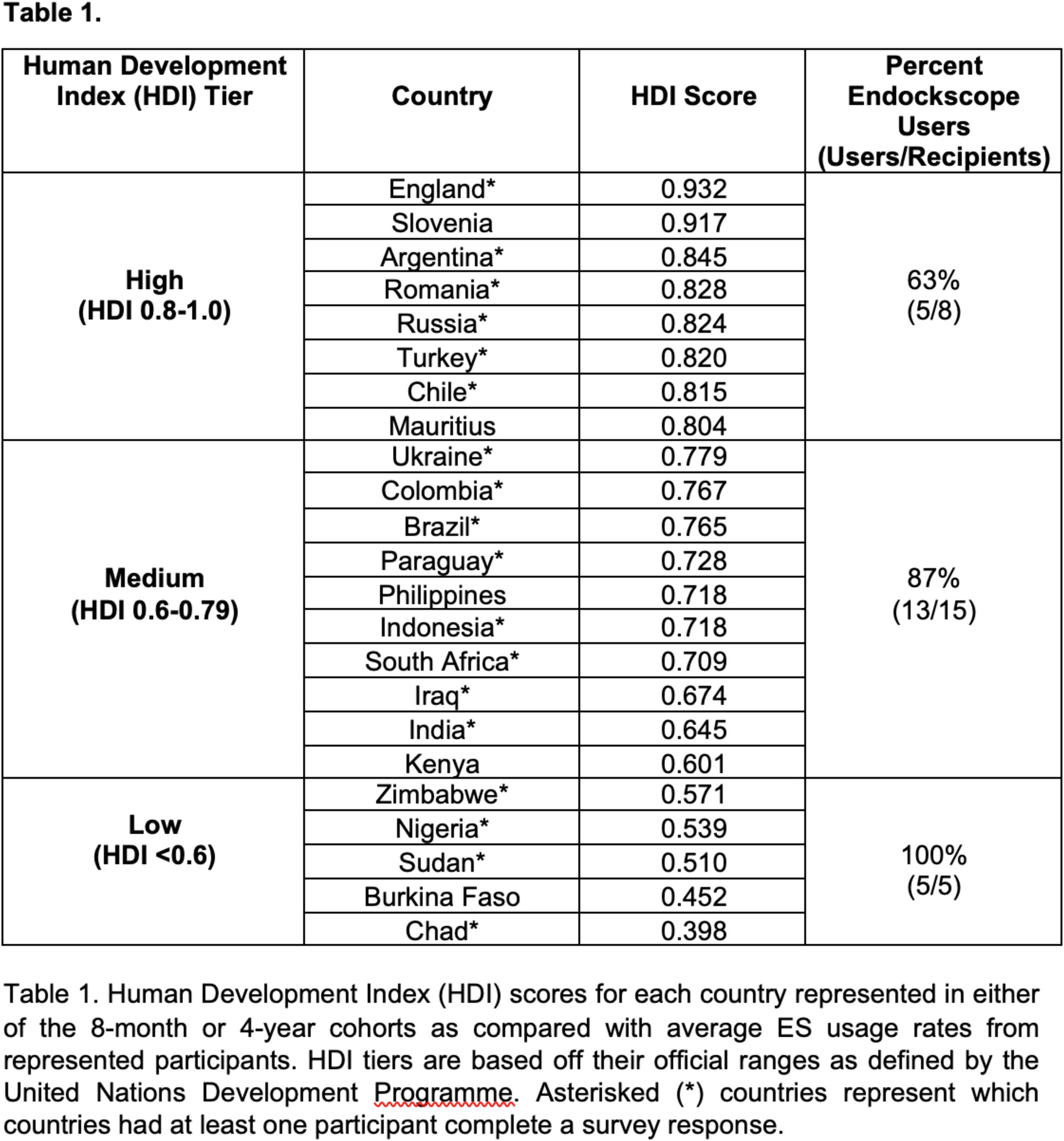
MP06‐16
Long‐Term Evaluation of the Endockscope System: An Assessment of Global Usage
AS Afyouni, M O'Leary, Z Okhunov, A Peta, A Brevik, M Ayad, R Yoon, RM Patel, B Dolan, J Landman, RV Clayman
Department of Urology, University of California, Irvine
MP06‐17
Benchtop Assessment of a New Single‐Use Flexible Ureteroscope
P Whelan, RS Terry, R Qi, C Tabib, F Soto‐Paulo, GM Preminger, M Lipkin
Duke University
MP06‐18
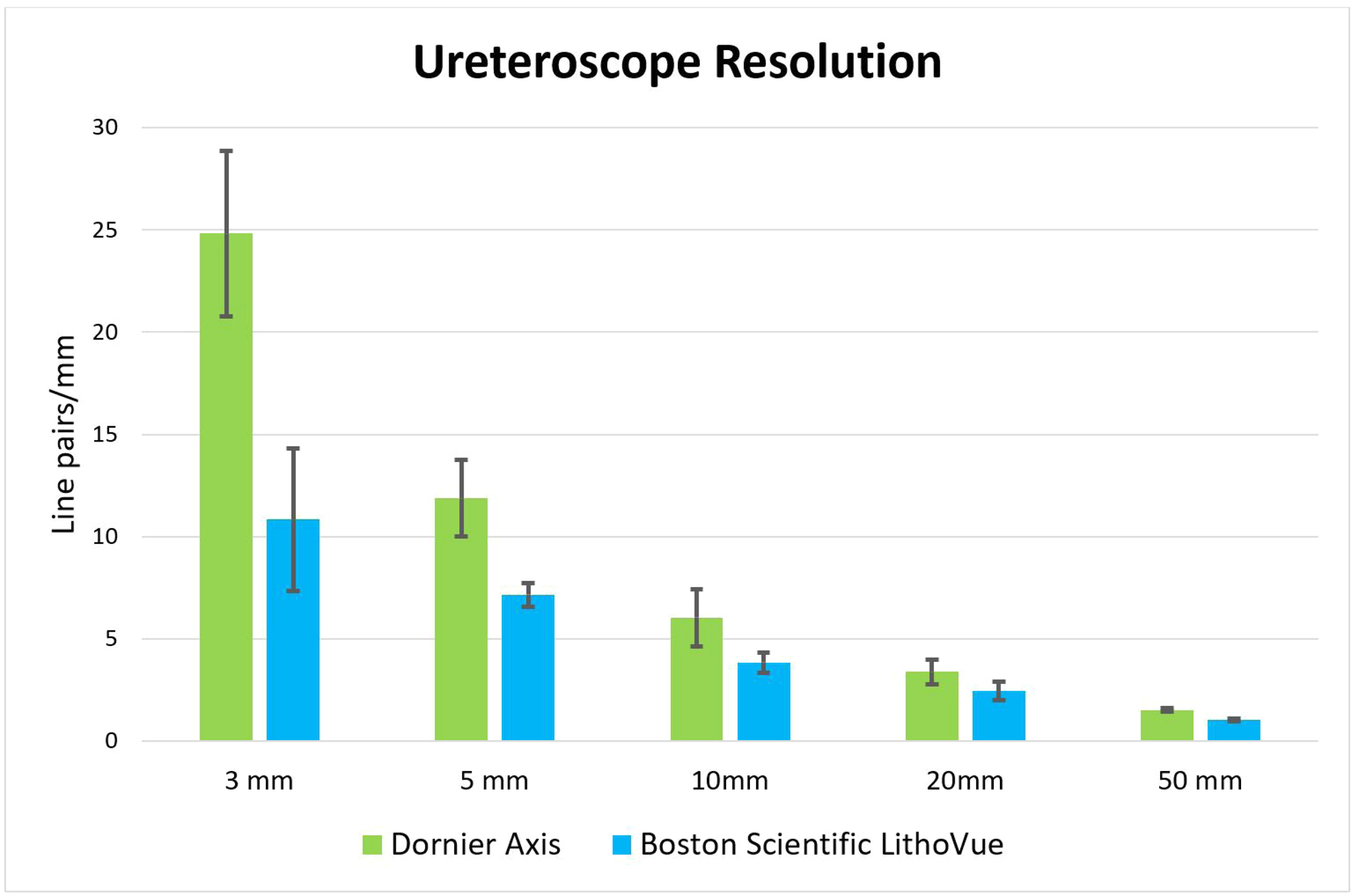
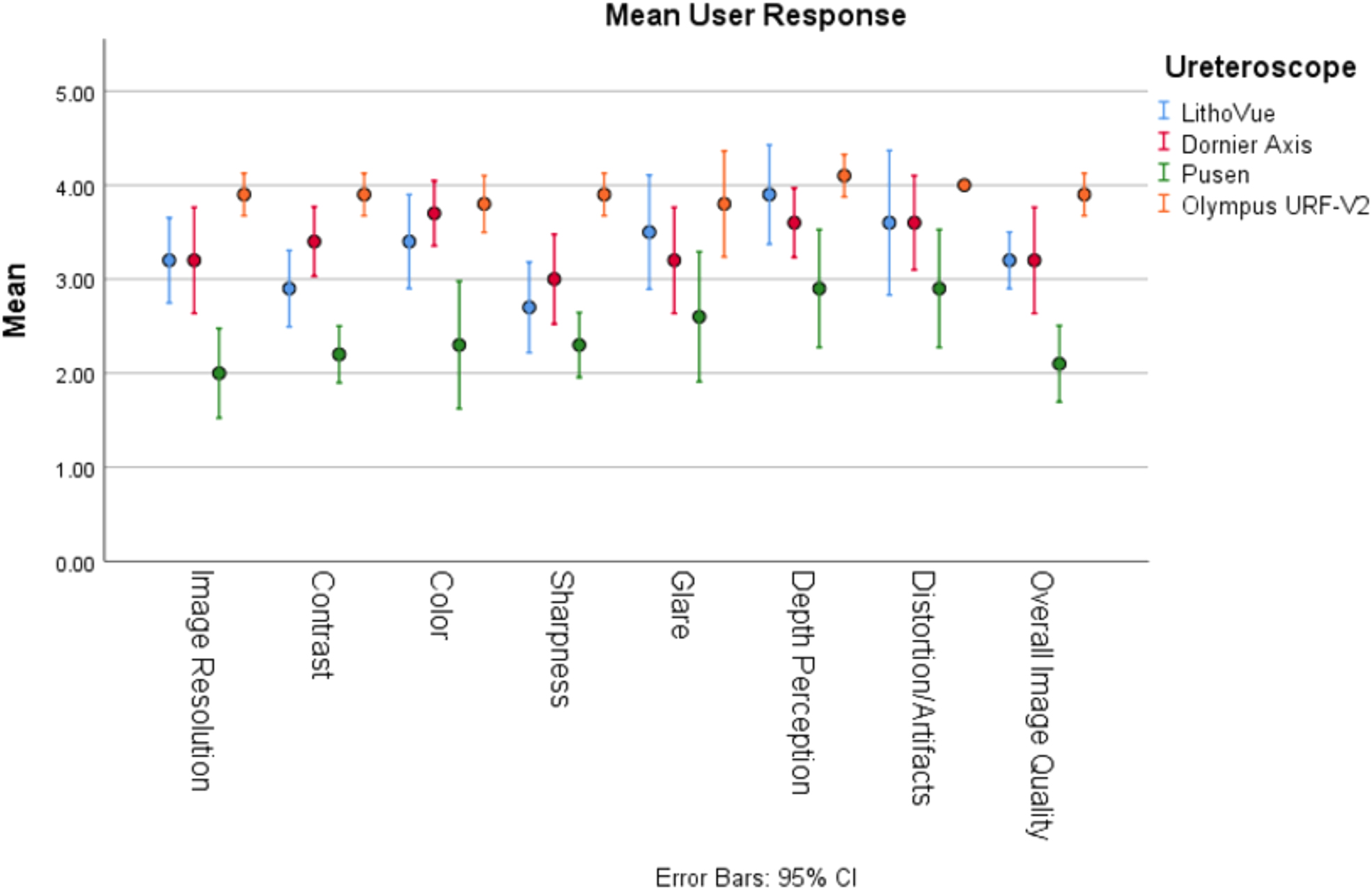
Novel Image Quality Evaluation Tool for Ureteroscopes: Validation Study Using Four Widely Available Digital Ureteroscopes
SN Patel, RK Jain, AT Cranwell, S Quarrier
University of Rochester
MP06‐19
Is uric acid stone the 6th component in metabolic syndrome? A marker for worsening health
H Johnson, H Musleh, A Mitry, H O'Callaghan, J Philip
Bristol Urological Institute
MP06‐20
Cost‐Effectiveness of 90‐Day Single‐Use Flexible Cystoscope Trial: Single Center Micro‐Costing Analysis
M Assmus, AE Krambeck, M Lee, DK Agarwal, M Mellon, ME Rivera, T Large
Northwestern University, Department of Urology
MP06‐21
Predictors of flexible ureteroscope instrument repair: analysis of the last 2 years at the University Hospital Zurich
D Lavrek, C Poyet, D Schmid, T Hermanns, T Sulser, D Eberli, E Keller
Department of Urology, University Hospital of Zurich, University of Zurich, Zurich, Switzerland
MP06‐22
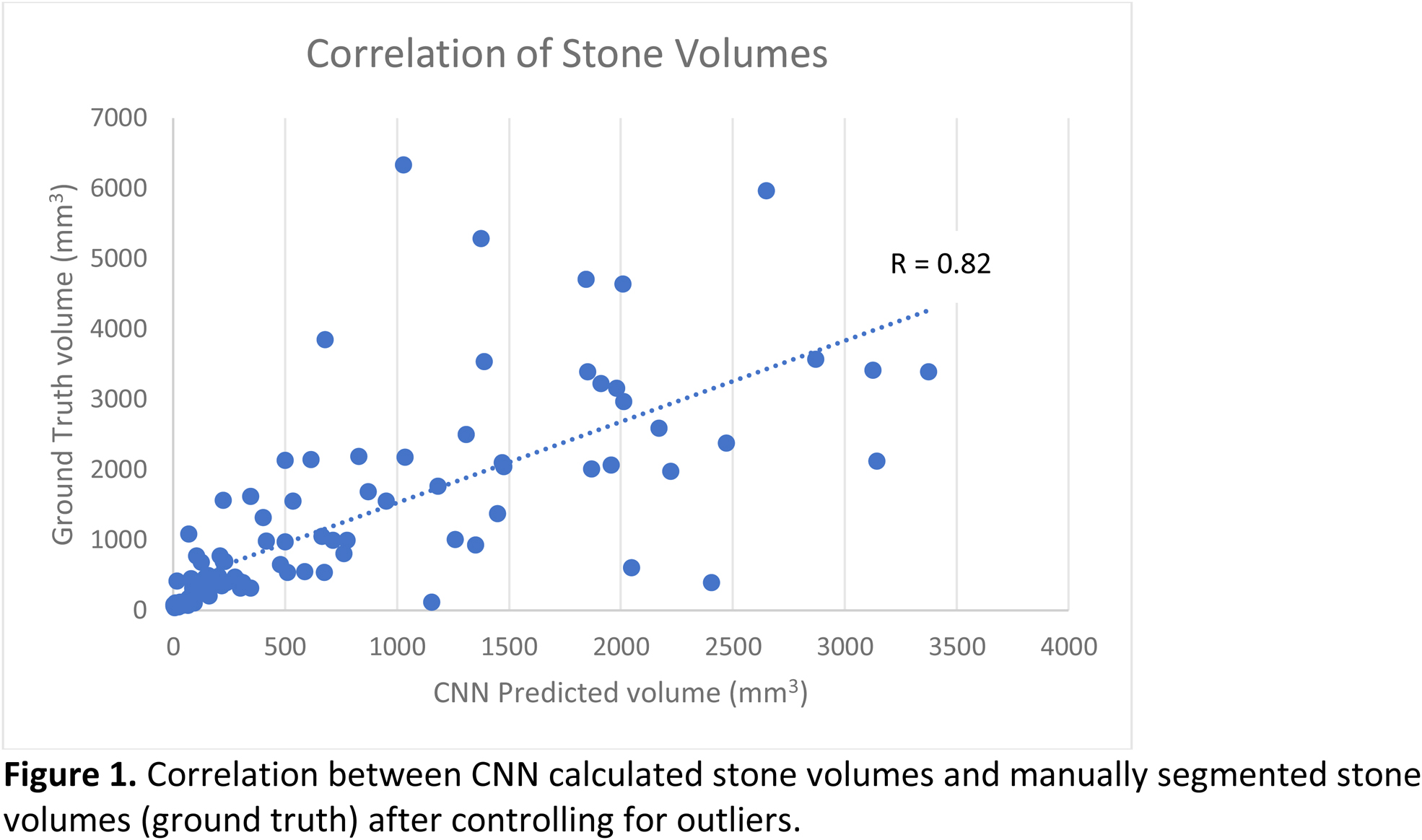
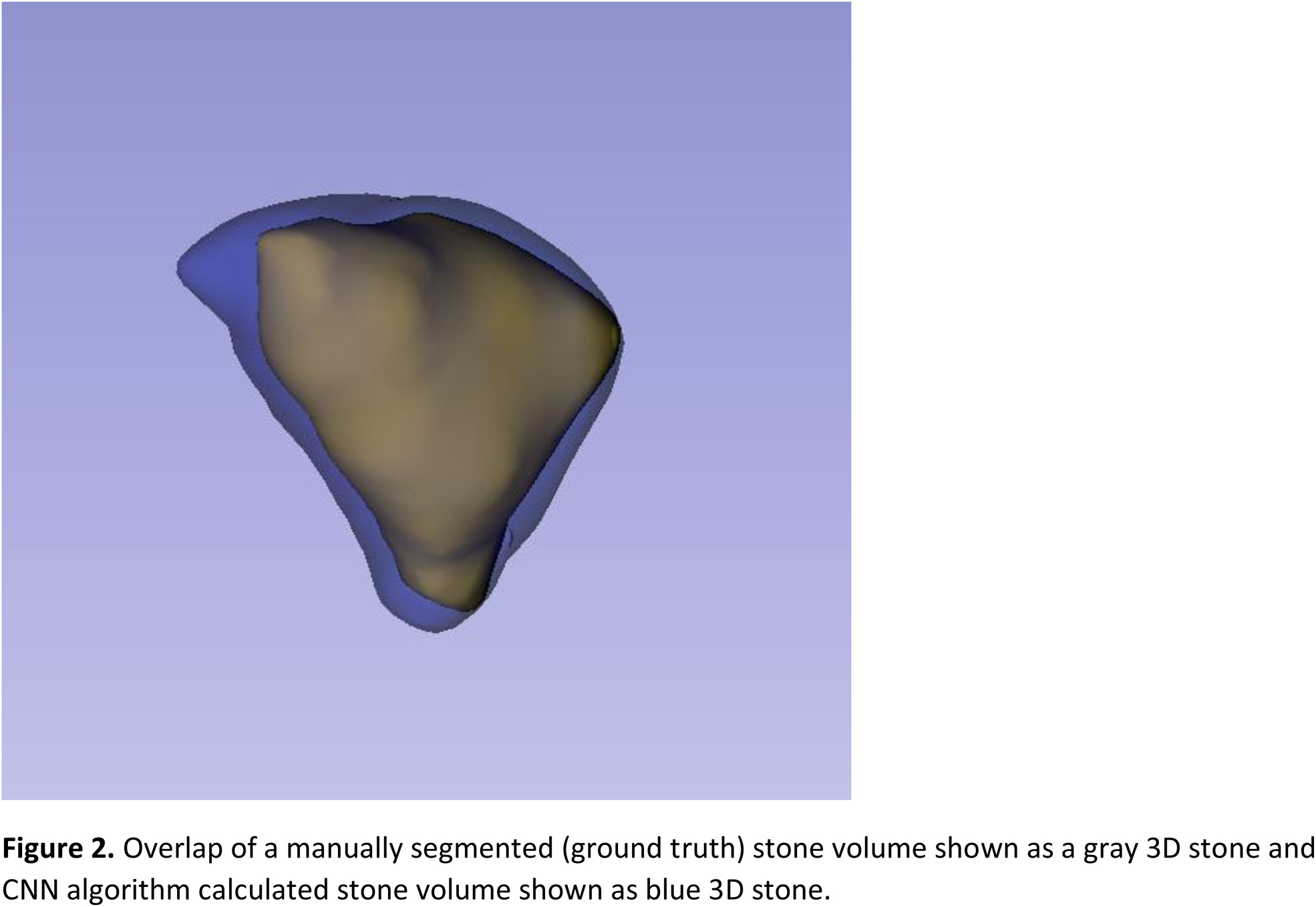
“Are we there yet?”: Assessing the Accuracy of Artificial Intelligence in Calculating Renal Stone Volume
A Peta, C Chantaduly, P Jiang, A Brevik, L Limfueco, R Karani, R Arada, RM Patel, J Landman, P Chang, RV Clayman
Department of Urology, University of California, Irvine
Moderated Poster Session 07: Imaging I
MP07‐01
Comparing PSMA‐PET, biopsy pathology, and MRI for prediction of Extra‐prostatic extension (EPE) and surgical guidance in prostate cancer
CD Bahler, M Green, M Tann, K Collins, J Swensson, E Brocken, L Cheng, D Alexoff, H Kung, M Koch
Urology
MP07‐02
Targeted MRI/US Fusion and Standard TRUS Prostate Biopsy: 563 Patients ‐ Relationship Between PIRADS Score and Prostate Cancer Detection Rate: A Single Urologist's Experience
A Kasraeian, M Alcantara, K Mola Alcantara, J Yellin, A Brochert, J Cesaretti, A Kasraeian
Kasraeian Urology
MP07‐03
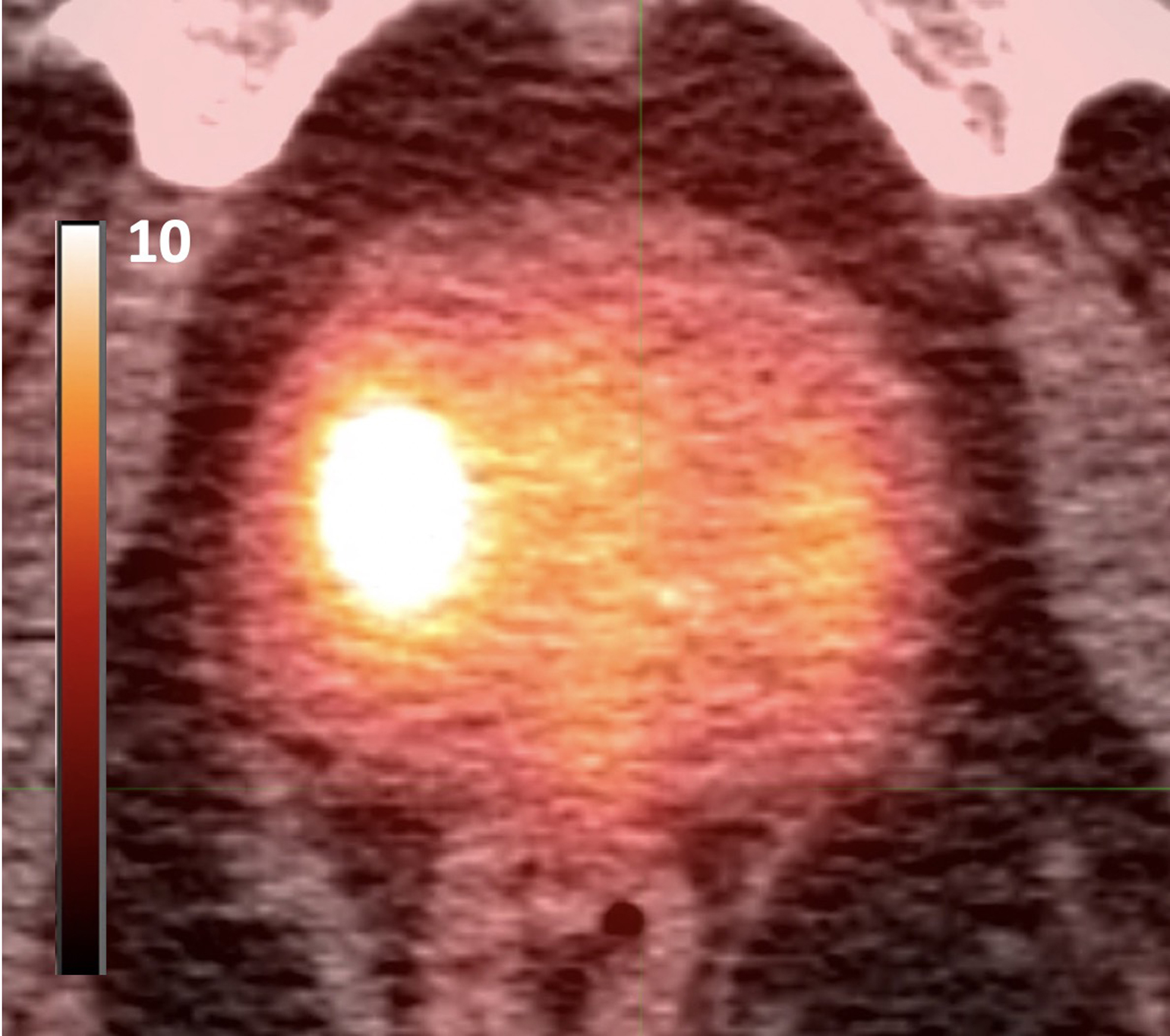
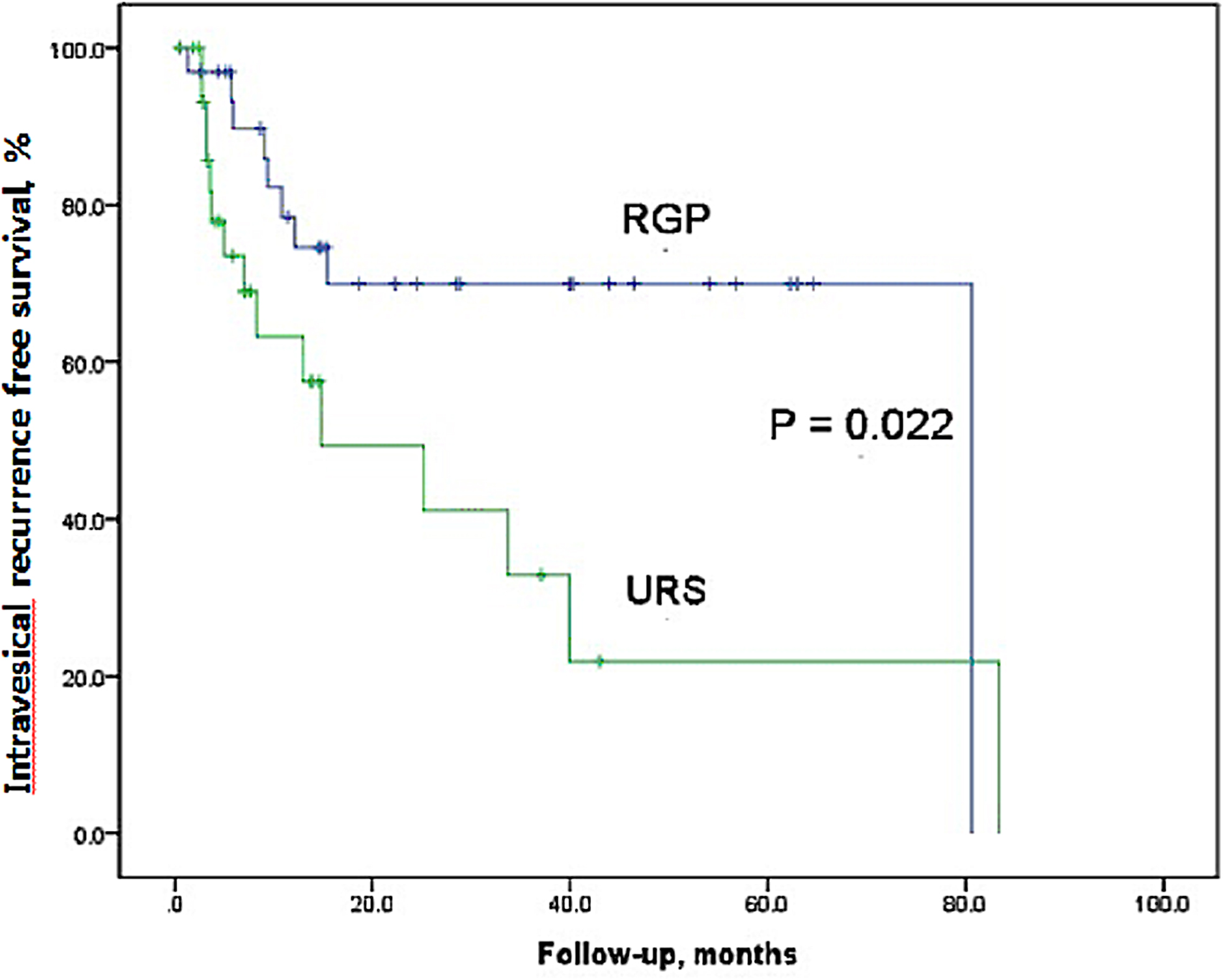
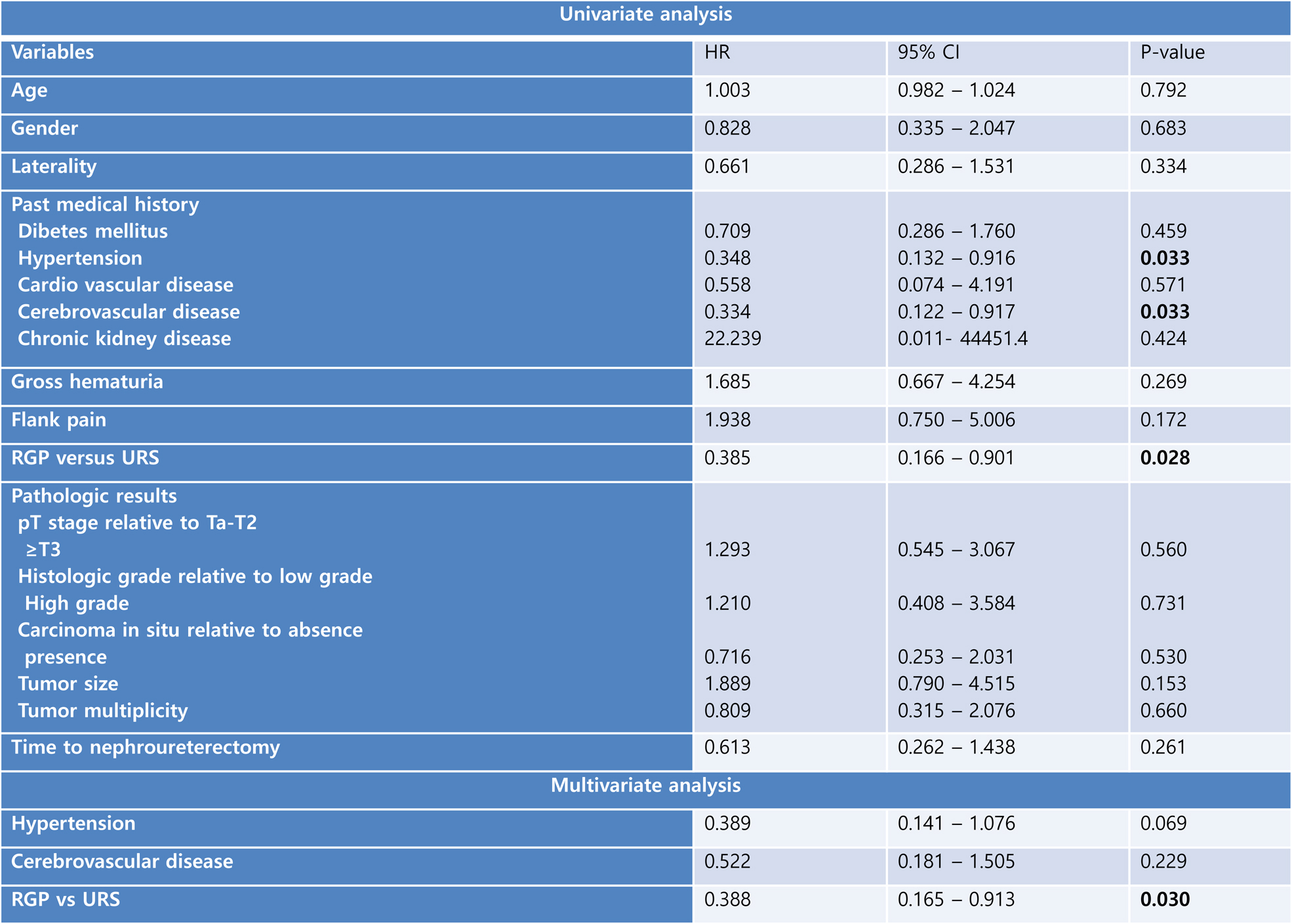
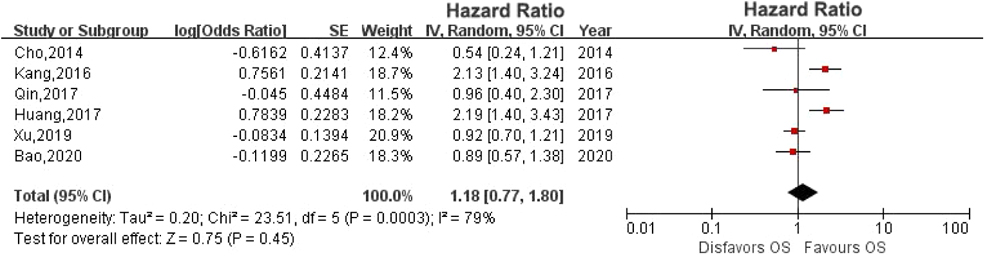
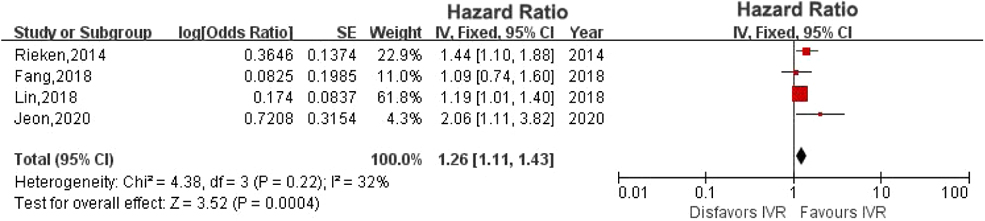
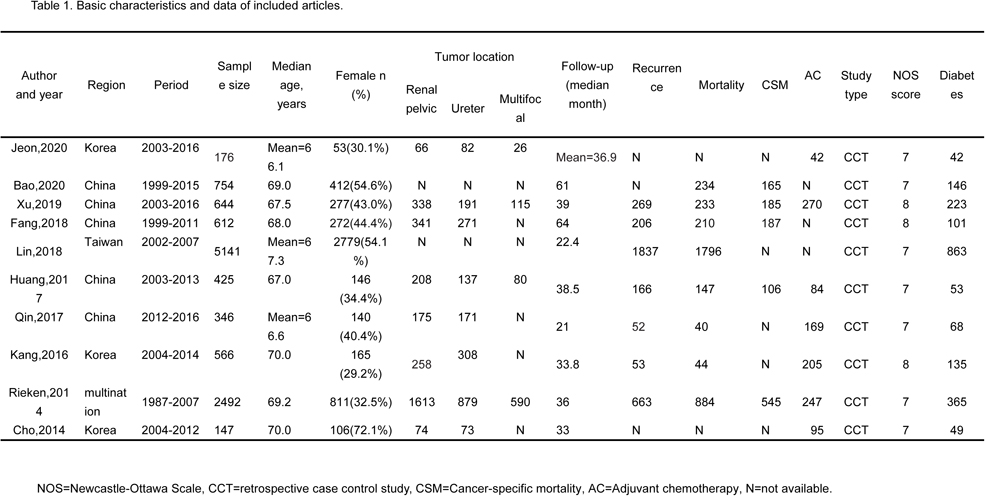
Retrograde uretero‐pyelography without diagnostic ureteroscopy has superior intravesical recurrence‐free survival compared to performing ureteroscopy in nephroureterectomy for upper urinary tract urothelial carcinomas
K Kim, H Yang, S Kim, D Kim, C Lee, Y Jeon
Department of Urology, Soonchunhyang University Cheonan Hospital, Soonchunhyang University College of Medicine
MP07‐04
Defining the non‐contrast computerized window setting for optimal colon identification prior to percutaneous nephrolithotomy
S Dekalo, Z Savin, I Mintz, H Hertzberg, I Masarwe, G Aviram, O Yossepowitch, M Sofer
Tel‐Aviv Sourasky Medical center, Sackler School of Medicine, Tel‐Aviv University
MP07‐05
Elevated radiation exposure and other dilemmas of ureteral access sheath (UAS) usage
T Ozimek, JR Wiessmeyer, JP Struck, MC Hupe, F Püschel, S Stockfisch, AS Merseburger, MW Kramer
MRI/TRUS target prostate fusion biopsy learning curve in two residents at a referral center: a retrospective analysis on more than 1000 procedures
E Checcucci, F Piramide, D Amparore, S De Cillis, G Volpi, A Piana, S Granato, A Pecoraro, P Alessio, B Carbonaro, J Mézière, G Cattaneo, F Ragni, M Manfredi, C Fiori, F Porpiglia
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
MP07‐07
New indication algorythms for Active Surveillance in the era of MRI‐targeted prostate biopsies
C Wetterauer, J Federer‐Gsponer, F Leboutte, R Mona, J Ebbing, C Rentsch, L Manka, H Seifert, S Wyler, F Recker, M Kwiatkowski
University Hospital Basel, Department of Urology
MP07‐08
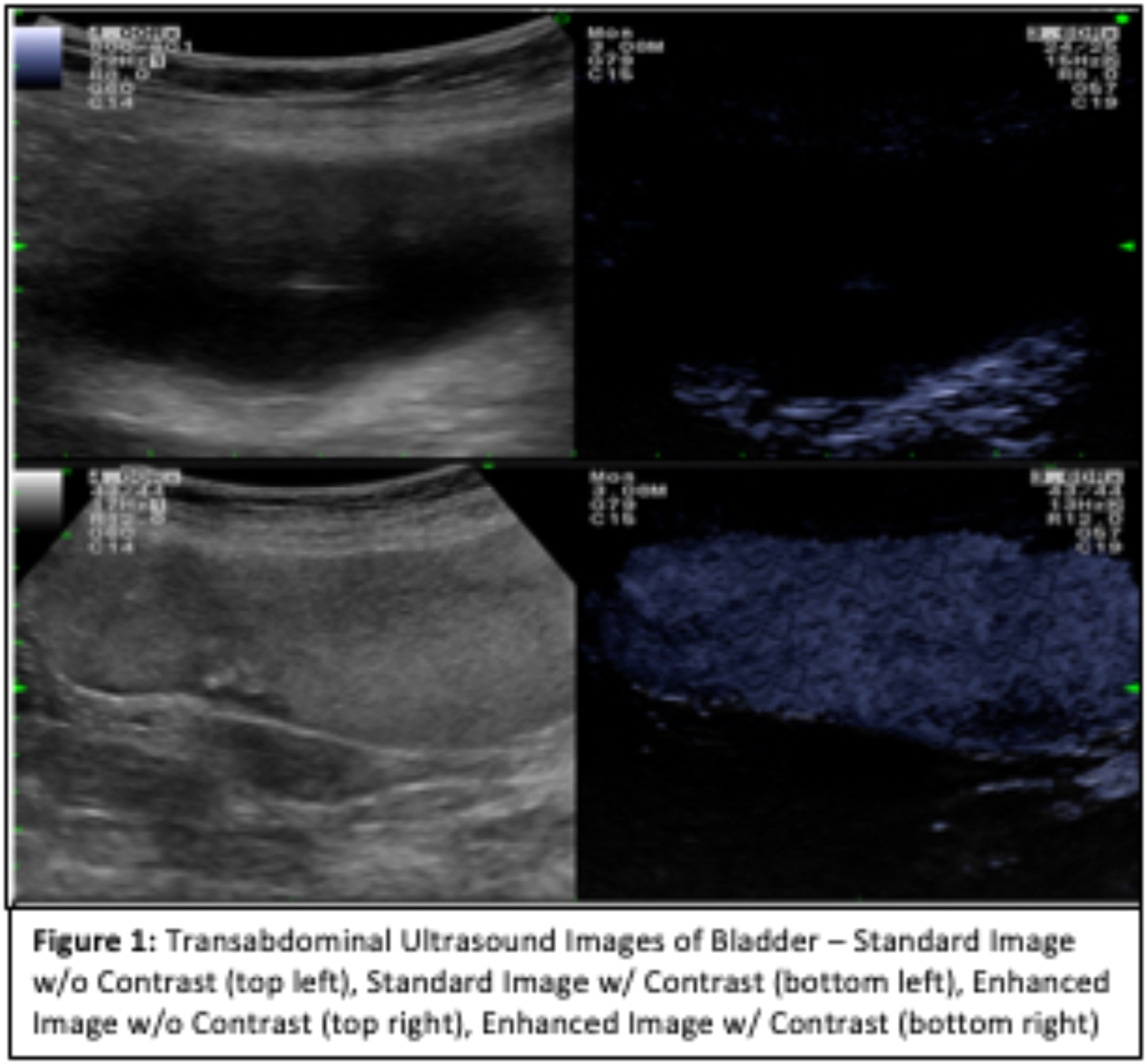
Intraoperative Contrast Enhanced Ultrasound To Reduce Unnecessary Ureteral Stent Placement After Ureteroscopy
J Ahn, D Bayne, F Hamouche, M Stoller, T Chi
UCSF
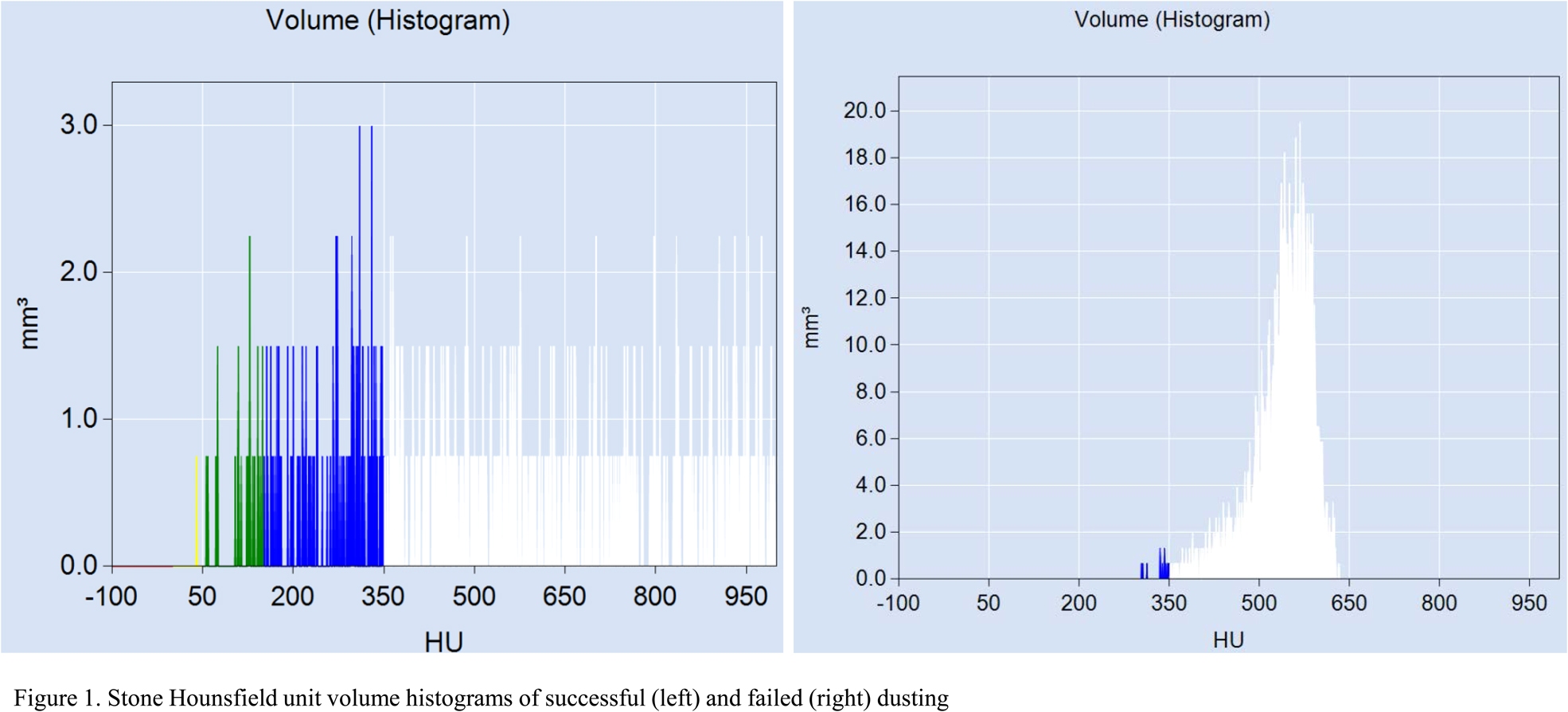
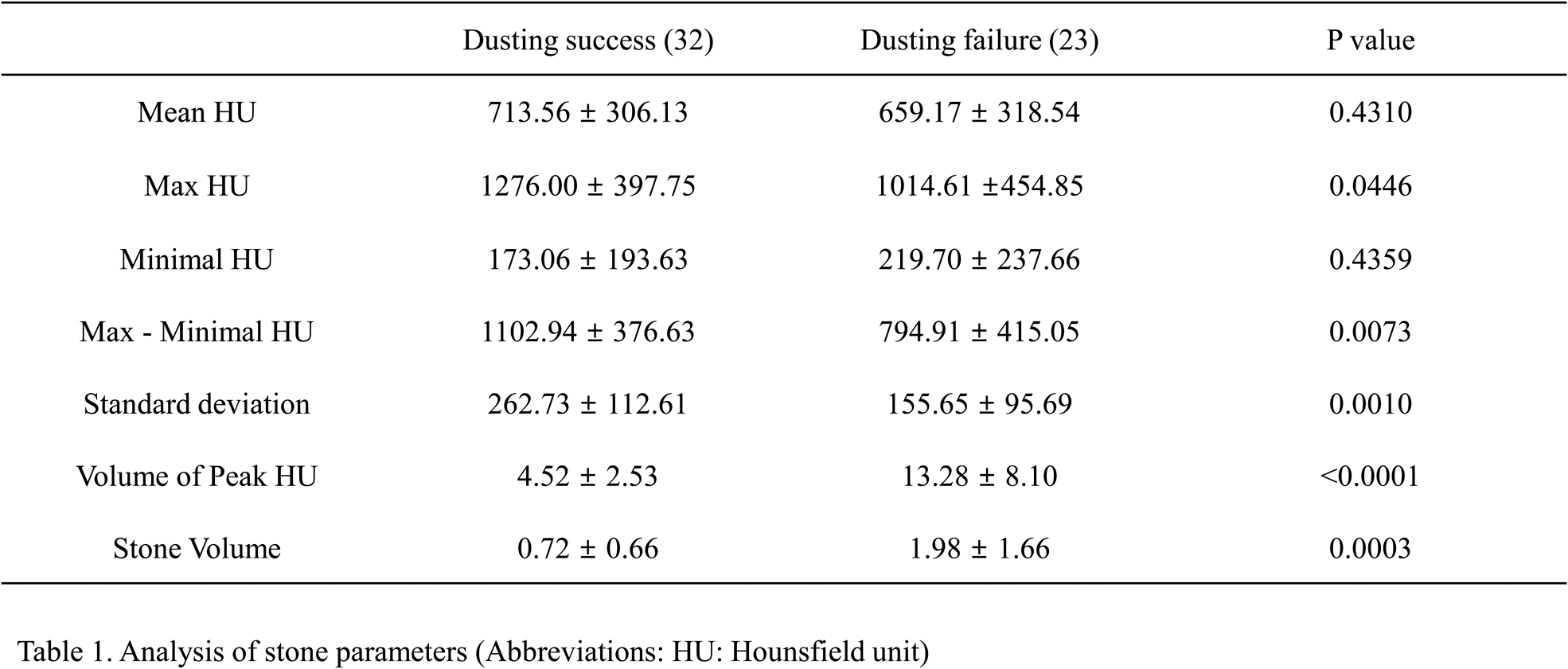
MP07‐09
Using Hounsfield unit (HU) ‐ volume models of kidney stones to predict successful stone dusting during retrograde intra‐renal surgery (RIRS)
D Kim, S Jeon, SJ Lee, C Lee, S Chang, SH Lee
Department of Urology, School of Medicine, Kyung Hee University
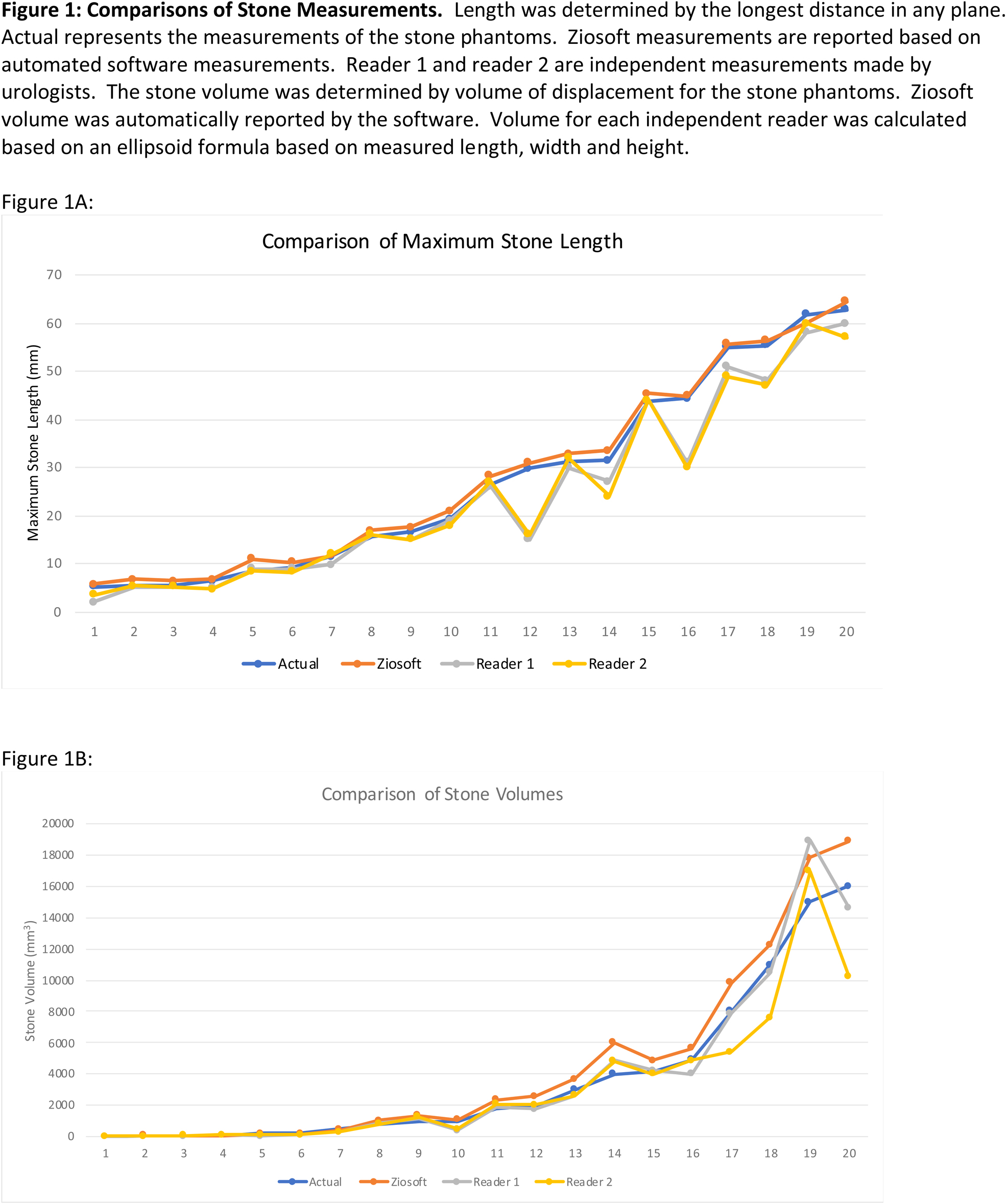
MP07‐10
Human vs Machine: Comparison Of Manual CT Measurements Versus Automated Software Of Stone Phantoms
L Peard, M Cash, I Mohamed, AM Harris, JR Bylund, AA Bhalodi, J Lee, J Bell
Univeristy of Kentucky
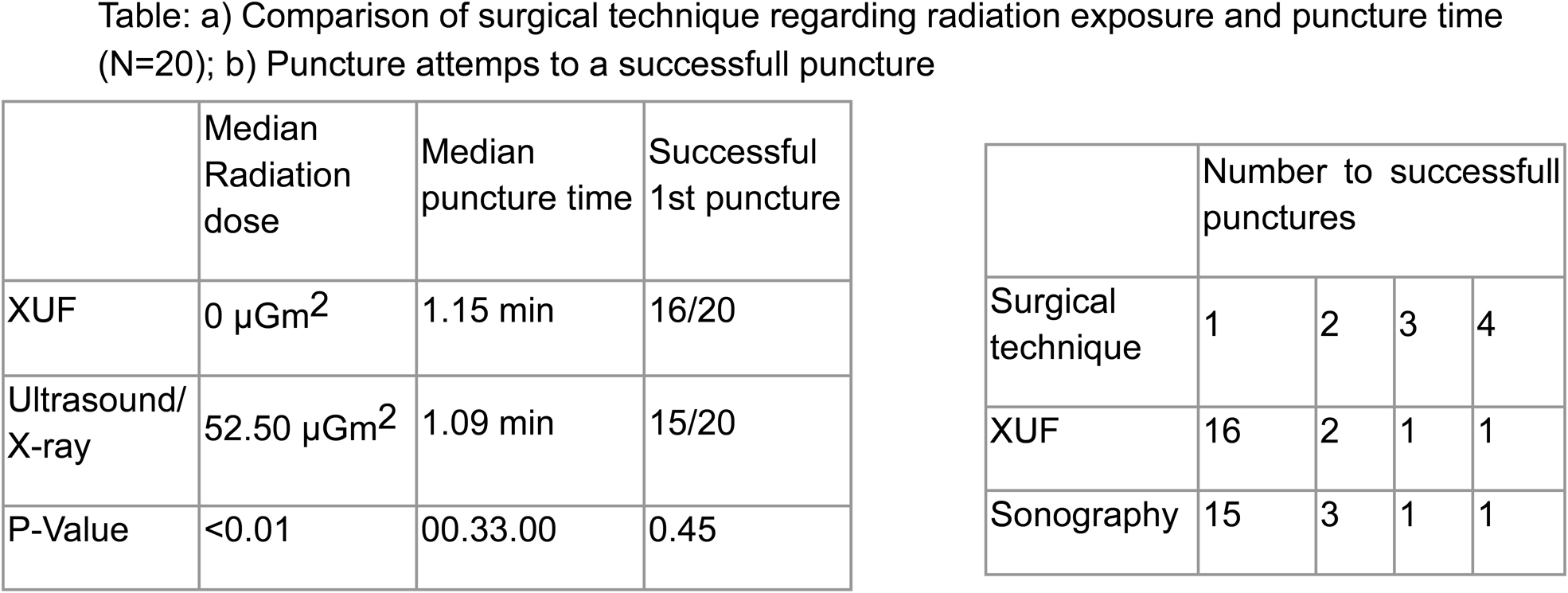
MP07‐11
Xray and US free calix puncture before PCNL (XUF PCNL). Comparison with standard Xray/US guided puncture
M Maltagliati, L Berti, C Buizza, U Besana, A Calori, M Justich, C Gastaldi, M Sighinolfi, S Micali, BC Rocco, G Bozzini
ASST Valle Olona
MP07‐12
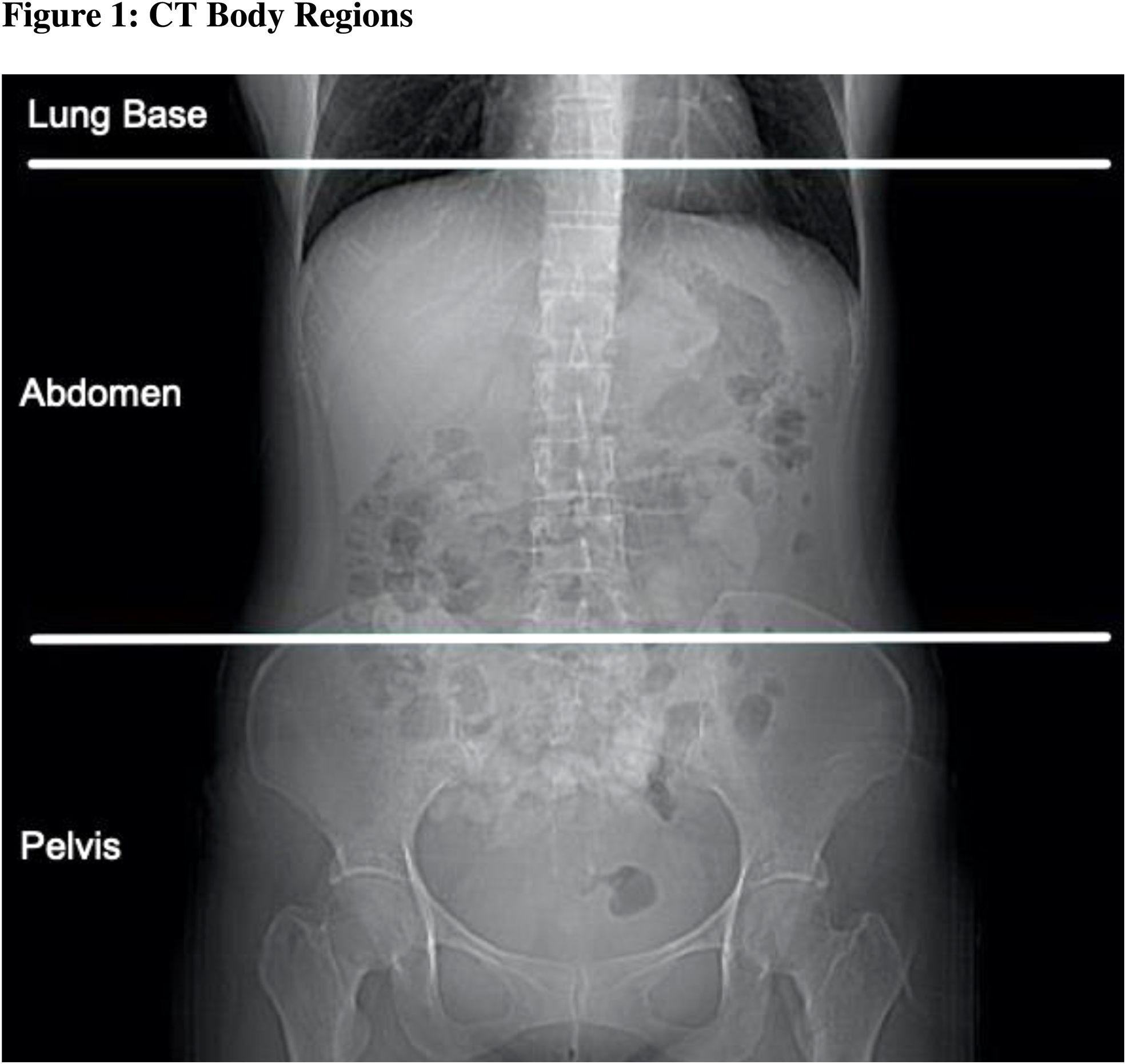
Should the Pelvis be Included in CT Imaging of Asymptomatic Urinary Stone Patients? A Retrospective Review
M Fritz, J Zhang, A Ayoob, J Bell
Univeristy of Kentucky
MP07‐13
Does CT scan after ultrasonography change surgical planning for nephrolithiasis?
A Ludvigson, P Motamedinia
Yale New Haven Hospital
MP07‐14
Utilization of low‐dose CT for evaluation of urolithiasis at a high‐volume stone referral centre
EP Chan, F Gabrigna Berto, O Daher, Z Syed, C Dawson, J Amann, J Bjazevic, H Razvi
Western University
MP07‐15
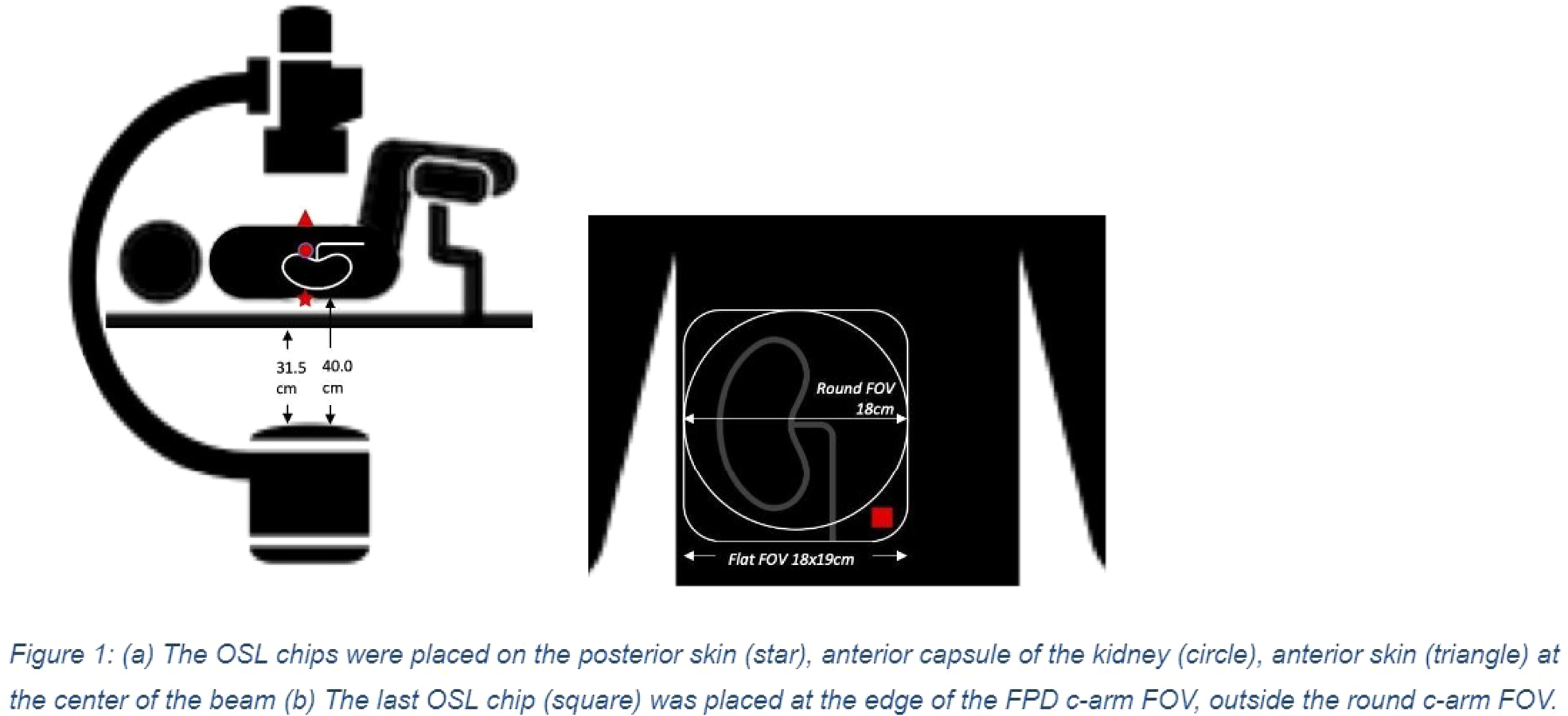
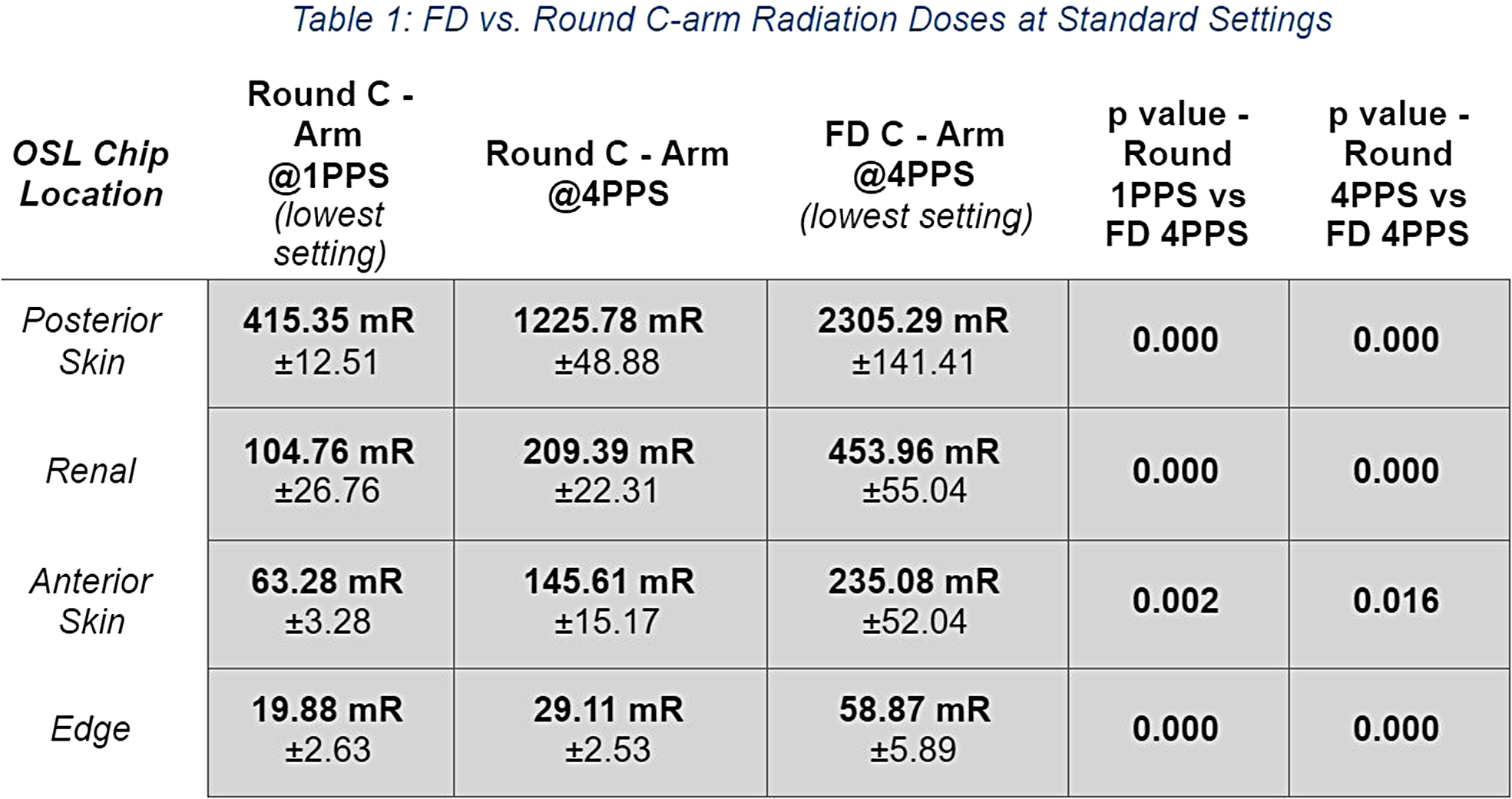
A Comparison of Radiation Exposure Between the New Flat Panel and the Conventional Round C‐Arm
JD Belle, M Keheila, N Chen, J Lee, N Srikureja, AS Amasyali, DD Baldwin, M Hajiha
Loma Linda University, Department of Urology
MP07‐16
Clear cell Likelihood Scores (ccLS) on Multiparametric MRI Decreases Benign Pathology Rates in Patients with Chronic Kidney Disease (CKD) Being Considered for Extirpative Nephron Sparing Surgery (NSS)
TN Morgan, JC Dai, V Kommidi, S Kusin, H Kominsky, I Pedrosa, JA Cadeddu
UT Southwestern
MP07‐17
Variation in Imaging after Stone Treatment
J DiBianco, B Conrado, S Daignault‐Newton, S Jafri, H Korman, KR Ghani, CA Dauw, f Urological Surgery Improvement Collaborative
Department of Urology, University of Michigan
MP07‐18
Observation of radiopaque renal lesions
A Keln, S Schmidt, DG Alifov
Tyumen State Medical University
MP07‐19
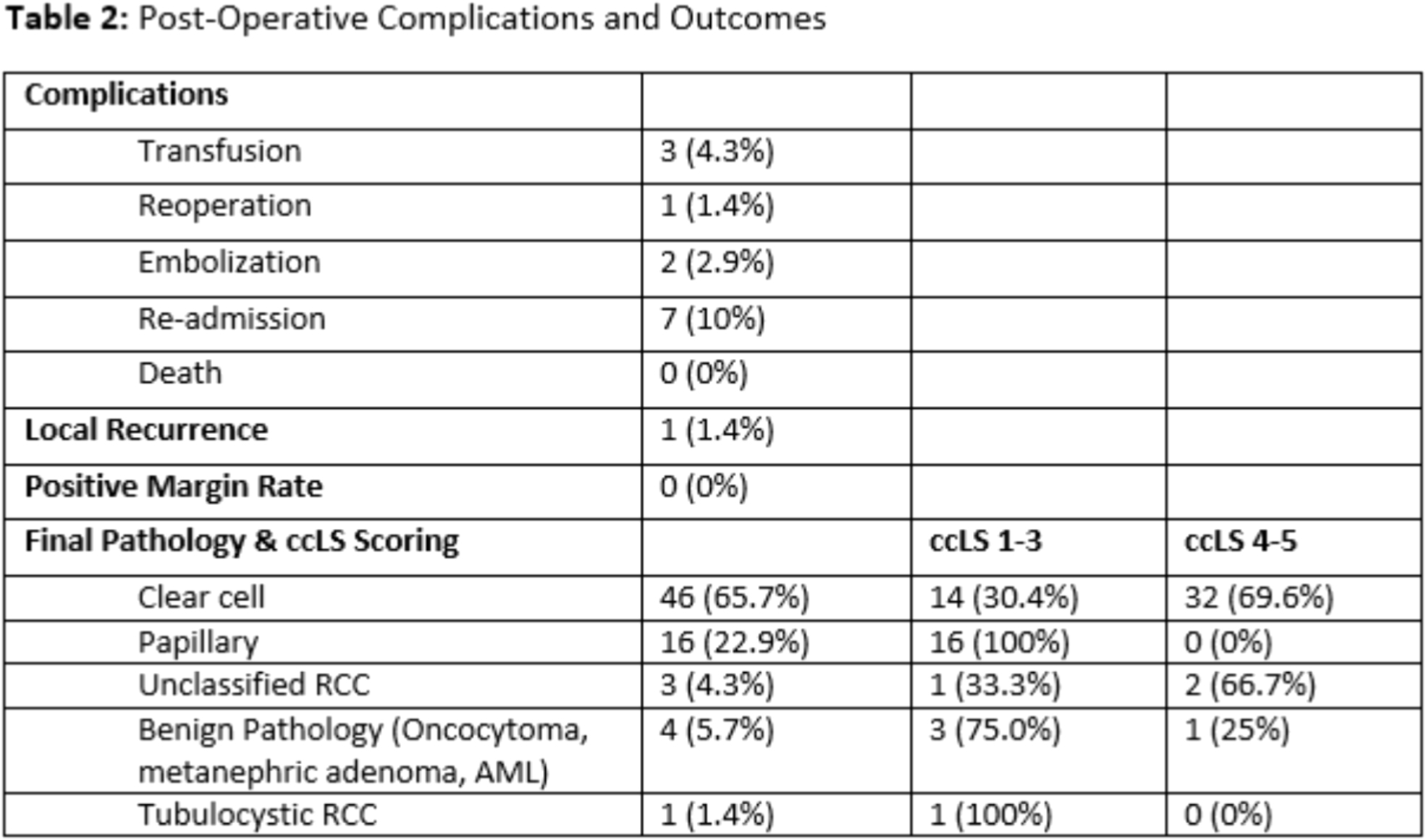
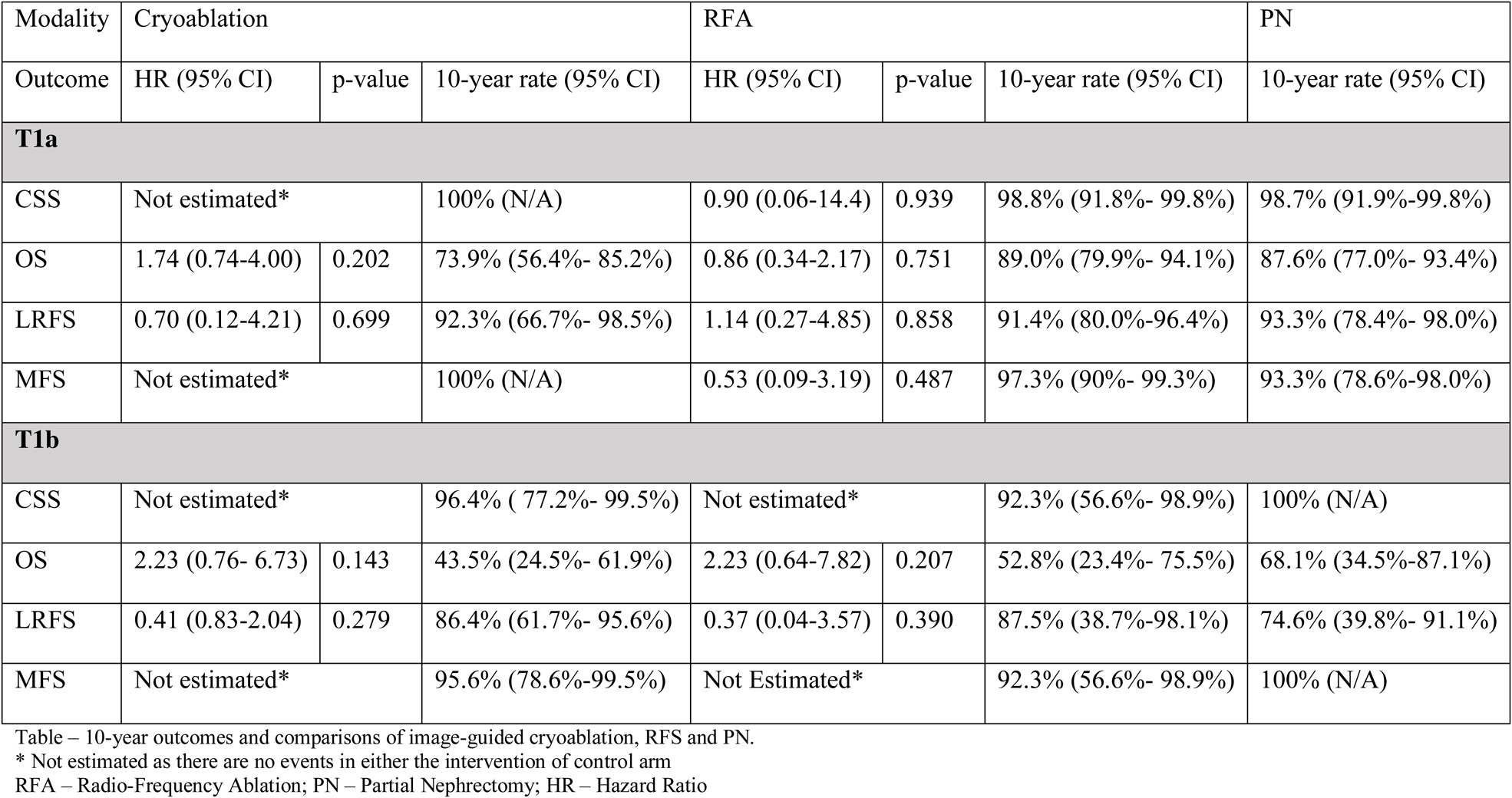
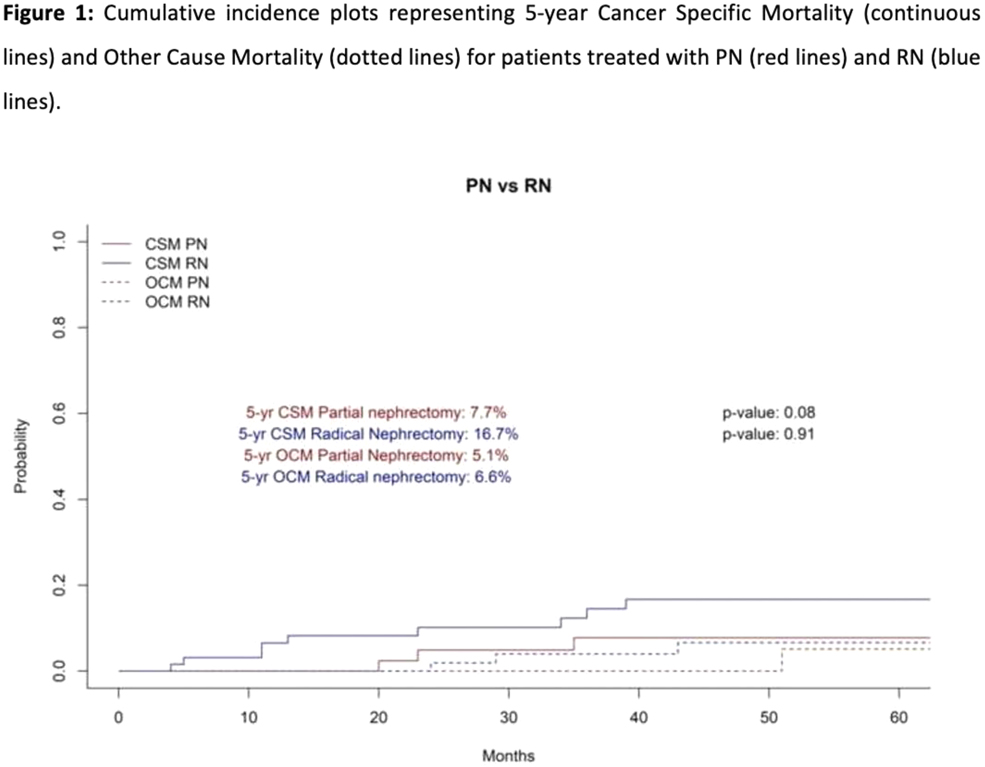
Percutaneous Image Guided Cryoablation and Radio‐frequency Ablation versus Partial Nephrectomy for small renal cell carcinomas: a ten‐years, single centre observational study
V Vinson, F Osman, J Cartledge, M Kimuli, N Vasudev, C Ralph, S Jagdev, S Bhattarai, J Smith, J Lenton, T Wah
School of Medicine, Faculty of Medicine and Health, University of Leeds, Leeds Department of Targeted Intervention, Division of Surgery and Interventional Science, University College London, London
MP07‐20
Withdrawn
MP07‐21
A Novel CO2‐Digital Subtraction Nephrostogram Imaging Technique For “Contrast‐free” Percutaneous and Retrograde Endoscopic Renal Surgery in the Severely Contrast Allergic Patient
AJ Hannemann, MD Sawyer, E Ballon‐Landa, SD Herrell, J Eun
VA ECHCS/University of Colorado School of Medicine
MP07‐22
Novel 3D Anatomical Modeling Facilitates Laparoscopic or Robotic Donor Nephrectomy in Patients with Complex Renal Anatomy that were Precluded from Donation based on Computed Tomography Angiography or Magnetic Resonance Imaging
J Kuo, N Velazquez, M Degen, R Munver
Hackensack Meridian School of Medicine
Abstract Video Session 01: Percutaneous Surgery
V01‐01
Percutaneous combined electrosurgical and Thulium Fiber Laser management of large renal pelvis urothelial tumor in a solitary kidney
A Martov, D Ergakov, N Baykov, A Andronov, SV Dutov
V01‐02
Mini‐PCNL for multiple Hem‐o‐lok clips forming stone nidus in the collecting system
T Aro, A Rai, D Hoenig, AD Smith, Z Okeke
V01‐03
Bilateral Nephrolithiasis And Upper Tract TCC in Horseshow Kidney
T Aro, A Rai, D Hoenig, AD Smith, Z Okeke
V01‐04
Gradual Percutaneous Nephrolithotomy For Complete Staghorn Stone Can Facilitate Renal Access, Prevent Complications And Improve Stone Free Rate
J Feghali
V01‐05
Supine Percutaneous Nephrolithotomy (PCNL) in Horseshoe Kidney
MO Breish, S Sriprasad, D Whiting, F Anjum, O Abdalla
V01‐06
Percutaneous nephrolithotomy in challenging cases of renal stones
J Park, H Park, H Shin
V01‐07
Encrustated Metallic Ureteral Stent Treated By Mini Percutaneous Nephrolithotomy
T Machado, R Astolfi, R Carrera, G Freschi, N Gattas, A Meller
V01‐08
Endoscopic Combined IntraRenal Surgery (ECIRS) with SOLTIVE Laser and Mini‐PCNL Technique
S Niu, SM Alam, WR Molina
V01‐09
Pediatric PCNL ‐ Past Challenges and Future Directions
C Ferari, C Crigger, M Ost, O Al‐Omar
West Virginia University
V01‐10
Using 3D Scanning to Create a CNC Machined Polyurethane Bed for Patient Positioning During Percutaneous Nephrolithotomy
DC Fedrigon, S Sivalingam
Cleveland Clinic‐ Glickman Urological & Kidney Institute
V01‐11
Thulium laser dusting of a partial staghorn stone via 14Fr Super‐mini percutaneous approach – technique and optimal laser settings
E Edison, T Reid, R Vitale, N de Luyk, V Arumuham, C Allen, S Choong
Moderated Poster Session 08: Reconstruction
MP08‐01
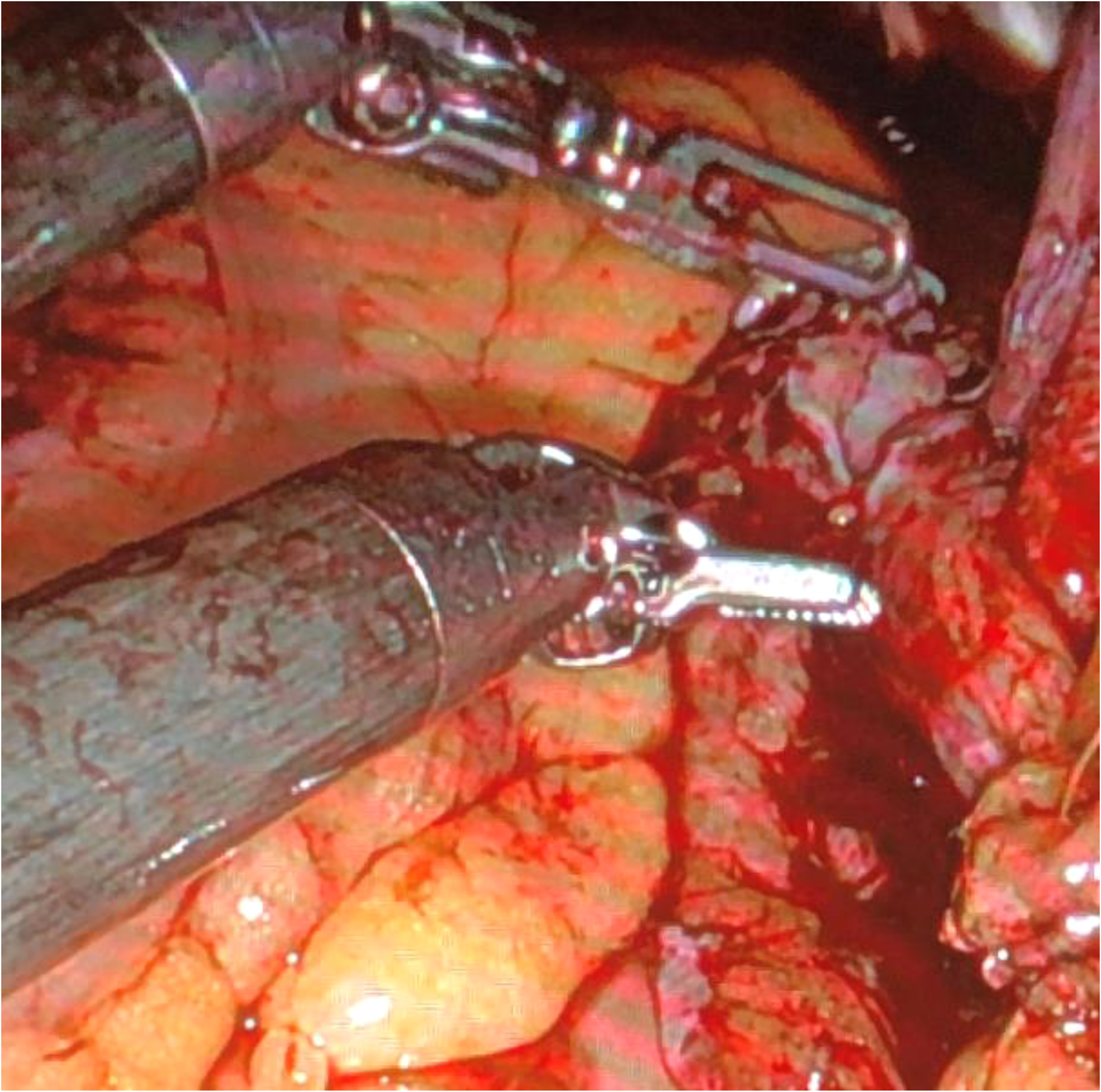
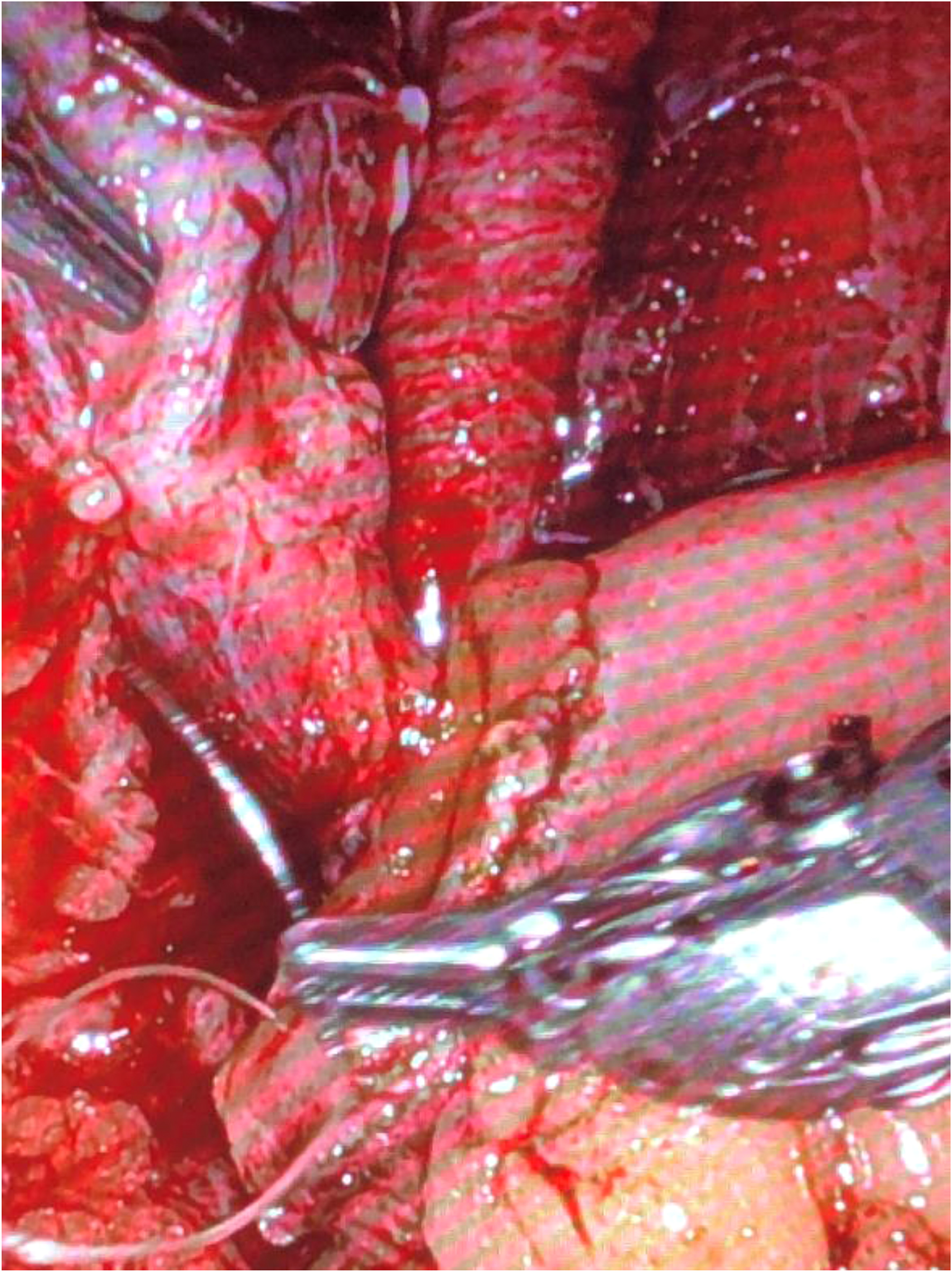
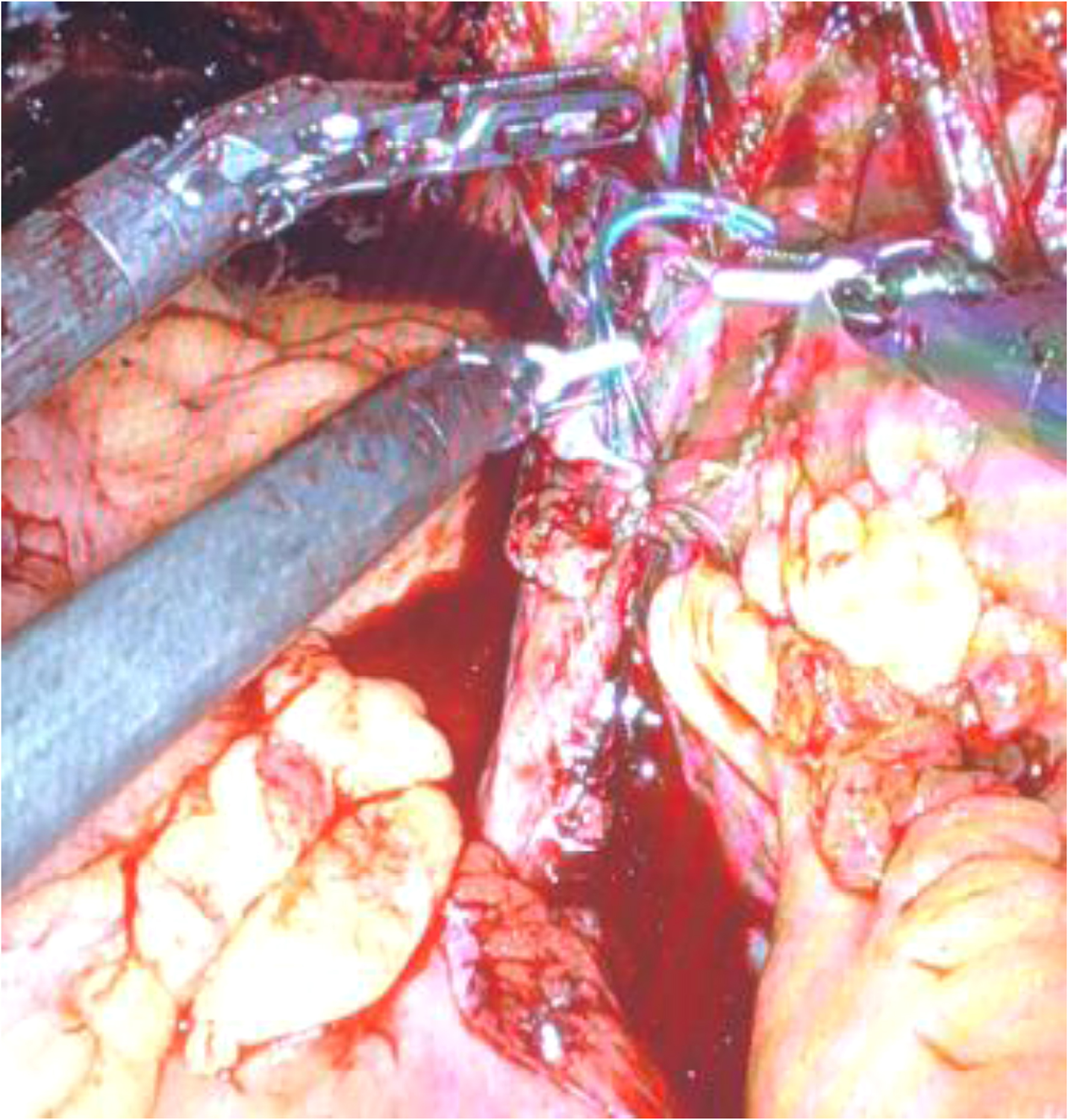
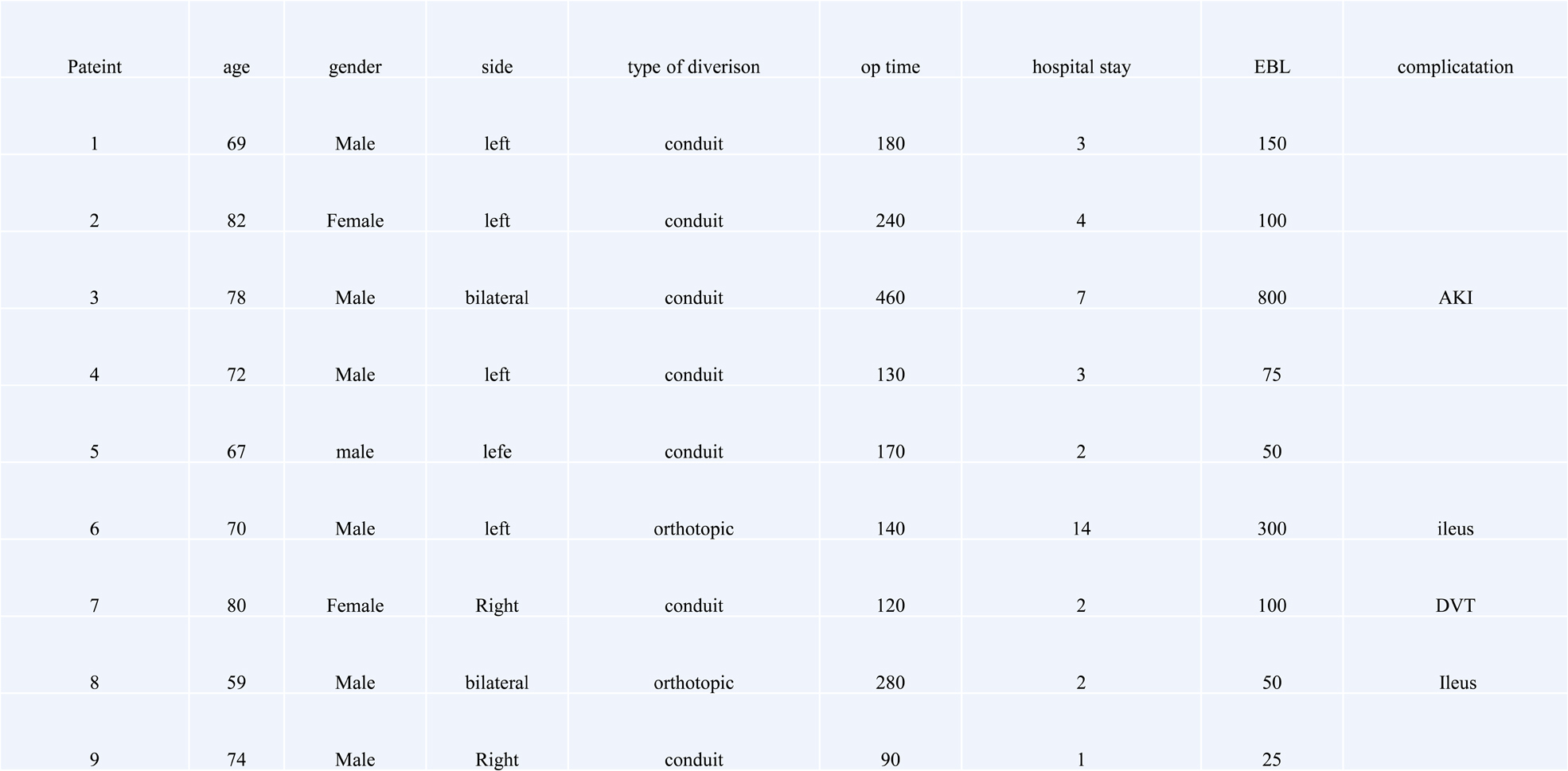
Robotic Repair of Ureteroenteric Strictures after Urinary Diversion
MW Salkini, A Dahman
West Virginia University
MP08‐02
Cutaneous Ureterostomy or Ileal Conduit urinary diversion: Can we spare the bowel following Radical Cystectomy in patients with solitary functioning kidney?
B Nayak, S Saini, P Singh, R Nayyar
All India Institute of Medical Sciences, New Delhi
MP08‐03
Approach to management of uretero‐vaginal fistula: Review of 15 cases over 10 years
P Singh
All India Institute of Medical Sciences, New Delhi, india
MP08‐04
Withdrawn
MP08‐05
Organ‐sparing surgery with Bracka's reconstruction for penile cancer: a single‐center experience
A Gallioli, A Rosales, JM Gaya, A Sánchez‐Puy, A Piana, P Diana, A Territo, P Gavrilov, J Caldéron, J Palou, A Breda
Department of Urology, Fundació Puigvert, Barcelona, Spain
MP08‐06
Uretero‐enteric Anastomotic Stricture Following Robotic Radical Cystectomy: Extracorporeal versus Intracorporeal Approaches in the Indocyanine Green Era
MB Tuna, T Doganca, OB Argun, I Tufek, SM Keskin, C Obek, AR Kural
Acibadem Maslak Hospital, Department of Urology
MP08‐07
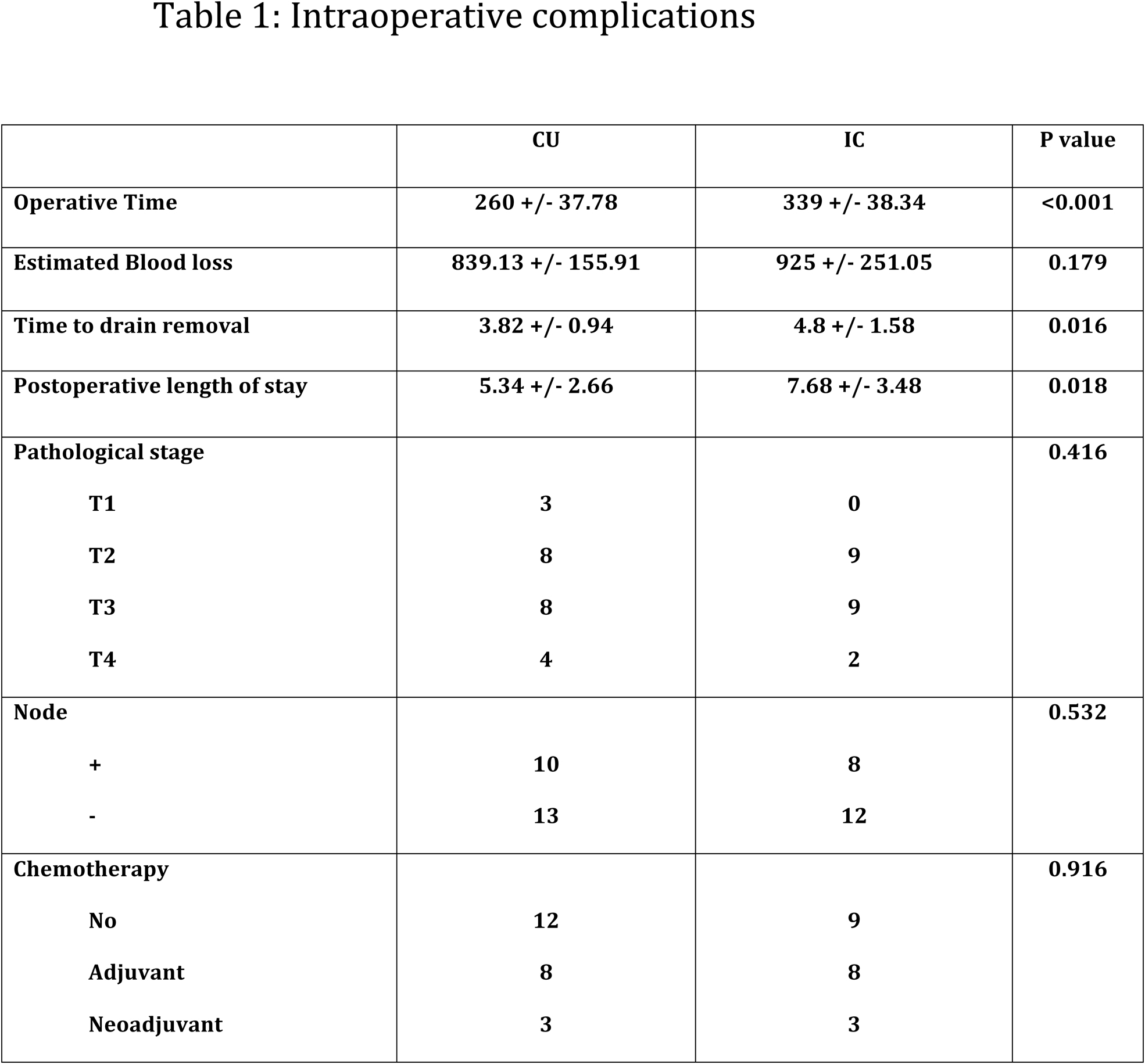
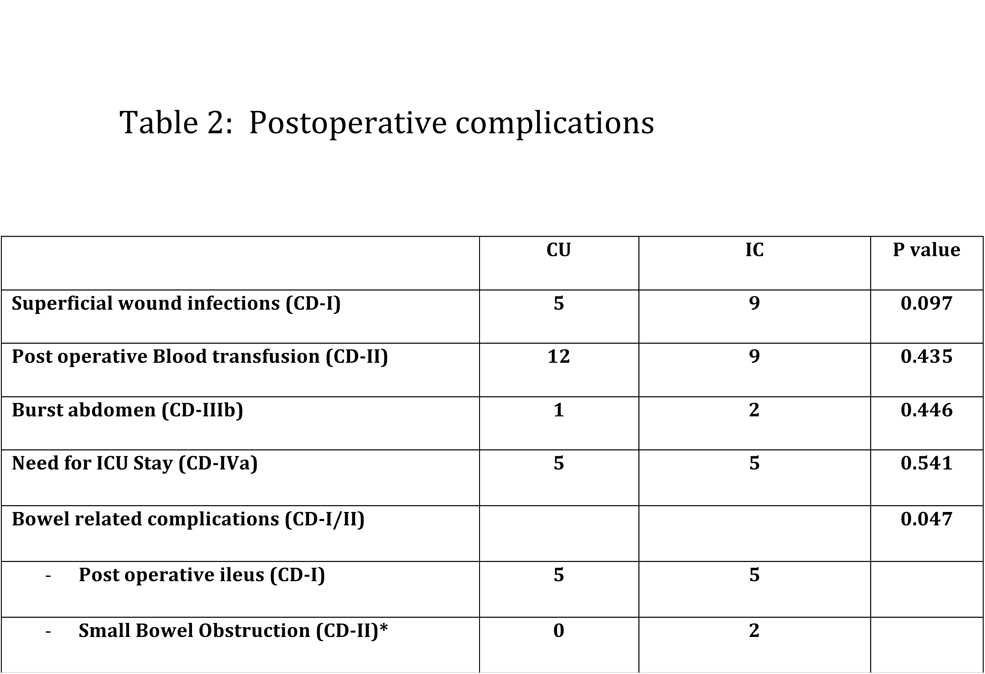
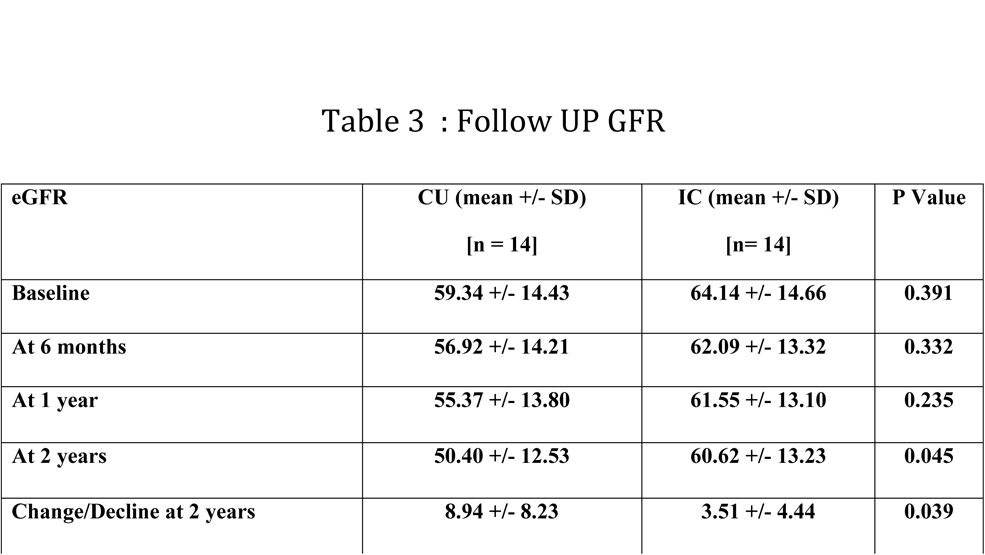
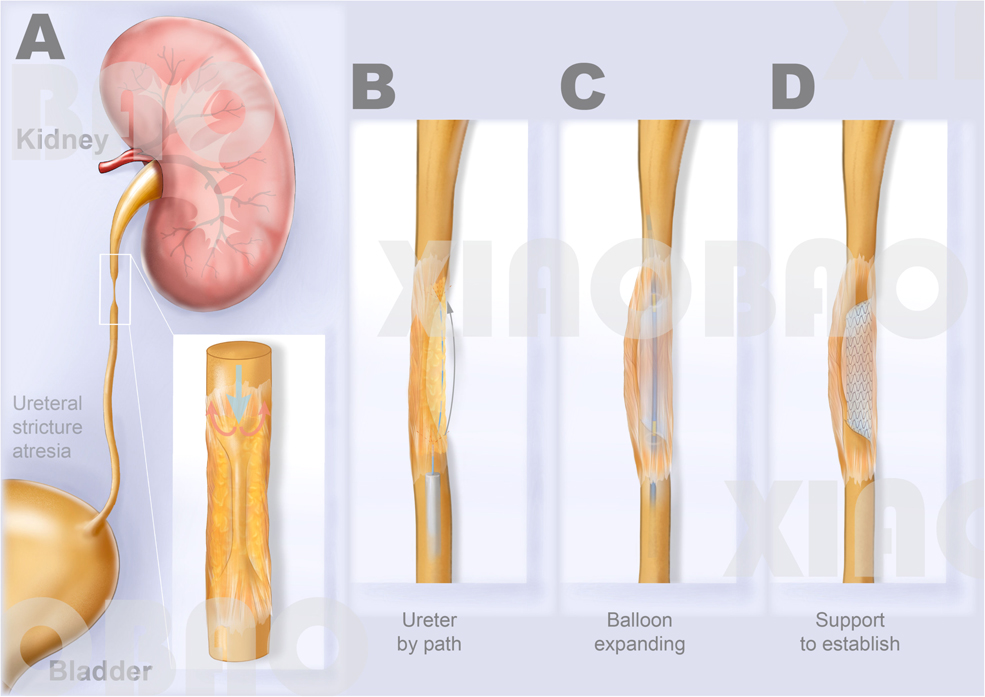
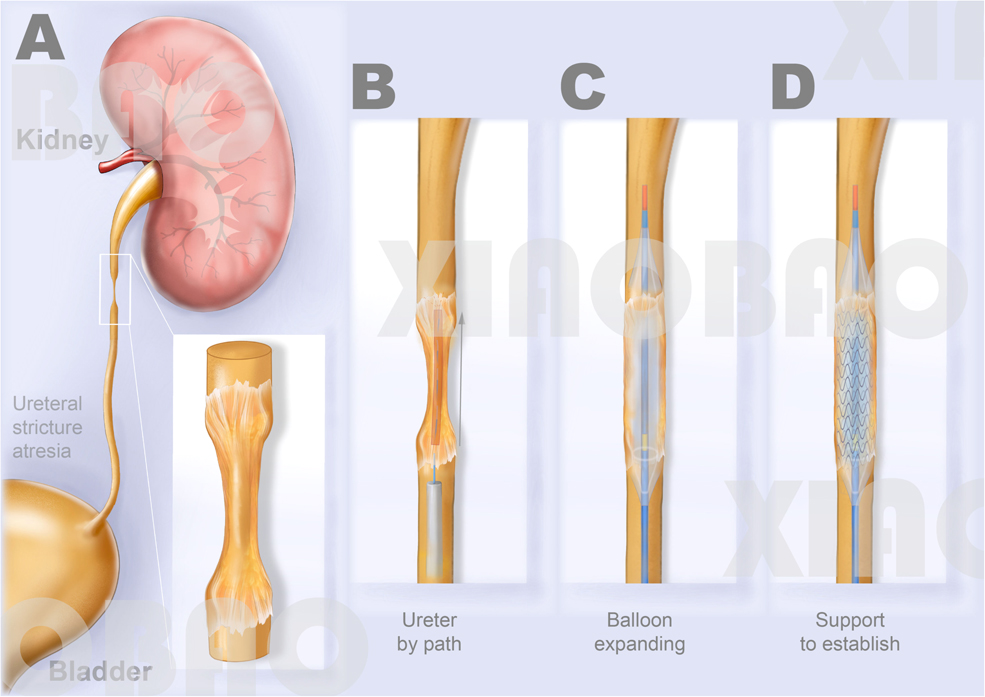
Ureteral bypass: a new technique for the treatment of ureteral atresia
X Gao, J Chen, W Wang, X Wei
Department of Urology, Institute of Urology (Laboratory of Reconstructive Urology), West China Hospital, Sichuan University, Chengdu, Sichuan, P.R. China
MP08‐08
Retroperitoneoscopic pyeloplasty for primary UPJ obstruction in Horseshoe kidney: Experience of a tertiary care center from Northern India
V Singh, RJ Sinha, G Singh
Dept of urology, King George Medical University
MP08‐09
Laparoscopic Boari Flap for the management of long segment ureteral defect: Long term follow‐up
V Singh, RJ Sinha, G Singh
Dept of urology, King George Medical University
MP08‐10
Reconstruction of obliterated ureteral strictures is associated with increased difficulty
RA Lee, Z Lee, AM Asghar, D Strauss, R Harrison, N Cheng, LC Zhao, M Stifelman, DD Eun
Lewis Katz School of Medicine ‐ Temple University Hospital
MP08‐11
Ureteral Reimplantation without Anti‐reflux Technique for Iatrogenic Ureterovaginal Fistula: Open Surgery vs. Laparoscopic Repair
Q He, D Luo, K Wang
Department of Urology, Institute of Urology (Laboratory of Reconstructive Urology), West China Hospital, Sichuan University, Chengdu, Sichuan, P.R.C
MP08‐12
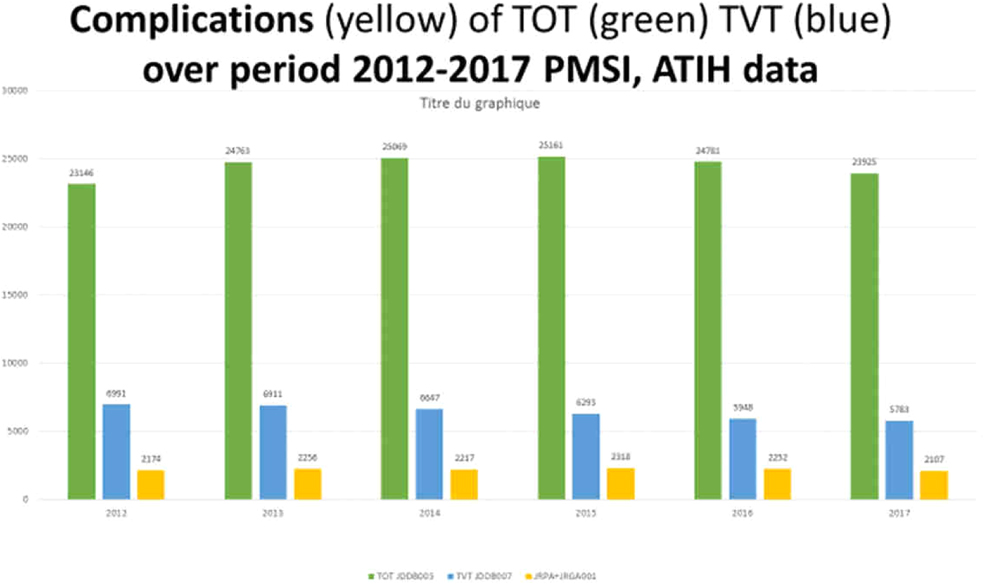
TOT‐TVT results revisited : an overestimated facility and an underestimated complication rate. Report on 280.000 cases in France (period 2009‐2018)
M Devonec
GH Lyon‐Sud, Urology department
MP08‐13
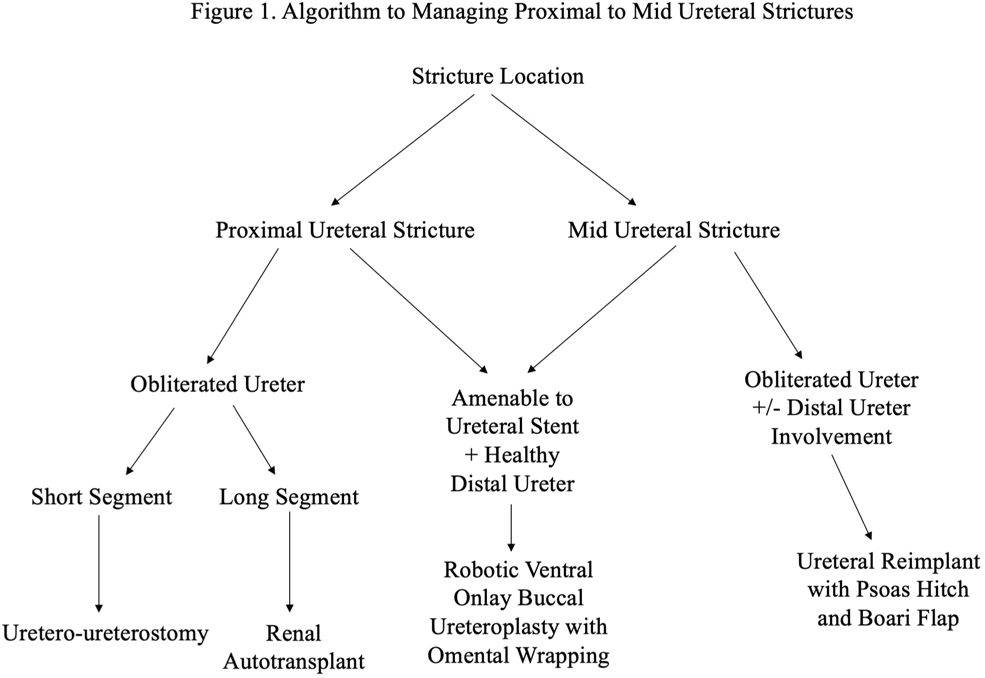
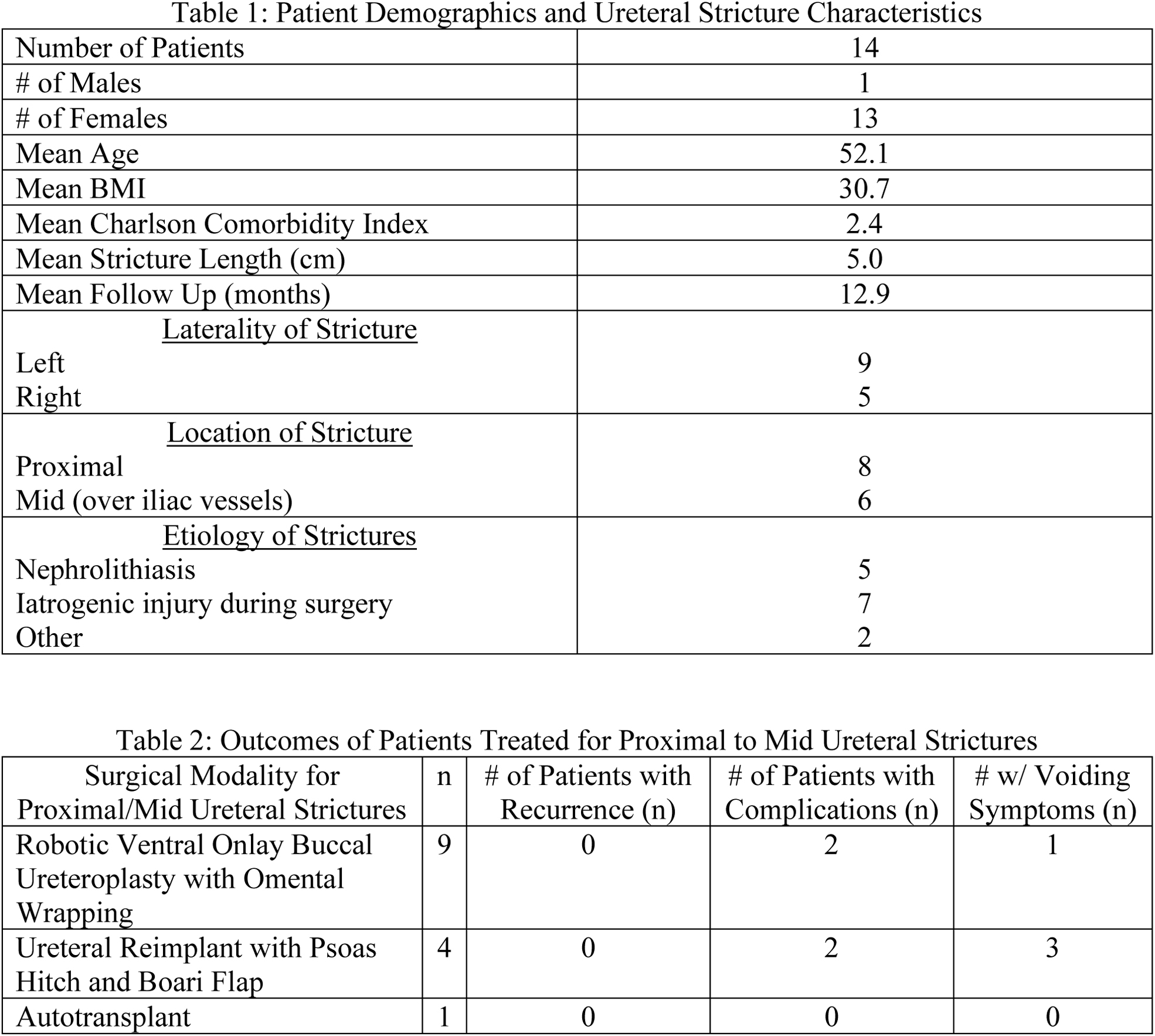
Buccal, Boari, or Autotransplant over Bowel: Management of Proximal to Mid Ureteral Strictures
K Radadia, AK Chow, KG Sands, S Ogawa, B Patel, K Du, E Kim, RS Figenshau, G Murphy
Washington University School of Medicine
MP08‐14
1‐year Outcome After Bilateral Uterosacral Ligament Replacement ‐ Comparison of Abdominal and Laparoscopic Surgical Techniques in Treatment of Pelvic Organ Prolapse and Urinary Incontinence
S Ludwig, F Thangarajah, C Eichler, B Morgenstern, P Mallmann
University of Cologne, Dept. of Obstetrics and Gynecology, Div. of Pelvic Floor Reconstructive Surgery
MP08‐15
Ureteral injuries: long term results of endoscopic ureteral realignment
H Johnson, S Parsons, P Mezes, G Collin, N Collin, J Philip
Bristol Urological Institute
MP08‐16
Differences in Surgical Treatment of De Novo Urge Incontinence Occurring Post‐Holmium Laser Enucleation of the Prostate
L Richards, BB Whiles, D Mazzotti, K Thurmon
University of Kansas Medical Center
MP08‐17
Application of bladder muscle flap in upper and/or middle ureteral stricture (9 cases)
Y Yuan, Z Zhang, W Yuting, L Folin, Z Guoxi, X Zou
MP08‐18
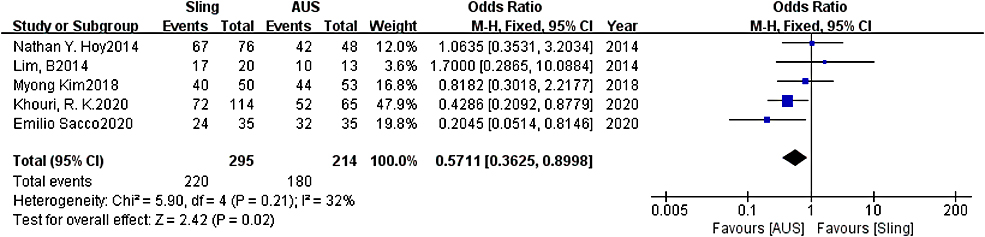
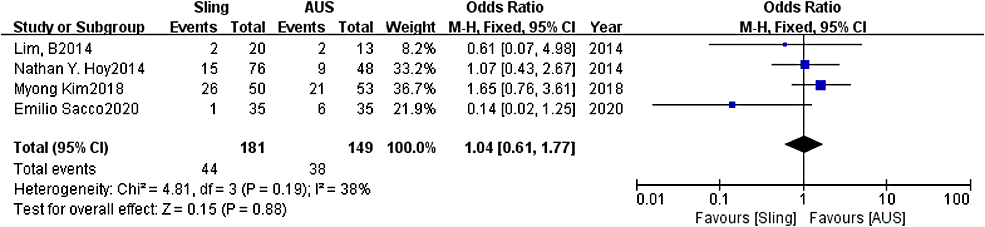
Artificial Urinary Sphincter Is Better than Slings for Moderate Male Stress Urinary Incontinence with Acceptable Complication Events: A Systematic Review and Meta‐analysis
L Lin, L Zhou, H Li, K Wang
MP08‐19
Robotic buccal ureteroplasty: early single institutional outcomes
MS Tonzi, B Waldorf, J Lange
University of Tennessee College of Medicine at Chattanooga
MP08‐20
Robotic assisted Vesico‐vaginal fistula repair: Our technique and outcomes
R Batra, A Singh, A Ganpule, R Sabnis, M Desai
Muljibhai Patel Urological Hospital, Nadiad
MP08‐21
Clinical outcomes of endoureterotomy on ureteral strictures which lasts after resolution of extrinsic benign causative disease
J Kim, S Bang, K Ko, J Chung, W Song, M Kang, H Sung, M Baek, S Jeon, K Lee, D Han
Department of Urology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, South Korea
MP08‐22
Treatment of mild to moderate stress urinary incontinence using the stromal‐vascular fraction of autologous adipose tissue
AO Papoyan, C Maксимовa, R Safiullin, V Pavlov, R Kazikhinurov
Utilizing da Vinci® Robotic Surgical System to Treat Challenging Urinary Stone
MW Salkini, A Dahman
West Virginia University
MP09‐02
Establishing the Japanese version of the Wisconsin Stone Quality of Life questionnaire (WISQOL)
K Taguchi, T Okada, S Hamamoto, S Okada, T Inoue, A Okada, T Yasui
Nagoya City University Graduate School of Medical Sciences
MP09‐03
Predictors of index percutaneous nephrolithotomy care setting and impact on perioperative outcomes and cost
SK Bechis, DF Friedlander, R Sur
University of California ‐ San Diego, Department of Urology
MP09‐04
Utilization of antibiotic irrigation and betadine for renal pelvis sterilization during PCNL to decrease infectious complications
D Mikhail, L Nyman, E Lynch, A Rai, T Aro, AD Smith, D Hoenig, Z Okeke
Lenox Hill/Northwell Health
MP09‐05
Opiates can be replaced with ‘music and mood lighting’ during lithotripsy: Comparative outcomes from ‘South Coast Lithotripsy Centre’
M Ramachandra, A Pietropaolo, L Tear, D Tanya, A Davies, S Miles‐board, A Humphrey, BK Somani
University Hospital Southampton, UK
MP09‐06
Complication rates after percutaneous nephrolithotomy in patients with neurological Conditions
A Garbens, V Kommidi, H Trivedi, JA Antonelli, M Pearle, BA Johnson
UT Southwestern
MP09‐07
Withdrawn
MP09‐08
Safety and Efficacy of Simultaneous Bilateral Percutaneous Nephrolithotomy: A Matched Retrospective Cohort Study
VK Wong, CJ Lundeen, R Paterson, KB Scotland, BH Chew
MP09‐09
Impact of Reverse Trendelenburg Position on Ureteral Stone Retropulsion: A Prospective Randomized Study
JA Khusid, H Anastos, R Chandhoke, D Lundon, AS Sadiq, J Bamberger, B Gallante, WM Atallah, M Gupta
Icahn School of Medicine at Mount Sinai
MP09‐10
Comparative effectiveness of empiric preventative pharmacologic therapies on stone recurrence among patients with urinary stone disease
R Hsi, P Yan, J Crivelli, V Shahinian, JM Hollingsworth
Vanderbilt University School of Medicine
MP09‐11
Initial experience of miniaturised PCNL with Swiss LithoClast® Trilogy: a European multicentre prospective study on behalf of ESUT
N Thakare, F Tanse, K Saeb‐Parsy, N Atassi, R Endriss, G Kamphuis, D Perez‐Fentes, M Hasan, M Brehmer, PJ Osther, HU Jung, BW Turney, W Finch, N Burgess, S Irving, L Dragos, E Liatsikos, T Knoll, V Cauni, O Wiseman
Cambridge University Hospitals Nhs Trust
MP09‐12
Some pulse types are more equal than others: A comparison of different pulse modulation modes for Holmium:YAG laser lithotripsy ablation in a benchtop model
RS Terry, D Ho, D Scialabba, P Whelan, R Qi, C Tabib, F Soto‐Paulo, B Ketterman, GM Preminger, P Zhong, M Lipkin
Duke University
MP09‐13
Reducing the incidence of unnecessary negative ureteroscopy with pre‐operative computed tomography for ureteric stones ≤7 mm
R Peggs, S Vaggers, T Tien, L Crabtree, S Folkard, K Atalar, Y Khan, S Graham, P Pal
Homerton University Hospital NHS Foundation Trust
MP09‐14
Impact of various refinements on a longitudinal 18 years consecutive series of percutaneous nephrolithotomy
H Hertzberg, Z Savin, I Masarwe, A Beri, O Yossepowitch, M Sofer
MP09‐15
Efficacy and safety of fluoroless ureteroscopy and retrograde intrarenal surgery for the treatment of urolithiasis: a comparative study
C Laranjo Tinoco, A Coutinho, A Cardoso, R Matos Rodrigues, S Anacleto, P Passos, E Lima, M Cerqueira Alves, P Mota
Hospital de Braga, EPE
MP09‐16
A Nomogram for Prediction of the Risk of Kidney Stone: A physical examination population‐based Study
H Qibo, J xi, t huairong, H Yan, W Kunjie
MP09‐17
Does the Use of Moses Technology Increase Efficiency During Flexible Ureteroscopy for Stone Disease? Single Center Experience
MA Knoedler, S Li, SL Best, SP Hedican, KL Penniston, SY Nakada
University of Wisconsin, Department of Urology
MP09‐18
Continued Aspirin Use during PCNL Surgery
H Brar, P Orji, S Agrawal, M Eila, J Fulla, B Li, P Prasanchaimontri, J Li, S De
Cleveland Clinic
MP09‐19
PerCutaneous Nephro‐ Lithotomy (PCNL): Minimum Hospital volume required to achieve financial sustainability in the UK
A Jha, C Ho, L Simmons, N Collin, J Philip
Bristol Urology Institute
MP09‐20
Kidney Stone Surgical Interventions: Nationwide Interest Trends and Qualitative Assessment of Popular Resources on Social Media from 2016‐2021
P Diaz, RA Takele, S Thaker, KN Thaker, J Ballon, KB Scotland
Department of Urology, UCLA
MP09‐21
How to evaluate a flexibleureterorenoscope? Systematic mapping of existing evaluation methods
N Hendriks, MM Henderickx, BM Schout, J Baard, FS van Etten‐Jamaludin, HP Beerlage, RC Pelger, GM Kamphuis
Amsterdam UMC
MP09‐22
Efficiency and Effectiveness for Ureteroscopic Stone Removal: Dual Lumen vs a Single Lumen Ureteroscope
A Brevik, A Peta, L Limfueco, R Karani, L Xie, R Arada, J Sung, FA Jefferson, E Parkhomenko, D Lama, S Safiullah, P Jiang, RM Patel, RV Clayman, J Landman
Department of Urology, University of California, Irvine
Moderated Poster Session 10: BPH II
MP10‐01
Prostatic Urethral Lift real‐world experience is consistent with controlled trial results in both non‐retention and retention subjects
NJ Barber, KL Ng, SN Gange, G Eure, M Rochester
Frimley Park Hospital
MP10‐02
Real‐World and Controlled Trial Predictors of Durability after Prostatic Urethral Lift (PUL)
NJ Barber
Frimley Park Hospital
MP10‐03
Continuous mode bipolar plasma vaporization of the prostate–Still a “go” after 6 years of follow‐up?
BF Geavlete, C Moldoveanu, C Ene, C Bulai, A Ene, PA Geavlete
“Saint John” Emergency Clinical Hospital, Department of Urology
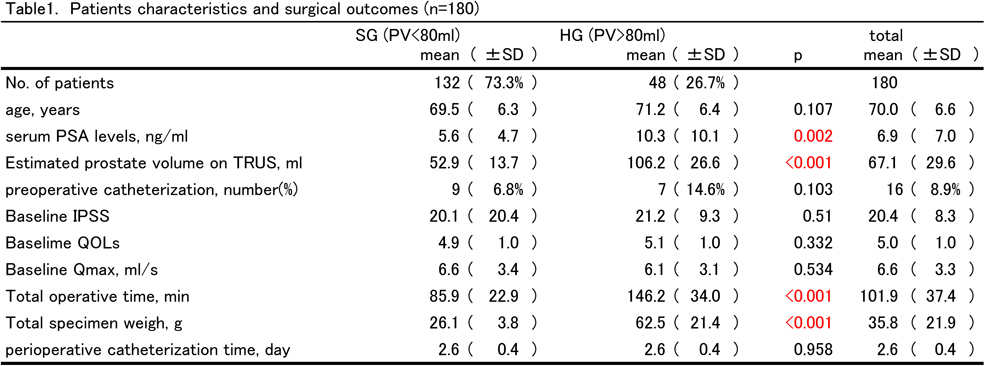
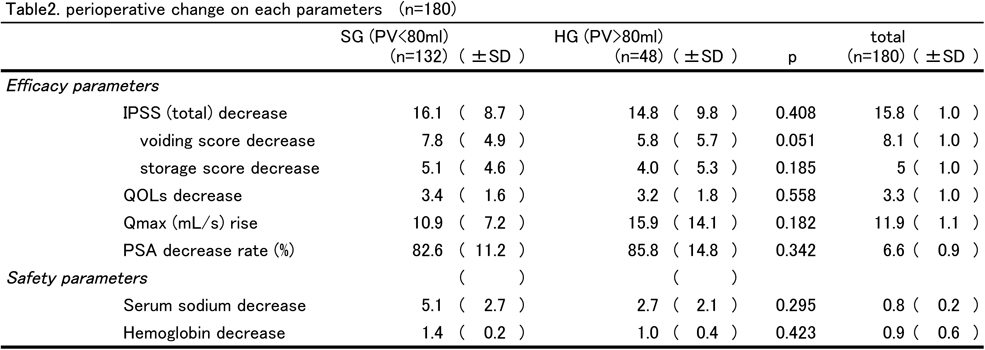
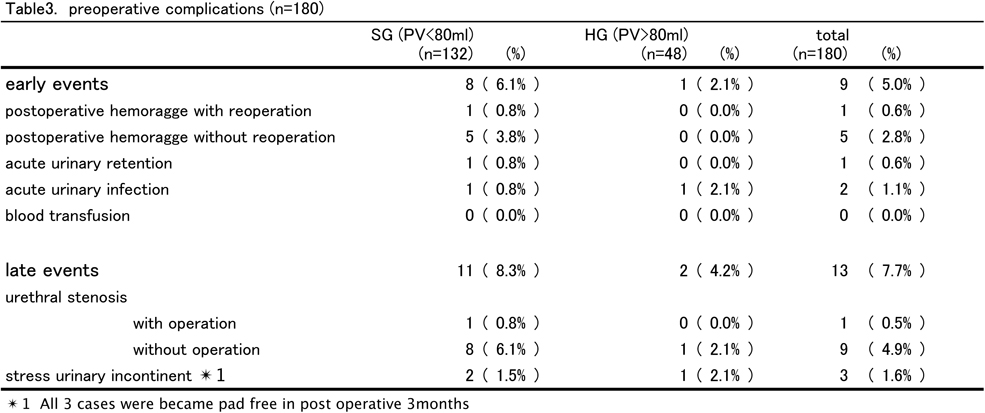
MP10‐04
Outcome of TransUrethral Enucleation with Bipolar(TUEB) in patients with huge prostate hyperplasia : comparison of prostate volume more than 80ml with less
Y Endo, H Shimizu, J Akatsuka, Y Kondo
Nippon Medical School
MP10‐05
Single Surgeon Experience with Procept Aquabeam Aquablation of Prostate: First 55 Cases (with 18‐month Follow‐up)
A Kasraeian, M Alcantara, K Mola Alcantara
Kasraeian Urology
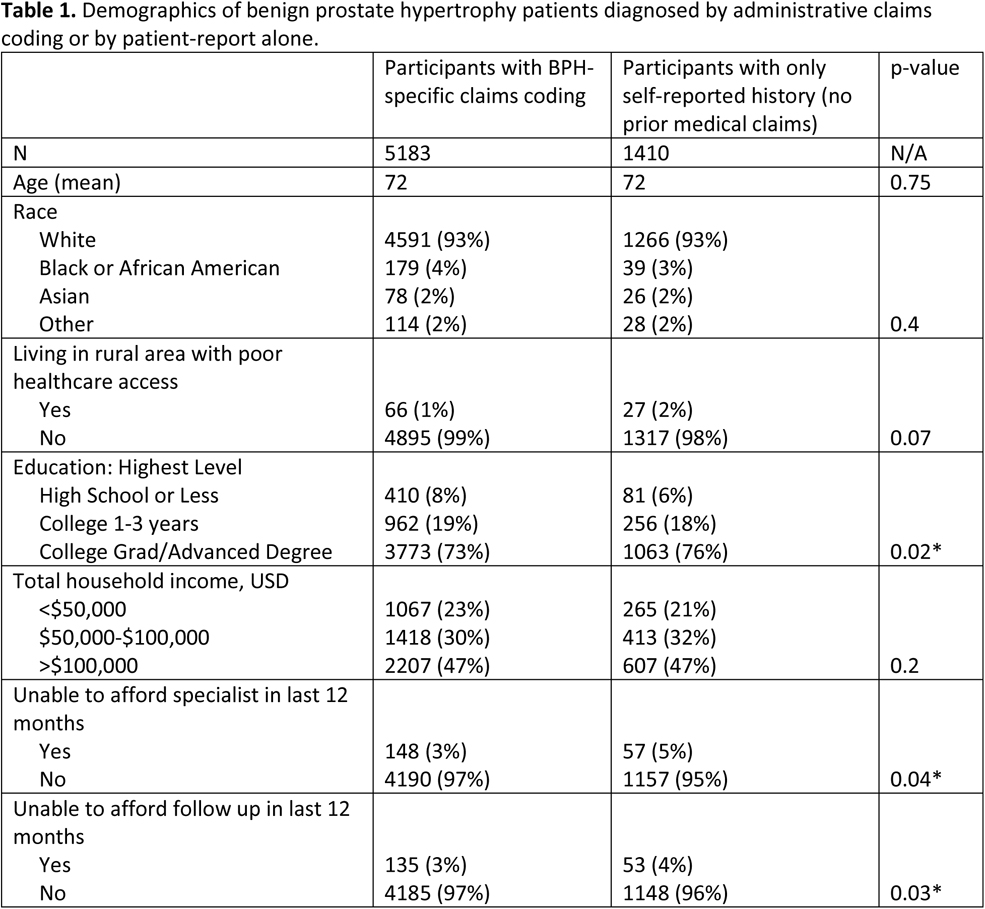
MP10‐06
Patients with self reported benign prostate hyperplasia without medical claims data have barriers to healthcare access
CM Forbes, R Hsi, NL Miller
Vanderbilt University Medical Center, Department of Urology
MP10‐07
12‐month Outcomes from the Large Real‐World Study and Urodynamic Results from PULSAR Demonstrate PUL is Safe and Effective in Retention Patients
M Rochester, NJ Barber, O Kayes, N Thiruchelvam, K Rajesh, T Page, G Eure, D Grier
Norfolk and Norwich University Hospital
MP10‐08
Interim 2 Year Results for the EVEREST‐I Trial Evaluating the Optilume BPH Catheter System
O Kayes, S Kaplan, M Pichardo, E Rijo Cedano, R Rodriguez‐Lay, G Espino, R Estrella
St James's University Hospital
MP10‐09
Withdrawn
MP10‐10
Management of benign prostatic hyperplasia with high tight bladder neck with minimally invasive approach of mini bladder neck distraction and prostatic urethral lift
KL Ng, NJ Barber
Frimley Park Hospital
MP10‐11
ThuLEP vs open simple prostatectomy for the treatment of prostates larger than 150 cc
M Maltagliati, L Berti, U Besana, C Buizza, M Sighinolfi, S Micali, BC Rocco, G Bozzini
ASST Valle Olona
MP10‐12
Evaluation of the learning curve for aquablation therapy of the prostate: a single‐center analysis
K Vogt, B Becker, AJ Gross, C Netsch
Department of Urology, Asklepios Hospital Barmbek, Hamburg, Germany
MP10‐13
Comparison of vaporization and enucleation techniques based on the functional outcomes and complications of patients with benign prostatic hyperplasia: systematic review and meta‐analysis
A Shpikina, A Morozov, M Taratkin, A Novikov, D Enikeev
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia
MP10‐14
The impact of benign prostatic hyperplasia surgery on erectile function: a systematic review and network meta‐analysis of randomized‐controlled trials
D Jabarkhyl, A Light, O El Hage, P Dasgupta
GKT School of Medical Education, King's College London
MP10‐15
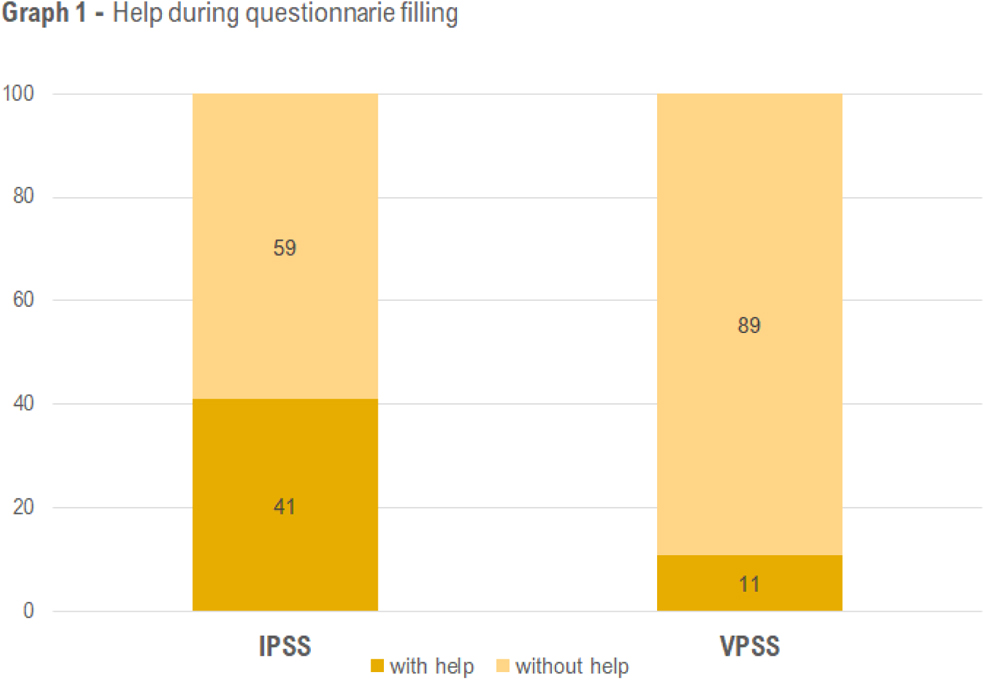
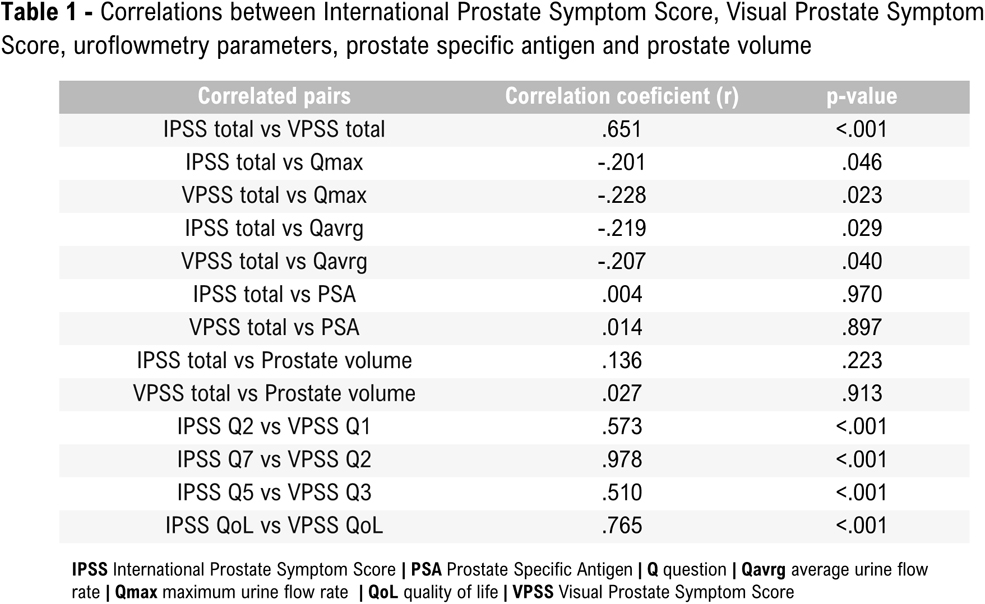
New Visual Prostate Symptom Score versus International Prostate Symptom Score in Men with Lower Urinary Tract Symptoms: a prospective comparison
C Laranjo Tinoco, F Diaz Ferreira, A Cardoso, R Matos Rodrigues, S Anacleto, P Passos, E Lima, M Cerqueira Alves, CA Oliveira
Hospital de Braga, EPE
MP10‐16
Withdrawn
MP10‐17
Withdrawn
MP10‐18
SoracteLite® Transperineal Laser Ablation as Novel Minimal Invasive Treatment for Benign Prostatic Obstruction: Initial Results of a Pilot Study
R van Kollenburg, LA van Riel, JR Oddens, TM de Reijke, HP Beerlage, M de Bruin
Department of Urology, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, the Netherlands
MP10‐19
Withdrawn
MP10‐20
Analysis of outcome of prostatic UroLift placement in benign enlargement of prostate in a District Hospital
K Biswas, S Ahmed, K Soundararasha, G Rix, R Pillai, J Corr, Z Maan, S Datta
Colchester General Hospital
MP10‐21
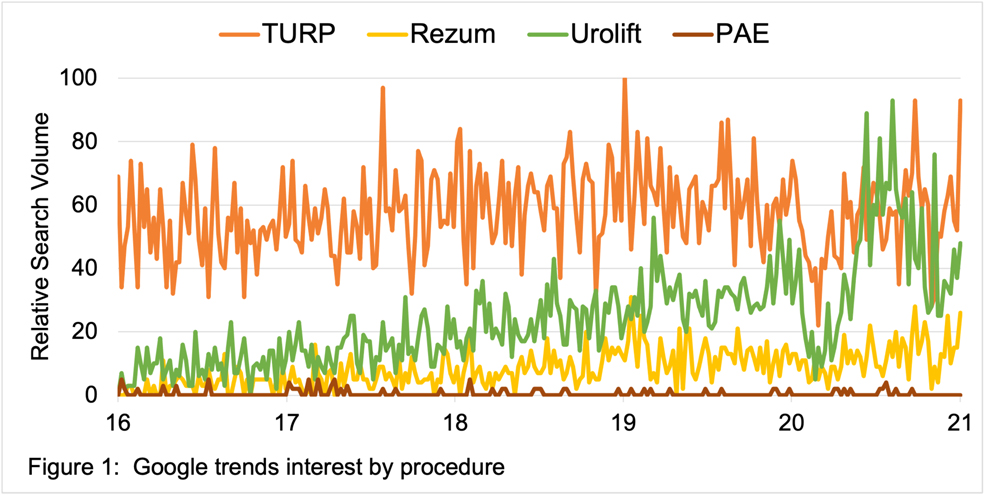
Online engagement with treatments for benign prostatic hyperplasia: Is interest in Urolift outpacing the gold standard?
MI Lucas, P Diaz, F Escobedo, B Limbrick, KB Scotland
Department of Urology, UCLA
MP10‐22
Major postoperative complications after Aquablation: initial experience
A Hambaryan, A Kugler, R Badalyan, T Krause, W Schafhauser
Klinikum Fichtelgebirge
Moderated Poster Session 11: Stones IV: PNL & URS
MP11‐01
Miniperc represents an effective middleground between standard PCNL and RIRS in the treatment of small to medium size stones
S Proietti, L Rico, M Pavia, MJ Basulto‐Martínez, Y Yeow, L Villa, E Ventimiglia, A Salonia, F Gaboardi, G Giusti
IRCCS Ospedale San Raffaele, Milan, Italy
MP11‐02
A randomized controlled trial of removal of asymptomatic small renal stones at the time of symptomatic stone removal
M Sorensen, JD Harper, M Borofsky, T Hameed, K Smoot, B Burke, B Levchak, MR Bailey, JC Williams, Z Liu, JE Lingeman
Indiana University
MP11‐03
Treatment of difficult ureteroscopy retreat due to rigid ureterostercopy incarcerated in ureter (report of 18 cases)
R Huang, X Rihai, W Xiaoning, L Folin, X Tianpeng, Z Guoxi, X Zou
MP11‐04
Revisiting the role of Oxalobacter formigenes in kidney stone formation: a deep dive into the microbiome at multiple body sites
KF Al, B Joris, JD Denstedt, J Chmiel, J Bjazevic, GB Gloor, H Razvi, JP Burton
MP11‐05
Ketorolac to reduce ureteroscopy symptoms trial
J Syed, AI Khan, M Goland‐Van Ryn, P Motamedinia
Yale University School of Medicine
MP11‐06
Which Endoscopic Methods in Prepubertal Patients with 10‐20 mm Bladder Stones: Transurethral Cystolithotripsy or Percutaneous Cystolithotripsy?
MM PİSKİN, MS Özkent, YE Goger, MT Kilinc, MS Sönmez
Konya City Hospital
MP11‐07
The Impact Of Metabolic Syndrome Components On Urinary Parameters and Risk of Stone Formation
JN Bamberger, DC Rosen, JA Khusid, E Kaplan‐Marans, B Gallante, A Kapoor, I Paranjpe, D Atashokhan, WM Atallah, AS Sadiq, M Gupta
Icahn School of Medicine at Mount Sinai
MP11‐08
Evaluating the use of a patient‐specific hydrogel model to measure the effects of various experimental conditions on renal pelvis pressure during ureteroscopy
R Melnyk, D Foster, A Ghazi
University of Rochester Medical Center Department of Urology
MP11‐09
Upper Pole Prone PCNL is Safe and Efficacious for Horseshoe Kidneys with High Volume Nephrolithiasis
DT Rubio, JA Abraham
National Kidney and Transplant Institute
MP11‐10
Beware the bolus size: Understanding intrarenal pressure during ureteroscopic fluid administration
J Lazarus, L Kaestner, P Wisniewski, S Yekani
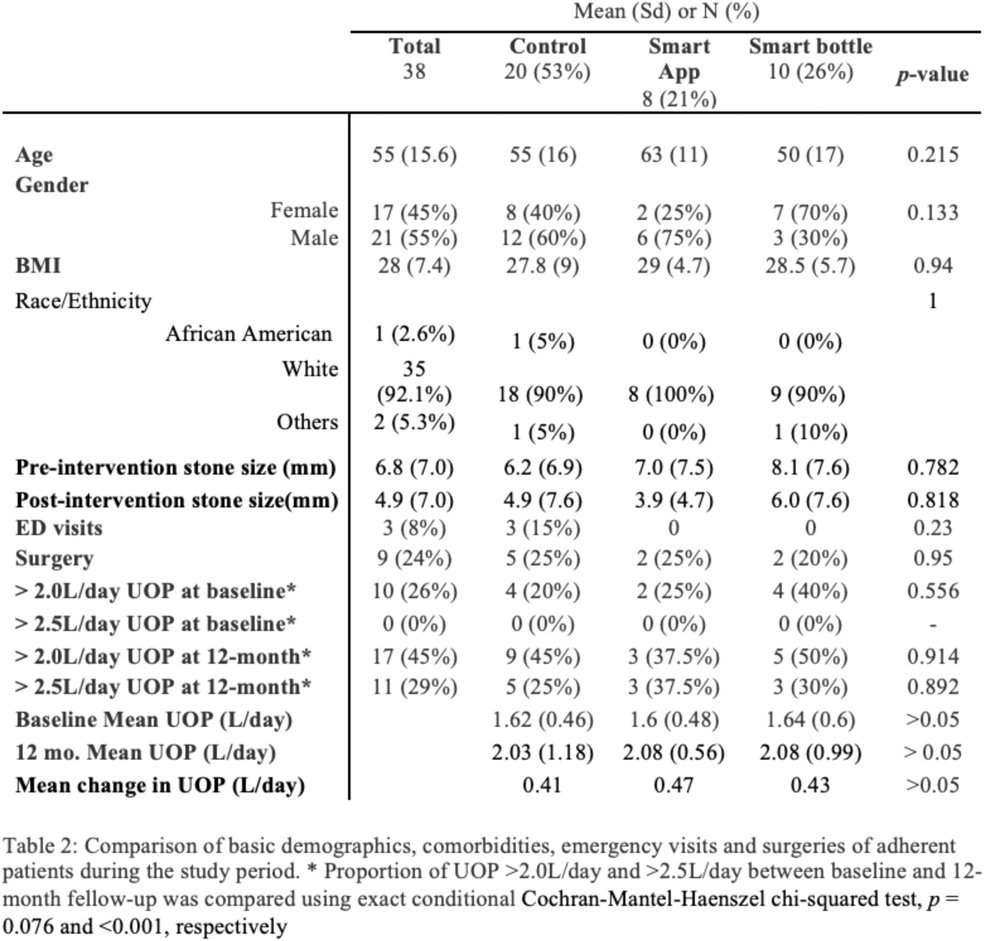
MP11‐11
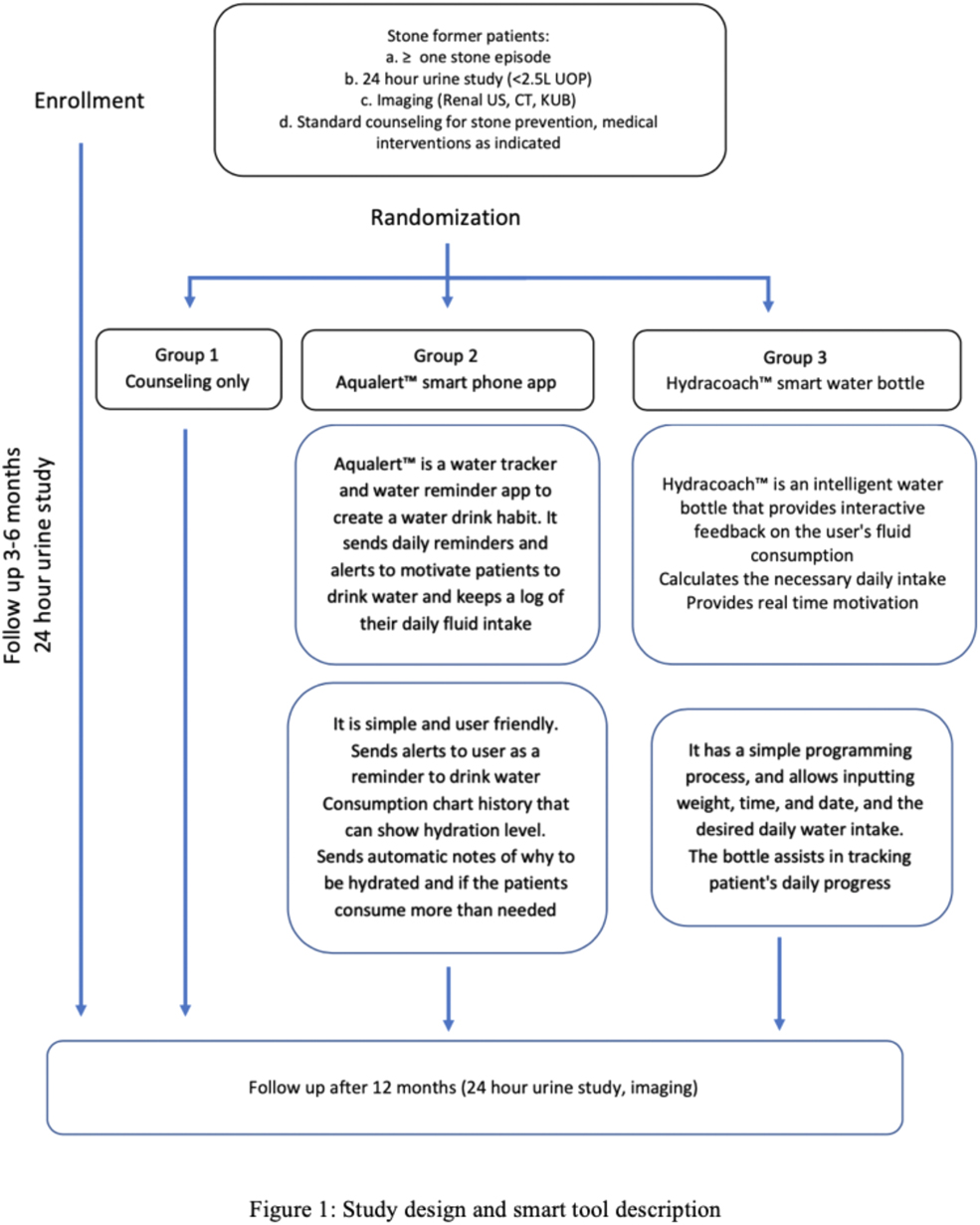
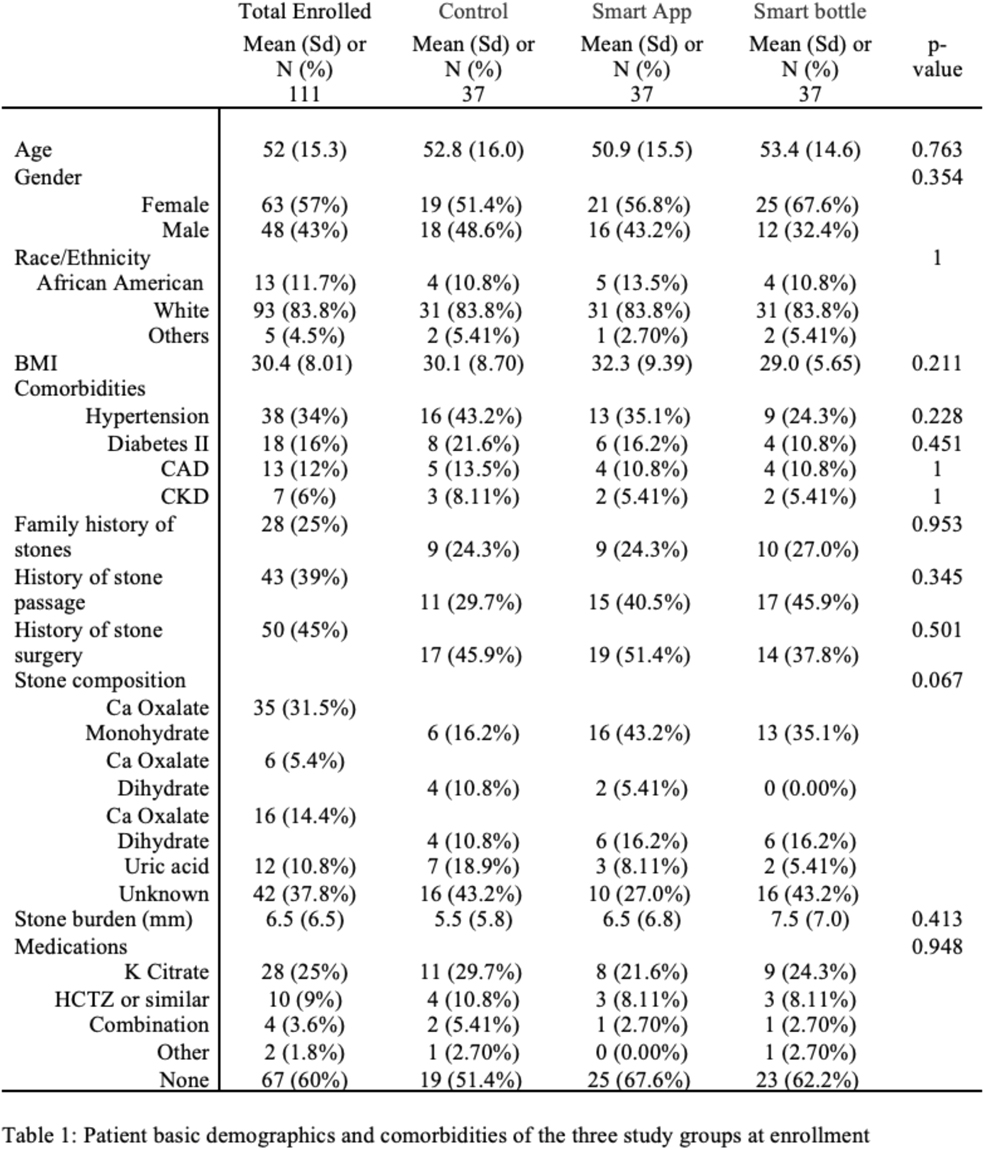
Can Smart Technology Improve Adherence to Fluid Management and Urine Output in Kidney Stone Patients? A Prospective Randomized Study
HC Wright, L Alshara, H DiGennaro, Y El Kassis, J Li, M Monga, J Calle, S Sivalingam
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
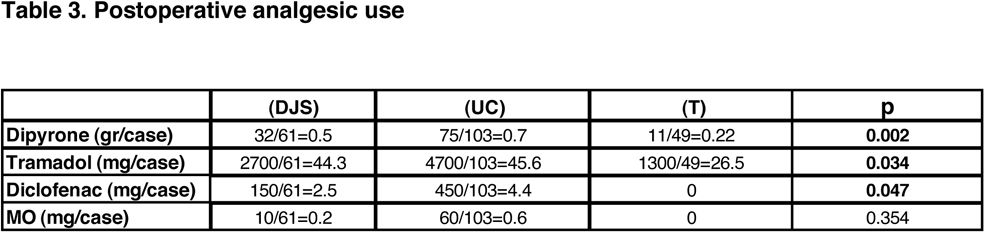
MP11‐12
Tubeless ureterorenoscopy. Our experience using 120‐W laser and dusting technique. Postoperative pain, complications and readmissions
G Verhovsky, M Haifler, E Gnessin, I Leotsakos, M Duvdevani, YI Siegel, A Zisman, IM Sabler
Shamir (Asaf HaRofeh) MC
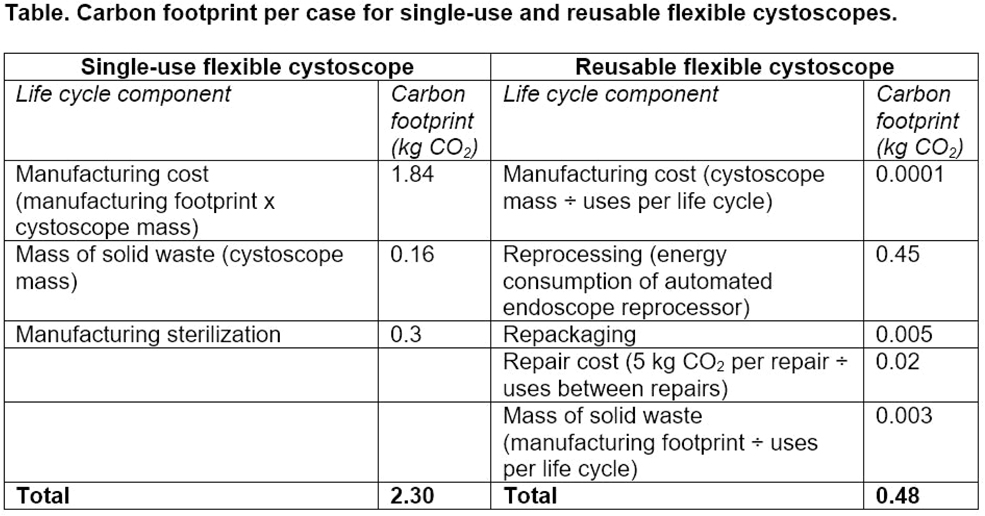
MP11‐13
The Cost of Convenience: Estimating the Environmental Impact of Single‐Use and Reusable Flexible Cystoscopes
K Koo, JS Winoker, S Patel, ZT Su, AM Potretzke, BR Matlaga
Mayo Clinic
MP11‐14
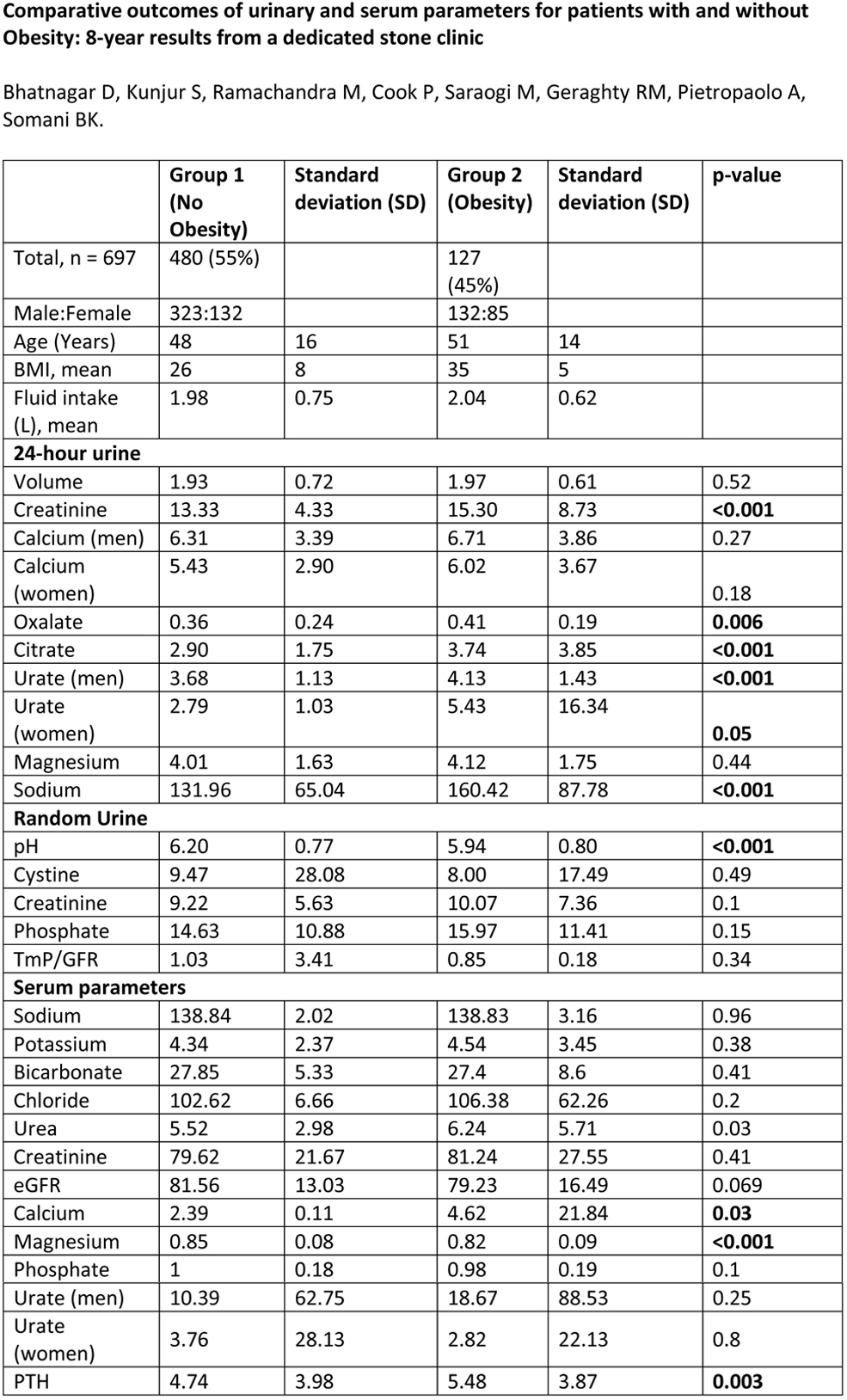
Comparative outcomes of urinary and serum parameters for patients with and without Obesity: 8‐year results from a dedicated stone clinic
D Bhatnagar, S Kunjur, M Ramachandra, P Cook, M Saraogi, R Geraghty, A Pietropaolo, BK Somani
University Hospital Southampton, UK
MP11‐15
Does the Urologist or Technologist Have More Influence on SWL Treatment Outcomes?
RG Seltzer, KJ Hamawy, BD Hamilton
Translational Analytics and Statistics
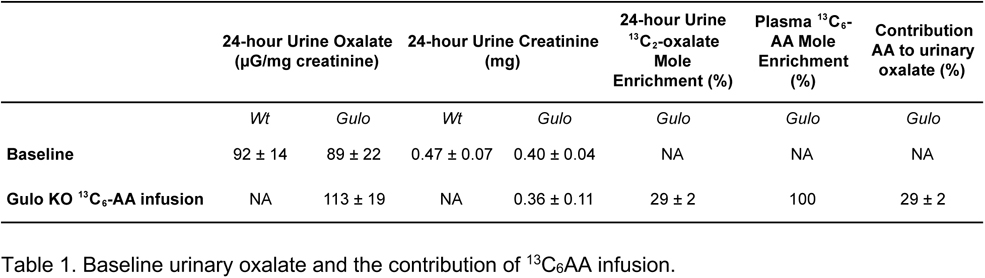
Mp11‐16
The Contribution of Ascorbic Acid to Urinary Oxalate in Mouse Model
J Crivelli, K Wood, Z Burns, R Holmes, DG Assimos, J Knight
The University of Alabama
MP11‐17
SWL Focus ‐ Does sizes matter?
J Veser, V Jahrreiss, C Seitz
MP11‐18
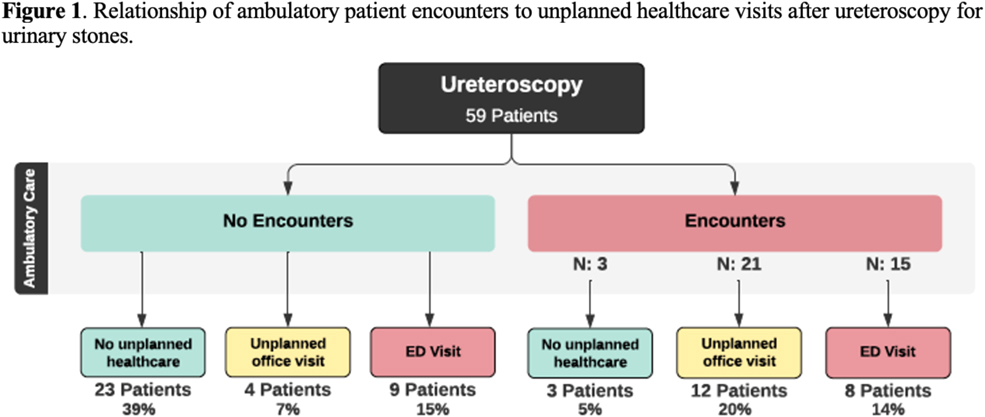
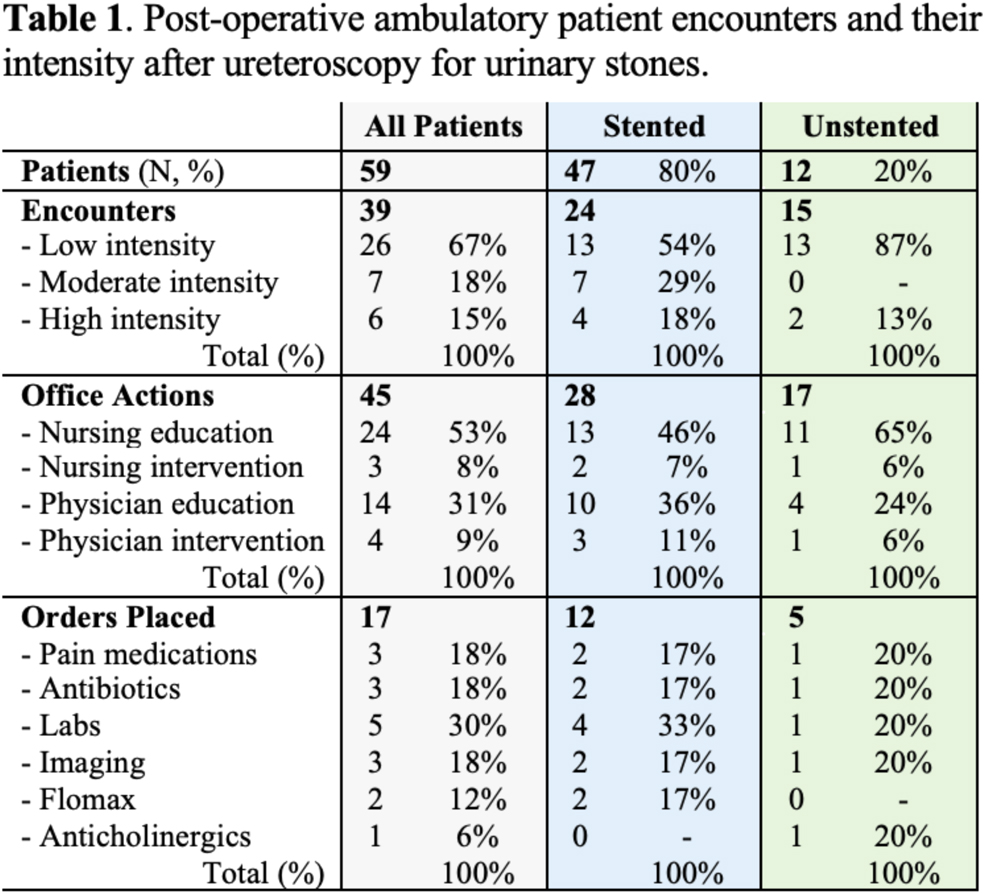
Failure to rescue? Ambulatory healthcare utilization after ureteroscopy for stone disease in a surgical collaborative
J DiBianco, R Navarrete, B Conrado, S Daignault‐Newton, CA Dauw, KR Ghani, f Urological Surgery Improvement Collaborative
Department of Urology, University of Michigan
MP11‐19
Pre‐operative stone volume measurement program (qSAS) is best predictor of percutaneous nephrolithotomy (PCNL) operative time and stone free rate
M Meagher, T Chiou, R Sur, SK Bechis
University of California ‐ San Diego, Department of Urology
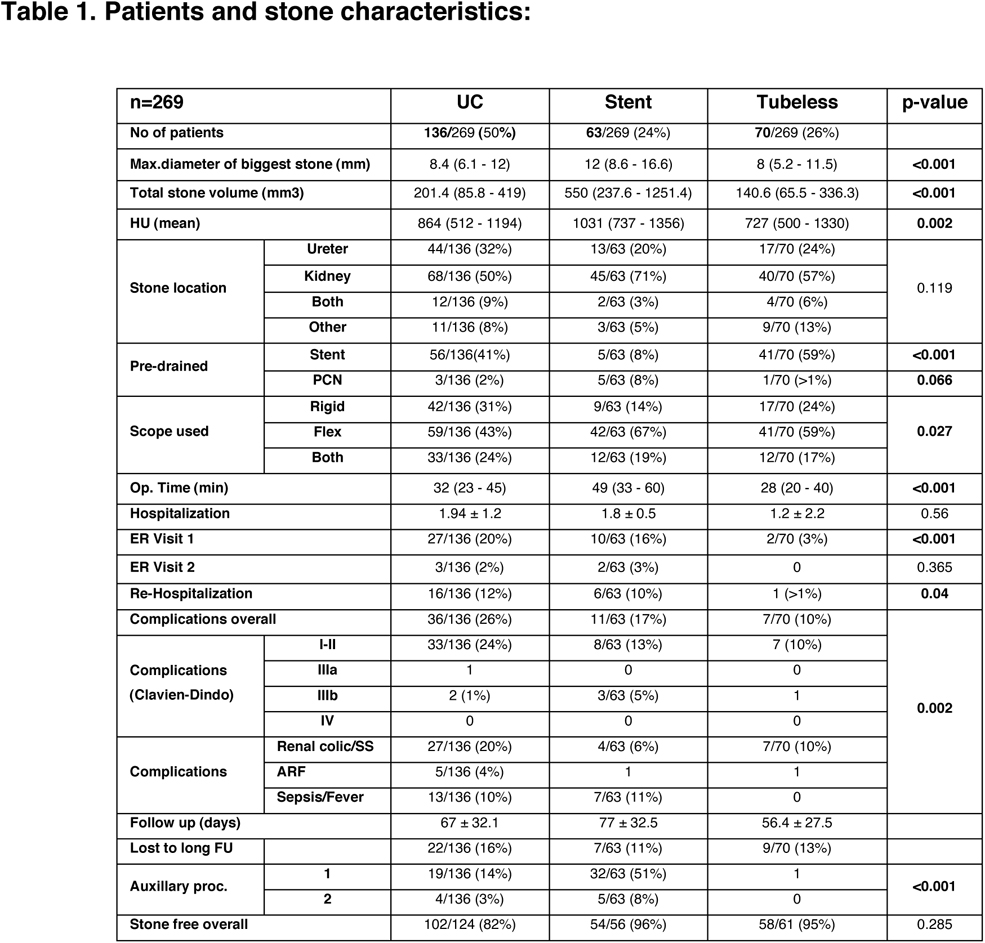
MP11‐20
Is percutaneous drainage a necessary exit strategy after supine percutaneous nephrolithotomy (PCNL)? Trends from a contemporary series
Z Sheng, R Warner, G Caddeo
University Hospitals of Derby and Burton NHS Foundation Trust
MP11‐21
Muscle Activation During Simulated Flexible Ureteroscopy: Effects of Surgeon Position and Scope Type
G Gheordunescu, K O'Laughlin, A Sun, J Fulla, N Kachroo, HC Wright, S De
Case Western Reserve University School of Medicine, Cleveland, OH, USA
MP11‐22
Management of nephrolithiasis with a large ureteral access sheath is not associated with increased risk of surgical complications and stricture formation on long term follow up
K Breen, C Driscoll, A Khambati, K Perry, RB Nadler
Northwestern Memorial Hospital
Moderated Poster Session 12: Imaging II
MP12‐01
Ultrasound to reposition and facilitate passage of distal ureteral stones
JD Harper, J Thiel, P Samson, P Sunaryo, RM Sweet, I Metzler, L Anderson, R Kessler, B Dunmire, C Popchoi, R Managuli, B Cunitz, B Burke, Z Liu, AD Maxwell, M Sorensen, M Hall, H Wessells, MR Bailey
University of Washington
MP12‐02
Narrow band imaging cystoscopy in non‐muscle invasive bladder cancer–Still “motive and opportunity” after 6 years of follow‐up?
BF Geavlete, C Moldoveanu, C Ene, C Bulai, A Ene, PA Geavlete
“Saint John” Emergency Clinical Hospital, Department of Urology
MP12‐03
A Multi‐class Classification Machine Learning Model of In Vivo Urinary Stone Compositions Using Dual‐energy CT and Radiomics
K Wang, X Jin, D Ye, Y Chen, L Cai, J Sun, L Xiang, H Li
West China Hospital, Sichuan University
MP12‐04
Simplified Biplanar (0°‐90°) Fluoroscopic Puncture Technique for Percutaneous Nephrolithotomy: The Learning Curve
BO Manzo, DD Cabrera, JE Torres, EE Lozada, E Flores, P Alarcon, C Morales, F Sepulveda
Hospital Regional de Alta Especialidad del Bajío
MP12‐05
Role of peri‐calculus ureteral thickness on CT Scan to predict stone impaction at time of surgery. A Single center analysis
N Iqbal, A Hasan, J Rahim, S Imtiaz Ali, S Akhter, T Bhatty
PKLI, Lahore, Pakistan
MP12‐06
The efficacy and safety of radiation‐free retrograde intrarenal surgery
B Kim, J Chung, Y Ha, S Choi, J Lee, H Kim, T Kim, E Yoo, T Kwon
Department of Urology, School of Medicine, Kyungpook National University
MP12‐07
A Comparison of Radiation Use During Fluoroscopic Guided Extracorporeal Shockwave Lithotripsy and Ureteroscopy for Renal Stones
AS Amasyali, M Keheila, JD Belle, M Hajiha, DD Baldwin, G Martin
Loma Linda University, School of Medicine
MP12‐08
Building a roadmap for initial evaluation and follow up for surveillance of renal masses: Results from MUSIC consensus panel
A Patel, B Lane, M Butaney, A Johnson, J Qi, C Rogers, f Urological Surgery Improvement Collaborative
Henry Ford Health System
MP12‐09
Predictors of Radiation Exposure During Ureteroscopy/RIRS: Can We Limit our Exposure?
A Rai, D Nethala, S Rastogi, T Aro, A Abraham, D Hoenig, AD Smith, Z Okeke
The Smith Institute for Urology
MP12‐10
Point of Care Smart Device Ultrasound Probes Versus Bladder Scanner ‐ A Prospective Randomized Trial
HC Wright, H Brar, S De
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
MP12‐11
A Prospective Study Using Abdomen Only CT Imaging For Routine Stone Imaging Follow‐Up
M Fritz, J Zhang, A Ayoob, J Bell
Univeristy of Kentucky
MP12‐12
In the era of MRI targeted biopsy what is the role for TRUS biopsy? Results from Largest Asian series
J Du, Y Lu, Z Law, H Huang, H Ho, J Yuen, L Lee, K Tay, K Chen, W Lau
Singapore General Hospital
MP12‐13
Novel Use of Dual Energy CT in Guiding Treatment of Complex Renal Cysts
M Davis, K Hart, BF Schwartz, DT Lybbert
Southern Illinois School of Medicine
MP12‐14
Challenging the Status Quo: Can Low Dose CT Diagnose Stones in Obese Patients?
JD Belle, G Martin, M Keheila, J Smith, M Hajiha, AS Amasyali, DD Baldwin
Loma Linda University, School of Medicine
MP12‐15
Emergency Department Non‐contrast Computed Tomography for Suspicion of Obstructive Urolithiasis: Yield and Consequences
Z Savin, S Dekalo, E Schreter, S Greenberg, G Aviram, O Yossepowitch, M Sofer
Tel‐Aviv Sourasky Medical center, Sackler School of Medicine, Tel‐Aviv University
MP12‐16
Index Prostate Lesion Density Does Not Improve the Diagnostic Performance of Detecting Clinically Significant Prostate Cancer
M Said, M Rajput, C Metz, P Gellhaus, CR Tracy, RL Steinberg
MP12‐17
Withdrawn
MP12‐18
Can ureteroscopy and retrograde intrarenal surgery be safe and effectively performed with no auxiliary fluoroscopy? A systematic review
C Laranjo Tinoco, I Marques, J Ribeiro, A Cardoso, R Matos Rodrigues, S Anacleto, P Passos, E Lima, M Cerqueira Alves, P Mota
Hospital de Braga, EPE
MP12‐19
Use of High‐Frequency Micro‐Ultrasound For Real‐Time Targeted Prostate Biopsy and Subsequent Prostate Cryoablation: Initial Clinical Experience
HE Moreland, RD Carr, LJ Smith, LT O'Connor, DB Rukstalis
University of South Carolina School of Medicine
MP12‐20
Evaluation of Triple‐D Score as a predictor of stone‐free‐status following extra corporeal shock wave lithotripsy: A single centre pilot study
K Biswas, K Bliss, Z Maan, G Rix, S Datta
Colchester General Hospital
MP12‐21
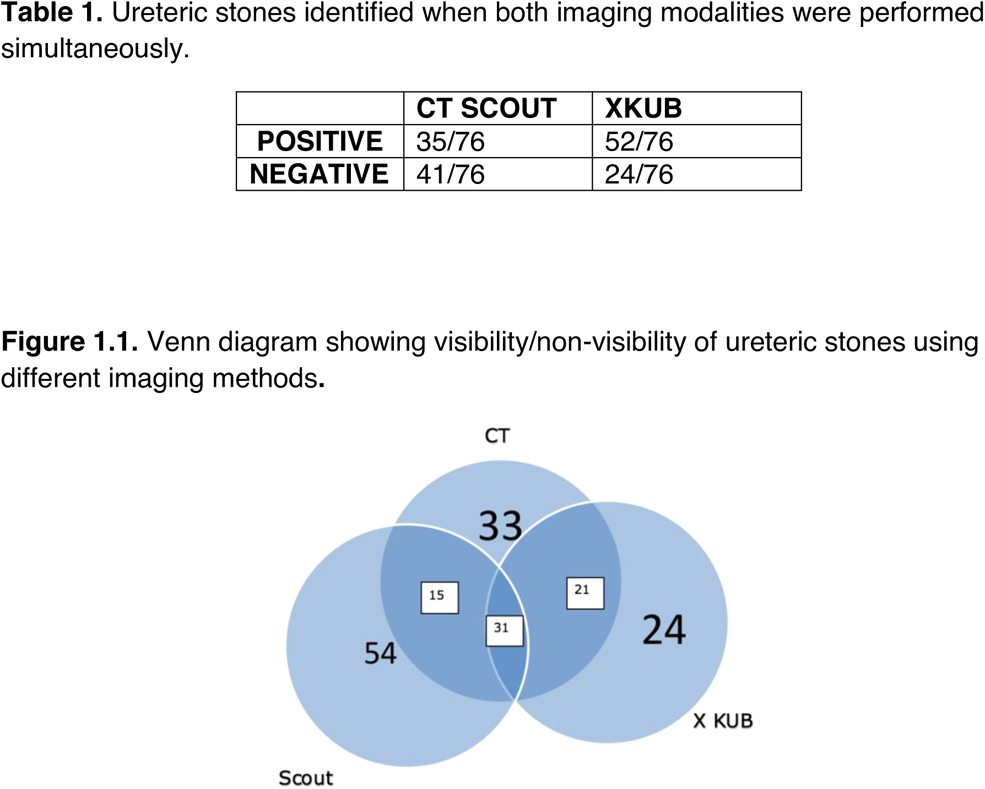
Do CT scout images obviate need to perform Xray KUB in the management of ureteric calculi
N Rokan, H Joshi, A Al‐Mitwalli
MP12‐22
The Changing Trends of image Guided Biopsy of Small Renal Masses before intervention‐ An Analysis of European Multinational Prospective EuRECA Registry
V Vinson, F Keeley, Jr, B Lagerveld, T Nielsen, G Lughezzani, T Wah
School of Medicine, Faculty of Medicine and Health, University of Leeds, Leeds Department of Targeted Intervention, Division of Surgery and Interventional Science, University College London, London
Abstract Video Session 02: Laparoscopy‐ Miscellaneous
V02‐01
Withdrawn
V02‐02
Does 3D Facilitate Technique of Laparoscopy Pyeloplasty in Infant
R Manickam, S Kallappan, S Nachimuthu
V02‐03
Novel Hybrid Technique Of Laparoscopic Nipple Valve Reimplantation With Portsite Rirs Through Exteriorised Distal Ureter In Pom With Renal Calculus
R Manickam, S Kallappan, S Nachimuthu
V02‐04
Laparoscopic Nipple Valve Reimplantation In A Ureterocele Of a Crossed Fused Ectopic Moiety Unit ‐ Challenges
R Manickam, S Kallappan, S Nachimuthu
V02‐05
Video Endoscopic Inguinal Lymphadenectomy: Step‐By‐Step Technique And Mid‐Term Oncological Outcomes
JM Gaya, A Rosales, A Gallioli, P Diana, P Gavrilov, A Territo, A Piana, A Sánchez‐Puy, J Calderón, H Vila‐Reyes, J Palou, A Breda
V02‐06
Transperitoneal Laparoscopic Excision of Mullerian Duct Cyst
C Yogeswaran, K Ekwueme
V02‐07
The Goyri‐O'Neill perfusion technique of cadaveric embalming: a novel approach to advanced laparoscopic surgical training
T Ribeiro de Oliveira, N Domingues, A Palmas, S Biyani, D Pais, J Goyri‐O'Neill
V02‐08
Bilateral uterosacral ligament replacement ‐ laparoscopic uterosacropexy (laUSA) with minimal use of material and uterus preservation
S Ludwig, B Morgenstern, P Mallmann
V02‐09
Laparoscopic single‐port varicocelectomy with the single‐channel fabric device (LEVD): A medium‐term follow‐up
M Roslan, M Przudzik, M Borowik, R Liss, M Łesiów, G Gronowicz, J Wójtowicz
Abstract Video Session 03: Transurethral Surgery: Prostate and Bladder Neck
V03‐01
Withdrawn
V03‐02
Holmium Laser Enucleation of the Prostate after Greenlight Photoselective Vaporization of the Prostate
KH Thai, M El Tayeb
V03‐03
Tips and Tricks of Morcellation
JC Smith, M El Tayeb
V03‐04
Cystolitholapaxy during Holmium Laser Ablation of the Prostate: Dual Utilization of the Side Fire Laser Fiber
BB Whiles, KL Thurmon
V03‐05
What to do When Unable to Reach the Bladder During Holmium Laser Enuncleation of the Prostate (HoLEP): An Incision‐Free Approach
DK Agarwal, ME Rivera
V03‐06
Design and Development of a Physical Simulation Platform for Holmium Laser Enucleation of the Prostate (HoLEP) using Expert Consensus
P Saba, R Melnyk, K Cameron, S Quarrier, N Gopal, MR Humphreys, AE Krambeck, NL Miller, RK Jain, A Ghazi
V03‐07
Thulium Laser Prostatectomy In High Risk Patients With Benign Enlargement Of Prostate
VK Poleboyina, V Akinapally, M Khan
V03‐08
Thulium Laser Prostate Surgery Using Slender Resectoscopes–Impact on Post Operative Urethral Stricture
VK Poleboyina, V Akinapally, M Khan
V03‐09
Endoscopic Enucleation of a 180g Prostate with 30W Thulium Fibre Laser
VK Poleboyina, M Khan
V03‐10
Urethra sparing simple prostatectomy as an alternative to transurethral resection of the prostate ‐ a disruptive point of view!
A Cardoso, S Anacleto, C Laranjo Tinoco, R Matos Rodrigues, E Lima
V03‐11
A Novel Technique for Effective Resection of Adenoma after Prostate Enucleation: An Economic Alternative to Morcellation
L Mo, JA Ivey, R Pak, J Cheng, D Chandler
Mayo Clinic Florida
V03‐12
Same‐day surgery approach to Holmium Laser Enucleation of the Prostate (HoLEP) using MOSES
L Cooley, J Guo, MS Lee, T Large, AE Krambeck
Abstract Video Session 04: Laparoscopy: Lower Tract, Ureter, UPJ
V04‐01
Laparoscopic Boari flap with port site RIRS in a case of Midureteric stricture with large renal stone
R Manickam, S Kallappan, S Nachimuthu
V04‐02
Obstructive Megaureter in Infants : Laparoscopic Intracorporeal Ureteric Tapering and Reimplantation
D Vaddi, P Ramakrishna, P Siddalinga Swamy, B Manas Babu, G Soundarya, A Hemnath, P Rakesh, S Chahar, S Gunadal
V04‐03
Laparoscopic Uretero‐calicostomy for a patient with uretero‐pelvic obstruction, intrarenal pelvis and multiple caliceal stones
A Kashi, S Farshid, I Ghanaat, N Ahmadian
V04‐04
Unusual pathology during laparoscopic pyeloplasty
S Saulat, S Saeed Uddin Qadri, J Sheikh, M Ejaz, A Ayub, H Ashraf, N Sadiq Kiani, S Tariq
V04‐05
Zinner syndrome a rare case of bladder outlet obstruction
C Conde Redondo, F Natal Alvarez, S Martin Martin, A Ruano Mayo, A Zamora Horcajada, J Torrecilla, L Cuellar Martin, A Herranz Arriero
V04‐06
Laparoscopic anterior pelvic exenteration in muscle invasive bladder cancer in female
R TP, D Sarma, S Pratihar
V04‐07
Experience of reduced port laparoscopic pyeloplasty for uretero‐pelvic junction obstructon in our hospital
K Mikami, K Ho, T Suyama, K Araki, H Masuda, S Kojima, Y Naya
V04‐08
Laparoscopic Dismembered Pyeloplasty In Five Differently Located Pelviureteric Junctions
V Chandra Mohan, P Ramakrishna, P Siddalinga Swamy, B Manas Babu, G Soundarya, A Hemnath, P Rakesh
V04‐09
Laparoscopic intraoperative blue light visualization of the ureters utilizing the novel fluorescent tracer agent MB‐102–an in vivo porcine study
J Palka, SP Argade, M Talcott, T Rogers, R Dorshow, R Venkatesh
V04‐10
Retrocaval Ureter, Laparoscopic Intervention
J Abad Vivas‐Pérez, S Gallardo Zúñiga, R Barrabino Martín, JM Molina Hernandez, J Gómez Jiménez, JA Hortelano Parras, J Nuevo Lara, JL Soler Soler
V04‐11
Technique of conisation of the uretero‐pelvic reconstruction during laparoscopic and robotic assisted pyeloplasty in cases of ureteropelvic junction obstruction in a single surgeon serie
W Khoder, J Michaelis, M Grabbert, S Astheimer, C Gratzke, C Stief
V04‐12
Laparoscopic approach to excision of giant, multiloculated, seminal vesicle cyst
AB McVey, E Polo Alonso, D Bolton, P Liodakis
Moderated Poster Session 13: Stones V: PNL & URS
MP13‐01
Analysis of morbidity and mortality after percutaneous nephrolithotomy in patients with renal calculi: evaluation of 16,201 patients from a nationwide German database
B Becker, C Schulz, T Herrmann, CM Rosenbaum, AJ Gross, H König, C Netsch
Department of Urology, Asklepios Hospital Barmbek, Hamburg, Germany
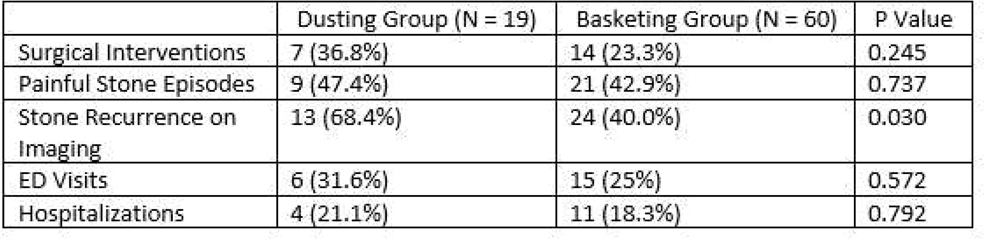
MP13‐02
Long‐term follow‐up on dusting versus basketing during ureteroscopy–a prospective multicenter trial from the EDGE research consortium
KL Stern, RL Sur, S Sivalingam, M Monga, SK Bechis, J Moore, VK Wong, H Brar, E Kong, MR Humphreys, BH Chew
Mayo Clinic Arizona
MP13‐03
Endoscopic combined intrarenal surgery (ECIRS)–Supine vs. Prone position and comparison with percutaneous nephrolithotomy: results of a systematic review
A Pérez‐Lanzac, M Alcoba García, G Bueno Serrano, G Ordaz Jurado, J Fernández Gómez, A Budia Alba
Ruber Internacional Hospital, Dept. of Urology
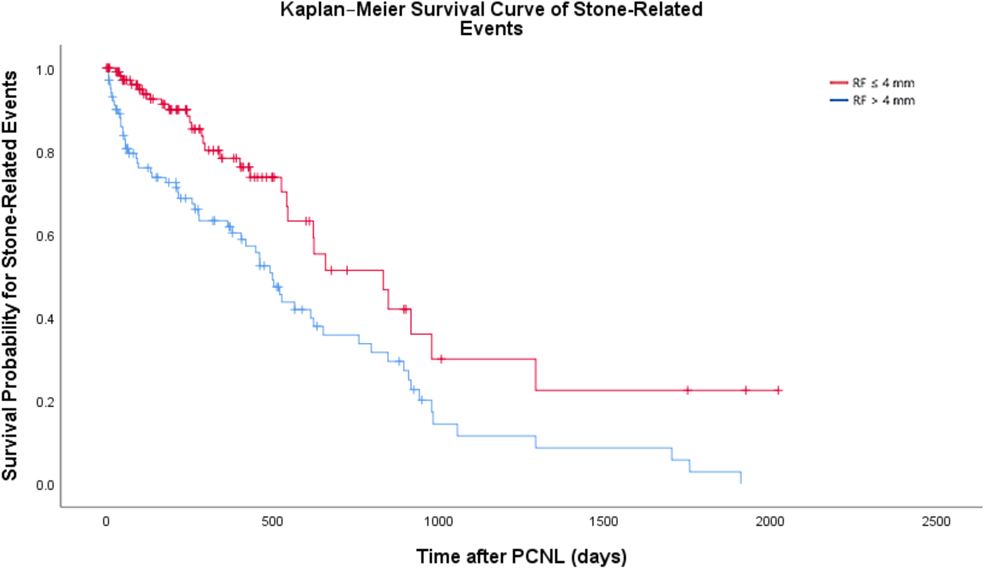
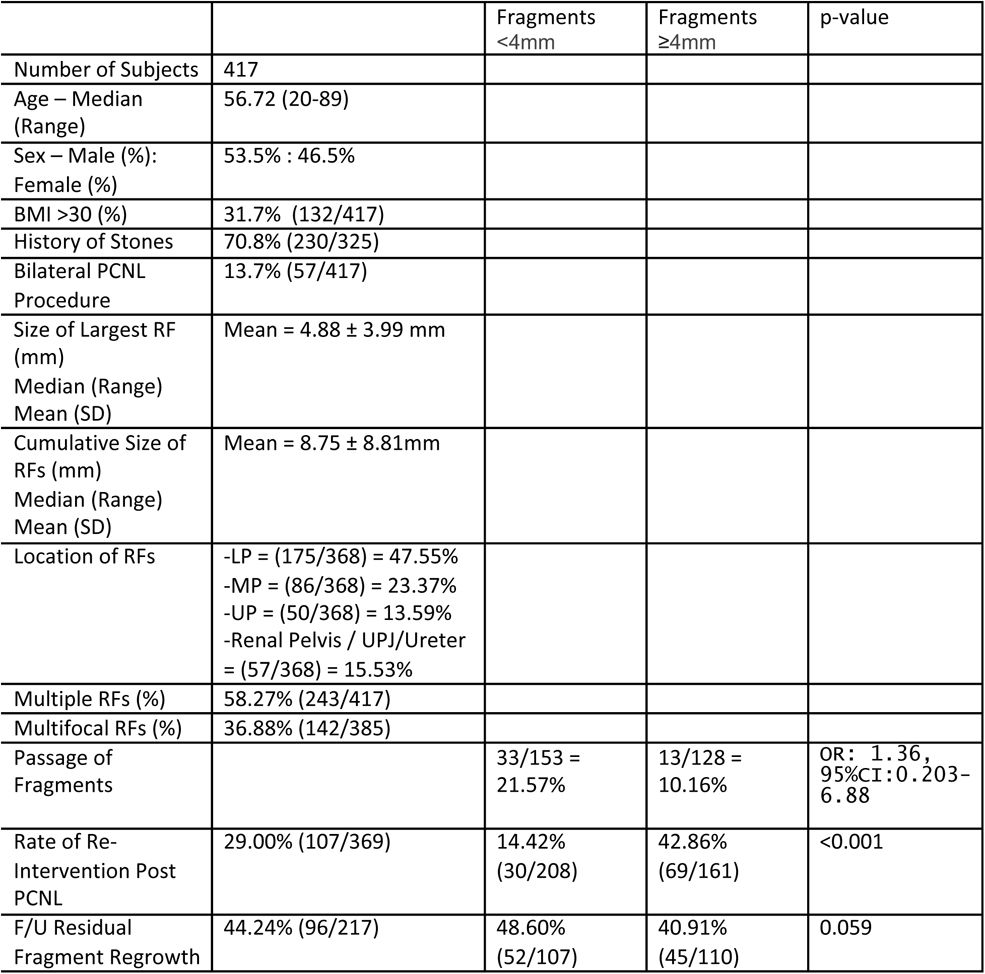
MP13‐04
Fate of residual fragments after PCNL: Results from the EDGE Research Consortium
BH Chew, VK Wong, AS Emmott, R Paterson, D Lange, CJ Lundeen, A Nevo, J Moore, A Yaghoubian, N Nimmagadda, RL Sur, SK Bechis, BE Knudsen, MR Humphreys, BH Eisner
MP13‐05
Is retrograde intrarenal surgery as effective in pediatric kidney stones as in adult patients?
MS Özkent, MM Piskin, M Balasar, Y Göger, MS Sönmez
Konya City Hospital
MP13‐06
Cross‐Sectional Survey of Patients Awaiting Nephrolithiasis Surgery During the COVID‐19 Pandemic Onset: A Multi‐Center Study from the Registry for Stones of the Kidney & Ureter Group
J Ahn, D Bayne, I Metzler, JD Harper, RL Sur, SK Bechis, BD Duty, D Tzou, N Sobhani, M Stoller, T Chi
UCSF
MP13‐07
Do Patient and Operative Risk Factors during PCNL Affect Radiation Exposure?
A Rai, D Nethala, S Rastogi, T Aro, A Abraham, D Hoenig, AD Smith, Z Okeke
The Smith Institute for Urology
MP13‐08
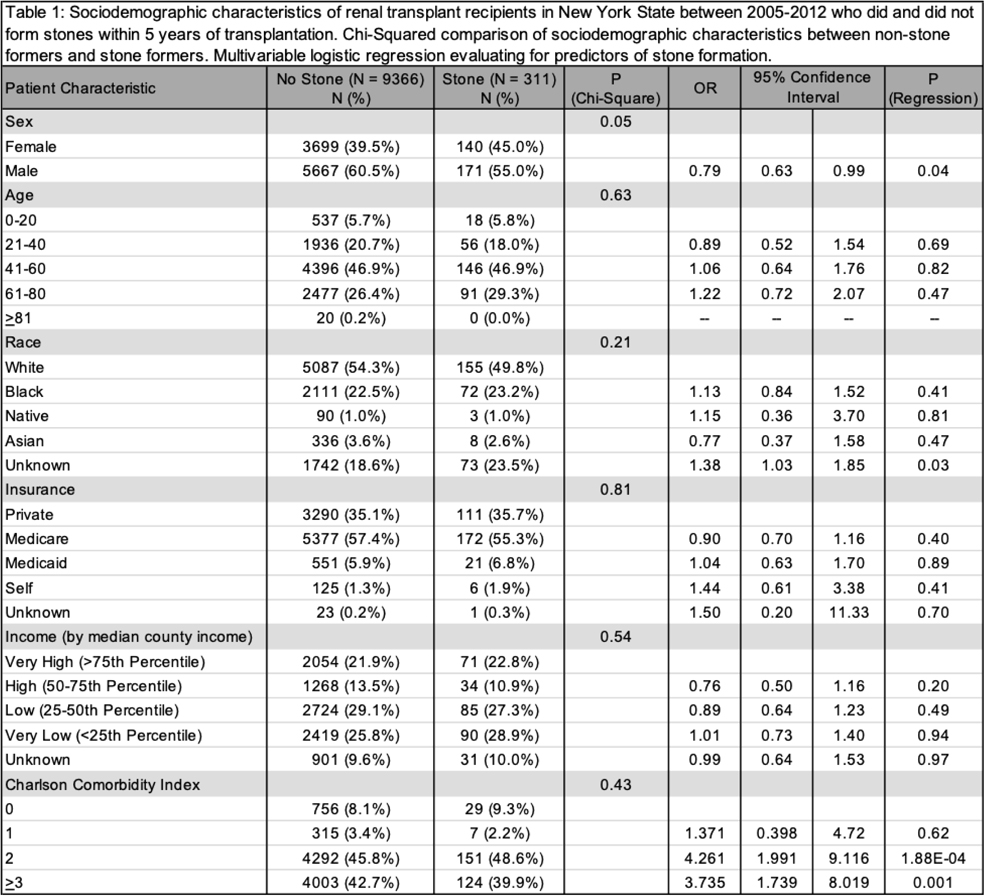
Urolithiasis after kidney transplantation: a New York statewide analysis with 5‐year follow up
EB Garden, N Tomer, J Pfail, KT Ravivarapu, AC Small, MA Palese
Icahn School of Medicine at Mount Sinai
MP13‐09
A comparison among RIRS and MiniPerc for renal stones between 1‐2 cm: a randomized controlled trial
L Berti, M Maltagliati, U Besana, C Buizza, A Calori, M Sighinolfi, S Micali, BC Rocco, G Bozzini
ASST Valle Olona
MP13‐10
Improving access and quality of care to kidney stone patients in an underserved community
M Stout, M Murtha, M Yudovich, A Scimeca, D Diab, T Posid, G Shidham, E Weinandy, BE Knudsen, MW Sourial
The Ohio State University
MP13‐11
Changes in Renal Parenchymal Volume and Long‐Term Function after Percutaneous and Ureteroscopic Stone Removal
P Jiang, R Arada, AS Afyouni, L Grimaud, R Karani, A Peta, A Brevik, CM Rhee, K Kalantar‐Zadeh, RM Patel, J Landman, RV Clayman
Department of Urology, University of California, Irvine
MP13‐12
Prospective study of retrograde intrarenal surgery(RIRS) for renal and upper ureteric calculus in prior non stented patients
VK Poleboyina, P Kalidindi, R Kalidindi, V Akinapally, M Khan
Care Hospital
MP13‐13
Withdrawn
MP13‐14
Horseshoe Kidney Compared to Orthotopic Kidneys: Anatomical Measurements Relevant for Percutaneous Access
AS Mouzannar, B Mora Garijo, L Horodyski, R Blachman‐Braun, I Estanga, J Katz, R Marcovich, L Deane
University of Miami Hospital
MP13‐15
Post‐Operative Pain and Recovery in Patients with Nephrolithiasis: Results from the Endourological Society TOWER Research Collaborative
AE Jones, G Lin, H Stambakio, BH Chew, JM Stern, JB Ziemba
University of Pennsylvania Perelman School of Medicine
MP13‐16
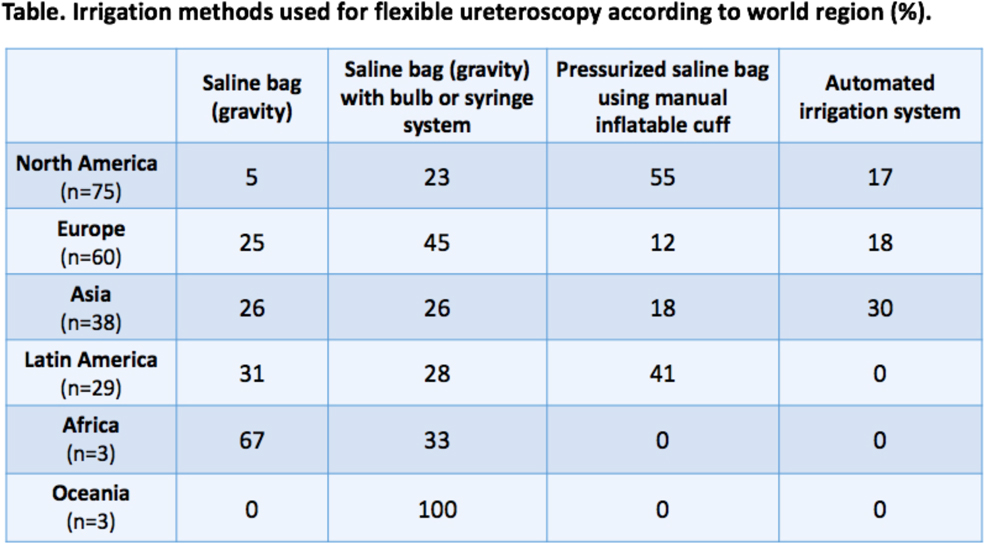
Irrigation practice patterns during flexible ureteroscopy: Results of a worldwide survey
J Bahaee, J Plott, KR Ghani
Department of Urology, University of Michigan
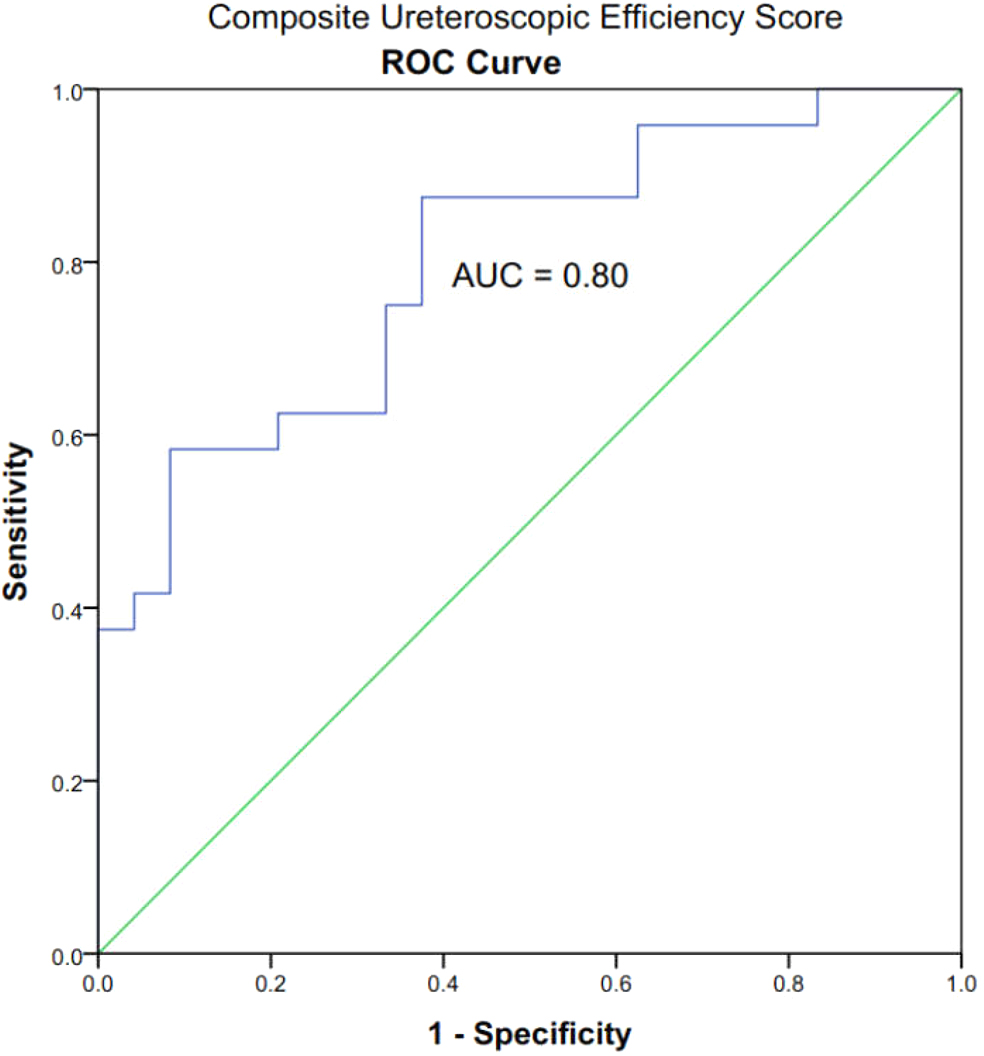
MP13‐17
Development of a Composite Ureteroscopic Efficiency Score Through Simulated Ureteroscopic Skills Assessment
N Chen, D Yu, D Wollin
Brigham and Women's Hospital Division of Urology
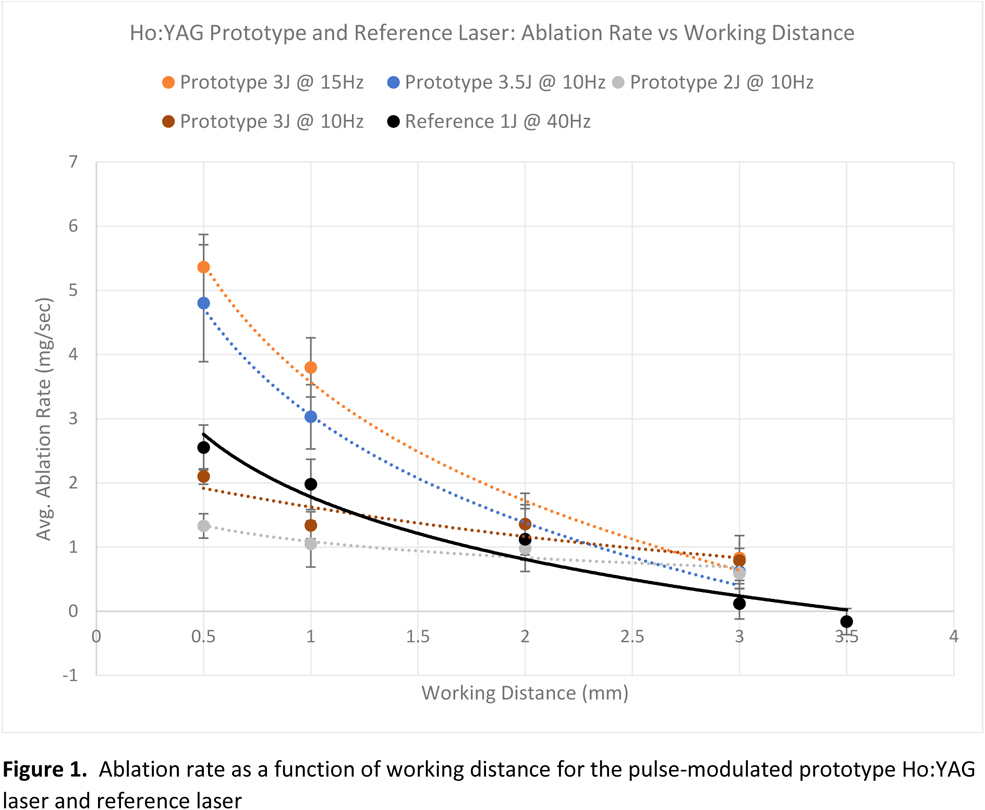
MP13‐18
Stone ablation efficacy of a new prototype Holmium:YAG pulse‐modulated laser at working distances of up to 3mm
B Yang, I Parab, J Cancino, S Liu, A Ray, TC Hasenberg, T Harrah, BW Turney
University of Oxford
MP13‐19
BMI and Nephrolithiasis in a Pediatric Cohort by Pubertal Status
A Hannallah, Z Baker, N Khouzam, S Sparks
Children's Hospital Los Angeles
MP13‐20
The relationship between renal pelvis pressures and pyelovenous backflow during ureterorenoscopy in a live porcine model
J Twum‐Ampofo, J Saunders, M Franco, B Eisner
MP13‐21
Between a stone and a hard place: symptom management prescribing trends in patients undergoing ureteroscopic lithotripsy and stenting
F Rahman, A Kandabarow, PM Patel, E Chuang, A Druck, AV Farooq, TT Turk, K Baldea
Loyola University Chicago Stritch School of Medicine
MP13‐22
Emergency external shockwave lithotripsy for acute ureteric obstruction
W Maynard, E Maher, S Wong, A Goyal, L Ajayi, S Murphy, D Allen, R Kucheria, D Beder, G Chiriaco
Royal Free Hospital London
Moderated Poster Session 14: Stents & Equipment I
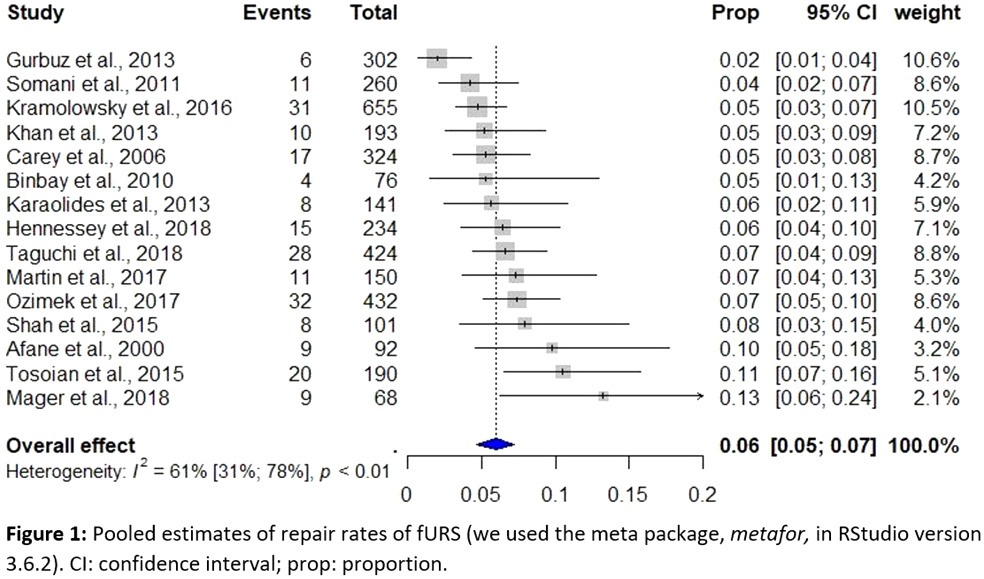
MP14‐01
Repair rate and associated cost of reusable flexible ureteroscopes: A systematic review and meta‐analysis
T Tailly, D Rindorf, BK Somani, O Traxer, GM Kamphuis, S Larsen, L Ockert, K Koo
University Hospital Ghent
MP14‐02
Withdrawn
MP14‐03
The efficacy and the safety of the J Fil Stent in the post operative endoscopic procedures: the experience on 237 cases
F de Marco
Urology Villa Betania Hospital
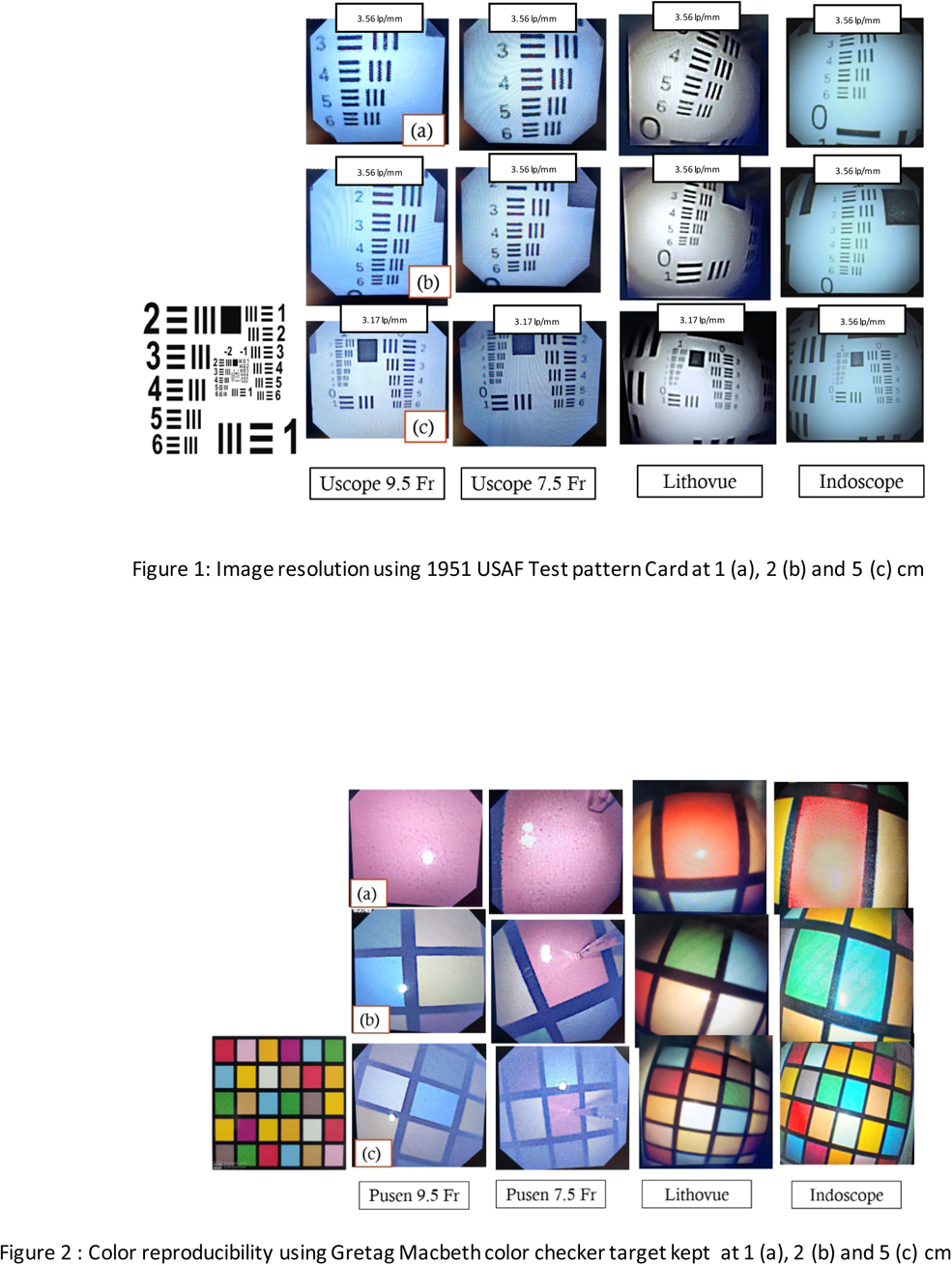
MP14‐04
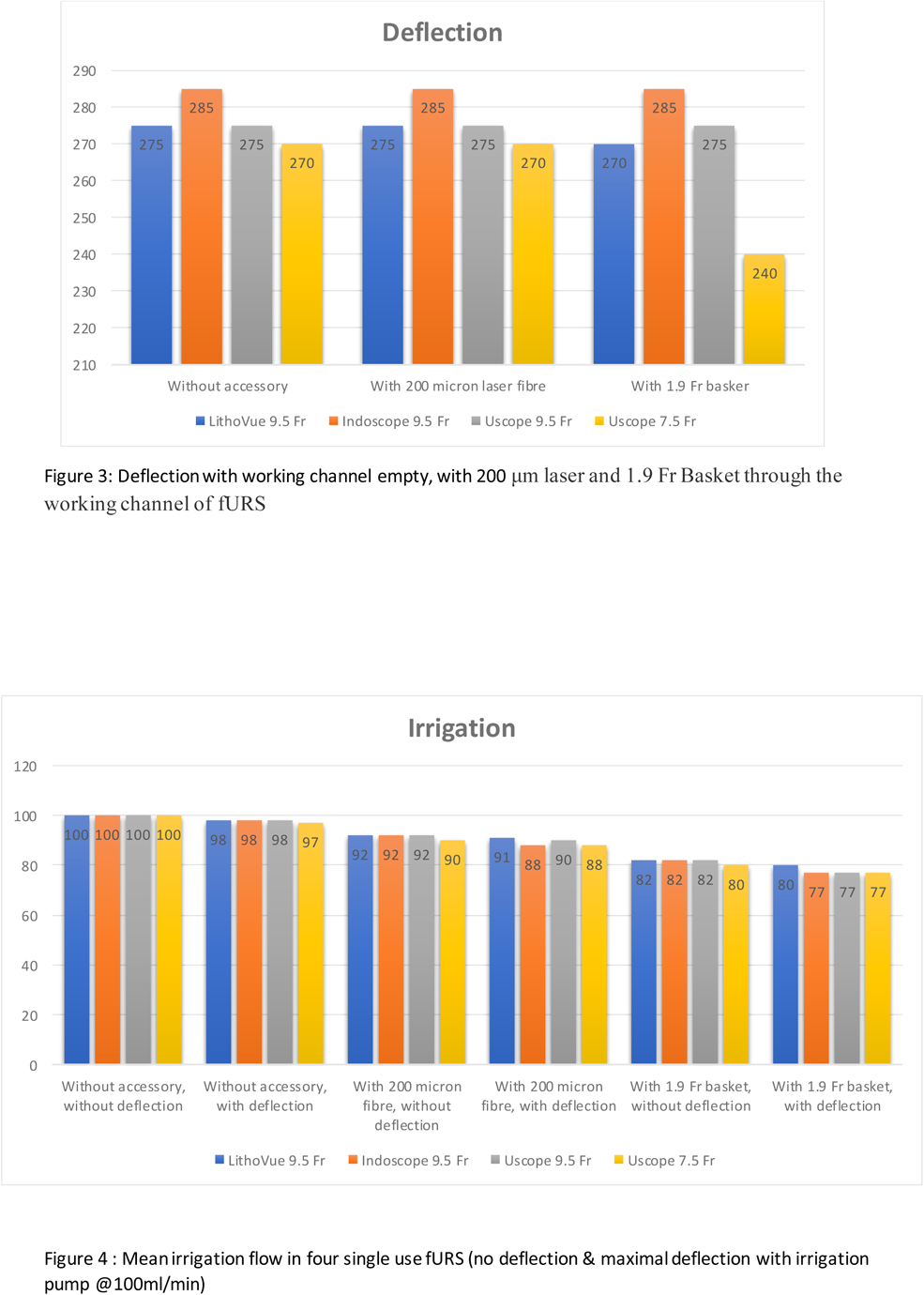
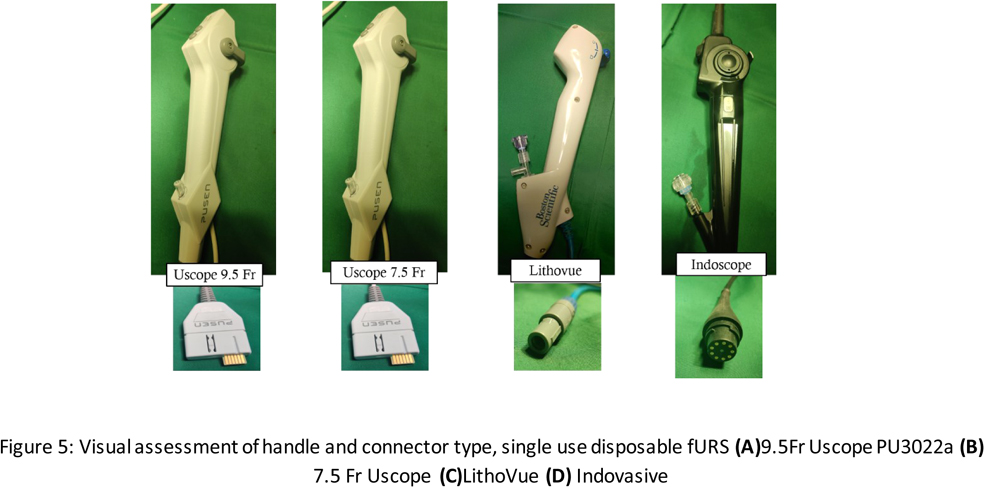
A Pilot Single Centre Prospective Comparative Study of two digital single use flexible ureterorenoscopes‐ Indoscope (Bioradmedisys™, Pune, India) and 7.5Fr Uscope™ PU3033A Zhuhai Pusen, China)
S Agrawal, A Singh, A Ganpule, R Sabnis, M Desai
MPUH
MP14‐05
Single‐use flexible ureteroscopes: comparative in‐vitro analysis of four scopes
AP Patil, S Agrawal, R Batra, A Singh, A Ganpule, R Sabnis, M Desai
Muljibhai Patel Urological Hospital Nadiad
MP14‐06
Stent Syndrome. Does the Diameter Matter? Results of a Randomized Prospective Trial
PN Contreras, M Frascheri, N Bonanno, S Butori, L Blas, C Ameri
Hospital Aleman
MP14‐07
Twelve Years of Experience with Metallic Stents for Malignant Ureteral Obstruction
N Bonanno, PN Contreras, M Frascheri, JN Bujaldon, L Blas, C Ameri
Hospital Aleman
MP14‐08
Comparison of two digital disposable flexible ureteroscopes: a prospective study
L Berti, M Maltagliati, C Buizza, A Calori, M Justich, P Marcangeli, BC Rocco, M Sighinolfi, S Micali, G Bozzini
ASST Valle Olona
MP14‐09
Changing stenting culture ‐ an audit of post ureteroscopic stent insertion against current NICE guidance
O Gbolahan, C Popanes, H Kadhim, A Raza
London North West University Healthcare NHS Trust
MP14‐10
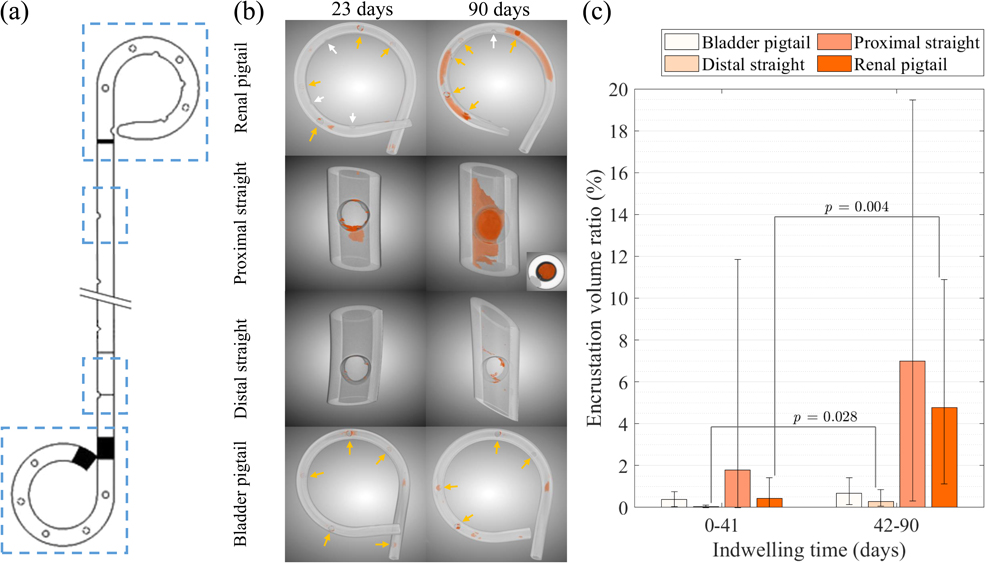
Quantitative analysis of ureteral stents: encrustation depends on indwelling time and stent region
S Zheng, P Amado, B Kiss, F Stangl, E Talon, A Häberlin, D Obrist, F Burkhard, F Clavica
ARTORG Center for Biomedical Engineering Research, University of Bern, CH
MP14‐11
Combined diamond‐like carbon and copper coating on polyurethane implants in a rat model
W Kram, C Ludwig, JE de La Cruz, H Rebl, A Springer, B Nebe, M Wienecke, N Buchholz, O Hakenberg
SVMC
MP14‐12
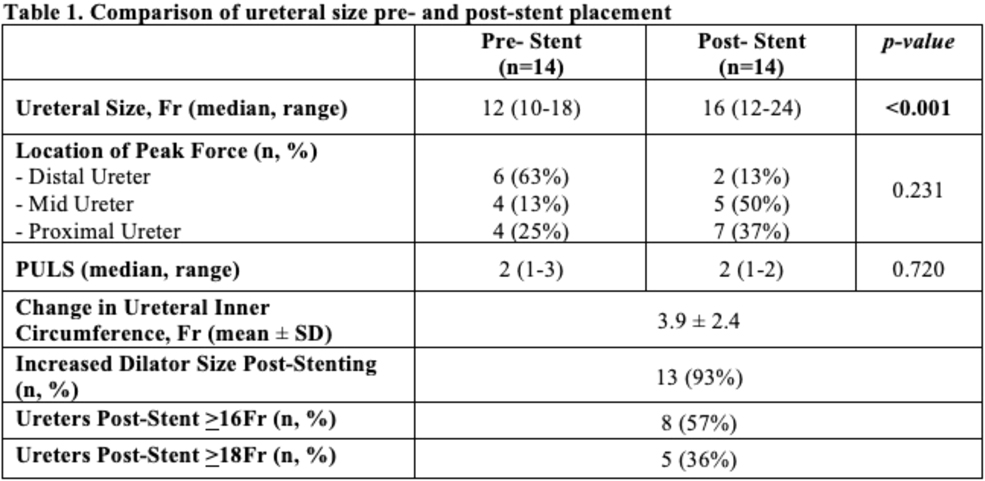
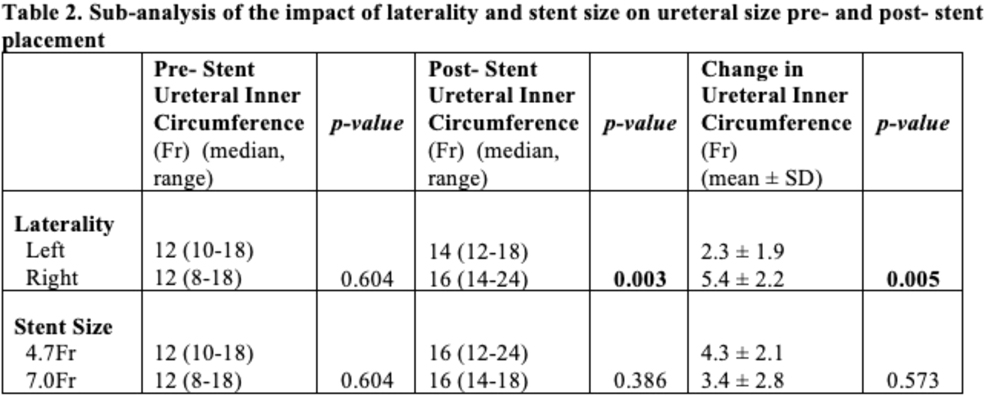
Evaluation of One Week of Pre‐stenting on Porcine Ureteral Diameter
P Jiang, AS Afyouni, T King, S Dinh, M Ayad, C Kosmala, A Peta, A Brevik, L Limfueco, Z Okhunov, RM Patel, J Landman, RV Clayman
Department of Urology, University of California, Irvine
MP14‐13
Withdrawn
MP14‐14
Evolution of Single‐Use Endoscopy: Benchtop and Clinical Assessment of a New Single‐Use Cystoscope
P Whelan, CJ Kim, C Tabib, K Boydston, GM Preminger, M Lipkin
Duke University
MP14‐15
Is routine urinalysis indicated prior to urodynamics in the asymptomatic patient?
Z Yasen, R Oliver, L Crabtree, R Peggs, Y Khan, S Chowdhury
J DiBianco, A Dupati, S Daignault‐Newton, N Kachroo, BD Seifman, H Pimentel, CA Dauw, KR Ghani, f Urological Surgery Improvement Collaborative, S Hiller
University of MIchigan Department of Urology
MP14‐18
Impact of ureteral stents on factors contributing to stricture pathogenesis
K Doersch, K Almutairi, BH Chew, D Lange
Department of Urology, University of Rochester Medical Center
MP14‐19
Biodegradable metals for ureteral stents applications: understanding the degradation profile under simulated urinary tract environment
M Pacheco, JM Silva, IM Aroso, J Bohlen, M Nienaber, S Lamaka, M Zheludkevich, E Lima, A A. Barros, R L. Reis
i3Bs Research Institute on Biomaterials, Biodegradables and Biomimetics, University of Minho
MP14‐20
Implementation of single use disposable digital ureteroscopes in a large public tertiary care center leads to decreased operative room and procedure times
C Schuster, MS Carey, RI Carey
Florida State University College of Medicine
MP14‐21
Proximal and distal ureteral stent curls exhibit differences in biofilm microbiota with high inter‐individual variability
G Werneburg, S De, R Rackley, D Shoskes, A Miller
Cleveland Clinic Foundation
MP14‐22
Double J‐eopardy: risk factors for seeking acute care due to ureteral stent discomfort
E Chuang, AM Kandabarow, PM Patel, F Rahman, A Druck, AV Farooq, TT Turk, KG Baldea
Loyola University Chicago Stritch School of Medicine
Moderated Poster Session 15: Lasers I
MP15‐01
First clinical results of a novel pulsed Thulium:YAG laser for lithotripsy during mini‐PCNL
B Becker, J Bergmann, CM Rosenbaum, AJ Gross, C Netsch
Department of Urology, Asklepios Hospital Barmbek, Hamburg, Germany
MP15‐02
HIGH POWER LASER FOR HIGH STONE FREE RATES in 1 sitting ‐ is it achievable?: A prospective single centre Asian experience
R Mangat, Q Yufei, S Biligere, Q Yufei
Dept. of Urology
MP15‐03
60Watt Superpulse Thulium Fiber Laser in Retrograde Intrarenal Surgery‐Aiming towards faster dust
D Vaddi, P Ramakrishna, P Siddalinga Swamy, B Manas Babu, G Soundarya, A Hemnath, P Rakesh
Preeti Urology & Kidney Hospital
MP15‐04
Thulium Fiber Laser: A Universal Device in Urology
M Taratkin, C Azilgareeva, L Rapoport, A Dymov, R Sukhanov, D Enikeev
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia
MP15‐05
Pulse modulation with MOSES technology can reduce operative time in miniaturised percutaneous nephrolithotomy
M Popiolek, S Jarl, P Georgouleas, M Wagenius, P Sundqvist
Örebro University Hospital
MP15‐06
The Novel Thulium Laser Results in Fewer Residual Stone Fragments During Lower Pole Lithotripsy
AS Amasyali, JD Belle, M Keheila, N Chen, M Hajiha, E Baldwin, DD Baldwin, A Assidon
Loma Linda University, Department of Urology
MP15‐07
Is Less More When Using the Novel Thulium Laser: What Fiber Size and Laser Settings Result in the Most Efficient In Situ Lower Pole Lithotripsy?
AS Amasyali, JD Belle, M Keheila, N Chen, A Assidon, M Hajiha, E Baldwin, DD Baldwin
Loma Linda University, Department of Urology
MP15‐08
Same‐Day Catheter Removal after Holmium Laser Enucleation of the Prostate (HoLEP): What Predicts Failure?
DK Agarwal, T Large, M Lee, E Sahm, M Assmus, ME Rivera
Indiana University Department of Urology
MP15‐09
Flexible ureterorenoscopy with holmium laser lithotripsy for upper urinary urolithiasis
M Jasser, R Mehdi, T Tarek, B Mohamed, B Wassim, K Ramzi, G Samir
Military Hospital of Tunis
MP15‐10
Superpulse Thulium, Holmium, and Holmium MOSES Laser Lithotripsy: An ex‐vivo Evaluation on the Effectiveness of “Dusting” Coupled with Ureteroscopic Fragment Aspiration
P Jiang, A Peta, R Arada, M Ayad, AS Afyouni, L Limfueco, A Brevik, N Nguyen, Z Okhunov, RM Patel, J Landman, RV Clayman
Department of Urology, University of California, Irvine
MP15‐11
HoLEP Performed with Moses Technology Generates Cost Savings in the Operating Room
N Nimmagadda, NL Kavoussi, CM Forbes, J Robles, A Wang, B Stone, NL Miller
Vanderbilt University Medical Center, Department of Urology
MP15‐12
The Effect of Scanning Speed in a Dusting Model of the Moses Pulse 120H 2.0 Laser
P Whelan, CJ Kim, D Ho, C Tabib, F Soto‐Paulo, J Chen, P Zhong, GM Preminger, M Lipkin
Duke University
MP15‐13
Which Laser Generates More Heat? A Comparison of the Novel Thulium and Conventional Holmium Lasers in a Benchtop Model
JD Belle, M Keheila, N Srikureja, AS Amasyali, A Assidon, M Hajiha, DD Baldwin
A Prospective Trial of Laser Fiber Degradation Following Holmium Laser Enucleation of the Prostate Utilizing Moses BPH Technology Vs Regular Mode
M Assmus, M Lee, M Sivaguru, DK Agarwal, T Large, BW Fouke, AE Krambeck
Northwestern University, Department of Urology
MP15‐16
Holmium Laser Enucleation of the Prostate Efficiency by Prostate Gland Size: Is there a sweet spot?
M Assmus, AE Krambeck, T Large
Northwestern University, Department of Urology
MP15‐17
Transurethral thulium laser resection of bladder tumor was performed to treat non‐muscle infiltrating bladder tumor
L Li, G Wu, Y Yuan, L Folin, X Zou, Z Guoxi, X Rihai
MP15‐18
Holmium Laser Enucleation of Prostate: What is the true rate of opioid use?
MS Lee, M Assmus, DK Agarwal, T Large, AE Krambeck
Northwestern University Feinberg School of Medicine
MP15‐19
Efficient Holmium Laser Enucleation of the Prostate Can Be Performed After Prostatic Artery Embolization for Massive Prostate Glands (>250 Grams)
MA Knoedler, C Manakas, A Eifler, DR Gralnek
University of Wisconsin, Department of Urology
MP15‐20
The Effect of Peak Power and Pulse Modulation on Lithotripsy Particle Size
B Yang, S Liu, J Cancino, A Ray, TC Hasenberg, T Harrah, BW Turney
University of Oxford
MP15‐21
An in vitro study of the use of high power Ho:YAG laser and the influence of MOSES technology settings in the retropulsion of stones in the upper urinary tract
A Natsos, G Koukiou, A Tsaturyan, M Lattarulo, A Vagionis, K Pagonis, C Adamou, A Peteinaris, E Liatsikos, P Kallidonis
MP15‐22
Improved Efficiency of Thulium versus Standard Holmium Ureteroscopic Laser Lithotripsy Leads to Large Cost Savings
SW Nowicki, JA Linscott, MH Nguyen, JR Ryan, JP Ingimarsson, B Jumper
Omeprazole Lowers 24‐Hour Urinary Magnesium Excretion in Patients with a History of Urolithiasis: Single Center Experience
KL Penniston, S Li, SY Nakada, RA Jhagroo
University of Wisconsin School of Medicine and Public Health
MP16‐02
Sodium Bicarbonate Does Not Increase Urinary Calcium Excretion and is an Effective Urinary Alkalization Strategy: Single Center Experience
KL Penniston, RJ Medenwald, SY Nakada, RA Jhagroo
University of Wisconsin School of Medicine and Public Health
MP16‐03
How much is preventative counseling effective in those patients who underwent stone surgery.a prospective study from developing country
N Iqbal, A Hasan, S Imtiaz Ali, T Bhatty, S Akhter, R Suarez‐Ibarrola
PKLI, Lahore, Pakistan
MP16‐04
Withdrawn
MP16‐05
Narcotic Free Ureteroscopy: A Prospective Randomized Study
JN Bamberger, B Gallante, AM Zampini, WM Atallah, JA Khusid, AS Sadiq, M Gupta
Icahn School of Medicine at Mount Sinai
MP16‐06
Evaluating the Lithogenic Potential of Dairy Milk Alternatives
SP Hager, B Balouch, K Lurz, Z Snow, PC Dreher, J Friedlander
Main Line Health
MP16‐07
Drivers of Calcium Oxalate Stone Formation in Octogenarians and Nonagenarians
B Gallante, H Kwun, JA Khusid, JN Bamberger, WM Atallah, M Gupta
Icahn School of Medicine at Mount Sinai
MP16‐08
Alkali Content of Common Over‐the‐Counter Supplements for Prevention of Recurrent Kidney Stones
BA Johnson, A Garbens, JA Antonelli, K Hill, N Maalouf, MS Pearle
UT Southwestern
MP16‐09
Inconsistency of Cystine Stone Parameters In Predicting Clinical Stone Activity
RL Steinberg, ME VanDyke, JC Dai, A Garbens, BA Johnson, JA Antonelli, MS Pearle
UT Southwestern
MP16‐10
Opiate Omission After Ureteroscopy Does Not Lead to Increased Emergency Department Visits: Results from a Statewide Quality Improvement Collaborative
S Hawken, S Hiller, K Swarna, J Slayton, D Wenzler, C Maitland, J Hollingsworth, KR Ghani, C Dauw
Michigan State University College of Human Medicine
MP16‐11
In‐Hospital Predictors of Post‐Discharge Opioid Utilization: Individualizing Prescribing after Radical Prostatectomy based on the ORIOLES Initiative
R Becker, ZT Su, M Huang, M Biles, K Harris, K Koo, M Han, ME Allaf, A Herati, HD Patel
James Buchanan Brady Urological Institute, The Johns Hopkins Medical Institutions
MP16‐12
Dietary Assessment of Lithogenic Factors in Plant‐Based Meat Products
C Liaw, K Koo, JS Winoker, A Potretzke, BR Matlaga, JC Lieske
Icahn School of Medicine at Mount Sinai
MP16‐13
Patients on Medical Expulsive Therapy for Obstructing Ureterolithiasis ‐ The Wisconsin Stone Quality of Life (WISQOL) Survey
T Phillips, J Palka, AK Chow, J Vetter, A Paradis, R Venkatesh
MP16‐14
Comparative outcomes of urinary and serum parameters for patients with and without diabetes mellitus (DM): Experience from a dedicated metabolic stone clinic
S Kunjur, D Bhatnagar, M Ramachandra, P Cook, M Saraogi, R Geraghty, A Pietropaolo, BK Somani
University Hospital Southampton, UK
MP16‐15
Over‐The‐Counter Alkali Agents to Raise Urine pH and Citrate Excretion: A Prospective Crossover Study in Healthy Adults
KB Scotland, ME Rivera, SK Becchis, JP Ingimarsson, J Knoedler, KL Stern, C Stoughton, D Wollin, MS Borofsky, N Bhojani, M El‐Tayeb, G Kamphuis, DA Leavitt, R Hsi, NE Canvasser
Department of Urology, UCLA
MP16‐16
Investigating fluid intake in an underserved community: what factors are associated with low urine volume on 24‐hour urine collections
A Nourian, E Ghiraldi, M Chen, J Friedlander
Einstein Medical Center
MP16‐17
Initial experience: ex vivo perfused pig kidney to study urinary oxalate excretion
J Pavlinec, M Martin, W Donelan, E Kwenda, P Dominguez‐Gutierrez, VG Bird, BK Canales
Department of Urology, University of Florida College of Medicine and Malcom Randall Gainesville VA Medical Center
MP16‐18
Specialty‐Specific Differences in the Use of Preventive Pharmacologic Therapy and Metabolic Testing for Urinary Stone Disease
J Crivelli, P Yan, R Hsi, JM Hollingsworth
The University of Alabama
MP16‐19
The Frequency of Metabolic Abnormalities Following Initiation of Preventive Pharmacologic Therapy for Urinary Stone Disease
J Crivelli, P Yan, R Hsi, JM Hollingsworth
The University of Alabama
MP16‐20
Adherence to Recommended Follow‐Up Testing Among Patients Prescribed Preventive Pharmacologic Therapy for Urinary Stone Disease
J Crivelli, P Yan, R Hsi, JM Hollingsworth
The University of Alabama
MP16‐21
Preliminary study on the role of selective regulation of CaSR‐Claudin‐14 pathway in the formation of calcium oxalate kidney stones in rats
B Qian, Z Guoxi, X Zou, G Wu, W Xiaoning, Y Yuan
MP16‐22
Opioid Free Ureteroscopy: what is the true failure rate?
MS Lee, M Assmus, DK Agarwal, ME Rivera, T Large, AE Krambeck
Northwestern University Feinberg School of Medicine
Percutaneous Nephrolithotomy (PCNL) As Outpatient Surgery: Analysis of Stone‐Free Rate and Complications at a Single Center
SK Bechis, E Kelly, E Kong, R Zupkas, J Roberts, S Attaluri, T DiPina, R Sur
University of California ‐ San Diego, Department of Urology
MP17‐02
Clinical Characteristics and Outcome of Living Kidney Donors with Obesity in the Era of Laparoscopic Donor Nephrectomy
DA Mendiola, JT Prodigalidad
National Kidney and Transplant Institute
MP17‐03
Interim Results for the ROBUST III Trial Evaluating the Optilume Drug Coated Balloon for Anterior Urethral Strictures
O Kayes, S Elliott, R Virasoro, J DeLong, K Coutinho, K Robertson, R D'Anna
St James's University Hospital
MP17‐04
Diverging Trends in Inpatient Admissions for Adult and Pediatric Kidney Stone Disease in the United States
R Alam, W Wu, BR Matlaga, JS Winoker
Johns Hopkins University School of Medicine
MP17‐05
Ambulatory Percutaneous Nephrolithotomy is Safe and Effective in Extended Criteria Patients
G Hosier, K Visram, N Touma, S Steele, D Beiko
Queen's University
MP17‐06
A Comparison of Hospital Charges Between Secondary Robotic Pyeloplasty and Chronic Ureteral Stenting for Management of Recurrent Ureteropelvic Junction Obstruction
M Lee, Z Lee, I Hollin, DD Eun, N Krishnan
Lewis Katz School of Medicine at Temple University
MP17‐07
Same‐day discharge after benign prostatic hyperplasia procedures: a case‐control matched analysis from the ACS‐NSQIP database
KT Ravivarapu, EB Garden, O Omidele, A Small, O Al‐Alao, MA Palese
Icahn School of Medicine at Mount Sinai
MP17‐08
Risk of Postpartum Urinary Stone Disease in Women with History of Urinary Stone Disease During Pregnancy
K Spradling, C Zhang, A Pao, JC Liao, J Leppert, C Elliott, S Conti
MP17‐09
One‐day Surgery bipolar vapo‐resection for benign prostatic hyperplasia : first experience
A Heddat, Y Houry, R Rabii
University Mohammed VI of Health Sciences UM6SS
MP17‐10
The Acute Stone Clinic model: Improving waiting times and patient care in a public funded health care system
T Tien, E Balai, S Folkard, K Atalar, B Berry, C Bastianpillai, Z Yasen, L Crabtree, R Peggs, S Graham, J Green, P Pal
Barts Health ‐ Urology
MP17‐11
Refractory Urethral Stenosis in Poor Surgical Candidates for Urethroplasty: Off‐label Use of the EpicTM Vascular Self Expanding Stent
JT Kurtzman, R Blum, S Mendonca, S Brandes
Columbia University Irving Medical Center
MP17‐12
Barriers to same‐day discharge after percutaneous nephrolithotomy
H Yang, J Holler, H Lee, G Hosier, R Unno, F Hamouche, J Ahn, D Bayne, A Odisho, M Stoller, T Chi
MP17‐13
Factors Contributing to Inpatient vs Ambulatory Percutaneous Nephrolithotomy
MM Dunne, J Chong, JE Abbott, JG Davalos
Chesapeake Urology, Univeristy of Maryland Baltimore Washington Medical Center
MP17‐14
Withdrawn
MP17‐15
Practice patterns and outcomes of urgent/emergent versus elective ureteroscopy
J DiBianco, A Dupati, S Daignault‐Newton, K Witzke, D Wenzler, KR Ghani, CA Dauw, f Urological Surgery Improvement Collaborative
Department of Urology, University of Michigan
MP17‐16
Scar‐Modulating Effect of Intraurethral Dexpanthenol on Urethral Healing Post Urethroplasty: An Experimental Study in Rats
M Hassaan, AH Elkashef, N Barakat, A Awadalla, A Hashem, F El‐Seddawy, M Abdel‐Maboud
Department of Urology, Urology and Nephrology Center, Mansoura University, Egypt
MP17‐17
Post‐operative outcomes in heavy weight versus lighter weight wide pore polypropylene mesh for robotic sacrocolpopexy: 10 year retrospective analysis of 351 cases
C Schuster, MS Carey, RI Carey
Florida State University College of Medicine
MP17‐18
Uterus preservation in women who undergo robotic sacrocolpopexy for complete vaginal vault eversion: ten year retrospective analysis
C Schuster, MS Carey, RI Carey
Florida State University College of Medicine
MP17‐19
Short‐Term Effect of Local and Systemic Adipose Tissue‐Derived Stem Cells on Stress Urinary Incontinence in Rats
A Elsharabasy, AH Elkashef, N Barakat, S Khater, A Awadalla, A Hussein, M Gomaa, M Abdel‐Maboud, A Shokeir
Department of Urology, Urology and Nephrology Center, Mansoura University, Egypt
MP17‐20
Recovery after surgical treatment for urolithiasis
A Kleijweg, R Kingma, J Stiksma, S Roemeling
MP17‐21
Robotic‐Assisted Laparoscopic Cystectomy with Ileal Urinary Diversion comparing Bricker vs. Wallace Ureteroileal Anastomoses: A Single Institution Study
R Sawhney, M Billah, R Harrison, J Zaifman, MD Stifelman, G Lovallo, M Ahmed
Hackensack Meridian Hackensack University Medical Center
MP17‐22
24 Hour Observation through Stone Observation Pathway Predicts Success of Medical Expulsive Therapy
MC Wasserman, S Marthi, D Sobel, E Godbout, C Tucci, G Pareek
Warren Alpert Medical School of Brown University
Abstract Video Session 05: Miscellaneous
V05‐01
When Hydronephrosis turn out to be a Parapelvic cyst
Y Xu, X Zhan, H Zhang, G Wang, A Kadier, P Wu, H Liu, D Liu, Y Dong, X Xu, H Zhou, Y Gao, T Xie
V05‐02
Transurethral Repair of a Vesicovaginal Fistula, A New Endoscopic Approach
C Martinez‐Arroyo, J Morales‐Montor, C Pacheco‐Gahbler, FM Santa Maria Orozco, G Fernandez Noyola, M Cantellano Orozco
V05‐03
C‐V GreenLight Laser Technique May Prevent Uncontrollable Bleeding During Management of Benign Prostate Enlargement
J Feghali
V05‐04
Antegrade endourological treatment for ureteral stones and ureteroenteric strictures after ileal conduit urinary diversion with Wallace I ureteroileal anastomosis
F Natal Alvarez, L Cuellar Martin, S Martin Martin, J Torrecilla Garcia‐Ripoll, M Bedate Nuñez, A Alonso Villalba, C Conde Redondo, A Ruano Mayo, A Zamora Horcajada, A Herranz Arriero, JM Diaz Romero, J Soto Rodriguez, F Lara Perez, C Marfil Peña, J Calleja Escudero
V05‐05
Zero‐exposure retrograde intrarenal surgery for ureteral stones
T Tsujioka, K Hirota, Y Atagi, K Seto, K Izumi, M Yamanaka, Y Kawanishi
V05‐06
Robotic Assisted Ureteroscopy: Combined Approach to Treating Difficult Ureteral Strictures and Stone Disease
DT Lybbert, BF Schwartz, MF Monn
V05‐07
Antegrade assisted bladder neck incision for complete bladder neck stenosis
C Van Haute, T Tailly
University Hospitals Leuven
V05‐08
Pelvic Lipomatosis ‐ Quintessence of Rarity with Stupendous Denouement
S Jayaprakash, M Thangarasu, N Jain
Apollo Main Hospitals, Chennai, Tamil Nadu, India
V05‐09
Transurethral incision with transverse mucosal realignment: an endoscopic repair of bladder neck contractures and vesicourethral anastomotic stenosis
JN Warner
V05‐10
Robot‐Assisted Laparoscopic Repair of A Huge Sliding Inguinal Hernia of The Urinary Bladder, Left ureter And Sigmoid Colon
AA Elbakry, C Crigger, T Trump, MW Salkini
V05‐11
Technique and Outcomes of Endoscopic Management for Postoperative Bladder Neck Contractures following Robot‐Assisted Radical Prostatectomy Using Injectable Human Amniotic Membrane and Umbilical Cord Bioregenerative Matrix
F Sheckley, N Velazquez, R Munver
V05‐12
An Initial Experience with the Real‐Time Detection of Kidney Stone Composition Using Artificial Intelligence and Smartphone Technology
A Peta, A Brevik, M Ayad, P Jiang, RM Patel, RV Clayman, J Landman
Abstract Video Session 06: Transurethral Surgery and Ureteroscopy
V06‐01
Laser Abalation of Urothelial Tumor of Upper Ureter
G Saber, E Lucas Filho, L Zaccaro
V06‐02
Endoscopic Incisional Uses of Thulium Fiber Laser in Upper Urinary Tract Strictures
AS Sadiq, JA Khusid, WM Atallah, M Gupta
V06‐03
5 Key Steps for High‐Frequency Ureteroscopic Dusting Technique: Illustration with Moses 2.0 Technology
NR Khajeh, KR Ghani
Department of Urology, University of Michigan
V06‐04
Exploring the Parameters that Impact the Laser Suction Effect in Holmium Laser Lithotripsy: A Video Analysis
NR Khajeh, TL Hall, WW Roberts, KR Ghani
Department of Urology, University of Michigan
V06‐05
Membranous and prostatic urethra calcification due to Corynebacterium urealyticum infection
SB Teles, ML Wroclawski, M Borrelli, JD Cha, OR Claros
Hospital Israelita Albert Einstein
V06‐06
First Experience of Inserting a thermo‐expandible Stent in Ureteral stenosis in Morocco
A Heddat, Y Houry, R Rabii
V06‐07
Using methylene blue to find the orifice of calyceal diverticulum calculi: a classical method of flexible ureteroscope
L Ye, J Wu, Y Wei
V06‐08
Zero‐exposure retrograde intrarenal surgery for obese patients
K Hirota, Y Atagi, K Seto, T Tsujioka, K Izumi, M Yamanaka, Y Kawanishi
V06‐09
Holmium laser deroofing of a prostatic abscess
A Coscione, J Campbell, P Acher
V06‐10
Enucleation and Morcellation of Bladder Leiomyoma
JC Smith, M El Tayeb
V06‐11
Combined endoscopic management of the distal ureteral obliteration with the Thulium Fiber Laser
A Martov, A Andronov, M Golubev, D Abdullaev, P Golubev
Abstract Video Session 07: Laparoscopy: Upper Tract
V07‐01
A novel technique to decrease Warm ischemia time In Laparoscopic Partial Nephrectomy with use of Satinsky Vascular Clamp
D Vaddi, P Ramakrishna, P Siddalinga Swamy, B Manas Babu, G Soundarya, A Hemnath, S Chahar, S Gunadal, P Rakesh
V07‐02
Laparoscopic heminephrectomy for left hilar kidney tumor T1b in the presence of nephrolithiasis
T Nguyen, M Thai, X Ngo, Q Chau, K Hoang, H Nguyen, L Dinh, H Le, T Nguyen, RW Dobbs
V07‐03
Laparoscopic stepwise approach for the treatment of renal carcinoma complicated with tumor thrombus of inferior lumen (or renal) vein
F Chen, K Li, S Li, S Tang
V07‐04
Withdrawn
V07‐05
Safety and Outcome of Laparoscopic Donor Nephrectomy with Early Branching Renal Artery
S Jayaprakash, M Thangarasu, N Jain
Apollo Main Hospitals, Chennai, Tamil Nadu, India
V07‐06
Laparoscopic Partial Nephrectomy for a Complex Right Renal Tumour
DNA methylation urine biomarkers test (EpiCheck® assay) in the diagnosis of upper tract urothelial carcinoma: results from a single‐center prospective study
A Gallioli, M Fontana, R Boissier, A Territo, P Diana, A Sánchez‐Puy, J Subiela, F Sanguedolce, JM Gaya, J Palou, A Breda
Department of Urology, Fundació Puigvert, Barcelona, Spain
MP18‐02
Outcome of Renal Transplantation after Laparoscopic Donor Nephrectomy: a Comparative Study Between Single and Multiple Renal Arteries
DA Mendiola, EL Gerial Jr., JA Abraham
National Kidney and Transplant Institute
MP18‐03
Open vs minimally invasive adrenalectomy for adrenal metastasis: a single center experience
A Pecoraro, D Amparore, M Burgio, E Checcucci, M Manfredi, P Alessio, S De Cillis, F Piramide, G Volpi, S Granato, M Sica, P Verri, S Piscitello, D Zamengo, B Carbonaro, J Mézière, L Ola, C Fiori, F Porpiglia
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
MP18‐04
Metabolic Disturbances During Topiramate Use and their Reversibility Following Drug Cessation
D Pelzman, E Kazi, M Semins, S Jackman
UPMC
MP18‐05
Withdrawn
MP18‐06
Withdrawn
MP18‐07
Minimal scrotoscopic epididymectomy vs open epididymtectomy for epididymal mass treatment: A multi‐center, middle‐term clinical trial
Y Gao, Y Wei, J Yang
MP18‐08
Comparison between the most used stone free predictor scales and the homologation of their rates, assisted by a new mobile application system, after retrograde intra renal surgery at a Mexican General Hospital
FM Santa Maria Orozco, C Martinez‐Arroyo, C Pacheco‐Gahbler, M Cantellano Orozco, I Navarro Ruesga, E davila Legorreta, M Aguilar Mendez
Dr. Manuel Gea Gonzalez General Hospital
MP18‐09
Outcomes of antegrade scrotal sclerotherapy for varicocele treatment: Our experience about 660 patients
M Jasser, R Mehdi, T Tarek, B Mohamed, K Ramzi, G Samir
Military Hospital of Tunis
MP18‐10
Pheochromocytoma of urinary bladder: a case report
M Jasser, R Mehdi, B Nadhir, K Ramzi, G Samir
Military Hospital of Tunis
MP18‐11
Prolonged Warm Ischemic Time is a Significant Risk Factor of Hemorrhagic Complication in Patients who Received Robotic Assisted Partial Nephrectomy
C Tsai, H Chung, E Huang, T Lin, T Huang, W Huang
MP18‐12
Patients experience and preference regarding subcutaneous venous thromboembolic prophylaxis following robotic assisted radical cystectomy
W Abou Chedid, GJ Nason, AT Evans, D Moschonas, MA Perry
Royal Surrey NHS Foundation Trust
MP18‐13
Analysis of the mid‐ and long‐term efficacy of suprapubic‐assisted laparoendoscopic single‐site nephroureterectomy
X Zou, C Chen, Z Guoxi, B Qian, L Quanliang, X Tianpeng
MP18‐14
Retrograde en bloc resection for non‐muscle invasive bladder tumor can reduce the risk of seeding cancer cells into the peripheral circulation
H Huang, J Xing, K Zhang
The First Affiliated Hospital of Xiamen University
MP18‐15
Minimally invasive retroperitoneal Adrenalectomy in oligometastatic disease recurrence post nephrectomy ‐ a safe and feasible approach
D Sri, S Sarkar, J Oakley, M Malki, M Hussain, NJ Barber
MP18‐16
Withdrawn
MP18‐17
En‐bloc versus conventional transurethral resection of bladder tumors: interim analysis of a single‐center prospective randomized trial
P Diana, M Fontana, A Territo, A Gallioli, A Piana, A Mercade', F Algaba, O Rodriguez Faba, JM Gaya, J Palou, A Breda
Department of Urology, Fundació Puigvert, Barcelona, Spain
MP18‐18
Management of the Adrenal Incidentaloma and Evaluation of Mass Size Alone as an Indication for Adrenalectomy: Our Experience
M Gabriel, O Prankerd ‐ Smith, J Saada, N Burgess
Norfolk & Norwich University Hospital
MP18‐19
Paraganglioma of the Organ of Zuckerkandl: laparoscopic resection via a transmesocolonic approach
SE Clements, FX Keeley
North Bristol NHS Trust
MP18‐20
Eleven years of experience with UTUC: survival and renal function after kidney sparing surgery versus radical nephroureterectomy
N Hendriks, J Baard, HP Beerlage, BM Schout, RC Pelger, KS Doherty, GM Kamphuis
Amsterdam UMC
MP18‐21
Endoscopic Submucosal Injection of a Human Amniotic Membrane Bioegenerative Matrix for the Management of Recalcitrant Bladder Neck Contractures
J Kuo, N Velazquez, B Desroches, R Munver
Hackensack Meridian School of Medicine
MP18‐22
Using a Natural Language Processing Program to Screen for Incidental Findings of Urolithiasis
J James, A Rai, L Richstone
The Smith Institute for Urology
Moderated Poster Session 19: Stents & Equipment II
MP19‐01
Technical trips and tricks for preserving a flexible ureteroscope during 270 interventions
PA Geavlete, R Multescu, C Ene, C Bulai, BF Geavlete
“Saint John” Emergency Clinical Hospital, Department of Urology
MP19‐02
Using the Quick Sequential Organ Failure Assessment Score to Predict Septic Shock after ureteral stenting for patients with ureteral stone and presumed urinary tract infection
JY Lee, C Kottooran, A Yaghoubian, N Uppaluri, K Hanson, M Borofsky, B Eisner
University of Toronto
MP19‐03
Delays in Ureteroscopy After Stent Placement Doubles the Cost of Treating Stone Patients
N Bhojani, R Paranjpe, B Cutone, S Rojanasarot, B Eisner
University of Montreal Hospital Center (CHUM)
MP19‐04
Development of a New Canadian Endourology Group Stent Symptom Score (CEGSSS)
N Bhojani, JY Lee, SK De, AG Lantz, S Sivalingam, M Ordon, KB Scotland, S Andonian, BH Chew
University of Montreal Hospital Center (CHUM)
MP19‐05
Reusable Digital Flexible Ureteroscope vs. a Single‐Use Flexible Ureteroscope in the Treatment of Urolithiasis: An EDGE Consortium Prospective Randomized Clinical Trial
BE Knudsen, T Posid, MW Sourial, VK Wong, R Paterson, KL Stern, J Moore, MR Humphreys, BH Chew
The Ohio State University
MP19‐06
A Novel Visual ‐ Grading for Ureteral Encrusted Stents Classification (V‐GUES) to Help Decide the Endourologic Treatment
BO Manzo, P Alarcon, EE Lozada, J Ojeda, C Morales, I Mehmet, BH Chew, F Sepulveda, M Ignacio, E Flores, a Cagri, E Emiliani
Hospital Regional de Alta Especialidad del Bajío
MP19‐07
Withdrawn
MP19‐08
Comparison of Tamsulosin, Tolterodine and their combination for the treatment of ureteral stent related symptoms: A Prospective, randomised, comparative study
N Reddy, S Vaddi, A Singh, A Ganpule, R Sabnis, M Desai
Muljibhai Patel Urological Hospital
MP19‐09
Comparison of ureteric stent removal procedures using reusable and single‐use disposable flexible cystoscopes following ureteroscopy and lasertripsy: a micro cost analysis
T Hughes, A Pietropaolo, L Tear, BK Somani
Southampton University Hospital
MP19‐10
Withdrawn
MP19‐11
How to reduce ‘double‐firing’‐induced scope damage by investigating the relationship between laser fiber core degradation and fiber jacket burn?
S Ryang, T Ly, H Yoon, D Park, J Han, S Jeong, H Jung, S Cho
MP19‐12
The new approach in the treatment of obstructive uropathy in pregnant women
SV Kotov, R Perov, PY Nizin
Pirogov Russian National Research Medical University (Pirogov Medical University)
MP19‐13
Recurrent Benign Urethral Strictures Treated with thermo‐Expandable Metallic Stents : 2 years follow up (first African experience)
A Heddat, Y Houry, R Rabii
University Mohammed VI of Health Sciences UM6SS
MP19‐14
Adoption of Single‐Use Flexible Cystoscopes for Outpatient Cystoscopy: A Micro‐Costing Analysis
ZT Su, M Huang, BR Matlaga, S Hutfless, K Koo
Mayo Clinic
MP19‐15
Clinical and postoperative characteristics of stentless ureteroscopy patients: a prospective analysis from ReSKU
R Unno, F Hamouche, H Yang, J Ahn, D Bayne, M Stoller, T Chi
University of California San Francisco
MP19‐16
Ureteral Stents with a Larger Diameter show Higher Rates of Unplanned 30‐Day Encounters
L Elson, D Wong, J Vetter, C Nottingham, A Desai
Washington University St Louis
MP19‐17
Initial experience of Allium ureteral stent in ureteral stricture after surgery and/or radiation treatment for malignancy
W Wang, X Gao, J Chen, L Peng, X Wei
MP19‐18
Image Distortion During Flexible Ureteroscopy: A Laboratory Model Comparing Super Pulse Thulium Fiber (SPTF) Laser vs High Power Ho:YAG Laser
CS Miller, BB Whiles, DA Duchene, DA Neff, WR Molina
University of Kansas Medical Center
MP19‐19
Follow‐Up of Patients Undergoing Ureteral Stent Placement With and Without Cloud‐Based Stent Tracking Software
L Subramani, J Crivelli, S Zhang, L Oliver, L Harvey, R Hsi, DG Assimos, JM Hollingsworth, K Wood
The University of Alabama
MP19‐20
Multi‐Institution Comparison of Nine Flexible Ureteroscopes Using a Validated Flexible Ureteroscope Evaluation Tool
MA Knoedler, S Quarrier, A Uhr, S Li, J Bell, SN Patel, KL Penniston, SG Hubosky, RK Jain, SY Nakada
University of Wisconsin, Department of Urology
MP19‐21
Single‐Centre Experience with Three Metallic Ureteric Stents (Allium URS, Memokath‐051 and Resonance) for Chronic Ureteric Obstruction
C Khoo, C Ho, V Palaniappan, A Ting, L Forster, M Kondjin‐Smith, H Abboudi, M Hanna, T El‐Husseiny, R Dasgupta
Imperial College Healthcare NHS Trust
MP19‐22
Lost to Follow‐up: A Prospective Risk Factor Analysis of Forgotten Ureteral Stents
F Stroie, D Raslan, A Roston, M Krajmerova, A Ghorayeb, J Stinson, C Hollowell, M Wille
Moderated Poster Session 20: Lasers II
MP20‐01
A matched‐paired comparison of a novel pulsed Thulium:YAG laser with standard lasers for endoscopic enucleation of the prostate (EEP)
C Netsch, CM Rosenbaum, AJ Gross, B Becker
Department of Urology, Asklepios Hospital Barmbek, Hamburg, Germany
MP20‐02
Does Metformin Protect Against Urinary Stone Formation In Diabetics?
DC Rosen, JN Bamberger, E Kaplan‐Marans, I Paranjpe, A Kapoor, D Atashokhan, AM Zampini, JA Khusid, B Gallante, WM Atallah, M Gupta
Icahn Mount Sinai School of Medicine, Urology
MP20‐03
Is the Faster Thulium Fiber Laser More Cost Effective Than the Holmium Laser When Treating Renal Stones?
AS Amasyali, N BROWN, J Maldonado, J Groegler, R Belay, D Baldwin, M Hajiha, JD Belle, DD Baldwin, A Assidon
Loma Linda University, Department of Urology
MP20‐04
How Low Can You Go? A Comparison of Low‐Dose, Very Low‐Dose, and Ultra Low‐Dose Fluoroscopy During Ureteroscopic Laser Lithotripsy
AS Amasyali, M Keheila, JD Belle, N Brown, M Hajiha, DD Baldwin
Loma Linda University, Department of Urology
MP20‐05
An in vitro analysis of Holmium:YAG and Thulium Fiber laser ablation rates
MJ Basulto‐Martínez, S Proietti, M Pavia, L Rico, Y Yeow, J Flores‐Tapia, A Esqueda‐Mendoza, F Gaboardi, G Giusti
Dept. of Urology, Hospital Regional de Alta Especialidad de la Península de Yucatán
MP20‐06
Unmet Needs in Postoperative Communication after Kidney Stone Surgery
M Huang, JS Winoker, ME Allaf, BR Matlaga, K Koo
Mayo Clinic
MP20‐07
Optimal Laser settings for maximal dusting in mini‐PCNL with suction using high power Holmium laser: a prospective study of 110 patients
N Reddy, M Desai, A Patil
Muljibhai Patel Urological Hospital
MP20‐08
Outcomes of Ureteroscopy and laser stone fragmentation (URSL) for kidney stone disease (KSD): Comparative cohort study using MOSES technology 60W laser system versus regular Holmium 20W laser’
T Hughes, A Pietropaolo, M Sinha, BK Somani
Southampton University Hospital
MP20‐09
Evaluation of the Learning Curve for Thulium Laser Enucleation of the Prostate Using Multiple Outcome Measures
L Berti, M Maltagliati, U Besana, A Calori, C Buizza, S Micali, BC Rocco, M Sighinolfi, G Bozzini
ASST Valle Olona
MP20‐10
Temperature Changes in the Collecting System and Renal Parenchyma of the Porcine Kidney during Dusting and Fragmentation Modes with a Superpulse Thulium Fiber Laser
Z Okhunov, P Jiang, AS Afyouni, M Ayad, R Arada, A Brevik, RM Patel, J Landman, RV Clayman
University of California, Irvine
MP20‐11
Vast Majority of Applied Laser Energy is Converted to Heat not Stone Ablation: in vitro Assessment
JJ Dau, TL Hall, NR Khajeh, SE Majdalany, AH Aldoukhi, KR Ghani, AJ Matzger, WW Roberts
University of Michigan
MP20‐12
Popcorn Laser Lithotripsy Efficacy of the Moses 2.0 Laser System: An In vitro Assessment
P Whelan, CJ Kim, D Ho, C Tabib, H Premo, P Zhong, GM Preminger, M Lipkin, F Soto‐Paulo
Duke University
MP20‐13
RIRS using SuperPulse Thulium Fiber Laser in patients with kidney stones 2 cm or greater
DA Sytnik, S Popov, I Orlov, I Pazin, M Suleymanov, A Kulikov
St.Luke's Clinical Hospital
MP20‐14
Effect of Concurrent Surgeries on Holmium Laser Enucleation of the Prostate: Retrospective Review of Single High‐Volume Center
M Assmus, T Large, AE Krambeck
Northwestern University, Department of Urology
MP20‐15
Three‐Dimensional Patterns of Stone Ablation with Different Ho:YAG Pulse Modes
NR Khajeh, TL Hall, KR Ghani, WW Roberts
University of Michigan
MP20‐16
Prospective single center study of SuperPulsed Thulium‐fiber laser in retrograde intrarenal surgery: first clinical data
C Azilgareeva, M Taratkin, E Goryacheva, Y Barghouthy, D Tsarichenko, G Akopyan, D Chinenov, S Ali, V Kozlov, D Enikeev
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia
MP20‐17
A cost‐comparison of Holmium laser enucleation of Prostate with and without MOSES
MS Lee, M Assmus, DK Agarwal, T Large, AE Krambeck
Northwestern University Feinberg School of Medicine
MP20‐18
Stone ablation efficiency of a new prototype pulse‐modulated laser and a 120W Holmium:YAG laser
B Yang, I Parab, J Cancino, S Liu, A Ray, TC Hasenberg, T Harrah, BW Turney
University of Oxford
MP20‐19
SuperPulsed Thulium‐fiber laser lithotripsy: an in vitro comparison of 200 μm and 150 μm laser fibers
C Azilgareeva, M Taratkin, S Ali, M Corrales, D Enikeev
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia
MP20‐20
Setting laser lithotripter parameters according to endoscopic view: a descriptive guide to optimize treatment outcomes
N Frego, D Maffei, L Domanico, M Paciotti, V Fasulo, D Pietro, R Hurle, M Lazzeri, P Casale, GF Guazzoni, G Lughezzani, NM Buffi, A Saita
Humanitas Clinical and Research Center ‐ IRCCS, via Manzoni 56, 20089 Rozzano (MI), Italy
MP20‐21
Thulium Fiber Laser Results in Shorter Operating Times During Ureteroscopy and Laser Lithotripsy
JR Ryan, MH Nguyen, JA Linscott, SW Nowicki, BM Jumper, JP Ingimarsson
Maine Medical Center Department of Urology
MP20‐22
Study of real time temperature changes during laser lithotripsy with Thulium Fiber Laser: An in‐vitro study
R Batra, R Sharma, A Singh, A Ganpule, R Sabnis, M Desai
Functional Outcomes of Focal Salvage MRI Fusion Guided HIFU for Localized Radiation Recurrent Prostate Cancer
A Kasraeian, M Alcantara, K Mola Alcantara, S Scionti
Kasraeian Urology
MP21‐02
Primary transrectal random prostate biopsy: is still actual?
A Campitelli, G Molisso, T Realfonso, M Addesso, G Napodano, R Sanseverino
MP21‐03
Complications after random TRUS guided transrectal prostate biopsy
G Napodano, M Addesso, T Realfonso, A Campitelli, G Molisso, A Pane, R Sanseverino
MP21‐04
Step‐by‐step development of a cold ischemia device for open and robot‐assisted renal transplantation
A Territo, M Fontana, A Gallioli, A Piana, P Diana, JM Gaya, J Huguet, P Gavrilov, O Rodriguez Faba, A Mottrie, C Facundo, L Guirado, J Palou, A Breda
Department of Urology, Fundació Puigvert, Barcelona, Spain
MP21‐05
Robotic assisted MRI‐US fusion guided target saturation biopsy of the prostate–diagnostic accuracy and clinical implications
C Wetterauer, P Trotsenko, M Matthias, P Brantner, T Vlajnic, L Bubendorf, D Winkel, M Kwiatkowski, H Seifert
University Hospital Basel, Department of Urology
MP21‐06
Is Biparametric MRI adequate to detect clinically significant prostate cancer in biopsy naïve patients? results from a prospective, single centre, non‐inferiority randomized trial
M Manfredi, E Checcucci, D Amparore, S De Cillis, G Volpi, A Pecoraro, F Piramide, A Piana, M Sica, S Granato, J Mézière, D Zamengo, G Cattaneo, F Russo, S De Luca, C Fiori, F Porpiglia
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
MP21‐07
Comparing target plus standard prostate biopsy vs target alone in naïve patients: a retrospective analysis on the basis of pathological examination of prostate specimens
E Checcucci, S De Cillis, D Amparore, G Volpi, F Piramide, S Granato, M Sica, P Alessio, A Pecoraro, G Cattaneo, D Garrou, M Manfredi, C Fiori, E Bollito, I Stura, G Migliaretti, F Porpiglia
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
MP21‐08
Utility of a Novel Platform for Performing Prostate Biopsy ‐ Results of the first 750 patients using a Free Hand Ultrasound Guided Local Anaesthetic Transperineal Prostate (LATP) Technology
M Yao, C Phelan, S Folkard, A Rajagopalan, B Varga, J Rusere, A Lamb, SS Kommu, R Popert, BA Eddy
East Kent Urology Department, Kent and Canterbury Hospital, East Kent Hospitals University NHS Foundation Trust
MP21‐09
Prostate biopsy is unnecessary in low Prostate Imaging ‐ Reporting and Data System (PI‐RADS) score lesions
D Kim, S Jeon, S Lee, C Lee, S Chang, S Lee
Department of Urology, School of Medicine, Kyung Hee University
MP21‐10
Focal transperineal laser ablation (TPLA) treatment of localized prostate cancer: short‐term functional outcomes and toxicity
LA van Riel, TM de Reijke, HP Beerlage, JR Oddens, M Martins, S Regusci
Department of Urology, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, the Netherlands
MP21‐11
Single center retrospective analysis of oncological and functional outcome in Magnetic resonance imaging‐guided transurethral ultrasound ablation (MRI‐TULSA) for the treatment of localized prostate cancer
F Leboutte, G Meskhia, L Meyer, O Lemmer, J Van de plas, W Willinek, A Neisius
Dept. of Urology, Krankenhaus der Barmherzigen Brüder Trier, University of Mainz, Germany
MP21‐12
Cancer control and safety outcomes following focal therapy using HIFU in 1,379 men with non‐metastatic prostate cancer: a multi‐institute 15 year experience
D Reddy, M Peters, T Shah, M Bertoncelli‐Tanaka, P Huber, D Lomas, A Rakauskas, S Guillaumier, T Dudderidge, R Hindley, A Emara, R Nigam, M Valerio, N Afzal, C Moore, M Arya, M Winkler, C Orczyk, M Emberton, H Ahmed
Imperial Prostate
MP21‐13
Suitability of focal therapy for prostate cancer in patients undergoing image guided transperineal biopsies
D Reddy, D Eldred‐Evans, N McCartan, F Hosking‐Jervis, H Ahmed
Imperial Prostate
MP21‐14
Withdrawn
MP21‐15
Withdrawn
MP21‐16
PROST: the future of robotic prostate biopsy
A Iseppi, S Puliatti, M Rizzo, M Bogdan, C Tenga, L Palladino, M Sighinolfi, BC Rocco, P Fiorini, S Micali
Azienda ospedaliero‐universitaria di Modena e Reggio Emilia, Modena, Italy
MP21‐17
Prospective analysis of MRI‐fusion and systematic biopsy. Do we overlook or overdiagnose?
A Morozov, M Taratkin, E Bezrukov, D Chinenov, A Amosov, K Puzakov, D Enikeev
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia
MP21‐18
Irreversible electroporation of localized prostate cancer: prospective assessment of safety and efficacy
A Shpikina, D Enikeev, M Taratkin, A Morozov, N Singla, J Rivas, E Barret, V Petov, P Glybochko
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia
MP21‐19
The safety and satisfaction of transperineal prostate biopsy under local anaesthetic in an outpatient setting
W Abou Chedid, GJ Nason, E Brokane, AT Evans, D Moschonas, MA Perry, S Langley
Royal Surrey NHS Foundation Trust
MP21‐20
Is prostate cancer detection influenced by biopsy needle length? A prospective study
A Cardoso, R Calaia, C Laranjo Tinoco, R Matos Rodrigues, S Anacleto, E Lima, E Dias
Hospital de Braga, EPE
MP21‐21
Does large prostate size, small lesion volume, or long lesion distance from biopsy probe reduce MRI targeted cancer detection?
M Bevill, J Drobish, B Barnes, CR Tracy, P Gellhaus
MP21‐22
Detection of Prostate Cancer using MRI US Guided Fusion Biopsy Processed and Contoured with Predictive Fusion: All in the Urologists Office
O Liseth, B Tran, N Sarantos, RI Carey, S Mclaughlin, ML Blute, V Bird
National Med. Assoc. and Research Group
Moderated Poster Session 22: Education
MP22‐01
3D automatic augmented reality Artificial intelligence technology during robot‐assisted radical prostatectomy: a new tool for a more accurate extracapsular extension identification
F Porpiglia, E Checcucci, D Amparore, P Piazzolla, M Manfredi, A Pecoraro, S De Cillis, A Piana, G Volpi, F Piramide, P Alessio, S Granato, E Vezzetti, C Fiori
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
MP22‐02
Does an endourology fellowship training affect practice patterns
T Aro, A Smith, A Rai, D Mikhail, D Hoenig, AD Smith, Z Okeke
The Smith Institute for Urology
MP22‐03
The History of Midwest Stone Institute (MSI) in Saint Louis: The Gateway to Endourology Training
AK Chow, BG Patel, J Palka, A Paradis, RS Figenshau, R Venkatesh
Washington University School of Medicine
MP22‐04
A Machine Learning Predictive Model of Post‐Ureteroscopy Urosepsis: A Case‐Control Study of 9 European centers from YAU endourology group
A Pietropaolo, A Rogers, R Geraghty, R Veeratterapillay, P Kallidonis, L Villa, L Boeri, E Montanari, G Atis, E Emiliani, E Sener, F Al Jaafari, J Fitzpatrick, M Shaw, C Harding, BK Somani
University Hospital Southampton
MP22‐05
National Implementation of a Virtual Subinternship in Urology
D Mikhail, EJ Margolin, A Paniagua‐Cruz, M Schwartz, M Feuerstein, LR Kavoussi, GM Badalato, L Richstone
Lenox Hill/Northwell Health
MP22‐06
3D virtual models guidance during minimally invasive partial nephrectomy: a new technology to reduce the loss of functioning renal parenchyma
D Amparore, A Pecoraro, E Checcucci, F Piramide, P Verri, S De Cillis, P Alessio, G Volpi, A Piana, J Mézière, M Burgio, F Solitro, A Veltri, C Fiori, F Porpiglia
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
MP22‐07
Comparing long term functional outcome between transperitoneal and the retroperitoneal approach in patients who have had robotic assisted partial nephrectomy
KE Okhawere, W Nkmedrim, A Beksac, TG Korn, KN Meilika, R Harrison, M Ahmed, JY Lee, R Abaza, DD Eun, A Bhandari, AK Hemal, J Porter, MD Stifelman, KK Badani
Icahn School of Medicine at Mount Sinai
MP22‐08
Transurethral Bladder Tumor Resection Simulator‐based Training, Courses and Curricula
K Pagonis, A Peteinaris, A Vagionis, C Adamou, T Tokas, D Liourdi, G ortner, M Obaidat, A Natsos, E Liatsikos, P Kallidonis
MP22‐09
Patient Safety in the Operating Room During Urologic Surgery: The OR Black Box Experience
A Rai, L Beland, T Aro, M Jarrett, LR Kavoussi
The Smith Institute for Urology
MP22‐10
Evaluation of Urology Trainee Preferences in Didactic Education: An International Choice‐based Conjoint Analysis
K Spradling, C Seufert, N Kern, MS Borofsky, M Sorensen, L Hampson, S Conti
MP22‐11
Authorship in Endourology: A Gender Reveal
G Jeng, L Beland, T Aro
MP22‐12
Analysis of Flexible Ureteroscopic Motion and Kinematic Efficiency ‐ A Simulation‐Based Pilot Study
G Gomez, L Stirling, D Wollin
Brigham and Women's Hospital Division of Urology
MP22‐13
Experiences and Attitudes Toward Surgical Simulation Among Urology Residents: A Five‐Year Survey Assessment of Participants in a Multi‐Institutional, Multimodal Simulation Workshop
DP Simon, S Setia, KG Baldea, SJ Kielb, S Crivellaro, S Eggener, AK Chow, C Coogan
Rush University Medical Center
MP22‐14
Withdrawn
MP22‐15
The Impact of Surgical Trainee Involvement in Laparoscopic Donor Nephrectomy on Perioperative Outcomes and Complications
J Kuo, B Desroches, M Degen, R Munver
Hackensack University Medical Center
MP22‐16
Evaluating the Acceptability of an Electronic Patient Decision‐Aid for the Surgical Management of Lower Urinary Tract Symptoms Secondary to Benign Prostatic Hyperplasia
D Bouhadana, D Nguyen, B Raizenne, J Schwarcz, H Gordon, B Chughtai, D Elterman, L Lavallée, P Martin, K McAlpine, R Paterson, H Razvi, K Zorn, N Bhojani
University of Montreal Hospital Center (CHUM)
MP22‐17
Impact of automation on the Aquablation learning curve: An international multicenter prospective study
AA Nasrallah, E Rijo, V Misrai, M Labban, J Najdi, A El Hajj
Department of Surgery, Division of Urology. American University of Beirut Medical Center
MP22‐18
Factors Informing Selection and Evaluation for Endourological Society Fellowships
K Gupta, JA Khusid, D Lundon, B Gallante, AS Sadiq, W Atallah, M Gupta
Icahn School of Medicine at Mount Sinai
MP22‐19
Evaluation of uroLogical tEAching in bRitish medical school Nationally: the LEARN multicentre cross‐sectional study
A Ng, V Vinson, A Asif, C Lam, A Light, K Jayaraajan, WA Cambridge, MG Matthews, KD Clement, M Kulkarni, NR Bhatt, S Khadhouri, V Kasivisvanathan
Leicester Medical School, University of Leicester, Leicester
MP22‐20
Three‐dimensional printing models of horseshoe kidney and duplicated pelvicalyceal collecting system for flexible ureteroscopy training: a pilot study
UJ Pereira‐Sobrinho, LA Favorito, J Albero, ML Becalli, FJ Sampaio
State University of Rio de Janeiro
MP22‐21
The impact of surgery on the intimate and social relationships of prostate cancer patients: a qualitative meta‐synthesis
O Eymech, O Brunckhorst, K Ahmed, P Dasgupta, C James
King's College London
MP22‐22
Ureteroscopy (URS) video consensus: a simple and effective way to improve awareness of patients undergoing URS
F Esperto, F Prata, A Civitella, P Tuzzolo, L Romei, V Crimi, F Tedesco, N Deanesi, T Bach, Y Tanidir, R Scarpa, R Papalia
Dept. of Urology, Campus Biomedico University of Rome, Rome, Italy
Robotic Retroperitoneal Lymph Node Dissection For Stage I Non‐Seminomatous Germ Cell Tumor
A Beksac, KN Meilika, AA Elbakry, KE Okhawere, O Ige, J Sfakianos, KK Badani
V09‐02
Withdrawn
V09‐03
Mayhem in the Retroperitoneum: Eroded IVC Filters
AM Asghar, D Strauss, RA Lee, H Hirsch, E Choi, DD Eun
V09‐04
Laparoscopic retroperitoneal lymphadenectomy in supine position: technical aspects
C Conde Redondo, V Pascual, M Bedate Nuñez, F Castroviejo Royo, F Natal Alvarez, A Zamora Horcajada, L Cuellar Martin, A Herranz Arriero
V09‐05
New technologies in robot‐assisted kidney transplantation: improving surgical performances, expanding the indication
A Piana, A Territo, A Gallioli, M Fontana, P Diana, JM Gaya, O Rodriguez Faba, J Huguet, P Gavrilov, A Mercade', J Subiela, L Guirado, C Facundo, A Bellin, D Amparore, J Palou, F Porpiglia, A Breda
V09‐06
Robotic Approach to Adrenal Mass with IVC Invasion: Managing a Difficult Case and Troubleshooting Failure of Equipment
M Billah, F Sheckley, S Ahsanuddin, J Cadwell, R Sawhney, R Harrison, M Ahmed
V09‐07
Intracorporeal and Extracorporeal Robot‐Assisted Kidney Auto‐Transplantation: Experience of the ERUS RAKT Working Group
A Breda, P Diana, I Giron‐Nanne, A Territo, A Gallioli, A Piana, JM Gaya, L Desender, B Van Parys, J Palou, N Doumerc, K Decaestecker
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
Robotic Partial Adrenalectomy in a Pediatric Patient
AA Elbakry, D Zekan, M Ost, O AL‐Omar
V09‐10
Step‐wise Surgery Guidance for Laparoscopic Left Adrenalectomy
H Yang, S Hung, L Chang, K Chiu
V09‐11
Utilization of Indocyanine Green for Performance of Robotic Nephroureterectomy in Patient with Prior Ileal Conduit
A Denisenko, M Ferretti, J Baber, N Patel
V09‐12
The Utility of Indocyanine Green Fluorescence in Robotic‐Assisted Adrenalectomy for Functional and Non‐functional Tumors ‐ An Initial Experience in Taiwan
P Liu, Y Lin, Y Ou, C Hsu, M Tung
V09‐13
Robotic Reconstruction of Uretero‐Ileal Anastamotic Stricture with VY Plasty
H Flynn, A Navaratnam, J Nielsen, S Davies
V09‐14
Robotic Partial Adrenalectomy for Syndromic Pheochromocytoma
A Woloshuk, J Farrow, CD Bahler, CP Sundaram
Video Session 10: Robotic Surgery: Bladder & Miscellaneous
V10‐01
Robot assisted laparoscopic vesico‐vaginal fistula repair with omental interposition : A prospective evaluation of Our experience
A Kumar, S Kumar, S Yadav, Y Prashanth, K Saurav
V10‐02
Perioperative outcomes of Robot assisted Lap Radical Prostatectomy in Locally Advanced High Risk Prostate Cancer :A prospective evaluation
A Kumar, S Kumar, S Yadav, Y Prashanth, K Saurav
V10‐03
Robotic cystectomy and neobladder / ileal loop operation due to invasive bladder tumor
OB Argun, MB Tuna, T Doganca, I Tufek, C Obek, AR Kural
V10‐04
Results of our series on oligometastatic prostate cancer. A case of robotic lymph node recurrence rescue surgery
A Pérez‐Lanzac, J Acebal Lúcia, A Allona Almagro
V10‐05
Robot‐assisted Laparoscopic Radical Cystectomy in a Rural Hospital Setting
M Ferretti, J Baber, N Patel, J Dungca, E Spencer, B Protyniak
V10‐06
Robotic Simple Cystectomy for Benign Disease
M Ferretti, J Dungca, J Baber, B Protyniak, N Patel
V10‐07
Robotic Radical Cystectomy with Intracorporeal Urinary Diversion in a Male using the daVinci Single Port System
M Billah, R Sawhney, M Zhang, S Ahsanuddin, M Ahmed
V10‐08
Use of Indocyanine Green and Near‐Infrared Imaging Assists with Intraoperative Localization of the Ureter and Margins during Robotic Bladder Diverticulectomy
B Desroches, N Gopal, R Munver
V10‐09
Robotic‐Assisted Diverticulectomy of Urinary Bladder for a Very Uncommon Case of Hutch Diverticulum with Obstructive Uropathy
C Yang, Y Lin, Y Ou, L Huang, C Hsu, M Tung
V10‐10
Robot‐assisted radical cystectomy with intracorporeal modified J‐pouch neobladder in female patient
P Li, Y Yang, L Tsai, C Huang
V10‐11
Robotic Bladder Diverticulectomy In a Pediatric Patient
AA Elbakry, O AL‐Omar
V10‐12
Robotic assisted laparoscopic partial cystectomy using the Da‐Vinci Single‐Port Robotic System
MS Tonzi, A Singh
V10‐13
Robotic assisted laparoscopic bladder diverticulectomy with urethrolysis
MS Tonzi, H Okafor
Moderated Poster Session 23: Robotics/Laparoscopy I
MP23‐01
Single Port Robotic Ureterolysis for Ureteral Obstruction From Idiopathic Retroperitoneal Fibrosis
S Crivellaro, GR Hale, L Morgantini
University of Illinois at Chicago
MP23‐02
Withdrawn
MP23‐03
Robotic Salvage Partial Nephrectomy: A Viable Approach for the Management of Local Tumor Recurrence Following Failed Nephron Sparing Surgery for Renal Tumors
C Griffin, F Zahwa, R Madi
Augusta University Health
MP23‐04
Perioperative Outcomes of Robotic Transvesical Single‐Port Simple Prostatectomy versus Holmium Laser Enucleation of the Prostate
D Aguilar Palacios, J Kaouk, HC Wright, M Abou Zeinab, S De
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
MP23‐05
Perioperative and Postoperative Outcomes of Single vs Multi‐Port Robotic‐Assisted Partial Nephrectomy
G Yankelevich, S Santarelli, D Kim, DC Edwards, Z Taylor, M Ahn
Medical University of South Carolina
MP23‐06
Robotic Retroperitoneal Partial Nephrectomy in pT1b/> tumors–pushing the boundaries of robotic retroperitoneal surgery
S Sarkar, D Sri, J Oakley, M Malki, NJ Barber, M Hussain
Frimley Park Hospital
MP23‐07
Perioperative Outcome in Robot‐Assisted Partial Nephrectomy with Surgical Navigation System for Highly Complex Tumors
J Mutaguchi, S Kobayashi, B Cho, K Lee, K Monji, E Kashiwagi, A Takeuchi, M Shiota, J Inokuchi, M Eto
Graduate School of Medical Sciences, Kyushu University Department of Urology
MP23‐08
Oncologic Outcomes of Dehydrated Human Amnion/Chorion Membrane After Nerve‐Sparing Robotic‐Assisted Radical Prostatectomy: A Propensity Score Matched Analysis
J Noël, S Reddy, M Sandri, S Bhat, M Moschovas, T Rogers, V Patel
Global Robotics Institute
MP23‐09
Robot‐Assisted Partial Nephrectomy: A Single‐Center Matched‐Pair Analysis of the Retroperitoneal versus the Transperitoneal Approach
A Eraky, C Hamann, N Harke, M Tropmann‐Frick, K Juenemann, D Osmonov
University Hospital Schleswig‐Holstein, Campus Kiel, Department of Urology and Pediatric Urology, Kiel, Germany
MP23‐10
Robotic Approach for Distal Ureteral Reconstruction in Post‐Radiation ureteral stricture
AA Elbakry, K Aldabek, T Trump, K Mitchell, MW Salkini
Department of Urology, West Virginia University Hospital
MP23‐11
Robotic‐assisted radical prostatectomy in young adults: age‐stratified oncological and functional outcomes
S Bhat, M Covas Moschovas, J Noël, S Reddy, T Rogers, V Patel
Global robotics institute
MP23‐12
Hospital Ownership, Geographic Region, Patient Age and Insurance Status Appear to Influence Patient Selection for Robotic‐Assisted Ureteral Reimplantation: A Population‐Based Analysis
JT Kurtzman, AS Ha, R Kosber, R Blum, S Brandes
Columbia University Irving Medical Center
MP23‐13
Racial Comparison of Patients Undergoing Minimally Invasive Partial Nephrectomy for Renal Masses at a Large Volume Tertiary Center
KG Sands, R Bhatt, J Vetter, A Paradis, AK Chow, S Bhayani, RS Figenshau, R Venkatesh
Washington University School of Medicine
MP23‐14
Contemporary pure laparoscopic vs robotic assisted laparoscopic radical nephrectomy: Cost and peri‐operative Outcomes at a high‐volume tertiary center
KG Sands, RS Figenshau, J Vetter, A Paradis, A Pierce, AK Chow, S Bhayani, K Du, E Kim, R Venkatesh
Washington University School of Medicine
MP23‐15
Standardizing robotic partial nephrectomy results in similar patient outcomes across the tumor complexity spectrum
KE Okhawere, A Beksac, R Patel, TG Korn, M Ahsan, KN Meilika, KK Badani
Icahn School of Medicine at Mount Sinai
MP23‐16
Comparing Partial Nephrectomy modalities in the Age of Robotics: Contemporary results from the US National Inpatient Sample
D Mikhail, M Nayan, M Kim, L Richstone, A Feldman
Lenox Hill/Northwell Health
MP23‐17
Robotic Partial Nephrectomy for Solitary Kidney Tumors –Expanding the Indication to T2 And T3 Disease?
A Beksac, S Kim, KE Okhawere, M Abou Zeinab, R Harrison, L Lenfant, ZR Schwen, MD Stifelman, DD Eun, R Abaza, KK Badani, J Kaouk
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
MP23‐18
The Outcome of Robotic Ureteral Reimplantation
MW Salkini
West Virginia University
MP23‐19
Robotic Inferior vena cava (IVC) Tumor thrombectomy: single center series of 11 cases
N Pokala
University of Missouri
MP23‐20
Automatic 3D augmented reality Robot Assisted Partial Nephrectomy with Indocyanine green guidance for a more precise and safety procedure
F Porpiglia, D Amparore, F Piramide, E Checcucci, P Verri, P Alessio, A Pecoraro, S De Cillis, A Piana, G Volpi, M Sica, P Piazzolla, A Bellin, M Manfredi, E Vezzetti, C Fiori
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
MP23‐21
Transitioning to the Extraperitoneal Single‐Port Robotic Kidney Transplantation
J Kaouk, M Abou Zeinab, A Beksac, Y Lin, A Aminsharifi, ZR Schwen, A Wee, M Eltemamy
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
MP23‐22
Transvesical Single‐Port Radical Prostatectomy: Our Initial Series
J Kaouk, M Abou Zeinab, A Beksac, ZR Schwen
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
Moderated Poster Session 24: Robotics/Laparoscopy II
MP24‐01
Suprapubic robot‐assisted transumbilical two‐port laparoscopic adrenalectomy for huge pheochromocytoma and paraganglioma with report of 5 cases
L Quanliang, Z Guoxi, X Zou, Y Yuan, X Rihai, G Wu
MP24‐03
Clipless and Athermal Pedicle Control with Selective Suturing Technique Proceeding with Neurovascular Bundle Preservation during Robot Assisted Radical Prostatectomy
MB Tuna, T Doganca, I Tufek, C Obek, AR Kural
Acibadem Maslak Hospital, Department of Urology
MP24‐04
A 10 year experience with retroperitoneal robotic‐assisted laparoscopic pyeloplasty
D Whiting, L Whitehurst, D Tsang, M Hussain, NJ Barber, M Malki
Frimley Park Hospital
MP24‐05
Application of holographic image and navigation in robotic assisted laparoscopic radical prostatectomy
G Zhu
Beijing United Family Hospital and Clinics, Urology Beijing, People's Republic of China
MP24‐06
Robotic Non Transecting Secondary Pyeloplasty Techniques for Recurrent Ureteropelvic Junction Obstruction
M Lee, Z Lee, AM Asghar, RA Lee, D Strauss, MD Stifelman, LC Zhao, DD Eun, N Krishnan
Lewis Katz School of Medicine at Temple University
MP24‐07
Outcomes of Robotic Simple Prostatectomy After Prior Prostate Surgery
M Lee, CU Okoro, JY Lee, AM Asghar, D Strauss, Z Lee, DD Eun, N Krishnan
Lewis Katz School of Medicine at Temple University
MP24‐08
Time of ligation of dorsal venous complex during RALP: evaluation of oncological safety and peri‐operative outcomes in organ‐confined and locally advanced prostate cancer patients
L Sarchi, M Sighinolfi, E Morini, A Cassani, B Filippi, S Assumma, A Piro, M Ticonosco, R Ferrari, S Puliatti, G Bianchi, S Micali, BC Rocco
Azienda ospedaliero‐universitaria di Modena e Reggio Emilia, Modena, Italy
MP24‐09
Utility of an Ultra Mini Doppler Ultrasound Probe Platform for Real‐Time Mapping for Nerve Spare during Robot Assisted Radical Prostatectomy
M Yao, D Mitchell, SS Kommu, BA Eddy
East Kent Urology Department, Kent and Canterbury Hospital, East Kent Hospitals University NHS Foundation Trust
MP24‐10
Does Type of Robotic Platform Make a Difference in the Final Cost of Robotic‐Assisted Radical Prostatectomy?
M Covas Moschovas, TA Helman, S Bhat, T Rogers, M Sandri, S Reddy, J Noël, V Patel
Global Robotics Institute
MP24‐11
Primary Results of in‐vivo Needle‐Based Confocal Laser Endomicroscopy in Human Prostate: A Safety and Feasibility Study
LA van Riel, A Swaan, CK Mannaerts, D Savci‐Heijink, TG van Leeuwen, TM de Reijke, M de Bruin, J Freund
Department of Urology, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, the Netherlands
MP24‐12
Preliminary results of in vivo focal transperineal laser ablation treatment of the prostate: correlation of mpMRI and CEUS imaging to histology in radical prostatectomy specimen
LA van Riel, R van Kollenburg, TM de Reijke, D Savci‐Heijink, MR Engelbrecht, HP Beerlage, TG van Leeuwen, M de Bruin, JR Oddens
Department of Urology, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, the Netherlands
MP24‐13
Effect of intraoperative use of electrosurgery on urinary incontinence after robot‐assisted radical prostatectomy
A Sawada, A Hamada, T Inoue, O Ogawa
Department of Urology, Kyoto University Graduate school of Medicine
MP24‐14
Robot‐Assisted Radical Cystectomy : Results from a Korean Multicenter Study
T No, J Tae, Y Choi, J Shim, S Kang, S Kim
MP24‐15
Withdrawn
MP24‐16
Evaluation of robotic versus open approaches for Unilateral ureteral reimplantation in pediatric patients
AA Elbakry, K Aldabek, O AL‐Omar
Pediatric Urology, Department of Urology, West Virginia Uninversity Hospital
MP24‐17
Intermediate Length Follow‐up of Single Port Laparoscopic Renal Cryoablation
HE Moreland, TC Peak, LJ Smith, MB Rothberg, JW Pike, LT O'Connor, DB Rukstalis
University of South Carolina School of Medicine
MP24‐18
The Application of Suprapubic Robotic‐assisted Transumbilical Two‐port Laparoscopy in Urology
X Zou, X Tianpeng, Z Guoxi, L Quanliang, Y Yuan, X Rihai
MP24‐19
Suprapubic‐assisted transumbilical laparoendoscopic single‐site surgery for treatment of middle and upper ureteral stricture
L Li, G Wu, Z Zhong, X Hui, X Zou, Z Guoxi
MP24‐20
Single‐Port Transvesical versus Multiport Robotic Simple Prostatectomy: A Comparison of Perioperative Outcomes
M Abou Zeinab, A Beksac, J Ulchaker, J Kaouk
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
MP24‐21
Automated machine learning segmentation and measurement of urinary stones on CT scan
K Lembrikova, R Babajide, JB Ziemba, Y Fan, GE Tasian
Comparison of Different Methods to Assess Kidney Volume Loss Following Partial Nephrectomy
A Beksac, KE Okhawere, C Dominy, TG Korn, KN Meilika, KK Badani
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
MP25‐02
Comparison of renal functional outcomes between warm and cold ischemia following minimally invasive partial nephrectomy
R Matsumoto, T Abe, S Yamada, J Furumido, H Kikuchi, T Osawa, N Shinohara
Department of Renal and Genitourinary surgery, Graduate School of Medicine, Hokkaido University
MP25‐03
Oncologic outcomes following partial nephrectomy versus percutaneous cryoablation: A propensity score matched analysis
NA Pickersgill, J Palka, J Vetter, G Henning, E Kim, H Kim, R Venkatesh, RS Figenshau
Washington University School of Medicine
MP25‐04
In vitro assessment of new ureteral biodegradable drug eluting stent design to adjuvant therapy in Upper tract urothelial carcinoma
F Soria, JE de La Cruz, M Soto, S Aznar, J Cenis Anadon, A Budia Alba, F Sanchez Margallo
Jesus Uson Minimally Invasive Surgery Centre
MP25‐05
The impact of diabetes on the prognosis of upper tract urothelial carcinoma after radical nephroureterectomy: a systematic review
X Gao, L Zhou, W Wang, H Li, K Wang
Department of Urology, Institute of Urology (Laboratory of Reconstructive Urology), West China Hospital, Sichuan University, Chengdu, Sichuan, P.R. China
MP25‐06
Is minimally invasive partial nephrectomy safe in case of cT2 renal masses? Comparative analysis after 10 years of follow‐up
D Amparore, A Pecoraro, F Piramide, E Checcucci, P Alessio, S De Cillis, G Volpi, A Piana, P Verri, M Sica, S Piscitello, M Burgio, B Carbonaro, D Zamengo, M Cossu, M Manfredi, C Fiori, F Porpiglia
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
MP25‐07
Predicting Renal Function after Radical Nephrectomy in Search for an Indication for Partial Nephrectomy
J Na, J Kim, S Alip, W Han
Yonsei University College of Medicine
MP25‐08
Analysis of risk factors predicting oncological outcome of the heterogenous T3aN0M0 kidney cancer
J Na, J Kim, J Kim, S Alip, W Han
Yonsei University College of Medicine
MP25‐09
Comparing perioperative outcomes between transperitoneal and retroperitoneal approaches in patient with obesity after robotic assisted partial nephrectomy
KE Okhawere, R Patel, A Beksac, KN Meilika, TG Korn, A Perez, S Kuppa, R Harrison, R Abaza, DD Eun, A Bhandari, AK Hemal, J Porter, M Stifelman, KK Badani
Icahn School of Medicine at Mount Sinai
MP25‐10
Prevalence of benign renal masses after partial or radical nephrectomy in Caucasian Americans versus African Americans
SP Argade, J Vetter, J Palka, KG Sands
Washington University School of Medicine
MP25‐11
Defining Patient Selection for Surveillance of Renal masses: Results from a MUSIC consensus panel
A Patel, B Lane, M Butaney, A Johnson, J Qi, C Rogers, F Urological Surgery Improvement Collaborative
Henry Ford Health System
MP25‐12
Risk factors for postoperative ileus after robot‐assisted radical cystectomy with intracorporeal urinary diversion
K Zennami, M Sumitomo, K Takahara, T Nukaya, M Takenaka, K Fukaya, M Ichino, N Fukami, H Sasaki, M Kusaka, R Shiroki
MP25‐13
hTERT, hTR and TERT promoter mutations as markers for urological cancers detection: a systematic review
A Morozov, N Potoldykova, M Enikeev, A Glukhov, A Shpikina, E Goryacheva, M Taratkin, B Malavaud, D Enikeev
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia
MP25‐14
Real world experience of metastatic urothelial carcinoma treated with immune check point inhibitors
H Hsiang‐Chen, L Jian‐Ri
Taichung Veterans General Hospital, Division of Urology, Department of Surgery, Taichung
MP25‐15
Establishment of Prognostic Nomogram and OS‐Calculator for Patients with Stage III and IV Renal Cell Carcinoma
l Hao, K Wang
MP25‐16
Withdrawn
MP25‐17
Incidence of benign tumors at partial nephrectomy for solitary renal mass presumed to be renal cell carcinoma: our experience of 195 cases
R Baio, U Di Mauro, O Intilla, G Molisso, A Pane, R Sanseverino
MP25‐18
High Risk Disease And Poor Followup: The Role Of Renal Mass Biopsy In A Cohort Of Veterans
K Anishchenko, S Antoine, R Lenzmeier, S Kim, GL Lloyd
Department of Urology, Rocky Mountain Regional Veterans Hospital
MP25‐19
Initial Management of Indeterminate Renal Masses in a Statewide Collaborative:a MUSIC‐KIDNEY analysis
M Butaney, A Patel, B Lane, J Qi, A Johnson, C Rogers, F Urological Surgery Improvement Collaborative
Henry Ford Health System
MP25‐20
Endoscopic exploration directly impacts clinical decision making in the management of patients with suspected upper tract urothelial carcinoma following radical cystectomy
J Aumatell, P Diana, J Huguet, J Subiela, A Piana, JM Gaya, O Rodriguez Faba, A Territo, A Gallioli, J Palou, A Breda
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
MP25‐21
Management of primary upper urinary tract carcinoma in situ diagnosed by ureteroscopic biopsy: is bacillus Calmette‐Guerin an alternative to nephroureterectomy?
S Fontanet‐Soler, A Territo, A Piana, A Gallioli, P Diana, J Huguet, JM Gaya, P Gavrilov, J Palou, A Breda
Department of Urology, Fundació Puigvert, Barcelona, Spain
MP25‐22
Pre‐Nephroureterectomy Diagnosis of Low‐Grade Urothelial Carcinoma Does Not Predict Low Grade Disease On Final Pathology
M Hout, B GOLIJANIN, C Tucci, F Kazal, TK O'Rourke, DW Sobel, G Pareek, D Golijanin
The Warren Alpert Medical School of Brown University
Moderated Poster Session 26: Clinical Oncology I
MP26‐01
Laser versus Electrical E‐Bloc resection of bladder tumors for treatment of non‐muscle invasive bladder cancer; critical appraisal through a randomized trial
A Elshal, M Bahy, M Laymon, A Hashem, A Mosbah, A Nabeeh
Mansoura Urology and Nephrology Center
MP26‐02
Clinical Significance of Preoperative Thrombocytosis in Patient with urothelial carcinoma from renal calyx to distal ureter
P Song, Y Kim, J Choi, Y Ko, K Moon, H Jung
Yeungnam University Medical Center
MP26‐03
Rate of Proliferation as Prognostic Marker in UTUC
C Malm, G Jaremko, M Brehmer
Karolinska Institutet. Stockholm South General Hospital
MP26‐04
Ureteroscopy Vs Radical Nephroureterectomy for low grade upper tract urothelial carcinoma
AY Lazarovich, AY Shvero, D Zillberman, E Fridman, M Laufer, Z Dotan, J Ramon, H Winkler, N Kleinmann
Sheba Tel‐Hashomer Medical Center
MP26‐05
Nephron sparing surgery in extreme cases of upper tract urothelial carcinoma
AY Lazarovich, AY Shvero, D Zillberman, M Laufer, Z Dotan, H Winkler, N Kleinmann
Sheba Tel‐Hashomer Medical Center
MP26‐06
Skeletal muscle mass effects on estimated‐GFR decremant after donor nephrectomy
J Na, N Hong, M Yoon, Y Rhee, W Han
Yonsei University College of Medicine
MP26‐07
The use of ureteral access sheath does not modify the pattern of disease recurrence during conservative management of upper tract urothelial carcinoma
E Ventimiglia, C Corsini, P Dioni, O Traxer, F Montorsi, A Salonia, L Villa, S Proietti
Division of Experimental Oncology/Unit of Urology; URI; IRCCS Ospedale San Raffaele
MP26‐08
How long should you wait in‐between follow‐up ureteroscopies during conservative management of upper‐tract urothelial carcinoma?
E Ventimiglia, F Montorsi, A Salonia, O Traxer, L Villa
Division of Experimental Oncology/Unit of Urology; URI; IRCCS Ospedale San Raffaele
MP26‐09
Withdrawn
MP26‐10
Comprehensive analysis of early outcomes in radical nephrectomy with Inferior Venacava thrombectomy ‐ a seven year single center experience
M Thangarasu, S Jayaprakash, T Ganesan, B Venugopal, N Ragavan, A Balakrishnan, D Raghavan, N Jain
Apollo Main Hospitals, Chennai, Tamil Nadu, India
MP26‐11
Utility of cognitive targeted transrectal ultrasound biopsy for prostate cancer detection in financially constrained hospitals
M Thangarasu, S Jayaprakash, A Balakrishnan, A Sivaraman
Apollo Main Hospitals, Chennai, Tamil Nadu, India
MP26‐12
Dioscin promotes prostate cancer cell apoptosis and inhibits cell invasion by increasing SHP1 phosphorylation and suppressing subsequent MAPK signaling pathway
S He, Y Wei, J Yang
MP26‐13
Oncological and Functional Outcomes after Salvage Prostate Cryotherapy for the Management of Primary Brachytherapy versus Cryotherapy Failures: A Propensity Score Matched Comparison
H Orabi, A El‐Shafei, A Aminsharifi, L Gerber, Y Wu, T Polascik
Duke University Medical Center, Department of Urology
MP26‐14
A matched analysis of salvage robot assisted radical prostatectomy following focal ablation vs radical robotic assisted radical prostatectomy
S Bhat, M Covas Moschovas, J Noël, S Reddy, T Rogers, V Patel
Global robotics institute
MP26‐15
Management of upper tract urothelial carcinoma (UTUC) in patients with urinary diversion ‐ the 14Fr antegrade supermini approach
T Reid, S Huq, E Edison, N de Luyk, R Vitale, C Allen, S Choong, R Hubbard
Department of Urology, University College London Hospital
MP26‐16
Prevention of Bladder Recurrence with Intraoperative Gemcitabine Instillation Following Bladder Closure During Radical Nephroureterectomy
M Said, H Warner, V Packiam, CR Tracy, P Gellhaus
MP26‐17
Irreversible Electroporation for the Treatment of Small Renal Masses: 5‐Year Outcomes
JC Dai, TN Morgan, RL Steinberg, BA Johnson, A Garbens, H Kominsky, JA Cadeddu
UT Southwestern
MP26‐18
A systematic review of the use of non‐HPV biomarkers in penile squamous cell carcinoma
JA Bowie, S Singh, C O'Hanlon, O Brunckhorst, A Muneer, K Ahmed
King's College London
MP26‐19
Salvage Peri‐Rectal Mass Resection of Locally Recurrent Prostate Cancer after Radical Prostatectomy Delays the Need for Systemic Intervention
E Huang, K Liang, LM Huynh, W Zhang, TE Ahlering
University of California, Irvine
MP26‐20
Documentation of Nephrometry Scores for cT1 Renal Masses Correlates with Avoidance of Radical Nephrectomy Across the MUSIC‐KIDNEY Statewide QI Collaborative
S Perkins, A Patel, M Butaney, A Johnson, J Qi, C Rogers, B Lane, F Urological Surgery Improvement Collaborative
Henry Ford Health System
MP26‐21
Effect of Surgical Approach on Risk of Post‐Operative Renal Failure in Radical Nephrectomy and Nephroureterectomy: a validated risk model and propensity score matching
AA Nasrallah, C Gharios, M Itani, D Bacha, H Tamim, A El Hajj
Department of Surgery, Division of Urology. American University of Beirut Medical Center
MP26‐22
Radiofrequency and hyperthermia appear to have limited effect on bladder cancer cell viability and membrane permeability in vitro
JW van Hattum, IS Brummelhuis, EM Scutigliani, A Lev, JR Oddens, R Zweije, J Crezee, PM Krawczyk, E Oosterwijk, TM de Reijke, JA Witjes
Department of Urology, Amsterdam University Medical Centers, University of Amsterdam
Clinical value of patient‐specific three‐dimensional printing of kidney before partial nephrectomy: Qualitative and quantitative assessments
R Nayyar, K Sharma, C Das, P Singh, B Nayak, A Seth
AIIMS
MP27‐02
Does Taping the Patient to the OR Table During Minimally Invasive Surgery Increase the Risk of Pressure Related Complications?
M Keheila, JD Belle, L Burke, AS Amasyali, M Hajiha, DD Baldwin, G Martin, B Yi
Loma Linda University, School of Medicine
MP27‐03
Black Light Illumination Improves Speed and Accuracy of Foot Pedal Activation Without Compromising Dark Adaptation
M Keheila, JD Belle, H You, J Maldonado, A Krause, AS Amasyali, M Hajiha, DD Baldwin, G Martin
Loma Linda University, Department of Urology
MP27‐04
Withdrawn
MP27‐05
Influence of Radiation's Risks Education on Urology Residents Practice in Urological Surgeries with Radiation
BO Manzo, Y Gomez, S Hector, MS Gonzalez, FC Vicentini, C Morales, E Tejeda, J Valero, J Sanchez Núñez
MP27‐06
Utilitzation of Surgical Skills Assessment Tool by Urologists At Health System Level–Trends in Implementation and Score Distribution
D Mikhail, S Pettit, J Sarcona, A Tabibzadeh, S Bolourani, D Thompson, A Antonacci, L Richstone
Lenox Hill/Northwell Health
MP27‐07
Hygienic Keyboards: Designed to Reduce Infections, But May Increase Mistakes and Medical Errors
P Stokes, R Belay, JD Belle, M Keheila, AS Amasyali, M Hajiha, DD Baldwin, A Assidon
Loma Linda University, Department of Urology
MP27‐08
Could 3D virtual models reduce positive surgical margins rate after robot‐assisted radical prostatectomy? A prospective comparative study
E Checcucci, A Pecoraro, S De Cillis, D Amparore, F Piramide, A Piana, G Volpi, P Alessio, M Sica, S Granato, S Piscitello, B Carbonaro, G Cattaneo, M Manfredi, C Fiori, F Porpiglia
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
MP27‐09
Thirty‐Year Trends in the Surgical Management of Urolithiasis in the United States
R Alam, JS Winoker, A Alam, BR Matlaga
Johns Hopkins University School of Medicine
MP27‐10
Development of a Customizable Dual‐modality Kidney Phantom Model
BA Johnson, JC Gahan, J Vargas, P Le, M Shahedi, J Dormer, S Shahub, M Pfefferle, B Judson, Y Alshara, Q Li, B Fei
UT Southwestern
MP27‐11
A Novel Cost Effective Platform for Remote Live Surgical Mentoring and Review ‐ Advanced Mentoring in a High Volume Robotic Urological Training Centre
M Yao, J Mackinlay, A Barker, M Thomas, EH streeter, BA Eddy, SS kommu
East Kent Urology Department, Kent and Canterbury Hospital, East Kent Hospitals University NHS Foundation Trust
MP27‐12
Simulation models and training curricula for training in endoscopic enucleation of the prostate: A systematic review
K Pagonis, A Peteinaris, A Vagionis, C Adamou, D Liourdi, T Tokas, A Natsos, M Obaidat, G ortner, E Liatsikos, P Kallidonis
Department of Urology, University of Patras, Greece
MP27‐13
How many cases are necessary to overcome the learning curve for retrograde intra‐renal surgery?
D Kim, S Jeon, SJ Lee, C Lee, S Chang, SH Lee
Department of Urology, School of Medicine, Kyung Hee University
MP27‐14
On the Rocks: Can Urologists Identify Stone Composition Based on Endoscopic Images Alone? A Worldwide Survey of Urologists
JH Randall, BB Whiles, RV Carrera, JA Thompson, DA Duchene, DA Neff, WR Molina
University of Kansas
MP27‐15
Withdrawn
MP27‐16
Analysis of hand/instrument motion during ureteroscopy: Development of an enhanced simulation platform to aid in resident training
S Koo, K Fok, N Seo, B Alsaikhan, B Carrillo, MA Farcas
University of Toronto
MP27‐17
Withdrawn
MP27‐18
Survivin(BIRC5)Regulates Bladder Fibrosis in Partial Bladder Outlet Obstruction Rat Model
X Di, X Jin, L Xiang, X Gao, L Peng, W Wang, K Xiao, Y Liu, G Chen, D Luo, H Li, K Wang
Department of Urology, Institute of Urology (Laboratory of Reconstructive Urology),West China Hospitgal, Sichuan University
MP27‐19
Contemporary pain management practices of transurethral therapies for benign prostate hypertrophy: Results of a global survey
MS Lee, M Assmus, DK Agarwal, T Large, AE Krambeck
Northwestern University Feinberg School of Medicine
MP27‐20
Effectiveness of the RIRS navigation training module using 3D‐printing
G Jung, H Jung, J Han, S Jeong, H Yoon, J Park, S Cho
SMG‐SNU Boramae Medical Center
MP27‐21
Developing a Synchronous Hand/Instrument Motion‐Tracking and Video Capture Tool: Objective Assessment for Flexible Ureteroscopy Training
MA Farcas, J Trac, B Carrillo
Department of Urology at St. Michael's Hospital
MP27‐22
Beyond Efficiency: Surface Electromyography Enables Additional Insights into the Quality of Surgical Motion of Expert Urologists
P Xu, D Haik, P Jiang, A Peta, Z Okhunov, A Brevik, S Tapiero, J Emmanuel, R Soangra, J Landman, RV Clayman
Abstract Video Session 11: Robotic Surgery: Prostate
V11‐01
Techniques to Reduce Robotic Prostatectomy Cost and Operative Time
M Billah, S Ahsanuddin, J Cadwell, R Sawhney, R Harrison, M Ahmed
V11‐02
Robot‐assisted Radical Prostatectomy After Focal Therapy
A Garayev, F Atuğ
V11‐03
Salvage Retzius‐Sparing Robotic Radical Prostatectomy: Step by step description
R Madi
V11‐04
Radio‐guided Surgery Experience During Robotic Radical Prostatectomy
MB Tuna, T Doganca, OB Argun, I Tufek, C Obek, L Guner, K Guven, AR Kural
V11‐05
Retrograde paraaortocaval lypmphadenectomy during robotic radical prostatectomy in a patient followed by neoadjuvant chemo‐hormonal treatment
T Doganca, MB Tuna, OB Argun, I Tufek, S Keskin, C Obek, AR Kural
V11‐06
Tips and Tricks of Super extended lymphadenectomy during robotic radical prostatectomy
T Doganca, MB Tuna, OB Argun, I Tufek, S Keskin, C Obek, AR Kural
V11‐07
Surgical Tips of robot‐assisted radical prostatectomy in very high‐risk prostate cancer
J Park, H Park, H Lee, H Shin
V11‐08
Robotic‐assisted Radical Prostatectomy Utilizing the DaVinci SP System in a Patient with Previous Kidney Transplant
JA Ivey, R Pak
Mayo Clinic Florida
V11‐09
Tips and tricks in salvage ralp post focal therapy failure for prostate cancer
S Bhat, M Covas Moschovas, S Reddy, J Noël, T Rogers, V Patel
Global Robotics institute
V1‐10
Withdrawn
V11‐11
Nerve spare RALP with amniotic membrane: medium term outcomes
J Noël, S Reddy, S Bhat, M Moschovas, T Rogers, V Patel
V11‐12
RALP: Anatomy & Planes by Fellows for Fellows
J Noël, T Rogers, S Reddy, S Bhat, M Moschovas, V Patel
V11‐13
Robotic Assisted Laparoscopic Prostatectomy with the Da Vinci Xi® and SynchroSeal™ Instrument: A Single Surgeon Experience
ZR Leopold, P Romeo, HV Patel, A Srivastava, J Sterling, IY Kim
V11‐14
Robotic Simple Prostatectomy Through the Posterior Transvesical Approach
AC Harbin, S Shekar, G Reyes
Abstract Video Session 12: Single Port Robotic Surgery I
V12‐01
Single‐Port Transvesical Robotic Radical Prostatectomy: Description of Technique
A Beksac, M Abou Zeinab, ZR Schwen, A Aminsharifi, J Kaouk
V12‐02
Single Port Robotic Radical Cystectomy with Intracorporeal Creation of Neobladder: Description of Technique and Perioperative Outcomes
M Billah, F Sheckley, R Sawhney, N Gopal, M Stifelman, D Ali, S Ahsanuddin, G Lovallo, M Ahmed
V12‐03
Withdrawn
V12‐04
Use of Remotely Operated Suction Irrigation (ROSI) during Single‐Port Robotic Surgery
M Billah, S Ahsanuddin, J Cadwell, MD Stifelman, R Sawhney, R Harrison, M Ahmed
V12‐05
Technical details comparing the da Vinci SP and da Vinci Xi approach to radical prostatectomy
M Covas Moschovas, S Bhat, T Rogers, S Reddy, J Noël, C Chew, E Mazzone, A Mottrie, V Patel
Global Robotics Institute
V12‐06
Single Port Robot‐assisted Laparoscopic Radical Prostatectomy (SP‐RALP) A Side‐by‐Side Comparison of Extraperitoneal and Transperitoneal approaches
KN Meilika, A Beksac, KE Okhawere, O Ige, TG Korn, KK Badani
The Icahn School of Medicine at Mount Sinai
V12‐07
Extraperitoneal Single Port Robot‐assisted Laparoscopic Radical Prostatectomy (SP‐RALP) After Prior Bilateral Laparoscopic Inguinal Hernia Repair
KN Meilika, KE Okhawere, A Beksac, O Ige, TG Korn, KK Badani
V12‐08
Pure Single Port Redo Robot‐Assisted Laparoscopic Inguinal Lymph Node Dissection for Penile Cancer
KN Meilika, A Beksac, KE Okhawere, O Ige, TG Korn, KK Badani
V12‐09
Single Port Simple Prostatectomy
S Talamini, S Crivellaro
V12‐10
Single‐Port Robotic Transvesical Total Prostatectomy
MJ Zuberek, O Feldman‐Schultz, S Crivellaro
V12‐11
SP Extraperitoneal Radical Prostatectomy: Technique and Lessons on the Brink of 200 Cases
ZR Schwen, A Beksac, L Lenfant, A Aminsharifi, M Abou Zeinab, J Kaouk
Robot‐Assisted Laparoscopic Nephroureterectomy in a Horseshoe Kidney: Use of Indocyanine Green and Near‐Infrared Imaging Assists with Intraoperative Assessment of Vascularity
B Desroches, N Velázquez, R Munver
V13‐05
Robotic Radical Nephrectomy For Recurrent Renal Tumors
KN Meilika, KE Okhawere, A Beksac, O Ige, TG Korn, KK Badani
V13‐06
Robotic Metastectomy for Recurrent Renal Tumors
KN Meilika, A Beksac, KE Okhawere, O Ige, TG Korn, KK Badani
V13‐07
Selective Clamping for Robotic Partial Nephrectomy Using Indocyanine Green
J Dungca, J Baber, M Ferretti, N Patel
V13‐08
Robotic Retroperitoneal Radical Nephrectomy
M Said, RL Steinberg, CR Tracy, P Gellhaus
V13‐09
Robotic Radical Nephrectomy and Left‐Sided Level II Caval Thrombectomy: A New Combined Technique
JH Zhang, M Abou Zeinab, ZR Schwen, A Beksac, A Aminsharifi, M Eltemamy, J Kaouk
V13‐10
Robot assisted laparoscopic partial nephrectomy in Horseshoe kidney: Anatomical challenges and techniques
S Singh, P Ahluwalia, S Prakash Ojha, G Gautam
V13‐11
Robot‐assisted radical nephrectomy with inferior vena cava tumor thrombectomy: Technique and initial outcomes
S Singh, P Ahluwalia, S Prakash Ojha, G Gautam
V13‐12
En Bloc Resection of Locally Advanced Recurrent Renal Cell Carcinoma After Partial Nephrectomy
A Beksac, KN Meilika, AA Elbakry, KE Okhawere, O Ige, KK Badani
V13‐13
Robotic Excision of Local Recurrence Post Laparoscopic Radical Nephrectomy
KN Meilika, KE Okhawere, MP Wilson, TG Korn, KK Badani
V13‐14
Robotic‐assisted laparoscopic heminephrectomy for T3a renal mass in a solitary kidney
J Elyaguov, G Lovallo, M Stifelman, M Ahmed
Moderated Poster Session 28: Robotics/Laparoscopy III
MP28‐01
Long Term Comparative Outcomes of Robotic Partial Nephrectomy and Cryoablation in Patients with Solitary Kidneys: A Single Center Analysis
A Beksac, D Corrigan, M Abou Zeinab, ZR Schwen, A Aminsharifi, J Kaouk
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
MP28‐02
Tumor Size Accurately Predicts Functional Outcomes following Radical Nephrectomy
A Beksac, KE Okhawere, D Ranti, KN Meilika, TG Korn, KK Badani
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
MP28‐03
Robot Assisted Radical Prostatectomy Following Kidney Transplantation
M Shahait, A Sandberg, RW Dobbs, J walker, J Kim, P Mucksavage, D Lee
King Hussein Cancer Center
MP28‐04
Robotic Radical Cystectomy Is Not Associated With Increased Incidence of Local Pelvic Recurrence
R Madi
Augusta University Health
MP28‐05
The prevalence of orgasmic dysfunction after robot‐assisted radical prostatectomy
M Honda, R Shimizu, S Teraoka, Y Kimura, T Yumioka, H Iwamoto, S Morizane, K Hikita, A Takenaka
Department of Urology, Tottori University Faculty of Medicine
MP28‐06
Comparison of Surgical Outcomes Between Single‐Port and Multiport Robotic‐Assisted Prostatectomy, Cystectomy, and Partial Nephrectomy: A High‐ Volume Tertiary Center Experience
NA Pickersgill, J Gross, N Barashi, R Bhatt, J Vetter, J Palka, G Henning, RS Figenshau
Washington University School of Medicine
MP28‐07
Oncological Outcomes of Laparoscopic and Open Radical Nephroureterectomy for Advanced Upper Tract Urothelial Carcinoma
J Correia, A Rocha, G Mendes, B Teixeira, A Fraga, M Silva‐Ramos
Department of Urology, Centro Hospitalar Universitário do Porto
MP28‐08
A Matched Analysis of Conventional Multi‐Port versus SP Single‐Site Robotic Partial Nephrectomy
J Na, S Alip, N Son, J Kim, W Jang, Y Lee, KH Rha, W Han
Yonsei University College of Medicine
MP28‐09
Withdrawn
MP28‐10
Robotic Assisted Kidney Transplantation–Point of technique with our experience of median follow up of 43 months (3.6 years)
AP Patil, A Ganpule, AK Parikh, A Singh, R Sabnis, M Desai
Muljibhai Patel Urological Hospital Nadiad
MP28‐11
Robotic Ureteral Reconstruction for Recurrent Strictures After Prior Failed Management: A Multi‐Institutional Experience
M Lee, Z Lee, AM Asghar, RA Lee, D Strauss, R Reddy, MJ Metro, LC Zhao, MD Stifelman, DD Eun, N Krishnan
Lewis Katz School of Medicine at Temple University
MP28‐12
Comparison between Tisseel an PuraStat as a hemostatic material in robot assisted and laparoscopic partial nephrectomies
A Femic, M Häggman, S Ladjevardi
Department of Urology, Akademiska University Hospital
MP28‐13
Same Day Discharge for Robotic‐assisted Radical Prostatectomy: Recommendations from a Referral Center
S Reddy, R Perera, S Bhat, TA Helman, T Rogers, M Moschovas, J Noël, V Patel
Can Retroperitoneal Robot Assisted Partial Nephrectomy (RRAPN) be the default approach?
D Sri, M Malki, S Sarkar, H Niraghallaigh, G Pydisetty, J Oakley, M Hussain, NJ Barber
MP28‐16
Salvage Pelvic Lymph Node Dissection of Locally Recurrent Prostate Cancer after Radical Prostatectomy Can Delay the Need for Systemic Interventions
E Huang, K Liang, LM Huynh, W Zhang, TE Ahlering
University of California, Irvine
MP28‐17
Revo‐i versus da Vinci in retzius‐sparing robot‐assisted radical prostatectomy: a propensity score analysis of surgical and oncologic outcomes
P Koukourikis, S Alip, J Kim, KH Rha, W Han, J Na
MP28‐18
Withdrawn
MP28‐19
Withdrawn
MP28‐20
Comparative analysis of trifecta outcomes in robot‐assisted partial nephrectomy(RAPN) for cT1a versus cT1b plus renal tumors: Is RAPN for cT1b plus renal tumors feasible?
S Singh, S Khanna, D Darlington, S Patil, A Tamhankar, P Ahluwalia, G Gautam
AIIMS,Rishikesh
MP28‐21
Single Port Robotic Kidney Autotransplantation: Minimizing an Invasive Surgery
ZR Schwen, A Beksac, L Lenfant, A Aminsharifi, S Kim, A Wee, M Eltemamy, MJ Noble, J Kaouk
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
Moderated Poster Session 29: Robotics/Laparoscopy IV
MP29‐01
Prospective randomized evaluation of organ retrieval site for hernia development following robot assisted laparoscopic radical prostatectomy
OB Argun, MB Tuna, T Doganca, I Tufek, C Obek, AR Kural
Acibadem Mehmet Ali Aydınlar University School of Medicine Urology Department
MP29‐02
Robotic Partial Nephrectomy for Hilar Tumors: Improving Outcomes to Replicate the Results of Non‐Hilar Tumors
A Beksac, M Abou Zeinab, ZR Schwen, A Aminsharifi, J Kaouk
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
MP29‐03
Redo Robotic Partial Nephrectomy for Recurrent Renal Masses: A Multi‐Institutional Analysis
A Beksac, U Carbonara, M Abou Zeinab, S Hemal, M Meagher, A Tafuri, G Tuderti, A Antonelli, R Autorino, G Simone, IH Derweesh, J Kaouk
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
MP29‐04
Is one Layer Mass Closure Enough in Robotic Partial Nephrectomy
A Dahman, MW Salkini
West Virginia University
MP29‐05
Assessment of GEARS scores and perioperative outcomes for Robotic Prostatectomy among high volume surgeons
D Mikhail, S Pettit, F Cascio, A Antonacci, L Richstone
Lenox Hill/Northwell Health
MP29‐06
Neurovascular structure‐adjacent frozen‐section examination (NeuroSAFE) Robotic Assisted Laparoscopic Radical Prostatectomy: Outcomes from 500 consecutive cases in the UK
J Noël, N Spencer, S Lodhia, S Karim, S Taneja, D Moghanchizadeh, A Nayak, A Tamhankar, R Swamy, S Agarwal, A Narula, T Lane, J Adshead, N Vasdev
Global Robotics Institute
MP29‐07
Surgical quality of robotic vs laparoscopic radical nephroureterectomy for upper tract urothelial carcinoma: a multicenter propensity score matched pair analysis (ROBUUST collaborative group)
A Veccia, U Carbonara, R Meherazin, DD Eun, ML Gonzalgo, V Margulis, R Uzzo, J Porter, CP Sundaram, F Abdollah, A Mottrie, A Minervini, KH Rha, G Cacciamani, G Simone, M Ferro, Z Wu, H Djaladat, I Derweesh, R Autorino
Division of Urology, Virginia Commonwealth University Health System, Richmond, VA, USA; b Urology Unit, ASST Spedali Civili Hospital, Brescia, Italy, Department of Medical and Surgical Specialties, Radiological Science, and Public Health, University of Brescia, Italy
MP29‐08
Endophytic Tumor Resection via Robotic Assisted Partial Nephrectomy: Comparison of Retroperitoneal and Transperitoneal Approaches
KE Okhawere, A Beksac, A Rambhia, KN Meilika, TG Korn, JY Lee, G Wayne, DD Eun, A Bhandari, J Porter, M Stifelman, KK Badani
Icahn School of Medicine at Mount Sinai
MP29‐09
Robotic surgical management of recurrent kidney tumors: operative and oncologic outcomes in a single center experience
J Daza, TG Korn, KE Okhawere, KN Meilika, A Beksac, KK Badani
Icahn School of Medicine at Mount Sinai
MP29‐10
Factors Affecting Robotic and Laparoscopic Partial Converted to Radical Nephrectomy: A Retrospective Multi‐Institutional Study in the Michigan Urologic Surgery Improvement Collaborative (MUSIC)
M Rudoff, C Rogers, J Qi, A Johnson, M Mirza, B Lane, D Wenzler
Michigan State University College of Human Medicine
MP29‐11
Impact of Multiple Renal Vessels on Graft Function in Laparoscopic Live Donor Nephrectomy
S Jayaprakash, M Thangarasu, N Jain
Apollo Main Hospitals, Chennai, Tamil Nadu, India
MP29‐12
Robotic approach and other factors associated with early discharge following simple prostatectomy: a New York statewide analysis, 2009‐2017
KT Ravivarapu, EB Garden, O Omidele, A Small, O Al‐Alao, MA Palese
Icahn School of Medicine at Mount Sinai
MP29‐13
Laparoscopic partial nephrectomy with Thulium Laser enucleation of the tumour: perioperative and functional outcomes
M Maltagliati, L Berti, C Buizza, L Rivolta, A Calori, M Sighinolfi, S Micali, BC Rocco, G Bozzini
ASST Valle Olona
MP29‐14
Comparison of Bladder Neck Contracture Formation between Robotic Intracorporeal versus Extracorporeal Neobladder Construction
R Bhatt, J Vetter, KG Sands, A Zafar, AK Chow, E Kim
Washington University School of Medicine
MP29‐15
Comparison of Decipher Score in patients with both biopsy and prostatectomy tissue specimens
S Reddy, R Perera, J Noël, M Moschovas, S Bhat, R Pokhrel, M Sandri, T Rogers, V Patel
Global Robotics Institute
MP29‐16
Single‐Port robotic assisted kidney surgery: 2 years of experience with a novel platform
MJ Zuberek, L Morgantini, A Ganesh, C Dennis, R Trippel, J Huang, S Francavilla, M Abern, S Crivellaro
University of Illinois Hospital and Clinics
MP29‐17
Single‐Port robotic assisted retroperitoneal vs transperitoneal partial nephrectomy : a retrospective analysis
MJ Zuberek, L Morgantini, A Ganesh, C Dennis, R Trippel, J Huang, S Francavilla, M Abern, S Crivellaro
University of Illinois Hospital and Clinics
MP29‐18
A novel risk index for cardiovascular adverse events following Partial Nephrectomy
AA Nasrallah, H Dakik, NF Abou Heidar, J Najdi, O Nasrallah, M Mansour, H Tamim, A El Hajj
Department of Surgery, Division of Urology. American University of Beirut Medical Center
MP29‐19
Results of a late clamping early declamping retroperitoneoscopic robotic assisted partial nephrectomy in a single surgeon series
W Khoder, S Astheimer, J Michaelis, M Grabbert, P Pohlmann, C Gratzke
Urology Department, Freiburg University
MP29‐20
Intraoperative Mannitol Administration During Laparoscopic Donor Nephrectomy and Impact on Long‐Term Graft Function
J Farrow, G Gryzinski, CD Bahler, CP Sundaram
Indiana University Health
MP29‐21
Propensity Score Matched Analysis of Single Port Versus Multiport Partial Nephrectomy
R Harrison, M Billah, T Lulla, C Caviasco, H Koster, R Sanchez De La Rosa, F Sheckley, A Sanders, G Lovallo, M Ahmed, MD Stifelman
Hackensack Meridian Hackensack University Medical Center
MP29‐22
Single‐center comparison hybrid vs robotic approach to nephrectomy and IVC thrombectomy
R Harrison, M Billah, R Sawhney, J Zaifman, M Wilderman, G Lovallo, M Ahmed, MD Stifelman
Hackensack Meridian Hackensack University Medical Center
Moderated Poster Session 30: Prostate Cancer
MP30‐01
Post Radical Prostatectomy Radiation Therapy with Androgen Deprivation Therapy Does Not Improve 10‐Year Overall and Prostate Cancer Specific Mortality Compared to Androgen Deprivation Therapy Alone
TE Ahlering, LM Huynh, E Huang, H Su
University of California, Irvine
MP30‐02
Active surveillance of post‐radical prostatectomy biochemical recurrence: Long term assessment of outcomes
TE Ahlering, E Huang, LM Huynh, H Su
University of California, Irvine
MP30‐03
Post‐radical prostatectomy prostate‐specific antigen doubling‐time kinetics: Observations of increasing versus decreasing doubling times
TE Ahlering, LM Huynh, E Huang, D Skarecky
University of California, Irvine
MP30‐04
Robotic Transversus Abdominis Plane Block is Clinically Equivalent to Ultrasound Guided Transversus Abdominis Plane Block and Local Anesthetic Injection:A Single Blind Randomized Clinical Trial in Robotic Prostatectomy Patients
DC Rosen, JS Winoker, G Mullen, E Moshier, A Sim, P Pathak, V Wagaskar, A Reddy, MA Palese, KK Badani, P Wiklund, A Tewari, R Mehrazin
Icahn Mount Sinai School of Medicine, Urology
MP30‐05
The value of PSA density per lesion in combination of PI‐RADS for improving the accuracy of prostate cancer detection
M Shahait, A Sandberg, A Achkar, D Lee, MC Strother, M Rosen, D Lee
King Hussein Cancer Center
MP30‐06
Is Retzius‐Sparing Robotic Radical Prostatectomy Oncologically Safe for High Risk Prostate Cancer Patients?
R Madi, N Hakam
Augusta University Health
MP30‐07
Advanced Reconstruction of Vesicourethral Support (ARVUS) during robot‐assisted radical prostatectomy:Early recovery of urinary continence and predictive factors
S Teraoka, Y Kimura, T Yumioka, N Yamaguchi, B Kawamoto, H Iwamoto, S Morizane, K Hikita, M Honda, A Takenaka
Department of Urology, Tottori University Faculty of Medicine
MP30‐08
Can direction of tumour growth predict prostate cancer grade?
D Papadopoulis, N Chari, D Ellis, U Ukwu, K Charitopoulos, I Donkov, S Bishara, S Mukherjee
London North West University Healthcare NHS Trust
MP30‐09
Association Between Oncotype DX Genomic Prostate Score and Final Tumor Pathology Report After Radical Prostatectomy
S Bhat, M Covas Moschovas, C Chew, M Sandri, T Rogers, P Dell'Oglio, S Roof, S Reddy, M Sighinolfi, BC Rocco, V Patel, J Noël
MP30‐10
Erectile function recovery prediction using a pre and post‐operative nomogram after Robot‐Assisted Laparoscopic Prostatectomy
S Bhat, M Covas Moschovas, J Noël, S Reddy, T Rogers, V Patel
Global Robotics institute
MP30‐11
Modelling of potency outcomes following robot assisted laparoscopic radical prostatectomy using cumulative incidence function for competing factors
S Bhat, M Covas Moschovas, S Reddy, J Noël, T Rogers, V Patel
Global robotics institute
MP30‐12
Withdrawn
MP30‐13
Increased cardiovascular risk after androgen deprivation therapies among newly diagnosed prostate cancer patients
H Hsiang‐Chen, L Jian‐Ri
Taichung Veterans General Hospital, Division of Urology, Department of Surgery, Taichung
MP30‐14
Anal sphincter length and power are associated with early continent after radical prostatectomy
H Hsiang‐Chen, L Jian‐Ri
Taichung Veterans General Hospital, Division of Urology, Department of Surgery, Taichung
MP30‐15
Fear of Recurrence and PSA Anxiety in Prostate Cancer
C James, O Brunckhorst, K Ahmed, P Dasgupta, O Eymech
Faculty of Life science and Medicine
MP30‐16
Accompanying the prostate cancer patient pathway: evaluation of novel clinical decision support software
T Horn, M Henkel, F Leboutte, P Trotsenko, S Dugas, S Sutter, G Ficht, C Engesser, M Matthias, J Ebbing, H Seifert, B Stieltjes, C Wetterauer
Research and Analytic Services, University Hospital Basel
MP30‐17
Urology Questionnaire for patients referred with high PSA
F Kapasi, J Spicer
East Sussex NHS Trust
MP30‐18
Baseline preoperative Comorbidity Illness Burden and Hypertension in Predicting Overall Cause Mortality in Men with Prostate Cancer
E Choi, LM Huynh, FM El‐Khatib, R Carillo Ceja, M Towe, E Huang, FA Yafi, TE Ahlering
MP30‐19
Baseline preoperative Comorbidity Illness Burden and calculated Free Testosterone association with Sexual Function in Prostate Cancer
E Choi, LM Huynh, FM El‐Khatib, R Carillo Ceja, M Towe, E Huang, FA Yafi, TE Ahlering
MP30‐20
Active surveillance of prostate cancer. Persuasion strategy in doctor‐patient communication
T Osipenko, V Fedorovskaya, M Taratkin, A Morozov, E Bezrukov, G Akopyan, E Shpot, W Imo, D Enikeev
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia
MP30‐21
Longitudinal Urinary Bother and Symptoms following Radical Prostatectomy with Membranous Urethral Length Preservation
R Carillo Ceja, LM Huynh, H Su, E Huang, D Skarecky, TE Ahlering
MP30‐22
Real time urethral and ureteral assessment during radical cystectomy using ex vivo optical imaging
F Esperto, F Prata, A Civitella, P Tuzzolo, V Crimi, L Romei, L Cacciatore, F Tedesco, C Taffon, A Crescenzi, R Scarpa, R Papalia
Dept. of Urology, Campus Biomedico University of Rome, Rome, Italy
Moderated Poster Session 31: Clinical Oncology II
MP31‐01
Pelvic nodal spread for metastatic melanoma: technique and benefits of robotic approach
BC Rocco, M Sighinolfi, L Sarchi, S Assumma, G Bozzini, A Cassani, E Morini, F Turri, C De Carne, S Micali
Azienda ospedaliero‐universitaria di Modena e Reggio Emilia, Modena, Italy
MP31‐02
Comparative Evaluation of Oncologic Outcomes According to the Anatomic Location of Surgical Margin Positivity After Partial Nephrectomy
A Beksac, S Kim, U Carbonara, M Meagher, A Tafuri, M Abou Zeinab, L Lenfant, A Antonelli, R Autorino, IH Derweesh, J Kaouk
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
MP31‐03
Withdrawn
MP31‐04
Perioperative and short‐term functional outcomes of robot‐assisted versus open partial nephrectomy : a single‐center retrospective study
K Takahara, K Fukaya, T Nukaya, M Takenaka, K Zennami, M Ichino, H Sasaki, M Sumitomo, R Shiroki
MP31‐05
Robotic versus laparoscopic living donor nephrectomy: A prospective study
M Thai, Q Chau, L Dinh, K Hoang, K Thai, D Vu, T Tran, X Ngo, H Tiong, T Nguyen
University of Medicine and Pharmacy at Ho Chi Minh City, Cho Ray hospital
MP31‐06
Animal model assessment of new ureteral biodegradable Mitomycin‐eluting stent to adjuvant therapy in Upper tract urothelial carcinoma. Safety study
F Soria, JE de La Cruz, M Soto, S Aznar, J Cenis Anadon, J Caballero Romeu, A Serrano, F Sanchez Margallo
Jesus Uson Minimally Invasive Surgery Centre
MP31‐07
miR‐223‐5p targeting ERG inhibits the biological behavior of prostate cancer
Y Gao, Y Wei
MP31‐08
The myth of the “July Effect” in urology: a study of oncology and BPH surgeries in the ACS‐NSQIP database
EB Garden, KT Ravivarapu, O Omidele, AC Small, O Al‐Alao, MA Palese
Icahn School of Medicine at Mount Sinai
MP31‐09
Bilateral Renal Cell Carcinoma: Neoadjuvant Tyrosine Kinase Inhibitor helps preserve Renal function prior to Robotic Partial Nephrectomy
J Zeng, AA Lwin, A Wong, K Batai, BR Lee
University of Arizona College of Medicine
MP31‐10
Neoadjuvant chemotherapy combined with immunotherapy followed by radical cystectomy
C Chang, C Lin, C Huang, K Chen, P Hsiao, C Tsai, Y Yang
MP31‐11
Real‐life practice of enbloc resection of bladder cancer among IEA and ESUT members: a survey
G bonfante, M Sighinolfi, T Calcagnile, M Ticonosco, L Sarchi, A Cassani, S Assumma, S Puliatti, G Bozzini, A Gozen, j Rassweiler, BC Rocco, S Micali
Azienda ospedaliero‐universitaria di Modena e Reggio Emilia, Modena, Italy
MP31‐12
Intravesical hyperthermic chemotherapy with Mitomycin C in intermediate‐high risk non muscle invasive bladder cancer: Our early results
S Pethe, R Nayyar, P Singh, B Nayak, A Seth
AIIMS
MP31‐13
Trends in 30‐Day Complications in Robotic‐Assisted Laparoscopic Prostatectomy (RALP)
S Marthi, DW Sobel, TK O'Rourke, C Tucci, G Pareek
Warren Alpert Medical School of Brown University
MP31‐14
Perioperative Serum Cytokine Levels in Patients Treated with Robot‐Assisted Laparoscopic Partial Nephrectomy
A Koizumi, S Narita, S Kashima, R Yamamoto, T Nara, M Huang, K Numakura, M Saito, S Satoh, T Habuchi
Department of Urology Akita University School of Medicine
MP31‐15
Renal biopsies performed before versus during ablation of T1 renal tumors: implications for prevention of overtreatment and follow‐up
C Widdershoven, B Aarts, PJ Zondervan, E Klompenhouwer, OM van Delden, W Prevoo, A Montauban van Swijndregt, M Henderickx, J van Moorselaar, A Bex, B Lagerveld
MP31‐16
Withdrawn
MP31‐17
Withdrawn
MP31‐18
Withdrawn
MP31‐19
The position of urine cytology within the diagnostic process for upper tract urothelial carcinoma
N Hendriks, GM Kamphuis, HP Beerlage, BM Schout, RC Pelger, KS Doherty, J Baard
Amsterdam UMC
MP31‐20
Ablative Therapies versus Partial Nephrectomy for Small Renal Masses–A systematic review and meta‐analysis of observational studies
V Vinson, A Abul, F Osman, H Ng, K Wang, Y Yuan, J Cartledge, T Wah
School of Medicine, Faculty of Medicine and Health, University of Leeds, Leeds Department of Targeted Intervention, Division of Surgery and Interventional Science, University College London, London
MP31‐21
Leveraging Natural Language Processing to Identify Incidental Renal Masses
J James, A Rai, L Richstone
The Smith Institute for Urology
Moderated Poster Session 32: Inflammation
MP32‐01
Gut microbiota and metabolites acetic acid were involved in the association between renal calcium oxalate stones and diabetes
K Wang, Q Jiang, X Jin, Y Liu, Y Ma, L Zhou, H Li
West China Hospital, Sichuan University
MP32‐02
Identifying Predictors of Sepsis Post‐Ureteroscopy in a US‐Based Population: Results from the Endourological Society TOWER Collaborative
N Bhojani, R Paranjpe, B Cutone, S Bhattacharya, BH Chew
University of Montreal Hospital Center (CHUM)
MP32‐03
What is the Cost of Sepsis after Ureteroscopy? Results from the Endourological Society TOWER Collaborative
N Bhojani, R Paranjpe, B Cutone, S Rojanasarot, BH Chew
University of Montreal Hospital Center (CHUM)
MP32‐04
The Endourologic Disease Group for Excellence (EDGE) Prospective Randomized Trial of 2 weeks vs 3 months of post‐operative antibiotics after percutaneous nephrolithotomy in complex patients with infection‐related kidney stones
BH Chew, AE Krambeck, NL Miller, R Hsi, KB Scotland, R Paterson, VK Wong, M Semins, D Lange
University of British Columbia
MP32‐05
Proteomic analysis of stone matrix: A window to the pathogenesis of urolithiasis
Q Wang, Y Yang, F Sun, S Wang
Department of Urology, Guizhou Provincial People's Hospital, Guizhou University, Guiyang, Guizhou, China
MP32‐06
Withdrawn
MP32‐07
The Optilume Drug Coated Balloon for recurrent anterior urethral strictures: 3‐year results for the ROBUST I study
O Kayes, S Elliott, R Virasoro, J DeLong, R Estrella, M Pichardo, R Rodriguez‐Lay, G Espino
St James's University Hospital
MP32‐08
The effect of urinary infection and antibiotics on calcium urolithiasis: A potential novel pathogenic role for zinc
J Bjazevic, KF Al, JP Burton, H Razvi
Western University
MP32‐09
Impact of Peri‐operative Antibiotic Choice on Infectious Complications After PCNL‐ A Prospective Randomized Trial
HC Wright, N Kachroo, RK Jain, O Mohammed, DC Fedrigon, A Zampini, S De, MJ Noble, M Monga, W Isac, S Sivalingam
Cleveland Clinic‐ Glickman Urological & Kidney Institute
MP32‐10
Withdrawn
MP32‐11
Urosepsi and Mortality, which aspects affect which outcomes
M Maltagliati, L Berti, U Besana, C Gastaldi, L Rivolta, C Buizza, M Sighinolfi, BC Rocco, S Micali, G Bozzini
ASST Valle Olona
MP32‐12
Withdrawn
MP32‐13
Preoperative Predictors of Positive Stone Culture
JA Khusid, BT Edelblute, D Lundon, AS Sadiq, WM Atallah, M Gupta
Icahn School of Medicine at Mount Sinai
MP32‐14
Kidney stones prevalence in Inflammatory Bowel Disease patients: An initial cohort report
V Dall'Aqua, L Macedo, A Lopes Neto
MP32‐15
Increased Prevalence of Urinary Tract Infections and Catheter‐Associated Urinary Tract Infections in Disorders Characterized by Iron Dysregulation
PR Patton, A Selva, B Prol, Z Chen, V Bird
Urologic Integrated Care
MP32‐16
Withdrawn
MP32‐17
Patient Predictors of 30 Day Post‐Operative Infectious Complications for Percutaneous Nephrolithotomy
V Kommidi, A Garbens, H Trivedi, BA Johnson, M Pearle, JA Antonelli
UT Southwestern
MP32‐18
Withdrawn
MP32‐19
Fighting uropathogen adhesion on stents with internal and external metal‐based coatings
B Domingues, IM Aroso, E Lima, A A. Barros, R L. Reis, R Bessa
University of Minho
MP32‐20
Drosophila melanogaster grown in cystine containing agar demonstrates cystine in malpighian tubules and absence of dose dependent survival
RI Carey, DL Carey, MS Carey
Florida State University College of Medicine
MP32‐21
Prevalence of bacteriuria among pregnant women and changes in antibiotic resistance patterns: a six‐year study
EC Cotton, BK Somani, K Saeed, R Geraghty, S Umranikar
University of Southampton
MP32‐22
Coeval xanthogranulomatous pyelonephritis and renal replacement lipomatosis
S Singh, A Upadhaya, A Mittal, T Aditya Narain, S Kumar, V Kumar Panwar, S Navriya
AIIMS
Abstract Video Session 14: Robotic Surgery: Ureter and Lower Tract
V14‐01
The Outcome of Ureteroneocystostomy Utilizing da Vinci ®
A Dahman, MW Salkini
V14‐02
Repair of Entero‐Conduit Fistula Using Robot‐Assisted Laparoscopy
Use of a Bioregenerative Amniotic Membrane Allograft Wrap During Robot‐Assisted Ureterolysis
B Desroches, N Velázquez, R Munver
V14‐05
Robotic‐Assisted Vesico‐Vaginal Fistula Repair with Omental Flap Interposition
CU Okoro, CJ Rutledge, DD Eun, N Krishnan
V14‐06
Tips and Tricks for Robotic Ureteral Reimplantation for Pediatric Age Group
AA Elbakry, M Ost, O AL‐Omar
V14‐07
Robot‐Assisted Vesico‐Vaginal Fistula Repair
H Hsiang‐Chen, C Kun‐Yuan
V14‐08
Robot‐Assisted Repair of Complex Benign Distal Ureteroenteric Strictures Following Radical Cystectomy
V Maxon, A Goh
V14‐09
Indocyanine Green Angiography for Use in Robotic Spermatic Cord Denervation
AM Makedon, JC Morrison, GL Lloyd
V14‐10
Robotic Techniques in the Management of Ureteral Anomalies
J Natarajan, J Farrow, CP Sundaram
V14‐11
Robotic Excision of a Large Mullerian Duct Cyst
A Srinivasan, P Kerr, C Kosarek, T Dafashy, L Alzweri, j sonstein
Abstract Video Session 15: Single Port Robotic Surgery II
V15‐01
Single Port Donor Nephrectomy Via Modified Pfannenstiel Incision: Initial Preclinical Experience
A Beksac, ZR Schwen, L Lenfant, M Abou Zeinab, A Aminsharifi, M Eltemamy, J Kaouk
V15‐02
Robotic Assisted Single Port Radical Nephroureterectomy Using the Intuitive SP Surgical System: Our Early Experience
AK Chow, BG Patel, G Henning, M Wahba, KG Sands, RS Figenshau
V15‐03
Robotic Assisted Single Port Retroperitoneal Off‐Clamp Partial Nephrectomy Using the Intuitive SP Surgical System: Our Early Experience
AK Chow, G Henning, B Patel, KG Sands, E Kim, RS Figenshau
V15‐04
Tips and Tricks for a True Single‐Site Surgery with the da Vinci SP platform: How to Increase Working Range of Assistant Instruments
J Na, J Kim, S Alip, W Han
V15‐05
Feasibility of Anterior Port Placement for Retroperitoneal Single‐Site SP Renal Surgery; a Cadaver Pilot Study
J Na, S Alip, J Kim, W Han
V15‐06
Single Port Robotic Assisted Laparoscopic Retroperitoneal Partial Nephrectomy
M Billah, S Ahsanuddin, J Cadwell, F Sheckley, M Ahmed
V15‐07
Single‐Port Robotic Kidney Transplantation via Extraperitoneal Approach
M Eltemamy, Y Lin, A Aminsharifi, A Beksac, ZR Schwen, M Abou Zeinab, D Goldfarb, A Wee, J Kaouk
V15‐08
Single Port Robotic‐assisted Laparoscopic Transmesenteric Dismembered Pyeloplasty
D Cao, D Simon, AK Chow
V15‐09
Use of Remotely Operated Suction Irrigation (ROSI) during Single Port Urologic Robotic Surgery: Creating a Truly Single Incision for Minimally Invasive Surgery
N Gopal, M Billah, C Cumarasamy, C Wright, M Stifelman, M Ahmed
V15‐10
Single Port Robotic‐Assisted Removal of an Eroded Inflatable Penile Prosthesis Reservoir and Repair of an Associated Bladder Fistula
DP Simon, S Brockman, A Beer, AK Chow
V15‐11
Minimally Invasive Lymphocele Drainage using the da Vinci® Single Port Platform: Step‐by‐Step Technique
S Reddy, M Moschovas, S Bhat, J Noël, R Perera, TA Helman, T Rogers, V Patel
V15‐12
Single Port Robotic Kidney Autotransplantation: Description of the Technique
ZR Schwen, A Beksac, M Abou Zeinab, MJ Noble, A Wee, M Eltemamy, J Kaouk
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
Abstract Video Session 16: Robotic Surgery: Kidney II
V16‐01
Robot assisted Laparoscopic transperitoneal “No clamp”‐ Zero Ischemia time partial nephrectomy in clinical T1a renal tumors
A Kumar, Y Prashanth, S Kumar, S Yadav, K Saurav
V16‐02
Retroperitoneal Robotic Partial Nephrectomy For a Hilar Renal Mass
A Beksac, KN Meilika, AA Elbakry, KE Okhawere, O Ige, KK Badani
V16‐03
Re‐do Robotic Pyeloplasty for Recurrent Ureteropelvic Junction Obstruction: A Case Series Review with Intraoperative Tips and Tricks for Success
BB Whiles, DA Duchene
V16‐04
A Standardized Technique for All Robotic Kidney Surgery
KN Meilika, MP Wilson, KE Okhawere, TG Korn, KK Badani
V16‐05
Robotic Partial Nephrectomy For Large Angiomyolipoma “12 cm” with zero ischemia time
A Mohamed, A Mansour, N Younes, A Al Ansari
V16‐06
Horseshoe Kidney Robotic Assisted Laparoscopic Pyeloplasty: A Case Series
Ureteral side‐to‐side anastomosis for transecting injury of completely duplicated collecting system
RA Lee, AM Asghar, D Strauss, MJ Metro, DD Eun
V16‐14
Combined Robotic and Endoscopic Pyelolithotomy in a Pelvic Kidney
A Higgins, A Nourian, J Cohn, J Friedlander
Moderated Poster Session 01: COVID‐19 & Beyond
Seasonal and COVID Pandemic‐Related Variations in Patients' Self‐Reported Adherence to Nutrition Recommendations for Stone Prevention Suggest Temporal Increases in Stone Recurrence Risk
KL Penniston, K Schobert, RJ Medenwald
University of Wisconsin School of Medicine and Public Health
Introduction & Objective: Nutrition therapy for stone prevention is indicated if risks are nutrition‐related. Common dietary recommendations (DRs) include higher fluid intake, lower salt intake, lower dietary acid load (e.g., more fruits/vegetables, F/V), and normal calcium intake (neither excessive nor insufficient). Adherence is challenging to assess and optimally includes multiple measures including patient‐reported outcomes. We assessed adherence to individualized, targeted DRs issued in our multidisciplinary stone prevention clinic.
Methods: From 1/2020‐1/2021 we invited patients to complete a questionnaire approximately 1 month after their appointment. We asked patients to estimate the number of days within the last week they followed the most common DRs and, in a separate question, days they followed all DRs. Questionnaires were sent by mail with postage‐paid envelopes for return. This was a quality improvement project; patients were thus offered to respond anonymously.
Results: Respondents (n = 132) represented 29% of patients who were sent questionnaires and were 50% female (61 ± 13 y). Of those providing clinical details, 77% were recurrent stone formers and 46% were on stone medication(s). There were no differences in adherence for men vs. women, recurrent vs. one‐time stone formers, nor for those on stone‐related medications vs. not. Overall, adherence to eating more F/V was lower (4.7 vs. nearly 5.5 d/week for all other DRs, P < 0.004). We separated responses by their receipt: summer/fall (April to mid‐November) and winter/spring (mid‐November to April), and by pre‐ vs. post‐COVID (before/after March 2020). F/V intake was significantly lower during winter/spring than summer/fall (4.4 vs. 5.5 d/week, P = 0.009). For the pre‐post COVID pandemic comparison, patients reported lower adherence to all DRs after the start of the pandemic (5.0 vs. 5.9 d/week, P = 0.009 for difference from before).
Conclusions: Overall, adherence to eating more F/V was significantly lower than for other DRs and was lower yet during winter/spring. The COVID pandemic did not affect F/V intake specifically but did reduce adherence to all DRs. F/V are important in stone prevention because they provide bicarbonate precursors that increase urine citrate and pH. F/V also provide other stone inhibitors, including phytate, which in urine inhibits calcium stone formation, and prebiotics, some of which selectively enhance oxalate‐degrading gut bacteria. Moreover, F/V intake can account for up to 30% of urine output and thus may help to meet fluid recommendations. Barriers to F/V intake, which may include seasonal variations in cost and availability, should be addressed.
Withdrawn
Percutaneous nephrostomy in Ureteropelvic junction obstruction with poorly functioning kidney: Is it still pertinent in adults
A Srivastava, S Kakoti, Z Tamboli, SK Sureka, UP Singh
Sanjay Gandhi Post Graduate institute of medical sciences. Lucknow
Introduction & Objective: To determine the pertinence of percutaneous nephrostomy (PCN) drainage in adult patients of primary uretero‐pelvic junction (UPJ) obstruction with poorly functioning kidneys (PFK; < 20% split renal function).
Methods: Clinical records of all patients with primary UPJ obstruction with PFK who underwent PCN drainage in our institute between February 2015 and January 2020 were retrospectively reviewed. The patients were divided into four groups according to their split renal function (SRF) obtained from Tc‐99m‐ethylenedicysteine (EC) diuretic renogram. Group I consisted of all patients having SRF ≤5%, Group II with SRF 6‐10%, Group III with SRF 11‐15%, and finally group IV with SRF 16‐20%. Those patients in whom SRF was improved by >10% and had daily PCN output >400 ml, underwent pyeloplasty and the rest underwent nephrectomy.
Results: 72 patients were studied, out of which 5 were in group I, 20 in group II and III each, and 27 in group IV. The mean age of presentation was 34.4 ± 14 years. The SRF improvement of >10% was seen in 55 patients (76.4%) after PCN drainage (p < 0.05). Pyeloplasty was done in 40 patients (55.6%) and nephrectomy was done in 32 patients (44.4%).
Conclusions: In conclusion, we recommend the use of Tc‐99m EC scan for estimation of SRF during an initial presentation in every patient followed by reconstructive surgery if SRF is above 15% and nephrectomy if it is below 5%. The trial of PCN is pertinent if SRF is between 6% to 15%.
Kidney stone disease prevalence from administrative coding compared to self‐report: a report from the All of Us Research Program
CM Forbes, N Nimmagadda, NL Kavoussi, NL Miller, R Hsi
Vanderbilt University Medical Center, Department of Urology
Introduction & Objective: Kidney stone prevalence estimates determined by administrative claims data and by self‐report differ due to their methodologic differences. To better characterize these differences and to identify contributing demographic and socioeconomic factors that influence how kidney stone diagnoses are ascertained, we sought to compare rates of patient‐reported diagnoses to administrative claims using a common dataset derived from recruitment of diverse populations in the U.S.
Methods: From the All of Us Research Program data, we identified adult participants with and without a patient‐reported history of kidney stones at enrollment in 2016‐2018, and with and without administrative claims (1980‐2017) for kidney stone diagnoses. Among 223,921 participants including 52% persons from racial minorities, there were 21,712 participants who had both patient‐reported medical history and medical claims data available for analysis. We compared differences in age, sex, race, education, employment status and healthcare access among patients with self‐reported kidney stone history without medical claims to those with claims‐based diagnoses.
Results: The claims‐based prevalence of kidney stones was 5.7% (n = 1231) and by self‐report it was 8.6% (n = 1877). Among participants with either kidney stone‐specific claims or self‐reported history (n = 2235), there were 45% (n = 1004) who had self‐reported history only. This indicates that that almost half of the participants with kidney stones did not have a prior kidney‐stone specific medical claim. Compared to participants with any kidney stone‐specific claim, participants with only self‐reported history were younger (62 vs 63, p < 0.001) (Table 1). No differences were observed in sex, race, education, employment status, and ability to afford healthcare between groups.
Conclusions: Kidney stone prevalence by self‐report is higher than claims‐based prevalence in this national research program. According to our findings, self‐managed stone disease without clinical care is common and occurs in almost half of patients with kidney stones. No notable differences in demographic and socioeconomic factors were observed among kidney stone patients with and without clinical care.
A Delphi Process Consensus Statement on Urinary Stone Treatment During COVID‐19: A World Endourological Society TOWER Research Initiative
R Smith, T Tailly, BH Chew, N Bhojani, KB Scotland
Institute of Urology, University College London Hospitals NHS Foundation Trust
Introduction & Objective: COVID‐19 continues to have a profound effect on urolithiasis management with varying recommendations for prioritization across different healthcare systems. We used the Delphi method to obtain international consensus recommendations for managing urolithiasis during the pandemic.
Methods: 53 key opinion leaders from 36 countries within the Endourological Society contributed to a three‐round Delphi process addressing the general organisation, inpatient and outpatient management and follow‐up care of urolithiasis patients to determine best practices for suspension and resumption of care.
Results: Consensus was achieved in 64/84 (76%) questions allowing the following recommendations to be made for the management of Urolithiasis during the pandemic.
1 Consultations should ideally be delivered via telephone or video conferencing, prioritizing patients with Infection, acute kidney injury, pain including acute ureteric colic and visible haematuria.
2 The Surgical focus should be to reduce the risk of complications even if it means a planned secondary procedure
3 Surgery should be reserved for high risk patients (solitary kidney, bilateral ureteral obstruction), infected patients, patients at risk of acute kidney injury or those with uncontrollable pain.
4 Primary definitive treatment of obstructing or symptomatic stones (both renal and ureteral) is preferred over temporizing drainage.
5 ESWL should be continued for ureteric stones but not for asymptomatic renal stones
6 Spinal Anaesthesia was recommended for distal Ureteric Stones under 10mm
7 For symptomatic renal stones, Flexible ureterorenoscopy (FURS) was recommended for 11‐20mm and PCNL/ECIRS for stones >20mm
8 Following Uncomplicated URS/FURS “Stent‐on‐a‐string” was recommended for stones 5‐20mm at all positions, with “stent and cystoscopic removal” for stones >20mm at all locations
9 Following Complicated URS/FURS stent and cystoscopic removal was recommended for all stone sizes and locations.
10 Following PCNL, some form of drainage was recommended for all complicated PCNLs and for uncomplicated PCNL for stones >11mm.
11 Surgical education should be maintained for trainees involved in the patients care.
12 Follow up imaging should continue for conservatively and actively treated ureteric colic and for patients with symptomatic renal stones
13 Imaging follow up can be deferred for asymptomatic prior stone formers including those with an established renal stone.
Conclusions: These recommendations can be applied currently during the ongoing Covid‐19 pandemic and be used as a framework for practice during a future catastrophic event that impacts the practice of renal and ureteric stone surgery.
Prospective non‐randomized comparison of transperitoneal transvesical versus extravesical laparoscopic supratrigonal vesico‐vaginal fistula repair: A single centre experience
V Singh, RJ Sinha, G Singh
Dept of urology, King George Medical University
Introduction & Objective: To compare the technique of transperitoneal transvesical versus extravesical laparoscopic repair of supratrigonal vesico‐vaginal fistula (VVF) and to assess the outcome of the two techniques.
Methods: Between January 2010 and September 2019, 22 patients with supratrigonal VVF underwent repair by laparoscopic technique. Single supratrigonal fistula was present in all these patients. Obstetric fistula was in present in 14 patients and gynaecologic fistula was present in 8. Mean fistula size was 1.5 cm (range 1 ‐ 3 cm). Transperitoneal transvesical laparoscopic repair (TTLR) was performed in 12 patients and transperitoneal extravesical laparoscopic repair (TELR) in 10 patients. The median follow‐up of these patients is 22 months in TTLR group and 24 months in TELR group.
Results: Mean operative time was 160.89 ± 12 minutes in TTLR versus 145.78 ± 0.8 minutes in TELR group (p < 0.001). Mean blood loss was 80.03 ± 0.7 ml in TTLR versus 60 ± 0.6 ml in TELR group (p < 0.001). Mean tramadol requirement on the first postoperative day was 200.06 ± 15 mg in TTLR versus 175.08 ± 12 mg in TELR group (p < 0.001). Mean hospital stay was 6.63 ± 0.74 days in TTLR versus 5.56 ± 0.67 in TELR group. None of the patients required open conversion. One patient in TTLR group had leakage on 12th day of fistula repair which was managed after 3 months by trans‐abdominal repair with omental flap interposition. The success rate of fistula repair was 91.6% in TTLR versus 100% in TELR group.
Conclusions: TTLR is associated with significantly long operative time, more blood loss, more analgesic requirement on first postoperative day in comparison to TELR. However the there was no difference between two groups with respect to overall success of fistula repair and length of hospital stay.
Identifying patients who will benefit from extended pelvic lymph‐node dissection during radical prostatectomy: a novel nomogram based on target biopsy only
E Checcucci, C Fiori, I Stura, D Amparore, S De Cillis, A Pecoraro, P Alessio, A Piana, F Piramide, G Volpi, P Verri, S Granato, B Carbonaro, D Zamengo, A De Pascale, D Gned, M Manfredi, G Migliaretti, F Porpiglia
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
Introduction & Objective: Nowadays, the role of synchronous pelvic extended lymphadenectomy (ePLND) during prostatectomy for prostate cancer still remains discussed. Various different tools aiming to identify patients who will benefit from ePLND are available such as mp‐MRI. However, also other instruments such as nomograms, can help the surgeon during the decision‐making process in case of positive target biopsy (TB) alone. The aim of our study was to develop a novel model based on mp‐MRI findings and TB alone in order to predict the risk of Lymph Node Invasion (LNI).
Methods: We retrospectively extracted from our prospectively maintained database patients with preoperative positive mp‐MRI and TB who underwent robotic prostatectomy with ePLND from April 2014 to March 2020. A logistic regression model was performed to evaluate the impact of pre‐ and intra‐operative factors on the risk of LNI. The results are shown in terms of Odds Ratio (OR) with a 95% Confidence Interval (95%CI). Model discrimination was assessed using an area under curve (AUC), the receiver operating characteristic (ROC) curve. A nomogram to predict the risk of LNI based on the logistic model was generated. The proposed model cut‐off was chosen maximizing both sensitivity and Youden score.
Results: Overall, 461 patients were included in our study; among them 52 (11.27%) had LNI. At logistic regression DRE, MRI findings (organ confined vs ECE, vs SVI), PI‐RADS, seminal vesicle invasion, PSA and worst GS at I and II target lesions were significant predictors of LNI. At multivariable model, DRE (OR 0.56; C.I.: 0.30‐1.05) and SVI (OR: 0.42; C.I.: 0.19‐0.93) were the most significant variables, followed by PSA (OR: 0.30; C.I.: 0.21‐0.73) and worst GS at I (OR: 0.37; C.I.: 0.17‐0.82) and II target lesion (OR: 0.33; C.I.: 0.14‐0.76). The AUC was 0.74 [0.67‐0.81] 95% CI. This predictive model was subsequently transformed into a visual nomogram, as shown in Figure 1. The cut‐off to discriminate LNI risk was set with a Youden index of 60 points, corresponding to a LIN risk of 7%.
Conclusions: The results of our study demonstrate that ePLND can be avoided in patients with positive TB only, being the risk of LNI below 7%, in order to spare approximately 59.1% of ePLNDs at the cost of missing only 4.7% positive LNs.
Clinical significance of markers of acute renal injury in predicting adverse outcomes in patients with coronavirus infection
V Pavlov, I Kabirov, A Alekseev, A Tarasenko, R Abdrakhimov, AO Papoyan
Bashkir State Medical University
Introduction & Objective: Coronavirus Disease 2019 (COVID‐19) is a newly emerging respiratory infection with frequent acute kidney injury (AKI). However, dynamic changes in kidney function and its relationship to predicting COVID‐19 outcomes are not sufficiently defined to apply preventive measures in patient management strategies. , especially in patients with concomitant diseases or undergoing surgery.
Methods: This single‐center retrospective cohort study analyzed the clinical characteristics, medical history, laboratory and instrumental studies and treatment data of 160 patients with COVID‐19, among whom at the time of hospitalization there were no clinical signs of AKI according to the criteria, there were 40 people who analyzed the data of the marker panel. AKI: urine NGAL, serum CisC, urine IL‐18, the sensitivity, specificity and threshold values of which were determined from the ROC analysis of 236 patients with initially diagnosed AKI during hospitalization. Renal function was assessed using the calculated GFR equation (CKD‐EPI 2009) based on serum creatinine levels.
Results: AKI at hospitalization was detected in 16 patients, Distribution by stages: 8.13%, 12.6% and 24.5% according to the KDIGO criteria. The ROC analysis determined the threshold value of the Marker Panel in patients with AKI at hospitalization, which was 156.87 ng / ml NGAL, 79.42 ± 13.69 for IL‐18, and 175.0 ± 16.63 for SCysC. The sensitivity of the method was 80% and the specificity was 73.7%. Based on the panel of markers, a subclinical form of AKI was identified, the outcomes of which were assessed within 3 months. In 14 patients of this group, a decrease in the GFR level was recorded within 30 days after hospitalization, associated with a lethal outcome. Mortality within 30 days from common causes was 8.3%
Conclusions: The increased risk of death from all causes was associated with increased levels of the AKI and Scr panel markers in the control group. Dynamic changes in the three markers of kidney function have been associated with varying degrees of severity and poor prognosis in COVID‐19 patients. The AKI marker panel has demonstrated high potential for predicting adverse outcomes in COVID‐19 patients for severity stratification and patient strategy.
The impact of the COVID‐19 pandemic on the presentation and management of renal colic patients
S Mukherjee, H Kadhim, I Sahibzada, D Feflea, L Goldsmith, C Popanes, A Raza
London North West University Healthcare NHS Trust
Introduction & Objective: Renal colic is one of the common urological emergencies. As the COVID‐19 pandemic significantly impacted the UK healthcare system, there were some changes in the presentation and management of renal colic patients during the pandemic compared to the pre‐pandemic period. We compared the presentation and management of renal colic patients between the pandemic and pre‐pandemic period.
Methods: Retrospective data analysis from electronic patient records was conducted for all adult patients presenting to our A&E department with a radiological diagnosis of renal colic between March‐May 2020 (the first peak of the pandemic) comparing similar data collected for the period March‐May 2019.
Results: During the pandemic, the total number of patients attending A&E with a clinical diagnosis of renal colic and CT scan confirming stone in ureter/PUJ reduced by 17% compared to the same period in 2019 (170 vs 204).
Relatively younger patients attended A&E during the pandemic compared to the pre‐pandemic period (median age in years [IQR] ‐ 43.5 [34, 52] vs 39 [31, 50], p = 0.016) and there were significantly more patients with PUJ stones in 2019 than in 2020 (18 vs 1, p = 0.0003). However, there was no difference in other patient characteristics or stone characteristics.
Also, there was no difference in the proportion of patients managed conservatively between the pandemic and pre‐pandemic period (79% vs 78%, p = 0.83). However, between 2020 and 2019, there was a significant reduction in hospitalization (18 (10.6%) vs 49 (24%), p = 0.0008), JJ stent insertion (6 (3.5%) vs 24 (11.7%), p = 0.004) and ureteroscopy as initial definitive treatment (4 (2.4%) vs 29 (14.2%), p = 0.0001) along with a significant increase in primary ESWL (25 (14.7%) vs 9 (4.4%), p = 0.0006).
Conclusions: The COVID‐19 pandemic resulted in a considerable drop in A&E attendance of renal colic patients. The reduction was more noticeable in older patients compared to the younger patients. In addition, there was change in standard management strategy from stent insertion followed by a second admission for ureteroscopy towards urgent primary ESWL.
“Pseudo‐renal colic” – a neglected common entity with significant impact on health service providers' resources during both pre‐ and peri ‐ COVID‐19 pandemic
S Mukherjee
London North West University Healthcare NHS Trust
Introduction & Objective: Renal colic is a common cause of A&E presentation. A significant proportion of patients presenting with renal colic go onto have entirely normal or pathology free CT scans (“pseudo‐renal colic”). Many patients therefore undergo unnecessary radiation exposure from imaging as well as require significant health service providers' resources. We compared the number of renal colic presentations both pre and peri pandemic period.
Methods: Retrospective data collection was conducted on all CT KUB scans performed in A&E following a clinical diagnosis of renal colic. Data collection, analysis and comparison were performed over two periods ‐ pandemic period of March‐May 2020 (first peak of COVID‐19) and pre‐pandemic period of March‐May 2019.
Results: In 2019 (pre‐pandemic period), 609 patients attending A&E with a clinical diagnosis of renal colic underwent low dose CT KUB. 204 (34%) patients had an index stone in the ureter/PUJ, 141 (23%) had non‐stone related pathology (urological and non‐urological) and 264 (43%) had pseudo‐renal colic.
In 2020 (pandemic period), attendances to A&E with a clinical diagnosis of renal colic reduced to 384. During the pandemic, there was significant increase in the proportion of patients with positive CT scans showing a stone in the ureter/PUJ (44% (170/384) vs 34%, p = 0.0006) and a drop in pseudo‐renal colic patients (34% (130/384) vs 43%, p = 0.0032) compared to the pre‐pandemic period. The proportion of patients with non‐stone related pathology (urological and non‐urological) remained relatively stable at 22%.
Conclusions: Pseudo‐renal colic comprised around 40% of renal colic patients during both the pandemic and non‐pandemic period leading to unnecessary radiation exposure and wastage of precious resources. Patients with pseudo‐renal colic possibly experience less pain than genuine ureteric colic and a significant proportion stayed at home during the pandemic. Clinical assessment with the use of the validated Stone Score as well as markers such as WC, CRP and renal function before ordering a CT KUB in suspected renal colic patients may help reduce the number of unnecessary CT scans in the future as well as minimize the drain on health service providers' resources during and after the pandemic.
Assessment of Emergency Department Urolithiasis Presentations During the COVID‐19 Pandemic
DK Agarwal, T Large, M Assmus, ME Rivera
Indiana University Department of Urology
Introduction & Objective: During the unprecedented COVID‐19 pandemic, there have been major changes in healthcare delivery, patients seeking care and access to care. We sought to determine if there were differences in Emergency Department (ED) presentations for urolithiasis and their triage from the ED.
Methods: We assessed the all ED presentations and those for urolithiasis (defined as codes N20.0 and N20.1) from January 2019 through December 2020 at four hospitals (one primary, two secondary and one tertiary/quaternary care) in a single hospital network in the Indianapolis metro area. We also assessed the patient's disposition, either discharged from the ED or admitted to the hospital.
Results: There were 109,656 total ED presentations in 2019 and 1369 ED presentations for urolithiasis (12.5%). In 2020, there were 94143 total ED presentations with 1212 for urolithiasis (12.9%). There was no significant difference between total stone presentation between the 2019 and 2020. In 2020, there were significant increases in the rate of stone presentations in May (1.39% vs 0.010%, p = 0.02) and August (1.64% vs 1.13%, p = 0.0035). There was a significant decrease in the rate of stone presentation in December 2020 compared to December 2019 (0.91% vs 1.34%, p = 0.0096). Figure 1 demonstrates the monthly ED Visits for urolithiasis compared between 2019 and 2020, with the monthly COVID‐19 cases in Indiana. There was a decline in total visits 71.5% of visits were dismissed from the ED in 2019 compared to 70.2% in 2020. There were no differences in the rates of ED discharge or hospital admission on a monthly basis between 2019 and 2020.
Conclusions: Within a hospital system in the Indianapolis metropolitan area, there does not appear to be a change in ED stone presentations or disposition patterns between 2019 and 2020 despite the COVID‐19 pandemic.
Are patients' fears of catching COVID‐19 during an emergency hospital admission with an acute urological problem justified? – A UK epicentre experience
O Gbolahan, V Bonatsos, A Raza
London North West University Healthcare NHS Trust
Introduction & Objective: During the first wave of COVID‐19 patients' anxieties around contracting the virus during an emergency hospital admission were high. Our aim was to establish the risk of catching COVID‐19 as a urology emergency inpatient in our Trust and to assess patients fears and attitudes towards seeking medical help for their acute urological problems.
Methods: A single centre retrospective audit of all urological emergency admissions was made over a 10‐week period (mid‐ March – end of May) in 2019 and compared to (mid‐March – end of May) 2020 during the COVID‐19 pandemic. The number of patients who developed new COVID‐19 symptoms whilst an in‐ patient or had positive swabs within 28 days of discharge was obtained. We performed a post discharge telephone survey of patients based on a COVID‐19 fear questionnaire (FC19‐HVQ) adapted from the validated Fear of COVID‐19 scale.
Results: Compared to 2019 (n = 187), 2020 (n = 122) there was a 35% reduction in the number of patients presenting acutely to our department. 43 of the 122 (35%) patients were swabbed on admission due to possible symptoms of COVID‐19. One patient was found to be COVID‐19 positive. 5 patients had further swabs during their admission; one patient who was negative on admission became positive whilst an inpatient. Accordingly, the overall in‐hospital infection rate with COVID‐19 was 0.82% (1 patient) during or within 28 days of discharge. There was no mortality (0%) related to COVID ‐19.
The majority of patients were afraid to visit A&E or the hospital during the COVID‐19 pandemic crisis. Fewer patients were afraid to visit their local Family Doctor (GP). 28% (n = 14) of responders ignored their symptoms during the pandemic.
Patients were reluctant to seek medical input during COVID‐19 by trying to treat themselves at home with 64% (n = 32) of them stating that they attempted to do so. There was also a degree of intentional delay to visit A&E and the hospital with 56% (n = 28) of our patients admitting to having delayed their attendance.
Conclusions: The risk of contracting COVID 19 whilst a urology in patient in a COVID‐ 19 epicentre was very low (0.82%) with no COVID‐19 related mortality. Our data supports the message that patients with urological emergencies should be educated and encouraged to attend hospital, rather than staying at home, during future surges in the current pandemic. This is to prevent further non COVID‐19 related harm from delayed presentations, undiagnosed pathologies and self‐ treatment approaches.
The effect of the COVID‐19 pandemic on management of urological emergencies including risk of contracting COVID‐19 – a UK epicentre experience
O Gbolahan, V Bonatsos, A Raza
London North West University Healthcare NHS Trust
Introduction & Objective: During the first wave of COVID‐19 we saw a reduction in urgent urological admissions. Concurrently, we had to adapt and change our standard management of urological emergency admissions. We wished to evaluate the impact of COVID‐19 on urological emergencies in a UK COVID‐19 epicentre.
Methods: Retrospective audit of all urological emergencies over a 10‐week period (mid‐March – end of May) in 2019 was compared to the same period during COVID‐19.
Results: From 2019 to 2020 we saw a reduction of 35% (187 [2019] and 122 [2020]) in urological emergency admissions. The average inpatient stay was 1.76 days (range 0‐24 days) in 2020 from 2.65 days (range 0‐38 days) in 2019. The largest reduction in presentation was seen in renal colic 43% (58 [2019] and 33 [2020]) followed by visible haematuria 39% (37 [2019] and 23 [2020]). There was a decrease in surgical management of urological emergencies during COVID‐19. Scrotal exploration for testicular pain went from 57% (21 of 37) 2019 to 39% (12 of 31) during COVID‐19. Stenting for colic and confirmed ureteric stones decreased from (20 of 25) 80% in 2019 to 11% (2 of 18) in 2020. “Hot” ESWL rates for ureteric stones increased from no patients [2019] to 61% (11 of 18) in 2020. In 2019, 12% (6 of 49) of emergency procedures were performed by Consultants however this increased to 48% (11 of 23) in 2020 due to redeployment of urological registrars. The overall in‐hospital COVID‐19 infection rate was only 0.82% during or within 28 days of discharge with no COVID‐19 related mortality (0%).
Conclusions: Inpatient infection rate from COVID‐19 was very low and there was no related mortality therefore patients should not fear hospital attendance or admission. Longer term follow‐up of patients managed conservatively rather than surgically is necessary to ensure no long‐term harm has been caused by a change in standard surgical management of urological emergencies.
Quality of Life of Urolithiasis Patients During the COVID‐19 Pandemic: A Wisconsin Stone Quality of Life (WISQOL) Research Consortium Cross‐Sectional Study
VK Wong, BH Chew, KL Penniston, VG Bird, NM Streeper, SY Nakada, N Bhojani
University of Montreal Hospital Center (CHUM)
Introduction & Objective: The COVID‐19 pandemic is an unprecedented global event that has caused significant fear and anxiety across all populations. To date, there have been no studies on how major health crises have affected the stone‐related quality‐of‐life (QOL) of patients with urolithiasis. In this study, we investigated whether the fear of COVID‐19 affects the QOL of patients with kidney stones during the COVID‐19 pandemic using the Fear of COVID‐19 Scale (FCV‐19S) and the Wisconsin Stone Quality of Life (WISQOL) questionnaires.
Methods: Patient‐reported FCV‐19S and WISQOL data for this multi‐institutional prospective cross‐sectional study were obtained from five sites within the North American Stone Quality of Life Research Consortium. Data collection occurred between the months of April‐October 2020 during the COVID‐19 pandemic where many procedures (radiological or surgical) and visits were either delayed or cancelled. The scores generated from patient‐reported responses were correlated by the Pearson Product‐Moment Correlation. The questionnaire scores were then further sub‐analyzed dependent on categorical responses related to procedural delays or care and were analyzed via the Student's T‐test. A single factor analysis of variance (ANOVA) was performed to analyze varying QOL scores across the FCV‐19S quartiles.
Results: 400 respondents participated in this study. Within the cohort, mean age was 57.0 ± 15.0 years. Overall mean total standardized FCV‐19S and WISQOL scores (both transformed to min‐max 0‐100) were 34.3 and 70.3 respectively. Correlation analysis between the two questionnaires demonstrated a significant inverse correlation (r = ‐0.265, p < 0.05) suggesting that greater fear for COVID‐19 may result in a lower stone‐related quality‐of‐life. A significant difference in fear and QOL scores was observed between the sexes, with women having more COVID‐19 fear (35.8 vs. 28.6, p < 0.01) and lower stone‐related QOL (64.2 vs. 75.2, p < 0.01) compared to men. Quartile ANOVA analysis revealed significant mean difference in WISQOL scores as well as within each domain of the WISQOL questionnaire across all FCV‐19S score quartiles (p < 0.05).
Conclusions: From our study, there appears to be a relationship between the between the fear of COVID‐19 and stone‐related QOL of patients with urolithiasis. Using two validated questionnaires (The Fear of COVID‐19 Scale and the Wisconsin Stone Quality of Life), we found that greater fear for COVID‐19 was associated lower stone‐related QOL.
COVID‐19 Pandemic Results in Decreased Non‐Urgent Urologic‐Related Presentations to the ED
A Balen, J Molino, C Tucci, G Pareek, DW Sobel
Warren Alpert Medical School of Brown University
Introduction & Objective: Urologic‐related visits to the emergency department (ED) are variable in their acuity, ranging from non‐emergent to life‐threatening. We sought to evaluate trends in urologic presentations to the ED during the COVID‐19 pandemic at a tertiary academic institution in the United States to determine the differences in frequency between urgent and non‐urgent visits and further elucidate delayed access to urologic care.
Methods: A retrospective analysis was performed comparing the frequency and type of urologic‐related ED visits at our institution in January‐April 2019 to those in January‐April 2020 during the initial pandemic phase. 1,838 urologic presentations between the two‐time intervals were organized by diagnosis and divided by acuity into urgent and non‐urgent categories. Interrupted time series regression models were used to determine how urologic‐related ED visits changed due to the COVID‐19 pandemic.
Results: The total number of urologic related ED visits by type for each time interval is demonstrated in Table 1. There was a statistically significant drop in total urologic‐related ED visits after the COVID‐19 pandemic began, with a drop in total visits of approximately 76 per month (p = 0.002). There was no difference in the number of urgent ED visits due to the COVID‐19 pandemic (p = 0.13). However, there was a statistically significant decrease in non‐urgent ED visits, with a decrease of 68 visits per month (p = 0.002). When examining the individual visit types, there were no differences in visit volume except for hematuria and nephrolithiasis/ureterolithiasis visits. There was a statistically significant reduction in hematuria‐related ED visits, with a reduction in visits of approximately 11 per month (p = 0.03). Similarly, there was a statistically significant decline in nephrolithiasis/ureterolithiasis‐related ED visits, with a decline of approximately 28 visits per month (p = 0.04).
Conclusions: The COVID‐19 pandemic coincided with a significant decrease in the number of non‐urgent urologic presentations to our institution's ED. Specifically, there was a significant decrease in the number of patients presenting with hematuria and nephrolithiasis‐related issues. There was no significant decrease in the number of urgent urologic consults. Follow up study is indicated to investigate the effect of delayed evaluation for these non‐urgent urologic diagnoses.
Transforming the Urology clinic to a procedure‐oriented center improves the quality of urological care and patient experience
F Hamouche, R Unno, J Ahn, D Bayne, H Yang, M Stoller, E Finlayson, s smith, R Pruthi, J Smith, T Chi
UCSF
Introduction & Objective: The global pandemic of COVID 19 necessitated limitations for in‐person visits to stop the spread of the virus. At our institution, we sought to maintain patient access while delivering safe socially distanced care. We hypothesized that transitioning the clinics into a procedure‐oriented center would create a safer, more efficient model for patient care delivery.
Methods: Transitioning the clinic consisted of adopting Telehealth visits for the majority of patient's consultations while augmenting the use of physical space in the clinic to facilitate urological procedures. Multiple productivity, financial and patients experience metrics were collected between two periods of time defined as P1‐ Pre Covid (Feb‐Jun 2019) and P2 Post‐Covid (Feb‐Jun 2020) and compared. Statistical analysis was performed using the Chi‐Square test and the Z‐test for two independent samples.
Results: The percentage of performed procedures amongst all clinical visits increased in P2 (45% vs 29% p < 0.001). There was an increase in the percentage of new patients scheduled within 5‐ and 14‐days during P2 (71 % vs 46%, p < 0.001, and 55 % vs 41%, p < 0.001) respectively. Total charges and RVUs decreased in P2 but the overall payments were higher compared to P1. This increase in revenue was due to a higher income generated by procedures. CGCAHPS and Press Ganey scores improved in P2 across all domains representing patient experience. This improvement was statistically significant for “Recommend this provider office” (90% vs 85.7% p = 0.01), “Access overall” (56% vs 49% p = 0.02), and “Moving through your visit overall” (59% vs 51% p = 0.007).
Conclusions: Our data suggests that transitioning the urology clinics into a space that is mainly dedicated to outpatient procedures can represent a model that improves the patient's access to care and clinical experience, as well as strategically bolstering financial revenues. This is a more efficient care model that could replace current practice and represent the future of outpatient Urology.
Quality Improvement for Quality of Life: Low‐Dose Buprenorphine Decreased Opioid Utilization Protocol in Robot‐Assisted Radical Cystectomy
LJ Smith, TC Peak, HE Moreland, DB Rukstalis
University of South Carolina School of Medicine
Introduction & Objective: Opioid‐naïve individuals often first encounter narcotics during major surgery such as robot‐assisted radical cystectomy (RARC) for the treatment of muscle‐invasive bladder cancer. Pain management following RARC with full‐agonist opioids has been the cornerstone of analgesia despite associated toxicity and risk for dependence. New literature describes non‐opioid enhanced recovery pathways, yet none define the merits of decreased opioid utilization (DOU) using partial‐agonist opioid low‐dose buprenorphine (LDB; LDB‐DOU protocol). With recent reevaluation of prescribing requirements by the FDA, LDB may become more accessible. We implemented a quality improvement initiative using an LDB‐DOU protocol to assess the feasibility and outcomes of minimized perioperative opioid burden.
Methods: The LDB‐DOU protocol includes standardized recovery pathways, a multimodal analgesia schedule, and shared pain management expectations. Analgesic management was recorded and converted to morphine milligram equivalent (MME) for comparison. Relevant preoperative, operative, and postoperative recovery details were documented to assess clinical milestones for recovery, readmission rates, and pain control. Prior opioid use was identified using the prescription drug monitoring program.
Results: Twenty medically complex patients (CCI 6, ASA 3) followed the LDB‐DOU protocol after admission for palliative or curative RARC with ileal conduit urinary diversion. The median operative time was 342 minutes, blood loss was 300mL, and hospital stay was three days. Respectively, median total dosage of LDB and MME were 0.375mg and 20/day, allowing for advancement to low‐residue diet on postoperative day (POD) two. One patient experienced transient ileus (POD 2) and two faced 30‐day complications (Clavien 2, 3). None required outpatient narcotic management.
Conclusions: The LDB‐DOU protocol allows for perioperative narcotic mitigation and enhanced quality of life. Improvements in clinical milestones of recovery included adequate analgesia, short hospital stays, fast diet advancement, and low incidence of postoperative ileus and 30‐day adverse events. Compared to morphine, LDB is 20‐50 times more potent for pain modulation but offers nominal euphoric reward due to its distinctive receptor‐binding. It delivers a profile of enhanced safety with optimal antinociception. Though further studies are needed, the use of an LDB‐DOU protocol is a feasible alternative to both standard practice and the newer non‐opioid approaches.
Theatre utilisation in the era of COVID‐19
A Brodie, A Pai
Northampton General Hospital
Introduction & Objective: The COVID‐19 pandemic has had wide reaching consequences on all aspects of health care. As the number of coronavirus cases has fluctuated, access to operating theatres has been similarly affected. However, when theatres are available and running, the impact of the pandemic on theatre utilisation needs to be quantified. There is a paucity of data on this topic. The aim of this study is to assess theatre utilisation prior to and during the pandemic.
Methods: A retrospective review of elective urology theatre utilisation during 2020 at a district general hospital was carried out to assess the impact of the COVID‐19 pandemic on theatre utilisation. Data was also collected on the number of procedures and cancellations.
Results: As expected, there were fewer elective procedures during the pandemic compared to pre‐pandemic. The utilisation of those theatres that were open decreased during the pandemic compared to pre‐pandemic levels. However, the efficiency of theatres improved as the pandemic progressed. The number of cancellations per month increased during the pandemic. The increased cancellations during the pandemic were commonly due to patients cancelling, refusing surgery or not attending their scheduled operations. Despite the presence of green elective theatres, where patients are swabbed for COVID prior to entry, the most common reason given was fear of contracting COVID‐19 in hospital.
Conclusions: It is evident that due to the additional complexities of operating during a pandemic that theatre utilisation is 14.4% lower than pre‐pandemic levels. Although this is multifactorial, during the pandemic, the main reason was due to patients cancelling. Measures must be in place to make patients feel comfortable to enter hospitals for elective procedures to reduce the number of cancellations. This will help improve theatre utilisation.
The impact of COVID‐19 on surgical care delivery for patients with urinary stones
J DiBianco, S Daignault‐Newton, J Ludlow, J Phelps, E Ratchford, M Cotant, KR Ghani, CA Dauw, f Urological Surgery Improvement Collaborative
Department of Urology, University of Michigan
Introduction & Objective: During the COVID‐19 pandemic, limits on elective surgical care were instituted by hospitals to preserve resources. Additionally, patients' desire to limit health care contact may impact surgical decision making. We aimed to understand how institutional pressures and patient preference affected the delivery, choice and outcome of ambulatory surgical care for urinary stone disease during the COVID‐19 pandemic.
Methods: Reducing Operative Complications from Kidney Stones (ROCKS) is a quality improvement initiative from the Michigan Urological Surgery Improvement Collaborative (MUSIC) that maintains a prospective clinical registry of ureteroscopy (URS) and shockwave lithotripsy (SWL) cases. Using this registry, we categorized all cases by time frame, defining July 1st ‐ December 31st 2019 as preCOVID (PC), March 16th ‐ June 15th 2020 as duringCOVID (DC) and June 16th ‐ September 15th 2020 as afterCOVID (AC). Patients in each cohort were characterized across a range of sociodemographic and clinical factors. We assessed changes in procedure choice (URS vs SWL), procedure acuity (elective vs emergent), and outcomes (ED visit and hospitalization within 30 days of surgery).
Results: 6375 cases were identified, 4513 URS and 1862 SWL. PC consisted of 3310 cases (2238 URS and 1072 SWL), DC consisted of 1141 cases (888 URS and 253 SWL) and AC consisted of 1924 cases (1387 URS and 537 SWL). A higher proportion of URS cases were performed DC compared to PC and AC (77.8% vs 67.6% vs 72.1%, p < 0.001, respectively). A higher percentage of emergent cases in DC compared to PC and AC (21.8% vs 13.7% vs 15.3%, p < 0.001, respectively). Significantly more cases in DC compared to PC and AC were prestented, had positive UA/urine culture, ureteral stones, had hydronephrosis, were stented and had longer stent dwell time. ED visits and unplanned hospitalizations were not significantly different.
Conclusions: The COVID‐19 pandemic resulted in a lower overall stone treatment rates and higher proportions of URS compared to SWL. Significantly more emergent cases for ureteral stones with positive UA/urine cultures and evidence of obstruction were performed duringCOVID with higher stent placement rates and longer stent dwell times. These data pointing towards preference for higher intensity or acuity cases without differences in unplanned healthcare encounters.
Health Related Quality of Life for Stone Patients During COVID‐19 Pandemic is Significantly Lower than Pre‐Pandemic
MA Knoedler, S Li, SL Best, SP Hedican, KL Penniston, SY Nakada
University of Wisconsin, Department of Urology
Introduction & Objective: The coronavirus disease 2019 (COVID‐19) pandemic has altered many aspects of life including quality of life and the way patients interact with the health care system. We assessed patients with stone disease seen in the urology clinic for health‐related quality of life (HRQOL) prior to and during COVID‐19 utilizing the Wisconsin Stone Quality of Life questionnaire (WISQOL).
Methods: The WISQOL is used routinely in our clinical practice to assess patients' HRQOL at every encounter. Patients seen in clinic with stone disease at a single institution were invited to complete a WISQOL and provide information as to their stone and stone‐related symptom statuses. Responses from patients seen from January 1, 2019 to December 31, 2019 (pre COVID‐19) were compared to patients seen from June 9, 2020 to December 31, 2020 (post COVID‐19). Patients were case matched based on symptomatic status (yes/no/not sure) and gender. WISQOL total and domain scores were standardized to scales of 0‐100. Symptomatic patients, asymptomatic patients and patients who were not sure if they were symptomatic from stone disease were analyzed separately using MANOVA.
Results: A total of 90 patients were included in the analysis (45 pre COVID‐19 and 45 post COVID‐19). In the post COVID‐19 cohort, 14 patients were symptomatic, 27 were asymptomatic and 4 were not sure if they were symptomatic. Symptomatic patients seen post COVID‐19 had statistically lower HRQOL compared to patients pre COVID‐19 (44.8 ± 18.6 vs 62.6 ± 29.2, p < 0.05). HRQOL did not differ significantly pre and post COVID for asymptomatic patients (86.9 ± 21.6 vs 90.4 ± 9.9, p = 0.37) or patients who were not sure if they were symptomatic (98.2 ± 1.3 vs 57.6 ± 42.3, p = 0.308). For patients with symptoms, HRQOL was particularly lower with respect to social functioning and vitality (Table).
Conclusions: Patients seen in urology clinic for stone disease during the COVID‐19 pandemic had significantly lower HRQOL then those seen prior to the onset of COVID‐19.
COVID‐19 pandemic and its effect on supra‐regional extracorporeal shock wave lithotripsy (ESWL) service
M Kay, J Lau, F Jarral, S Rajpal, N Boucher, J Patterson
Royal Hallamshire Hospital
Introduction & Objective: The COVID‐19 pandemic brought significant challenges to all healthcare systems around the world. We studied its impact on our supra‐regional ESWL service.
Methods: Patients who received ESWL using our onsite lithotripter (Storz Modulith SLX‐F2) during the initial National Lockdown (NL) period were compared with those treated over a similar time period in 2019. Patients with renal calculi were excluded for direct comparison as only a small number of patients with renal calculi were treated during NL. As the supra‐regional centre, we continued to provide acute treatment during NL albeit with restricted access due to staff redeployment, and within safety restrictions, and continued to receive patients from other network centres.
Results: 25 patients with ureteric calculi treated in 2019 were compared with 23 patients treated during NL. The mean ages were 56.6 VS 50.0 (2019 VS NL). The mean time to treat were 20.9 VS 19.4 days (2019 VS NL). Two patients' 2nd treatment got delayed during NL. Treatment outcomes are outlined in table 1. The mean residual stone sizes were 4.9mm VS 5.7mm (2019 VS NL). In 2019, complication rate was 16.0% with the commonest being pain (75.0%) when compared to 21.7% during NL (80% pain). Steinstrasse were not seen in either group. One patient treated during NL sustained a moderate peri‐renal haematoma managed conservatively. Treatment parameters such as number of shocks delivered and screening time were equivalent between groups.
Conclusions: COVID‐19 led to pressures on health services and also patients changed their patterns of presentation. Restricted access to the operating theatre made use of non‐invasive treatments an essential part of patient management during the lockdown period. We show equivalent outcomes to normal practicedespite treating larger and potentially more challenging stones, with few complications and while minimising COVID‐19‐related risks to the patient.
#AUAMatch: The Impact of COVID‐19 on Social Media Use in the Urology Residency Match
P Ho, EJ Margolin, E Sebesta, A Small, GM Badalato
Columbia University Vagelos College of Physicians and Surgeons
Introduction & Objective: Social Media (SoMe) use has rapidly expanded within the urological community over the last decade and has become an important tool in the residency application process. SoMe was particularly relevant to medical students during the 2020‐2021 application cycle, as the COVID‐19 pandemic limited in‐person interactions. In this study, we examined changes in SoMe use among urology residency applicants before and after the pandemic.
Methods: We distributed surveys to all individuals who applied to our residency program for application cycles ending in 2018, 2019, and 2021. The surveys included questions about applicants' SoMe use and their perceptions of programs' SoMe use. We evaluated the ways applicants used SoMe during the application process, both before (2018/2019) and after (2021) the COVID‐19 pandemic. The primary outcome was SoMe use for professional purposes.
Results: We received survey responses from 33% (162/496) and 29% (84/294) of applicants from the 2018/2019 and 2021 cohorts, respectively. There was a significant increase in professional SoMe use in the 2021 cohort (80%) compared with the 2018/2019 cohort (44%) (p < 0.001). When controlling for age and gender, applicants in 2021 were more likely to use SoMe for professional purposes (odds ratio 4.68, p < 0.001). Applicants more frequently used Twitter (p < 0.001) and LinkedIn (p = 0.036) and less frequently used Doximity (p < 0.001) in 2021 compared to 2018/2019. In 2021 compared to 2018/2019, a larger proportion of applicants used SoMe to connect directly with residents (69% vs 34%, p < 0.001) and with faculty members (65% vs 15%, p < 0.001). Applicants in 2021 compared to 2018/2019 more often found SoMe to be useful for making decisions about applying to (33% vs 10%), interviewing at (26% vs 7%), and ranking programs (20% vs 9%) (all p < 0.05). Twitter was the most common platform for applicants to access program information, increasing from 38% to 71%. Of the 2021 survey respondents who reported using SoMe, 74% (59/80) reported that application changes due to the pandemic directly caused them to increase their SoMe use. Overall, 31% of applicants felt that SoMe engagement had a positive impact on the application process, and 61% would like to see similar or more interaction between applicants and programs in future cycles.
Conclusions: The COVID‐19 pandemic ushered in a period of unprecedented SoMe usage among urology applicants, who used it to learn about and connect with residency programs in new ways. The use of SoMe by residency programs has become an important component of trainee recruitment and is likely to continue in the future.
Moderated Poster Session 02: Epidemiology
Development of the Short Form of the Wisconsin Stone Quality of Life (WISQOL) Questionnaire for Assessing the Health‐Related Quality of Life of Patients with Urolithiasis
KL Penniston, S Li, SY Nakada
University of Wisconsin School of Medicine and Public Health
Introduction & Objective: The 28‐item Wisconsin Stone Quality of Life questionnaire (WISQOL) is a specific, self‐administered, health‐related quality of life (HRQOL) instrument for assessing the impact of urolithiasis. Prior reports confirm the WISQOL's reliability, validity, and responsiveness. Its use has helped to identify specific HRQOL decrements in patients with urolithiasis, including after or between stone events. To address needs of large clinical studies and long‐term monitoring, for which efficiency competes with precision, we developed a short‐form (SF) version of the WISQOL.
Methods: We use the WISQOL in our clinical stone practice. Patients are invited to complete it at every appointment. Data for this study were from patients (n = 704) who completed the WISQOL between June 2017 and February 2020 at a Urology Clinic appointment with either the primary stone surgeon or a nurse practitioner. Of these, 196 had >1 missing item and were excluded. Remaining patients were 53% female, 54 ± 15 y, and mixed for stone history (min‐max, 1 to >50 lifetime stone events). Nearly half (49%) had current stones; 30% were experiencing stone‐related symptoms or had done so within the past 4 weeks. We calculated WISQOL total and domain (n = 40 scores. We used item analysis and factor analysis to evaluate all 28 WISQOL items.
Results: Items with item‐total correlation coefficients <0.84 were eliminated (n = 20). Of the 8 remaining items, linear regression analysis and cross loading identified 6 that best predicted total WISQOL scores (P < 0.001, figure), representing 2 of the 4 WISQOL domains (D1, social; and D2, emotional). Using these items, 80% of patients placed in the same quantile for total score as with the original WISQOL. Item‐score correlation coefficients (original vs WISQOL‐SF) ranged from 0.84‐0.93; correlation with total score was 0.95 (P < 0.001 for all comparisons). The WISQOL‐SF Cronbach alpha coefficient was 0.94 compared to 0.97 for the original WISQOL. Of patients misplaced for quantile by the WISQOL‐SF, 32 and 30% were patients with stones and/or stone symptoms at the time; they tended to score higher for HRQOL with the WISQOL‐SF.
Conclusions: We produced the WISQOL‐SF, a 6‐item version of the WISQOL suitable for efficient assessments. While more testing is needed, the WISQOL‐SF appears best suited for long‐term follow up of HRQOL in stones.
Where do you practice? And its effect on equipment, technique, and more
T Aro, A Smith, A Rai, D Mikhail, D Hoenig, AD Smith, Z Okeke
The Smith Institute for Urology
Introduction & Objective: Endourology is constantly developing with new techniques, modalities, surgical instruments, and perhaps no less important, the surgeon experience and expertise. We looked into differences in basic endourology practice patterns in the united states vs the rest of the world.
Methods: An online questionnaire comprised of 6 categorizing questions, and 31 multiple choice questions looking into common endourologic scenarios and practice pattern was sent using the endourology society contact list.
Results: 279 responses were sorted into 207 from outside, and 72 from inside the USA. In a ureteroscopy setting, responses outside the USA use an access sheath almost always in 64%, compared to 46% in the USA. In PCNL, responses from outside the USA don't have a preferable calyx in 53% and in 30% prefer the lower calyx, compared to 61% and 17% respectively inside the USA. Inside the USA, 83% of responses would use balloon dilators compared to only 30% outside, and 78% prefer the prone position, compared to 52% outside the USA. Lastly, in a prone position setting, 54% of responses inside the USA use vertical placement of the bolsters compared to 31% in the outside the USA group.
Conclusions: Although there are no guidelines or specific recommendation on some of the basic practice patterns, it appears there are many differences between the USA endourologists and the rest of the world. USA practitioners use access sheath less, more likely to choose an entry calyx for PCNL based on case and not a personal preference, use balloon dilators much more, and prefer the prone position. Future, larger scale research might be needed to explain the basis for such differences.
Withdrawn
Racial Disparity in Prostate Cancer Diagnosis: A Comparison of Prostate Biopsy Results in African American and White Men using an MRI based Biopsy Strategy
A Kasraeian, M Alcantara, K Mola Alcantara, J Cesaretti, A Kasraeian
Kasraeian Urology
Introduction & Objective: African American (AA) men in the United States have an increased burden of morbidity and mortality from prostate cancer (PCa). The roles of factors related to both racial disparities and intrinsic biological traits remain to be determined. We quarried our prospective database of standard and MRI fusion biopsies (tMRI/US FPB) to determine if any pre‐biopsy characteristics predicted adverse tumor pathology.
Methods: Between January 2017 and December 2020, 560 men underwent prostate biopsy (PBx) using an MRI based algorithm. Men with negative MRI underwent standard PBx (n = 293), while those with lesion on mpMRI underwent tMRI/US FPB (n = 267). All patients underwent mpMRI of the prostate, interpreted by a single radiologist using the PIRADS scoring system. 3D rendering of the regions of interest was performed by the radiologist prior to tMRI/US FPB performed by a single urologist using the Invivo UroNav Fusion Biopsy System. A standard 14 core PBx was performed at the same time in all tMRI/US FPB cases. Prospective data was collected and analyzed.
Results: Of 560 men who underwent standard and tMRI/US FP with 14Bx (tMRI/US FP‐14Bx), 422 presented with rise in PSA and 182 had a suspicious digital rectal exam. 256/418 (61%) of White men and 62/92 (67%) of AA men were found to have PCa (p = 0.29). 153/418 (37%) of White men and 46/92 (50%) of AA men had a Gleason score of 7‐10 (p = 0.019). Age, DRE status, PIRADS score and the incidence of Gleason 6 PCa were not found to be significantly different by race. 112/415 (27%) of White men and 10/91 (11%) of AA men had a PSA upon presentation of 0‐3.9 ng/ml (p = 0.001). The PSA levels of 4.0‐9.9 ng/ml and PSA >10 ng/ml at presentation were not significantly different. Of the 50/560 men who identify as not White and not Black no significant difference was found for any tested factor but interestingly 12/50 (24%) presented with a PSA between 0‐3.9 ng/ml (p = 0.053 NS) which was very close to the effect seen relative to White men.
Conclusions: In this dataset, it appears that AA men present with a higher PSA than White men. It is likely that this is related to disparities in access to care rather than biological intrinsic factors. We did observe a higher incidence of Gleason 7‐10 which one would expect in a cohort of patients who presented for biopsy in the community with a significantly higher PSA presentation. Continuing education of primary care providers regarding the importance of PSA testing in the AA community should be emphasized by both the urological and primary care professional medical societies.
Economic Burden of Complicated Ureteral Stent Removal in Patients with Kidney Stone in the United States
KR Ghani, S Rojanasarot, B Cutone, S Bhattacharya, AE Krambeck
Northwestern University
Introduction & Objective: Cystoscopy‐based stent removal (CBSR) is a common procedure following ureteroscopy with stent placement. Although the American Urological Association (AUA) designated complicated stent removal CPT® code 52315 for encrusted stent removal, no previous research has examined if complicated stent removal is associated with increased healthcare costs to the US healthcare system. This study investigated the economic burden of complicated versus simple stent removal among commercially insured US patients.
Methods: A retrospective cohort study was conducted to identify patients who had ureteroscopy with stent placement for stone disease between January 2014 and June 2018 from IBM MarketScan Commercial database, a nationally representative data sample of the US population with employer‐sponsored health insurance. We included patients who were ≥18 years old and had CBSR within 6 months post‐index ureteroscopy. Patients were categorized as those with simple or complicated CBSR using CPT codes 52310 and 52315, respectively. To understand the patients' profiles, we explored their baseline characteristics and comorbidities. Medical costs of stent removal encounters were calculated and adjusted to 2020 US dollars to estimate the economic burden.
Results: Out of 16,682 patients undergoing ureteroscopy with stent placement, 465 (2.8%) had complicated CBSR. Most patients with simple and complicated CBSR were males (52.9% vs 58.1%; 0.03), aged 55‐64 years (37.5% vs 39.8%; p = 0.08), located in South region (41.2% vs 52.2%; p < 0.0001), and had stone comorbidity (55.4% vs 55.7%; p = 0.95). The mean days to stent removal for simple vs complicated CBSR were 16.5 vs 13.2 (p = 0.0004), respectively. Medical costs of complicated CBSR were significantly higher than simple CBSR ($2,206 vs $1,149; p < 0.0001).
Conclusions: Complicated stent removal is associated with an increased economic burden. Ureteral stents designed to reduce the need for complicated CBSR may provide cost‐savings to the US healthcare system.
Cost‐Effectiveness of Retrograde Intrarenal Surgery, Standard and Mini Percutaneous Nephrolithotomy, and Extracorporeal Shock Wave Lithotripsy for the Management of 1‐2cm Renal Stones
KM Wymer, T Juvet, V Sharma, K Koo, MR Humphreys, AM Potretzke
Mayo Clinic
Introduction & Objective: Options for treating 1‐2cm renal stones include retrograde intrarenal surgery (RIRS), percutaneous nephrolithotomy (PCNL), and extracorporeal shock wave lithotripsy (ESWL). Despite the high prevalence and associated costs of nephrolithiasis, a cost‐effectiveness evaluation comparing these treatment modalities has not been performed.
Methods: A Markov model was created to compare cost‐effectiveness of PCNL, URS, and ESWL for 1‐2cm lower pole renal stones. Stone free, complication, retreatment, and secondary procedure rates were based on a systematic literature review, costs were drawn from 2020 Medicare rates, and quality adjusted life years (QALYs) were assigned from the literature. The incremental cost‐effectiveness ratio (ICER) was compared with a willingness‐to‐pay (WTP) threshold of $100,000/QALY. Univariable and multivariable sensitivity analyses were performed, as were additional analyses for non‐lower pole stones and mini‐PCNL.
Results: At 3 years, mean costs per patient were $10,290 (PCNL), $5,930 (RIRS), and $10,916 (ESWL). PCNL resulted in the highest QALYs at 2.951 compared to 2.946 and 2.943 for RIRS and ESWL, respectively. For lower pole stones, RIRS was most cost‐effective followed by PCNL (ICER $948,101/QALY); ESWL was dominated with higher costs and lower effectiveness. Results were more pronounced for non‐lower pole stones with RIRS dominating both PCNL and ESWL. Lastly, although mini‐PCNL resulted in lower costs ($10,109) and higher QALYs (2.953) compared to standard PCNL, it was still not cost‐effective relative to RIRS with an ICER of $633,228/QALY. The lower pole model was sensitive to the stone free rate (SFR) and cost of each modality. ESWL became cost‐effective with SFR ≥75% or cost < $1,247 and PCNL became cost‐effective if cost ≤$5,086. On multivariable sensitivity analysis, the most cost‐effective strategy was RIRS in 99%, PCNL in 1%, and ESWL in 0% of simulations.
Conclusions: For 1‐2cm renal stones, RIRS is the most cost‐effective approach. However, at lower costs, PCNL could become more cost‐effective, particularly for lower pole stones. Additionally, mini‐PCNL offers a promising alternative warranting further investigation.
Seasonal Variations in Inpatient Pediatric Admissions for Urolithiasis
R Alam, W Wu, BR Matlaga, JS Winoker
Johns Hopkins University School of Medicine
Introduction & Objective: It is believed that higher temperatures in the summer months are associated with increased risk of stone formation and subsequent utilization of hospital resources, including inpatient admission. However, these observations have been derived primarily from the adult population. We sought to examine if this purported association between seasonal temperature changes and inpatient stone admissions extends to the pediatric population.
Methods: The most recently available Kids' Inpatient Database (KID) from 2016 was used to estimate nationwide pediatric inpatient admissions in the United States. Patients with a stone‐related admission were identified based on hospital billing codes. KID was linked to temperature data from the National Oceanic and Atmospheric Administration (NOAA) to identify the average monthly temperature at the time and location of admission. Admissions were grouped into seasons: winter (December‐February), spring (March‐May), summer (June‐August), and fall (September‐November). This analysis was replicated using the National Inpatient Sample (NIS) from 2016 to evaluate associations in the adult population as a frame of reference.
Results: There were 6.27 million pediatric inpatient admissions in 2016, of which 8502 (0.14%) had a stone diagnosis. Although the summer months were warmer, there was no significant difference in the number of inpatient stone admissions based on season. Furthermore, there was no significant association between stone admission and temperature (RR 1.00 per degree Fahrenheit, P = 0.15). In adults, however, there was a significant association between inpatient stone admissions and season (P < 0.001), with an increase seen in the summer months. Furthermore, the risk of stone admission increased by 1% with every degree increase in temperature (RR 1.01 per degree Fahrenheit, P < 0.001).
Conclusions: Consistent with prior observational data, increased temperatures were associated with an increased risk of admission in adults. However, there was no observed relationship with seasonal temperature in the pediatric population. This may underscore the differing physicochemical factors driving lithogenesis in children, as compared to adults.
Analysis of urological discussions on Reddit: an emerging platform for patient‐to‐patient information, advice and support
KT Ravivarapu, EB Garden, A Small, O Al‐Alao, MA Palese
Icahn School of Medicine at Mount Sinai
Introduction & Objective: Reddit is a website that hosts thousands of niche discussion boards (subreddits) that are user‐driven and managed. The use of other online platforms such as YouTube and Twitter in urology has been well documented, but the presence and nature of urological discussions on Reddit has not been explored. Here, we aim to present an overview of urology related subreddits with usage statistics and growth trends.
Methods: A scoping search of Reddit was performed for common urological conditions. Nine subreddits with substantial usage were identified: reddit.com/r/interstitialcystitis, r/kidneystones, r/maleinfertility, r/testicularcancer, r/prostatitis, r/prostatecancer, r/erectiledysfunction, r/incontinence, and r/varicocele. Data for each urology related subreddit were obtained from the website subredditstats.com with results updated through March 13, 2021.
Results: All 9 urology related subreddits showed an upward trend in number of users (Figure 1). The interstitial cystitis subreddit had the largest user base (8791 users), followed by erectile dysfunction (6781 users), kidney stones (5983 users), prostatitis (4152 users), male infertility (3153 users), testicular cancer (2762 users), varicocele (2746 users), prostate cancer, (1767 users), incontinence (1218 users). These subreddits had between 2 and 15 new posts per day and 5 and 98 comments per day. Of the top 5 posts on each board, common post types emerged: patient experience stories (57.8%), humor (24.4%), and pictures (17.8%).
Conclusions: Patients use the anonymous online forums Reddit to share unbiased and uninhibited real world experiences. Urology related discussions on Reddit are increasing rapidly and will only continue to expand as a technology focused generation joins the urologic patient population. While a wide variety of urologic conditions are represented on Reddit, conditions that affect younger patients seem to have larger presence. Future analysis of online patient discussions can facilitate better patient care by offering insights into prevailing concerns, common misconceptions, and patient experiences.
Understanding patients' concerns regarding kidney stones using quantitative thematic analysis of social media
KT Ravivarapu, A Small, EB Garden, M Levy, O Al‐Alao, MA Palese
Icahn School of Medicine at Mount Sinai
Introduction & Objective: Analysis of online patient discussions can offer insights into concerns, attitudes and misconceptions from unfiltered and unbiased datasets. We identified key themes and insights from kidney stone patients on Reddit, one of the world's most popular online discussion forums, using quantitative natural language processing (NLP).
Methods: We extracted 3 years of posts (8/2016‐8/2019) and comments (1/2017‐12/2019) from the Reddit community r/kidneystones with 6,010 members. Computational NLP analysis was performed using the meaning extraction method with principal component analysis (MEM/PCA) to identify discussion topics and their relative frequencies (Fig. 1). Kaiser‐Meyer‐Olkin Measure of Sampling Adequacy (KMO) and Bartlett's test were calculated to validate methods.
Results: 2,009 posts and 18,255 comments were analyzed. Overall, patients use this space to crowdsource medical information, diagnoses, and emotional support. The six key themes included: lifestyle/emotional impacts, dietary modifications, symptoms, medical evaluation, surgery/procedures, and pharmacotherapy/alternative therapies. Common terms in the lifestyle/emotional impacts cluster included scared (4.3%), anxiety (2.7%), and stress (1.8%). Dietary modification posts mentioned water (22.1%) and lemon (3.2%). Symptom posts overwhelmingly commented on pain (67.5%) and blood (21.2%). Regarding surgery/procedures, lithotripsy (7.9%) was mentioned more than ureteroscopy (5.3%) or PCNL (1.1%). Discussion of pharmacotherapy/alternative therapies commonly included [tamsulosin] (9.4%) and pain relievers like ibuprofen (3.4%), morphine (3.4%), [oxycodone] (1.6%) and [phenazopyridine] (1.1%). Interestingly, alternative therapies were mentioned in the same cluster, including beer (1.2%) and chanca [piedra] (1.1%).
Conclusions: Kidney stone patients use social media communities to share their real world experiences. NLP offers robust statistical methods to characterize prevailing themes of discussion online. Familiarity with the content of these discussions may allow providers to improve shared‐decision making, patient satisfaction, and quality of care.
Thulium laser enucleation of the prostate versus open prostatectomy: A prospective cost analysis
M Maltagliati, L Berti, U Besana, A Calori, C Buizza, S Micali, BC Rocco, M Sighinolfi, G Bozzini
ASST Valle Olona
Introduction & Objective: Thulium laser enucleation of the prostate (ThuLEP) has emerged as an alternative to open prostatectomy (OP) and is recommended in EAU Guidelines for Prostate bigger than 80 ml. Short‐term results demonstrate minimal morbidity making it safe for patients with prostates of any size, leading to a decrease in hospital stay. The objective of this study is to compare the cost of OP with ThuLEP in the treatment of bladder outlet obstruction (BOO) attributed to benign prostatic hyperplasia.
Methods: From January 2015 to January 2017 a total of 150 consecutive and equivalent patients with large prostate (80 to 300 ml) and documented BOO underwent surgical treatment with either OP (75 in Group 1) or ThuLEP (75 in Group 2). All costs associated with the procedures during the hospital stay and at least 1 year follow up including routine office visits and management of complications were assessed prospectively. A cost analysis of each individual clinical event was performed.
Results: Two groups were set up for the cost analysis. Group 1 for OP, Group 2 for ThuLEP considering a 5 year amortization purchase program. The cost analysis showed a mean cost of 4.407 € for group 1; and 4.047 € for group 2 (Table 1).
Conclusions: ThuLEP is associated with a significant net cost saving compared with OP, in patients undergoing surgery for symptomatic benign prostatic hyperplasia in large glands, especially in a long term purchase program.
Seasonal variation in the incidence of acute renal colic
A Alkhayal, O Alfraidi, T Almudlaj, A Nazer, N Alboqami, K Alrabeeah, AH Alathel
Schulich School of Medicine & Dentistry, Western University
Introduction & Objective: Urolithiasis is one of the most common medical diseases affecting the general population. Many epidemiological studies have shown association between geographic area with high mean daily temperature and urolithiasis disease. However, it is unclear if the seasonal variation within high temperature geographical area will affect the acute presentation of renal colic to the Emergency department (ED). The aim of this study is to identify the influence of seasonal variation in the acute presentation with urolithiasis disease.
Methods: In this retrospective study, the database in King Abdullah International Medical Research Center (KAIMRC), Riyadh, Kingdom of Saudi Arabia has been reviewed in the last 4 years. All patients that have presented with renal colic and have been diagnosed with urolithiasis by non‐contrast enhanced CT scan have been included in our study.
Results: A total number of 1057 patients have been enrolled in this study . 753 (71.24%) were males and 304 (28.76%) were females, with a mean age of 42.33 ± 16.12 years. Most of the patients presented in summer (31.22%), followed by spring (26.87 %), fall (24.12%) then winter (17.79%) respectively. Most of the patients (84.77%) presented with ureteral stones, while (15.23%) presented with kidney stones. (78.33%) of patients have no history of previous stone formation, while (21.67%) of patients were recurrent stone former.
Conclusions: Acute presentation with urolithiasis is higher during summer followed by spring, fall then winter respectively. Public educational program is highly recommended to increase awareness about stone formation and appropriate methods to avoid it. To this end, further study is needed to know the stone composition and appropriate methods to avoid developing urolithiasis.
Health‐Related Quality of Life Disparities among Hispanic/Latinx Patients with Nephrolithiasis
AR Flores, G abedi, C Girgiss, KL Penniston, S Li, D Norena, DF Friedlander, SK Bechis, RL Sur
Introduction & Objective: It is documented that Hispanic/Latinx kidney stone formers have inferior health‐related quality of life (HRQoL) compared to the general population.1‐3 We hypothesized that socioeconomic factors are primary drivers of this finding. Our objective was to identify factors that explain HRQoL discrepancies among Hispanic/Latinx stone formers.
Methods: This was a prospective cohort observational study of patients with kidney stones at UC San Diego Health who were enrolled over 2 years from June 2018 to August 2020. Patients enrolled completed a validated English or Spanish copy of the Wisconsin Stone Quality of Life questionnaire (WISQoL) based on their language preference. Patient characteristics and self‐reported HRQoL were compared between Hispanic/Latinx and non‐Hispanic/Latinx stone formers. Matched and unmatched group comparisons were performed based on age, gender, body mass index, stone symptoms, and insurance type.
Results: A total of 270 patients were enrolled (Hispanic/Latinx n = 88; non‐Hispanic/Latinx n = 182). Hispanic/Latinx stone formers had higher rates of public insurance at baseline (p < 0.001) with significantly lower HRQoL [social impact (p = 0.007), emotional impact (p = 0.005)]. However, a matched cohort comparison demonstrated no differences.
On multivariate analysis, patients with private insurance had double the likelihood of having higher HRQoL (OR 2.21, 95% CI 1.12‐4.02, p < 0.05). Stone symptoms (OR = 0.06, 95% CI 0.03‐0.14, p < 0.001) and ED visits (OR = 0.04, 95% CI 0.228‐0.803, p = 0.008) were associated with lower HRQoL. Ethnicity was not a significant factor in quality of life scores on multivariate analysis.
Conclusions: Our analysis suggests that differences in HRQoL amongst Hispanic/Latinx stone formers are primarily driven by socioeconomic factors as opposed to clinical differences. Specifically, source of insurance appears to have significant effect on HRQoL in this ethnic group.
What is the kidney stone related nephrectomy prevalence in an emerging country?
V Dall'Aqua, R Borges, A Rodrigues, A Lopes Neto
Introduction & Objective: Kidney stone disease is a preventable renal failure etiology. However, this management could be an important public health concern in emerging countries. To access the local scenario about stone related nephrectomy, we review our data from a tertiary center.
Methods: Medical records from three hospitals integrated to ABC Medical School, at Santo Andre ‐ Brazil, were reviewed including 2008 to 2019 data. All nephrectomies were accessed, however partial nephrectomies were excluded after first analysis.
Results: There were performed 398 nephrectomies between 2008 to 2019. From these cases, 62 (15.5%) were partial nephrectomies. Ninety‐eight surgeries (29.1%) were due kidney stone disease and more than one third of the patients (35.7%) was admitted without renal failure, but they lost the kidney function on behalf of public health program slowness.
Conclusions: Brazilian National Health Program should improve the patients access to urology team and measures to prevent kidney stones development, once upon this is a very prevalent disease and an important renal failure preventable etiology.
Withdrawn
Trends in the Influence of Gender, Race, and Ethnicity on the Prevalence of Kidney Stones: A Multi‐Institutional and Claims Analysis
J Crivelli, N Maalouf, P Yan, A Hughes, R Hsi, NE Canvasser, N Kachroo, D Leavitt, K Wood, G Oates, JM Hollingsworth, DG Assimos
The University of Alabama
Introduction & Objective: Significant increases in kidney stone prevalence have been reported for Black and Hispanic individuals in the US, but the gender‐specific contribution to this trend is unclear. We evaluated the distribution of prevalent stone disease by gender, race, and ethnicity in contemporary cohorts.
Methods: We identified patients with a kidney stone diagnosis between 2010‐2019 from three centers (University of Alabama at Birmingham [UAB, n = 32,745], University of Texas Southwestern [UTSW, n = 51,354], and Parkland Memorial Hospital [PMH, n = 22,967]). We also utilized a claims database (Optum Clinformatics Data Mart) to identify working‐age adults with a kidney stone diagnosis from 2010‐2019 (n = 68,594). Differences in male‐to‐female ratio between groups across all datasets were assessed with the Mann‐Whitney U test. In the Optum cohort, temporal trends in male‐to‐female ratio were modeled with linear regression.
Results: In each cohort, most Black stone formers were female, most White stone formers were male, and most non‐Hispanic stone formers were male; in two of the four cohorts, most Hispanic stone formers were female (Figure 1). We observed a significant difference in male‐to‐female ratio between Black vs. White stone formers, but not between Hispanic vs. non‐Hispanic stone formers (Figure 1). In the Optum cohort, a significant linear decline in male‐to‐female ratio was observed in White and non‐Hispanic stone formers, but not in Black and Hispanic stone formers (Figure 2).
Conclusions: An analysis of multi‐institutional and claims data showed that most Black stone formers were female, whereas most White stone formers were male, demonstrating a significant difference in gender distribution. Based on insurance claims, the male‐to‐female ratio decreased in all groups over time, but most consistently among White and non‐Hispanic patients. Further evaluation of these findings and their association with comorbidities and socioeconomic factors is needed to understand disparities in stone disease.
Withdrawn
The Social Impact of Surgery for Nephrolithiasis: Results from the Endourological Society TOWER Research Collaborative
AE Jones, G Lin, H Stambakio, BH Chew, JM Stern, JB Ziemba
University of Pennsylvania Perelman School of Medicine
Introduction & Objective: Nephrolithiasis is among the most common urological conditions; however, the social impact of the disease remains significantly understudied, particularly following surgical intervention. We prospectively captured patient‐reported ability to participate in social roles and activities in patients following ureteroscopy (URS) or percutaneous nephrolithotomy (PCNL) for nephrolithiasis.
Methods: Adults undergoing URS or PCNL for renal/ureteral stones were eligible for inclusion (10/2020‐1/2021). Patients prospectively completed PROMIS‐Ability to participate in social roles and activities instrument pre‐operatively (POD 0) and via email on POD 1, 7, and 14. Scores are reported as T‐scores (normalized to US pop., mean = 50) with a change of 5 (0.5 SD) considered clinically significant.
Results: A total of 33 patients completed enrollment at POD 0 (POD 1 = 21, POD 7 = 21, POD 14 = 15). For the overall cohort, there was a clinically and statistically significant difference in scores over each subsequent time comparison (repeated measures ANOVA; p < 0.001). Repeated measures ANOVA show statistically significant difference in scores over each subsequent time comparison for URS patients (p = 0.003), but not PCNL patients (Figure 1). URS patients return to baseline social participation by POD 14, but PCNL patients do not see a return to baseline. Among the entire cohort, increasing age was predictive of greater social participation preoperatively (CI: 0.02–0.66; p = 0.04) and at POD 1 (CI: 0.06 – 0.86; p = 0.03).
Conclusions: Ability to participate in social roles and activities declines immediately post‐operatively. URS patients see normalization in social participation by POD 14, but PCNL patients experience social interference for longer than 14 days. Results offer meaningful insight to assist counseling patients for surgical treatment of nephrolithiasis.
Contemporary practice patterns of transurethral therapies for benign prostate hypertrophy: Results of a worldwide survey
MS Lee, M Assmus, DK Agarwal, T Large, AE Krambeck
Northwestern University Feinberg School of Medicine
Introduction & Objective: Benign prostatic hypertrophy (BPH) is one of the most common medical conditions affecting men. The most recent AUA and EAU guidelines on BPH/LUTS offer Urologists the ability to choose from multiple options. The guidelines offer recommendations based on prostate volume, bleeding risk, and side effect profile, but otherwise give Urologists the freedom to choose. With so many transurethral surgical therapies available, the surgical and postoperative management practices of urologists are unknown. Herein, we present the results of a contemporary global survey on practice patterns of transurethral BPH therapies.
Methods: A REDCap survey was distributed to the ∼3500 members of the Endourological Society. Surgeons completed demographic information. Surgeons selected the BPH therapies they perform ≥10 cases/year. There were four categories of BPH therapies: ablation, enucleation, resection/vaporization, and MISTs. Within each category, there were subcategories to account for different energy modalities. All statistical analyses were performed using SAS 9.4 (2019. Cary, NC).
Results: A total of 175 surgeons responded to our survey. Prostate resection/vaporization remained the most commonly utilized category (n = 147/283, 51.9%) followed by enucleation (n = 64/283, 22.6). Within each category, Bipolar TURP (bTURP) was the most common modality for prostate resection (n = 102/147, 69.4%). Holmium laser enucleation (HoLEP) was the most common modality for enucleation (n = 30/64, 46.9%). Urolift® was performed more often than Rezūm™ (n = 19/34, 55.9% vs. n = 15/34, 44.1%). Among surgeons performing ablation, country of practice was a significant variable for LOS (p < 0.0001). For surgeons performing enucleation, academic urologists and those who had completed a fellowship predicted POD1 catheter removal (p = 0.0240 and p = 0.020, respectively).
Conclusions: In this contemporary, global survey of the Endourology society, resection/vaporization techniques remain the most commonly performed surgical BPH therapies. Rates of MIST remained relatively low at 12.0%. 73.7% of Urolift®, 66.7% of Rezūm™, and 60% of Aquablation® procedures were performed as outpatients.
Impact of flow disruptions on mental workload and performance during Percutaneous Nephrolithotomy
S Hussain, SM Nazim, M Ather, N Zahid, M Ather
Aga Khan UNiversity
Introduction & Objective: To study the impact of intraoperative disruptions on surgeons' mental workload and performance during percutaneous nephrolithotomy (PCNL).
Methods: A structured standardized tool was used to identify disruptions and interference during 33 PCNL procedures. The surgical steps during PCNL were divided into 4 phases i.e., ureteric catheter placement, puncture and tract dilation, intra‐calyceal navigation and stone fragmentation and tube placement. Surgeons' workload was evaluated using a validated tool i.e. Surgery Task Load Index (SURG‐TLX), and correlated with the mean observed intraoperative disruptions. All operating team members evaluated teamwork immediately after the procedure. Statistical analysis was done on SPSS version 22.
Results: A total of 1897 disruptions were observed, with an average of 57.48 ±16.36 disruptions per case. The highest number 32.06 ±14.12 were observed during phase III (Lithotripsy). Most disruptions were due to people entering or exiting operating room (OR) 29.1 + 10.03/ case followed by ringing phone or pagers 6.42 + 2.4. Mean observed intraoperative disruptions were significantly associated with surgeon's mental workload, with people entering or exiting OR being the most frequent disruptions, showed its impact on all domains of surgeons' mental workload measured by SURG‐ TLX. Compared to other team members, surgeons' assistant experienced inferior teamwork (r = ‐0.433; p = 0.012.
Conclusions: Significant intraoperative disruptions were observed during PCNL and correlated with surgeons' workload and have negative impact on the teamwork. Improving operating room dynamics by reducing unnecessary disruptions would help establish efficient and smooth surgical work environment for safe surgical care.
Racial Differences in Utilization of Cytoreductive Surgery among Metastatic Renal Cell Carcinoma Patients Receiving Systemic Therapy
A Becerra, D Cao, N Buac, M Greydanus, M Sturgis, C Feng, C Coogan, E Cherullo, S Vourganti, A Stephenson, AK Chow
Rush University Medical Center
Introduction & Objective: Systemic targeted therapy (STT) is considered first‐line treatment for the management of metastatic renal cell carcinoma (mRCC), which presents in 3 out of 10 patients diagnosed with RCC. National guidelines also support the role of initial cytoreductive surgery (CS) in combination with STT in suitable patients with favorable risks given the potential benefit in overall survival in this population. There is a paucity of literature examining contemporary utilization of CS with STT and whether it varies among racial subgroups. The objective of this study was to evaluate whether racial differences exist in the use of CS among mRCC patients receiving STT.
Methods: Clinical stage IV RCC patients who received STT were identified in the National Cancer Database (2006‐2017). Patients were categorized as undergoing CS+STT vs. STT. Racial subgroups that were evaluated were White, Black, Hispanic, and Other. A multivariable logistic regression was used to assess the association between race/ethnicity and utilization of CS+STT while controlling for patient, tumor, and hospital factors.
Results: We identified 21,763 mRCC patients who met inclusion criteria, of which 29% underwent CS. Black, Hispanic, and Other patients comprised 9%, 7%, and 3% of the cohort, respectively. The unadjusted rates of CS utilization among White, Black, Hispanic, and Other patients were 29%, 22%, 29%, and 30%, respectively and remained stable over time. In adjusted models, independent of patient, tumor, and hospital factors, the only racial differences were that Black patients had 29% lower odds of undergoing CS compared to White patients (OR = 0.71, 95% CI = 0.61‐0.81). Other factors associated with lower CS utilization were older age, Medicaid/no insurance (compared to private), nonacademic hospitals, and urban/rural residence (compared to metro). Black patients experienced worse 5‐year overall survival (HR = 1.11, p = 0.01).
Conclusions: The use of CS for mRCC in the STT era has remained stable for all patients, yet Black patients are still less likely to undergo CS. These effects were not explained by differences in income, education, insurance, or other sociodemographic factors. Given that the survival benefit of CS may only be seen in select populations, it Is unclear whether lower utilization of CS among Black patients reflects specific patient selection criteria or is a product of other patient factors that are difficult to capture in analysis, such as differences in access to health care, certain comorbid conditions, or varying patient attitudes towards surgical intervention.
Withdrawn
Five Year Survival Outcome Comparison amongst Patients with Unfavorable vs. Favorable Renal Cell Carcinoma Subtypes
D Roadman, A Becerra, N Buac, M Greydanus, M Sturgis, D Cao, C Coogan, E Cherullo, S Vourganti, A Stephenson, AK Chow
Rush University Medical Center
Introduction & Objective: Renal cell carcinoma (RCC) tumors vary widely with respect to oncologic risk and are composed of heterogenous histological subtypes that can affect treatment decisions and patient management. While they are rare, certain RCC histologies may possess inherent biological features that make them more aggressive at presentation and throughout treatment. However, no study has quantified the long‐term survival differential between favorable and unfavorable RCC histologies.
Methods: Clinical or pathological stage I‐IV RCC patients who underwent partial or radical nephrectomy were identified in the National Cancer Database (2004‐2017). Patients were categorized as having unfavorable (medullary cell, collecting duct, unspecified) and favorable histologies (papillary, chromophobe, cystic, and clear cell). 5‐year overall survival was compared between those with favorable vs. unfavorable histology using Kaplan‐Meier curves and a multilevel Cox proportional hazards models to account for clustering by hospital. Propensity score matching was conducted to adjust for confounding by patient, treatment, tumor, and hospital factors.
Results: We identified a total of 282,623 RCC patients who met inclusion criteria, of which 839 (< 1%) were unfavorable histologies. Overall, median follow‐up was 4.6 years. The 5‐year survival rates among those with favorable and unfavorable were 75% (95% CI = 74%‐76%) and 39% (95% CI = 38%‐40%), respectively (Figure 1). In propensity score matched models, unfavorable histologies were associated with worse 5‐year overall survival (HR = 1.75, 1.71‐1.80). Results were consistent when individual unfavorable histologies were compared to favorable histologies. Medullary cell (HR = 1.82, 1.65‐2.02), collecting duct (HR = 1.65, 1.58‐1.75), and unspecified RCC (HR = 1.71, 1.44‐2.10) were associated with worse 5‐year overall survival compared to favorable histologies.
Conclusions: In this large national study of RCC patients who underwent partial or radical nephrectomy, unfavorable histologies have almost a 2‐fold higher risk of dying within 5 years. These effects were independent of tumor characteristics such as grade, T, N, and M stage suggesting that unfavorable histologies are mechanistically different than favorable histologies. These results have implications for developing personalized therapies that target high‐risk, aggressive tumors that are otherwise reasonable to manage.
Moderated Poster Session 03: BPH I
Three‐Year Outcomes after Aquablation Compared to TURP: Efficacy and Ejaculatory Improvements Sustained
PJ Gilling
Urology Bay of Plenty
Introduction & Objective: To compare three‐year (last follow‐up of the protocol) safety and efficacy outcomes after Aquablation or transurethral resection of the prostate (TURP) for the treatment of lower urinary tract symptoms (LUTS) related to benign prostate hyperplasia (BPH).
Methods: 181 patients with BPH were assigned at random (2:1 ratio) to either Aquablation or TURP. Patients and follow‐up assessors at each site were blinded to treatment. Assessments included International Prostate Symptom Score (IPSS), Male Sexual Health Questionnaire (MSHQ), International Index of Erectile Function (IIEF) and uroflow.
Results: At three years, IPSS scores improved by 14.2 points in the Aquablation group and 15 points in TURP (p = .7050, 95% CI for difference −3.6 to 5.3 points). Three‐year improvements in maximum flow rate (Qmax) were large in both groups at 10 and 9.7 cc/sec for Aquablation and TURP, respectively (p = .9078, 95% CI for difference −2.9 to 6.4). Sexual function as assessed by MSHQ‐EjD was stable in the Aquablation group and decreased slightly in the TURP group; these changes persisted at year 3. At three years, PSA was reduced significantly in both groups but showed no difference between groups (p = .4074 for difference). The average annual retreatment occurrence was less than 2% in both treatment groups.
Conclusions: Three‐year efficacy outcomes after TURP and Aquablation were similar and the rate of surgical retreatment was low and similar to TURP. Efficacy results have maintained their improvement since the 90 day follow‐up for both groups that are consistent with all other resective surgical techniques.
The OPEN WATER trial: Aquablation in a real‐world setting 1 year follow‐up
PJ Gilling
Urology Bay of Plenty
Introduction & Objective: Waterjet‐based prostate ablation(the Aquablation procedure) is an increasingly utilized treatment world‐wide for the treatment of symptomatic benign prostatic hyperplasia (BPH). The study was designed to investigate the safety and effectiveness of the Aquablation procedure in a real‐world setting.
Methods: Prospective multi‐national 5‐center single‐arm study with follow‐up to date of 1 year. Sites in New Zealand, Australia, England, Lebanon and Germany enrolled patients.
Results: 178 men underwent the Aquablation procedure at 5 international sites. Mean prostate volume was 60cc. Procedure time averaged 24 minutes and total anesthesia duration was 50 minutes. Five patients (2.7%) underwent blood transfusion in the first week after the procedure; of these, one was for delayed (day 6) bleeding. Prostate volume assessed with transrectal ultrasound decreased 36% by month 3. International Prostate Symptom Score (IPSS) decreased from 21.6 at baseline to 6.1 at 1‐year follow‐up, a 15.5‐point improvement (p < .0001). Maximum urinary flow rate increased from 10.1 at baseline to 21.4 cc/sec at 1 year (an increase of 9.9 cc, p < .0001). No surgical retreatments have occurred due to BPH symptoms.
Conclusions: Real‐world evidence shows that the Aquablation procedure is safe and effective for the treatment of symptomatic benign prostatic hyperplasia. Transfusion rates are higher than other minimally invasive therapies. Trial registration: ClinicalTrials.gov number, NCT02974751.
Pulsed thulium laser enucleation of the prostate (ThuLEP) utilizing a novel pulsed Thulium:YAG laser: first clinical results
C Netsch, B Becker, CM Rosenbaum, AJ Gross
Department of Urology, Asklepios Hospital Barmbek, Hamburg, Germany
Introduction & Objective: A novel pulsed Tm:YAG laser has been introduced for endoscopic enucleation of the prostate (EEP). Aim of this study was to evaluate the safety and efficacy of a pulsed Tm:YAG laser for thulium laser enucleation of the prostate (ThuLEP) in patients with symptomatic benign prostatic obstruction (BPO).
Methods: 41 consecutive patients, undergoing ThuLEP at our institution between September and December 2020, were evaluated prospectively. ThuLEP was carried out using a pulsed 2μm 150‐W Tm:YAG laser (RevoLix® HTL, LISA Laser products, Katlenburg, Germany) at 100‐W (200 Hz, 0.5 J). Depending on lobe configuration and size of the prostate, a 1‐ or 2‐lobe technique was performed. The baseline parameters, perioperative parameters, immediate functional outcomes (International Prostate Symptom Score (IPSS), Quality of Life (QoL), maximum urinary flow rate (Qmax), post‐void residual urine (PVR)), and the incidence of complications were assessed, respectively. The perioperative complications were noted and classified according to the modified Clavien classification system. Patient data were expressed as median (interquartile range) or numbers (%).
Results: Median age was 72 (63‐75) yrs, preoperative prostate volume was 60 (47.5‐98.5)ml and ASA score 2 (2‐3). A total of 8 patients (19.5%) were treated under continuous antiplatelet therapy (aspirin), while anticoagulant/antiplatelet therapy was temporarily stopped in 11 (26.8%) patients. Total operation time was 44 (29.75‐61.25) min, and the enucleation time 13.33 (8.27‐15.96) min, respectively. Median resected weight was 50 (25‐91) gm, haemoglobin decrease 2 (1.1‐3) g/dl, catheter time 2 (2‐2.75) days and postoperative stay 3 (3‐4) days. Clavien 1 (19.5%), Clavien 2 (7.3%), Clavien 3b (4.9%), and Clavien 4a (2.4%, n = 1, allergic shock due to analgesics) complications occurred. At discharge, Qmax (10.6 vs. 18.9 ml/s), PVR (130 vs. 35 ml), IPSS (21 vs. 13), and QoL (5 vs. 2) differed significantly from baseline (p < 0.001).
Conclusions: The pulsed Tm:YAG laser is safe and effective for EEP in patients with symptomatic BPO. Prospective studies are necessary to assess the value of this new laser device for EEP.
Aquablation vs. thulium laser enucleation of the prostate (ThuLEP): early functional results of a matched‐paired analysis
B Becker, K Vogt, AJ Gross, CM Rosenbaum, C Netsch
Department of Urology, Asklepios Hospital Barmbek, Hamburg, Germany
Introduction & Objective: The aim of this study wastocompare the complications and early functional outcomes afteraquablationwith an established laser enucleation procedurein the therapy ofbenign prostatic hyperplasia (BPH).
Methods: Based on the prostate volume, 44 patients that were treated with aquablation were matched with 44 patients who received a ThuLEP procedure. ThuLEP wasperformed with a2 μm (vela®XL, StarMedTec, Starnberg, Germany) thulium laser (90‐W) andaquablation therapy with the AquaBeam system(PROCEPT BioRobotics, Redwood Shores, USA). All data are expressed as median (interquartile range).
Results: The prostatevolume was 70 (45‐86) ml. The surgical time did not differ significantly between ThuLEP andaquablation with 44.5 and 42 min, respectively. The hemoglobin drop after aquablation was significantly higher compared to ThuLEP (‐2 vs. ‐1.5 g/dl, p < 0.02). At discharge, IPSS(21 and 20.5 vs. 14 and 9) and QoL (4 and 5 vs. 3 and 2) improved significantly after ThuLEP and aquablation (p < 0.001), with QoL being significantly lower after aquablation therapy (5 vs. 2, p = 0.018). The catheterizationand hospitalization timewere 2 and 3 daysin both groups, respectively(p = 0.5). Reoperationswere necessary in 3 patients (6.5%) afteraquablation and in 2 patients (4.5%) after ThuLEP. Urinary retentionoccurredin 4 patients (8.7%)after aquablation and in 2 patients (4.5%) after ThuLEP. 3 patients (6.5%) that were treated with aquablation developed a urinary tract infection. 5 patients (10.9%) after aquablation developed a postoperative bladder tamponade that could be evacuated via catheter, however, no patient after ThuLEP (p < 0.05).
Conclusions: Aquablation and ThuLEP are fast and safe procedures with immediate micturition improvement postoperatively. Bleeding‐related complications after aquablationoccur more frequently in comparison to thulium laser enucleation of the prostate.
Prostatic Urethral Lift (PUL) demonstrates real world effectiveness in subjects with obstructive median lobes
NJ Barber, KL Ng, G Eure, D Grier, M Rochester, D Rukstalis
Frimley Park Hospital
Introduction & Objective: Results from the MedLift trial revealed prostates with middle lobe obstruction can be treated safely and effectively with the minimally invasive PUL procedure. Utilizing the real‐world retrospective (RWR) study of PUL, we assess outcomes of the treatment in subjects with obstructive middle lobes (OML), compared to subjects with obstructive lateral lobes (LL) only and MedLift results
Methods: 2090 patients across 18 USA and Australian sites who underwent PUL after market clearance through May 2019 were included in the RWR database. Patients were filtered for non‐retention status at baseline and stratified into OML (n = 228) or LL (n = 1311) cohorts. Baseline demographics were compared between RWR OML vs. RWR LL and MedLift subjects. Absolute IPSS, QoL, Qmax, and PVR were evaluated at 1, 3, 6, and 12 months post‐PUL. Adverse events of RWR OML subjects were calculated. All outcomes were compared to RWR LL subjects and absolute IPSS was compared to MedLift OML.
Results: RWR OML subjects were on average 69.8 y.o. with larger prostate volumes (53.3cc ±21.3) than RWR LL (45.4cc ±19.6) and MedLift (44.2 ± 11.2) subjects, and lower baseline IPSS (19.5 ± 6.9) than MedLift subjects (24.2 ± 4.9). Qmax was also significantly lower in RWR OML subjects than RWR LL and MedLift patients. Following PUL, we report similar absolute IPSS and QoL scores following PUL between RWR OML and RWR LL subjects throughout follow‐up, with significantly better IPSS and QoL at 3 months in the RWR OML cohort (Figure 1). Despite differences in IPSS at baseline between RWR OML and MedLift subjects, follow‐up absolute IPSS scores were equivalent at each timepoint between both groups (Figure 1). QoL, Qmax, and PVR in RWR OML subjects were similar to or better than RWR LL subjects throughout follow‐up. The rate of post‐procedure catheterization in RWR OML (7.9%) subjects was no different from RWR LL subjects (5.8%) when catheterization was not the standard of care. No difference was seen in all AE rate or rate of specific AEs between RWR OML and LL subjects.
Conclusions: The large multicenter real‐world study of PUL reveals OML subjects exhibit similar symptom response and safety profile compared with LL patients and confirm results from the controlled MedLift study.
The UroLift® Implant Long‐Term Biological Mechanism Behind Relief from Prostatic Obstruction
CG Roehrborn, P Chin, H Woo
UT Southwestern
Introduction & Objective: The prostatic urethral lift (PUL) using UroLift® implants has been shown to widen the prostatic urethra, providing safe and effective relief from LUTS in BPH patients. Here, we utilize histological data from pre‐clinical canine tissue, resected tissue from human subjects treated with the UroLift System, and post‐market surveillance data to elucidate the long‐term biological mechanism of action of the UroLift implant.
Methods: Cystoscopy and subsequent histology was analyzed from 4 human PUL patients ‐ cystoscopy at 6‐27 months post‐procedure and tissue resection/histology at 13‐43 months. PUL was performed on 24 dogs and histopathology conducted on surrounding prostatic tissue at 1, 3, 6 and 12 months after implantation. Worldwide post‐market data were reviewed for implant migration, encrustation, and breakage from April 2018 to September 2020.
Results: Clinical cystoscopy of human PUL subjects reveals that UroLift® implants maintain compression of the urothelium, which results in widening of the urethra and retracted lobes. Canine histopathology demonstrate tissue compression occurring immediately, paired with locally decreased blood flow which is followed by benign lobular atrophy by 1 and 6 months (Fig 1). Human histopathology reveals a similar process. Minimal‐mild chronic inflammation was observed at the implant‐tissue interface at 1‐month post‐implantation. At 6 and 12 months post‐implantation, signs of a stable and normal healing response were observed with minimal chronic inflammation and minimal‐mild fibrosis. Increased lobular atrophy and scarring occur through 12 months post‐implantation, and the implant may become fully encapsulated within prostatic tissue by 6 months. Post‐market data from over 770,000 implants did not demonstrate evidence of migration after a successful deployment, and revealed a 0.006% rate of stone formation from encrustation and a 0.004% breakage rate.
Conclusions: The UroLift implants immediately provide localized compression and induces chronic tissue remodeling through 12 months. When implants are placed properly, these changes occur safely and with minimal risk of migration, encrustation, or breakage, affirming the benign nature of this non‐thermal approach.
Aquablation Outcomes in Superlarge Prostates
A Kasraeian, M Alcantara, K Mola Alcantara, S Sterious, N Patel, R Gonzalez, D Elterman, B Helfand, B Chughtai, L Kriteman, A Te
Kasraeian Urology
Introduction & Objective: To determine if Aquablation can safely and effectively treat prostates that exceed 150cc in size (defined as superlarge) in men suffering from lower urinary tract symptoms (LUTS) due to benign prostatic hyperplasia (BPH). The most commonly performed procedure in this prostate size category would be a simple prostatectomy that is associated with severe bleeding complications ranging from 12% to 29%(1).
Methods: Data from Aquablation procedures from surgeons who had performed multiple procedures on superlarge prostates since 2018 in North America was collected and analyzed. A retrospective analysis was performed on procedural details and short term clinical outcomes.
Results: Seventy‐eight (78) Aquablation cases were performed on men with prostates meeting the definition of superlarge with a mean prostate size of 195cc (range 150 to 363cc) across eight hospitals and 18 surgeons. The average number of Aquablation treatment passes was 2.3 (range 1 to 5). Fifty‐five (55%) of patients were done under spinal anesthesia. Postoperative bleeding requiring transfusion occurred in three cases and no take‐back for fulguration was noted in this cohort.
Conclusions: Aquablation performed in superlarge prostates has demonstrated a similar procedural safety profile as reported in previous Aquablation clinical trials (WATER, WATER II, and OPEN WATER).
References
1. Pariser JJ, Pearce SM, Patel SG, Bales GT. National Trends of Simple Prostatectomy for Benign Prostatic Hyperplasia With an Analysis of Risk Factors for Adverse Perioperative Outcomes. Urology. 2015 Oct 1;86(4):721–6.
Post‐operative pelvic pain after prostate enlargement transurethral procedures: A systematic review and meta‐analysis.
ML Wroclawski, D Castellani, F Heldwein, SB Teles, JD Cha, H Zhao, T Herrmann, V Vinson, J Teoh
School of Medicine, Faculty of Medicine and Health, University of Leeds, Leeds Department of Targeted Intervention, Division of Surgery and Interventional Science, University College London, London
Introduction & Objective: We performed a systematic review and meta‐analysis to evaluate and compare the incidences of post‐operative pelvic pain in patients undergoing ablation, enucleation and conventional transurethral resection of the prostate (TURP).
Methods: A systematic review and meta‐analysis was conducted according to the PRISMA guidelines. Using MEDLINE via PubMed and Cochrane CENTRAL, randomised control trials (RCTs) and observational studies reporting dysuria rates post‐ablation, enucleation or TURP were identified using relevant keywords. The risk of biases in included comparative RCTs and observation studies were assessed using the Cochrane Risk of Bias tool and the Newcastle‐Ottawa Scale respectively.
Results: 62 studies were included for qualitative analysis, while 51 of them reported number of patients with dysuria post‐intervention. Three observational studies and 13 RCTs compared the rates of dysuria in patients undergoing ablation, enucleation or TURP. The pooled incidence of dysuria in patients undergoing ablation, enucleation and TURP were 0.15 (95% CI 0.10 – 0.22), 0.01 (95% CI 0.00‐0.03) and 0.10 (95% CI 0.06‐0.15) respectively. Upon comparison of the three interventions, ablation is associated with a higher risk of dysuria than enucleation (RR 2.19, 95% CI 1.04‐4.62) and TURP (RR 2.40, 95% CI 1.03 – 5.62) in observational studies but not RCTs; and there were no significant differences in the rates of dysuria in the other comparisons.
Conclusions: Persistent dysuria is relatively common after transurethral benign prostatic hyperplasia surgery. Patients undergoing ablation had a higher rate of post‐intervention dysuria than those undergoing enucleation and TURP in observational studies. It is important to counsel our patients on the possibility of prolonged dysuria after surgery.
WATER vs WATER II: Three Year Comparison of Aquablation Therapy for Benign Prostatic Hyperplasia
D Nguyen, KC Zorn, N Bhojani
University of Montreal Hospital Center (CHUM)
Introduction & Objective: Surgical options are limited when treating large (>80cc) prostates for lower urinary tract symptoms (LUTS) due to benign prostatic hyperplasia (BPH). Open simple prostatectomy remains the most common procedure performed for large prostates. As such, there is a need for novel surgical approaches with shorter learning curves and effective treatment. Aquablation (AquaBeam System, PROCEPT BioRobotics, Inc., USA), an ultrasound‐guided, robotically executed waterjet ablative procedure, could fill this gap. This analysis compares the outcomes of Aquablation in 30cc to 80cc prostates with the outcomes in 80cc to 150cc prostates.
Methods: WATER (NCT02505919) is a prospective, double‐blind, multicenter, international clinical trial comparing the safety and efficacy of Aquablation and TURP in the treatment of LUTS/BPH in men 45 to 80 years old with a prostate between 30cc and 80cc. WATER II (NCT03123250) is a prospective, multicenter, single‐arm international clinical trial of Aquablation in men with a prostate between 80cc and 150cc. We compare 36‐month outcomes amongst 116 WATER and 101 WATER II study subjects undergoing Aquablation. Students' t‐test or Wilcoxon tests were used for continuous variables and Fisher's test for binary variables.
Results: International Prostate Symptom Score (IPSS) scores improved from 22.9 and 23.2 at baseline in WATER and WATER II, respectively, to 8.0 and 6.4 at 36 months, with 36‐month reductions of 14.4 and 16.7 points, respectively (p = .07 for difference in change scores). At baseline, urinary flow rate (Qmax) was 9.4 and 8.7 cc/sec in WATER and WATER II, improving to 20.6 and 19.0 cc/sec, respectively (p = .70 for difference in change scores) at 36 months. Improvements in both IPSS and Qmax were immediate and sustained throughout follow‐up. Change in IPSS, Qmax, and post‐void residual (PVR) can be found in Figure 1.
Conclusions: Aquablation clinically normalizes outcomes between patients with a 30cc to 80cc prostate and patients with an 80cc to 150cc prostate treated for LUTS/BPH. It is effective in patients with large prostate glands (>80cc) with acceptable complications out to three years.
Withdrawn
Withdrawn
Prostatic Urethral Lift ‐ Influence of advanced techniques on benign prostatic enlargement patient pathway
A Dhanasekaran
Sandwell And West Birmingham NHS Trust
Introduction & Objective: Prostatic urethral lift (PUL) is an approved minimally invasive surgical procedure to relieve voiding urinary symptoms associated with a benign prostatic enlargement (BPE). It is a day‐case procedure, recommended by the United Kingdom National Institute for Health and Care Excellence (NICE). Advanced techniques to treat men with Obstructing Median Lobe (OML) and high bladder neck have been developed. This study assessed whether using advanced techniques and a modified, simplified patient pathway could shorten and improve the patient pathway, thereby helping to reduce waiting time and overall cost.
Methods: Eligible patients were men who were referred to hospital for BPE treatment. Group A followed the traditional BPE pathway (clinic assessment, prostate volume and flexible cystoscopy, flow rate and bladder scan, surgery under general anaesthesia, and clinic‐based outpatient follow‐up). Group B followed a simplified pathway, using advanced techniques, involving clinical assessment, flow rate and bladder scan, PUL under local anaesthetic, and telephone follow‐up. Differences in time to PUL, quality of recovery visual analogue scale (QoR‐VAS) and pelvic pain tolerability visual analogue scale scores (VAS), International Prostate Symptom Scores (IPSS), quality of life (QoL), and overall costs were compared between groups.
Results: In the last twelve months from March 2019 to February 2020, 24 patients were treated in group A and 15 in group B (average prostate size: 84g and 79g respectively). The simplified pathway was associated with shorter waiting times for PUL than the traditional pathway. Similar mean outcomes 3 months after PUL were seen for QoR‐VAS (group A 89% vs. group B 87%), IPSS, QoL, and pain tolerability score (Table 1). The number of implants between group A and group B was also comparable; 2.8 ± 0.9 (range: 2‐4) and 3.2 ± 1.0 (range: 2‐5) respectively. Overall expenditure was reduced in group B due to less need for preoperative investigations and telephone follow‐up.
Conclusions: Outcomes were not affected by fewer preoperative investigations. Our findings support using PUL to treat a broadened group of men with obstructive urinary symptoms from BPE (including men with OML and high bladder neck) in an ambulatory setting via a simplified pathway.
The major new findings of the study ‐ New advanced techniques in PUL simplify BPE pathway and offer excellent results.
Prognostic factors predicting late bleeding after ThuLEP
M Maltagliati, L Berti, U Besana, A Calori, C Buizza, BC Rocco, S Micali, M Sighinolfi, G Bozzini
ASST Valle Olona
Introduction & Objective: To evaluate late bleeding risk and its predicting factors in patients operated for benign prostatic obstruction with Thulim Laser Enucleation of the Prostate (ThuLEP).
Methods: Patients operated with ThuLEP between 2015 and 2018, in three departments of Urology were included. Each patients had an indication to ThuLEP acording to EAU guidelines. Each of them was controlled for the first month and re‐admitted if a late post‐operative hematuria showed off. A monovariate and a multivariate analysis was conducted to understand if any of the following conditions would have lead to an encreasing risk of bleeding after hospitalization: Age, BMI, Prostate size bigger than 150 ml, Hypertension, non insulin‐depndent diabets mellitus (NIDDM), history of constipation, anticoagulants therapy (early or late bridging), antiaggregant therapy, previous transfusion, ASA status, previous urinary catheter.
Results: 748 patients were included in this study, 52 (6.9%) of them were re‐admitted after the discharge because of gross hematuria (with or without cloths retention). Mean duration of the first hospitalization was 2.1 days while the the mean duration of the re‐admission was 5.6 days. No on of the re‐admitted patiens required a re‐intervention while 46.1% of them had blood transfusion.
We found a statistical significance difference in patient re‐admitted for hematuria if they had NIDDM as a comorbidity (p < 0.05), had a late (i.e. at home and not during hospitalization) bridging of their oral anticoagulant drug with low molecular weight eparin (p < 0.05) and had a clinical history of constipation (p < 0.05).
Conclusions: Bleeding risk of BPO surgery using ThuLEP is less then in other procedures but it is still a concern. Patient with clinical history of NIDDM, constipation and who had a late bridging of their oral anticoagulant therapy are in risk for a late bleeding after ThuLEP.
Post Enucleation Morcellation procedure: Lights and Shadows
L Berti, M Maltagliati, P Marcangeli, A Calori, U Besana, C Buizza, M Sighinolfi, S Micali, BC Rocco, G Bozzini
ASST Valle Olona
Introduction & Objective: To compare clinical intra and early postoperative outcomes after Endoscopic Enucleation of the Prostate (EEP) with different morcellators to treat benign prostatic hyperplasia (BPH).
Methods: This prospective randomized study enrolled consecutive patients with BPH to be treated with EEP (Holep, ThuLEP, ES ThuLEP, VB HoLEP). Three different morcellators where randomizly used thus to divide pts into 3 groups. A for Wolf Piranha, B for Storz drllcut and C for Quanta Cyber Blade. All patients were evaluated preoperatively with regards to blood loss, complications, catheterization time, irrigation volume, hospital stay and operative time.
Results: 312 patients were enrolled. 103 in group A, 107 in B and 102 in C. Patients in each study arm each showed no significant difference in preoperative parameters with main regard to prostatic volume. Compared with A, and B group C had faster operative time (42.54 ± 31.55 minutes, P = 0.04) but not resulted in a less hemoglobin decrease (A vs C and B vs C, p = 0.31 and p = 0.28). The same happened to complication rate which is mostly related to bladder injury morcellation‐related and reflected an higher catheterization time and hospital stay. Despite this Quanta Morcellator had an higher cost per procedure. During the 12 months of follow‐up, the procedures did not demonstrate a significant difference in Qmax, IPSS, PVR, and QOLS.
Conclusions: All the morcellators tested equally allowed a good procedure with and higher efficacy in terms of time for the Quanta which (due to its disposable nature) exposed to higher costs per procedure. Complications are mainly related to operator skill in morcellation procedure than to the device used.
The Gold Standard Technique for Robotic‐Assisted Simple Prostatectomy: A Multi‐Institutional Assessment of Postoperative Urinary Function Outcomes
CU Okoro, M Lee, JY Lee, S Shekar, G Reyes, M Loecher, N Krishnan, AC Harbin, DD Eun
Department of Urology, Lewis Katz School of Medicine at Temple University
Introduction & Objective: Robotic‐assisted simple prostatectomy (RASP) has been readily adopted by robotic surgeons for management of patients with refractory lower urinary tract symptoms (LUTS) and large prostate glands. We assess the degree and durability of postoperative urinary function improvement in patients who underwent RASP using a transvesical technique with a 360° circumferential urethrovesical anastomosis.
Methods: We retrospectively reviewed a multi‐institutional series of patients who underwent RASP by two separate surgeons utilizing a similar technique. The indication for surgery was bothersome LUTS or urinary retention refractory to medical management. The severity of LUTS was assessed using the International Prostate Symptom Score (IPSS) and quality of life (QOL) score. Urinary function outcomes were assessed at 2 weeks, 3 months, 6 months, 9 months, 12 months, 18 months, 24 months and greater than 24 months postoperatively.
Results: A total of 520 patients were identified between May, 2013 and February, 2021. Patient demographics and perioperative outcomes are outlined in Table 1. Mean IPSS and QOL scores improved between 2 weeks and 6 months, with durable results at follow intervals greater than 24 months (Figure 1). Postoperative complications (Clavien Grade >2) were noted in 4.2 % (22/520) of patients. Three patients (0.6%) developed postoperative de‐novo stress urinary incontinence and no patient developed a bladder neck contracture. One patient required reoperation for LUTS.
Conclusions: Robotic‐assisted simple prostatectomy is a safe and effective option for patient with refractory LUTS. Given the durable urinary functional outcomes and minimal complications, we propose this our technique be adopted as the gold standard for RASP.
Outcomes and Complications of bipolar enucleation by prostate size
JN Warner
City of Hope
Introduction & Objective: Bipolar enucleation of the prostate (BipoLEP) is an alternative to holmium laser enucleation of the prostate. Whether pre‐operative prostate size affects BipoLEP outcomes remains unclear.
Methods: We retrospectively reviewed a prospectively collected single‐institutional database of BipoLEPs. We collected demographics, peri‐operative details, complications and patient‐reported outcomes at 6 weeks, 4 months and 1 year post‐operatively.
Results: From 9/2015‐11/2020, 310 patients underwent BipoLEP; 296 had accurate volume data and minimum 4‐month follow‐up. Median pre‐operative prostate volume was 74.5g (range 17‐360g). Patients were analyzed by large (>75g n = 148) versus small (< 75g n = 148) volume. Larger volume patients were older (72 vs. 69; p < 0.05) and were more likely to be in retention (37% vs. 25%; p < 0.05). Patient reported outcomes are detailed in Figure 1. Patients reported similar rates of stress incontinence (any degree) at 4 months (20% large vs. 14% small, p = 0.21). Only 3 patients (2 large, 1 small) requested anti‐incontinence interventions at 1‐year. Bladder neck contracture occurred exclusively in patients with smaller prostates (n = 16, 11%); small volume patients also had more urethral strictures (7% vs. 1%, p < 0.05)
Conclusions: Following BipoLEP, patients with small prostates have higher rates of bladder neck contractures and urethral strictures along with worse IPSS scores and BI's at all time points. Alternative modalities may be considered for smaller glands.
Outcomes Following Surgical Treatment of BPH in Patients with Neurologic Diseases
M Wahba, J Vetter, A Paradis, C Nottingham
Washington University School of Medicine
Introduction & Objective: Clinical outcomes after treatment of Benign Prostatic Hyperplasia (BPH) are poorly defined in patients with neurologic deficits. The efficacy of treatments for BPH may be impacted by presence of comorbid detrusor underactivity in these patients, and the potential for complications such as incontinence may be a deterrent for surgery. We set out to define clinical outcomes for patients with neurologic deficits undergoing BPH treatment.
Methods: We conducted a retrospective review at a tertiary care center of patients with neurologic diseases undergoing surgical treatment of BPH surgery with either laser vaporization or transurethral resection of the prostate. We included patients with a chart diagnosis of cerebrovascular accident, spinal cord injury, myasthenia gravis, and Parkinson's from 2017 through 2019. We performed chi‐squared analysis to compare voiding dysfunction, use of medication, complications, and AUA symptom questionnaires before and after treatment of BPH.
Results: We included 30 patients with a mean follow‐up of 5.7 months. Urinary retention rates (48.3% vs 16.7%, p = 0.009) and use of alpha‐blocker medications (66.7% vs 26.7%, p = 0.002) were significantly lower after surgical treatment. The median American Urological Association (AUA) symptom score decreased from 23 to 19 post‐operatively (p = 0.317), with half of patients experiencing an increase in their score. There was no impact of surgical treatment on infection rates, incontinence, or use of other medications.
Conclusions: Patients with neurologic disorders who underwent treatment of BPH had improvements in urinary retention and use of alpha‐blocker medications. However, there was no significant change in AUA symptom score. Larger studies are needed to determine which patients among this population may derive the most benefit or harm from surgical intervention.
Identifying Predictors of Antispasmodic use Following Robotic Assisted Simple Prostatectomy
JC Dai, TN Morgan, A Garbens, S Kusin, H Trivedi, H Kominsky, CG Roehrborn, JC Gahan
UT Southwestern
Introduction & Objective: Predictors of anticholinergic or beta‐3 agonist use following robotic simple prostatectomy (RASP) are not well established. We describe the rate of anti‐spasmodic use following RASP and identify potential predictors of medication use to better counsel patients pre‐operatively.
Methods: A retrospective review of all RASP patients from 2/2016 ‐ 1/2020 was conducted. Patients with no pre‐operative International Prostate Symptom Score (IPSS) were excluded. Demographic data and pre‐operative clinical characteristics were collected. Post‐operative medication use was determined through electronic medical record review, with at least 1 week of utilization required. Multivariable logistic regression analysis using a priori determined variables was performed to identify independent factors associated with anti‐spasmodic use.
Results: 255 patients underwent RASP at a mean age of 70.0 years ±7.3 and mean BMI of 28.6 kg/cm ±5.0. Median pre‐operative prostate volume was 132.3 cc ±45.0. Rates of pre‐operative diabetes, obstructive sleep apnea (OSA), smoking and alcohol use (≥7 drinks/week) were 19.6%, 6.3%, 3.1%, and 11.8% respectively. Mean pre‐operative IPSS and quality of life scores were 17.6 ± 7.8 and 3.6 ± 1.6, respectively. Median pre‐operative post‐void residual and Qmax were 118 cc (IQR 61‐225) and 8.3 cc/sec (IQR 6.2‐11.8), respectively. 8.6% of patients (n = 22) initiated anti‐spasmodics post‐operatively at a median time of 2.5 months (IQR 1.3‐4.2). These patients were more likely to have a history of OSA than the remainder of the cohort (22.7% vs 5%, p = 0.007). Median duration of anti‐spasmodic use was 6.5 months (IQR 1.7‐14.7). Mirabegron was the most commonly used medication (31.8%). On multivariable logistic regression analysis including history of smoking, diabetes, OSA, alcohol use, BMI, and pre‐operative IPSS score, OSA was independently associated with post‐operative anti‐spasmodic use (OR 8.5, 95% CI 2.12‐34.2, p = 0.003). 68.8% of OSA patients were treated with continuous positive airway pressure (CPAP), but treatment did not appear to impact post‐operative anti‐spasmodic use.
Conclusions: Rates of new anti‐spasmodic use following RASP are comparable to those following other bladder outlet procedures. Patients who are diagnosed with OSA are almost 9 times more likely to require anti‐spasmodic medications following RASP in the short term. These patients may benefit from more tailored pre‐operative counseling.
Surgical Treatment of Large Gland BPH : A Comparison Between ThuLEP and Single Port Transvesical Robotic Simple Prostatectomy
S Talamini, HT Vigneswaran, MJ Zuberek, S Crivellaro
University of Illinois at Chicago
Introduction & Objective: The surgical management of large gland benign prostatic hyperplasia (BPH) can pose significant challenges. In the large gland, guidelines suggest the use of innovative approaches including endoscopic enucleation and robotic simple prostatectomy, traditionally performed using a multiport platform. The daVinci Single Port robot offers a less invasive approach to the simple prostatectomy. We compare our experience using Thulium laser enucleation of prostate (ThuLEP) to the Single Port robotic assisted simple prostatectomy (SP RASP).
Methods: A retrospective review was conducted from 2019 to 2021 of men that underwent SP RASP and ThuLEPs performed by a single surgeon with an enucleation experience of >300 cases. We evaluated preoperative factors such as age, BMI, preoperative prostate medications, IPSS scores, and post void residual(PVR); perioperative measures including operative time, and dry weight of the specimen were recorded; postoperative outcomes including complications, length of foley catheter, IPSS score, urinary incontinence and PVR were recorded. When comparing SP RASP and ThuLEPs, continuous variables were compared using Kruskal Wallace tests. Categorical variables were compared using chi squared tests with two sided p‐values.
Results: In total 16 SP RASPs and 41 ThuLEPs were performed. Median age was 68 years (IQR: 63 – 73), median BMI was 28 (25 – 31), median preoperative PSA was 7.2 ng/mL (IQR: 2.8 – 12.4) and median follow up was 3 months (IQR: 1.3 – 7.0). ThuLEP had shorter operative times (min) (100 vs 175, p < 0.001), smaller specimen weight (g) (46.5 v 80, p = 0.027), and shorter postoperative catheter time (d) (3 vs 7, p < 0.001). SP RASP was associated with fewer postoperative complications such as dysuria, hematuria requiring CBI, and UTI. IPSS reduction was similar between the two procedures. Incontinence rates were less with SP RASP as compared to ThuLEP (5.6% vs 7.3%, p = 0.002). Same day discharge was higher in the ThuLEP group (78% vs 43%).
Conclusions: ThuLEP is associated with shorter postoperative catheter days, decreased operative times, and decreased length of stay (LOS), likely confounded by the initial cases performed on the SP platform, who tended to have longer hospital stays. Subsequent cases have trended towards same day discharge. SP RASP demonstrates improved continence rates, likely a consequence of the bladder neck reconstruction. Though SP RASP is within the initial learning curve at our institution, early results demonstrate the role for this modality alongside ThuLEP in the treatment of large gland BPH.
Pivotal roles of macrophage recruitment and polarization in bladder outlet obstruction
W Wang, K Xiao, H Chen, L Zhou
Introduction & Objective: Partial bladder outlet obstruction (pBOO) is a ubiquitous problem in urology, and lead to significant morbidity in the population. It is characterized by an initial inflammatory response, smooth muscle hypertrophy, exaggerated extracellular matrix accumulation and eventual decompensation to fibrosis. The development of pBOO involve a series of cells and are modulated by complicated molecular networks. Macrophages, the most plastic cells of the hematopoietic system, regulate immunity and are pivotal for tissue repairment. However, the relationship between macrophage and pBOO remains unclear. We established an experimental pBOO rat model to investigate the role of macrophage during pBOO progression.
Methods: Heathy, adult, Sprague Dawley rats underwent surgical creation of a pBOO for either 1, 3, 6 weeks and were compared with sham‐operated rats. Bladder tissue was collected for flow cytometry, quantitative reverse transcription polymerase chain reaction, histology examinations, immunostaining and immunofluorescence assay.
Results: The polarization of bladder macrophages was dysregulated during pBOO development. In the initial stage of pBOO, M1 macrophages were induced and played a leading role (M1/M2 > 4) in eliciting inflammatory.; in the late stage, M2 macrophages were induced (M1/M2 < 0.5) to promote tissue fibrosis. Moreover, our results showed a direct pro‐fibrotic role for M2 macrophage via transition into myofibroblast in a process termed macrophage‐myofibroblast transition (MMT). Co‐expression of M2 macrophages (CD163), myofibroblast antigens α‐smooth muscle actin (α‐SMA) and collagen I identifies the MMT process in the development of pBOO. The number of MMT cells increased with the development of PBOO and accounting for more than 60% of α‐SMA+ collagen‐producing myofibroblasts. Additionally, levels of several cytokines in bladder tissue microenvironment changed with macrophages polarization. Inflammatory cytokines such as monocyte chemoattractant protein‐1, chemokine (C‐C motif) ligand 5 (CCL5), and interleukin (IL)‐1β were significantly increased in the inflammation stage compared with sham group (p < 0.05); While collagen I, collagen III, fibronectin, matrix metalloproteinases (MMP)‐2, tissue inhibitor of matrix metalloproteinase 2 (TIMP‐2) and TIMP‐1 were upregulated in the fibrosis stage compared with sham group (p < 0.05).
Conclusions: In summary, macrophages play a pivotal role in the development of pBOO and might be a key point for elucidating pBOO pathogenesis.
Minimally Invasive Surgical Treatment of Benign Prostatic Hyperplasia: A Systematic Review
A Ting, N Shanmugathas, C Khoo, T El‐Husseiny, H Abboudi
Imperial College Healthcare NHS Trust
Introduction & Objective: Minimally invasive surgical treatments (MISTs) of benign prostatic hyperplasia (BPH) have evolved to offer men daycase care with preservation of urinary continence and sexual function. This systematic review evaluates trends in minimally invasive BPH surgery over the last decade.
Methods: Systematic review (PRISMA) of Embase/MEDLINE databases (2010‐2020). MISTs included Rezum, Urolift, Prostatic Artery Embolisation (PAE), Temporary Implantable Nitinol Device (TIND), Intraprostatic Injection (II), Transurethral Microwave Therapy (TUMT) and Transurethral Needle Ablation (TUNA). The primary outcome was change in urinary function (International Prostate Symptom Score (IPSS)/IPSS‐Quality of Life (IPSS‐QoL)/maximum flow (Qmax)). Secondary outcomes included change in sexual function (International Index of Erectile Function‐5 (IIEF5)), technical failures and complications. Risk of bias was assessed using Cochrane RoB 2.0/MINORS (for randomised/non‐randomised studies, respectively).
Results: 74 studies were included (total: 8,917 patients). The most studied intervention was PAE (36 studies). All interventions offered improvement in urinary function at various points of follow‐up. PAE achieved the greatest improvement in IPSS, IPSS‐QoL and QMax, but also had the largest range of results in every domain. 6 studies reported outcomes ≥48 months (PAE: 2; Rezum, Urolift, TUMT, TUNA: 1); improvements in urinary function were sustained in all. 33 studies across all interventions except TIND and TUMT reported IIEF5 change‐ sexual function was largely preserved (figure 1). Technical failures and Clavien‐Dindo ≥3 complications were rare. Overall, risk of bias was low.
Conclusions: MISTs for BPH are effective and safe. However, there is high clinical heterogeneity within the existing literature. Randomised multi‐arm comparative studies with long‐term urinary and sexual follow‐up are needed to help inform choice. Until then, patients should be carefully counselled based on individual priorities and circumstances.
Minimally Invasive and Endoscopic Therapies of Benign Prostatic Hyperplasia (BPH): Head‐to‐Head Comparison of Short‐Term outcomes by Multiple Treatments (Network) Meta‐Analysis
L Hamed, E Olweny
Rush University Medical Center
Introduction & Objective: There has been a recent explosion in the number of endoscopic and minimally invasive surgical therapies for the treatment of lower urinary tract symptoms related to BPH (LUTS/BPH), with an associated increase in the volume of BPH surgery. However, outcomes for the available BPH surgeries have not previously been compared in head‐to‐head fashion, and we sought to do so using network meta‐analysis.
Methods: We systematically reviewed randomized controlled trials from 1998 to 2018 reporting BPH surgical outcomes in men with moderate‐severe LUTS based on International Prostate Symptom Score (IPSS), maximum urinary flow rates (Qmax) of <15 mL/s and prostate sizes <100 g. Subjects received any of 10 different treatments, i.e. mono‐ or bipolar transurethral resection of the prostate (mTURP, bTURP), aquablation, vaporization, enucleation, transurethral microwave thermotherapy (TUMT), transurethral needle ablation (TUNA), water vapor thermotherapy (Rezum), prostatic urethral lift (PUL) or sham. The primary outcomes were IPSS, quality of life (QOL), Qmax and international index of erectile function (IIEF) scores at 1 year. Multivariable random effects network meta‐analysis was used to compare the treatments using direct and indirect evidence. For each outcome, treatments were ranked from best to worst using the surface under the cumulative ranking curve (SUCRA) method (higher SUCRA = better treatment). Referent treatment was mTURP.
Results: A total of 26 studies with 3,950 patients met inclusion criteria. Relative to mTURP, 1‐year mean IPSS and QOL scores were statistically similar for all treatments except sham, which had a worse QOL score. Mean Qmax was similar for all treatments except TUNA, Rezum, PUL and sham, which had significantly lower flow rates. IIEF data were available for only 7 of the treatments, with mean scores for vaporization, Rezum, PUL and sham significantly better than for mTURP, while those for enucleation and bTURP were similar (Figure). By SUCRA, the treatment with the highest probability of best urinary function was enucleation, while that with the highest probability of best sexual function was Rezum.
Conclusions: Compared with mTURP, Rezum and PUL achieved inferior flow rates but better IIEF scores, while vaporization achieved similar flow rates and higher IIEF scores. These findings may be of value in patient counseling regarding surgical outcomes of LUTS/BPH therapy.
First comminution of stones in humans by burst wave lithotripsy
JD Harper, JE Lingeman, I Metzler, RM Sweet, P Sunaryo, JC Williams, AD Maxwell, J Thiel, B Cunitz, B Dunmire, MR Bailey, M Sorensen
University of Washington School of Medicine
Introduction & Objective: We report stone comminution in the first human subjects by burst wave lithotripsy (BWL), which is the transcutaneous application of focused, cyclic ultrasound pulses.
Methods: This is a prospective multi‐institutional feasibility study recruiting subjects undergoing clinical ureteroscopy (URS) for at least one stone ≤12 mm on computed tomography (CT). During the planned URS, BWL is administered with a handheld probe, and any stone fragmentation and tissue injury are observed. Up to 3 stones can be treated, each for a maximum of 10 min to be respectful of operating room time. The primary effectiveness outcome is the volume percent comminution into fragments ≤2 mm, where fragment volume is determined by μCT of basketed fragments or image processing of the URS video using the laser fiber as a size reference. The primary safety outcome is independent, blinded grading of tissue injury from the video.
Results: Comminution data to date are from 6 female and 6 male subjects with an average BMI of 25 ± 5 kg/m2 and average age of 57 ± 15 years. Overall, 13 of 15 stones were comminuted with BWL (Table 1). In 8 of 15 cases, ≥85% of the stone was comminuted to fragments ≤2 mm in under 10 min. One stone in the distal ureter was 87% comminuted after 4 min before passing into the bladder. Seven stones were <85% comminuted, potentially because of their size ( > the beam width or < the acoustic wavelength), composition, structure, or the introduction of air by URS that shielded the stone from BWL. Figure 1 shows fragments from the 20% comminuted stone and tissue around the 99% comminuted stone. Only mild reddening with some hematuria was observed ureteroscopically.
Included in the tissue observations were 2 additional BWL‐treated subjects where the stone identified on CT was determined to be most likely submucosal on URS. For another additional BWL‐treated subject, fragments were noted, but the URS video did not record for comminution or tissue measurement.
Conclusions: The first study of BWL in human subjects resulted in an average of 63% comminution of stones into fragments ≤2 mm within a treatment time of only 10 min and with only mild tissue injury.
Comparison of Laparoscopic Pyelolithotomy versus Percutaneous Nephrolithotomy for the Treatment of patients with Staghorn Kidney Stones referred to Labbafinezhad hospital in 2019; a randomized clinical trial
M Soltani, S Farshid, R Valizadeh, N ahmadian
Introduction & Objective: Percutaneous nephrolithotomy is a standard treatment for Staghorn kidney stones but due to parenchymal damage and the possibility of pseudoaneurysms and severe hemorrhage, selective alternative to low invasive alternative such as laparoscopy was considered to compare therapeutic results and complications with percutaneous nephrolithotomy.
Methods: This study was a parallel randomized clinical trial study. 68 Patients with Staghorn stones (one‐piece or maximally two‐pieces stones with large extra renal part) over 18 years were Included in this study. The patients were randomly divided into two equal groups of laparoscopic Pyelolithotomy and PCNL using random allocation software. The primary outcome was the success rate of stone free rate, And Secondary outcomes were pre‐operative creatinine, post‐operative creatinine, duration of surgery, bleeding, fever, post‐operative pain, length of hospital stay, pre‐operative hemoglobin and post‐operative hemoglobin. Independent t‐test or Mann‐Whitney test were used to compare quantitative variables between the two groups.
Results: The mean age of patients in PCNL and laparoscopic Pyelolithotomy groups was 48.50 ± 13.33 years and 52.17 ± 15.74 years, respectively (p = 0.303). Laparoscopic Pyelolithotomy strongly had longer surgery time (196.55 ± 26.58 minutes) than PCNL group (110.88 ± 34.82 minutes) (t = ‐11.404, p = 0.001). Regarding high grade clavien complications( III‐V), the results showed no significant differences between two groups . Regarding hemoglobin decrease, the patients in the PCNL group showed more Hb decrease (‐2.6676 ± 2.61 g/dl) compared to the Laparoscopic Pyelolithotomy (‐0.7912 ± 1.06 g/dl) (t = ‐3.852, p = 0.001). )Stone free rate was observed in 76.5% (n = 26) of patients in laparoscopic Pyelolithotomy group, which was significantly higher than the PCNL group (n = 17) (p = 0.043).
Conclusions: Given that during the laparoscopy the entire pyelocalyceal system is accessible, it is possible to remove the stone completely, but in PCNL surgery it may require multiple accesses to remove the stone in a single session. Also, according to the results, laparoscopic Pyelolithotomy had more stone free rate accompanied with low hemorrhage requiring transfusion compared to PCNL procedure for single piece staghorn stones with large extra renal part.
Complications after 4,500 flexible ureteroscopy (academic single center experience)
BF Geavlete, R Multescu, C Ene, C Bulai, PA Geavlete
“Saint John” Emergency Clinical Hospital, Department of Urology
Introduction & Objective: Nowadays flexible ureteroscopy became a routine procedure utilized all‐around of the world. The aim of this study was to evaluate the indications, limits and efficacy of flexible ureteroscopy on a significant number of cases and on a long follow‐up period.
Methods: The procedures were performed by three surgeons, between January 2003 – January 2019 and involved 7 types of flexible ureteroscopes: Storz 11274AA, Storx Flex‐X, Storx Flex‐Xc, Storz Flex‐Xc2, Olympus URF‐P5, Olympus URF‐V, Olympus URF‐V23000. We retrospectively reviewed the indications, endoscopes' types, procedural efficacity and complications rates.
Results: Overall complications occurred in 18.9% of the procedures. Septic complications (ranging from fever to septic shock) occurred in 12.1% of the cases, most of them being mild. In this complications category, 69% were Clavien II, 16% Clavien IIa, 10% Clavien IVa and 5% Clavien IVb. Mortality was 0% in this group. 51.9% of the septic patients were pre‐stented, and only 25% of them were operated using a ureteral access sheath. In 6.8% of the cases non‐septic complications (severe upper urinary tract wall lesions, postoperative pain, persistent hematuria, liquid retroperitoneal extravasation, intrarenal or subcapsular hematoma) were encountered. No Clavien V cases were encountered in this group either. Ureteral access sheath was used in 78% of the non‐septic complications group. During the diagnostic procedures inspection of the entire upper urinary tract was possible in 90% of the cases (2,700 patients). Stone free rate in lithiasis cases was 93.3% after one procedure, 95.2% after the second and 97.3% after the third one. In 22 cases intraparenchimatous (5 cases) or subcapsular hematoma (17 cases) were diagnosed during the postoperative period, while 3 cases presented massive liquid extravasation of the fluid in the retroperitoneum. Regarding the use of ureteral access sheath, in 4.8% of the cases we encountered grade 2 and 3 ureteral wall injuries.
Conclusions: Retrograde flexible ureteroscopic approach is an efficient diagnostic and treatment method for renal pathology. Also the complication rate is relatively reduced, but a serious training is indicated before using this device.
Role of stone size, stone density, and skin‐to‐stone distance by non‐ contrast computed tomography abdomen in predicting success of shock‐wave lithotripsy for kidney stones
A Hamid, A Ahmad, N Choh, S Malik, R Khawaja, M Wani
Department of Urology, SKIMS, Srinagar, Kashmir, India
Introduction & Objective: Shock‐wave lithotripsy (SWL) is a minimally invasive treatment procedure for kidney stones, commonly employed as one of the first line therapy for properly selected renal and ureteric stones. Multiple factors influence the outcome of shock‐wave lithotripsy and assessment of certain CT characteristics of the these stones prior to the procedure can help in predicting outcome of shock‐wave lithotripsy. The aim of this study was to assess the influence of these factors in predicting the outcome of shock‐wave lithotripsy for kidney stones.
Methods: Between March 2016 and June 2018, 96 patients who underwent shock‐wave lithotripsy for renal or proximal ureteric stones at our centre were included in the study. The CT characteristics of the calculi, shock‐wave lithotripsy settings applied, and the final outcome observed were recorded in a proforma and subjected to statistical analysis.
Results: There were 58 (60.42%) males and 38 (39.58 %) females in the study. The age of patients varied from 18 to 72 years with a mean of 36.4 ± 13.8 years. Majority of patients 69 (71.88%) had renal (non‐lower pole) calculi while 27(28.12%) had upper ureteric calculi. Stone size varied from 7.4 mm to 20.0 mm with a mean of 13.1mm ±3.8 mm. The stone density ranged from 536 HU (Hounsfield unit) to 1232 HU with a mean of 826.3 ± 194.3 HU. The mean skin‐to‐stone distance (SSD) varied from 5.58 – 12.5 cm with a mean of 8.84 ± 1.92 cm. Complete stone fragmentation was observed in 65 (67.70%) patients after first session; 16 (16.67%) after second session and 7 (7.30%) after third session. However, 8 (8.33%)patients had failure of shock‐wave lithotripsy and needed alternative treatment. Overall success rate of 91.67% (88/96) was observed. The mean number of shock‐waves required to achieve complete stone fragmentation was observed to increase with the increased stone size and stone density, however, stone density had more significant influence than stone size and mean SSD.
Conclusions: From the study it was concluded that the use of NCCT‐KUB for determining the stone size, stone density, and skin‐to‐stone distance of kidney stones before shock‐wave lithotripsy helps in predicting treatment outcome. The combination of these factors helps to identify ideal candidates for shock‐wave lithotripsy. The increase in mean skin‐to‐stone distance is associated with an increase in the number of shock‐wave lithotripsy sessions required as well as an overall decreased success rate. However stone density appears to be more significant than stone size and skin‐to‐stone distance in predicting fragmentation of kidney stones with shock‐wave lithotripsy.
Upper Urinary Tract Stones: Evolution of Surgical Management Trends in Germany, France and England over the Past Decade
BW Turney, C Demaire, S Klöcker, H Sommerfeld, O Traxer
University of Oxford, Nuffield Department of Surgical Science, Department of Urology, Churchill Hospital
Introduction & Objective: Global Upper Urinary Tract (UUT) stone prevalence is rising. As a consequence, the increased service demand on hospitals may be difficult to manage, increasing the burden on healthcare providers (HCPs) as well as on patients. In this European analysis we explore the evolution of stone diagnoses and surgical procedures in Germany (DE), France (FR), and England (EN) over the past ten years.
Methods: We identified the codes related to UUT stones diagnoses using the International Classification of Diseases (ICD‐10) and extracted procedure counts for Extracorporeal Shock Wave Lithotripsy (ESWL), Ureteroscopy (URS), Percutaneous Nephrolithotomy (PCNL) and Open Surgery (OS). We used procedure codes from the National databases in DE, FR and EN, and analyzed the hospital diagnosis counts versus surgical procedure counts related to UUT stones from 2010 to 2019.
Results: Between 2010‐2019, the ICD‐10 N20 codes for calculus of kidney and ureter increased by 8%; 26% and 15% in DE, FR, EN respectively, whereas stone procedures increased by 3%; 38% and 18%.
Over time the dominant surgical UUT stone procedure shifted from ESWL (49‐60% of all procedures in 2010) to URS (51‐75% of all procedures in 2019). PCNL and OS represent <5% of UUT stones procedures in FR and EN. The highest use of PCNL is observed in DE (increase from 7% in 2010 to 11% in 2019).
Over the past decade, the overall length of stay (LoS) decreased for all procedures across the three countries. The URS average LoS decreased by 21% in DE; 37% in FR and 6% in EN. Daycase stone procedures volume increased in FR by 68% and in EN by 23%. In DE most cases involve at least one overnight stay.
Conclusions: This analysis confirms the rise in stone prevalence globally, including an increase in UUT stones diagnoses and surgical procedures in DE, FR, EN over the past decade.
The dominant surgical procedure to treat UUT stone has shifted from ESWL to URS, and the average LoS has decreased. These observed trends may be due to clinical advantages, technological advancement as well as, other factors such as HCP preference or costs.
The continued rise of UUT stone prevalence has implications for patients, HCPs and hospitals. If we add to that the COVID19 repercussions, solutions to optimize workforce planning, service delivery and length of stay could help to address the situation.
The effect of smaller residual stones after minimal invasive endourology procedures for renal stones: prospective study
N Iqbal, A Hasan, S Imtiaz Ali, S Akhter
PKLI, Lahore, Pakistan
Introduction & Objective: The new era in urology with the advent of minimally invasive surgical techniques has helped in reduction of morbidity associated with surgical treatment of renal stones. Nevertheless, there is lack of agreement as to what has to be done to residual stones, as it has been known that these fragments might have the potential to cause complications after these elective procedures. The objective of our study was to evaluate the natural course followed by residual stones after percutaneous nephrolithotomy (PCNL) or flexible ureterorenoscopy (F‐URS) procedures for treatment of kidney calculi.
Methods: Total of 373 patients were submitted to prospective follow‐up after elective endoscopic procedures such as PCNL and URS for treatment of kidney stones. The presence and features of residual fragments was followed on radiologic scans and the frequency of revisiting hospital for complications or the necessity of additional procedures were sorted out.
Results: The overall stone‐free rate was 76.3% in F‐URS and 67.7% in PCNL. The natural history of 257 patients having residual stone fragments was followed. There was spontaneous passage of these fragments in 13.4% (34) of cases. While 18.2% (47 patients) developed pain or colicky symptoms, 10.5% (26 patients) had complications such as readmission for pain, fever and Urinary tract infection. Total of the 257 patients followed, 16.7% (43 subjects) needed a next surgical procedure. The residual stones larger than 4mm had more complications (p < 0.003), more recurrence of pain symptoms (p = 0.04) and need for additional surgeries (p < 0.002) as compared to the stones of smaller than 4mm in size. Number of the residual fragments even less than 4 mm were more prone to the complications. Size and number of the residual fragments and the multi‐calicial distribution were strong predictors of the development of new symptoms and the need of surgical re‐intervention. (p = 0.04).
Conclusions: Residual stones are frequently seen in endourological procedures for renal stones treatment and might cause morbidity and complications. Number of stone fragements and poles involved have role in these complications. More multicenter prospective studies are needed in this regard.
Total Power is the Most Important Factor Determining Efficiency in Treatment of Large Bladder Stones
M Hajiha, AS Amasyali, M Keheila, J Groegler, A Goyne, D Baldwin, JD Belle, DD Baldwin
Loma Linda University, Department of Urology
Introduction & Objective: Surgeons have a wide array of technology to choose from during laser cystolitholapaxy. Recently, the Lumenis 120W holmium laser with Moses technology and the Olympus 60W thulium laser have been shown to treat renal and ureteral stones efficiently. The purpose of this study was to compare the efficacy and cost of four different holmium laser platforms with the 60W thulium laser in the treatment of a 4cm bladder stone in a benchtop model.
Methods: In a simulated laser cystolitholapaxy, 25 identical 4 cm BegoStones (CaOx monohydrate consistency) were placed on a 5.3 x 5.3 mm mesh in a 3D printed bladder model and fragmented using one of five different laser platforms. The platforms used were the 30W Dornier at 2.5 J/8 Hz (20W), the 100W Olympus Empower at 3.3 J/30 Hz (99W), the Lumenis P120H laser without Moses contact setting at 4 J/30 Hz (120W), the Lumenis P120H with Moses contact setting at 4 J/30 Hz (120W), and the Olympus Soltive Premium TFL 60W at 3J/20 Hz (60W). All lasers were operated at maximal energy using a 550 μm fiber. The cost of the lasers, laser fibers, and procedure time per laser multiplied by the mean cost of OR time ($37/min) were used to model cost effectiveness. ANOVA and Tukey's B post‐hoc analysis were used to compare outcomes.
Results: The Moses laser required less mean lasering time (60.85 min) compared to all other groups (conventional 120W (69.41) min, 100W (79.18 min), TFL 60W (256.3 min), 30W (281.2 min); p = 0.000). Similarly, overall operating time with the Moses laser (68.3 min) was less compared to all others (conventional 120W (86.73 min), 100W (102.8 min), TFL 60W (261.4 min), 30W (297.5 min); p = 0.000). While the 100W and TFL 60W lasers required fiber stripping only 1 and 1.4 times, the Moses, conventional 120W and 30W laser fibers required mean fiber stripping 6.0, 7.8, and 17.4 times, respectively (p = 0.000). Use of the Moses technology would result in an estimated cost savings of $522, $820, $8023 and $6764 per case compared to regular 120W, 100W, 30W lasers and TFL 60W, respectively. When factoring in purchase price, the P120 with Moses became cost effective after 140 cases compared to the 100W laser and only 22 cases in comparison to the 30W laser.
Conclusions: Total power is very important when treating large bladder stones. Based on our model, the Moses contact laser at 120W setting would be the most cost effective in a high volume stone center due to a much shorter operative time. The 100W laser was cost effective in low to moderate volume centers, while lasers with less than 100W of energy are probably not ideal for treating large dense bladder stones.
Effect of Low‐Energy Shock Wave Therapy on Behavioral, Histopathological and Molecular Changes in a Rat Model of Epirubicin‐Induced Cystitis
AH Elkashef, N Barakat, S Khater, A Awadalla, M El‐Ghar, A El‐assmy, K Sheir, A Shokeir
Department of Urology, Urology and Nephrology Center, Mansoura University, Egypt
Introduction & Objective: Epirubicin (EPI) has commonly been used as an adjuvant intravesical therapy for the treatment of non‐muscle invasive bladder cancer (NMIBC). However, its frequent instillation is mainly complicated with cystitis. Low‐energy shock wave therapy (LESW) has been shown to have both anti‐inflammatory and analgesic effects, so we evaluated the effect of LESW on the bladder inflammatory changes associated with EPI‐induced cystitis in rats.
Methods: Thirty female Fischer rats were randomly allocated into 3 groups (10 rats each); Control, EPI and EPI plus LESW groups. Saline (0.6 mL) or EPI (0.6 mg/0.3 mL added to 0.3 mL saline) was instilled and retained in the bladders for 1 hour. LESW treatment (300 pulses, 0.12 mJ/mm2) was applied simultaneously to the bladders in EPI plus LESW group. This was repeated daily for 1 week. Behavioral assessment of pain, eye movement and locomotion was performed 1 hour after instillation. Magnetic resonance imaging (MRI) was also carried out. After sacrification, bladders were harvested for bladder weight estimation, histopathological examination and molecular studies of interleukin (IL)‐6 and tumor necrosis factor (TNF)‐α relative gene expression levels.
Results: LESW significantly improved pain, eye movement and locomotion scores, reduced bladder weights and down‐regulated IL‐6 and TNF‐α expression levels (Table 1). MRI of EPI plus LESW group showed that bladder wall thickness was 0.73 ± 0.25 mm vs. 1.64 ± 0.27 mm in EPI group (p < 0.001) and bladder capacity was 8.7 ± 1.53 μL vs. 5.07 ± 1.31 μL in EPI group (p < 0.001). Yet, there was no significant difference regarding the degree of bladder inflammation between EPI and EPI plus LESW groups (Table 2).
Conclusions: LESW suppresses the bladder inflammatory changes induced by intravesical instillation of EPI, so LESW might be nominated as a promising method for relieving bladder inflammation associated with EPI instillation for the treatment of NMIBC.
Short chain fatty acids reduce renal calcium oxalate stones by regulating oxalate transporters SLC26A3/6 in intestine
Y Liu, X Jin, Y Ma, Z Jian, L Zhou, L Xiang, Q Sun, H Li, K Wang
Introduction & Objective: The prevalence of renal stones is increasing rapidly. The most common component of stones is calcium oxalate (CaOx). High urinary oxalate is a risk factor for CaOx stones. In the gut, the oxalate is secreted by oxalate transporter SLC26A6, and absorbed by SLC26A3. We previously found that the relative abundance of bacteria which produced short chain fatty acids (SCFAs) was lower in the gut microbiota of renal stone patients than healthy people. SCFAs are products from bacterial fermentation of dietary fiber, which had beneficial role in chronic metabolic diseases. The aim of this study was to explore the effect of SCFAs on the formation of renal CaOx stones and demonstrate the involvement of intestinal oxalate transporters in oxalate metabolism.
Methods: Twenty five rats were equally divided into five groups, named control group, model group, acetate group, propionate group and butyrate group. 1% (v/v) ethylene glycol (EG) was added into the drinking water to develop renal CaOx stone model rats. The drinking water of the latter three groups had extra sodium acetate, sodium propionate or sodium butyrate, respectively. Renal crystals were examined using Hematoxylin Eosin (HE) and Von Kossa (VK) staining. The urinary oxalate was measured by liquid chromatography‐mass spectrometry. The gut microbiota was analyzed through 16S rRNA gene sequence. The expression of SLC26A3/6 was measured by quantitative real‐time polymerase chain reaction and western blot.
Results: HE and VK staining showed that there were plenty of crystals in the kidney. Renal crystals reduced after the administration of acetate, propionate or butyrate. The level of urinary oxalate also reduced in rats receiving acetate, propionate or butyrate. The expression of SLC26A3 in the cecum was higher in model group than in control group. It decreased after the administration of acetate, propionate and butyrate. Acetate and propionate increased the SLC26A6 expression in small intestine. Additionally, the relative abundance of Lachnospiraceae, Ruminococcus, Eubacterium and Prevotellaceae were higher in rats receiving acetate, propionate or butyrate, which could produce SCFAs.
Conclusions: SCFAs could reduce urinary oxalate and renal CaOx stones by increasing intestinal SLC26A6 and decreasing SLC26A3 expression. It may provide a new strategy for preventing the occurrence and recurrence of renal CaOx stones.
Extracorporeal shockwave lithotripsy: a good option for treating distal ureteric stones
G Celentano, M Creta, G Cancelmo, F Mangiapia, M Marsicano, M Capece, R La Rocca, G Califano, C Collà Ruvolo, L Napolitano, S Morra, C Turco, C Imbimbo, V Mirone, N Longo
University of Naples Federico II
Introduction & Objective: Extracorporal shock wave lithotripsy (ESWL) is a great option for the treatment of kidney stones but has been accepted worldwide as a reasonable approach to ureteric stones. It is a non‐invasive procedure that uses shock waves to break up stones so they can easily pass through the urinary tract. The recent EAU guidelines state that the ESWL is an appropriate treatment if active stone removal is indicated. The aim was to assess the efficacy of ESWL on distal ureteric stones.
Methods: Between January 2018 to December 2020, 146 patients with monolateral, single, radiopaque and distal ureteric stones without hydronephrosis or with mid or mild hydronephrosis without an acute colic and good renal function underwent ESWL. The stones were identified using the X‐ray guidance (fluoroscopy).
Stone parameters such as size, Hounsfield unit and peri‐operative outcomes like pain (VAS score), complications and stone‐free status were evaluated. A pragmatic view was taken on stone free status, with either Xray or CT, depending on the clinical situation, used to determine this.
The stone‐free status was defined as no residual fragments of any size. Treatment failure was defined as the failure to become stone‐free within 3 months.
Results: The mean stone size was 0.9 cm (0.5– 1.5mm). The frequency of the shockwaves was 120 shocks/min and the mean (range) number of shockwaves delivered during each treatment session was 3200 (2800–4500).
One hundred and twenty three patients (84.2 %) passed the stones and were completely stone free after the treatments.
In 61/123 cases (49.5%), one ESWL session was sufficient to achieve complete stone clearance, while in 52/123 cases (42.2%) and in 21 cases (17,0 %), two and three treatment sessions were required, respectively.
Twenty three patients (15,7 %) required a rigid ureteroscopy for being rendered stone free after a failed ESWL
In 15 cases mild pain was reported. Eleven patients were admitted due to a renal colic and were stented with a double J stent.
No patients required the nephrostomy insertion.
Conclusions: The shock wave lithotripsy could be a valid option for treating ureteric stones once they are visible with the lithotripter. It is safe and not invasive with a small amount of complications. It is not invasive and avoids the general anaesthetic reducing morbidity.
External shockwaves lithotripsy a multi‐institutional international study
M Sighinolfi, M Benedetti, T Calcagnile, A Cassani, M Amato, G Saraceni, N Ferrari, G Bozzini, z ahmed, E Ahmed, E Ahmed, D Cosimo, A Nacchia, P Fedelini, F Chiancone, S Ferretti, p Curti, G Bianchi, BC Rocco, S Micali
Azienda ospedaliero‐universitaria di Modena e Reggio Emilia, Modena, Italy
Introduction & Objective: ESWL is a minimally invasive treatment for small‐medium size urolithiasis. EAU guidelines recommend either ESWL, RIRS and PNL for 10‐20 mm renal stones. ESWL success rate rely on several factors: stone size, location, density, patients' characteristic (BMI) and lithotripter specimens. Endourology advance in technology and procedures decreased the ESWL rate in favor of surgical treatment especially RIRS. The aim of this study is to highlight the role of ESWL in a contemporary series of patients with a single 10‐20 mm renal stone.
Methods: ESWL data were collected prospectively from 6 Italian centers (“Sant'Andrea” Rome, AORN “A. Cardarelli” Naples, “Mater Salutis” Verona, “Maggiore” Parma, University of Modena and Reggio Emilia and Tanta University). We performed a retrospective observational study of data. Inclusion criteria was single renal 10‐20mm stone treated with ESWL. Patients' characteristic analyzed were age, gender, comorbidities, previous surgery, concomitant UTI and stone features (size, location, HU density, stone to skin distance, hydronephrosis). Primary endpoint was stone free rate (SFR: absence of clinically significant residual fragment at 3 months and need for auxiliary procedure); Secondary endpoint was a regression analysis of factors impacting SFR. Data were analyzed with SPSS; after a descriptive analysis, T test for unpaired sample and non‐parametric test (correlation, chi square test) were applied.
Results: 700 patients with a single renal stone were included (440 M, 260 F). Mean age 50,7 yr. (range 18‐96, SD 15). Mean stone size 12,6 mm (range 10‐25, DS 2,8); mean HU density 832 (260‐1643), mean stone to skin distance 89 mm (range 51‐160, SD 16,3). 182 patients had previous renal surgery; 14 patients had a concomitant UTI requiring antibiotic therapy. Renal stone location was pielic in 303 (43%), lower caliceal in 177 (25%), upper and middle calyx in 220 (32%). Pre‐treatment hydronephrosis was evident in 213 (30%). SFR at 3 months was 88,4% (630); of SFR patients, 54,8% were SF after 1 session, the remaining had repeated treatment (21,6% had 2, 17,6% had 3, 10% had ≥4). HU density (p = 0.00) and number of sessions (p = 0.04) were the covariates significantly related to SFR. No major complications occurred.
Conclusions: Our study confirmed the efficacy of ESWL treatment for 10‐20mm renal stones with high success rates. Eligible patients should be counseled on the possibility of repeated sessions, balanced by safety and outpatient feature ‐ without the need for OR availability – particularly fitting the current pandemic scenario.
Is extracorporeal shock wave lithotripsy (ESWL) still suitable for >1.5cm intrarenal stones? Data Analysis of 1902 ESWLs
M Pachecco, E Soares Morales, R Nardi Pedro, L O. Reis, W Azal Neto, L Castro Santos
Endourology Staff UNICAMP, AME/SBO Lithotripsy Center Coordinator, Professor Faculdade São Leopoldo Mandic, Medicine.
Introduction & Objective: According to the AUA and EAU guidelines, ESWL is the least invasive treatment option for stones smaller than 2 cm. However, it is well known that SWL stone‐free rates (SFR) decline as stone size increases. We sought to evaluate whether the size limit of 1.5cm could be a better predictor of success after a single ESWL session than current recommendations.
Methods: Data from an ESWL‐dedicated center were prospectively scrutinized according to stone locations and sizes. Information on patient's demography, lithotripsy parameters, and outcomes was evaluated by multivariate analysis among 1902 consecutive ESWLs.
Results: The overall SFR was 70.8% (1347/1902). SFRs according to Stone size Groups were <1cm: 73.7% (825/1118), 1‐1.5cm: 70.4% (401/569) and >1.5cm: 56.2% (121/215); and according to Stone location groups were lower pole (LP): 64.4% (398/618), mid pole (MP): 73.8% (339/459), upper pole (UP): 73.7% (273/370) and renal pelvis (Pelvis) 74.1 % (337/455). Multivariate analysis revealed better SFR in <1cm and 1‐1.5cm groups (p = 0.000001, p = 0.0003 respectively) and non‐LP groups (p = 0.004).
Conclusions: ESWL is an effective treatment modality for kidney stones with SFRs up to 74.8% for stones <1cm. Patients with stones >1.5cm or >1cm located in LP show significantly lower SFRs after a single ESWL session.
The benefit of obtaining 24‐hour urine testing before prescribing preventive pharmacological therapy to patients with high‐risk urinary stone disease
R Hsi, P Yan, J Crivelli, V Shahinian, JM Hollingsworth
Vanderbilt University School of Medicine
Introduction & Objective: Recent studies show no benefit to a selective approach to preventive pharmacological therapy (PPT) for patients with urinary stone disease (i.e., obtaining 24‐hour urine testing before prescribing). However, these studies estimated the average treatment effect of selective PPT. Because selective PPT may produce nonrandom differences in outcomes across patients based on individual recurrence risk, we compared the frequency of stone‐related events among patients with and without 24‐hour urine testing before PPT use in high‐risk subgroups.
Methods: Using medical claims data (2008 to 2019), we identified working‐age adults with urinary stone disease who had a prescription fill for a thiazide diuretic, alkali therapy, or allopurinol. We stratified them into subgroups based on the presence of a concomitant condition or other factors that raise stone recurrence risk (children, urinary tract infection, gout, bone disease, intestinal malabsorption, hyperparathyroidism, staghorn calculus, renal anomalies, sarcoidosis, cystinuria, and prior stone recurrence). We fit multivariable regression models to compare the frequency of a stone‐related event (emergency department visit, hospitalization, and surgery) among patients with and without 24‐hour urine testing before PPT prescription in these subgroups.
Results: Among 5,275 patients with urinary stone disease who had a concomitant condition or other factor raising their recurrence risk, 37% (n = 1,954) were prescribed PPT after 24‐hour urine testing (median follow‐up, 631 days), while 63% (3,321) received PPT empirically (median follow‐up, 623 days). Patients with prior stone recurrence had a significantly lower hazard of a subsequent stone‐related event if they received selective PPT (hazard ratio, 0.83; 95% confidence interval, 0.71 to 0.96). The adjusted predicted probability of a stone‐related event among patients in this group was five percentage points lower at two years of follow‐up for those on selective versus empiric PPT. No significant associations were noted for selective PPT in the other high‐risk subgroups.
Conclusions: Patients with a history of recurrent urinary stone disease benefit from PPT when guided by findings from 24‐hour urine testing. These data highlight the importance of examining for heterogeneity in treatment effect when comparing stone prevention approaches.
Shockwave Lithotripsy for Distal Ureteric Stones ‐ Results from the Endourological Society T.O.W.E.R. Research Initiative
F Gabrigna Berto, H Razvi, J Bjazevic, VK Wong, L Nott, M Hossny, R Dasgupta, PJ Osther, BW Turney, BH Chew
Western University
Introduction & Objective: Clinical practice guidelines for the treatment of distal ureteral stones are varied. The American Urological Association (AUA) guideline recommends ureteroscopy (URS) as first line treatment while the European Association of Urology (EAU) lists both URS and shock wave lithotripsy (SWL) as potential first line options for stones ˂10mm. Various factors influence stone free rates in SWL patients therefore, patient selection is key. The objectives of this study were to evaluate stone free rates and to identify factors predictive of treatment failure in patients undergoing SWL for distal ureteric stones in four centers from the Team of Worldwide Endourological Researchers (TOWER) from the Endourological Society.
Methods: Consecutive patients undergoing SWL with the Storz SLX‐F2 lithotripter as initial treatment for distal ureteric calculi at four institutions (United Kingdom, Oman and two centers in Canada) were retrospectively reviewed. Treatment success, defined as clearance of the treated stone, was assessed by post‐operative imaging using computerized tomography, plain film x‐ray or ultrasound. Descriptive statistics were used to analyze patients' pre‐operative and post‐operative characteristics. Comparison of means was utilized to assess for predictors of treatment failure.
Results: 384 patients with distal ureteric calculi were treated between October 2011 and November 2020. Mean age was 51.24 years (±15.75) and 67.7% were male. Mean body mass index (BMI) was 28.03 (±5.05 Kg/m2). Mean stone size was 6.51mm (±2.54mm). 83.1% were treated in the supine position and 48.7% of stones were left sided. 236 patients (69.6%) were considered stone free on post‐operative imaging. 38 patients (11.2%) underwent a second procedure (32 URS and 6 repeat SWL). In 64 patients, treatment success was not known and for analytic purposes were assumed to have failed treatment (intent to treat). Patients who failed SWL were older (mean 54.37 ± 15.91 vs. 50.5 ± 15.87), p = 0.036, 95%CI, and had larger stones (7.12 ± 2.85 vs. 6.23 ± 2.19), p = 0.002, 95%CI). Those that failed treatment had a mean larger stone size of 0.89 mm. BMI, gender, total energy, number and frequency of shocks and were not statistically significant.
Conclusions: SWL for distal ureteral stones is an effective treatment option. In this analysis, larger stone size and older patients were predictive of treatment failure and this should be taken into account when counselling patients about their treatment options. SWL should be considered a first‐line option for stones ∼6mm with a 69.6% chance of success.
How Necessary is Post‐Operative Ultrasound Imaging for Ureteroscopic Stone Procedures?
N O'Connell, C Ashley, Z Yasen, R Peggs, J Stephenson, T Tien, R Oliver, P Pal, S Graham
Barts Health NHS Trust
Introduction & Objective: Ultrasound sonography (USS) is a cheap, radiation‐free modality used to diagnose hydronephrosis following ureteroscopic stone procedures for the purpose of detecting potential renal obstruction due to stones or strictures. At our centre there is no protocol for imaging following ureteroscopic stone procedures. We aim to assess the use and efficacy of post procedure USS and outcome in this patient group.
Methods: A retrospective analysis was carried out of 100 consecutive patients who underwent ureteroscopic stone procedures at our teaching hospital in London, UK from the beginning of January 2017 onwards. We reviewed modality and timing of post procedure imaging for the detection of hydronephrosis as well as outcome.
Results: There were 94 patients (6 excluded as solely percutaneous procedures). 31 had semi‐rigid ureteroscopy, 61 had flexible ureteroscopy and 2 had flexible ureteroscopy with percutaneous nephrolithotomy. 57 were left sided, 34 right sided and 3 bilateral. 33 patients were female and 61 were male. Mean age was 52. Average time from operation to USS was 8.4 weeks. 76.6% of patients had USS as the initial post‐operative imaging modality. Sonographic evidence of hydronephrosis was present in 12 of these patients (16.7%) and half of them went on to have CT Urinary Tract (CT). 83% had persistent hydronephrosis on CT (5 patients). Of these, 2 required further procedures for stones and 3 had repeat imaging showing resolving or ‘mild’ hydronephrosis, no further procedures and were discharged to primary care. There were no cases of ureteric stricture reported. 16 patients had a CT rather than USS as their initial post‐operative imaging modality (17%) and 3 had no imaging at all (3.2%). In 44 cases USS was the single modality used throughout the entire treatment episode (46.8%). Outcome as of February 2020 is as follows: 55.3% discharged to primary care (+/‐USS surveillance), 27.7% under urology follow up for stones, 5.3% under urology for other issues, 5.3% lost to follow up, 4.3% did not attend follow up/self‐discharge, 2.1% deceased (for other reasons).
Conclusions: The majority of our patients had USS as the initial imaging modality post ureteroscopy. A small proportion had hydronephrosis and of them none had ureteric strictures but required either further imaging and/or procedures for residual stones. Routine use of USS post ureteroscopy is beneficial both economically and in terms of diagnostic yield as early identification of a potential silent obstruction that requires further imaging is easily achievable and also allows for reassurance in discharging the negative group without exposure to radiation and the higher cost of CT.
Using Artificial Intelligence to Identify Stones on SWL Intra‐Operative Fluoroscopic Images
RG Seltzer, D Soetemans, I Okwuchi, BD Hamilton, SY Nakada
Translational Analytics and Statistics
Introduction & Objective: Most attempts to use Artificial Intelligence (AI) to identify and characterize kidney stones have been from CT scans. While these pre‐operative images are the gold standard for diagnosing urolithiasis, fluoroscopy is the predominant intra‐operative imaging for SWL, used to localize, track, and assess fragmentation of stones. Using AI to identify stones from intra‐operative SWL fluoroscopic images is much more difficult because of the relatively lower image quality and the presence of fragmented or partially disintegrated stones that are not as salient as non‐molested stones. Identifying and characterizing fragmenting stones visible on fluoroscopic images during SWL can help urologists align treatment parameters to the exact stage of stone fragmentation at a specific point in the procedure.
Methods: A labeled dataset of dicom images with stone locations outlined was generated and pre‐processed to generate stone vs. no‐stone images. A Convolutional Neural network was used to extract image features to identify if kidney stone(s) are present on an image via the RESNET deep neural network and Tensorflow. AI algorithms were then used to determine the presence or absence of stones in a set of pre‐defined images.
Results: A total of 6501 static images with stones labeled by 14 technologists were used. A training accuracy of 0.92 and a loss of 0.14, and a validation accuracy of 0.91 and a loss of 0.16 were achieved.
Conclusions: With sufficient data comprising stones in various stages of fragmentation and disintegration during an SWL procedure, AI algorithms showed strong accuracy metrics for identifying stones on fluoroscopic images. Once identified, relevant characteristics of the stone can be extracted and, with additional technology, presented to urologists during a treatment. This intra‐operative feedback may better assist urologists in selecting the optimal shock parameters based on the exact state of the stone.
Medical Impulsive Therapy: Early results from a Randomized Controlled Trial to evaluate tamsulosin use before ureteral access sheath deployment
V Dall'Aqua, A Lopes Neto, A Rodrigues, M Mattos, L Costa, S Glina
Introduction & Objective: As retrospectively proposed by Clayman et al., tamsulosin use before endourological procedures may have an effect in distal ureter that could improve large diameter (16Fr) ureteral access sheath (UAS) deployment. In order to explore this relationship, we conducted the present trial.
Methods: The study is designed to randomize 140 patients in two groups: none pre‐surgical medication (control group) and daily tamsulosin 0,4mg at bedtime one week before surgery (intervention group). All procedure was performed by only one surgeon, which was blind for medication use. An external study coordinator managed the surgery schedule. Primary outcome success was defined as complete UAS deployment. Secondary outcomes were ureteral injury, UAS deployment rate in patients with previous endourologic procedures and patient characteristics (BMI and height).
Results: The preliminary results are demonstrated in table 01. Forty‐two patients underwent retrograde intrarenal surgery (RIRS) and have fulfilled trial requirements. Nineteen patients (45.2%) used tamsulosin before surgery and 23 (54.8%) was in control group. In eight procedures (four in tamsulosin group and four in control) UAS deployment failed. No statistically significant difference was demonstrated (p = 0.764). No difference in UAS deployment rate was observed in patients who had previous endourological procedure (p = 0.166). Patients physical biotype – BMI (p = 0.241) and height (p = 0.09) ‐ did not show differences in UAS deployment rate. Ureteral injury was significantly higher in tamsulosin (42.1% vs. 13.1%) than control group (p = 0.04).
Conclusions: At this moment, in contrast to Clayman et. al. data, no benefit was demonstrated prospectively to support tamsulosin use before surgery when UAS deployment is needed and it uses can elevate ureteral injury rate, as demonstrated in our date. Obesity and lower stature may have a role in UAS insertion failure, but no significant differences were shown. Previous ureteral surgery could work as an obstacle to UAS deployment, due to ureteral reduced complacence, but the trial failed to prove this hypothesis. This is a preliminary trial analysis. Mature data is needed to prove the real effectiveness of tamsulosin use before surgery in UAS deployment rate.
Maternal family history of urolithiasis is associated with earlier onset of urinary stone disease: results from ReSKU
R Unno, K Taguchi, M Usawachintachit, H Yang, F Hamouche, J Ahn, D Bayne, M Stoller, T Chi
University of California San Francisco
Introduction & Objective: Family history of urolithiasis is a known risk factor for kidney stones. The direct relationship between family history and the severity of clinical presentation for kidney stone formers is not yet well documented. In this study, we evaluated the impact of family history on the severity of disease and age of onset in patients with urolithiasis.
Methods: This was an analysis of prospectively collected data from Registry for Stones of the Kidney and Ureter (ReSKU) from a single institution between October 2015 and December 2020. Demographics, clinical, and family history information from urolithiasis patients were collected. The family history information was further characterized to highlight the type of relationship (first vs first‐ and second‐degree relatives) as well as the parental sidedness of the relationship (paternal vs maternal). This detailed family history was then linked to patient clinical data, including number of previous stone episodes, bilaterality, age of stone onset, 24‐hour urine evaluation, and recurrent stone events during follow‐up. Our primary endpoint was the number of patients experiencing at least one recurrent stone event during the study period.
Results: A total of 1566 patients were analyzed for this study. 603 patients (38.5%) had a family history of urolithiasis. On univariate analysis, a positive family history was associated with a higher number of recurrent stone events during the follow‐up period (38.2% vs 27.6% p = 0.001), an earlier onset of kidney stones, a higher percentage of bilateral disease, a higher number of previous stone episodes as well as more significant hypercalciuria on 24 hours urine collections (Table1). On multivariate analysis, any family history was associated with an increased risk of recurrent stone events. The presence of both a first and a second degree relative was associated with the highest odds ratio for recurrent stone event (OR 2.23 p < 0.001), while having a maternal side relative conferred a higher odds ratio for a younger onset of stones (OR 2.53 p < 0.001).
Conclusions: The presence of any family history of kidney stone disease imparts an increased severity of urinary stone disease on patients. Furthermore, the presence of a maternal side relative with kidney stones may be a predictor for an earlier onset of urolithiasis.
Extracorporeal shock wave lithotripsy in patients with spinal cord injury: have contemporary outcomes improved?
MS Yassin, BW Turney, JS Reynard
Oxford University Hospitals NHS Foundation Trust
Introduction & Objective: Spinal cord injury (SCI) is a risk factor for significant urolithiasis. 34% of patients developing one stone will have a second stone episode within five years. Effective stone treatment is essential, as stones are associated with decreasing renal function. We present our extracorporeal shock wave lithotripsy (ESWL) experience in spinal cord injury (SCI) patients.
Methods: We conducted a single centre retrospective study, including all spinal cord injury (SCI) patients who underwent extracorporeal shock wave lithotripsy (ESWL) for urolithiasis from Sep 2013 to Aug 2019. 17 patients underwent 51 treatments and comprised the study cohort. Statistical analysis was performed with SPSS v. 24.0 (IBM Corp, Armonk, NY), and statistical significance was defined as a P‐value of <0.05.
Results: Demographic, stone, treatment and follow‐up parameters are presented in table 1 and 2. Clear stone fragmentation was seen in 19.6% (n = 10), good in 33.3% (n = 17) and satisfactory in 47.1% (n = 24). Post‐treatment stone burden was reduced from a mean of 21.53 (range 39) mm to 13.47 (range 32) mm. 78.6% (n = 11) had their treatment outcome assessed by CT which reflects the lower clearance rate in our series compared others. Pain tolerance was excellent in 84.3% (n = 43), good in 7.8% (n = 4) and satisfactory in 3.9% (n = 2). 5.9% (n = 1) had autonomic dysreflexia requiring treatment termination. No other complications encountered.
Conclusions: Extracorporeal shock wave lithotripsy (ESWL) is a safe, effective and straightforward treatment modality for urolithiasis in spinal cord injury (SCI) patients.
Emergency Ureteroscopy Service Reduces Patient morbidity and need for secondary procedures in Acute Stone Patients
A Jha, C Ho, S Lee, S Albuheissi, F Keeley, A Timoney, J Philip
Bristol Urology Institute
Introduction & Objective: 60% of patients attending hospitals with acute stone colic are treated conservatively during their acute presentation, a reported median of 20% of patients had a ureteric stent insertion in all NHS trusts in England. We aim to assess the outcome after introduction of dedicated emergency ureteroscopy theatre slots to help reduce the demand on generic emergency lists and to improve patient outcomes.
Methods: A prospective study over a 3‐month period ending January 2020 following the introduction of emergency ureteroscopy (URS) care pathway with dedicated theatre slots, in a teaching hospital in UK. Predating retrospective study of all patients admitted with ureteric colic/ obstructing ureteric stones over three months ending December 2018 was the initial pilot study to identify the acute burden of stones.
Results: Between October and December 2018, 42% underwent conservative management during initial presentation while 42% had ureteric stent inserted (antegrade or retrograde). 4% underwent primary URS and 7% underwent emergency ESWL (Extracorporeal Shockwave Lithotripsy). 4 patients (8%) represented to the hospital within 28 days.
Conclusions: Almost a fifth of the emergency urology admissions and a third of the emergency surgical procedures are stone related. The emergency ureteroscopy pathway reduces patients having temporising stents by half and the need for secondary procedures. Emergency ESWL uptake almost tripled; with primary emergency ureteroscopies increasing fivefold. Implementing a Primary Ureteroscopy pathway has reduced stone patient morbidity, stent insertions and need for secondary procedures with improved quality of life.
Matched Pair Analysis of Extended versus Precise Focus Shockwave Lithotripsy for Urolithiasis
AJ Sharp, CE Lovegrove, R Sreekumar, M Spencer, BW Turney, SA Howles
University of Oxford
Introduction & Objective: Evidence for the optimal focus size during shockwave lithotripsy (SWL) for urolithiasis is lacking. To increase understanding, we compared stone clearance and complication rates when using an ‘extended’ focus treatment field (9 x 50mm) to a ‘precise’ field (6 x 28mm), when undertaking SWL in patients with renal or ureteric calculi.
Methods: Data from patients undergoing SWL to renal or ureteric stones using a Storz Modulith SLX‐F2 lithotripter at a single centre were prospectively collected between February 2018 to September 2020. A precise focus treatment field was used until July 2019; after this date, an extended focus treatment field was employed. Patients were matched according to stone size, location, and number of SWL treatments. Stone clearance rates, re‐presentation to hospital within 31 days, symptoms, complications, and subsequent treatment were recorded, and compared using McNemar's test. Energy level reached during SWL was compared using the Wilcoxon signed‐rank test.
Results: In total, 152 patients received extended focus SWL, and were matched with 152 patients treated with precise focus SWL. Median stone size was 6mm (IQR 5‐7mm). Maximum energy delivered was comparable between groups (p = 0.08, median maximum energy level of 6 for both groups). Extended focus SWL achieved complete stone clearance in 55% of patients (N = 84), compared to 41% (N = 63) in the precise focus group (p = 0.009). Complete clearance was defined by a lack of residual fragments on follow‐up plain radiograph, ultrasound, or non‐contrast CT. Where overall treatment success was defined as having no need for further follow up or treatment of the index stone, use of the extended focus resulted in a 74% success rate (N = 113) compared to 66% (N = 100) of precise focus patients (p = 0.05). Extended focus SWL was also associated with greater rates of urinary tract infection and requirement for analgesia (7% (N = 10) versus 1% (N = 2), p = 0.02, and 17% (N = 26) versus 9% (N = 14), p = 0.046, respectively). No differences in rates of re‐presentation to hospital, haematuria, or treatment of complications under general anaesthetic were identified.
Conclusions: This study indicates that extended focus SWL results in greater complete stone clearance, and may improve overall treatment success rates. However, extended focus treatment was also associated with increased rates of post‐procedural infection, and requirement for analgesia. Our findings will inform urologists and radiographers when evaluating the relative advantages and disadvantages of each focus size during SWL.
Suction Assisted Mini Percutaneous Nephrolithotomy as a day care procedure for medium sized renal stones
MS Agrawal, D Mishra
Global Rainbow Hospital, Agra, India
Introduction & Objective: Mini PCNL (Percutaneous Nephrolithotomy) with Laser lithotripsy has been a modality of choice for medium sized renal stones. Vacuum cleaner effect works very effectively for removal of stone fragments. We evaluated the use of Suction in Mini PCNL to augment the vacuum cleaner effect and also lowering the Intra Pelvic Pressure(IPP) using a specially designed SHAH sheath in our center.
Methods: Data was collected prospectively from 64 consecutive patients undergoing Mini PCNL for medium sized renal stones (>1cm, <2.5cm) from January 2019 till December 2019. All patients underwent a preoperative evaluation and Non Contrast Computer Tomography(NCCT) scan to assess stone burden. We used 12 Fr Mini Neproscope(Karl Storz, Gemany) for all cases. The initial steps of puncture were same as standard PCNL. Tract Dilation was single step. Stone fragmentation was performed using holmium laser. The metallic Super‐perc sheath has a rear suction channel, allowing application of surgeon‐controlled suction to the outflow tract, thus helping extraction of the fragments and keeping IPP low.
Results: Mean age of the group was 43.5 years (range 18‐76) with 40 males and 24 females. Mean stone size was 16.5mm (range 10‐25mm) and mean operative time was 43.9 min (range 25‐90 min) with mean fragmentation and removal time of 28.4 min(Range 18‐60 min). 6 renal units had upper calyceal puncture whereas 30 had middle, 24 lower calyceal and 2 with two punctures. DJ stent was placed in 18 patients whereas 46 patients were totally tubeless, with only a ureteric catheter left indwelling overnight. No patient required a nephrostomy tube and surgical site was sutureless in 54 cases. The mean Hemoglobin drop was 0.24 units with no blood transfusion. Post‐op 2 patients reported fever and 3 had minimal hematuria. 7 patients had minimal discharge from surgical site. The mean hospital stay was 22.5 hours with most patients discharged within 24 hours of admission. The stone clearance rate on follow‐up NCCT was 96.8%. The follow up was for 3 months duration.
Conclusions: Suction assisted Mini PCNL has outstanding stone clearance rates in medium sized renal stones with good safety profile.
Comparison of pain scores and recovery after Percutaneous Nephrolithotomy in patients with and without regional anesthesia block. Prospective Randomized controlled study
N Iqbal, A Hasan, S Imtiaz Ali, J Rahim, S Akhter
PKLI, Lahore, Pakistan
Introduction & Objective: Achieving effective pain control is vital for early patient mobilization and eventually returning back to normal routine life following percutaneous nephrolithotomy (PCNL) surgeries. The use of an intraoperative local anesthetic or postoperative analgesic has been reported for pain control in PCNL. Erector spinae block is a regional anaesthetic technique applied in other surgeries under ultrasound guidance. The aim of our study was to see the effectiveness of this block on postoperative pain in PCNL.
Methods: This prospective, randomized, double‐blinded study was carried out since May 2018 till September 2019. The Erector spinae block was administered to a total of 47 patients who had undergone elective PCNL under General anesthesia. While other group of the patients (Group 2, n = 67) didn't receive such block. Postoperatively the pain level was measured using the visual analog scale (VAS), and the opioids consumptions at the postoperative 1, 2, 6, 12, 18, 24, 48 and 72 hours.
Results: The postoperative VAS was found to be statistically significantly lower in the Erector spinae block group (2.1) as compared to the group without Erector spinae block (mean VAS score = 3.2, p < 0.05). The postoperative opioid analgesic use was found to be statistically significantly higher at the 3hours, 6 hours, 12 hours, and 24th hour in Group without Erector spinae block (p < 0.05).
Conclusions: The Erector spinae block was observed to be effective in pain control and reducing opioid use during the postoperative 48 hours follow‐up after PCNL. It may help in avoiding the use of opioids keeping in view the opioid epidemic challenges nowadays.
Withdrawn
The Use of Peripheral Nerve Blocks Provides a Significant Opioid‐Sparing Analgesic Effect for Percutaneous Nephrolithotomy: A Systematic Review
R Alam, K Koo, BR Matlaga, JS Winoker
Johns Hopkins University School of Medicine
Introduction & Objective: Multimodal analgesia regimens incorporating peripheral nerve blocks (PNB) have demonstrated reduced postoperative pain, opioid use, and recovery time in various disease states. However, this remains a controversial subject of limited investigation in the percutaneous nephrolithotomy (PCNL) domain. In the face of an ongoing opioid epidemic and collective push to enhance prescribing stewardship, we sought to examine the evidence for PNB in PCNL.
Methods: A systematic review of Embase and PubMed was performed to identify all randomized controlled trials evaluating the use of a PNB with general anesthesia (GA) versus GA alone for pain control following PCNL. Studies evaluating neuraxial (epidural and spinal) anesthesia, those without GA as the control arm, and those not evaluating pain scores were excluded. Pain scores up to 24 hours after surgery were based on visual analog scale (VAS). Due to study heterogeneity, meta‐analysis of effect sizes was deemed inappropriate and outcomes were summarized descriptively, except where pooled analysis was suitable.
Results: Sixteen trials evaluating 878 procedures were included (Table). Five different blocks were identified and evaluated: paravertebral (PVB, n = 8 studies), intercostal nerve (ICNB, n = 2), quadratus lumborum (QLB, n = 2), transversus abdominis plane (TAPB, n = 1), and erector spinae (ESB, n = 3). Nine studies observed lower pain scores with PNB use throughout the 24‐hour postoperative period. By contrast, 5 studies showed improved pain scores with PNB that was limited to the early (< 6 hours) recovery period, and 2 studies found no difference. However, the total analgesia requirement was significantly higher in the control arm in 5 of these 7 studies and in 11 of 13 studies overall. Operative times were similar, and there were no differences in rates of intercostal access or nephrostomy tube insertion between study arms within any trial.
Conclusions: While greater pain medication use with GA alone likely minimizes or obscures differences in patient‐reported pain scores, PNBs may offer a significant opioid‐sparing analgesic effect for PCNL.
Withdrawn
Feasibility of a Non‐opioid Pathway Post Ureteroscopy: Joint Analysis from Two Academic Centers
M Awad, M Assmus, a Berg, M Lee, L Hallgarth, AE Krambeck, K Sternberg
Northwestern University, Department of Urology
Introduction & Objective: In an effort to combat the alarming amount of postoperative opioid prescribing in the United States (U.S.), many surgical specialties are implementing pathways to limit the routine use of postoperative opioids with the goal of zero opioid prescribing. We sought to examine the durability of established non‐opioid post ureteroscopy (URS) pathways previously implemented at two academic urology centers in the U.S.
Methods: We examined patients who underwent URS at two academic centers utilizing a non‐opioid postoperative pathway between November 2016 to March 2020. Primary outcomes evaluated included adverse events (Emergency Department (ED) presentation, and Office phone calls for postoperative genitourinary symptoms) for patients discharged with and without opioids. Secondary outcomes were factors associated with adverse events.
Results: In total, 699 patients underwent URS with stent placement. Of these, 652 (89.4%) were discharged without opioids and 74 (10.6%) received opioids postoperatively. Of those discharged without opioids, 484 (77.4%) received non‐steroidal anti‐inflammatory medications. The majority of patients were prescribed adjunct medications (acetaminophen, phenazopyridine, and/or tamsulosin) upon discharge. Compared to patients discharged without opioids, patients who were prescribed opioids were more likely to present to the ED (67 (10.7%) vs 14 (19.9%), p = 0.037) and call the clinic postoperatively for genitourinary symptoms (102 (16.3%) vs 22 (29.7%), p = 0.004). In a multivariate analysis, patients prescribed opioids post URS (OR 1.9, 95% CI 1.1 – 3.5, p = 0.024) and patients who had an opioid prescription preop (OR 2.2, 95% CI 1.1 – 4.5, p = 0.032) were associated with higher odds of calling the clinic for genitourinary symptoms. Older patients (OR 0.98, 95% CI 0.97 – 0.99, p = 0.006) were less likely to call the clinic for genitourinary symptoms.
Conclusions: The study highlights that almost 90% of patients can be discharged safely without opioids following URS. In our cohort, patients prescribed opioids experienced higher postoperative healthcare interactions (ED visits and office phone calls). We hope our results will encourage other urologists to consider non‐opioid pathways post URS.
The effect of topical tranexamic acid on postoperative hemoglobin level in patients undergoing PCNL
S Farshid, V Rezvankhah, N ahmadian, M sadri
Introduction & Objective: PCNL is a selective treatment for kidney stones larger than 2 cm in diameter and many smaller stones. One of the side effects of PCNL is hemorrhage, for which interavenous tranexamic acid may be used. There is no study on the effect of topical tranexamic acid on the prevention of bleeding during PCNL but there are studies in orthopedic and maxillofacial surgeries showed the efficacy of topical tranexamic. This study was performed to compare the rate of postoperative hemoglobin loss in patients undergoing PCNL using topical tranexamic acid in nephrostomy compared with control group.
Methods: In this double‐blind clinical trial study, 90 patients undergoing PCNL were randomly divided into two groups, topical tanzanexamic acid and control (without tranexamic acid injection). Inclusion criteria were age between 18‐65 years, ASA class
Results: The mean age of patients in this study was 45.21 ± 11.69 years and there was no significant difference between the two groups (p = 0.058). There was no significant difference between the two groups regarding hospital stay and its mean was 2.34 ± 0.83 days. Hemoglobin loss was ‐1.19 ± 1.28 in tranexamic acid group and ‐3.07 ± 1.20 in the control group (t = 7.141, p = 0.001). Comparison between groups was statistically significant (p = 0.001) after hemoglobin surgery. Regarding stone free rate, the two groups had similar status and about 72% in intervention group and 70% in control group. There was no significant difference between the two groups in the time of surgery, in such a way that in the tranexamic acid group was 82.57 ± 33.57 minutes and in the control group was 87.15 ± 33.39 minutes (p > 0.05).
Conclusions: This study showed that topical application of tranexamic acid after the end of PCNL can prevent hemoglobin loss in patients with low preoperative hemoglobin level, as well as in cases of longer surgical length or large and numerious stones. Those who are more likely to bleed can reduce the amount of bleeding using topical tranexamic acid.
Safety and feasibility of intraoperative real‐time digital stone fragment measurement during ureteroscopy
R Becker, K Koo, T Aro, JS Winoker, S Lim, D Petrisor, D Stoianovici, BR Matlaga
James Buchanan Brady Urological Institute, The Johns Hopkins Medical Institutions
Introduction & Objective: Estimating the size of stone fragments during ureteroscopy is critical for determining the adequacy of stone fragmentation, likelihood of spontaneous fragment passage, and ability to safely extract fragments through the ureter or ureteral access sheath. We previously developed and validated an image processing software that enables digital measurements of stone fragment size during ureteroscopy. This study assesses the safety and feasibility of performing real‐time in vivo stone fragment measurement and integrating its use into live operating room workflow.
Methods: Adult patients >18 years old undergoing ureteroscopic stone procedures for renal or proximal ureteral calculi by 2 surgeons at a single center were enrolled prospectively. The software was used to perform a representative series of real‐time intraoperative stone fragment measurements. The time required to perform each measurement or series of measurements was recorded, including snaring the fragment with a stone retrieval basket, initiation of the digital measurement by the surgeon, and confirmation of size calculation. Software‐related failures, clinical complications, and delays were also recorded. Ethics approval of the feasibility study protocol required that the measurements have no impact on clinical decision‐making; thus surgeons were blinded to the results.
Results: Nine patients undergoing ureteroscopic stone treatment were enrolled. Median age was 50 years (range 25‐75). Six (67%) patients were female. Five (56%) procedures were right‐sided. Intraoperative real‐time measurement of stone fragments was successfully completed in all patients. The median number of measurements performed was 5 (range 3‐10). The mean time for each measurement, from snaring the fragment until size calculation, was 9.9 seconds (s) (range 7.1‐14.9 s). The median total time spent performing digital measurement per procedure was 50 s (range 25‐99 s). There were no technical failures of the software or ureteroscope. No measurement‐related delays or clinical complications were observed peri‐operatively.
Conclusions: Intraoperative digital stone measurement can be safely performed during ureteroscopy and integrated into operating room workflow, with minimal additional time and no observed complications. These data support a prospective trial of digital stone measurement to guide intraoperative decision‐making.
In‐Vivo Porcine Evaluation of the Thermal Effects of the Superpulse Thulium Laser Lithotripsy during Ureteral Stone Laser Lithotripsy
P Jiang, A Peta, M Ayad, A Brevik, K Larson, Z Okhunov, RM Patel, T Farzaneh, J Landman, RV Clayman
Department of Urology, University of California, Irvine
Introduction & Objective: The superpulse thulium fiber laser (sTFL) is a promising emerging technology for laser lithotripsy; however, there have been concerns due to its thermal output which in the kidney may exceed 44°C, the threshold for thermal cellular injury. Given the limited space within the ureteral lumen, we sought to evaluate the thermal effect on the ureter of sTFL for treatment of ureteral stones in an in‐vivo porcine model.
Methods: One juvenile female Yorkshire pig was used for the in‐vivo study (three trials in each ureter). Via an open surgical pyelotomy from an extraperitoneal approach, calcium oxalate stones (total of 6 stones) measuring 3‐4mm were deposited into each ureter at three locations (distal, mid, and proximal) via antegrade ureteroscopy using a nitinol 4‐wire basket. Two K‐type thermocouples were placed (one inside the ureteral lumen and one adjacent to the adventitia of the ureter. Retrograde flexible ureteroscopy (37°C warmed irrigation at 100mmHg) and laser lithotripsy was performed with a 200μm sTFL fiber with dusting settings of 0.2J, 80Hz (16W). Each stone was dusted for a maximum of five minutes, with lithotripsy paused whenever either thermocouple reached 44°C; lithotripsy was resumed once the thermocouple cooled to 37°C. The time to peak temperature as well as cooldown to body temperature and baseline temperature were recorded. Ureters were harvested for histopathologic analysis.
Results: Upon initial laser activation during the 6 trials, the intraluminal thermocouple registered 44°C at 83 ± 45 seconds (mean ± SD) of lasing; however, the peri‐ureteral thermocouple never reached 44°C (max 40.3°C). After the inside thermocouple peaked at 44°C, it required an average of 4 ± 4 seconds (mean ± SD) to cool down to 37°C. With each subsequent laser activation, it took an average of 6 ± 5 seconds (mean ± SD) to peak to 44°C; however, under no circumstance did the adventitial thermocouple reach 44°C.
Conclusions: The use of the superpulse thulium fiber laser (sTFL) for dusting ureteral stones results in rapid elevation of intraluminal temperatures at the level of the urothelium; however, this is not mirrored at the level of the ureteral adventitia. Cessation of lasing resulted in rapid cooling of the temperature. We recommend utilizing short 5 second bursts of laser activation when performing lithotripsy in the ureter to avoid exceeding intraluminal temperature above 44°C.
Adaptive Percutaneous Nephrolithotomy: Modifying Positioning & Access for Each Patient
N Nimmagadda, CM Forbes, NL Kavoussi, R Hsi
Vanderbilt University Medical Center, Department of Urology
Introduction & Objective: Surgeons typically perform percutaneous nephrolithotomy (PCNL) in a preferred position using one access method. We sought to evaluate the feasibility and outcomes of an “adaptive PCNL” approach – adapting positioning and access techniques to patient and stone characteristics, performed during a learning curve period for PCNL.
Methods: All PCNL cases performed by a single surgeon immediately after fellowship training (primarily prone PCNL with fluoroscopic access), were retrospectively reviewed from 9/2016 ‐ 5/2020. Positioning was categorized as prone ± split leg, supine (0 degrees), modified supine (15‐45 degrees), or flank (>45 degrees). Access was achieved with fluoroscopic, ultrasound, and/or endoscopic guidance. We evaluated differences in patient factors and outcomes across positions, and then evaluated the learning curve necessary to achieve stability in procedure time.
Results: Among 19 PCNLs performed, prone PCNL comprised the first 23 cases. Positioning subsequently varied every 1.67 cases on average with 49% performed supine/flank (Figure 1). Prone PCNL was more commonly associated with fluoroscopic access, larger stone size, and bilateral PCNL, whereas modified supine cases were associated with ultrasound ± endoscopic access, and contralateral ureteroscopy or lower urinary tract procedures (Table 1). No differences were seen in upper pole stone location or access (p = 0.13 and p = 0.08, respectively). The second 32 cases had significantly higher mean procedure time vs the subsequent groups of 32 cases (164.2 min vs 112.0‐125.4 min, respectively, p < 0.01). Needing fluoroscopy during access decreased over the learning curve (p < 0.01). Mean residual fragment size was less in the latter 96 cases (0.289 vs 0.469 mm, p = 0.01).
Conclusions: Adaptive PCNL is feasible for optimizing procedural complexity, operative time, and fluoroscopy. The learning curve for adopting adaptive PCNL is comparable to other series utilizing fixed techniques.
Holmium laser lithotripsy with Moses™ Technology in percutaneous nephrolithotomy: preliminary results from a comparative study
E Lievore, S Zanetti, M Turetti, L Boeri, M Fontana, A Gallioli, F Longo, E De Lorenzis, G Albo, E Montanari
Dept. of Urology, Foundation IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Milan
Introduction & Objective: Moses™ is a pulse delivery technology aiming to maximize laser energy transmission in lithotripsy. The aim of this study is to compare efficacy and safety of Moses Lumenis Pulse (LP) 120W laser and VersaPulse PowerSuite (VPPS) 100 W laser during aspiration‐assisted mini‐percutaneous nephrolithotomy (vmPCNL).
Methods: We prospectively collected data from 20 consecutive vmPCNL procedures performed with the VPPS laser from November 2018 to March 2019, and 20 consecutive vmPCNL procedures performed with the Moses LP laser from March to October 2019 in a single center. All procedures were performed with a Storz MIP 12 Fr nephroscope and 16 Fr Clear Petra nephrostomic sheath with aspiration. Collected data included patients' and stones' characteristics, intra‐ and post‐operative data, complete stone‐free (SF) status at the 45 days CT scan and complications according to the Clavien score. These variables were compared between the two groups
Results: Results are shown in Table 1. The two groups resulted homogeneous in terms of patients' and stones' characteristics. The overall median stone volume was 1,83 cm3. No significant differences were observed in procedural times, laser total energy and haemoglobin drop. In the Moses group no high grade (Clavien >2) complications were recorded, in the non‐Moses group one Clavien 3A complication (i.e. renal colic needing DJ stent positioning) was reported. The SF status was obtained in 15 patients in the Moses group and in 10 in the non‐Moses group. All other patients had residual fragments <5 mm except from one patient in the LP group who was retreated in a pre‐operatively planned multi stage treatment
Conclusions: The Moses™ technology seems to be as safe and effective as the standard Ho:YAG laser. Although no significant differences were reported, we noted a tendency towards lower laser energy, lasing time and combined lithotripsy and lapaxy time in the Moses group. In addition, in this group we reported a 50% increase in the SF rate. Probably, the Clear Petra aspiration‐assisted system, by quickening the procedure and enhancing fragments lapaxy in both groups, could play a confounding role in evaluating laser contribution to procedural times and SF rates. However, this study sample is too small to draw firm conclusions and the descripted tendencies may be confirmed with further studies
Factors affecting the ability to offer emergency primary ureteroscopy in a tertiary teaching hospital
C Fontaine, R Sehgal, Y Abu‐Ghanem, L Forster, G Ellis, P Singh, R Kucheria, A Goyal, D Allen, L Ajayi
Introduction & Objective: According to current UK NICE guidelines, definitive treatment (primary ureteroscopy (URS) or shock wave lithotripsy (SWL)), should be offered to patients with symptomatic renal colic (ongoing pain) or likely impassable stone, within 48 hours of diagnosis. In the current analysis, we aim to review the factors that may influence the ability to achieve these guidelines in a well‐resourced tertiary centre in Central London.
Methods: Retrospective review of all patients presenting to the emergency department at our institution between January 2019 and December 2019 with the diagnosis of a ureteric or renal stone. The emergency intervention rate, risk factors for intervention, and other qualitative data were analysed.
Results: A total of 258 patients required surgical management for symptomatic ureteric colic. Of those, 91 patients (35%) underwent definitive treatment by either primary URS (82 patients) or ESWL (9 patients), at a mean time to procedure of 25.5 hours (range 1 – 118). Majority of patients (50/82 61%) undergoing primary URS had distal ureteric stones compared to a preference of proximal ureteric stones in SWL (5/9 56%) and those undergoing emergency stenting alone (116/167 69%). Primary URS was more likely to be performed in a supervised setting compared with emergency stenting; resident supervised 51%, resident alone 31% and consultant alone 18%. A larger mean stone size was associated with emergency stenting (7.8mm versus 6.9mm for primary URS and 6.2mm for SWL).
Conclusions: Although definitive treatment carries high success rates, in a high‐volume tertiary referral centre, it may not be feasible to offer it to all patients, with emergency stenting providing a safe and quick interim measure. Factors determining the ability to provide definitive treatment are stone location, stone size and resident supervision in theatre.
Dusting Efficiency of the Moses Pulse 120H 2.0 Laser System: An In vitro Assessment
P Whelan, CJ Kim, D Ho, C Tabib, F Soto‐Paulo, J Chen, P Zhong, GM Preminger, M Lipkin
Duke University
Introduction & Objective: Moses™ Pulse 120H 2.0 Extended Frequency Range (EFR) technology is a second‐generation Holmium:YAG laser system designed to introduce higher frequency pulse settings. Our aim is to assess the efficiency of Moses 2.0 technology lithotripsy in an automated in vitro “dusting model.”
Methods: All tests were conducted using a Moses™ Pulse 120H 2.0 laser system on “hard” (5:1) and “soft” (5:2) Begostone phantoms. Treatment efficiency is compared between Moses Distance (MD) and Moses EFR settings of comparable power (0.3J/80Hz MD to 0.2J/120Hz EFR; 0.4J/80Hz MD to 0.3J/120Hz EFR) at a fiber‐stone standoff distances (SD) of 0 and 1mm. The laser fiber was scanned in a spiral to deliver 1kJ of energy over a 1 cm2 area with a 3D positioning system across a polished and submerged Begostone surface. Stone mass loss was compared following treatment. Additionally, the ablation efficiency of MD vs EFR pulses trough segments at an adjusted fiber scanning rate of 50 pulses/mm was compared across equivalent energies (0.2, 0.3, and 0.4J). Ablation volumes of 1 mm trough segments were quantified by optical coherence tomography (OCT).
Results: In spiral scan testing, EFR was similar or slightly superior to MD (Figure 1). At SD 0mm, EFR had superior trough ablation volume to MD across all pulse energies (p < 0.05) by approximately 20‐80%. This is most prominent at lower energy and soft stones. Ablation volume increased with increasing pulse energy. There was little damage observed at SD 1mm.
Conclusions: The EFR provided by Moses 2.0 technology offers superior trough ablation volumes, although this does not translate into spiral scan mass lost. The Moses 2.0 treatment modes may offer a more efficient treatment method in practice by lowering retropulsion with lower pulse energy while negating loss in ablation efficiency with higher pulse frequency.
Reducing the rate of negative ureteroscopy: predictive factors and the role of pre‐ureteroscopy imaging
AC Brodie, TJ Johnston, P Lloyd, L Hemsworth, S Keoghane, M Barabas
Mr
Introduction & Objective: In an increasingly litigious healthcare environment, a negative ureteroscopy (URS) performed for an already passed ureteric calculous exposes the patient to unnecessary risk and represents an avoidable misuse of resource. This study investigates the factors predictive of negative URS and assesses the impact of pre‐operative imaging in reducing the rate of unnecessary negative URS.
Methods: A single‐centre retrospective review was performed for all patients who underwent emergency ureteric stenting for a ureteric calculous during two study periods; April 2011 to February 2016 and October 2016 to October 2019 in the second cohort. From October 2016 onwards change pre‐URS imaging was introduced in the form of computed topography (CT) or abdominal x‐ray (AXR). Data collected included patient demographics, indication for stent, stone characteristics, baseline bloods, admission urine culture, stent duration, re‐admission rate, negative URS rate and the use of pre‐URS imaging. Multivariate logistic regression and Pearson's Chi‐square were used for statistical analysis.
Results: In total 257 patients underwent emergency insertion and deferred URS for ureteric calculous. The mean age was 56. Indications for stent insertion were pain (n = 109, 42%), sepsis (n = 101, 39%) and acute kidney injury (n = 47, 19%). Mean stone size was 7.8mm (range 2mm‐25mm), mean stone density was 702 Hounsfield units (HU) (50 – 1588HU) and the stone locations were upper (n = 160, 62%), mid (n = 32, 13%) and lower ureter (n = 65, 25%). In the initial cohort the negative URS rate was 14% decreasing to 9%. In the second cohort and 7 patients avoided URS altogether due to pre‐op imaging. Analysis of the entire cohort revealed a negative URS rate of 14% in the non pre‐URS imaged patients compared to 6% in pre‐URS imaged patients (p = 0.19). Multivariate logistic regression analysis revealed stone size <5mm (ß = 0.75, 95% CI: 0.60‐0.94 p = 0.011) was predictive for negative URS.
Conclusions: This study demonstrates that pre‐URS imaging leads to a clinically significant reduction in negative URS rate. Furthermore, stone size <5mm is predictive for negative URS and represent the subgroup most likely to benefit from pre‐URS imaging.
Risk of unplanned postoperative re‐admissions in children undergoing ureteroscopy: a post‐hoc analysis of the pediatric National Surgical Quality Improvement Program database
Y Ding, J Davidson, EP Chan, J Bjazevic, G Filler, S Dave, Z Wang
Western University
Introduction & Objective: The incidence of pediatric urolithiasis has increased over the last two decades. Ureteroscopy (URS) with laser lithotripsy is currently recommended for the treatment of mid to distal ureteral calculi; however, there is currently no consensus regarding whether URS is appropriate for all pediatric patients. We aimed to examine the risk of unplanned postoperative hospital readmissions in children undergoing URS.
Methods: A post‐hoc analysis of data collected from the American College of Surgeons National Surgical Quality Improvement Program® (ACS NSQIP) Pediatric Version. The ACS NSQIP Pediatric datasets are validated and risk‐adjusted and include 127 institutions across Canada and the US to date. This study examined the outcomes of 299,865 pediatric patients with urolithiasis who underwent URS between 2015 and 2017. These children were identified using the International Statistical Classification of Diseases and Related Health Problems (ICD) codes ‐ 9th and 10th revision and by the Current Procedures Terminology (CPT) codes for URS.
Results: A total of 1,122 pediatric URS cases were identified. The median age was 14.4 years (interquartile range [IQR]: 10.2‐16.5) and 55.4% of these cases were female. Overall, 8.9% of URS cases required a re‐admission to hospital within 30 days of the index procedure, and of these 71% were unplanned re‐admissions. The two most common reasons for unplanned re‐admissions were postoperative urinary tract infections (UTIs, 26.4%) and persistent ureteral calculus (21.8%). On univariate analysis, children with unplanned re‐admissions were significantly younger in age (median 11.3 years; IQR 8.3‐16.7) compared to those without unplanned re‐admissions (median 14.5 years; IQR: 10.5‐16.5; p = 0.028). The relative risk (RR) of an unplanned readmission was 2.4 times higher for children aged 6‐11 years (95% confidence interval [CI]: 1.51‐3.93), and 4.5 times (95% CI: 1.80‐11.50) for children under 2 years old when compared to children 12‐18 years old.
Conclusions: Our study demonstrates that younger children undergoing URS are at a higher risk of unplanned re‐admissions secondary to postoperative UTI and persistent calculi. As such, age should be taken into consideration when deciding on the optimal surgical modality or perioperative care for children with urolithiasis. Further prospective studies are needed to better elucidate the indications of URS for pediatric urolithiasis, as well as the postoperative management and outcomes of these children.
Mini percutaneous nephrolithotomy using SuperPulse Thulium Fiber Laser: Evaluation of clinical efficacy and safety
DA Sytnik, S Popov, I Orlov, I Pazin, M Suleymanov, A Kulikov
St. Luke's Clinical Hospital
Introduction & Objective: As a rule, the Ho: YAG laser was used as a source of lithotripsy when performing mini percutaneous nephrolithotomy (miniPCNL) due to its high efficiency and safety. But in recent years the SuperPulse Thulium Fiber Laser (SPTFL) has become more and more interesting. The aim of this work was to evaluate the clinical efficacy and safety of the miniPCNL using SPTFL.
Methods: The study included 53 patients who underwent miniPCNL including 30 men and 23 women. The average age of the patients was 61 ± 13 years. Average stone size 26.32 ± 5.56 mm, with an average density of 1165 ± 314 Hu. Exclusion criteria: multiple renal stone, stone size larger than 3 cm and less than 1 cm, urinary tract abnormality Surgical technique: miniPCNL was performed with tract dilatation up to 15/16 Fr (Karl Storz, MIP M) in the patient's supine position. The energy source for lithotripsy was a SPTFL (IPG Photonics, FiberLase U2), fiber thickness 400 μm. The fragmentation of the stone occurred in the dusting mode (0.2 J, 150‐200 Hz). On the 1st day computed tomography of kidneys, ureter and bladder was performed to evaluate the SFR level. The following parameters were evaluated: time of surgery; lithotripsy time, SFR level; exit strategy; postoperative complications according to the Clavien‐Dindo classification.
Results: The average duration of surgery was 34.8 ± 14.7 minutes. Lithotripsy time: 806.73 ± 487.6 seconds. Drainage methods: Totally tubeless ‐ 12 cases (22.64%), Tubeless (JJ stent) ‐ 25 cases (47.17%), nephrostomy tube ‐ 16 cases (30.19%). SFR ‐ 96.3%. Complication was registered in 3 patients, namely urinary tract infection (Clavien‐Dindo 2) ‐ 2 patients; renal colic initiated by blood clots ‐ 1 patient (Clavien Dindo 3a).
Conclusions: MiniPCNL using a SPTFL is a highly effective and safe treatment for patients with kidney stones 2 cm or larger.
Micro‐ureteroscopy for treatment of mid and upper ureteral stones and kidney stones in pediatric patients younger than 3 years
R Zhan, Y Ge, W Wang
beijing friendship hospital
Introduction & Objective: This study was aimed to demonstrate the efficacy and safety of micro‐ureteroscopy in the treatment of upper ureteral stones and kidney stones in pediatric patients younger than 3 years.
Methods: A retrospective analysis was performed on data from 25 children younger than 3 years old who received micro‐ureteroscopic lithotripsy in our hospital from July 2018 to June 2020. The procedures were performed with the patient in the lithotomy position under general anesthesia using the standard ureteroscopic technique with a micro‐ureterocope that has a caliber of 4.85 Fr all along its length. Demographics, perioperative data, including surgical time, irrigation fluid volume, stone‐free rate (SFR), and complications were analyzed.
Results: The patients' mean ages were 21.4 ± 9.7 months(9‐36months), 11 patients had ureteral stones; 12 patients had kidney stones, 2 patients had kidney and ureter stones. The mean stone size was 1.0 ± 0.2cm (0.6‐1.4cm). The mean stone density was 620 ± 192 HU(185‐982HU). Hydronephrosis was found in 21 patients. The mean surgical time was 43 ± 9 min (25‐60min), and the mean lithotripsy time was 18 ± 6 min (10‐30min); the mean irrigation fluid volume was 241 ± 134 ml (60‐610 ml), and the SFR at one month after surgery was 84%. As a postoperative complication fever (Clavien grade 1) was observed in two cases and required antibiotic treatment. MicroPCNL was needed in three patients with impacted stone in one case and with lower pole stones in two cases.
Conclusions: This study showed that micro‐ureteroscopic lithotripsy was safe and effective for mid and upper ureteral stones and kidney stones in selected pediatric patients under three years of age, however, the impacted ureter stone and the presence of lower pole stones will decrease the success rate of micro‐ureteroscopy.
Ambulatory Percutaneous Nephrolithotomy Performed in a Free‐Standing Surgery Center: Outcomes of 1000 Cases
MM Dunne, N Ariasvillela, JE Abbott, J Davalos
Chesapeake Urology, Univeristy of Maryland Baltimore Washington Medical Center
Introduction & Objective: Percutaneous Nephrolithotomy (PNL) is a procedure that has traditionally been performed in an inpatient setting with at least an overnight stay. Many surgical procedures have evolved over time from an inpatient setting to an ambulatory surgery center (ASC) setting. Feasibility of Ambulatory PNL (aPNL) was shown in our initial pilot series of 25 cases [1]. This 1000 case series is reviewed to further evaluate outcomes with a more robust data set.
Methods: We present our series of 1000 patients who underwent PNL in an ASC from April 2015 to January 2021. Each aPNL was performed by one of two surgeons with the same operative team. All procedures were performed with the urologist obtaining renal access and all procedures were performed tubeless (ureteral stent without a nephrostomy tube). All patients also had hemostatic plugs placed into the access tract with a local intercostal block to aid with pain control. [2] All cases were reviewed and demographic data and case details were analyzed.
Results: 1000 consecutive aPNL cases were reviewed, identifying 488 men and 512 women, 460 right side and 535 left, mean age 57 years (15‐86), mean BMI 30 (15‐49), mean ASA of 2.3 (1‐4) and mean stone burden 31 mm (4‐170), mean fluoroscopy time 84 sec (0‐322). Mean OR time was 95 min (32‐305) and mean treatment time was 14.9 min (1‐262). Mean PACU time was 91 min (37‐247). A mini‐PNL (mPNL) procedure was conducted in 255 (25.5%) patients. The remaining 745 cases were standard tract size of which 449 were 30Fr and 296 were 24Fr. Stone free rate was 83%. Thirty nine patients had complications ranging from Clavien II‐IVa, of which 15 were hospital transfers.
Conclusions: These consecutive 1000 cases may serve as a landmark series demonstrating the feasibility of aPNL. Transitioning PNL to an ambulatory setting is a paradigm shift in the treatment of complex kidney stones. 39 patients experienced complications of Clavien II or higher. Each complication that occurred was managed in an appropriate fashion and the site of service did not lead to an alteration in the outcomes of the adverse events. With an experienced surgeon, well trained operative team and with modifications to the procedure focusing on post‐operative pain control, PNL can be safely and effectively performed in a free standing ASC. 1. Davalos JG, Abbott JE. Ambulatory PCNL: Initial Case Series. J Urology. April 2016 2. Abbott JE, Cicic A, Jump R, Davalos JG. Hemostatic Plug: Novel Technique for Closure of Percutaneous Nephrostomy Tract. J Endourol. March 2015
Cost‐Analysis of Mini‐Percutaneous Nephrolithotomy (PCNL) and Standard Tract PCNL for Stone Burden Greater/Less Than 20 mm in an Ambulatory Setting
MM Dunne, J Chong, B Magnan, J Davalos
Chesapeake Urology, Univeristy of Maryland Baltimore Washington Medical Center
Introduction & Objective: Percutaneous Nephrolithotomy (PCNL) has traditionally been the standard of care for kidney stones >20 mm. With the advent of smaller instruments and efficiency of holmium laser technology, Mini‐PCNL (MIP, Karl Storz, Tuttlingen, Germany) which encompasses three sizes, (small, medium, and large) has become a viable option for stones between 10‐20 mm and has also demonstrated efficacy in stones >20 mm. MIP has been touted to have significant cost savings in direct‐items costs due to reusable dilator and sheath sets. The cost analysis of MIP in comparison to standard tract PCNL (sPCNL) has not previously been elucidated for various stone sizes.
Methods: All PCNL procedures (33 MIP and 61 sPCNL) performed at a single ambulatory surgery center from April 2019‐September 2019 were reviewed. All MIP tracts were MIP‐medium (16.5/17.5 French). sPCNL ranged from 24/28‐30/34 French. All dual‐tract procedures and patients needing transfer to hospital were excluded. Patient and stone characteristics such as age, sex, BMI, skin‐to‐stone distance, Hounsfield Units (HU) and operative characteristics such as operating room (OR) time, fluoroscopy time, intracorporeal (IC) time and total treatment (TT) time were compared between groups. Cost in US Dollars (USD) were separated into two categories, <20 mm and >20 mm, based on the surgical CPT codes 50080 vs. 50081 and compared between the MIP and sPCNL groups.
Results: here were no differences in sex, BMI, skin‐to‐stone distance or stone HU between groups. Patients having MIP tended to be younger (50.4 vs. 59.1, p = 0.0045) and have lower overall stone burden (17.73 mm vs. 33.38 mm) compared to sPCNL procedures. There were no differences between groups in regard to operative time characteristics. The direct‐items cost to patient was greater in sPCNL compared to MIP regardless of whether the stone treated was <20 mm ($1805.20 vs. $1382.42, p = 0.0087) or >20 mm ($1774.22 vs. $1293.31, p < 0.0001).
Conclusions: The reusable MIP‐medium single dilator and sheath 16.5/17.5 French combination has significant direct‐items cost savings to the patient compared to patients having sPCNL. The cost savings remain even if stone burden is greater than 20 mm. MIP can be offered as a cost‐saving procedure to the patient even up to 40 mm of stone burden.
Ambulatory PCNL may be cost‐effective compared to Standard PCNL
MS Lee, M Assmus, DK Agarwal, ME Rivera, T Large, AE Krambeck
Northwestern University Feinberg School of Medicine
Introduction & Objective: In March 2020, hospitals across America locked down to prevent the spread of COVID‐19. This resulted in catastrophic financial losses and massive surgical backlog. While multiple groups have shown that ambulatory percutaneous nephrolithotomy (aPCNL) is safe and feasible, to our knowledge, a cost‐analysis comparing aPCNL against standard PCNL (sPCNL) has not been performed. Prior to March 2020, our group was not performing routine aPCNL, but to conserve hospital resources, we performed aPCNL more often. Our objective was to compare the safety and cost‐effectiveness of sPCNL vs. aPCNL.
Methods: 98 patients underwent PCNL at Indiana University Methodist hospital, a tertiary referral center, by three expert surgeons from January 2020 to September 2020. sPCNL (n = 75) and aPCNL (n = 23). All patients had at least 30‐days of follow up. The primary outcome of the study was to compare the 30‐day rates of ED‐visits, readmissions, and complications between sPCNL and aPCNL. Secondary outcomes included: cost analysis and stone free rates (SFRs). Statistical analysis was performed using SPSSv26 using independent t‐tests for continuous variables and chi‐square analyses for categorical variables.
Results: We found no difference in 30‐day ED‐visits, readmissions, or complications between the two groups. aPCNL resulted in cost savings of $5689 ± 237 per case, a 29.6% reduction.
Conclusions: aPCNL appears safe to perform and does not have a higher rate of ED‐visits or readmissions compare to sPCNL. aPCNL also is also costeffective compared to sPCNL. Patients undergoing same‐day discharge were not at higher risk of ED‐visits or readmission to the hospital.
Economic Burden of Urolithiasis Management in United States Adults 2011‐2018: Analysis of Surgical vs. Non‐Surgical Interventions
E Olweny, A Becerra, JA Khusid, M Sturgis, L Fink, M Gupta, B Konety
Rush University Medical Center
Introduction & Objective: The United States (US) healthcare landscape has witnessed numerous changes over the past decade including population growth and implementation of the Affordable Care Act. Alongside these has been a rising prevalence of upper urinary tract stone disease (SD). Data on the economic burden of treating SD during this period are lacking, providing the objective of our study.
Methods: Patients aged ≥18 years, diagnosed with SD from 2011‐2018 (N = 838,113), were identified from PearlDiver Mariner, an all‐payer database reporting direct reimbursements and prescription costs across all treatment settings, representing all 50 states. Patients undergoing surgical intervention as well as those managed non‐operatively were identified via ICD 9/10 and CPT codes. Total 1‐year cost data in the year following SD diagnosis were obtained. Data were analyzed descriptively, with trends evaluated using the Cochran‐Armitage test. Multivariable analysis (MVA) was used to evaluate determinants of spending.
Results: A total of $10B were spent on SD management over the study period, with a median overall annual expenditure of $1.3B. Inpatient, prescription and outpatient costs accounted for 34.3%, 20.8% and 44.9% of expenditures respectively. 73% of patients were managed non‐operatively, at a total cost of $6.4B. Overall per capita cost was $11,971 ($15,981 for surgical vs. $10,503 for non‐surgical care). For surgical and non‐surgical management, expenditure on inpatient care decreased significantly over the study period, while expenditures on prescriptions and outpatient care increased significantly (each p < 0.0001). On MVA, higher Charlson comorbidity index (CCI) was associated with higher spending, while associations for age, insurance status and region varied by treatment modality.
Conclusions: The economic burden of SD management is substantial, dominated by expenditure on non‐operative management and outpatient care. Expenditures for prescription and outpatient care are rising, with the only consistent predictor of higher spending being CCI. Per capita expenditure exceeded US National Health Expenditure estimates for the period, driven by surgical costs.
Determinants of ureteral patency after percutaneous nephrolithotomy
H Lee, H Yang, R Unno, F Hamouche, J Ahn, D Bayne, M Stoller, T Chi
Introduction & Objective: Alleviating ureteral obstruction is one of the primary indications for nephrostomy tube or double‐J stent placement after percutaneous nephrolithotomy (PCNL), but it is not well understood how to recognize when tube placement is needed. The goal of this study was to identify predictors of ureteral obstruction after PCNL based on antegrade studies performed on postoperative day one (POD1).
Methods: Prospective data from PCNLs was collected from adult patients enrolled in the Registry for Stones of the Kidney and Ureter (ReSKU) from 2016‐2020. Patients who had postoperative nephrostomy tubes and underwent antegrade imaging‐based flow assessment on POD1 were included. Patients without preoperative imaging within 6 months of the procedure or who had transplanted kidneys were excluded. We assessed patient demographics, stone characteristics, and intraoperative factors, using POD1 antegrade flow as the primary outcome. Forward selection was used to develop a multivariate logistic regression model controlling for age, staghorn classification, stone location, stone burden, number of dilated tracts, access location, and operative time.
Results: A total of 242 patients were included in the study, of which 77 patients had no antegrade flow on POD1. A multivariate logistic regression showed that non‐renal pelvis stones (OR 2.44, 95% CI 1.19‐5.19; p = 0.02), larger stone burden (OR 1.23, 95% CI 1.05‐1.48; p = 0.01), and mid/upper pole access during surgery (OR 3.52, 95% CI 1.74‐7.45; p < 0.01) increased the likelihood of obstruction. The presence of staghorn stones, use of concurrent multiple tracts, and operative time were not significant predictors of antegrade flow in our model.
Conclusions: Patients who had non‐renal pelvis stones, a larger stone burden, and non‐lower pole access were more likely to have postoperative ureteral obstruction. Access location appears to be the strongest predictor. Recognizing these risk factors can help determine which patients may benefit from renal drainage tubes after surgery or which patients may be good candidates for tubeless PCNL.
Moderated Poster Session 06: Stones III: New Technology/Outcomes
Resolution of Hydronephrosis and Pain to Predict Stone Passage for Patients with Acute Renal Colic: Analysis from the STONE trial
S Jackman, A Maganty, A Wolfson, P Burrows, C MacPherson, N Montano, Z Kirkali, A Meltzer
UPMC
Introduction & Objective: To study patients presenting to the Emergency Department with acute renal colic to determine if resolution of hydronephrosis and pain accurately predicts stone passage on follow‐up CT.
Methods: This is a secondary analysis of a multi‐center prospective randomized clinical trial of patients diagnosed by computed tomography (CT) scan with a symptomatic ureteral stone <9 mm in diameter. Participants were followed to evaluate for analgesic use and to assess stone passage and hydronephrosis on a repeat CT scan obtained at 29‐36 days.
Results: Four‐hundred‐three patients were randomized in the original study and patients were included in this analysis if they did not have surgery for stone removal and had a CT scan and information on pain medication at follow‐up (N = 220). Hydronephrosis was detected in 181 (82%) on initial CT. At follow‐up CT, 43 (19.5%) participants had a persistent ureteral stone. Of these participants, 36 (84%) had no pain, 26 (60%) did not have hydronephrosis and 23 (53%) had neither pain nor hydronephrosis. Resolution of hydronephrosis was associated with stone passage (RR 4.6, 95% CI 1.9, 11.0), while resolution of pain was not (RR 1.1, 95% CI 0.9, 1.4).
Conclusions: In patients with urinary stone disease, stone passage is associated with resolution of hydronephrosis but not resolution of pain. In patients with persistent ureteral stones, neither pain nor hydronephrosis are consistently present. These findings have important implications on follow‐up imaging of patients with urinary stone disease.
Visual clarity of irrigants used during flexible ureterorenoscopy: an in vitro comparison
V Ulker, Z Gulerce, O Celik, C Yucel, E Can, B Turna
Department of Urology, University of Health Sciences Izmir Tepecik Training and Research Hospital
Introduction & Objective: Saline solution is the standard irrigant used during flexible ureteroscopy (f‐URS). However, there is an opinion that water has better visual clarity. Obtaining optimal image quality is quite important during f‐URS with fiberoptic devices, since suboptimal image quality may interfere with the efficacy of the procedure. In this in vitro study, we aimed to compare the visual clarity of isotonic saline, distilled water, and additionally 5% mannitol as irrigants for f‐URS.
Methods: An in vitro model consisting of an irrigant‐filled container and a fiberoptic f‐URS (Karl Storz Flex x2S ) was designed. A 1951 USAF Resolution Test Target (3x3 inch) within irrigants were used to evaluate the clarity of vision. The visual clarity was compared for 0.9% saline, distilled water and 5% mannitol solution by evaluaters with screen resolution. The tests were repeated after adding human blood (2/400 ml) and contrast (20/400 ml) to the irrigants.
Results: There was no significant difference in resolution values of three plain irrigants at a distance of 10 mm. However, when blood was added to the irrigants, a better resolution of 29.3% for water and 20.6% for mannitol was achieved compared to saline. At 20 mm of distance, it was observed that the difference was more pronounced in irrigants with blood. Water and mannitol had 55.6% and 37.1% better resolution than saline, respectively.
Conclusions: Water and 5% mannitol did not provide a significant image clarity advantage compared to saline. However, when blood was added to the irrigants, water provided significantly better visual clarity compared to saline. The use of water during various clinical scenarios in f‐URS should be further investigated.
Chloroquine attenuates hyperoxaluria‐induced renal oxidative injury and calcium oxalate crystal depositions via inhibiting NADPH oxidases
X Duan, S Yin, Y Liu, G Zeng
Introduction & Objective: Our previous study had indicated that chloroquine could attenuate hyperoxaluria‐induced oxidative injury of renal tubule cells, as well as calcium oxalate (CaOx) crystal depositions in rat kidney, but its underlying mechanism still has not been fully clarified. This study was carried out to reveal its possible underlying mechanism.
Methods: Sprague‐Dawley rats were randomly divided into three groups: control group, ethylene glycol‐induced hyperoxaluria model group and the model group pretreated with chloroquine. The renal CaOx crystal depositions were detected using Pizzolato staining method. The expressions of NADPH oxidases in rat kidney were detected via using real‐time qPCR and immunohistochemical staining. For the cell experiments, the expression and phosphorylation of PKCα and PKCδ, as well as NADPH oxidases' expressions, were detected by western blot, whereas the role of PKCs (including PKCα and PKCδ) in chloroquine‐mediated NADPH oxidases' expressions was confirmed though using PKC activator PMA in NRK‐52E cells.
Results: Chloroquine significantly decreased the mRNA and protein expressions of NADPH oxidases, including NOX2 and NOX4, as well as NADPH oxidase‐mediated oxidative injury of renal tubular cells in vivo and in vitro. In addition, chloroquine could attenuate oxalate‐induced phosphorylation of PKCα and PKCδ, whereas PKC activator PMA could obviously reverse the effects of chloroquine on oxalate‐induced oxidative injury of NRK‐52E cells and NADPH oxidases' expressions.
Conclusions: Chloroquine could significantly attenuate oxalate‐induced oxidative injury of renal tubular cells in vitro and in vivo, as well as hyperoxaluria‐induced CaOx crystal depositions in rat kidney, at least in part, via inhibiting PKC‐mediated expressions of NADPH oxidases, thus suggesting a novel possible application of chloroquine for the clinical prevention and management of CaOx nephrolithiasis.
Automatic computer‐aided in‐situ recognition of morphological features of pure and mixed urinary stones using intraoperative endoscopic images
V Estrade, m Daudon, f Bladou, j Bernhard, G Robert, B Denis De Senneville
Chu Pellegrin
Introduction & Objective: Endoscopic Stone Recognition (ESR) provides essential observations of stone morphologies. Artificial intelligence (AI) algorithms applied to various types of microscopic images of stones ex‐vivo proved to be a promising asset for automatic ESR using both peri‐ and post‐operative images [1]. In this study, we report the preliminary results of the automatic ESR of the morphological components of both pure and mixed urinary stones..
Methods: A urologist (VE, 20 years of experience) prospectively examined per‐operative endoscopic digital images of stones acquired between January 2018 and November 2020 (single‐center) using a flexible digital ureterorenoscope (Olympus URF‐V CCD sensor). Morphological criteria were collected and classified according to recommendations outlined in [2]. A deep convolutional neural network (CNN), ResNet‐152‐V2, was trained to predict five morphology classes from images obtained before LASER fragmentation: three pure stones (Ia/COM, IIb/COD and IIIb/UA) and two mixed stones divided into two morphologies (Ia/COM+IIb/COD and Ia/COM+IIIb/UA).
Results: The study included 347 observations of stone surface (pure stones: Ia = 191, IIb = 53, IIIb = 29; mixed stones: Ia+IIb = 64, Ia+IIIb = 10). Table 1 provides the performance of the implemented CNN classifier. In average, the accuracy was higher than 87 % for both pure and mixed stones.
Conclusions: AI is a good candidate for the automatic ESR of the morphological features of pure and mixed urinary stones composed of two morphologies. Combined with didactic boards of confirmed endoscopic images, both computer‐aided diagnosis and associated activation maps may be useful for urologists to recognise stones in‐situ using an endoscopic examination before destruction.
[1] Black et al. BJUI 2020, 125(6):920‐924
[2] Estrade et al. BJUI 2020, 10.1111/bju.15312
Postoperative Urinary Tract Infections After Flexible Ureteroscopy Using High‐Level Disinfection With 2 % Glutaraldehide for Flexible Scopes
P Alarcon, E Flores, EE Lozada, S Hector, BO Manzo
Hospital Regional de Alta Especialidad del Bajío
Introduction & Objective: Objective To describe the urinary tract infection incidence in flexible ureteroscopy using reusable scopes subjected to disinfection with 2% Glutaraldehyde.
Methods: Patients and Methods A cross‐sectional retrospective study was carried out. 347 patients treated with flexible ureteroscopy for lithiasis treatment were identified, and data was collected. The 2% Glutaraldehyde was used to disinfect the scopes in all surgeries. Disinfection protocol took 20 min. We included preoperative, intraoperative, and postoperative variables in statistical analysis. The SPSS statistics program was used for the statistical analysis. All variables were subjected to a normality test and subsequently Chi‐square. Fisher's exact test, Student's T‐test, or Mann Withney's U were applied, depending on the type of variable.
Results: A total of 233 patients met inclusion criteria and had complete data. An incidence of urinary tract infections of 8.5% was encountered. The side affected and gender was similar between infected and not infected patients (p = 0.614, and p = 0.109, respectively). There was a difference in age and BMI between the infected and not infected patients (p = 0.019 and p = 0.046). Schemes and antibiotic agents for prophylaxis were equally given between infected and non‐infected patients (p = 0.847). Other relevant variables like patients' comorbidities, stone burden, positive preoperative urine culture, or surgical time were not statistically significant (p > 0.05). The two most frequently isolated germs were Pseudomonas Aeruginosa and Escherichia coli, with five patients in each group. We obtained a negative urine culture in 4 patients (20%).
Conclusions: After flexible ureteroscopy with reusable ureteroscopes disinfected with 2% Glutaraldehyde, the urinary tract infection has an acceptable incidence. Moreover, similar to the incidence previously reported in the worldwide literature. The two most common germs isolated were Pseudomonas Aeruginosa and Escherichia coli.
A critical assessment of digital single‐use flexible ureteroscopes in a porcine model
SK Bechis, B Eisner, BR Matlaga, O Shah
University of California ‐ San Diego, Department of Urology
Introduction & Objective: Following the introduction of the digital single‐use flexible ureteroscope several years ago, an increasing number of products have come to the market. Each of these scopes has unique attributes that can affect their functionality. We undertook a study to characterize the performance of presently available digital single‐use flexible ureteroscopes in a porcine model.
Methods: Four female pigs (50‐60kg) were placed under general anesthesia, positioned supine, and retrograde access to the renal collecting system was obtained. The LithoVue™ (Boston Scientific), EU‐Scope (AnQing Medical; available in the US as Dornier Axis™), and WiScope® (OTU Medical) were each evaluated by four experienced surgeons. The following parameters were assessed quantitatively: time for navigation to the upper and lower pole calyces with and without implements (1.9F basket, 200 μm laser fiber, and 365 μm laser fiber). A qualitative rating (scale 1‐5) assessed: handle ergonomics, irrigation flow, image quality, and scope maneuverability. ANOVA statistical analysis was performed for comparisons among the groups, with statistical significance established at p < 0.05.
Results: The qualitative metrics included both baseline and last pass image quality ratings, which were significantly better for LithoVue than the AnQing and WiScope devices. Similarly, both baseline and last pass access metrics were also significantly better for LithoVue. The quantitative time measurements were not significantly different among the scopes when the upper pole was accessed with an empty working channel, 1.9F basket, and 200 μm laser fiber and when the lower pole was accessed with a 1.9F basket. Time measurements significantly favored the LithoVue for the remainder of the tests. Qualitative ratings significantly favored AnQing for upper and lower pole access with the 365 μm fiber. The remainder of the qualitative ratings related to navigation significantly favored LithoVue with the exception of empty working channel navigation to the upper and lower poles, which were not significantly different among the scopes. The comparisons are presented in the Table.
Conclusions: This study represents the first in vitro comparison of single‐use ureteroscopes from multiple vendors. In this study, the LithoVue performed significantly better than the AnQing and WiScope products. Further studies in clinical practice will provide additional information that will enable surgeons to distinguish the performance characteristics of these devices.
Predictive factors for ureteric stricture formation after ureteroscopic treatment of impacted ureteric stones
M Ramachandra, Z Al‐Nabulsi, Y Phan, P Osborn, A Auer, C Rowbotham, M Ismail
University Hospital Southampton, UK
Introduction & Objective: Introduction Ureteric stricture is a potential complication of impacted ureteric stone. In this study we investigated predicting factors of stricture formation after ureteroscopy for impacted ureteric stone
Methods: Surgical and radiological data for patient who underwent ureteroscopy for impacted ureteric stone were retrospectively reviewed.
Results: Between 2014 and 2019, 1340 patient presented with renal colic secondary to ureteric stone. A total of 297 ureteroscopy procedures were performed for impacted stones. Stricture rate was 3.3%. Analysis of radiological and surgical factors revealed that degree of hydronephrosis, intraoperative ureteric injury and residual stone fragments are statistically significant predicting factors for ureteric stricture formation.
Conclusions: Rate of stricture formation following ureteroscopic treatment of impacted ureteric stone remains low. Ureteric stricture may be a silent disease and can present with renal impairment. Therefore, it is essential to arrange postoperative imaging for high risk patients.
Prospective randomized comparison of classical retroperitoneoscopic pyelolithotomy versus percutaneous nephrolithotomy for solitary large pelvic kidney stones
V Singh, RJ Sinha, G Singh
Dept of urology, King George Medical University
Introduction & Objective: Percutaneous nephrolithotomy (PCNL) can be difficult in large pelvic stones in undilated systems. Retroperitoneoscopic pyelolithotomy can a feasible treatment option in these cases. We performed a prospective randomized comparison of retroperitoneoscopic pyelolithotomy (RP) versus percutaneous nephrolithotomy (PNL) for solitary pelvic stones >3 cm and assessed the outcome results.
Methods: From 2016 to 2019, 44 patients with a solitary pelvic stone >3 cm without any anatomical abnormality were randomized to either RP or PNL on a 1: 1 ratio. Stone‐free rate, number of procedures per patient and complications were recorded.
Results: The stone‐free rate on the first postoperative day was 95.5% in the RP group versus 72.7% in the PNL group (p = 0.04). The stone‐free rates at 3 months were similar between the two groups. Blood loss, visual pain analog score and analgesic requirement on the first postoperative day were significantly higher in the PNL group whereas the mean operative time and overall complications were similar between the two groups.
Conclusions: In patients with solitary large pelvic stones, RP is associated with lesser blood loss, postoperative pain and analgesic requirement as well as with a higher stone‐free rate in the immediate postoperative period in comparison to PNL. However, the stone clearance rate remains the same at 3 months in both groups.
Endoscopic Combined Intrarenal Surgery (ECIRS) – The new standard in the treatment of complex stone disease?
J Correia, M Madanelo, B Teixeira, G Mendes, S Mesquita, A Fraga, M Silva‐Ramos, V Cavadas
Department of Urology, Centro Hospitalar Universitário do Porto
Introduction & Objective: Percutaneous nephrolithotomy (PCNL) is currently the gold standard in the treatment of large urolithiasis. Although it is a safe and effective technique, it is still associated with important complications. Endoscopic Combined Intrarenal Surgery (ECIRS) combines the simultaneous approach of PCNL with retrograde URS, with the objective of treatment in a single procedure, reducing radiation exposure, complications and renal damage associated to PCNL. We aimed to evaluate the safety and efficacy of ECIRS in the treatment of high stone burden.
Methods: We performed a retrospective analysis of perioperative data and complications of all 148 patients submitted to ECIRS at our institution between January 2017 and November 2020. All surgeries were performed in modified supine Valdivia position. Stone free rate (SFR), defined as ≤3mm size, was evaluated by CT scan at 3 months.
Results: Patient's mean age was 52 ± 14 years, the majority of them females (72%). 16 had anatomical anomalies (11%), 5 had solitary kidney (3%) and 2 an urinary diversion with cutaneous ureterostomy (1%). 36 were previously stented with JJ (24%). Mean stone size was 38mm [IQR 31‐554], with a density of 819 ± 291 HU. The majority of patients had multiple or staghorn stones (73%), 6 of them being operated bilaterally (4%). Mean operative time was 128 ± 40min, using mainly pneumatic (70%) and LASER (15%) lithotripsy. 80% of the procedures used a single access (n = 118); the working sheath most commonly used was 17,5Fr (80%). Postoperative nephrostomy was placed solely in 24% of the patients during a median of 2 days [IQR 2‐4]. 1 of the procedures was totally tubeless. Median of hospital stay was 3 days [IQR 2‐3]. SFR was 65%, but only 9% needed a second procedure. There was a significant association between SFR and stone size (p = 0,034) but not its location (p = 0,70). The most common complication was transient fever promptly responsive to antibiotic (n = 25, 17%), and only 2 patients had complication grade ≥3 (arteriovenous fistula requiring embolization). Mean haemoglobin drop was 1,3gr/dL [0,6‐2,4], with only 6 patients needing blood transfusion (4%). None of the analysed variables (sex, BMI, diabetes, previous JJ, structural anomalies, struvite stones, location and number of accesses, surgery time and stone size) was associated with the occurrence of post‐operative complications.
Conclusions: ECIRS is a safe and effective procedure, offering an additional option for patients with multiple and complex lithiasis. Although in our analysis SFR was inferior to the described in the literature, stone size and his complexity were superior to previous reports, yet maintaining a low rate of complications.
A preoperative predictive score for uric acid kidney stones
MJ Basulto‐Martínez, S Proietti, M Pavia, L Rico, Y Yeow, J Flores‐Tapia, A Esqueda‐Mendoza, F Gaboardi, G Giusti
Dept. of Urology, Hospital Regional de Alta Especialidad de la Península de Yucatán
Introduction & Objective: Uric acid calculi (UAC) account for up to 15%. Recent evidence points that UAC <2 cm can be first treated by alkalinizing therapy with good results. Furthermore, alkalinizing larger UAC, may decrease the stone burden and therefore improve the chance of achieving a stone‐free rate in a further surgical procedure. We aimed to create a preoperative score for predicting UAC.
Methods: Patients who underwent kidney stones surgery from to March 2018 to March 2019 with available preoperative abdominal non‐contrast computed tomography (CT) scan and stone analysis composition were included and clinical data was obtained. Mean Hounsfield Units (HU) and standard deviation from the stone density (SDSD) were calculated from CT scans, as computed by growing Regions of Interest using OsiriX DICOM viewer Software. The stone analysis composition was carried out by infrared spectroscopy. Stones >80% of uric acid were dichotomized as UAC or otherwise as non‐uric acid calculi (NUAC). Categorical data were compared by X2 test, continuous data by the U‐Mann‐Whitney test, and logistic regression test was performed for categorical data and UAC. ROC curve analysis was conducted for the HU, SDSD, and UAC, and cutoff points were set. Using data associated with UAC, a score was constructed and tested.
Results: Ninety‐two patients were included with a median age of 55 (46 – 65) years and 53.3% were female. The stone composition was 67% calcium‐containing, 14% uric acid, 10 % infective, 7.7% cystine, and 1% other stones. HU was significantly lower in UAC group [400 (304 – 565) vs 689 (521 – 689), p < 0.001] as well as SDSD [152.2 (125.9 – 319.4) vs 358.1 (267.6 – 446.5), p < 0.001]. T2D and HTN were associated with UAC (p = 0.007 and p = 0.041, respectively) ROC curves for UAC and mean HU showed an area under the curve (AUC) of 0.851, [Coefficient Interval (CI) 95% 0.73 – 0.97], p < 0.001. As for SDSD, AUC was 0.808 (CI95%, 0.67 – 0.94). Cutoff points were selected according to the best specificity and sensitivity. Thus, a score ranging from 0‐4 was created based upon variables significantly related to UAC, which were HTN, T2D, mean HU <400, and SDSD <350. Score of 0, 1, 2, 3, and 4, resulted in UAC proportion of 0%, 6.7%, 25%, 66.7%, and 100%. The AUC for the score was 0.86 (CI 95% 0.77 – 0.96) p < 0.001. Patients with a score of 3‐4 had 71.4% of UAC (p < 0.001)
Conclusions: This easy‐to‐use preoperative score is useful in detecting patients who might have UAC and a better selection for an alkalinizing therapy can be performed. A score of 3‐4 is a powerful predictor of UAC and adds to clinical decision‐making for alkalizing therapy.
Pattern of key opinion leaders talks at major international urological meetings reflect the main differences in flexible ureteroscopy and PCNL diffusion
E Ventimiglia, F Quadrini, F Pauchard, H Kamkoum, S Doizi, O Traxer
Division of Experimental Oncology/Unit of Urology; URI; IRCCS Ospedale San Raffaele
Introduction & Objective: To analyze the pattern of speaker activity related to both flexible ureteroscopy (fURS) and percutaneous nephrolithotomy (PCNL) during plenary sessions at the main (endo)urological international meetings over the last 10 years.
Methods: We retrospectively reviewed the meeting programs of the main endourological international meetings (EAU, AUA, WCE, and SIU) during the period 2011‐2019. We detected all invited speakers at plenary and thematic sessions discussing either fURS or PCNL and collected both name and age at presentation. The proportion of fURS and PCNL talks was evaluated yearly during the study period. In order to analyze the variety of plenary session composition in terms of different panelists, we estimated and compared the mean number of talks per speaker according to surgical technique. We also analyzed possible differences in age distribution according to the topic of the talk as well as the presence of young (i.e. <45 years) speakers. Data were analyzed using descriptive statistics.
Results: During the last 10 years, a total of 498 plenary talks were found. Of those, 260 (52.2%), 211 (42.4%), and 27 (5.4%) discussed PCNL, fURS, or both respectively. The relative proportions of fURS vs PCNL changed during the last 10 years, with PCNL being more frequently discussed at the beginning and the end of the study period. Mean [SD] number of talks per speaker was higher for PCNL speakers (2.9 [3.4] vs 1.6 [1.4], p < 0.001), meaning that a wider variety of speakers was invited to give fURS talks. Speakers discussing fURS were younger (mean [SD] age 51 [9.5] vs 54 [8.5] years, p < 0.001), and a higher proportion of young speakers was observed in the fURS group (26% vs 15% p < 0.001). PCNL speakers were more commonly discussing fURS than fURS speaker discussing PCNL (23% vs 17%, p = 0.43).
Conclusions: We found a wider variety of speakers at fURS plenary sessions as compared to PCNL ones. Age at presentation was lower for fURS speakers, and a higher proportion of young experts was able to be invited to give a plenary talk. These data suggest that it is easier and quicker to become an internationally recognized expert in the field of fURS rather than PCNL. Moreover, PCNL speakers were able to master fURS as well more frequently than the other way around.
Withdrawn
Natural history of small asymptomatic kidney and residual stones over a long‐term follow‐up: Systematic review over 25 years
CE Lovegrove, R Geraghty, B Yang, E Brain, SA Howles, BW Turney, BK Somani
Department of Urology, Oxford University Hospitals NHS Foundation Trust; Nuffield Department of Surgical Sciences, University of Oxford
Introduction & Objective: Incidental identification of small, asymptomatic renal calculi has risen with increasing high‐resolution imaging. The natural history of such stones and small residual fragments remains unclear, however kidney stone disease (KSD) demands growing healthcare resource utilisation with wide‐ranging costs of treatment and varying management recommendations.
Methods: We systematically reviewed the natural history of small asymptomatic kidney and residual stones using the Cochrane and PRISMA methodology. We searched Medline, Scopus, Embase, EBSCO, Cochrane library and Clinicaltrials.gov using themes of “asymptomatic”, “nephrolithiasis”, “observation”, “symptoms”, “admission”, “intervention” and similar allied terms for all English language articles from 1996‐2020 (25 years). Inclusion criteria were studies of minimum 50 patients, stones ≤10mm, and mean follow‐up of ≥24 months. Primary outcomes were occurrence of symptoms, emergency admission and intervention.
Results: Our literature search returned 2247 results of which 10 papers were included in the final review. Risk of symptomatic episodes ranged from 0‐59.4%. Meta‐analysis did not identify any significant difference in the likelihood of developing symptoms when comparing stones <5mm to those >5mm, nor those <10mm to those >10mm. Risk of admission varied from 14‐19% and risk of intervention from 12‐32%. Meta‐analysis demonstrated significantly decreased likelihood of intervention for stones <5mm vs. >5mm and <10mm vs. >10mm. Studies had variable risk of bias due to heterogeneous reporting of outcome measures with significant likelihood that observed differences in results were compatible with chance alone (Symptoms: I2 = 0%, Cochran's Q = 3.09, P = 0.69; Intervention: I2 = 0%, Cochran's Q = 1.76, P = 0.88).
Conclusions: This systematic review indicates that stone size is not a reliable predictor of symptoms, however risk of intervention is greater for stones <5mm vs >5mm and <10mm vs >10mm. This review will inform urologists as they discuss management strategies with patients who have asymptomatic renal stones and offer insight to committees during the development of evidence‐based guidelines.
The T‐Tilt Position: a Novel Modified Patient Position to Improve Stone‐Free Rates in Retrograde Intrarenal Surgery
C Liaw, JA Khusid, B Gallante, JN Bamberger, WM Atallah, M Gupta
Icahn School of Medicine at Mount Sinai
Introduction & Objective: Residual fragments following retrograde intrarenal surgery (RIRS) can lead to future symptomatic stone episodes. The lower pole of the kidney presents a unique challenge as it is the most difficult location for RIRS. The T‐Tilt position is a novel modified patient position for RIRS in which the patient is positioned 15˚ Trendelenburg and 15˚ airplane away from the surgical‐side kidney (Figure 1). We investigated the efficacy of the T‐Tilt position in improving stone‐free rate (SFR).
Methods: In this IRB‐approved, prospective, randomized study, we recruited adult patients undergoing RIRS for stone removal. Patients were excluded if they had kidney abnormalities, pre‐existing ureteral stents, or a medical contraindication to the T‐Tilt position (e.g. congestive heart failure). Patients were preoperatively randomized to the standard or T‐Tilt position. Demographics, comorbidities, and operative parameters were recorded. SFR was determined with renal ultrasound and x‐ray at 1‐month follow‐up by a urologist blinded to the patient's study group. All complications, ER visits, and secondary procedures were recorded. Variables were compared using Kurskal‐Wallis test for continuous variables and chi‐square test for categorical variables.
Results: A total of 138 patients were enrolled with 75 patients in the standard cohort and 63 patients in the T‐Tilt cohort. The groups had similar patient demographic, clinical, and stone factors. The most common stone position was the lower pole (68.0% standard, 74.6% T‐Tilt). SFR was significantly greater in the T‐Tilt cohort amongst all patients (92.1% in T‐Tilt vs. 76.7% in standard, p = 0.015) and on sub‐analysis of patients with lower pole stones (95.6% in T‐Tilt vs 68.2% in standard, p < 0.001). There were no significant differences in operative times or Clavien‐Dindo scores.
Conclusions: The T‐Tilt position was associated with higher SFR. It is an atraumatic, cost‐effective technique in RIRS which may improve SFR and prevent future stone episodes.
Stone clearance using the EMS Swiss LithoClast® Trilogy: results of the European multicentre prospective study in comparison to the BAUS national PCNL outcomes on behalf of the European Society of UroTechnology
N Thakare, F Tanse, K Saeb‐Parsy, N Atassi, R Endriss, G Kamphuis, D Perez‐Fentes, M Hasan, M Brehmer, PJ Osther, HU Jung, BW Turney, W Finch, N Burgess, S Irving, L Dragos, E Liatsikos, T Knoll, V Cauni, O Wiseman
Cambridge University Hospitals Nhs Trust
Introduction & Objective: The EMS Swiss LithoClast® Trilogy is the latest generation lithotrite for PCNL, with a high clearance efficiency and faster stone fragmentation ability. The safety and efficacy of Trilogy has been evaluated in a prospective European multicentre study. We aim to assess the stone clearance rates in comparison to the BAUS PCNL audit outcomes obtained prior to the introduction of Trilogy.
Methods: 10 European centres evaluated the LithoClast® Trilogy, in a prospective non‐randomized study from 2019 to 2020. Data including stone characteristics, PCNL technique and stone clearance at the end of the procedure were recorded. Analysis was undertaken to determine the stone clearance rates with respect to stone size and stone complexity categorised by Guy's stone scores (I – IV). The findings were compared to the outcomes from the BAUS national PCNL audit data (2016 ‐ 2019), whose contributors used a variety of different lithotrites, other than Trilogy. Statistical analyses were performed using the Chi‐square test.
Results: 157 patients undergoing PCNL using Trilogy were included (53% male, 47% female; mean age 55 years, range 13 ‐ 84 years). The overall stone free rate on fluoroscopy screening at the end of the procedure was 82.8% [BAUS: n = 7431; overall stone free rate = 79.4% (p = 0.23)]. Stone clearance for sizes = < 2cm and >2cm were 90.7% and 78.6% respectively compared to 88.9% and 74.5% respectively for BAUS audit (p > 0.05). The clearance rates for Guy's stone score I, II, III and IV were 89%, 97%, 84% and 65% respectively, compared to 95.6%, 86.3%, 75.5% and 51.9% reported by BAUS (p > 0.05). The results are summarised in Table 1.
Conclusions: Our results demonstrate that when stratified according to stone size and stone complexity, the clearance rates for LithoClast® Trilogy are at least as effective as the outcomes reported from the prospective BAUS national database. None of the results reached a statistical significance, possibly due to low numbers in the Trilogy cohort. However, there is an indication that Trilogy could be a more efficient lithotrite in terms of stone clearance. These findings should be further evaluated, using clearance rates for stone size and complexity score in prospective studies for PCNL.
Long‐Term Evaluation of the Endockscope System: An Assessment of Global Usage
AS Afyouni, M O'Leary, Z Okhunov, A Peta, A Brevik, M Ayad, R Yoon, RM Patel, B Dolan, J Landman, RV Clayman
Department of Urology, University of California, Irvine
Introduction & Objective: The high costs of cutting‐edge endoscopic light sources and cameras restrict urologists from performing endoscopy in many underserved countries. Given the global prevalence of smartphones, we engineered a $45 smartphone alternative utilizing three‐dimensional (3D) printed attachments, an 8x lens, and a 1,000‐lumen light‐emitting diode (LED) cordless flashlight (the Endockscope System, ES).
Methods: Forty complimentary ES kits were distributed to urologists from 23 countries at the 2019 Congress of Société Internationale d'Urologie (8‐month group) and at the 2016 World Congress of Endourology (4‐year group) (Figure 1). Each participant was trained to use the ES. Urologists given an ES were asked to complete a survey in June 2020; the survey included questions regarding user satisfaction, comparability of the ES to standard endoscopic systems, and ease of use.
Results: All 18 urologists (100%) in the 8‐month group and 10/22 urologists (45%) in the 4‐year group completed the questionnaire. The ES was utilized by 83% (15/18) of urologists in the 8‐month group and by 80% (8/10) of urologists in the 4‐year group. Among urologists who used the ES, 67% in the 8‐month group and 57% in the 4‐year group noted that the ES performed equal or better than their standard endoscopic equipment. Using the human development index (HDI), a holistic measure of living standards across life expectancy, education, and the GDP per capita, we determined that the greatest impact was among urologists from the most fiscally challenged countries; indeed, in the 8 month and 4‐year groups, 100% of urologists from these countries were using the ES system. (Table 1) Lastly, although developed for fiberoptic cystoscopy, participants also used the ES for rigid cystoscopy, rigid and flexible ureteroscopy, and laparoscopy.
Conclusions: The ES provided an effective and inexpensive substitute for the standard high powered light source and endoscopic camera system at a cost of only $45. It was uniformly adapted by urologists in resource‐challenged countries.
Benchtop Assessment of a New Single‐Use Flexible Ureteroscope
P Whelan, RS Terry, R Qi, C Tabib, F Soto‐Paulo, GM Preminger, M Lipkin
Duke University
Introduction & Objective: Single‐use flexible ureteroscopes are an increasingly popular alternative to reusable ureteroscopes. In this study, we examined physical and optical properties of the new Dornier Axis™ (Webling, Germany) single‐use ureteroscope.
Methods: Ten new, never‐used Dornier Axis™ ureteroscopes were assessed for maximal tip deflection and irrigation flow rate with empty working channel and with insertion of a 200μm Flexiva™ (Boston Scientific, Marlborough, MA), 200μm and 365μm Moses™ (Lumenis, Yokneam, Israel) laser fibers and a 1.9Fr Zero Tip™ (Boston Scientific, Marlborough, MA) nitinol basket in the working channel. All ureteroscopes were then fully deflected 100 times in each direction, and maximal deflection angles were re‐measured. All measurements were performed in duplicate. In‐vitro optical testing for resolution, image distortion, and depth of field was performed against the LithoVue™ (Boston Scientific, Marlborough, MA) ureteroscope. Statistical analyses using t‐test and ANOVA were performed in R.
Results: Mean maximal deflection angles exceeded 300 degrees in both directions before and after 100 full deflection cycles except for the 365μm group. There was no change in maximal deflection following the 100 deflection cycles. There was difference in flexion with the various instruments in the working channel with the 365μm Moses™ fiber having the lowest flexion (downward flexion 293.3°, p < 0.002) (Figure 1).
Mean flow rate through an empty channel was 46.7 ml/min and decreased significantly with all used instruments (p < 0.001) (Figure 1).
Compared to the LithoVue™, the Axis™ demonstrated superior resolution at all tested distances and less distortion (‐6.59 ± 4.24% vs ‐19.72 ± 10.81%, p = 0.028) (Figure 2). The LithoVue demonstrated superior depth of field (Dornier vs Lithovue 4.5cm (IQR 4.3 ‐ 4.5 cm) vs 5.0cm (IQR = 5.0 ‐ 5.0cm) at 15 line‐pairs/mm, p = 0.014).
Conclusions: The Dornier Axis™ single‐use ureteroscope demonstrates high deflection angles that remain unchanged after 100 manual flexions in each direction and superior optical resolution compared to the LithoVue™
Novel Image Quality Evaluation Tool for Ureteroscopes: Validation Study Using Four Widely Available Digital Ureteroscopes
SN Patel, RK Jain, AT Cranwell, S Quarrier
University of Rochester
Introduction & Objective: We sought to compare the image quality of three single‐use ureteroscopes (Boston Scientific LithoVue, Dornier Axis, Pusen Uscope; all use CMOS sensors) to a standard digital reusable ureteroscope (Olympus URF‐V2; uses CCD sensor).
Methods: We recorded video from several ureteroscopy cases using each ureteroscope. A representative 1 minute clip of one case with each scope was created. Blinded urology attendings (n = 5) and residents (n = 5) rated image resolution, contrast, color, sharpness, glare, depth perception, distortion/artifacts, and overall image quality on a 5 point Likert scale using a novel evaluation instrument. Internal consistency was tested and MANOVA was used to compare responses.
Results: Forty surveys were completed. The results demonstrated internal consistency (Cronbach α = 0.95). The domain most correlated with overall image quality was image resolution (0.71). Overall image quality, image resolution and contrast were rated higher in the Olympus than the LithoVue while the Uscope was rated lower than other scopes; sharpness was higher in the URF‐V2 than other scopes; color, glare, depth perception, and distortion/artifacts were better in the URF‐V2 than the Uscope (all p < 0.05).
Conclusions: The standard digital reusable scope performed superiorly in nearly every category, suggesting a CCD sensor may provide better image quality and performance for cases where excellent visuals are required. It is notable that the single‐use LithoVue and Axis scopes performed quite well in overall image quality. The novel evaluation instrument demonstrated internal consistency, indicating appropriateness for use in future studies.
Is uric acid stone the 6th component in metabolic syndrome? A marker for worsening health
H Johnson, H Musleh, A Mitry, H O'Callaghan, J Philip
Bristol Urological Institute
Introduction & Objective: A 4%‐15% lifetime risk of developing urinary stones exists. Stone disease burden is increasing, with worsening morbidity and significant economic detriment to society. Recurrence risk of 50% within ten years has been reported, suggesting an exponential financial and health burden . Uric acid stone patients are a small subgroup with significantly associated co‐morbidity. This study evaluates the natural history of uric acid stone patients.
Methods: Over five years ending 2012, medical records of all patients with a uric acid stone composition were reviewed. Medical records (primary and secondary) were reviewed for co‐morbidity, baseline blood results, subsequent interventions, and follow‐up health trajectory.
Results: 203 of 2388 stone patients (8.5%) had Uric acid stones. Mean age was 61.4 years at diagnosis (range‐17‐91 years); with average follow‐up of 40 months. Male to female ratio was 2.4:1. Half of the stones were pure uric acid. Only 63 patients had hyperuricemia on diagnosis: with 17 patients reporting a gout diagnosis. Almost all patients had significant health compromise on stone diagnosis. 112 patients had metabolic syndrome parameters, with five having cancer. Over the follow‐up period, ten patients developed metabolic syndrome with one more cancer diagnosis.
Conclusions: Uric acid stones occur in <10% stone formers. These patients have significant health compromise on diagnosis with almost all patients having metabolic syndrome. These patients should have metabolic evaluation, dietary modifications, and pharmacotherapy to reduce risk factors for metabolic syndrome. Uric acid stone diagnosis implies worsening health risk and should trigger a more aggressive multi‐disciplinary management.
Cost‐Effectiveness of 90‐Day Single‐Use Flexible Cystoscope Trial: Single Center Micro‐Costing Analysis
M Assmus, AE Krambeck, M Lee, DK Agarwal, M Mellon, ME Rivera, T Large
Northwestern University, Department of Urology
Introduction & Objective: Use of flexible cystoscopy for hospital based urologic care (Emergency Department, intraoperative, inpatients) is invaluable for evaluation and management of many urologic diseases. Reusable flexible cystoscopes have widespread utilization with known associated upfront purchasing, processing and service costs. Advances in single‐use flexible cystoscope development have introduced alternative options to reusable flexible cystoscopes. However, there is a paucity of cost‐effectiveness studies examining implementation of a hospital based transition to single‐use scopes. Our primary objective was a 90‐Day cost‐effectiveness evaluation of utilizing single‐use flexible cystoscopes at a tertiary care center in the United States.
Methods: Following institutional device‐approval we initiated a 90‐Day trial period (November 1, 2020 ‐ January 29, 2021) where urologic care was provided with a single‐use disposable AMBU® aScopeTM 4 Cysto with reusable flexible cystoscopy only in cases where the single‐use scope failed or was unavailable. We performed a micro‐costing analysis examining per case cost (USD) of reusable flexible cystoscopy (including all servicing and processing costs) to the cost of the single‐use.
Results: Over the 90 day period, we encountered 85 cases (78 operative, 6 inpatient, 1 ED) where flexible cystoscopy was required. 78/85 (92%) cases were successfully completed with one single‐use disposable flexible cystoscope. Of the 7 failures, 4 were intraoperative cases where the AMBU scope failed to complete the required surgery and a reusable flexible cystoscope was required and 3 where access to the AMBU scope/monitor itself resulted in transition to reusable cystoscope use. Per use cost of the reusable flexible cystoscope at our center was $272.41 while per use cost for the single‐use is $185.00. Accounting for backup reusable scopes for disposable failures at a rate of 3 uses/month, extrapolating our data over an average 3 month period results in $9,785.71 cost savings or $39,142.84 annually.
Conclusions: This single center 90‐Day trial of single‐use flexible cystoscopies identified that based on our micro‐costing analysis, per‐use costs favor transitioning to single‐use flexible cystoscopes.
Predictors of flexible ureteroscope instrument repair: analysis of the last 2 years at the University Hospital Zurich
D Lavrek, C Poyet, D Schmid, T Hermanns, T Sulser, D Eberli, E Keller
Department of Urology, University Hospital of Zurich, University of Zurich, Zurich, Switzerland
Introduction & Objective: Flexible ureteroscopes are prone to damages. This study aims at evaluating procedural lifespan and hazards causing instrument repair.
Methods: All patients undergoing ureteroscopy (URS) between January 2018 and December 2019 were retrospectively identified. Medical charts were reviewed for data extraction. Only patients undergoing flexible URS were considered for analysis. Primary outcome was need for instrument repair after surgery.
Results: At total of 586 patients were identified. Of these, 486 patients (83 %) underwent flexible URS and were considered for analysis. Combination with percutaneous nephrolithotomy was found in 13 patients (3 %). Indication for surgery was stone disease in 397 (82 %), tumor in 57 (12 %), or other in 32 (7 %). Median age was 53 years (range 20 – 93). Male/female ratio was 2.03. Left/right side ratio was 1.25, with 30 bilateral cases (6%). Resident/senior operator ratio was 1.09. Lower pole URS was reported in 205 (42 %). Median operative time was 75 minutes (range 7 – 258). Ancillary device use was as follows: ureteral access sheath in 285 (59 %); laser fiber in 258 (53 %); basket in 352 (72 %). A total of 44 flexible URS needed to be sent for repair after surgery, resulting in a mean 11 interventions per instrument. Median instrument service time was 5 months (range 0.5 – 15). Univariable analysis revealed significant predictors for instrument repair: operative time (OR 1.31 for every additional 30 minutes; 95% CI 1.08 – 1.59; p = 0.007), lower pole URS (OR 2.12; 95% CI 1.13 – 4.00; p = 0.038) and laser fiber use (OR 2.01; 95% CI 1.04 – 3.90; p = 0.04). On multivariable analysis, only operative time was an independent significant predictor for instrument repair.
Conclusions: In an academic setting, each single flexible URS performs a mean 11 interventions until need for instrument repair. Operative time, lower pole URS and laser fiber use seem to be predictors of instrument repair.
“Are we there yet?”: Assessing the Accuracy of Artificial Intelligence in Calculating Renal Stone Volume
A Peta, C Chantaduly, P Jiang, A Brevik, L Limfueco, R Karani, R Arada, RM Patel, J Landman, P Chang, RV Clayman
Department of Urology, University of California, Irvine
Introduction & Objective: True stone burden in urolithiasis patients is vastly underestimated due to the use of only one or two dimensional measurements on plain x‐ray images or on computed tomography (CT) scans. With modern software, manual segmentation of a stone in CT images is able to create a true three‐dimensional (3D) volume. We sought to employ a deep learning technique, using convolutional neural networks (CNN), to automate the segmentation and volume calculation of renal stones on CT imaging.
Methods: A total of 771 renal stones from 119 unique patients were included in the study. For each stone, volume was calculated based on manual 3D volumetric segmentations of CT imaging, considered the ground truth. Volumes of each stone were also calculated with the European Association of Urology (EAU) ellipsoid formula. Using an initial seed point manually identified for each stone, a CNN algorithm was trained for stone detection and segmentation. Specifically, a 20 layer fully‐convolutional contracting‐expanding CNN spanning 473,410 parameters was designed to detect and segment renal calculi within a 48 x 48 x 48 voxel cube in the vicinity of the seed point. Both a Pearson correlation coefficient and Dice score, a metric of spatial overlap, were used to assess model performance against manual segmentations. Total statistics were aggregated after five‐fold cross‐validation.
Results: The CNN algorithm calculated stone volumes compared to manually segmented stone volumes had a dice score of 0.56 and a Pearson correlation coefficient (r value) of 0.82. Volume calculations with the EAU ellipsoid formula had a weaker correlation with the manually segmented volumes (r = 0.75).
Conclusions: Deep learning convolutional neural networks can automatically segment renal stones and estimate stone volume better than traditional validated volume formulas. Further refinement of the CNN is needed for auto‐segmented stone volumes to reach the same accuracy as manual segmentations.
Moderated Poster Session 07: Imaging I
Comparing PSMA‐PET, biopsy pathology, and MRI for prediction of Extra‐prostatic extension (EPE) and surgical guidance in prostate cancer
CD Bahler, M Green, M Tann, K Collins, J Swensson, E Brocken, L Cheng, D Alexoff, H Kung, M Koch
Urology
Introduction & Objective: Injury to nerves and muscle tissue during prostatectomy causes incontinence and impotency. However, preserving nerves and muscle adjacent to prostate cancer risks positive margins; therefore, prostatectomy would benefit from guidance of more accurate imaging.
Methods: A retrospective analysis was performed of clinical trials for PSMA‐PET targeted imaging (68Ga‐P16‐093 or 68Ga‐PSMA‐11) prior to prostatectomy. 68Ga‐P16‐093 has up to 3‐times less excretion in urine as compared to PSMA‐11. A blinded review of PET and MRI scans was performed to predict the risk of extra‐prostatic (EPE) extension at the right or left nerve bundle. Stata 13.1, Pearson's Chi2, and McNemar's Chi2 were used for accuracy statistics.
Results: A total of 46 patients were imaged with either 68Ga‐P16‐093 (n = 25) or 68Ga‐PSMA‐11 (n = 21) PET imaging. Age (62 vs 63 years), PSA (7.3 vs 7.9), and biopsy pathology (3 + 3: 0 vs 5%, 3 + 4: 28 vs 29%, 4 + 3: 24 vs 19%, ≥4 + 5: 48 vs 48%) were similar between the groups (p > 0.30). There were 17 (37%) with pT3a (EPE) and 12 (26%) with pT3b on final pathology. Overall positive margin rate was 12 (26%). Index lesion SUVmax was similar between P16‐093 and PSMA‐11 (10.3 vs 10.0). EPE Sensitivity (87 vs 94%), Specificity (77 vs 76%), and ROC area (82 vs 85%) were similar between P16‐093 and PSMA‐11, respectively (p = 0.32). MRI (available in 23) found high specificity (89%) but low sensitivity (63%) and the overall ROC area was lower when compared to pooled PSMA‐PET (.76 vs .84, p = 0.04). For pooled PSMA‐PET imaging, a treatment change from “non‐nerve sparing” to “nerve sparing” was recommended in 17/46 (37%) of patients. A total of 10 men had nerve‐sparing (treatment change) based on PSMA‐PET imaging with one (10%) having a positive margin. Figure 1 shows a case where the cancer was away from the nerve‐bundle on PSMA‐PET imaging.
Conclusions: PSMA‐PET imaging can improve surgical guidance resulting in preservation of nerve‐bundles. 68Ga‐P16‐093 PET and 68Ga‐PSMA‐11 PET had similar accuracy for predicting extra‐prostatic extension.
Targeted MRI/US Fusion and Standard TRUS Prostate Biopsy: 563 Patients ‐ Relationship Between PIRADS Score and Prostate Cancer Detection Rate: A Single Urologist's Experience
A Kasraeian, M Alcantara, K Mola Alcantara, J Yellin, A Brochert, J Cesaretti, A Kasraeian
Kasraeian Urology
Introduction & Objective: Multi‐parametric MRI (mpMRI) and targeted MRI/Ultrasound fusion prostate biopsy (tMRI/US FPB) are important tools in the diagnosis of prostate cancer (PCa). We report our experience with a total of 563 patients. Specifically, we report the relationship between PIRADS score and overall positive biopsy rate as well as detection rate of Gleason (G) 7 or higher PCa in men.
Methods: Data was prospectively collected and analyzed on 563 men undergoing tMRI/US FPB and TRUS standard biopsy between January 2017 and December 2020. In all patients, mpMRI was interpreted by a single radiologist using the PIRADS scoring system. 3D rendering of regions of interest was performed prior to tMRI/US FPB performed by a single urologist using the Invivo UroNav System. Concurrent standard 14 core biopsy (14Bx) was performed in all cases. Data was Prospectively collected and analyzed.
Results: Prostate biopsy was performed on 563 men between January 2017 and December 2020 of whom 62% (350/563) were diagnosed with PCa. Of men diagnosed, 63% (220/350) were diagnosed with G7 or higher disease. Among PIRADS 3 Fusion biopsies, the positive rate for PCa was 68% (127/178) with 46% (82/178) being G7 or higher disease (15% (26/178) G8‐9 PCa). Additionally, among PIRADS 4 Fusion biopsies, the positive rate for PCa was 95% (38/40) with 93% (37/40) being Gleason 7 or higher disease (38% (15/40) G8‐9 PCa). Lastly, among PIRADS 5 Fusions prostate biopsies 93% (14/15) were positive for a PCa with all but one being a G7 PCa or higher 87% (13/15) and 67% (10/15) being G8‐9 PCa. The overall positive rate for MRI‐US Fusion prostate biopsies was found to be 74% (198/268). G7 or higher disease was found in 53% of those men (with 20% being G8‐9 PCa). The TRUS standard prostate biopsy positive rate was 51% (151/295) with 18% being G7 or higher disease (3.7%, G8‐9 PCa).
Conclusions: tMRI/US FPB is an important technology which increases the diagnostic yield of prostate biopsy when combined with 14Bx. In our series, the increased positive biopsy rate with combined tMRI/US FPB‐14Bx was statistically significant when compared to 14Bx alone. In addition, tMRI/US FPB‐14Bx found more Gleason 7 or higher PCa. Lastly, PIRADS 4 and 5 lesions on mpMRI were associated with higher rate of both overall and Gleason >7 PCA detection.
Retrograde uretero‐pyelography without diagnostic ureteroscopy has superior intravesical recurrence‐free survival compared to performing ureteroscopy in nephroureterectomy for upper urinary tract urothelial carcinomas
K Kim, H Yang, S Kim, D Kim, C Lee, Y Jeon
Department of Urology, Soonchunhyang University Cheonan Hospital, Soonchunhyang University College of Medicine
Introduction & Objective: Ureteroscopy prior to nephroureterectomy (NU) is a practical and powerful tool to diagnose upper urinary tract urothelial carcinomas (UTUC). However, ureteroscopy before NU has a potential limitation which could pose a risk factor for intra‐vesical recurrence. Therefore, we tried to identify the risk factor of intravesical recurrence after NU, and to investigate whether retrograde uretero‐pyelography (RGP) without diagnostic ureteroscopy could be another diagnostic option in UTUC.
Methods: From total 77 UTUC patients who underwent NU, 65 patients were finally enrolled in this study, 12 patients who underwent NU without further evaluation after a computed tomography examination were excluded. Univariate and multivariate analyses based on Cox's regression were performed to identify independent prognostic factors for intravesical recurrence‐free survival (IVRFS) after NU.
Results: From the total 65 patients, 32 patients have underwent diagnostic ureteroscopy and 33 patients have underwent RGP without ureteroscopy before nephroureterectomy. Patients who received RGP without diagnostic ureteroscopy were found to have significantly superior IVRFS compared to patients who received diagnostic ureteroscopy by Kaplan‐Meier curve analysis (p = 0.022). RGP without ureteroscopy before nephroureterecomy (hazard ratio, 0.388; p = 0.030) was a significant independent predictor of IVRFS after radical nephroureterectomy.
Conclusions: The diagnostic ureteroscopy procedure prior to nephrouretrectomy has a significant effect on IVRFS. RGP without diagnostic ureteroscopy can be another diagnostic option to reduce intravesical recurrence after NU in UTUC.
Defining the non‐contrast computerized window setting for optimal colon identification prior to percutaneous nephrolithotomy
S Dekalo, Z Savin, I Mintz, H Hertzberg, I Masarwe, G Aviram, O Yossepowitch, M Sofer
Tel‐Aviv Sourasky Medical center, Sackler School of Medicine, Tel‐Aviv University
Introduction & Objective: Colonic injury during percutaneous nephrolithotomy (PCNL) is a rare, however, disastrous complication. Therefore, preoperative accurate identification of colon on cross sectional imaging, usually non‐contrast computed tomography (NCCT), is essential in planning the access and reducing the risk of its occurrence. The lack of contrast material, collapsed bowel segments and previous intraabdominal operations may limit proper colonic recognition on NCCT. We aimed this study to assess which NCCT window setting provides the optimal colonic identification for PCNL preoperative planning.
Methods: Twenty‐two axial NCCT images of 11 consecutive patients scheduled for PCNL were reviewed by a senior endourologist who chose the most representative ones for planning the PCNL puncture. Ten urologic surgeons (4 specialists, 6 residents) reviewed these images in a randomized blinded order using 2 window settings (abdomen and lung). They were asked to mark the colonic area in each image using a dedicated commercially available area calculator software (Bluebeam, Pasadena, USA). Statistical assessment was conducted.
Results: Overall, the mean marked colonic area was greater in the lung window in comparison to abdomen window: 8.82 cm2 vs 7.4 cm2, respectively, p < 0.001). Changing the CT‐window from abdomen to lung resulted in increased identified colonic area in 44 images (50%), similar area in 30 images (34%) and decreased area in 14 images (16%). Intraclass correlation showed good agreement between the senior readers and among all readers (0.92 and 0.87 respectively). Senior urologists had consistent area measurements (no difference in area measurements between abdomen and lung windows) in 13/22 cases, while residents had no difference in area measurements in only 17/66 cases (p = 0.008).
Conclusions: Lung window solely or in combination with abdomen window appear to provide the most accurate colonic demarcation for pre‐operative planning of PCNL access. This pattern is more evident among young urologists and may reduce the risk of colonic injury.
ABSTRACT WITHDRAWN
MRI/TRUS target prostate fusion biopsy learning curve in two residents at a referral center: a retrospective analysis on more than 1000 procedures
E Checcucci, F Piramide, D Amparore, S De Cillis, G Volpi, A Piana, S Granato, A Pecoraro, P Alessio, B Carbonaro, J Mézière, G Cattaneo, F Ragni, M Manfredi, C Fiori, F Porpiglia
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
Introduction & Objective: During last years, prostate cancer (PCa) detection has been improved by the implementation of software allowing to perform MRI‐transrectal ultrasonography fusion‐guided prostate biopsy (MRI/TRUS fusion biopsy, FB). The aim of our study was to assess the learning curve (LC) of two urology residents in the execution of fusion biopsy (FB) considering overall prostate cancer (PCa) and clinically significant (cs) PCa detection rate (DR), based on different lesions' characteristics at the MRI.
Methods: We extracted data from our prospectively maintained database from January 2015 to December 2019. FB was carried out with the BioJet fusion system (D&K Technologies, Barum, Germany) either by a transrectal or transperineal approach. An ANOVA test was used to assess the homogeneity of the cohort. Multivariable linear and logistic regression analysis were used to assess the correlation between operator experience and DR for PCa and csPCa. At last, the postprocedural complication rate trend was determined.
Results: 1005 men were enrolled in the study. During the five years of the study, the pre‐biopsy characteristics of the patients enrolled did not change significantly except for the proportion of patients who previously underwent prostate biopsy (p < 0.001) and the number of mpMRI performed at referral centers (p = 0.002), both showing a decreasing trend over time. The overall DR of PCa was 61.2% (615/1005) [IC 0.58 ‐ 0.64]; whilst DR for csPCA was 54.6% (549/1005) [IC 0.51 – 0.57]. Operator experience does not appear to impact the DR of overall PCa and csPCa. On the contrary, in case of lesions with diameter <8 mm, PCa and csPCa DR were significantly higher with operator experience (p = 0.048 and p = 0.038, respectively). Considering the suspicious tumours located in the more challenging areas of the prostate (transitional or posterolateral zone) were not significantly better diagnosed with experience improvement (p = 0.34 and p = 0.22 for PCa DR and csPCa DR respectively). The specific analysis focused on PI‐RADS 5 lesions, mpMRI performed in referral centers, or for patients at repeated‐biopsy did not reveal a significant relationship between operator experience and PCa or csPCa DR. Complication rate was stable during the whole study (p = 0.75).
Conclusions: A standardized FB approach demonstrated to be feasible, safe, and effective since the start of residents' LC. PCa and csPCa DR was stable, after >1000 biopsies. Nevertheless, in case of lesions <8 mm, the execution of at least 100 FB is fundamental in order to correctly sample the area.
New indication algorythms for Active Surveillance in the era of MRI‐targeted prostate biopsies
C Wetterauer, J Federer‐Gsponer, F Leboutte, R Mona, J Ebbing, C Rentsch, L Manka, H Seifert, S Wyler, F Recker, M Kwiatkowski
University Hospital Basel, Department of Urology
Introduction & Objective: Active surveillance (AS) strategies have been established to avoid overtreatment of low risk prostate cancer (PCa) patients. Low tumor volume, as reflected by the number and the percentage of positive biopsy cores, represents one of the indication criteria for AS. Applying this criterion after MRI targeted prostate biopsies might lead to an overestimation of the tumor volume, wherefore patients who would actually be suitable for an AS strategy would be exposed to the risk of being over‐treated.
Methods: This retrospective analysis included 318 patients in which PCa was detected by MRI‐TRUS‐fusion prostate biopsy. Biopsies were performed at two Urological centers in Switzerland between January 2016 and November 2018. We assessed the effect of targeted biopsies and temporary rating strategies on eligibility for AS, and developed new algorithms. Patients were grouped according to “classic” Epstein criteria and an “extended” definition including Gleason 7a. We developed a “composite 1” definition based on the prostate specific antigen (PSA) and the Gleason Score in all biopsies in combination with the number of positive random biopsies and according tumor involvement; and a “composite 2” definition based on PSA, the Gleason Score in all biopsies in combination with MRI measured tumor volume.
Results: Based on random biopsies only, 44 of the 318 patients (13.8%) qualified for AS according to current guidelines, and 60 patients (18.9%) fulfilled the extended indication criteria for AS including Gleason 7 disease. Targeted biopsies identified ineligibility for AS according to the classic indication in 24 of the 44 patients (54.5%), and according to the extended indication in 36 of the 60 patients (60.0%). The reasons for ineligibility for AS according to classic and extended indication were upstaging of Gleason score in 9 and 5 patients, identification of more than 2 positive biopsies in 11 and 19 patients, and identification of more than 50% tumor load in 5 and 8 patients, respectively. Application of the “composite 1” definition led to the AS eligibility of 52 of 248 patients (20.97%) in the “classic” and of 77 of 248 patients (31.05%) in the “extended” group. Classic rating strategies as well as the “composite 1” score included a significant rate of patients with tumor volume of more than 0.5cm3.
Conclusions: Classic rating strategies tend to underestimate tumor volume whereas targeted biopsies lead to overstimation of tumor volume. We could demonstrate that classic algorithms led to formal ineligibility of patients for AS and propose a new imaging based rating algorithm to improve tumor assessment for a more accurate indication for AS.
Intraoperative Contrast Enhanced Ultrasound To Reduce Unnecessary Ureteral Stent Placement After Ureteroscopy
J Ahn, D Bayne, F Hamouche, M Stoller, T Chi
UCSF
Introduction & Objective: Ureteral stents are a significant source of morbidity. The decision to place one at the time of retrograde intrarenal surgery (RIRS) is often subjective and based on limited clinician judgement. A reliable tool is needed to guide urologists and avoid unnecessary stent placement. Contrast enhanced ultrasound (CEUS) is a safe, readily adaptable technology where a microbubble contrast agent is instilled into the upper urinary tract (Figure 1). We propose an intraoperative retrograde CEUS test during RIRS to help predict post‐operative ureteral drainage and the need for ureteral stent placement.
Methods: For this pilot feasibility study, we performed CEUS in patients undergoing RIRS for nephrolithiasis. After stone treatment, the renal collecting system was decompressed, then 1 ml of CEUS contrast and a 2 ml flush was instilled per ureteral catheter. For the flush, iodinated contrast was substituted for saline to permit comparison of CEUS with fluoroscopic drainage. After catheter removal and 2 minutes for ureteral rest, the bladder was cycled with irrigation and then scanned with CEUS and fluoroscopy for passage of either contrast agent (Figure 1). Ureteral stent placement was determined based on preexisting standard of care. Post‐operative unplanned encounters (PUE) including patient calls, emergency visits, and hospital admissions were tracked.
Results: 41 renal units from 39 patients underwent CEUS during RIRS (Figure 2). Stent omission was successful with no PUE in 91% (21/23 units) with CEUS drainage. Compared to those who had a stent placed based on no CEUS drainage, those who did not have a stent based on drainage had a significantly lower incidence of complications (9% vs 53%, p = 0.006) Fluoroscopic drainage was discordant with CEUS drainage in 12 renal units. In all cases of discordance, drainage was seen on CEUS but not on fluoroscopy.
Conclusions: CEUS is a novel means to objectively assess upper tract drainage at the time of RIRS. Our results suggest that retrograde CEUS could predict successful stent omission and may be more sensitive for predicting drainage than fluoroscopy due to low contrast volumes.
Using Hounsfield unit (HU) ‐ volume models of kidney stones to predict successful stone dusting during retrograde intra‐renal surgery (RIRS)
D Kim, S Jeon, S Lee, C Lee, S Chang, S Lee
Department of Urology, School of Medicine, Kyung Hee University
Introduction & Objective: Computer tomography (CT) of renal stones and measurement of their Hounsfield unit (HU) is commonly used for evaluation before the treatment of urolithiasis. We measured the volume of all HUs in a single stone and drew a model depicting the stone's HU distribution in order to predict success of dusting technique during retrograde intrarenal surgery (RIRS).
Methods: The medical records of 131 patients who underwent RIRS from January 2018 to January 2019 at Kyung Hee University Hospital were reviewed and 168 kidney stones were initially examined. Stones that were larger than 1cm were included and a total of 49 patients with 55 stones were evaluated. The stones were divided into two groups according to intra‐operative dusting success. Dusting was considered successful when stone disintegration was achieved with a laser setting of energy 0.2‐0.4 J and frequency 50 Hz. If higher laser energy settings (fragmentation) and extraction was needed, it was considered as dusting failure. 3‐dimensional models of the stones were reconstructed, and maximal HU, minimal HU, difference between max and minimal HU, HU standard deviation, stone volume, volume of peak HU was evaluated.
Results: Among the total 55 stones, 32 were successfully dusted and 23 were fragmented during surgery. Dusted stones showed a more heterogenous distribution of HU while fragmented stone HUs were more homogenous. “Success of dusting” group had higher mean difference in max and minimal HU (1102.94 ± 376.63 vs 794.91 ± 415.05, p = 0.0073), higher HU standard deviation (262.73 ± 112.61 vs 155.65 ± 95.69, p = 0.001)) and smaller volume of peak HU (4.52 ± 2.53 vs 13.28 ± 8.10, p < 0.0001). When we drew histograms of the HU, dusted stones were wide and rugged while fragmented stones were mostly narrow and peaked.
Conclusions: Stone reconstruction models and evaluation of HU volumes showed that stones with smaller peak HU volumes and higher differences in max and minimal HU could be considered more fragile and prone to successful dusting. Stones that show this type of HU distribution should be considered candidates for RIRS even if their size is larger than current recommendations.
Human vs Machine: Comparison Of Manual CT Measurements Versus Automated Software Of Stone Phantoms
L Peard, M Cash, I Mohamed, AM Harris, JR Bylund, AA Bhalodi, J Lee, J Bell
Univeristy of Kentucky
Introduction & Objective: Given the significance of stone size in management of urolithiasis, obtaining accurate and precise measurements is paramount. We compared software and manual stone length and volume measurements to actual measurements of stone phantoms.
Methods: Seventeen unique stone phantoms were created in a variety of shapes and sizes using BegoStone Plus. Stone length, width, and height were measured with electronic calipers. Stone volume was measured using volume of displacement in water. Stone phantoms were placed in saline and imaged with CT. CT images were uploaded into post‐processing software which analyzed the stones for maximum length and volume. Two urologists assessed the imaged stones for length, width and height and were blinded to the software measurements. Stone volume was calculated using the ellipsoid formula 0.52 x length x width x height.
Results: The stone phantom length ranged from 5.5mm to 63mm with volumes of 40mm3 to 16,000mm3 (Figure 1). The software had the closest approximation to the actual stone length with a median percent error of 6.2% (IQR 3.1%‐9.4%). Readers 1 and 2 had median percent errors of 5.7% (IQR 3.7%‐14.1%) and 7.8% (IQR 2.1%‐17.2%) respectively. Reader 1 and 2 both differed from the software with median percent differences of 16% (IQR 8.6%‐22.4%) and 17.1% (IQR 5.2%‐28.4%). The readers had a median percent difference from each other of 4.1% (IQR 3%‐6.6%). None of the length measurements by the software or the human readers differed significantly from the actual stone phantoms (P > 0.610). The percent errors with regards to volume for the software, reader 1 and reader 2 compared to actual stone volume were 20% (IQR 14.2%‐30%), 18% (IQR 5.2%‐39.8%), 24.1% (IQR 10.2%‐33.2%), respectively. Reader 1 and 2 differed from the software with median percent differences of 33.1% (IQR 21.7%‐59.5%) and 26.3% (IQR 15%‐48%), respectively. The readers had a median percent difference from each other of 17.3% (IQR 7.5%‐32.5%). None of the measurements by the software or the human readers differed significantly from the actual stone phantom volume (P > 0.697).
Conclusions: Software measurements approximated the actual measurements for the stone phantoms while eliminating interobserver variability. Using post‐processing software to measure urinary stones appears to be as accurate as human readers, but with greater precision.
Xray and US free calix puncture before PCNL (XUF PCNL). Comparison with standard Xray/US guided puncture
M Maltagliati, L Berti, C Buizza, U Besana, A Calori, M Justich, C Gastaldi, M Sighinolfi, S Micali, BC Rocco, G Bozzini
ASST Valle Olona
Introduction & Objective: The most challenging part of a percutaneous nephrolithotomy (PCNL) is the perfect puncture of the planned calyx. HoloLens based augmented reality system has been descibed as an helpful tool to assist the surgeons in different fields. After the evaluation of this new technique with an ex vivo model we planned a clinical study to compare the standard puncturing technique fluoroscopy and ultrasound guided with the this new Augmented Reality Technique.
Methods: We performed a matched pair analyses and created two groups with 20 patients each. In one group a standard ultrasound and fluoroscopy guided puncture was perfomed and in the other group the XUF PCNL assisted puncture of the renal pelvis was performed. To puncture the collecting system with the HoloLens augmented reality, we placed three radiopaqued markers from the radiotherapy on the patients skin around the kidney. A preoperative multi‐slice CT with a low dose and a late‐contrast phase was taken in prone position on a specific PCNL‐cushion as it is used during surgery. The markers, as well as all needed organs such as kideny, stone, bowel, liver etc. were segmented with a proper software to mimic also their movement during puncture. For the surgery the patient is placed in the same position as for the CT and the radiopaqued marker are replaced with coloured markers in two rows. The HoloLens are used as a glass‐camera to guide surgeon's hands and needle. The puncture is then perfomed. We measured the radiaion exposure, puncture time and attempts to a successful puncture in the two Groups. The complications were also documented.
Results: There was a significant difference between the radiation exposure and the puncturing time regarding the two techniques. There was no significant difference regarding the puncture attempts between the two puncturing techniques (p‐value = 0.45).
Conclusions: The XUF guided puncture can be compared to the standard puncturing techniques and is a feasible method for planning a puncture for patients with complicated nephrolithiasis. The great advantage is the Xray free exposure An HoloLens device is mandatory to complete a XUF PCNL.
Should the Pelvis be Included in CT Imaging of Asymptomatic Urinary Stone Patients? A Retrospective Review
M Fritz, J Zhang, A Ayoob, J Bell
Univeristy of Kentucky
Introduction & Objective: CT is often used for surveillance of urinary stone disease because of its superior stone imaging characteristics, however, it confers more radiation than renal US or x‐ray. In an effort to decrease radiation, we evaluated the effects of eliminating the pelvis from the CT scan for asymptomatic follow‐up patients with urolithiasis.
Methods: We queried our medical record for any CT Abdomen/Pelvis (Abd/Pelvis) between January 2017 to April 2019. We then narrowed the cohort by looking at patients who had this done in preparation for a routine stone visit with one of our endourology providers. Patients were excluded from analysis if the record was incomplete or if it indicated they were symptomatic from stones at the time of the visit. The abdominal region was defined as T11‐L5 (Figure 1). CT scan images were reviewed to see if any stones or significant pathology would have been missed by only having the abdominal images. Effective radiation doses (ED) were estimated from CT imaging using VirtualDoseTMCT software (Virtual Phantoms, Inc). Institutional charges for Medicare were queried and compared for: CT Abdomen/Pelvis, CT Abdomen, Renal US, and KUB.
Results: 80 patients were included in our analysis with 61 patients having non‐obstructing stones on these scans. The mean age was 53 (range = 20‐81) with a mean BMI was 32 (± 8.7). None of the patients were found to have any new, clinically significant stone‐related pathology in the pelvis. 13 patients had incidental pelvic findings that required no intervention (ex, prostatomegaly or thickened bladder). The mean effective dose reduction of eliminating the pelvis was 45% (7.9 mSv vs 4.4 mSv). The mean Medicare charges for imaging studies were as follows: CT Abd/Pelvis = $4,179, CT Abd = $2,458, Renal US = $1,190, and KUB = $471.
Conclusions: Excluding the pelvis does not appear to miss any ureteral stones in asymptomatic patients presenting for routine follow‐up. This appears to be an effective and easy way to reduce both cost and radiation while not missing any significant pathology.
Does CT scan after ultrasonography change surgical planning for nephrolithiasis?
A Ludvigson, P Motamedinia
Yale New Haven Hospital
Introduction & Objective: Ultrasound (US) is often used to diagnose nephrolithiasis, but it is less accurate than CT scan, potentially affecting surgical plans. We examined how often obtaining a CT scan after US changed the indicated management of nephrolithiasis, to see if risk factors that determine inaccurate US scans could be identified.
Methods: Approval was obtained through our institutional IRB. From those who presented to our health system over the past 3 years with suspected nephrolithiasis, we selected patients who had undergone a retroperitoneal US, and then a CT scan within 30 days. We recorded stone size and location for all studies. We recorded stone density and skin‐to‐stone distance for each CT scan. Using current AUA guidelines, we determined the indicated procedure based on findings of each imaging study: shockwave lithotripsy (SWL), ureteroscopy (URS), or percutaneous nephrolithotomy (PCNL). We used Minitab software to perform all statistical analysis, i.e. general linear models and two‐tailed Student's t‐tests.
Results: 305 patients met inclusion criteria. Of these, the CT scan changed the indicated procedure 108 times (35.4%). 26 US studies indicated SWL; CT changed 19 of these (73%). 129 US studies indicated URS; CT changed 62 of these (48%). 24 US studies suggested PCNL; CT changed 9 of these (37.5%). Using CT as the gold standard, 18 US studies were false positive for stones (sensitivity = 0.72). 51 US studies were false negative for stones (specificity = 0.86). Average body mass index (BMI) was significantly lower in the patients with a false positive US as compared to those with a true positive US (26.59 versus 29.13 kg/m2, t(24) = 2.33, p = 0.029). When comparing patients who had their indicated procedure changed by the CT scan to those who did not, there were no significant differences in age, BMI, or skin‐to‐stone distance. However, those who had their procedure changed had significantly lower density stones (566.1 versus 747.5 HU, t(154) = 2.92, p = 0.004). When patients were examined in subgroups based on what their indicated procedure was before and after the CT scan, there were also no significant differences based on age, BMI, or skin‐to‐stone distance. There was a significant difference based on HU, with stone density explaining 22.88% of the variation (F(11,154) = 4.15, p < 0.001).
Conclusions: US has many advantages over CT, but cannot always be used in place of it. Our study demonstrates that a CT scan changes the indicated stone treatment in more than 1/3 of cases, and that lower‐density stones are a risk factor for inaccurate US findings. US should be used with particular caution in those with a history of low‐density stone types, and for SWL surgical planning.
Utilization of low‐dose CT for evaluation of urolithiasis at a high‐volume stone referral centre
EP Chan, F Gabrigna Berto, O Daher, Z Syed, C Dawson, J Amann, J Bjazevic, H Razvi
Western University
Introduction & Objective: Non‐contrast computed tomography of the kidneys, ureters, and bladder (CT KUB) is the gold standard for evaluation of urolithiasis. Radiation from repeat CT increases the risk of secondary malignancy and physicians should strive for radiation doses as low as reasonably achievable. Low‐dose CT (LDCT; < 4mSv) has excellent performance in the diagnosis of urolithiasis. The objective of this study is to evaluate the utilization of LDCT at a high‐volume endourology centre.
Methods: A retrospective study was performed for CT KUB performed at St. Joseph's Hospital (London, Canada) in the month of January in 2011, 2013, 2015, 2017, and 2019 for stone assessment. Mean radiation dosage, tube voltage, encounter type, requisition details, umbilical fat thickness (UFT) was obtained from imaging software. UFT <2.5cm was used as a surrogate for BMI <30m/kg2. Patient age, sex, and need for further imaging for diagnosis following initial CT KUB was documented from the electronic record.
Results: A mean of 50 scans were performed each January (N = 250). Studies were performed with 120 kV on the GE 64 Slice Discovery HD 750. Mean radiation dosage was 5.7 mSv (2.9‐20.4 mSv). Overall LDCT utilization was 50.8% and was 35.7%, 54.5%, 53.2%, 49.1%. and 58.1% in 2011, 2013, 2015, 2017, and 2019, respectively. Of CT KUB ordered by urologists for stone evaluation, only 50.5% were LDCT (mean: 5.6 mSv). Factors associated with LDCT included female gender (59.3% vs 43.8%; p = 0.016) and low UFT (64.2% vs. 42.9%, p < 0.001) No patients required further imaging tests to clarify the diagnosis of urolithiasis following the initial CT scan.
Conclusions: Reducing radiation exposure is important for patients being evaluated for urolithiasis. Despite widespread knowledge regarding LDCT protocols and urologist expectations that LDCT should be employed, this only occurs about half the time at a high‐volume centre, even when the requisition is specific for evaluation of stones and BMI <30 kg/m2. Regular evaluation of LDCT utilization and collaboration between urology and medical imaging departments is critical for improvement of radiation safety outcomes.
A Comparison of Radiation Exposure Between the New Flat Panel and the Conventional Round C‐Arm
JD Belle, M Keheila, N Chen, J Lee, N Srikureja, AS Amasyali, DD Baldwin, M Hajiha
Loma Linda University, Department of Urology
Introduction & Objective: Radiation exposure is a significant concern for patients and health care providers. Manufacturers of flat panel C‐arms have claimed reduced radiation exposure, however, the dose delivered at the lowest possible settings for each C‐arm type has not been compared. The purpose of this study was to compare the cumulative radiation dose between the OEC Elite CMOS Flat Detector (FD) and the conventional OEC 9800 Image Intensifier C‐Arm (Round) in a cadaver model.
Methods: Optically stimulated luminescence (OSL) chips were implanted into a cadaver as seen in Figure 1. Five trials were performed at six different C‐arm settings: round 1PPS (lowest possible setting) at standard and low dose, round 4PPS at standard and low dose, and FD 4PPS (lowest possible setting) at standard and low dose. All trials used five minutes of fluoroscopy with automatic brightness control. Radiation dose and settings were compared using t‐tests, with p < 0.05 considered significant.
Results: When comparing the FD and Round C‐arms at their lowest possible pulse settings, the FD produced 3‐5 times more radiation exposure at all locations using standard dose settings (Table 1). This difference was maintained in all locations at low dose settings (p < 0.05 for all, data not shown). When comparing FD and Round C‐arms at 4PPS, radiation exposure from the FD was about 2x higher when using standard exposure settings (Table 1). At low dose settings and 4PPS, the FD and Round C‐arms produced equivalent radiation exposure at all locations (P > 0.05 for all).
Conclusions: While modern flat panel detector C‐arm manufacturers advertise lower radiation exposure, when FD machines are utilized at the lowest pulse settings they produce approximately 4x greater radiation exposure than the Round panel at the lowest pulse settings. At both standard and low dose settings, the round C‐arm produced significantly less radiation exposure. When it is imperative to have the lowest possible radiation exposure, for example when operating on pregnant patients or in children, older round C‐arms should be utilized.
Clear cell Likelihood Scores (ccLS) on Multiparametric MRI Decreases Benign Pathology Rates in Patients with Chronic Kidney Disease (CKD) Being Considered for Extirpative Nephron Sparing Surgery (NSS)
TN Morgan, JC Dai, V Kommidi, S Kusin, H Kominsky, I Pedrosa, JA Cadeddu
UT Southwestern
Introduction & Objective: NSS is favored for patients with solid renal masses (SRM) and concurrent CKD. Complication rates are higher than average and operating for benign disease is less permissible. We describe complications and benign pathology rates in a cohort of CKD patients undergoing roboticassisted partial nephrectomy (RAPN) with utilization of MRI and clear cell likelihood scoring (ccLS).
Methods: A retrospective chart review was performed on 70 patients with CKD (eGFR 15‐60) and a pre‐operative MRI who underwent RAPN between 4/2016 and 2/2020. CcLS scores from 1 to 5 (1‐very unlikely, 2‐unlikely, 3‐equivocal, 4‐likely, and 5‐very likely) were assigned prospectively pre‐operatively in 54 (77.1%), and post‐operatively in the remainder by a blinded radiologist. Clinical characteristics were analyzed using SPSS. Wilcoxon signed rank test compared change in post‐operative GFR from baseline (IBM, Armonk, NY).
Results: Patient demographics and pre‐operative tumor characteristics are in Table 1. The median OR time, blood loss, warm ischemia time and length of stay were 180.5 minutes (IQR 156.0‐204.0), 200.0 cc (IQR 100.0‐300.0), 23.0 minutes (IQR 18.0‐26.0), and 2.0 days (IQR 1.0‐3.0), respectively. ccLS scores were 1‐5 in 13 (18.6%), 5 (7.1%), 17 (24.3%), 14 (20.0%), and 21 (30.0%), respectively. All patients had a negative margin, and only 4 patients (5.7%) had benign final pathology, outlined in Table 2. One or more complications occurred in 8 patients (11.4%). The median post‐operative eGFR (45.0, IQR 33.0‐56.0) obtained at a median of 24.9 months (IQR 5.5‐51.3) was not significantly lower than baseline (49.0, IQR 36.0‐53.0, p = 0.67).
Conclusions: RAPN in CKD patients requires careful consideration given increased risk of complications and progression to ESRD. MRI with ccLS scoring may decrease the rate of benign or indolent pathology and even obviate the need for renal biopsy or radical nephrectomy in select cases. Further prospective studies are required.
Variation in Imaging after Stone Treatment
J DiBianco, B Conrado, S Daignault‐Newton, S Jafri, H Korman, KR Ghani, CA Dauw, f Urological Surgery Improvement Collaborative
Department of Urology, University of Michigan
Introduction & Objective: Imaging after stone treatment is an important recommended step to assess stone clearance and identify potential complications. We assessed prevailing practice patterns of post‐SWL and post‐URS imaging to identify areas for quality improvement.
Methods: Reducing Operative Complications from Kidney Stones (ROCKS) is a quality improvement initiative from the Michigan Urological Surgery Improvement Collaborative (MUSIC). Trained abstractors prospectively record standardized data elements from the health record in a web‐based registry. Using the ROCKS registry, we identified patients undergoing SWL and URS between June 2016 and December 2019. The frequency and modality of postoperative imaging within 60 days was assessed. Variation in imaging was evaluated at the practice level by those with ≥10 SWL and URS cases per year, as well as the urologist level with ≥5 SWL and URS cases per year. Demographic, clinical and operative data were compared using bivariate and multivariable analyses to understand factors associated with post‐SWL and post‐URS imaging.
Results: 14,894 cases were identified (5273 SWL and 9621 URS) from 33 practices and 205 urologists. Overall, postoperative imaging was obtained in 49.1% of patients. Significant differences were seen with respect to imaging following SWL and URS (72.4% vs 36.3%, p < 0.01). The most common imaging modality for patients following SWL was KUB (63.9%), KUB plus US (17.2%), and US (11.1%) while after URS it was US (35.5%), KUB (34.7%), CT (13.7%), and KUB plus US (9.6%). Substantial practice and provider‐level variation was seen in postoperative imaging following SWL (range 36‐95.2%) and URS (range 0 – 93.1%) (Figure). The odds of imaging post‐URS compared to post‐SWL were significantly different by practice (p < 0.001) after factor adjustment (odds by practice: range 0.02 – 1.96). Additional factors associated with 60‐day postoperative imaging included higher Charlson comorbidity index (CCI), larger stone size and renal stone location.
Conclusions: The postoperative imaging rate for SWL is almost double the rate for URS in the state of Michigan. Wide variation exists amongst practices and providers with respect to imaging, with no apparent correlation amongst those practices imaging at a high rate for either SWL or URS. Future efforts are needed to better align postoperative imaging practices with best practice guidelines.
Observation of radiopaque renal lesions
A Keln, S Schmidt, DG Alifov
Tyumen State Medical University
Introduction & Objective: Every year, 403.3 thousand new cases of kidney cancer and 175.1 thousand deaths from this pathology are registered in the world. More than half of the patients are over 65 years old at the time of diagnosis. Most primary kidney tumors are diagnosed incidentally as asymptomatic small <4 cm tumors. These tumors have a high degree of differentiation and rarely require surgical treatment, and if the operation is performed, the data of the pathomorphological result are benign. Due to the slow progressive growth and asymptomatic course, the method of dynamic observation of kidney tumors avoids unnecessary risks of surgical treatment. Trace the growth rate of renal tumors that accumulate contrast agent.
Methods: In the period from 2009 to 2019, all cases of radiographically confirmed renal masses were collected. Researched 50 people aged from 58 to 90 years. The study group included patients with renal neoplasms ≤7 cm in size. CT scan was performed on a regular basis, every 3 to 6 months, to assess the dynamics of growth. The diameter of the tumor in the largest dimension was taken as the size of the tumor. The tumor growth rate was calculated as the average change in diameter for 1 year during the entire observation period.
Results: The average age of the patients was 74.8 ± 7.4 years. The average tumor size at the time of detection was 35.0 ± 6.9 mm. The average linear tumor growth rate was 6.6 ± 2.4 mm / year. Tumor size at the time of diagnosis did not correlate with growth rates (p > 0.05). No dependence was revealed of the rate of increase in the size of formations depending on their structure ‐ solid (median 6 mm / year; average ‐ 10 mm / year) or cystic solid (median 7 mm / year; average 9 mm / year; p > 0.05 ). The absence of the dynamics of tumor growth during the entire observation period was revealed in 22 people.
Conclusions: Most malignant kidney tumors have a slow growth rate. This conclusion allows us to take a differential approach in the choice of surgical treatment, which is optimal for elderly patients with low somatic status.
Percutaneous Image Guided Cryoablation and Radio‐frequency Ablation versus Partial Nephrectomy for small renal cell carcinomas: a ten‐years, single centre observational study
V Vinson, F Osman, J Cartledge, M Kimuli, N Vasudev, C Ralph, S Jagdev, S Bhattarai, J Smith, J Lenton, T Wah
School of Medicine, Faculty of Medicine and Health, University of Leeds, Leeds Department of Targeted Intervention, Division of Surgery and Interventional Science, University College London, London
Introduction & Objective: There is a lack of long‐term evidence supporting the non‐inferiority of cryoablation (CRYO) and radio‐frequency ablation (RFA) when compared to partial nephrectomy (PN) for the management of small renal cell carcinomas (RCCs). This is the first‐ever study to report 10‐years long‐term evidence comparing CRYO or RFA and PN for the management of small RCCs.
Methods: Following institutional health and research authority approval, all patients in the prospective registry (2004‐2015) with a solitary, biopsy‐ or histology‐proven T1N0M0 sporadic RCCs had RFA, CRYO or PN were included in this retrospective analysis. The primary outcome is 10‐years cancer‐specific survival (CSS). Secondary outcomes include overall survival (OS), local recurrence‐free survival (LRFS), metastasis‐free survival (MFS), complication rates and change in renal function pre‐operatively and post‐operatively. Survival outcomes are evaluated using the Kaplan‐Meier method and Cox Proportional‐Hazards Model, while complication rates and change in renal function are evaluated using logistic regression and linear regression, respectively.
Results: A total of 296 patients (187 males, 109 females) with a median [IQR] age of 68 [16] years. Median tumour sizes for CRYO (3.3 [1.6]), RFA (3 [1.1]) and PN (2.7 [1.3]) are similar. Amongst them, 239 (81%) had T1a disease, and 57 (19%) had T1b disease. The median follow‐up periods are 75.5 [26], 99.4 [74] and 71.7 [32] months for CRYO, RFA and PN group, respectively. A total of 104 (35%), 99 (34%) and 93 (31%) of patients had CRYO, RFA and PN, respectively. CRYO and RFA are similar to PN in all oncological outcomes (Table). Both the rates and severity of complications did not differ between the three groups. Using linear regression model, the predicted eGFR reduction of T1a patients are smaller in CRYO (8.0%) and RFA (12.4%) patients when compared to PN patients (p < 0.01). Similarly, in T1b patients, predicted eGFR reduction is 16.5% and 22.2% smaller in those undergoing CRYO and RFA, respectively compared to PN patients.
Conclusions: Our long‐term experience found CRYO and RFA to be similar to PN for oncological outcomes and potentially superior for peri‐operative outcomes in T1a RCC patients; and should be considered as a first‐line treatment. More data is needed to evaluate the efficacy of ablative therapies for T1b tumours.
Withdrawn
A Novel CO2‐Digital Subtraction Nephrostogram Imaging Technique For “Contrast‐free” Percutaneous and Retrograde Endoscopic Renal Surgery in the Severely Contrast Allergic Patient
AJ Hannemann, MD Sawyer, E Ballon‐Landa, SD Herrell, J Eun
VA ECHCS/University of Colorado School of Medicine
Introduction & Objective: Use of iodinated contrast in endoscopic urology cases even with recognized allergy is generally considered low risk. However, there is potential for extra‐luminal exposure from pyelo‐venous back flow or contrast extravasation.
A severely debilitated paraplegic patient with numerous allergies was referred for recurrent severe UTIs. CT scan demonstrated >2 cm stone burden with Hounsfield units consistent with struvite. She elected definitive treatment with percutaneous nephrolithotomy. This patient reported a prior severe anaphylactoid reaction with IV contrast despite steroid premedication.
Carbon dioxide (CO2) angiography has an established role in endovascular surgery in setting of nephropathy or iodinated contrast allergy. We describe a novel adaptation for endoluminal imaging to avoid contrast in a two‐stage treatment.
Methods: “Contrast‐free” Micro‐PCNL was successfully performed in a hybrid OR. Percutaneous renal access was obtained by Urology with ultrasound guidance using retrograde methylene blue instillation. A 12/14 French ureteral access sheath was advanced percutaneously. The surgery was performed using a Lithovue disposable ureteroscope with holmium laser and extensive stone basketing. Indications for micro‐PCNL were anemia and facilitation of healing given thin parenchyma.
CO2‐nephrostogram was performed using arterial pressure tubing connected to the sheath. Digital subtraction imaging was obtained with biplanar fluoroscopy as gas was injected. This outlined the renal pelvis, calyces and proximal ureter and confirmed interpolar positioning of the access sheath. In a second stage procedure, retrograde CO2‐pyelogram was obtained in a standard OR.
Results: No iodinated contrast was used in either procedure. The patient tolerated each well without complications. Digital subtraction imaging technique was successful with biplanar and traditional fluoroscopy. Adequate imaging of the renal pelvis and calyces was achieved without the use of traditional contrast media.
Conclusions: CO2 is a non‐nephrotoxic and non‐allergenic alternative to contrast for endovascular angiograms, when iodinated contrast is contraindicated. We report a novel, safe, and easily reproducible adaptation to obtain upper tract imaging. This facilitated performance of two complex endoscopic urologic surgeries without using iodinated contrast in a highly allergic patient.
Novel 3D Anatomical Modeling Facilitates Laparoscopic or Robotic Donor Nephrectomy in Patients with Complex Renal Anatomy that were Precluded from Donation based on Computed Tomography Angiography or Magnetic Resonance Imaging
J Kuo, N Velazquez, M Degen, R Munver
Hackensack Meridian School of Medicine
Introduction & Objective: In the setting of complex renal anatomy, patients may not be considered suitable candidates for donor nephrectomy due to concerns of surgical complexity for the donor and recipient surgeons. We describe the use of IRIS™ (Intuitive Surgical, Inc) segmented three‐dimensional (3D) anatomical modeling for preoperative planning and intraoperative navigation to facilitate laparoscopic or robotic donor nephrectomy. This technology delivers a 3D model of kidney anatomy that is created from CT scan imaging with maximum 3 mm slice width. The images are delivered to an iOS device and can be displayed via a hardwire connection from the iOS device to the robotic surgical console.
Methods: Since June 2020, a total of 28 potential living renal donors underwent preoperative computed tomography angiography (CTA) as part of the routine evaluation. In addition, segmented 3D modeling was performed for all patients based on the CTA images, highlighting the renal anatomy, arterial and venous vasculature, collecting system, and ureteral course. The CTA and 3D models were reviewed by the living donor and recipient teams for those patients with complex renal anatomy to further assess the candidacy of the renal donors.
Results: Three of the 28 patients (10.7%) were not considered to be suitable candidates for renal donation based on CTA or magnetic resonance imaging findings of renal abnormalities, including 3 renal arteries bilaterally (n = 1), 3 right renal arteries and 2 left renal arteries with a circumaortic left renal vein (n = 1), and a right 3 cm perirenal mass of unclear origin in the area of the renal hilum (n = 1). Following review of the 3D anatomical reconstructed images, all patients were cleared to undergo donor nephrectomy based on the additional information that was provided from these images. In the patient with the perihilar mass, the 3D imaging delineated the mass as arising from the renal parenchyma. This patient underwent robot‐assisted donor nephrectomy with ex‐vivo excision of the mass (pathology: lipid‐poor renal angiomyolipoma), with successful subsequent renal transplantation. The other 2 patients underwent uneventful left laparoscopic donor nephrectomy. There were no complications in the renal donors or recipients.
Conclusions: 3D anatomical modeling with IRIS™ allows surgeons to perform donor nephrectomy in patients that may otherwise be excluded from renal donation. This technology offers preoperative interpretation of renal anatomy, provides confidence in the setting of complex vasculature, and facilitates planned procedural completion.
Video Session
Video Session 01: Percutaneous Surgery
V01: percutaneous surgery
RK Jain, J Bjazevic
Percutaneous combined electrosurgical and Thulium Fiber Laser management of large renal pelvis urothelial tumor in a solitary kidney
A Martov, D Ergakov, N Baykov, A Andronov, SV Dutov
Introduction & Objective: The endourological management of upper tract urothelial carcinoma is indicated in cases of solitary renal unit. Ureteroscopic approach is used routinely. The cases then it couldn't be established always present clinical challenge. We describe the clinical case of combined percutaneous management of large renal pelvis urothelial tumor in a solitary kidney
Methods: 68 y.o. male with complains of hematuria and right dull low back pain was admitted to the urologic clinic with the CT findings of 2,7 cm renal pelvis tumor. He underwent left nephrectomy due to renal cancer (RCC or UTUC ???) in 1998. In 2002 right lower ureter urothelial tumor has been detected, ureter resection and ureterocystoneostomy has been done, cava‐filter has been made to prevent thromboembolic complications. In 2009 left ureteral cuff resection with partial cystectomy was done and in 2009‐2018 four TURBT +2 BCG has been performed. 2,7 x 2,1 mm renal pelvis urothelial tumor has been detected on CT‐urography. Ureteroscopic approach was failed due to rigid fixed deviation at the level of anastomosis. There're no bladder recurrence. The X‐ray guided percutaneous approach through the lower pole calyx has been done. After tract dilation up to 24F nephroscopy has been done. The large papillary pelvis tumor has been visualized. With the 22F monopolar resectoscope the exofitic tumor part was resected till the base. In order to avoid the perforation of pelvis wall, we continued with the novel thulium fiber laser (10J, 1Hz) vaporization of the tumor base. After completion the ablation the flexible nephroscope has been introduced and the entire collection system has been visualized. No additional tumor has been found, after it the 20F Malecot Nephrostomy tube has been placed. Pathology report was low‐grade urothelial carcinoma with negative intraoperative cytology
Results: Nephrostomy was removed on 3 post‐op day and the patient has been discharged and still under active surveillance (36 mo.). Creatinine serum level remained stable – 1,26mg/dl. Control MRI‐urographies (12mo, 22mo.) showed no additional mass in the upper tract. Cystoscopy and urine cytology were also negative
Conclusions: Percutaneous endourological papillary tumor management is still available option even in the era of the flexible ureteroscopy, especially in the cases then the nephron‐sparing approach is indicated and ureteroscopic access is impossible or tumor is too bulky
Mini‐PCNL for multiple Hem‐o‐lok clips forming stone nidus in the collecting system
T Aro, A Rai, D Hoenig, AD Smith, Z Okeke
Introduction & Objective: With the advancement of technology and medicine, minimally invasive surgery became the standard in many fields. Laparoscopic and robot assisted laparoscopic surgery is the preferred surgical treatment for renal masses, and Percutaneous NephroLithotomy (PCNL) is the standard of care for large renal calculi. And more and more frequently we are encountering patients with both conditions.
Methods: We present a case of a patient undergoing mini‐PCNL for nephrolithiasis, one year following robotic assisted laparoscopic partial nephrectomy. Computed Tomography (CT), Magnetic resonance (MRI), and Flouroscopy imaging are provided, as well as live video of the mini‐PCNL.
Results: The video demonstrates a total of three hem‐o‐lok clips found inside the collecting system, constituting a nidus for stone formation.
Conclusions: Although we do not fully understand the mechanism of clip migration, it has been demonstrated in several previous case reports. We present a rare case of multiple clips migration into the collecting system. We should always be suspicious of migrated hem‐o‐lok clips as a nidus for stone formation in patients following robotic or laparoscopic surgery.
Bilateral Nephrolithiasis And Upper Tract TCC in Horseshow Kidney
T Aro, A Rai, D Hoenig, AD Smith, Z Okeke
Introduction & Objective: Nephroureterectomy is the gold‐standard treatment for High grade Upper tract urothelial carcinoma to date. Current guidelines and expert opinions offer some exceptions to this based on patient characteristics, disease status, and the contralateral kidney.
Methods: We present a rare case of a patient with horseshoe kidney, bilateral large nephrolithiasis, high‐grade upper tract urothelial carcinoma in one moiety, and relative parenchymal thinning of the contralateral side. The patient was treated in a percutaneous minimally invasive, nephron sparing approach. Computed Tomography (CT) and Fluoroscopy images are provided, as well as live video of all procedures.
Results: Videos of multiple procedures are provided to demonstrate percutaneous resection of the tumor, stone lithotripsy, and repeat biopsies. The patient also had Intra collecting system instillations of gemcitabine and docetaxel, and video of post‐installation percutaneous flexible nephroscopy is provided.
Conclusions: Minimally invasive percutaneous resection of high‐grade upper tract urothelial carcinoma is a safe procedure in select cases. Current guidelines may not apply to all patients; unique scenarios with upper tract urothelial carcinoma may require personalized decision making and treatment at specialized centers.
Gradual Percutaneous Nephrolithotomy For Complete Staghorn Stone Can Facilitate Renal Access, Prevent Complications And Improve Stone Free Rate
J Feghali
Introduction & Objective: Standard Percutaneous nephrolithotomy (PCNL) is the gold standard for the treatment of renal stones larger than 2cm. when treating full staghorn calculi; urologists encounter difficulty while creating renal tract due to limited space in the pyelocaliceal system around the stone, and difficulty to bypass the stone and insert a wire down the ureter. Objective: evaluate a new technique called gradual PCNL defined as treating large stones in single procedure by MiniPCNL followed by standard PCNL through the same tract In order to reduce complications, perform the ideal tract; and improve the Stone Free rate (SFR)
Methods: During 2019, five men with mean age of 59 years old, and complete staghorn stones were treated with Gradual PCNL technique by single surgeon . Ureteral occlusion balloon catheter 34fr/100cm was placed in lithotomy position in order to dilate the pyelocaliceal system; followed by renal punction in prone position via an 18 gauge needle under fluoroscopic and/or ultrasound guidance. A 0.035 inch hydrophilic tip wire was then inserted in the pyelocaliceal system ; followed by MiniPCNL technique in order to confirm appropriate punction , prevent traumatic dilation; open a stone window by laser or pneumatic lithotripsy and insert the wire down the ureter. Once the wire has reached the bladder, we removed the MiniPCNL operating sheath (15/18Fr) and dilated the same tract with nephrostomy balloon catheter 30 Fr , then we switched to standard PCNL (using nephroscope sheath24 Fr) and removed the stone with ultrasonic lithotripsy. At the end of procedure a 7Fr/28cm ureteral stent was placed in an antegrade fashion, and 20 Fr nephrostomy tube was left in place.
Results: Mean Gradual PCNL operation time was 130.2 minutes; mean fluoroscopy time was 4.2min; Nephrsotomy tube was removed on day 1, all patients were discharged 48 hours after procedure ; no blood transfusion was needed ; mean Hemoglobin drop after surgery was 1.38g/dl; no major postoperative complications; SFR was 80% 1 month after surgery
Conclusions: Gradual PCNL for complete Staghorn Stone is a single procedure that can facilitate renal access, prevent complications and Improve Stone Free Rate
Supine Percutaneous Nephrolithotomy (PCNL) in Horseshoe Kidney
MO Breish, S Sriprasad, D Whiting, F Anjum, O Abdalla
Introduction & Objective: Horse‐shoe kidney (HSK) is the most common renal fusion anomaly, with reported incidence of 1:400 mainly in males (M: F = 2:1). Nephrolithiasis is frequently occurred in HSK patients with an estimated range of 21%‐ 60% due to ureteropelvic junction obstruction, urinary stasis, recurrent infections, and metabolic abnormalities. Percutaneous nephrolithotomy (PCNL) is a procedure of choice for a high stone burden in a HSK with overall stone free rate of 72 % to 93.1%, and usually performed while patient in a prone position. In this video we present a case of a supine PCNL performed in our institution to treat stones in HSK.
Methods: 59 years old gentleman known to have HSK presented with left sided abdominal pain and a past medical history of renal stones. Previously, he was treated for renal calculi using shock wave lithotripsy and ureteroscopy. Blood investigations showed normal kidney function, however non contrast CT KUB demonstrated multiple calculi within the left moiety of HSK. He was counselled to undergo supine PCNL to treat the stone burden. Intraoperatively, the patient was prepared and positioned in the lithotomy position in order to perform retrograde studies. An Occlusion balloon catheter was placed within the ureter. An upper calyx puncture was performed to access the left moiety of HSK. Both hydrophilic and extra stiff guidewires were passed into the lower calyx. the puncture needle was removed leaving the guidewires in place. Balloon dilatation was performed followed by placement 30F Amplatz sheath. Flexible nephroscopy was performed in order to identify and basket the stones out of the kidney. 16 F Malecot nephrostomy was placed and secured.
Results: 1‐2 days post operatively, the patient developed fever and was treated with Intravenous antibiotics. Post‐ operative CT KUB showed a patent nephrostomy in situ and confirmed stone free kidney. The nephrostomy was removed on day 7 and the patient was discharged 8 days post‐ operatively . The patient made a good recovery without major complications and was deemed stone‐free following supine PCNL.
Conclusions: Supine PCNL is therefore feasible and safe option to treat stones in patients with HSK.
Percutaneous nephrolithotomy in challenging cases of renal stones
J Park, H Park, H Shin
Introduction & Objective: To report our surgical techniques of percutaneous nephrolithotomy (PNL) which were performed in challenging cases including calyceal diverticular, renal parenchymal stones, and renal pelvic impacted stone with multiple infundibular narrowing.
Methods: 42‐year‐old man (patient 1) and 48‐year‐old woman (patient 2) were referred for persistent right flank pain. The two patients had been treated with shock wave lithotripsy under diagnosis of renal calyceal stones at other hospitals, but not fragmented. The other patient, 49‐year‐old man (patient 3), visited outpatient clinic due to left flank pain that developed one year ago. After 3‐phase CT scans, the patients were diagnosed with 2.9 cm‐sized calyceal diverticular stone (patient 1), 2.2 cm‐sized renal parenchymal stone (patient 2), and 2.8 cm‐sized renal pelvic impacted stone with multiple infundibular narrowing (patient 3). The three patients were treated with PNL. Direct puncture into diverticulum and dilation of diverticular neck (patient 1), laser incision of parenchyma overlying stone (patient 2), and infundibulotomy (patient 3) was performed
Results: Patient 1 and 2 were completely stone‐free after PNL, while two third of stone burden of patient 3 was removed. The nephrostomy tube was removed at 4 to 5 days after surgery, and the patients recovered without specific complication. At postoperative 1 month follow‐up, patient 1 and 2 were symptom‐free, and patient 3's symptom much improved. On excretory urography, diverticulum size decreased while wide diverticular neck was identified (patient 1), and previous stone cavity was visualized with pelvocalyceal system (patient 2). In patient 3, residual stones were identified in upper pelvocalyceal system at follow‐up CT.
Conclusions: Though PNL represents a technically challenging procedure that requires specific endourologic skills, PNL has still advantage in treating patients with complex renal anatomy, such as calyceal diverticular stone, renal parenchymal stone, and infundibular narrowing.
Encrustated Metallic Ureteral Stent Treated By Mini Percutaneous Nephrolithotomy
T Machado, R Astolfi, R Carrera, G Freschi, N Gattas, A Meller
Introduction & Objective: The use of polymeric double J stents for the management of ureteral strictures is effective for a short period of time, although they have limited use due to the risk of obstruction and to the need for periodic stent changes. Metal stents have been developed with the aim of maintaining greater ureteric patency, alleviating symptoms, and, especially, allowing less frequent exchanges. Although metallic stent changes are approved for 12 months, there are no concrete data defining a safe dwell‐time to prevent clinically significant encrustations. Likewise, there are no reports of surgeries performed to treat metal stent encrustations. Our objective with this video is to describe a case of a large metallic ureteral stent encrustation successfully treated by Mini Percutaneous Nephrolithotomy (MiniPerc) in an obese patient.
Methods: A 48‐year‐old female was admitted at our hospital for treatment. The patient had previously undergone a metallic DJ stent implantation for the treatment of a chronic ureteral stricture but hasn't had a stent exchange in the last 18 months due to loss of follow‐up. Radiological exams revealed a large encrustation at the right renal pelvis (2,5x1,6cm). After the attempt of removing the stent by cystoscopy failed, a mini percutaneous nephrolithotomy was performed to treat the kidney stone and to implant another stent.
Results: After the procedure, the patient became stone‐free and had a silicone DJ stent implanted. Metabolic evaluation of the urine did not reveal hypercalciuria or any other contributing factor for this severe complication.
Conclusions: Large encrustations on a metallic ureteral stent are rare complications and may require surgical treatment. Mini percutaneous nephrolithotomy seems to provide a safe and feasible treatment option for these cases, even in obese patients.
Title: Endoscopic Combined IntraRenal Surgery (ECIRS) with SOLTIVE Laser and Mini‐PCNL Technique
S Niu, SM Alam, WR Molina
Introduction & Objective: Endoscopic Combined IntraRenal Surgery (ECIRS) is a combined rigid and flexible antegrade and retrograde approach for the treatment of large kidney stones and provides an opportunity to exploit the full array of endourologic equipment. As more urologists are adopting the mini‐percutaneous nephrolithotomy (mini‐PCNL) technique to decrease morbidity associated with conventional PCNL while preserving high stone free rates when compared to ureteroscopy, we aim to determine the feasibility and efficacy of ECIRS using the SOLTIVETM laser combined with mini‐PCNL for treatment of moderate sized renal stones.
Methods: After Institutional Review Board approval, we retrospectively reviewed two patients with stones between 1.5‐2.5cm who underwent treatment with ECIRS using simultaneous mini‐PCNL with SOLTIVETM laser and retrograde ureteroscopy. Access was obtained intraoperatively. We selected one of the cases to highlight our ECIRS experience using the novel combination of technology and technique.
Results: In modified supine position, the flank is elevated to create 15 degrees of rotation to expose the puncture area, demarcated by the 12th rib, iliac crest and posterior axillary line. The 15/16Fr rigid access sheath was used for access. The 365‐micrometer fiber achieved exceptional ablation rate and dusting with the setting of 1J and 36Hz. Simultaneous retrograde ureteroscopy facilitated mini‐PCNL by amplifying the vortex effect with maneuvers such as “pass the ball” technique. Neither patient had a postoperative complication, and both were considered stone free based on postoperative imaging. This is a descriptive video of our technique that has been performed on a total of 2 patients. No statistical analysis was calculated due to the rarity of this procedure.
Conclusions: ECIRS with SOLTIVETM laser and mini‐PCNL technique is a safe and effective strategy for treatment of stones with sizes that fall in between conventional PCNL or flexible ureteroscopy alone. The optimal wavelength of the SOLTIVETM laser created superior ablative properties which facilitated the performance of faster and more effective lithotripsy. Simultaneous retrograde ureteroscopy allowed for complete surveillance of the collecting system, relocation of stone fragments for ease of treatment, and amplification of the vortex effect. Further studies with larger cohorts are needed to assess the generalizability of our outcomes with this novel combination of technique and technology.
Pediatric PCNL ‐ Past Challenges and Future Directions
C Ferari, C Crigger, M Ost, O Al‐Omar, O Al‐Omar
West Virginia University
Introduction & Objective: Pediatric percutaneous nephrolithotomy (PCNL) for large stone burden is an under‐utilized approach to stone removal in younger patients. This stems from the large instrumentation traditionally used interchangeably in adult and pediatric populations. Though large instrumentation has shown efficacy in pediatric patients, recent efforts to “miniaturize” the approach, and therefore the associated morbidities, have made PCNL more amenable in the pediatric patient.1,2
Methods: Through the case of a 10‐month‐old female presenting with painless hematuria and a 10‐year‐old female with left flank pain and hematuria, both secondary to renal calculi, we present an overview of the challenges inherent to PCNL, the push for miniaturization, and examples of the preferred technique employed by fellowship trained pediatric urologists at our institution. Our 10‐month‐old female presented with painless gross hematuria and our 10‐year‐old female presented with left flank pain and gross hematuria. PCNL was chosen as the operative approach to remove their stone burden based on imaging (Figure 1, Figure 2).
Results: Complete removal of stone burden was achieved in both of our patients using mini‐PCNL tract sizes with no complications.
Conclusions: Our video highlights two cases of successful use of mini‐PCNL technique to remove stone burden in pediatric patients with no complications. A variety of smaller tract sizes for pediatric PCNL have been described over the last several decades, including mini‐PCNL (typically 14‐22 Fr), ultramini‐PCNL (typically 11‐13 Fr), and micro‐PCNL (typically 4.8‐10 Fr). A recent meta‐analysis concluded that miniaturized PCNL was at least as efficacious and safe and standard PCNL but had longer operating times.3 In demonstrating this technique that is currently actively evolving, we hope to shed some light on the exciting new trend in “miniaturized” PCNL and its applicability – with regard to efficacy and safety – in the pediatric population.
Using 3D Scanning to Create a CNC Machined Polyurethane Bed for Patient Positioning During Percutaneous Nephrolithotomy
DC Fedrigon, S Sivalingam
Cleveland Clinic‐ Glickman Urological & Kidney Institute
Introduction & Objective: Nephrolithiasis is a cause of significant morbidity in patient populations with musculoskeletal abnormalities, spinal cord injury, and multiple sclerosis often requiring surgical intervention such as percutaneous nephrolithotomy (PCNL). Safely positioning patients with limb contractures or other musculoskeletal abnormalities in the prone position for PCNL can be a challenge intraoperatively and is an area that has not been previously explored in the literature. Therefore, we present a case report on the production and implementation of a custom foam bed designed from a 3D‐scan of a percutaneous nephrolithotomy patient with upper extremity contractures.
Methods: A female patient with a history of congenital hydrocephalus, seizures, developmental disabilities, and a left upper extremity permanently contracted across her chest was identified preoperatively as a candidate for a custom bed. Informed consent was obtained from the family in accordance with our institutional review board policies. Prior to surgery, a Microsoft Kinect V2 was used to 3D scan a patient with Meshmixer and Fusion 360 (Autodesk) being used to develop the 3D custom bed model. The model was then machined out of Airtex 5'' 160 oz High‐Density Foam using a ShopBot PRSAlpha 96x48 CNC machine with an Amana HSS1614 router bit.
Results: The custom foam bed was successfully utilized in place of traditional positioning padding in the operating room during the patient's surgery. The foam bed was used to cushion the patient's upper body during the prone split leg procedure while appropriately relieving pressure on the patients arm that needed to be positioned across her chest.
Conclusions: We report a novel use for custom contoured polyurethane beds in the operating room and we demonstrated a reproduceable workflow for a 3D‐scanning and CNC milling production process. The custom bed performed as expected within the operating room, providing both easy prone positioning and adequate cushioning for the patient's contracted upper limb. This technique is reproducible with equipment accessible to most academic care centers and has applications across multiple surgical disciplines that commonly utilize prone positioning such as endourology and spinal surgery.
Thulium laser dusting of a partial staghorn stone via 14Fr Super‐mini percutaneous approach – technique and optimal laser settings
E Edison, T Reid, R Vitale, N de Luyk, V Arumuham, C Allen, S Choong
Introduction & Objective: The capability of Thulium Fibre Laser (TFL) lithotripsy to dust stones compliments the continuous suction of Super‐mini percutaneous approach (SMP) in treating kidney stones. Compared to Holmium:YAG, TFL can deliver more power, through smaller fibres, with a wider range of energy, frequency and pulse length parameters, with higher water absorption and more efficient stone ablation. Thus TFL is an excellent novel technique for SMP lithotripsy. The objectives of this video are to demonstrate use of TFL via SMP for a partial staghorn, and by varying the energy, frequency and pulse duration, to demonstrate optimal laser settings.
Methods: Video is recorded from the 14Fr SMP of a partial staghorn cystine stone, 3.5 x 2.5 cm (650 HU). SMP access was obtained with ultrasound and fluoroscopic guidance and serial dilation to 14Fr. A 14Fr 13cm ClearPetra sheath and a 7.5Fr Storz Nephroscope was used, with a 365μm TFL (Olympus Soltive). There was continuous irrigation through the scope, and independently controlled continuous suction through the sheath. Modifiable parameters of energy (0.025 to 6J) and frequency (1 to 2400Hz) are available in combinations up to maximum power of 60w. Pulse duration is short, medium or long (200μs to 50ms). Various laser settings are demonstrated and evaluated.
Results: With a total laser time of 22 minutes, delivering 71.01kJ, the kidney was clear of stone on direct vision and fluoroscopy. A ureteric stent was left, with no nephrostomy. The patient was discharged on the same day with no complications. Follow up CT at 1 month demonstrated a 3mm interpolar calcification. Relook ureterorenoscopy during stent removal demonstrated this to be parenchymal. The optimal laser setting was found to be 0.6J / 100Hz / long pulse. This allowed for rapid, efficient stone dusting with fine fragments large enough for stone analysis. Higher frequencies involved extremely fine dusting which was slower. Some settings (as seen on video) induced large amounts of bubbles that obscured the view. These findings are corroborated by the authors' experience in other patients.
Conclusions: Thulium fibre laser lithotripsy allows for safe, rapid stone dusting. Super‐mini access allows for continuous irrigation and suction to maintain views, dissipate heat, and maintain low renal pelvic pressure, enabling uninterrupted lasering. The convergence of these technologies means that larger stones and partial staghorns can be managed safely and effectively as a day case procedure.
Moderated Poster Session
Moderated Poster Session 08: Reconstruction
Robotic Repair of Ureteroenteric Strictures after Urinary Diversion
MW Salkini, A Dahman
West Virginia University
Introduction & Objective: Ureteroenteric strictures develop in up to 20 % of patients after urinary diversion. The surgical revision of the anastomosis is challenging and needs large midline incision due to the adhesions and scarring following urinary diversion. We are reporting on the outcome of robotic repair of ureteroenteric strictures after urinary diversion
Methods: Nine patient presented to our service with anastomotic stricture of the Ureteroenteric anastomosis after urinary diversion. Two patient presented with left ureteral anastomotic structure to ileal neobladder. The remaining seven presented with ureteroenteric structure at the ileal conduit. 3 patients had bilateral ureteral anastomotic stricture, 2 right sided stricture of a solitary kidney and 2 patient had isolated left ureteral anastomotic stricture.
Results: The average patients' age at presentation was 72 years (range 59‐82) with 2 females (22 %). All cases were done robotic with no conversion. The average length of the procedures was 201 min (90 min‐ 460). An average blood loss of 183 ml (50‐800). The average hospital length of stay was 4.2 days (1‐14). 2 patient developed transient ileus that resolved with no intervention. One patient had DVT (11%) after surgery, and another had AKI (11%). All the anastomosis were open after follow up of 28 months (18 – 44). None of the patient progressed to chronic renal failure or needed dialysis.
Conclusions: Robotic ureteral anastomotic repair is viable option for ureterointestinal anastomotic structure. The robotic approach minimize the invasiveness of the procedure with good outcome. Longer follow up is needed to insure the reliability of the technique.
Cutaneous Ureterostomy or Ileal Conduit urinary diversion: Can we spare the bowel following Radical Cystectomy in patients with solitary functioning kidney?
B Nayak, S Saini, P Singh, R Nayyar
All India Institute of Medical Sciences, New Delhi
Introduction & Objective: To compare the outcomes following radical cystectomy in a group of patients with a solitary functioning kidney who either underwent cutaneous ureterostomy or ileal conduit urinary diversion.
Methods: We retrospectively analyzed clinical records of patients with a solitary functioning kidney who underwent radical cystectomy at our institute between Jan 2014 and May 2019. We included patients who either received cutaneous ureterostomy or ileal conduit urinary diversion. Baseline characteristics, perioperative outcomes including complications encountered and final histopathological stage were evaluated, and compared between the two groups. For the assessment of renal function outcomes, we only included the patients with a follow up for at least 2 years.
Results: A total of 43 patients were included in the comparative analyses. Of these, 23 & 20 patients underwent cutaneous ureterostomy & ileal conduit diversion, respectively. The two groups were similar concerning baseline demographic and clinical characteristics. Operating time (p < 0.001), time to drain removal (p = 0.016), postoperative length of hospital stay (p = 0.018) and bowel‐related complications (p = 0.047) were significantly higher in patients who underwent ileal conduit diversion. Although, the eGFR was comparable between the two groups at baseline, at 6 months, and at 1 year of follow up. There was a greater decline in eGFR at 2 years of follow up in patients who received cutaneous ureterostomy (p = 0.039).
Conclusions: The present study shows that cutaneous ureterostomy has better perioperative outcomes, including postoperative complications and comparable short term renal function outcomes over ileal conduit urinary diversion. However, over two year follow up there was an increased likelihood and greater degree of decline in eGFR in patients who received cutaneous ureterostomy.
Approach to management of uretero‐vaginal fistula: Review of 15 cases over 10 years
P Singh
All India Institute of Medical Sciences, New Delhi, india
Introduction & Objective: The prevention and management of gynaecological fistula always remains a big challenge. The rate was highest among women who had hysterectomy following cervical cancer. Isolated ureterovaginal fistula is rare. Patient can present lately with poorly functioning of kidney. So early diversion or corrective surgery is warranted in this condition. Most common site involved is lower ureter. The aim of this study is to describe our experience of management of iatrogenic uretero‐vaginal fistula resultant of gynecological surgery and obstructed labour over a span of 10 years and outcomes
Methods: We reviewed our database from 2009 ‐2019 and followed up this cohort of patient prospectively for outcomes.
Results:: A total of 15 patients with uretero‐vaginal fistula were identified. None of this cohort of patients had concurrent vesico‐vaginal fistula. Mean age of patient was 39 years. All patients presented with continuous urine leak with normal voiding in between. Five patients had laparoscopic hysterectomy, 7 underwent open transabdominal hysterectomy (caesarean hysterectomy for hemorrhage), 3 underwent transvaginal hysterectomy. Mean time to develop symptoms was 5 days after surgery. Mean time to discharge after primary surgery leading to iatrogenic fistula was 17 days. Time from fistula to corrective surgery was 9 months (1 month‐3 years). 14 patients had percutaneous nephrostomy placed prior to surgery as a diversion measure. Kidney function was preserved in all patients. Before definitive surgery, check cystoscopy to rule out vesicovaginal fistula and nephrostogram was done in all patients. 13 patients underwent open extraperitoneal ureteroneocytostomy. 2 out of 13 patients needed Boari reconstruction as an adjunctive to ureteroneocystostomy. 1 patient underwent robot assisted and 1 underwent laparoscopic ureteroneocystostomy (transperitoneal). All the procedures used modified Lich‐Gregoir technique for ureteric reimplantation. 1 patient was treated with just DJ stenting. Urethral catheters were removed at a mean of 10 days and DJ stents were removed at a mean of 5 weeks. Mean follow up of patient is 5 years (1‐10 years). None of the patient had recurrent symptoms and all the patients are completely dry at present.
Conclusions: Ureterovaginal fistulae are complicated by virtue of their cause and can be well managed by minimally invasive or open surgery. At times Psoas hitch or Boari reconstruction is warranted.
Withdrawn
Organ‐sparing surgery with Bracka's reconstruction for penile cancer: a single‐center experience
A Gallioli, A Rosales, JM Gaya, A Sánchez‐Puy, A Piana, P Diana, A Territo, P Gavrilov, J Caldéron, J Palou, A Breda
Department of Urology, Fundació Puigvert, Barcelona, Spain
Introduction & Objective: Penile cancer is a rare disease requiring a dedicated team to perform a patient‐tailored treatment. The crucial point to avoid local recurrence or progression of the disease is to achieve radicality. Classic surgical approach, based on the belief that a 2 cm surgical margin is needed to guarantee negative surgical margin, consists in partial or total penectomy with closure of the penile stump using a skin graft drown from the shaft. This technique carries aesthetical and psychological dysfunctions which can be reduced with less mutilating approaches without compromising the oncologic outcome. The aim of this study was to assess the outcomes of organ‐sparing surgery with Bracka's reconstruction.
Methods: In this retrospective analysis carried out from our prospective penile cancer database, we evaluated patients who underwent penile‐sparing surgery with Bracka's technique from 2002 to 2020 in our center. The technique includes the harvesting of a rectangular piece of medium‐thickness split‐skin graft of the upper outer aspect of the thigh. The graft is fixed to the distal part of penis and the meatus with 6/0 Vicryl Rapide suture to create the neo‐glans. Demographic variables, perioperative data, surgical and oncological outcomes were analyzed.
Results: 30 patients were included, with a median (IQR) age of 62 (12) years. 14 (46,6%) patients underwent total glansectomy, 10 (30%) glans demucosation, 5 (16,6%) partial penectomy, 1 (3,3%) partial penectomy with glans preservation. Mean operative time was 172 minutes. Absence of intraoperative complications. At the final pathological examination, 6 (20%) patients were diagnosed squamous cell carcinoma pT1, 13 (43,3%) pT2, 3 (10%) pT3, 7 (23,3%) PeIN and 1 (3,3%) pT0, with grade G1 in 10 (33,3%) patients, G2 in 11 (36,6%) and G3 in 6 (20%). Median follow‐up was 37 months (88). In 14 (46,6%) cases perioperative Clavien Dindo I and II complications were reported. 6 (20%) patients suffered from partial graft necrosis, treated conservatively. No local recurrence was observed. Lymphatic progression occurred in 1 (3,3%) case of pT2G2 tumor with negative sentinel lymph node after 58 months from surgery. 2 (6,6%) urethral neo‐meatus stenosis occurred treated in 1 case with surgical reconstructive meatoplasty, and in the other with periodic urethral dilations was started 7 months after surgery.
Conclusions: Organ‐sparing surgery with Bracka's reconstruction for penile cancer is a suitable and oncologically safe approach. It provides good phallic length preservation along with a neo‐glans reconstruction without compromising the urinary function.
Uretero‐enteric Anastomotic Stricture Following Robotic Radical Cystectomy: Extracorporeal versus Intracorporeal Approaches in the Indocyanine Green Era
MB Tuna, T Doganca, OB Argun, I Tufek, SM Keskin, C Obek, AR Kural
Acibadem Maslak Hospital, Department of Urology
Introduction & Objective: The aim of the study is to compare the early period(6th week after the catheter removal) iatrogenic benign uretero‐enteric anastomotic stricture formation between robotic radical cystectomy with intracorporeal urinary diversion, robotic radical cystectomy with intracorporeal urinary diversion(without utilizing ICG) and robotic radical cystectomy with intracorporeal urinary diversion(with utilizing ICG)
Methods: A total of 30 patients(59 renal units) who underwent robotic radical cystectomy with intracorporeal and extracorporeal urinary diversion between 2014‐2021 in our clinic included in our study. We retrospectively reviewed the demographic and perioperative results. The primary endpoint of our study was postoperative stricture rate 6th after the catheter removal; suspicious of uretero‐enteric stricture formation.
Results: From our study cohort; 13 of these patients(26 renal units) underwent robotic radical cystectomy with Extracorporeal intracorporeal urinary diversion, 10 of these patients(20 renal units) underwent robotic radical cystectomy with intracorporeal urinary diversion(without utilizing ICG) and 7 of these patients(13 renal units) underwent robotic radical cystectomy with intracorporeal urinary diversion(with utilizing ICG). The overall incidence of early period uretero‐enteric stricture formation(was post‐operative 6th week after the catheter removal) was 8.5%(5 renal units); 11,5% (3 renal units) after extracorporeal approach; 10%(2 renal units) after intracorporeal approach. None of the patients with intracorporeal approach with utilizing ICG had demonstrable uretero‐enteric strictures post‐operative 6th week after the catheter removal.
Conclusions: In the ICG era; robotic cystectomy with intracorporeal diversion is a promising approach in terms of benign uretero‐enteric stricture formation when compared with robotic cystectomy with extracorporeal urinary diversion and intracorporeal urinary diversion without utilizing ICG. Larger prospective studies are required to confirm our outcomes.
Ureteral bypass: a new technique for the treatment of ureteral atresia
X Gao, J Chen, W Wang, X Wei
Department of Urology, Institute of Urology (Laboratory of Reconstructive Urology), West China Hospital, Sichuan University, Chengdu, Sichuan, P.R. China.
Introduction & Objective: Ureteral bypass is a new surgical technique for the treatment of ureteral atresia, including two surgical types. Under ureteroscopy, if a thick layer of fat is found between the ureteral atresia and the outer fascia, use a holmium laser to burn the fat to create a small channel (Figure 1A, 1B). If the ureteral atresia is closely adhered to the outer fascia, the atresia scar is directly burned to establish a channel (Figure 2A, 2B). The aim of this study was to assess the safety and effectiveness of ureteral bypass in treatment of ureteral atresia.
Methods: Between January 2019 to June 2020, 16 patients with ureteral atresia and were performed with ureteral bypass were included in this study. Ureteral bypass includes three key steps. First, the holmium laser endoureterotomy to establish a small channel (Figure 1B, 2B). Then, the balloon dilatation to create a large channel (Figure 1C, 2C). Finally, the Allium stent was inserted (Figure 1D, 2D). Prospective collection of indicators such as hydronephrosis volume, serum creatinine, urea nitrogen, operative time, hospital stay time, operative complications. Compare the changes in these indicators before and after surgery.
Results: During a median follow‐up time of 12 months (range 6–16 months), the success rate of ureteral bypass surgery is 93.75% (15/16). The median operative time is 78 minutes and median hospital stay time is 7.5 days. The incidence of pain is 25% (4/16), and the incidence of fever is 6.25% (1/16). Preoperative hydronephrosis volume (18.81 + 15.32 mm3) reduced postoperatively (16.52 + 34.81 mm3). Urea nitrogen level decreased from preoperatively (5.77 + 1.28 mmol /L) to postoperatively (5.26 + 1.61 mmol /L). Blood creatinine did not change significantly before and after surgery.
Conclusions: This shows that ureteral bypass is a safe and effective surgical method for ureteral atresia.
Retroperitoneoscopic pyeloplasty for primary UPJ obstruction in Horseshoe kidney: Experience of a tertiary care center from Northern India
V Singh, RJ Sinha, G Singh
Dept of urology, King George Medical University
Introduction & Objective: Primary UPJ obstruction (UPJO) is seen in 30% Cases of Horseshoe kidney. Retroperitoneoscopic pyeloplasty is less reported for surgical management of UPJO in such cases. We report our experience of performing classical retroperitoneoscopic pyeloplasty in 6 cases of Horseshoe kidney.
Methods: All cases of horseshoe kidney with unilateral primary UPJO who were operated by retroperitoneoscopy from 2013 to 2019 were included. Ultrasound (USG) kidney, ureter and bladder (KUB) and contrast CT Scan KUB were performed in all cases and revealed findings suggestive of primary UPJO. DTPA renal scan revealed obstructed system in all cases. Classical retroperitoneoscopic dismembered pyeloplasty was performed over a 6 F/26 cm DJ stent in all cases with 3 port technique. The DJR was performed after 6 weeks. A renal USG and DTPA scan at 2 weeks following stent removal were performed in all cases.
Results: The mean age was 18 years and all were male. Left to right ratio was 4:2. Pain was the predominant symptom. Total six cases were operated and mean operative time was 150 ± 30 minutes. The mean blood loss was 75 ± 20 ml, mean tramadol requirement for pain control during hospital stay was 125 ± 25 mg. The mean hospital stay was 2 days. No immediate postoperative complication occurred. The success rate of pyeloplasty is 100% till last follow‐up. None of the patient developed any long term complication in mean follow‐up of 36 months.
Conclusions: The classical retroperitoneoscopic pyeloplasty for primary UPJ obstruction shows excellent surgical outcome with no complication in long term follow‐up.
Laparoscopic Boari Flap for the management of long segment ureteral defect: Long term follow‐up
V Singh, RJ Sinha, G Singh
Dept of urology, King George Medical University
Introduction & Objective: The incidence of ureteral stricture is showing a rising trend due to increased use of laparoscopic and upper urinary tract endoscopic procedures. Boari flap is the preferred method of repairing long segment ureteral defects of 8‐12 cm. The procedure has undergone change from classical open surgery to laparoscopic surgery and recently robotic surgery. Laparoscopic repair is cosmetically appealing, less morbid and with shorter hospital stay.
Methods: This prospective study was conducted from 2016 to 2019. The patients with a long segment ureteral defect (8‐12 cm) were included. IVU was performed in 2 cases and CT urogram in 3 patients. DTPA scan was performed in all cases. Transperitoneal laparoscopic repair with 3 ports were performed in all cases.
Results: The procedure was performed in 5 cases with male to female ratio of 3:2. All had unilateral stricture. The mean stricture length was 8.8 cm (8.2 – 9.8cm). The mean operating time was 206 minutes (190‐230 minutes). The average estimated blood loss was 100 ml (9‐120 ml) and mean hospital stay was 6 days (5 to 7 days). The mean follow‐up was 22 months (19–32 months). None of the patient had any postoperative complications. DTPA scan was performed in all cases at 3 months in all cases.
Conclusions: Laparoscopic ureteral reimplantation with Boari flap is safe, feasible and has excellent long term results. However, the procedure is technically challenging, requires extensive experience of intracorporeal suturing.
Reconstruction of obliterated ureteral strictures is associated with increased difficulty
RA Lee, Z Lee, AM Asghar, D Strauss, R Harrison, N Cheng, LC Zhao, M Stifelman, DD Eun
Lewis Katz School of Medicine ‐ Temple University Hospital
Introduction & Objective: There is currently a paucity of literature evaluating predictors of increased difficulty for ureteral reconstruction. Herein, we evaluate whether stricture patency (ie. obliterated versus narrowed) affect the difficulty of ureteral reconstruction.
Methods: The multi‐institutional Collaborative of Reconstructive Robotic Ureteral Surgery (CORRUS) database was queried for patients who underwent ureteral reconstruction from June 2012 to February 2019. Strictures were identified as obliterated versus narrowed. Patients with obliterated strictures were defined as those unable to be traversed with contrast or an endoscopic guidewire. We utilized operating time (OT), estimated blood loss (EBL), and frequency of utilization of adjunctive mobility procedures (downward nephropexy, psoas hitch) as surrogates for procedure difficulty. Surgical success was defined as the absence of flank pain and the improvement or absence of obstruction on renal scan.
Results: A total of 361 patients presented for surgical management. A total of 55 obliterated strictures and 206 narrowed strictures were identified. There was no difference in stricture length between two subsets (P = 0.162). Obliterated strictures had significantly longer OT when located in the proximal/mid ureter(239 vs 160 min, P = 0.002 and 278 vs 190 min, P = 0.05, respectively). The EBL was slightly higher with proximal/mid ureteral reconstruction (100 vs 50 cc, P = 0.005). Reconstruction of obliterated strictures at the proximal/mid ureter required significantly more adjunct mobilization procedures, 32% vs 14.7% (P = 0.029). Obliterated strictures at the proximal/mid ureter had significantly increased major complications (24% vs 7.9%, P = 0.01), but the clinical and radiographic success rates remained similar regardless of location (P = 0.3 and P = 0.94).
Conclusions: We demonstrate that reconstruction of obliterated proximal and mid ureteral strictures are associated with increased complexity and likelihood to utilize adjunct mobilization procedures. Despite the increased complexity, success rates of obliterated strictures are similar to narrowed strictures. Defining stricture patency aids in preoperative planning and managing intraoperative expectations. No differences were seen when managing distal ureteral strictures.
Ureteral Reimplantation without Anti‐reflux Technique for Iatrogenic Ureterovaginal Fistula: Open Surgery vs. Laparoscopic Repair
Q He, D Luo, K Wang
Department of Urology, Institute of Urology (Laboratory of Reconstructive Urology), West China Hospital, Sichuan University, Chengdu, Sichuan, P.R.C
Introduction & Objective: To show the safety and efficacy of the mucosa‐to‐mucosa anastomosis in ureteroneocystostomy without anti‐reflux technique, and to compare the therapeutic outcome between laparoscopic repair and open surgery using same procedure principles for iatrogenic ureterovaginal fistula.
Methods: A retrospective cohort study was conducted at a high‐volume referral hospital. 87 female patients, previously diagnosed with ureterovaginal fistula, underwent ureter reimplantation between 2008 and 2018. Those patients were contacted and underwent a follow‐up examination. The modified ureteroneocystostomy (mucosa‐to‐mucosa anastomosis without anti‐reflux technique) was conducted to restore urinary continuity. Vesicoureteric reflux was assessed by voiding cystogram, and effectiveness and safety in the laparoscopic repair group and open surgery group were compared.
Results: No vesicoureteric reflux occurred in postoperative follow‐up. Women whose ureterovaginal fistula treated by open surgery underwent a longer follow‐up time (12‐126 months) than the laparoscopic group (7‐39 months). The successful repair of the ureterovaginal fistula was achieved similarly in the open surgery group (96.67%) and laparoscopic group (95.00%). There was no immediate or delayed complication in the laparoscopic group. No significant difference was found between the laparoscopic repair group and the open surgery group in postoperative complications.
Conclusions: Our study preliminarily indicates that mucosa to mucosa anastomosis ureteroneocystostomy without anti‐reflux technique is feasible, effective and offers durable results without apparent complications, and laparoscopic ureteroneocystostomy with can be performed safely with a success rate compared to that of open surgery but with less morbidity and quick convalescence.
TOT‐TVT results revisited : an overestimated facility and an underestimated complication rate. Report on 280.000 cases in France (period 2009‐2018).
M Devonec
GH Lyon‐Sud, Urology department
Introduction & Objective: To analyze the re‐operation rate, after more than 280.000 cases of TVT and TOT operated in the period 2009 and 2018, as reported in France by surgeons from public hospitals and private clinics.
Methods: The official national records of the ATIH (Technical Agency on Hospitalization Information) and PMSI data (Medicalization Program of health Information Systems) were consulted for the period 2009‐2018.
The number of TVT and TOT reported each year were examined, as well as the number of complications reported each year for these two operations. Before 2012, the same code JDDB001 was used for TVT or TOT. After 2012, a different code was used for TVT JDDB007 and for TOT JDDB005. Six types of re‐operations were reported and analyzed :tape section vaginal route JRPA0010, tape ablation vaginal route JRGA0010, tape partial ablation laparotomy route JRGA0020, tape total ablation vaginal and laparotomy routes JRGA0030, tape total ablation vaginal and laparoscopy routes, tape partial ablation laparoscopy route JRGC0010. It was not possible to distinguish separately the complications related respectively to TVT or to TOT. The delay before re‐operation was also studied.
Results: Over the 10 years of the study a total number of 281.166 cases of TVT or TOT were performed . The number of TVT or TOT per year decreased slightly from 32.845 cases in 2009 to 28.166 in 2018. The number of re‐operations was remarkably stable, and varied from 2.300 in 2009 to 2.394 cases in 2018. The percentage of re‐operations each year was 8.4 % of the TVT or TOT operated each year. The most frequent re‐operations were tape ablation vaginal route 54% and tape section vaginal route 33% of the re‐operations performed each year. The longitudinal analysis of the delay before re‐operation showed 44% of the re‐operations were performed during the first year after tape implantation, 76% during the first 3 years and 84 % during the 4 first 4 years. After 4 years the number of re‐operations was low but still kept going.
Conclusions: TOT or TVT have the reputation of a simple operation, « an intern operation ». However, there is a discrepancy between surgeons opinion of facility and facts : an elevated rate of re‐operations, without considering medical complications (pain, hyperactive bladder …) the immersed part of the iceberg. Whose responsibility ? Surgeon competence probably not ; tape material, TVT ‐TOT technique possibly both. There is a need to reconsider the relevance of the prefered use of the former and to look for other material and technique. Autologous material, readjustability, totally removable material if needed should be the next objective.
Buccal, Boari, or Autotransplant over Bowel: Management of Proximal to Mid Ureteral Strictures
K Radadia, AK Chow, KG Sands, S Ogawa, B Patel, K Du, E Kim, RS Figenshau, G Murphy
Washington University School of Medicine
Introduction & Objective: Advances in surgical technique have changed management of proximal to mid ureteral strictures (PMUS). We evaluate our institutional experience with these strictures.
Methods: A retrospective review was performed from 3/2018‐10/2019 on management of patients with PMUS by a single surgeon. Robotic ventral onlay buccal ureteroplasty with omental wrapping (RBU), ureteral reimplant with psoas hitch and boari flap (Boari), or renal autotransplant (RA) were performed depending on stricture etiology, length, location, and health of ureteral plate. Patients had a ureteral stent for six weeks and followed for recurrence with a renal Lasix scan at three months and ultrasound at one year. Post‐operative complications, voiding symptoms (LUTS), and stricture recurrence were recorded.
Results: Fourteen patients had PMUS with a mean age of 52.1 years and stricture length of 5.0 cm (Table 1). Robotic buccal ureteroplasty was performed in seven proximal and two mid ureteral strictures. A ureteral stent was placed preoperatively to ensure a reasonable ureteral plate and a healthy distal ureter. A boari flap was performed open on four patients with concomitant operations by hernia or colorectal surgeons. Renal autotransplant was performed on one patient with a prior gun shot injury to the ureter causing a 4 cm proximal obliterated segment. No patients have recurred to date with 12.9 months mean follow up. Two patients undergoing RBU and one Boari developed urinary tract infections and one Boari patient had a small bowel obstruction that resolved with conservative management. LUTS were more common in Boari patients than RBU (Table 2).
Conclusions: Robotic ventral onlay buccal ureteroplasty with omental wrapping is an excellent technique for PMUS with a low recurrence rate in our series with 12.9 months of mean follow up. Ureteral stents prior to RBU ensured a wider plate to graft. We prefer this technique to Boari if possible due to lower rates of LUTS. Our algorithm (Figure 1) favors RBU, RA or Boari over ileal interposition if possible due to lower complication rates.
1‐year Outcome After Bilateral Uterosacral Ligament Replacement ‐ Comparison of Abdominal and Laparoscopic Surgical Techniques in Treatment of Pelvic Organ Prolapse and Urinary Incontinence
S Ludwig, F Thangarajah, C Eichler, B Morgenstern, P Mallmann
University of Cologne, Dept. of Obstetrics and Gynecology, Div. of Pelvic Floor Reconstructive Surgery
Introduction: Laxity of the anterior vaginal wall leads to the funnelling of the bladder neck and triggering inappropriate micturition reflexes and thus might lead to urinary incontinence. In the upright body position the anatomical support of the anterior vaginal wall (on which urethra and bladder base rest) is mainly ensured by the cervix / uterus, thus an intact apical suspension is mandatory. Sacrocolpopexy (SCP) is the gold‐standard for apical reconstruction. The technical performance of each SCP varies according to the surgeon's discretion, and comparison of clinical outcomes may be hampered. Therefore, a comprehensible surgical technique for bilateral apical fixation with a minimum amount of synthetic material was developed. Therefore, a comprehensible surgical technique for bilateral apical fixation with a minimum amount of synthetic material was developed.
Objective: Evaluation of the clinical 1‐year results after cervicosacropexy (either abdominal or laparoscopic) and its effect on prolapse and urinary incontinence.
Methods: Retrospective analysis in a tertiary center of women with POP‐Q stages I‐IV and urinary incontinence. All patients received a standardized bilateral uterosacral ligament (USL) replacement using polyvinylidene‐fluoride tapes (PVDF) either open abdominal (cervicosacropexy, CESA) or laparoscopic (laCESA). These PVDF tapes were identical in shape, that is 0.4cm width and 8.8cm length. Clinical outcome was assessed at 12 months.
Results: 145 patients were evaluable, 75 patients were operated with the abdominal, 70 patients with the laparoscopic approach. No major complications occurred intraoperatively and no mesh erosions were detected within 1‐year postoperatively. There was no significant difference in clinical outcome one year after surgeries. Apical support (POP‐Q stage 0) was restored in 100% of patients and urinary continence restored in 59% of patients (59% after laparotomy vs 62% after laparoscopy, respectively). After laCESA, patients stayed 3 days in mean compared to 5 days after CESA. Regarding the operating time, a CESA lasted in mean 120 minutes (89 ‐ 168 minutes), whereas a laCESA lasted in mean 89 minutes (58 ‐ 128 minutes).
Conclusions: In contrast to many other apical fixations, both USL were replaced using a clearly defined surgical technique (in term of type of material, size, shape of mesh, and positioning). This standardization ensured comparable and reproducible clinical outcomes, despite different surgical access paths.
Ureteral injuries: long term results of endoscopic ureteral realignment
H Johnson, S Parsons, P Mezes, G Collin, N Collin, J Philip
Bristol Urological Institute
Introduction & Objective: Ureteral injuries can occur in complex pelvic surgeries or trauma. Endoscopic ureteric re‐alignment (EUR); either with antegrade or rendezvous approach for ureteric injury obviates the need for open or minimally invasive complex surgery. Long term results of endoscopic management for ureteric injuries are described with technical modifications to enable increased success.
Methods: Over an eight‐year period, patients who were referred with ureteric injury were included. These patients had had pelvic surgery (open or minimally invasive), with an interval CT scan identifying ureteric injury post‐surgery. Management was a four‐tiered approach with nephrostomy decompression, antegrade pyelogram, antegrade stenting, rendezvous realignment with tandem or covered stents.
Results: 57 patients with a mean age of 65 years underwent ureteric re‐alignment with the majority of patients having mid‐/ lower ureteric injuries. Half of these patients needed rendezvous re‐alignment. 91% of the patients had successful realignment with 58% stent‐free at follow‐up (mean 2.5 years). Obstetric and Gynaecologic injuries accounted for the majority of non‐urological causes, with 33% of patients being stent‐free. Urological diseases associated injuries were often stent dependant.
Conclusions: Endoscopic ureteral realignment has a high (91%) success rate especially in patients with ‘clean’ injuries. This can be attributed to modifying rendezvous realignment technique, such as enabling multi‐planar endoscopic evaluation to minimise retroperitoneal defect, balloon dilatation of strictures, tandem stents; and use of Allium® stents in patients with a longer ureteric defect. It enables avoidance of complex re‐implantation surgery. Patients should be counselled regarding the period of stenting & possible further endoscopic surgery.
Differences in Surgical Treatment of De Novo Urge Incontinence Occurring Post‐Holmium Laser Enucleation of the Prostate
L Richards, BB Whiles, D Mazzotti, K Thurmon
University of Kansas Medical Center
Introduction & Objective: Holmium laser enucleation of the prostate (HoLEP) is an effective option for patients with lower urinary tract symptoms secondary to benign prostate hyperplasia. Although HoLEP has well‐established and durable outcomes, it carries a risk of iatrogenic urinary incontinence. Most patients with de novo urge incontinence (UI) experience transient symptoms with resolution rather quickly, but some patients have persistent incontinence. Due to its relative rarity, patient factors that increase the risk of post‐HoLEP persistent UI requiring surgical treatment have not been examined. In this study, we identify management options for persistent UI after HoLEP and examine patient risk factors for the condition. Furthermore, we examine symptom response to three surgical treatment options for de novo UI post‐HoLEP.
Methods: A retrospective study was performed to identify patients who underwent HoLEP at a single institution between 2016 and 2019. Patient demographics including age, BMI, race, smoking status, history of previous procedures, diabetes, erectile dysfunction, UTI, and pelvic floor physical therapy were evaluated. Prescriptions for alpha blockers, 5‐alpha reductase inhibitors, anticholinergic agents, and beta‐3 agonists were also identified. Bidirectional stepwise regression was performed using the history of a surgical treatment for UI as the outcome. These procedures include intravesical onabotulinumtoxinA (Botox) injection, peripheral tibial nerve stimulation (PTNS), or sacral neuromodulation (SNM). AUA symptom and quality of life scores were compared in patients with persistent UI that progressed to surgical treatment to those that did not.
Results: A total of 340 patients underwent HoLEP during the study period. We evaluated 28 possible risk factors for persistent UI requiring surgical management. Eight (2.4%) patients received one of the third line therapies, with 1 receiving PTNS, 6 receiving SNM alone, and 1 receiving both SNM and Botox. Our current model suggests that a history of UTI prior to HoLEP procedure increases the odds of developing the UI outcome by 36.98‐fold; 95% CI [2.75, 496.90]; p = 0.006.
Conclusions: Although persistent UI after HoLEP is rare, its management and associated risk factors are important to understand. Prior UTI is associated with increased risk of post‐HoLEP UI. These are preliminary results and future study will further investigate risk factors for persistent UI post HoLEP as well as compare outcomes for management options.
Application of bladder muscle flap in upper and/or middle ureteral stricture(9 cases)
Y Yuan, z Zhang, W Yuting, L Folin, Z Guoxi, X Zou
Introduction & Objective: To explore the clinical effect of bladder muscle flap in the treatment of middle and upper ureteral stricture.
Methods: 9 patients with upper and/or middle ureteral stenosis were treated with bladder muscle flap from February 2018 to December 2019, including 7 cases of ureteral calculi lithotripsy and 2 cases of ureteral injury secondary to gynecological surgery. There were 2 males and 7 females with an average age of 48 years (range, 26‐69 years). There were 5 cases on the left side and 4 cases on the right side. Laparoscopic ureteroplasty with bladder muscle flap and ureteroplasty with open bladder muscle flap were performed in 4 cases and 5 cases respectively. 7F ureteral stent was placed in the ureter. The length of bladder muscle flap ureter was 17‐25 cm, with an average of 20.4
Results: Operations were successful in all of the 9 cases, no conversion to open surgery in laparoscopic surgery. The operation time was 90‐180 min (mean 125 min). Intraoperative blood loss was estimated to be 50‐200 ml, with an average of 100 ml. The drainage tube was removed 2‐5 days after operation, with an average of 4 days. The average postoperative hospital stay was 9 days. The catheter was removed 2 weeks after operation, and the serum creatinine and urea nitrogen were normal. The ureteral stent was removed 2 months after operation. At 3months after operation, IVU or CTU showed that the ureter was unobstructed, no stenosis was found, and hydronephrosis was remissive. All the cases were followed up for 6 to 18 months, no ureteral stricture and hydronephrosis aggravation were found.
Conclusions: Ureteroplasty with bladder muscle flap in the treatment of middle and/or upper ureteral stricture is safe and effective, which is worthy of clinical application.
Artificial Urinary Sphincter Is Better than Slings for Moderate Male Stress Urinary Incontinence with Acceptable Complication Events: A Systematic Review and Meta‐analysis
L Lin, L Zhou, H Li, K Wang
Introduction & Objective: This meta‐analysis aimed to compare the efficacy of artificial urinary sphincter (AUS) and slings for the treatment of moderate male stress urinary incontinence (SUI) based on existing data.
Methods: The study was in accordance with the Preferred Reporting Items for Systematic Reviews and Meta‐Analysis. We searched the widely acknowledged database including PubMed, Embase (Ovid version), Medline (Ovid version) and Cochrane Central Register of Controlled Trials (till August 2020). Male patients with moderate SUI who underwent AUS or slings procedure over 18 years old and had been monitored with mean follow‐up time of at least 12 months were included. The primary outcome were success events defined as daily pad use with 0‐1 pad/d post‐operatively. Articles with similar outcome were considered suitable for inclusion. Secondary outcome included complication events of infection, erosion, acute urinary retention and surgical revision.
Results: Five studies with a total of 509 patients (295 for slings and 214 for AUS) were recruited. Success events were higher in AUS with odds ratio (OR) = 0.57 (95% confidence intervals (CIs): 0.36‐0.90). As for complication events, no significant difference was discovered between slings and AUS groups (OR = 1.04, 95% CIs: 0.61‐1.77, P = 0.88).
Conclusions: To conclude, AUS was better than slings for moderate male SUI treatment according to daily pad use with acceptable complication events. Slings also had clinical value and were options when patients refused inserted mechanical devices. More higher‐quality evidences are needed to confirm the efficacy of AUS and slings in moderate male SUI.
Robotic buccal ureteroplasty: early single institutional outcomes
MS Tonzi, B Waldorf, J Lange
University of Tennessee College of Medicine at Chattanooga
Introduction & Objective: Ureteral stricture disease, especially in the proximal and mid ureter, is a challenging surgical problem. Traditional approaches, such as ileal ureter interposition or renal auto‐transplantation, have significant associated morbidity. Robotic buccal mucosal graft (BMG) ureteroplasty is an alternative technique for managing complex ureteral stricture disease. We present early outcomes for six patients who underwent robotic BMG ureteroplasty at our regional tertiary care center.
Methods: Six patients underwent robotic BMG ureteroplasty for benign ureteral stricture disease between January 2019 and February 2021 at our institution. The decision to proceed with robotic BMG ureteroplasty was made by the primary surgeon at the time of the operation based on preoperative imaging analysis, patient characteristics, and intraoperative findings. Patient demographics, perioperative data, and short‐term results were analyzed retrospectively. The primary outcome was successful repair of the ureteral stricture, defined as resolution of flank pain on the affected side, without need for secondary intervention.
Results: All strictures were secondary to iatrogenic injury or recurrent nephrolithiasis, except for one resulting from a failed robotic pyeloplasty. All six patients underwent technically successful robotic BMG ureteroplasty by a single surgeon. There were no significant intraoperative complications. Mean OR time was 280 min (Range 146‐375 min), mean EBL was 25 ml (range 0‐50 ml), and each patient was discharged home on post‐operative day 1. Mean stricture length was 3.3 cm (range 2.5‐4cm). 5 of 6 strictures were located in the proximal ureter, while 1 stricture was located in the distal ureter. Follow up data was available in 4 of 6 patients. Average follow up time was 10 months. Each patient demonstrated clinical success defined as resolution of flank pain in the affected kidney. To date, no patient has developed stricture recurrence, and no patient has required secondary intervention. There were no complications involving buccal harvest sites.
Conclusions: Early results indicate that robotic BMG ureteroplasty is a safe and effective option for the management of complex ureteral stricture disease. However, longer term data on patient outcomes is necessary for a full assessment of this technique. With adequate surgeon experience, robotic BMG ureteroplasty can be performed safely and effectively.
Robotic assisted Vesico‐vaginal fistula repair: Our technique and outcomes
R Batra, A Singh, A Ganpule, R Sabnis, M Desai
Muljibhai Patel Urological Hospital, Nadiad
Introduction & Objective: Vesico‐vaginal fistula (VVF) is an abnormal communication between the bladder and the vagina. Correct diagnosis and prudent timing of repair are essential for successful management of these cases. The clinical scenario is different in all the patients. Most common causes of vesico‐vaginal fistula are abdominal hysterectomy, cesarean sections, malignancy and radiation related VVF, obstructed labour. Robotic assisted VVF repair has shown to be safe and feasible in many studies. Here, we show our technique of robotic assisted VVF repair and our outcomes of last 10 years.
Methods: Retrospective analysis was done for all the cases of Robotic assisted VVF repair done at our institute Muljibhai Patel Urological Hospital, Nadiad, India. Variables analysed were age, cause, location of VVF, size of defect, operative time, catheterisation and post‐operative complications and long term outcomes.
Results: 24 robotic assisted VVF repairs were done in last 10 years. The mean age of patients was 41.37 ± 7.1 years. Mean duration from insult to operation was 7.19 months. The mean size of the defect was 1.5 ± 1.1 cm. Mean duration of catheterisation was 17 ± 3.3 days, and mean duration of drain was 3.7 ± 1.2 days. There were 4 complications. 3 patients required prolonged catheterisation while 1 patient required repeat repair. Location of fistula was supratrigonal in 19 cases. Most common cause of VVF was abdominal hysterectomy (12 cases) followed by laparoscopic hysterectomy (4 cases) follows by caesarean section (2 cases) and malignancy and radiation related fistula ( 2 cases).
Conclusions: Robotic assisted VVF repair is safe, feasible and has excellent success rates. Technical modification with horizontal cystotomy had good results in all the patients.
Clinical outcomes of endoureterotomy on ureteral strictures which lasts after resolution of extrinsic benign causative disease
J Kim, S Bang, K Ko, J Chung, W Song, M Kang, H Sung, M Baek, S Jeon, K Lee, D Han
Department of Urology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, South Korea.
Introduction & Objective: Endoureterotomy is generally accepted as the first choice for treatment of ureter stricture. But the success rate can vary depending on the patient selection. Both endometriosis(EM) and retroperitoneal fibrosis(RPF) are typical benign disease that cause extrinsic ureteral strictures. And in both of them, there are effective medical therapeutic agents that can reduce the size of extrinsic causative disease. In many cases, ureter stricture persist even after medical treatment has eliminated extrinsic lesion on imaging. But, there are few data of endoureterotomy in this situation. We assessed the outcome of endoureterotomy on ureteral strictures which lasts after resolution of extrinsic benign causative disease.
Methods: Frome 2011 to 2020, we retrospectively reviewed medical records of patients who treated with medication for EM or RPF, and who underwent endoureterotomy for persistent ureteral stricture after complete resolution of periureteral lesion on imaging. Patient who had underwent open or laparoscopic surgery for ureter were excluded. Surgical outcomes were assessed at 3months, 6months after treatment. Success was defined as improvement of radiologic findings and improved excretion on diuretic renal scan.
Results: Total 19 ureter units (17 patients) were evaluated including 8 cases of EM and 11 cases of RPF. All of them were followed at 3 months and 17 ureter units (16 patients) were followed at 6 months. The overall success rate at 3 and 6 months were 94.7%(18 of 19 cases), 94.4%(16 of 17 cases). In EM group, the success rate at 3 and 6 months were 100% (8 of 8 cases). In RFP group, the success rate at 3 and 6 months were 90.9%(10 of 11 cases) and 88.9%(8 of 9 cases). The failed case underwent no further treatment because of severely decreased renal function.
Conclusions: In this study, the success rate of endoureterotomy after successful medical treatment for the causative extrinsic ureteral disease was dramatically high. In case of ureteral stricture combined with extrinsic diseases such as EM and RPF, sufficient medical treatment should be preceded by surgical intervention. In addition, endoureterotomy should be considered as the first treatment option rather than conservative management or reconstructive surgery in persistent ureter strictures with resolved EM or RPF.
Treatment of mild to moderate stress urinary incontinence using the stromal‐vascular fraction of autologous adipose tissue
AO Papoyan, C Maксимовa, R Safiullin, V Pavlov, R Kazikhinurov
Bashkir State Medical University
Introduction & Objective: Stress urinary incontinence (SUI) after radical prostatectomy is a major problem that affects 9‐16% of patients. Post‐prostatectomy incontinence results from surgical damage to the urethral sphincter as well as to surrounding nerves and supportive tissue. Treatment of urinary incontinence can be conservative including drug therapy, behavioral therapy, physiotherapy, pelvic floor exercises, surgical including sling operations, or periurethral injection therapy with bulking agents. Whereas more invasive approaches like sling operations are more effective but have higher morbidity, while the injection of allogeneic bulking agents is minimally invasive but has poor long‐term efficacy. Various studies have shown the effectiveness of the autologous stromal‐vascular fraction (SVF) as a bulking agent and for the regeneration of local tissues.
Methods: Here we report our experience of SVF transplantation into the periurethral region as a method of stress urinary incontinence treatment. Patients with symptoms of stress urinary incontinence (grade 1‐2) after radical prostatectomy of prostate were treated by injections of SVF into the bladder sphincter. The first stage is lipoaspiration. After this, the stromal‐vascular fraction is separated using special double syringes and centrifugation. After excretion of SVF, transurethral introduction to the zone of the external sphincter of the bladder is performed. Part of the SVF is sent to the BSMU Cell Culture Laboratory for study of the cellular composition using flow cytofluorimetry. Analysis of the SVF obtained from autologous adipose tissue by flow cytometry revealed the expression of markers of mesenchymal stem cells CD44, CD73, CD90. Successful differentiation of the obtained cells into bone, muscle, cartilage tissue demonstrates the presence of multipotent mesenchymal stem cells.
Results: Our study showed that injection of the SVF into the bladder sphincter area is a safe treatment option for SUI. The effectiveness of the method was 58% according to the results of the Pad test, ISIQ‐SF and QoL, complex urodynamic research, uroflowmetry. In the group with a positive effect, the Pad test value decreased on average from 2‐3 to 0‐1, the score on the ISIQ‐SF questionnaire from 7‐11 to 1‐3 and the QoL test from 4‐6 to 1‐2. There were no side effects.
Conclusions: Laboratory diagnostic methods prove the presence of multipotent mesenchymal stem cells and their ability to differentiate. The use of stromal‐vascular fraction in the treatment of mild to moderate stress urinary incontinence in men is an effective and safe method.
Moderated Poster Session 10: BPH II
Prostatic Urethral Lift real‐world experience is consistent with controlled trial results in both non‐retention and retention subjects
NJ Barber, KL Ng, SN Gange, G Eure, M Rochester
Frimley Park Hospital
Introduction & Objective: Real world studies reflective of heterogenous populations should serve as a litmus test for new technologies, including those within the minimally invasive field for BPH. In order to determine how the UroLift System performs in the real‐world setting compared to previous experience in controlled settings, an analysis was conducted on the large, actively enrolling Real World Retrospective (RWR) study in comparison to the L.I.F.T. pivotal and P.U.L.S.A.R. urinary retention Prostatic Urethral Lift (PUL) trials.
Methods: The Real‐World Retrospective (RWR) study gathered data from 2491 subjects across 22 USA, UK, and Australian sites who had undergone PUL after market clearance. RWR data was then filtered into non‐retention (RWR Group A, n = 2117) and retention (RWR Group B, n = 374) groups. Controlled studies used for comparison were L.I.F.T. ‐ the randomized controlled trial for PUL following non‐retention subjects over 5 years (n = 140), and P.U.L.S.A.R. ‐ a controlled study following retention subjects post‐PUL for 12 months (n = 52). Absolute IPSS scores across all studies were compared at 1, 3, 6, and 12 months post‐procedure using a one‐way ANOVA. Adverse events and catheterization rates of RWR subjects were calculated and compared to L.I.F.T. and P.U.L.S.A.R. studies.
Results: We report similar absolute IPSS scores among all groups at all timepoints following PUL (Figure 1), demonstrating no differences in symptom outcome after treatment between real‐world and controlled studies. Analyses also revealed equivalent safety profiles when comparing real‐world groups with their respective controlled studies. Adverse events in both RWR Groups (A: non‐retention; B: retention) were mild‐moderate, transient, and not elevated compared to L.I.F.T. or P.U.L.S.A.R. 84% of RWR Group A subjects were catheter‐free post‐procedure (excluding catheter placement for standard of care), which is slightly better than the 68% catheter‐free rate of the L.I.F.T. trial. Catheter‐independence of RWR Group B subjects was consistent with P.U.L.S.A.R. results at 1 month (p = 0.2) and at longest available follow up (p = 0.3).
Conclusions: Analysis of PUL real world study results vs. controlled trials demonstrate consistent symptom response, safety, and patient experience, revealing positive and novel findings for minimally invasive therapy in the BPH space.
Real‐World and Controlled Trial Predictors of Durability after Prostatic Urethral Lift (PUL)
NJ Barber
Frimley Park Hospital
Introduction & Objective: Durability is an important component in any BPH treatment, and should be studied in minimally invasive therapies. The LIFT pivotal controlled study demonstrates PUL durability to 5 years, and data in the real‐world have revealed successful outcomes in various BPH populations. Here, we sought to understand how baseline characteristics correspond to PUL durability in the real world and in a controlled setting.
Methods: Uni‐ and multivariate predictive assessments were calculated for the likelihood of a successful response for 2714 non‐retention subjects from the Real‐World Retrospective (RWR) database, i.e. lack of subsequent BPH surgery through the point at which 90% of the population was censored or follow‐up data were no longer available. The analysis included baseline variables such as age, comorbidities, medical history and BPH disease severity (e.g. IPSS, QoL, Qmax). Univariate predictive assessments were performed for subjects from the LIFT trial (LIFT, n = 140). A stepwise procedure was used to select predictors for the multivariate logistic regression models. An odds ratio >1 indicated a higher probability of retreatment.
Results: The variables of age at baseline, duration of LUTS prior to PUL, and comorbidities such as diabetes and obstructive median lobe did not influence PUL durability. Higher IPSS and QoL at baseline significantly predicted an increased likelihood of surgical retreatment for RWR and LIFT patients. Large prostate volume ( >100cc, not applicable to the LIFT study) was not a predictor compared to <100cc prostates. Lower Qmax was a predictor in the LIFT group, but not in RWR. Odds ratios for all significant RWR predictors were close to 1, and the largest significant odds ratio for LIFT was 3.4 with the QoL baseline variable. When QoL was entered into a multivariate model, no other covariates added significantly to the prediction. The RWR analysis included 1070 days of follow‐up based on the density of available data; 154 patients were retreated during this time.
Conclusions: This analysis of baseline variables in the real world and controlled LIFT trial reveals worsened IPSS and QoL as possible predictors of reintervention following PUL, suggesting that a more severe disease state at baseline may increase the likelihood of undergoing subsequent BPH surgery. Urologists may utilize these findings as support to consider BPH interventions earlier in the disease process.
Continuous mode bipolar plasma vaporization of the prostate – Still a “go” after 6 years of follow‐up?
BF Geavlete, C Moldoveanu, C Ene, C Bulai, A Ene, PA Geavlete
“Saint John” Emergency Clinical Hospital, Department of Urology
Introduction & Objective: A prospective, long term, randomized‐controlled study evaluated the efficiency and safety of an energy source enabling a continuous bipolar plasma vaporization of the prostate (C‐BPVP) to be achieved by comparison to the first generation standard bipolar vaporization (S‐BPVP) as well as to conventional monopolar transurethral resection of the prostate (TURP) in medium size benign prostatic obstruction (BPO) cases.
Methods: A total of 180 BPO patients with prostate volume between 30 and 80 mL, maximum flow rate (Qmax) below 10 mL/s and International Prostate Symptom Score (IPSS) over 19 were equally randomized for C‐BPVP, S‐BPVP and classical TURP. All cases were evaluated preoperatively and every 12 months' for a total period of 6 years after surgery by IPSS, Qmax, quality of life score (QoL) and post‐voiding residual urinary volume (PVR).
Results: The mean operation time was significantly shorter in C‐BPVP cases by comparison to conventional plasma‐button vaporization and to monopolar resection (31.5 versus 40.6 and 49.8 minutes). Consequently, a substantial 22.4% and respectively 39.1% difference in surgical length was emphasized in favor of C‐BPVP when compared to S‐BPVP and TURP. Significantly lower capsular perforation (1.7% and 1.7% versus 8.3%), and intraoperative bleeding (1.7% and 3.3% versus 11.7%) rates as well as mean hemoglobin drops (0.4 and 0.6 versus 1.4 g/dL) were emphasized in the C‐BPVP and S‐BPVP series when compared to TURP. Also, significantly reduced mean catheterization periods (24.1 and 23.8 versus 73.6 hours) and hospital stays (2.1 and 2.2 versus 4.5 days) were described for the C‐BPVP and S‐BPVP groups. The rate of re‐catheterization imposed by acute urinary retention (1.7% and 1.7% versus 6.7%) was significantly higher among the monopolar resection cases. During all the yearly periodical check‐ups up to 6 years after the initial intervention, statistically superior IPSS and Qmax measurements were determined in the 2 bipolar vaporization study arms.
Conclusions: The new technical improvement of the BPVP procedure was able to reduce the surgical time by an average proportion of 20%. The bipolar plasma vaporization approach emphasized significantly superior perioperative safety features and improved follow‐up voiding and symptom scores' parameters over the standard monopolar resection during the 6 years' long term follow‐up.
Outcome of TransUrethral Enucleation with Bipolar(TUEB) in patients with huge prostate hyperplasia : comparison of prostate volume more than 80ml with less
Y Endo, H Shimizu, J Akatsuka, Y Kondo
Nippon Medical School
Introduction & Objective: Transurethral resection of the prostate has been the standard surgical treatment for benign prostatic hyperplasia (BPH). We reported that the efficacy and safety of TransUrethral Enucleation with Bipolar (TUEB) is comparable to those of TURP for managing BPH. Despite the remarkable progress in minimally invasive treatment, rescent guidelines still recommend open surgery for the treatment of patients with large prostate of more than 80ml. The aim of the present study was to investigate the impact of preoperative prostate volume on the outcome of TUEB. We analyzed the difference of the efficacy and safety of TUEB between patient with PV of more then 80ml and less.
Methods: A total of 180 patients with medication resistant BPH who underwent TUEB in our institution by single surgeon from 2008 to 2015 were retrospectively examined. All patients were evaluated with the international prostate symptom score (IPSS), quality of life score (QoLs), uroflowmetry (Qmax), serum prostate specific antigen (PSA), and transrectal ultrasonography (TRUS) of the prostate. Patients were divided into two groups based on whether their preoperative prostate volume (PV) was greater than 100ml measured by TRUS (PV> = 80ml : huge group (HG), PV <80 : standarad group (SG) ). Perioperative change of IPSS, QoLs, Qmax and PSA were assessed as efficacy. Perioperative serum sodium and hemoglobin decrease and all adverse events were assessed as safety. Chi‐square test and student t‐test was performed to compare outcomes of two groups.
Results: All patients were performed collected with sufficient data performed TUEB. As preoperative baseline value, mean IPSS was 20.4, QOLs 5.0, Qmax 6.6 (mL/s), PSA 6.9 (ng/dL). Postoperatively all of those were improved with statistically significance, mean IPSS was 4.9, QoLs was 1.1, Qmax was 18.9(mL/s), PSA was 1.1 (ng/mL). Mean PSA level decreased 89.8 ± 1.2% after TUEB. There was neither hyposodemia nor blood transfusion around operation. There were 48 patients (27%) in the HG and 132 (73%) in the SG. Mean PV of each group was 106.2ml ±26.6 (HG) and 52.9ml ±13.7 (SG). Mean operative time of HG (146.2min ±34.0) is significantly longer than SG (85.9min ±22.9). On efficacy decrease of IPSS voiding score on SG is significantly larger than HG, improvement of Qmax on HG is significantly smaller than LG. On safety parameters and AE were comparable.
Conclusions: The efficacy and safety of this novel procedure seem very promising. TUEB also showed sufficient efficacy and safety for the patient with huge PV of more than 80ml. TUEB could be a new gold standard procedure for BPH regardless of PV. Longer follow‐up and larger prospective studies are necessary to confirm these promising results.
Single Surgeon Experience with Procept Aquabeam Aquablation of Prostate: First 55 Cases (with 18‐month Follow‐up)
A Kasraeian, M Alcantara, K Mola Alcantara, A Kasraeian
Kasraeian Urology
Introduction & Objective: Procept Aquabeam Aquablation is a novel, minimally invasive technology for management of BPH, regardless of prostate size or shape. The Aquabeam system is an innovative combination of robotic technology, multi‐dimensional real‐time imaging, and (&) heat‐free waterjet to precisely & accurately remove obstructive prostate tissue in men with BPH. We report our initial experience with our first 55 cases.
Methods: Between July 2018 & May 2019, data was prospectively collected on 55 men who underwent Aquablation of the prostate. Evaluation of LUTS included cystoscopy, urodynamics (UDS), & transrectal ultrasound (TRUS) to measure prostate volume. Pre‐operative (op), intra‐op & post‐op outcomes were prospectively collected & reported.
Results: Pre‐op demographics include mean age of 67 (50 to 84) & mean prostate volume of 100 cc (27 to 252). Of our 55 patients, 39 had prostates larger than 80cc (71%), 24 greater than 100cc (44%) & five (9%) greater than 150 cc. An obstructing median lobe was noted in 47 (85%) of the 55 men. Pre‐op UDS demonstrated severe bladder outlet obstruction (BOO) in 51 of the 55 men (93%). Detrusor instability was noted in 31 men (56%), & 27 of the 55 (49%) suffered from urinary retention with 17 (31%) requiring catheterization prior to procedure. Mean op time was 58 minutes (25‐108). Thirty‐five of the 55 men were discharged on post‐op day (POD) 1, with 13 discharged on POD 2 & three on POD 3. Two patients received transfusions, but in association with pre‐op anemia and hematuria associated with their enlarged prostate. One of two had also received transfusions pre‐operatively. Mean pre‐op hemoglobin (Hgb) was 14 (8.6 to 16.7). Mean immediate post‐op & day of discharge Hgb levels were 13 (9.3 to 16) & 11.8 (7.2 to 15.3), respectively. Of note, 47 of the 55 men reported erectile dysfunction at baseline. Post‐operatively, a 17 point (2‐29) mean decrease in AUA symptom score (AUASS) was noted from 22 (5 to 35), pre‐operatively, to 5 (1‐13), post‐operatively. Post‐op uroflow studies after 4‐6 weeks demonstrated a mean maximum flow rate (Qmax) of 21 ml/s (4.3 to 45), an increase of 13.3 points from 7.4 ml/s (1.9 to 15), pre‐operatively. Erectile function was maintained post‐operatively with a mean SHIM score of 11.5 (range 1 to 25) versus 10.5 (1 to 25), pre‐operatively. All patients completed successful voiding trials post‐operatively, & of those with baseline urinary retention, none currently require any form of catheterization.
Conclusions: The PROCEPT AQUABEAM Aquablation is an innovative technology that offers predictable & reproducible outcomes, independent of prostate size. Aquablation has a short learning curve & is easily reproduced regardless of prostate size or shape
Patients with self reported benign prostate hyperplasia without medical claims data have barriers to healthcare access
CM Forbes, R Hsi, NL Miller
Vanderbilt University Medical Center, Department of Urology
Introduction & Objective: Estimates of the prevalence of benign prostate hyperplasia (BPH) differ by administrative claims data or self‐report based on methodologic differences. We compared patient‐reported BPH diagnoses to administrative claims BPH diagnoses in order to assess prevalence estimates and to assess demographic and socioeconomic factors that influence how BPH is diagnosed.
Methods: We queried the All of Us Research Program, a common dataset of U.S. patients which actively recruits populations which are traditionally underrepresented in biomedical research. We identified adult male participants with and without a history of BPH according to either self‐reported history at enrollment from 2016‐2022, or administrative claims from 1980‐2020. Among 314,277 participants, which included 47% persons from racial minorities, there were 19,384 men over age 50 who had both medical history and medical claims data available. We compared age, race, education, household income, and healthcare affordability and access among patients with a self‐reported history of BPH without medical claims data to those with a claims‐based diagnosis.
Results: The prevalence of BPH was 27% (n = 5259) according to medical claims, and it was 21% (n = 4064) according to self report. Of patients with BPH by either medical claim or self‐reported history (n = 6716), 22% (n = 1457) had a self reported history only. This shows that a significant proportion of patients with BPH did not have a prior BPH‐specific medical claim. Furthermore, patients with only a self‐reported history of BPH were more likely be unable to afford a specialist (p = 0.04) or follow up (p = 0.03), and were more highly educated (p = 0.02) (Table 1).
Conclusions: Determinations of BPH prevalence by claims‐based data alone will not account for 22% of patients according to this national dataset in the US. These patients self‐report a history of BPH without associated medical claims data. These patients are more likely to have barriers to healthcare access. Advocacy and outreach efforts may improve care for this disadvantaged population.
12‐month Outcomes from the Large Real‐World Study and Urodynamic Results from PULSAR Demonstrate PUL is Safe and Effective in Retention Patients
M Rochester, NJ Barber, O Kayes, N Thiruchelvam, K Rajesh, T Page, G Eure, D Grier
Norfolk and Norwich University Hospital
Introduction & Objective: Minimally invasive surgical therapies for BPH should be evaluated in controlled studies and in the real world, and should be tested in various populations of patients including those in urinary retention. Here, we evaluate outcomes of real‐world PUL retention patients and report newly analyzed urodynamics data from the PULSAR retention controlled study.
Methods: The controlled PULSAR study evaluated outcomes after PUL of 52 retention subjects (with ≥1 failed TWOC on alpha blocker at baseline) over 12 months, including SHIM, satisfaction, and urodynamics. The Real‐World Retrospective (RWR) database included PUL subjects across 22 international sites, 512 of which were in active urinary retention status at the time of the PUL procedure. Baseline demographics, absolute symptom response, and AE and catheter‐independence rates were compared between RWR retention (RWR‐r) and PULSAR subjects.
Results: RWR‐r and PULSAR subjects were similar in baseline characteristics of age (71yo for both groups), prostate size (48cc vs. 55cc), and number of implants (4.7 vs. 4.8). Satisfaction was overall high among PULSAR subjects with 90% of PULSAR subjects feeling better, and duration of catheterization before PUL did not differ between most and least satisfied patients (140d vs 114d, correlation p‐value 0.5). Erectile function (SHIM) of PULSAR patients was preserved. 12 PULSAR patients had UDS data available, and at 12 months showed improvements in pdet@Qmax (23%) and BOOI (41%). 5 patients moved out of the obstructed zone (Fig 1); 86% of those who were technically obstructed at 12 months were catheter‐independent, and 83% felt very much better. IPSS, Qmax, and PVR outcomes of RWR‐r subjects were equivalent to PULSAR, and PULSAR QoL was significantly better at 12 months (1.4 vs. 2.1). Catheter‐independence rates were better for RWR‐r vs. PULSAR subjects at 1 month (81% vs. 60%) and at longest available follow‐up (84% vs 73%). Total AE rates were not elevated in RWR‐r subjects vs. PULSAR, and most AEs in both studies were mild‐moderate and transient.
Conclusions: Results from the RWR database were stable and largely consistent with the controlled PULSAR study at 12 months, indicating that PUL is safe and effective in retention patients and may be a viable option for this population of BPH patients.
Interim 2 Year Results for the EVEREST‐I Trial Evaluating the Optilume BPH Catheter System
O Kayes, S Kaplan, M Pichardo, E Rijo Cedano, R Rodriguez‐Lay, G Espino, R Estrella
St James's University Hospital
Introduction & Objective: The Optilume BPH Catheter System is a novel Minimally Invasive Surgical Therapy (MIST) for the treatment of lower urinary tract symptoms (LUTS) secondary to benign prostatic hyperplasia (BPH). The Optilume BPH System utilizes mechanical dilation of the prostatic urethra to achieve an anterior commissurotomy while delivering the drug paclitaxel to maintain urethral patency. The EVEREST‐I study is a prospective, single arm, multicenter study evaluating the Optilume BPH System.
Methods: A total of 80 subjects were enrolled at 6 centers in Panama and the Dominican Republic. Key eligibility criteria included an International Prostate Symptom Score (IPSS) of ≥13, peak urinary flow rate (Qmax) of 5‐15 mL/sec, and prostate volume 20‐80g with no prior MIST or surgical intervention. Medication washouts included 3 weeks for alpha blockers and 6 months for 5 alpha‐reductase inhibitors. Follow up is ongoing, with 54 of 75 expected subjects with 2‐year follow‐up complete. The primary endpoint was responder rate, defined as subjects experiencing a ≥40% improvement in IPSS without receiving additional therapy. Additional outcomes included IPSS, Qmax, and BPH Impact Index. Impact on sexual function was assessed by the International Index of Erectile Function (IIEF) and Male Sexual Health Questionnaire for Ejaculatory Dysfunction (MSHQ‐EjD).
Results: Symptom scores were significantly improved from baseline, with this improvement maintained through the 2‐year follow‐up. The responder rate was 81.8% at 2 years. A single subject received a prostatectomy 18‐months post‐treatment. Qmax improved from 10.9 mL/sec at baseline to 17.7 mL/sec at 2 years (p < 0.001). There was no change in sexual function as measured by the IIEF Overall Satisfaction score or the MSHQ‐EjD Satisfaction/Bother score.
Conclusions: The Optilume BPH System exhibited a significant improvement in both objective and subjective outcomes through 2‐years post treatment. A randomized, controlled trial is ongoing and long‐term follow‐up is planned through 5 years to further define the durability of the results.
Withdrawn
Management of benign prostatic hyperplasia with high tight bladder neck with minimally invasive approach of mini bladder neck distraction and prostatic urethral lift
KL Ng, NJ Barber
Frimley Park Hospital
Introduction & Objective: Optimal urinary flow outcomes from urolift surgery for BPH associated with high and tight bladder necks have been rather challenging. We describe our technique of mini bladder neck distraction with urolift for patients with BPH and concomitant high and tight bladder necks.
Methods: Patients with BPH associated with high and tight bladder necks were diagnosed in our one stop BPH clinic with flexible cystoscopy. They were counselled and consented for the procedure. Surgeries were performed under sedation in day surgery and were discharged on same day. Mini bladder neck distraction was achieved with minimal electrocautery of a shallow depth by incision at 6oclock midline before further urolift implants delivered in 4D fashion to enhance the bladder neck widening.
Results: 36 patients were recruited in our centre from June 2018 – Oct 2020. Median age was 66 (44 ‐ 80), mean preop mean PSA 1.27ng/mL and median prostate volume of 32.5cc. Mean preop Qmax of 11mls/s improved to 25.8mls/s post op and a mean 52% reduction in post void residual volumes. There was a reduction of 13 points in IPSS (66%) with preop mean IPSS 19 to 6.7 post op, with QoL improvement from 4.3 to 1.3. All men who had normal antegrade ejaculation preop reported no deterioration in ejaculation post operatively.
Conclusions: Mini bladder neck distraction with urolift is a safe and effective minimally invasive technique for BPH with high/tight bladder neck with excellent improvement in LUTS and preservation of ejaculatory function.
ThuLEP vs open simple prostatectomy for the treatment of prostates larger than 150 cc
M Maltagliati, L Berti, U Besana, C Buizza, M Sighinolfi, S Micali, BC Rocco, G Bozzini
ASST Valle Olona
Introduction & Objective: Thulium Laser Enucleation of Prostate (ThuLEP) is currently one of the alternatives to open simple prostatectomy (OP) in patients with benign prostatic hyperplasia (BPH) and prostates over 80 cc. However, enucleation of large prostates is believed to be a more challenging and time‐consuming procedure. The aim of our study is to report intraoperative, early and long term postoperative outcomes of ThuLEP and OP in patients with prostates larger than 150 cc.
Methods: We performed a prospective study on 385 patients with chronic and acute urinary obstruction (IPSS >20, Qmax <12) due to BPH and prostates >150 cc. 193 patients (Group A) underwent ThuLEP and 192 patients (Group B) underwent OP. Patients with urethral strictures, bladder stones, acute urinary tract infection, or with a history of prostate surgery were excluded. Ethical committee approval was obtained, and patients signed the informed consent. The Cyber TM 200 (Quanta System, Italy) and the Cyber Blade morcellator (Quanta System, Italy) were used to perform ThuLEP. All patients were evaluated preoperatively and postoperatively. Blood loss, catheterization time, irrigation volume, hospital stay and operative time were compared between the two groups. 3 months after surgery patients were also evaluated using the International Prostate Symptom Score (IPSS), maximum flow rate (Qmax), and postvoid residual urine volume (PVR).
Results: Mean prostate volume was 196.0 cc (150‐350 cc) in the ThuLEP group and 189.0 cc (150‐280 cc) in the OP group. Mean surgical time was 115.5 ± 44.7 minutes for ThuLEP and 98.5 ± 26.2 minutes for OP. Mean removed tissue weight was 149.0 g in group A and 172.7 g in group B. Catheterization time was 1.7 days in group A and 8.5 days in group B. Hospital stay was 2.3 days in group A and 11.9 days in group B. Median haemoglobin decrease was 1.05 g/dl in group A vs 5.43 g/dl in group B. 27 patients in group B (14.06%) vs 3 patients (1.55%) in group A required blood transfusions due to postoperative bleeding. During the 3‐month follow‐up, the procedures did not demonstrate significant differences in terms of Qmax, IPSS and PVR.
Conclusions: Despite similar results after three months from the procedure, simple transvescical prostatectomy is characterized by longer postoperative hospitalization and catheterization time and higher blood loss compared to ThuLEP. ThuLEP is slightly longer to perform, but has proved to be a safer treatment option in patients with prostates over 150 cc.
Evaluation of the learning curve for aquablation therapy of the prostate: a single‐center analysis
K Vogt, B Becker, AJ Gross, C Netsch
Department of Urology, Asklepios Hospital Barmbek, Hamburg, Germany
Introduction & Objective: In aquablation therapy, an automatic ablation is carried out after sonographic measurement of the prostate adenoma. It is postulated that the surgical result depends less on the ability of the surgeon than on the computer‐controlled tissue removal. The aim of our study was to evaluate the individual learning curve of aquablation therapy.
Methods: 45 consecutive patients with benign prostatic hyperplasia (BPH) were treated by a single surgeon (CN) without technical experience. The surgeon completed a cadaver course and was accompanied by a proctor during the first 10 procedures. The learning curve was determined by the change in the surgical time over the patient series. All data is expressed as median (interquartile range).
Results: The median age was 67 (62 ‐ 71) years and prostate volume was 70 (50 ‐ 85) ml. The surgical time was 44 (30 ‐ 55) min. Aquablation has been successfully performed in all patients. IPSS (20. 5 vs. 9) and QoL (5 vs. 2) significantly improved at discharge (p < 0. 001). The catheterization time and the postoperative stay were 2 (2 ‐ 3) days, respectively. Hemoglobin loss was 2 (1. 3 ‐ 2. 9) g/dl. Transfusions were not necessary. Reoperations (bladder tamponade, persistent bleeding) were performed in 3 patients (6. 6 %). A postoperative urinary retention occurred in 4 (8. 8 %) patients and 3 (6. 6 %) patients developed a urinary tract infection. 5 (11. 1 %) patients developed a bladder tamponade that could be evacuated via catheter. The median operation time decreased from 55 (patients 1 ‐ 10) to 30 minutes (patients 31 ‐ 40, p < 0. 001).
Conclusions: Aquablation therapy is a safe surgical procedure and leads to an immediate improvement of the micturition during the learning curve of the procedure. After 30 procedures, a significant reduction in the surgical time has been shown.
Comparison of vaporization and enucleation techniques based on the functional outcomes and complications of patients with benign prostatic hyperplasia: systematic review and meta‐analysis.
A Shpikina, A Morozov, M Taratkin, A Novikov, D Enikeev
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia
Introduction & Objective: Nowadays the most commonly used methods of BPH surgical treatment are vaporization (PVP) and enucleation of the prostate (EEP). We aimed to compare intra‐ and perioperative results of the patients who underwent PVP and EEP.
Methods: A systematic literature search was performed in 3 databases (MEDLINE, Web of Science and Scopus) on a search query: (EEP OR «prostate enucleation» OR «BPH enucleation») AND (PVP OR prostate AND vaporization) according to PRISMA guidelines. The detailed search strategy is available at Prospero, CRD42020204739. The scope of the review according to PICO process is as follows:
P ‐ patients with BPH.
I ‐ any types of EEP or PVP
C ‐ preoperative data, operation characteristics, outcomes of different types of EEP and PVP
O ‐ functional outcomes, effectiveness of the procedures, safety.
Primary outcomes were functional results (IPSS, QoL, PVR, Qmax). Secondary outcomes were intraoperative results, postoperative PSA and prostate volume, complications, and recurrence rate.
Results: The search identified 436 articles, and the final sample contained 15 articles covering a period 2011‐2020 years. Functional outcomes (IPSS, QoL и Qmax) were comparable at 12 months follow‐up (Figure 1). Elkoushy et al. showed benefit of EEP over PVP at 36 months follow‐up, IPSS 7.2 ± 8.4 vs 3.1 ± 4.6, p = 0.01, and Qmax 24.3 ± 16.2 ml/s vs 28.1 ± 10.2 ml/s, p = 0.001. While EEP and PVP duration did not differ significantly in BPH <80 cm3, higher BPH volume was associated with longer operative time. Complication rate (Clavien‐Dindo I and II) was higher in the EEP group (13 – 42%) comparing to PVP (10.3 – 21.7%), especially the percentage of blood transfusion and transient urinary incontinence. But the rate of complications grade IIIa and higher was similar (3 – 6%). Reoperation rate was significantly higher in the PVP group at 60 mo. follow‐up, 2.7% vs 0%, p < 0,05. Postoperative prostate volume and PSA level were also higher in the PVP group.
Conclusions: Short‐term outcomes of the patients were comparable in both enucleation and vaporization groups. Long‐term results including the percentage of relapse were better in patients who underwent enucleation of the prostate.
The impact of benign prostatic hyperplasia surgery on erectile function: a systematic review and network meta‐analysis of randomized‐controlled trials
D Jabarkhyl, A Light, O El Hage, P Dasgupta
GKT School of Medical Education, King's college London
Introduction & Objective: Benign prostatic hyperplasia (BPH) is an independent risk factor for erectile dysfunction. Numerous treatment modalities have recently emerged for BPH. These all risk erectile dysfunction yet may also improve function. A systematic review with network meta‐analysis is crucial for identifying how modalities benefit or worsen erectile function, an important patient‐centred outcome.
Methods: In October 2019, MEDLINE, Embase, and Web of Science were searched for randomized‐controlled trials (RCTs) comparing BPH surgical interventions. The primary outcome was post‐operative International Index of Erectile Function‐5 (IIEF‐5) score at 6, 12, 24, and 36 months. Bayesian network meta‐analysis using a random‐effects model was performed with meta‐regression. Baseline IIEF‐5 score was chosen as the covariate. Using monopolar transurethral resection of the prostate as the reference intervention, mean differences (MD) with 95% credible intervals (95% CrI) and rank probabilities (p) were calculated. PROSPERO registration: CRD42019155506.
Results: From 4606 results, 48 RCTs (5156 patients) encompassing 12 techniques were included (Fig.1). Prostatic urethral lift (PUL) ranked highest for IIEF‐5 score at 6 months (11 techniques; p = 0.581; MD 2.4, 95% CrI ‐0.71 to 5.6), 12 months (12 techniques; p = 0.782; MD 2.9, 95% CrI ‐0.26 to 6.1), and 24 months (9 techniques; p = 0.948; MD 3.6, 95% CrI 0.14 to 7.1). At 36 months (6 techniques, not including PUL), bipolar transurethral resection of the prostate ranked highest (p = 0.424; MD 0.25, 95% CrI ‐0.53 to 0.91). Lowest ranking treatments were laparoscopic simple prostatectomy at 6 months (p = 0.360; MD ‐0.65, 95% CrI ‐2.5 to 0.98) and 36 months (p = 0.461; MD ‐0.48, 95% CrI ‐1.8 to 0.77), prostatic arterial embolization at 12 months (p = 0.709; MD ‐3.3, 95% CrI ‐8.3 to 1.9), and Aquablation at 24 months (p = 0.464; MD ‐0.97, 95% CrI ‐3.7 to 1.7).
Conclusions: Based on network meta‐analysis, PUL produces superior erectile function benefit up to 24 months. In contrast, laparoscopic simple prostatectomy produced worse erectile function at 6 and 36 months. PUL data with longer follow‐up is required, plus further RCTs analyzing other new modalities.
New Visual Prostate Symptom Score versus International Prostate Symptom Score in Men with Lower Urinary Tract Symptoms: a prospective comparison
C Laranjo Tinoco, F Diaz Ferreira, A Cardoso, R Matos Rodrigues, S Anacleto, P Passos, E Lima, M Cerqueira Alves, CA Oliveira
Hospital de Braga, EPE
Introduction & Objective: The International Prostate Symptom Score (IPSS) is an important tool in assessing lower urinary tract symptoms (LUTS) in men with benign prostate hyperplasia (BPH). Due to its limitations, alternative scores emerged, like the New Visual Prostate Symptom Score (VPSS). The aim of this study was to compare and correlate both these questionnaires.
Methods: 100 BPH patients with LUTS were prospectively evaluated between August and November 2017. Exclusion criteria included impared cognitive disfunction, marked visual difficulties, recent urethral catheterization (in the previous month), inability to perform uroflowmetry or voided volume <150mL. Patients answered both questionnaires in the presence of the main investigator. Data collected included the patients' age; level of education; IPSS and VPSS filling time, need of investigators' assistance during filling and total scores; uroflowmetry parameters (Qmax and Qavrg); Prostate Specific Antigen (PSA) value; and prostate volume on vesical ultrasonography. Statistical analysis was performed with Spearman correlations and the Wilcoxon test.
Results: Mean age was 68 years (SD = 9.74) and less than 30% of the patients had completed more than 4 years of schooling. 89% of the patients were able to complete the VPSS without help as opposed to 59% in the IPSS (Graph 1). Spearman correlation results showed significant correlation of IPSS total with VPSS total (r = .651, p < .001). Both the IPSS and the VPSS had a negative correlation with Qmax (r = ‐.201, p = .046 and r = ‐.228, p = .023, respectively). More correlation results can be found in Table 1. The median time spent filling the IPSS (175s, IQR = 54) and the VPSS (93.5s, IQR = 50) was significantly different (Z = 8.68, p < .001).
Conclusions: VPSS correlates significantly with IPSS and Qmax. It can be completed without assistance by a greater number of men and it requires a shorter time to fill in. These findings suggest that VPSS can accurately assess presence and severity of LUTS in a wider population than IPSS.
Withdrawn
Withdrawn
SoracteLite® Transperineal Laser Ablation as Novel Minimal Invasive Treatment for Benign Prostatic Obstruction: Initial Results of a Pilot Study
R van kollenburg, LA van Riel, JR Oddens, TM de Reijke, HP Beerlage, M de Bruin
Department of Urology, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, the Netherlands
Introduction & Objective: Surgical treatments for lower urinary tract symptoms (LUTS) caused by benign prostatic obstruction (BPO) provide good outcomes, but require transurethral approach and anesthesia. Recent minimal invasive treatments are more patient friendly, but risks such as strictures and hematuria persist due to the transurethral approach. SoracteLite® transperineal laser ablation (TPLA) is a novel office based technique that can be applied under local anesthesia with optional conscious sedation, by a transperineal approach. In this prospective pilot study, we determine 1) safety and feasibility, 2) possibility of TPLA using local anesthetics and 3) functional outcomes of TPLA for men with LUTS due to BPO.
Methods: This study will enroll 20 patients. Men aged ≥40 yrs, with a Qmax of 5–15 mL/sec, prostate volume of 30–120 cc and urodynamically proven bladder outlet obstruction are eligible for inclusion. TPLA treatment consists of placement of one or two fibers in the transition zone of each prostate lobe, depending on the prostate volume. Tissue is treated with 1800J at 3W at 1064 nm. Depending on the prostate length, a second ablation is performed following fiber retraction. The TPLA procedure is performed under ultrasound guidance. Safety and feasibility are measured by adverse events using Clavien Dindo score and successfully completed procedures. Functional outcomes are assessed by uroflowmetry and International Prostate Symptom Score (IPSS) at 3, 6 and 12 months.
Results: 15 men have been enrolled and treated so far. Mean age (range) was 68.7 (59–80) years, Qmax 9.4 (5–15) mL/s, prostate volume 67.5 (31–117) cc, IPSS 21.4 (12–28) and QoL 4.7 (3–6). No device related adverse event occurred, nor any grade ≥3 adverse events during follow‐up. First two patients were treated under general anesthesia, the following patients under local anesthetics alone (n = 7), or combined with conscious sedation (n = 6). After treatment 7 men continued spontaneous voiding, 8 men needed an indwelling Foley catheter for 16.7 (10–20) days. Functional outcomes of 12 men were available for analysis and showed an improved Qmax of 13.3 (4–25) mL/s, IPSS of 13.8 (3–29) and QoL 2.5 (0–6) at 3 months.
Conclusions: This study is the first to show that TPLA can be performed using local anesthetics. The preliminary functional outcomes are encouraging. Longer‐term follow‐up data are awaited.
Withdrawn
Analysis of outcome of prostatic UroLift placement in benign enlargement of prostate in a District Hospital
K Biswas, S Ahmed, K Soundararasha, G Rix, R Pillai, J Corr, Z Maan, S Datta
Colchester General Hospital
Introduction & Objective: We aim to analyse the outcome of Prostatic UroLift (PUL) placement done at our hospital for the treatment of Benign Prostatic Hyperplasia (BPH).
Methods: Demographic and perioperative data were collected for all patients who underwent PUL placement at out hospital from December 2017 to December 2019 for the treatment of BPH. International Prostate Symptom Score (IPSS), Quality of Life (QoL), urinary flow rate (Q‐max), complications and requirement of auxiliary procedures were noted till date. Paired Student's t‐test was used to compare the pre‐operative and post‐operative parameters.
Results: Total of 45 patients underwent PUL placement and were followed‐up for a median period of 26 months (14 months, 37 months). Mean age of the patients was 74.8 ± 8.4 years. Mean prostatic volume was 49.5 ± 9.8 ml (5 patients had median lobe). Average 3.2 ± 1.1 numbers of clips were placed. The mean IPSS, QoL and Q‐max in the pre‐operative and latest follow‐up period were 19.3 ± 5.9 and 11.1 ± 5.6 (p < 0.001); 4.3 ± 1.1 and 2.5 ± 1.4 (p < 0.001); 9.8 ± 5.0 ml/s and 12.8 ± 6.2 ml/s (p = 0.004) respectively. Complications noted were dysuria (1 patient, 2.2%), urinary tract infection (1 patient, 2.2%), haematuria (1 patient, 2.2%), transient urinary retention (2 patients, 4.4%), post‐void dribbling (2 patients, 4.4%), bladder stone (1 patient, 2.2%) and migration of clip (1 patient 2.2%). Six patients (13.3%) required auxiliary treatment during follow‐up.
Conclusions: PUL placement improved the IPSS, QoL and Q‐max significantly over a median follow‐up of 26 months. It is a safe procedure with only few transient and easily‐manageable complications.
Online engagement with treatments for benign prostatic hyperplasia: Is interest in Urolift outpacing the gold standard?
MI Lucas, P Diaz, F Escobedo, B Limbrick, KB Scotland
Department of Urology, UCLA
Introduction & Objective: Patients suffering from progressive symptoms of benign prostatic hyperplasia (BPH) increasingly turn to the internet for information on invasive and minimally invasive surgical therapies (MIST). This study aimed to identify online articles accessed by patients seeking guidance on said options and to evaluate the quality of their content.
Methods: Google Trends was used to evaluate search term popularity for BPH procedures from February 2016 to February 2021. The BuzzSumo social media analysis tool was used to identify articles related to procedural treatments for BPH with the most engagements on social media platforms over the same time span. Engagements were calculated as the sum of comments, likes, and shares of articles identified on Facebook, Twitter, Pinterest, and Reddit. Two individual reviewers rated the quality of the articles based on the average score obtained using the DISCERN tool. Google trends data and DISCERN ratings were analyzed with ANOVA and paired t‐test, respectively.
Results: The top 18 articles obtained from BuzzSumo analyses were selected and accounted for 19,805 total engagements. Facebook was the most used platform, accounting for 97% (19,198) of total engagements. Nine articles (50%) came from news organizations and none came from a scientific peer reviewed journal. Thirty‐three percent of articles discussed prostatic artery embolization (PAE) and Rezum. Thirty‐nine percent of identified articles were rated as low quality, 39% as moderate quality, and 22% as high quality using the DISCERN tool, with no significant difference among reviewer ratings. Google Trends data reveal a rising popularity of MIST such as Rezum, Urolift, Aquablation, and PAE in the study period, far exceeding interest in invasive procedures like HoLEP and laser surgery. Urolift interest has specifically increased in the past 6 months. However, transurethral resection of the prostate (TURP) remained popular with no significant difference between MIST and TURP on Google Trends (Figure 1).
Conclusions: Patients are more likely to encounter online sources of low to moderate quality with serious to important shortcomings regarding information on procedural treatments for BPH. Urologists should consider the role of social media platforms when guiding patients to sources of accurate and comprehensive information for BPH treatment, especially with the rise in popularity of MIST.
Major postoperative complications after Aquablation: initial experience
A Hambaryan, A Kugler, R Badalyan, T Krause, W Schafhauser
Klinikum Fichtelgebirge
Introduction & Objective: Aquablation is a new robotically controlled minimally invasive treatment of benigne prostatic obstruction related lower urinary tract symptoms. The available data indicate a high efficacy of Aquablation, which is comparable to the TURP.
A potential obstacle to wider promotion of Aquablation may be the fear of possible complications, especially at the initial stage of implementation.
Our aim was to evaluate perioperative major complications after Aquablation immediately after its implementation in our clinic, and after gaining initial experience.
Methods: The study included males operated with Aquablation with prostate volume (PV) 35‐100 ml. Exclusion criteria were previous transurethral surgery, usage of anticoagulants, urinary tract infection, urogenital malignancies, previous urinary tract catheterization. After completion of Aquablation a urethrocystoscopy with superficial cautery of bladder neck was done in all cases. As a major complication we defined complications grade III‐V according to Clavien‐Dindo. The patients were divided into “early” and “late” groups according to intervention time.
Results: Total 73 patients were included, 37 patients were in the early group and 36 patients in the late group. The descriptive statistic is presented in the table. The most common major complication was an acute urinary retention, with or without haemotamponade. In most cases it was managed with short‐term catheterization. There were 2 re‐coagulations in the early group. One patient was re‐operated at the day of Aquablation, and the second after 2 months due to bleeding in hypertensive crisis. In the late group we performed one TURP after 1 month due to recurring urinary retention. In the late group we were able to reduce the duration of catheterization, hospitalization and the operation time without increasing the risk of complications. There were no cases of grade IV‐V complications, haemodynamic complications, infections or blood transfusion in both groups.
Conclusions: We can conclude that the Aquablation is a low risk procedure, even performed in early stage after implementation. Gaining the experience leads to mild decrease of major complications with shortening the operating time and duration of hospital stay.
Moderated Poster Session 11: Stones IV: PNL & URS
Miniperc represents an effective middleground between standard PCNL and RIRS in the treatment of small to medium size stones
S Proietti, L Rico, M Pavia, MJ Basulto‐Martínez, Y Yeow, L Villa, E Ventimiglia, A Salonia, F Gaboardi, G Giusti
IRCCS Ospedale San Raffaele, Milan, Italy
Introduction & Objective: After an initial skepticism on its potentiality, the development of dedicated miniaturized armamentarium, the understanding of the physics behind the vacuum cleaner effect together with the increased efficacy of modern laser generators, the increasing request for minimally invasive procedures have made the indication to MINIPERC for renal calculi increasingly attractive, easing a widespread dissemination of the technique among the endourological community worldwide. The aim of this study is to report the outcomes of our series of patients with renal stones who underwent MINIPERC, reporting its effectiveness and safety
Methods: A prospective analysis of 344 consecutive patients who underwent supine MINIPERC at our institution between September 2016 and December 2020, was performed. Intraoperative and postoperative outcomes were assessed. Abdominal noncontrast computerized tomography scan was performed in all cases preoperatively and 1‐month postoperatively. Patients were reported to be stone free if there were no residual fragments. Peri/postoperative complications were reported according Clavien‐Dindo classification system. The primary endpoint of the study was stone free rate (SFR) and the secondary endpoints were Clavien‐Dindo complications grade 1 or higher
Results: The demographic and stone characteristics of patients and the outcomes are reported in the Table.
Conclusions: MINIPERC is an effective and safe technique for treating small‐medium size renal stones that represents a reasonable middleground between standard PCNL and flexible ureteroscopy (FURS). Miniaturized PCNL is a further weapon that a modern endourologist should be familiar with in order to be always able to deliver a tailored therapy for every patient according to his stone features.
A randomized controlled trial of removal of asymptomatic small renal stones at the time of symptomatic stone removal
M Sorensen, JD Harper, M Borofsky, T Hameed, K Smoot, B Burke, B Levchak, MR Bailey, JC Williams, Z Liu, JE Lingeman
Indiana University
Introduction & Objective: The purpose of the study is to test whether removing small, asymptomatic stones from the kidneys of patients being treated for kidney or ureteral stones will reduce recurrence of stone events in subsequent years.
Methods: Patients scheduled to undergo ureteroscopy for treatment of nephrolithiasis were candidates for the study if they had a primary symptomatic ureteral stone and a small asymptomatic kidney stone(s) (ipsilateral or contralateral) or if they were undergoing treatment of primary kidney stones and had a small contralateral asymptomatic kidney stone(s). Subjects were randomized to have only the primary stone site treated (control) or to also have the asymptomatic kidney stone(s) treated. Subjects were followed for up to 5 years with CT imaging and clinical follow up. Appropriate candidates were offered and underwent metabolic prevention. Fisher's exact test and Pearson's chi‐square test were used to compare groups. The primary outcomes of interest were the odds of an additional surgery, presentation to the emergency department (ED), or future stone event from the same side as the asymptomatic kidney stone during the period of follow up.
Results: Seventy‐one subjects were included with similar demographics and follow up between treatment and control groups (Table 1). Subjects that were randomized to have their asymptomatic stones treated were 83% less likely require a surgery and 74% less likely to return to the ED for their asymptomatic stones over the follow up period. On the other hand, 3 subjects where the asymptomatic kidney stones were surgically removed returned to the ED within 2 weeks for pain that went away after stent removal versus one short term return in the control group (p = 0.61).
Conclusions: Removing asymptomatic stones from a kidney at the time of ureteroscopy reduced return visits to the ED and future surgical procedures. Based on these results, we would recommend treatment of distant asymptomatic stones at the time of ureteroscopy.
Treatment of difficult ureteroscopy retreat due to rigid ureterostercopy incarcerated in ureter (report of 18 cases)
R Huang, X Rihai, W Xiaoning, L Folin, X Tianpeng, Z Guoxi, X Zou
Introduction & Objective: To summarize the clinical data of difficult ureteroscopy after transurethral ureteroscopy, and discuss the causes and effective treatment methods of rigid ureteroscopy incarceration.
Methods: A retrospective review was made on 18 cases, including 7 female and 11 male patients, who have difficulty withdrawing ureteroscopy due to ureteral incarceration during ureteroscopy. Among them, two cases were communicated adequately with the anesthesiologist to properly enhance muscle relaxants. At the end of the operation, we successfully withdrew from the lens body by injecting a small amount of water‐based lubricant and warm water. The six female patients, after fully draining the urine in the bladder, can be removed the ureteroscope smoothly by using the index finger and middle finger to reach the vagina against the anterior fornix among the female patients. The other female case, it was necessary to pack gauze into the vagina while combining the index finger and middle finger, which was also smoothly removed because of the index finger and middle finger were not able to exert force. In addition, eleven male patients removed the ureteroscope successfully after fully draining the urine in the bladder with the index finger and middle finger extended into the rectum against the body of the ureteroscope. However, there was one patient who could not remove the ureteroscope and had to undergo surgery to remove it smoothly.
Results: Seventeen patients could withdraw the ureteroscope smoothly without serious complications after adopting appropriate treatment measures. In one case, the ureteroscope was successfully pulled out after the open operation because of repeated attempts to withdraw it. All patients recovered and discharged after surgery.
Conclusions: In ureteroscopy operation, the incarceration of the ureter can be detected in time and appropriate treatment measures can be taken to avoid the occurrence of serious complications such as avulsion of the ureteral mucosa and rupture of the ureter caused by forced withdrawal.
Revisiting the role of Oxalobacter formigenes in kidney stone formation: a deep dive into the microbiome at multiple body sites
KF Al, B Joris, JD Denstedt, J Chmiel, J Bjazevic, GB Gloor, H Razvi, JP Burton
Introduction & Objective: There is a longstanding belief that intestinal colonization by Oxalobacter formigenes can reduce the risk of oxalate‐based stone disease through its capacity to degrade calcium oxalate. However, literature on the topic remains controversial, and mounting evidence instead suggests that a polymicrobial effect from both the urinary and gut microbiomes may play a greater role in the disease. The aim of the present study was to address this knowledge gap by comprehensively characterizing the microbial communities of interest in kidney stone formers and healthy controls.
Methods: In the largest study of its kind, the microbiota of fecal and urine samples from 83 stone formers (SF) and 30 healthy controls (HC) was evaluated with whole shotgun metagenomic sequencing and 16S rRNA amplicon sequencing, respectively. Stone fragments and intraoperative urine from SF were also analyzed, and urinary oxalate concentrations were determined with HPLC.
Results: The findings demonstrate that despite similar dietary micronutrient consumption between the groups, urinary oxalate concentrations were higher in the SF cohort. Alongside these differences, the SF gut microbiota was significantly enriched in Enterobacteriaceae and several presumptive uropathogens, while depleted in microbes known to be beneficial such as Faecalibacterium prausnitzii. The gut microbiota of SFs was also aberrant compared to HC in several metabolic capacities. Importantly, there was no difference between groups in the relative abundance of O. formigenes, nor genes involved in oxalate catabolism including formyl‐CoA transferase and oxalyl‐CoA decarboxylase. The urinary microbiota was altered between HC and SF, and significantly differed in the SF over time (pre‐operative vs. intraoperative urine samples), exhibiting enrichment in pathogenic bacteria following perioperative antibiotic treatment that were similar to those elevated in the SF gut. Interestingly, kidney stones harboured a microbiota distinct from urine, and this was not dictated by the stone's crystalline composition
Conclusions: Together these findings suggest that the microbiome of SF is dysfunctionally altered in a multimodal manner, aggravating stone formation. The microbiome at multiple body sites, as an interconnected system, likely plays a far more significant role in nephrolithiasis beyond the dogmatic perspective that O. formigenes colonization is the key to stone prevention.
Ketorolac to reduce ureteroscopy symptoms trial
J Syed, AI Khan, M Goland‐Van Ryn, P Motamedinia
Yale University School of Medicine
Introduction & Objective: To assess the use of intraoperative IV ketorolac on the peri‐operative total morphine equivalent (ME) requirements of patients undergoing ureteroscopy for nephrolithiasis.
Methods: Patients undergoing ambulatory ureteroscopy for nephrolithiasis were prospectively randomized to receive ketorolac at the time of anesthesia induction. Patients and surgeons were blinded to treatment. Exclusion criteria included NSAID related asthma or allergy, renal insufficiency, peptic ulcer disease, bleeding diathesis, pregnancy/breast feeding, advanced age, and inability to provide consent. Intraoperative, postoperative, and combined morphine milligram equivalents (MME) were calculated. Multivariable regression was used to identify independent predictors of MME requirement. Complications were recorded.
Results: A total of 94 patients were analyzed following randomization. There were 46 patients in the treatment arm and 48 patients in the control arm. There were no statistically significant differences in gender, age, BMI, operative length or baseline pain medication use between groups (p > 0.05). Patients in the treatment arm required lower intraoperative MME when compared to the control arm (17.1 vs 24, p < 0.01). There were no statistically significant differences in the postoperative MME requirements between groups. The combined peri‐operative MME was lower in the treatment arm compared to the control arm (22.2 vs 30.4, p < 0.02). Ketorolac use was an independent predictor of lower MME use on multivariable analysis (beta coefficient ‐5.1, p < 0.01). There was no statistically significant difference with regards to complication numbers between the treatment arms.
Conclusions: Administering ketorolac at the time of ureteroscopy is associated with a 37% reduction in total narcotic requirement use for patients and is an independent predictor of decreased peri‐operative narcotic needs. A one‐time dose of ketorolac was not associated with an increase in complications for patients undergoing routine ureteroscopy for nephrolithiasis. These findings show that intra‐operative use of ketorolac effectively reduces narcotic requirements and should be considered independently or as part of a multimodal pain control protocol, unless otherwise contraindicated.
Which Endoscopic Methods in Prepubertal Patients with 10‐20 mm Bladder Stones: Transurethral Cystolithotripsy or Percutaneous Cystolithotripsy?
MM Piskin, MS Özkent, YE Goger, MT Kilinc, MS Sönmez
Konya City Hospital
Introduction & Objective: Bladder stones smaller than 10 mm usually treated with TUC and stones greater than 20 mm treated with PCC or open surgery. But, there is no clear consensus on which endoscopic method should be applied for 10‐20 mm stones. In this retrospective study, we aimed to evaluate the efficacy and safety of TUC and PCC in prepubertal pediatric patients with 10‐20 mm bladder stones.
Methods: The files of patients under 12 years' age who admitted our clinic for bladder stones from January 2007 to January 2021 were reviewed retrospectively. Inclusion criteria were patients who under 12 years' age with 10‐20 mm bladder stones, and performed endoscopic surgery (TUC or PCC). The patients were divided into two groups (Group 1: PCC Group and Group 2: TUC Group) and collected data (preoperative, intraoperative and postoperative characteristics) were compared between the Groups.
Results: This present study was enrolled 52 patients (21 patients in Group 1 and 31 patients in Group 2). The mean age of the patients was 4.7 ± 3.1 (Group 1: 4.7 ± 3.6; Group 2: 4.7 ± 3.2) years. The mean ages of the groups were similar (p: 0.978). The mean stone size was 15.8 ± 3.5 in Group 1, and 12.3 ± 2.8 mm in Group 2. It was higher in the PCC Group than TUC Group (p < 0.001). The operative time was 36.4 ± 12.9 min in Group 1, and 43.5 ± 16.7 min in Group 2. The operative time lower in Group 1 than Group 2 but there was no difference statistically between groups (p: 0.108). We achieved to SFR all of the patients in Group 1, but this were 30 patients (96.8%) in Group 2. There was no statistical difference between the SFR (p: 0.645). Complications were observed in four (7.7%) cases. One patient was in Group 1 and three patients in Group 2. There was no difference for complication rates between groups (p: 0.465).
Conclusions: The endoscopic surgeries have become almost a routine method in the treatment of bladder stones. However, there is no consensus about which endoscopic method is more effective. Percutaneous cystolithotripsy provides shorter operation time in larger stones. Therefore, it can achieve SFR with a shorter operative time in increased stone size. However, both transurethral cystolithotripsy and percutaneous cystolithotripsy have taken their place as safe methods in the treatment of prepubertal patients with moderate bladder stones.
The Impact Of Metabolic Syndrome Components On Urinary Parameters and Risk of Stone Formation
JN Bamberger, DC Rosen, JA Khusid, E Kaplan‐Marans, B Gallante, A Kapoor, I Paranjpe, D Atashokhan, WM Atallah, AS Sadiq, M Gupta
Icahn School of Medicine at Mount Sinai
Introduction & Objective: To investigate the relationship between metabolic syndrome (MS) and urinary abnormalities in stone‐forming patients. Additionally, to delineate whether severity of urinary derangements is impacted by the number of co‐occurring MS components.
Methods: Stone‐forming patients who underwent initial metabolic workup prior to medical intervention at a comprehensive stone clinic were retrospectively reviewed and included in the study. Patients were given a six point (0‐5) Metabolic Syndrome Severity Score (MSSS) based on the number of co‐occurring MS components and split into six respective groups. Baseline clinical characteristics and metabolic profiles were compared between groups.
Results: Baseline and metabolic characteristics of the 495 patients included in the study are presented in Table 1. Several significant metabolic differences were noted, including a downward trend in median urinary pH (p < 0.001) and an upward trend in median urinary SSUA (p<0.001) across groups as MSSS increased. Multivariate analysis demonstrated an independent association between higher MSSS and increasing number of urinary abnormalities (Table 2). A second multivariate analysis revealed that all MS components except hyperlipidemia were independently associated with low urinary pH. Additionally, obesity was independently associated with the greatest number of urinary abnormalities and had the strongest association with hyperuricosuria.
Conclusions: Prior research has attributed the strong association of nephrolithiasis and MS to high prevalence of UA nephrolithiasis and low urinary pH. Our findings indicate that all MS components with the exception of hyperlipidemia were independently associated with low urinary pH suggesting a mechanism independent from insulin resistance.
Evaluating the use of a patient‐specific hydrogel model to measure the effects of various experimental conditions on renal pelvis pressure during ureteroscopy
R Melnyk, D Foster, A Ghazi
University of Rochester Medical Center Department of Urology
Introduction & Objective: During ureteroscopy, the use of high irrigation pressures to optimize visualization must be balanced with the risk of systemic infection due to pyelovenous backflow (PVB) (estimated to occur at 30 mmHg). Previous clinical studies have examined the effects of various operative parameters and use of ureteral access sheaths (UAS) on the renal pelvis pressure (RPP), but there are currently no in vitro simulation models that can quantitatively measure all of these conditions. We evaluated if an anatomical hydrogel kidney model previously developed for patient‐specific endourology simulation can mimic these operative parameters.
Methods: A ureteroscope (Olympus URF‐P6) was inserted through the ureter into the pelvis of a model derived from a patient scan. RPP was continuously measured in the upper and lower calyx using a pressure wave monitor (Figure 1). A compression band simulated the uteropelvic junction and RPP was calibrated to replicate physiological conditions (40 mmHg RPP under 150 mmHg irrigation) between each test. Pressure changes in the upper and lower calyx both with and without a 11/13 Fr UAS were measured under 150, 200, and 300 mmHg irrigation pressures.
Results: Introduction of the sheath lowered RPP from 36 to 5 mmHg (‐86% reduction) and 34 to 3 mmHg (‐91%), in the upper and lower poles respectively at an irrigation pressure of 150 mmHg. At 200 mmHg of irrigation, upper and lower pole pressures dropped from 42 to 12.5 mmHg (‐70%) and 42 to 9.5 mmHg (‐77%). At an irrigation pressure of 300 mmHg, upper and lower pole pressures dropped from 38 to 16 mmHg (‐58%) and 50 to 15 (‐70%) mmHg. All pressures remained under 30 mmHg when using a sheath decreasing the risk of PVB.
Conclusions: These results are consistent with previous work that UAS use reduces RPP. Future investigation will explore how variation in patient anatomy effects fluid flow and pressures under various experimental conditions.
Upper Pole Prone PCNL is Safe and Efficacious for Horseshoe Kidneys with High Volume Nephrolithiasis
Dt Rubio, JA Abraham
National Kidney and Transplant Institute
Introduction & Objective: Our preferred approach to nephrolithiasis among horseshoe kidneys (HK) is an upper pole prone PCNL. This helps us overcome the alterations in renal vasculature and calyceal malrotation which can make percutaneous access difficult and even treacherous. We summarized our experience on these patients with high volume stones.
Methods: A chart review was done on all patients who underwent PCNL in our institution from 2010‐2019. Those with HK were analyzed. The patient (age, gender) and stone demographics (Guy's stone score, laterality), intraoperative parameters such as number of access sites (single vs. multiple), operative time (OT), and estimated blood loss (EBL), length of hospital stay (LOS) were analyzed. The primary endpoints were stone‐free and complication rates.
Results: During the study period, a total of 2,354 PCNLs were performed of which 42 were done for HK. The mean age was41 ± 6.6 (R = 22‐61) with a male to female ratio of 3:1. Twenty (48%) and 22 (52%) were left and right‐sided, respectively. The Guy Stone Scores were 3 and 4 in 12 (30%) and 30 (70%) patients, respectively. Mean stone diameter was 3.6 ± 0.6 cms. (R = 2.3‐5.5). Thirty‐eight (91%) needed a single upper pole access while four (9%) patients required additional tracts. The mean OT was 137.8 ± 28.1 mins. (R = 90‐210), EBL was 358 ± 278.4 cc (R = 200‐700) and LOS was 3.5 ± 0.94 days (R = 2‐7). The stone‐free rate was 95%. According to the Clavien‐Dindo classification, three (7%) had fever: Grade I, and five (12%) required transfusion: Grade II. There was no mortality.
Conclusions: Upper pole prone PCNL provides a high stone‐free and low complication rates among patients with nephrolithiasis in horseshoe kidneys.
Beware the bolus size: Understanding intrarenal pressure during ureteroscopic fluid administration
J Lazarus, L Kaestner, P Wisniewski, S Yekani
Introduction & Objective: The aim of this study is to evaluate how bolus administration of irrigant fluid impacts intrarenal pressure (IRP) during flexible ureteroscopy (FURS). We also investigated how ureteral access sheaths (UAS) of varying sizes mitigates elevated IRP.
Methods: Using a porcine cadaveric model, IRP is evaluated using an arterial invasive pressure measurement system. Given a fluid column height (driving force) of 80cm H2O, and varying bolus administration (1, 2, 3, 5, 10ml), IRP was studied with and without a UAS. An IRP of <40mm Hg was considered the cut off for “safe” FURS. The drainage (flow) capacity of UAS was also evaluated. At varying fluid column heights, three sizes of UAS were used 10/12 Fr, 11/13 Fr and 12/14 Fr, all 36cm long.
Results: Bolus administration with a UAS of <5ml with a starting fluid column height of 80cm H2O is “safe” (<40mm Hg). In contrast, where no UAS is used, bolus sizes as small as 2ml produce “unsafe” peak pressures.
The flow (drainage capacity) through a 10/12 Fr UAS is poor but improves greatly with larger UAS.
Conclusions: This study suggests that 10/12 Fr UAS may be inadequate to maintain drainage from the kidney at acceptable pressures. Bolus fluid administration produces “unsafe” (>40mm Hg) elevated IRP in the absence of a UAS. When a UAS is used, a fluid bolus of <5ml is likely “safe”.
Can Smart Technology Improve Adherence to Fluid Management and Urine Output in Kidney Stone Patients? A Prospective Randomized Study
HC Wright, L Alshara, H DiGennaro, Y El Kassis, J Li, M Monga, J Calle, S Sivalingam
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA.
Introduction & Objective: Implementation of Smart technology (ST) can enhance chronic disease management, yet little is known about the benefits of ST on kidney stone prevention. Our aim was to prospectively evaluate the impact of two different ST modalities on adherence rates and urine output (UOP) in patients with nephrolithiasis.
Methods: Kidney stone patients with low UOP (< 2.5L/24 hours) were randomized into three intervention groups: 1) standard dietary/medical counseling alone (control), 2) control + smartphone fluid management application (app), and 3) control + smart water bottle (bottle). Demographics, adherence rates, kidney stone events, and 24‐hour UOP were collected and analyzed at baseline, 3‐6 months, and 12 months. Enrollment parameters and ST information are shown in Figure 1.
Results: We randomized 111 patients (37 per group). There was no difference in baseline demographics or kidney stone history between groups (Table 1). Twenty (55%), 8 (26%), and 10 (33%) patients completed the 12‐month follow‐up in the control, app, and bottle groups respectively. Control group patients were the most likely to adhere to follow‐up (p = 0.004). Overall mean UOP increased by 0.4L in each group (p < 0.05), with no difference in mean baseline 24 hour UOP (1.6L) and 12 month 24 hour UOP (2.0 L) between groups (p > 0.05). Twenty‐nine percent of patients achieved a daily UOP goal of >2.5L across the treatment groups (p < 0.001, Table 2).
Conclusions: In this prospective study, 24 hour UOP improved across all groups compared to baseline, although adherence to follow up remained low. Notably, the use of ST did not further augment UOP, underscoring the importance of dietary/medical counseling for kidney stone prevention.
Tubeless ureterorenoscopy. Our experience using 120‐W laser and dusting technique. Postoperative pain, complications and readmissions
G Verhovsky, M Haifler, E Gnessin, I Leotsakos, M Duvdevani, YI Siegel, A Zisman, IM Sabler
Shamir (Asaf HaRofeh) MC
Introduction & Objective: Both double J stent (DJS) and ureter catheter (UC) drainage represent routine practice following ureterorenoscopy. In selected situations tubeless (T) approach is possible and safe. In tubeless cases we use sheathless dusting technique with Lumenis® MOSES Pulse™120H Holmium: YAG laser. We evaluated these three drainage subgroups, and compared postoperative complications, readmissions and pain.
Methods: Retrospective database of 269 consecutive patients that underwent primary ureterorenoscopy for treatment of upper urinary tract stones between October 2018 and August 2019. The cohort was divided according to post‐operative drainage as: T, UC and DJS. The choice as whether to leave or nor to leave drainage was left to the surgeon. Demographic parameters, stone location, number and burden, hydronephrosis grade, postoperative complications (fever, acute renal failure, obstruction of the upper urinary tract by stone street) were assigned, pain had been assessed by Visual Analog Scale (VAS) and use of analgesics by dose/case in each group.
Results: There were 70 (26%) T, 136 (50%) UC and 63 (24%) DJS cases. Patients that were drained with DJS had significantly higher stone burden, more severe obstruction and prolonged operative time. T and UC had same stone characteristics (table 1). Postoperative ER visits, readmissions, complications (table 1), VAS (table 2) and analgesic use (table 3) were significantly less in T group.
Conclusions: Tubeless approach is safe in selected cases. While DJS should be considered in complex cases, UC may be omitted since it does not appear to reduce immediate postoperative complications. Powerful laser dusting, may add to usefulness of postoperative drainage. Those fitted for tubeless procedure did better postoperatively in terms of analgesic use and complications, facilitating outpatient approach to upper urinary tract stones treatment and patient satisfaction.
The Cost of Convenience: Estimating the Environmental Impact of Single‐Use and Reusable Flexible Cystoscopes
K Koo, JS Winoker, S Patel, ZT Su, AM Potretzke, BR Matlaga
Mayo Clinic
Introduction & Objective: Flexible cystoscopy is one of the most common outpatient procedures performed in urology practices. Single‐use flexible cystoscopes may confer cost savings associated with reduced device reprocessing and repair. However, the environmental impact of disposable devices is not well‐characterized. This study aimed to compare the carbon footprint of single‐use (SU) and reusable flexible cystoscopes.
Methods: We analyzed the expected life cycle of SU (Ambu aScope 4 Cysto) and reusable (Olympus CYF‐V2) flexible cystoscopes. Performance data on cumulative procedures between repairs and before decommissioning were derived from a high‐volume multispecialty practice; to simulate practices with lower and higher volumes, we also estimated life cycle costs at 50% and 200% of case volumes. We estimated carbon expenditures per case using published data on endoscope manufacturing, energy consumption during reprocessing, and solid waste disposal
Results: Our fleet of 16 reusable cystoscopes in service for up to 135 months averaged 207 cases between repairs and 3920 cases per life cycle. Based on a manufacturing carbon footprint of 11.5 kg CO2/kg device for flexible endoscopes, the per‐case manufacturing cost was 1.84 kg CO2 for SU devices and 0.0001 kg CO2 for reusable devices (Table). The solid mass of SU and reusable devices was 0.16 and 0.57 kg, respectively. The energy consumption of device reprocessing using an automated endoscope reprocessor was 0.45 kg CO2. Per‐case costs of device repackaging and repair were 0.005 and 0.02 kg CO2. The total estimated per‐case carbon footprint of SU and reusable devices was 2.30 and 0.48 kg CO2, respectively. The estimated footprint of reusable devices at 50%–200% of case volume assumptions was not meaningfully different (0.47–0.51 kg CO2).
Conclusions: The environmental impact of reusable flexible cystoscopes is markedly less than SU cystoscopes over the life cycle of the devices, regardless of case volumes. The primary contributor to the per‐case carbon cost of reusable devices is energy consumption of reprocessing, which may be offset with renewable energy sources.
Comparative outcomes of urinary and serum parameters for patients with and without Obesity: 8‐year results from a dedicated stone clinic
D Bhatnagar, S Kunjur, M Ramachandra, P Cook, M Saraogi, R Geraghty, A Pietropaolo, BK Somani
University Hospital Southampton, UK
Introduction & Objective: The incidence and prevalence of both kidney stone disease (KSD) and obesity is increasing. The relationship between KSD and obesity has been widely studied, with a potential link between the two. We wanted to look at comparative outcomes of urinary and serum parameters for patients with and without Obesity
Methods: Data was analysed for all high‐risk patients who underwent metabolic stone screening between March 2012‐Jan 2020. Three independent non‐medical personnel not involved in treating these patients transcribed the data. Serum measurements of sodium, potassium, creatinine, bicarbonate, chloride, corrected calcium, magnesium, inorganic phosphate, urate and PTH were done. 24‐hour urinary and random urinary parameters were also measured. The eligible patients were divided into two groups depending on the absence (group 1) or presence (group 2) of Obesity.
Results: A total of 697 patients were identified, of which 55% were in group 1. The mean age and BMI were higher for group 2. On comparing the urinary parameters, the oxalate, citrate and sodium levels were significantly high; urate and urinary pH values were significantly low for group 2. On comparing the serum parameters, the magnesium values were significantly high; calcium and PTH was significantly low in group 1.
Conclusions: Based on our data, metabolic screening for patients with obesity is a good strategy with a reasonable yield of abnormal urinary and serum parameters, which can help target tailored management in these patients. Urine pH was low in obese group and underlies the importance of assessing this parameter in patients with stone disease.
Does the Urologist or Technologist Have More Influence on SWL Treatment Outcomes?
RG Seltzer, KJ Hamawy, BD Hamilton
Translational Analytics and Statistics
Introduction & Objective: Successful Shockwave Lithotripsy (SWL) depends on numerous elements, ranging from patient and stone characteristics, delivery of the treatment, patient positioning, and physical properties of the shock wave. Quantifying the impact that the physician and technologist have on outcomes can direct quality improvement efforts. The International Stone Registry (ISR) contains almost 300,000 SWL treatments with overlapping physician‐technologist pairings. This dynamic of multiple physicians treating with the same technologist and multiple technologists treating with the same physician offers an excellent opportunity to parse out the influence the physician and technologist have on patient outcomes.
Methods: A Pairwise Intraclass Correlation Coefficient (PICC) variance components analysis estimated the variance that physician and technologist have on stone free rate. A second PICC was run to include control variables (stone size and location, patient BMI, anesthesia type, total shocks delivered, mean and maximum power level used, and total x‐ray time). A total of 3,640 SWL, renal treatment records with outcomes were analyzed from the ISR from January 2018 through June 2019.
Results: There were 281 unique physician‐technologist pairs, ranging in treatment counts from 1 to 269. The variance components analysis revealed that 19.76% of the variance in outcomes is due to the physician, whereas 1.85% of the outcomes are due to technologist. This pattern holds up with the inclusion of control variables, with urologist accounting for 21.7% of the variance in outcomes and technologist accounting for 2.2% of the variance in outcomes.
Conclusions: Physicians have a much greater impact on stone free rate compared to the technologist. This likely results from factors controlled only by the physician, such as patient selection. Other factors, such as delivery of treatment parameters (shock rate and power level) can be influenced by both the physician and the technologist. The physician may direct the technologist to deliver a specific shock protocol or the physician will grant autonomy to the technologist to choose a shock protocol. The results indicate that while the technologist may sometimes select shock protocols and is actively involved in coupling the patient and positioning the stone in the shockwave focal zone, these elements either do not vary much across technologists or they have only a relatively small impact on outcomes compared to physician‐only elements.
The Contribution of Ascorbic Acid to Urinary Oxalate in Mouse Model
J Crivelli, K Wood, Z Burns, R Holmes, DG Assimos, J Knight
The University of Alabama
Introduction & Objective: Increased urinary oxalate is a risk factor for kidney stone disease. Ascorbic acid (AA) may contribute up to 50% to endogenous oxalate synthesis. The factors that influence the breakdown of AA to urinary oxalate are not well known. The Gulo‐/‐ mouse does not synthesize ascorbic acid and thus, like humans, must obtain AA from the diet. Our objective was to evaluate the contribution of AA to the endogenous oxalate pool in this mouse model.
Methods:Gulo‐/‐ mice (5M, 5F), 12 weeks old, were single housed in metabolic cages and 3 consecutive 24‐hour baseline urines were collected. They were given a purified ultra‐low oxalate diet to negate the contribution of dietary oxalate to urinary oxalate excretion. During baseline collections, water was supplemented with 330 mg/L AA. Following baseline urine collections, Gulo‐/‐ animals were deprived of dietary AA for 5 weeks to reduce body stores. Three 24‐hour urines were then collected. The mice were intravenously infused via a catheter implanted in the jugular vein for 8 days with 18 μmol/kg/h 13C6‐AA. On the last 3 days of infusion, 24‐hour urine specimens and tail blood were collected for measurement of oxalate and AA in both urine and plasma. Contribution of AA to urinary oxalate excretion is determined by the formula: [Urinary 13C2‐oxalate % mole enrichment / Plasma 13C6‐AA % mole enrichment] X 100.
Results: Urinary oxalate excretion was similar at baseline between wild type and Gulo‐/‐ animals, and between male and female mice. Following 5 weeks of dietary AA deprivation, urinary oxalate excretion decreased 44% and 65% in a male and female Gulo‐/‐ animal, respectively. The infusion studies demonstrate that AA turnover contributed 29 ± 2% to the urinary oxalate pool (Table 1).
Conclusions: The Gulo‐/‐ mouse is a model that can be used to increase our knowledge of the contribution of AA breakdown to urinary oxalate excretion. Understanding this pathway may provide future therapeutic targets for oxalate reduction.
SWL Focus ‐ Does sizes matter?
J Veser, V Jahrreiss, C Seitz
Introduction & Objective: Together with the introduction of the piezoelectric shockwave generators, the Wolf Piezolith 3000 lithotriptor implemented three adjustable focus sizes, small (2,1mm), medium (3,7mm) and large (8,1mm). Even if variation of the focus size in SWL‐treatment is not a novelty, there has not been a randomized controlled study comparing the effect of different focus sizes on the treatment of kidney and ureter stones so far. The aim of this study was to analyze, if there is a difference in efficacy and pain levels between different focus sizes.
Methods: In this randomized, prospective, double‐blinded trial we included patients undergoing SWL with kidney stones between 5‐15 mm and ureter stones ≤10mm, with no prior treatment of the stone. A standardized SWL‐treatment with either focus 1 (small) or focus 3 (large) was performed, during which we regularly assessed the pain level with the visual analog scale (VAS). We then reevaluated the treatment success with sonography and/or KUB after one day (ureteral stones) or 14 days (kidney stones) and did a second SWL if there was a residual fragment ( >4mm kidney stones). After 4 weeks we assessed the stone free rate with an abdominal CT‐Scan. This is a preliminary evaluation after 134 of 150 planned patients.
Results: After exclusion of 8 patients (lost to follow up), a total of 126 patients were analysed so far, within 65 patients with focus 1 (small) and 61 with focus 3 (large). A stone free rate of 77% in the small focus group vs. 72% in the large focus was achieved (p = 0,713). With focus 1 the stone free status was reached in a single procedure in 48% of the cases, with focus 3 in 44% (p = 0,649). In a total of 204 procedures, an additional pain medication (on demand or VAS ≥8) was applied in 33% of the patients with focus 1 and in 25% of those with focus 3 (p = 0,258).
Conclusions: This preliminary data suggests, that there is no association between the focus size of the shock wave and the stone free rate. We observed a stone free status in fewer procedures within the smaller focus group, however the rate of higher pain levels (VAS > = 8), associated with a need of further pain medication, was also elevated in this group. Final results can be drawn after inclusion of the total study population.
Failure to rescue? Ambulatory healthcare utilization after ureteroscopy for stone disease in a surgical collaborative
J DiBianco, R Navarrete, B Conrado, S Daignault‐Newton, CA Dauw, KR Ghani, f Urological Surgery Improvement Collaborative
Department of Urology, University of Michigan
Introduction & Objective: We assessed postoperative healthcare utilization after ureteroscopy (URS) for nephrolithiasis to determine how ambulatory encounters relate to unplanned hospital visits. Using the Michigan Urological Surgery Improvement Collaborative (MUSIC) data we aimed to quantify and categorize the nature of ambulatory encounters and investigate pathways for preventing emergency department (ED) visits.
Methods: Patients undergoing URS by practices with ≥10 cases in the MUSIC clinical registry in 2019 were stratified by outcome (ED visit, office visit and no visits). One patient from each strata per practice was randomly selected for chart review. Data elements and classification were defined a priori. Communication between the office and patient prior to an unplanned visit was labeled an encounter. We examined the nature of complaints, timing and office action taken per encounter. Encounter intensity was categorized as low, moderate or high based on nursing or physician decision‐making and action needed.
Results: In 2019 there were 4526 URS cases with a 30‐day ED visit rate of 6.4% in MUSIC. 59 patients underwent chart review. Fig. 1 demonstrates the number of encounters after surgery and their relationship to unplanned healthcare. In total, 36 (61%) patients had some form of care after URS. 23 (39%) patients generated at least one encounter, with a total of 39 encounters. Mean time to first encounter was 3.7 and 11.9 days for stented and unstented patients, respectively. 15% of patients had an ED visit without a prior ambulatory encounter. In contrast, 14% of patients had an ED visit despite ambulatory encounters. No patients required hospitalization. Nursing education was the most common office action (53%) (Table 1). Stented patients had more moderate/high intensity encounters (45.9%) compared to unstented patients (13.3%).
Conclusions: Post‐operative ambulatory care utilization after URS poses a high burden on the healthcare system. Stented patients had higher intensity ambulatory encounters than unstented patients. Despite nursing or physician level input, some patients were unable to be rescued from a modifiable ED visit.
Pre‐operative stone volume measurement program (qSAS) is best predictor of percutaneous nephrolithotomy (PCNL) operative time and stone free rate
M Meagher, T Chiou, R Sur, SK Bechis
University of California ‐ San Diego, Department of Urology
Introduction & Objective: Linear dimensions have historically been used to measure stone burden. However, emerging data suggests that volume may offer advantages in predicting outcomes. We hypothesize that for larger stones with more complex anatomical shapes, volume is more accurate than linear dimension in predicting PCNL outcomes.
Methods: Single institution retrospective analysis of patients treated via standard PCNL from 7/2017‐1/2020 was performed. Pre‐operative CT scan images were analyzed manually to calculate stone diameter and by using the quantitative Stone Analysis Software (qSAS) to measure total stone volume (SV) and maximum diameter (MD). Primary outcome was post‐operative stone‐free rate (SFR) (logistic and ordinal regression). Secondary outcome was operative time (linear regression). Potential variables associated with the outcomes of interest (univariate regression) were compared using OR or R‐values, with p < 0.1 eligible for inclusion in the multivariate analysis.
Results: 324 patients were analyzed. Average age was 59 years with average BMI of 28.7 kg/m2. 23.1% and 11.7% of patients had complete and partial staghorn morphology, respectively, with a mean pre‐operative SV of 1,568mm3 and mean MD of 2.3cm. Logistic regression revealed staghorn morphology (OR = 3.98, p = 0.031), increasing SV (OR = 1.11, p = 0.007), and higher GUYS score (OR = 1.68, p = 0.031) to be independently associated with a lower likelihood of clinical stone free status (Table 1A). Ordinal regression found that pre‐operative SV (pseudo‐ R2 = 0.791, p < 0.001) better predicted post‐operative SFR when compared to urologist (pseudo‐R2 = 0.644, p < 0.001) and software (pseudo‐R2 = 0.68, p < 0.001) measured MD. Higher average Hounsfield Units (B = 0.03, p = 0.047), larger pre‐operative SV (B = 0.17, p = 0.006), and partial staghorn morphology (B = 23.05, p < 0.001) were independently associated with longer operating time (Table 1B).
Conclusions: Software‐calculated total stone volume more accurately predicts clinical stone free status post‐PCNL compared to maximum linear dimension. SV also aids in predicting OR times and may add value for presurgical planning. Calculation of stone volume in addition to linear dimension should be considered to more precisely counsel patients in efficacy of PCNL.
Is percutaneous drainage a necessary exit strategy after supine percutaneous nephrolithotomy (PCNL)? Trends from a contemporary series
Z Sheng, R Warner, G Caddeo
University Hospitals of Derby and Burton NHS Foundation Trust
Introduction & Objective: Exit strategies after percutaneous nephrolithotomy (PCNL) may include internal or external urinary drainage. The choice varies according to stone and patient characteristics, intraoperative complications and the surgeon's preference. We assessed whether percutaneous drainage offered any advantage over ureteric drainage in a large supine PCNL series.
Methods: We reviewed all supine PCNLs performed by a single surgeon between January 2014 and December 2020. Patient factors including age and BMI, stone complexity and the exit strategy were collected. Outcomes included length of stay, operating duration, inpatient complications, and postoperative tube indwelling time. Statistical analysis was performed using the Mann‐Whitney U test.
Results: In total 104 supine PCNLs were reviewed. A ureteric stent was placed in 55 cases (53%), retrograde ureteric catheter in 6 (6%), percutaneous nephrostomy in 19 (18%), antegrade ureteric catheter in 9 (9%) and combination of nephrostomy and stent/ureteric catheter in 15 (14%). Median indwelling time for stents was 14 days and nephrostomy 7 days. The use of nephrostomy correlated with longer operative time (median 125 minutes, p < 0.0001), higher stone complexity (median Guy's stone score ≥2, p = 0.005) and longer postoperative stay (median 2 days, p < 0.0001). When percutaneous drainage was used, no patients required an emergency second look or additional procedures. There was one Clavien‐Dindo Grade complication greater than 2. No transfusions were required.
Conclusions: Ureteric stenting was the preferred exit strategy following uncomplicated PCNL. A nephrostomy or percutaneous ureteric catheter is typically left post‐procedure to maintain the tract enabling emergency re‐entry, however, this was not required in our series. When postoperative drainage is the only indication for a percutaneous tube, placing a ureteric stent may be sufficient.
Muscle Activation During Simulated Flexible Ureteroscopy: Effects of Surgeon Position and Scope Type
G Gheordunescu, K O'Laughlin, A Sun, J Fulla, N Kachroo, HC Wright, S De
Case Western Reserve University School of Medicine, Cleveland, OH, USA
Introduction & Objective: Ergonomics in flexible ureteroscopy is poorly understood. We sought to quantify the effects of ureteroscope type (disposable vs. non‐disposable) and surgeon position (sitting vs. standing) on muscle activation as measured by electromyography (EMG) during ureteroscopy in an endourology box‐trainer model and kidney phantom.
Methods: For this exploratory study, EMG was used to quantify muscle activation of three endourologists during several ureteroscopic tasks. “Real world” operative settings were re‐created: a cystoscopy table with surgical drapes and an endoscopic video tower were used and subjects wore fitted lead aprons in an operating room suite. Surface EMG electrodes (ADInstruments, Colorado Springs, CO) were placed on the scope‐holding side of the following muscle groups: thenar, forearm flexor, forearm extensor, biceps, triceps, deltoid, and trapezius. Subjects completed each trial while using a disposable and non‐disposable scope, and while sitting and standing. Each subject performed an identical set of tasks in a phantom silicone kidney and ureteroscopy box trainer used to mimic the procedural components of dusting, basketing, and navigating a renal collecting system. Raw continuous EMG data for each task was processed and normalized as a percent of each subject's maximum voluntary contraction (MVC) to allow comparison. The EMG activity of all subjects and tasks were compiled (Figure 1). Tasks were analyzed individually and then in aggregate because muscle activation trends were similar and a full set of tasks better represented a complete ureteroscopy procedure.
Results: The forearm extensor muscle had higher activation with the heavier non‐disposable scope vs. the disposable scope. There was increased activation of the trapezius muscle during sitting vs. standing. The forearm extensor was the most heavily utilized muscle regardless of posture or scope type.
Conclusions: Our preliminary data show differences in muscle activation based on both surgical posture and type of scope used. This highlights the need for more extensive EMG studies to identify techniques and equipment to optimize ergonomics and potentially minimize repetitive use injury during flexible ureteroscopy.
Management of nephrolithiasis with a large ureteral access sheath is not associated with increased risk of surgical complications and stricture formation on long term follow up
K Breen, C Driscoll, A Khambati, K Perry, RB Nadler
Northwestern Memorial Hospital
Introduction & Objective: Ureteral access sheaths (UAS) are commonly used in the management of nephrolithiasis. There is limited data on long term complications associated with UAS, especially with the large 14/16 F sheath. We evaluated and compared surgical complications and long term outcomes associated with UAS use between the smaller (10‐14 F) and the large (14/16 F) UAS sheaths.
Methods: We identified 355 patients who underwent ureteroscopy for proximal or renal stones with a UAS between 2010 and 2015 at our institution. All patients had an initial 3 month follow‐up CT scan. Patient demographic and clinical information including comorbidities, stone location and size, pre‐operative and post‐operative JJ stent status, intraoperative and postoperative surgical complications, hospital admission and 90‐day readmission rates, and post‐operative hydronephrosis and strictures were assessed on most recent long term follow up.
Results: In total, 335 patients were included, 170 men (50.7%) and 165 (49.3%) women. Median age was 55. The stones were larger in the 14/16 UAS group (10 vs 12mm, p < 0.001). There was no significant difference in the rate of intraoperative (3.8% vs 2.8% p = 0.24) and post‐operative (6.3% vs 3.9%, p = 0.84) complications, hospital admissions (14.6% vs 16.8%, p = 0.58), readmissions (9.5% vs 6.1%, p = 0.24) and stone‐free rates (79.6% vs 75.8%, p = 0.40) between the 10‐14 F and 14/16 UAS groups. In total, 3 (0.8%) strictures were diagnosed, with only 1 in the 14/16 UAS group. No difference was detected in total complications based on sheath size on logistic regression analysis. Mean follow‐up was 68 months and imaging at the time of last follow up did not demonstrate any late stricture formation.
Conclusions: The risk of surgical complications and stricture formation associated with UAS is low. The use of a 14/16 sheath allows treatment of large renal stones safely without an increased risk of complications including late stricture formation at 5 year follow up.
Moderated Poster Session 12: Imaging II
Ultrasound to reposition and facilitate passage of distal ureteral stones
JD Harper, J Thiel, P Samson, P Sunaryo, RM Sweet, I Metzler, L Anderson, R Kessler, B Dunmire, C Popchoi, R Managuli, B Cunitz, B Burke, Z Liu, AD Maxwell, M Sorensen, M Hall, H Wessells, MR Bailey
University of Washington
Introduction & Objective: The feasibility of ultrasonic propulsion and burst wave lithotripsy (BWL) to non‐invasively reposition distal ureteral stones to facilitate passage and relieve pain was tested.
Methods: Patients presenting to the kidney stone clinic or emergency department (ED) with a distal ureteral stone were recruited after standard of care pain management. To attempt to move the stone, 10 subjects underwent ultrasonic propulsion (lower amplitude, longer duration bursts) alone, and 10 subjects also received intermittent BWL (higher amplitude, shorter duration bursts). All participants were awake without anesthesia and underwent:· a screening ultrasound to ensure the stone was visible· a pain assessment pre‐ and post‐procedure · contact once a week for three weeks to assess for adverse events· follow‐up imaging and chart review within 12 weeks Subjects were sub‐categorized based on whether their stone was acute or chronic (≤ 10 days or >10 days from their ED visit, respectively).
Results: Demographic data and effectiveness outcomes are presented in Tables 1 and 2. Overall, 93% of acute stones passed in an average of 3.6 days postprocedure. There was no control group, but Table 2 includes published passage rates and times for potentially similar untreated groups as reference. Stone motion was observed in 16 of 20 cases, including a stone pushed into the bladder, ureteral jets were observed following propulsion bursts in 9 of 20 cases and fragmentation was observed in 3 of 10 BWL cases. Pain reduced post‐procedure in 10 of 20 subjects, while pain increased in only one subject; although, the average score was low prior to treatment, and the average decrease was statistically significant (p = 0.0215). Adverse events were limited to slight reddening of the skin (N = 6), hematuria on only the initial urination post‐procedure (BWL only, N = 3), and a mild sensation, akin to a pinprick, on fewer than 10 of 620 propulsion bursts among 3 subjects.
Conclusions: This feasibility study showed the potential for facilitating stone passage of distal ureteral stones and relieving pain with ultrasonic propulsion and BWL.
Narrow band imaging cystoscopy in non‐muscle invasive bladder cancer – Still “motive and opportunity” after 6 years of follow‐up?
BF Geavlete, C Moldoveanu, C Ene, C Bulai, A Ene, PA Geavlete
“Saint John” Emergency Clinical Hospital, Department of Urology
Introduction & Objective: The trial was aimed to determine the impact of narrow band imaging (NBI) guided transurethral resection of bladder tumors (TURBT) by comparison to the standard white light (WL) cystoscopy and resection concerning the non‐muscle invasive bladder cancer (NMIBC) long‐term recurrence rates.
Methods: The study included 190 NMIBC cases prospectively enrolled and equally randomized in the 2 series. Patients of the study arm benefitted from both WL and NBI cystoscopy and TURBT, while solely the standard diagnostic and therapeutic approach was applied in the control arm. The inclusion criteria were represented by positive urinary cytology and/or abdominal ultrasound/contrast CT. Chemotherapeutic/BCG instillations were performed in accordance with the NMIBC recurrence and progression EORTC risk tables' classification. The follow‐up protocol was extended for 6 years and scheduled as resulting from the risk categories.
Results: The overall NMIBC (96.2% vs. 87.2%) and CIS (100% vs. 66.7%) patients' detection rates were significantly improved for NBI when compared to WL. On a tumors' related basis, NBI cystoscopy emphasized significantly superior detection rates regarding the CIS (95.2% vs. 61.9%), pTa (93.9% vs. 85.2%) and overall NMIBC (94.8% vs. 83.9%) lesions. Additional tumors were diagnosed by NBI in a significant proportion of CIS (55.5% vs. 11.1%), pTa (26.5% vs. 10.2%), pT1 (30% vs. 10%) and overall NMIBC (30.8% vs. 10.3%) patients. The postoperative intravesical instillation treatment was significantly improved due to NBI additional findings leading to risk category modifications (16.7% versus 5.1%). The NBI series was characterized by a statistically significant reduction in the cumulated recurrence rates at 1 (16.2% vs. 28.9%), 2 (22.9% vs. 39.5%), 3 (27% vs. 44.7%), 4 (29.7% vs. 47.4%), 5 (30.3% vs. 49.8%) and 6 (32.1% vs. 51.9%) years by comparison to the WL‐TURBT group. Differences between study arms gradually lowered and lost statistical significance after 2 years.
Conclusions: The NBI assisted TURBT emphasized a statistically significant improvement in terms of patients' and tumors' detection rates as well as additionally found lesions and superior postoperative instillation treatment. The NBI endoscopic assessment provided a significant advantage regarding the NMIBC long‐term oncologic outcome, while differences between methods decreased in time and eventually lost statistical significance.
A Multi‐class Classification Machine Learning Model of In Vivo Urinary Stone Compositions Using Dual‐energy CT and Radiomics
K Wang, X Jin, D Ye, Y Chen, L Cai, J Sun, L Xiang, H Li
West China Hospital, Sichuan University
Introduction & Objective: To improve the diagnostic accuracy of dual‐energy computed tomography (DECT) in discriminating urinary stone compositions in vivo.
Methods: Patients with suspected urolithiasis who received a preoperative DECT and subsequent endoscopic stone extraction in our institution between September 2017 and August 2020 were enrolled. Using ITK‐SNAP software to perform three‐dimensional radiomics mask labels, and using python's pyradiomics library for radiomics features extraction. The dual‐energy features were evaluated under two modes: Monoenergetic mode and Rho/Z Maps mode. Ten clinical features, four dual‐energy features, and 130 radiomics features were recorded for analysis. An ensemble learning model composed of logistic regression, support vector machine and random forest machine learning model was exploited for the multi‐class classification of urinary stone compositions. The model performance was evaluated by leave‐one‐out cross‐validation. ROC curves, PR curves, and AUC were calculated for the evaluation.
Results: A total of 119 patients with 168 stones were included in the final analysis. The compositions of calculi include 119 calcium oxalate (CaOx), 29 calcium oxalate mixed carbon apatite (CaOx+CaP), 9 uric acid (UA), 5 struvite (STR), and 6 cystine (CYS). The AUC of ROC curves of the ensemble learning model for each composition are as follows: CaOx [0.907], CaOx+CaP [0.824], UA [0.963], STR [0.993], CYS [1.000].
Conclusions: DECT has the potential to become a one‐stop noninvasive examination for both detection of calculi and predicting their compositions based on radiomics and machine learning, which is beneficial for early medical management and treatment determination.
Simplified Biplanar (0°‐90°) Fluoroscopic Puncture Technique for Percutaneous Nephrolithotomy: The Learning Curve
BO Manzo, DD Cabrera, JE Torres, EE Lozada, E Flores, P Alarcon, C Morales, F Sepulveda
Hospital Regional de Alta Especialidad del Bajío
Introduction & Objective: The main limitation of all the current fluoroscopic approaches is a low precision in calculating the exact caliceal depth, and the exact place to puncture in the skin. Another disadvantage is the amount of fluoroscopic radiation used, especially with the “bull's eye” technique in which the surgeon's hand is mainly exposed to the radiation field.
Purpose: To evaluate the learning curve of the simplified fluoroscopic biplanar (0‐90o) puncture technique for percutaneous nephrolithotomy.
Methods: We prospectively evaluated patients with renal stones treated with percutaneous nephrolithotomy by a single institutiońs fellows employing the simplified bi‐planar (0‐ 90o) fluoroscopic puncture technique. The learning curve was assessed with the fluoroscopic screening time and the percutaneous renal puncture time. Data obtained were compared to a subset of patients operated by a senior surgeon.
Results: Eighty‐nine patients were included in the study. Forty patients were operated on by fellow‐ 1, thirty‐nine by fellow‐2, and 10 patients by the senior surgeon.
Demographic data of all patients between groups were homogeneous, with no difference in gender (p = 0.432), age (p = 0.92), stone volume (p = 0.78), puncture laterality (p = 0.755), and body mass index (p = 0.365). The mean puncture time was 7.5, 4, and 3.1 min for fellow‐1, fellow‐2, and expert, respectively. The mean fluoroscopic screening time for the puncture was 10, 11, and 5.1s for fellow‐1, fellow‐2, and the expert, respectively. In stone cases, both fellows needed to complete 10 procedures to match the senior surgeon in the mean puncture time (p = 0.046); meanwhile, the fluoroscopic screening time was equal even before completing 10 procedures.
Conclusions: This study suggests that with the simplified biplanar (0‐90o) puncture technique, the fluoroscopic screening time used in the learning process is brief. A novice fellow could require to complete ten cases to flatten the learning curve treating complex stone cases, and a flat learning curve is seen since the beginning when treating simple renal stones.
Role of peri‐calculus ureteral thickness on CT Scan to predict stone impaction at time of surgery. A Single center analysis
N Iqbal, A Hasan, J Rahim, S Imtiaz Ali, S Akhter, T Bhatty
PKLI, Lahore, Pakistan
Introduction & Objective: Impacted ureteral stones are thought to be associated with hypertrophy and edema of the ureteral mucosa, which might make endoscopic ureteral stone surgery challenging. Use of preoperative CT scan may predict significant ureteral stone impaction, and as such can help urologist for patient counseling of associated risks and outcomes of surgery.
Methods: We collected data on 93 patients who had a preoperative CT scan and had ureteroscopy (URS) for ureteral stones. Radiologists watched for the thickness while Surgeons were allowed to see only stone size, location, and hydronephrosis. Stones were deemed impacted at surgery if a guidewire could not pass or if contrast had difficulty passing proximal to the stone, or if stone was not moving on touching glide wire under vision also. We looked for association of intra‐operative findings to preoperative CT measurements of ureteral thickness on a coronal series directly above, around, and below the stone. Chi‐square was used for categorical variables and Annova test for continuous variables.
Results: Of the 93 patients, 31 subjects had an impacted ureteral stone at the time of surgery. Patients who had an intra‐operative finding of an impacted stone had significantly higher ureteral thickness above, around and below the stone area (all three p‐values <0.03) compared to non‐impacted ureteral stones.
Conclusions: Increased ureteral thickness as measured on CT coronal imaging above, around and below the calculus can be a useful predictive tool for impacted ureter stones. This can be helpful for surgical planning and patient counseling.
The efficacy and safety of radiation‐free retrograde intrarenal surgery
B Kim, J Chung, Y Ha, S Choi, J Lee, H Kim, T Kim, E Yoo, T Kwon
Department of Urology, School of Medicine, Kyungpook National University
Introduction & Objective: Retrograde intrarenal surgery (RIRS) has been commonly performed under the fluoroscopy guidance. Although fluoroscopy is necessary for safe and smooth procedure of RIRS, there is an increasing concern regarding the hazards of frequent radiation exposure to patients and surgeons. Thus, we established a technique for radiation‐free RIRS and retrospectively evaluated the efficacy and safety of radiation‐free RIRS for management of renal stone.
Methods: From January 2015 to December 2019, 462 patients who underwent RIRS for unilateral renal stone less than 2cm were enrolled in this study. The data was collected retrospectively and the patients were divided into two groups according to the usage of fluoroscopy during surgery. The patients' demographic data, operation time, hospital stay, complications, and stone‐free rate (SFR) were compared between fluoroscopy‐free and ‐usage groups.
Results: Of 462 patients, the initial consecutive 206 patients underwent RIRS under fluoroscopy guidance, and the other 256 consecutive patients underwent RIRS without fluoroscopy. The patients and stones characteristics were not statistically different between the two groups. Mean operation time was significantly shorter in fluoroscopy‐free group (103 ± 33.9 vs 110 ± 30.6 minutes, p = 0.022), while mean hospital stay (3.5 ± 2.0 vs 3.6 ± 2.5, p = 0.126), complication (18.4% vs 22.8%, p = 0.247) and stone‐free rate (85.2% vs 85.0%, p = 0.377) were not significantly different between both groups.
Conclusions: This study showed that there was no statically significant difference in stone‐free and complication rate after RIRS between fluoroscopy‐free and ‐usage groups. Radiation‐free RIRS can be safely and effectively performed with our established technique.
A Comparison of Radiation Use During Fluoroscopic Guided Extracorporeal Shockwave Lithotripsy and Ureteroscopy for Renal Stones
AS Amasyali, M Keheila, JD Belle, M Hajiha, DD Baldwin, G Martin
Loma Linda University, School of Medicine
Introduction & Objective: There are minimal data comparing fluoroscopy time between ureteroscopy (URS) and extracorporeal shockwave lithotripsy (SWL). One prior study showed no difference in fluoroscopy time between the two modalities. Over time, techniques to reduce fluoroscopy during URS have evolved. The purpose of this study was to compare the outcomes and fluoroscopy times between URS and SWL for renal stones in modern practice.
Methods: Outcomes were retrospectively collected from 364 patients who underwent URS and 444 patients who underwent SWL for urolithiasis targeted using fluoroscopy in a single academic institution from July 2012 to February 2019. Patients with ureteral stones, renal stones <5 mm and >20 mm, and those who underwent both URS and SWL were excluded. After patient matching, 86 URS and 237 SWL patients were included for analysis. Mann‐Whitney U and Chi‐square tests were used to compare fluoroscopy time and clinical outcomes with p < 0.05 considered significant.
Results: Gender distribution, age, BMI, stone size, and stone location were not different between patients. Total mean number of stones was higher in the URS group (2.4 ± 1.4) compared to SWL group (1.5 ± 0.9, p < 0.05). Fluoroscopy time was greater in patients who underwent SWL (189.3 ± 98.5 seconds) compared to those undergoing URS (6.7 ± 11.9 seconds; p < 0.05). Ureteroscopy had a significantly higher SFR compared to SWL (p < 0.05). Both groups had similar complication rates (4.7 vs. 7.0%, p = 0.32) and Clavien‐Dindo scores.
Conclusions: Our study demonstrates that in the modern era, SWL results in ∼27x increased radiation exposure compared to URS. In addition, this study agrees with prior findings demonstrating that URS has a higher stone free rate with a similar complication rate compared to SWL. This highlights the importance of developing strategies for reducing fluoroscopy time while performing SWL such as the use of ultrasound guidance.
Building a roadmap for initial evaluation and follow up for surveillance of renal masses: Results from MUSIC consensus panel
A Patel, B Lane, M Butaney, A Johnson, J Qi, C Rogers, f Urological Surgery Improvement Collaborative
Henry Ford Health System
Introduction & Objective: Current guidelines are limited for the selection of patients pursuing surveillance for renal masses. The Michigan Urological Surgery Improvement Collaborative ‐ Kidney mass: Identifying and Defining Necessary Evaluation and therapY (MUSIC‐KIDNEY) has seen variability in initial evaluation, follow up and compliance to planned strategies. We aim to establish a consensus roadmap to initial evaluation and follow up of patients entering surveillance.
Methods: A consensus panel (CP) following the modified Delphi method was organized within MUSIC. Participants indicated their agreement with statements relating to initial evaluation and follow up for surveillance via an online tool. Factors not achieving agreement were iteratively developed during three rounds of questionnaires. Level of agreement necessary to achieve consensus was set at 80%.
Results: Twenty‐six MUSIC urologists (69% fellowship trained, 73% practicing in the community) formed the CP. 58% felt current surveillance guidelines were useful. 39% (31/80) of questions relating to initial evaluation and follow up achieved consensus by round 3. Consensus for initial evaluation: All patients should undergo axial imaging, assessment of tumor complexity, renal function and chest imaging only for tumors >3 cm. Renal biopsy is not required prior to entering surveillance. Consensus was achieved for safety of CT and MRI for GFR >60 and >30 respectively. Consensus for follow up: 1st imaging (axial) should be between 3‐6 months, with subsequent imaging (axial or US) timing varying per tumor size (Figure 1), chest imaging should be reserved for tumors >5 cm, tumor growth rate was an appropriate trigger to intervention, duration of surveillance should be >5 years for healthy pts and at least 3 years for comorbid pts.
Conclusions: A consensus panel using a modified Delphi approach helped define a roadmap for surveillance of renal masses in the MUSIC‐KIDNEY collaborative. We were able to highlight several areas for further discussion where consensus was not achieved. Future directions are to bring MUSIC‐KIDNEY data to the attention of other national and international kidney cancer groups for further expert‐based opinions and construction of tools for a broader range of patients.
Predictors of Radiation Exposure During Ureteroscopy/RIRS: Can We Limit our Exposure?
A Rai, D Nethala, S Rastogi, T Aro, A Abraham, D Hoenig, AD Smith, Z Okeke
The Smith Institute for Urology
Introduction & Objective: Fluoroscopy has become critical to the completion of a variety of endourologic procedures and as such, exposure to the surgeon and other members of the operative suite has increased. Our understanding of risk factors that may predispose surgeons and OR staff to increased radiation exposure is relatively poor. We therefore sought to examine the variables associated with higher radiation exposure during URS/RIRS in hopes to raise awareness regarding exposure.
Methods: A retrospective examination of URS/RIRS cases was performed between July 2019 and September 2019. Data was collected primarily between two endourologic, fellowship‐trained surgeons completing URS/RIRS at a tertiary academic center. Fluoroscopy data was collected from the C‐arm radiation dose reports at the conclusion of the case.
Results: A total of 33 ureteroscopy cases were completed, however 4 cases were excluded as they were completed for UTUC management or had incomplete data. Of the remaining 29 cases, stone location appeared to be the associated with a higher average radiation exposure associated with ureteral location (18.9 mSv vs 9.6 mSV, p = 0.04). Interestingly, stone size ( >1 cm vs <1 cm) was not associated with significant difference however did appear to have a higher average radiation exposure (18.5 mSv vs 10.5 mSv, p = 0.13). Radiation exposure did appear to be different between surgeons as well, but did not achieve significance (17.6 mSv vs 10.6 mSv, p = 0.14). Patient characteristics did not appear to be associated with greater radiation exposure, as neither age ( >65), gender, or obesity (BMI >30) appeared to be significant.
Conclusions: Our study demonstrates that ureteral stone location was significantly correlated with higher radiation exposure when compared to renal stone location. In addition, stone size greater than 1 cm may also be associated with higher radiation exposure despite not achieving significance. Further study will likely be helpful in elucidating factors most contributory towards elevated radiation exposure during RIRS/URS and guiding surgeons towards intelligent fluoroscopy utilization.
Point of Care Smart Device Ultrasound Probes Versus Bladder Scanner ‐ A Prospective Randomized Trial
HC Wright, H Brar, S De
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA.
Introduction & Objective: Smart device ultrasound (SDUS) probes connect directly to smartphones or tablet personal computers. They show promise in their ease of use and accuracy as a point of care ultrasound (POCUS), yet have not been evaluated in a urology clinic. We sought to evaluate two different SDUS probes, in comparison to a standard bladder scanner (BS), in the accuracy of predicting urine volumes. Specifically, we assessed the Clarius C3 and Butterfly IQ probes. We also compare pricing for a simple cost analysis.
Methods: Adult male patients who presented to the urology clinic were enrolled and randomized to undergo transabdominal pre and post‐void bladder volumetrics with the BS and one of the two SDUS. Each probe came with an application that automatically calculates volume via bladder imaging. Actual voided volume (VV) was measured with a volume marked urinal. BS was performed by qualified urology nurses, and the same machine was used for all patients. SDUS was performed by a urologist trained to use the devices. BS and SDUS were performed within 2 minutes of each other, and each user was blinded to the other's results. The SDUS probes were connected to an Apple (Cupertino, CA) iPad 7th generation tablet. Patient demographics, BPH related medical history, and voided volume were recorded. Statistics were reported as either mean and standard deviations (SD) or number and percent. Error was defined by the absolute value of the mean actual VV minus the mean calculated VV (with either the SDUS or BS).
Results: 44 patients were enrolled (21 Clarius, 23 Butterfly). Baseline demographics were similar between groups (p > 0.05, table 1). In the Clarius arm, the mean SDUS error was 60.72mL (SD 48.57), compared to the mean BS error of 50.43mL (SD 71.99, p = 0.6). In the Butterfly arm, the mean SDUS error was 33.04mL (SD 21.97), significantly lower compared to the mean BS error of 54.83mL (SD 31.95, p = 0.01). Both SDUS were more affordable than the BS, costing 45‐76% less.
Conclusions: The Butterfly IQ SDUS more accurately measured the VV (and pre/post void volumes) compared to BS, while there was no difference between the Clarius C3 and BS. Both probes were more affordable than the BS, indicating that they are a more cost effective device to utilize, without sacrificing (and even gaining) the accuracy of bladder volumetrics. The SDUS probes have the added benefit of being able to POCUS other organs, which is not possible with the BS.
A Prospective Study Using Abdomen Only CT Imaging For Routine Stone Imaging Follow‐Up
M Fritz, J Zhang, A Ayoob, J Bell
Univeristy of Kentucky
Introduction & Objective: In order to reduce radiation exposure for urinary stone patients, we implemented an abdomen only CT protocol for patients presenting for routine follow‐up for their stone disease. This study follows a prospective cohort of patients who underwent an Abdomen‐only CT protocol.
Methods: Endourology providers at a tertiary care hospital ordered abdomen only CT scans on patients being scheduled for future routine stone imaging follow‐up. The decision to use CT abdomen versus another imaging modality was left to the discretion of the ordering provider. After the scan, the patients were followed for 60‐days to see if additional imaging was needed due to missed items on the CT abdomen only. In addition, clinic notes were analyzed to see if the patient was having stone‐related symptoms within a 2‐week window prior to the scan. CT abdomen protocol was performed using a low‐dose protocol beginning at the lung base and extending to the iliac crest with no IV or oral contrast given.
In order to assess the radiation reduction, we selected patients from this larger cohort who had a prior CT Abd/Pelvis without IV contrast scan at our institution on a similar CT scanner. CT imaging parameters were then compared and the effective dose was estimated using dose estimating software (VirtualDoseTMCT, Virtual Phantoms, Inc).
Results: This prospective cohort currently has twenty‐one patients to date, fifteen of whom have completed their imaging. Nine of these patients had stones on imaging. No patients required additional imaging after their scan. Twelve patients had a prior CT Abd/Pelvis scan to perform dose comparison statistics. The average effective dose reduction in these patients was 59% (Figure 1).
Conclusions: This prospective study suggests that restricting the CT scan to the abdomen does not miss any significant pelvic pathology and appears to be a safe and easy way to reduce radiation exposure in asymptomatic stone patients presenting for routine follow‐up.
In the era of MRI targeted biopsy what is the role for TRUS biopsy? Results from Largest Asian series
J Du, Y Lu, Z Law, H Huang, H Ho, J Yuen, L Lee, K Tay, K Chen, W Lau
Singapore general Hospital
Introduction & Objective: Transperineal prostate biopsy has been reported to have fewer septic complications and higher cancer detection rate especially with guidance of Magnetic resonance imaging (MRI). However, this was associated with higher cost and longer diagnostic cycle; thus case selection is crucial. In this study we compared cancer detection rate between robotic guided transperineal prostate biopsy (RTPB) and transrectal prostate (TRUS) biopsy together with other parameters to guide clinical case selection.
Methods: Patients who underwent RTPB for suspected prostate cancer at the Singapore General Hospital (SGH) between September 2006 and February 2016 were retrospectively analyzed. Consecutive patients who underwent TRUS biopsy in SGH between March 2012 to Dec 2013 were also analyzed for comparison. For cancer detection rate comparison patients who underwent biopsy for active surveillance or brachytherapy were excluded as well as patients with PSA >100 ng/ml and abnormal DRE. Pearson Chi‐Square test was used to compare cancer detection rates in different groups.
Results: Total 950 patients were included in RTPB group. After excluding patients with inadequate data total 865 patients were included. Total of 731 patients were included in TRUS biopsy group after excluding cases with missing data. MRI targeted biopsy had significantly higher cancer detection rate compare to TRUS biopsy for both biopsy naïve and previous negative biopsy patients. Template transperineal biopsy had similar cancer detection rate compare to TRUS biopsy for patients who had pervious negative biopsy. Higher PSA densities were associated with higher cancer detection rates for all three biopsy groups. We calculated when PSA density cut off at 0.18 and below MRI targeted biopsy had significantly higher cancer detection rate compare to TRUS biopsy while PSA density cut off at 0.26 and above this benefit was no longer observed.
Conclusions: Template transperineal prostate biopsy has limited diagnostic benefit compare to TRUS biopsy and MRI targeted biopsy. Transperineal MRI targeted biopsy had higher cancer detection rate compare to TRUS biopsy in both biopsy naïve and previous negative biopsy groups. However when PSA density >0.26 this benefit was no longer observed.
Novel Use of Dual Energy CT in Guiding Treatment of Complex Renal Cysts
M Davis, K Hart, BF Schwartz, DT Lybbert
Southern Illinois School of Medicine
Introduction & Objective: Current management of complex renal cysts is dependent on imaging characteristics suggestive of malignant features. Standard CT and MRI have limitations (hemorrhage, pseudoenhancement , hyper attenuation/calcifications ). DECT utilizes simultaneous scans at two different voltages to quantify iodine uptake, theoretically allowing for better determination of malignancy potential. We reviewed our early cases using this novel technology
Methods: Retrospective case series of 17 patients with complex renal cysts imaged via DECT. All patients had prior ultrasound or CT imaging. DECT imaging obtained when initial imaging was indeterminate. Per standard DECT protocol, two simultaneous abdominal scans obtained at 80 kVp and 140 kVp; virtual noncontrast images reconstructed by a subtraction algorithm. All imaging and subsequent treatments reviewed.
Results: Seventeen patients with DECT imaging were identified with mean cyst size 3.83 cm (1.2 – 8.1 cm). Eleven patients had no iodine uptake on DECT; 10 were placed on active surveillance (6 DECT, 4 US) while one, due to personal preference, underwent RALPN with benign final pathology.
Of the six patients with positive iodine uptake on DECT, 2 elected to undergo close surveillance while four underwent RALPN, with 2 final pathologies of G3 clear cell RCC, one G3 papillary RCC, and one benign tumor.
Conclusions: DECT allows less radiation exposure by omitting precontrast images. DECT allows direct determination of iodine uptake as surrogate measure for malignant potential. Future research is needed to quantify iodine uptake, determine “cut‐off” points beyond which a lesion ought to be determined potentially malignant as well as for post‐surgical monitoring protocols
Challenging the Status Quo: Can Low Dose CT Diagnose Stones in Obese Patients?
JD Belle, G Martin, M Keheila, J Smith, M Hajiha, AS Amasyali, DD Baldwin
Loma Linda University, School of Medicine
Introduction & Objective: Obesity is a significant risk factor for both stone formation and recurrence. Obese patients receiving conventional CT scans are exposed to substantially greater radiation than normal weight patients., placing them at increased risk for radiation related complications, including cancer. Although low dose CT would potentially reduce radiation exposure, it is not currently recommended in obese patients, due to concerns that sensitivity will be decreased. The purpose of this study was to evaluate the utility of low dose CT scan in clinical patients with nephrolithiasis.
Methods: A retrospective chart review of 734 patients at a single institution undergoing CT scan for kidney and ureteral stones from 2014‐2020 was conducted. Patients with BMI <30, those without conventional and low dose CT within 3 months, and those undergoing interval treatment or stone passage were excluded. Low dose (LD) CT was defined as dose length product (DLP) <266 mGy*cm (< 4 mSv), and ultra‐low dose (ULD) was defined as <126 mGy*cm (< 1.9 mSv) per the American Association of Physicists in Medicine. LD and conventional dose (CD) CT scans were stripped of identifying information and reviewed in a randomized fashion by a blinded board‐certified abdominal imaging radiologist specializing in kidney stones. Data were collected on radiation exposure, stone presence, location, size, and Hounsfield units (HU). Results were analyzed using a Wilcoxon matched pairs signed rank test with p < 0.05 considered significant.
Results: Twenty‐six patients met inclusion criteria. Patient BMI ranged from 30.5 to 63.8 (mean 37.3) with 18 < 40 and 8 ≥ 40. Mean radiation exposure was 15.14 mSv for conventional dose CT. Four patients had ULD (mean 1.37 mSv) and 22 had LD (mean 2.72 mSv) studies. 49/55 stones (89%) were seen on LD CT when compared to CD CT. All 6 stones missed on LD CT were ≤2mm. One false positive or newly formed 2.1 mm stone was identified on a LD CT done 36 days after CD CT. Stone size on CD CT ranged from 1 to 26 mm (mean 7.5mm) with 29 ≤ 5mm and 21 > 5mm. Median difference in stone size between CD and LD CT was 0.2mm (p = 0.1). None of the false negatives or the false positive on LD CT would have altered management.
Conclusions: LD CT in patients with BMI >30 accurately identifies clinically significant stones while reducing radiation exposure by 82% in the LD and 91% in the ULD groups. These data suggest that LD CT scan is an effective option for evaluation of obese patients, and if these results are confirmed in future studies, a modification of the AUA guidelines to include LD CT scan in obese patients should be considered.
Emergency Department Non‐contrast Computed Tomography for Suspicion of Obstructive Urolithiasis: Yield and Consequences
Z Savin, S Dekalo, E Schreter, S Greenberg, G Aviram, O Yossepowitch, M Sofer
Tel‐Aviv Sourasky Medical center, Sackler School of Medicine, Tel‐Aviv University
Introduction & Objective: Our goal is to analyze patterns of referral, yield, and clinical implications of non‐contrast computed tomographic scans (NCCTs) in the acute evaluation of flank pain suspected as obstructive urolithiasis (OU) in a high‐volume emergency department (ED).
Methods: The study comprised 506 consecutive NCCTs performed in the ED during 4 months. Detection rates of OU, incidental, and alternative findings were calculated. Imaging signs suspicious for recent passage of stones were considered positive for OU, while renal stones without signs of obstruction were considered unrelated to the acute presentation. OU, other findings requiring hospitalization, and incidental findings warranting further workup were considered situations in which NCCTs were warranted.
Results: NCCTs confirmed an OU diagnosis in 162 (32%) patients and non‐clinical significant nephrolithiasis in 125 (25%). The radiological distribution of the NCCT findings is presented in figure 1. NCCTs revealed other findings in 108 (21%) patients, including 42 (8%) with clinically significant incidental findings and 26 (5%) with alternative diagnoses requiring hospitalization. They were entirely negative in 111 (22%) patients. Corroboration of these outcomes together with overlapping of OU, incidental, and alternative significant findings in some patients resulted in an overall justified NCCT request rate of 44%. All incidental and alternative findings data are presented in tables 1 & 2.
Conclusions: The yield of NCCTs performed in acute presentations of flank pain suspected as OU is relatively low, and over one‐half of the scans are unwarranted. The pattern of requesting NCCTs in the ED needs refinement in order to avoid abuse that may led to radiation overexposure, psychological burden, physical harm, and financial overload.
Index Prostate Lesion Density Does Not Improve the Diagnostic Performance of Detecting Clinically Significant Prostate Cancer
M Said, M Rajput, C Metz, P Gellhaus, CR Tracy, RL Steinberg
Introduction & Objective: Lesion volume on multiparametric magnetic resonance imaging (MR) can be an indicator of biological aggression. Smaller prostate volume has also been associated with greater detection of clinically significant prostate cancer (csPC). Given this relationship, normalizing lesion volume to prostate volume (or lesion density; LD), may improve detection of csPC. We sought to evaluate the predictive ability of LD in identifying csPC in the index region of interest on MR‐targeted biopsy (MR‐TB).
Methods: A single institution retrospective review of all MR‐TB from May 2017 to April 2020 was performed. Only men without prior PC diagnosis were included in the analysis. MRI lesions ≥3 on the Prostate Imaging and Reporting and Data System (PIRADS) were biopsied by one of 2 urologists using the UroNav system (Philips Healthcare, Best, Netherlands). csPC was defined as Grade Group ≥2. LD was calculated by dividing the lesion volume (spheroid shape estimate) by the prostate volume. Logistic regression was utilized to assess for risk factors for csPCa. Using criteria similar to the Rotterdam Risk Calculator (age, prior biopsy status, PIRADS score), predictive probabilities were generated via logistic regression using LD alone in model 1, LD+ prostate specific antigen (PSA) in model 2 and PSA density (PSAD) in model 3. Receiver‐operator curves were constructed and compared using the DeLong test (p < 0.05).
Results: 508 men underwent MRI‐TB during the study period, of which 384 met study criteria. Median age was 65 yr (IQR 60‐69) with 1 (IQR 1‐2) prior biopy. Median PSA and PSAD were 8.2 (IQR 6.0‐12.3) and 0.14 (IQR 0.10‐0.22), respectively. Prior biopsy (OR 0.335, p < 0.001), prostate volume (OR 0.99, p = 0.02) and PIRADS (p < 0.001) were predictive of csPC on multivariable analysis, while age (OR 1.04, p = 0.38), PSAD (OR 2.992, p = 0.21) and LD (OR 0.465, p = 0.764) were not. Models 1 (AUC = 0.744) and 2 (AUC = 0.743) were not statistically different than Model 3 (AUC = 0.753, p = 0.79 for both, Figure 1).
Conclusions: LD does not appear to provide added diagnostic value to already utilized variables in predicting the presence of clinically significant prostate cancer. Continued exploration of novel parameters to improve the diagnostic accuracy of MRI‐TB is warranted.
Withdrawn
Can ureteroscopy and retrograde intrarenal surgery be safe and effectively performed with no auxiliary fluoroscopy? A systematic review
C Laranjo Tinoco, I Marques, J Ribeiro, A Cardoso, R Matos Rodrigues, S Anacleto, P Passos, E Lima, M Cerqueira Alves, P Mota
Hospital de Braga, EPE
Introduction & Objective: Ureteroscopy (URS) and retrograde intrarenal surgery (RIRS) are usually performed under fluoroscopic guidance for the treatment of urolithiasis, with high stone‐free rates (SFR) and infrequent complications. Fluoroscopy‐free techniques are being developed due to concerns regarding radiation exposure during fluoroscopy and its risks. The purpose of this systematic review is to assess the efficacy and safety of fluoroscopy‐free URS and RIRS.
Methods: We performed a systematic review based on the PRISMA statement and searched Pubmed and Scopus databases for eligible articles until 31 March, 2020. Studies providing data on SFR, complications or retreatment rate for fluoroscopy‐free URS or RIRS were included. We assessed the quality of evidence and risk of bias using the Critical Appraisal Skills Programme or the Institute of Health Economics Appraisal Checklist, depending on the study type.
Results: 17 publications were included with a total of 2957 patients. The process of study selection is explained in Figure 1. None of the comparative studies found significative differences in results between fluoroscopy‐free or conventional fluoroscopic guided procedures in terms of SFR, complications, or retreatment rate. Most case series reported SFR >85% and low complication rates. Detailed results are described in Table 1. Most studies had moderate quality and 3 were high‐quality studies.
Conclusions: The analysis of the collected data in this systematic review suggests URS and RIRS remain effective without fluoroscopy, having no negative impact on the management of kidney stones disease while preserving the health of patients and workers. However, large prospective studies are needed for higher quality evidence.
Use of High‐Frequency Micro‐Ultrasound For Real‐Time Targeted Prostate Biopsy and Subsequent Prostate Cryoablation: Initial Clinical Experience
HE Moreland, RD Carr, LJ Smith, LT O'Connor, DB Rukstalis
University of South Carolina School of Medicine
Introduction & Objective: The 29 MHz transrectal ExactVu micro‐ultrasound system (microUS, Exact Imaging, Markham, Canada) has demonstrated effectiveness in real‐time identification and targeted biopsy of suspicious prostate lesions due to its MRI‐comparable visualization capabilities. Therefore, it is likely that its enhanced imaging will also improve targeted prostate ablations. We describe the first series of patients who have undergone microUS‐guided targeted prostate cryoablation.
Methods: A retrospective review of a prospective quality improvement database was performed. Nineteen prostate cryoablations with the microUS system were performed (median age 73, PSA 5.78 ng/mL, IPSS 12), with eight having previously undergone microUS‐guided targeted prostate biopsy. Information was collected regarding cancer identification, location, and technical aspects of each cryoablation procedure.
Results: In the biopsy population, a median of seven cores (range, 4‐12) were obtained from visible lesions, with a median of three positive cores. The median Gleason sum was 7.5 (6‐10) with 81.25% clinically significant lesions. Eleven whole gland and eight individualized ablations were performed, with a median number of six (4‐6) cryoprobes used. The ExactVu probe has a 13‐degree angulation from horizonal, altering the visuospatial relationship between the probes and the prostate. This requires adjustment of the cradle to ensure proper orientation of the grid. Due to its higher frequency, greater compression of the rectal wall is required to visualize the anterior prostate. All lesions seen on biopsy were visible at the time of the ablation. In 84.2% of cases, all probes were placed through the perineal grid into targeted regions of the prostate. Otherwise, some probes were placed freehand, usually beneath the grid, to accurately access the posterior gland.
Conclusions: MicroUS‐guided targeted biopsy facilitates microUS‐guided individualized cryoablation. Additional surgical proficiencies are required to accurately place cryoprobes under high‐frequency imaging. It is likely that microUS will enhance the performance and outcomes of prostate ablations.
Evaluation of Triple‐D Score as a predictor of stone‐free‐status following extra corporeal shock wave lithotripsy: A single centre pilot study
K Biswas, K Bliss, Z Maan, G Rix, S Datta
Colchester General Hospital
Introduction & Objective: Triple‐D score is a simple and reproducible score to predict the stone‐free‐status (SFS) after extra‐corporeal shock wave lithotripsy (ESWL) that has been validated in the literature. We review the accuracy of this score in our set‐up and its usefulness to predict the SFS in our ESWL management pathway.
Methods: A retrospective review of demographic, clinical and Computed Tomography (CT) based stone characteristics data including Triple‐D score was undertaken for patients who underwent ESWL at our hospital from August 2020 to November 2020. Follow up analysis determined if patients were stone‐free or planned for other procedures. Comparison of the peri‐procedural parameters between stone‐free and residual‐stone cohorts was performed using standard statistical methods.
Results: A total of 46 patients underwent 98 sessions of ESWL of which 23 patients were stone‐free (50%). The stone‐free rate for Triple‐D score of “3”, “2”, “1” and “0” were 87.5%, 57.5%, 44.4% and 0% respectively (p = 0.012). The receiver operator characteristics curve showed significant accuracy of Triple D score (AUC = 0.751, p = 0.003) in predicting the SFS, better than the maximum stone dimension (AUC = 0.731, p = .007), stone volume (AUC = 0.722, p = 0.010) or stone density (AUC = 0.691, p = 0.026) alone.
Conclusions: Triple‐D score is a simple, CT based, easy‐to‐calculate and reasonably accurate scoring system to predict the post‐ESWL SFS. This may be incorporated into the ESWL management pathway both for outcome prediction and patient counselling. Further larger scale population studies would be desirable.
Do CT scout images obviate need to perform Xray KUB in the management of ureteric calculi
N Rokan, H Joshi, A Al‐Mitwalli
Introduction & Objective: It is unclear if CT scout films performed as part of planning a CTKUB can replace the need of undertaking a simultaneous X‐ray KUB (XKUB) in the management of patients with ureteric stones.
Methods: We undertook a review of patient imaging from November 2019 to March 2020 for all ureteric stones diagnosed by CTKUB. We looked at diagnostic yield and the need for follow‐up imaging.
Results: Of 562 CTKUB performed, 100 diagnosed ureteric stones (72% male; mean age 57years old). The mean size of ureteric stones was 4.85mm (2mm ‐13mm), the majority at the VUJ (41.7%). The sensitivity for scout films was 46% (n = 46%). From the 54 scouts with no visible stones, 75% (n = 40) had stone size <5mm. 76 patients had simultaneous AXR with a sensitivity of 68% (n = 52) for visible stones. Of the 32% where a stone was not visualised (n = 24), 83% were <5mm. Stones were visible on both CT scout and XKUB in 31 patients. Expectant management occurred in 91% patients, with 74% requiring subsequent imaging throughout their management. The average number of follow‐up imaging was 2.93 (one to six more times).
Conclusions: CT scouts and XKUB are complementary to each other, however one does not completely obviate the need for the other. HU of <630 and a stone size <5mm predicts non‐visibility for stones in XKUB films and scout films.
The Changing Trends of image Guided Biopsy of Small Renal Masses before intervention‐ An Analysis of European Multinational Prospective EuRECA Registry
V Vinson, F Keeley, Jr, B Lagerveld, T Nielsen, G Lughezzani, T Wah
School of Medicine, Faculty of Medicine and Health, University of Leeds, Leeds Department of Targeted Intervention, Division of Surgery and Interventional Science, University College London, London
Introduction & Objective: Up to 30% of all treated small renal masses (SRMs) are benign. This study aims to assess the trends and potential factors influencing the decision to perform image‐guided biopsy before cryoablation treatment and compare the histological outcomes of pre‐cryoablation biopsy and biopsy at the time of treatment.
Methods: From December 2014 to October 2020, patients with T1N0M0 SRMs undergoing percutaneous cryoablation from 14 European institutions within the European Registry For Renal Cryoablation (EuRECA) were included for the retrospective analysis. The trends of performing image‐guided biopsy as a separate session before cryoablation of SRMs were analysed over time, and the potential factors influencing the decision to perform image‐guided biopsy before treatment were analysed using univariate and multivariate logistic regression models.
Results: 1,050 patients (Median [IQR] age, 69[13], 695 men) were evaluated. The median tumour size of the cohort is 3[1.4] cm. The use of pre‐cryoablation biopsy has significantly increased from 39% (67/171) in 2015 to 72% (88/122) in 2019 (p < 0.001; Figure 1). Rates of undiagnosed histology and benign histology is significantly higher in patients undergoing biopsy at the time of treatment (16% [50/313] vs 0.16% [1/636], p < 0.001; Figure 3). For every 4.5 patients receiving pre‐cryoablation biopsy, one less patient receives cryoablation treatment for a non‐malignant renal tumor. Aged 70‐79 (OR 0.53, 95%CI 0.29‐0.96), 80‐89 (OR 0.47, 95%CI 0.24‐0.92), obesity (OR 0.73, 95% CI 0.55‐0.98) and having a solitary kidney (OR 0.40, 95%CI 0.27‐0.61) are three patients' factors associated with less likelihood of pre‐cryoablation biopsy (p < 0.05). R.E.N.A.L. nephrometry score of 10+ (OR 1.86, 95% CI 1.11‐3.10) and a Charlson Comorbidity Index >1 (OR 2.11, 95%CI 1.54‐2.88) are factors associated with higher likelihood to have received a pre‐cryoablation biopsy (p < 0.05).
Conclusions: The increased use of pre‐cryoablation biopsy should be advocated as it is more likely to lead to confirmatory histological diagnosis than biopsy at the time of cryoablation, thus reducing overtreatment of non‐malignant SRMs.
DNA methylation urine biomarkers test (EpiCheck® assay) in the diagnosis of upper tract urothelial carcinoma: results from a single‐center prospective study
A Gallioli, M Fontana, R Boissier, A Territo, P Diana, A Sánchez‐Puy, J Subiela, F Sanguedolce, JM Gaya, J Palou, A Breda
Department of Urology, Fundació Puigvert, Barcelona, Spain
Introduction & Objective: The diagnosis and risk stratification of upper urinary tract urothelial carcinoma (UTUC) can be challenging. Urinary cytology (UC) has low sensitivity and CT scan is not sufficient as in about 50% of cases ureteroscopy (URS) changes treatment choice. Bladder EpiCheck® (Nucleix, Israel) is an innovative assay able to detect a panel of epigenetic DNA methylation patterns found in urothelial cancer cells, especially in high‐grade diseases. Our aim is to evaluate the performance of this assay in the detection of UTUC.
Methods: We prospectively enrolled patients undergoing URS at our center between 01/2019 and 01/2021 for the diagnosis, treatment or follow‐up of UTUC. Patients with synchronous BC were excluded from the study. We retrieved 20 mL urine samples both from the lower and upper tract, respectively by bladder or ileal conduit and ureteral catheterization for EpiCheck® and UC analysis. Flexible URS was carried out according to standard technique. Test performance was evaluated by sensitivity, specificity, positive (PPV), and negative predictive values (NPV), both for any‐grade and high‐grade disease. The study (NCT04702347) was approved by the Ethical committee (C2018/35).
Results: We enrolled 80 consecutive patients for a total of 87 URS. 2 patients were excluded from the analysis because synchronous BC, while 5 samples resulted unsuitable for epigenetic testing. Overall, we retrieved 72 and 82 valid samples from lower and upper tract respectively (Table 1). Lower tract Sensitivity and NPV for any‐grade disease are 58.5% and 80.0% vs 30% and 85.7% in EpiCheck® vs UC; sensitivity and NPV for high grade disease are 73.7% and 88.1% vs 64.4% and 82.7% in EpiCheck® vs UC. Upper tract sensitivity and NPV for any‐grade disease are 84.8% and 80.6% vs 52.2% and 60% in EpiCheck® vs UC; sensitivity and NPV for high grade disease are 95.8% and 97.2% vs 64% and 83.6% in EpiCheck® vs UC.
Conclusions: EpiCheck® appears to be a useful tool in the UTUC setting and it could find a crucial role in the diagnosis and follow‐up of UTUC, particularly in detecting the absence of a high‐grade disease. As EpiCheck® results are remarkable, this assay is now included in the diagnostic work‐up of UTUC at our center
Outcome of Renal Transplantation after Laparoscopic Donor Nephrectomy: a Comparative Study Between Single and Multiple Renal Arteries
DA Mendiola, EL Gerial Jr., JA Abraham
National Kidney and Transplant Institute
Introduction & Objective: Laparoscopic retrieval of renal allografts (donor nephrectomy) with multiple arterial supply can be challenging because of the complexity of the surgery. It can lead to longer operative and warm ischemia times and inferior 1‐year allograft surivival. We compared the donor and recipient outcomes between laparoscopic donor nephrectomy in single artery (LDNS) vs. multiple renal arteries (LDNM) in a large volume transplant center in the Philippines.
Methods: A chart review was done on all laparoscopic donor nephrectomies performed from January 2011 to December 2015. Donor characteristics (age, gender, BMI) were summarized. Intraoperative parameters: [operative time (OT), estimated blood loss (EBL) and warm ischemia time (WIT)] and postoperative outcomes: length of hospital stay (LOS) and mean rise in creatinine; and recipient outcomes [delayed graft function (DGF)] and one‐year allograft survival were compared between the two groups. Complications were analyzed using the Clavien‐Dindo classification.
Results: A total of 390 donors, 300 (77%) LDNS and 90 (23%) LDNM were performed during the study period. The donor characteristics were similar for both groups except for sex where the male to female ratio is 1.5:1 for LDNS and and 2.7:1 in LDNM. Donor OT was shorter in LDNS (175min[45‐398]) vs. LDNM (185min[118‐360]). Recipient OT was shorted in LDNS (175min[45‐398]) vs LDNM (185min[50‐415]). There was no significant difference in EBL in LDNS (100mL[10‐800]) vs. LDNM (100mL[10‐1600]); LOS in LDNS (3days[2‐6]) vs LDNM (3days[2‐8]); WIT in LDNS (3min[1‐32]) vs. LDNM (3min[1‐21]) and DGF in LDNS 6/300(2%) and LDNM 1/83(1.2%). There was neither conversion to open, morbidity nor mortality for both. The one‐year allograft survival was also similar in LDNS 295/300(98.3%) vs. LDNM 83/83(100%).
Conclusions: In the setting of laparoscopic donor nephrectomy, multiple renal arteries (double and triple) are associated with a longer donor and recipient operative time. Allografts with multiple renal arteries however have comparable warm ischemia time and allograft survival to those with single arterial supply.
Open vs minimally invasive adrenalectomy for adrenal metastasis: a single center experience
A Pecoraro, D Amparore, M Burgio, E Checcucci, M Manfredi, P Alessio, S De Cillis, F Piramide, G Volpi, S Granato, M Sica, P Verri, S Piscitello, D Zamengo, B Carbonaro, J Mézière, L Ola, C Fiori, F Porpiglia
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
Introduction & Objective: To test for differences in survival rates between minimally invasive and open adrenalectomy for solid tumor metastases.
Methods: Descriptive statistics included medians and interquartile ranges, as well as frequencies and proportions for continuous and categorical variables, respectively. The statistical signicance of differences in medians and proportions was evaluated with the Kruskal‐Wallis and chi‐square tests. Kaplan Meier methodology was used to test differences in overall survival (OS) and recurrence‐free survival (RFS) rates.
Results: We retrospectively analyzed 66 adrenal metastasectomies from our prospectively maintained database (2001‐2019). Of those 51 (77.2%) and 15 (22.7%) were treated with minimally invasive and open adrenalectomy, respectively. The vast majority of patients (n = 39, 59%) harbored non‐small‐cell lung carcinoma (NSCLC) and adrenal carcinoma (n = 12, 18.2%) as the primary tumor. Relative to open surgery, minimally invasive adrenalectomy patients harbored usually <2 adrenal metastases (p = 0.02) and of smaller size (3.6 vs. 5.3, p = 0.02). At nal pathology, adrenal metastases were more often from NSCLC (62.1%) and adrenal carcinoma (22.7%). No differences in terms of surgical margins, intra and postoperative complications were recorded according to type of adrenalectomy. Kaplan‐Meier derived OS rates (Fig. 1) were 62% (median survival 45 mo) vs. 53% (median survival 23 mo) and no differences were observed according to the site of primary tumor (p = 0.51) and in terms of RFS.
Conclusions: Adrenal metastases originated more often from NSCLC and adrenal carcinoma. Minimally‐invasive adrenalectomy patients showed a longer OS than open adrenalectomy individuals, as minimally invasive approach could have been attempted more common in less advanced disease. Further studies are needed to validate our results.
Metabolic Disturbances During Topiramate Use and their Reversibility Following Drug Cessation
D Pelzman, E Kazi, M Semins, S Jackman
UPMC
Introduction & Objective: Topiramate is a commonly used medication which inhibits carbonic anhydrase, causing renal tubular acidosis and hypocitraturia, thereby increasing the risk for kidney stone formation. Despite the strong association between topiramate use and kidney stone formation, few studies have examined the characteristics of stone formers taking topiramate. Additionally, the reversibility of the metabolic disturbances with cessation of the medication has not been previously studied. To fill this knowledge gap, we investigated the stone composition and 24‐hour urine samples of a large cohort of stone formers taking topiramate.
Methods: All progress notes written by 5 endourologists from a single academic center were retrospectively reviewed from January 2010 to July 2020 containing the words “topiramate” or “topamax.” Inclusion criteria were age >18 and presence of either a 24‐hour urine sample or stone analysis while on topiramate. In addition, a subgroup of 17 patients with 24‐hour urine samples before and after stopping topiramate were identified.
Results: A total of 93 patients were identified and included for final analysis. Twenty‐four hour urine samples were available in 65 patients and showed mean citrate excretion of 333 mg/day (95% confidence interval (CI) [254‐412]), mean pH of 6.54 (95% CI [6.41‐6.68]), and mean calcium phosphate supersaturation of 1.8 (95% CI [1.6‐2.1]). In the subgroup analysis, mean urinary citrate excretion increased from 233 mg/day (95% CI [135‐330]) to 633 mg/day (95% CI [471‐796], p < 0.01), and pH decreased from 6.61 (95% CI [6.34‐6.89]) to 6.34 (95% CI [6.12‐6.56], p = 0.06) after stopping topiramate (Figure 1). 114 stone events occurred in 73 distinct patients with 50% either pure or majority (≥ 50%) calcium phosphate by composition.
Conclusions: Hypocitraturia and elevated pH is seen during topiramate use with resultant higher rate of calcium phosphate stone formation compared to the general population. Stopping topiramate leads to significant increase in citrate excretion and normalization of pH. Patients and providers should be aware of this risk when starting topiramate therapy. These metabolic disturbances appear to be reversible with medication cessation.
Withdrawn
Withdrawn
Minimal scrotoscopic epididymectomy vs open epididymtectomy for epididymal mass treatment: A multi‐center, middle‐term clinical trial
Y Gao, Y Wei, J Yang
Introduction & Objective: To compare the middle‐term efficacy and safety results between minimal scrotoscopic epididymectomy (MSE) and open epididymectomy (OE) for the treatment of epididymal mass in multiple medical centers.
Methods: A total of 253 males with surgery for epididymal mass from 2012 to 2018 were included in this retrospective study. The preoperative, intraoperative and post‐operative follow‐up data of these patients were recorded. The effectiveness, safety and patient satisfaction of epididymal mass treatment were compared between MSE and OE. Results were presents as means, standard error of the mean, and 95% confidence intervals unless otherwise indicated.
Results: 174 of all 253 patients were underwent MSE and other 79 were underwent OE. All patients underwent surgery successfully. The average follow‐up time was 20.8 ± 8.2 months in MSE group vs 19.4 ± 8.6 in OE group(P = 0.219). 27 in MSE group vs 17 in OE group were reported complications graded I‐III. Postoperative recurrence occurred in 5 MSE cases vs 2 OE cases, but all the other one' preoperative symptoms were operatively relieved. The overall satisfaction of patients was high, with an average score of 94.8 ± 3.7 vs 91.7 ± 4.9 (MSE vs OE).
Conclusions: MSE is emerging as a safe and effective treatment option with promising perspectives for therapy in epididymal mass.
Comparison between the most used stone free predictor scales and the homologation of their rates, assisted by a new mobile application system, after retrograde intra renal surgery at a Mexican General Hospital
FM Santa Maria Orozco, C Martinez‐Arroyo, C Pacheco‐Gahbler, M Cantellano Orozco, I Navarro Ruesga, E davila Legorreta, M Aguilar Mendez
Dr. Manuel Gea Gonzalez General Hospital
Introduction & Objective: Retrograde intra renal surgery (RIRS) for renal and proximal ureteral stones is used globally. New technologies such as wide deflection gadgets and energies, help achieve high stone free rates, although can still be modified by stone and renal complexity factors. The most used nephrolithometric scales are R.I.R.S., RESORLU‐UNSAL (RUSS) and SEOUL, we added an internal validated scale, GeaNASA. All of them giving special importance to the inferior localization of the stone and infundibulum‐pelvic angle.
Objective: Compare the predictive stone free rates (PSFR) of each scale and their homologation, facilitated by a mobile application (app). Identify the predictive certainty of each scale based on our hospitaĺs data and surgery results. Generate an app, to capture patient data and obtain PSFR. Update the app to include RIRS and percutaneous nephrolithotomy (PCNL) scales.
Methods: Create a database with results from each of the mentioned scores. Retrospective analysis and a cross match of data and obtained a mean predictive rate (homologation of scales) and stablished an average rate to compare them. CHI square test to correlate data, each patient́s PSFR and the average score, and compare each positive and negative predictive value.
Results: Database with data of 99 patients diagnosed with renal stones and treated with RIRS in year 2019. A PSFR of 92.9%, 84.8%, 50.5%, 52.5% and 61.6% by R.I.R.S., RUSS, SEOUL, GeaNASA and the average score respectively. We obtained a 90.9% SFR post surgery (final outcome). A CHI2 test value of .246, .0177, .445, .036 and 3.11 with a statistic p of .619, .89, .3, .84 and .077 respectively. The PSFR positive/negative value of 84.8 and 1.01% for RIRS, 76.7/1.01% for RUSS, 44.4/3.1% for SEOUL, 47.4/4.4% for GeaNASA, 53.5/1.01% for the average.
Conclusions: The most accurate rate, compared with the final outcome, was obtained by R.I.R.S. All of them got a positive predictive rate that stands below the post surgery outcome. We obtained a statistically significant p when using the stablished average (p = .077), (homologation of scale items). There isńt significant inferiority among the scales individually. We updated the app so it can be a practical tool in the management of renal stones.
Outcomes of antegrade scrotal sclerotherapy for varicocele treatment: Our experience about 660 patients
M Jasser, R Mehdi, T Tarek, B Mohamed, K Ramzi, G Samir
Military hospital of Tunis
Introduction & Objective: Varicocele is one of the mean causes of male infertility. Treatment aims to improve the chance of conception. Many techniques have been described for varicocele management including the antegrade scrotal sclerotherapy (ASS). We provide a brief overview of the our experience with AAS for varicocele, including success and complications of this treatement.
Methods: Over the last 18 years at our institution, we performed 660 ASS. We present our own retrospective data of treating AAS including preoperative characteristics, perioperative and follow‐up data. The materiality level of p values less than 0.05 were considered significant.
Results: The average age was 30 years old. Mean operative time was 16 min (range 13 to 50 min). No significant intraoperative complications were reported. The average duration of hospitalization was 19 hours [9‐36 hours]. Postoperatively, we observed a statistically significant improvement in all the spermiological characteristics. Oligospermia decreased from 41 % to 29 % (p = 0,01). The median value of the percentage of progressive motile forms at 1 h improved from 52 % to 33 % (p = 0,02). Percentage of normal forms increased from 24 % before surgery to 14 % one year after the procedure (p = 0,006). In the subgroup of the infertile population, 145 patients (22%) fathered offspring at a 12‐month‐minimum. Within 90 days from the procedure, postoperative complications were recorded in overall 70 patients (10.6 %) such as hydrocele (27 patients), scrotal hematoma (14 patients), chemical orchitis (20 patients) and testicular atrophy (9 patients). Recurrence was detected in 73 (11 %) cases.
Conclusions: ASS is associated with a significant improvement in sperm concentration, motility, morphology, and pregnancy rate. It is presented as a safe, easy, and cost‐effective procedure with a low recurrence and complication rate.
Pheochromocytoma of urinary bladder: a case report
M Jasser, R Mehdi, B Nadhir, K Ramzi, G Samir
Military hospital of Tunis
Introduction & Objective: Paraganglioma of the urinary bladder is rarely encountered. Its clinical signs and symptoms are usually nonspecific.
Methods: .
Results: We report a case of a 48‐year‐old woman who presented with recurrent hematuria for last 2 months with a recently detected hypertension. Computed tomography (CT) revealed a lobulated mass arising from the posterior wall of the urinary bladder and protruding into the vesical lumen measuring 3cm with inhomogeneous postcontrast enhancement. Transurethral resection of the mass has instantly produced a hypertensive peak (200/110 mmHg) leading to an interruption of operation. Pathology of the specimen found a pheochromocytoma. Our patient denied a history of dizziness, sweating, and palpitations during micturition. Hormonal evaluation showed a normal level of both plasmatic and urinary metanephrine and normetanephrine. Metastatic workup was negative. Both adrenal glands were normal at CT. MIBG scan showed an increased localized activity in the bladder. After preoperative stabilization of hypertension and medical preparation, a complete transurethral resection of the tumor was performed. This case was discussed at a tumor board meeting and surveillance was decided. The patient has been disease‐free for 9 months.
Conclusions: In patients with unusual, striking symptoms and an increase in blood pressure with micturition, diagnosis of pheochromocytoma of the urinary bladder must be considered. Imaging will help in confirming the diagnosis and localizing the tumor. Surgical removal is the treatment of choice.
Prolonged Warm Ischemic Time is a Significant Risk Factor of Hemorrhagic Complication in Patients who Received Robotic Assisted Partial Nephrectomy
C Tsai, H Chung, E Huang, T Lin, T Huang, W Huang
Introduction & Objective: The most frequent and potentially life‐threatening events associated with partial nephrectomy (PN) are hemorrhagic complications (HC). The aim of this study was to analysis the risk factors of HC in patients who received robotic assisted partial nephrectomy (RAPN).
Methods: We retrospectively reviewed medical records of 260 patients who underwent RAPN between January 2010 and July 2018. Patient demographics, comorbidities, perioperative outcomes, and complications data were analyzed. HC was defined as bleeding, gross hematuria or arteriovenous fistula requiring blood transfusion or therapeutic intervention, which were divided as intraoperative, postoperative and delayed (after hospital discharge) bleeding. The severity of HC was graded according to the modified Clavien classification system. We investigated whether there is a relevant association between perioperative factors and HC.
Results: Of 260 patients included in this study, 32 (12.3%) patients had HC, which were intraoperative in 16 (6.2%), postoperative in 6 (2.3%) and delayed in 10 (3.8%). As classified by the modified Clavien system, HC were grade I in 2.3%, grade II in 6.5%, grade IIIa in 3.1% and grade IIIb in 0.4% of cases. No complication‐related deaths occurred. HC group had significantly more essential blood loss (712.5 ± 518.4 mL vs 229.6 ± 212.3 mL, P < 0.0001) and longer length of hospital stay (7.0 ± 2.2 days vs 5.6 ± 1.8 days, P < 0.0001). In univariate analysis, type 2 DM, RENAL score, prolonged console time (>180 minutes), prolonged warm ischemic time ( >25 minutes) and method of pedicle control were the statistically significant risk factors. In multivariate logistic regression analysis, warm ischemic time >25 minutes was the only significant risk factor for HC (OR, 3.51; 95% CI 1.28‐9.59; p = 0.01).
Conclusions: Patients who underwent RAPN with prolonged warm ischemic time ( > 25 minutes) correlated significantly with hemorrhagic complications and should be carefully monitored.
Patients experience and preference regarding subcutaneous venous thromboembolic prophylaxis following robotic assisted radical cystectomy
W Abou Chedid, GJ Nason, AT Evans, D Moschonas, MA Perry
Royal Surrey NHS Foundation Trust
Introduction & Objective: The European Association of Urology recommend post‐operative venous thromboembolic prophylaxis for 28 days for patients following radical cystectomy. Currently, subcutaneous low molecular weight heparin is the standard of care for prophylaxis. The aim of this study was to assess patients experience with dalteparin prophylaxis.
Methods: A telephone interview was performed of the last 100 patients who underwent a robotic assisted radical cystectomy at our center. These patients all received 28 days of dalteparin subcutaneously following discharge.
Results: 80 patients took part in our survey. 59 (73.8%) patients self‐administered, 16 (20%) had it administered by a family member and 5 (6.3%) required a daily visit by a district nurse. 31 (38.9%) patients reported no pain over the course, 22 (27.5%) mild pain, 18 (22.5%) moderate pain while 9 (11.3%) reported severe pain. 33 (41.3%) patients described some degree of bruising. 4 (5%) patients reported hematomas and 3 (3.8%) skin irritation. 4 (5%) patients described difficulty with injecting. 69 (86.3%) patients reported they would prefer an oral agent if possible. No patient developed a VTE by 90 days.
Conclusions: Patients who receive extended venous thromboembolic prophylaxis would prefer an oral agent to a subcutaneous injection if possible. A prospective multi‐center study for major urological surgery is required to establish the gold standard.
Analysis of the mid‐ and long‐term efficacy of suprapubic‐assisted laparoendoscopic single‐site nephroureterectomy
X Zou, c Chen, Z Guoxi, B qian, L Quanliang, X Tianpeng
Introduction & Objective: To evaluate the mid‐ and long‐term efficacy of suprapubic‐assisted laparoendoscopic single‐site nephroureterectomy(SA‐LESS NU) by comparing the postoperative cosmetic effects, complications, prognosis and the effects of operation on renal function and quality of life with laparoscopic nephroureterectomy(LNU).
Methods: The clinical data of 68 patients who underwent nephroureterectomy. 39 patients were performed SA‐LESS NU(study group) and 29 patients were performed LNU(control group). All patients were followed up by telephone, WeChat or other ways and returned to hospital regularly to review renal function, abdominal CT, and cystoscopy if necessary. All patients filled in the SF‐36 Quality of Life Scale (SF‐36) and Patient Scar Evaluation Questionnaire (PSAQ). The complications, survival status and tumor recurrence was recorded. The data obtained was performed statistical analysis.
Results: A total of 59 patients were fully followed up and included in the study, including 28 males and 7 females in the study group and 12 males and 12 females in the control group. The age was (64.49 ± 9.85)years old n the study group and (59.46 ± 10.12)years old in the control group(P = 0.062). The tumor diameter was (44.11 ± 14.52)mm in the study group and (40.25 ± 12.07)mm in the control group(P = 0.288). There was significant difference on the eGFR decrease before and after operation between the two group. The total PSAQ score of patients at 6 months, 12 months, 18 months, 24 months, 36 months and 48 months after surgery were 41.23 ± 8.86, 38.45 ± 6.90, 37.15 ± 5.89, 36.38 ± 5.33, 36.00 ± 4.05 and 34.00 ± 3.34 respectively in the study group, and 45.75 ± 6.96, 42.80 ± 5.76, 41.35 ± 5.18, 41.15 ± 4.34, 40.71 ± 4.46 and 39.67 ± 3.79 respectively in the control group. There were 7 patients with related complications in the middle and long term after operation, and the complication rate was 11.9%. In the control group, there was 1 case of abdominal incisional hernia and 4 cases of urinary tract infection. In terms of tumor prognosis, the OS at 1 and 3 years was 88.6%, 70.0% respectively in the study group and 83.3%, 66.7% respectively in the control group. The DSS at 1 and 3 years was 91.4%, 73.3% respectively in the study group and 87.5%, 72.2% respectively in the control group. The recurrence‐free survival at 1 and 3 years was 85.6%, 63.3% respectively in the study group and 83.3%, 61.1% respectively in the control group.
Conclusions: SA‐LESS NU can achieve the same effect as LNU in improving the prognosis in the middle and long term postoperative, without increasing the negative impact on renal function and patient's quality of life.
Retrograde en bloc resection for non‐muscle invasive bladder tumor can reduce the risk of seeding cancer cells into the peripheral circulation
H Huang, J Xing, K Zhang
The First Affiliated Hospital of Xiamen University
Introduction & Objective: To ascertain whether en bloc resection could reduce the risk of seeding cancer cells into the circulation during the resection of non‐muscle invasive bladder cancer (NMIBC).
Methods: Patients with primary NMIBC were enrolled in this prospective study from October 2017 to May 2018. Patients were allocated to receive conventional transurethral resection of the bladder (TURB) or retrograde en bloc resection technique of the bladder tumor (RERBT). The process of the RERBT technique was introduced briefly as follows. Blood vessels entering the tumor were blocked before resection by electro‐coagulating the macroscopic normal mucosa approximately 0.5 to 1.0 cm away from the tumor base to reduce intraoperative hemorrhaging. During the resection, bleeding vessels were coagulated simultaneously, providing a better visualization. Therefore, the time and degree of vascular opening was reduced and the opportunity for tumor cells to enter the bloodstream was kept to a minimum. Most importantly, the tumors were removed en bloc resection in RERBT rather than a piece‐by‐piece resection as in TURB; there was no tumor chip floating in the bladder during the resection. We employed a new device, a size‐dictated immunocapture chip (SDI‐Chip), to measure the CTC counts(Fig 1). Blood samples (1 ml) for circulating tumor cell (CTC) enumeration were drawn from the peripheral vein prior to resection (PV1), immediately after resection of the tumor base (PV2) and at 12 hours after resection (PV3). Intra‐group comparisons of the changes in the number of CTCs identified among the PV1, PV2 and PV3 blood samples were performed in each group.
Results: A total of 21 patients (12 in the RERBT group and 9 in the TURB group) were recruited. There were no statistically significant differences in terms of demographics, smoking history, operation duration, postoperative tumor grade or stage (Table 1). For patients receiving TURB, the level of CTCs identified in PV3 was significantly higher than that in PV1 (p = 0.047). However, there was no significant difference in CTC counts before and after resection in the RERBT group.
Conclusions: RERBT did not increase the number of tumor cells in the bloodstream.
Minimally invasive retroperitoneal Adrenalectomy in oligometastatic disease recurrence post nephrectomy ‐ a safe and feasible approach
D Sri, S Sarkar, J Oakley, M Malki, M Hussain, NJ Barber
Introduction & Objective: Adrenal recurrence post radical nephrectomy for renal cell cancer (RCC) is comparatively rare and in most surgically treated cases the transperitoneal approach appears to be standard of care. We explore the role and feasibility of minimally invasive (laparoscopic/robotic) retroperitoneal adrenalectomy in this challenging group of patients with solitary or oligometastatic disease and their long term oncological outcome at a tertiary robotic referral centre for RCC
Methods: : From a prospectively collected database of 73 minimally invasive retroperitoneal adrenalectomy cases (2006 – 2020), 14 patients underwent adrenal metastectomy for renal cell cancer (RCC). Five of these patients had undergone prior ipsilateral adrenalectomy with no adrenal involvement identified. We utilise a 3 port laparoscopic / 4 port robotic approach in our practice to retroperitoneal adrenalectomy. Patient demographics including age, BMI, ASA grade were analysed. Intraoperative data including operative time, estimated blood loss (EBL), post‐operative pathology and complications were assessed. Local and distant recurrence rates, and cancer free survival were our primary oncological outcome measures.
Results: Of the 14 patients, 10 (71%) developed contralateral adrenal metastases. Median time to adrenal metastasis was 50.9 months post radical nephrectomy (range of 8.1 to 133.3 months). We saw an even split of 7 cases each between the robotic and laparoscopic approach, with a mean operative time of 144 mins. Our intraoperative complication rate is low with one patient (7%) sustaining significant bleeding resulting in conversion to open surgery. The median blood loss in our cohort in 37.5mls. Our median length of stay is 1 day and we did not have any post‐operative complications or re‐admissions. Over a mean follow up of 42.7 months (range 1.3 – 110 months), we had 3 recurrences post adrenalectomy giving an overall recurrence rate of 21%, with a mean time to recurrence of 27 months. One patient had local recurrence whilst the remainder developed distant metastatic disease. Our cancer specific survival at 1 year was 100% and at 10 years post operatively was 85.7%.
Conclusions: We demonstrate that minimally invasive retroperitoneal adrenalectomy is technically feasible and oncologically safe irrespective of prior surgery. The oncological outcomes in selected patients has been demonstrated to be good, and these cases should be discussed at MDT level, with operative options considered in those with oligometastatic disease who are fit for surgery.
Withdrawn
En‐bloc versus conventional transurethral resection of bladder tumors: interim analysis of a single‐center prospective randomized trial
P Diana, M Fontana, A Territo, A Gallioli, A Piana, A Mercade', F Algaba, O Rodriguez Faba, JM Gaya, J Palou, A Breda
Department of Urology, Fundació Puigvert, Barcelona, Spain
Introduction & Objective: Transurethral resection of bladder tumor (TURBT) is considered the gold standard in the diagnosis and risk stratification bladder cancer (BC). En‐bloc resection of bladder tumor (ERBT) has been proposed to improve resection quality. Recently, the International Collaborative Consensus Statement on ERBT underlined the lack of high‐quality prospective studies precluding the achievement of solid conclusion on ERBT. The aim of this study is to compare TURBT and ERBT in terms of pathological diagnosis, surgical, and oncological outcomes.
Methods: This study is an ongoing, prospective, randomized trial enrolling patients diagnosed with BC and undergoing endoscopic intervention. Inclusion criteria were with tumor size of <3 cm, and ≤3 lesions, and no sign of muscle invasion and/or ureteral involvement. The primary outcome is the staging of BC. Secondary outcomes included T1 substaging (microstaging systems T1a/b/c), intraoperative complications, rate of adjuvant treatment, postoperative complications, oncologic outcomes. A total of 300 subjects will be included in the study with 1:1.5 treatment allocation for ERBT. The trial (NCT04712201) was approved by the Institutional Review Board (2017/09c).
Results: From 03/2018 to 01/2020, 180 patients met inclusion criteria and 158 (87.8%) of these were underwent the assigned intervention. 64 (40.5%) and 94 (59.5%) patients were submitted to TURBT and ERBT. Pre‐operatively, the populations were comparable. Table 1 shows the pathological results per lesion. The rate of Tx was comparable (3.4% TURBT vs 3.7% ERBT). T1 substaging was feasible in 80% TURBT vs 100% ERBT (p = 0.07). The rate of obturator nerve reflex and perforation were comparable (both p = 0.3). Adjuvant treatment was planned in 84% and 94% in TURBT and ERBT (p = 0.1). Clavien‐Dindo >2 complications were 5.3% vs 3.1% for TURBT and ERBT. Surgical, irrigation, and catheterization time were all comparable (all p > 0.2). Recurrence at 3 months was 3.1% vs 2.1% in TURBT and ERBT (p = 0.7).
Conclusions: According to our interim analysis ERBT and TURBT have comparable results in terms pathological, surgical, and oncological outcomes, while ERBT shows a tendency to significance in T1 substaging feasibility. This is the first randomized study in this setting and it is warranted to define the role of ERBT.
Management of the Adrenal Incidentaloma and Evaluation of Mass Size Alone as an Indication for Adrenalectomy: Our Experience
M Gabriel, O Prankerd ‐ Smith, J Saada, N Burgess
Norfolk & Norwich University Hospital
Introduction & Objective: The prevalence of adrenal incidentalomas (AI) is estimated to be 4% on computed tomography (CT) scans and most of these lesions are benign (85%). Current guidelines recommend surgical intervention for adrenal lesions which have either a diameter greater than 40 mm or are hormonally active or demonstrate suspicious features. We present a 19‐year review of patients undergoing adrenalectomy for incidental adrenal masses and consider whether we should continue to remove based on size alone?
Methods: Patients were identified retrospectively from hospital records between 2001 and 2020. Adrenal incidentalomas (AI) were defined as any adrenal lesion >10 mm in the absence of known malignancy or symptomatic adrenal disease found on imaging. All patients had biochemical and clinical assessment with multidisciplinary team (MDT) discussion.
Results: 179 patients underwent laparoscopic adrenalectomy and 11 (6%) were converted to open from 2001 ‐ 2020. Mean patient age was 58 years and male to female ratio 1:1.18. A total of 54 (31%) adrenalectomies were performed for adrenal incidentalomas (AI). Mean mass size on histology were 44 mm (range 13 to 90 mm). Pathology of all AI revealed adenoma (42%), benign pheochromocytoma (36%), nodular cortical hyperplasia (6%), cortical cyst (8%), adrenal carcinoma (2%) and ‘other’ (14%). 19 (35%) adrenal incidentalomas were removed for the indication of lesion size alone and all were benign on histology.
Conclusions: Adrenal incidentalomas are increasingly common and the decision for surgery should be based on clinical, imaging and biochemical assessment. All patients should be discussed in MDT with the involvement of endocrinologists, urologists, and radiologists. In our population surgical intervention based solely on the current size threshold of 40 mm, in the context of a non‐functioning indeterminate adrenal incidentaloma, did not identify any additional cases of malignancy, thus the potential benefit of surgery may not outweigh the risks to patients. We therefore conclude that re‐evaluation of the mass size threshold is warranted.
Paraganglioma of the Organ of Zuckerkandl: laparoscopic resection via a transmesocolonic approach
SE Clements, FX Keeley
North Bristol NHS Trust
Introduction & Objective: Paragangliomas are uncommon neuroendocrine neoplasms occurring in characteristic locations. Below the neck, the most common location for these tumours is in the adrenal glands. Rarely, these tumours arise from extra adrenal locations. We present the case of a young man presenting with nonspecific symptoms and his subsequent diagnosis with a paraganglioma at the Organ of Zuckerkandl. We discuss the identification, resection, and the physiological impact of this tumour. While existing case reports discuss the perioperative management of these tumours, we go further to highlight the surgical approach used and discuss the need for a risk stratification tool to guide follow up.
Methods: A 38 year old man presented with persistent diarrhoea. A computed tomography (CT) scan showed a 3 cm mass anterior to the bifurcation of the aorta. Meta‐iodobenzylguanidine (MIBG) scintigraphy showed neuroendocrine activity at this location. Urine and plasma metanephrines were within normal limits. We carried out a laparoscopic resection of the tumour with the patient in the right lateral recumbent position using a transmesocolonic approach to access the retroperitoneal space.
Results: The paraganglioma was resected with clear margins and histology demonstrated low risk of metastatic disease with a Ki‐67 of <1% and no staining indicating SDHB loss. The patient made a good post operative recovery. At the most recent follow up, he reported experiencing retrograde ejaculation. The patient has been referred to a clinical geneticist.
Conclusions: The right lateral recumbent position provided an optimal view of the tumour. Resection in this way is more time efficient than reflecting the colon and provides optimal views for removal of a tumour at this location.
Eleven years of experience with UTUC: survival and renal function after kidney sparing surgery versus radical nephroureterectomy
N Hendriks, J Baard, HP Beerlage, BM Schout, RC Pelger, KS Doherty, GM Kamphuis
Amsterdam UMC
Introduction & Objective: The gold standard treatment for upper urinary tract urothelial carcinoma (UTUC) is by radical nephroureterectomy (RNU). Criteria to qualify for kidney sparing surgery (KSS) have become less strict in consecutive guidelines, thereby gaining a more prominent position. In this study we compare the oncological outcomes and renal function in patients with UTUC treated by KSS and RNU in a tertiary referral center.
Methods: In this retrospective cohort study, we included 174 adult patients with histopathological confirmed non‐metastatic UTUC from 2010 through 2020 treated with either RNU or KSS (segmental ureter resection, ureterorenoscopy, percutaneous tumor resection). Risk stratification was based on the current EAU guidelines for UTUC.
Results: The RNU arm had a larger population (86.2%) of high risk tumors compared to the KSS arm (74.4%; p = 0.030). Recurrence Free Survival (RFS), Metastasis Free Survival (MFS), Overall Survival (OS) and Cancer Specific Survival (CSS) concerning KSS and RNU are presented in figure 1. Within the high risk KSS arm 73.2% did not have an imperative reason for choice of treatment. MFS (p = 0.004), CSS (p = 0.027) and OS (p = 0.033) were all significantly higher in the KSS arm when comparing high risk patients in both treatment groups (figure 2). There were no significant long‐term differences in renal function, except for three months and one year after intervention (figure 3).
Conclusions: Current guidelines indicate that high risk UTUC is best treated by RNU. In this study we conclude that MFS, CSS and OS are significantly higher in KSS in all tumors as well as in high risk tumors treated outside the scope of current guidelines.
Endoscopic Submucosal Injection of a Human Amniotic Membrane Bioegenerative Matrix for the Management of Recalcitrant Bladder Neck Contractures
J Kuo, N Velazquez, B Desroches, R Munver
Hackensack Meridian School of Medicine
Introduction & Objective: The management of bladder neck contractures (BNC) with injectable therapeutic agents after prior incision or resection has been primarily limited to mitomycin and steroid injection. Both mitomycin and steroids have not consistently demonstrated prevention of BNC recurrence, with steroids only having been shown to have an effect in delaying BNC recurrence. Herein, we present a series of recalcitrant BNCs that previously failed prior therapies and were subsequently managed endoscopically with a novel amniotic membrane and umbilical cord injectable bioregenerative matrix agent, Clarix Flo (Amniox Medical, Inc.), which reduces inflammation and promotes healing.
Methods: Five men with prostate cancer developed BNC from: 1) salvage external beam radiation therapy (XRT) following robot‐assisted radical prostatectomy (RARP) (n = 3); 2) anastomotic urine leak after RARP (n = 1), 3) after primary XRT for prostate cancer (n = 1). Mean age was 67 years (range: 57‐81). Patient cancer staging included: 3C, Gleason 4 + 5 (n = 1), 3B, Gleason 4 + 3 (n = 1), 3B, Gleason 4 + 4 (n = 2), and prostate cancer of unknown stage (n = 1). All patients were managed initially with direct vision internal urethrotomy (DVIU) or transurethral resection of bladder neck (TURBN) with steroid injection therapy, and then developed BNC recurrence. One patient had 2 previous TURBNs, 3 patients had 1 previous DVIU or TURBN, and 1 patient had 3 previous endoscopic surgeries for the treatment of BNC. All patients subsequently underwent TURBN or DVIU at time of circumferential injection of 100 mg of Clarix Flo. Postoperative urethral catheters were removed in 1 week.
Results: At a median follow‐up of 12 months, no patients developed BNC recurrence nor required repeat catheterization or urethral calibration. All patients continue to void with a steady stream without retention of urine. On longest follow‐up, at 17 months, the patient remains without bladder neck contracture recurrence and continues to void without complaints. All patients are continent of urine with 4 patients using no pads and 1 patient using 1 liner daily. Follow‐up cystoscopy on all patients at 6 and 12 months postoperatively demonstrated an open bladder neck that accommodated a 16F flexible cystoscope.
Conclusions: The use of an amniotic membrane and umbilical cord regenerative matrix agent adds to the armamentarium of injectable therapeutic agents for the management of bladder neck contractures. The long‐term benefits of Clarix Flo in the management of BNC appears favorable as compared to other injectable agents.
Using a Natural Language Processing Program to Screen for Incidental Findings of Urolithiasis
J James, A Rai, L Richstone
The Smith Institute for Urology
Introduction & Objective: Incidental findings of renal pathologies have been rising with increasing use of radiological imaging. While urolithiasis is commonly reported in imaging reports as incidental findings, some uroliths are not clinically relevant while others may require future intervention. Natural language processing is the field of computer science, linguistics and artificial intelligence that enables the use of algorithms to interpret natural language text. We therefore sought out to create a search algorithm to identify these patients in the aim of quickly providing care to these patients.
Methods: Retrospectively, we screened for urolithiasis in computed tomography reports from a four‐week period at a tertiary academic center. We created a search algorithm leveraging Boolean expressions utilizing Nuance mPower Clinical Analytics, a natural language processing program. The goal of the search algorithm was to search every computed tomography radiology read performed at our institution and select for those studies with clinically significant urolithiasis (defined as stone size ≥2 mm). Radiology reports were then grouped by patient to avoid duplication.
Results: Using the natural language processing program, the CT reports of 1735 patients were screened for urolithiasis. Of the 1735 patients, 123 patients had verified clinically significant nephrolithiasis, while 1612 patients did not. The algorithm identified 115 patients potentially having stones. Of the 115 screened positive by the algorithm, 89 patients had true stones while 26 patients did not have stones. Of the 89 patients with stones identified by the algorithm, 68 patients had clinically relevant stones (≥ 2 mm). The sensitivity, specificity, positive predictive value, and negative predicative values of the search query for nephrolithiasis were 72% (89/123), 98% (1586/1612), 77% (89/115), and 98% (1586/1620), respectively.
Conclusions: As the rate of imaging and incidental findings arise, leveraging natural language processing may be a useful adjunct in quickly identifying multiple urologic conditions. Our data demonstrate that this search algorithm may be a potential adjunct to capture patients with incidental findings of urolithiasis from the moment the imaging is read by the radiologist. This search query may be used to automate a patient follow up system for lower acuity stones and triage patients with significant potentially problematic nephrolithiasis.
Video Session
Video Session 02: Laparoscopy‐ Miscellaneous
V02: laparoscopy‐ miscellaneous
JY Lee, R TP, A Rane
Withdrawn
Does 3D Facilitate Technique of Laparoscopy Pyeloplasty in Infant
R Manickam, S Kallappan, S Nachimuthu
Introduction & Objective: Laparoscopic pyeloplasty, especially suturing in infants can be challenging. With the advent of 3D camera it has become less challenging.
Methods: A 3 months old baby was referred with the history of antenatally detected PUJ obstruction. As the baby had repeated positive urine culture, though the baby was weighing 5.5 KG, after treating UTI we planned Laparoscopic pyeloplasty. By transperitoneal approach using 4 ports, left colon was reflected, upper ureter , pelvis were adequately mobilized and UPJ and a segment of pelvis was excised. Lateral spatulation of ureter was done. Pyelo‐ureteral anastomosis was done with 5‐0 Polydioxanone interrupted suture over 3 F double j stent . Tube drain was placed. Procedure was completed in 120 minutes.
Results: Postoperative period was uneventful. Total drainage was 75 ml over 72 hours. Foley catheter was removed on 2nd postoperative day and drain tube was removed in 3 days.
Conclusions: With the availability of 3D camera we are able to do laparoscopic pyeloplasty safely , more efficiently and comfortably even in infants.
Novel Hybrid Technique Of Laparoscopic Nipple Valve Reimplantation With Portsite Rirs Through Exteriorised Distal Ureter In Pom With Renal Calculus
R Manickam, S Kallappan, S Nachimuthu
Introduction & Objective: Laparoscopic Nipple valve ureteric reimplantation of ureter with portsite RIRS is a innovative minimally invasive management of renal calculus and Primary Obstructive Megaureter.
Methods: A 42 years old male, presented with 7 month history of left loin pain. CET scan of abdomen revelead 14 mm left upper calyceal calculus with primary obstrutive mega ureter. By a transperitonial approach using 4 ports lower ureter was disected and divided above level of obstruction. The ureter was brought out through the 10mm port in the left iliac fossa and flexi URS passed through the ureter and laser lithrotripsy was done. Nipple valve ureteric reimplantation was done. Procedure was completed in 160 minutes.
Results: Postoperetive period was uneventful. Foley catheter was removed 10th day, and stent was removed at the end of 4th week
Conclusions: Portsite RIRS during laparoscopic nipple valve reimplantation of ureter is a useful innovative minimally procudure.
Laparoscopic Nipple Valve Reimplantation In A Ureterocele Of a Crossed Fused Ectopic Moiety Unit ‐ Challenges
R Manickam, S Kallappan, S Nachimuthu
Introduction & Objective: Laparoscopic Nipple valve reimplantation in a ureterocele of a crossed fused ectopic moiety unit ‐ challenging procedure
Methods: 28 years old male patient was incidentlly found to have crossed fused ectopic right renal moiety with gross hydronephrosis and ureterocele on ultrasonogram. CT urogram confirmed the large ureterocele. The video illustrates the technical difficulties in laparoscopic dissection in hiatus and intravesical area. As distal ureter was very wide, after transfixing the distal end tailoring was done and nipple valve was created and stent was placed. The hiatus was closed and reimplantation was done in the right anterolateral aspect of bladder using 4‐0 polydioxanone as interrupted sutures.
Results: Drain tube was placed. Post operative period was uneventful. Patient discharged on 3rd postoperative day after removing drain. Cystoscopy and Ultrasound scan showed Nipple valve reimplant in Right side of dome.
Conclusions: Laparoscopic dissection of large intravesical urerocele before reimplantation though challenging is feasible and less morbid procedure.
Video Endoscopic Inguinal Lymphadenectomy: Step‐By‐Step Technique And Mid‐Term Oncological Outcomes
JM Gaya, A Rosales, A Gallioli, P Diana, P Gavrilov, A Territo, A Piana, A Sánchez‐Puy, J Calderón, H Vila‐Reyes, J Palou, A Breda
Introduction & Objective: Penile cancer is a rare disease which disseminates via lymphatic system in a sequential fashion. However, inguinal physical examination is challenging, where 50% of palpable nodes are pN0 and 25% of cN0 nodes are pN+. Moreover, imaging is not recommended by the EAU guidelines. Therefore, we should balance the risk of undertreatment, as N staging is the most important prognostic factor and lymphadenectomy might be curative, with the high morbidity (up to 75% of complications) of open inguinal lymphadenectomy. The aim of the study is to report our technique and outcomes in video endoscopic inguinal lymphadenectomy (VEIL) for penile cancer.
Methods: We retrospectively analyzed the Institutional database on VEIL for penile cancer from 2008 to 2020. Demographic variables, perioperative data, surgical and oncologic outcomes were analyzed. We present our technique of modified saphenous‐sparing VEIL. The patient is positioned in supine position, with 45‐degree hip abduction and 90‐degree knee flexion. The limits of the surgical field (the inguinal ligament, the sartorius and adductor longus muscles) are marked, as for the femoral artery. The working space is created by finger blunt dissection and gas pressure (12mmHg), under Camper's fascia and over the Scarpa Fascia. Two 5‐mm trocars are placed 8 cm from the camera port on the triangle lines. The saphenous vein, located at the roof of the surgical field, is identified and spared to decrease risk of limb edema. The dissection is 1‐2 cm above the inguinal ligament, on the cranial border of the surgical field. The lymph node dissection is started from the lateral attachment towards the pubic tubercle and completed at the sapheno‐femoral junction. To avoid lymphatic leakage, all the vessels should be ligated with titanium Ligaclip®. The node packet is then removed through the incision for camera port and a drainage is positioned through a 5‐mm port.
Results: A total of 52 VEILs were performed (22 bilateral, 8 monolateral) in 30 patients. Median operative time was 182 minutes (91 minutes per limb). Median lymph node excised per limb was 7 (26/365 pN+; 12/30 (40%) pN+ patients). 14/30 (46.7%) patients had postoperative complications. 4 (13.3%) patients had wound complications without skin necrosis. 10 (33%) patients developed lymphocele requiring percutaneous drainage in 9/10 cases (Clavien 3 complications). All patients that experienced local recurrence (10.5%) and distant metastasis (10.5%) at 2 years follow‐up were pN2/3.
Conclusions: VEIL is a safe and feasible technique. In tertiary referral centers, minimally invasive inguinal lymphadenectomy should be considered the gold standard approach.
Transperitoneal Laparoscopic Excision of Mullerian Duct Cyst
C Yogeswaran, K Ekwueme
Introduction & Objective: Mullerian duct cyst (MDC) is rare and present a challenge for diagnosis and treatment due to its location within the pelvis. MDC affects younger age group therefore less radical treatment options are often preferred but with high recurrence rate. Studies describing definitive treatments using minimally invasive techniques are lacking. In this video, we demonstrate a step‐by‐step transperitoneal laparoscopic excision of a MDC in a young adult.
Methods: 43‐year‐old Caucasian male presented with lower abdominal and groin pain associated with urinary urgency. Investigations including an ultrasound scan, CT and MRI scan confirmed an 8cm midline pelvic cyst consistent with MDC with left renal agenesis and normal bladder at flexible cystoscopy. Following counselling, patient opted for Transperineal aspiration as an initial treatment. The procedure was successful however the cyst recurred within 6 months. He elected for further aspiration, but the cyst recurred again within a few months at which point he was counselled and agreed for laparoscopic excision as a definitive treatment. A preoperative MRI Pelvis with sagittal views was performed for surgical planning. Rigid cystoscopy and right ureteric stent was performed in Lloyd Davies position to protect the solitary kidney and with catheter placement. The patient was then placed supine in 30 degrees Trendelenburg position. A 4‐port laparoscopic technique was used (12mm midline supraumbilical camera port, 3x10mm ports; 1 – suprapubic, 2 – halfway between anterior‐superior iliac spine and umbilicus on both sides). The MDC was identified posterior to bladder. Posterior peritoneum was opened at the pouch of Douglas and superiorly at boundary with bladder enabling en bloc dissection of the cyst down to the base of the prostate between the seminal vesicles and excised. A pelvic drain was inserted post resection.
Results: The patient made an unremarkable postop recovery. Drain was removed on day 2 post op and patient discharged. At 3 months review, the patient had made excellent recovery without any symptom. Final histology confirmed a benign cyst consistent with MDC. Subsequent follow up CT scan at 12 months revealed no further recurrence of the cyst.
Conclusions: Transperitoneal Laparoscopic excision of MDC is feasible. It offers a minimally invasive definitive surgical treatment option for patients with good outcomes.
The Goyri‐O'Neill perfusion technique of cadaveric embalming: a novel approach to advanced laparoscopic surgical training
T Ribeiro de Oliveira, N Domingues, A Palmas, S Biyani, D Pais, J Goyri‐O'Neill
Introduction & Objective: Over the past decades, laparoscopy has become the standard surgical approach for many urological conditions. However, due to the steep learning curve, achieving proficiency in laparoscopic surgery requires considerable training. Given the obvious ethical concerns with patient safety, it is recommended that urologists achieve a certain level of expertise before performing procedures on patients. In line with these concerns, several artificial models have been developed for basic and intermediate laparoscopic training. Nevertheless, there is still no consensus on the best model to train advanced laparoscopic skills. The Goyri‐O'Neill perfusion technique (GOPT) is a novel technique of cadaveric embalming, that avoids the use of formol and provides specimens with optimal anatomical landmarks and realistic tissue characteristics, making it ideal for surgical training. We present a video of several advanced laparoscopic urological procedures performed in cadaveric models prepared with the GOPT.
Methods: Cadaveric specimens were provided by the Nova Medical School Department of Anatomy, from the voluntary Body Donation to Science program, after the mandatory informed consent was obtained, in accordance to the previously designed protocol approved by the National Committee for the Sciences of Life and in line with the principles of the Declaration of Helsinki.
Results: The GOPT cadaveric model was tested for its applicability in advanced laparoscopic skills training, using several laparoscopic urological procedures, including both the upper and lower urinary tract. Procedures were performed during three editions of a 3‐day advanced laparoscopic skills course, both by experts (performed >50 laparoscopic procedures) and non‐experts (performed ≤50 laparoscopic procedures). The following laparoscopic procedures of the upper urinary tract were performed: pyeloplasty, adrenalectomy, partial nephrectomy, radical nephrectomy and retroperitoneal lymph node dissection. The following laparoscopic procedures of the lower urinary tract were performed: radical cystectomy (both in male and female specimens), radical prostatectomy and pelvic lymph node dissection.
Conclusions: The GOPT of cadaveric embalming is a novel approach to cadaveric specimen preservation that provides optimal tissue structure and organ anatomy, making it the ideal model for advanced laparoscopic surgical training.
Bilateral uterosacral ligament replacement ‐ laparoscopic uterosacropexy (laUSA) with minimal use of material and uterus preservation
S Ludwig, B Morgenstern, P Mallmann
Introduction: Prolapse of the uterus in premenopausal women is a concerning condition and therapeutic options are limited especially if uterine preservation is demanded.
Objective: We present a newly developed laparoscopic surgical technique to restore apical suspension in case of uterine preservation. A curved tunneling device was used to replace both uterosacral‐ligaments (USL) and, thereby, the peritoneum's integrity was preserved while a minimum amount of alloplastic tape (polyvinylidene‐fluoride, PVDF) was used.
Methods: Women with apical prolapse and urinary incontinence were referred to our tertiary unit. The patients have failed or declined conservative management none of them had undergone previous urogynecological surgery. For the laparoscopic uterosacropexy:
1. The bladder was identified on the anterior cervix and their peritoneum was incised laterally until the left and right uterine vessels were displayed. The space lateral to these vessels was prepared blunt.
2. The peritoneum over the promontory was incised for 2 cm on the right side of the rectosigmoid colon in order to prepare both lateral margins of the promontory for posterior fixation;
3. For USL replacement, a PVDF‐structure of 9.3 cm in length and 4 mm in width was used. A semi‐circular curved hook was used for insertion.
4. The semi‐circular tunneler was inserted via the right lateral trocar incision. In order to tunnel the left USL, the rectosigmoid was undertunneld and the tunneler's blunt tip was slightly forwarded under the peritoneum along the run of the left USL toward the cervix, paracervical. The lateral end of the PVDF‐structure was threaded through the hole of the tunneler's tip, and then carefully pulled back. Same was done to tunnel the right USL.
5. The central fixation part of the PVDF‐structure was sutured horizontally to the anterior cervix by using 2 interrupted nonabsorbable sutures.
6. Each arm of the PVDF‐structure was attached (at the allocated mark) with 3 titanium helices to the right and left lateral prevertebral fascia of S1/promontory by using a fixation device.
Results: Apical support was restored in all 10 patients. No intraoperative complications like major vessel or ureter injury and bowel or bladder lesions occurred. Blood loss was less than 20ml per patient. Within follow‐up of 6 months no mesh erosions or relapse of original prolapse were detected.
Conclusions: Restoration of apical prolapse under uterine preservation was achieved by bilateral USL replacement. This was technically achieved using a semi‐circular tunneling device in order to preserve the integrity of the USL, uterus, and uterine vessels with a minimum amount of alloplastic material.
Laparoscopic single‐port varicocelectomy with the single‐channel fabric device (LEVD): A medium‐term follow‐up
M Roslan, M Przudzik, M Borowik, R Liss, M Łesiów, G Gronowicz, J Wójtowicz
Introduction & Objective: Varicocele constitutes a significant abnormality in young men that may be a causative factor for infertility or chronic scrotal pain. It may also be an esthetic problem. The standard treatment includes open or laparoscopic spermatic vein ligation, with excellent results. Nevertheless, the common tendency to minimize surgical approaches has gained varicocelectomy as well. One of the latest concepts is the Laparoscopic Single‐channel Varicocele Dissection (LEVD). Here we present our three‐year experience with this technique.
Methods: From April 2017 to February 2021, we carried out LEVD procedures in 20 males of mean age 30.7 (range 22–40) suffering from infertility or scrotal pain. We used the fabric kit (LEVD, Wolf, Tuttlingen, Germany) that consists of a 5.5 mm trocar, a 3.5 mm optic and appropriately designed working instruments (dissector, monopolar forceps and scissors) and was introduced via a 4‐mm skin incision in the umbilicus. The spermatic vein was dissected, coagulated and cut. No drainage was needed. We assessed operative and hospitalization times, as well as safety and effectiveness of the method.
Results: All patients were operated on successfully, with no complications or extra port insertion. The blood loss was minimal. The mean operative time was 15.9min (range 7–38). The patients were discharged within 10.4 (range 5–24) hours of surgery. During a mean 18‐month follow‐up (range 1–45 months) 19 patients reported significant release of symptoms and three patients became fathers. No hydrocele was observed. In one patient a recurrent varicocele was managed with standard laparoscopy
Conclusions: The LEVD procedure is a safe and effective option for spermatic vein ligation because of its minimal invasiveness, short hospital stay and fast recovery time. It seems to reduce the surgical trauma and provide a “scarless” method. Nevertheless, further observations and comparisons with standard laparoscopy are needed.
Video Session 03: Transurethral Surgery: Prostate and Bladder Neck
V03: transurethral surgery: prostate and bladder neck
S De, T Large, MS Agrawal
Withdrawn
Holmium Laser Enucleation of the Prostate after Greenlight Photoselective Vaporization of the Prostate
KH Thai, M El Tayeb
Introduction & Objective: Greenlight Photoselective Vaporization of the Prostate (PVP) is a common procedure for BPH management. However, studies have shown that patients who undergo Greenlight PVP are at risk for recurrent obstructing prostate adenoma1. In the last 20 years, the Holmium Enucleation of the Prostate (HoLEP) has emerged as a comparable alternative for BPH surgery. HoLEP has demonstrated to require fewer reoperations than some alternative therapies1. Thus, our goal is to show the safety and technique of HoLEP on a patient who has recurrent obstructing prostate adenoma post‐Greenlight PVP.
Methods: Our index patient is a 60‐year‐old male who had undergone Greenlight PVP three years prior. He represented with recurrent lower urinary tract symptoms. Evaluation demonstrated left lateral lobe prostatic regrowth. The patient elected to undergo HoLEP.
Results: In our video, our patient had significant adhesions within the prostate that made enucleation with the holmium laser challenging. With his prior Greenlight PVP, the patient developed adhesions in nodules that infiltrated the capsule, as well as distorted anatomy. The success of the surgery was dependent on identifying landmarks, avoidance of excessive force, and patience by the surgeon.
Conclusions: It is essential for a surgeon to understand the distorted anatomy, identify landmarks, and have patience while performing the HoLEP on patients who have previously had transurethral prostate surgery. Patients who have had prior Greenlight PVP can successfully undergo a HoLEP for recurrent obstructing prostate adenoma.
Tips and Tricks of Morcellation
JC Smith, M El Tayeb
Introduction & Objective: Morcellation is a crucial step in the process of performing a Holmium Laser Enucleation of the Prostate (HoLEP). Morcellation typically is straightforward, but it can be cumbersome. Troubleshooting the device and knowing techniques to assist difficult morcellations can help mitigate obstacles that are occasionally encountered.
Methods: We compile a list of steps to troubleshoot the morcellator and suction device during difficult morcellation. In the process of discussing morcellation tricks, we describe a patient with 225‐gram prostate and a history of high intensity focused ultrasound therapy for prostate cancer who developed significant lower urinary tract symptoms refractory to other therapies. This patient was taken to the operating room for a HoLEP, and due to the previous therapy, his tissue was dense and challenging to morcellate. We utilize all stated tricks to help with his morcellation
Results: When evaluating for poor morcellation, start with ensuring the suction is adequate by priming the suction tubing, checking the suction switch seal, and removing any prostate tissue clogging the apparatus. When dealing with tissue that is not engaging the morcellator, you can reduce the morcellation speed to 800 rpms, morcellate in the prostate fossa if small, or laser the enucleated prostate tissue to create edges that improve engagement with the blades.
Conclusions: When dealing with difficult morcellations, having techniques to manage the situation can be an asset to your operative armamentarium.
Cystolitholapaxy during Holmium Laser Ablation of the Prostate: Dual Utilization of the Side Fire Laser Fiber
BB Whiles, KL Thurmon
Introduction & Objective: Benign prostatic hyperplasia (BPH) is a predominate cause for lower urinary tract symptoms (LUTS) in aging men. Prolonged outlet obstruction can lead to poor bladder emptying and ultimately to the formation of bladder stones. When recurrent bladder calculi occur, it is recommended by the American Urological Association's BPH surgical management guidelines that we perform a bladder outlet relief procedure as well as treat the bladder stones. In patients planning for holmium laser ablation of the prostate (HoLAP) with concurrent bladder calculi, we hypothesized that we could utilize the same side fire holmium laser fiber for both the HoLAP as well as the cystolitholapaxy.
Methods: This is a descriptive case report demonstrating our experience utilizing the Xpeeda 550‐micron side fire holmium laser fiber for the treatment of bladder stones followed by HoLAP with the same fiber. The specific steps, materials, and intraoperative findings are described in one patient who underwent this procedure.
Results: The patient is a 56‐year‐old male with bothersome LUTS and bladder stones measuring >5cm in total stone burden. He was counseled in our clinic regarding possible management options and ultimately opted for HoLAP and cystolitholapaxy. The patient was prepped and draped in the dorsal lithotomy position. The 550‐micron side fire holmium laser fiber was inserted and utilized to dust the large bladder stones. The most effective setting was 2J, 50Hz. However, once the stones were small in size, we noted that less energy was more efficient, so 0.4J, 50Hz was utilized. All bladder stones were treated in 32 minutes with use of 7.42 kJ of energy. Routine HoLAP then occurred in an uncomplicated fashion, requiring 40 minutes and 142.4kJ of energy. There were no complications intraoperatively or in the immediate post‐operative period.
Conclusions: Cystolitholapaxy followed by HoLAP with the same side fire holmium laser fiber is both safe and effective. Dual utilization of this fiber can clinically translate into significant cost savings, as the typical end fire 1000‐micron holmium laser fiber for bladder stone treatment costs around $700 USD.
What to do When Unable to Reach the Bladder During Holmium Laser Enuncleation of the Prostate (HoLEP): An Incision‐Free Approach
DK Agarwal, ME Rivera
Introduction & Objective: The situation of not being able to reach the bladder during HoLEP is a rare situation. Currently, this situation requires some external incision (temporary perineal urethrostomy (PU) or conversion to open/MIS simple prostatectomy) which requires additional catheterization time. We present an alternative, incision‐free technique for this situation to complete HoLEP transurethrally.
Methods: We present a case of HoLEP in a 73 year old male with a 225 ml gland on preoperative imaging in which the laser scope could not reach the bladder due to urethral length. We utilized the early apical release technique, and dissected to the bladder through the anterior plane. As this is the shortest distance across the prostate to the bladder endoscopically, we were able to reach the bladder anteriorly and complete the HoLEP without additional incisions. This also enabled us to perform catheter removal promptly after surgery.
Results: The total procedure time was 146 minutes, enucleation time was 97 minutes and morcellation time was 24 minutes. All of the 199 grams of enucleated tissue was benign adenoma on final pathology. In the 15 minutes between procedure end time and extubation, continuous bladder irrigation was run through a 22 french three‐way urinary catheter. The catheter was removed prior to extubation and the patient voided within 2 hours. At two week follow‐up, the patient was voiding without issue, having only minimal stress urinary incontinence, and no hematuria.
Conclusions: We propose the technique of first following anterior plane to the bladder after early apical release as an when the laser scope cannot reach the bladder transurethrally at the time of HoLEP. The shorter distance of the anterior plane from the apex of the prostate to the bladder neck, opposed the longer distance through the urethral lumen is the likely reason for the success of this approach. This anterior‐first technique may avoid external incisions and prolonged catheter time from a temporary PU or open/MIS prostate enucleation in these rare cases.
Design and Development of a Physical Simulation Platform for Holmium Laser Enucleation of the Prostate (HoLEP) using Expert Consensus
P Saba, R Melnyk, K Cameron, S Quarrier, N Gopal, MR Humphreys, AE Krambeck, NL Miller, RK Jain, A Ghazi
Introduction & Objective: HoLEP is an underutilized, minimally invasive approach for the management of benign prostatic hyperplasia (BPH). The steep learning curve and lack of simulation platforms with incorporated objective metrics has hindered its adoption. Despite the steady increase in the number of procedures, only 4% of the surgeries performed for BPH utilize HoLEP. We sought to design and fabricate a high‐fidelity, non‐biohazardous hydrogel platform based on expert consensus feedback.
Methods: The Delphi method was used to gain consensus from a panel of 6 endourologists. 250 questions were asked across 4 categories to optimize a simulation platform for training and evaluating the procedure. The consensus defined 81 elements covering: overall utility, anatomical and procedural components, tissue fidelity, and performance evaluation. The goal was to create a safe environment to bridge the gap between the classroom and live surgery while also providing trainee performance metrics. The model was required to incorporate realistic tissue texture, bleeding, and be able to replicate different anatomical variations all within an enclosed fluid management system for portability and safety.
Operable interchangeable hydrogel components were registered into a 3D printed housing that was created to allow for easy setup and anatomical variations. The hydrogel components were created using negative molds which were 3D printed and sequentially filled with mechanically tested hydrogel mixtures to mimic the intended tissue properties. The simulation was completed by an expert endourologist in a standard operating room with all necessary instrumentation and a recording was reviewed by the original panel to confirm fulfillment of the consensus.
Results: The platform fulfilled 78% of the elements, meeting 82% of overall utility, 78% of anatomical and procedural components, 73% of tissue fidelity and 82% of assessment requirements. The platform contained all 9 anatomic components, 7 evaluation metrics and 5 procedural steps except for hemostasis and morcellation. All experts agreed the platform: could provide a safe training alternative, be used to evaluate trainee performance, and trial new approaches in a risk‐free environment.
Conclusions: This is the first consensus‐based approach to design and fabricate a hydrogel HoLEP simulation platform with incorporated evaluation metrics. Further development will include morcellation and bleeding to prepare for the next phase of validation prior to incorporation into training environments.
Thulium Laser Prostatectomy In High Risk Patients With Benign Enlargement Of Prostate
VK Poleboyina, V Akinapally, M Khan
Introduction & Objective: Thulium Laser Prostate Enucleation methods have emerged as one of the Prime modalities for the surgical treatment of Benign Enlargement of Prostate. The Aim of the study is to assess the Safety and Efficacy of the modality in high Risk individuals with BPH.
Methods: This is a retrospective analysis of 58 high risk patients who underwent Thulium laser prostatectomy at Care hospital, Hyderabad , India between December 2017 and January 2020. High risk patients included were those who were On Anticoagulation Therapy, patients with Cardiac Rhythm Abnormalities and with Intra Cardiac Devices(ICD), patients with Severe Heart Failure (EF <35%), Coronary Artery Disease(CAD) patients, patients Post CABG/PTCA or Both. Patients With Multiple Comorbities Like CVA, COPD, CKD, DM, HTN, Bronchial Asthma were also included.
Results: Overall, the IPSS(21.2 to 3.6), maximum flow rate (Qmax ‐ 9.6ml/s to 31.2ml/s), significantly improved after the procedure. Of the 58 patients two patients required reintervention in the immediate postoperative period ‐ one for Staged Morcellation due to poor vision and another for clot evacuation after two weeks post surgery. One patient had transient stress urinary incontinence. None had significant peri operative (Modified Clavian Dildo Classification) complications.
Conclusions: Thulium Laser Prostatectomy is safe and effective in the surgical treatment of Symptomatic BPH in High Risk individuals . More Studies are required as this is a retrospective analysis.
Thulium Laser Prostate Surgery Using Slender Resectoscopes – Impact on Post Operative Urethral Stricture
VK Poleboyina, V Akinapally, M Khan
Introduction & Objective: Various studies have shown around 1‐5% incidence of Post TURP Urethral Strictures. One of the risk factors for this is the sIze of the Resectoscope. We studied the Use of Thulium laser for Surgical treatment of Benign enlargement of Prostate through a slender resectoscope (22.5 f) or an Integrated Cystoscope (17 F0 and its impact on the incidence of Urethral stricture.
Methods: A retrospective analysis of 64 patients who underwent Thulium laser prostate intervention at Care Hospitals, Hyderabad, India, between January 2018 and January 2019 was performed. Techniques used were‐3 Lobe Enucleation,2 Lobe Enucleation, Median Lobe Enucleation And Vaporisation, and Bladder Neck Incision. Resectoscope size‐22.5 Fr or a 17 Fr Integrated Cystoscope for BNI. Laser used was continuous firing Thulium YAG at 60 watt. Average gland size was 44.5g(22g ‐ 56.5g).
Results: Patients were followed upto one year at 3 monthly intervals using IPSS score, Uroflowmetry anf Ulttasound measurement of Post void residual urine.all the parameters improved and consistently maintained during the period of the study. None of the patients developed Urethral obstruction or any other significant complication.
Conclusions: Use of finer/slender resectoscopes which is possible because of Thulium Laser, for the Surgical treatment of BPH, may lower the incidence of Post Operative Urethral Stricture. More Studies are needed for confirmation.
Endoscopic Enucleation of a 180g Prostate with 30W Thulium Fibre Laser
VK Poleboyina, M Khan
Introduction & Objective: Endoscopic Enucleation of Prostate (EEP) is evolving day by day. Thulium Fibre Laser(TFL) is the latest entrant in the gamut of lasers for performing EEP. There are few studies showing use of a 30W TFL for this purpose. We hereby present our data of use of 30W TFL for EEP along with a video of a patient with 180 g prostate
Methods: A retrospective analysis of 45 patients who underwent Thulium Fibre Laser prostate surgery at Care Hospitals, Hyderabad, India, between October 2020 and December 2020 was performed. Techniques used were‐3 Lobe Enucleation,2 Lobe Enucleation, Median Lobe Enucleation And Vaporisation, and Bladder Neck Incision. A 400 micron fibre was used which was comparatively better compared to a 600 micron fibre to deliver 30 W power at Continuous Wave mode.
Results: Overall, the improvement in IPSS(drop by 18 points) and maximum flow rate (Qmax ‐ 15ml/s) was significant. The Mean operative time(45min) , catheterisation time(29 hours), were comparable to Thulium YAG and other Endoscopic Enucleation Techniques.
Conclusions: Thulium Fibre Laser(30W) has promising initial results for Endoscopic Enucleation of Prostate. Further studies are needed.
Urethra sparing simple prostatectomy as an alternative to transurethral resection of the prostate ‐ a disruptive point of view!
A Cardoso, S Anacleto, C Laranjo Tinoco, R Matos Rodrigues, E Lima
Introduction & Objective: Surgery for benign prostatic obstruction (BPO) includes: endoscopic transurethral, and simple prostatectomy, either open (OSP) or minimally invasive, procedures. The gold standard remains: transurethral incision of the prostate (TUIP) for glands <30mL; transurethral resection of the prostate (TURP) for glands 30‐80mL; and for larger glands, endoscopic enucleation techniques or OSP. All BPO surgeries present risk of complications, namely ejaculatory dysfunction. In order to avoid it, urethra‐sparing simple prostatectomy (USSP) techniques have been developed since 1990, but classically applied for large glands. Yet, there is still no widespread USSP technique, that has not been abandoned due to technical difficulty. Thus, we aim to present our view for USSP.
Methods: We present a case report surgical video of our technique for laparoscopic extraperitoneal 5‐port USSP.
Results: The main goal of USSP is to remove adenomatous tissue preserving an intact urethra. We expose the anterior prostatic‐bladder neck junction, make a transverse incision, and deepen it until the cleavage plane between prostatic surgical capsule and the adenoma. Antegrade dissection begins between each adenoma lobe and the prostatic capsule, and proceeds into the inner portion, in contact with the urethra, signalled by the Foley catheter. Urethral injury is potentiated: for prostates >100mL, by asymmetrical enlargement of the adenoma that alters urethra position, shape, and makes it thinner; as well as for the presence of a medium lobe, which emanates from behind, and is covered by a thin mucosa. So, we consider these bad indications for USSP. However, after bilateral adenoma enucleation, a medium lobe, bladder stones or diverticulum, can be addressed through a small longitudinal anterior bladder wall incision. In the end, bladder and prostatic incisions are closed by running suture. Some technical key points for success are: definition of clear anatomical planes between the prostatic adenoma and urethra, optimal bleeding control, and immediate urethral repair if it is injured. Besides preservation of antegrade ejaculation, urethra preservation leads to reduced postoperative haematuria, with subsequent reduced need for irrigation, early catheter removal, and shorter hospital stay.
Conclusions: Our disruptive point of view is that the ideal candidates for USSP are men who wish to preserve antegrade ejaculation, with prostate volumes between 40 and 100 mL, without medium lobe! Thus, we suggest minimally invasive USSP should be, in fact, a direct competitor for TURP!
A Novel Technique for Effective Resection of Adenoma after Prostate Enucleation: An Economic Alternative to Morcellation
L Mo, JA Ivey, R Pak, J Cheng, D Chandler
Mayo Clinic Florida
Introduction & Objective: Morcellation is the most common tool used to remove adenoma from the bladder after prostate enucleation. Morcellators are relatively expensive and are not available at every medical center. We present a cost‐effective, safe, and efficient alternative to morcellation.
Methods: Prostate enucleation is first carried out in standard fashion. At our institution, this is completed with a combination of blunt dissection and electrocautery with a plasma kinetic button device and an electric loop. After the adenoma is fully dissected off the prostatic capsule, it is floating freely in the bladder. A suprapubic puncture is made with a laparoscopic insufflation needle under direct cystoscopic visualization. A laparoscopic grasper is then passed through the needle and into the bladder. The grasper is then used to immobilize the adenoma. The adenoma is then resected into small fragments with an electric loop, which are then easily evacuated from the bladder through the cystoscope.
Results: The laparoscopic grasper passed through the suprapubic puncture successfully immobilizes the adenoma in the bladder. This results in safe and efficient harvesting of the adenoma with the electric loop.
Conclusions: This technique is a safe, efficient, and cost‐effective method for removing adenoma after prostate enucleation. It is less invasive than a suprapubic cystostomy, and less costly than a commercial transurethral morcellator. This method could be expanded to be used with HoLEP for institutions equipped with a holmium laser but not a morcellator.
Same‐day surgery approach to Holmium Laser Enucleation of the Prostate (HoLEP) using MOSES
L Cooley, J Guo, MS Lee, T Large, AE Krambeck
Introduction & Objective: Traditionally, holmium laser enucleation of the prostate (HoLEP) has required an inpatient hospital stay post‐operatively. However, advances in technology with MOSES 2.0 and operative technique have allowed for better operative efficiency and hemostasis. Here, we present a video of our HoLEP technique and same‐day discharge pathway.
Methods: This video presents intra‐ and post‐operative considerations to facilitate a same‐day, catheter‐free discharge. It utilizes a representative patient case of a 65 year old male with obstructive lower urinary tract symptoms and a 100 gram prostate undergoing HoLEP.
Results: Our video highlights intraoperative techniques to minimize bleeding, operative time, and minimizing patient exposure to narcotics or muscle relaxants post‐anesthesia induction. Operative techniques to minimize bleeding include favoring laser over blunt dissection, coagulation of bleeding as it arises, and thorough hemostasis of the prostatic fossa pre and post morcellation. Post operatively, avoidance of narcotics, early and frequent ambulation, and oral hydration aid in a successful trial of void.
Conclusions: Same‐day discharge after HoLEP utilizing MOSES 2.0 is a safe and feasible option for many patients. Our video provides live operative content and instruction as well as post‐operative management to facilitate a same‐day, catheter free discharge.
Video Session 04: Laparoscopy: Lower Tract, Ureter, UPJ
V04: laparoscopy: lower tract, ureter, upj
L Richstone, E Olweny, A Aminsharifi
Laparoscopic Boari flap with port site RIRS in a case of Midureteric stricture with large renal stone
R Manickam, S Kallappan, S Nachimuthu
Introduction & Objective: Laparoscopic Boari Flap ureteric reimplantation for ureteric strictures is a complex reconstructive procedure involving lower urinary tract. To additionally treat a large renal stone, exteriorized ureter and port site RIRS is technically a demanding procedure.
Methods: 36 year old female presented with complaints of right renal colicky abdominal pain and on evaluation with Contrast Enhanced CT abdomen she had right side large renal stone of size 2 X2 cms in the upper calyx along with right mid ureteric stricture. She did not have any comorbidities. She had past history of Ureterorenoscopy for ureteric stone on the right side. Under General Anaesthesia, she underwent Cystoscopy and RGP which revealed long segment ureteric stricture from pelvic brim upto bladder. Laparoscopy was done through four ports and right ureter was divided above the stricture segment. The ureteric end was brought out through one of the 10mm port and spatulated. Flexible Ureteroscope was introduced through the exteriorized ureter and stone in the upper calyx fragmented with laser energy source. After satisfactory fragmentation, 6F double J stent was placed and ureter put into the abdomen. Boari Flap raised in a routine fashion and Ureteric reimplantation completed with barbed sutures. Drain placed.
Results: Patient recovered well and drain was removed on fourth post operative day. Catheter was removed after two weeks from procedure.
Conclusions: Laparoscopic Boari Flap ureteric reimplantation though a complex procedure is widely performed one. To combine RIRS through exteriorized ureter is technically demanding one but a feasible procedure.
Obstructive Megaureter in Infants : Laparoscopic Intracorporeal Ureteric Tapering and Reimplantation
D Vaddi, P Ramakrishna, P Siddalinga Swamy, B Manas Babu, G Soundarya, A Hemnath, P Rakesh, S Chahar, S Gunadal
Introduction: The principles of megaureter correction are simple but the surgical procedure is challenging. The stenotic distal part of the ureter is excised, megaureter is straightened, tapered and reimplanted in a nonrefluxing manner. The preferred approach for surgery is open approach with reported success rates of 90%‐96%. Though the evolution in laparoscopic surgeries in urology have seen a spike recently, this approach for megaureter correction is been taken up at limited number of centres only. Some case reports and case series have demonstrated laparoscopic ureteric tapering and reimplantation in adults and children, most of them demonstrating extracorporeal tapering and reimplantation.
Objectives: Our objective is to present the demonstration of the technique of laparoscopic intracorporeal ureteric tapering and extravesical reimplantation in infants, and its effectiveness and outcomes.
Methods: Two children with congenital obstructive megaureter, aged 1 year and 1year 9months, underwent laparoscopic surgery. The dilated ureter was dissected and divided at the stenotic distal most part just proximal to the uretero‐vesical junction. Proximally, a transverse incision was made on ureter and it was laid open longitudinally up to the distal cut end. The distal end was approximated over the bladder after straightening the ureter. The redundant part of the laid open ureter was excised and the tapered ureter was sutured over a 10fr infant feeding tube that was held in position through a suprapubic port. The bladder was distended and the distal end of refashioned ureter was anastomosed over a 3.5fr double J stent. The detrusor tunnelling was done to make the anastomosis non refluxing.
Results: The operating times were between 90 to 100 minutes in two surgeries. Blood loss was minimal. Abdominal drain was removed at 4th postoperative day. Foley's catheter was removed at postoperative day 7 and the double J stent was removed at 14 days post operatively in all cases. The postoperative period was uneventful and the radioisotope scan at 2 and 4 months showed good drainage. The micturating cystourethrogram showed no reflux in all patients.
Conclusions: The basic principles of megaureter correction, if applied judicially can give excellent results even in laparoscopic intracorporeal ureteric tapering and reimplantion in infants. This approach has benefits of fast recovery in a short time follow up.
Laparoscopic Uretero‐calicostomy for a patient with uretero‐pelvic obstruction, intrarenal pelvis and multiple caliceal stones
A Kashi, S Farshid, I Ghanaat, N ahmadian
Introduction & Objective: Ureterocalicostomy is reconstructive surgery to establish upper system continuity in the condition such as recurrent UPJO with fibrotic and intra‐renal pelvis or primary stenosis of ureteropelvic junction with intrarenal pelvis
Methods: A 30‐year‐old female with history of recurrent urinary tract infections and left side pain, was referred to our clinic. After imaging work‐up left side UPJO with calyceal stones was diagnosed, intravenous urography showed dilated calyx without prominent pelvis. In DMSA scan, left side differential renal function was 35%. Since the pelvis wasn't dilated and the parenchyma of kidney lower pole was thin, ureterocalicostomy was the planned.
Results: During laparoscopy, after finding the ureter and chasing it up to pelvis, a small intrarenal pelvis was found. The proximal ureter was ligated with 0 silk sutures, then lower pole kidney parenchyma was resected. For stone extraction, an 8.5 F Wolf ureteroscope was introduced through lower trocar and entered inside kidney through opening of lower pole calyx and stones were extracted by basketing. The ureter was spatulated and anastomosed to lower pole calyceal system with 0‐4 vicryl sutures in running mode. Finally, the anastomose was dependent and water tight. The patient was discharged 3 days after surgery without complication, and after 6 weeks double‐j stent was extracted. During follow up after 6 months, no urologic complaint was observed.
Conclusions: laparoscopic pyeloplasty is surgery of choice for UPJO, recently laparoscopic ureterocalicostomy was advised , particularly in patients with UPJO and thin parenchyma in lower pole of the kidney , during laparoscopic surgeries sometimes it is difficult to extract calyceal stones, ureteroscope can be used through the trocars for calyceal stone extraction.
Unusual pathology during laparoscopic pyeloplasty
S Saulat, S Saeed Uddin Qadri, J Sheikh, M Ejaz, A Ayub, H Ashraf, N Sadiq Kiani, S Tariq
Introduction & Objective: Retroperitoneal Laparoscopic Pyeloplasty is a minimally invasive technique for Uretropelvic junction obstruction. How to handle unusual situation during laparoscopic surgery
Methods: 12 years old male presented with abdominal pain and urinary tract infection. Ultrasound shows mild to moderate dilatation of pelvicalyceal system with ballooning of (left) renal pelvis (APD 35mm). MAG3 Scan confirmed 30% function and partial obstruction.
Results: Retroperitoneal Laparoscopic was performed using 10mm camera port just below the tip of twelve rib, 5mm working port near to angle of louis and 10mm working port just above the ilac crust anterior to mid axillary line. Renal pelvis and proximal ureter was dissected and mobilized. During surgery noticed dilatation of proximal ureter with renal pelvis which was firm in consistency when hold with grasper. Uretropelvic junction was opened with scissor. There was emerging of multiple fingers of mucosal growth through opening. The growth looks like octopus that causing obstruction. After relieving obstruction, the renal pelvis and ureter was soft in consistency. The mucosal growth was excised. During surgery, antegrade semi‐rigid Ureteroscopy was also performed to assess mucosa of the distal ureter and renal pelvis. After that dismembered Pyeloplasty was performed over 4.7 fr JJ Stent. Foley uretheral catheter was left in situ. The patient was discharged in 48 hours following the removal of the catheter.
Conclusions: Retroperitoneal Laparoscopic is the feasible, safe and useful technique in suitable or unusual PUJO pathology.
Zinner syndrome a rare case of bladder outlet obstruction
C Conde Redondo, F Natal Alvarez, S Martin Martin, A Ruano Mayo, A Zamora Horcajada, J Torrecilla, L Cuellar Martin, A Herranz Arriero
Introduction & Objective: Zinner syndrome , was first described by Zinner et al. in 1914, is a rare congenital malformation characterized by the association of an ipsilateral renal agenesis, ipsilateral seminal vesicle cyst, and ipsilateral ejaculatory duct obstruction.
Zinner syndrome is caused by malformations of the distal portion of the mesonephric duct and is considered the Mayer‐Rokitansky‐Kuster‐Hauser (MRKH) counterpart in males. The frequency of this condition is reported to be 0.0046%.fewer than 100 cases have been reported in literature
Methods: We present a case of a 24‐year‐old male with recurrent episodes of urinary tract infection (UTI) and poor urinary stream and finally bladderotlet obstruction.
On digital rectal examination, there was a soft, smooth, nontender bulge just above the prostrate.
Uroflometry done initially showed a maximum flow rate of 7 ml/min.
Cystoscopy reveals a bulge on the right side of the verumontanum abutting the neck of the bladder.
Ultrasound (US) : there is a left pelvic mass. Computed tomography (CT) and magnetic resonance imaging (MRI) showed diffuse distension of left seminal vesicle (9 X 7 cm) cyst with ipsilateral right renal hipoplasia.
CT findings might include an ipsilateral kidney agenesis in addition to a retrovesicular periprostatic cystic mass.
Results: We use four ports; one of 10 mm and three of 5 mm. We conclude the cystic mass excision of the cystic mass, the ureter, and the right kidney completely by laparoscopy. The surgical time was 120 min, bleeding 50 ml, and hospital stay 3 days.
Conclusions:
• Minimally invasive surgeries including the laparoscopic and robotic‐assisted approaches are considered the best option due to their better outcomes, less blood loss, and shorter hospitalization.
• In the literature we have only found three cases of complete excision of the cyst, ureter and complete atrophic kidney
Laparoscopic anterior pelvic exenteration in muscle invasive bladder cancer in female
R TP, D Sarma, S Pratihar
Introduction & Objective: Bladder cancer remains a disease of the elderly with relatively few advances that have improved survival over the last 20 years. Radical cystectomy (RC) has long remained the principal treatment for muscle‐invasive bladder cancer (MIBC). Muscle invasive bladder cancer has been traditionally treated by open radical cystectomy with ileal conduit or neobladder formation. Laparoscopic approaches have been performed for both the bladder extirpative and bowel reconstructive portions. It has been proved in different studies that laparoscopic approach provides equal oncological outcome if proper expertise available. The objective of this video is to show that laparoscopic anterior pelvic exenteration can be performed safely and efficiently in experienced hands with early recovery.
Methods: It is a video graphic presentation of a single patient. Surgery was done on February, 2019 at Gauhati Medical College Hospital. Our patient was a 55 years old lady, presented with urinary bladder mass. Imaging showed no extravesical extension of mass or lymph node enlargement. Transurethral resection of bladder tumour (TURBT) was done. Histopathology came out to be muscle invasive bladder tumour. After proper patient counseling laparoscopic anterior pelvic exenteration was done with open ileal conduit formation.
Results: Operative time was 310 minutes with blood loss of approximately 300 ml. Post operative period uneventful with early ambulation. Patent was discharged on 6th post operative day.
Conclusions: Laparoscopic anterior pelvic exenteration for muscle invasive bladder cancer in female patient is very safe in experienced hands with early patient recovery.
Experience of reduced port laparoscopic pyeloplasty for uretero‐pelvic junction obstructon in our hospital
K Mikami, K Ho, T Suyama, K Araki, h masuda, S Kojima, Y Naya
Introduction & Objective: Both adult and pediatric urologists frequently encounter uretero‐pelvic junction obstruction (UPJO), and laparoscopic pyeloplasty is an established treatment procedure for UPJO.UPJO apper in any age or which gender, So younger patients or woman want scarless surgery. Thus, we attempted reduced port surgery in reduced port laparoscopic pyeloplasty (RPSP) to reduce the size of wound, which is an advantage of laparoscopic pyeloplasty.
Methods: We performed 78 laparoscopic pyeloplasty since April 2006 and we started reduced port pyeloplasty from December 2011. We included 27 patients who underwent reduced port surgery in RPSP from November 2017 to March 2019 at Teikyo University Chiba Medical Center. Firstly, oval type easy accessⓇ was put from umbilical port. 5mm port for flexible laparoscope and 12mm port were put form easy accessⓇ. After obeservation of abdominal cavity, 3mm port was put at the adequate position in the upper abdomen. After dissecting colon, ureter and UPJ is identified. Crossed vessel is fixed to upper renal pelvis and the renal pelvis is lifted. After incising renal pelvis, ureteral stent was inserted into the ureter. Ureter is incised carefully and anastomosis of renal pelvis and ureter is performed.
Results: The median duration of surgery was 206 ± 45 minutes. Length of hospital stay was 6.7days (3‐8). 1 patient had a Clavien‐Dindo IIIa complication (pyelonephritis after removing ureteral stent). E‐GFR is improved in all patients 3month and 1 year after surgery comparing before surgery. C20/Cmax by Mag3 renogram is improved significantly after surgery (Before surgery:1.142 ± 0.964, 3 months after surgery: 0.307 ± 0.244, p = 0.0007). All patients were satisfied the umbilical scar.
Conclusions: RPSP is safe and effective for UPJO patients with inconspicuous scar. Especially, it is usefull for young healthy woman for whom this is an important consideration to be peformed RPSP.
Laparoscopic Dismembered Pyeloplasty In Five Differently Located Pelviureteric Junctions
V Chandra Mohan, P Ramakrishna, P Siddalinga Swamy, B Manas Babu, G Soundarya, A Hemnath, P Rakesh
Introduction & Objective: Pelviureteric junction (PUJ) can be located laterally, posterolaterally or anteriorly in Malrotated /ectopic kidneys. PUJ can be anterior or posterior even in normally located kidneys. Approach to these PUJs during surgical management of pelviureteric junction obstruction is a challenge. Here we present a video of the approach to different locations of PUJ and assess the dependent part intraoperatively to achieve unobstructed drainage.
Methods: Case 1: 9 months male baby, with antenatally detected hydronephrosis, presented with recurrent febrile UTI. DTPA renogram showed obstructive drainage. Intraoperatively PUJ was medially located. Case 2: 23 yr male with right loin pain for 3 months. CT KUB and DTPA renogram showed right hydronephrosis with obstructed drainage. Intraoperatively, PUJ was posterolaterally located. Case 3: 11 yr female child with left loin pain since 5 months. CT KUB and DTPA renogram showed left hydronephrosis with obstructed drainage. Intraoperatively, PUJ was posteriorly located. Case 4: 53 yr female with right loin pain since 3 months. CT KUB and DTPA renogram showed obstructed drainage. Intraoperatively, PUJ was anteriorly located. Case 5: 30 yr male with right lower abdomen pain since 1 month. CT KUB and DTPA renogram showed right ectopic malrotated kidney with obstructed drainage. Intraoperatively, PUJ was anteriorly located.
Results: Intraoperatively, the ureter was anastomosed to the most dependent part of the pelvis as depicted in the video. In case 1, inferior anastomosis done. In case 2, inferomedial anastomosis was done. In case 3, anteroinferior anastomosis was done. In case 4, postero‐inferior anastomosis was done. In case 5, anteroinferior anastomosis was done. Our video depicts five differently positions of PUJs and the technique to assess the most dependent part intraoperatively to achieve unobstructed drainage
Conclusions: Repair of PUJ obstruction in various locations is technically demanding. Reconstruction needs to be planned meticulously to accomplish dependent drainage and good intracorporeal suturing skills are required for the same.
Laparoscopic intraoperative blue light visualization of the ureters utilizing the novel fluorescent tracer agent MB‐102 – an in vivo porcine study
J Palka, SP Argade, M Talcott, T Rogers, R Dorshow, R Venkatesh
Introduction & Objective: Abdominal and pelvic laparoscopic and robotic surgical procedures carry a risk of iatrogenic injury to the ureters. Intraoperative identification of the ureters or ureteral injury is critical to prevent serious complications. We evaluated MB‐102, a novel fluorescent tracer agent constructed to be excreted by the renal system only, currently in ongoing clinical studies for renal function determination. We evaluated MB‐102 for locating the ureters during laparoscopic surgery.
Methods: We evaluated MB‐102 in 2 domestic pigs weighing approximately 30 kg. MB‐102 was injected intravenously at 3.2 mg/kg, and using a Karl Storz laparoscopic unit, the ureter was visualized under white & blue light laparoscopy before and after transperitoneal laparoscopic dissection. The ureteral fluorescence from the agent in ureteral lumen was evaluated at different light intensity settings. The plasma kinetics of MB‐102 was monitored simultaneously with the appearance and presence of ureteral fluorescence. In the second pig, a 5Fr retrograde catheter was inserted into the ureter under cystoscopic guidance for instillation of MB‐102 in a retrograde fashion at different concentrations. A deliberate partial and total transection of ureter and intra‐renal collecting system was performed for ease of visualization of extravasated MB‐102.
Results: The ureter was very well visualized within 5 minutes after intravenous injection of MB‐102 under the blue light as a bright yellow‐orange tubular fluorescent structure with peristalsis before and after exposing the ureter. This was best visualized at a light setting of 20% intensity. The ureteral fluorescence lasted for more than 45 minutes following intravenous injection. In the second pig, upon retrograde administration of the agent, the ureter illuminated with bright fluorescence under blue light easily at different concentrations. Finally, deliberate transection of the ureter and the intrarenal collection system showed bright fluorescent urine leaking from the injured site akin to a volcanic lava.
Conclusions: The novel fluorescent agent MB‐102 facilitated easy and early visualization of the ureter under blue light during laparoscopy. MB‐102 with its renal‐only filtration property and bright fluorescence is potentially a very good agent to identify the ureters and ureteral injuries.
Retrocaval Ureter, Laparoscopic Intervention
J Abad Vivas‐Pérez, S Gallardo Zúñiga, R Barrabino Martín, JM Molina Hernandez, J Gómez Jiménez, JA Hortelano Parras, J Nuevo Lara, JL Soler Soler
Introduction & Objective: Retrocaval ureter (RCU) is a rare congenital abnormally with the ureters passing posterior to the inferior vena cava (IVC). Patients do not normally present with symptoms until the third and fourth decades of life, from a resulting hydronephrosis. We showed a patient's treatment by laparoscopic and repositioning the ureter anterior to the inferior vena cava and pyeloplasty.
Methods: The patient is a 30 years old female with history of right flank pain and recurrent urine tract infections. CT Urography showed delayed function of the right kidney and a right hydronephrosis and hydroureter of the proximal ureter, and possible RCU. We operated her by a transperitoneal laparoscopic repair of RCU (involves division of the ureter and repositioning it anterior to the inferior vena cava, with anastomosis between the renal pelvis and the ureter over a double‐j stent). Operative time in our case was 145 minutes. Blood loss was 100 cc. Postoperative time for hospitalization was 2 days. The patient was asymptomatic on follow‐up (52 months). Ultrasound was suggestive of resolution of hydronephrosis.
Results: RCU is a rare congenital anomaly (1 in 1800 people). Over 200 cases reported worldwide. Similar male to female ratios is seen in clinical practice. Embryologically, the developing metanephros lies between paired set of three venous channels on each side which is called periureteric ring. The fully developed ureter hooks arounds the IVC as it courses down. The cause of the condition is developmental anomaly of IVC and not ureter.
Regarding minimally invasive approaches, different authors have used either transperitoneal laparoscopic or retroperitoneoscopic or robotic or minilaparotomy approach for RCU. Baba done for the first time by laparoscopic surgery. Ricciardulli and Lijun have described their experience of retroperitoneal laparoscopic approach. Fidalgo described technique of suspending pelvis with suture from abdominal wall for the ease of suturing, like our group. Tobias‐Machado used retroperitoneoscopy for dissection followed by minilaparotomy for extracorporeal anastomosis. Abdel‐Karim done a prospective randomized comparison between laparoendoscopic single‐site surgery and minilaparoscopy for treatment of upper urinary tract pathologie, included RCU.
Conclusions: Transperitoneal laparoscopic approach provides good working space for intracorporeal suturing. Minimally invasive surgery for RCU repair in symptomatic cases or those with severe hydronephrosis leads to complete resolution of symptoms and restoration of the normal anatomy and function.
Technique of conisation of the uretero‐pelvic reconstruction during laparoscopic and robotic assisted pyeloplasty in cases of ureteropelvic junction obstruction in a single surgeon serie
W Khoder, J Michaelis, M Grabbert, S Astheimer, C Gratzke, C Stief
Introduction & Objective: Anderson‐Hynes technique is the most popular surgical technique for pyeloplasty in patients with ureteropelvic junction obstruction (UPJO). Besides transperitoneal approaches, the retroperitoneoscopic approach is emerging. We present a modified dismembered pyeloplasty technique through retroperitoneoscopic laparoscopic (RLP) and robotic (RRP) approach in a single surgeon series.
Methods: The diagnosis of UPJO was confirmed preoperatively with imaging (retrograde pyelography or computed tomography), as well as functional mercaptoacetyltriglycine renal scans (MAGIII). The renal pelvis was resected in a fish mouth pattern, with app. ¾ of the ureteric circumference at UPJ. Stenotic ureteric part was excised and the ureter was spatulated longitudinally (V‐shaped flap). Anastomosis begins with 3 to 5 stitches using 4/0 monocryl sited at the edge of spatulation transversally to widen the lumen with conisation of UPJ. These sutures were set under enough tension to straighten the ureter. The anastomosis at the base of ureteric‐flap with the upper pelvic part (upper fish mouth) followed in same manner. Finally, reconstruction is completed with closure of anterior and posterior walls using 5/0 monocryl continuous sutures. All patients had a DJ‐stent for 6–8 weeks postoperatively.
Results: 176 patients underwent the described pyeloplasty technique (. Mean patients' age was 28years (14‐82), Mean BMI was 23.5 kg/m2 (10.2% (18/176 patients) classified as obese). Preoperatively, 70.5 % (124/176) reported pain or urinary stones 27.3% (24/176). All procedures were successfully completed without conversion or revision. Mean operative time was 137 minutes, mean blood‐loss was 68 ml with a mean hospital stay of 8days. There was no significant change between pre‐ and postoperative creatinine levels with a mean change of 0.0 (‐0.4, +0.9) mg/dl. Postoperatively, one patient had small pulmonary embolism, transient fever in 4patients, otherwise uneventful. The Dj was removed after successful postoperative retrograde pyelography at a mean of 56days. MAG III after 3 months showed stable to improved function with a mean of 1.1% (‐34%, +24%) more partial renal function assigned to the treated kidney.
Conclusions: The presented modified technique of RRP has favorable morbidity and functional outcomes. It is an easy to learn technique for surgeons already practicing dismembered pyeloplasty.
Laparoscopic approach to excision of giant, multiloculated, seminal vesicle cyst
AB McVey, E Polo Alonso, D Bolton, P Liodakis
Introduction & Objective: Seminal Vesicle cysts are extremely rare with an incidence of 0.005% reported in literature. The objective of this abstract is to present our laparoscopic approach to surgical excision of a giant, seminal vesicle cyst.
Methods: We retrospectively collected information related to clinical presentation, investigations and relevant past medical history of a single, individual case of seminal vesicle cyst at our institution. Consent was obtained to video record the laparoscopic procedure.
Results: A 54 year old man with a past medical history of Gleason 3 + 3 = 6 prostate adenocarcinoma was found to have a giant, multiloculated, seminal vesicle cyst on active surveillance imaging. He became severely symptomatic from rectal compression and was initially managed with transperineal drainage but had reaccumulation within 1 month. He had definitive management with a laparoscopic assisted 4 port transperitoneal excision and made a good post operative recovery.
Conclusions: Laparoscopic transperitoneal excision is a viable, successful approach to surgical management of symptomatic seminal vesicle cysts. With the aid of this procedure video surgeons can consider this as a future management option in the rare instance of symptomatic, seminal vesicle cysts.
Moderated Poster Session
Moderated Poster Session 13: Stones V: PNL & URS
Analysis of morbidity and mortality after percutaneous nephrolithotomy in patients with renal calculi: evaluation of 16,201 patients from a nationwide German database
B Becker, C Schulz, T Herrmann, CM Rosenbaum, AJ Gross, H König, C Netsch
Department of Urology, Asklepios Hospital Barmbek, Hamburg, Germany
Introduction & Objective: The aim of this study was to evaluate the percutaneous nephrolithotomy (PCNL) in patients with renal calculi. All complications, re‐intervention and re‐hospitalization rates within 30 days after surgery based on data of a German health insurance (AOK) were analyzed.
Methods: All AOK policyholders who were treated with a PCNL between 2008‐2016 were analyzed. All coded complications, re‐intervention and re‐hospitalization rates within the first 30 days after surgery were assessed.
Results: In total, 16,201 patients treated with PCNL were included. Median age was 55.3 years and 56.1% of policyholders were male. Arterial hypertension (39.6%), diabetes mellitus (19.1%) and obesity (10.7%) were the most common comorbidities. Re‐intervention rates were 18.9% and the most common treatment was the insertion and replacement of a double‐J stent in 1,951 (12%) and 551 (3.4%) patients, respectively. For the analysis of the patients who received a second stone treatment within the same hospital stay, 15,842 policyholders were evaluated. Out of this group, 1,450 (9.2%) patients were re‐treated with a second PCNL, 543 (3.4%) with ureteroscopy (URS) and 430 (2.7%) with shockwave lithotripsy (SWL). The total re‐hospitalization rate was 14.1% within the first month after surgery.
Conclusions: There are only few studies with large PCNL series in which the complications and re‐intervention rates after PCNL have been investigated. By analyzing the data of the AOK database, a deeper insight into big data of endoscopic stone treatment can be achieved. It was shown that the PCNL is associated with higher re‐intervention and re‐hospitalization rates than previously stated in the literature.
Long‐term follow‐up on dusting versus basketing during ureteroscopy – a prospective multicenter trial from the EDGE research consortium
KL Stern, RL Sur, S Sivalingam, M Monga, SK Bechis, J Moore, VK Wong, H Brar, E Kong, MR Humphreys, BH Chew
Mayo Clinic Arizona
Introduction & Objective: In 2018 the Endourology Disease Group for Excellence (EDGE) published a prospective trial comparing dusting versus basketing during ureteroscopy. One hundred fifty‐nine patients were included in the original analysis, which compared stone‐free rates at 3 months. Short‐term stone‐free rate was higher for the basket retrieval group on univariate analysis, but not multivariate analysis. This study investigates the long‐term outcomes of those patients included in the original trial.
Methods: IRB approval was obtained across all sites. Patients who were enrolled in the original study were contacted via phone and asked to report stone surgical interventions, painful stone episodes, stone recurrences on imaging, and Emergency Department (ED) visits for stones and hospital admissions for stone‐related care since their procedure. Chart reviews were also completed. The primary study outcome was the need for secondary surgical procedures for stone treatment.
Results: Seventy‐nine patients were contacted from 4 sites (Mayo Clinic, University of British Columbia, Cleveland Clinic and the University of California San Diego). Sixty patients were in the basketing arm and 19 in the dusting (p < .001). Mean follow‐up was 6.28 years for the dusting group and 6.49 years for the basketing group. There was no statistically significant difference in stone interventions, painful stone episodes, Emergency Department visits, or hospital admissions between the two groups (see table). There was a statistically significant difference in documented stone recurrence on imaging for dusting versus basketing (68.4% vs 40%, p = 0.030).
Conclusions: Long‐term outcomes of dusting versus basketing during ureteroscopy indicate that dusting is associated with higher stone recurrence on imaging, but there is no difference in secondary stone interventions, painful stone episodes, ED visits or hospital admissions for stone events.
Endoscopic combined intrarenal surgery (ECIRS) – Supine vs. Prone position and comparison with percutaneous nephrolithotomy: results of a systematic review
A Pérez‐Lanzac, M Alcoba García, G Bueno Serrano, G Ordaz Jurado, J Fernández Gómez, A Budia Alba
Ruber Internacional Hospital, Dept. of Urology.
Introduction & Objective: We conducted a systematic review and meta‐analysis to evaluate the differences in outcomes and complications between supine vs. prone Endoscopic Combined IntraRenal Surgery (sECIRS vs. pECIRS). We also compared s/pECIRS with percutaneous nephrolithotomy (PCNL). Our objectives were 1) to demonstrate that sECIRS has similar or better outcomes (Stone Free Rate, SFR) / complications with respect to pECIRS or PCNL, 2) to demonstrate that sECIRS favours combined accesses to the urinary system with respect to pECIRS (Prospero code CRD42019119952).
Methods: A literature review was performed in The Cochrane Library, PubMed, EMBASE and Web of Science. We included randomised controlled trial (RCT), quasi‐experimental and observational trials in Spanish or English for aduts (>14 years old). Two researchers (GB, MPA) excreened the articles according with the inclusion criteria and another two unmasked reviewers extracted data and assessed the quality of eligible studies. The methodological approach was assessed with the PRISMA checklist and for quality purposes the Quadas‐2 tool was used.
Results: Eight studies compared ECIRS with other minimally invasive techniques. Only one randomized controlled trial was found, the rest of them were retrospective. Among them, only 1 (12.5%) compared sECIRS vs. pECIRS, 4 (50%) compared s/pECIRS vs. PCNL, 2 (25%) analized outcomes of two cohorts of patients operated by standart ECIRS (CECIRS) or minimally invasive ECIRS (MECIRS) and 1 (12.5%) compared MECIRS vs. retrograde intrarrenal surgery (RIRS). No data were available to complete a meta‐analysis. The supine position was the preferred approach, used by 6 authors. sECIRS demonstrated the same stone clearance with respect pECIRS but lower renal pelvic pressure and better puncture of the medial calyces. ECIRS was associated with better stone free rates (SFR) compared with PCNL and also allowed single accesses. In most of the selected publications PCNL was performed with mini‐approaches (≤20 Ch) (3 vs. 1). MECIRS revealed less bleeding and pain with the same SFR than CECIRS. ECIRS vs. RIRS could be performed in one single session on the same patient with no significant differences in SFR. The studies resported no differences in complications between approaches (ECIRS vs. PCNL/RIRS). In addition, there was a wide heterogeneity among studies in the definition of SFR and image evaluation after the surgery.
Conclusions: There is no robust evidence that compare ECIRS in supine vs. prone or with PCNL/RIRS. The supine position for ECIRS or PCNL and mini‐approaches were the preferred choices. With respect with PCNL, the studies reported better SFR for ECIRS but no differences in complications.
Fate of residual fragments after PCNL: Results from the EDGE Research Consortium
BH Chew, VK Wong, AS Emmott, R Paterson, D Lange, CJ Lundeen, A Nevo, J Moore, A Yaghoubian, N Nimmagadda, RL Sur, SK Bechis, BE Knudsen, MR Humphreys, BH Eisner
Introduction & Objective: Residual fragments (RFs) after percutaneous nephrolithotomy (PCNL) are more evident with the increasing use of high‐resolution CT‐scan. The fate of RFs after PCNL are poorly studied in large multi‐institutional studies. We reviewed our databases to identify patients with residual fragments after PCNL to determine the rate of stone growth, complications, and further surgery were different between patients with fragments less than 4 mm or those with fragments larger than 4mm.
Methods: Sites from the Endourologic Disease Group for Excellence (EDGE) research consortium examined data of PCNL patients from 2015‐ 2017 with at least 1 year follow‐up. Rates of fragment passage, re‐intervention, and RF regrowth were recorded and stratified into <4mm and ≥4mm groups. Fisher's exact tests were performed. Potential predictors for stone‐related events following PCNL were determined using multivariable logistic regression analysis.
Results: A total of 417 patients received a postoperative CT‐KUB within 6 weeks and had RFs that were 1 mm or larger (Table 1). Rates of re‐intervention in patients with ≥4mm RFs post‐PCNL were found to be significantly higher (p < 0.001): 42.6% and 14.4% for patients with ≥4mm RFs and <4mm, respectively. Kaplan‐Meier curve analysis showed significantly higher rates of requiring intervention in patients with ≥4mm residual fragments (Figure 1). Passage and RF regrowth was not found to be significant between groups(p = 0.712, and p = 0.059, respectively). On multivariable analysis, age, BMI, and size of RF were found to be predictive for stone‐related events (p = 0.008, 0.046 and <0.001, respectively).
Conclusions: Patients with fragments ≥ 4mm after PCNL were more likely to undergo intervention despite having similar growth rates of fragments. Older patients with higher BMI and larger fragments were more likely to undergo re‐intervention. A prospective study would help explain the indicaions and rationale for further surgery for RFs after PCNL.
Is retrograde intrarenal surgery as effective in pediatric kidney stones as in adult patients?
MS Özkent, MM Piskin, M Balasar, Y Göger, MS Sönmez
Konya City Hospital
Introduction & Objective: Stone disease has been known for centruies, in recent decads its prevalence is increasing in children and adults. Technological developments, miniaturization of endoscopic instruments have enabled the effective use of retrograde intrarenal surgery in the treatment of kidney stones. There are limited number of studies in pediatric patients. The aim of this study was to compare the efficacy and safety of RIRS performed by using same instruments among the children and adults with similar stone burdens and locations.
Methods: In our study, the files of patients who were diagnosed with kidney stones and treated with retrograde intrarenal surgery using the same instruments between 2010‐ 2018 were retrospectively reviewed. The patients were divided into children (under 18 years) (group 1) and adult (18 years of age and older) (group 2) age groups. The stone load, stone size, stone localization, operation time, use of ureteral access sheath, intraoperative complication rates, complete stone‐free rates, postoperative complication rates, hospitalization duration, preoperatve and postoperative stenting were compared between in both groups.
Results: A total of 275 patients (55 patients in group 1 and 220 patients in group 2) were included in the study. The mean age of the patients was 36.5 ± 20.1 (8 months‐89 years) years. The mean stone size was 14.6 ± 6.7 mm (5‐47 mm). The mean operation time was 62.9 ± 24.4 (25‐170 min) minutes (min). The hospitalization period was 1.9 ± 2.4 (1‐15 days) days. In both groups, stone load, number of stones (single‐multiple), stone opacity, side, degree of hydroureteronephrosis and duration of operation were similar. The exact stone‐free rate between the groups (group 1 81.8%, group 2 78.2%, p: 0.554) was similar after the first session. Total complication rate was 13.8% (group 1 16.4%, group 2 13.2%) and no difference was observed between the two groups.
Conclusions: In our study, we found that RIRS is a minimally invasive surgical procedure that can be used effective and safely in pediatric patients with kidney stones. We found that the presence of lower pole stone, increased stone burden and presence of more than one stone were the most important factors affecting postoperative success for both child and adult patients.
Cross‐Sectional Survey of Patients Awaiting Nephrolithiasis Surgery During the COVID‐19 Pandemic Onset: A Multi‐Center Study from the Registry for Stones of the Kidney & Ureter Group
J Ahn, D Bayne, I Metzler, JD Harper, RL Sur, SK Bechis, BD Duty, D Tzou, N Sobhani, M Stoller, T Chi
UCSF
Introduction & Objective: The Coronavirus pandemic led to wide‐spread reductions in surgical volume. Many patients were hesitant to undergo surgery, despite appropriate hospital precautions. Kidney stone patients pending surgical intervention have distinct risks associated with surgical delay including pain, infection, and loss of renal function. It is important to understand the risks of surgical delay during the pandemic and to better understand patient concerns and preferences for undergoing surgery.
Methods: A prospective, multi‐institutional patient survey during April and May 2020 was performed. Nephrolithiasis patients pending stone removal surgery including ureteroscopy, shockwave lithotripsy, percutaneous nephrolithotomy, and nephrectomy were interviewed at clinical encounters regarding their symptoms, unplanned clinical events, presence of nephrostomy tubes /double J stents, concerns and reassurances for coming to the hospital, and willingness to undergo surgery. The association of patient demographics, stone burden, renal function, stone‐related symptoms, and COVID risk factors with willingness to undergo surgery, and concerns for contracting COVID were examined.
Results: 142 patients pending stone surgery completed surveys, with 66% willing to proceed with surgery, while 34% requested to delay. There was no statistical difference in patients willing versus unwilling to proceed with surgery, with regards to patient demographics, type of surgical procedure, stone burden, stone‐related symptoms, renal function compromise, presence of hydronephrosis, unplanned clinical events, or COVID risk factors. Those willing to proceed were more likely to have a ureteral stone (32% vs 15%, p = 0.03) or have a ureteral stent or nephrostomy tube in place (35% vs 6%, p < 0.01). Willingness to proceed with surgery was inversely correlated with COVID19 concerns. COVID19 concern was not impacted by age, sex, clinical site, distance to hospital, or COVID 19 risk factors.
Conclusions: Kidney stone patients pending surgical treatment were more willing to proceed with surgery based on the presence of a ureteral stone, upper urinary tract drainage tube, or low concern for COVID. Patient demographic, symptoms, kidney function, and other stone risk factors were not associated with willingness for surgery. Patients that are hesitant to proceed with surgery, despite appropriate hospital precautions should be educated appropriately regarding their risks with regards to COVID and nephrolithiasis.
Do Patient and Operative Risk Factors during PCNL Affect Radiation Exposure?
A Rai, D Nethala, S Rastogi, T Aro, A Abraham, D Hoenig, AD Smith, Z Okeke
The Smith Institute for Urology
Introduction & Objective: The use of fluoroscopy is integral to the completion of PCNL, and as the adoption of the technique become widespread, unfortunately exposure to the surgeon and other members of the operative suite has increased. In order to mitigate radiation exposure during PCNL, we must first understand the risk factors that may predispose surgeons and OR staff to increased radiation exposure. We therefore sought to examine the variables associated with higher radiation exposure during PCNL in hopes to raise awareness regarding exposure.
Methods: A retrospective examination of PCNL cases was performed between July 2019 and September 2019. Data was collected primarily between two endourologic, fellowship‐trained surgeons completing PCNL at a tertiary academic center. Fluoroscopy data was collected from the C‐arm radiation dose reports at the conclusion of the case.
Results: A total of 26 PCNL cases were completed, however 1 case was excluded as percutaneous access was achieved for UTUC management. Of the remaining 25 cases, dilation of the percutaneous tract was the step associated with the highest level of radiation exposure (52.4 mSv), whereas both lithotripsy and tube placement were noted to have the lowest radiation exposure (21.4 and 19.1 mSv respectively). Despite this discrepancy, this difference failed to achieve statistical significance (p = 0.07). Stone location (renal pelvis only vs. calyceal vs. staghorn) and stone size (>2 cm vs <2 cm) did not demonstrate significantly different average radiation exposures. Radiation exposure did not appear to vary based on surgeon. Patient characteristics did not appear to be associated with greater radiation exposure, as neither age ( >65), gender, or obesity (BMI >30) appeared to be significant.
Conclusions: The data demonstrates that percutaneous renal tract dilation is associated with the highest use of radiation. While stone size and location failed to demonstrate statistical significance, this may be secondary to small number of cases analyzed. Further study will likely be helpful in elucidating factors most contributory towards elevated radiation exposure during PCNL and guiding surgeons towards intelligent fluoroscopy utilization.
Urolithiasis after kidney transplantation: a New York statewide analysis with 5‐year follow up
EB Garden, N Tomer, J Pfail, KT Ravivarapu, AC Small, MA Palese
Icahn School of Medicine at Mount Sinai
Introduction & Objective: Following kidney transplantation (KT), urolithiasis is an uncommon but morbid problem given the potential for acute obstruction. The incidence, pathophysiology, and optimal treatment strategy of post‐transplant lithiasis is poorly defined. Here, we sought to describe the five‐year incidence of urolithiasis in KT recipients, identify risk factors for stone formation, and describe disease management.
Methods: After identifying all KT recipients (International Classification of Diseases‐9 [ICD‐9] procedure code 55.6) from 2005‐2012 in the New York Statewide Planning and Research Cooperative System database, patients were evaluated for urolithiasis diagnosis (ICD‐9: 592.0, 592.1, 592.9; ICD‐10: N20.1, N20.2, N20.9) within five years of KT. ICD‐9, ICD‐10, and Current Procedural Terminology (CPT) codes were used to identify all urological procedures performed after stone diagnosis. Data were then analyzed to identify demographic and clinical factors related to stone formation.
Results: 9,677 patients underwent KT between 2005‐2012. The five‐year urolithiasis rate was 3.2% (N = 311). Median time to diagnosis was 533 days (IQR = 113.8 days); 17.7% (N = 55) of stones were diagnosed <30 days postoperatively, 16.1% (N = 50) between 1‐6 months, and 66.2% (N = 206) >6 months. On multivariate regression, male sex was associated with decreased risk of lithiasis, while comorbidity burden correlated with increased risk (Table 1). For the 88 patients (28.3%) who required surgery, the mean number of procedures required was 1.55 (SD: 0.95). Procedures were most commonly performed via ureteroscopic or percutaneous approaches (Table 2). 71.7% (N = 223) of patients were managed nonoperatively.
Conclusions: Urolithiasis is rare after KT, affecting 3.2% of patients most commonly >6 months post‐transplant. Women were identified as being at increased risk for stone formation. Most patients were managed nonoperatively, while those receiving surgery commonly required ureteroscopy or percutaneous surgery.
A comparison among RIRS and MiniPerc for renal stones between 1‐2 cm: a randomized controlled trial
L Berti, M Maltagliati, U Besana, C Buizza, A Calori, M Sighinolfi, S Micali, BC Rocco, G Bozzini
ASST Valle Olona
Introduction & Objective: We performed a prospective randomized comparison between Retrograde Intrarenal Surgery (RIRS) and MiniPerc (MP) for renal stones between 1 and 2 cm, to evaluate the efficacy and safety of these procedures.
Methods: Patients with CT scan evidence of a single renal stone between 1 and 2 cm in diameter were enrolled in this multicenter study. Exclusion criteria were the presence of coagulation impairment, age below 18 or above 75, presence of acute urinary tract infection, or cardiovascular or pulmonary comorbidities. Patients were randomized in two groups: patients treated with RIRS (group A) and patients treated with MP (Group B). To assess stone‐free status, the patients were evaluated with a CT scan 3 months after surgery. Stone‐free status was defined as a negative CT scan, or as presence of stone fragments <3 mm, in asymptomatic patients, with negative urine culture. A statistical analysis was carried out to assess preoperative patient data, success and complication rates, re‐treatment rate and need for auxiliary treatment. Ethical committee approval was obtained, and patients signed the informed consent.
Results: Between January 2016 and January 2019, 356 consecutive patients were enrolled in this study. 174 patients in group A and 182 in group B. Mean stone size was 18.01 mm in Group A and 19.33 mm in Group B (p = 0.18). Overall stone‐free rate was 71.3% in group A and 80.7% in group B. A higher stone‐free rate was achieved for upper calyceal stones in group A (38/40, 95%), while group B showed a better performance on lower calyceal stones (42/45, 93.3%). Retreatment rate was similar between the two groups (p = 0.31). Necessity of an auxiliary procedure was comparable between the two groups (p = 0.18). Complication rate was 9.7% in group A, and 5.4% in group B.
Conclusions: RIRS and MP are two safe and effective procedures for the treatment of renal stones between 1 and 2 cm. The effectiveness of each procedure depends on stone location: RIRS appears to be more effective for upper calyceal stones, whereas MP for lower calyceal stones.
Improving access and quality of care to kidney stone patients in an underserved community
M Stout, M Murtha, M Yudovich, A Scimeca, D Diab, T Posid, G Shidham, E Weinandy, BE Knudsen, MW Sourial
The Ohio State University
Introduction & Objective: Federal programs are implemented to improve Medicaid patient access to healthcare, enhance quality and outcomes of care, as well as reduce overall financial burden. We sought to build a comprehensive kidney stone program at our institution to address this specific population by helping patients navigate through the acute and preventative aspects of stone disease, thereby improving various stone related outcomes.
Methods: A collaborative, multi‐disciplinary program was established at our single institution consisting of urology, nephrology, dietary specialists, and a nursing care coordinator. Patients were evaluated for initial stone intervention (observation versus surgical management) by urology, and referred to nephrology and dietitians whenever indicated for targeted preventative measures.
Results: One hundred and eighteen Medicaid stone patients were evaluated from September 2018 to January 2020. Seventy percent of patients identified as white, 17.2% identified as black/African‐American, and 12.9% identified as “other”. Patients were seen by nephrology or a dietician in 22% and 20% of cases, respectively. Eighty‐two percent reported making dietary changes while 14% utilized preventative medications or nutritional information at last follow‐up visit. Since the program's implementation, no‐show rates for initial urology follow‐up decreased from 24.6% to 19.4%. Emergency Department stone encounter rates remained stable, while outpatient clinic appointment volume increased by 21% after the first year. Reported patient compliance of dietary changes, medication utilization, and nutritional education was 73% at first follow up.
Conclusions: There is supporting evidence of the importance of a comprehensive kidney stone program targeting patients of lower socioeconomic status by improving access to all facets of stone disease management, with resultant promising preliminary improvement in various stone related outcomes.
Changes in Renal Parenchymal Volume and Long‐Term Function after Percutaneous and Ureteroscopic Stone Removal
P Jiang, R Arada, AS Afyouni, L Grimaud, R Karani, A Peta, A Brevik, CM Rhee, K Kalantar‐Zadeh, RM Patel, J Landman, RV Clayman
Department of Urology, University of California, Irvine
Introduction & Objective: Recent CT‐based volumetric studies have raised concerns regarding significant renal parenchymal loss following standard percutaneous nephrolithotomy (PCNL); the short‐term impact on renal function has previously been reported to be nil. We sought to evaluate renal parenchymal volume changes after PCNL and after ureteroscopic removal of stones (URS) in a matched group of stone patients and explore whether renal parenchymal volumetric alterations impacted on long‐term renal function.
Methods: Since 2013, patients undergoing PCNL or URS at our institution have been entered into a database. Patients with accessible preoperative and postoperative CT imaging and preoperative and >6 month postoperative serum creatinine levels were reviewed. PCNL and URS patients were matched based on age and comorbidities. Statistical analysis was performed using R version 4.0.2.
Results: Thirty‐five patients met the strict matching criteria (17 PCNL and 18 URS). Median follow‐up was 26.1 months (Table 1). The PCNL group, all with a single 30Fr tract, experienced a renal parenchymal volume loss of 6.0% (p < 0.01); in contrast, the URS group had minimal loss in renal parenchymal volume of 2.3% (p = 0.12). On univariate and multivariate analysis, there was no statistically significant difference in renal parenchymal volume loss between PCNL and URS (p = 0.08, p = 0.06, respectively).
With respect to eGFR, PCNL patients had a 13.1% decline (preop eGFR = 87.9 postop eGFR = 76.0, p < 0.01) while the URS patients had a 3.9% improvement (preop eGFR = 89.8, postop eGFR = 93.3, p = 0.34). On univariate and multivariate analysis, PCNL was associated with significantly greater loss in eGFR compared to URS: ‐17.6 mL/min/1.73m2 [9.6, 25.7] (p < 0.01, p < 0.01, respectively).
Conclusions: Unlike patients following URS, PCNL patients had both a significant decline in renal parenchymal volume as well as a significant decline in long‐term eGFR.
Prospective study of retrograde intrarenal surgery(RIRS) for renal and upper ureteric calculus in prior non stented patients
VK Poleboyina, P Kalidindi, R Kalidindi, V Akinapally, M Khan
care hospital
Introduction & Objective: To clarify the surgical outcomes&determine stone free rate(SFR)at one month of surgery with primary RIRS(without preoperative stenting )by flexible ureteroscopy (fURS) for managementof renal and upper ureteric calculi of size less than 2cm.
Methods: A total of 40 patients who underwent RIRS procedure for renal and upper ureteric calculi of less than 2cm were included. All procedures were done without preoperative ureteric stenting. Distal 4 cm of tge lower ureter was dilated using a balloon dilator after urrteroscopy with a 6‐7.5 F Semirigid Ureteroscope. Baseline characteristics of patients, stone burden, operation time, stone‐free rates, and complications wereanalysed. Stone free rate was defined as a complete absence of stones or stones <3 mm, which were deemed insignificant on ultrasonography and plain radiography.
Results: Successful primary access to upper ureter and renal pelvis was achieved in 38 patients without preoperative stenting. A total of 36 RIRS procedures were done in primary sitting. In 2 of the 36 patients, ureteral stenting was done in view of features of infection in the form of turbid or purulent fluid effux. and later definitive procedure was done in second sitting. After one month of follow up 34 patients had complete stone free rate. Two patients required relook flexible ureteroscopy for residual fragments. No significant side‐effects or complications were in encountered during the study period.
Conclusions: Primay RIRS by Flexible Ureteroscope for management of renal and upper ureteric calculi without preoperative ureteral stenting is associated with satisfactory outcome in short term follow‐up.
Withdrawn
Horseshoe Kidney Compared to Orthotopic Kidneys: Anatomical Measurements Relevant for Percutaneous Access
AS Mouzannar, B Mora Garijo, L Horodyski, R Blachman‐Braun, I Estanga, J Katz, R Marcovich, L Deane
University of Miami Hospital
Introduction & Objective: Horseshoe kidney (HSK) is the most common congenital fusion anomaly of the urinary tract. 21 – 60% of HSK are associated with urolithiasis. Percutaneous nephrolithotomy (PCNL) in HSK is thought to present a challenge for urologists given altered anatomical relationships, which may require technique modifications. The purpose of this study is to compare the anatomic relationships between horseshoe and orthotopic kidneys in order to identify necessary technical adaptations for PCNL.
Methods: From January 2010 to December 2019, 114 patients who underwent abdominopelvic computed tomography (CT) at Jackson Memorial Hospital, and were diagnosed with horseshoe kidney, were reviewed. They were compared to 121 subjects of similar age and BMI who served as controls. Radiological measurements and surface anatomy relationships of HSK and orthotopic kidneys were performed by radiologists and senior urology residents. Comparison of numerical variables between groups was performed using the Mann‐Whitney U or Student t‐test as required. Categorical variables were analyzed using the Chi‐square test.
Results: The mean age, BMI, and gender of patients with HSK and orthotopic kidneys are detailed in Table 1. When compared to orthotopic right kidneys, the median distances from the right upper pole (UP) of HSK to the posterior abdominal wall were 9.8 cm versus 7.9 cm, respectively. When comparing orthotopic left kidneys, the median distances from left UP of HSK to the posterior abdominal wall were 9.6 cm versus 7.7 cm, respectively. The median vertical distance from the bilateral 12thribs to the right UP and left UP were 1.3 cm and 0.8 cm, respectively. However, the upper poles of orthotopic kidneys were at or above (median vertical distance = 0 cm) the 12th ribs bilaterally.
Conclusions: Despite HSK being at a slightly lower level anatomically, we conclude that the level for percutaneous access is unlikely to differ significantly from that in orthotopic kidneys when accessing the upper pole of an HSK.
Post‐Operative Pain and Recovery in Patients with Nephrolithiasis: Results from the Endourological Society TOWER Research Collaborative
AE Jones, G Lin, H Stambakio, BH Chew, JM Stern, JB Ziemba
University of Pennsylvania Perelman School of Medicine
Introduction & Objective: Urolithiasis is among the most common urological conditions, however, the impact of pain on patients with the disease remains understudied, particularly following surgical intervention. We prospectively captured patient‐reported pain interference and intensity in patients following ureteroscopy (URS) or percutaneous nephrolithotomy (PCNL) for nephrolithiasis.
Methods: Adults undergoing URS or PCNL for renal/ureteral stones were eligible for inclusion (10/2020‐1/2021). Patients prospectively completed PROMIS‐Pain Intensity and Pain Interference instruments pre‐operatively (POD 0) and via email on POD 1, 7, and 14. Scores are reported as T‐scores (normalized to US pop., mean = 50) with a change of 5 (0.5 SD) considered clinically significant.
Results: A total of 33 patients completed enrollment at POD 0 (POD 1 = 21, POD 7 = 21, POD 14 = 15). Repeated measures ANOVA show statistically significant difference in both pain intensity and interference scores over each subsequent time comparison for URS and PCNL (both p < 0.05) (Figure 1). URS patients return to baseline pain intensity and interference by POD 14, however, PCNL patients do not see a return to baseline, and pain interference remains above the national mean. No demographic or perioperative characteristics were predictive of greater pain intensity or interference.
Conclusions: Pain intensity and interference increases immediately post‐operatively. URS patients see a reduction below the baseline in pain intensity and interference by POD 14, but PCNL patients experience pain intensity and interference above baseline for at least 14 days. Results offer meaningful insight to assist with patient counseling for surgical treatment of nephrolithiasis.
Irrigation practice patterns during flexible ureteroscopy: Results of a worldwide survey
J Bahaee, J Plott, KR Ghani
Department of Urology, University of Michigan
Introduction & Objective: Flexible ureteroscopy (fURS) has emerged as the primary modality for the treatment of renal stones in North America. Irrigation methods and parameters during fURS may impact intrarenal pressure and patient safety, yet there is limited data on practice patterns for irrigation. We assessed this across surgeons in different regions of the world through an online survey.
Methods: An anonymous online questionnaire on URS practice patterns was sent to Endourology Society members in January 2021. Responses were collected through QualtricsXM over a 1‐month period. The study was reported according to the Checklist for Reporting Results of Internet E‐Surveys (CHERRIES). Surgeons were from the following regions: North America (US and Canada), Latin America, Europe, Asia, Africa, and Oceania.
Results: Questionnaires were answered by 208 surgeons (response rate 14%). U.S and Canadian surgeons accounted for 36% of all respondents, 29% from Europe, 18% from Asia, 14% from Latin America, 1% from Africa, and 1% from Oceania. fURS was routinely performed by all respondents with 54% performing >101 cases/year. In North America the most common irrigation method was the pressurized saline bag using a manual inflatable cuff (55%) (Table). In Europe, the most common method was the saline bag (gravity) with a bulb or syringe injection system (45%). Automated systems were most common in Asia (30%). For pressures used during URS, the majority of respondents used 75‐150 mmHg (Figure). The clinical scenario which had the greatest issue with adequate irrigation during URS was biopsy of urothelial tumor.
Conclusions: In this survey, we found that irrigation practices during fURS differ across the world. North American surgeons primarily used a pressurized saline bag, in contrast to European surgeons who preferred a saline bag with a handheld bulb/syringe system. Overall, automated irrigation systems were not commonly used.
Development of a Composite Ureteroscopic Efficiency Score Through Simulated Ureteroscopic Skills Assessment
N Chen, D Yu, D Wollin
Brigham and Women's Hospital Division of Urology
Introduction & Objective: Flexible ureteroscopy (fURS) is a common urologic procedure used to treat many conditions, from kidney stones to upper tract urothelial tumors. While many methods have been studied to teach and assess ureteroscopic skills, this remains an inconsistently organized area of urologic training. We attempted to better understand ureteroscopic movement proficiency and skill acquisition through simulation and computer vision methods.
Methods: A video camera was used with a ureteroscopic simulation box to track device position during various tasks performed by urologists of varying skill levels. Two tasks (with multiple repetitions) were analyzed to better understand ureteroscopic skill acquisition. Computer vision methods were utilized to track overall ureteroscope tip travel distance (DIST), task time (TIME), spectral arc length (SPARC, a measure of path smoothness), and number of times the device tip collided with the wall of the simulation box (COLL). These metrics were compared across all participants and a mixed effects model was utilized to differentiate between initial and final attempts at each task. A composite ureteroscopic efficiency score (CUES) was defined that summed the normalized values of these metrics.
Results: 12 urologists completed multiple movement tasks in the simulation box as described. Utilizing the average values, TIME, DIST, SPARC, and COLL were all correlated, with the TIME:DIST correlation strongest (r = 0.84, p < 0.05). Each metric improved on average from the initial tasks to their final repetitions, suggesting increase in efficiency; in fact, each metric could be used to differentiate between first and final repetition (ROC curves with AUC ranging 0.73 ‐ 0.83). The CUES was able to differentiate between first and final repetition with AUC of 0.80.
Conclusions: This study suggests that various ureteroscope movement variables are interconnected and may differentiate between efficient and non‐efficient scope movement. Task performance factors including TIME, DIST, SPARC, and COLL (which can be combined into the CUES) may assist in teaching and skills assessment in a simulation setting. Further study is needed to determine the generalizability of these factors as markers of skill in various simulation settings and to assess transition to clinical efficiency.
Stone ablation efficacy of a new prototype Holmium:YAG pulse‐modulated laser at working distances of up to 3mm
B Yang, I Parab, J Cancino, S Liu, A Ray, TC Hasenberg, T Harrah, BW Turney
University of Oxford
Introduction & Objective: Holmium:YAG laser has been the lithotrite of choice for around 30 years in kidney stone surgery. The relatively high absorption in water is clinically useful but also limits the effective range of these lasers. Laser technology has taken advantage of the “Moses effect” to improve energy delivery to the target while reducing heating of the irrigation fluid. We report on a new prototype Holmium laser that fires multiple micro‐pulses in pulse packets and present stone phantom ablation rate results at fiber‐to‐stone working distances of up to 3mm utilizing a bench model.
Methods: Uniform, homogeneous BegoStones (15:3 BegoStone:water) were used. A 242μm core fiber was attached to the prototype laser and the fiber was moved over the surface of the stone in a predetermined pattern using an automated system. A range of pulse packet energy/frequency settings from 20W to 45W were investigated. Stone ablation efficiency was measured by dry‐weight difference before and after treatment. A range of working distances (WDs) from 0.5mm to 3mm were used to investigate the effect of increased distance to the stone.
Results: Measurable ablation rates were observed with the prototype pulse‐modulated laser up to a working distance of 3mm, across a range of powers (Figure 1). The ablation rate at 3mm WD was 27.6% of that at 0.5mm WD (range 12.9‐44.4%). Results from a reference holmium laser using the same methodology are also included.
Conclusions: The prototype laser demonstrated an impressive working range in our bench testing across a range of power settings, with measurable ablation even at a WD of 3mm. This suggests that these micro‐pulses produce a significant Moses effect. We feel that pulse‐modulation with packets of micro‐pulses can synergise well with the Moses effect to increase the effective range and needs to be further tested in a clinical setting. (Disclaimer: Concept device or technology. Not available for sale).
BMI and Nephrolithiasis in a Pediatric Cohort by Pubertal Status
A Hannallah, Z Baker, N Khouzam MD, S Sparks MD
Children's Hospital Los Angeles
Introduction & Objective: The link between obesity and nephrolithiasis is established in adults, but not in children. We hypothesize postpubertal pediatric kidney stone formers will have higher body mass index (BMI) and obesity rates when compared to prepubertal stone formers.
Methods: This was a retrospective review of pediatric patients with nephrolithiasis. Patients with significant comorbidities or less than 2 years in age were excluded. Puberty was defined using the American Academy of Pediatrics guidelines. Per the Centers for Disease Control (CDC) guidelines, overweight was defined as 85th to 95th percentile BMI for age, and obesity as 95th percentile and above. Gender, height/weight at visits, and surgeries were recorded. Associations among pubertal status, BMI, surgeries, and stone compositions were assessed with one‐way analysis of variance (ANOVA) and Pearson X2 tests.
Results: 196 patients met inclusion criteria. There was a significant difference in mean BMI among patients with stones by pubertal status and by gender (p < 0.001, Table 1). Rates of overweight and obese patients was highest in the postpubertal group, followed by pubertal patients (Figure 1). There was a statistically significant difference in BMI percentiles according to pubertal status among females (p = 0.05, Table 1). 98 patients (50.0%) required at least one surgery. BMI, BMI percentile, and pubertal status were not associated with intervention (p = 0.34, p = 0.40, and p = 0.44). Overweight/obese patients were significantly more likely to form calcium oxalate stones (n = 25/30; 83.3%) compared to healthy/underweight patients (n = 25/45; 55.6%; p = 0.003).
Conclusions: In our cohort of pediatric kidney stone formers, pubertal and postpubertal patients have higher BMIs and obesity rates than pre‐pubertal patients, particularly among female patients. Overweight/obese children form more calcium oxalate stones, similar to obese adults. Future studies should focus on pubertal and postpubertal cohorts when assessing the role of obesity on nephrolithiasis.
The relationship between renal pelvis pressures and pyelovenous backflow during ureterorenoscopy in a live porcine model
J Twum‐Ampofo, J Saunders, M Franco, B Eisner
Introduction & Objective: Renal pelvis pressures and pyelovenous backflow during ureteroscopy are hypothesized to play a role in the development of infection after ureterorenoscopy. However, there are few studies in the literature which investigate this phenomon and the relationship between renal pelvis pressure, operative time, and pyelovenous backflow is poorly understood. Herein we present a pilot study of ureteroscopy in a swine model designed to evaluate these relationships.
Methods: In anesthetized pigs (n = 9; female; ∼60 kg each), ureteroscopy was performed as follows: cystoscopy was performed to position a 0.018” pressure sensor guidewire (Comet™, Boston Scientific, Marlborough, MA) and standard guidewire. A flexible ureteroscope was then introduced into the renal pelvis and the position of the ureteroscope and the pressure sensor wire were confirmed. Infusion of irrigation fluid (5% ethanol in saline) at target renal pelvic pressures (37‐150 mmHg) was maintained for 60 minutes using a pressure bag and instantaneous feedback from the pressure‐sensing guidewire. Venous blood sampling was performed every 10 minutes. Each trial started with blood EtOH of 0 mg/dL. Volume of irrigant absorbed was determined with established equations utilizing animal blood EtOH, weight, and irrigation concentration.
Results: Fourteen (14) pig kidneys were used during the study. The average irrigation volume absorbed after 60 minutes of irrigation were 4.9, 7.9, 24.9, and 72.5 mL of fluid at renal pelvis pressures of 37, 55, 75, and 150 mm Hg, respectively (P = 0.07) . At renal pelvis pressures of 55 mm Hg and above, pyelovenous backflow occurred as early as 20 minutes. At renal pelvis pressures of 37 mm Hg, pyelovenous backflow was not measured until at least 40 minutes of procedure time. Increasing renal pelvis pressures were associated with increases in fluid absorption for all pressures tested.
Conclusions: In this study of a swine model of ureteroscopy, increasing renal pelvis pressures during ureteroscopy were associated with increases in fluid absorption as well as more rapid fluid absorption, and the timing of the onset of pyelovenous backflow was delayed at lower pressure. This model may be used in the future to better understand the relationship between renal pelvis pressure and pyelovenous backflow during ureterorenoscopy.
Between a stone and a hard place: symptom management prescribing trends in patients undergoing ureteroscopic lithotripsy and stenting
F Rahman, A Kandabarow, PM Patel, E Chuang, A Druck, AV Farooq, TT Turk, K Baldea
Loyola University Chicago Stritch School of Medicine
Introduction & Objective: Ureteral stent discomfort is a major concern post‐ureteroscopy. Its etiology is complex and symptoms include bladder and ureteral spasms and pain. Ideal combinations of medications to reduce stent discomfort have been investigated, with earlier studies focusing on narcotics. However, physicians have recently been encouraged to minimize opioid use. As urologists find themselves stuck between managing ureteral stent discomfort and exacerbating the opioid epidemic, we analyzed physician prescribing behaviors in patients with uncontrolled stent discomfort after ureteroscopic lithotripsy.
Methods: We performed a retrospective review of all cases of ureteroscopic lithotripsy with ureteral stent placement at a single institution from 2014‐2017. Data included patient factors, medical history, intraoperative elements, medications prescribed at discharge for symptom control, and unplanned patient contact either via telephone or emergency department visit regarding stent discomfort within 30 days of surgery. We stratified additional prescriptions ordered during these unplanned contacts into narcotics (NA) vs. non‐narcotics (NN). We used multivariate logistic regression to analyze physician prescribing trends.
Results: Within our cohort of 532 cases, 92 patients (17%) received additional analgesics within 30 days of surgery. Younger age (OR 0.97 [0.95‐0.99], p = 0.03 for NA, OR 0.97 [0.95‐0.99], p = 0.02 for NN), female sex (OR 2.3 [1.0‐5.2], p = 0.05 for NA, OR 2.3 [1.2‐437], p = 0.02 for NN), intervention on a non‐obstructing stone (OR 0.34 [0.15‐0.78], p = 0.01 for NA, OR 0.47 [0.24‐0.95], p = 0.03 for NN), and not being pre‐stented prior to intervention (OR 0.38 [0.15‐0.99], p = 0.05 for NA, OR 0.25 [0.10‐0.61], p < 0.01 for NN) were all associated with receiving both additional NA and NN. Further, preoperative use of opioids for chronic pain was associated with receiving additional NA (OR 3.4 [1.5‐7.8], p < 0.01), and having bilateral ureteral stents was associated with receiving additional NN (OR 2.2 [1.1‐4.5], p = 0.03).
Conclusions: Younger age, female sex, surgery on a non‐obstructing stone, not being pre‐stented prior to surgery, prior chronic opioid use, and bilateral stents were all risk factors for receiving additional analgesia after ureteroscopic lithotripsy and stent placement, while medications prescribed at surgery discharge were not. More work is needed to understand whether these patients experience stent‐related symptoms more severely than others or whether providers are more likely to offer these patients additional prescriptions.
Emergency external shockwave lithotripsy for acute ureteric obstruction
W Maynard, E Maher, S Wong, A Goyal, L Ajayi, S Murphy, D Allen, R Kucheria, D Beder, G Chiriaco
Royal Free Hospital London
Introduction & Objective: Extracorporeal shock wave lithotripsy (ESWL) is an established, effective and safe first line non‐invasive therapy modality for the treatment of urinary tract stones. Its benefit in the emergency treatment of stones in the presence of acute renal colic and ureteric obstruction has not been widely studied. The objective of this study was evaluate the effectiveness of ESWL in the emergency management of obstructing ureteric calculi
Methods: A retrospective review of all patients referred and treated through the emergency pathway for ESWL between February 2019 to January 2021. Data was collected from electronic patient records and the local imaging (PACS) database.
Results: There were 42 patients identified who underwent ESWL for ureteric stones. Mean stone size was 6.8mm +/‐ 1.9. Stone position: 19% (8) PUJ, 35.7% (15) proximal ureter, 11.9% (5) middle ureter, 21.4% distal ureter and 9.5% (4) VUJ stones. . Average stone density was 640 HU +/‐ 262. 95.2% (40) patients had hydroureter or hydronephrosis, 28.6% (12) had more than one stone, 85% (34) patients had a reduced eGFR and 35.7% (15) had a white cell count outside of the normal reference range. The mean number of shocks used was 2219, with 3000 shocks most commonly delivered. The median number of treatments for the targeted stone was 1 (range 1‐2). Treatment was abandoned in 1 patient (2.57%) due to pain. Following up imaging was available in 34 patients. 82.35% (28) patients had passed the targeted stone, 14.71% (5) had evidence of stone fragmentation and 2.94% (1) stone was unchanged. 4.76% (2) patients progressed ureteroscopy for complete stone clearance. 11.9% (5) patients attended the emergency department following ESWL, 2 due to pain, 2 due to ureteric obstruction and 1 due to infection.
Conclusions: This series shows ESWL is an emergency treatment for obstructing ureteric calculi. ESWL should be considered in the acute setting wherever suitable and available.
Moderated Poster Session 14: Stents & Equipment I
Repair rate and associated cost of reusable flexible ureteroscopes: A systematic review and meta‐analysis
T Tailly, D Rindorf, BK Somani, O Traxer, GM Kamphuis, S Larsen, L Ockert, K Koo
University Hospital Ghent
Introduction & Objective: The refined mechanics of the flexible ureteroscope (fURS) is known to be vulnerable to damage necessitating routine repair. Repair of fURS is costly and makes the device unavailable for clinical use. With the introduction of single‐use ureteroscopes, accurate assessment of the resources required for fURS maintenance and repair is especially relevant. The aim of this study was to systematically review available literature and estimate 1) the total weighted repair rate of reusable fURS and 2) the average repair cost per ureteroscopy using meta‐analysis.
Methods: A systematic review was conducted by searching the databases MEDLINE, EMBASE, Web of Science and Cochrane library for studies estimating the repair rate of fURS used for ureteroscopy procedures. Study eligibility and data extraction was evaluated by two reviewers independently. Data on average repair cost of all repairs identified in the included studies was extracted if reported. A random‐effects model was used to calculate the pooled total repair rate of fURS. The total weighted repair rate and the average cost per repair were multiplied to provide an average cost of repair per ureteroscopy procedure.
Results: We identified 15 studies that fulfilled the inclusion criteria, which included 219 repairs from 3,642 investigated ureteroscopy procedures. The calculated weighted repair rate was 5.96% ± 0.646 (95% confidence interval [Cl]: 4.70% ‐ 7.23%; I2 = 60.8%), equivalent to 17 ureteroscopy procedures before repair. The average cost per repair was 5,746 USD and according to the weighted repair rate of 5.96%, this corresponds to an average repair cost of 357 USD per procedure. Egger's regression test did not indicate significant publication bias (Egger's test p > 0.05). A subgroup analysis of the repair rate of major repairs showed a weighted repair rate of 4.52% ± 2.571 (95% Cl: 2.00% ‐ 7.04%; I2 = 76.0%).
Conclusions: This is the first meta‐analysis to estimate the repair rate of fURS used for ureteroscopy. Our analysis demonstrates a repair rate of 5.96%. This indicates an average of 17 ureteroscopy procedures in between fURS repairs and a repair cost of 357 USD per procedure. High‐volume ureteroscopy practices should consider fURS breakage rates and repairs costs to optimize the use of reusable versus disposable devices.
Withdrawn
The efficacy and the safety of the J Fil Stent in the post operative endoscopic procedures: the experience on 237 cases
F de Marco
Urology Villa Betania Hospital
Introduction & Objective: The insertion of a drainage device into the urinary tract, after an endoscopic procedures, is sometimes controversial. The use of a drainage after an endoscopic procedure is necessary to drain the urinary tract, to facilitate the passage of residual fragments, to permit a safe healing of the ureter and in two steps procedures to prepare the ureter. In some cases the insertion of a stent is the first step for the 2 staged F‐URS. Despite all these advantages the presence of a double J stent is very often responsible in the patients for back pain, lower urinary tract symptoms, sexual dysfunction and social impaiment.
Methods: We evaluted the efficacy, the safety and the tolerability of a new design drainage device: the J Fil. This new designed device consists of a proximal part ring with a shaft of 16 or 8 cm and a 3 cm distal part cut in angled way where two, 14 or 22 cm, 5/0 prolene strings are connected. In a series of 237 patients who underwent to an endoscopic procedures we inserted the J Fil (228 the 16 cm and 9 the 8 cm). The series included 109 renal stones, 111 ureteral stones and 7 patients with other ureteral disorders. All the patients the insertion was obtained under fluoroscopy and an endoscopic control of the right positioning into the bladder at the end of the application. All the patients were followed up at 30 days using an KUB and ultrasound scan. The evaluated the efficacy of the J Fil as drainage and the tolerability using the USSQ. We evaluated also the best way and the problems due to the JFil removal.
Results: We reported 2 cases of the upward dislocation of the strings into the ureter during the first period of the learning curve. One case of self expulsion of the mini Jfil. One early removal of the Jfil due to fever. We removed the Jfil on 150 patients at 30‐60 days of the follow up using the Perez Castro forceps without technical problems. The ultrasound renal scan revealed a reduction of the hydronephrosys in 144 of 150 patients (96%). In 6 patients we reported back pain who requested some more drugs: the kub evaluation revealed a wrong positioning of the ring of the Jfil in the upper calyx (learning curve). In 2 patients we observed very small rounded calcification of the strings. The evaluation of the USSQ showed a very low impact of the Jfil insertion on the quality of life. In particular all the patients who were stented in the past referred a “completely different and better tolerance” with the Jfil
Conclusions: The stenting of the urinary tract is very common after the endourological procedures. But the presence of a Double J has a important impact on the quality of life of the patients. The Jfil seems to be effective as drainage and on the reducing the lower urinary tract symptoms associated to its presence.
A Pilot Single Centre Prospective Comparative Study of two digital single use flexible ureterorenoscopes‐ Indoscope (Bioradmedisys™, Pune, India) and 7.5Fr Uscope™ PU3033A Zhuhai Pusen, China)
S Agrawal, A Singh, A Ganpule, R Sabnis, M Desai
MPUH
Introduction & Objective: A single‐use disposable digital flexible ureteroscope (fURS) has become a cost‐effective alternative option to reusable fURS. Requirement of large diameter access sheath for passage of 9.5 Fr single‐use fURS have not always achieved in the first attempt in all cases leading to stage stone clearance. Recently two slimmest single‐use digital disposable fURS have been introduced by Bioradmedisys™ and Pusen™ to mitigate the accessibility problem without the requirement of access sheath or with small size access sheath.
The primary objective was to compare in‐vivo performance and surgical outcomes with two single‐use ureteroscopes: 7.5 Fr Indoscope (Bioradmedisys™, Pune, India) and 7.5 Fr Uscope PU3033A (Pusen, Zhuhai, China).
Methods: 60 patients undergoing Retrograde Intrarenal Surgery (RIRS) with <2cm renal stones, were prospectively randomized into: Group 1(30 patients) for Indoscope and Group 2 (30 patients) for Uscope PU3033A. Pre‐operative, intra‐operative, and postoperative parameters were evaluated. In vivo visibility, maneuverability was rated on a 5‐point Likert scale by the operating surgeon. At one month stone clearance was assessed with USG KUB and X‐ray KUB. Data was analyzed using SPSS 24.0. Continuous variables were analyzed with Mann‐Whitney U tests and two proportion tests was used for other parameters.
Results: Patient demographic and stone characteristics were comparable in both groups. The Indoscope had significantly higher visibility (p < 0.01) and outperforms the Uscope PU3033A however the maneuverability scores were comparable between both the groups(p > 0.05). One patient in group 1 needed ureteral dilatation before scope insertion (p = 0.31).
No differences in operative time, stone clearance, scope failure or complication rates were observed in both groups.
28 patients in group 1 and 26 patients in group 2 achieved complete stone clearance(p = 0.38). Scope failure was seen in 1 case of group 2 (p = 0.31) and the postoperative complication rate were comparable between both the groups.
Conclusions: We conclude that 7.5Fr Indoscope has better vision than 7.5Fr Uscope PU3033A and rest of the in vivo performance were comparable in clinical settings with similar outcomes and complications amongst both scopes. Larger clinical trials are needed to confirm the efficacy of these two single‐use flexible ureteroscopes.
Single‐use flexible ureteroscopes: comparative in‐vitro analysis of four scopes
AP Patil, S Agrawal, R Batra, A Singh, A Ganpule, R Sabnis, M Desai
Muljibhai Patel Urological Hospital Nadiad
Introduction & Objective: Single‐use digital flexible ureteroscope(fURS) have recently become attractive option to reusable fURS for various reasons. Many single‐use scopes have been introduced by different companies. Goal of our in‐vitro study was to compare four single‐use fURS, regarding deflection, optical characteristics and irrigation
Methods: We performed in‐vitro analysis of‐7.5Fr Uscope and 9.5Fr Uscope(Pusen™, China), LithoVue™(Boston Scientific, USA) and Indoscope(Bioradmedisys™, India). Optical characteristics(image resolution, color representation and luminosity) were compared at various distances. Deflection and irrigation were evaluated with empty working channel and with accessories.
Results: Color perception was comparable for all scopes at 1cm(p < 0.05), while Lithovue 9.5Fr was comparable with Indoscope 9.5Fr at 2 and 5 cm. Both these scopes were statistically better than both Uscopes at 2 and 5 cm. Image resolution power were comparable amongst all ureteroscopes at 10 and 20‐mm distance(3.56 lp/mm). However, Indoscope(3.56 lp/mm) was superior to LithoVue and Uscope scopes(3.17 lp/mm) at 50mm. Luminosity at 10 mm was comparable for LithoVue and Uscope 9.5Fr. But at 20 and 50mm, LithoVue had highest and Uscope7.5Fr had lowest luminosity. Indoscope had lower luminosity than other 9.5Fr scopes at all distances. With empty working channel and 200‐μm laser fiber, Indoscope had maximum deflection(2850) than rest scopes. With basket, 7.5Fr Uscope had maximum loss of deflection(30 degree) while Indoscope had no deflection loss. With empty working channel, all scopes had comparable irrigation flow in both deflected and undeflected state. Similarly, with 200‐μm laser or basket, irrigation flow was comparable in all scopes
Conclusions: Color representation was equivalent for Indoscope and LithoVue, while being better than Uscope 9.5 and 7.5Fr Uscopes. Image resolution were comparable in all scopes at 10 and 20mm. Beyond 10mm, luminosity of LithoVue was highest and that of Uscope 7.5Fr was lowest. Deflection loss was minimum with Indoscope and is maximum with Uscope 7.5Fr. Irrigation flow was comparable in all scopes in all scenarios.
Stent Syndrome. Does the Diameter Matter? Results of a Randomized Prospective Trial
PN Contreras, M Frascheri, N Bonanno, S Butori, L Blas, C Ameri
Hospital Aleman
Introduction & Objective: Ureteral catheter related symptoms may vary amongst people, depending on many factors. Our objective was to compare the symptoms produced by three different catheter diameters and the impact in the quality of life using a validated questionnaire.
Methods: Between June 2016 and February 2021 we conducted a prospective trial of 180 adults patients with a single ureteral stone who required an ureteral stent placement as a primary treatment. Patients were randomized 1:1:1 depending on catheteŕs diameter: 4.7, 6 or 7 Fr, 60 patients in each group. A 26 cm Universa® stent was used in every cases. During the seventh and fourteenth day after the surgery, patients were requested to answer the ureteral stent symptoms questionnaire (USSQ). Results were compared using the unidirectional ANOVA test.
Results: The mean age was 48.3 years (±14.9 ), male/female relation was 2.37/1. Most of the patients referred pain: 93% claim being unable to live with symptoms, 47 % could not engage in sexual activity and 70% would be very unhappy in case of requiring another stent again. After the statistical analysis, 4.7 Fr. stents produced significantly less urinary symptoms than 6 and 7 Fr. catheters.
Conclusions: Ureteral catheter related symptoms deeply affected the quality of life in most cases. The 4,7 Fr. catheter produced significantly less urinary symptoms than 6 and 7 Fr. catheters.
Twelve Years of Experience with Metallic Stents for Malignant Ureteral Obstruction
N Bonanno, PN Contreras, M Frascheri, JN Bujaldon, L Blas, C Ameri
Hospital Aleman
Introduction & Objective: Obstructive uropathy due to oncological extrinsic compression is usually presented at advanced stages of the disease, announcing a poor prognosis. The management of these cases can be controversial for the urologist. Our objective was to study the results of the use of a metallic ureteral stents and the survival analysis of this population.
Methods: We retrospectively analyzed a series of patients with malignant obstructive uropathy treated with metallic ureteral stent (RESONANCE, Cook Medical) from 2008 to 2020. Hydronephrosis was evaluated by ultrasound (US) or tomography (TC). All patients underwent at least one imaging study (US or TC) within 3 months postoperatively. We focus on the need for urgent unscheduled surgical intervention as a catheter failure definition.
Results: Between Jannuary 2008 and December 2020, 57 patients showed a malignant obstructive uropathy treated with metallic ureteral stent, 18 of them underwent a bilateral stent placement. The mean age was 61.2 years (SD 14.4). The most frequent primary pathology was cervix cancer in 16 patients (28%). The median preoperative creatinine was 1.1 ng/ml (IQR 0.88‐1.68). 40 patients (70%) had moderate to severe ectasia. 48 patients were followed‐up and performed at least one imaging and blood test within of 30 postoperative days. 9 patients died or were lost to follow up within the first month and were excluded. The median follow‐up was 10.3 months (IQR 5.7‐20.4). 23 patients presented at least one complication (47.9%). Of these, 13 cases were treated conservatively while 10 (20.8% of the total) required an unscheduled surgical intervention with catheter removal. In those group, the median time to intervention was 6.2 months (IQR 2.5‐11.6). 39 patients died during study analysis (68.4%). The median overall survival was 6.8 months (IQR 1.4‐15.3) with a survival at 3, 6 and 12 months of 73.2, 65.1 and 49.4% respectively. On univariate analysis, ascites (p = 0.034), pleural effusion (p = 0.0) or 2 or more Alawneh risk factors were significantly associated with risk of death within 12 months.
Conclusions: In our series, most of malignant ureteral obstruction could be solved with a metallic ureteral stent. Only 20% of patients required an unscheduled intervention. Median survival was 6.8 months and was significantly associated with ascites, pleural effusion or 2 or more Alawneh risk factors.
Comparison of two digital disposable flexible ureteroscopes: a prospective study
L Berti, M Maltagliati, C Buizza, A Calori, M Justich, P Marcangeli, BC Rocco, M Sighinolfi, S Micali, G Bozzini
ASST Valle Olona
Introduction & Objective: Advances in the design of flexible ureteroscopes have recently led to the emergence of single‐use equipment. This technology allows to use a new endoscope for each case, saving resources with respect to maintenance, replacement and sterilization among others. The aim of this study was to compare clinical results achieved with 2 types of disposable flexible ureteroscopes: the LithoVue (Boston Scientific) and the Uscope 3022 (Pusen).
Methods: A prospective comparative study was performed on patients undergoing endoscopic upper urinary tract lithotripsy between October 2016 and August 2018. The first group underwent surgery with the Uscope 3022 flexible ureteroscope and the second group with the LithoVue flexible ureteroscope. Ethical committee approval was obtained, and patients signed the informed consent. Analyzed variables included total surgical time, fluoroscopy time, post‐procedural ureteral catheter requirement, stone free rate and complications among others. The results were evaluated using the Student's t‐test, the Mann‐Whitney test and Fisher's test.
Results: 70 cases were performed with the Uscope 3022 and 40 cases with the LithoVue. The two groups were comparable with respect to demographic and clinical variables, including stone size, location and Hounsfield units, as well as the presence of a double‐j stent prior to the procedure. Multivariate analysis showed no differences with respect to stone free rate (92.8% with the LithoVue vs 91.4% with the Uscope 3022, p = 0.7), need for post‐procedural double‐j stent, complications and hospital stay. Significant differences were found in total surgical time (45 vs 35 minutes, p = 0.04) and in fluoroscopy time (50 vs 20 seconds, p < 0.01), both in favor of the LithoVue. No issues regarding the performance of these two single‐use ureteroscopes, such as loss of deflection or image quality, were found.
Conclusions: This study shows that both devices are highly effective in achieving an adequate treatment of kidney stones. The reason for the differences in total surgical and fluoroscopy times (in favor of the LithoVue) are not clear. However, these findings could be related to better optical resolution, deflection capacity, field of view and irrigation flow compared to the Uscope 3022, as shown in previous reports.
Changing stenting culture ‐ an audit of post ureteroscopic stent insertion against current NICE guidance
O Gbolahan, C Popanes, H Kadhim, A Raza
London North West University Healthcare NHS Trust
Introduction & Objective: NICE's recent guidance on leaving patients with uncomplicated ureteric stones less 20mm stent free post ureteroscopy is controversial. Is the NICE guidance being followed by urologists?
Our aim is to audit local practice of stent insertion post ureteroscopy. We wish to compare local practice of stenting versus the new recommendations from NICE.
Methods: Retrospective audit of all patients (emergency and elective) who had ureteroscopy for stone disease followed by JJ stent insertion. Indications for post procedure stenting were recorded. Surgeons performing ureteroscopy completed a survey relating to the NICE guidance.
Results: 51 ureteroscopies were performed in 2 months (57% ureteric and 35% renal). Ureteric stone size mean was 8mm (4mm‐21mm) in the stented group and 4.5mm (1mm‐8mm) in the unstented group. Total post ureteroscopic stenting rate was 88% (45 patients) with only 2% of cases documenting the indication for stenting. 12/20 surgeons completed the survey (60%), 91% had performed more than 100 ureteroscopies, 36% were unaware of the guidance, 50% thought it was unsafe, 72% felt advice on when not to stent should be more specific in the guidance. Indications such as bilateral stones, high ASA score and procedure length were not seen as absolute indications for stenting.
Conclusions: Increased awareness and compliance with NICE guidance is necessary in order to decrease stenting rates and therefore reduce patient associated morbidity and cost to the NHS. Local urologists particularly trainees felt more detail on when not to stent would have increased their confidence in leaving appropriate patients unstented.
Quantitative analysis of ureteral stents: encrustation depends on indwelling time and stent region
S Zheng, P Amado, B Kiss, F Stangl, E Talon, A Häberlin, D Obrist, F Burkhard, F Clavica
ARTORG Center for Biomedical Engineering Research, University of Bern, CH
Introduction & Objective: Encrustations on indwelling ureteral stents cause significant complications which strongly affect patients' quality‐of‐life. Identifying the initial anchoring sites for encrusting deposits on the stent and their growth over time is extremely valuable for patient management and future innovations in stent design. This study aims to quantitatively assess the volumetric distribution of stent encrustations.
Methods: Double‐J polyurethane stents (6Fr/26cm) with mean indwelling time of 37.2 (11‐90) days were collected from patients with stone disease (n = 14). Each stent was divided into four different sample regions (figure 1a). Micro–Computed Tomography was used to acquire three‐dimensional images, which were segmented using a U‐Net (Convolutional Neural Network) to extract the volume of encrustations and stents. Encrustations on the external surface of the stent were excluded as they could partially fall off during stent removal. Luminal encrustations were analyzed in two groups with indwelling time shorter than 6 weeks (n = 10) and longer than 6 weeks (n = 4), respectively. Two sided Mann–Whitney U test was used for all statistical tests.
Results: Most side holes (marked by arrows in figure 1b) are found with significant traces of encrustations (orange color), and complete obstruction of stent lumen is observed from one sample with 90‐day indwelling time. Encrustation volume ratios (EVR), defined as the sectional encrustation volume divided by the sectional stent volume, in the renal pigtail and distal straight part both increase significantly after 6 weeks (figure 1c). The highest EVR is found in the proximal straight part in both groups, although its difference over time is not significant (p = 0.052) based on current data.
Conclusions: To the best of our knowledge, this study presents the first volumetric assessment of stent encrustations with information on spatial distribution. Current results suggest that encrustations in the renal pigtail and distal straight part increase most significantly over 6 weeks of indwelling time. Most side holes are associated with early encrustation developments, in line with the recent in‐vitro study by Mosayyebi et al. (J Endourol, 2018). These results warrant further investigations on the interplay between urine flows and micro‐particles/bacteria near the side holes.
Combined diamond‐like carbon and copper coating on polyurethane implants in a rat model
W Kram, C Ludwig, JE de La Cruz, H Rebl, A Springer, B Nebe, M Wienecke, N Buchholz, O Hakenberg
SVMC
Introduction & Objective: Ureteral stents are used for short and long‐term use in ureteral obstruction. Common complications are biofilm formation, encrustation, and cellular adherence which promote urinary tract infections and cause cellular proliferation in the ureter. The aim of this study was to assess surface‐modified polyurethane implants to inhibit bacterial adherence and encrustation using a new animal model.
Methods: The surface of the implants is composed by an alternating amorphous carbon layer (a‐C:H) with diamond‐like properties (DLC) and copper. Copper has antibacterial properties. In vitro investigations were carried out under standardized conditions for encrustation, biocompatibility and antibacterial properties. Synthetic urine was saturated with urease until the dynamic equilibrium was reached and an infection situation was simulated. In vivo, 54 Rats underwent subtotal unilateral transection of the ureter with insertion of a ureteric stent and end‐to‐end uretero‐vesical anastomosis. Animals were distributed into three groups: polyurethane implants only, polyurethane with DLC coating, and polyurethane with both, DLC and copper (Cu) coating, respectively. In‐vivo, encrustation of the ureteral implants was provoked by precipitation of calcium oxalate crystals through administration of ethylene glycol to the drinking water of the rats. Tissue changes were investigated by urine cytology and histology. Encrustation on the implants was analyzed qualitatively by energy‐dispersive X‐ray spectroscopy (EDX). Fourier‐transform infrared spectroscopy (FTIR) was used to determine both, quantity of encrustation and its crystalline components.
Results: This model allowed us to establish a safe antibacterial copper coating concentration. In combination with DLC, the coating may have a beneficial effect on biofilm formation and resulting encrustation.
Conclusions: The above described methodology including our established rat model can efficiently be used to assess material resistance to encrustation and infection, but also to assess inter‐ and re‐action between stent surface coating and urothelium.
Evaluation of One Week of Pre‐stenting on Porcine Ureteral Diameter
P Jiang, AS Afyouni, T King, S Dinh, M Ayad, C Kosmala, A Peta, A Brevik, L Limfueco, Z Okhunov, RM Patel, J Landman, RV Clayman
Department of Urology, University of California, Irvine
Introduction & Objective: Ureteral access sheaths (UAS) are used during ureteroscopy to facilitate passage of the ureteroscope and the extraction of renal and ureteral stone fragments. Larger UAS have the potential to improve surgical outcomes, but are often avoided by surgeons due to concerns of ureteral injury. Using a novel UAS force sensor developed at our university, we sought to evaluate the impact of ureteral stent placement on ureteral circumference and the force needed to pass dilators of increasing size.
Methods: Seven juvenile female Yorkshire pigs (14 ureters) were included in the study. The inner circumference of each ureter was determined using a set of Cook urethral dilators (ranging from 8‐24Fr in 2Fr increments, 37cm in length) in combination with the UAS force sensor before and after one week of stent placement. Each ureter was randomized to receive either a 4.7Fr or 7.0Fr stent (20cm in length). Maximum ureteral size was defined as successful passage of the dilator to the ureteropelvic junction at <6 Newtons (N) of force. Prior porcine and clinical studies have shown that 6N is the maximum force that can be placed on a UAS without incurring ureteral damage. Following passage of the largest dilator at 6N, flexible ureteroscopy was performed and a post‐ureteroscopic lesion score (PULS) was recorded.
Results: After one week of stent placement, the median ureteral inner circumference increased from 12Fr to 16Fr (p < 0.001). Thirteen (93%) of the 14 ureters increased in diameter following stent placement (Table 1). The ureteral inner circumference recorded after stenting reached 18Fr in 36% of cases with a maximum size of 24Fr. Right ureters had a greater increase in ureteral diameter after stenting than left ureters (p = 0.005). Stent size did not have an impact on the change in ureteral diameter (p = 0.573) (Table 2).
Conclusions: One week of ureteral stenting resulted in a 4F (1.33mm) increase in the inner circumference (diameter) of porcine ureters. Right ureters enlarged to a greater degree than left ureters.
Withdrawn
Evolution of Single‐Use Endoscopy: Benchtop and Clinical Assessment of a New Single‐Use Cystoscope
P Whelan, CJ Kim, C Tabib, K Boydston, GM Preminger, M Lipkin
Duke University
Introduction & Objective: Flexible cystoscopy is a frequently performed urologic procedure. However, single‐use flexible cystoscopes remain relatively unproven. Ambu has released a single‐use cystoscope, expanding their single‐use endoscopy profile. We performed a benchtop and clinical evaluation of the Ambu single‐use cystoscope.
Methods: Ten new Ambu cystoscopes were assessed for optical performance, flexion and flow rate with an empty working channel, a 0.035in hydrophilic‐tipped wire, 365μm laser fiber, 1.9Fr nitinol basket and 1.8mm flexible stent grasper. All cystoscopes were fully flexed 25 times and flexion remeasured. Optical resolution, distortion and depth of field (DOF) were compared to Olympus HD and SD cystoscopes. Clinical feedback was assessed for inpatient bedside procedures using a Likert scale (1‐5) assessing visibility, handling, flexion, and desire to use again and the NASA Task Load Index.
Results: Maximal upward and downward flexion exceeded 200° and 160°, respectively, for all working instruments. Within each instrument, there was no clinical difference in pre‐ or post‐cycling flexion. Working channel instrument did not affect upward flexion. The flexible grasper and laser had less downward flexion (p < 0.001) vs other instruments in pre‐ and post‐cycling. Flow rate was greatest with an empty channel and decreased with increasing working instrument size (p < 0.001). The Olympus HD scope resolution was superior at 3mm and 5mm, but not at other distances. The Ambu scope was superior to the Olympus SD scope at all distances except 3mm. DOF and distortion were similar. The Ambu scope (n = 17) rated better inpatient bedside visibility, flexion, desire to use again and overall rating (19 [19‐20] vs 16 [14.5‐17.5], p = 0.023). The Frustration index was superior with the Ambu scope.
Conclusions: The Ambu single‐use cystoscope shows good flexion performance and comparable optics to reusable cystoscopes. Inpatient bedside use rated superior user feedback vs the Olympus reusable cystoscope.
Is routine urinalysis indicated prior to urodynamics in the asymptomatic patient?
Z Yasen, R Oliver, L Crabtree, R Peggs, Y Khan, S Chowdhury
Barts Health ‐ Urology Department
Introduction & Objective: Symptomatic Urinary Tract Infection (UTI) is a relative contraindication to performing urodynamic studies, with patients either postponed until their infection is fully treated or covered with antibiotics in the case of recurrent or persistent UTI to minimise risk of sepsis. However, the role for routine urinalysis prior to urodynamics in the asymptomatic patient is unclear and currently there are no guidelines as to whether this should be performed, with practices varying between centres. The objective of our study was to assess the UTI rate within 30 days following urodynamics in asymptomatic patients who did not undergo routine pre‐procedure urinalysis testing.
Methods: A retrospective analysis was performed on patients who had undergone video urodynamics (VUDS) in our university hospital in London, UK, between August 2019 and January 2020. Inclusion criteria were asymptomatic patients over 18 years old who did not receive urinalysis testing prior to VUDS or peri‐procedural antibiotics. Data was obtained from patient clinical records, microscopy results and through patient telephone follow‐up. UTI was defined as any patient with either symptoms of UTI, treated by a clinician for UTI or positive urine microscopy within 30 days following VUDS.
Results: Of the 50 patients undergoing VUDS during the study period, 13 were not contactable, 4 were cancelled on the day, 3 lacked adequate data for analysis and 1 patient died prior to follow‐up. Therefore, 29 patients were included in the analysis. UTI within 30 days was identified 6 patients (20.7%). Of these, 4 had a history of recurrent UTIs. New UTI occurred in 2 patients (6.9%) both of whom were treated in the community by their general practitioner. No patients presented to the emergency department or required hospitalisation for UTI.
Conclusions: There is no clear guidance on the role of routine urinalysis in the asymptomatic patient prior to urodynamic studies. Our study suggests the rate of UTI in asymptomatic patients who did not undergo pre‐procedural urinalysis is high at 21%, although 14% had a history of recurrent UTIs. As such, clinicians should consider offering routine urinalysis to all patients undergoing urodynamics, including those who are asymptomatic. Furthermore, use of peri‐procedural antibiotics in asymptomatic patients with a history of recurrent UTI may be beneficial. However, larger prospective studies involving routine urinalysis prior to urodynamics would be desirable in assessing for a correlation between urinalysis result and associated UTI rates.
J DiBianco, A Dupati, S Daignault‐Newton, N Kachroo, BD Seifman, H Pimentel, CA Dauw, KR Ghani, f Urological Surgery Improvement Collaborative, S Hiller
University of MIchigan Department of Urology
Introduction & Objective: AUA guidelines advocate stent omission after uncomplicated URS in patients with ≤1.5 cm stones, but prestenting is not considered as criteria for stent omission. We aimed to determine if prestented patients should be included in the criteria for stent omission within the Michigan Urological Surgery Improvement Collaborative (MUSIC).
Methods: Using the MUSIC clinical registry we identified uncomplicated URS cases from 2016 to 2019. We defined this as low comorbidity (≤1 CCI), no anticoagulation/antiplatelet therapy, no anatomic abnormality, no positive preoperative urinalysis or culture, single stage procedure for ≤1.5 cm stone, and no intraoperative complication. We divided cases into prestented and non‐prestented groups. We assessed practice and surgeon variation in stent omission in those with ≥5 cases in each category. We fit multivariable models to assess if prestenting was associated with 30‐day emergency department (ED) visits.
Results: In total, 6263 uncomplicated URS were performed in 33 practices by 209 surgeons. 2243 (36%) patients were prestented. Stent omission rates in prestented and non‐prestented cases were 47.3% (range 0‐77.8%) and 26.3% (range 0‐62.1%), respectively (Fig. A). 15/17 (88%) practices performed stent omission at higher rates if the patient was prestented. Surgeon‐level data in prestented patients demonstrated stent omission rates from 0 to 100%, with 22.3% never performing stent omission (Fig. B). Prestented cases that were stented, compared to stent omission, had higher rates of ED visit (6% vs 3.1%, p < 0.0001) and unplanned hospitalization (2.6% vs 1.3%, p < 0.0001). In non‐prestented cases, there were no significant differences in ED visits (7.7% vs 8.3%; p = 0.48) or hospitalization (2.2% vs 1.9%; p = 0.63) in those stented vs stent omitted, respectively. Multivariate analysis demonstrated stenting in prestented cases was associated with increased ED visits (OR: 2.12; 95%CI: 1.37‐3.29, p < .0.001).
Conclusions: Data from our clinical registry shows that stent omission in prestented patients undergoing URS decreases unplanned healthcare utilization, and this scenario is an opportunity for quality improvement. Prestenting should be considered an inclusion criteria for stent omission in the AUA stone management guidelines.
Impact of ureteral stents on factors contributing to stricture pathogenesis
K Doersch, K Almutairi, BH Chew, D Lange
Department of Urology, University of Rochester Medical Center
Introduction & Objective: Ureteral stenting is common for the management of obstructive uropathy. While much research into complications associated with stents has been completed, none has focused on understanding the molecular response of the ureter to stents, which may drive pain and discomfort. Recent preliminary work suggests that stents trigger pre‐fibrotic changes in ureteral tissues. To investigate this concept further, the objective of this work was to evaluate the impact of ureteral stents on pro‐fibrogenic signaling associated with stricture pathogenesis.
Methods: Pigs (n = 3) were stented unilaterally for 14 days with the unstented side serving as the control. Additional pig ureters (n = 3) were stented for 14 days and then allowed to recover for 7 days (recovered group). Ureters were analyzed by RNAseq and proteomic analysis to evaluate the presents of pro‐fibrotic factors.
Results: RNAseq demonstrated that the stented ureter had increased transforming growth factor (TGF)‐β2, and TGF‐β‐receptor(R)‐2 compared with the unstented ureter. Stenting altered Collagen (Col) RNA levels, with increases in Col 8A1, 4A2, 6A5, 1A2, and 3A1, among others, compared to the unstented group. Compared to the stented group, the recovered group had reductions in TGF‐β2 and Col 4A2, 6A5, 1A2, and 3A1 RNA expression. Compared to the unstented group, the recovered group had increased expression of Col 12A1, 17A1 and 8A1 RNA and decreased Col 53A and 8A2. Proteomic analysis demonstrated that compared to the unstented group, the recovered group had increased Col 6A2, 6A3, and 7A1 and decreased Col6A6 and 5A3. The recovered group had few differences in protein expression and no changes in Col levels compared to the stented group.
Conclusions: Indwelling stents result in alterations in signaling pathways associated with stricture formation, an effect that has not been reported previously and may contribute to stent‐associated ureteral dysfunction, pain, and discomfort. Some of these alterations revert to patterns similar to unstented ureters, while others remain aberrant 7 days after a stent has been removed. Studies investigating whether these changes revert to normal following stent removal or result in longer‐lasting decreased ureteral function are warranted.
Biodegradable metals for ureteral stents applications: understanding the degradation profile under simulated urinary tract environment
M Pacheco, JM Silva, IM Aroso, J Bohlen, M Nienaber, S Lamaka, M Zheludkevich, E Lima, A A. Barros, R L. Reis
i3Bs Research Institute on Biomaterials, Biodegradables and Biomimetics, University of Minho
Introduction & Objective: A biodegradable metallic ureteral stent (BMUS) is expected to have unique properties, such as a slower degradation rate and improved radial strength, ideal characteristics for prolonged treatments and/or cases of high external compressions (e.g. tumour). Therefore, a BMUS will be a ground‐breaking step in the ureteral stent's development. In this work, the corrosion profile of different biodegradable metals in simulated urinary conditions was addressed in detail.
Methods: AZ31, Mg‐1Zn, Mg‐1Y, pure Mg and Mg‐4Ag wires were produced by direct extrusion at 350⁰C with 0.2 mm/s speed. The study was performed under static and dynamic conditions with constant artificial urine (AU) flow – ASTM Standard F 1828 – 97 (2006) ‐ for 1, 2 and 4 weeks. Scanning electron microscopy with energy dispersive spectroscopy (SEM‐EDS), inductively couple plasma optical emission spectrometry (ICP), X‐ray photoelectron spectroscopy (XPS), X‐ray powder diffraction (XRD) analysis and weight loss were performed. Further analysis are ongoing.
Results: Different corrosion/encrustation layers were observed. In Mg‐1Zn, the layer was intense and with a lighter colour, whereas AZ31 formed spots with higher accumulation of compounds along the wire, which disintegrated after metal's drying. The layers are mostly composed of O, Mg and P, as indicated by EDS and XPS, and XRD results indicated the presence of struvite in all samples. The SEM analysis suggested that Mg‐4Ag had the highest corrosion degree. AZ31, Mg‐1Zn and Mg‐4Ag presented an inhomogeneous corrosion with notable pitting points, whereas Mg‐1Y and pure Mg had a more homogeneous surface. The weight loss results showed that the continuous flow accelerates the metal's degradation and that corrosion prevails in the upper part of the wires. Preliminary mechanical tests showed that JJ spring‐shaped stents, with shape memory, can be produced from Mg metal wires (Fig1.)
Conclusions: It is evident, and confirmed by the literature, that the metal's degradation also depends on its own composition, as demonstrated in this work by the different corrosion profiles and surface layers. The layers' composition seems to be a mixture of both encrustation and metal's degradation products. These preliminary outcomes do not meet the required characteristics of preventing encrustation or homogeneous degradation, but optimizations are currently on going regarding the metal's processing procedure. Additionally, an Mg‐based JJ stent can be produced.
Implementation of single use disposable digital ureteroscopes in a large public tertiary care center leads to decreased operative room and procedure times
C Schuster, MS Carey, RI Carey
Florida State University College of Medicine
Introduction & Objective: We evaluate the improvement in operating room time (ORT) and procedural time (PT) in an 836 bed tertiary care county hospital that underwent conversion to disposable digital ureteroscopes (DDUs) from an inventory of refurbished flexible ureteroscopes (RFUs).
Methods: Data is collected from an IRB approved prospectively maintained database of flexible ureteroscopy cases performed between January 1, 2014 and January 1, 2021 at a hospital that previously provided ureteroscopes exclusively through an inventory of RFUs until conversion to exclusive use of DDUs. The same 120 watt holmium laser and laser fibers were used throughout the study. There was no change in the disposable wires, access sheaths or ureteral catheters and stents. All refurbished scopes were provided by an out‐sourced third party vendor, not the original manufacturer.
Results: Combining the cases of two Endourology Fellowship trained surgeons, a total of 640 ureteroscopies were performed using RFUs and 865 with DDUs. Upon switching from the inventory of RFUs to single use DDUs , there was a 9.5 % decrease in the ORT and a 9.3% decrease in the PT. The mean OR time dropped from 78.6 min to 71.1 min. The mean procedure time dropped from 38.9 min to 35.3 min.
Conclusions: Replacing an inventory of RFUs with single use DDUs results in significant decrease in ORT and PT for all ureteroscopy. The decrease in ORT and PT is in part due to superior performance of the DDU but also avoiding inconvenience of starting a case with a catastrophically damaged unusable RFU and having to wait for another to be procured. The decrease in ORT and PT results in financial gain as does the cost savings of having no scope cleaning, no sterile processing and no scope repair costs. Those savings must be weighed against the cost of the single use DDUs.
Proximal and distal ureteral stent curls exhibit differences in biofilm microbiota with high inter‐individual variability
G Werneburg, S De, R Rackley, D Shoskes, A Miller
Cleveland Clinic Foundation
Introduction & Objective: Ureteral stents, which are frequently utilized to establish urinary tract drainage, or transiently maintain ureteral patency, may serve as a nidus for infection through biofilm formation. Antimicrobial prophylaxis does not reduce stent‐associated biofilms or urinary tract infections. Thus, there is immense interest in the development of stent materials and coatings resistant to microbial adhesion and subsequent infection. In this investigation, we sought to determine the microbial composition of stents in different stent regions and individuals. We hypothesized that ureteral stents would consistently harbor microbiota and exhibit patient‐to‐patient variability similar to that of urine microbiota.
Methods: We identified patients scheduled to undergo ureteral stent removal. Patients were consented per our IRB‐approved protocol, and upon stent removal, both the proximal and distal ends were sampled using standard culture swabs. The swab samples, alongside controls, were subjected to next‐generation 16S rRNA sequencing to determine their composition and diversity. Microbial diversity between proximal and distal ends of the stents, as well as between individuals, was compared using t‐tests and principal components analyses.
Results: Analysis was performed on 38 stent regions from 19 stents. The proximal and distal ends of the stents exhibited significant differences in microbial composition (p < 0.001, Figure left panel). Stents harbored significantly different microbiota across individuals (Figure right panel, p < 0.001, greater difference between points reflects greater dissimilarity; each dot on a line represents a proximal or distal stent end for a particular patient).
Conclusions: All ureteral stent regions harbored bacteria. Microbiota composition differed between the proximal and distal stent ends, as well as from individual to individual. The inter‐individual variability was greater than the variability between the proximal and distal ends. Our results open avenues for efforts to design targeted stent coatings and materials to prevent and disrupt biofilm formation, which in turn may reduce stent‐associated urinary tract infection risk. Based on these results, ongoing investigations aim to compare the stent microbial composition between patients with and without clinical infection, as well as determine associations between stent microbiota and that of the urinary tract.
Double J‐eopardy: risk factors for seeking acute care due to ureteral stent discomfort
E Chuang, AM Kandabarow, PM Patel, F Rahman, A Druck, AV Farooq, TT Turk, KG Baldea
Loyola University Chicago Stritch School of Medicine
Introduction & Objective: Ureteral stent placement is both common and necessary in ureteroscopic lithotripsy. However, many patients with stents experience bothersome urinary symptoms and pain, often causing them to seek unplanned medical care for symptom control. While studies generally agree that the pathophysiology of stent discomfort is multifaceted, there is no consensus on what patient risk factors are associated with it. In this study, we sought to detect risk factors associated with stent discomfort by examining the incidence of unplanned postoperative healthcare encounters following ureteroscopic lithotripsy with stent placement.
Methods: We retrospectively reviewed all cases of ureteroscopic lithotripsy with stent placement at a single institution from 2014‐2017. Patient demographics, medical and surgical history, procedure details, and discharge prescriptions were recorded. We noted if patients called our telephone triage line or presented to the emergency department complaining of discomfort within thirty days of their procedure. Multivariate logistic regression was used to determine factors associated with this event.
Results: Five hundred and thirty two patients met our inclusion criteria, with one hundred and fifty three (29%) generating unplanned encounters within thirty days for symptom control. Patients seeking symptom control were younger (0.98 [0.96, 0.99], p = 0.02), more likely to be female (3.0 [1.6, 5.6], p < 0.01), have a psychiatric diagnosis (2.1 [1.1, 3.8], p = 0.02), not pre‐stented (0.44 [0.26, 0.76], p < 0.01), have a longer stent (1.18 [1.02, 1.37], p = 0.03), and not prescribed nonsteroidal anti‐inflammatory drugs (NSAIDs) at discharge (0.18 [0.04, 0.83], p = 0.03). No intraoperative variables such as access sheath use, ureteroscope type, operative time, or the presence of residual stones after lithotripsy were significant predictors of seeking unplanned care.
Conclusions: Patient characteristics, stent length, and postoperative prescribing behavior, rather than procedural factors, were shown to be the strongest drivers of ureteral stent discomfort. More work is needed to identify interventions that can reduce excess healthcare utilization in these at‐risk populations.
Moderated Poster Session 15: Lasers I
First clinical results of a novel pulsed Thulium:YAG laser for lithotripsy during mini‐PCNL
B Becker, J Bergmann, CM Rosenbaum, AJ Gross, C Netsch
Department of Urology, Asklepios Hospital Barmbek, Hamburg, Germany
Introduction & Objective: Laser lithotripsy plays a key role in stone treatment during mini‐PCNL. Innovative pulsed thulium lasers promise extensive possibilities to carry out the procedure with high precision and effectiveness. This study was carried out to investigate the safety and efficacy of the new Revolix HTL 150W Hybrid Thulium Laser (Lisa Laser Products GmbH) during mini‐PCNL.
Methods: 40 patients were recruited prospectively. All patients undergoing mini‐PNL using the pulsed thulium laser were included regardless of stone size. Operation times, stone size, laser time and laser settings were noted. The stone‐free rate was assessed postoperatively using sonography, x‐ray or computed tomography as clinical standard. The complications were analyzed using the Clavien‐Dindo classification.
Results: A total of 40 patients with an average age of 50 years were included. The average stone size was 248 mm2 with an average density of 830 (+/‐ 337). The mean operating time was 23 (+/‐10.3) minutes and the laser on time was 06:04 (+/‐ 07:18) minutes. The most commonly used settings were 0,4 J and 115 Hz (46 W). The mean total energy for stone ablation was 13.573 (+/‐ 16.753) kJ. The total stone‐free rate was 82 % with an overall complication rate of 34,5% according to Clavien‐Dindo (grade 1: n = 8, grade 2: n = 3). One major complication (grade 4a) occurred.
Conclusions: The novel pulsed Revolix HTL enables safe and efficient lithotripsy during mini‐PCNL with high stone‐free rates and short operation times.
HIGH POWER LASER FOR HIGH STONE FREE RATES in 1 sitting ‐ is it achievable?: A prospective single centre Asian experience
R Mangat, Q Yufei, S Biligere, Q Yufei
Dept. of Urology
Introduction & Objective: 60‐120 watt Holmium laser has revolutionized Retrograde Intrarenal surgery (RIRS) . Best outcome is when we can produce high Stone Free Rates (SFR) in a single sitting .
Assess our outcomes in SFR with high power laser (HP‐RIRS) for renal stones and analyse the predictive factors for stone free rate (SFR) in our practice.
Methods: Single centre, prospective study, Jan 2018‐2020. 133 renal units underwent HP‐RIRS in the MEL position (figure 1) with a Lumenis 120watt laser (1). SFR defined as: no visible stones or clinically insignificant residual fragments (CIRF) <3 mm on postop CT scan 1‐3 months post‐op. Predictive factors for SFR were evaluated based on demographics, stone burden and stone location.
Results: Table 1 Table 2 Chart 1 The mean cumulative stone burden was 16.79 ± 10.42 mm. Overall SFR was 92.5%. The overall complication rate was 5.6%.
Conclusions:We achieved excellent overall SFR in a single setting. Like most studies predictably low stone burden had most favourable outcome However with Lithovue and HPRIRS in our series we had excellent lower pole SFR despite in‐situ , non respositioning pop‐dusting . This because with HP laser we can vary multiple settings favourably. MEL position, gated respiration and endoflow Traxier pump allowed for focussed lithotripsy with better vision.
60Watt Superpulse Thulium Fiber Laser in Retrograde Intrarenal Surgery‐Aiming towards faster dust
D Vaddi, P Ramakrishna, P Siddalinga Swamy, B Manas Babu, G Soundarya, A Hemnath, P Rakesh
Preeti Urology & Kidney Hospital
Introduction & Objective: In the recent years, Thulium fiber laser (TFL) has been producing promising results in preclinical studies. Objective is to evaluate the efficacy and safety of TFL during Retrograde intrarenal surgery (RIRS). Secondary aim is to analyse the optimal mode of lithotripsy with 60Watt TFL
Methods: A prospective study was done on 109 patients with less than 20mm renal stones, who underwent RIRS using TFL (IPG Photonics, Oxford, Massachusetts, United States). Stone size, volume, density, laser on time (LOT), total energy delivered (kJ), fiber burn‐back were recorded. Laser efficacy (J/mm3), ablation speed (mm3/sec) were calculated. Visibility was graded using 5‐point Likert's scale (5 – best, 4 ‐ good, 3 – intermediate, 2 ‐ bad, 1 – worst). Stone‐free rate (SFR) was calculated using CT at 3 months post operatively
Results: Mean age was 42.03 ± 11.30 years; mean stone size was 13.34 ± 3.59mm, mean stone volume was 1061.85 ± 806.81 mm3, mean stone density was 985.82 ± 302.57 HU. The settings used were 0.1‐0.2J, 60‐ 100Hz (6‐20W) in Dusting mode, 1‐2J, 6‐30Hz (6‐45W) in Fragmentation mode and 0.1 – 0.2J, 100‐ 300Hz (5‐55 W) in Popcorning mode. Mean LOT was 19.78 ± 12.32 minutes. Mean energy consumed was 13.06 ± 8.93 KiloJoules.
Mean laser efficacy was 14.35 ± 5.70 J/mm3. Mean ablation speed was 0.86 ± 0.31mm3/sec. Subgroup analysis revealed LOT was lesser with fragmentation mode compared to dusting mode (18.49 ± 11.90 vs 21.25 ± 12.75min, p = 0.169), ablation speed was higher in fragmentation mode (0.94 ± 0.32mm3/sec vs 0.77 ± 0.27, p = 0.005). Visibility was poor in fragmentation mode (Visibility > grade 3 was present in 57.1% vs 81.1%) and fiber burn‐back was higher (2.46 ± 3.83 vs 0.48 ± 0.97mm, p < 0.001). Overall SFR was 95.4%. 39.4% had complications namely hematuria and fever, out of which 37.6% (41/109) were Clavien grade 1.
Conclusions: Superpulse TFL is efficacious and safe. Faster lithotripsy was achieved with fragmentation mode, at the cost of increased fiber burn‐back
Thulium Fiber Laser: A Universal Device in Urology
M Taratkin, C Azilgareeva, L Rapoport, A Dymov, R Sukhanov, D Enikeev
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia
Introduction & Objective: The SuperPulsed Thulium fiber (SP TFL) laser was recently proposed as a new surgical tool for multiple applications in urology. In this study, we assess how effective this new tool is when it comes to both stone lithotripsy and genitourinary soft tissue surgery. Recent modification of TFL incorporates both SuperPulsed (500 W peak power, for lithotripsy) and quasi‐continuous (100 W peak power, for soft tissue surgery) lasers within a single apparatus.
Methods: After local IRB approval a prospective clinical trial in lithotripsy and soft tissue surgery have been started. Lithotripsy was performed with Thulium‐fiber laser (NTO IRE‐Polus, Russia), using 200 or 400 μm laser fibers in SuperPulsed mode. The postoperative stone‐free rate was assessed with low dose computed tomography three months after the surgery. Thulium fiber en bloc resection of bladder tumor (TFL‐ERBT) was performed using the following settings: quasi‐continuous mode, energy at 1.0 J, power at 10 W. Relapse free survival rates (RFS), pathologic assessment of specimens and perioperative complications were assessed. For thulium‐fiber laser enucleation of the prostate (ThuFLEP), TFL with 600‐μm laser fiber and 26 Ch resectoscope (Karl Storz, Germany) with continuous irrigation (0.9% saline) were used.
Results: A total of 268 patients underwent TFL lithotripsy, 118 patients – TFL‐ERBT, 1081 patients underwent ThuFLEP and 13 patients ‐ TFL urethrotomy. A total of 268 patients with urinary calculi were treated with Tm‐fiber laser (kidney – 153 (mean size 11.4 mm, mean density – 987 HU), ureter – 96 (mean size 7.6 mm, mean density – 995 HU), bladder – 19 (mean size 22.2 mm, mean density – 1050 HU). The stone‐free rate revealed 92%. En bloc resection of NMIBC was done in 118 patients and revealed muscularis propria in 91.5% of cases after TFL‐ERBT. The relapse‐free survival at 6 months was 82.2%. Laser enucleation was done in 1081 patients with a mean prostate volume of 90.3 ccs. Catheter stay and hospitalization duration were 1.3 days and 3.4 days respectively. At six months, IPSS and Qmax were significantly better than prior to surgery (p < 0.001). TFL optical urethrotomy in the patients with short urethral strictures (< 1.5 cm) was effective in 92% of cases at 6 months follow up.
Conclusions: Thulium fiber laser shows high efficiency and acceptable safety profile in the treatment of urinary stones, NMIBC, BPH and urethral strictures. The application of SuperPulsed and quasi‐continuous modes within a single device allowed for creation of universal tool for urologic surgery.
Pulse modulation with MOSES technology can reduce operative time in miniaturised percutaneous nephrolithotomy
M Popiolek, S Jarl, P Georgouleas, M Wagenius, P Sundqvist
Örebro University Hospital
Introduction & Objective: MOSES technology is a method for pulse modulation which can improve efficiency of lithotripsy and reduce stone retropulsion. However, the clinical impact on procedure time in miniaturised percutaneous nephrolithotomy (mPCNL) has not yet been well studied. The aim of this study was to investigate whether introduction of MOSES pulse modulation compared to the standard mode in holmium high‐power laser system (Lumenis Pulse 120H) may shorten operation time in mPCNL.
Methods: A retrospective analysis of 104 consecutive patients who underwent mPCNL in a tertiary center between March 2018 and February 2020 was performed. Procedures performed utilising the MOSES technology were identified and included in the study group (MG, n = 35). A control group (CG, n = 35) was recruited from the remaining 69 procedures, performed with a regular mode on the same holmium laser platform (Pulse 120H), through case controlled matching to avoid confounding. The groups were then compared with regard to patient‐ and surgery‐related variables.
Results: A total of 70 patients were included (35 in MG and 35 in CG). There were no significant differences between the groups regarding age, body mass index, sex distribution and Guy's stone score. Mean stone diameter and density were 21 (± 7) mm and 1025 (± 286) HU in MG and 21 (± 6) mm and 1081 (± 275) HU in CG. A 16 F access sheath with an active suction system was utilised during mPCNL in all cases. Similar laser settings, 1‐2 J, 20 Hz for fragmentation and 0.3‐0.5 J and 70‐80 Hz for dusting (contact or distance mode in MG and short/long pulse width in CG) were used in both groups. Mean operation time was approximately 18% shorter in MG compared to CG, 62 (± 19) min and 76 (± 24) min respectively (p = 0.004). Mean laser time and median total energy were similar in both groups (403 ± 305 s and 5.8 kJ in MG; 365 ± 283 s and 6.5 kJ in CG; p = 0.7). Total stone clearance (no residuals) was achieved in 76% and 74% (p = 0.78) in MG and CG respectively according to CT scans performed on the first postoperative day. One patient in MG developed a pseudoaneurysm and underwent selective angioembolization. The groups did not differ regarding postoperative hemoglobin drop or hospitalisation time.
Conclusions: Our findings suggest that MOSES pulse modulation can reduce procedure time compared to regular mode holmium lithotripsy in mPCNL. Laser time and total energy were similar in both groups suggesting that the time saved with MOSES technology depended mostly on reduced retropulsion facilitating efficient lithotripsy and evacuation of fragments.
The Novel Thulium Laser Results in Fewer Residual Stone Fragments During Lower Pole Lithotripsy
AS Amasyali, JD Belle, M Keheila, N Chen, M Hajiha, E Baldwin, DD Baldwin, A Assidon
Loma Linda University, Department of Urology
Introduction & Objective: Lower pole stones represent a unique challenge in ureteroscopic laser lithotripsy. Due to the dependent nature of the lower pole, residual fragments may persist and lead to stone growth. The novel thulium fiber laser (TFL) has smaller caliber laser fibers and a wider range of power frequency settings which may allow surgeons to individualize in situ lower pole stone treatment. The purpose of this study was to compare the TFL with a conventional holmium laser to determine what energy settings and fiber sizes result in the lowest residual stone fragments during in situ lower pole lithotripsy.
Methods: In a benchtop model, a 3D printed kidney and ureter were attached to a 2 x 2 mm metal mesh and submerged in a saline bath. Sixty‐five 1cm BegoStones (calcium oxalate monohydrate consistency) were placed in the lower pole and fragmented in situ by the same surgeon using a flexible ureteroscope. The stone was considered treated once all fragments had passed through the 2mm mesh grid. Laser lithotripsy was performed with the following fiber and setting combinations: 60W TFL at 1J x 20Hz (20W), 0.4J x 50 Hz (20W), 0.2J x 100Hz (20W), 0.1J x 200Hz (20W) for both 150 and 200 μm fibers; 100W Empower at 1J x 20Hz (20W), 0.4J x 50Hz (20W) for both 200 and 272 μm fibers. Residual stone fragments were collected, dried, and weighed. Independent T‐test and ANOVA were performed for statistical analysis and significance was set at p < 0.05.
Results: Pre treatment stone weights were similar between groups (p = 0.985). When using the thulium laser, less residual stone fragments remained compared to the holmium laser (10.99% vs. 17.28%, p < 0.01, Fig 1). Overall operating time was significantly different between 12 trials (p < 0.01). The TFL at 100Hz and 0.2J with the 150μm fiber had the fastest procedure time (18.5 min, p < 0.05). Thulium trials required less fiber stripping than holmium trials (0.15 vs. 0.44 times, p < 0.05).
Conclusions: Our study showed that use of the 60W TFL resulted in 57% less residual stone fragments when compared to the 100W holmium laser. This results in less need for spontaneous stone passage and potentially reduces stone reformation, making the TFL particularly desirable when treating lower pole stones in situ.
Is Less More When Using the Novel Thulium Laser: What Fiber Size and Laser Settings Result in the Most Efficient In Situ Lower Pole Lithotripsy?
AS Amasyali, JD Belle, M Keheila, N Chen, A Assidon, M Hajiha, E Baldwin, DD Baldwin
Loma Linda University, Department of Urology
Introduction & Objective: The novel thulium fiber laser (TFL) has advantages compared to the Holmium laser (HL) including smaller fiber size (150 μm) and higher frequency settings (up to 2000 Hz). These characteristics may be of particular benefit when performing in situ treatment of calcium oxalate monohydrate (COM) lower pole kidney stones. The purpose of this study was to determine the optimal fiber size and laser settings for in situ treatment of COM lower pole stones.
Methods: In a benchtop model, a 3D printed kidney and ureter were attached to a 2 x 2 mm metal mesh and submerged in a saline bath. Forty 1cm BegoStones (COM consistency) were placed in the lower pole and fragmented in situ by the same surgeon using a flexible ureteroscope. The stone was considered fully treated when residual fragments were small enough to fit through the 2mm mesh grid. Laser settings used were: 1J x 20Hz (20W), 0.4J x 50 Hz (20W), 0.2J x 100Hz (20W), and 0.1J x 200Hz (20W) for both the 150 and 200μm fiber sizes. Data collected included lasing time, procedure time, total pulse energy, and fiber stripping. ANOVA and independent T‐tests were used to compare outcomes between treatment arms with p < 0.05 considered significant.
Results: Pre‐procedure stone weights were similar between trials (0.99 gm, p = 0.944). Lasing time, overall procedure time, and total pulse energy were significantly different across all 8 trials (p < 0.05 for all; Fig 1 and 2). Overall, use of the 150μm fiber resulted in less total lasing time, procedure time, and pulse energy compared to the 200μm fiber (p < 0.05 for all). Lasing with 0.2J and 100Hz and the 150μm fiber had the shortest procedure time (18.5 min) compared to all other laser setting and fiber combinations (p < 0.05). There was no difference in the number of fiber strippings between groups (p > 0.05).
Conclusions: In this benchtop lower pole model of in situ treatment of COM stones, the 150μm laser fiber resulted in shorter lasing time, procedure time, and lower total pulse energy compared to the 200μm fiber overall. When comparing different laser energies and frequencies, the fastest procedure time was seen when using 100Hz and 0.2J. Understanding these data can help improve efficiency of treatment for dense lower pole COM stones in situ.
Same‐Day Catheter Removal after Holmium Laser Enucleation of the Prostate (HoLEP): What Predicts Failure?
DK Agarwal, T Large, M Lee, E Sahm, M Assmus, ME Rivera
Indiana University Department of Urology
Introduction & Objective: Since the introduction of same‐day catheter removal, there is limited data on factors associated with success or failure of this approach. We assessed our one year experience with this technique.
Methods: We performed a retrospective review of two surgeon's experiences with same‐day catheter removal after HoLEP at our institution. Preoperative, intraoperative and postoperative data were analyzed to see what factors were associated with failure of same‐day catheter removal.
Results: A total of 85 patients underwent HoLEP with same‐day catheter removal from January 2020‐February 2021. Mean age was 69 ± 8.8 years, preoperative catheter‐dependent urinary retention rate was 38% and prostate volume was 107.2 ± 51.6 ml. Antiplatelet/anticoagulant medications were used in 7%, and 11% had underwent a prior non‐medical BPH therapy. Operatively, ASA score was ≥3 in 40% of patients and 75% of cases utilized laryngeal mask airway. Bladder stones were present in 7%. Pulse modulated laser was used in 92% of cases. Mean enucleation time was 50.5 ± 21 min, morcellation time was 7 ± 6.2 min, energy usage was 132 ± 58.8 kJ, and tissue weight was 62.1 ± 45.8 g. The rate of successful same‐day catheter removal was 88% (75/85). Of the 10 patients who failed same‐day catheter removal, 80% successfully passed on postoperative day 1. There were 5 complications postoperatively, and only one was Clavien 3 or higher (bedside cystoscopic catheter placement). On a univariate statistical analysis, increasing age (OR 0.908 [0.840‐0.982]) and ASA score (OR 0.205 [0.0536‐0.785]) were associated with failure of same‐day catheter removal.
Conclusions: Same‐day catheter removal is a highly successful approach to HoLEP. Increasing age and were risk factors for failure.
Flexible ureterorenoscopy with holmium laser lithotripsy for upper urinary urolithiasis
M Jasser, R Mehdi, T Tarek, B Mohamed, B Wassim, K Ramzi, G Samir
Military hospital of Tunis
Introduction & Objective: The management of urinary stones has radically evolved over the years. The recent advent of flexible ureterorenoscopy made endoscopic approach to kidney calculi evolve to a real challenging procedure capable to treat the vast majority of renal stone.
We provide a brief overview of our experience with ureterorenoscopy for treating upper urinary tract stones, including success and complications of this treatment.
Methods: Over the last 5 years, 93 Patients underwent ureterorenoscopy with Holmium Laser lithotripsy for renal and proximal ureteral stones using flexible Ureteroscope (URF‐P6/P6R Olympus). Demographic informations, disease characteristics, perioperative data were gathered. The “stone‐free” status was defined as no evidence of stones or stones less than 4 mm on 3‐months postoperative Computed Tomography
Results: Our study included 57 male and 36 female patients. The mean age was 50 years. Half of patients (45%) had history of urolithiasis and 48% of them had already received a previous treatment. Among the treated subjects, 19 had proximal ureteral stones and the 73 patients had renal stones. Among subjects with renal stones, stone locations included upper calyx (10%), middle calyx (11%), lower calyx (21%), renal pelvis (22%). The mean number of stones per patient was 1,2. The mean stone size was 17.7 mm (range: 0.5–2.6 cm). The stone‐free status was achieved after the first procedure in 51% of cases. A second and third procedure were performed successively in 18 and 11 patients achieving a stone free rate of 71% and 81%. The mean number of procedures per patient was 1,2. Intra‐operative and post‐operative complications were seen in 14 (14%) and 26 (28%) cases, respectively.
No major ureteral injuries occurred. Mucosal abrasions were noted in 4 patients (4%) and managed successfully with a stent placement. All adverse events were classified by the Clavien Dindo grading system. Grade 1 complications were observed in 9 (10%) of patients including moderate pain. Grade 2 complications were observed in 17 (18%) subjects including fever, severe pain, and postoperative obstruction. No complications higher than Clavien grade 3 were observed. The average duration of hospitalization was 48 hours.
Conclusions: In this study, flexible ureteroscopy can be safely used to treat renal and proximal ureteral stones with a low rate of complications. Nevertheless, cost and maintenance represent a critical issue that should be resolved to make this procedure available in all urological departments and not just in a few tertiary centers.
Superpulse Thulium, Holmium, and Holmium MOSES Laser Lithotripsy: An ex‐vivo Evaluation on the Effectiveness of “Dusting” Coupled with Ureteroscopic Fragment Aspiration
P Jiang, A Peta, R Arada, M Ayad, AS Afyouni, L Limfueco, A Brevik, N Nguyen, Z Okhunov, RM Patel, J Landman, RV Clayman
Department of Urology, University of California, Irvine
Introduction & Objective: Conventional renal stone dusting is challenging, as both the holmium laser (Ho:YAG) and holmium with MOSES technology (MOSES) fail to reliably reduce calculi to fragments <100 microns (i.e. dust). The Superpulse thulium fiber laser (sTFL) is an emerging technology that may allow for more effective “dusting” of uroliths. We evaluated each of the three laser options using “dusting” settings and then evaluated the effectiveness of fragment aspiration via a dual lumen ureteroscope.
Methods: Seventy‐two ex‐vivo porcine kidney‐ureter models were divided into 12 groups: laser type (Ho:YAG, MOSES, sTFL), ureteroscope (URS) with a single or dual lumen, and use of a 14Fr ureteral access sheath (UAS) or no sheath. Calcium oxalate stones were pre‐weighed and implanted into each kidney via a pyelotomy. Stones were treated at 16 watts using dusting settings of 0.4Jx40Hz (Ho:YAG and MOSES), and 0.2Jx80Hz (sTFL) for a maximum period of 20 minutes. No stone basketing was performed; however, aspiration via the dual lumen ureteroscope was performed. The kidneys were bi‐valved and residual fragments were collected, dried, weighed, and then sieved to determine what proportion of the remnants were larger than dust (i.e. >100 microns).
Results: Initial stone mass (mg), procedure time (sec), and laser energy expenditure (kJ) were similar amongst groups. The greatest stone clearance was seen with sTFL+dual URS+UAS (94%) compared to conventional technique (Ho:YAG+single+no UAS) at 65% (p < 0.01). The use of sTFL resulted in significantly greater stone clearance than either Ho:YAG or Ho:YAG‐MOSES. Aspiration via the dual lumen URS significantly improved stone clearance for sTFL (p = 0.01) but not for Ho:YAG or Ho:YAG‐MOSES. The use of a 14F UAS significantly improved stone clearance regardless of the type of laser or URS used (p < 0.01).
Conclusions: sTFL when combined with a 14F UAS, a dual lumen ureteroscope, and endoscopic suction resulted in a 94% stone clearance rate.
HoLEP Performed with Moses Technology Generates Cost Savings in the Operating Room
N Nimmagadda, NL Kavoussi, CM Forbes, J Robles, A Wang, B Stone, NL Miller
Vanderbilt University Medical Center, Department of Urology
Introduction & Objective: Holmium laser enucleation of the prostate (HoLEP) performed using MosesTM technology has been shown to be efficacious and safe for the treatment of benign prostatic hypertrophy. However, the cost benefit of this technology is unknown. This study seeks to determine if the use of MosesTM technology for HoLEP is cost‐effective from the perspective of operating room resource utilization.
Methods: Post‐hoc cost analysis was performed using data obtained from patients with ≥80 gram prostates randomized to undergo HoLEP using MosesTM laser settings (M‐HoLEP) or standard laser settings (HoLEP). Surgeon and patient blinding were maintained. Prostatic enucleation was performed via a 2 lobe technique using energy settings of 2J and frequency between 20‐40Hz. Twenty‐eight patients were analyzed in each group and served as the basis for cost calculations. Capital costs were estimated at $220,000 for the Lumenis P120H laser machine and $145,130 for the Lumenis VersaPulse PowerSuite 100W (an alternative high‐power laser suitable for HoLEP). Institutional charges for the MosesTM 550 micron laser fiber were $535 versus $406 for a standard SlimLineTM 550 micron laser fiber. The cost to the hospital of operating room time per minute was estimated at $37, as commonly cited. Reliability and repair costs were assumed equal.
Results: Mean total operative time was 101 min for M‐HoLEP and 126 min for HoLEP (p < 0.01). There were no other significant differences in factors affecting operative time including comorbidities, pre‐operative prostate volume, and weight of tissue removed. The mean cost to the hospital per case between M‐HoLEP and HoLEP were $4,272 versus $5,068, respectively. When considering the cost of each machine amortized over 1000 procedures, the mean cost of each M‐HoLEP increases to $4,492 compared to $5,213.13 per HoLEP, favoring M‐HoLEP. When considering upgrading to a Lumenis P120H system from an existing high‐power laser, ∼277 M‐HoLEPs would need to be performed to recover the purchase price of the machine.
Conclusions: MosesTM holmium laser technology provides a cost benefit for HoLEP in high volume centers. The benefit is driven by the reduced operative time per case.
The Effect of Scanning Speed in a Dusting Model of the Moses Pulse 120H 2.0 Laser
P Whelan, CJ Kim, D Ho, C Tabib, F Soto‐Paulo, J Chen, P Zhong, GM Preminger, M Lipkin
Duke University
Introduction & Objective: Moses™ Pulse 120H 2.0 Extended Frequency Range (EFR) technology is a second‐generation Holmium:YAG laser system that allows for higher frequency pulse settings. We assessed the effects of variation of scanning speed on stone treatment efficiency in a benchtop dusting model.
Methods: All tests were conducted using a Moses™ P 120H 2.0 laser system on “hard” (5:1) and “soft” (5:2) Begostone phantoms. Treatment efficiency was compared between Moses Distance (MD) at 80Hz and Moses EFR at 100, 120Hz with settings of 0.2 and 0.3J across five scanning speeds (10, 25, 50, 75, 100 pulses/mm) at a fiber‐stone standoff distances (SD) of 0mm. Using a 3D positioning system, the laser was fired across a polished and submerged Begostone to create trough segments. Ablation volumes (mm3) of 1 mm trough segments were quantified by optical coherence tomography (OCT). Volumetric damage per second was then calculated from laser and scanning settings.
Results: Volumetric stone treatment rate (mm3/s) is highest with higher scanning speed (p < 0.0005). 0.3J is superior to 0.2J at all frequencies (p < 0.05). Slower movement of the fiber across the stone resulted in a slower rate of stone ablation, but greater total ablation.
Conclusions: Although slower fiber scanning results in higher ablation volumes, the volumetric stone treatment rate decreases as stone damage begins to plateau with repeated pulses delivered to the same area. Thus, a higher treatment efficiency can be achieved with more rapid scanning of the laser fiber. However, in practice, rapid scanning must be limited to safely maneuver the ureteroscope while maintaining close contact with the stone. Further testing is warranted to optimize laser treatment strategies.
Which Laser Generates More Heat? A Comparison of the Novel Thulium and Conventional Holmium Lasers in a Benchtop Model
JD Belle, M Keheila, N Srikureja, AS Amasyali, A Assidon, M Hajiha, DD Baldwin
Loma Linda University, Department of Urology
Introduction & Objective: The novel thulium fiber laser (TFL) has been shown to break stones more rapidly than the traditional holmium:YAG laser (HL). However, some evidence suggests that the TFL may generate comparatively more heat. The purpose of this study is to compare ureteral temperatures generated by these lasers during flexible ureteroscopic laser lithotripsy in a benchtop model.
Methods: A 1‐cm BegoStone (CaOx monohydrate consistency) was manually impacted in the proximal ureter of a 3D printed kidney‐ureter model and submerged in 35°C saline. Lithotripsy was performed using a 7.6 French flexible ureteroscope and a 200 m laser fiber without a ureteral access sheath. Three lasers were compared (Dornier 30W HL, Olympus 100W HL, and Olympus 60W TFL). A needle thermocouple to measure temperature was inserted 2 mm from the laser tip. Irrigation was maintained at 35cc/min at room temperature using the Thermedx FluidSmart System. Intraluminal temperature was continuously recorded for 60 seconds of laser activation. Time was given between each trial for the intraureteral fluid to return to room temperature. 5 trials were performed for each of 4 different power settings: 3.6, 10, 20, and 30 Watts. ANOVA and Mann‐Whitney U tests were performed, with p < 0.05 considered significant.
Results: Intraureteral fluid temperature increased as laser power settings increased for all lasers trialed (p < 0.05, table 1). The TFL produced significantly higher temperatures at both 3.6W (26.36°C vs. 24.57°C (Dornier) and 23.23°C (Empower); p < 0.05) and 30W (41.76°C vs. 37.28°C (Empower); p < 0.05). There was no difference in intraureteral temperature between lasers at the 10W and 20W settings. At 30W, the TFL generated supraphysiologic intraluminal temperature.
Conclusions: The TFL generated significantly more heat at both the 3.6W and 30W settings. Supraphysiologic ureteral temperatures may be generated by the TFL with extended use at high energy settings and low irrigation rates. Understanding the heat generation properties of both the Holmium and Thulium lasers during ureteroscopy could help improve the safety of ureteroscopic laser lithotripsy.
ABSTRACT WITHDRAWN
A Prospective Trial of Laser Fiber Degradation Following Holmium Laser Enucleation of the Prostate Utilizing Moses BPH Technology Vs Regular Mode
M Assmus, M Lee, M Sivaguru, DK Agarwal, T Large, BW Fouke, AE Krambeck
Northwestern University, Department of Urology
Introduction & Objective: To compare perioperative and post‐operative outcomes for holmium laser enucleation of the prostate (HoLEP) between cases performed with a 550um standard laser fiber versus a 550um MOSES 2.0 fiber in BPH mode, with primary outcome of fiber degradation.
Methods: We prospectively collected outcomes for 50 consecutive HoLEP cases using a 550um MOSES fiber with MOSES 2.0 BPH mode. All patients were treated at 2J and 40Hz for enucleation and 1J and 20Hz for coagulation. Outcomes were compared to our historical cohort of 50 patients using 550um standard fibers on standard mode. The length of exposed fiber was measured at the start and end of each case with the difference being our primary outcome of degradation length. Additionally, five consecutive 550um standard fibers and five 550um MOSES fibers and their respective controls underwent high resolution 3‐D microCT postoperatively. Four 2D Line profile (4‐pixel width average) analyses were performed for each fiber at its area of maximum damage. Peak to trough ratios based on 8‐bit relative intensity versus distance in pixels for each line profile were performed. Control fibers were assigned a peak to trough ratio of 1.0. Mann‐Whitney U, 2‐tailed T‐tests and Chi‐squared tests were used, significance set to p < 0.05.
Results: The 550um standard fibers demonstrated greater degradation than the 550um MOSES fibers with 2.0 BPH mode (2.9cm (IQR 1.7‐4.3cm) vs 0.2cm (IQR 0.1‐0.4cm), p < 0.01). This difference remained significant when comparing degradation per energy used, per minute enucleation and per gram enucleated (all p < 0.05). None of the 50 cases with MOSES fiber and 2.0 BPH mode required intraoperative interruption to re‐strip the fiber. Pertinent post‐operative outcomes were similar between cohorts (dysuria, median hemoglobin decrease, AUASS, Qmax, QOL score. All p > 0.05). Objective laser fiber degradation by 2D line profile analysis showed more damage to standard fibers (average peak to trough ratio for MOSES compared to standard was, 1.35 ± 0.37 versus 1.82 ± 0.80 respectively, p = 0.026).
Conclusions: Use of the 550um MOSES fiber with MOSES 2.0 BPH mode resulted in significantly less fiber degradation when compared to a standard 550um laser with standard mode.
Holmium Laser Enucleation of the Prostate Efficiency by Prostate Gland Size: Is there a sweet spot?
M Assmus, AE Krambeck, T Large
Northwestern University, Department of Urology
Introduction & Objective: Holmium laser enucleation of the prostate (HoLEP) is one of only two AUA guideline recommended prostate size independent surgeries for benign prostate hyperplasia (BPH). The significant variation in prostate gland size treated results in a wide range of enucleation, morcellation and total operative times. We sought to better understand the effect of prostate size on HoLEP efficiency to better educate patients and improve operating room utilization.
Methods: With IRB approval we queried our EMR and retrospective clinical registry to identify patients who underwent HoLEP between July 1, 2016 – Jan 1, 2020 by two endourologists at our center. Inclusion criteria required intraoperative documentation of prostate tissue resected(grams), enucleation, morcellation and total operative times. Our primary objectives were to assess the effect of increasing increments (25g) of prostate tissue resected on average enucleation and morcellation efficiency (g/min). Our secondary objective was to determine the effect of increasing prostate size on overall (enucleation & morcellation) efficiency. One‐way Kruskal‐Wallis ANOVA with Dunn's post‐hoc test was used, significance p < 0.05.
Results: Between July 1, 2016 and January 1, 2020, 675 HoLEPs were performed meeting inclusion criteria. All comer average (mean) prostate tissue weight resected was 72.1g (Range 1‐448g), energy used 110.00kJ(Range 10.73‐340kJ), enucleation time 48.6min(Range 5‐151min) and morcellation time 10.1min(Range 0.5‐113min). Average enucleation efficiency increased with increasing prostate size categories (Ex. <25g‐0.48g/min, >325g‐3.91g/min) (K‐W ANOVA p < 0.001, Dunn's post‐hoc p < 0.001). Average morcellation efficiency decreased with increasing prostate size (Ex. <25g‐8.41g/min, >325g‐5.49g/min) (K‐W ANOVA p = 0.004, Dunn's post‐hoc p = 0.004) (Figure 1). Combined average enucleation and morcellation efficiency was ≥5g/min between 55‐271g. Inefficiency for cases <55g were driven by enucleation, while >271g case inefficiency was driven by morcellation.
Conclusions: Increasing prostate tissue weight at time of HoLEP is associated with a linear relationship of increasing efficiency of enucleation and decreasing efficiency of morcellation.
Transurethral thulium laser resection of bladder tumor was performed to treat non‐muscle infiltrating bladder tumor
L Li, G Wu, Y Yuan, L Folin, X Zou, Z Guoxi, X Rihai
Introduction & Objective: To observe the efficacy and safety of transurethral thulium laser resection for non‐muscle infiltrating bladder tumor.
Methods: 26 patients with bladder tumor were underwent transurethral thulium laser resection from January 2019 to January 2020. The preoperative clinical stages were TaN0M0 and T1N0M0. The number, size and location of tumor were confirmed by some preoperative images. The way to use laser continuous wave inludes two kinds. The maximum power was set at 50W and the optical fiber was set at 600 μM. A fan‐shaped incision was made at the position of 0.5cm in the tumor base. After the tumor was removed, laser hemostasis was carried out. The larger tumor was cut and removed and the smaller tumor was directly washed out or removed by foreign body forceps. After the operation, the basal tissue was sent for pathological examination.
Results: All the cases were successfully completed. The average operation time was 28 (15‐45) min. The blood loss was 0‐5ml during operation. There was no blood loss and obturator nerve reflex. Bladder irrigation was not performed after operation. Catheter was inserted for 1‐2 days. 25 cases in all were urothelial carcinoma (also known as transitional cell carcinoma) and 1 case was squamous cell carcinoma. 21 cases in all were low grade carcinoma and 4 cases were high grade. 9 cases were at Ta stage, 13 cases were at T1 stage and 4 cases were at T2 stage. Tumor recurrence was not found during the follow‐up of 6‐18 months.
Conclusions:Transurethral thulium laser resection of bladder tumor for non‐muscle invasive bladder tumor has definite effect, (such as less blood loss, fast postoperative recovery and no obturator reflex), That was much worthy of to be put into practice. But the long‐term effects need to be further observed.
Holmium Laser Enucleation of Prostate: What is the true rate of opioid use?
MS Lee, M Assmus, DK Agarwal, T Large, AE Krambeck
Northwestern University Feinberg School of Medicine
Introduction & Objective: Holmium Laser Enucleation of Prostate (HoLEP) is a size‐independent treatment option for benign prostatic hypertrophy (BPH) with excellent long‐term outcomes. We do not prescribe postoperative opioids for HoLEP. However, multiple studies have shown that 24.0‐50.4% of urologists prescribe opioids after BPH surgery. It is possible we are undertreating pain. Therefore, using a national prescription drug monitoring program (PDMP), we reviewed all patients who underwent HoLEP at our institution (where no opioids are prescribed) to determine if opioids were obtained from other sources.
Methods: We performed a retrospective review of all patients undergoing HoLEP by two fellowship‐trained surgeons. Patient data was abstracted from the medical record. We utilized a national PDMP to determine the true rate of postoperative opioid use. The primary outcome was filling of an opioid prescription within 31 postoperative days. Student t‐tests and chi‐square tests were used to compare continuous and categorical variables, respectively. Multivariate logistic regression was then performed using all variables that met a pre‐defined criterion of p < 0.15. All tests were two‐sided, and significance was set at p < 0.05. SAS v9.4 was used.
Results: 284 men underwent HoLEP from July 2018‐July 2020. 35 men (12.4%) received postoperative opioids despite our opioid‐free pathway. 40% of opioids were prescribed by an inpatient physician assistant on his own accord. To prevent skewed results, these patients were excluded from primary statistical analyses. On univariate analysis, surgeon experience (p = 0.0184), chronic opioid use (p < 0.0001), any opioid exposure (p = 0.0039), benzodiazepine use (p = 0.0036), and chronic pain (p = 0.0057) were associated with postoperative opioid use. On multivariate analysis, patients who had preoperative opioid exposure (OR 51.80, p = 0.0273) and greater surgeon experience (OR 0.20, p = 0.0311) were identified as significant variables.
Conclusions: The rate of opioid use after HoLEP was 12.4% despite our opioid‐free pathway. Proper education of the surgical team is key to prevent inappropriate opioid prescribing. On multivariate analysis we identified that preoperative opioid exposure was associated with increased risk, while greater surgeon experience was associated with decreased risk of obtaining postoperative opioids.
Efficient Holmium Laser Enucleation of the Prostate Can Be Performed After Prostatic Artery Embolization for Massive Prostate Glands (>250 Grams)
MA Knoedler, C Manakas, A Eifler, DR Gralnek
University of Wisconsin, Department of Urology
Introduction & Objective: Prostatic artery embolization (PAE) has the ability to decrease blood supply to the prostate and shrink the prostate, but it is unclear if PAE makes subsequent surgical intervention for benign prostatic hyperplasia (BPH) technically difficult. Our objective was to evaluate if holmium laser enucleation of the prostate (HOLEP) could be performed efficiently and safely after PAE for massive prostate glands ( > 250 grams).
Methods: Patients with prostate glands over 250 grams on imaging (CT or MRI) and symptomatic BPH were offered HOLEP with PAE ahead of time. PAE was performed by a single interventional radiologist and HOLEPs by two experienced urologists. Pre‐operative factors including prostate size and catheter status were evaluated. PAE procedural time and HOLEP procedural time, enucleation time, enucleated volume, and enucleation efficiency (grams of prostate tissue resected per minute of enucleation time) were evaluated along with post‐operative catheter duration and complications.
Results: Nine patients had prostate glands >250 grams and underwent HOLEP with PAE prior. Prostate size on pre‐operative imaging was 290.3 ± 38.5 grams and 6 (66%) patients were catheter dependent prior to intervention. 8 (89%) patients underwent bilateral PAE while one patient underwent unilateral PAE with a procedure time of 174.4 ± 64.6 minutes. HOLEP was successfully performed in all patients with procedural time of 159.4 ± 48.5 minutes, enucleation time of 91.4 ± 22.3 minutes, and enucleated volume of 130.8 ± 41.5 grams. Enucleation efficiency was 1.43 grams per minute. All patients passed a void trial on their first attempt after surgery. Post‐operative catheter duration was 3 ± 2.6 days. One patient required repeat surgery for morcellation of a retained fragment.
Conclusions: HOLEP can be performed efficiently without increased complications after PAE by an experienced surgeon. This is important as PAE has the potential to be an adjunct treatment in massive prostate glands that are otherwise technically difficult to resect.
The Effect of Peak Power and Pulse Modulation on Lithotripsy Particle Size
B Yang, S Liu, J Cancino, A Ray, TC Hasenberg, T Harrah, BW Turney
University of Oxford
Introduction & Objective: An ideal laser lithotripsy technology for urinary stone surgery should promote the efficiency of stone destruction, reduce retropulsion, and decrease particle size. We report on a prototype Holmium:YAG laser with a unique pulse modulation technology that delivers long‐duration, high energy pulse packets with numerous micro‐pulses per packet. The technology combines high pulse packet energy and moderate peak power and has the potential to increase ablation efficiency and reduce retropulsion. In this study, we evaluate three pulse modulation modes of the prototype laser to determine the efficacy of post‐ablation particle size.
Methods: 242um core fibres were attached to the prototype laser to ablate canine kidney stones in DI water. Two ablation test methods were used to characterize stone ablation performance with and without retropulsion (method‐A: hand‐held; method‐B: hands‐free). At fixed total energy delivery, three pulse modulation modes at a range of pulse packet energy/power settings were investigated: 1) standard mode with specialized sub‐frequency; 2) special mode at 24 micro‐pulse per packet; 3) special mode at 7 micro‐pulse per packet. Post‐ablation product was sieved via a 2‐mm mesh, and the sieved sample was measured to evaluate particle size distribution.
Results: Preliminary results of both test methods showed that the prototype laser breaks canine MAPH stones into fine dust with between 90% and 100% of post‐ablation particle smaller than 250 μm. Among them, special modes with multiple micro‐pulses showed slightly higher percentage of fine dust. At higher power (3J‐20Hz‐60W) the special modes presented both high ablation rate and fine particle size. At 1J‐10Hz‐10W, the hand‐held test method presented similar ablation rate within three laser modes, while the hands‐free test method (allows retropulsion) presented an ablation rate 2.6 times higher in the special modes.
Conclusions: The prototype laser, across all settings, demonstrated fine lithotripsy particle size that meets the standard for real‐time evacuation during ureteroscopy. The special modes, benefiting from high packet energy and moderate peak power, successfully achieved efficient stone dusting at reduced retropulsion. Overall, the prototype laser is a promising tool for stone ablation with fine particle generation. (Disclaimers: Concept device or technology. Not available for sale).
An in vitro study of the use of high power Ho:YAG laser and the influence of MOSES technology settings in the retropulsion of stones in the upper urinary tract
A Natsos, G Koukiou, A Tsaturyan, M Lattarulo, A Vagionis, K Pagonis, C Adamou, A Peteinaris, E Liatsikos, P Kallidonis
Introduction & Objective: To investigate the retropulsion of stones under different energy and frequency settings with or without the use of MOSES™ pulse delivery technology in an experimental model. The investigation aimed to provide evidence for the optimal settings in clinical practice.
Methods: For the experiment, Plaster of Paris stones were used in a custom‐made experimental configuration including a glass tube set in a water bath filled with saline. Power settings from 20 to 60W were applied with the use of a Lumenis 120H Ho:YAG laser and a MOSES™ 365 D/F/L fiber. The power was delivered with different settings of energy and frequency with the use of MOSES™ or conventional pulse delivery technology. The stone displacement was measured by using a high‐speed slow‐motion camera and a custom made image analysis algorithm.
Results: The retropulsion of stones was the lowest with the combination of low energy (0.5J) and high frequency while using MOSES™ for each power setting (20‐40‐60W). The MOSES™ technology was associated with less retropulsion in all energy and frequency settings compared to the use of conventional pulse delivery technology.
Conclusions: Retropulsion was less using the MOSES™ technology in comparison with the conventional pulse delivery technology. The lowest retropulsion was observed with the combination of low energy, high frequency and MOSES™ technology.
Improved Efficiency of Thulium versus Standard Holmium Ureteroscopic Laser Lithotripsy Leads to Large Cost Savings
SW Nowicki, JA Linscott, MH Nguyen, JR Ryan, JP Ingimarsson, B Jumper
Maine Medical Center Department of Urology
Introduction & Objective: Nephrolithiasis prevalence approaches 10% in the United States with an almost $5 billion/year associated cost of care. As laser lithotripsy is one of the most common urologic procedures, small cost savings per case can have a large financial impact. Recently, the FDA approved thulium fiber laser (TFL) lithotripsy. This technology decreased our average ureteroscopic lithotripsy case time for comparable stones when compared to a standard 100W holmium laser (Hol:YAG). Here, we perform a cost benefit analysis to show projected cost savings at our institution.
Methods: Capital cost for Olympus SOLTIVE™ SuperPulsed Laser system was obtained. Price of individual Hol:YAG and TFL fibers were compared. Direct and indirect operating rooms costs per min when using laser at our institution in 2020 were calculated by the financial department. TFL was not introduced until late October and therefore weighted Hol:YAG fiber cost contribution in direct cost calculations was also considered. Indirect costs were assumed to be equal for Hol:YAG and TFL lithotripsy. Average operative times for each modality were determined. Expected annual cost savings were calculated as follows: Time saved (min/case) x Direct OR cost ($/min) x Cases/year = Annual cost saving ($/year).
Results: Initial capital costs for 2 SOLTIVE SuperPulsed laser systems based on list price was $350,000. Individual TFLs cost $319.50 vs $450.00 for holmium fibers. Direct operating room costs for the facility were calculated at $33.82/min, which includes a blended average of Hol:YAG and TFL fiber costs, heavily weighted to Hol:YAG. Average operation time with TFL was 13 min less than with Hol:YAG, saving $440/case. Including laser fiber cost savings not fully accounted for in the calculated direct cost/min raises estimated savings to as high as $570/case. Annually ∼670 cases are performed at our institution, giving a range of $294,800 to $381,900 savings per year.
Conclusions: Switching from standard Hol:YAG to TFL lithotripsy reduced our operative time significantly, leading to large cost savings ($440/case). TFLs are $150.50 less expensive than Hol:YAG fibers. Together, yearly cost savings are estimated to be $294,000‐$381,900. We conservatively expect to cover TFL capital expenditure for 2 laser systems within five fiscal quarters.
Omeprazole Lowers 24‐Hour Urinary Magnesium Excretion in Patients with a History of Urolithiasis: Single Center Experience
KL Penniston, S Li, SY Nakada, RA Jhagroo
University of Wisconsin School of Medicine and Public Health
Introduction & Objective: Urine magnesium (Mg) inhibits calcium oxalate (CaOx) stone formation. While highly variable, 24h urine Mg (UMg) is typically >two‐fold higher than oxalate. Proton pump inhibitors, frequently used for gastroesophageal reflux disease and peptic ulcer, inhibit active intestinal Mg absorption by interfering with transcellular cation channels. Alterations in Mg absorption are balanced by changes in renal Mg reabsorption. We hypothesized that patients taking omeprazole (OM) have lower UMg.
Methods: With IRB approval, we evaluated sequential patients with a history of urolithiasis seen in our multidisciplinary stone prevention clinic or individually by the registered dietitian nutritionist (RDN). We documented clinical parameters, including OM dosage and duration of treatment, if prescribed. We used 24h urine collections from patients' initial encounters in the stone clinic or with the RDN (i.e., collected while patients were naive to preventive therapy). Power analysis demonstrated we would need ≥240 subjects in order to identify statistically significant differences in UMg between patients taking and not taking OM.
Results: Within the past 6 months (7/15/2020 to 1/15/2021), 325 patients were seen. We excluded patients if: they had no history of urolithiasis (n = 9); they had no 24h urine collection prior to starting prevention (n = 15); 24h urine creatinine was <500 mg or >3,000 mg; they initiated pharmacological and/or nutrition therapy prior to starting OM (n = 20). Patients (n = 276) were 43% female and 91% white Caucasian. At their most recent clinical encounters, they were 58 ± 14 y; calculated BMI was 31 ± 8.2. Patients taking OM (OM+) for >3 months (n = 45) took 24 ± 8.2 mg/d (median 20 mg) and were taking it for 7.3 (median 6.4) y. Compared to those not taking OM (OM‐; n = 231), OM+ patients had lower UMg (figure). There were no differences for any other 24h urine stone risk parameters. As bowel disease is known to affect UMg, we examined this as a potential confounder. Though prevalence of bowel disease was different (figure), the prevalence of UMg ≤70 mg/d was not (figure; P = 0.39, Chi square), suggesting bowel disease was not a confounder.
Conclusions: Patients taking OM have lower UMg, increasing their risk for CaOx stone recurrence. Studies to investigate whether Mg supplementation reverses low UMg in patients taking OM are needed.
Sodium Bicarbonate Does Not Increase Urinary Calcium Excretion and is an Effective Urinary Alkalization Strategy: Single Center Experience
KL Penniston, RJ Medenwald, SY Nakada, RA Jhagroo
University of Wisconsin School of Medicine and Public Health
Introduction & Objective: Sodium bicarbonate (NaHCO3) has long been used for renal alkalization. Urinary alkalization increases urine citrate (UCit) and pH and thus reduces calcium and uric acid stone risk. Yet Na in any form is thought to increase urine calcium (UCa), potentially outweighing beneficial effects. As literature suggest that the calciuric effect of Na is limited to when it is complexed with chloride (Cl), such as in salt (NaCl), we hypothesized that NaHCO3 does not increase UCa excretion.
Methods: We currently recommend NaHCO3 for low UCit or pH or both. With IRB approval, we retrospectively identified patients to whom NaHCO3 was prescribed and who met these criteria: 24h UCit <420 mg and/or pH <5.9 at baseline; two 24h urine collections within 1 y wjth <40% variation in 24h urine creatinine; seen in our clinic within 2.5 y; self‐reported adherence (as documented in provider's clinical note); and an increase in either 24h UCit or pH in the 2nd urine collection (the latter criterion was to control for non‐compliance).
Results: Patients (n = 39) were mostly male (77%) and were 61 ± 12 y. NaHCO3 dosage differed based on severity of risk and was 32 ± 11 mEq/d alkali (min‐max 15‐60 mEq), assuming that ½ level tsp provides 29.5 mEq alkali. Baseline and follow‐up 24h urine collections were 7.9 ± 2.7 months apart (median 6.5). At baseline, 38% of patients had 24h UCit <420 mg, 72% had urine pH <5.9, and 19% had both. Baseline 24h urine Na:Cl ratio (mEq:mEq) was 1.0 ± 0.13. In follow‐up, 24h UCa did not change (figure), but pH, citrate, and Na:Cl increased (figure). We stratified patients by follow‐up Na:Cl ratios: ≥1.05 vs <1.05. We used these ratios to estimate actual compliance, assuming that higher urine Na than Cl meant that Na came from both NaHCO3 and NaCl vs from primarily NaCl. Interestingly, the change in 24h urine pH was significantly higher among compliant vs non‐compliant (P = 0.021); change in UCit was also higher, but only marginally so (P = 0.087). Among compliant patients, 56% of hypercalciurics normalized (lowered) their 24h UCa compared to none of the non‐compliant. Among those with new‐onset hypercalciuria (18% overall), higher 24h urine Cl (+77 vs ‐15 mEq) than in those whose UCa was <250 mg suggested that higher NaCl intake was responsible.
Conclusions: NaHCo3 is an effective alkalinizing agent and does not raise UCa. Compliance can be estimated by higher 24h urine Na compared to Cl.
How much is preventative counseling effective in those patients who underwent stone surgery.a prospective study from developing country
N Iqbal, A Hasan, S Imtiaz Ali, T Bhatty, S Akhter, R Suarez‐Ibarrola
PKLI, Lahore, Pakistan
Introduction & Objective: Urolithiasis is a multifactorial disease. After definitive surgery effective use of preventative strategies and counseling is necessary to decrease recurrence rate. Dietary recommendations, exercise levels, fluid intake, Weight loss, Lemonade water and medication supplementation are pivotal to prevent recurrence according to recent urologic guidelines. However no prospective study has been done as to how much patients adhere to these recommendations after their stone surgery. We looked to evaluate the effectiveness of counselling regarding preventive strategy in those who underwent stone surgery.
Methods: Those with surgical treatment for stones were prospectively analyzed over a 9‐month period. Patients were given verbal and written information regarding the general strategies to prevent stones recurrence in future. At follow up visits in clinic, patients were asked as to how much they remembered and how much they practiced those preventative strategies. Patient recall was compared with respect to the possible causes of recall. The relationship between correct recall of stone history and the recommended preventative strategies was evaluated using appropriate statistical measures.
Results: The study comprised of 207 patients with 63% male and a mean age of 43 years. Prior stone passage was reported in 62% and 85% required surgical intervention. Stone composition was documented in 103 patients with 83% having calcium stones. Of them with known stone composition, 23% recalled their stone composition type. Patients were recommended 5.1 mean preventative strategies each.23% correctly recalled all strategies while 36% recalled half of recommendations.27% recalled 2 recommendations and 14% recalled 1 recommendation. Education level, family history stones, past stone surgery and pain episodes were related significantly on multivariate analysis on recall of these preventive strategies (p < 0.002).
Conclusions: Patients who are educated, live in bigger cities correctly recall their recommended preventative strategies. Secondly involvement of a dedicated nurse for stone preventive strategies discussion with patient at end of clinical visit results in greater understanding of preventative strategy counseling. Family members support was also important factor in pursuing these strategies. But there is need of future prospective studies to see why the patients don't recall everything on the strategy despite a detailed counseling. There is need for stone social groups to provide platform to these patients to motivate each other to pursue the stone preventive strategies.
Withdrawn
Narcotic Free Ureteroscopy: A Prospective Randomized Study
JN Bamberger, B Gallante, AM Zampini, WM Atallah, JA Khusid, AS Sadiq, M Gupta
Icahn School of Medicine at Mount Sinai
Introduction & Objective: Prescription opioid abuse has reached epidemic levels in the US, fueled in part by unused prescription narcotic reservoirs within communities. The aim of this study is to evaluate the efficacy of non‐narcotic analgesics and preoperative counseling in managing post‐operative pain following ureteroscopy (URS).
Methods: Adult patients undergoing URS for urolithiasis were recruited. Exclusion criteria were: pre‐existing stent, contradictions to oxycodone, acetaminophen, or ibuprofen, or current prescription analgesic use. After informed consent, subjects were randomized into 3 groups: 1. Narcotic—15 oxycodone‐acetaminophen(OXY) 5/325mg, 2. Non‐narcotic—15 ibuprofen(IBU) 600mg, 3. Counseling—15 oxycodone‐acetaminophen 5/325mg, 15 ibuprofen 600mg, and counseling from the surgeon to avoid narcotic if possible. Patients without a post‐op stent were excluded. At stent removal subjects completed the Universal Stent Symptom Questionnaire (USSQ) and a pill count was performed. Demographic information, operative data, USSQ, and analgesic consumption postoperatively were analyzed between the three groups.
Results: Of 102 patients enrolled, 87 have completed the study, 10 are in progress and 5 were excluded. No significant differences were noted in patient demographic, clinical nor operative characteristics (Table 1). No differences were noted in mean sum of USSQ pain scores, visits to the emergency department, calls to the office, or requests for additional medication between the three groups. The counseling group used a significantly lower number of OXY pills compared to the narcotic group (2.56 vs. 5.29, p < 0.027), and less IBU compared to the non‐narcotic group (3.15 vs. 6.02, p < 0.031), but however no differences in mean total pill count were noted between groups.
Conclusions: Our data suggest that patients can achieve equivalent post‐operative analgesic satisfaction with non‐narcotic pain medication compared to opiates following URS. Further, counseling patients on post‐operative pain before surgery can reduce the number of postoperative narcotic and non‐narcotic medication taken individually.
Evaluating the Lithogenic Potential of Dairy Milk Alternatives
SP Hager, B Balouch, K Lurz, Z Snow, PC Dreher, J Friedlander
Main Line Health
Introduction & Objective: The rising popularity of vegan and vegetarian diets has created an increasing demand for plant based dairy alternatives. Non‐dairy milk sales grew 61% in the United States from 2012‐18, with worldwide sales of 21 billion in 2015. While the impact of traditional dietary factors on stone formation has been well elucidated, the effect of dairy milk alternatives (DMAs) has not been explored. The objective of this study is to review the ingredients in DMAs and discuss the potential implications on nephrolithiasis.
Methods: A list of the most popular plant‐ based DMAs was compiled from a web‐based search utilizing Amazon.com®. Nutritional information was recorded directly from the label, the manufacturer website or via company inquiry. Powdered products and those with added flavoring were excluded. Nutrient amounts for DMAs with n > 3 were compared with ANOVA to the most popular whole milk products on Amazon.com®. A literature review of identified nutrients was performed with search terms “nephrolithiasis” and “kidney stones” to identify categories in Table 1.
Results: 13 DMAs were identified (Table 1). All DMAs contain significantly lower amounts of cholesterol (p < 0.05). Almond, coconut, oat and cashew milk had significantly (p < 0.05) lower sugar. Sodium was significantly lower in coconut milk (p < 0.05) and higher in almond milk (p > 0.05). Total carbohydrates were significantly lower in Almond milk (p = 0.05). No products contained vitamin C or B6. Oxalate and citrate were not reported. Whole milk had more Calcium than all DMAs other than Hemp, however, differences were not significant ( p > 0.05). Almond milk contained significantly (p < 0.05) less potassium. When present, magnesium content was greater in DMAs, although not significantly (p > 0.05). All DMAs, excluding soy, had significantly (p < 0.05) less protein. Fat content did not reach statistical significance, but was generally lower in DMAs.
Conclusions: Plant based DMAs are a rapidly growing market worldwide. DMAs generally had less lithogenic content, while lithoprotective nutrients were statistically similar. No products reported citrate or oxalate content. However, several DMA's are derived from foods known to be rich in oxalate. Urologists should consider the impact of DMAs and incorporate this into patient specific counseling on stone prevention.
Drivers of Calcium Oxalate Stone Formation in Octogenarians and Nonagenarians
B Gallante, H Kwun, JA Khusid, JN Bamberger, WM Atallah, M Gupta
Icahn School of Medicine at Mount Sinai
Introduction & Objective: Nephrolithiasis affects approximately 9% of the population, and its prevalence in the elderly is rising. We sought to identify which urinary metabolic risk factors drive calcium oxalate stone formation in the very old (patients aged >80 years).
Methods: We retrospectively identified kidney stone formers and extracted patient level demographic and clinical data including baseline 24‐hour urine studies prior to initiating any treatment. Subjects were categorized by age (< 80 versus >80 years), gender, and underlying renal dysfunction. Statistical analysis of group comparisons was conducted using chi‐square, Mann‐Whitney U tests, and t‐tests where appropriate.
Results: Metabolic urinary abnormalities associated with nephrolithiasis were demonstrated by age and gender. Hypocitraturia was more common in patients aged >80 years compared to those <80 years old in both males (72.2% vs. 49.9% p = 0.002, respectively) and females (75% vs. 53.5% p = 0.006, respectively). This finding remained significant among females after excluding those with renal insufficiency. Hypercalciuria was less common amongst women aged >80 as compared to women aged <80 years (15.9% vs. 33.5%, p = 0.016, respectively). Hyperoxaluria was less common amongst men aged >80 as compared to men aged <80 years (29.6% vs. 50.5%, p = 0.003, respectively).
Conclusions: Hypocitraturia is more common amongst those aged 80 years or older while hypercalciuria and hyperoxaluria is less common. Accordingly, when providing empiric dietary counseling and modifications in the advanced elderly population emphasis on citrate supplementation may improve outcomes.
Alkali Content of Common Over‐the‐Counter Supplements for Prevention of Recurrent Kidney Stones
BA Johnson, A Garbens, JA Antonelli, K Hill, N Maalouf, MS Pearle
UT Southwestern
Introduction & Objective: : Recurrent nephrolithiasis is an increasingly common problem worldwide. Administration of alkali to recurrent stone formers has been shown to decrease the rate of recurrent stones. For potassium citrate, the most common alkali, cost can be a barrier to patient compliance. Several overthe‐counter (OTC) supplements purport to prevent recurrent kidney stones, but there is little corroborating evidence to support these claims or that validate the claimed alkali content of these supplements.
Methods: A total of nine non‐prescription supplements were purchased online, with two separate orders placed 6 months apart to test for lot variance. The claimed total alkali or citrate content per serving was obtained from the packaging or website. Tablets/capsules were diluted in 16 oz of water. Using a single recommended serving of each product, the actual content of each item listed in table 1 was analyzed. Net gastrointestinal absorption of alkali (NGIA) and mean cost per 10 mEq were calculated. Chi‐squared and two‐tailed independent t‐tests were utilized.
Results: Table 1 lists the content of each analyte for each product, the calculated NGAI and cost. MoonStone and KSP Tabs yielded the highest NGIA per serving. Horbaach Potassium Citrate demonstrated lower NGIA compared to competitive products (1.2‐1.4 mEq/serving). Moonstone, Now K Citrate, Kidney COP, and KSP Tabs demonstrated NGIA and citrate lot variance less than 10%, while LithoBalance showed a 49% NGIA variance between lots. Sodium content was significantly higher in KSP Tabs (p < 0.001). Oxalate and uric acid content were low in all products, although Litholyte Coffee contained of 10‐11 mg/L of oxalate (p < 0.001) and 74‐98 mg/L of uric acid (p < 0.001). The cost per 10 mEq of alkali varied widely among products, with MoonStone the costliest at $0.87/10mEq and LithoBalance powder the least costly at $0.03/10mEq.
Conclusions: A variety of OTC products claim efficacy for prevention of kidney stones. While actual clinical efficacy has not been proven in most cases, some products do contain sufficient alkali. MoonStone and KSP tabs contain the most alkali per serving. While LithoBalance was the most cost‐effective, the alkali content was highly variable between batches. Additional studies are underway to assess the urinary response to consumption of these products.
Inconsistency of Cystine Stone Parameters In Predicting Clinical Stone Activity
RL Steinberg, ME VanDyke, JC Dai, A Garbens, BA Johnson, JA Antonelli, MS Pearle
UT Southwestern
Introduction & Objective: Urinary cystine concentration (Ccon) is often used to assess cystine stone risk but measurements of cystine excretion may be unreliable with use of cystine‐binding thiol drugs (CBTDs). Cystine capacity (Ccap) is a proprietary assay (Litholink, Chicago, IL) purportedly unaffected by CBTDs. Optimal goal values have yet to be definitively determined but our prior work suggested Ccap >90 mg/L indicates minimal risk of stone formation (favorable, +). We have noted discordance between Ccon and Ccap in some CSFs, where one parameter is favorable and the other is unfavorable. We evaluated the occurrence of stone events with respect to concordant and discordant Ccon and Ccap measurements.
Methods: Cystine stone formers (CSFs) seen in our stone clinic from 2005‐2020 were retrospectively reviewed. Demographic, diagnostic and therapeutic data were collected. Ccon ≥250 mg/L and Ccap <90 mg/L were considered unfavorable (‐). Stone activity was defined as new stone formation, growth of existing stones, or passage or treatment of a stone not previously detected. Urinary cystine parameters were considered in the context of recent imaging and patient history and labeled as stone active or quiescent. Chi squared and binary logistic regression was performed (p < 0.05).
Results: A total of 58 CSFs with 292 24‐hour urine collections had sufficient data for analysis. The rate of stone activity was lower (8.6%, p < 0.001) in +Ccon/+Ccap CSFs compared to ‐Ccon/‐Ccap (39.4%) CSFs (Table). Stone activity was higher, but not statistically, in +Ccon/‐Ccap CSFs (15.7%, p = 0.185) compared to +Ccon/+Ccap CSFs, but lower than in ‐Ccon/‐Ccap CSFs (p < 0.001). With only 2 samples in the ‐Ccon/+Ccap group, no meaningful analyses could be performed. Binary logistic regression revealed that relative to +Ccon/+Ccap CSFs, CSFs with ‐Ccon/‐Ccap were significantly more likely to have a stone event (OR 6.94, p < 0.001) but +Ccon/‐Ccap CSFs were not (OR 1.98, p = 0.109).
Conclusions: CSFs with discordant and concordant unfavorable parameters have higher stone activity rates than CSFs with concordant favorable values. Although Ccap considers more factors involved in cystine stone formation than Ccon, its ability to better predict stone activity remains unclear. The predictive value of urinary cystine parameters remains incompletely understood.
Opiate Omission After Ureteroscopy Does Not Lead to Increased Emergency Department Visits: Results from a Statewide Quality Improvement Collaborative
S Hawken, S Hiller, K Swarna, J Slayton, D Wenzler, C Maitland, J Hollingsworth, KR Ghani, C Dauw
Michigan State University College of Human Medicine
Introduction & Objective: Emergency department (ED) visits after ureteroscopy (URS) are common and are often due to postoperative pain. As a part of a statewide quality initiative to reduce ED visits, we sought to determine if opiate omission following URS is associated with unintended consequences, such as increased ED visits.
Methods: The Michigan Urological Surgery Improvement Collaborative's Reducing Operative Complications from Kidney Stones (MUSIC ROCKS) initiative was established in 2016. It is comprised of urologists across the state whose goal is to improve the care of patients with stone disease. We identified patients that underwent primary URS and examined quarterly trends in postoperative opiate prescription. Variation in opiate prescribing was assessed at the practice level. Using demographic, clinical, and operative data, we constructed a multivariable model to define risk factors for opiate prescription. After adjusting for patient and practice‐level factors, we determined whether opiate omission was associated with postoperative ED visits within 30 days of surgery.
Results: We identified 9,268 patients who underwent URS (2016‐2019). Post‐URS opiate prescriptions have shown an absolute decline of 43.4% since the inception of MUSIC ROCKS (Figure). There was wide variation in practice‐level opiate use (8.8% to 98.7%, p < 0.01). The odds of receiving an opiate were higher in males (OR 1.32, 95%CI 1.17‐1.49, p < 0.01), those with a stent (OR 1.72, 95%CI 1.49‐1.99, p < 0.01), or a diagnosis of chronic pain (OR 1.68, 95%CI 1.01‐2.66, p = 0.04). Those less likely to receive opioids were older (OR 0.99, 95%CI 0.98‐0.99, p < 0.01), had greater comorbidity (OR 0.82, 95%CI 0.69‐0.98, p = 0.03), and were prescribed an NSAID (OR 0.23, 95%CI 0.19‐0.28, p < 0.01). Omission of opiates following URS was not associated with increased ED visits (OR 0.83, 95%CI 0.67‐1.04)
Conclusions: Since establishment of a statewide quality improvement program in Michigan, opiate prescriptions following URS have declined substantially without an increase in ED visits. Patient factors and practice variation contribute to the risk of receiving an opiate underscoring the need for continued efforts in this area.
In‐Hospital Predictors of Post‐Discharge Opioid Utilization: Individualizing Prescribing after Radical Prostatectomy based on the ORIOLES Initiative
R Becker, ZT Su, M Huang, M Biles, K Harris, K Koo, M Han, ME Allaf, A Herati, HD Patel
James Buchanan Brady Urological Institute, The Johns Hopkins Medical Institutions
Introduction & Objective: Judicious opioid stewardship would match each patient's prescription to their true medical necessity. However, most prescribing paradigms apply preset quantities and clinical judgment without objective data to predict individual use. We evaluated individual patient and in‐hospital parameters as predictors of post‐discharge opioid utilization after radical prostatectomy (RP) to provide evidence‐based guidance for individualized prescribing.
Methods: A prospective cohort of patients who underwent open or robotic RP were followed in the Opioid Reduction Intervention for Open, Laparoscopic, and Endoscopic Surgery (ORIOLES) initiative. Baseline demographics, in‐hospital parameters, and inpatient and post‐discharge pain medication utilization were tabulated. Opioid medications were converted to oral morphine equivalents (OMEQ). Predictive factors for post‐discharge opioid utilization were analyzed by univariable and multivariable linear regression, adjusting for opioid reduction interventions performed in ORIOLES.
Results: Of 443 patients, 102 underwent open and 341 underwent robotic RP. The factors most strongly associated with post‐discharge opioid utilization included inpatient opioid utilization in the final 12 inpatient hours before discharge (+39.6 post‐discharge OMEQ if inpatient OMEQ was >15 versus 0; p < 0.001), maximum patient‐reported pain score (range 0‐10) in the final 12 hours before discharge (+27.6 post‐discharge OMEQ for pain score ≥6 versus ≤1; p = .01), pre‐operative opioid use (+76.2 post‐discharge OMEQ; p = .002), and BMI. A final predictive model to guide post‐discharge opioid prescribing was constructed.
Conclusions: Following RP, inpatient opioid use, patient‐reported pain scores, prior opioid use, and BMI are strongly correlated with post‐discharge opioid utilization. These data can help guide individualized opioid prescribing at discharge to balance individual needs with risks of both overprescribing and underprescribing.
Dietary Assessment of Lithogenic Factors in Plant‐Based Meat Products
C Liaw, K Koo, JS Winoker, A Potretzke, BR Matlaga, JC Lieske
Icahn School of Medicine at Mount Sinai
Introduction & Objective: Kidney stone patients are advised to limit animal protein intake. Plant‐based meat products have recently gained popularity and may be an alternative protein source for these patients. However, the potential lithogenic risks associated with plant‐based meat are not well‐characterized.
Methods: US Department of Agriculture databases were queried with a sample of plant‐based meat products widely available to US consumers. Nutrient profile data were compared to animal protein data. Oxalate content was extrapolated based on dietary data sources.
Results: Plant‐based meat products simulating beef (n = 16), pork (n = 11), chicken (n = 10), and seafood (n = 10) were analyzed. Compared to respective animal protein sources, most plant‐based alternatives contained fewer calories, less protein, and less fat (Table). In terms of oxalate content, 55% of plant‐based products used soy protein as the primary protein source. Soy‐based beef contained the highest average oxalate content (18 mg/serving), while soy‐based seafood had the lowest (7 mg/serving). In contrast, animal protein contained negligible oxalate. Sodium content was higher in most plant‐based products overall (34 products, 72%) and in each class; individual products contained as much as 216% of sodium vs. animal protein.
Conclusions: The majority of plant‐based meat products consist of high‐oxalate protein sources and have higher sodium content compared to animal protein, with dietary implications for stone‐forming patients.
Patients on Medical Expulsive Therapy for Obstructing Ureterolithiasis ‐ The Wisconsin Stone Quality of Life (WISQOL) Survey
T Phillips, J Palka, AK Chow, J Vetter, A Paradis, R Venkatesh
Introduction & Objective: Though controversial, alpha blockers continue to be used widely for ureteral stone passage. However, its effects on the patient reported Quality of life (QoL) is not known. We compared the QoL of patients on medical expulsive therapy (MET) to patients not on MET (noMET) utilizing a validated Wisconsin Stone Quality of Life (WISQOL) survey.
Methods: After IRB approval, we performed a prospective study including patients on either MET or noMET after presenting to a tertiary‐care ED with symptomatic, obstructing ureteral stones. Treatment type was decided at the point of care by the initial treating physician. Both treatment arms consisted of medications for analgesia and nausea. Additionally, tamsulosin (0.4mg orally, daily) was prescribed for the MET group. The WISQOL survey was administered at baseline, 7‐, 14‐, 21‐ and 28‐days following discharge from the ED or until stone expulsion.
Results: A total of 196 patients were enrolled, of which 115 (58.6%) completed questionnaires for analysis, 91 in the MET group and 24 in noMET. Average ureteral stone size was 4.7 (STD 1.8) mm and 3.1 (STD 1.0) mm for MET and noMET, respectively. Of completed surveys, 104 (90%) were completed at day 7, 66 (57.4%) at day 14, 52 (45.2%) at day 21, and 39 (33.9%) at day 28. Spontaneous stone passage occurred in 38 (41.8%) while on MET compared to the 7 (29.2%) in noMET(p = 0.26). In total, 8 (7.0%) patients returned to the ED for intractable pain and 11 (9.6%) required surgical intervention. MET was associated with an improved QoL scores across all WISQOL domains compared to noMET (Fig.1). Stone size, age, race, sex, comorbidity score and a prior stone history were not associated with risk of negative effect on QoL (Table 1).
Conclusions: In the above cohort, use of MET showed benefit on all WISQOL metrics with significant differences noted in all assessed impact domains and standard scores compared to noMET patients. Validation with a larger study is needed which may also provide reasons for better quality of life in MET patients.
Comparative outcomes of urinary and serum parameters for patients with and without diabetes mellitus (DM): Experience from a dedicated metabolic stone clinic
S Kunjur, D Bhatnagar, M Ramachandra, P Cook, M Saraogi, R Geraghty, A Pietropaolo, BK Somani
University Hospital Southampton, UK
Introduction & Objective: The incidence and prevalence of both kidney stone disease (KSD) and diabetes mellitus (DM) is increasing. The relationship between KSD and DM has been widely studied, with a potential link between the two. We wanted to look at comparative outcomes of urinary and serum parameters for patients with and without DM.
Methods: Data was analysed for all high‐risk patients who underwent metabolic stone screening between March 2012‐Jan 2020. Three independent non‐medical personnel not involved in treating these patients transcribed the data. Serum measurements of sodium, potassium, creatinine, bicarbonate, chloride, corrected calcium, magnesium, inorganic phosphate, urate and PTH were done. 24‐hour urinary and random urinary parameters were also measured. The eligible patients were divided into two groups depending on the absence (group 1) or presence (group 2) of DM.
Results: A total of 697 patients were identified, of which 89% were in group 1 (See table). The mean age and BMI were higher for group 2. On comparing the urinary parameters, the citrate and sodium levels were significantly high, and urinary pH values were significantly low for group 2. On comparing the serum parameters, the bicarbonate and magnesium values were significantly high, and renal function was significantly better in group 1.
Conclusions: Based on our data, metabolic screening for patients with DM is a good strategy with a reasonable yield of abnormal urinary and serum parameters, which can help target tailored management in these patients. Urine pH was low in diabetic group and underlies the importance of assessing this parameter in patients with stone disease.
Over‐The‐Counter Alkali Agents to Raise Urine pH and Citrate Excretion: A Prospective Crossover Study in Healthy Adults
KB Scotland, ME Rivera, SK Becchis, JP Ingimarsson, J Knoedler, KL Stern, C Stoughton, D Wollin, MS Borofsky, N Bhojani, M El‐Tayeb, G Kamphuis, DA Leavitt, R Hsi, NE Canvasser
Department of Urology, UCLA
Introduction & Objective: Urinary citrate is a potent inhibitor of kidney stones; hypocitraturia is a common abnormality in the recurrent stone former. The American Urological Association guidelines specifically recommend potassium citrate for urinary alkalization based on the significant improvement in urinary parameters, and the reduced risk of recurrent stone disease. However, there is poor adherence to prescribed potassium citrate therapy. More recently, patients have had increased access to alternative over‐the‐counter alkali preparations. Our goal was to assess the effect of two over‐the‐counter alkalizing agents on 24‐hour urinary parameters in healthy adults without a history of kidney stones.
Methods: Ten healthy volunteers without a history of kidney stones were recruited to complete a baseline 24‐hour urinalysis with a four‐day diet inventory. Participants were randomized 1:1 to take LithoLyte® (20 mEq two times per day) or KSPtabsTM (1 tablet two times per day) while maintaining the same diet and submit another 24‐hour urinalysis. The process was repeated with the other supplement. Urinary parameters including citrate, pH and ammonium were compared to baseline. Side effects of each supplement were elicited with a questionnaire after each urine collection
Results: LithoLyte® intake resulted in a non‐significant increase in citrate (597 to 758 mg/day, p = 0.058, an increase in urine pH (6.46 to 6.66, p = 0.028), and a decrease in urine ammonium (41 to 36 mmol/day, p = 0.005) compared to baseline (table 1). KSPtabsTM resulted in an increase in citrate (597 to 797 mg/day, p = 0.037) and urine pH (6.46 to 6.86, p = 0.037), with a non‐significant decrease in ammonium (41 to 34 mmol/day, p = 0.059). No significant differences were seen comparing urinary analytes between LithoLyte® and KSPtabsTM supplements. With Litholyte®, no side effects, mild, moderate, and severe side effects were seen in 50%, 40%, 10%, and 0%, respectively. With KSPtabsTM, rates were 60%, 20%, 10%, and 10%, respectively
Conclusions: In healthy participants without a history of kidney stones, LithoLyte® and KSPtabsTM are effective over‐the‐counter alkali supplements. Their side effect profiles appear similar to prescription potassium citrate.
Investigating fluid intake in an underserved community: what factors are associated with low urine volume on 24‐hour urine collections
A Nourian, E Ghiraldi, M Chen, J Friedlander
Einstein Medical Center
Introduction & Objective: Stone prevention is dependent on high fluid intake, with evidence that low urine volume (LUV) can promote nephrolithiasis in the absence of other metabolic abnormalities. Herein, we investigate patient‐related factors associated with LUV on initial 24‐hour urine collection in an underserved population.
Methods: A retrospective chart review was performed of patients treated by a single surgeon for nephrolithiasis from August 2014‐January 2019. Patients who submitted 24‐hour urine samples were divided into two groups based on whether their initial collection was greater than two liters or not. Factors associated with 24‐hour urine volume were analyzed using bivariate and multivariate analyses. As a secondary outcome, we investigated factors associated with corrected 24‐hour urine volume on repeat 24‐hour urine collection.
Results: Two‐hundred eight patients (45.1%) submitted 24‐hour urine collections, 63.9% (133/208) of which demonstrated urine volume <2 liters. LUV was more common in females (77.1% vs. 49.5%; p = 0.001), and patients with no insurance and Medicaid (no insurance (100%) vs. Medicaid (74.1%) vs. Medicare/private (58.6%); p = 0.02). Female gender and insurance status were independent predictors of LUV on multivariable analysis. 39.5% (17/43) of patients with LUV who provided a subsequent collection were able to correct their urine volume. Patients who successfully improved their LUV were older (58.5 vs. 45.9 years, p = 0.0149), and more likely to have surgical intervention for their kidney stones (94.1% vs. 53.8%, p = 0.006). In our multivariable analysis, surgical intervention was associated with correcting urine volume.
Conclusions: Female patients and those with no insurance or Medicaid were more likely to have LUV on an initial 24‐hour urine collection. Further research into barriers to fluid intake is important for these two groups, along with directed patient education on strategies for increasing fluid intake.
Initial experience: ex vivo perfused pig kidney to study urinary oxalate excretion
J Pavlinec, M Martin, W Donelan, E Kwenda, P Dominguez‐Gutierrez, VG Bird, BK Canales
Department of Urology, University of Florida College of Medicine and Malcom Randall Gainesville VA Medical Center
Introduction & Objective: Existing animal models of renal oxalate excretion utilize either gut or peritoneal cavity for oxalate absorption. Ex vivo renal perfusion is an established tool for graft preservation. We sought to repurpose this concept in order to study the early pathogenesis of urinary lithiasis.
Methods: Juvenile female Yorkshire porcine kidneys were removed laparoscopically and placed on an ex vivo neonatal cardiopulmonary bypass circuit utilizing whole‐blood based perfusate oxygenated with 95% carbogen. Pre‐defined goals were identified for each attempt (n = 5) with plans to increase physiologic model complexity. Tissue perfusion and oxygenation was monitored by serial perfusate iSTAT testing. Once steady urine production was achieved, aqueous oxalate was injected into the perfusate. Renal outcomes were assessed by histology and blood/urinary assays.
Results: After demonstrating proof‐of‐concept in early trials, normothermic (37°C) ex vivo whole‐blood perfusion with Steen SolutionTM was performed exceeding three hours at physiologic mean arterial pressures. Circuit parameters remained in the physiologic range for electrolytes, temperature, mean arterial pressure, lactate, and pH. Urine was produced in three experiments, with two additional attempts stopped early due to challenges related to hilar cannulation. Urinary filtrate demonstrated consistently higher urine creatinine compared to perfusate, and arterial perfusate oxalate boluses lead to urinary oxalate spikes followed by continuous oxalate clearance. Histopathologic analysis with H&E and Pizzolato's method staining demonstrated formation of calcium oxalate crystals.
Conclusions: In light of promising renal urinary oxalate and creatinine clearance, ex vivo porcine renal perfusion appears to be a feasible alternative to study oxalate excretion. Longer validation studies are necessary to establish this technique as a model for kidney stone pathogenesis.
Specialty‐Specific Differences in the Use of Preventive Pharmacologic Therapy and Metabolic Testing for Urinary Stone Disease
J Crivelli, P Yan, R Hsi, JM Hollingsworth
The University of Alabama
Introduction & Objective: While surgical stone treatment falls under the domain of Urology, stone prevention is often the responsibility of nephrologists, endocrinologists, and primary care physicians. Because of their training in and experience with preventive care, these non‐urologists may approach stone prevention differently than urologists. In this context, we assessed differences between urologists and non‐urologists in their use of preventive pharmacologic therapy (PPT) and metabolic testing among patients with urinary stone disease (USD).
Methods: Using medical claims data from working‐age adults with USD (2008 to 2017), we identified patients who were prescribed a PPT agent (i.e., a thiazide diuretic, alkali citrate therapy, or allopurinol) and had at least three years of continuous insurance coverage following their first prescription fill. We determined the specialty of the prescribing physician. Next, we distinguished between patients who completed a 24‐hour urine collection prior to their prescription fill (hereinafter referred to as selective PPT) and those who did not (empiric PPT). For the subset of patients on selective PPT, we assessed whether they completed a repeat 24‐hour urine collection and recommended blood work within six months of initiating therapy, as well as a subsequent 24‐hour urine collection within 12 months. Finally, we fit multivariable logistic regression models to evaluate for an association between use of metabolic testing and prescribing physician specialty.
Results: Among a cohort of 3648 patients on PPT for USD, 1118 (30.6%) were prescribed selective PPT. Urology patients were more likely to receive selective PPT than non‐urology patients (801/1495 [53.6%] versus 317/2153 [14.7%], P < 0.001). Compared to non‐urology patients on selective PPT, those managed by urologists had significantly higher odds of completing a repeat 24‐hour urine collection within six months of initiating therapy (odds ratio [OR], 1.58; 95% confidence interval [CI], 1.10 to 2.27). However, they had significantly lower odds of undergoing recommended blood work during the same timeframe (OR, 0.74; 95% CI, 0.55 to 0.99). No significant difference in odds of completing subsequent 24‐hour urine evaluation within 12 months was detected (OR, 0.92; 95% CI, 0.46 to 1.84).
Conclusions: There exist specialty‐specific differences in the use of PPT and metabolic testing for USD. Such differences could serve as targets for future quality improvement initiatives.
The Frequency of Metabolic Abnormalities Following Initiation of Preventive Pharmacologic Therapy for Urinary Stone Disease
J Crivelli, P Yan, R Hsi, JM Hollingsworth
The University of Alabama
Introduction & Objective: While thiazide diuretics, alkali citrate therapy, and allopurinol—collectively referred to as preventive pharmacologic therapy (PPT)—are a mainstay of urinary stone disease (USD) prevention, their adverse effect profiles remain poorly characterized. Physicians must often extrapolate from data on other conditions (e.g., hypertension, gout) for which these medications are also prescribed, even though the dosing can differ. In this context, we assessed the frequency of metabolic abnormalities following initiation of PPT in a cohort of patients with USD.
Methods: Using medical claims data from working‐age adults with USD (2008 to 2017), we identified patients who were prescribed a PPT agent and had at least three years of continuous insurance coverage following their first prescription fill. We measured the frequency of class‐specific metabolic abnormalities among these patients: hyperkalemia for alkali citrate therapy; hypokalemia, hyponatremia, hyperglycemia, or hypercalcemia for thiazide diuretics; and elevated liver function tests for allopurinol. We then fit a multivariable logistic regression model to evaluate for an association between the occurrence of a metabolic abnormality and the PPT drug class prescribed.
Results: Among a cohort of 3914 patients with USD who were prescribed a PPT agent, 54.3%, 34.5%, and 20.7% received a thiazide diuretic, alkali citrate therapy, and allopurinol, respectively. Overall, 708 patients (18.1%) had at least one metabolic abnormality during a three‐year period after PPT prescription. Hyperglycemia after initiating a thiazide diuretic was most frequent, while thiazide‐induced hyponatremia was least frequent (Table). Compared to patients prescribed alkali citrate therapy, those prescribed a thiazide diuretic (odds ratio [OR], 11.95; 95% confidence interval [CI], 8.40 to 17.00) or allopurinol (OR, 3.35; 95% CI, 2.16 to 5.20) had significantly higher odds of experiencing a metabolic abnormality.
Conclusions: Nearly one in five patients prescribed PPT for USD prevention will experience a medication‐induced metabolic abnormality. These data can be used to counsel patients prior to prescribing PPT. Furthermore, they highlight the importance of guideline‐recommended follow‐up serum testing after the initiation of PPT.
Adherence to Recommended Follow‐Up Testing Among Patients Prescribed Preventive Pharmacologic Therapy for Urinary Stone Disease
J Crivelli, P Yan, R Hsi, JM Hollingsworth
The University of Alabama
Introduction & Objective: The AUA's Medical Management of Kidney Stones guideline outlines specific recommendations on follow‐up testing for patients prescribed preventive pharmacologic therapy (PPT). We conducted a study assessing adherence to these recommendations and how adherence relates to subsequent urinary stone disease (USD) events.
Methods: Using claims data from working‐age adults with USD (2008 to 2017), we identified patients who were prescribed a PPT agent (i.e., a thiazide diuretic, alkali citrate therapy, allopurinol, or a combination thereof) following completion of a 24‐hour urine collection. Among these patients, we measured adherence to three recommendations outlined in the AUA guideline: 1) repeat 24‐hour urine collection within six months of PPT prescription, 2) drug class‐specific serum testing within six months of PPT prescription, and 3) subsequent 24‐hour urine collection within 12 months. We then determined whether patients experienced a USD event (emergency department [ED] visit, hospitalization, or surgery) within three years of PPT receipt. Finally, we fit multivariable logistic regression models, evaluating for an association between USD event occurrence and non‐adherence to recommended follow‐up testing.
Results: Among 1160 patients with USD who were prescribed a PPT agent after a 24‐hour urine collection, adherence to individual follow‐up testing recommendations outlined in the AUA guideline was low (Table). Follow‐up testing varied by drug class prescribed, with 16.7% of patients on allopurinol completing a repeat 24‐hour urine collection within six months of initiating therapy, compared to 30.6% of those on combination therapy (P = 0.01 for the difference). Non‐adherence to guideline recommendations was associated with the occurrence of a USD event. Namely, patients who did not complete a repeat 24‐hour urine collection within six months of initial PPT prescription had significantly higher odds of an ED visit, hospitalization, or surgery (odds ratio, 1.69; 95% confidence interval, 1.02 to 2.79).
Conclusions: Most patients prescribed PPT do not receive recommended follow‐up testing, which is important because non‐adherence was associated with higher odds of a USD event.
Preliminary study on the role of selective regulation of CaSR‐Claudin‐14 pathway in the formation of calcium oxalate kidney stones in rats
B qian, Z Guoxi, X Zou, G Wu, W Xiaoning, Y Yuan
Introduction & Objective: Through selectively regulating the calcium sensitive receptor‐tight junction protein 14 (CaSR‐Claudin‐14) pathway, this study preliminarily explore the role of this protein pathway in the formation of calcium oxalate kidney stones in rats.
Methods: 120 Wistar male rats were selected and randomly divided into blank control group (NC group), ethylene glycol (EG group), agonist group (EG+ group) and inhibitor group (EG‐ group), with 30 rats in each group. After modeling, 3 rats were randomly selected from each group and sacrificed every week. Kidney tissue was taken to observe the pathological changes and detect the expression of CaSR and Claudin‐14 by Immunofluorescence and Western blot.
Results: Except NC group, crystal was found in the pathological smears of the other groups. The EG+ group had the most crystals, followed by the EG group, and the EG‐ group had the least; Western blot and immunofluorescence results showed that CaSR and Claudin‐14 were expressed in the four groups. From the third week, the expression levels of CaSR and Claudin‐14 in the remaining three groups gradually decreased except NC group. By the eighth week, the difference in expression of CaSR and Claudin‐14 reached the maximum. The expression level from low to high were EG+ group, EG group, EG‐ group, NC group respectively, and the difference between each group was statistically significant.
Conclusions: The expression of CaSR is negatively correlated with the amount of crystals. The change of Claudin‐14 is positively correlated with CaSR. The CaSR‐Claudin‐14 pathway plays a role in inhibiting the formation of stones.
Opioid Free Ureteroscopy: what is the true failure rate?
MS Lee, M Assmus, DK Agarwal, ME Rivera, T Large, AE Krambeck
Northwestern University Feinberg School of Medicine
Introduction & Objective: Due to the opioid epidemic in America, opioid overdose is now the leading cause of death in adults under the age of 55. In response, physicians have attempted to reduce or eliminate unnecessary opioid usage. At Indiana University, we implemented a opioid free ureteroscopy (OFURS) pathway in February 2018. While OF‐URS has been shown to be feasible by several groups, success is usually defined as whether or not the patient was discharged with opioids, overlooking the possibility that the patient obtained opioids from another source (e.g. primary care doctor or local ED). Therefore, our objective was to determine the true failure rate of OF‐URS and rates of new‐persistent opioid use utilizing a national prescription drug monitoring program (PDMP).
Methods: We identified 239 patients utilizing our retrospective stone database who underwent OF‐URS from Februrary 2018‐March 2020. Our OF‐URS pathway consists of diclofenac, tamsulosin, acetaminophen, pyridium and oxybutynin. Patients who had a contraindication to NSAIDs were excluded from primary analyses. A PDMP was then utilized to determine the number of patients who failed OF‐URS (defined as receipt of an opioid within 31 days of surgery) as well as rates of new‐persistent opioid use (defined as receipt of opioid 91‐180 days after surgery). All statistical analyses were performed using SAS 9.4. Tests were two‐sided and statistical significance was set at p < 0.05
Results: We found a OF‐URS failure rate of 16.6% and 14.0% in the total and opioid naïve cohorts, respectively. Rates of new‐persistent opioid use were 0.9% and 1.2%, respectively (lower than published expected rate of ∼6%). 91.0% of patients obtained opioid from alternative sources. Uni/multivariate analyses were performed for both cohorts. In the total cohort, benzodiazepine use was a risk factor for nf‐URS failure on multivariate analysis. In the opioid naïve cohort, no associated variables were identified as risk factors for OF‐URS failure.
Conclusions: The true failure rate of OF‐URS is higher than previously thought at 16.6% and 14.0%. However, efforts to reduce opioid prescriptions have successfully reduced new‐persistent opioid use.
Percutaneous Nephrolithotomy (PCNL) As Outpatient Surgery: Analysis of Stone‐Free Rate and Complications at a Single Center
SK Bechis, E Kelly, E Kong, R Zupkas, J Roberts, S Attaluri, T DiPina, R Sur
University of California ‐ San Diego, Department of Urology
Introduction & Objective: There has been a shift towards performing PCNL as same day surgery in select patients. We previously reported our initial experience with outpatient surgery. The goal of this study is to evaluate the outcomes in an updated cohort of patients who underwent outpatient PCNL.
Methods: 151 patients at a single institution underwent outpatient PCNL from October 2016 to June 2019 by two different surgeons. Patients were included in the study if they had a postoperative Computed Tomography (CT) scan to evaluate true residual stone burden. A retrospective chart review of these 113 patients was performed to evaluate the stone‐free rate as well as rate of post‐operative complications and readmissions. Other variables assessed included initial stone size, renal access method (fluoroscopic vs ultrasonic), access location, patient positioning (supine vs prone), and operative time.
Results: Of the 113 patients included in the study, 46% (n = 52) were stone free as defined by no identifiable fragments seen, 11% (n = 12) had residual fragments 0‐2mm, 7% (n = 8) had residual fragments 2‐4mm and 36% (n = 41) had residual fragments greater than 4mm. 63 (56%) patients were ASA Class 2, 49 (43%) were class 3, and 1 (0.9%) was class 4. Mean initial stone size was 23.6 (STDdev 14.3) mm. Mean operative time was 119.9 (+‐ 38.6) minutes. 47% (n = 53) of access was achieved via ultrasound alone. 20% (n = 23, Table 1) had a complication within 30 days of surgery. Complications included Clavien‐Dindo 1 (14), Clavien‐Dindo 2 (3), and Clavien‐Dindo 3 (6). No patients required transfusion. 27 out of 113 (24%) patients returned to the Emergency Department, and 20 (18%) were readmitted within 30 days.
Conclusions: In this large contemporary series of outpatient PCNL we demonstrate acceptable stone free and complication rates similar to our initial report1 and those of others. In appropriately selected patients, outpatient PCNL should be considered a safe and effective approach to treatment of urolithiasis.
1. Bechis SK, Sur RL et al. Outpatient PCNL: The UC San Diego Health Experience. J Endourol. 2018 May;32(5): 394‐401.
Clinical Characteristics and Outcome of Living Kidney Donors with Obesity in the Era of Laparoscopic Donor Nephrectomy
DA Mendiola, JT Prodigalidad
National Kidney and Transplant Institute
Introduction & Objective: With millions of Filipinos being obese, a potential living donor coming in for work‐up is inevitable. Obesity is associated with an increased risk of wound‐related complications and operative time in open donor nephrectomy. In the era of laparoscopic donor nephrectomy, we looked into the outcome of laparoscopic donor nephrectomy among obese donors and compared it with non‐obese donors.
Methods: A chart review was done on all obese and non‐obese patients who underwent laparoscopic donor nephrectomies from January 2011 to December 2015. Donor demographics (age, gender, BMI) intraoperative [operative time (OT), length of hospital stay (LOS), estimated blood loss (EBL) and warm ischemia time (WIT)] and postoperative outcomes [mean creatinine rise, delayed graft function (DGF)], complications and one‐year allograft survival were compared between the two groups.
Results: A total of 439 patients underwent laparoscopic donor nephrectomy from January 2011 to December 2015. 38 of which were obese. The donor characteristics were similar for both. Donor OT (179min vs 178 min, p = 0.64), EBL (100mL vs 100mL, p = 0.15), LOS (3 days vs 3 days, p = 0.95), and WIT (4min vs 4 min, p = 0.79) were statistically not different. There was no significant change in the mean donor and recipient creatinine up to one year. There was neither conversion to open nor mortality for both. The one‐year allograft survival was also similar between the two groups (p = 1.00).
Conclusions: Laparoscopic donor nephrectomy in obese patients has a safety profile comparable to non‐obese patients. One year follow‐up shows graft survival comparable between obese and non‐obese donors.
Interim Results for the ROBUST III Trial Evaluating the Optilume Drug Coated Balloon for Anterior Urethral Strictures
O Kayes, S Elliott, R Virasoro, J DeLong, K Coutinho, K Robertson, R D'Anna
St James's University Hospital
Introduction & Objective: Endoscopic management of anterior strictures includes dilation or direct visualization internal urethrotomy (DVIU). Multiple treatments lead to progressively worse outcomes. The Optilume® Drug Coated Balloon (DCB) is a dilation balloon with a paclitaxel coating that combines mechanical dilation for immediate symptomatic relief with local drug delivery to maintain urethral patency. The ROBUST III study is a randomized, single blind trial evaluating the safety and efficacy of the Optilume DCB against endoscopic management of recurrent anterior urethral strictures.
Methods: 127 subjects were enrolled at 23 sites. Key eligibility criteria included anterior strictures with ≥2 prior treatments and a length ≤3cm. Subjects with previous urethroplasty or unresolved confounding etiologies were excluded. The primary study endpoint compared the proportion of subjects that were stricture free at 6 months, measured by the ability to pass a 16Fr flexible cystoscope or 14Fr catheter through the treated area. Key secondary endpoints included freedom from repeat treatment, International Prostatic Symptom Score (IPSS), and peak flow rate (Qmax). The primary safety endpoint included freedom from serious device or procedure related complications.
Results: Baseline characteristics were similar between groups, with subjects having an average of 3.6 prior treatments and average length of 1.7cm. Primary 6 month follow up is complete and one year follow up is ongoing. Stricture free rate for Optilume DCB was significantly higher than Control at 6 months (76% vs 27%, p < 0.001). Outcomes were consistent among subgroups with ≥5 vs <5 dilations and for lengths <2cm vs ≥2cm. Freedom from repeat intervention was significantly higher in the Optilume DCB arm. Immediate symptom improvement was significant in both groups, with the benefit being more durable in the Optilume DCB group. Improvement in Qmax showed a similar trend. No subjects experienced a serious device related complication. The most frequently adverse events included common events such as urinary tract infection, post‐procedural hematuria, and dysuria.
Conclusions: The Optilume Urethral DCB exhibited a significant improvement in both objective and subjective outcomes through 1‐year post treatment compared to standard of care and represents a potential breakthrough in the endoscopic management of recurrent anterior urethral strictures. Long term follow‐up is planned through 5 years to further define the durability of the results.
Diverging Trends in Inpatient Admissions for Adult and Pediatric Kidney Stone Disease in the United States
R Alam, W Wu, BR Matlaga, JS Winoker
Johns Hopkins University School of Medicine
Introduction & Objective: The growing incidence of kidney stone disease (KSD) is well supported by evidence for both the adult and pediatric populations. At the same time, prior work suggests that this evolving epidemiology has been accompanied by increases in hospitalizations and surgical interventions for KSD. Acknowledging the advancements in surgical technology and techniques over the last decade, we hypothesized that the relative frequency of requiring inpatient care for KSD over time would decrease.
Methods: In this population‐based cohort study, the National Inpatient Sample (NIS) and Kids' Inpatient Database (KID) were used to estimate nationwide inpatient admissions in the United States related to urolithiasis for adults and children, respectively. To evaluate for regional differences, patients were categorized into one of four regions as defined by the United States Census Bureau. Data from 2006 and 2016 were used to evaluate for trends in prevalence over time. The relative risk (RR) of admission for KSD in 2016 versus 2006 was compared within NIS and KID separately. The RR of admission for KSD in adults versus children was compared within the year 2006 and 2016 separately, as well.
Results: The incidence of KSD requiring admission nationwide was 1080 per 100,000 adults in 2016, up from 849 per 100,000 adults in 2006 (RR 1.27, P < 0.001; Table). A significant increase in KSD admissions was found in all four regions. By contrast the incidence of KSD in children nationwide dropped over time, from 166 per 100,000 children in 2006 to 136 per 100,000 children in 2016 (RR 0.82, P < 0.001). Three of 4 regions demonstrated a decline in childhood urolithiasis, but children in the Western region demonstrated no significant change (RR 1.07, P = 0.52). In 2006, adults were 5 times more likely to be admitted for KSD than children (RR 5.10, P < 0.001), but this gap widened to nearly 8 times in 2016 (RR 7.96, P < 0.001).
Conclusions: Between 2006 and 2016, the nationwide incidence of KSD requiring admission increased in adults, but decreased in children. Further work is warranted to uncover the factors driving these discrepancies in management.
Ambulatory Percutaneous Nephrolithotomy is Safe and Effective in Extended Criteria Patients
G Hosier, K Visram, N Touma, S Steele, D Beiko
Queen's University
Introduction & Objective: Ambulatory tubeless percutaneous nephrolithotomy (aPCNL) has been shown to be safe and effective in highly selected patients. However, these selection criteria preclude the vast majority of patients that undergo PCNL. The objective of our study was to compare complication and stone free rates after aPCNL in standard selection criteria vs. extended criteria patients.
Methods: Retrospective review of prospective data on all patients who underwent aPCNL at one academic center from 2007‐2018. Extended criteria patients were defined as any: Age >75 years, BMI >30 kg/m2, ASA >2, bilateral stones, solitary kidney, staghorn calculi, stone burden >40 mm, multiple tracts, or prior nephrostomy tubes/stents. Primary outcomes were complication rates (Clavien‐Dindo classification) and stone free rates (no fragments >/ = 3 mm). All patients were discharged with a ureteric stent and no nephrostomy tube after meeting discharge criteria which included hemodynamic stability, no fever, and no significant pain.
Results: We identified 118 patients of which 92 (78%) met extended criteria. Mean BMI was 31 kg/m2 and 45% were ASA 3 or higher. Mean sum maximum stone diameter was 24 mm. Multiple stones were present in 25%, bilateral stones in 7%, staghorn stones in 4%, and pre‐existing tubes/stents in 4%. There was no difference in complication (12% vs. 18%, p = 0.56), Emergency department visit (12% vs 18%, p = 0.56), or readmission (4% vs. 5%, p = 1) rates between standard and extended criteria patients respectively (Table 1). Of the complications, 85% were Clavien‐Dindo grade 1. Stone free rates were not different between standard (84%) and extended (83%) criteria patients (p = 1). No extended criteria variables were associated with complications in univariate analysis. Stone burden >40 mm (OR 5.8, 95% CI 1.4‐25.2, p = 0.018) and multiple tracts (13.1, 95% CI 1.1‐154.7, p = 0.041) were associated with residual stone fragments.
Conclusions: Complication and stone free rates were not different between standard and extended selection criteria patients undergoing aPCNL. This data supports the safety and efficacy of aPCNL in patients using extended selection criteria. As the COVID‐19 pandemic continues to strain hospital resources, aPCNL offers a solution to deal with a growing backlog of patients with complex stone disease.
A Comparison of Hospital Charges Between Secondary Robotic Pyeloplasty and Chronic Ureteral Stenting for Management of Recurrent Ureteropelvic Junction Obstruction
M Lee, Z Lee, I Hollin, DD Eun, N Krishnan
Lewis Katz School of Medicine at Temple University
Introduction & Objective: We compared hospital charges for patients undergoing secondary robotic pyeloplasty (SRP) versus chronic ureteral stenting (CUS) for management of recurrent ureteropelvic junction obstruction (UPJO) after prior failed pyeloplasty.
Methods: We constructed a decision tree to demonstrate two options for UPJO management (Figure 1). We performed probability‐weighted calculations based on success rates to determine total hospital charges for CUS and SRP. CUS was assumed to have a 100% success rate. The success rate for SRP was determined using data from our Collaborative of Reconstructive Robotic Ureteral Surgery database. Hospital charges were determined using the Pennsylvania Health Care Cost Containment Council (PHC4) database. PHC4 contains hospital charge data from inpatient and outpatient centers across 5 counties in Pennsylvania. Total hospital charges to payers were calculated using room/board, ancillary, drug, equipment, specialty, and miscellaneous charges. We determined how many ureteral stent exchanges would be required for CUS to result in higher hospital charges compared to SRP.
Results: The success rate for SRP is 90%. Mean hospital charges for an SRP and a single ureteral stent exchange are $40,871.40 and $5,894.10, respectively. Total probability‐weighted charges for both options were determined in terms of the number of stent exchanges. The total charge for CUS was $5,894.10 × Number of Stent Exchanges. The total charge for SRP was calculated by adding the probability‐weighted charge of a successful SRP (0.9 × $40,871.40) to the probability‐weighted charge of a failed SRP (0.1 x [$40,871.40 + $5,894.10 × Number of Stent Exchanges]). We determined that hospital charges for CUS were higher than hospital charges for SRP after 8 ureteral stent exchanges.
Conclusions: After 8 ureteral stent exchanges, CUS may result in higher hospital charges to payers versus SRP for management of recurrent UPJO after prior failed pyeloplasty. These data may play a role in the decision‐making process for patients undergoing management of recurrent UPJO.
Same‐day discharge after benign prostatic hyperplasia procedures: a case‐control matched analysis from the ACS‐NSQIP database
KT Ravivarapu, EB Garden, O Omidele, A Small, O Al‐Alao, MA Palese
Icahn School of Medicine at Mount Sinai
Introduction & Objective: Same‐day discharge (SDD) for benign prostatic hyperplasia (BPH) procedures may be feasible, but the safety of this approach on a wider scale remains to be evaluated. Using a national cohort, we compared 30‐day outcomes among SDD versus standard‐length discharge (SLD) for transurethral resection (TURP), holmium laser enucleation (HoLEP), and GreenLight photovaporization (GL‐PVP).
Methods: We reviewed all patients who underwent TURP, HoLEP, and GL‐PVP for BPH in the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database between 2014‐2019. SLD was defined as length of stay of 1‐3 days for TURP, 1‐2 days for HoLEP, and 1‐2 days for GL‐PVP. For each procedure, SDD and SLD patients were matched based on age, body mass index (BMI), ASA score, and modified Charlson Comorbidity Index (mCCI) score. We compared 30‐day readmissions and Clavien‐Dindo (CD) complications between SLD and SDD cohorts for each procedure and evaluated predictors of adverse outcomes using multivariate logistic regression.
Results: Overall, there were 46898 BPH procedures performed including 31872 TURP, 2901 HoLEP, and 12125 GL‐PVP. For TURP, 15330 matched SDD and SLD cases showed no differences in reoperation, CD I/II and CD IV complications. SDD for TURP resulted in less 30‐day readmissions (3.65% SDD vs. 4.46% SLD; p = 0.011). For HoLEP, comparison of 1760 matched cases showed no differences in reoperation, CD I/II and CD IV complications between SDD and SLD cohorts. The 30‐day readmission rate for SDD HoLEP was lower than SLD (2.50% SDD vs. 4.88% SLD; p = 0.008). For GL‐PVP, 6710 cases were matched, and there were no differences in 30‐day readmission, reoperation, CD I/II and CD IV complications. When controlling for other demographic and clinical factors, SDD correlated with decreased odds of 30‐day readmission compared to SLD for TURP (OR 0.822, 95% CI 0.694‐0.974, p = 0.023) and HoLEP (OR 0.479, 95% CI 0.275‐0.831, p = 0.009) (Table 1).
Conclusions: SDD after TURP, HoLEP and GL‐PVP did not confer increased risk of 30‐day readmissions, reoperations, or complications. These results from a large nationwide cohort indicate that patient selection for SDD is being done with appropriate safety, but further work is needed to define specific selection criteria.
Risk of Postpartum Urinary Stone Disease in Women with History of Urinary Stone Disease During Pregnancy
K Spradling, C Zhang, A Pao, JC Liao, J Leppert, C Elliott, S Conti
Introduction & Objective: Urinary stone disease during pregnancy is a clinical challenge and is associated with fetal and maternal morbidity. While several physiologic changes during pregnancy are thought to increase the risk of developing stone disease, it is unclear if women with urinary stone disease during pregnancy are at risk for recurrent urinary stone disease after pregnancy. We aimed to determine the risk of postpartum urinary stone disease in women with a history of stone disease during pregnancy.
Results: We identified a total of 1,395,783 pregnant women with a median postpartum follow‐up of 4.0 years, including 5,971 (0.4%) women diagnosed with a urinary stone during pregnancy. Of these, 736 (10.5%) had an additional urinary stone diagnosis claim after pregnancy, compared with 13,275 (0.95%) women without a history of stone disease during pregnancy (p < 0.0001). In multivariable proportional hazards models urinary stone disease during pregnancy (HR 12.8, 95% CI [11.8 – 13.8]) was independently associated with a higher hazard of urinary stone disease after pregnancy (Figure 1).
Conclusions: Women urinary stone disease during pregnancy have an increased risk of developing urinary stone disease after pregnancy. Given the 1 in 10 chance of needing further care, women with history of stone disease during pregnancy may benefit from risk counseling, surveillance, or secondary prevention efforts in the postpartum period.
One‐day Surgery bipolar vapo‐resection for benign prostatic hyperplasia : first experience
A Heddat, Y Houry, R Rabii
university Mohammed VI of health sciences UM6SS
Introduction & Objective: This prospective study evaluated the efficacy, safety and post‐operative complications of benign prostate hypertrophy using Bipolar Photo Vaporisation TURis (BPV) in day surgery settings.
Methods: Over a 48 months period, 1120 patients who fulfilled selection criteria, were recruited to have day surgery prostate resection using BPV. Pre‐operative International Prostate Symptoms Score (IPSS) and urine flow were obtained in every patient. Per‐operatively, we measured prostate resection time, weight of resected tissue and occurrence of any complications. Bladder residual content, duration of transurethral drainage were measured post‐operatively.
Results: the mean prostate tissue weight was 51 g (45‐140g). The mean operative duration was 45 minutes (35‐70 min). No major complications occurred in all cases. The trans‐urethral catheter was removed the following day. All cases left Hospital the same day. All patients had noticeable improvement of the IPSS and maximal urine flow (Qmax). The mean specimen prostatic tissue weight was 25 g.
Conclusions: Bipolar Photo Vaporisation of benign prostate hypertrophy in selected patients could be carried out safely as day care procedure and has beneficial outcomes for patients and services.
The Acute Stone Clinic model: Improving waiting times and patient care in a public funded health care system
T Tien, E Balai, S Folkard, K Atalar, B Berry, C Bastianpillai, Z Yasen, L Crabtree, R Peggs, S Graham, J Green, P Pal
Barts Health ‐ Urology
Introduction & Objective: The management of patients with ureteric stones can be logistically challenging in large volume centres with long waits for outpatient clinics and definitive interventions. Many units in publicly funded health systems resort to temporising obstructed kidneys with stent insertion and a subsequent plan for elective ureteroscopy at a later date. This can result in unnecessary stent insertions, repeated attendances to the emergency department and an overall poor experience for patients. We aimed to reorganise resources to improve waiting times for definitive intervention, reduce the need for pre‐stenting, reduce emergency department re‐attendance and improve the overall patient experience.
Methods: All patients diagnosed with ureteric stones between March – September 2017 were collected as baseline data. Time to clinic review and definitive treatment were measured. By collaborating with the emergency department, radiology and operation schedulers, our intervention for improvement where a consultant led acute stone clinic (ASC) with a pathway for primary ureteroscopy was implemented and a second cycle was performed June 2018 – January 2019. Further data was collected January – October 2020 to assess performance during the COVID‐19 pandemic.
Results: After implementing the ASC model, median time from diagnosis to clinic consultation reduced from 77 to 9 days. Median time to definitive procedure reduced from 56 to 25 days. Emergency ureteric stent insertion reduced from 69.1% to 27.9%. Reattendance to the emergency department reduced from 3.0 to 1.6 episodes/month. Primary definitive treatment increased from 31.0% to 72.1%. Patients receiving definitive treatment within 4 weeks improved from 26.2% to 51.2% post intervention and sustained at 54.5% during the pandemic period.
Conclusions: Implementation of the ASC model has led to a reduced time from diagnosis to clinic review and from diagnosis to definitive treatment. Further improvement is limited by the lack of extra operating lists to reduce the waiting times for ureteroscopy. The ASC model can provide a blueprint for other hospitals to improve outcomes and care of patients with acute ureteric stones.
Refractory Urethral Stenosis in Poor Surgical Candidates for Urethroplasty: Off‐label Use of the EpicTM Vascular Self Expanding Stent
JT Kurtzman, R Blum, S Mendonca, S Brandes
Columbia University Irving Medical Center
Introduction & Objective: The UroLumeTM, a permanent urethral wall stent (UWS), was previously available to treat short, recurrent bulbar strictures, particularly in elderly and comorbid patients who were poor surgical candidates or refused urethroplasty. It also demonstrated promise in treating recalcitrant bladder neck contractures (BNC) in select patients. Currently, there are no UWS on the United States market. This was a pilot study was to investigate the off‐label use of a vascular stent in the urethra in select patients.
Methods: Retrospective review identified all patients who underwent vascular stent placement. Inclusion criteria: Age‐adjusted Charlson Comorbidity Index Score (CCI) ≥4 (maximum 53% 10‐year estimated survival), recurrent (≥ 2 prior interventions) for stenosis ≤3.5 cm, ability to dilate to ≥24Fr, poor open surgical candidate, desire to void via the penis. The EpicTM Vascular Self Expanding Stent (Boston Scientific) was chosen because of its excellent radial force, deployment accuracy and metal flexibility. Procedure: stenotic region was dilated to ≥24, under cystoscopic and fluoroscopic guidance a 12mm (diameter) EpicTM stent (2‐4cm length) was deployed over a wire to cover the stenosis and region just beyond, proximal and distal.
Results: A total of 12 patients were included, median age: 75 years (IQR 66 ‐ 79) and mean CCI score: 6 (range 4‐10). 8 patients (67%) had prior prostate cancer, of which 88% had radiation therapy (RT) and 38% prostatectomy. 1 additional patient had RT for colorectal cancer. Mean stricture length 2.4cm (range 1.5‐3.5). 6 strictures were membranous, 4 bulbomembranous, 1 bulbar, and 1 BNC. 8/12 (67%) were in retention prior to stent. Of patients able to void, mean AUA Symptom Score was 23, Q‐max 6.8 ml/s and PVR 68cc. Post stenting, 100% of patients were initially able to void and mean PVR among those previously in retention was only 68cc. At mean follow up of 14.8 months, 3 patients (25%) required a 2nd intervention for recurrent stenosis: 2 had second stenting at 17 and 23 months, respectively; 1 had balloon dilation and periurethral steroid injection at 20 months. All 3 had a history of ≥4 treatments prior to initial stenting. One stent was removed during explant of an infected/eroded artificial urinary sphincter.
Conclusions: The EpicTM stent, at short term follow‐up, is a viable option for elderly patients with devastated, obstructed outlets who have failed multiple prior interventions, and are medically unfit for reconstructive surgery, but strongly desire to be able to void. Larger and long‐term studies are needed.
Barriers to same‐day discharge after percutaneous nephrolithotomy
H Yang, J Holler, H Lee, G Hosier, R Unno, F Hamouche, J Ahn, D Bayne, A Odisho, M Stoller, T Chi
Introduction & Objective: The COVID‐19 pandemic has provided an impetus to reconsider traditional urologic practices and adapt to the unprecedented healthcare burden. Reducing length of stay after minimally invasive procedures is now more important than ever. Using percutaneous nephrolithotomy (PCNL) as a model, we sought to evaluate clinical barriers to same‐day discharge in order to better understand the feasibility of outpatient surgery.
Methods: Prospective data collected from 500 inpatient PCNLs performed at our institution between 2016 and 2020 was analyzed via the Registry for Surgery of the Kidney and Ureter (ReSKU). Preadmissions and aborted procedures were excluded. We analyzed issues and complications that warranted postoperative admission. Major categories included infection, bleeding, and excessive pain, which was defined as either a documented pain complication or administration of intravenous opioids within 24 hours after discharge from the recovery room. Multivariate statistics were used to assess risk factors for each outcome.
Results: Excessive pain was the most common postoperative issue (40.9%). ASA score was inversely correlated with odds of having increased pain (OR 0.64, 95% CI 0.42‐0.98) and was the only statistically significant predictor in our multivariate model that included dilated tract number, diameter, and location. The postoperative SIRS/sepsis rate within 7 days was 9.7%, and higher ASA score (OR 3.6, 95% CI 1.8‐7.6) and incomplete stone clearance (OR 2.7, 95% CI 1.2‐6.3) were significant predictors. Age, sex, body mass index (BMI), stone burden, and positive preoperative urine cultures were not associated with overall infection rate. In patients who had a postoperative infection, 34.1% of infections were detected intraoperatively or in the recovery room, and 48.8% were associated with the nephrostomy tube removal process on postoperative day 1. Patients who had a postoperative double‐J stent rather than a nephrostomy tube had a lower overall infection rate (1.8%, p = 0.047). Finally, only 1.9% of patients had a bleeding complication, and 1.1% required a blood transfusion.
Conclusions: Pain is the major barrier to same‐day discharge after PCNL. Bleeding is infrequent and most infections can be recognized perioperatively or avoided with alternative tube management strategies. Rigorous patient selection for same‐day discharge does not appear to be necessary. Optimizing pain control may be the key to performing outpatient surgery on a large scale.
Factors Contributing to Inpatient vs Ambulatory Percutaneous Nephrolithotomy
MM Dunne, J Chong, JE Abbott, JG Davalos
Chesapeake Urology, Univeristy of Maryland Baltimore Washington Medical Center
Introduction & Objective: Percutaneous nephrolithotomy (PCNL) surgery has traditionally been performed with at least an overnight stay in a hospital for a variety of reasons including medical, social and surgeon preferences. There continues to be a trend toward moving surgical procedures to an ambulatory setting. To date there have been no criteria established to ascertain which patients require inpatient hospitalization after PCNL. The purpose of this review is to determine what factors lead to inpatient versus outpatient PCNL surgery.
Methods: We reviewed 259 consecutive PCNL procedures performed from December 2018 to October 2019 in both a hospital and an ambulatory surgery center (ASC) setting by a single surgeon. 185 cases were performed in an ASC and 74 were performed in the hospital. These patients were separated into two groups, those that required hospital admission (n = 31) or were transferred from ASC (n = 1) and those that were either discharged same day from the hospital (n = 43) or ASC (n = 184). Demographics, co‐morbidities, stone characteristics, and operative times were compared with univariate analyses and odds ratios were calculated to find those factors associated with inpatient hospitalization.
Results: Overall 32 patients (12.4%) required inpatient hospitalization after PCNL. Patients requiring admission were more likely to have a positive preoperative urine culture (OR = 5.37, p < 0.0001), be on anticoagulation (OR = 8.42, p = 0.002), have an American Society of Anesthesiologists Physical Status Classification System (ASA) level >2 (OR = 9.2, p = 0.0001), stone burden >mean of 40mm (OR = 2.98, p = 0.0061), and total operative time > mean of 125 min (OR = 5.32, p < 0.0001).
Conclusions: ASA level >2 and preoperative anticoagulation predict for inpatient hospitalization. This correlates with increased cardiac anesthetic risk. Operative time >125 min and stone burden >40mm also predict inpatient hospitalization, reflecting increased case complexity. Finally, having a pre‐PCNL positive urine culture predicts for inpatient hospitalization, which correlates with concerns for post‐operative infectious complications. Continued efforts to understand patient and surgical factors that are favorable for same day discharge PCNL can lead to the development of criteria to determine which patients are best suited for ambulatory surgery.
Withdrawn
Practice patterns and outcomes of urgent/emergent versus elective ureteroscopy
J DiBianco, A Dupati, S Daignault‐Newton, K Witzke, D Wenzler, KR Ghani, CA Dauw, f Urological Surgery Improvement Collaborative
Department of Urology, University of Michigan
Introduction & Objective: Urgent indications for ureteroscopy (URS) include obstructing stones causing intractable pain or renal impairment without infection. Most patients receive urinary drainage and postpone definitive treatment for subsequent intervention. However, patients and hospitals may benefit from urgent primary URS to avoid morbidity. Moreover, utilization and outcomes associated with urgent URS are unknown. We examined variation in urgent/emergent URS utilization and its associated outcomes.
Methods: Reducing Operative Complications from Kidney Stones (ROCKS) is a quality improvement initiative from the Michigan Urological Surgery Improvement Collaborative (MUSIC) that maintains a prospective clinical registry of ureteroscopy (URS) and shockwave lithotripsy (SWL) cases. We identified all URS procedures from 2016 through 2019 in the ROCKS registry. Cases are classified according to elective versus urgent acuity. Urgent is defined as URS performed within 48 hours after emergency department (ED) visit. We assessed practice and surgeon variation in urgent URS performance. We characterized patients across demographic, operative and outcomes data. We made bivariate comparisons with elective URS to understand implications of urgent surgery. Finally, we performed multilevel modeling to understand factors associated with unplanned healthcare encounters after urgent URS.
Results: 12859 cases were identified from 33 practices and 204 urologists, 10854 (84.4%) elective and 2005 (15.6%) urgent. Urgent URS rates by practice and surgeon ranged from 2.3‐70% and 0‐97.7%, respectively (Fig.). Patients who underwent urgent compared to elective URS were significantly younger (53 vs 57, p < 0.001), ureteral stone location (72.8% vs 56.8%, p < 0.001), presence of hydronephrosis (89.1% vs 69.4%, p < 0.001) and had a higher stenting rate (77.4% vs 72.5%, p < 0.001). Urgent URS patients had higher ED visit rates (11% vs 7.2%, p < 0.001) and higher stone free rates (66% vs 58.4%, p < 0.001). There was no difference in intraoperative complications or unplanned hospitalizations. Factors predictive of ED visits included concomitant ureteral and renal stone location (OR = 1.58, p = 0.03).
Conclusions: Wide variation exists in the rate of urgent URS in the state of Michigan. Urgent URS is associated with increased rate of postoperative ED visits and a higher stone free rate than those cases performed electively.
Scar‐Modulating Effect of Intraurethral Dexpanthenol on Urethral Healing Post Urethroplasty: An Experimental Study in Rats
M Hassaan, AH Elkashef, N Barakat, A Awadalla, A Hashem, F El‐Seddawy, M Abdel‐Maboud
Department of Urology, Urology and Nephrology Center, Mansoura University, Egypt
Introduction & Objective: Urethroplasty is a complex procedure that depends on functional wound healing to be successful. Excessive inflammation and fibrosis post urethroplasty may lead to recurrent urethral stricture. Dexpanthenol (DXP) is an alcoholic form of pantothenic acid that has been used for wound healing for a long time. Therefore, we evaluated the effect of intraurethral DXP on urethral healing, inflammation and fibrosis after urethroplasty in rats.
Methods: 54 male Sprague–Dawley rats were randomly allocated into 3 groups (18 rats each); control, urethroplasty and DXP groups. Urethroplasty was performed by creating a 0.8‐cm vertical midline urethral incision with a microknife, then closing the urethra and overlying corpus spongiosum using 7‐0 PDS. Saline solution 0.9% and DXP (500 mg/kg) was then administered intraurethrally once daily till sacrification to urethroplasty and DXP groups, respectively. 6 rats from each group were sacrificed on the postoperative days 4, 8 and 15. Penectomy was performed and the penises were then sent for routine histopathological examination, interleukin (IL)‐6, transforming growth factor (TGF)‐ß1, ß‐catenin, vascular endothelial growth factor (VEGF) and collagen I & III relative gene expression and assessment of malondialdehyde (MDA) and nitric oxide (NO) activity.
Results: There was significant improvement in inflammation and fibrosis scores after intraurethral DXP application for 8 and 15 days (table 1). There was also significant up‐regulation of VEGF, down‐regulation of IL‐6, TGF‐ß1, ß‐catenin and collagen I & III expression and decrease in collagen I/III ratio, after 4, 8 and 15 days of intraurethral DXP administration (Table 2). DXP group showed significant reduction in MDA and NO activity on days 4, 8 and 15 (Table 1). Apart from histopathology and collagen I/III ratio, intraurethral application of DXP up to 15 days significantly provided more beneficial effects.
Conclusions: Administration of intraurethral DXP might minimize urethral fibrosis and scarring post urethroplasty.
Post‐operative outcomes in heavy weight versus lighter weight wide pore polypropylene mesh for robotic sacrocolpopexy: 10 year retrospective analysis of 351 cases
C Schuster, MS Carey, RI Carey
Florida State University College of Medicine
Introduction & Objective: All FDA approved wide pore polypropylene Y‐mesh grafts available for robotic sacrocolpopexy have variance in the mesh weight, pore size, thickness, surface area ratio and suture pull out strengths. In this study we evaluated results observed for robotic sacrocolpopexy performed with four separate wide pore polypropylene Y meshes that differ markedly in their physical properties.
Methods: Data is collected from an IRB approved prospectively maintained retrospective database of robotic sacrocolpopexy cases performed at an 836 bed tertiary care hospital by a single surgeon. Using analysis matched for covariates of BMI, POP‐Q stage, surgeon, and previous attempts at repair, we evaluated whether the weight of the Y‐mesh influenced the anatomic outcome and rate of de novo SUI at two year follow‐up.
Results: Between 2011 and 2020, a total of 351 patients underwent robotic sacrocolpopexy for POP‐Q Stage IV VVP. The cases were divided between 4 different Mesh materials (n = 50, 50, 100, and 151) in patients undergoing repair. The mesh material varied from the heaviest mesh weight (52 g/m2, 527 microns thick, and a suture pull out strength of 18.3 N) to the lightest weight mesh ( 25 g/m2, 200 microns thick, and suture pull out strength of 23.3 N). At mean 46 month follow‐up, anatomic success for apical prolapse was 100% and there was no difference in the rates of Grade 2 or less anterior or posterior prolase in each group (4%). De novo SUI was found in 5 patients (10%) in the heavy mesh group and 4 patients (8%) in the lighter mesh group. All de novo SUI patients did not have a mid urethral sling, MUS, placed at the time of the procedure. There was one mesh erosion in the light weight mesh group in a salvage patient that underwent concomitant pre‐existing mesh removal at the time of surgery.
Conclusions: Although the two Y‐meshes are markedly different in their weight, surface area, thickness and suture pullout strength, there was no observed significant difference in the anatomic success of repair, the rate of de novo stress urinary incontinence or mesh erosion. The rates of de novo SUI seen in this study, have led us to perform a MUS procedure at the time of sacrocolpopexy for all Grade IV prolapse patients
Uterus preservation in women who undergo robotic sacrocolpopexy for complete vaginal vault eversion: ten year retrospective analysis
C Schuster, MS Carey, RI Carey
Florida State University College of Medicine
Introduction & Objective: Robotic sacrocolpopexy with uterus preservation (RASCP‐UP) is a transabdominal approach to repair of pelvic organ prolapse (POP) that avoids placement of transvaginal mesh and preserves female sexual organs. Although hysterectomy may be performed at the time of POP repair, many women choose to preserve their uterus for reasons of sexuality, female identity, religion, maintenance of maximal vaginal length, and resistance to removal of a normal organ.
Methods: Data is collected from an IRB approved prospectively maintained database of robotic POP repair in an 836 bed tertiary care hospital. The surgery is performed with a da Vinci Si or Xi system with 4 robotic ports and 1 assistant port. Commercially available 4 x 24 cm Y‐shaped wide pore polypropylene mesh is modified to accommodate >10 cm anterior and posterior dissections of the vaginal walls. The anterior vaginal wall component is brought through the broad ligament and joined with the posteriorly placed component for attachment to the Anterior Longitudinal Ligament with GoreTex sutures. The mesh is then completely covered by peritoneum. . All patients for RASCP‐UP had Stage 4 prolapse with maximal anterior, posterior and apical descent with the cervix at the apex of the descent. All patients had normal PAP smears and pelvic ultrasounds.
Results: Between 2010 and 2021 a total of 351 patients underwent RASCP at the same institution. Of these, 51 presented with complete vaginal vault eversion requesting RASCP‐UP. Mean age was 66.7 years and mean BMI 27.4. Cases were completed with robotic console time between 61 and 121 minutes and all patients discharged within 24‐48 hours. At mean 60 month (12 – 124 month) follow‐up, there were no mesh erosions, hernias, or reoperations for prolapse. There was one reoperation for hysterectomy at 6 year follow up for suspected endometrial carcinoma and one reoperation for small bowel obstruction in a patient with extensive lysis of adhesions. Mid‐urethral slings were placed at the time of sacrocolpopexy to prevent de novo stress incontinence.
Conclusions: RASCP‐UP is feasible for patients with severe POP who desire uterus preservation. The surgery restores normal vaginal axis and length without placement of mesh material through vaginal mucosa. Long‐term results show durable functional repair. Is the “unnecessary” removal of an otherwise normal uterus “necessary” for repair of POP? For a number of female patients, the answer appears to be no.
Short‐Term Effect of Local and Systemic Adipose Tissue‐Derived Stem Cells on Stress Urinary Incontinence in Rats
A Elsharabasy, AH Elkashef, N Barakat, S Khater, A Awadalla, A Hussein, M Gomaa, M Abdel‐Maboud, A Shokeir
Department of Urology, Urology and Nephrology Center, Mansoura University, Egypt
Introduction & Objective: Stress urinary incontinence (SUI) is a major health problem that has many social and economic impacts, so we evaluated the short‐term effect of locally and systemically administrated adipose tissue‐derived mesenchymal stem cells (ADMSCs) on the treatment of SUI‐induced in a rat model.
Methods: Thirty‐two female Sprague‐Dawley rats were randomly allocated into 4 groups (8 rats each); control, SUI, local ADMSCs and systemic ADMSCs groups. SUI was induced by vaginal dilatation of the rats via inflating the balloon of a urethral catheter with 5 mL sterile saline in the vagina for 8 hours. Rats then received 0.9% saline, local ADMSCs treatment (periurethal injection at 5 and 7 o'clock positions of the vesico‐urethral junction) and systemic ADMSCs treatment (injection in the tail vein) in SUI, local and systemic ADMSCs groups, respectively for 2 weeks. Urodynamic study in terms of abdominal leak point pressure (ALPP), threshold pressure (TP) and bladder capacity (BC) was performed. Rats were then sacrificed and their periurethral regions were sent for routine histopathological examination.
Results: There was significant improvement in the results of urodynamic study in terms of ALPP, TP and BC after administration of either local or systemic ADMSCs for 2 weeks relative to SUI group (Figure 1). There was also significant evidence of regeneration of the muscle layers in the periurethral regions with less inflammation and fibrosis in local and systemic ADMSCs groups compared to SUI group (Figure 2). Apart from BC, the locally administrated ADMSCs significantly provided more favorable effects than the systemically administrated ADMSCs.
Conclusions: Short‐term administration of ADMSCs either locally or systemically in the periurethral regions in SUI improves the morphological and urodynamic dysfunctions of the urethral sphincters.
Recovery after surgical treatment for urolithiasis
A Kleijweg, R Kingma, J Stiksma, S Roemeling
Introduction & Objective: In order to better inform patients and colleagues about the convalescence that can be expected after treatment for urolithiasis, questionnaires were sent to patients after retrograde ureterorenoscopy with stone treatment (URS) and percutaneous nephrolithotomy (PCNL).
Methods: From July to December 2020, adult patients who underwent URS or PCNL in either an academic center for complex stone treatments or in a nearby regional hospital were asked to complete a questionnaire. The authors composed a questionnaire with 62 questions about recovery which was sent to the patients two weeks after the procedure. If patients had not fully recovered after two weeks, they were called 3 weeks later for additional information about their recovery. Main outcome parameters were the number of days until complete absence of complaints postoperatively and the duration until complete resumption of work.
Results: Fifty out of 67 invited patients completed the questionnaire (i.e. response rate 75%). Of these 50 patients, 29 underwent URS and 21 PCNL. The mean age was 59.7 years (SD 12.7). The mean time to full recovery (absence of all complaints) was 20 days; namely 20.3 days (SD15.9) after URS and 19.5 days (SD 11.5) after PCNL. Fatigue was the most frequently reported complaint after two weeks (50% of responders), 41% after URS and 62% after PCNL. The mean duration of postoperative pain was 5.4 days; 4.3 days after URS and 6.8 days after PCNL. In people in paid employment (n = 22), the mean time for full return to work was 9.3 days; 8.4 days after URS and10.2 days after PCNL.
Conclusions: The mean time to complete recovery after treatment for urolithiasis was 20 days. Despite the fact that PCNL is a more invasive procedure, the difference in time to complete recovery compared with URS is limited. However, the duration of post‐operative pain, fatigue and absence from work was longer after PCNL compared to URS.
Robotic‐Assisted Laparoscopic Cystectomy with Ileal Urinary Diversion comparing Bricker vs. Wallace Ureteroileal Anastomoses: A Single Institution Study
R Sawhney, M Billah, R Harrison, J Zaifman, MD Stifelman, G Lovallo, M Ahmed
Hackensack Meridian Hackensack University Medical Center
Introduction & Objective: In patients undergoing robotic cystectomy with ileal urinary diversion and ureteroileal anastomosis (UA), the two frequently used approaches to UA are the Bricker and Wallace techniques. The Bricker is an end to side refluxing UA. The Wallace involves suturing the ureters together and placing the combined ureter at the end of the bowel anastomosis. The Wallace has lower reported stricture rates but there is a concern that problems with one ureter could affect the other. We switched from Bricker to Wallace at our institution in 2019 to minimize stricture rates. Our objective is to evaluate differences between the Wallace and Bricker techniques in patients undergoing robotic cystectomy.
Methods: We performed non‐parametric tests such as Chi‐Square, Mann‐Whitney U and Fisher Exact tests in SPSS to evaluate for differences between the two groups.
Results: In this cohort study, we queried patients undergoing robotic radical cystectomies with ileal urinary diversion from May 2016 to December 2020 and identified 118 patients with 38 undergoing the Wallace and 70 undergoing the Bricker. No differences were noted in demographics or intra‐operative characteristics, and final pathology (Table 1) between the two groups. There were also no differences in recurrence, location of recurrence, and the 3‐, 6‐, and 12‐month rates of hydronephrosis and need for intervention (Table 2) between the two groups.
Conclusions: The Bricker and Wallace techniques for UA is are used variably across institutions. The Bricker is cited for its simplicity but higher stricture rates. Whereas the Wallace historically was used for dilated ureters and leads to easier endoscopic surveillance. In our experience with robotic cystectomies, both techniques have similar outcomes regardless of ureter dilation at our institution. This finding may be due to utilization of ICG and the robot for UA. We recommend surgeon preference when deciding anastomotic technique.
24 Hour Observation through Stone Observation Pathway Predicts Success of Medical Expulsive Therapy
MC Wasserman, S Marthi, D Sobel, E Godbout, C Tucci, G Pareek
Warren Alpert Medical School of Brown University
Introduction & Objective: The incidence of ureterolithiasis continues to increase and emergency department management of acute renal colic is critical to patient outcomes. As most ureteral stones pass with outpatient medical expulsive therapy (MET), treating pain and associated symptoms for safe discharge is paramount. We developed a novel stone observation pathway (SOP) within our Clinical Decision Unit (CDU) for patients with acute renal colic to have 24 hours of observation to achieve discharge on MET without hospital admission or urologic consultation. This study evaluates the safety and efficacy of this SOP.
Methods: A retrospective review of patients admitted to the CDU using the SOP from January 2016 to November 2019 was performed. Patients were excluded from CDU admission if any criteria from Table 1 were met.
Results: 189 patients with uncomplicated ureterolithiasis were admitted via the SOP to the CDU (Table 2). Mean stone size was 4.6mm (SD +/‐ 1.9mm). 148 (78%) patients were discharged within the observation period and 42 (22%) were admitted for operative intervention. 17 of the discharged patients (9%) returned to the emergency department for recurrent renal colic, of which 8 (53%) required operative intervention. 85 of the discharged patients (57%) followed up with a urologist, of which 30 (22%) required operative intervention.
Conclusions: 24‐hour observation before discharge from a CDU predicts success of outpatient MET. The protocol is effective (< 10% readmission rate), safe (0% readmission for urinary tract infection/pyelonephritis) and reduces unnecessary resource utilization. Future research will evaluate the cost effectiveness and target low follow‐up rate after discharge for quality improvement.
Video Session
Video Session 05: Miscellaneous
V05: Miscellaneous
R Venkatesh, R Manickam
When Hydronephrosis turn out to be a Parapelvic cyst
Y Xu, X Zhan, H Zhang, G Wang, A Kadier, P Wu, H Liu, D Liu, Y Dong, X Xu, H Zhou, Y Gao, T Xie
Introduction & Objective: To explore the surgical strategy of kidney stone accompanied with parapelvic cyst.
Methods: Patient information: Male 69 years old, presented to our hospital with right flank pain for 5 days. Physical examination showed right renal percussive pain and slight tenderness along the right ureter walking zone. Further ultrasound and CT scan showed typical image features of kidney stone (right UPJ) with hydronephrosis, so we performed percutaneous nephrolithotomy. During operation, the hydronephrosis turned out to be a parapelvic cyst, which caused trouble finding the right way to the renal pelvis. Therefore, we developed a surgical strategy using methylene blue to mark the junction wall of the cyst. As we retrogradely pumped in methylene blue solution through the ureteral stent, the junction wall between the cyst and pelvis became raised and blue, which gave us a “green light” for further operation.
Results: We successfully entered renal pelvis by cutting through the methylene blue‐marked wall, subsequent lithotripsy was carried out smoothly. Moreover, due to the drainage function of ureteral stent, the parapelvic cyst was treated as well, postoperative ultrasound showed obvious retraction of collecting system.
Conclusions: Retrogradely injection of methylene blue is an effective surgical strategy mark the thinnest junction wall between the pelvis and the cyst. Kidney stone and parapelvic cyst can be treated simultaneously.
Transurethral Repair of a Vesicovaginal Fistula, A New Endoscopic Approach
C Martinez‐Arroyo, J Morales‐Montor, C Pacheco‐Gahbler, FM Santa Maria Orozco, G Fernandez Noyola, M Cantellano Orozco
Introduction & Objective: Vesicovaginal fistulas (VVF) are the most commonly acquired fistulas of the urinary tract, but we lack a standardized algorithm for their management. Surgery is the most commonly preferred approach to treat women with primary gynaecologic or urological surgery. All fistula surgeries should be conducted under the basic principle that the fistula and scar will be completely excised. The success rate of treatment of a simple VVF is reported to be 75% to 97%. Most surgeries are performed with an open approach. We describe a transurethral repair of a vesicovaginal fistula using a nephroscope and mini‐laparoscopic surgery equipment
Methods: his is the case of a 58 yo female with past medical history of total hysterectomy, 3 cesarean sections and a pneumatic cystolithotripsy due to a bladder calculi. She developed urine leaking from the vagina that began 3 months after cystolithotripsy. This leakage was continuous and related to activities that increased intra‐abdominal pressure. Her quality of life was affected using 3 pads per day. During speculoscopy we identified an orifice in the anterior wall of the vagina near the scar of the previous gynecologic surgery that continuously leaked urine. We completed the study protocol and diagnosed a retro‐trigonal VVF after performing a cystography and cystoscopy. Our surgical repair consisted in a transurethral approach using a 24 Fr nephroscope. First, we used Amplatz dilatators in the urethra and introduced a 26 Fr renal access sheath to the bladder. After that, we worked with the nephroscope and a Collins loop to resect the fistula and we closed the defect with mini‐laparoscopic surgery equipment (needle driver and scissors).
Results: Bladder catheter was removed 3 weeks after surgery, with a postoperative cystography that showed no evidence of urine leakage. In the 2nd month follow‐up, the patient reported complete absence of urinary symptoms.
Conclusions: VVF can be repaired with this new approach safety and with good results. We need to reproduce this technique and if postoperative results are similar, this could be a new standard of minimally invasion surgery for these patients.
C‐V GreenLight Laser Technique May Prevent Uncontrollable Bleeding During Management of Benign Prostate Enlargement
J Feghali
Introduction & Objective: Since the introduction of GreenLight laser in 1997; many studies has shown that it has comparable results to transurethral resection of the prostate in treating benign prostatic hyperplasia with fewer complications and side effects especially bleeding; but one of its disadvantage is the difficulty to proceed once there is an uncontrollable active bleeding
Objective: Evaluate a new technique that we call C‐V (Coagulation then Vaporization) GreenLight Laser Treatment (GLLT) defined as treating the prostatic mucosa with coagulation mode followed by vaporization of the prostatic tissue in order to reduce the risk of uncontrollable bleeding during surgery
Methods: From january 2019 to january 2021; eight men with mean age of 72.3 years had benign prostate enlargement (mean prostate volume: 82.5 cc) were treated with C‐V GLLT by single surgeon. Half of the patients had chronic urinary retention. After spinal anesthesia, patients were placed in the standard dorsal lithotomy position, continuous‐flow laser cystoscope 23 French (Fr) was inserted into urethra and slowly advanced into the bladder with normal saline (NS) 0.9% as irrigation fluid; after visualization of the ureteral orifices we inserted the MoXy Fiber for the GreenLight XPS. Under coagulation mode and energy 40 W we started the coagulation of the prostatic mucosa from the bladder neck to the pre‐verumontanum area; followed by vaporization of the prostatic tissue under vaporization mode and energy up to 180 W; once a large urethral channel was created, we stopped the irrigation fluid to check for any passive bleeding. At the end of procedure a three way 20 Fr foley catheter was inserted over a stiff hydrophilic 0.035 inch guide wire to prevent any traumatic foley insertion and to provide NS irrigation in case of postoperative bleeding
Results: Mean C‐V GLLT operative time was 69 minutes; no active or passive bleeding was encountered during surgery; NS irrigation was not needed post treatment; none of the patients had blood transfusion; mean drop of hemoglobin was 0.5 g/dl after C‐V GLLT. No minor or major postoperative complications; all patients voided normally after 24 hours; 1 month post‐treatment mean International Prostate Symptom Score (IPSS) was 8, Quality of Life (QoL) 1.1, and Post Void Residue (PVR):11cc
Conclusions: C‐V Green Light Laser Technique may prevent uncontrollable bleeding during treatment of large inflamed and non inflamed benign hypertrophic prostate
Antegrade endourological treatment for ureteral stones and ureteroenteric strictures after ileal conduit urinary diversion with Wallace I ureteroileal anastomosis
F Natal Alvarez, L Cuellar Martin, S Martin Martin, J Torrecilla Garcia‐Ripoll, M Bedate Nuñez, A Alonso Villalba, C Conde Redondo, A Ruano Mayo, A Zamora Horcajada, A Herranz Arriero, JM Diaz Romero, J Soto Rodriguez, F Lara Perez, C Marfil Peña, J Calleja Escudero
Introduction & Objective: The incidence of lithiasis and ureteroenteric strictures after ileal conduit urinary diversion are respectively 1‐11% and 1.7‐29%. Our aim is to present the resolution of both complications by using an endourological approach, in a patient who underwent radical cystectomy and ileal conduit urinary diversion with Wallace I ureteroileal anastomosis.
Methods: We present a 76‐year‐old male, referred to our center, who had underwent radical cystectomy and ileal conduit urinary diversion with Wallace I ureteroileal anastomosis in 2013. A right percutaneous nephrostomy was inserted in the previous months to treat sepsis secondary to urinary obstruction due to a 9 mm stone located in mid ureter, diagnosed by non‐contrast enhanced computerized tomography (NCCT). Levels of serum creatinine before surgery: 1.9 mg/dl. Antegrade flexible ureterorenoscopy was performed after placement of a 10‐12 French (Fr) ureteral access sheath through the previous nephrostomy. Holmium laser lithotripsy was performed, all the fragments were removed with a basket. Several unsuccessful attempts were made to place a Sensor® guidewire into the urinary diversion, but minimum contrast passing was seen. Finally, a Terumo® guidewire and a 4 Fr ureteral stent allowed access to the urinary diversion. The previous guidewire was replaced with an Amplatz® guidewire. Pneumatic dilatation of the ureteral stricture was carried out (high‐pressure balloon). An M‐Drain® 8 Fr catheter was passed in an antegrade way to the ileal conduit at the end of the procedure.
Results: In the early postoperatory period the patient developed fever, left renal colic pain and acute kidney failure. Compression of the contralateral ureter by the M‐drain® was suspected, leading to the withdrawal of the catheter by the 5th postoperative day after having checked its permeability and the absence of ureteral leakage. The previous signs and symptoms quickly disappeared. Neither residual stone fragments nor hydronephrosis were found at his 3‐months NCCT assessment. Current serum creatinine levels: 1.87 mg/dl.
Conclusions: Antegrade flexible ureterorenoscopy might be the most effective treatment for stones and ureteric strictures in these patients. Endoscopic pneumatic balloon dilation could be a non‐invasive solution for the treatment of ureteric strictures in these cases. Ureteral stents must be used carefully in Wallace I ureteroileal anastomosis, as they can induce contralateral ureter compression.
Zero‐exposure retrograde intrarenal surgery for ureteral stones
T Tsujioka, K Hirota, Y Atagi, K Seto, K Izumi, M Yamanaka, Y Kawanishi
Introduction & Objective:
• Fluoroscopy is still conventionally used for retrograde intrarenal surgery (RIRS). Fluoroscopy exposes patients and medical staff to the health hazard of radiation. On the other hand, ultrasound guidance techniques have increased precision and are not invasive. Therefore, we considered that zero‐exposure retrograde intrarenal surgery (RIRS) could be performed for all types of patients by using ultrasound guidance. The aim of this study is to determine the safety and effectiveness of zero‐exposure RIRS for treating ureteral stones compared with renal stones.
Methods: This study includes all patients (n = 205) who underwent zero‐exposure RIRS for either ureteral stones (n = 133, U) or renal stones (n = 72, R) at our institution between April 2018 and December 2019. Operative time , rates of zero exposure, stone‐free rates, and perioperative complications were compared between the ureteral stone and renal stone groups. Ultrasound guidance was used to place guidewires, insert ureteral access sheaths into the ureteral orifice, appropriately position sheaths in the ureter, measure the size of stones, identify residual stone fragments, and place ureteral stents. All ultrasound guidance was performed by an ultrasonography technician.
Results: We completed zero‐exposure RIRS for ureteral stones in 201 cases, 98.0% ( U:130 97.7% vs. R:71 98.6% ). The mean operative time was 90.6 ± 41.3 min. ( U:79.3 ± 37.5 vs. R:107.3 ± 37.0 ). Stone‐free rate was 83.1% ( U:96.2 vs. R:58.3 ). Complications developed in eighteen patients, 8.9%( U:8 vs. R:10) and comprised of febrile urinary tract infection (n = 8, U:3 vs. R:5), ureteral mucosal injury (n = 8, U:4 vs. R:4), ureteral perforation (n = 1, U:1 vs. R:0), and inability to position a ureteral stent (n = 1, U:0 vs. R:1).
Conclusions: Zero‐exposure RIRS for ureteral stones can be performed easily and safely. In addition, it has several advantages, which include confirmation of the proximal ureter in patients with impacted stones, and recognition of X‐ray negative stones. Zero‐exposure RIRS is safe, effective, and useful for treating both ureteral and renal stones.
Robotic Assisted Ureteroscopy: Combined Approach to Treating Difficult Ureteral Strictures and Stone Disease
DT Lybbert, BF Schwartz, MF Monn
Introduction & Objective: Robotic assisted laparoscopic ureteroplasty with buccal mucosa grafting is a relatively new procedure being performed in limited locations in the United States. Although this has provided an opportunity for many with complex ureteral stricture disease to receive treatment, patients with complex ureteral stricture disease who live far from tertiary medical centers have additional challenges in getting appropriate care. In this video we demonstrate our approach to treating complex ureteral strictures and significant renal and ureteral stone burden by way of robotic assisted ureteroplasty combined with ureteroscopy in order to minimize hospitalization, recovery time, health care costs, and patient burden
Methods: This is a case report of a 74 year old male who was found to have a significant mid‐ureteral stricture and large stone burden. We use radiographic imaging and footage from the surgery to present his case and demonstrate the utility of combined surgical approaches to treat multiple medical problems simultaneously.
Results: Our patient, after diagnosis, was able to undergo a combined procedure to treat his stricture and significant stone burden with success. His stones were removed at the same time his stricture was repaired by way of robotic assisted laparoscopic ureteroplasty with buccal graft onlay. Follow up ureteroscopy demonstrated patency of the repaired ureter and the patient reported complete resolution of his symptoms.
Conclusions: Advances in medical and surgical treatment have provided the possibility of treating and curing many diseases and disorders. Unfortunately, many in rural settings have limited access to these treatments and procedures. By combining procedures to treat multiple medical problems, we can ease the burden put on patients far from larger medical centers where the most up to date and advanced treatments and procedures are available.
Antegrade assisted bladder neck incision for complete bladder neck stenosis
C Van Haute, T Tailly
University Hospitals Leuven
Introduction & Objective: This video will present the endoscopic management of a complete bladder neck stricture in a kidney transplant recipient (KTR).
Methods: A 50‐year‐old male patient with a medical history of TURP developed end‐stage renal failure without residual diuresis. During kidney transplantation, a complete bladder neck stricture was identified and subsequently a percutaneous bladder drain had to be inserted via cystotomy. Patient and transplant kidney recovered well after kidney transplantation. Two months after kidney transplant, we decided to proceed to a minimal invasive approach to treat the bladder neck stenosis and to move on to an antegrade assisted incision of the bladder neck. Via a combined ante‐and retrograde approach the bladder neck was identified and incised using laser energy and plasma vaporization. The video shows an exceptional endoscopic view on the bladder neck during plasma vaporization.
Results: Postoperatively, there were no complications. Patient remained continent. At 9 months follow‐up, a cystoscopy showed a wide and open bladder neck. At 24 months patient is doing well with a max flow rate of 23 ml/s.
Conclusions: This video illustrates in a fascinating way how bladder neck vaporization looks like from an antegrade point of view.
Pelvic Lipomatosis ‐ Quintessence of Rarity with Stupendous Denouement
S Jayaprakash, M Thangarasu, N Jain
Apollo Main Hospitals, Chennai, Tamil Nadu, India
Introduction & Objective: Pelvic lipomatosis is a rare condition characterized by diffuse pelvic overgrowth of non‐malignant but infiltrative adipose tissue in perivesical and perirectal space. It was first reported by Engels in 1959 in 5 patients. However, Fogg and Smith first coined the term in 1968. The incidence is 06‐1.7/100,000 hospital admissions. So far only less than 150 cases are reported worldwide. Mean age of presentation is 48 years with strong male predominance (M: F – 1.8:1). It is more common in African Americans than the Caucasians (67% vs 33% respectively). It presents with broad range of symptoms caused by compression of pelvic structures.
Methods: We have treated 4 patients between 2016 & 2019. All presented with flank pain was identified to have bilateral hydroureteronephrosis secondary to distal ureteric compression. Three cases were imaging diagnosed and one case was an intraoperative surprise. All our patients underwent Robotic Assisted Bladder Fat Extirpation with Bilateral Ureteric Reimplantation. We descibe two such cases and our technique with tips and tricks in the video.
Results: All our patients underwent Robotic Assisted Bladder Fat Extirpation with Bilateral Ureteric Reimplantation successfully. Postoperative period was uneventful. Drain was removed on POD 5‐6 and foley on POD 10. All our patients are on regular follow up with USG KUB initially at 3 months and thereafter annually.
Conclusions: Pelvic lipomatosis causing B/L HUN has good surgical outcome. Imaging cannot always reliably detect this condition. We have had good success and outcome with this technique. However, patients require long term follow up although no guidelines are available on this. The choice of surgical technique purely depends upon the surgeon's comfort.
Transurethral incision with transverse mucosal realignment: an endoscopic repair of bladder neck contractures and vesicourethral anastomotic stenosis
JN Warner
Introduction & Objective: In an effort to improve outcomes for patients with vesicourethal anastomotic stenosis (VUAS) and bladder neck contractures (BNC), a novel surgical technique is investigated. This study tests the hypothesis that endoscopically employing a laparoscopic suturing device can successfully reapproximate the mucosa in a transverse fashion after a longitudinal incision of a VUAS or BNC.
Methods: Patients with VUAS and BNC were treated with a novel technique, transurethral incision with transverse mucosal reapproximation (TUI TMR) from July 2019 to December 2020. The cause of stricture, radiation history, and number of prior treatments were reviewed. Foley was left in place for one week post op. Cystoscopy assessed patency 4 months post‐op. Failure was defined as recurrence of stricture. Stone formation on the titanium clip was also assessed.
Technique
A needle tip electrode (Olympus Surgical) was introduced. Incisions were made at 3 and 9 o'clock. The outer sheath of the resectoscope was left in place. A 5mm RD‐180® (LSI solutions, Rochester, NY) suture device and a short rigid ureteroscope were simultaneously passed into the sheath. Using a 2‐0 absorbable suture, the mucosa was grasped at the mid point of the proximal edge and then the midpoint of the distal edge of the incision. The instruments were removed and the titanium TK Ti‐Knot suture device® (LSI solutions) reapproximated the mucosa in a Heineke‐Mikulicz fashion.
Results: 20 patients have undergone TUITMR with at least 4 months follow up (median 13, range 4‐21). 18/20 were successful after one treatment, and 2 patients underwent successful second operation. At last follow up all patients were patent. 11 patients had VUAS, and 9 had BNC. 6 had radiation, and all were successful after one treatment. 15/20 had prior incisions. 4 clips required removal. One was removed in the operating room, the others were removed in office at 4 months.
Conclusions: Early outcomes of TUI TMR of posterior urethral stenosis and anterior urethral strictures seem promising, even in refractory and radiation cases. Further follow up will be needed, and imaging modalities will need to be improved for wide spread adoption.
Robot‐Assisted Laparoscopic Repair of A Huge Sliding Inguinal Hernia of The Urinary Bladder, Left ureter And Sigmoid Colon
AA Elbakry, C Crigger, T Trump, MW Salkini
Introduction & Objective: We are presenting a challenging case of huge sliding inguinal hernia with herniated bladder, left ureter and sigmoid colon. We are presenting robotic approach as an alternative for classic open approach.
Methods: Our patient is an 82‐year‐old male who presented with an enlarged scrotum with dull pain that was worsened with ambulation. Additionally, he complained of lower urinary tract symptoms, specifically prolonged voiding and urinary hesitancy. Work up, including cross sectional imaging revealed a large left inguino‐scrotal herniation of the bladder, along with the left ureter and sigmoid colon. Our patient desired restoration of his anatomy and for normal function and so a joint decision was made to proceed with hernia repair with possible left orchiectomy via a robotic approach. Patient was positioned in low dorsal lithotomy and moderate Trendelenburg position. We utilized 4 robotic 8 mm ports and a 5/15mm assistant port placed contralaterally on the right side. We began by incising the peritoneum along the borders of the hernia. This was continued circumferentially until the hernia contents were freely mobile. Due to the distance of the distal aspect of the hernia contents and sac, manual pressure was applied to the scrotum externally by our bedside assistant. With dissection revealed an atrophic left testicle, we proceeded with left simple orchiectomy to decrease the likelihood of recurrent hernia after our repair. Next, we focused our attention on closure of the hernia defect. For this we utilized a Bard Composix® 4 x 6 inches polypropylene and ePTFE mesh secured with 3‐0 V‐loc Prolene suture. We ran this suture circumferentially after clearing the edges of the fasci for strong incorporation. Finally, insufflation pressure was dropped to 5 mmHg and hemostasis was confirmed.
Results: Our operation proved successful with a total operative time was 3 hours and 50 minutes, and estimated blood loss of 30 cc. He was admitted overnight for postoperative monitoring and tolerated a regular diet beginning the morning of postoperative day 1. He regained bowel function on postoperative day 2 and was subsequently discharged on postoperative day 6 due to social situation and placement with an uncomplicated hospital course.
Conclusions: Robotic approach for management of huge challenging inguinal hernia with herniated multiple abdominal organs including bladder, ureter and sigmoid colon, is feasible and safe approach. It provides enhanced visualization and minimal blood loss and decreases the morbidity of the procedure.
Technique and Outcomes of Endoscopic Management for Postoperative Bladder Neck Contractures following Robot‐Assisted Radical Prostatectomy Using Injectable Human Amniotic Membrane and Umbilical Cord Bioregenerative Matrix
F Sheckley, N Velazquez, R Munver
Introduction & Objective: Management of bladder neck contractures (BNC) following failed prior incision or resection has been primarily limited to injectable therapeutic agents including mitomycin and steroids. While the results have not been consistent, only steroid injection has shown a modest effect in prolonging BNC recurrence. We present an endoscopic technique for the management of recalcitrant BNCs, in men that previously failed prior therapies, using a novel amniotic membrane and umbilical cord injectable bioregenerative matrix agent, that acts by reducing inflammation and scar tissue, while promoting healing.
Methods: A total of 4 men with prostate cancer, median age of 61 years (range: 57‐67), underwent robot‐assisted radical prostatectomy and subsequently developed a BNC following salvage external beam radiation therapy (n = 3), or an anastomotic urine leak (n = 1). All patients were initially managed with direct vision internal urethrotomy (DVIU) or transurethral resection of the bladder neck (TURBN), with steroid injection therapy. All patients developed symptomatic BNC recurrence. One patient had 2 previous TURBNs and 3 patients had 1 previous DVIU or TURBN. All patients subsequently underwent TURBN with circumferential submucosal injection of 100 mg of an amniotic membrane and umbilical cord bioregenerative matrix that was reconstituted in 5 mL normal saline. Postoperative urethral catheters were removed in 1 week.
Results: At 12‐month follow‐up, all patients continued to void with a strong stream and without retention of urine. Office cystoscopy demonstrated an open bladder neck that accommodated a 16F flexible cystoscope, and no patients developed BNC recurrence. At longest follow‐up of 17 months, the patient was asymptomatic and remained without bladder neck contracture recurrence. In addition, all patients were continent of urine.
Conclusions: The use of an injectable amniotic membrane and umbilical cord bioregenerative matrix agent adds to the armamentarium of therapeutic agents for the management of recurrent bladder neck contractures. The endoscopic technique using this novel injectable matrix is reproducible and is associated with favorable outcomes at 12‐month follow‐up as compared to previously used injectable agents.
An Initial Experience with the Real‐Time Detection of Kidney Stone Composition Using Artificial Intelligence and Smartphone Technology
A Peta, A Brevik, M Ayad, P Jiang, RM Patel, RV Clayman, J Landman
Introduction & Objective: Kidney stone composition is becoming increasingly important in treatment algorithms as the composition/hardness of stones determines treatment success. Artificial intelligence (AI) and machine learning (ML) have previously been employed to identify kidney stone composition from static endoscopic images. In this study, we used AI and ML in a smartphone application to determine stone composition in ex‐vivo porcine kidneys in real time during ureteroscopy.
Methods: Two hundred human kidney stones of four unique compositions: 50 calcium oxalate monohydrate predominant (>50%) (CaOx), 50 cystine, 50 uric acid (UA) and 50 mixed struvite (calcium phosphate, carbonate apatite) were visualized in both an ex vivo porcine model and a saline basin model using a Dornier Axis: Single‐Use Ureteroscope. Images of each stone were captured and transferred to an AI software that produced a ML model for use as an iPhone app (i.e. “Rockognition”). The application was then utilized to identify stone compositions of 16 unique stones in real‐time during ureteroscopy in both the ex vivo porcine and saline models. Three fellowship trained endourologists (PJ, RMP, JL) were similarly “trained” using the same 200 stones; afterwards they were asked to identify the composition of the same 16 “test” stones as the AI/ML program in the ex‐vivo porcine model.
Results: The iPhone developed stone composition identification application, when coupled to a Karl Storz ureteroscopic video feed in real time was able to correctly identify the stone composition of 15 (94%) of the 16 stones in the saline model, with only a cystine stone being mischaracterized as UA. In the ex‐vivo porcine model, the app was able to correctly identify 14 (85.5%) stones, with only two UA stones being mischaracterized as CaOx. The model was able to correctly identify all CaOx and struvite stones. In contrast, endourologists were only able to successfully identify the stone composition in 58% of cases in the ex‐vivo porcine kidney model (p = 0.03).
Conclusions: After training, an artificial intelligence/machine learning program built into a smartphone application was able to accurately identify kidney stone composition in an ex‐vivo ureteroscopic porcine model. The visual app performed better than fellowship‐trained endourologists.
Video Session 06: Transurethral Surgery and Ureteroscopy
V06: Transurethral Surgery and Ureteroscopy
JD Desai, M Borofsky
Laser Abalation of Urothelial Tumor of Upper Ureter
G Saber, E Lucas Filho, L Zaccaro
Introduction & Objective: Accounting for only 5% of all renal and urothelial tumours, upper tract urothelial carcinoma (UTUC) is a rare genitourinary malignancy. Although management guidelines for UTUC recommend radical nephroureterectomy (RNU) with resection of a bladder cuff as the ‘gold standard’ treatment, the solitary kidney status after this procedure may lead to higher rates of dialysis, cardiovascular morbidity, and overall mortality. In an effort to mitigate these attendant risks, ureteroscopy (URS) and laser photoablation represent a valid treatment option for these patients with high comorbidities and/or low‐risk disease and willing to undergo an intensive surveillance program.
Minimally‐invasive endoscopic management of UTUC was first suggested for imperative cases as chronic kidney disease, solitary kidney, bilateral UTUC, and the good results obtained in terms of cancer control lead clinicians to offer this approach also to elective cases (patients with normal contralateral kidney).
The endoscopic treatment of upper tract TCC coincided with the development and refinement of percutaneous renal surgery, ureteroscopy, and laparoscopy. These techniques can now be combined to provide histologic diagnosis of filling defects of the upper urinary tract, remove small to even large intraluminal lesions, or remove the distal ureter or the entire kidney and ureter with endoscopes alone.
Methods: We present the case of an 85‐year‐old male with asymptomatic gross hematuria for 1 month. The patient, despite advanced age, presented good performance status, and as comorbidities, presented cardiomyopathy, previous stroke (one year) and using Xarelto, AAS, simvastatin and digoxin.
In the requested imaging tests, with better accuracy, the MRI revealed a lesion in the upper right ureter of a superficial and non‐invasive character.
Results: Proceed to ureteroscopy that then revealed a typical urothelial, pedunculated lesion of approx. 1 cm, and was then chosen by endoscopic resection with YAG‐Holmium laser, and extraction of the specimen with Dormia's basket.
The surgery was performed without any complications, with a total time of 30 minutes and the patient was discharged on the first postoperative day, with a double‐j stent, and asymptomatic.
Conclusions: Laser Ablation of Ureteral Tumors are feasable with good outcomes in selected patients.
Endoscopic Incisional Uses of Thulium Fiber Laser in Upper Urinary Tract Strictures
AS Sadiq, JA Khusid, WM Atallah, M Gupta
Introduction & Objective: Endoscopic laser incision of upper tract strictures is a minimally invasive option usually utilizing the Holmium:YAG laser. The thulium fiber laser (TFL) has an effective ablation and coagulation profile that has been successfully applied for prostate enucleation and en bloc bladder tumor excision, and may make it a new option for laser incision of strictures. We review our experience and outcomes using the TFL for treatment of upper tract strictures.
Methods: Our prospectively maintained Endourology database was queried and 15 patients with mean age of 56 underwent endoscopic stricture incision with TFL from February 2020 to January 2021. Preoperative imaging consisted of CT scans, renal scans, and ultrasonography. The procedure was performed ureteroscopically using a 200u fiber with settings of 1J and 20 Hz. Only patients with a short (< 2cm stricture) were considered candidates. Post‐operative imaging was then compared to assess radiologic resolution, improvement, or worsening.
Results: Of the cohort, 3 had calyceal diverticula and 12 had ureteral/ureteropelvic junction (UPJ) strictures. Of these, 8 (53%) had a prior history of ureteroscopy or percutaneous nephrolithotomy, 2 (13%) had robotic reconstruction, and 2 (13%) had open reconstruction. The most common indications for surgery were stones (87%), hydronephrosis (80%), and pain (66%). Ureteral strictures were encountered at the UPJ (9), ureterovesicular junction (1), mid ureter (1), and ileal ureteral anastomosis (1). Of 12 patients with ureteral/UPJ strictures, 10 had a ten‐week post op CTU/ultrasound; 6 (60%) had resolution and 4 (40%) had improved hydronephrosis. Of 3 patients with calyceal diverticulum, all had resolution of symptoms with ten‐week post op ultrasound with no evidence of stone or diverticulum reformation. Of the entire cohort, 3 patients had six month post op imaging; all demonstrated maintained resolution of hydronephrosis. Every patient was discharged same day with no reported post‐operative complications.
Conclusions: Endoscopic laser incision of ureteral strictures using TFL may be a feasible method of managing strictures requiring a minimally invasive approach. It is versatile and can be applied to treating many areas of the upper tract including calyceal diverticula, UPJ obstruction, and strictures at ureteroenteric anastomosis. Preliminary results on short term outcomes are encouraging and more long term follow up will be required to better define the TFL's potential.
5 Key Steps for High‐Frequency Ureteroscopic Dusting Technique: Illustration with Moses 2.0 Technology
NR Khajeh, KR Ghani
Department of Urology, University of Michigan
Introduction & Objective: Advances in holmium laser technology such as pulse modulation with Moses TechnologyTM have resulted in greater fragmentation efficiency and reduced stone retropulsion. With the release of Moses 2.0, pulse frequencies of up to 120 Hz are now available. In this video we highlight key steps for ureteroscopy (URS) high‐frequency dusting technique through an illustrative example using the Moses 2.0 holmium laser.
Methods: Five key strategies for high frequency dusting technique reviewed in this video include: 1) stent omission criteria, 2) ureteral access sheath (UAS) decision making, 3) irrigation, 4) patient & stone positioning, and 5) laser parameter selection. A single case of a patient with a large renal stone treated with high frequency (120 Hz) dusting technique using Moses 2.0 Ho:YAG laser (Lumenis) with a 230‐core ball‐tip laser fiber is presented.
Results: A patient with a left‐sided 1.7 cm renal pelvis stone underwent dusting URS. UAS was used to decrease intrarenal pressure and allow higher irrigation flow rates. The patient was positioned in Trendelenburg and stone nudged into an upper pole location to control fragments and optimize eventual pop‐dusting. Contact laser lithotripsy was performed to systematically debulk the stone via chipping, painting, and dancing techniques using 0.3 J x 120 Hz. Once the stone fragmented, non‐contact pop‐dusting was used with the same laser setting and higher power setting (0.5 J x 80Hz). The renal stone was treated in a single stage for a total lithotripsy time of 23 minutes (lasing time 16 minutes 34 seconds; 33280 J). Post‐operative computed tomography 6 weeks later demonstrated a 1 mm residual fragment.
Conclusions: Advances in pulse modulation have made it feasible to dust large (1.5‐2 cm) renal stones in a single stage in less than 30 minutes with excellent stone clearance. When using Moses 2.0 we have found the optimal setting to be 0.3J x 120Hz, which is feasible for both contact and non‐contact laser lithotripsy.
Exploring the Parameters that Impact the Laser Suction Effect in Holmium Laser Lithotripsy: A Video Analysis
NR Khajeh, TL Hall, WW Roberts, KR Ghani
Department of Urology, University of Michigan
Introduction & Objective: Holmium laser lithotripsy transmits energy to the stone through vapor bubbles that undergo expansion and collapse which can cause stone movement. While retropulsion has been well studied, movement of the stone towards the laser fiber tip (laser suction effect) s poorly understood. Our objective was to use high‐speed video analysis to better understand the principles of the laser suction effect and how it is impacted by laser fiber tip position on stone, laser fiber tip distance from stone, and pulse mode settings.
Methods: An in vitro horizontal ureteral model with a 5 mm inner diameter was utilized with 3 mm spherical BegoStones (15:6). A laser (P120, Lumenis) with 230‐um core fiber were used to deliver a single pulse of 1 J for all trials (n = 3) without irrigation. We assessed: (1) Fiber tip position: centered on the stone or above the stone, (2) Fiber tip distance: 2, 4, and 6 mm away from stone, (3) Pulse mode: short pulse (SP) and Moses Contact mode (MC. A Photron SA1.1 camera was used to capture videos at 30000 fps to measure stone travel distance. The stone's travel distance towards the fiber (mm) was measured and the (%) travel distance from the stone's starting position to fiber tip was calculated.
Results: When the laser fiber tip was positioned above the stone, SP demonstrated more stone attraction compared to MC at 2 mm (SP = 4.0mm, MC = 1.3mm, 200% vs. 83%; p = 0.001) and 6‐mm (SP = 1.8mm, MC = 1.3mm, 31% vs. 22%; p = 0.05) distances. When the laser fiber tip was positioned on the center of the stone, both SP and MC exhibited retropulsion at 2 mm distance with no attraction seen. At 4 mm distance, SP exhibited more attraction compared to MC (SP = 1.8mm, MC = 0.5mm, 46% vs. 12%; p = 0.03). However, at 6 mm fiber distance, MC demonstrated more attraction compared to SP (MC = 3.0mm, SP = 2.0mm, 51% vs. 34%; p = 0.01). Overall, greatest stone attraction occurred when the laser fiber tip was positioned above the stone, at 2 mm distance utilizing SP mode.
Conclusions: Stone attraction was observed in an in vitro model and is impacted by fiber tip position, fiber tip distance from stone, pulse mode and stone shape. SP was more effective when the fiber tip was above the stone, and at closer distances to the stone. MC was more effective when the fiber tip was centered on the stone, and at further distances from the stone. Future studies using multiple pulses and a range of irrigation conditions are needed to more fully understand how best to control and manipulate stone fragments.
Membranous and prostatic urethra calcification due to Corynebacterium urealyticum infection
SB Teles, ML Wroclawski, M Borrelli, JD Cha, OR Claros
Hospital Israelita Albert Einstein
Introduction & Objective:Corynebacterium urealyticum is a rare gram positive, urease producer bacteria, responsible for 1‐2% of the urinary tract infections (UTI), presented in most cases as encrusted cystitis. This video aims to show an 85 years old man with a history of radiotherapy for prostate cancer and the diagnosis of bladder neoplasia, submitted to several endourological resections and intravesical chemotherapy, as well as previous treated UTIs (but with a negative pre‐operative urine culture), who developed a C. urealyticum urinary infection, detected by tissue culture, with calcification of the membranous and prostatic urethra, with preservation of the vesical urothelium.
Methods: A review of the patient's chart and surgeries was performed and a research was done in the literature to seek for the epidemiology, risk factors and treatment of C. urealyticum infection.
Results: Infections by C. urealyticum, an opportunistic nosocomial pathogen, are being reported more frequently, mainly in patients with indwelling catheters. The capacity of hydrolysis of urea leads to hyperammonuria and the alkalinization of human urine, which can cause hypersaturation with struvite and calcium phosphate crystallization. The mean risk factors for this condition are: 1. prolonged use of a urinary catheter. 2. Hospitalization for long periods. 3. Immunocompromised patients. 4. Kidney transplantation. 5. Recent urologic procedure. 6. Chronic debilitating disease. 7. Broad spectrum antibiotic treatment. 8. Cytotoxic drug usage. 9. History of previous UTIs. Our patient presented 5 of the previously listed factors. The majority of C. urealyticum strains obtained from clinical samples display multiple resistance to antibiotics. The appropriate treatment is teicoplanin, vancomycin, linezolid or quinupristin‐dalfopristin, the only antibiotics to which this organism is universally susceptible.
Conclusions: This video shows an elderly patient with a history of radiotherapy for prostate cancer who developed a bladder cancer with several surgical manipulations and intravesical BCG and chemotherapy, as well as UTIs and consequently antibiotic use. This patient developed a C. urealyticum infection with calcification of the membranous and prostatic urethra, clearly seen in a tomography, that led to dysuria and worsening of the voiding pattern, treated with resection of the calcified tissue and vancomycin for 6 weeks followed by control trans‐urethral resection, that led to significant improvement of the local aspect and urinary symptoms.
First Experience of Inserting a thermo‐expandible Stent in Ureteral stenosis in Morocco
A Heddat, Y Houry, R Rabii
Introduction & Objective: Ureteral stents are an indispensable tool in contemporary urologic patient care. They have become first‐line devices for maintenance of ureteral patency postoperatively and in cases of ureteral narrowing. Despite their widespread use, these implants are associated with multiple complications.
Methods: Metallic Stent is an effective instrument which we used for the first time in Morocco in the treatment of our patient who had a ureteral stenosis after ureteroscopy for urolithiasis.
Results: We report a case of a 28 year old who consulted for a lumbar pain and whose CT scann showed a ureteral stenosis of 1 cm. We used a Novel, Double‐Layered, Coated, Self‐expandable Metallic Mesh Stent (Uventa Stent) to keep the ureter open. After six months of follow up with ureteroscopy, there was no obstruction anymore.
Conclusions: the short‐term result of the use of thermo‐expandible stent for the treatment of ureteral stenosis for our patient shows that it is an efficient and reproductible mininally invasive procedure. However, a long‐term study seems necessary for a better evaluation.
Using methylene blue to find the orifice of calyceal diverticulum calculi: a classical method of flexible ureteroscope
L Ye, J Wu, Y Wei
Introduction & Objective: The success of flexible ureteroscopy depends on the ability to gain access to the diverticulum. Calyceal diverticula are lined with transitional cell epithelium but lack secretory function. Thus, calyceal diverticula are filled by passive flow of urine from outside the diverticulum. We can use methylene blue based on this feature in flexible ureteroscope for finding the orifice of calyceal diverticulum and/or accompanied with calculi. This aim of this study is to perform this classical method to treat diverticulum calculi and to assess its effectiveness and complications.
Methods: We retrospectively analyzed all patients with calyceal diverticula with calculi from January 2013 to October 2019 in our Hospital. Patients are placed in the prone position under general anesthesia, a retrograde flexible ureteroscope was placed through ureteral and then reached into renal pelvis. Methylene blue was injected into renal pelvis quickly through the work tract of ureteroscope. Then we observed carefully in order to find the residual methylene blue rising from the orifice of calyceal diverticulum calculi (CDC). A 200mm laser was used to cut‐through the narrow passage, find and fragment the calculi.
Results: A total of 35 cases were included. The average diverticulum size was 2.5 cm and the average stone burden was 1.5 cm in max diameter. 71%(25/35) of CDC were observed methylene blue outflowing from their orifices. The success rate of this methods of flexible ureteroscope to confirm the orifice of calyceal diverticulum calculi was nearly 66% (23 of 35), based on the success to gain access to the diverticulum, stone clearance and ablate the diverticular mucosa. 44% (12/35) of CDC were treated by percutaneous nephrolithotomy, laparoscopic or open surgery after the failure of flexible ureteroscope. Only Grade 2 complications were found among all the cases.
Conclusions: Using methylene blue is a conducive method to identify the orifice of calyceal diverticulum calculi, resulting in a promising rate to treat it and no obvious complications.
Zero‐exposure retrograde intrarenal surgery for obese patients
K Hirota, Y Atagi, K Seto, T Tsujioka, K Izumi, M Yamanaka, Y Kawanishi
Introduction & Objective: Fluoroscopy is conventionally used for retrograde intrarenal surgery (RIRS) but exposes both the medical team and patient to radiation. To avoid intraoperative radiation exposure, we perform RIRS under ultrasound guidance. One concern is the effect that thick subcutaneous fat may have on surgical success rates in obese patients. The aim of this study was to present the safety and efficacy of ultrasound‐guided RIRS for obese patients. Ultrasound guidance was used to place guidewires, insert ureteral access sheaths into the ureteral orifice, identify residual stone fragments, and place ureteral stents.
Methods: In this study, data for 189 patients who underwent ultrasound‐guided RIRS at our institution between April 2018 and December 2019 were retrospectively reviewed. Mean BMI was 24.6 ± 4.6 (range 13.9‐46.1), with a mean stone size of 1.0 ± 0.6 cm (range 0.3–4.4 cm). The 189 patients included 17 obese patients with a Body Mass Index over 30. Stone‐free rates (SFR) and perioperative complications were evaluated, and a comparison was made between obese and non‐obese patients. Binary logistic regression models were used to assess the significance of stone‐free status and patient factors such as age, sex, BMI, and stone size.
Results: The overall SFR for all patients was 88.9%. In the obese group, the SFR was 94.1%. In the non‐obese group, the SFR was 86.2%. The complication rate was 5.9% in obese patients compared to 9.3% in non‐obese patients. Regarding multivariate analysis, the only factor that was significant for SFR was stone size. BMI was not a significant factor in stone‐free status.
Conclusions: Surgical results were not worse for the obese group than for the non‐obese group. High BMI, up to 46.1, did not affect the surgical success under ultrasound guidance. Zero‐exposure RIRS is effective and safe for obese patients.
Holmium laser deroofing of a prostatic abscess
A Coscione, J Campbell, P Acher
Introduction & Objective: There are multiple techniques for draining a prostatic abscess. The traditional transurethral approach consists of using a loop or knife with monopolar or bipolar diathermy to deroof the abscess. We present a video recording of our technique for effective deroofing of a prostatic abscess using a Holmium Laser fibre and HoLEP kit. The patient presented with urosepsis not responding to antimicrobial treatment and a very tender prostate on rectal digital examination.
Magnetic resonance imaging confirmed a sizeable prostatic abscess and the decision was made to proceed to transurethral drainage using a Holmium laser fiber.
Methods: The procedure was performed using a 24 Fr Olympus resectoscope with a HoLEP bridge and a 550 micron Lumenis laser fibre connected to a 120Watt laser.
The patient underwent transurethral deroofing of the abscess followed by urethral catheterisation with an 18Fr 2‐way catheter over a guidewire to ensure the catheter did not end in the abscess cavity. Pus was sent for microbiological culture and sensitivity and targeted antimicrobial treatment was commenced.
Results: The patient made a good post operative recovery and was discharged on day 4 following his procedure with appropriate antibiotics. He did not experience severe urethral bleeding or other immediate surgical complications.
Conclusions: We found this technique to be a safe and effective way to deroof a prostatic abscess. The benefits include high accuracy of the laser fiber allowing precise and effective incision and haemostasis. The improved vision expedited the procedure which is key in a septic patient receiving a general anaesthetic. A further benefit over traditional monopolar diathermy was the ability to use 0.9% Saline solution for irrigation as opposed to hypotonic irrigants such as glycine which we wanted to avoid given the patient's age and septic state
Enucleation and Morcellation of Bladder Leiomyoma
JC Smith, M El Tayeb
Introduction & Objective: Bladder leiomyomas are rare benign bladder lesion that occurs in less than 0.5% of all bladder tumors. The etiology remains mostly unclear with some evidence pointing to possible hormonal disturbances, infectious or inflammatory pathways, or even errors in embryological development. Due to the lesion's rarity, there is minimal data on therapy options for this tumor. Historically, most tumors are resected or excised if larger in size. We present a patient found to have a bladder leiomyoma where we were able to enucleate the tissue from the wall of the bladder, followed by morcellation.
Methods: The patient is a 50‐year‐old female with no significant past medical history who was referred to our urology clinic after a 2.2cm incidental bladder mass was seen on CT. She reported symptoms of frequency, intermittency, and incomplete emptying sensation. She denied hematuria, dysuria or a history of urinary tract infections. Family history is significant for Lynch syndrome after therapy for uterine cancer, but there is no urinary malignancy history in the family. Cystoscopy revealed a 2.5cm polypoid mass just posterior to the trigone.
Results: A transurethral resection was attempted. The tissue was dense and required steady pressure with the bipolar loop to engage the cutting current. Due to the location, a bimanual exam was done that revealed the mass was not connected to the cervix or uterus. It was noted that the tissue was freely mobile in the wall, and the loop was used to enucleate the remaining portion of the mass from the wall with the capsule remaining intact. After failed attempts to remove the tissue with the grasper and basket, morcellation was attempted and completed successfully.
Conclusions: The cystoscopic appearance of a bladder leiomyoma does not mimic that of a urothelial tumor. The tumor is composed of smooth muscle giving it that dense homogenous appearance seen in this case. A majority of these lesions are endovesical and based on our experience, are mobile in the wall of the bladder. Enucleation with subsequent morcellation may be a viable option for small to moderately sized lesions if failed standard resection. Further studies would need to be conducted before drawing any further conclusions.
Combined endoscopic management of the distal ureteral obliteration with the Thulium Fiber Laser
A Martov, A Andronov, M Golubev, D Abdullaev, P Golubev
Introduction & Objective: To describe combined antegrade and transurethral technique for the treatment of distal ureteral obliteration. We present a “cut‐to‐the‐light” technique that has been described before, but which we consider useful and decisive. The key points and difficult aspects of the technique are shown, along with our experience with it.
Methods: 42 y.o. female with right nephrostomy tube has been referred to the urologic clinic. In 2017 she underwent complicated hysterectomy due to giant myoma. Intraoperatevely there were blood transfusions and postoperatively several days she was at ICU, DVT has been occurred, cava‐filter has been made to prevent thromboembolic complications. She had also stroke with left side lower hemiparesis. 12 weeks before admission right side hydronephrosis with fever has been diagnosed and the nephrostomy tube has been placed. The distal obliteration of right ureter has been detected. She wasn't undoubtedly candidate to reconstruction due to her psychoneurological status, precluding planned general anesthesia (ASA score: 4‐5). We decided to reestablish the ureteral continuity with a combined transurethral and percutaneous approach under spinal anesthesia. Initially we performed rigid ureteroscopic examination and realized the total obliteration of the lumen at the 7 cm from the orifice. Then, we performed antegrade nephrostogramm and checked the short‐length distal ureteral obliteration. We introduced through the percutaneous access special lightning ureteral catheter (Karl Storz) and passed it up to the obstruction place. Next step was the ureteroscopic “cut‐to‐the‐light” procedure with the novel thulium fiber laser (fiber – 400mkm, 10W, 10Hz, 1J). As soon as the laser ureteral recanalization has been performed the percutaneously placed guide‐wire has been retrogradly removed by the rigid ureteroscopic forceps. Using this guide‐wire as a safety one, the rigid ureteroscopy has been made and laser ablation of any debris and fiber remnants to establish the natural ureteral lumen has been proceed. Finally, we drained the renal unit with two double‐J 6F ureteral stents for 12 weeks.
Results: On 3 month ureteroscopy there were no any signs of obstruction and the stents have been removed. Finally we present 12 months IVU, showing ideal contrast passage from the right kidney. At the moment she is still under our surveillance (27 months).
Conclusions: Distal ureteral obstruction often requires any type of reconstruction surgery. Here we present the endourologic technique to reestablish distal ureteral continuity in cases with either the contraindication for general anesthesia or then the reconstruction is anticipated or contraindicated.
Video Session 07: Laparoscopy: Upper Tract
V07: Laparoscopy: Upper Tract
FJ Sampaio, R Link
A novel technique to decrease Warm ischemia time In Laparoscopic Partial Nephrectomy with use of Satinsky Vascular Clamp
D Vaddi, P Ramakrishna, P Siddalinga Swamy, B Manas Babu, G Soundarya, A Hemnath, S Chahar, S Gunadal, P Rakesh
Introduction & Objective: Laparoscopic Partial nephrectomy(LPN) is an established treatment option for small renal tumors . The duration for which vascular supply to kidney temporarily blocked is called Warm Ischemia time(WIT). Many case series have proved that , WIT >30 minutes has adverse impact in long term renal function . LPN in Postero‐lateral & Hilar renal tumors, has always been a challenge while tumor dissection as well as renorrhpahy . In this study we used Satinsky vascular clamp, to flip the kidney. This stabilised kidney while tumor excision, as well as suturing, which helped in reducing WIT
Methods: Port positions and initial colon mobilisation were done according to standard LPN. Lower pole dissection done , ureter identified. Lower pole was separated from ureter. Hilar dissection done by blunt dissection and both supra & infra‐hilar window created to provide free mobility to kidney. After arterial clamping with Bulldog clamp, kidney was flipped by Satinsky vascular clamp. While cutting the tumor, this also decreased venous bleed by compression and due to better ergonomics & vision we could suture faster .
Results: From 2020 July to 2021 January,05 cases of LPN were done. Mean tumor size was 4.5cm. Mean age of patients was 54.2 years. Out of 5 cases,4 were male,1 female. WIT duration ranged from 17‐19 minutes in all cases. We could reduce WIT to <20 minutes , by use of above technique. Longer WIT duration is directly related to increased ischemic injury to nephrons. In all the cases surgical margin was free, no cases of urinary leakage,1 case had minor bleeding, which was managed conservatively. All cases on follow‐up after 3 months, had good renal uptake in DMSA Scan.
Conclusions: Laparoscopic partial nephrectomy with use of Satinsky vascular clamp decreases WIT , by stabilizing kidney with better ergonomics.
Laparoscopic heminephrectomy for left hilar kidney tumor T1b in the presence of nephrolithiasis
T Nguyen, M Thai, X Ngo, Q Chau, K Hoang, H Nguyen, L Dinh, H Le, T Nguyen, RW dobbs
Introduction & Objective: To date, there have been few case reports of hilar large renal tumor excised using the laparoscopic heminephrectomy approaches. Therefore, the incidence, treatment, and outcome of the technique remain unclear. We describe a case of laparoscopic heminephrectomy for left hilar kidney tumor T1b in the presence of nephrolithiasis.
Methods: A 36‐year‐old man went to the hospital because of his left flank pain. The patient had no hematuria and had no history of surgery and kidney disease. His serum creatinine was 1.37 mg/dL and eGFR was 66 ml/min/1.73 m2. According to his renal scintigraphy, GFRs of the right kidney and left kidney was respectively 42.1 and 19.6 ml/min. The computed tomography of the abdomen revealed the left kidney with a 5.1 × 4.7 cm hilar tumor arising from the upper moiety and an incidentally discovered lower pole stones. R.E.N.A.L. nephrometry score was 10PH. In summary, he had a hilar kidney tumor cT1bN0M0 with nephrolithiasis in the left kidney. After discussion, the patient elected a minimally invasive approach to treating his malignancy.
Results: The operative time was 190 minutes. The warm ischemia time was 19 minutes. The estimated blood loss was 200 mL for the heminephrectomy. The patient was discharged at day 4thpostoperatively. The final pathologic examination of the tumor specimen revealed organ‐confined clear cell renal cell carcinoma, Fuhrman grade II, with negative surgical margins. Local recurrence or metastasis was not detected by follow‐up CT imaging at 2 months after surgery. There was no hydronephrosis and no nephrolithiasis. The renal function was stable, with the serum creatinine levels before surgery and at 2 months postoperatively was the same 1.37 mg/dL.
Conclusions: In conclusion, the transperitoneal laparoscopic technique is safe and effective for this complex clinical case.
Laparoscopic stepwise approach for the treatment of renal carcinoma complicated with tumor thrombus of inferior lumen (or renal) vein
F Chen, k Li, S Li, S Tang
Introduction & Objective: Laparoscopic stepwise approach for renal carcinoma complicated with inferior luminal (or renal) venous tumor ambolus. These are two cases where this method was used
Methods: Case 1: The male patient, 73 years old, was admitted to the hospital due to painless gross hematuria for half a year, aggravated with dysphoria for 3 days. Ultrasound: Right kidney mass was 6.7cm × 8.7cm × 9.5cm, kidney cancer was considered. Abnormal echo in bladder 7.0cm × 7.7cm × 8.4cm, blood clot? Plain and contrast‐enhanced CT scan showed a blood rich mass of 80*67*92mm in the right kidney, perirenal varicose veins in the right kidney, and tumor thrombus in the inferior vena cava (27mm).
Diagnosis:
(1) Right kidney mass, kidney cancer ? T3bN0M0, Mayo grade 2
(2) Inferior vena cava tumor thrombus 27mm, Mayo grade 2
(3) Bladder tamponade, anemia
Treatments :
1. Cystoscopy was performed, and the clot was cleared, and the right ureter was seen to spout blood, but no abnormality was found.
2. Retroperitoneal laparoscopic stepwise approach for radical nephrectomy of lower vena cava tumor thrombus removal (Mayo grade 2)
3. The operation time was 180mins, the operation was successful, and EBL was 330ml.
• patient showed good recovery during follow‐up for 17m.
In case 2, Retroperitoneal laparoscopic stepwise approach for radical nephrectomy of vena cava tumor thrombus removal was used. The operation time was 120mins, the operation was successful, and EBL was 100ml. Postoperative pathological examination: ccRCC, renal venous tumor embolus. Followed up for more than 1m, the patient recovered well.
Conclusions: Laparoscopic stepwise approach for the treatment of renal carcinoma complicated with tumor thrombus of inferior lumen (or renal) vein is safe and effective.
Withdrawn
Safety and Outcome of Laparoscopic Donor Nephrectomy with Early Branching Renal Artery
S Jayaprakash, M Thangarasu, N Jain
Apollo Main Hospitals, Chennai, Tamil Nadu, India
Introduction & Objective: Renal transplantation is the only cure for patients with end‐stage renal disease. Due to the ongoing supply‐demand mismatch most of the transplant centers have adopted laparoscopic donor nephrectomy (LDN). LDN increases the number of kidneys available for transplantation by minimizing morbidity, lowering costs, and expediting recovery of living kidney donor. Laparoscopically procured renal allografts has been shown to provide short and long term out comes comparable to outcomes of open donor nephrectomy. Multiple renal arteries (MRAs) and early branching arteries represent a surgical challenge by the difficulty in performing an anastomoses, bleeding and stenosis. However, it can be performed safely and outcomes are comparable with single vessel donor nephrectomy. We are presenting a series of videos, both right and left side with early renal artery branching, to show the safety of laparoscopic donor nephrectomy in such cases.
Methods: Early branching on the right side is defined as segmental branching behind the IVC (retrocaval branching) or when it occurs 1 cm from the right IVC margin and on the left side defined as segmental branching less than 1–1.5 cm from the origin of the left renal artery. 170 LDN cases were performed since December 2017, 27 cases had early branching arteries among them. All pts evaluated and approved by the Transplant Co‐ordination Committee were enrolled and site of organ procurement was decided in the committee.
Results: Renal artery was harvested as a single stump with adequate length and successfully incorporated as a single vessel in the recipient. All parameters were comparable to single vessel LDN and none of our cases were converted to open surgery. Recipient outcomes were also comparable.
Conclusions: Donor kidneys with early arterial branching pattern can be safely procured by LDN.
Laparoscopic Partial Nephrectomy for a Complex Right Renal Tumour
S Jayaprakash, N Jain
Apollo Main Hospitals, Chennai, Tamil Nadu, India
Introduction & Objective: Historically, open radical nephrectomy has been the treatment of choice for renal masses, with nephron‐sparing surgery (NSS) reserved for imperative indications. However, successful outcomes with NSS have prompted its application to patients with nonimperative indications. Partial nephrectomy (PN) currently represents the standard of care for clinical T1 renal masses, as it can provide oncologic outcomes equivalent to those of radical nephrectomy (RN). Accumulating evidence suggests that PN can reduce the morbidity and mortality resulting from renal insufficiency. LPN was first described in 1993, and duplication of open PN (OPN) techniques in a laparoscopic setting was described by Gill et al. in 2002. Preliminary efforts to perform laparoscopic partial nephrectomy (LPN) evolved in an attempt to improve patient outcome, morbidity, and mortality. LPN initially entailed wedge resection of small, peripheral, exophytic tumors. As the technology and surgical expertise have improved, the indications for LPN have expanded. Our objective is to consider LPN for complex tumors with proper selection of cases.
Methods: A 55yr old male with no co‐morbidities, essentially asymptomatic, was incidentally identified to have a right renal mass. CECT abdomen revealed a 3.68x2.8cm mostly exophytic anteromedial interpolar mass extending to upper pole and abutting the renal hilum with R.E.N.A.L nephrometric score of 8a. He was planned for laparoscopic right partial nephrectomy with consent for conversion to radical nephrectomy. Right sided DJ stenting was done. Routine port placement as for right nephrectomy was done and routine steps followed. Hilum was clamped with Lap Satinsky. Hilar dissection was done and individual vessels supplying the tumour were clipped and cut. Renorrhaphy was done and clamp was released.
Results: WIT was 40mins and total blood loss was nearly 250ml. HPE was reported as clear cell carcinoma, WHO nuclear grade II with all margins negative for tumour, pT1aN0Mx. Postoperative period was uneventful. Pt was discharged on POD 3, foley was removed on POD 5 and drain on POD 6. DJ stent was removed after 6 weeks. His creatinine was stable.
Conclusions: LPN can be considered safe for complex tumours with proper selection of cases.
M Aslzare, MR Darabi Mahboub, AA Asadpour, M Farzin, A Etesami, MH Shakibi
Introduction & Objective: Management of complete staghorn stones is challenging. Surgical management of nephrolithiasis has changed dramatically in past half of the century due to advances in endourological techniques including percutaneous nephrolithotomy (PCNL), retrograde intrarenal surgery (RIRS) and Shock Wave Lithotripsy (SWL). Indications for open stone surgery have markedly diminished. The complete removal of the stone is the ultimate goal, but might not be achieved even after several sessions of PCNL and/or SWL and/or RIRS.
The objective of this study is to assess efficacy and technique of laparoscopic anatrophic nephrolithotomy (LAN) as an alternative treatment for complete bulky staghorn.
Methods: A 65‐year‐old male patient underwent 4‐port transperitoneal LAN for left large, complete staghorn. The stone size was 72 mm. After clamping the artery, the incision was made laterally and longitudinally on Brodel line through full thickness of cortex using a laparoscopic scissor and electrocautery. A running one layer cortical suture was performed with Hem‐o‐lok reinforcement for renorrhaphy repair.
Results: Procedure was completed laparoscopically. The operative time was 120 minutes, and the warm ischemia time was 27 minutes. The estimated blood loss was 50 ml. The hospital stay was 3 days without complications. The renal function was unaffected based on serum creatinine levels before and after surgery. Stone‐free status of the left kidney was confirmed postoperatively with renal CT‐scan.
Conclusions: Although PCNL is the standard of care for treatment of staghorn stone, laparoscopic AN is effective in management of large staghorn with an acceptable rate of stone clearance and operative complications. This technique minimizes the barriers of an open flank incision, need for secondary procedures and reduced hospital stay and recovery period compared to open surgery.
Laparoscopic Pyelolithotomy For Complete Staghorhorn Stone With Extraction Of Small Calceal Stones
M Soltani, S Farshid, H akbari gilani, N ahmadian
Introduction & Objective: Percutaneous nephrolithotomy is a standard treatment for Staghorn kidney stones but due to parenchymal damage and the possibility of pseudoaneurysms and severe hemorrhage, selective alternative to low invasive alternative such as laparoscopy was considered to compare therapeutic results and complications with percutaneous nephrolithotomy.
Methods: Patient was 30 years old male with bilateral Stone , Right side upper ureter and left side Staghorn Stone , At first patient undergone Laparoscopic ureterolithotomy ,2 months later patient referred to our clinic for left side staghorn stone , there were different modalities for left side stone management such as , multi session Pcnl , Open Pyelo‐nephrolithotomy, Laparoscopic pyelolithtomy . Since this stone had large extrarenal part with dilated calyx , and patient denied multi session pcnl , patient was scheduled for Laparoscopic Pyelolithotomy with the probablity of open surgery,
Results: during laparoscopy after finding the ureter and the pelvis , the pelvis attachments was freed upto renal parenchyma in the latteral and upper border , this helps for stone extraction without injury to ureteropelvic junction and convenient suturing of pelvis incision, after horizental incision of the pelvis by monopolar cautery , first the stone attachment to calyceal urothelium was freed by maryland, then tensile strenght was made to lower part of the stone by Babcock grasper and leverage force made behind the stone by maryland , finally the stone was extracted outside the pelvis, since pelvis is large , laparoscopic lens can easily enter inside the kidney and small stones inside calyx were extracted , finally Double J stent was inserted and pelvis urothelium was repaired by0‐4 vicryl from both ends of incision , stones were get out of tyhe body through the extended incision of lower trocar
Conclusions: Given that during the laparoscopy of staghorn stones with large pelvis the entire pyelocalis system is accessible, it is possible to remove the stone completely, but in PCNL surgery it may require multiple accesses to remove the stone in a single session. Also, in staghorn stones with large extrarenal part, according to our study comparing PCNL and laparoscopic pyelolithotomy for staghorn stones with large pelvis, laparoscopic Pyelolithotomy had more stone free rate and lower Hb drop compared to PCNL procedure .
LAPAROSCOPIC UPPER‐POLE HEMINEPHRECTOMY IN DUPLEX KIDNEY
C Conde Redondo, A Alonso Villalba, S Martin, F Natal Alvarez, A Zamora Horcajada, A Ruano Mayo, J Torrecilla, L Cuellar Martin, A Herranz Arriero
Introduction & Objective: The most common congenital abnormality of the urinary tract is ureteric duplication. Pelvi‐ureteric junction obstruction in a duplex kidney is the most common site of obstruction in the upper urinary system. The combination of ureteric duplication and pelvi‐ureteric junction obstruction is a rare association, and infrequently reported.
It occurs in 0.7% of the healthy adult population and in 2‐4% of patients investigated for urinary tract symptoms. Most of the time they are asymptomatic, but they may present with repeated urinary infections due to obstruction or reflux flank pain if they produce hydronephrosis. It is frequently associated with ureterocele. The indication for treatment is: Marked hydronephrosis of the upper skin that produces a mass effect and or infection or vesicoenteric reflux of the lower pole .
In this video we present a 45 years old women diagnosed of Upper‐pole obstruction in a left duplex kidney, treated by laparoscopic upper‐pole heminephrectomy
Methods: We present the case of a 45‐year‐old patient who consults for repeated urinary infections. Ultrasound is reported as a severe left ureteropielocalical ectasia with complete atrophy of the underlying cortex. In the urographie: functional anulation of the upper pole and lower normofunctionalism is observed. The CT shows a left kidney, larger than the contralateral, with a double system excretor, confirming the existence of a non‐functional upper pole, which continues with a dilated ureter to its mouth in the bladder.
• Once decolated , the main renal pedicle , and the upper‐pole pedicle is identified and we localized two renal arteries.
• We identify the plane of separation between upper and lower pole that is avascular
• We release the upper pole of its caudal anchors
• We release and dissect the upper pedicle of the upper pole
• We identify another superior polar ateria that is clamped and sectioned
• We can identify the inferior artery and renal vein of the lower‐pole that are intact
• We completely release the upper pole following the cleavage plane
• We put a clip to the ureter and section it
• We check hemostasis, it is not necessary to make a renal raffia having followed an avascular plane. For security we place a surgicel mesh
• We check that there is no bleeding, we remove the piece and finally put the drain.
Results: Surgical time 60 minutes. Bleeding: 200 ml 48 hours hospital stay
Conclusions: Surgical treatment of the upper skin is rarely necessary. When there is an indication, the laparoscopic approach is a fast, feasible technique that is accessible to all hospitals.
Laparoscopic pyelolithotomy in an ectopic pelvic kidney: Case report of a successful management of a Staghorn Stone
V Elorrieta, J Salvadó, A Velasco, A Kompatzki, S Moreno, P Guerrero
Introduction & Objective: We report the case of a 24‐year‐old female patient afflicted by a 7 cm Staghorn stone in a left ectopic pelvic kidney. This challenging case was discussed by our team due to the possible surgical approaches we had. Literature supports a laparoscopic approach for cases where the renal position and rotation defects may significantly interfere with outcomes. After consideration, we performed a laparoscopic pyelolithotomy and the patient was discharged on the third postoperative day with no complications. This case discusses the management of large stones in unusual conditions.
Methods: A 24‐year‐old female patient with no medical or surgical history reported being afflicted by an intermittent left flank pain for the last two months. She is a truck driver in Northern Chile's mining industry. Creatinine levels in blood were 0,9 mg/dL. A Computed Tomography (CT) scan revealed a 7 centimeters maximum‐diameter Staghorn stone in her left pelvic kidney. We considered the abnormal location and rotation of the kidney, size of the stone and risk of colon injury by a percutaneous approach. We also considered that an endourological approach would require multiple interventions. After thorough discussion with our team and the patient, we opted for a laparoscopic pyelolithotomy treatment.
Results: The surgical procedure lasted 160 minutes. Under general anesthesia, and in a right lateral recumbent position, we proceeded with a left transperitoneal laparoscopic pyelolithotomy. A four‐centimeter‐long longitudinal pyelolithotomy was performed and the stone was extracted. We proceeded with the renal pelvis closure, leaving a double‐J stent as a tutor. After confirming hermeticity we placed a drain and proceeded with closure. The patient had an excellent postoperative evolution, and she was discharged on the third day after surgery. The double‐J stent was removed after 4 weeks, with complete resolution of the clinical symptoms.
Conclusions: This patient presented a very challenging case. The anatomical alterations, renal position and rotation, size and location of the stone, and the need for immediate and optimal resolution due to the patient's occupation. Therefore, we were able to safely resolve a rare and challenging case, by performing a laparoscopic pyelolithotomy in an ectopic kidney, resulting in a stone‐free procedure.
Utilizing da Vinci® Robotic Surgical System to Treat Challenging Urinary Stone
MW Salkini, A Dahman
West Virginia University
Introduction & Objective: A worldwide mounting in the incidence and prevalence of urolithiasis has been observed. The standard treatment of urologic stone disease (USD) has changed from open surgery to extracorporeal shock wave lithotripsy (ESWL), percutaneous nephrolithotomy (PCNL) or ureteroscopy depending on the size and location of the stone. Open stone surgery is reserved for challenging urinary stone (CUS) that is not amenable to the above‐mentioned less invasive techniques. We utilized de Vinci robotic surgical system to treat CUS. We are sharing our experience in utilizing Da Vinci® robotic surgical system to treat patient with urolithiasis instead of open surgical approach.
Methods: We reviewed prospectively collected data of 31 patients who underwent robotic assisted stone surgery (RSS) between January 2010 and February 2020 at our institute for USD involving 34 nephroureteral units.
Results: A total number 34 RSS were accomplished with no conversion to open. 3 patients had bilateral stone and needed to have RSS on each side separately. 17 RSS were performed on the right. The indications for RSS included: morbid obesity (n = 13, mean BMI 52.7 kg/m2), need for concurrent renal surgery (n = 6) severe contractures limiting positioning for retrograde endoscopic surgery or PCNL (n = 3), symptomatic calyceal diverticular stone with failed endoscopic approach (n = 4) and inability to position the patient (n = 5). 31 nephroureteral unit (91 %) were rendered stone free on the first attempt with complication occurring after 5 surgeries (15 %).
Conclusions: RSS is viable options in the treatment of CUS with high success rate and low risk of complication. The need for open stone surgery was eliminated by RSS at our center. Multiple center need to participate in RSS with bigger number of patients to create an established role for RSS.
Establishing the Japanese version of the Wisconsin Stone Quality of Life questionnaire (WISQOL)
K Taguchi, T Okada, S Hamamoto, S Okada, T Inoue, A Okada, T Yasui
Nagoya City University Graduate School of Medical Sciences
Introduction & Objective: The Wisconsin Stone Quality of Life questionnaire (WISQOL) is a quality of life measure designed for patients with urinary stones that has been translated and used in several languages. This study aimed to establish and validate the Japanese version of the WISQOL (J‐WISQOL).
Methods: The J‐WISQOL was translated and validated using a multistep process proposed by the World Health Organization that involved forward translation, back‐translation, and pilot testing using a group of patients. This study enrolled 150 patients with urinary stones who visited three academic hospitals for stone treatment. We assessed the convergent validity of correlation patterns and internal consistency of the J‐WISQOL and Short‐Form 36‐item survey version 2 (SF‐36v2).
Results: The median total scores for the J‐WISQOL and SF‐36 v2 were 108.2 ± 20.3 and 117.7 ± 8.4, respectively. Regarding each domain, the median scores for social, emotional, disease, and vitality impact were 75.9 ± 21.2, 68.6 ± 20.1, 66.9 ± 20.5, and 71.4 ± 23.0, respectively; moreover, urinary stones decreased the health‐related quality of life. In the SF‐36 v2, which was completed by the same patients, the norm‐based scoring (NBS) was 47.7 ± 11.8 for social functioning, 47.3 ± 9.8 for mental health, 45.6 ± 8.3 for general health perceptions, and 52.6 ± 16.0 for energy vitality; moreover, there was a small deviation from the standard score. The J‐WISQOL showed good internal consistency (Cronbach's α = 0.88‐0.96) in the total scores and each domain. Besides, there were strong inter‐domain associations (Spearman's correlation coefficient r = 0.67‐0.94) within the J‐WISQOL. Most importantly, the J‐WISQOL was correlated with the SF‐36v2 in all domains: social, emotional, health, and vitality impact (r = 0.47‐0.66). (Table 1)
Conclusions: The J‐WISQOL is a reliable instrument for evaluating health‐related quality of life measures in patients with urinary stones and will be a useful quality of life questionnaire for urinary stones in Japan.
Predictors of index percutaneous nephrolithotomy care setting and impact on perioperative outcomes and cost
SK Bechis, DF Friedlander, R Sur
University of California ‐ San Diego, Department of Urology
Introduction & Objective: Percutaneous nephrolithotomy (PCNL) is an appropriate treatment option for patients with a large renal stone burden or complex anatomy. Cost pressures and newer minimally invasive approaches have led to a migration away from the traditional inpatient care setting toward ambulatory surgical centers. However, it is unclear what clinical and non‐clinical factors determine where patients receive their surgical care and whether perioperative outcomes and costs differ among these cohorts. We sought to identify predictors of index surgical care setting as well as perioperative outcomes and cost associated with these unique care settings following PCNL surgery.
Methods: All‐payer data from the 2014 Healthcare Cost and Utilization Project (HCUP) State Databases from Florida (FL) and New York (NY) were used to identify all patients undergoing an index PCNL. Patient demographics, regional data, 30‐day revisit/reoperation rates, and total index/30‐day costs were determined. Multivariable logistic regression adjusted for facility clustering was utilized to identify predictors of index surgical care setting and 30‐day revisit/reoperation, while gamma generalized linear regression was used to compare index/30‐day costs.
Results: Of the 747 patients undergoing PCNL, 314 (42.0%) received care in the inpatient setting compared to 433 (58.0%) in the ambulatory care setting at an adjusted mean cost of $11,904.66 vs. $8,876.438 (P < 0.001). Predictors of receiving care in the ambulatory care setting included gender (female vs. male: OR 0.49, 95% CI 0.34‐0.72; P < 0.001), fewer comorbidities (CCI ≥2 vs. 0: OR 0.41, 95% CI 0.24‐0.68; P = 0.01), insurance status (Uninsured vs. private: OR 0.10, 95% CI 0.04‐0.27; P < 0.001), and rural vs. metropolitan care setting (OR 22.36, 95% CI 6.46‐77.38; P < 0.001). The 30‐day adjusted revisit/reintervention rate for cases performed in the ambulatory vs. inpatient setting was comparable (22.4% vs. 16.2%, P = 0.9). Mean cost attributable to a 30‐day revisit was $6,918.13.
Conclusions: We demonstrated that both clinical and non‐clinical factors predict where patients undergo PCNL, with patients receiving care in the ambulatory setting experiencing dramatically lower costs but comparable 30‐day perioperative outcomes. Our findings suggest that ambulatory‐based PCNL offers significant cost savings without compromising 30‐day outcomes in appropriately selected patients.
Utilization of antibiotic irrigation and betadine for renal pelvis sterilization during PCNL to decrease infectious complications
D Mikhail, L Nyman, E Lynch, A Rai, T Aro, AD Smith, D Hoenig, Z Okeke
Lenox Hill/Northwell Health
Introduction & Objective: Percutaneous nephrolithotomy (PCNL) utilization continues to rise with complex stone disease incidence. Efforts are made to prevent infectious complications, including pre‐ and postoperative antibiotic regimens. Despite this, infectious complications, such as SIRS and urosepsis, are the most common complications following PCNL. We developed a technique to further sterilize the collecting system during PCNL and aimed to compare our early outcomes with this intervention to our previous series.
Methods: Starting Feb. 2019, we modified our PCNL technique to include sterilization with 10mL betadine solution into the renal pelvis, mixed betadine with contrast for pyelography and additionally used antibiotic irrigation throughout the case (gentamicin 80mg into two 3L bags). Surgical technique including prone position, fluoroscopic access, stone treatment and drainage were otherwise unchanged. We retrospectively reviewed our PCNLs over a 2‐year period looking for differences in patient demographics and perioperative outcomes with our new sterilization technique. Our primary outcomes were post‐operative SIRS response and post‐operative sepsis, defined as SIRS response and positive post‐operative culture. Statistical analysis was performed using Stata 16.
Results: Data was extracted for a total of 438 consecutive PCNLs performed in adults at our institution over a 2‐year period – with our betadine intervention group making up 178 (41%) of all PCNLs. The intervention group was similar in age (59 vs. 61), sex (∼51% female), Charlson comorbidity index (3.7 vs. 3.6), ASA (∼2.5) and positive pre‐operative culture rate (17% vs 20%, p = 0.5). There was no difference in median length of stay (2 days), ICU admission (∼5%) or 30‐day readmission (11% vs. 8%, p = 0.25) . There was no significant difference between the two groups in post‐op fevers (∼8%) or SIRS response (∼8%). Sepsis rates were lower in the intervention group but not significantly different (2.8% vs. 5%, p = 0.25). Female sex (OR 4.2, p = 0.026) and positive or contaminated pre‐operative culture (OR 2.8, p = 0.04) were associated with post‐operative sepsis.
Conclusions: We report the first data comparing outcomes of PCNL with our novel sterilization technique ‐ utilizing intrarenal betadine and antibiotic irrigation. We found this technique did not significantly change our average LOS, SIRS rate, ICU admissions or 30‐day readmission. Perioperative sepsis rates were slightly lower, at 2.8% vs. 5%, however this was not statistically significant. A larger, higher powered prospective study will be required to conclude whether antibiotic irrigation and betadine can truly decrease infectious complications post‐PCNL.
Opiates can be replaced with ‘music and mood lighting’ during lithotripsy: Comparative outcomes from ‘South Coast Lithotripsy Centre’
M Ramachandra, A Pietropaolo, L Tear, D Tanya, A Davies, S Miles‐board, A Humphrey, BK Somani
University Hospital Southampton, UK
Introduction & Objective: Shockwave lithotripsy (SWL) is usually performed with some form of analgesia or anaesthesia, with practices varying worldwide. We wanted to look at the outcomes of SWL where we replace parenteral opiates with oral non‐opiate based analgesia and ‘music and mood lighting’ during lithotripsy.
Methods: We looked at all patients treated for renal stones with intramuscular pethidine and per‐rectal (PR) diclofenac (group 1) and compared it to patients who received oral paracetamol and PR diclofenac, (or dihydrocodeine, if contraindicated for diclofenac or needing stronger analgesia) along with music and mood lighting (group 2). Data was collected for patient and stone demographics, stone free rate and complications
Results: Data was analysed for 148 patients (201 procedures) and 48 patients (71 procedures) for groups 1 and 2 respectively. The stone size was 7.4 and 6.7mm in the groups with more lower pole stones in group 2. The procedures were done as day cases in both groups, with SFR of 32% in group 1 and 48% in group 2. Sixty‐five patients (92%) did not need opiate analgesia in group 2. The overall complications in both groups were 3% and were all Clavien I complications.
Conclusions: Parenteral opiates can be completely omitted for SWL by decreasing patient anxiety and need for analgesia by ‘music and mood lighting’. More than ninety percent of our patients did not need any opiates with this setting. Our results reflect better stone free rates in group 2 perhaps reflecting better patient comfort, less involuntary movement leading to better stone focus.
Complication rates after percutaneous nephrolithotomy in patients with neurological Conditions
A Garbens, V Kommidi, H Trivedi, JA Antonelli, M Pearle, BA Johnson
UT Southwestern
Introduction & Objective: Despite the minimally invasive nature of percutaneous nephrolithotomy (PCNL), complication rates associated with PCNL are upwards of 20%. Patients with neurological conditions are at increased risk of stone disease and their condition may place them at higher risk of peri‐operative complications. We sought to compare the risk of post‐operative complications, between patients with and without neurological conditions who underwent PCNL.
Methods: We reviewed all patients who underwent PCNL between January 2014 until December 2020 at our academic high volume stone center. Patients with history of stroke, brain hemorrhage, spinal cord injury, neural tube defect, multiple sclerosis , cerebral palsy, traumatic or anoxic brain injury and degenerative brain diseases were considered to have a neurological condition (NC). Patient demographic data were collected and compared between groups. Thirty‐day post‐operative complications, major complications (Clavien‐Dindo 3 or higher), infectious complications (urinary tract infection, pyelonephritis or sepsis) and transfusion rates were compared between groups using multivariable logistic regression analysis.
Results: A total of 578 patients underwent 680 PCNL procedures during the study period, including 48 bilateral simultaneous and 23 asynchronous bilateral procedures. Among this group, 14% (83 patients) had a NC. The 2 groups were comparable with regard to race, age, gender, median income and initial stone burden. In addition, there was no difference in operative time between the 2 groups. However, patients with NC were significantly more likely to initially present to urology with sepsis from a urinary source (21% vs. 3%), have lower body mass index (27 kg/m2 vs. 32 kg/m2), have a lower pre‐operative hemoglobin (12.9g/dl vs. 13.7g/dl) and have a higher ASA score (p < 0.05 for all) than patients without NC. On multivariable logistic regression analysis, having a NC was an independent risk factor for any complication (OR 1.7, 95% CI = 1.01 – 3.0, p = 0.05), infectious complications (OR 2.7, 95% CI = 1.2 – 5.9, p = 0.02), and requiring a transfusion (OR 5.4, 95% CI = 1.4 – 20.9, p = 0.02). Having an NC was not an independent risk factor for major complications (OR 1.5, 95% CI = 0.7 – 3.3, p = 0.26).
Conclusions: Patients with NC carry a higher risk of complications after PCNL, particularly infectious complications and need for transfusion . Patients with NC should be counseled regarding increased complication risk prior to undergoing PCNL.
Withdrawn
Safety and Efficacy of Simultaneous Bilateral Percutaneous Nephrolithotomy: A Matched Retrospective Cohort Study
VK Wong, CJ Lundeen, R Paterson, KB Scotland, BH Chew
Introduction & Objective: Traditionally, patients presenting with large bilateral renal stones are treated with two unilateral PCNL (U‐PCNL) procedures performed in a staged fashion to reduce complications. However, with advances in anesthesia, antibiotic therapies, and surgical techniques, simultaneous bilateral PCNL (SB‐PCNL) may now be a safe and feasible option in treating large bilateral stone burdens. In this matched retrospective cohort study, we investigated the safety and efficacy of SB‐PCNL by comparing intraoperative and post‐operative outcomes to U‐PCNL.
Methods: A retrospective review was conducted to evaluate the intraoperative and patient outcomes following SB‐PCNL to U‐PCNL. Electronic Medical Records at Vancouver General Hospital were queried for patients who underwent PCNL procedures between the dates of 2010‐2015. SB‐PCNL patients identified were retrospectively matched by age, gender and American Society of Anesthesiologists physical status classification to unilateral stone patients who underwent U‐PCNL. Target stone characteristics, operative time, hospitalization length, post‐operative complications, blood loss, opioid use, pain, and stone‐free rates were compared using the Wilcoxon signed‐rank test and Fisher's exact test.
Results: 85 patients (42 SB‐PCNL and 43 U‐PCNL) with large renal stones ( >20mm2) were identified for this study. SB‐PCNL patients had a much greater total stone burden when compared to U‐PCNL (P = 0.096), however stone burden per individual kidney was comparable (p = 0.824). SB‐PCNL patients had longer operative times (p < 0.001) and length of hospitalization (p = 0.020). Post‐operative complications (p = 0.344), blood loss (p = 0.296), opioid use (0.287), and pain (p = 0.547) were not statistically significant. 38% of patients in the SB‐PCNL group achieved stone‐free status with no residual fragments apparent on postoperative day one CT imaging, compared to 74% in the U‐PCNL group (p < 0.001). Maximum residual fragment size was not significant (p = 0.753), with 78.6% of SB‐PCNL residual fragments being >4mm.
Conclusions: The rates of blood loss, post‐operative complications, opioid use, and pain was similar between SB‐PCNL and U‐PCNL. SB‐PCNL was associated with longer operative times, length of hospitalization, and lower stone‐free rates. Despite this, the potential benefits of a single procedure and anesthesia to treat bilateral stone burdens, lower total MED prescribed, and lower hospital costs render SB‐PCNL to be an attractive option in the treatment of bilateral kidney stones.
Impact of Reverse Trendelenburg Position on Ureteral Stone Retropulsion: A Prospective Randomized Study
JA Khusid, H Anastos, R Chandhoke, D Lundon, AS Sadiq, J Bamberger, B Gallante, WM Atallah, M Gupta
Icahn School of Medicine at Mount Sinai
Introduction & Objective: Minimizing retropulsion may improve surgical efficiency during ureteroscopic lithotripsy. This study seeks to determine if reverse Trendelenburg (RT) positioning during ureteroscopic lithotripsy effects rates of stone retropulsion in patients with ureteral stones.
Methods: We prospectively recruited adult patients with radiographic evidence of a single ureteral stone and plans to undergo ureteroscopic lithotripsy. Patients were randomized to one of two positioning cohorts: standard supine dorsal lithotomy or dorsal lithotomy with RT position. In all cases in which retropulsion occurred, flexible ureteroscopy/pyeloscopy was performed to retrieve residual stone fragments. The primary endpoint of the study was any amount of stone retropulsion. Secondary endpoints were stone retropulsion into the kidney, stone free status, and post‐operative hydronephrosis.
Results: To date, 91 patients have completed the study; 44 in the standard positioning group and 47 in the RT group. There were no significant differences between groups in age, gender, ASA score, BMI, stone location and stone composition at the time of ureteroscopy. In the RT group, retropulsion occurred significantly less often (9.0% of cases vs 63.8% of cases; odds ratio (OR) 0.06, p < 0.001). Similarly, in the RT group, retropulsion to the kidney occurred less often (6.8% of cases vs 34% of cases; OR 0.15, p = 0.001). Among the patients with adequate follow up imaging to assess for stone free status (74 patients) and hydronephrosis (65 patients), there were no significant differences betwe
Conclusions: Reverse Trendelenburg positioning during ureteroscopic lithotripsy decreases both retropulsion in general, and retropulsion into the kidney. There was no significant impact on stone free status or post‐operative hydronephrosis, which was likely secondary to our routine use of flexible ureteroscopy/pyeloscopy to retrieve any retropulsed fragments. The use of the RT position has the potential to decrease operative time, decrease the need for use of extra equipment, and potentially improve stone free rates in practice setting in which flexible ureteroscopes are not routinely available.
Comparative effectiveness of empiric preventative pharmacologic therapies on stone recurrence among patients with urinary stone disease
R Hsi, P Yan, J Crivelli, V Shahinian, JM Hollingsworth
Vanderbilt University School of Medicine
Introduction & Objective: Given recent studies that show similar recurrence outcomes among patients with urinary stone disease regardless of whether 24‐hour urine testing is evaluated prior to initiating preventative pharmacologic therapy (PPT), some have argued for an empiric approach. However, it remains unknown whether any of the PPT medication subclasses is more beneficial than the others. In this context, we compared the frequency of stone‐related events among patients receiving thiazides, alkali citrate, and allopurinol without prior 24‐hour urine testing.
Methods: Using medical claims data from working‐age adults with a diagnosis of urinary stone disease (2008 to 2017), we identified those with a prescription fill for a PPT agent—a thiazide diuretic, alkali therapy, or allopurinol. We excluded those who received 24‐hour urine testing prior to initiating PPT (i.e., selective therapy) and those with less than 3 years of follow‐up data. We then fit multivariable regression models to estimate the association between the occurrence of a stone‐related event (emergency department visit, hospitalization, or surgery) and PPT medication subclass.
Results: Our cohort consisted of 550 (17%), 639 (20%), 1,819 (57%), and 203 (6%) patients who were empirically prescribed allopurinol, alkali citrate, thiazides, or combination therapy, respectively. After controlling for patient factors including medication adherence and concomitant conditions that increase recurrence risk, we found that thiazide therapy (versus allopurinol) was associated with lower odds of a stone‐related event (odds ratio, 0.68; 95% confidence interval, 0.52 to 0.88). No such association existed for alkali citrate therapy (versus allopurinol) or for combination therapy (versus thiazide monotherapy). Put differently, the predicted probability of a stone‐related event among patients prescribed thiazide therapy was six and six percentage points lower at three years of follow‐up than that for those prescribed alkali citrate and allopurinol, respectively (Figure).
Conclusions: Empiric PPT with thiazides is associated with significantly lower odds of subsequent stone‐related events. When 24‐hour urine testing is unavailable, these data suggest that thiazides should be considered first for empiric PPT.
Initial experience of miniaturised PCNL with Swiss LithoClast® Trilogy: a European multicentre prospective study on behalf of ESUT
N Thakare, F Tanse, K Saeb‐Parsy, N Atassi, R Endriss, G Kamphuis, D Perez‐Fentes, M Hasan, M Brehmer, PJ Osther, HU Jung, BW Turney, W Finch, N Burgess, S Irving, L Dragos, E Liatsikos, T Knoll, V Cauni, O Wiseman
Cambridge University Hospitals Nhs Trust
Introduction & Objective: The Swiss LithoClast® Trilogy has demonstrated high efficiency in stone clearance. Recent studies show that the miniaturised PCNL (mPCNL) technique can achieve comparable stone free rates to standard PCNL (sPCNL), even for larger stones, and is safe. Published data for LithoClast® Trilogy shows clearance efficiency of 370.5 ± 171 mm3/min for mPCNL and 590.7 ± 250 mm3/min for sPCNL. We report our European multicentre initial experience of the efficacy and safety of Trilogy for mPCNL using track size 20F or less and compare it to the outcomes for track sizes over 20F.
Methods: Data was prospectively collected from 10 European centres, evaluating the efficiency and safety of LithoClast® Trilogy, in a non‐randomized trial. Objective measures of stone clearance, device malfunction and complications were assessed. Each surgeon evaluated subjective parameters, including ergonomic and device effectiveness, for each case, on a 1‐10 scale (10 = extremely ergonomic/effective), and compared it to their usual lithotrite on a 1‐10 scale (10 = extremely effective).
Results: 24 out of 157 Trilogy PCNL cases were performed using the miniaturised technique (58% male, 42% female; mean age 50 years, range 13 ‐ 82 years). Median track size was 17.5F (range 8.7 ‐ 18F) and median probe size was 1.5mm (range 1.1 ‐ 1.9mm) for mPCNL. Stone characteristics were mean crosssectional area = 264.67 mm2 (range 37.68 ‐ 1047.19), 3D volume = 1847.84 mm3 (range 263.76 ‐ 5097.35) and HU = 896.55 (lowest 610.42 and highest 1102.88). Mean stone clearance rate was 46.80 mm2/min (vs 69.06 mm2/min for sPCNL), or 274.17 mm3/min (vs 1071.05 mm3/min for sPCNL) based on calculated 3D stone volume. Stone free rate on fluoroscopy for mPCNL at end of the case was 88% (vs 82.6% for sPCNL). Surgeon feedback for ergonomic score was 7.3 (mean), the least satisfactory element. Feedback for suction effectiveness was 7.8, with 8.3 for combination effectiveness and 8.1 for overall effectiveness compared to lithotrite most commonly used previously. 2 (8.3%) cases experienced probe breakage, none of which required using a different device. No major complications (Clavien Grade >or = III) were reported.
Conclusions: This multicentre prospective study has demonstrated that LithoClast® Trilogy is highly effective and safe for miniaturised PCNL and has high user satisfaction. The efficiency of stone clearance is lower for mPCNL when compared to LithoClast® Trilogy for sPCNL in our series, which is to be expected given the smaller probe size, but similar to that for other lithotrites.
Some pulse types are more equal than others: A comparison of different pulse modulation modes for Holmium:YAG laser lithotripsy ablation in a benchtop model
RS Terry, D Ho, D Scialabba, P Whelan, R Qi, C Tabib, F Soto‐Paulo, B Ketterman, GM Preminger, P Zhong, M Lipkin
Duke University
Introduction & Objective: It is widely recognized that varying Holmium:YAG (Ho:YAG) laser parameters such as pulse energy, frequency, and duration can impact laser lithotripsy ablation efficiency. In 2017, Lumenis introduced Moses™ Technology which uses pulse modulation to enhance the delivery of energy from fiber to stone and to minimize retropulsion. Since the introduction of Moses™ Technology, other companies have brought additional pulse modulation concepts to market. The purpose of this in vitro study is to compare the pulse characteristics and stone ablation efficiency of Lumenis' Moses™ Technology with Quanta's Vapor Tunnel™.
Methods: Submerged BegoStone phantoms were systematically ablated using either the Lumenis MOSES™Pulse 120H or the Quanta Litho 100 clinical laser system. Two pulse energies (0.4J and 1J), three fiber‐stone standoff distances (0.5, 1, 2mm), and all available pulse duration and modulation modes for each laser were tested in combination. The fiber speed was adjusted to scan across the stone surface at either 1 pulse/mm or 10 pulses/mm to form single pulse craters or an ablation trough, respectively. Volumes of single craters and 1 mm trough segments were imaged and quantified using optical coherence tomography.
Results: Ablation volumes increased with higher pulse energy and shorter standoff distance. Among pulse modulation modes, Moses Distance was superior at 0.5mm in all testing and at 2mm in trough testing. Vapor Tunnel was superior in 2mm single crater testing and demonstrated similar crater depth at all distances. Quanta Long Pulse was the only modality at 0.4J that had an ablation volume at 2mm. All modulated pulses performed similarly at 1mm.
Conclusions: In this benchtop model of laser lithotripsy, stone ablation was significantly impacted by pulse type. Moses Distance demonstrated superior or non‐inferior stone ablation at all tested parameters. Vapor Tunnel maintained its efficacy the best as standoff distance increased.
Reducing the incidence of unnecessary negative ureteroscopy with pre‐operative computed tomography for ureteric stones ≤7 mm
R Peggs, S Vaggers, T Tien, L Crabtree, S Folkard, K Atalar, Y Khan, S Graham, P Pal
Homerton University Hospital NHS Foundation Trust
Introduction & Objective: Patients with ureteric calculi listed for ureteroscopy (URS) may pass their stone spontaneously while they wait for their surgery. The probability of spontaneous stone passage is dependent on a number of factors including stone size, shape and location. The rate of negative URS (where no stone is found) is estimated to be 10%. Complications of URS include infection, bleeding, ureteric injury, ureteric stricture formation and anaesthetic risk.
We aim to see if a pre‐operative repeat CTKUB in asymptomatic patients with ureteric stones ≤7mm can reduce the rate of negative URS.
Methods: A retrospective study was performed which included all patients with ureteric calculi on waiting for URS from February 2017 to September 2017. Data on age, stone size and location, completion of CT KUB within 1 week of surgery, and negative pre‐surgical CT KUB or URS were collated. This method was repeated for two further re‐cycles to include the periods July 2018 ‐ March 2019 and June 2019 ‐ September 2019.
Results: A total of 42 patients were listed for URS in the initial cycle, with an additional 41 patients included in the first re‐cycle. Average age was 67.48 (SD 14.49) and average stone size 7.16mm (SD 2.84). The average spontaneously passed stone size was 5.89mm (SD 1.92mm) with the largest being a proximal 8mm stone. For stones ≤7mm there was a 32.65% rate of spontaneous stone passage compared to 12.50% for stones >7mm. A further 25 patients were included in the second re‐cycle.
Patients with stones >7mm were hereafter excluded. The percentage of patients scanned within 1 week of surgery increased across the three cycles (16.67%, 37.04%, 50.00%) and the incidence of negative URS reduced (11.90%, 7.14%, 4.00%). The percentage of operations cancelled following negative CT KUB was 9.52%, 9.76% and 16.00% in the 1st, 2nd and 3rd cycles respectively. In this study, CT KUB produced an average radiation dose of 9.98 mGy compared to 4.13 mGy for a negative URS.
Conclusions: Increased use of CT KUB in patients with ureteric calculi measuring ≤7mm reduced the incidence of unnecessary negative URS and thereby avoids complications and saves money. Although standard CT KUB produces higher radiation doses than negative URS, low dose CT KUB (< 3.50 mGy) are becoming increasingly common and should be considered.
Impact of various refinements on a longitudinal 18 years consecutive series of percutaneous nephrolithotomy
H Hertzberg, Z Savin, I Masarwe, A Beri, O Yossepowitch, M Sofer
Introduction & Objective: Although practiced already for 45 years, percutaneous nephrolithotomy (PCNL) is still in course of modelling. This study analyses the impact of various refinements on the outcome of PCNL in a longitudinal, consecutive large series of patients.
Methods: All 1160 PCNLs files treated in our institution between 2002‐2020 were retrospectively reviewed. Refinements in the technique were analysed for their influence on the intra and postoperative outcome. The influence of each modification was defined by comparison to the outcome of PCNLs treated before its implementation. The relevant chosen criteria included operating time, complications, hospital stay, stone clearance rate (mm3 of stone divided by minutes of operation), urine leakage from the access site, opiate consuming, back to work time and number, supracostal and upper calyx accesses.
Results: The refinements implemented in this series and their consequences are presented in the table.
Conclusions: This 2 decades series reveals that PCNL is still evolving. In our opinion, the most significant refinements along this series were the glue sealing and the tubeless approach that reduced the hospital stay to 1 day and the supine and ECIRS approaches that brought tremendous ergonomic improvements and made obsolete the need for upper calyx or multiple accesses.
Efficacy and safety of fluoroless ureteroscopy and retrograde intrarenal surgery for the treatment of urolithiasis: a comparative study
C Laranjo Tinoco, A Coutinho, A Cardoso, R Matos Rodrigues, S Anacleto, P Passos, E Lima, M Cerqueira Alves, P Mota
Hospital de Braga, EPE
Introduction & Objective: Ureteroscopy (URS) and retrograde intrarenal surgery (RIRS) are minimally invasive procedures frequently used for the treatment of urolithiasis. Traditionally, these procedures are guided by fluoroscopy, but the risks of exposure to ionizing radiation may present a matter of concern both for patients and urologists. The aim of this study is to evaluate the efficacy and safety of fluoroless URS and RIRS compared with conventional fluoroscopy‐guided procedures for the treatment of ureteral and renal stones.
Methods: Patients submitted to URS or RIRS for urolithiasis between August 2018 and December 2019 were retrospectively evaluated and split in two groups, according to the use of fluoroscopy. A subgroup analysis by type of procedure and a multivariate analysis to identify predictors of residual stones and postoperative complications were conducted.
Results: 231 patients met the inclusion criteria: 120 (51.9%) submitted to fluoroscopy and 111 (48.1%) with a fluoroless technique. No significant differences were found between groups regarding stone‐free rate (82.5% vs 90.1%, p = .127), postoperative complication rate (35.0% vs 31.5%, p = .675) and complications' grade (p = .981) (Table 1). In the subgroup analysis these variables did not present significant differences, regardless of the procedure considered (Table 2). In the multivariate analysis the fluoroless technique was not a significant predictor of residual lithiasis (p = .983), when adjusted for procedure type, stone size and stone number (Table 3).
Conclusions: Results suggest that both URS and RIRS can be done with no fluoroscopy in selected cases without affecting the efficacy or safety of the procedure.
A Nomogram for Prediction of the Risk of Kidney Stone: A physical examination population‐based Study
H Qibo, J xi, t huairong, H Yan, W Kunjie
Introduction & Objective: Urolithiasis is one of the most common diseases in Urology. The incidence of kidney stones grows rapidly these years, which not only brings pain to patients but also causes a huge economic burden to society. Thus, this study aims to develop and verify an effective kidney stone prediction model in patients undergoing health examination.
Methods: A retrospective analysis was performed on 19,920 consecutive physical examination subjects from January 2018 to January 2019 in the Health Examination Center of West China Hospital of Sichuan University. A total of 440 patients with the first stone episode were enrolled voluntarily for this study. Preliminary screening of risk variables was performed by univariate analysis and LASSO regression. The risk variables were substituted into various predictive regression models (ENet, kNN, LDA, LASSO, Logistic, RF, Ridge, and SVM), and the average AUC values of each model were compared and analyzed to select the optimal model, which was then visualized by a nomogram. The performance of the nomogram was evaluated by internal and external verification.
Results: Among the 440 patients, 68.9% (303) were males and 31.1% (137) were females. The median age was 47 years (interquartile range: 39,55). Univariate and LASSO analysis results showed that gender, fasting blood glucose, serum albumin, liver function indicators, renal function indicators, leucocyte level, blood pressure, Body Mass Index, Waist‐to‐Hip Ratio were identified as significantly associated factors that could be combined for accurate prediction of Urolithiasis. The Logistic regression model showed the best discrimination, with an area under curve of 0.758. The calibration curves of the internal and external verification showed the nomogram was well‐calibrated.
Conclusions: Our nomogram was effective in the preliminary prediction of kidney stones in the physical examination population.
Does the Use of Moses Technology Increase Efficiency During Flexible Ureteroscopy for Stone Disease? Single Center Experience
MA Knoedler, S Li, SL Best, SP Hedican, KL Penniston, SY Nakada
University of Wisconsin, Department of Urology
Introduction & Objective: The objective of this study was to evaluate the efficiency of Moses technology compared to the regular mode during flexible ureteroscopy for stone disease. Moses technology has been shown to improve stone fragmentation both in vitro and in vivo, but it is unclear if this translates into improved efficiency in the operating room.
Methods: An IRB approved database of patients with upper tract stones was analyzed for ureteroscopies from January 1, 2020 to December 31, 2020. Patients who underwent flexible ureteroscopy with the Lumenis Pulse P120H holmium laser system with the regular or Moses mode were included. Patient characteristics including age, gender, BMI, diabetes, hypertension, gout, chronic urinary tract infection, chronic kidney disease, bowel disease and cumulative stone size were evaluated. Outcome measures included procedural time, laser time, total energy used, laser efficiency (laser time per stone size), complication rate and stone free rate. Univariate analysis with chi squared and MANCOVA controlling for cumulative stone size and co‐morbidities were performed. Patients were excluded if they had a staged procedure.
Results: Of the 200 surgical cases, 184 met the inclusion criteria. Moses was utilized in 114 cases and the regular mode in 70 cases. There was no difference in the cumulative stone size between the Moses and regular mode (11.6 ± 7.4 vs 10.5 ± 8.4 mm, p = 0.314). Procedural time (44.5 ± 33.6 vs 38.5 ± 23.8 min, p = 0.282), laser time (7.3 ± 11 vs 6.6 ± 8.2 min, p = 0.927), total energy used (4.9 ± 6.7 vs 3.7 ± 4.9 kJ, p = 0.373), and laser efficiency (4.7 ± 6.5 vs 5.5 ± 9.8 mm/min, p = 0.501) were also similar between the two groups. Complications (6.1% vs 5.7%, p = 0.906) and stone free rates (67.4% vs 70.4%, p = 0.712) did not differ between the two.
Conclusions: At our institution, Moses technology did not demonstrate a significant change in procedural time, laser time, total energy used or laser efficiency. Moreover, there was no difference in complications or stone free rate. There may be other technical benefits to Moses technology not captured in this analysis.
Continued Aspirin Use during PCNL Surgery
H Brar, P Orji, S Agrawal, M Eila, J Fulla, B Li, P Prasanchaimontri, J Li, S De
Cleveland Clinic
Introduction & Objective: Percutaneous nephrolithotomy (PCNL) is recommended as the first line surgical treatment for kidney stones >2 cm. Due to potential bleeding complications, antiplatelet and anticoagulant therapy are considered relative contraindications and should be discontinued prior to PCNL per the American Urological Association (AUA) guidelines for surgical stone management. However, there is also concern regarding increased cardiovascular risk with peri‐procedural withdrawal of aspirin. We aimed to evaluate the intra‐ and post‐operative outcomes and complications in patients on chronic aspirin therapy who underwent PCNL, with and without discontinuation of aspirin.
Methods: We retrospectively identified all patients on chronic aspirin therapy who underwent PCNL at our institution between January 2014 and May 2019. Patients were classified based on whether they continued or discontinued aspirin >5 days preoperatively. Patient demographics were collected including comorbidities, American Society of Anesthesiologists (ASA) scores, indication for aspirin, BMI, and stone characteristics. Change in hemoglobin was primarily assessed with a univariate logistic regression. Secondary outcomes included estimated blood loss (EBL), need for transfusion, change in creatinine, length of stay (LOS), complications, 30‐days re‐admission rates, and 30‐day emergency room (ER) visits. Factors associated with continued aspirin use were assessed with univariate and then multivariate logistic regression models.
Results: 326 patients on chronic aspirin therapy underwent PCNL in the study time period. 86 and 240 patients were classified as continued and discontinued aspirin, respectively. Between the two groups, there were no statistically significant differences in change in hemoglobin, EBL, rates of transfusion, change in post‐operative creatinine, 30‐days re‐admission rate, complications, or 30‐days ER visits. Patients who continued aspirin did have a longer LOS (1.6 vs 1.88 days, p = 0.046). Variables associated with continued aspirin use included ASA score of 3 (OR 3.47, p = 0.011, 95% CI [1.43‐9.78]), ASA score of 4 (OR 5.14, p = 0.007, 95% CI [1.71‐18.21]), smoking history (OR 1.99, p = 0.026, 95% CI [1.06‐3.71]), and cardiac stent as an indication for aspirin use (OR 7.32, p = 0.003, 95% CI [1.06‐3.71]). A BMI ≥30 was associated with aspirin discontinuation (OR 0.36, p < 0.001, 95% CI [0.21‐0.61]).
Conclusions: Our data suggest perioperative aspirin use may not result in increased bleeding in some patients undergoing PCNL. However, larger prospective studies are needed for further evaluate this question.
PerCutaneous Nephro‐ Lithotomy (PCNL): Minimum Hospital volume required to achieve financial sustainability in the UK
A Jha, C Ho, L Simmons, N Collin, J Philip
Bristol Urology Institute
Introduction & Objective: As set out in the Health and Social Care Act 2012, the national tariff covers the pricing of healthcare services provided for the purpose of the NHS[1]. The current tariff for patients with low complexity and co‐morbidity score is set at £3788 whilst more complicated cases are set at £4351.
Previous studies have investigated the relationships between case volumes and outcomes in PCNL with some studies demonstrating high volume centres achieving better results. However there is little evidence or studies demonstrating the cost benefit in higher case volume centres.
We aim to investigate the relationship between case volume and cost benefit based on data from a large tertiary centre in the UK.
Methods: The cost calculation was performed by adding up (i)disposable/ single use items, (ii) reusable equipment used during a standard PCNL procedure, (iii) estimated cost of personnel (theatre staff, surgeon, radiologist, radiographer and anaesthetist) per session and (iv) cost of bed day at our unit over 5 year period. However, the costs for estate/facility are excluded in this study as this varies significantly across different units.
Results: The total cost for disposable equipment and medication is £1814.2 per case. The total cost for reusable equipment (over 5 years) is £34580.58. This includes the nephroscope, intracoporeal Lithotrite and the Lithotrite machine. The average cost per bed day in the NHS is £222. Estimated personnel cost totals £950/ session. The average length of stay (LOS) for PCNL in the NHS is 4 days for complex cases and 3 days for uncomplicated cases. An average LOS of 3.5 days is used to re‐present the case mix that most centres treat and an average is taken of the 2 tariffs amounting to a payment of £4069.5 per case.
Conclusions: Over a 5‐year period, each centre would require to perform 66 PCNL cases in order to maintain financial sustainability i.e.: that is over 13 cases per year. As this does not take into account the overhead costs and cost for infrastructure, the actual number of cases that is required to achieve financial balance could be higher and we estimate that to be around 20 cases/year.
Kidney Stone Surgical Interventions: Nationwide Interest Trends and Qualitative Assessment of Popular Resources on Social Media from 2016‐2021
P Diaz, RA Takele, S Thaker, KN Thaker, J Ballon, KB Scotland
Department of Urology, UCLA
Introduction & Objective: Patients with kidney stones have traditionally relied on their urologists for information on surgical management. As technology advances and online resources become more accessible, patients may often scour the internet for answers before consulting their physicians. We sought to evaluate online interest in kidney stone surgical interventions and assess the quality of the most popular resources on social media.
Methods: Google Trends was used to evaluate public interest in different kidney stone interventions over a 5‐year period between March 2016‐February 2021 and reported as search volume index(SVI). SVI is defined as the frequency of keywords used on the entire Google search engine relative to total search volume in a given time period ranging from 0‐100. Next, BuzzSumo, a social media analysis tool, was used to identify the most popular stone surgery content on various social media platforms over the same 5‐year period. Finally, to evaluate the quality of health information present in the most popular articles online, three individual raters used the DISCERN instrument. Quantitative data were examined by Analysis of Variance (ANOVA).
Results: The top three search terms related to kidney stone surgical interventions on Google Trends were identified as Ureteroscopy(URS), Percutaneous Nephrolithotomy (PCNL) and Extracorporeal shock wave lithotripsy(ESWL) with mean SVI's of 47.75, 42.98, and 45.74 respectively (all p < 0.012). The 9 articles chosen for analysis (Figure 1) were examined using the DISCERN tool and had a mean score of 2.82 with no statistically significant difference among evaluators. Thus, article quality fell below the DISCERN threshold of 3.0 required to be considered “Moderate Quality”.
Conclusions: Our research suggests that of the various stone surgery interventions, patients are most interested in ureteroscopy, but engaged more often with content related to PCNL on social media platforms. This indicates there may be a discrepancy in what patients want and what information is available. The low quality of articles popular on social media pertaining to kidney stone surgical interventions highlights the need for involvement of urologists in the creation of engaging high‐quality content and accurate information sharing in a social media‐driven society.
How to evaluate a flexibleureterorenoscope? Systematic mapping of existing evaluation methods
N Hendriks, MM Henderickx, BM Schout, J Baard, FS van Etten‐Jamaludin, HP Beerlage, RC Pelger, GM Kamphuis
Amsterdam UMC
Introduction & Objective: Since the inroduction of flexible ureterorenoscopes in the 1970's, efforts have been made to reduce size, including working channel and space for digital optics, whilst introducing numerous accessory instruments, bidirectional deflecting tips and constant improvement in image quality. In the attempt to serve these seemingly conflicting interests, ureterorenoscopes have become fragile. This study systematically identified and reviewed scope‐related and user‐related parameters used to evaluate the quality of flexible ureterorenoscopes to identify key items and variability in grading systems.
Methods: A literature search of five databases (MEDLINE (Pubmed), Embase (Ovid), Web of Science, Google scholar and the Cochrane Library) was performed according to the PRISMA‐guidelines enclosing articles published up to August 2020. A total of 2386 articles were screened.
Results: A total of 48 articles were included in this systematical review. All studies had a prospective design. Five key items in the assessment of flexible URS were distinguished Maneuverability (87.5%), Optics (64.6%), Irrigation (56.3%), Handling (39.6%) and Durability (35.4%). After regrouping, every key item could be divided into specific subcategories. However, the quality‐assessment showed a wide variation in denomination, method of measurement, circumstances of measurement, tools used during measurements, number of measurements performed, number of observers and units of outcomes.
Conclusions: The research field regarding quality assessment of ureterorenoscopes is extremely heterogeneous. In this systematic review we identified five key characteristics (Maneuverability, Optics, Irrigation, Handling and Durability) used to grade flexible ureterorenoscopes. However, within these categories there was tremendous heterogeneity in terms of method of measurement. Therefore, a systematic, uniform grading tool to assess the quality of flexible ureterorenoscopes is desperately needed to structure outcomes and facilitate comparison in future studies.
Efficiency and Effectiveness for Ureteroscopic Stone Removal: Dual Lumen vs a Single Lumen Ureteroscope
A Brevik, A Peta, L Limfueco, R Karani, L Xie, R Arada, J Sung, FA Jefferson, E Parkhomenko, D Lama, S Safiullah, P Jiang, RM Patel, RV Clayman, J Landman
Department of Urology, University of California, Irvine
Introduction & Objective: Improved irrigant flow characteristics of the dual lumen flexible ureteroscope (DLFU) (Richard Wolf, Knittlingen, Germany) have been reported since its introduction in 2010; however, no studies have evaluated whether the DLFU results in a more efficient or effective urolithiasis procedure than a single lumen flexible ureteroscope (SLFU).
Methods: Seventy‐nine patients undergoing ureteroscopy between 2016‐2020, for a proximal ureteral or renal stone burden ≤ 2 cm were randomly assigned to a SLFU or DLFU. Ureteroscopy, laser lithotripsy and stone basketing times were recorded. Primary outcomes were procedural efficiency (i.e., ureteroscopy time and rate of stone clearance (mm3/min)) and procedural effectiveness (i.e., absolute (no stones) and relative (≤ 4 mm fragments) stone free rates) based on a post‐operative CT scan completed within six months of surgery. For patients with accessible pre‐operative and post‐operative CT imaging, stone volumes were calculated using a 3D Slicer program. Statistical analysis was performed with R package.
Results: Demographics and stone characteristics were similar between the SLFU and DLFU groups (Table 1). With a median follow‐up of 50 days (range 1‐168 days), the absolute and relative stone free rates were 48% and 77% in the DLFU group compared to 26% and 63% in the SLFU group (p = 0.045 and p = 0.161), respectively; ureteroscopy time was similar for SLFU and DLFU (p = 0.984); however, in cases requiring laser lithotripsy, the lasing time was more than doubled in the SLFU group (2 min, 6 min; p = 0.017). Among 57 patients with pre‐operative and post‐operative CT images, the median rate of stone clearance was 7.1 mm3/min for the DLFU group and 3.7 mm3/min for the SLFU group (p = 0.025) (Table 2).
Conclusions: Among patients with proximal ureteral or renal stones ≤ 2 cm, DLFU was associated with a more efficient (i.e. stone clearance rate) and more effective (i.e. absolute and relative stone free rate) procedure than SLFU.
Moderated Poster Session 19: Stents & Equipment II
Technical trips and tricks for preserving a flexible ureteroscope during 270 interventions
PA Geavlete, R Multescu, C Ene, C Bulai, BF Geavlete
“Saint John” Emergency Clinical Hospital, Department of Urology
Introduction & Objective: In the last years, flexible ureteroscopy (fURS) has become a viable option for the treatment of renal stones because of its high stone‐free rates (SFRs) and low morbidity. Our objectives were to describe surgical technique (tips and tricks) for fURS, in order to preserve a digital flexible ureteroscope during over 200 procedures.
Methods: A retrospective analysis of 210 consecutive patients of which were performed 270 interventions of fURS (using one flexible ureteroscope) between March and October 2017. The ureteroscopy and laser lithotripsy were done using a standardized technique with an Olympus URF‐V2 flexible ureteroscope.
Results: The mean overall stone size was 17.3 ± 7.2 mm. Ureteral access sheath placement was possible in 203 patients (96.6%). At 1‐mo follow‐up, the overall primary SFR was 80%; the secondary and tertiary SFRs were 84.7% and 91.9%, respectively. The mean operative time was 72.1 ± 23.6 min. Complications were reported in 57 patients (27.1%) overall, with Clavien grade 1 in 37 patients, grade 2 in 12 patients, grade 3 in 8 patients and none grade 4 and 5 complications. The flexible ureteroscope had one major repair of the sheath during all the procedures. In order to gain these outcomes, it is essential to properly prepare the patients, select the type of laser and laser settings. The smallest laser fibers are encouraged to be used due to the fact that scopes will be needed to deflect into the lower pole to manage the stone, the optimal fiber size being <275 microns. The patients must be operated under general anesthesia; this will allow the surgeon and the anesthesiologist to control the patients breathing to limit the stone move during fURS. If the stone type allows the stone to be dusted, lower laser setting must be used. Ureteral access sheath must be used at all times to reduce the pressure in the kidney and increase the life of the ureteroscope. Pre‐stented cases helped to a better ureteral access. Additionally, this will help to clear the stone by facilitating the stone passage towards the lower pressure in the sheath.
Conclusions: The fURS procedure is safe and effective for the treatment of renal stones. Respecting some preoperative and operative steps, a large number of procedures could be achieved using the same device.
Using the Quick Sequential Organ Failure Assessment Score to Predict Septic Shock after ureteral stenting for patients with ureteral stone and presumed urinary tract infection
JY Lee, C Kottooran, A Yaghoubian, N Uppaluri, K Hanson, M Borofsky, B Eisner
University of Toronto
Introduction & Objective: Recent studies have proposed that the Quick Sequential Organ Failure Assessment (qSOFA) score may better predict septic shock than the traditionally used Systemic Inflammatory Response Syndrome (SIRS) Criteria. The purpose of the current study was to compare qSOFA and SIRS criteria ability to predict septic shock in patients who present to the emergency department with an obstructing ureteral stone and concern for urinary tract infection.
Methods: An IRB‐approved retrospective review was performed at two institutions. All patients who met each of the following criteria during the time period from July 2016 to April 2020 were included in the study: emergency department visit with obstructing ureteral stone, concern for urinary tract infection documented in consultation note, and ureteral stent placement. The primary outcome of interest was the development of post‐operative septic shock defined by hypotension requiring vasopressor support for at least one hour. Patients who required vasopressor treatment prior to ureteral stenting were excluded from the analysis. All SIRS and qSOFA criteria were collected between the time of emergency room presentation to the time of stent placement.
Results: The study included 187 patients with a mean age of 58.8 ± 18 and gender distribution of 60% female: 40% male. 35 of 143 patients (18.7%) met the criteria for postoperative septic shock. SIRS criteria were met for 103 patients (55.1%) for the entire cohort and 30 patients who experienced septic shock. qSOFA criteria were met for 24 patients (12.8%) in the entire cohort and 18 patients who experienced septic shock. Specificity for postoperative sepsis was significantly higher for qSOFA than for SIRS criteria (75 vs 29.1%, McNemar test p < 0.001). Sensitivity was higher for SIRS criteria than for qSOFA (85.7 vs 51.4%, McNemar test p < 0.01). qSOFA criteria had a significantly higher positive predictive value than SIRS (89.6% vs. 29.1%) while negative predictive values were similar (89.6 vs. 94%).
Conclusions: qSOFA score demonstrated superior specificity and positive predictive value for post‐operative septic shock than SIRS criteria in this study, whereas SIRS criteria demonstrated superior sensitivity. qSOFA score may be a useful tool for emergency evaluation of patients who present with ureteral stone and urinary tract infection.
Delays in Ureteroscopy After Stent Placement Doubles the Cost of Treating Stone Patients
N Bhojani, R Paranjpe, B Cutone, S Rojanasarot, B Eisner
University of Montreal Hospital Center (CHUM)
Introduction & Objective: Delays in definitive stone treatment may be associated with inferior post‐operative outcomes and greater health care expenditure. The current study evaluates the effects of ureteral stent duration prior to ureteroscopy (URS) on health care utilization.
Methods: Two retrospective analyses were conducted using IBM MarketScan commercial data. Patients were included if they underwent URS within 6‐months of stent placement. Cohort 1 was comprised of patients who did not have a diagnosis of sepsis and pyelonephritis at the time of initial stent placement, whereas Cohort 2 was comprised of patients who did have a diagnosis of sepsis and pyelonephritis at the time of stent placement. The time to URS was calculated and categorized into two groups: ≤15 days and >15 days. Healthcare utilization included infectious complications (urinary tract infection, cystitis, pyelonephritis, sepsis), Emergency Department (ED) visits, inpatient stays, medical costs adjusted to 2020 USD, and were measured until 3‐months post‐URS. A logistic regression model and a generalized linear model with gamma distribution were conducted using Instant Health Data platform.
Results: Cohort 1 included 6,302 patients. Among this cohort, 42.32% patients underwent URS after 15 days of stent placement. Patients who underwent URS more than 15 days after stent were significantly associated with increased ED visits (OR = 1.31; p = 0.001), inpatient stays (OR = 2.15; p < 0.0001), infectious complications (OR = 1.72; p < 0.0001), and medical costs (OR = 1.40; p < 0.0001). Average medical costs in the >15 days group were significantly higher than ≤15 days group ($18,238 vs $12,712; p < 0.0001). Cohort 2 included 400 patients. Among this cohort, 57% patients had URS more than 15 days after stent placement.
Patients who underwent URS more than 15 days after stent placement were significantly associated with increased infectious complications (OR = 3.03; p < 0.0001), and medical costs (OR = 1.49; p = 0.001). Average medical costs in the >15 days group were significantly higher than ≤15 days group ($23,652 vs $12,806; p < 0.0001).
Conclusions: In this study, patients who underwent URS more than 15 days after ureteral stent placement were associated with increased risk of infectious complications, increased health care utilization and increased costs compared with patients who underwent URS within 15 days of stent placement.
Development of a New Canadian Endourology Group Stent Symptom Score (CEGSSS)
N Bhojani, JY Lee, SK De, AG Lantz, S Sivalingam, M Ordon, KB Scotland, S Andonian, BH Chew
University of Montreal Hospital Center (CHUM)
Introduction & Objective: Placement of a ureteral stent is a common urological intervention, and it is known that stents can significantly impact quality of life for some patients. The ureteral stent symptom questionnaire (USSQ) has been used since its development in 2003 but its length hinders its use in clinical practice. Therefore, we sought to develop a new, shorter, practical and validated tool.
Methods: We sought to create a new quality of life questionnaire using a 2 phase schema:
Phase 1: Using the USSQ as a starting point, a team of 9 Canadian Endourology Group (CEG) members and 21 patients evaluated the items of each section of the USSQ to determine its importance and relevance in assessing symptoms associated with a ureteral stent. Face‐to‐face meetings were used to rate each item using a Likert scale (1 to 5). All accepted items were then evaluated using experts' consensus. Five rounds of consultations were necessary to achieve the final CEGSSS.
Phase 2 (Pilot trial): Patients undergoing stent placement completed the newly developed CEGSSS in addition to a short survey evaluating the tool itself. Five rounds of 5 patients, with modifications of the CEGSSS based on feedback after every round was anticipated.
Results: Phase 1: After consultation with patients and CEG experts, items were accepted if the mean patient or expert rating was ≥4.0 (out of 5) with a SD of ≤0.75. Questions with mean patient or mean expert ratings of ≥4.0 but SD ≥0.75 were flagged for discussion. Those items that did not meet these requirements were rejected. In addition, those items with divergent results between experts and patients were also discussed to ensure that the final version of the CEGSSS was representative of the objective. The final CEGSSS contains 15 questions divided into 3 domains: Urination (8 questions), Pain (3 questions) and Quality of Life (2 questions).
Phase 2: 16 patients were recruited. After 3 rounds of patient feedback, no new feedback was received and therefore this process was deemed complete (Table 1). Median time to complete the questionnaire was 7 minutes (2‐20minutes). 2/16 patients required assistance to complete the questionnaire, but all patients rated it as easy to navigate. Mean level of difficulty was 1.75 (out of 5).
Conclusions: Through a process of expert and patient consultation and a pilot trial with patients receiving a ureteral stent, a new stent symptom questionnaire was developed that is both short, easy for patients to understand and clinically relevant. The next step will be external validation of the newly developed CEGSSS.
Reusable Digital Flexible Ureteroscope vs. a Single‐Use Flexible Ureteroscope in the Treatment of Urolithiasis: An EDGE Consortium Prospective Randomized Clinical Trial
BE Knudsen, T Posid, MW Sourial, VK Wong, R Paterson, KL Stern, J Moore, MR Humphreys, BH Chew
The Ohio State University
Introduction & Objective: Flexible ureteroscopes are routinely used to treat kidney stones. Both single‐use and reusable models are available. The high cost of purchase and repair of reusable ureteroscopes has led to the development of single‐use options. This trial compared a single‐use digital flexible ureteroscope (LithoVue, Boston Scientific) to a state‐of‐the art reusable digital flexible ureteroscope (Flex‐Xc, Storz) in a multicenter, prospective randomized trial from the EDGE Group.
Methods: Patients were randomized across 3 sites to either the single use flexible ureteroscope (n = 53) or a reusable flexible ureteroscope (n = 49) (brand new at each site and used only for study cases). Ureteroscopies were performed using a standardized technique in patients with renal stone burdens ranging from 5‐20 mm. The reusable ureteroscope was used until it was damaged to the point that a major repair was required. Primary outcomes were stone‐free rate 6‐10 weeks post‐procedure and secondary outcomes included length of surgery, laser time, basketing time, deflection of scope at the beginning and end of the case, and a rating scale of scope handling.
Results: The mean age was 57.9 years (±13.2), 53.3% male, 73% Caucasian, and 77.6% non‐Hispanic or Latino. Upward and downward deflection was significantly better both at the beginning (p < 0.007) and end of the case (p < 0.001, Table 1) with LithoVue. Performance was comparable between scopes for all other intraoperative measures (Table 1). However, scope handling as rated by each surgeon favored the reusable ureteroscope for maneuverability (p = 0.004), visualization (p < 0.001), ability to target the laser on stone (p < 0.001), and overall scope rating (p < 0.001). There was no difference in stone free rate at 4‐10 days or 6‐10 weeks). The 3 reusable ureteroscopes failed and required a total of 5 repairs during the trial (2 each at OSU and Mayo, 1 at UBC) and averaged 6.6 uses before repair.
Conclusions: The LithoVue single‐use ureteroscope had better deflection angles pre‐ and post‐operatively when compared to the reusable digital Flex‐Xc. Surgeons preferred the reusable flexible ureteroscope handling and visualization, although both scopes produced similar stone free rates. The high rate of breakage of reusable ureteroscopes is concerning and the single‐use ureteroscope produced equivalent patient outcomes.
A Novel Visual ‐ Grading for Ureteral Encrusted Stents Classification (V‐GUES) to Help Decide the Endourologic Treatment
BO Manzo, P Alarcon, EE Lozada, J Ojeda, C Morales, I Mehmet, BH Chew, F Sepulveda, M Ignacio, E Flores, a Cagri, E Emiliani
Hospital Regional de Alta Especialidad del Bajío
Introduction & Objective: To propose a visual classification for encrusted stents to help to choose the appropriate endourologic treatment.
Methods: A multi‐center, retrospective and descriptive study was performed. A total of 140 patients with encrusted double J stents were collected from 5 different institutions. The novel Visual–Grading for Ureteral Encrusted Stents (V‐GUES) classification system goes from A to D, increasing the severity of encrustation.
Results: Encrusted stents could be removed with a single intervention in 112 patients (86.8%). Type A and B encrusted stents could be successfully removed in all patients (100 % success). Type D stents had minor retrieval and stone‐free rates (p = 0.006 and p < 0.0001, respectively). Stone‐free status was achieved after the first procedure in 89 patients (69%). Flexible ureteroscopy had a low success rate (77.7%) in type C stents (OR 0.21). Combined access had a 100 % success rate to retrieve type C encrusted stents and a 92.9% success rate for type D encrusted stents (OR 9.18). Type D stents were associated with more than one session needed to get the stent (OR: 0.11) and stones retrieved (OR 0.21).
Conclusions: The V‐GUES grading system is associated with treatment success rates of encrusted stents retrieval and stone‐free status. It is also associated with complications rate and the number of sessions needed to leave patients stent and stone free. The V‐GUES classification could help counsel patients about the best treatment options and their outcomes. Further prospective studies will be needed to provide external validation.
Withdrawn
Comparison of Tamsulosin, Tolterodine and their combination for the treatment of ureteral stent related symptoms: A Prospective, randomised, comparative study
N Reddy, S Vaddi, A Singh, A Ganpule, R Sabnis, M Desai
Muljibhai Patel Urological Hospital
Introduction & Objective: Stent related symptoms are a matter of significant concern among patients undergoing URS or RIRS. Various medications have been tried world over. In our study we intend,
• To study the efficacy of Tamsulosin, Tolterodine, and combination therapy of both the agents for the treatment of ureteral stent related symptoms.
• To study the effect of Tamsulosin with Tolterodine on pain and analgesic requirement in comparison with Tamsulosin and Tolterodine alone.
• To study the side effects of combination of Tamsulosin with Tolterodine.
Methods: This prospective, randomised, double blind study was conducted in the Department of Urology, Muljibhai Patel Urological Hospital, Nadiad, which included 180 patients who underwent URS/RIRS with DJ stent between August 2018 and January 2020. The patients were divided into three groups: Tamsulosin(Group A), Tolterodine (Group B) and Tamsulosin+Tolterodine(Group C). Stent related symptoms were assessed by VAS scores at Postoperative day 1(POD 1) and IPSS and VAS scores at fourth week before stent removal.
Results: The demographic profile (Age, Sex, comorbidity), operative parameters (Side of surgery, Stone size, location of stone, type of surgery) were all comparable between the three groups. IPSS and VAS pain score at fourth week were also comparable between the groups. The number of haematuria episodes and the analgesic requirement were comparable. All the three groups had comparable number of side effects, but there was significant association between the complications in the three groups (p = 0.039). Mainly, Dizziness was a significant complication in the Group A while dry mouth was a significant complication in Group B. All the side effects were tolerable in all the patients and none of them discontinued the treatment for these symptoms.
Conclusions: Tamsulosin, Tolterodine and the combination of these two drugs are effective and safe for the DJ stent related symptoms with manageable side effects. The combination of Tamsulosin and Tolterodine did not show any significant advantage over either of the monotherapies, though we observed that Tolterodine was as effective as Tamsulosin in alleviating the stent related symptoms. Thus, we recommend that Tamsulosin plus Tolterodine combination is not statistically better than Tamsulosin alone in alleviating stent related symptoms and that either of the monotherapy would be sufficient to alleviate the ureteral stent related symptoms.
Comparison of ureteric stent removal procedures using reusable and single‐use disposable flexible cystoscopes following ureteroscopy and lasertripsy: a micro cost analysis
T Hughes, A Pietropaolo, L Tear, BK Somani
Southampton University Hospital
Introduction & Objective: Flexible cystoscopy with with reusable or single use scopes allow safe and effective ureteric stent removal. However, reusable scopes require built ‐in stack system, endoscopy room and dedicated staff. Cancer diagnostic pressure on endoscopy suite can lead to delays in flexible cystoscopic stent removal. We wanted to compare the cost and organizational impact of reusable flexible cystoscope versus single use cystoscope in a tertiary care University Hospital.
Methods: Data for the reusable cystoscopic stent removal performed in endoscopy room, group A (period 1) were compared to single use flexible cystoscope with a built‐in stent grasper (Isiris®) performed in outpatient clinic, group B (period 2). We chose the same calendar months in successive years for these two different groups (9 months each). A micro cost analysis was performed evaluating the impact on costs, complications and organizational benefit.
Results: A total of 72 patients (37, group A; 35, group B) were analysed (Table 1). In group A, 5 patients (14%) developed stent encrustation, of which 3 needed a ureteroscopic removal subsequently. No complication occurred in group B. More staff on average were needed for procedures done in group A, than group B (p < 0.001). The relevant difference in cost and organizational impact is described in table 2.
Conclusions: Isiris significantly reduced stent dwell time, procedural time and staff needed to carry out the stent removals. It also allowed the procedures to be done in the outpatient setting thereby reducing the organizational pressure on endoscopy related diagnostic procedures.
Withdrawn
How to reduce ‘double‐firing’‐induced scope damage by investigating the relationship between laser fiber core degradation and fiber jacket burn?
S Ryang, T Ly, H Yoon, D Park, J Han, S Jeong, H Jung, S Cho
Introduction & Objective: 'Double‐firing effect' in which laser firing occurs in the fiber tip and its proximal part is caused by different breakdown rates between fiber jackets and cores. This study investigated a new safe distance concept to prevent scope damage by analyzing the breakdown of the laser fiber jacket and cores.
Methods: Laser fibers were fixed in a benchtop simulation model. The fiber tip was in contact with uniform phantom stones and submerged in saline. Four different energy settings (1.0 or 2.0J x 10Hz or 30Hz) and two different fiber sizes (200 μm and 365 μm) were tested. After three minutes of use at each energy setting, the length of fiber shortening and jacket burn were measured. The fibers were stripped to measure the length of core degradation.
Results: Mean degradation lengths were 4.2 to 7.8 mm. There was no statistical difference in the mean lengths of fiber core degradation and jacket burn. However, core degradation was longer than the jacket burn in half of the samples. The mean difference in lengths between core degradation and jacket burn was 0.49 ± 0.90 mm. Lengths of core degradation and the jacket burn were longer at the setting of high‐power energy and 200 μm fiber ‐ 2J with 30 Hz.
Conclusions: To reduce ‘double‐firing’‐induced damage, the authors recommend that laser fiber should be cut 1.0 mm longer than visible jacket burn at high‐power settings after 3‐min continuous fragmentation. After cutting the fiber, the laser should be checked whether ‘double‐firing’ is no more seen.
The new approach in the treatment of obstructive uropathy in pregnant women
SV Kotov, R Perov, PY Nizin
Pirogov Russian National Research Medical University (Pirogov Medical University)
Introduction & Objective:
• It is retrospective evaluation of short‐term selective drainage tactics in the treatment of pregnant women with obstructive uropathies (OUP). Comparison of the developed algorithm with the traditional approach–routine chronic drainage of the upper urinary tract (UUT) during gestation, which is accompanied by a significant decrease in the quality of life.
Methods: The retrospective analysis of the results of treatment of 248 pregnant women with OUP was performed. The inclusion criteria were a clinically significant urodynamic disorder of the UUT, not associated with urolithiasis, in combination with or without signs of a systemic inflammatory reaction. All patients underwent an examination: the collection of complaints, anamnesis, examination by an gynecologist, Doppler color scanning to determine the release of urine from the mouths of the ureters, laboratory tests. All patients signed an informed consent to participate in the study.
Results: The average age is 27.8 years(min‐17, max‐40). The average term is 21.6 weeks(min–5, max–35). The average leukocytosis‐13.9*109/l(min‐5.04, max‐26.8). Urine culture in 154(66%)‐sterile, in 71(30%)bacteriuria >103 CFU/ml). 2 groups: I–162 pregnant women with gestational pyelonephritis and UUT retention, II‐86 pregnant women with UUT retention without an inflammatory reaction. In group I, based on the presence of an outflow from the mouth of the ureter in 64(40%)‐conservative therapy (gestational pyelonephritis against the background of UUT dyskinesia without obstruction). Drainage was performed in 98 (60%) patients with gestational pyelonephritis with obstruction. 4 refusal of drainage‐conservative therapy. 4% patients underwent percutaneous puncture nephrostomy, but in most cases‐the installation of an internal ureteral stent. After 72 h of conservative therapy, the indications for drainage in 8(12%) were an internal ureteral stent. After stopping the inflammatory process and removing the drains, repeated drainage was performed in 12 patients(7.4%). In group II, conservative therapy was initially performed. After 72h, indications for drainage in 32(37%)–an internal ureteral stent. After removal, re‐drainage was required for 5(5.8%). According to Clavien‐Dindo:I degree of complications–7(5%), II–23(17%), IIIA–4(3%), IVA–4(3%). The average days of hospital stay were 4.2(min‐1, max‐15).
Conclusions: Tactics of routine drainage of pregnant women with OUP, most of the manipulations aren't justified. In turn, in most pregnant women with OUP, short‐term drainage is advisable, the risk of relapse of OUP doesn't exceed 7.4%, which is much less than the risk of developing stent‐induced complications.
Recurrent Benign Urethral Strictures Treated with thermo‐Expandable Metallic Stents : 2 years follow up (first African experience)
A Heddat, Y Houry, R Rabii
university Mohammed VI of health sciences UM6SS
Introduction & Objective: The urethral stent is a minimally invasive therapeutic means that opposes the forces of contraction of the urethral wound after an endoscopic urethrotomy or dilation.
The ideal stent should be inert, cause no symptoms, suitable for long‐term use and allow normal drainage without increasing sensitivity to encrustation.
Objective: to evaluate the medium‐term results of the placement of a heat‐expandable metal stent for recurrent urethral strictures.
Methods: a prospective study was carried out on 21 male patients who benefited from the placement of a thermo‐extensible urethral stent (polytetrafluoroethylene PTFE membrane‐covered self‐expandable metallic stent) the urethra after several attempts at endoscopic uretrotomy and / or urethroplasty. All patients were followed by retrograde urethro‐cystography, debimetry and bacteriological examination of the urine every 3 months for 18 months.
Results: The mean age of the patients was 53.4 years and the mean length of the narrowing was 2.1 (0.9) cm. The preoperative urine flow was 5.4 (4 to 8) ml / s. All but 2 tolerated the stent (9.5%), who experienced minimal discomfort. The postoperative urine flow rate was 17.4 (16 to 19) ml / s. 2 patients (9.5%) had a urinary tract infection, 4 (19%) had hematuria, 1 patient (4.7%) had an embedded stent, the stent migrated in one case (4.7%). After stent removal, one patient (4.7%) developed a recurrence of the stenosis. 12 patients had no complications.
Conclusions: The medium‐term results of the Uventa PTEF heat‐expandable stent show that it is an acceptable and reproducible minimally invasive procedure for selected patients with recurrent stenoses of the bulbar urethra. However, complications are described and a long‐term study seems necessary for a better evaluation.
Adoption of Single‐Use Flexible Cystoscopes for Outpatient Cystoscopy: A Micro‐Costing Analysis
ZT Su, M Huang, BR Matlaga, S Hutfless, K Koo
Mayo Clinic
Introduction & Objective: Single‐use flexible cystoscopes may confer clinical and workforce benefits. However, the potential impact on cost containment is not well‐characterized. We aimed to evaluate the total cost of outpatient flexible cystoscopy and assess the economic impact of adopting single‐use cystoscopes.
Methods: Cost data regarding the purchase, maintenance, and reprocessing of reusable cystoscopes were collected using a micro‐costing approach at a high‐volume outpatient urology clinic. We estimated the costs for facilities performing a range of annual procedure volumes (1,000‐3,000) using a fleet ranging from 10 to 25 cystoscopes. We also compared the total cost for cystoscopic ureteral stent removal procedures performed using single‐use vs. reusable devices.
Results: The per‐procedure cost associated with reusable flexible cystoscopes ranged from $105 to $224 depending on annual procedure volume and number of available cystoscopes devices (Figure). As a practice became more efficient by increasing the ratio of procedures performed to cystoscopes in the fleet, the proportion of the total cost due to cystoscope reprocessing increased from 22% to 46%. For ureteral stent removal procedures, the per‐procedure cost for reusable cystoscopes (range $165‐$1,469) was higher than for single‐use devices ($244‐$420), unless the annual procedure volume was sufficiently high relative to the number of reusable cystoscopes in the fleet (≥350 for a practice with 10 reusable cystoscopes, ≥700 with 20 cystoscopes).
Conclusions: The cost of reprocessing reusable cystoscopes represents the dominant component of the total procedural cost, especially at high‐volume centers. Adoption of single‐use cystoscopes appears to be most cost‐advantageous for stent removal procedures, especially for lower‐volume centers.
Clinical and postoperative characteristics of stentless ureteroscopy patients: a prospective analysis from ReSKU
R Unno, F Hamouche, H Yang, J Ahn, D Bayne, M Stoller, T Chi
University of California San Francisco
Introduction & Objective: The indications for placement of a ureteral stent after ureteroscopy for kidney stones remains an area of debate amongst urologists, where the benefit of post‐operative emergency visit reduction is weighed against the significance of stent related morbidity. We aimed to describe the clinical characteristics as well as the postoperative course of urolithiasis patients undergoing a ureteroscopy without stent placement.
Methods: This was a prospective case cohort study utilizing data collected in the Registry for stones of the Kidney and Ureter (ResKU), a stone registry that interfaces with the electronic medical record to record clinical data on urinary stone patients on an ongoing basis. We identified all consecutive patients undergoing ureteroscopy for stone disease at our institution between October 2015 and December 2020. We analyzed data encompassing demographics, medical history, intra‐ and post‐operative characteristics including complications and postoperative symptoms. Univariate and multivariate logistic regression analyses were performed based on the presence or absence of an indwelling ureteral stent.
Results: A total of 470 patients were included for analysis, 92 patients in the stentless group (19.5%) and 378 patients in the stented group (80.5%). Factors associated with stentless ureteroscopy were a lower stone burden (P < 0.001), the pre‐existence of a ureteral stent (38.9% vs 28.1% p = 0.004), absence of an access sheath (14.6% vs 69.5% P < 0.001) and a shorter operative time (31 vs 58 min p < 0.001). Post‐operative gross hematuria and lower urinary tract symptoms (LUTS) were reported less frequently in stentless patients (p = 0.02, p = 0.01, respectively). There was no difference in post‐operative complications between both groups (p = 0.385). On multivariate analysis, the risk of post‐operative complications was associated with obesity, stone burden≧1cm, and positive pre‐operative urine culture (Table 1). There was no patient who required emergent stent placement in the stentless group.
Conclusions: Our data shows that, in well selected patients, omitting ureteral stent placement after ureteroscopy can decrease post‐operative gross hematuria and LUTS without increasing post‐operative complications.
Ureteral Stents with a Larger Diameter show Higher Rates of Unplanned 30‐Day Encounters
L Elson, D Wong, J Vetter, C Nottingham, A Desai
Washington University St Louis
Introduction & Objective: Ureteral stents are routinely placed following ureteroscopic retrograde surgery (URS) to aid in urinary drainage post‐operatively. Up to 80% of patients, however, experience stent‐related symptoms (SRS), including pain and bothersome urinary symptoms. Previous studies have attempted to characterize the relationship between stent design characteristics and SRS. However, the correlation between characteristics such as stent diameter and SRS is conflicting. In this study, we assessed whether stent type and diameter were associated with unplanned encounters within 30 days after stent placement.
Methods: We performed a retrospective chart review on patients who received a unilateral ureteral stent following unilateral URS for treatment of nephrolithiasis between January 2016 and September 2019. Univariate and multivariable analyses were performed to evaluate for an association between stent design (company and diameter) and any unplanned encounters within 30 days after stent placement. An unplanned 30‐day encounter included patient‐initiated clinical phone calls, emergency department visits, and readmissions.
Results: Of 368 patients, 16 (4.3%) received a Boston Scientific (BS) 4.8F stent, 113 (30.7%) a Bard 6F, 223 (60.6%) a Cook 6F, and 16 (4.3%) a BS 7F. The largest diameter stent, BS 7F, trended towards having a higher rate of unplanned 30‐day encounters compared to the BS 4.8F, Bard 6F, and Cook 6F (56.3% vs 37.5%, 26.5%, 28.3%, p = 0.089). Multivariable analysis showed that the 7F stent was an independent predictor of unplanned 30‐day encounters; compared to the Bard 6F stent, the BS 7F had a 30‐day unplanned encounter odds ratio of 3.84 (CI: 1.29‐11.47, p = 0.016).
Conclusions: A larger diameter ureteral stent is independently associated with having a higher rate of unplanned 30‐day encounters. These findings suggest using smaller diameter stents may reduce adverse SRS and potential complications.
Initial experience of Allium ureteral stent in ureteral stricture after surgery and/or radiation treatment for malignancy
W Wang, X Gao, J Chen, L Peng, X Wei
Introduction & Objective: Ureteral stricture is a relatively rare, but challenging field of reconstructive urology. Currently, there are several treatment options available, including reconstructive surgery, percutaneous nephrostomy, and endourological methods. Stent placement has been widely used but is associated with complications such as infection, tissue ingrowth and encrustation. Here, we present our experience with the Allium® ureteral stent in the treatment of ureteral stricture following surgery and/or radiation treatment for malignancy.
Methods: We performed 40 Allium® ureteral stent insertion procedures (35 patients) between May 2019 to June 2020. The primary endpoint was the patency rate of the Allium® ureteral stent, while the secondary endpoint were the postoperative complications and renal function. Stent patency was defined as stent in situ without obvious migration, unanticipated stent exchange or recurrent ureteral obstruction (increasing hydronephrosis and associated deterioration of renal function).
Results: 17 patients suffered ureteral stricture following surgery and/or radiation therapy for cervical cancer, 10 after surgery and/or radiation treatment for rectal cancer, 5 following surgery for ovarian cancer, and 3 patients had ureteral stricture after surgery for bladder cancer. The median length of ureteral stricture was 6.7 cm (range 3‐17 cm). The total cost of per patient was $10544.1 US dollars (range $9394.4‐$33527.4 US dollars). During a median follow‐up time of 16 months (range 8‐21 months), 31 cases (33 sides, 82.5%) remained stent patent, four stents occluded for the reason of stent migration. There was no patient experienced stent encrustation in our study. Additionally, the postoperative average width of pelvis was significantly reduced compared with preoperation (4.58 ± 1.94 vs 3.06 ± 1.67, P = 0.002), and we observed an increased glomerular filtration rate (GFR) after stent insertion (27.56 ± 11.1 vs 40 ± 11.96, P = 0.043). However, no statistically significant differences regarding creatinine levels, blood urea nitrogen and hemoglobin exist between preoperation and last follow‐up.
Conclusions: The current study demonstrated that Allium® ureteral stent is effective and safe in the treatment of ureteral stricture following surgery and/or radiation therapy for malignant cancer. Patients renal function and hydronephrosis could be improved by the stent placement.
Image Distortion During Flexible Ureteroscopy: A Laboratory Model Comparing Super Pulse Thulium Fiber (SPTF) Laser vs High Power Ho:YAG Laser
CS Miller, BB Whiles, DA Duchene, DA Neff, WR Molina
University of Kansas Medical Center
Introduction & Objective: Digital ureteroscopes employ “chip on the tip” technology which allows significant improvement in image resolution. However, image distortion often occurs during laser lithotripsy due to acoustic wave production. We sought to compare the Super Pulse Thulium Fiber (SPTF) laser with the high power Holmium (Ho:YAG) laser in terms of image distortion using variable laser power settings and laser fiber tip distance from the scope's tip.
Methods: Utilizing a silicone renal model fitted with a 12/14F access sheath, we developed a laboratory model to simulate ureteroscopy. The LithoVue (Boston Scientific), disposable digital flexible ureteroscope was used with 200 micron laser fibers for both the SPTF (Soltive‐Olympus) and High power Ho:YAG laser (P120‐Lumenis). At defined laser parameters (10, 20, 30, and 40W; short pulse) the laser fiber was slowly retracted toward the tip of the scope during laser activation. Image distortion was identified, and distance from the laser tip to the scope tip was determined. Data from the two lasers were compared utilizing a paired t‐test.
Results: Image distortion occurred at greater distance with the Ho:YAG compared to SPTF at all laser settings (Table 1). Additionally, higher power (W) was associated with image distortion occurring further from the tip of the scope (p < 0.01 for Ho:YAG; p = 0.02 for SPFT). At the same power (W) with either 1J or 0.5J, there was no difference in distance for image distortion for the Ho:YAG, but distortion occurred differently with the SPTF (20 and 40W; p < 0.01 and p = 0.02, respectively).
Conclusions: Increased total power as well as decreased distance between the scope and laser fiber tip results in image distortion during flexible ureteroscopy. Image distortion occurs at a greater distance with the Ho:YAG laser than with SPTF fibers at the same laser settings. SPTF seems to have a better safety profile in terms image distortion and potential scope damage. Further evaluation utilizing Ho:YAG on modulated pulse mode is warranted.
Follow‐Up of Patients Undergoing Ureteral Stent Placement With and Without Cloud‐Based Stent Tracking Software
L Subramani, J Crivelli, S Zhang, L Oliver, L Harvey, R Hsi, DG Assimos, JM Hollingsworth, K Wood
The University of Alabama
Introduction & Objective: Forgotten ureteral stents can cause complications such as obstruction and infection, and often require more invasive procedures for removal. Stent tracking applications have been developed to combat this problem. We evaluated the follow‐up of patients with ureteral stents with and without the aid of an automated system for stent tracking.
Methods: We performed a retrospective review of all patients at the University of Alabama at Birmingham Medical Center undergoing endoscopic procedures including ureteral stent placement or exchange over two six‐month time periods: 7/2019‐12/2019 and 7/2020‐12/2020. Stents placed by 2 surgeons (Group 1) were followed using cloud‐based stent tracking software integrated into the electronic health record beginning 7/2020; the remaining 13 surgeons' stents (Group 2) were not tracked. The two primary outcomes of interest were 1) at least one no show to a visit with a urology provider and 2) a lapse in follow‐up defined as either no follow‐up visit or communication following stent placement, no confirmation of stent removal or exchange, or a documented delay in follow‐up or loss to follow‐up. We assessed differences in categorical variables and outcomes between groups and time periods using chi square tests.
Results: There were 1,053 stent placements or exchanges in total. Tethered stents were placed in 325/464 (70.0%) and 81/589 (13.8%) of cases in Groups 1 and 2, respectively (p < 0.001), which were consistent between time periods (173/251 [68.9%] vs. 152/213 [71.4%], p = 0.6 for Group 1; 43/289 [14.9%] vs. 38/300 [12.7%], p = 0.4 for Group 2). The Table lists rates of no shows to urology visits and lapses in follow‐up. No significant differences in no show rates were observed over time. Lapses in follow‐up decreased significantly in Group 1 for 7/2020‐12/2020 compared to 7/2019‐12/2019 (p < 0.001); this was not observed in Group 2 (p = 0.6).
Conclusions: Following ureteral stent placement or exchange, lapses in follow‐up decreased for the subset of patients followed through an automated stent tracking system.
Multi‐Institution Comparison of Nine Flexible Ureteroscopes Using a Validated Flexible Ureteroscope Evaluation Tool
MA Knoedler, S Quarrier, A Uhr, S Li, J Bell, SN Patel, KL Penniston, SG Hubosky, RK Jain, SY Nakada
University of Wisconsin, Department of Urology
Introduction & Objective: Clinical urologists need a standardized way to compare the quality of flexible ureteroscopes for clinical and research purposes. We validated a flexible ureteroscope evaluation tool (Bell 2017). Our objective was to apply the tool widely to test its consistency across multiple institutions and multiple ureteroscopes.
Methods: Ureteroscopes (n = 9) were assessed using the ureteroscope evaluation tool by three academic institutions. Surgeons completed the evaluation tool at the end of cases for which a variety of flexible ureteroscopes were used [Stortz Flex Xc (Xc), Stortz Flex X2 (X2), Olympus URF‐P5 (P5), Olympus URF‐P6 (P6), Olympus URF‐P7 (P7), WiScope, LithoVue, Dornier and Pusen]. The tool contains nine evaluation domains designed to provide a comprehensive assessment of the ureteroscope (Figure 1). The domains are: historic experience with the device, quality of image, strength of deflection, scope maneuverability, intuitiveness of controls, ease of irrigation, ease of ureteroscopic access, functionality of working channel and overall satisfaction. SPSS was used to conduct statistical analysis for internal consistency of the tool and MANOVA for comparing the scopes across domains.
Results: A total of 311 responses distributed across three institutions were completed for the nine ureteroscopes. Results demonstrated the tool's internal consistency (Cronbach alpha coefficient = 0.85). The ureteroscope with the highest overall satisfaction score was the P7 (4.81 ± 0.26) and the lowest overall satisfaction score was the Pusen (1.43 ± 0.79). Mean scores across domains are reported in Figure 2.
Conclusions: Our evaluation tool can be used to assess new ureteroscopes as they come to market. This tool is applicable to a variety of ureteroscopes with consistent results across multiple institutions and over time. This is extremely important as urologists do not always have the ability to test each ureteroscope in hand.
Single‐Centre Experience with Three Metallic Ureteric Stents (Allium URS, Memokath‐051 and Resonance) for Chronic Ureteric Obstruction
C Khoo, C Ho, V Palaniappan, A Ting, L Forster, M Kondjin‐Smith, H Abboudi, M Hanna, T El‐Husseiny, R Dasgupta
Imperial College Healthcare NHS Trust
Introduction & Objective: Chronic ureteric obstruction (CUO) is traditionally managed with polymer stents/nephrostomy; however, these are prone to failure and require regular exchange. This study evaluates efficacy of Allium URS, Memokath‐051 and Resonance metallic ureteric stents in managing CUO.
Methods: Retrospective analysis of consecutive patients with CUO managed with Allium URS, Memokath‐051 or Resonance (September 2015/July 2020). Baseline patient (age, gender, underlying aetiology, ASA) and stricture characteristics (length, level, continuity) were recorded. Intra‐ and post‐operative clinical and radiological assessments at 6 weeks, 3 months and then 6‐monthly, as well as any emergency attendances, were reviewed. Outcomes included placement success rate, functional stent survival (Kaplan‐Meier estimates), and mean renal function.
Results: 129 stent insertion episodes (SIEs) (Allium URS: 23, Memokath‐051: 48, Resonance: 58) occurred in 76 patients (Allium URS: 16; Memokath‐051: 31; Resonance: 29). Placement success was high (Allium URS: 95.7%; Memokath‐051/Resonance: 100%). Median functional stent survival was 11.4 months for Allium URS, 5.5 months for Memokath‐051 and 11.7 months for Resonance. Resonance provided the most durable Kaplan‐Meier estimates (figure 1). 47.8% of Allium URS SIEs (11/23), 64.6% of Memokath‐051 SIEs (31/48) and 19% of Resonance SIEs (11/58) failed (most frequently obstruction followed by migration and infection). In the first year following SIE, serum creatinine ranged from +21.3% to +46.7% for Allium URS, ‐7.8% to +8.9% for Memokath‐051, and ‐9.4% to +27.3% for Resonance (figure 2).
Conclusions: Allium URS, Memokath‐051 and Resonance metallic ureteric stents are all viable management options for CUO. In this cohort, Resonance provided superior functional stent survival. Prospective large‐scale comparisons are needed to inform stent choice dependant on individual patient and stricture characteristics.
Lost to Follow‐up: A Prospective Risk Factor Analysis of Forgotten Ureteral Stents
F Stroie, D Raslan, A Roston, M Krajmerova, A Ghorayeb, J Stinson, C Hollowell, M Wille
Introduction & Objective: Ureteral stents are of fundamental importance to contemporary urology practice for relief of ureteral obstruction or to promote postoperative ureteral healing. Despite widespread use, ureteral stents can be associated with multiple short and long‐term complications. Indwelling time is the most important risk factor for ureteral stent encrustation. Routine removal or exchange is an important preventative measure. There is a paucity of data exploring risk‐factors that make patients less likely for ureteral stent removal or exchange. Herein, our objective is to identify these risk factors so that more effective prevention and counseling may be directed toward this patient population.
Methods: A single‐institution prospective analysis of patients who underwent first‐time ureteral stent placement between April 2018 and February 2021. Patients who underwent ureteral stent removal beyond the intended maximal stent life of 6 months were consented to complete the study survey developed by the authors. Patients who followed up for timely ureteral stent maintenance were included in the control group and were given the same study questionnaire. Twenty patients were included in the retained stent study group and fifteen in the control group. All patients completed the study questionnaire at their first postoperative visit. The EuroQol standardised 5 dimension questionnaire was utilized to assess the overall quality of life of the patient cohort.
Results: Average indwelling stent time in the retained cohort was 35.5 months. 85% had less than a college education and 65% relied on external means of transportation to the hospital. The majority reported being informed that their ureteral stent needed maintenance, however; only half understood the implications of developing a retained stent. 65% did not know how long a stent can safely remain indwelling. Statistically significant findings were noted in that the retained cohort was more likely to have no symptoms (p = 0.036), more likely to have an annual income of less than $20,000 (p = 0.015) and less likely to have private insurance (p = 0.014).
Conclusions: Retained ureteral stents carry complex urologic sequelae. The study emphasizes identifiable patient risk factors for developing retained ureteral stents in order to mitigate expensive and complicated urologic interventions. The present study emphasizes identifiable risk factors of patients deemed to be at higher risk for developing retained ureteral stents so that additional focus and education can be targeted toward these patients.
Moderated Poster Session 20: Lasers II
A matched‐paired comparison of a novel pulsed Thulium:YAG laser with standard lasers for endoscopic enucleation of the prostate (EEP)
C Netsch, CM Rosenbaum, AJ Gross, B Becker
Department of Urology, Asklepios Hospital Barmbek, Hamburg, Germany
Introduction & Objective: A novel pulsed Thulium:YAG laser has been currently introduced for EEP. Aim of this study was to compare the perioperative results of pulsed Thulium laser enucleation of the prostate (ThuLEP) with continuous wave (cw) Thulium VapoEnucleation of the prostate (ThuVEP) and Holmium laser enucleation of the prostate (HoLEP) in patients with symptomatic benign prostatic obstruction (BPO).
Methods: A retrospective matched‐paired comparison of 120 patients with symptomatic BPO treated with pulsed ThuLEP (n = 40), cw ThuVEP (n = 40), and HoLEP (n = 40) was done according to prostate size. ThuLEP was carried out using a pulsed Tm:YAG laser (RevoLix® HTL, LISA Laser products, Katlenburg, Germany) at 100‐W (200 Hz, 0.5 J). ThuVEP was carried out using a cw Tm:fibre laser (vela® XL, Boston Scientific, Ratingen, Germany) at 90‐W, while HoLEP was performed using a pulsed Ho:YAG laser (Auriga® XL, Boston Scientific, Ratingen, Germany) at 39.6‐W (2.2 J, 18 Hz). The groups were compared regarding baseline parameters, perioperative parameters, functional outcomes (International Prostate Symptom Score (IPSS), Quality of Life (QoL), maximum urinary flow rate (Qmax), post‐void residual urine (PVR)), and the incidence of complications. Patient data were expressed as median (interquartile range) or numbers (%).
Results: There were no significant differences between the surgical groups pre‐operatively. Median age at surgery was 72.5 (67‐76) yrs., prostate volume 63.5 (45‐100) gm, and ASA score 2 (2‐3), respectively. A total of 22 patients (18.3%) were treated under continuous antiplatelet therapy (aspirin), while anticoagulant/antiplatelet therapy was temporarily stopped in 17 (14.2%) patients. The operative time was 51 (33.5‐73.5) min and was significantly different between HoLEP and ThuLEP (65 vs. 43 min, p < 0.043). There were no differences between the groups regarding resected weight (48 (25‐76) g), haemoglobin decrease (1.8 (0.8‐2.6) g/dl), catheter time (2 (2‐2) days) and postoperative stay (3 (3‐4) days). Clavien 1 (13.3%), Clavien 2 (3.3%), Clavien 3b (5.8%), and Clavien 4a (0.8%) complications occurred without differences between the groups. At discharge, Qmax (10 vs. 16.6 ml/s), PVR (150 vs. 30 ml), IPSS (21 vs. 13), and QoL (4 vs. 3) differed significantly from baseline (p < 0.001). However, Qmax was significantly different between HoLEP and ThuLEP (13.7 vs. 18.55 ml/s, p < 0.02) at discharge.
Conclusions: Thulium and Holmium lasers are safe and effective for EEP in patients with symptomatic BPO. However, the pulsed Thulium:YAG laser might decrease the operative time compared to HoLEP.
Does Metformin Protect Against Urinary Stone Formation In Diabetics?
DC Rosen, JN Bamberger, E Kaplan‐Marans, I Paranjpe, A Kapoor, D Atashokhan, AM Zampini, JA Khusid, B Gallante, WM Atallah, M Gupta
Icahn Mount Sinai School of Medicine, Urology
Introduction & Objective: Diabetes Mellitus (DM) is associated with an increased risk of nephrolithiasis. Metformin is widely used as a first line treatment of DM, yet the relationship between metformin and nephrolithiasis formation remains unclear as studies have demonstrated conflicting results.
Methods: We conducted a cross sectional analysis of stone‐forming patients at our stone clinic prior to the initiation of stone directed medical management. Patients were grouped based on diabetic status and diabetic medication regimen. Outcomes evaluated were 24‐hour urinary parameters and specimen stone type using univariate Kruskal‐Wallis and chi‐square analyses. Multivariate analyses controlling for metabolic syndrome components and HgA1c were performed.
Results: Pre‐treatment data were available for 505 patients, of whom 147 were diabetic, and 358 were not (Table I). On multivariate analyses (Tables II, III) controlling for HgA1c and other comorbidities, diabetic patients on metformin still had worse urinary parameters, including urine pH, than non‐diabetic patients (pH = ‐0.33,‐0.37 p < .05). Diabetics on metformin did not exhibit significant differences in 24‐hour urine findings compared to those not on metformin (p > 0.05 for all urinary parameters). Diabetic patients on Metformin were more likely to have uric acid stones than non‐diabetic patients (OR 3.88 (1.74, 8.69) p < .001)
Conclusions: Diabetic stone‐forming patients on metformin did not exhibit a return to normal of urinary parameters. This suggests that diabetic status rather than medication selection drives stone formation in diabetics, and that metformin is insufficient to combat the underlying metabolic milieu in these patients and prevent stone formation. Studies prospectively comparing urinary parameters of patients started on metformin are necessary to further elucidate metformin's role, if any, in combatting nephrolithiasis.
Is the Faster Thulium Fiber Laser More Cost Effective Than the Holmium Laser When Treating Renal Stones?
AS Amasyali, N Brown, J Maldonado, J Groegler, R Belay, D Baldwin, M Hajiha, JD Belle, DD Baldwin, A Assidon
Loma Linda University, Department of Urology
Introduction & Objective: New laser technologies including the 60W Thulium fiber laser (TFL) and 100W holmium laser with long pulse duration and stabilization mode (LPDSM) have been developed. The purpose of this study was to evaluate the cost effectiveness of these new laser technologies compared to a conventional 30W holmium laser (HL) using a 1 cm upper pole kidney stone in a benchtop model.
Methods: A 2x2 mm metal mesh was placed in the upper pole of a 3D printed kidney and ureter model. Ten identical 1 cm BegoStones (CaOx monohydrate consistency) were placed into the upper pole calyx and treated by the same surgeon using a flexible ureteroscope (Fig. 1a). Stones were fragmented using 3 different laser/mode combinations: A Soltive Premium 272 ⌊ m TFL at 0.5J and 20Hz (10W), the 272 ⌊ m Empower laser LPDSM at 1J and 10Hz (10W) and the 272 ⌊ m Dornier 30W with no pulse modulation at 1J and 10Hz (10W). The cost of the laser box (Soltive Premium $125,000, Empower $95,000, Dornier $35,000), the fibers (Soltive Premium $340.00/fiber, Empower and Dornier $313.73/fiber), and the mean cost of OR time in California ($37/min) were used to model cost effectiveness. An ANOVA test was performed for comparison.
Results: Stone weights were similar between groups (p = 0.422). Lasing time (13.6 vs. 19.8 vs. 24.0 min, p = 0.000) and overall operating time (14.2 vs. 24.5 min vs. 44.3 min, p = 0.000) were significantly lower in the 60W Thulium laser compared to the 100W HL with LPDSM and 30W HL, respectively (Fig.1b). The 60W Thulium and 100W HL with LPDSM required no fiber stripping, but 1 fiber stripping was required with the 30W HL. Shorter procedure time resulted in $1087.4 and $731.9 cost savings/case with the 60W Thulium and 100W HL with LPDSM over the 30W HL, and when modeling cost, factoring in the original purchase price, the 60W Thulium and 100W HL with LPDSM became cost effective over the 30W HL after treating 83 and 81 one cm kidney stone cases, respectively. The Thulium laser was more cost effective compared to the 100W HL with LPDSM after 85 cases.
Conclusions: Our study showed that the 60W Thulium laser was 67.8% faster than the 30W HL and 41.8% faster than the 100W Empower with long pulse duration and stone stabilization in breaking a 1 cm upper pole renal stone. The Thulium fiber laser will be more cost effective in high volume centers.
How Low Can You Go? A Comparison of Low‐Dose, Very Low‐Dose, and Ultra Low‐Dose Fluoroscopy During Ureteroscopic Laser Lithotripsy
AS Amasyali, M Keheila, JD Belle, N BROWN, M Hajiha, DD Baldwin
Loma Linda University, Department of Urology
Introduction & Objective: There are significant risks associated with radiation exposure. Recurrent stone formers and the urologists that treat them are exposed to significant intraoperative radiation. Recently, reduced fluoroscopy protocols during ureteroscopy (URS) have been developed. No large previous series have determined whether a minimum fluoroscopic threshold is required to maintain quality of outcome during URS. In this study, the clinical outcomes of URS were compared based upon the amount of fluoroscopy to determine whether a minimum safe fluoroscopic threshold exists.
Methods: A retrospective review of 520 patients undergoing URS for urolithiasis between January 2015 and June 2019 performed by a single fellowship trained endourologist was conducted. Patients undergoing multiple procedures or URS for entombed stents were excluded. Patient characteristics, operative, and post‐operative outcomes were collected and stratified by fluoroscopy time into ‘ultra‐low’ (0‐1.5 sec) ‘very low’ (1.5‐6 sec) and ‘low’ ( >6 sec) groups. ANOVA and Chi‐square tests were used with p < 0.05 considered significant.
Results: Of the 335 patients included in the study, 120 were in the ‘ultra‐low,’ 107 were in the ‘very low,’ and 108 were in the ‘low’ fluoroscopy groups. The mean fluoroscopy times were 0.45, 3.4 and 18.0 sec. for the ‘ultra‐low’ ‘very low’ and ‘low’ groups, respectively. The mean BMI (30.3; p = 0.856), total stone burden (117.7mm2; p = 0.252), stone location (p = 207), and density (810.9HU; p = 0.878) were similar between all groups. Fifty patients had no fluoroscopy used (14.9%). Stone free rate overall was 80.7% and did not differ between groups (p = 0.067). Hospital stay (10.9h, 23.6h and 20.1h, p = 0.154), re‐operation rate (14.9%, 9.3% and 12%, p = 0.444), and complication rates (5%, 7.5% and 7.3%, p = 0.687) were not different between the ‘ultra‐low’ ‘very low’ and ‘low’ groups, respectively.
Conclusions: Our study showed that both ultra‐low and very low fluoroscopy times did not compromise clinical outcomes. This suggests that there is no minimum fluoroscopic threshold during uncomplicated URS required to ensure safe and effective surgery. Surgeons should strive to achieve the lowest possible fluoroscopy times to reduce both patient and clinician radiation exposure.
An in vitro analysis of Holmium:YAG and Thulium Fiber laser ablation rates
MJ Basulto‐Martínez, S Proietti, M Pavia, L Rico, Y Yeow, J Flores‐Tapia, A Esqueda‐Mendoza, F Gaboardi, G Giusti
Dept. of Urology, Hospital Regional de Alta Especialidad de la Península de Yucatán
Introduction & Objective: The different settings and pulse modulation combinations of Holmium:YAG (Ho:YAG) and the new thulium fiber laser (TFL) may impact their performance. We aimed to analyze the ablation rates of both laser devices under different settings combinations.
Methods: Flat BegoStones simulating calcium oxalate monohydrate stones were created. The ablation experiments were carried out lasering the BegoStone's flat surface by a computed spiral pattern through a stepper motor bearing a magnetic holder with the laser fiber. BegoStones were placed inside a water container under continuous circulation and lasered therein. BegoStones were weigthed before and after each experiment to calculate the ablation rate. Different combinations were tested for ∼12 Watts (W) for Ho:YAG and TFL lasers. Further 25 W combination for TFL were conducted testing higher frequencies.
Results: A total of 101 experiments were conducted. Using ∼12 W, the highest ablation rate for Ho:YAG was obtained with 40 Hz/0.3 J, and Virtual BasketTM (VB) emission mode [114.35 (88.30 – 126.40) mg/min] whereas for TFL, using 40 Hz/0.3 J, and long pulse [143.40 (137.40 – 146) mg/min]. A matched‐comparison for 12 Hz/1 J settings showed that TFL outperformed Ho:YAG using medium pulse [63.30 (55.30 – 81.30) vs 132.00 (115.70 – 228.60) mg/min, p = 0.016] and long pulse [62.90 (51.60 – 78.90) vs 134.70 (110.60 – 149.30) mg/min, p = 0.016]. In the 40 Hz/0.3 J settings, TFL outperformed Ho:YAG (p = 0.034). Nonetheless, Ho:YAG with VB's ablation rate increased [114.35 (88.30 – 126.40)], being comparable to that of TFL with medium pulse [127.5 (88.90 – 141.70)] (p = 0.400). In TFL 25 W experiments, the ablation rate of 500 Hz / 0.05 J, was higher than those of 1000 Hz / 0.025 J (p = 0.049)
Conclusions: The current in vitro experiment found that the TFL ablation rate is higher than that of Ho:YAG. Furthermore, the Virtual BasketTM emission mode, increased Ho:YAG ablation rates, reaching similar to that of TFL in certain modalities. Very high frequencies with very low pulse energy dropped the ablation rate in TFL.
Unmet Needs in Postoperative Communication after Kidney Stone Surgery
M Huang, JS Winoker, ME Allaf, BR Matlaga, K Koo
Mayo Clinic
Introduction & Objective: Patient‐centered communication can enhance patient satisfaction and facilitate shared decision‐making. However, patients' information needs following urological surgery are not well‐characterized. We aimed to identify unmet needs in postoperative communication among patients undergoing kidney stone surgery.
Methods: A survey about the content, format, and experiences of postoperative communication was administered to patients in five urology clinics who had undergone any kidney stone procedure in the past two years. Responses were collected anonymously and analyzed.
Results: Among 52 respondents (response rate 88%), 38 (73%) underwent ureteroscopy, 11 (21%) PCNL, and 3 (6%) shockwave lithotripsy. The majority of patients (75%) identified deficiencies in the content or amount of information they received after surgery. Respondents were most interested in knowing how their surgery went (47, 90%), the plan for follow‐up care (44, 85%), and the specific location of their stone (44, 85%). Respondents also expressed interest in several aspects of intraoperative findings and postoperative care (stone appearance, stone location, the need for stent placement, stent symptoms, and stent location), but the majority did not recall receiving enough information. When patients had questions after surgery, the sources they trusted most were their surgeons, discharge paperwork, information in the electronic health record, and the person with whom their surgeons spoke after surgery; among these, the majority of respondents (54%) said that their urologist was the single most helpful source of information.
Conclusions: Patients who undergo kidney stone surgery may have unmet communication needs related to intraoperative findings and long‐term stone care. The findings support quality improvement efforts to optimize patient‐centered communication after surgery.
Optimal Laser settings for maximal dusting in mini‐PCNL with suction using high power Holmium laser: a prospective study of 110 patients
N Reddy, M Desai, A Patil
Muljibhai Patel Urological Hospital
Introduction & Objective: To evaluate optimal laser settings for maximum stone dusting in miniPCNL with suction and high‐power Holmium laser with Moses Technology (Lumenis Ltd., Israel) and evaluate stone free rate(SFR) by CT imaging.
Methods: Prospective, single arm study from August 2018 ‐ October 2019 using miniPCNL with suction in 110 patients with renal stones <3cm. Laser energy setting ranged from 0.2‐1.2J energy and 20‐80Hz frequency. Stone fragments for each laser setting were segregated according to size(< 1mm,1‐3mm, >3mm) and weighed. Optimal laser settings for maximum dusting was then analysed among different stone density groups. CT scan imaging was performed in all patients within 48 hours and at 30 days to assess SFR. SFR was defined as no residual fragments on CT imaging.
Results: Mean stone size was 17.5 ± 8.9mm, and stone density was 1140 ± 287.02HU. Total operative time was 38.55 ± 13.48min, laser time was 7.9 ± 7.4 min and stone fragmentation rate was 5.65 ± 5.11 mm3/s. The procedure was tubeless in 53.6% and JJ ureteral stent in 30% and nephrostomy tube in 16.4%. Optimal laser settings for maximum dusting were 0.4‐0.5J and 50‐60Hz across all stone densities. Postoperatively, four patients had urinary infection(Clavien 2). SFR within 48 hours was 77.3%. Residual fragments in 25 patients(22.7%) ranged from 1‐ 6mm, all of whom had complete clearance on CT imaging at 1 month.
Conclusions: MiniPCNL with suction using Moses laser technology can result in maximum dusting with laser energy setting of 0.4‐0.5J and 50‐60Hz and incorporating suction to the sheath allows for simultaneous fragment aspiration resulting in improved SFR.
Outcomes of Ureteroscopy and laser stone fragmentation (URSL) for kidney stone disease (KSD): Comparative cohort study using MOSES technology 60W laser system versus regular Holmium 20W laser’
T Hughes, A Pietropaolo, M Sinha, BK Somani
Southampton University Hospital
Introduction & Objective: Ureteroscopy and laser stone fragmentation (URSL) has risen over the last 2 decades. The use of laser technology has also shifted from low power to higher power lasers and the addition of MOSES technology, that allows for ‘dusting and pop‐dusting’ of stones. We wanted to compare the outcomes of URSL for MOSES technology 60W laser system versus matched regular Holmium 20W laser cases.
Methods: Prospective data was collected for patients who underwent URSL for kidney stone disease (KSD) using a MOSES 60W laser (Group A) to historical matched control data using a regular Holmium 20W laser (Group B), performed by a single surgeon. Data was collected for patient demographics, stone location, size, pre‐ and post‐operative stent, operative time, length of stay, complications and stone free rate (SFR).
Results: A total of 38 patients in each group underwent URSL procedure. The stones were matched for their location with 17 renal and 11 ureteric stones in each group. The mean single and cumulative stone sizes (mm) were 10.9 ± 4.4 and 15.5 ± 9.9, and 11.8 ± 4.0 and 16.5 ± 11.3 for groups A and B respectively. The mean operative time (min) was 51.6 ± 17.1 and 82.1 ± 27.0 (P = < 0.0001) for groups A and B. The initial stone free rate (SFR) was 97.3% and 81.6% for groups A and B respectively (P = 0.05), with 1 and 7 patients in both group needing a second procedure (P = 0.05), for a final SFR of 100% and 97.3% in both the groups. While there were 2 and 5 complications for groups A and B, none of the patients in group A had any infection related complication.
Conclusions: Use of MOSES technology with higher power was significantly faster for stone lithotripsy and reduced operative time and the number of patients who needed a second procedure to achieve a stone free status. The complications were all Clavien I/II in both groups, but with lower complications in group A and no infectious complications noted in this group. It seems that the use of MOSES technology with a high power laser is likely to set a new benchmark for treating large stones, bilateral or multiple stones in a single setting, without the need for secondary procedures in most patients.
Evaluation of the Learning Curve for Thulium Laser Enucleation of the Prostate Using Multiple Outcome Measures
L Berti, M Maltagliati, U Besana, A Calori, C Buizza, S Micali, BC Rocco, M Sighinolfi, G Bozzini
ASST Valle Olona
Introduction & Objective: To assess and quantify the surgical learning curve of Thulium laser enucleation of the prostate (ThuLEP) of a single surgeon.
Methods: A prospective analysis of 143 consecutive cases performed by the same surgeon from 2014 to 2017 was conducted. Primary outcomes included enucleation ratio and morcellation efficiencies and complication rates. Three‐month postoperative prostate‐specific antigen values were used as secondary measures. Cases were divided into cohorts of 20 cases and divided according to prostate volume into three different steps (x < 50 ml; 50 ml < x < 100 ml; x > 100 ml) to assess changes in means analyzed through Analysis of Variance (ANOVA) tests. Scatter plots of cases with a best‐fit line were drawn to analyze the learning curve.
Results: The mean age of patients across the cases was 73.13 years with an average transrectal ultrasound prostate volume of 89.77 ml. Enucleation ratio efficiency was significantly different between cohorts (P = .03) plateau after 60 cases conducted to skip to the next level of prostate size. Similarly, a significant difference is shown for morcellation efficiency (P = .01) with stabilization in performance after 40 cases. Complication rates decreased through the caseload but did not show a statistical difference (P = .47) or plateauing on the graph. Finally, no difference between 3‐month postoperative prostate‐specific antigen values was seen (P = .075); however, a learning curve of 60 cases was observed graphically.
Conclusions: Within our single‐surgeon cohort, we experienced a learning curve of 60 cases for the ThuLEP procedure. Large variability in performance late into the caseload demonstrates the technical difficulty of ThuLEP. Owing to this, adjuncts to training such as simulation‐based training may be of use for the new surgeon to shorten the initial phase of learning.
Temperature Changes in the Collecting System and Renal Parenchyma of the Porcine Kidney during Dusting and Fragmentation Modes with a Superpulse Thulium Fiber Laser
Z Okhunov, P Jiang, AS Afyouni, M Ayad, R Arada, A Brevik, RM Patel, J Landman, RV Clayman
University of California, Irvine
Introduction & Objective: Given concerns regarding temperature alterations with the superpulse thulium fiber laser (STFL), we proceeded with a detailed temperature mapping study of the collecting system and renal parenchyma during sTFL dusting and fragmentation in an in vivo porcine kidney.
Methods: Two female Yorkshire pigs underwent fluoroscopic placement under endoscopic guidance of three multipoint thermal sensor (MTS) probes that measure temperature at 5, 15, 25, and 35 mm along the probe. Probes were placed via the upper, middle, and lower calyces. The tip of each MTS probe was more than 5 mm into the calyx such that it recorded temperatures in the collecting system (Figure 1). Four protocols were performed per kidney: dual lumen ureteroscope (URS) with either warmed (37°C) or room temperature (20‐22°C) irrigation and single lumen URS with warmed and room temperature irrigation. Of note, in each pig, one kidney had a 14F ureteral access sheath (UAS), while the other kidney had no UAS placed. A 200μm sTFL fiber was fired at three laser settings: 1) dusting at 0.5J, 80Hz (40W) with continuous activation for 5 minutes or until a temperature of 44⁰C was reached, 2) low power fragmentation 1J, 10Hz, (10W), and 3) high power fragmentation at 1.5J, 20Hz (30W). For fragmentation, the laser was activated for 10 seconds with a 2‐second intermission for 5 minutes.
Results: Absent a UAS, in all but one circumstance, temperatures in the collecting system were ≥ 44°C at all laser settings with both single and dual lumen URS and regardless of whether warm or room temperature irrigation was used. In contrast, with a 14F UAS in place, using room temperature irrigation, the single lumen URS only exceeded 44°C in the dusting mode, while the dual lumen never exceeded 44°C in either fragmentation or dusting mode. Of note, in no instance did the 15, 25, or 35 mm temperature sensors within different levels of the renal parenchyma exceed 44°C.
Conclusions: Superpulse thulium fiber laser lithotripsy in either fragmentation or dusting mode, when used in the absence of a UAS, results in temperatures above 44°C within the collecting system; however, temperatures within the renal parenchyma remain under 44°C.
Vast Majority of Applied Laser Energy is Converted to Heat not Stone Ablation: in vitro Assessment
JJ Dau, TL Hall, NR Khajeh, SE Majdalany, AH Aldoukhi, KR Ghani, AJ Matzger, WW Roberts
University of Michigan
Introduction & Objective: Laser lithotripsy can cause excessive heating of fluid within the collecting system and lead to tissue damage. To better understand this effect, it is important to determine the percentage of applied laser energy that is converted to heat and the percentage used for stone ablation. Our objective was to calculate the percentage of laser energy used for stone ablation based on the difference in fluid temperature measured in an in vitro model when the laser was activated without stone ablation versus with stone ablation.
Methods: Flat BegoStone (15:5) disks were submerged in 10 ml of deionized water. A Moses 200 D/F/L laser fiber was positioned above the surface of the stone ‐ 3.5 mm for control (no stone ablation) and 0.5 mm for experimental (stone ablation) trials. The laser was activated and scanned at 3 mm/s across the stone in a pre‐programmed pattern for 60 s delivering 2400 J. Temperature of the fluid was recorded using four thermocouples. Three experimental and control trials were performed for each of the 40 W laser settings applied ‐ 0.5 J x 80 Hz, short pulse (SP), 0.5 J x 80 Hz, Moses distance (MD), and 1 J x 40 Hz, Moses distance (MD).
Results: Control trials produced no stone ablation, while experimental trials produced a continuous groove in the stone surface, simulating efficient lithotripsy. Fluid temperature rose in a linear fashion during laser activation for each trial. Control trials produced 3.1, 2.2, and 2.1°C greater temperature increase compared to experimental trials for laser settings of 0.5 J x 80 Hz SP, 0.5 J x 80 Hz MD, and 1.0 J x 40 Hz MD, respectively.
Conclusions: Laser activation for 1 minute at 40 W without stone ablation resulted in a 2‐3°C greater maximum temperature elevation compared to laser activation with stone ablation. This temperature difference equates to 123 J less energy converted to heat in the trials with stone ablation, based on specific heat capacity of water (4.18 J/g°C). This means that only 5% of total applied laser energy was used for stone ablation; the remainder, 95%, was converted to heat.
Popcorn Laser Lithotripsy Efficacy of the Moses 2.0 Laser System: An In vitro Assessment
P Whelan, CJ Kim, D Ho, C Tabib, H Premo, P Zhong, GM Preminger, M Lipkin, F Soto‐Paulo
Duke University
Introduction & Objective: Non‐contact or “popcorn” lithotripsy utilizes continuous laser firing within a group of stone fragments causing random stone movement and subsequent interaction with the laser pulse and further lithotrips. Moses™ 2.0 (Lumenis, Yokneam, Israel) technology offers an extended frequency range (EFR) of 90‐120Hz for lower pulse energies from 0.2J to 0.4J. We studied the efficacy of these new and previously studied laser settings in a popcorn lithotripsy model.
Methods: Using a Moses™ Pulse 120H 2.0 laser system, “hard” (5:1) and “soft” (5:2) BegoStone phantoms mimicking calcium oxalate monohydrate and uric acid stones, respectively, were crushed and sieved to 2.8‐4mm size. About 1g of fragments were placed in a 2cm diameter spherical flask to mimic a renal calyx, with the laser fiber positioned just above the stones. The laser was fired for 3 min with continuous irrigation (0.33cc/sec) at EFR 0.3J/120Hz, 0.4J/100Hz, 0.5J/100Hz, 0.5J/90Hz; and with short pulse (SP) and Moses distance (MD) setting for 0.5J/70Hz, 0.6J/80Hz, 1J/20Hz. Testing was performed in triplicate. After drying, stone fragments were sieved into sub‐1mm, 1 to 2mm, and greater than 2mm fragments and weighed. Comparison amongst settings was performed.
Results: Evaluating hard stones with <1mm residual stone fragments, EFR 0.5J/100Hz was superior vs SP 0.5J/70Hz (p = 0.032); and EFR 0.5J/90Hz was superior vs SP 0.5J/70Hz (p = 0.005) and MD 0.5J/70Hz (p = 0.02). EFR 0.5J/90Hz resulted in the greatest fragmentation with a mean 29.9% of treated stone fragments <1mm. 1.0J/20Hz SP and MD performed worst.
On soft stones, SP 0.6J/80Hz left fewer residual fragments >2mm vs SP 0.5J/70Hz (p = 0.004), MD 0.5/70Hz (p = 0.035) and EFR 0.5J/100Hz (p = 0.036). 1.0J/20Hz SP and MD performed worst. EFR did not demonstrate benefit on soft stones for similar total power.
Conclusions: The EFR settings provided efficient, high power, popcorn lithotripsy of hard stones. Overall, EFR and SP provided the most effective popcorn lithotripsy.
RIRS using SuperPulse Thulium Fiber Laser in patients with kidney stones 2 cm or greater
DA Sytnik, S Popov, I Orlov, I Pazin, M Suleymanov, A Kulikov
St. Luke's Clinical Hospital
Introduction & Objective: Percutaneous nephrolithotomy is the «gold» standard in the treatment of kidney stones greater than 2 cm. Retrograde intrarenal surgery (RIRS) using Ho:YAG laser is the operation of choice for these stone sizes and is highly effective and safe. In recent years the SuperPulse Thulium Fiber Laser (SPTFL) has become increasingly popular in intrarenal surgery. The aim of the study was to assess the effectiveness and safety of RIRS with using SPTFL in patients with kidney stones 2 cm or greater.
Methods: The study included 12 patients: 7 men and 5 women. The average age of the patients was 64 ± 11 years. Inclusion criteria: the size of the stone was not less than 2 cm (25 ± 4 mm), the solitary stone of the kidney, the presence of a ureteral stent at least 6 days before surgery. Exclusion criteria: the presence of urinary tract infection, urinary tract abnormalities. RIRS was performed using a flexible ureteroscope Olympus URF‐V3 with using a SPTFL (IPG Photonics, FiberLase U2). Fiber thickness was 150 microns. Fragmentation mode was “dusting' (0.1Jx200Hz). All patients underwent ureteral stenting at the end of the surgery. The following parameters were evaluated: time of surgery; SFR level, based on Computed tomography of kidneys, ureters and bladder (CT KUB); complications in the postoperative period.
Results: The average duration of surgery was 49.3 ± 12.3 minutes. The SFR level was 91.6%. According to CT KUB, residual fragments of more than 4 mm were visualized in one patient. The total percentage of complications was 8.33% (1 patient had a Grade 1 complication, according to the Clavien‐Dindo classification (fever on the 1st day after surgery). On the 7th day after surgery 10 patients had a ureteral stent removed after CT KUB. One patient underwent repeated RIRS
Conclusions: RIRS with the use of SPTFL in patients with kidney stone 2 cm or greater was characterized by high efficiency and safety.
ABSTRACT WITHDRAWN
Three‐Dimensional Patterns of Stone Ablation with Different Ho:YAG Pulse Modes
NR Khajeh, TL Hall, KR Ghani, WW Roberts
University of Michigan
Introduction & Objective: High‐power Ho:YAG lasers provide a variety of pulse mode settings, including modulated pulse sequences such as Moses contact (MC) and Moses distance (MD). Previous studies have examined crater volumes produced by different pulse modes when conducting single point or linear experiments on stone surfaces. However, no studies have compared the ablation patterns of pulse modes using a three‐dimensional laser lithotripsy technique that more accurately replicates clinical treatment. The objective of this study was to characterize ablation patterns created with different pulse modes on model stone when using an automated gridded “drilling” algorithm.
Methods: A novel laser drilling algorithm was developed to better replicate clinical laser lithotripsy techniques. A 3D positioner (securing the laser fiber) was programmed using MATLAB (MathWorks, MA) to create a 5 x 5 grid of drill holes (25 holes total, spaced 1 mm apart). The laser fiber (stripped and cleaved before each trial) was positioned 0.5 mm above the surface of a 15:5 BegoStone and advanced 2 mm towards and into the stone for each target point. The laser was activated for 115 seconds at 0.5 J x 20 Hz (10W), delivering 1.2 kJ of energy. Four trials of each pulse mode (short pulse (SP), long pulse (LP), MC, MD) were completed. Outcome measures were qualitative assessment of lattice preservation between drill holes and quantitative mass of ablated stone.
Results: MC yielded the smallest mass of ablated stone (50.5 mg; p < 0.002 compared to MD and SP) and complete preservation of the stone lattice between each drill hole, while LP (56.4 mg of stone ablated; p < 0.05 compared to MD and SP) partially spared the stone lattice. MD and SP produced the greatest mass of ablated stone (66.4 mg and 69.4 mg, respectively) and complete destruction of the lattice between drill holes, creating a large square crater.
Conclusions: Distinct patterns of stone ablation were observed for each pulse mode with this novel laser drilling algorithm. MC produced a precise ablation pattern, while MD and SP demonstrated more extensive ablation. An understanding of ablation patterns will inform proper selection of pulse modes to enhance efficiency of laser lithotripsy.
Prospective single center study of SuperPulsed Thulium‐fiber laser in retrograde intrarenal surgery: first clinical data
C Azilgareeva, M Taratkin, E Goryacheva, Y Barghouthy, D Tsarichenko, G Akopyan, D Chinenov, S Ali, V Kozlov, D Enikeev
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia
Introduction & Objective: The aim of the study is to present our clinical experience with using the SuperPulsed Thulium‐fiber laser (SP TFL) in retrograde intrarenal surgery (RIRS).
Methods: A prospective clinical study was conducted once IRB approval (Sechenov University, Russia) had been gained. Patients with stones <30 mm were treated with SP TFL (NTO IRE‐Polus, Russia) through a 200‐μm diameter fiber. Stone size, density, the duration of the operation and Laser On time (LOT) were measured. Based on the surgeon's feedback, retropulsion and intraoperative visibility were also assessed (Likert scale). The stone free rates (SFR) were assessed with a low dose CT scan 90 days postoperatively.
Results: Between January 2018 and December 2019, 153 patients (mean age 54 ± 2.8 years) underwent RIRS with SP TFL.Intraoperative data presented in Table 1. Retropulsion was present in 23 (15.1%) patients. Visibility was estimated as optimal in most patients, with poor visibility reported in only 13 (8.5%) patients. On the basis of a multivariable statistical analysis, the density (OR = 0.998, 95% CI: 0.998‐0.999, p < 0,001) and frequency (OR = 1.005, 95% CI: 1.001‐1.010, p < 0,001) were closely correlated with poorer visibility. A multivariable analysis which adjusted for retropulsion showed a significant correlation with frequency (OR = 0.987, 95% CI: 0.977‐0.997, p = 0.008) There was a significant correlation between LOT, stone volume (r = 0.733 with p < 0.001) and total energy (r = 0.922 and p < 0.001).
The SFR (at 3 months) was 89% (136 of 153 patients). The postoperative complication rate was low, with Clavien I‐II complications present in 13 (8.4%) patients. No complications specific to the use of SP TFL were identified.
Conclusions: The SP TFL laser is a safe and efficient tool in lithotripsy, irrespective of the stone type and density. Retropulsion is minimal and visibility is maintained with SP TFL. Nonetheless, further clinical studies are needed to ensure an optimal comparison with conventional Ho:YAG lithotripsy.
A cost‐comparison of Holmium laser enucleation of Prostate with and without MOSES
MS Lee, M Assmus, DK Agarwal, T Large, AE Krambeck
Northwestern University Feinberg School of Medicine
Introduction & Objective: Holmium Laser Enucleation of Prostate (HoLEP) is a size‐independent treatment for benign prostate hypertrophy (BPH). Moses™ is a new technology developed by Lumenis® for its 120H laser system, which utilizes pulse‐modulation technology to increase energy delivered to tissue/stone. Several studies have shown Moses™‐augmented HoLEP (m‐HoLEP) results in faster enucleation and hemostasis. Therefore, we performed a cost‐analysis of HoLEP cases performed with and without Moses™ to determine if it resulted in cost‐savings.
Methods: A retrospective review of all HoLEP cases from May 2018‐Nov 2020 performed by one fellowship‐trained surgeon was performed. Variables were abstracted from the electronic medical record. Patients were stratified into two groups based on the use of Moses™. Student t‐tests and chi‐square tests were used to compare the two groups. All statistical analyses were performed using SAS 9.4. All tests were two‐sided and statistical significance was set at p < 0.05. Cost analysis was obtained by the IU Office of Clinical Effectiveness.
Results: 312 patients who underwent HoLEP during the study period. Procedure time was shorter in the Moses™ group, but the result was not statistically significant (74.1 ± 35.0 vs. 80.8 ± 45.4 min, p = 0.686). Morcellation time was shorter with Moses™, and this trended towards significance (9.9 ± 9.8 vs. 12.6 ± 14.6 min, p = 0.0704). Cost analysis showed that Moses™ resulted in decreased surgical costs by $840, despite the fact that the surgeon was well past the learning curve. Cost savings were related to ability to discharge patients the same day without return to the ED or readmission and decreased procedure times.
Conclusions: m‐HoLEP resulted in shorter procedure time even for a seasoned surgeon. Interestingly, we found a costs savings of $840 with Moses™, which is likely related to the ability to perform same‐day discharge safely.
Stone ablation efficiency of a new prototype pulse‐modulated laser and a 120W Holmium:YAG laser
B Yang, I Parab, J Cancino, S Liu, A Ray, TC Hasenberg, T Harrah, BW Turney
University of Oxford
Introduction & Objective: Holmium:YAG laser has been the lithotrite of choice for around 30 years in kidney stone surgery. Lasers have evolved over the years to offer higher power, increased pulse frequencies and longer pulse durations. The drivers for change have been to improve stone ablation and to minimise retropulsion. We report on a new prototype Holmium laser that fires multiple micro‐pulses in pulse packets and discuss the stone phantom ablation rate results utilizing a bench model.
Methods: Uniform, homogeneous BegoStones (15:3 BegoStone:water) were used. A 242μm core fiber was attached to the prototype laser and the fiber was moved over the surface of the stone in a predetermined pattern using an automated system. A range of pulse packet energy/frequency settings from 5W to 60W were investigated. Stone ablation efficiency was measured by dry‐weight difference before and after treatment.
Results: High ablation rates were observed with the prototype pulse‐modulated laser across the tested range of powers (Figure 1). Ablation rate scales linearly with total average power across this range (r2 = 0.88). Results from a reference holmium laser using the same methodology are also included.
Conclusions: The prototype laser demonstrated impressive stone ablation rates in our bench testing across a range of power settings. We will discuss the details of these results and feel that pulse‐modulation with packets of micro‐pulses is a promising technological development and needs to be studied in a clinical setting. (Disclaimer: Concept device or technology. Not available for sale).
SuperPulsed Thulium‐fiber laser lithotripsy: an in vitro comparison of 200 μm and 150 μm laser fibers
C Azilgareeva, M Taratkin, S Ali, M Corrales, D Enikeev
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia
Introduction & Objective: This study aimed to investigate the thermal effects, stone retropulsion and ablation rate of SuperPulsed Thulium‐fiber laser (SP TFL) with two different fibers measuring 200 μm and 150 μm in diameter.
Methods: SP TFL (NTO IRE‐Polus, Fryazino, Russia) with 200 μm and 150 μm fibers were compared. SP TFL was operated at a wavelength of 1.94 μm, a maximum average power up to 40 W and a peak power up to 500 W. Single‐sized (5x5x5 mm) Cubic BegoStone phantoms with a completely flat surface (Bego GmbH, Bremen, Germany) were used. Several laser setups were used to assess energy transmission, retropulsion, ablation efficacy, fiber burnback and safety.
Results: Both fibers showed a deflection angle of 270o, which was comparable with the flexibility without fiber. Fiber energy transmission in a straight configuration revealed a 4.7% power drop for a 200 μm (14.3 ± 0.5 W) and 7.3% for a 150 μm fiber (13.9 ± 0.5 W) versus the nominally indicated power (15.0 W). At 180o bend, the power drop was 6.7% (14 ± 0.5 W) and 8% (13.8 ± 0.5 W). No significant differences in the results were noted (p = 0.109).
We found neither clinically relevant temperature differences between 200 μm and 150 μm fibers nor differences in local and global temperatures. During the retropulsion experiment, the maximum stone displacement for 1 sec of laser firing was 14.7 ± 1.0 mm and 15.0 ± 0.6 mm for 200 and 150 μm fibers, respectively. No differences in stone displacement were found (p > 0.05 in all tests). The retropulsion threshold was 2 J for both fibers and then the retropulsion increased in a linear manner as pulse energy increased.
During the ablation testing, we found no statistically significant superiority in lithotripsy. Both the dust weight on filters and the mean stone particle mass after the experiment were similar (from 0.08 to 0.14 mg with 200 μm fiber and from 0.10 to 0.15 mg with 150 μm fiber). On visual examination, all the particles were categorized into groups depending on size. No stone fragments larger than 5 mm (in the largest surface) were found in tests after lithotripsy with a 150 μm fiber, whereas in a 200 μm fiber group they were present in all cases.
The fiber burnback was an average of 0.5 mm for both fibers (0.47‐0.56 for 200 μm, and 0.41‐0.5 for 150 μm, p = 0.287) (tested at 1.5 J/ 30 W, with total of 5000 J).
Conclusions: The smaller fiber (150 μm) is not inferior to 200 μm fiber in terms of fiber burnback, retropulsion, safety, and ablation rate. Moreover, it has the potential to decrease the diameter of fragments during lithotripsy, which may facilitate dusting during RIRS.
Setting laser lithotripter parameters according to endoscopic view: a descriptive guide to optimize treatment outcomes
N Frego, D Maffei, L Domanico, M Paciotti, V Fasulo, D Pietro, R Hurle, M Lazzeri, P Casale, GF Guazzoni, G Lughezzani, NM Buffi, A Saita
Humanitas Clinical and Research Center ‐ IRCCS, via Manzoni 56, 20089 Rozzano (MI), Italy
Introduction & Objective: Stone composition and physical properties are important data in the setting of the laser lithotripser. The aim of the study was to investigate the hypothesis that a senior endourologist may foresee stone composition by direct endoscopic view and set the most appropriate laser frequency and energy power.
Methods: This was a prospective observational pilot study enrolling 36 patients, from December 2018 to April 2019, with a diagnosis of urolithiasis, scheduled for URS/RIRS/PNL. For each stone we recorded the morphological analysis (stone surface, shape and colour to define the composition) and consequently we set the laser's frequency, energy and pulse. All stones were subsequently analyzed at infrared spectroscopy to determine their composition. For all the procedures, Lumenis 120 Watt laser lithotripter was used. The primary endpoint was to report the correspondence between endoscopic examination and ex vivo stones analysis. The secondary end point was the stone free rate (SFR) at 6 months after surgery.
Results: Visual characteristics correlated with stone's composition and the corrisponding laser setting were summarized in Table 1. The correspondence between endoscopic examination and stone analysis was found in 91,7% of cases. Three cases of calcium oxalate dihydrate (weddellite) were not correctly identified at endoscopic view, because of the presence of brushite. Using this approach SFR at 6 months were 82%.
Conclusions: Our preliminary findings showed a correspondence between endoscopic stone composition and ex vivo stone analysis. Moreover, adequate setting of laser lithotripter based on endoscopic appearance of stone results in effective lithotripsy.
Thulium Fiber Laser Results in Shorter Operating Times During Ureteroscopy and Laser Lithotripsy
JR Ryan, MH Nguyen, JA Linscott, SW Nowicki, BM Jumper, JP Ingimarsson
Maine Medical Center Department of Urology
Introduction & Objective: Ureteroscopy (URS) procedure duration has been associated with complications such as ureteral perforation and urosepsis, as well as higher costs. A new FDA approved lithotripter, the thulium fiber laser (TFL), was made commercially available in June of 2020 and was acquired by our institution. This retrospective study was designed to determine if TFL lithotripsy decreased operative time when compared to standard Holmium:YAG (Hol:YAG) lithotripsy without pulse modulation.
Methods: A retrospective review of URS with laser lithotripsy at a tertiary stone center was conducted for cases performed 2 months before and 2 months after conversion to TFL lasers for URS. 152 procedures were identified. Cases that involved bilateral procedures, aberrant anatomy, had no recorded kidney stone composition, and those that were aborted due to complications or tight ureters were excluded from analysis. 102 cases met inclusion criteria, 51 in each arm. Operative time was measured from scope in to scope out. Variables including stone size, location, chemical composition, prior ureteral stenting and ureteral access sheath use were recorded. In cases with 2 or more stones, the cumulative stone diameter was measured from pre‐op CT imaging and reported as the summation of diameters from all treated stones.
Results: Baseline characteristics of the patients and stones treated did not differ significantly between laser groups (table 1). Compared to Hol:YAG, use of TFL resulted in an average decrease of 12.94 minutes per case (p = .021, 95% CI [2.03‐23.85]). In subgroup analysis of cases with cumulative stone diameter less than 15 mm, the difference was 13.95 minutes (p = .007, CI [3.95‐23.95]). For cases less than 10 mm, the mean difference was 17.27 minutes in favor of TFL (p = .002, 95% CI [6.89‐27.62]). Stone free states confirmed by retroperitoneal ultrasound were similar between groups but could not be reliably estimated due to low (36%) compliance with post op imaging in the COVID era.
Conclusions: TFL is a substantially faster means of laser lithotripsy than Hol:YAG with average case time reduced by 20% overall (13 min). As the number of URS laser lithotripsy procedures being performed in the United States continues to increase, reducing procedure times has the potential to improve patient outcomes and decrease costs. Longer term follow up is needed to see if recurrence rates are affected.
Study of real time temperature changes during laser lithotripsy with Thulium Fiber Laser: An in‐vitro study
R Batra, R Sharma, A Singh, A Ganpule, R Sabnis, M Desai
Muljibhai Patel Urological Hospital, Nadiad
Introduction & Objective: Thulium Fiber Laser is a high‐powered laser. There are many concerns regarding the heat generated with the use of thulium Fiber laser. The aim of the study was to measure real time temperature changes with Thulium Fiber Laser (TFL) at different irrigation rates and different energy levels in an in‐vitro model.
Methods: We measured temperatures of irrigation fluid in a 25 ml overflow flask having continuous irrigation with inlet and outlet which were precisely controlled. The flask had stones inside it. A temperature probe and TFL laser fiber (IPG Photonics) were inserted inside the flask and laser lithotripsy was performed. The settings kept were 400‐micron laser fiber at 200 Hz frequency and energy settings of 0.1, 0.15 an 0.2 Joules with a total power of 20 watts, 30 watts and 40 watts at dusting mode. The irrigation was at 0 ml/min, 10 ml/ min and 20 ml/min. The temperature was measured at every 60 seconds for 5 minutes.
Results: The baseline temperature during the experimental set up is shown in the graph. Without irrigation, the maximum temperatures were reached. At 20 watts, 30 watts and 40 watts, the temperature reached at 46.6° Celsius; 59° Celsius and 67.6° Celsius respectively. At 10 ml/min irrigation, the temperatures at 20 watts, 30 watts and 40 watts was 40° Celsius, 47.2° Celsius and 55.4° Celsius respectively. At 20 ml/min irrigation, the temperatures at 20 watts, 30 watts and 40 watts was 38° Celsius, 43° Celsius and 48.2° Celsius respectively.
Conclusions: Average temperature increases when the total energy of the laser increases. Maximum rise in temperature is without irrigation. With an irrigation of 20 ml/min, the rise in temperature is the least and does not reach beyond 50 degree Celsius at 5 minutes. Thus, Thulium Fiber laser should be used with a good irrigation and at low power settings as much as possible to prevent thermal injury to the tissues of ureter and pelvis.
Functional Outcomes of Focal Salvage MRI Fusion Guided HIFU for Localized Radiation Recurrent Prostate Cancer
A Kasraeian, M Alcantara, K Mola Alcantara, S Scionti
Kasraeian Urology
Introduction & Objective: Only two percent of men in the United States with localized radiation recurrence are offered local salvage therapy, often due to the high morbidity associated with whole gland salvage therapy for their recurrent prostate cancer. If, however, the recurrent tumor can be identified with advanced diagnostic techniques, such as MRI/US Fusion biopsy, and focally targeted, treatment morbidity can possibly be reduced. We discuss our experience with Focal Salvage MRI Fusion Guided HIFU with dose escalation ( FS‐mfHIFU). Functional outcomes and data were prospectively collected, analyzed and reported.
Methods: Between December 2015 and October 2019, 14 patients underwent FS‐mfHIFU. Median age was 65 years of age. Gleason Scores ranged from 6 to 10, with one low risk, 7 intermediate risk, and 6 high risk patients undergoing salvage focal therapy. Seven patients underwent focal HIFU of the MRI target with margin, four were treated with hemiablation, and three using a subtotal (urethral sparing) technique.
Results: A Foley catheter was used in all 14 patients who underwent FS‐msHIFU. Mean catheterization time was 7.25 days. Only 2 patients required catheter replacement due to urinary retention (14%). Only 2 (14%) required endoscopic intervention (due to urethral stricture). No rectal fistulae were noted in our series. Twelve of the 14 men treated reported pad free urinary continence (86%). Functional outcomes included mean serial IPSS measurements of 8.6 (pre‐treatment), 9.78 (3 months), 7.4 (12 months). IIEF measures of mean erectile function demonstrated scores of 11.7 (pre‐treatment), 9.2 (3 months), and 7 (12 months). Additionally, mean PSA was 4 (pre‐treatment), 0.59 (3 months), 0.74 (6 months), and 0.67 (12 months).
Conclusions: With careful selection, advanced diagnostic techniques, and appropriate and honest counseling, focal salvage HIFU can offer men with localized radiation recurrence disease control with better preservation of their urinary and bowel function than whole gland salvage therapies for recurrent prostate cancer
Primary transrectal random prostate biopsy: is still actual?
A Campitelli, G Molisso, T Realfonso, M Addesso, G Napodano, R Sanseverino
Introduction & Objective: Random prostate biopsy is still the gold standard procedure to detect prostate cancer. Multiparametric MRI has been introduced to guide target prostate biopsy to improve detection of clinically significant prostate cancer. Today is debated whether primary biopsy should be performed with random or target approach. We evaluated outcomes of patients undergone first transrectal random prostate biopsy. We also evaluated predictive factors of prostate cancer diagnosis
Methods: Patients with suspicious of prostate cancer based on PSA, DRE, ultrasound findings underwent a TRUS guided transrectal biopsy. Procedure were performed under local anaesthesia or intravenous sedation as indicated. Clinical and pathological data were prospectively collected from May 2010 to September 2019 in our database. We calcolated cacer detection rate and we identified predicitve factors of cancer. Statistical analysis was performed using Chi square test, Mann Whitney, logistic regression test, as appropriate (SPSS 19).
Results: Data on 1974 patients were available. Patients characteristics are reported in table 1. Indications for biopsy are reported in table 2. Prostate cancer has been diagnosed in 46.4% of the patients (table 3). There is an increasing trend in cancer detection rate per year (table 4). Positive patients presented ≥3 positive cores or Gleason ≥3 + 4 in 78,5% and 86,7%, respectively. At multivariate analysis, age, PSA, DRE, prostate volume, number of cores, and year of biopsy are predictive of cancer diagnosis.
Conclusions: Random transrectal prostate biopsy identified cancer in 46% of all patients. In the last three years, cancer detection rate is more than half of the patients. More than three quarters of patients presented a clinically significant cancer. Age, PSA, positive DRE, prostate volume and number of cores are correlated with presence of cancer.
Complications after random TRUS guided transrectal prostate biopsy
G Napodano, M Addesso, T Realfonso, A Campitelli, G Molisso, A Pane, R Sanseverino
Introduction & Objective: Prostate biospy is the gold standard procedure to diagnose prostate cancer. The technique is usually performed under transrectal ultrasound (TRUS) guidance with transrectal or transperineal approach. Every year more than 1 milion pof procedure are realized in Europe. Complication rate is quite low; however fearsome infectious complications are increasing. We have retrospectively evaluated complication rate in our database and we have analyzed predictive factor of complications
Methods: From database of our institution we have evaluated complications of patients undergone transrectal random prostate biopsy for suspicion of prostate cancer. Complications were classified as bleeding more than 3 days after biopsy (hematuria, hematospermia, rectal bleeding), infection defined as fever more than 38°C, acute urinary retention (RUA). Hospitalization due to complication was ha salso been recorded. We have correlated every complication with age, prostate volume, PSA, PSAD, BMI, number of cores, cancer detection, diabetes mellitus, previous urinary or genital infection, BPCO, previous urological surgery, previous or concomitant tumor. Statistical analysis was performed using Chi square test, Mann Whitney, logistic regression test, as appropriate (SPSS 19).
Results: Data on 2.106 patients were collected. Patients characteristics are reported in table 1. Complications occurred in 6.4% of the patients (table 2). Multivariate analysis revealed correlation only for infection with previous history of urinary or genital infection (p0.001, OR 0.012 ‐ CI 0.001‐0.162) (table 3). A minority of patients (15 out of 2.106 0.7%) required hospitalization because of complications (11 for infection, 2 for hematuria, 1 for rectal bleeding, 1 for AUR). However 11.2% (15 of 134) of patients with complicatons needed hospital admisison. Previous urinary or genital infection was the only factor associated with hospitalization (p0.001 ‐ 0.005 0.000‐0.125).
Conclusions: Transrectal random prostate biopsy is a common and safe procedure. Complications rate is generally low (6.4%); hematospermia is more frequent complication (4.7%). Hospitalization is rarely needed (0.7%). However fearsome and lifethreatening infectious complications are main causes of hospital admission
Step‐by‐step development of a cold ischemia device for open and robot‐assisted renal transplantation
A Territo, M Fontana, A Gallioli, A Piana, P Diana, JM Gaya, J Huguet, P Gavrilov, O Rodriguez Faba, A Mottrie, C Facundo, L Guirado, J Palou, A Breda
Department of Urology, Fundació Puigvert, Barcelona, Spain
Introduction & Objective: Rewarming time can be associated with delayed graft function (DGF) due to ischemia/reperfusion damage. In both open kidney transplantation (OKT) and robotic assisted kidney transplantation (RAKT), ice slush is used to maintain graft temperature (GT) (target <20°C), preventing its impairment due to the rewarming time. This cooling technique is not able to keep a constant, equal temperature over the entire graft surface and can potentially provoke local or systemic hypothermia. The aim of a cold ischemia device (CID) is to maintain a constant low temperature of the entire graft while performing vascular anastomosis.
Methods: In IDEAL phase 1, CID was developed with bioengineers from GRENA Ltd. It consists of 2 layers of a thin film sealed to create a circuit, through which saline could flow in a closed system thanks to silicone tubes connected to a peristaltic pump and saline reservoir. CID was tested in the dry lab to determine whether it could keep a kidney at a constant low temperature, using 15 porcine kidneys: in 5 the device was used (group 1), in 5 a gauze jacket filled with ice slush was used (group 2), and in 5 no covering was used (group 3). The three groups of kidneys were introduced into a closed box with a predetermined temperature of 37.5°C, simulating the temperature of the abdominal cavity (38°C). The temperature was evaluated at scheduled timepoints from T0 (baseline) to T11 (50th minute). In phase 2a, CID was evaluated in porcine model (in‐vivo) undergoing OKT and RAKT. In phase 2b, CID was tested in patients undergoing OKT and RAKT from living donors, monitoring GT with a thermal probe. Surgical procedures were performed according to standard technique.
Results: In IDEAL phase 1, CID proved able to maintain a low GT (< 20° C) and was superior to both the gauze jacket filled with ice slush and no covering (p = 0.002). In IDEAL phase 2a, CID allowed maintenance of a low and constant GT during both OKT (n = 3) and RAKT (n = 3), with a mean temperature at T11 of 10.8°C (SD 0.2) and 14.9°C (SD 0.1), respectively. In IDEAL phase 2b, demonstrated that both OKT (n = 2) and RAKT (n = 3) can be performed using CID in a clinical setting. In both approaches, GT never exceeded 20°C, with mean temperatures of 15.7°C and 18.3°C in OKT and RAKT, respectively. In all 5 cases, surgical times using CID were similar to the conventional approach. All (n = 5) patients were discharged at post‐op day 7; no cases of DGF were recorded.
Conclusions: CID showed to keep a constant low GT in both OKT and RAKT. In terms of maneuverability and feasibility, it allows to perform vascular anastomosis within a satisfactory length of time.
Robotic assisted MRI‐US fusion guided target saturation biopsy of the prostate – diagnostic accuracy and clinical implications
C Wetterauer, P Trotsenko, M Matthias, P Brantner, T Vlajnic, L Bubendorf, D Winkel, M Kwiatkowski, H Seifert
University Hospital Basel, Department of Urology
Introduction & Objective: MRI‐targeted prostate biopsy improves detection of clinically significant prostate cancer (PCa) and reduces overdetection of clinically insignificant cancer. However, up to 70% of PCa lesions display intralesional tumor heterogeneity and current sampling strategies do not yet adequately account for this finding. This study aims to assess the potential of robotic assisted target saturation biopsies in terms of intralesional diagnostic accuracy as well as the potential clinical implications.
Methods: This prospective study included 88 patients who underwent transperineal robotic assisted biopsy of the prostate at the University Hospital Basel from January 2020 – January 2021. We identified a total of 47 PCa‐positive PI‐RADS lesions in 38 patients that were sampled by targeted saturation biopsies. We compared the diagnostic accuracy of a target‐saturation biopsy strategy to the accuracy of single, two or three targeted biopsies, respectively and analyzed the potential clinical implications.
Results: Intralesional detection of clinically significant cancer (ISUP ≥2) was 78.9% (30/38) for target‐saturation biopsy and 28.9% (11/38), 39.5% (15/38) and 50% (19/38) for one, two and three targeted cores, respectively. Target‐saturation biopsies led to a significantly more accurate characterization of PCa in terms of Gleason score and significantly reduced rates of cancer missed (p < 0.05). Compared to one, two and three targeted biopsies, target‐saturation biopsies led to intensified staging procedures in 11 (28.9%), 9 (23.7%) and 7 (18.4%) and ultimately to a potential change in therapy in 19 (50%), 15 (39.5%) and 11 (28.9%) patients, respectively.
Conclusions: This work presents the concept of robotic assisted target saturation biopsy and demonstrates the potential of this technique to improve diagnostic accuracy and its impact on individual treatment decisions.
Is Biparametric MRI adequate to detect clinically significant prostate cancer in biopsy naïve patients? results from a prospective, single centre, non‐inferiority randomized trial
M Manfredi, E Checcucci, D Amparore, S De Cillis, G Volpi, A Pecoraro, F Piramide, A Piana, M Sica, S Granato, J Mézière, D Zamengo, G Cattaneo, F Russo, S De Luca, C Fiori, F Porpiglia
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
Introduction & Objective: European and American urological guidelines of 2020 recommend to perform multiparametric (mp) MRI in men with suspicion of prostate cancer (PCa), before the execution of prostate biopsy. The new guidelines will furtherly increase the requests of MRI exams, but the restricted accessibility of scanners and costs' increase might determine an important pressure on healthcare systems. A single plane biparametric MRI (fast‐MRI) could decrease exam execution time and costs, hereby augmenting test availability, considering that fast‐MRI maintains a high detection rate of clinically significant PCa (CsPCa).
Methods: In this study, biopsy‐naïve men with PSA <15 ng/ml and non‐suspicious digital rectal examination were randomly submitted to either fast‐MRI (axial T2w and DWI, arm A) or mp‐MRI (arm B), in a 2:1 ratio. If the results of fast‐MRI were ambiguous, men in arm A underwent mp‐MRI. The reference standard was systematic core biopsy and/or fusion biopsy on MRI suspicious lesions. CsPCa was defined as Grade Group ≥3 or a maximum cancer core length involvement ≥6 mm.
Results: 311 men were enrolled in our study from January 2018 to March 2020: 213 underwent fast‐MRI and 98 mp‐MRI using a 1.5 Tesla scanner. 26 men with ambiguous fast‐MRI underwent mp‐MRI. CsPCa was diagnosed in 56 patients in arm A and 29 patients in arm B. Sensitivity and negative predictive values (NPV) of mp‐MRI and of the fast‐MRI workout were 100% (95%CI 88‐100%) versus 87.5% (76‐95%), (p = 0‧96) and 100% (94‐100) versus 95% (90‐97%) (p = 0.97), respectively. Compared to fast‐MRI both mp‐MRI and PSA density with a cut‐off of 0.12 ng/ml detected 9 additional CsPCa.
Conclusions: In biopsy‐naïve men, fast‐MRI followed by mp‐MRI or PSA density evaluation in case of ambiguous findings has sensitivity and NPV similar to mp‐MRI. In future, fast‐MRI protocols might represent a solution in order to reduce costs and exam acquisition time of mp‐MRI in selected biopsy‐naïve men. The proposed diagnostic workflow should be tested in a multicentre, multi‐observer setting.
Comparing target plus standard prostate biopsy vs target alone in naïve patients: a retrospective analysis on the basis of pathological examination of prostate specimens
E Checcucci, S De Cillis, D Amparore, G Volpi, F Piramide, S Granato, M Sica, P Alessio, A Pecoraro, G Cattaneo, D Garrou, M Manfredi, C Fiori, E Bollito, I Stura, G Migliaretti, F Porpiglia
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
Introduction & Objective: The wider use of multiparametric Magnetic Resonance Imaging (mpMRI) and its application for target fusion biopsy (FB) has increased prostate cancer (PCa) detection rate. However, the necessity to add standard biopsy (SB) to FB in biopsy naïve patients is still discussed. The aim of this study is to assess if the addition of SB to FB still has a role in the diagnosis of PCa or clinical significant PCa (csPCa) in biopsy naïve patients with positive mpMRI imaging.
Methods: We analysed data from our prospectively maintained FB database, from March 2014 to December 2018. The detection rates (DR) of PCa and csPCA were analysed in a cohort of biopsy naïve patients submitted to FB alone (Group A) or FB+SB (Group B). Subsequently, the complication rate between the two group was examined. Finally, the International Society of Urological Pathology grade group diagnosed with prostate biopsy was compared with the grade group determined at radical prostatectomy (RP) final pathology.
Results: PCa was diagnosed in 249/389 (64.01%) and 215/337 (63.8%) patients in Group A and B respectively (p = 0.98). The DR OF csPCa was 57.8% and 55.1% (p = 0.52) respectively. No significant differences in terms of complications were recorded. Among the patients with positive biopsy, in 270 the ISUP grade was also determined after robotic RP (156 in Group A and 114 in Group B). At final pathology, upgrading occurred in 32 (20.5%) and 22 (19.3%) cases in Group A and Group B respectively (p = 0.92). In addition, an upgrading with change of risk group (according to EAU risk groups for biochemical recurrence) was recorded in 15 (9.6%) patients in Group A and 6 (5.2%) patients in Group B (p = 0.26). Regarding Group B, no differences in rates of upgrading between systematic and targeted biopsy cores were recorded (16.6% for both types of approach). At last, considering RP as the reference standard, we noticed that csPCa was correctly identified with biopsy in 131 (83.97%) and 105 (92.10%) patients in Group A and B respectively (p = 0.07). On the contrary, csPCa diagnosis was missed in 9 (5.76%) and 5 (4.38%) patients in Group A and B, respectively (p = 0.82).
Conclusions: In biopsy naïve patients, with suspicion of PCa and positive mp‐MRI the addition of SB to FB did not significantly improve the DR of PCa or csPCa based on the analysis of RP specimens. Furthermore, the rate of upgrading of ISUP grade group between biopsy and final pathology was not conditioned by the addition of SB to FB.
Utility of a Novel Platform for Performing Prostate Biopsy ‐ Results of the first 750 patients using a Free Hand Ultrasound Guided Local Anaesthetic Transperineal Prostate (LATP) Technology
M Yao, C Phelan, S Folkard, A Rajagopalan, B Varga, J Rusere, A Lamb, SS Kommu, R Popert, BA Eddy
East Kent Urology Department, Kent and Canterbury Hospital, East Kent Hospitals University NHS Foundation Trust
Introduction & Objective: Prostate Biopsy remains the gold standard for histological confirmation of prostate cancer. The near exponential increase in the need for biopsies, in selected men, has ushered an evolving need for improving detection rates while reducing side effects. Diagnostic accuracy and infection complication rates remain obstacles in transrectal prostate biopsy. PrecisionPoint is a disposable, low cost device which enables transperineal biopsy in the outpatient setting under local anaesthetic.
We present data from a predominantly nurse‐performed LATP service using PrecisionPoint, which was newly started in July 2019. Initial indications were; repeat biopsy, anterior lesions, and active surveillance patients. Service was expanded in March 2020 to all prostate pathway patients following national COVID guidance.
Methods: All patients underwent prebiopsy MRI and dedicated image‐review meetings. Biopsies were performed in PIRADS 3‐5, or PSAD >0.15. PIRADS 3‐5 lesions were targeted with ≥3 cores (sent separately). Systematic Ginsburg protocol biopsies were also performed (each zone sent separately). Tamsulosin was started for BOO patients.
No antibiotics were used unless immunocompromised or previous sepsis. A prospective database at point of care was created detailing patient information, MRI and biopsy characteristics. Patient Reported Outcome Measures (PROMs) are collected. Histology and complications are also reported.
Results: 750 consecutive patients analysed. Detection of significant cancer (Gl ≥3 + 4) in PIRAD1‐2, 3, 4, 5 groups was 25%, 40%, 59%, 92% respectively. Systematic biopsy alone detected significant cancer in 36%, systematic plus targeted achieved 63%. Of AS patients; 40% with Gl3 + 3 were upgraded, and 49% with Gl3 + 4 were upgraded to Gl ≥4 + 3. 5 experienced vasovagal episodes. Only 5 patients were readmitted (0.6%): 2 UTI, 2 AUR, 1 urosepsis.
PROMs demonstrated majority favourable results regarding pain (98%), discomfort (97%), embarrassment (96%) and further biopsies (89%).
Conclusions: Adoption of this new technology into an integrated prostate cancer diagnostic pathway has enabled us to set up a safe, effective, antibiotic free LATP biopsy service in the outpatient setting. Data shows high cancer detection rates and low complication rates. PROMs data suggests this is well tolerated by patients.
Prostate biopsy is unnecessary in low Prostate Imaging ‐ Reporting and Data System (PI‐RADS) score lesions
D Kim, S Jeon, S Lee, C Lee, S Chang, S Lee
Department of Urology, School of Medicine, Kyung Hee University
Introduction & Objective: We evaluated if the Prostate Imaging ‐ Reporting and Data System (PI‐RADS) could reduce unnecessary prostate biopsies.
Methods: Patients with prostate‐specific antigen (PSA) levels ≤20 ng/ml who underwent prostate magnetic resonance imaging (MRI) for evaluation from January 2018 to November 2019 were analyzed. Among them, 105 patients who received transrectal ultrasonography (TRUS)‐guided biopsy were included. PSA, PI‐RADS scores, biopsy results and Gleason scores (GS) were evaluated. Biopsies with GS higher than 3 + 4 were considered significant and biopsies with no cancer or Gleason 3 + 3 were considered insignificant.
Results: Among the 105 patients, 45 patients had low PI‐RADS and 60 showed high PI‐RADS scores. There were no patients with significant prostate cancer in the low PI‐RADS groups. For the high PI‐RADS group, 28 (46.7%) had significant cancer and 32 (53.3%) had insignificant cancer. The sensitivity and specificity of high PI‐RADS to detect significant cancer was 100% and 58.4%. Positive predictive value was 46.7% and negative predictive value 100%.
Conclusions: Low PI‐RADS scores on MRI did not show significant prostate cancer and surveillance should be in selected cases to prevent unnecessary invasive procedures and overdiagnosis.
Focal transperineal laser ablation (TPLA) treatment of localized prostate cancer: short‐term functional outcomes and toxicity
LA van Riel, TM de reijke, HP Beerlage, JR Oddens, M Martins, S Regusci
Department of Urology, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, the Netherlands
Introduction & Objective: Standard radical therapy of localized prostate cancer (PCa) has a high risk of side effects, such as incontinence and erectile dysfunction. As an alternative, several focal ablative techniques are under investigation. SoracteLite™ TPLA is such a novel minimal invasive treatment that is expected to result into reduced side effects with an acceptable toxicity profile. In order to evaluate if TPLA preserves urinary and sexual function with low toxicity we analyzed prospectively collected data on patients with localized PCa that opted for TPLA. We analyzed short‐term functional outcomes and the toxicity profile after TPLA.
Methods: SoracteLite™ TPLA was performed in 60 patients with localized disease from May 2018 until February 2021, of which 6‐months follow‐up data was available of 44 patients (treatment naïve n = 31, salvage TPLA n = 13). TPLA was performed using a one‐ or multi‐laser fiber configuration at 3W or 5W, dependent on PCa distribution on MRI and biopsies. TPLA procedures were conducted under continuous ultrasound guidance using the Echolaser device and local anesthesia, sedoanalgesia or general anesthesia. Functional outcomes (Qmax, IIEF‐5, IPSS and QoL) and toxicity (adverse events) until 6‐months follow‐up were compared with baseline.
Results: Median patient age was 70.5 years, and median prostate‐specific antigen (PSA) was 6.2 (IQR 4.94) ng/mL. Gleason score was 3 + 3 = 6 in 16 (36.4%), 3 + 4 = 7 in 23 (52.3%), 4 + 3 = 7 in 4 (9.1%) and 4 + 4 = 8 in 1 (2.2%) patient(s). Tumor stage was T1c in 37 (86%) and T2a in 6 (14%) patients. No adverse events were reported until 6 months follow‐up (n = 44). There were no significant differences between baseline and 6 months follow‐up regarding urinary and sexual function (figure 1).
Conclusions: These results show that TPLA is a safe minimal invasive focal treatment of localized PCa that preserves urinary and sexual function with no toxicity, oncological outcome has to be awaited.
Single center retrospective analysis of oncological and functional outcome in Magnetic resonance imaging‐guided transurethral ultrasound ablation (MRI‐TULSA) for the treatment of localized prostate cancer
F Leboutte, G Meskhia, L Meyer, O Lemmer, J Van de plas, W Willinek, A Neisius
Dept. of Urology, Krankenhaus der Barmherzigen Brüder Trier, University of Mainz, Germany
Introduction & Objective: Magnetic resonance imaging‐guided transurethral ultrasound ablation (MRI‐TULSA) is an alternative to the current HIFU minimal‐invasive treatment for focal ablation of prostate tissue. Real‐time thermometry acquired during treatment may be beneficial in terms of therapy results and safety.
Since April 2019, our institution has performed a total of 41 MRI‐TULSA therapies. This retrospective study analyses oncological and functional outcomes of this novel therapy for localized prostate cancer with a follow‐up up to 22 months
Methods: We evaluated retrospectively all MRI‐TULSA therapies performed in a tertiary‐level urology center.
In total, 16 patients had a low‐risk (Gleason 6) prostate cancer, and 24 patients had an intermediate‐risk (Gleason 7a or 7b) prostate cancer. One patient received a salvage MRI‐TULSA in a palliative post‐radiotherapy setting.
Treatment extent reached from focal (9.7%), half gland (29.3%) to whole gland (61%).
Results: The median follow‐up was 11.3 months (range 1‐22). The mean pre‐treatment PSA was 10.2 ng/ml (1.6‐39.8 ng/ml). Post‐treatment PSA nadir was 2.0 ng/ml (0.0‐14.8 ng/ml). Early remission in MRI was 46.3%. Two salvage procedures due to high‐risk prostate cancer relapse have been performed. Therapy needed to be repeated in two cases because of technical issues during the first session. 30‐day postinterventional complications were assessed by the Clavien Dindo Classification with 34.1% Grade 1, 12.2% Grade 2, and 4.9% Grade 3 complication.
Conclusions: First results of our retrospective single‐center trial show promising therapy results in terms of safety, oncological and functional outcome. Patient selection and counseling are crucial for compliance and oncological results. Follow‐up data is still sparse. Further evaluation in a prospectively conducted cohort study is planned.
Cancer control and safety outcomes following focal therapy using HIFU in 1,379 men with non‐metastatic prostate cancer: a multi‐institute 15 year experience
D Reddy, M Peters, T Shah, M Bertoncelli‐Tanaka, P Huber, D Lomas, A Rakauskas, S Guillaumier, T Dudderidge, R Hindley, A Emara, R Nigam, M Valerio, N Afzal, C Moore, M Arya, M Winkler, C Orczyk, M Emberton, H Ahmed
Imperial Prostate
Introduction & Objective: Focal therapy aims to treat areas of cancer to confer oncological control whilst reducing treatment‐related functional detriment. We report the oncological outcomes and adverse events following focal HIFU for treating non‐metastatic prostate cancer.
Methods: Analysis of 1379 patients with 6 months follow‐up or greater prospectively recorded in the HEAT registry from nine UK centres (17/11/2005‐30/01/2020). Intervention Focal HIFU therapy using a transrectal ultrasound‐guided device (Sonablate, Sonacare).
We report Failure‐free survival (FFS) was primarily defined as avoidance of salvage whole‐gland or systemic treatment, metastases or prostate cancer‐specific mortality. Differences in FFS between D'Amico risk groups were determined using log rank analysis. Adverse events were reported using Clavien‐Dindo classification.
Results: Of all 1379 treated, median (IQR) age was 66 years (60‐71) and PSA 6.9ng/ml (4.9‐ 9.4) with D'Amico intermediate in 65.0% (896/1379) and high‐risk in 28.0% (386/1379). Median follow‐up for all patients was 32.1 (17.0‐58.1) months. 252/1379 (18.3%) had a repeat focal ablation due to residual or recurrent cancer; overall 92/1379 (6.7%) patients transitioned to salvage whole‐gland treatment. Kaplan‐Meier 3, 5 and 7 year FFS was 93% (91‐95%), 82% (79‐86%), and 69% (64‐ 74%), respectively (figure 1). There was no statistically significant difference in 7 year FFS between intermediate and high‐risk disease (68% [95% CI 62‐75%] and 65% [95% CI 56‐74%], p = 0.30). Adverse events with Clavien‐Dindo score >2 occurred in 0.4% (6/1379). 10‐15‐ year follow‐up is lacking.
Conclusions: Focal HIFU in carefully selected patients with clinically significant prostate cancer has good cancer control in the medium term. Patient Summary Focal HIFU treatment to areas of prostate with cancer can provide an alternative to treating the whole prostate. This treatment modality has good 5‐7 (medium‐term) cancer control, whilst 10‐15‐year data is awaited.
Suitability of focal therapy for prostate cancer in patients undergoing image guided transperineal biopsies
D Reddy, D Eldred‐Evans, N McCartan, F Hosking‐Jervis, H Ahmed
Imperial Prostate
Introduction & Objective: Commonplace concerns regarding the uptake of focal therapy are the proportion of men with suitable disease characteristics. We evaluated the suitability of focal therapy in cases reported within a number of prospective studies incorporating the use of pre‐biopsy MRI and transperineal prostate biopsies.
Methods: The databases analysed were: Cohort 1) 330 men with negative or equivocal TRUS‐guided biopsies underwent mapping +/‐ targeted biopsies; Cohort 2) 2372 men referred by their GP with a clinical suspicion of prostate cancer, Cohort 3) 411 men recruited into community‐based screening study and Cohort 4) 740 biopsy naïve men with elevated serum PSA . Criteria determining suitability for focal therapy were: i)PSA = /< 20ng/ml, ii)MRI stage = /< rT3aN0M0, iii)proposed treated area to contain either Gleason 3 + 3 = 6 and cancer length >/ = 6mm, or any cancer length of Grade 3 + 4 = 7 or 4 + 3 = 7, iv)out‐of‐field can have up to 5mm Gleason 3 + 3 = 6 placed on surveillance, and v)no more than 50% of the gland to be treated.
Results: Within cohort 1, 2, 3, and 4 168/330 (50.9%), 495/2372 (20.9%), 35/411 (8.5%) and 406/740 (54.9%) had prostate cancer, respectively. Of these, 100/168 (59.5%), 327/495 (66.1%), 17/35 (48.5%) and 186/406 (45.8%) had disease suitable for focal therapy (Figure1). High‐grade ± high‐volume disease does not appear to be a significant limitation to offering focal therapy to patients with T‐stage ≤rT3a, with 6/168 (3.6%), 142/495 (28.7%), 0/35 (0%) and 129/406 (31.8%) reported within cohort 1, 2, 3 and 4 respectively.
Conclusions: Proportions of men diagnosed with prostate cancer and suitable for focal therapy using various diagnostic pathways are highly consistent with about 4‐6 in 10 of newly diagnosed men being eligible for focal treatment.
Withdrawn
Withdrawn
PROST: the future of robotic prostate biopsy
A Iseppi, S Puliatti, M Rizzo, M Bogdan, C Tenga, L Palladino, M Sighinolfi, BC Rocco, P Fiorini, S Micali
Azienda ospedaliero‐universitaria di Modena e Reggio Emilia, Modena, Italy
Introduction & Objective: PROST is a novel robotic device for transperineal prostate biopsy designed to minimize the human error by introducing a level of autonomy in the execution of the key steps of the procedure., i.e. target selection, image fusion and needle positioning, each of which must be approved by the physician.
The robot can execute targeted biopsy with ultrasound (US) guidance, fusion biopsy with magnetic resonance (MR) images, where the target was defined. To decrease error rates, PROST can track the US images and has the ability of 3D reconstruction, real‐time US segmentation, and automatic or semi‐automatic image registration. The aim is to evaluate the targeting ability of the PROST system.
Methods: We evaluated the system performance by assessing its pointing capabilities to the target, leaving the biopsy core sampling to the human operator. The accuracy tests were first performed on a 3D printed object with 9 spherical targets of 2 mm diameter and the results were computed by comparing its CAD model to the real‐time US images. Then, we used an anatomical commercial phantom that simulates the human prostate and some internal and external structures. The phantom contains 3 lesions of about 10 mm diameter, which are visible in both MR and US images. The registration of the phantom with the reference image (CAD or MRI) was realized semi‐automatically in the first test and automatically by using a real‐time segmentation algorithm in the second test. Although the robot can duplicate by software any desired biopsy pattern, its main application is envisioned for focused biopsy, where a suspicious area is sampled several times. To reduce the number of the insertion points, the robot can compute the minimum number of entry points for a given target and more samples can be acquired through a single entry point by changing the needle orientation.
Results: The accuracy reached in the laboratory experiments was 1.30 ± 0.44 mm in the first test and 1.54 ± 0.34 mm in the second test for all 3 lesions.
Conclusions: We introduced the first prototype of PROST a robot for transperineal biopsy that has the potential to increase the detection of clinically significant prostate cancer and, by including some level of autonomy, to simplify the procedure. The robot prototype was tested in‐vitro and we are currently collecting results from tests on cadavers.
Prospective analysis of MRI‐fusion and systematic biopsy. Do we overlook or overdiagnose?
A Morozov, M Taratkin, E Bezrukov, D Chinenov, A Amosov, K Puzakov, D Enikeev
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia
Introduction & Objective: MRI‐fusion biopsy seemed to be a promising addition to precise prostate cancer (PCa) lesion targeting, but its role in PCa detection is perceived to be increasingly controversial. Our study aimed to determine the role of software MRI‐guided fusion and systematic biopsy in biopsy naïve and secondary patients in order to understand what the potential benefits and drawbacks of MRI‐guidance and systematic biopsy are.
Methods: We included prospectively patients with PCa suspicion, and both biopsy naïve and secondary patients were included. All patients have undergone MRI on Siemens «Magnetom Verio» 3T, obtained data were analyzed by one, highly experienced radiologist. For MRI‐fusion a MIM software was used (bkFusion™, MIM Software Inc., Cleveland). All MRI‐guided/systematic biopsies were done by a single surgeon. During MRI‐guided/systematic biopsies firstly specimens were obtained from the suspicious lesion (according to MRI), then systematic biopsy through brachytherapy grid was performed.
Results: The study included 150 patients, 114 (76%) of them underwent primary MRI‐guided/systematic biopsy; 36 (24%) patients were secondary. Mean age 63.9 ± 6.9 years, median age 64 (IQR 59‐69) years, mean prostate volume 62 ± 41 сm3, median – 49 (IQR 35‐70) cm3, mean PSA 11.9 ± 14.7 ng/ml, median −7.8 (IQR 5.1‐13.4) ng/ml. Pi‐RADS 2 score distribution was as follows: score 2 – 21 (14%) cases, 3 – 36 (24)%, 4 – 52 (34.7%), 5 – 41 (27.3)%. During MRI‐fusion a median 5 (IQR 4‐7) cores were obtained, during systematic biopsy a median 26 (IQR 22‐30) cores were obtained. The cancer detection rate for primary fusion biopsy was 64%, for secondary – 75%. In 4 secondary cases (11% of this group) MRI‐fusion biopsy allowed to detect ISUP 4 or 5 (clinically significant) PCa. The additional cancer detection rate for systematic biopsy was 16.5%. Of these, 89% had ISUP 1 and 11% ‐ ISUP 2 PCa. The additional cancer detection rate for targeted biopsy was 10.4%. Out of these, 16.7% had ISUP 4 and 8.3% ‐ ISUP 5 PCa.
Conclusions: The efficacy of both primary and secondary fusion biopsy in prostate cancer detection is high. The supplementation of template‐guided random biopsy during targeted led to an increase in the detection rate by detecting a clinically insignificant prostate cancer. Targeted biopsy showed increased accuracy in detecting clinically significant cancer, deeming a minimal need for additional systematic biopsy.
Irreversible electroporation of localized prostate cancer: prospective assessment of safety and efficacy
A Shpikina, D Enikeev, M Taratkin, A Morozov, N Singla, J Rivas, E Barret, V Petov, P Glybochko
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia
Introduction & Objective: Irreversible electroporation (IRE) is an emerging non‐thermal modality for prostate cancer (PCa) treatment. We aimed to assess the preliminary data on focal IRE efficacy and safety in patients with localized PCa.
Methods: After local IRB approval and registration of the protocol (NCT03504995), patients with localized PCa (PSA ≤15 ng/ml; ISUP 1‐2; T2aN0M0) were prospectively enrolled. PSA, TRUS, Qmax, IPSS and IIEF‐5 were assessed prior to the surgery and at 1, 3, 6 and 12 months postoperatively. Patients were followed up (FU) with MRI and MRI‐guided and systematic biopsy 6 and 12‐month intervals, respectively. Failure was defined as the presence of any residual PCa lesion in the treated area. The primary and secondary endpoints were the in‐site relapses and the safety of the treatment.
Results: 18 patients underwent IRE. The mean age was 64 (52‐79) years, median PSA was 7.2 (IQR 5.2; 8.1) ng/ml. The median PSA was 3.8 (IQR 1.6; 7) ng/ml, 3.9 (IQR 1.6; 6.4) ng/ml, and 4.1 (IQR 2.4; 5.2) ng/ml at 3‐, 6‐ and 12‐months FU respectively. The median preoperative IPSS, QoL and IIEF‐5 was 12 (IQR 8; 15), 4 (IQR 2; 5) and 17 (IQR 9; 21) respectively. The mean time of each procedure did not exceed one hour. Data on patients who reached the FU periods are presented in Table 1. At 6‐ and 12 months FU, mp‐MRI revealed PiRADSv2.1 ‐ 2 and 4 lesions in 2 (11.1%) and 3 cases (16.7%). After 1 yr., in‐field relapse was observed in 4 patients (22.2%) with ISUP grade 1 (n = 3) and 2 (n = 1) at follow‐up biopsy. In 3 cases out‐field relapse were found (16.7%), follow‐up biopsy was positive with an ISUP grade 1 (n = 2) and 2 (n = 1). Focal IRE was not associated with urinary incontinence of sexual toxicity. The median IPSS, QoL and IIEF‐5 were 8 (IQR 4; 13), 2 (IQR 2; 5) and 17 (IQR 10; 20) at 6 months FU. One patient refused to continue sexual activity and to fill out the questionnaire due to his psychological concerns about possible cancer progression. The postoperative complications were recorded in 2 patients (11.1%) and were classified between Clavien grades I–II (hematuria and hematospermia).
Conclusions: Focal IRE can be safely performed in selected patients with adequate short‐term cancer control and low morbidity rate. Results of a longer follow‐up series is awaited.
The safety and satisfaction of transperineal prostate biopsy under local anaesthetic in an outpatient setting
W Abou Chedid, GJ Nason, E Brokane, AT Evans, D Moschonas, MA Perry, S Langley
Royal Surrey NHS Foundation Trust
Introduction & Objective: The aim of this study was to assess the safety and satisfaction of transperineal prostate biopsy under local anesthetic in an outpatient setting.
Methods: A telephone survey was performed of 100 consecutive patients who underwent transperineal biopsy of the prostate under local anesthetic in the outpatient setting.
Results: 84 patients responded. Overall cancer and clinically significant (Grade group 2 or above) cancer detection rates were 65.5% and 62%, respectively. One (1.2%) patient was readmitted to hospital following biopsy. Nine (10.7%) patients developed acute urinary retention. There was no difference in median prostate volume (40cc vs 43cc, p = 0.79) nor number of biopsy cores taken (19.8 vs 18.1 p = 0.36) between those who developed retention and those who did not. Perineal pain lasted for one day or less in 58(70%) of patients. Hematuria was reported by 33(39.3%). Transient erectile dysfunction was apparent in 16(19%). When asked if they required a further biopsy in the future, 75(89.3%) patients reported they would undergo a biopsy under local anesthetic as opposed to general anesthetic.
Conclusions: Transperineal biopsy of the prostate under local anesthetic in the outpatient setting is safe and well tolerated by patients. Cancer detection rates are comparable to other methods of prostate biopsy.
Is prostate cancer detection influenced by biopsy needle length? A prospective study
A Cardoso, R Calaia, C Laranjo Tinoco, R Matos Rodrigues, S Anacleto, E Lima, E Dias
Hospital de Braga, EPE
Introduction & Objective: Transrectal ultrasound‐guided prostate biopsy (TRUSPB) is one of the main procedures for prostate cancer (PCa) definite diagnosis. Studies have been focused on its diagnostic value improvement, some through the analysis of the impact of the number, fragmentation and length of biopsy cores obtained. Thus, we aim to compare 25 millimetres (mm) and the conventional 18mm depth biopsy needles (DBN) regarding: sample core length, Gleason scores (GS) obtained, PCa detection and complications rate.
Methods: In this prospective study, we included 124 patients submitted to randomized 12‐core TRUSPB, who were divided in 2 groups: A for 18mmDBN, and B for 25mmDBN. We collected data regarding age, digital rectal examination (DRE), prostate‐specific antigen (PSA) serum levels, prostate volume, GS, and biopsy cores characteristics. Complications were evaluated: immediately (pain scale), and 1 week (questionnaire) after TRUSPB.
Results: Group B presented significantly higher prostate volumes (45.69 ± 9.51mL versus 40.60 ± 9.98mL, p = 0.004), and higher mean core’ lengths (21.07 ± 1.54mm versus 15.53 ± 0.99mm, p < 0.001). PCa detection rate, GS, number of positive cores, and percentage affected, were not significantly different between groups (Table 1). Although without statistical significancy, PCa detection rate was higher for group B patients with prostate volumes of 40‐60mL, suspicious DRE, and PSA >10ng/mL, in comparison with equivalent A subgroups (Table 2). There were no differences on pain intensity and complications rate.
Conclusions: TRUSPB with 25mmDBN retrieves longer cores. However, this does not seem to translate into a significant PCa detection advantage. Still, our results suggest that patients with larger prostate glands, suspicious DRE and/or higher PSA levels, might benefit more from 25mmDBN TRUSPB, which is equally safe than 18mmDBN. Further studies are sugested.
Does large prostate size, small lesion volume, or long lesion distance from biopsy probe reduce MRI targeted cancer detection?
M Bevill, J Drobish, B Barnes, CR Tracy, P Gellhaus
Introduction & Objective: MRI targeted prostate biopsies increase prostate cancer detection. We hypothesize that large prostate size, small lesion volume, or long lesion distance from the ultrasound probe would decrease cancer detection with transrectal MRI targeted biopsies.
Methods: Patients undergoing UroNav‐assisted MRI target biopsy at our institution from 5/2017 to 8/2019 were enrolled in a prospective database. Three to five cores were obtained from ≥3 PI‐RADSv2 lesions. A multivariate model was created and included lesion distance from the ultrasound probe, PSA, PIRADS, lesion volume, and prostate volume.
Results: 377 patients with 533 lesions were registered. 233 lesions (44%) were positive for any prostate cancer and 173 lesions (32%) had clinically significant prostate cancer (csPCa). The mean distance from the rectum to lesion was 11.7 mm (IQR 7.6‐15.5 mm), prostate volume 44 grams, lesion diameter 13 mm, and PSA 8.18 ng/dl. The likelihood of obtaining a positive core on biopsy decreased as distance from the ultrasound probe increased for all prostate cancer and csPCa (p = 0.018 and p = 0.004, respectively (Figure 1). For every 10 mm away from the rectum, there was 18% less cancer detection. Similarly, as prostate volume increased, the odds of obtaining a positive core also decreased (p = 0.039) (Figure 2). For every 50g increase in prostatic volume, there was a 10% reduction in cancer detection. There was no significant association between lesion size and amount of cancer detected. Lastly, the probability of obtaining a positive core on biopsy increased with PSA, PIRADS, and an apical location (p = 0.036, p = 0.054, and p = 0.021 respectively).
Conclusions: Transrectal MRI targeted biopsy cancer detection decreased the further away the lesion was from the ultrasound probe and with large prostate volume, while it did not change with lesion volume.
Detection of Prostate Cancer using MRI US Guided Fusion Biopsy Processed and Contoured with Predictive Fusion: All in the Urologists Office
O Liseth, B Tran, N Sarantos, RI Carey, S Mclaughlin, ML Blute, V Bird
National Med. Assoc. and Research Group
Introduction & Objective: The aim of this study was to evaluate the early results of using in office based contouring software for MRI US guided fusion biopsy and to report detection rates in MRI PIRADS 1‐5 in lesions identified by a urologist.
Methods: The study included 44 consecutive patients who had an elevated prostate‐specific antigen level over 4 ng/dL, and/or abnormal digital rectal examination. MRI 3T images were analyzed using contouring software which included analysis of T2W axial and coronal images, Diffusion weighted images and Apparent Diffusion Coefficient mapping. MRI PIRADS 1‐5 scored images were analyzed, and lesions identified were contoured and traced. All MRI‐US guided fusion core biopsies as well as 12 core systematic biopsies were performed in office with local sedation. Statistics were done using Fisher's Exact Test and Microsoft Excel software (version 16.35).
Results: Our cohort included PIRADS 1 and 2, 3, 4, and 5 which were 36%, 39%, 18% and 7% respectively. The overall PCa (Prostate Cancer) detection rate was 65.8% (MRI PIRADS 1‐5). In PIRADS 1 and 2, PCa was detected in 63%, of which 10% were found to have clinically significant PCa (csPCa). In this group systematic biopsies identified 33% of PCa including csPCa. In PIRADS 3, 53% had PCa of which 67% were csPCa. Systematic biopsies identified 10% of Pca. In PIRADS 4, 63% had PCa of which 100% were csPCa. Systematic biopsies did not add any additional significant information. In PIRADS 5, 100% had PCa of which 100% were csPCa. Systematic biopsies did not add any additional significant information. PSA densities in csPCa found in PIRADS 1‐2, 3, 4 and 5 were 0.12, 0.34, 0.56 and 0.32 respectively.
Conclusions: It is possible and feasible for urologists to process MRI data for contouring and tracing lesions across PIRADS 1‐5 for MRI US guided fusion biopsies, which allows MRI fusion biopsy to be incorporated as part of the regular in office procedures with comparable results to radiologist contoured MRI processing. Future efforts which may include genomic studies should identify the significance of PCa present in the PIRADS 1‐2 cohort.
Moderated Poster Session 22: Education
3D automatic augmented reality Artificial intelligence technology during robot‐assisted radical prostatectomy: a new tool for a more accurate extracapsular extension identification
F Porpiglia, E Checcucci, D Amparore, P Piazzolla, M Manfredi, A Pecoraro, S De Cillis, A Piana, G Volpi, F Piramide, P Alessio, S Granato, E Vezzetti, C Fiori
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
Introduction & Objective: The aim of this study was to evaluate the accuracy of our new Artificial Intelligence based Automatic Augmented Reality (AR) system, in order to identify tumour's extracapsular extension (ECE) at the end of the extirpative phase of robot assisted radical prostatectomy (RARP) for cT3 tumours.
Methods: From December 2020, RARP candidates with suspicious ECE at preoperative high‐resolution multi‐parametric magnetic resonance imaging (mpMRI, 1‐mm slices) were enrolled in the study according to a dedicated protocol. The obtained three‐dimensional (3D) reconstruction was overlapped to the endoscopic in‐vivo anatomy and sent back to the DaVinci robotic console by using the Tile‐Pro, allowing to perform AR‐RARP. Specifically for this study we developed a new AR software based on artificial intelligence convolutional neuronal networks that was able to automatically identify the catheter in the prostatic lodge at the end of the extirpative phase, overlapping automatically the 3D virtual images. Selective biopsies guided by 3D AR images were then performed at the level of suspicious ECE.
The Cohen kappa coefficient (k) was calculated to define correspondence between preoperative suspected ECE and pT3 stage at final pathological examination.
Results: 10 patients with suspicious ECE detected with preoperative mpMRI were enrolled. The final pathology confirmed ECE (pT3a) in 8/10 cases, with a Cohen Kappa coefficient (κ) of 0,68. After standard nerve‐sparing RARP, AR guided biopsies of the surgical bed revealed the presence of cancer in 75% of the cases, confirming the accuracy of the 3D models overlapping.
Conclusions: Present findings suggest that the new evolution of our AR platform based on artificial intelligence convolutional neuronal networks allows an effective Automatic AR RARP. The 3D virtual images, automatically anchored to the catheter, allow to correctly identify the location of ECE at the level of NVBs.
Does an endourology fellowship training affect practice patterns
T Aro, A Smith, A Rai, D Mikhail, D Hoenig, AD Smith, Z Okeke
The Smith Institute for Urology
Introduction & Objective: Endourology is a constantly growing field, with a large volume of practitioners and training background worldwide. We aim to examine the effect of fellowship training on practice patterns
Methods: An online questionnaire comprised of 6 categorizing questions, and 31 multiple choice questions looking into common endourologic scenarios and practice pattern was sent using the endourology society contact list.
Results: 279 responses were sorted into 102 fellowship‐accredited (FA), 58 fellowship‐unaccredited (FU), and 119 no fellowship (NF) trained responses. See table for full results.
Conclusions: Fellowship training has some minor affects such as 54% more likely to using balloon dilators in PCNL and positioning bolsters vertically. And more pronounce practice changes, like 140% more likely to be flexible with supine and prone positioning, and 63% more likely to utilize ultrasound‐guidance in certain scenarios. Specifically, an accredited fellowship training results in a higher chance of feeling comfortable with a same day bilateral PCNL compared to both an unaccredited fellowship and no fellowship training urologist.
The History of Midwest Stone Institute (MSI) in Saint Louis: The Gateway to Endourology Training
AK Chow, BG Patel, J Palka, A Paradis, RS Figenshau, R Venkatesh
Washington University School of Medicine
Introduction & Objective: Prior to the development of minimally invasive technology and techniques, open surgical treatment of urolithiasis was the sole modality of stone treatment. Moving in parallel with the evolution of surgical technology, we saw the development of medical technology allowing for stone treatment from within the urinary tract, omitting the need for surgical incisions. Endourology now exists today in every façade of practice setting across the globe and unbeknownst to most, has its significant ties to a Midwest city (St. Louis) in America.
Methods: This is a historical review of Midwest Stone Institute (MSI) at Washington University School of Medicine (WUSM) in St. Louis. Information was obtained through review of MSI historical timeline and interviews with previous endourology fellows and Washington University staff and faculty
Results: St. Louis, Missouri in the United States, the city dubbed as the gateway to the American Western frontier, found itself as a gateway once again in the late 1980's, this time to Endourology. In 1984, a Missouri state level committee installed the Midwest Stone Institute (MSI) as a consortium of over 50 urologists from the St. Louis area. In collaboration with MSI, Ralph V Clayman, MD established the first endourology fellowship in 1984 at WUSM. Since then, the fellowship has had several pioneering achievements including the first successful lithotripsy utilizing the Dornier HM‐3 lithotriptor (1985), the EDAP LT‐02 (1993), and the mobile Dornier HM‐3 (1994), just to name a few. In addition to fellowship training, MSI was certified as the first AUA certified site in Missouri, providing physician teaching in ESWL (1986). Other landmark achievements in the field of Endourology include the first laparoscopic nephrectomy (1991), laparoscopic partial nephrectomy and laparoscopic nephroureterectomy. Since its inception, MSI and WUSM has contributed to the training of 53 endourology fellows with 24 (45%) pursuing academic careers and 9 attaining ranks of full professorships. Six of these graduates now practice in international grounds. There are currently six graduates in active leadership roles: 3 department chairs and 3 chief of service of premier urology programs. Furthermore, Endourology fellowships have /bourgeoned under the guidance of the past graduates, lending specialized endourology teaching to many practicing urologists today.
Conclusions: MSI and WUSM is strongly rooted to the beginnings of endourology training. Under the auspices of MSI, we have seen significant contributions to the development and proliferation of both surgical techniques, leadership and teaching at the national and international level.
A Machine Learning Predictive Model of Post‐Ureteroscopy Urosepsis: A Case‐Control Study of 9 European centers from YAU endourology group
A Pietropaolo, A Rogers, R Geraghty, R Veeratterapillay, P Kallidonis, L Villa, L Boeri, E Montanari, G Atis, E Emiliani, E Sener, F Al Jaafari, J Fitzpatrick, M Shaw, C Harding, BK Somani
University Hospital Southampton
Introduction & Objective: Ureteroscopy is becoming an increasingly common procedure to treat kidney and ureteral stones. Post‐ureteroscopic urosepsis is an uncommon but serious complication. There are no machine learning models of this in the literature.
Methods: Cases were patients who developed post‐ureteroscopic urosepsis requiring ITU care, these were identified from 9 European hospitals. Controls were matched for age and sex, and as far as possible for: diabetes, immunosuppression, neurological disorders, previous urinary tract reconstruction and abnormal upper tract anatomy. A random forests machine learning model was generated using the random. Forest package in R with 300 trees. Random 30% sample of dataset was used as the test set.
Results: There were 57 cases and controls (total, n = 114). Mean age was 60 years (SD:16) for both and there were 26 men in each group (46%). The model correctly predicted 14/17 cases and 12/15 controls. Model accuracy was 81.3% (95% CI: 63.7%‐92.8%), sensitivity = 0.80, specificity = 0.82, area under the curve = 0.89. Predictive values most commonly accounting for nodal points in the trees were: increasingly proximal stone location, increasing stent time, increasing stone size and increasing operative time.
Conclusions: Post‐ureteroscopic urosepsis is reasonably accurately predicted by this machine learning model. External validation is required.
National Implementation of a Virtual Subinternship in Urology
D Mikhail, EJ Margolin, A Paniagua‐Cruz, M Schwartz, M Feuerstein, LR Kavoussi, GM Badalato, L Richstone
Lenox Hill/Northwell Health
Introduction & Objective: In‐person subinternships for visiting medical students were discouraged during the COVID‐19 pandemic. The Society of Academic Urologists (SAU) endorsed virtual subinternships in urology (vSIU) and provided all institutions with a standardized vSIU Guidebook containing a structured curriculum and curated resources. We sought to evaluate the successes and limitations of the vSIU at a national level.
Methods: In December 2020, we sent anonymous surveys via email to all medical students who submitted applications to the urology residency match and to all urology residency program directors (PDs) and associate PDs on the SAU email list. Surveys evaluated goals, curriculum composition, satisfaction, and future reusability. Outcomes were evaluated on a 5‐point Likert scale.
Results: A total of 162 students (30%) and 78 PDs (48%) completed the survey, including 76 students (47%) and 32 PDs (41%) who participated in vSIU at 29 institutions. Of these electives, 66% were 1‐2 weeks in duration, 48% were full‐time, and 76% utilized the SAU guidebook. Electives consisted of a wide range of curricular elements (Figure). The most important goals for both students and PDs were experiencing/demonstrating program culture and evaluating whether the program/student are a good fit (≥ 50% rated “extremely important”). These goals were achieved by >80% of students and PDs. Overall, 79% of students and 78% of PDs rated the vSIU “excellent” or “very good.” On multivariable ordinal logistic regression, duration ≥3 weeks and class size ≤4 students were associated with higher student ratings (p < 0.05). Full‐time electives, class size ≤4 students, and utilization of the SAU guidebook were associated with higher PD ratings (p < 0.05). Although the majority of respondents found the vSIU less effective overall than in‐person subinternships, 46% of students and 66% of PDs recommended incorporating virtual components into future electives.
Conclusions: Amid a global pandemic, the vSIU was a successful nationwide initiative to provide virtual urological education to medical students. Though the vSIU should not replace in‐person subinternships, the electives were highly rated and achieved the most important goals for students and PDs. The most successful courses were full‐time, longer, had smaller class sizes and utilized the SAU Guidebook.
3D virtual models guidance during minimally invasive partial nephrectomy: a new technology to reduce the loss of functioning renal parenchyma
D Amparore, A Pecoraro, E Checcucci, F Piramide, P Verri, S De Cillis, P Alessio, G Volpi, A Piana, J Mézière, M Burgio, F Solitro, A Veltri, C Fiori, F Porpiglia
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
Introduction & Objective: 3D virtual models (3DVMs) are nowadays under scrutiny to improve partial nephrectomy (PN) outcomes. We aimed to analyze if 3DVMs could impact the renal function preservation after minimally‐invasive PN.
Methods: 100 patients treated with minimally‐invasive PN were prospectively enrolled. Inclusion criteria were the availability of contrast‐enhanced CT from which a 3DVM was obtained, baseline and 3rd‐month postoperative renal scan. These patients were then compared with a control group of 251 patients underwent minimally‐invasive PN with the same renal function assessments but without 3DVMs. Weighted‐differential values of preoperative and 3rd‐month postoperative renal can based estimated renal plasmatic flow (ERPF) was calculated, according to the availability of 3DVMs and PADUA risk category (6‐7 vs. 8‐9 vs. >10). Multivariable logistic regression (MLR) models predicting a significant loss of renal function (defined as ERPF drop >20%) were performed, overall and according to each PADUA risk category.
Results: Concerning functional outcomes, 3DVMs group baseline weighted differential ERPF showed significantly lower loss of renal function (‐10%) in comparison with the control group (‐19.6%), p = 0.02. In MLR, the availability of a 3DVM was found to be the only protective factor against a significant loss of renal function (OR = 0.3, p = 0.002). After stratification per tumor surgical complexity, this protective role was observed also in both PADUA 8‐9 and ≥10 category risk patients (OR = 0.3, p = 0.03 and OR = 0.1, p = 0.01) (figure 1).
Conclusions: The operated kidney function drop was significantly lower in those surgeries assisted by 3VDMs, resulting their availability the only protective factor against a significant functional damage, and justifying their introduction in clinical practice.
Comparing long term functional outcome between transperitoneal and the retroperitoneal approach in patients who have had robotic assisted partial nephrectomy
KE Okhawere, W Nkmedrim, A Beksac, TG Korn, KN Meilika, R Harrison, M Ahmed, JY Lee, R Abaza, DD Eun, A Bhandari, AK Hemal, J Porter, MD Stifelman, KK Badani
Icahn School of Medicine at Mount Sinai
Introduction & Objective: Both the trans‐peritoneal (TP) and retro‐peritoneal (RP) approaches have been well studied and effective approaches for robotic partial nephrectomy (RPN). Although the literature demonstrates equivalency of operative and hospital‐based complications, no studies have evaluated the functional outcome of these approaches. We sought to compare the long term renal functional outcomes between TP and RP after robotic assisted partial nephrectomy.
Methods: Data was obtained from our multicenter database of patients who underwent robotic partial nephrectomy (RPN) between January 2006 and January 2019. We identified 898 patients that met the eligibility criteria and underwent either TP‐RPN (n = 568, 63.25%) or RP‐RPN (n = 330, 36.75%). Patients were propensity scores matched using baseline demographic, clinical and tumor characteristics: transperitoneal ‐RPN (n = 252, 50%) and retroperitoneal ‐RPN (n = 252, 50%). The associations between baseline demographic and clinical data, perioperative data, postoperative and renal functional outcome data were compared in the propensity matched cohort at a median follow‐up of 14 months using chi‐square, Fisher's exact test, Mann‐Whitney and a linear mixed effect model.
Results: There was no significant difference in the baseline demographic, clinical and tumor characteristics in the PS matched cohort. Operative time (P = <0.001) and blood loss (P = <0.001) were significantly different and low in the RP group; However, there was no differences in ischemia time (P = .257), overall post‐operative complications (P = .096), major complication (P = .240). There was also no difference in last follow‐up eGFR (P = .567), delta eGFR (P = .137), and denovo chronic kidney disease at median 14 months (P = .096). In the linear mixed effect model, the difference in mean eGFR at baseline (TP vs RP; b = ‐1.12 95% confidence interval [CI]: ‐5.10, 2.85) and the change in eGFR over time (TP vs RP; b = 0.08 95% CI: ‐0.06, 0.23) were also not significantly different between surgical approaches.
Conclusions: Our large study comparing TP and RP‐RPN demonstrates equivalent clinical outcomes for ischemia time, LOS, and complication rates for both approaches. The RP has a modestly shorter operative time and blood loss. Importantly, renal functional outcome between the RP and TP groups were not significantly different in a propensity‐matched cohort. The next step to validate these findings is a randomized trial
Transurethral Bladder Tumor Resection Simulator‐based Training, Courses and Curricula
K Pagonis, A Peteinaris, A Vagionis, C Adamou, T Tokas, D Liourdi, G ortner, M Obaidat, A Natsos, E Liatsikos, P Kallidonis
Introduction & Objective: Transurethral bladder tumor resection is one of the most common everyday urological procedures. Nevertheless, this kind of surgery demands a set of skills that need training and experience. In this review we investigated the current literature to find out if simulators, phantoms and other training models that could be used as a tool of teaching urologists alone, or within the boundaries of a course or a curriculum for transurethral bladder tumor resection.
Methods: A systematic review was performed according to PRISMA statement and the recommendations of the European Association of Urology Guidelines office for conducting systematic reviews. 14 out of 924 studied met our inclusion criteria and are presented in the current review.
Results: It was found that Uro‐trainer achieved positive feedback and an excellent face and construct validity by the participants of two surveys. The use of this VR training simulator showed an improvement of inexperienced urologists and medical students for the percentage of bladder mucosa detected, blood loss, tumor resection and surgery time after the training. In addition, SIMBLA® simulator was found a realistic and useful tool by expert and intermediate (based on experience) urologists and TOCO model that was based on SIMBLA® simulator could be used for evaluating urologists. The porcine model of AUSTEG received also positive feedback by the participants that tried it. The STeLI project had an extraordinary face and content validity and 60% of participants would like to use the simulators in the future. The 5‐day multimodal training “Boot Camp” in the UK and its changes through two consecutive years achieved an increase of the level of confidence of the participants that lasted months after the project.
Conclusions: Simulators and courses or curricula based on a simulator‐based training could be a valuable learning tool for any surgeon and there is no doubt that they should be a part of an urologist's technical education.
Patient Safety in the Operating Room During Urologic Surgery: The OR Black Box Experience
A Rai, L Beland, T Aro, M Jarrett, LR Kavoussi
The Smith Institute for Urology
Introduction & Objective: A significant portion of complications in hospitalized patients occur following a surgical procedure with both recognized as well as under‐recognized events playing a role. As such, there is interest putting in place measures to identify, remediate and prevent these intra‐operative adverse events. To mitigate intraoperative adverse events, it is important to understand the context in which these errors occur. The purpose of this study is to characterize the IAEs and potential distractions that occur in minimally invasive urologic procedures.
Methods: We conducted a prospective cohort study in patients undergoing laparoscopic urologic surgery at an academic health center. The OR Black Box, a unique technology system which captures video and audio recordings of the operating room as well as the operative field, was used to collect data regarding procedure type, critical step, IAEs, and distractions.
Results: Of a total of 80 cases analyzed, the majority of these cases were partial nephrectomy (n = 36; 45%), radical nephrectomy (n = 20; 25%) and adrenalectomy (n = 4; 5%). Across all cases there were a total of 138 clinically significant IAEs, 10 of which (14%) were of the highest severity (5 on the SEVerity of intraoperative Events and Rectification Tool (SEVERE) matrix). Of these, 70 (51%) occurred during an a priori defined critical step of the operation. Distractions were common across all cases. The median rate of external communication per case was 16 events (IQR 11‐22); and per critical step was 4 (IQR 2.75‐8), while median room traffic per case was 58 entries/exits (IQR 42‐76); and per critical step was 17 (IQR 10‐65).
Conclusions: Our data demonstrate that IAEs occur frequently during all phases of the operation at hand. Future study will be required to examine the role of distractions and IAE as well as IAE and their relationship to post‐operative clinical outcomes.
Evaluation of Urology Trainee Preferences in Didactic Education: An International Choice‐based Conjoint Analysis
K Spradling, C Seufert, N Kern, MS Borofsky, M Sorensen, L Hampson, S Conti
Introduction & Objective: Didactic lectures are a commonly used educational tool during urology residency training. Although all residency programs are expected to provide didactic content for their residents, the format of these sessions vary by presenter and institution. Currently, it is not clear which didactic format provides the most educational benefit. Herein, we aimed to evaluate which attributes of didactic education are most preferred by contemporary urology trainees.
Methods: Urology trainees during the 2020‐21 academic year were invited to complete an online choice‐based conjoint analysis exercise assessing four attributes associated with didactic education: method of delivery, presentation style, presenter credentials, and curriculum design. The survey was distributed via social media platforms and the Urology Collaborative Online Video Didactics (COViD) website. A sensitivity analysis (Sawtooth Software, Inc. Utah, USA) was used to determine relative importance of each attribute and predict trainee preferences in didactic format (online/virtual vs. in‐person).
Results: Of the 431 trainees who received the survey, 73 (17%) completed the conjoint analysis exercise, including 60 participants from the United States and 11 from international training programs. Nearly all trainees (72/73) preferred at least 1 hour of dedicated didactic education per week, with 67% responding that 2‐ 3 hours of didactic time per week is ideal. Overall, the majority of respondents preferred online/virtual presentations (77%, 95% CI 70‐84%) compared to in‐person presentations. Respondents placed the most importance on presenter credentials, preferring national experts from visiting institutions to faculty members from their local institutions. Conjoint analysis revealed a preference trend toward an online didactic curriculum by increasing PGY year, with senior residents and fellows showing stronger preferences for online didactics compared to more junior trainees (Figure 1).
Conclusions: Contemporary urology trainees prefer didactic education that is available in an online/virtual format, standardized across training institutions, and organized and presented by national experts in the field. This data should inform national educational efforts to standardize didactic learning for urology trainees.
Authorship in Endourology: A Gender Reveal
G Jeng, L Beland, T Aro
Introduction & Objective: According to the American Urological Association (AUA) 2019 census, the percentage of women practicing urologists is 9.9% of the workforce in the USA, making urology one of the least gender‐diverse specialties recognized by the Accreditation Council for Graduate Medical Education.
The purpose of this study is to identify the proportion of urologic studies published in 5 major urologic journals by women in 2019 in the USA. We also aim to determine if any significant difference exists in the proportion of women publishing within endourology as compared to men.
Methods: A cross‐sectional study was designed to analyze trends in women authorship of urology publications in 2019 compared to AUA 2019 census data. All studies published by authors from USA institutions between January and April of 2019 in Journal of Endourology, BJU International, Journal of Urology, European Urology, and Prostate Cancer and Prostatic Diseases were evaluated. The gender of first and senior authors were collected. Studies were categorized as basic science, clinical medicine, economics/practice management, review/meta‐analysis, editorial, and case report/technique. Chi‐squared test was used for statistical analyses and p values <0.05 were considered statistically significant.
Results: 184 publications were included in this study. The proportion of women first authors was significantly higher than would be expected based on population proportions, X2 (1, N = 178) = 9.65, p = 0.002, but there was no significant difference in proportion of women first authors in the Journal of Endourology compared to population proportions, (X2 = 0.19, df = 1, p = 0.66). There was no significant difference in proportion of women senior authors compared to expected, X2 (1, N = 165) = 2.18, p = 0.14. Of the different study types, only the proportion of women with basic science publications was significantly higher than would be expected, X2 (1, N = 18) = 6.45, p = 0.011.
Conclusions: A recent study showed that amongst physicians, women were less likely than men to be promoted in academic medicine. Women in urology publish as first author at higher rates than expected, particularly in the basic sciences. However, there continues to exist a gender gap in academic leadership such that high productivity is not enough for the professional promotion of women in medicine. As one of the least gender‐diverse specialties, it is imperative that urologic institutions not only encourage productivity amongst women trainees and urologists but ultimately take actions to promote the advancement of women urologists within the ranks of academic leadership.
Analysis of Flexible Ureteroscopic Motion and Kinematic Efficiency ‐ A Simulation‐Based Pilot Study
G Gomez, L Stirling, D Wollin
Brigham and Women's Hospital Division of Urology
Introduction & Objective: The most common surgical procedure to treat stones is flexible ureteroscopy (fURS). Despite frequency of utilization, there is no undisputed method for evaluating fURS skill or success. Various surgical disciplines and subspecialties have examined surgeon kinematics to improve assessment and generate measures of success. Our pilot study utilizes kinematic evaluations for fURS to determine whether specific surgeon movements, techniques, and strategies correlate with measures of ureteroscopic efficiency.
Methods: A motion capture system and standard video camera were employed to characterize surgeon movement variables. A ureteroscopic simulation box was used by practicing urologists at various skill levels to perform a set of simple and complex ureteroscopic movement tasks. Body kinematics, time to task completion, and ureteroscope movements were analyzed. Two tasks were chosen for this initial pilot analysis. Task efficiency was defined as quicker time to task completion and smaller ureteroscope end effector travel distance. A performer efficiency score (PES) was calculated using the root sum square of these two measures.
Results: Urologist (n = 12) average age was 37; 50% were female, 50% were residents; and 33% participated in an Endourology fellowship. High efficiency performers (HEPs) tended to have a shorter length of clinical practice (mean, 6 vs 14 years) and higher ratio of performed‐to‐proctored cases (mean, 7.4 vs 5.6), although these measures were not statistically significant (p = 0.23, p = 0.49, respectively). For the simple task, no kinematic data assessed correlated with the associated PES; for the complex task, participant head and torso movement were correlated with PES (r = 0.60, p = 0.04 for head, r = 0.65, p = 0.02 for torso), with decreased body movement associated with higher efficiency.
Conclusions: This study suggests that movement economy measures are associated with efficient ureteroscopic manipulation for complex tasks. Decreased head and torso movement were associated with higher efficiency, suggesting that more body movement may lead to or stem from extraneous or improper movements of the ureteroscope. Additional study of these variables is warranted, including assessment in a clinical setting, as they may serve as a basis for improvement in endoscopic training and evaluation.
Experiences and Attitudes Toward Surgical Simulation Among Urology Residents: A Five‐Year Survey Assessment of Participants in a Multi‐Institutional, Multimodal Simulation Workshop
DP Simon, S Setia, KG Baldea, SJ Kielb, S Crivellaro, S Eggener, AK Chow, C Coogan
Rush University Medical Center
Introduction & Objective: Surgical simulation is becoming an increasingly important educational adjunct to overcome the challenges facing contemporary urology residents who must become proficient with a rapidly expanding array of surgical technologies and instrumentation. Over a 5‐year period, we evaluated the experiences and attitudes toward surgical simulation among urology residents participating in a multi‐institutional, multimodal simulation workshop.
Methods: Between 2016 and 2020, residents from six Chicago‐area urology residency programs participated in an annual surgical simulation workshop. During these workshops, participants completed a series of simulated endourological procedures, including ureteroscopy, percutaneous nephrolithotomy (PCNL), and transurethral vaporization of the prostate (PVP) while faculty with pertinent expertise provided instruction and verbal feedback. Participants were invited to complete an exit survey after the workshop evaluating their simulation experience and attitudes toward surgical simulation.
Results: Over a five‐year period, 120 out of 132 participants completed an exit survey (response rate = 90.9%), including 73 junior residents (60.8%) and 47 senior residents (39.2%). Among respondents, 71.7% (86/120) had prior simulation experience, and 93.3% (112/120) felt that the simulation workshop was a useful exercise. Overall, 52.5% (63/120) believed simulation should be required during residency, and 78.3% (94/120) agreed that simulation is more useful for senior residents (≥PGY‐4) than junior residents (≥PGY‐3).
Conclusions: The vast majority of urology residents hold favorable views of surgical simulation, and our survey responses indicate the utility of a multi‐institutional, multimodal simulation workshop model for simulated surgical education. Furthermore, many residents feel simulation should be required in residency, and the majority agree that these experiences are most useful in the later years of training.
Withdrawn
The Impact of Surgical Trainee Involvement in Laparoscopic Donor Nephrectomy on Perioperative Outcomes and Complications
J Kuo, B Desroches, M Degen, R Munver
Hackensack University Medical Center
Introduction & Objective: Laparoscopic donor nephrectomy (LDN) is extremely challenging with no room for error. The procedure is routinely performed by an experienced attending surgeon, while residents/fellows may serve as assistants. We assessed the impact of surgical involvement of fellows and residents in performing portions of the LDN procedure on donor/recipient outcomes.
Methods: An IRB‐approved study was performed in patients who underwent LDN since 2003 by a single primary surgeon. Patient demographics, perioperative data, length of stay, and 30‐day postoperative complications were analyzed. Surgeries were categorized based on surgeons: (1) attending only, (2) attending+fellow, (3) attending+fellow+resident, and (4) attending+resident.
Results: A total of 188 consecutive LDNs were assessed. (Table) The mean age, BMI, EBL, and LOS was similar for all groups. The variance of EBL was higher in group 3 (attending+fellow+resident) but the difference was not statistically significant. The mean OR time and WIT were higher (P < 0.05) in group 1 (attending surgeon only). Complications for the groups were 2 (8.3%) (group 1), 1 (3.3%) (group 2), 3 (2.4%) (group 3), and 0 (0%) (group 4). Five complications were minor (Clavien I‐II), and 1 complication was major (Clavien IIIb) in group 1 (attending surgeon only).
Conclusions: The attending surgeon only group had the longest OR time and WIT which was attributed to a higher degree of case complexity. Based on our experience, allowing a fellow or an experienced resident to perform portions of a laparoscopic donor nephrectomy procedure does not adversely affect perioperative outcomes or postoperative complication rates.
Evaluating the Acceptability of an Electronic Patient Decision‐Aid for the Surgical Management of Lower Urinary Tract Symptoms Secondary to Benign Prostatic Hyperplasia
D Bouhadana, D Nguyen, B Raizenne, J Schwarcz, H Gordon, B Chughtai, D Elterman, L Lavallée, P Martin, K McAlpine, R Paterson, H Razvi, K Zorn, N Bhojani
University of Montreal Hospital Center (CHUM)
Introduction & Objective: With the help of a steering committee that included patient advocates, and both methodological and clinical experts, an electronic patient decision aid (PtDA) that includes all benign prostatic hyperplasia (BPH) guideline‐approved surgical modalities was developed. The goal of this study is to assess the acceptability of the PtDA within former BPH surgery patients and urologists that treat BPH surgically.
Methods: The Ottawa Decision Support Framework was used to develop a PtDA that addresses monopolar transurethral resection of the prostate (TURP), bipolar TURP, GreenLight photovaporization, enucleation, Rezum, Urolift, Aquablation, open retropubic prostatectomy, and robotic retropubic prostatectomy. The PtDA was divided into 3 sections according to prostate volumes. 11 urologists that regularly treat BPH surgically and 15 former BPH surgery patients were recruited. Alpha‐testing was achieved through a survey developed from a validated acceptability scoring system.
Results: For all sections of the PtDA, the urologists agreed that the language used was easy to follow, that the amount of information provided was about right, that the length of the PtDA was appropriate, and that the outcomes reported were correct. All 11 urologist participants found that the description of the treatments within the moderate to large prostate section of the PtDA was well balanced. For both the small to moderate, and large prostate sections, 91% (10/11) of participants found treatment descriptions were well balanced. Overall, urologists agreed that they anticipate using this PtDA once complete and that they are satisfied with the overall quality of the PtDA. Alpha‐testing within the patient population is currently underway with finalized results expected by April. To date, 15/20 participants have been recruited. These participants included 11 from the small to moderate (< 80ml) prostate volume cohort, 1 from the moderate to large (80‐150ml) cohort, and 3 from the large prostate volume cohort ( >150ml). Preliminary results for the patient population showed that for all sections of the PtDA, the patients agreed that the language used was easy to follow, that the amount of information provided was about right, that the length of the PtDA was appropriate, and that the outcomes reported were clearly explained.
Conclusions: Our PtDA was found to be acceptable amongst clinicians. These results demonstrate that the majority of the participants were satisfied with the quality of this PtDA and plan to incorporate this tool in their practice.
Impact of automation on the Aquablation learning curve: An international multicenter prospective study
AA Nasrallah, E Rijo, V Misrai, M Labban, J Najdi, A El Hajj
Department of Surgery, Division of Urology. American University of Beirut Medical Center
Introduction & Objective: Aquablation is a novel technique utilizing robotic‐assisted high‐velocity saline jet technology for treatment of benign prostatic obstruction. It aims to standardize clinical outcomes regardless of surgeon expertise. Despite being semi‐automated, multiple factors are surgeon‐controlled. The authors aim to describe the impact of automation on Aquablation learning curve.
Methods: A prospective multicenter observational study was conducted by three endourologists, experienced in AEEP and TURP but not in Aquablation, in centers from France, Lebanon, and Spain. The learning curve was represented by Trifecta (TF) and Pentafecta (PF) achievements. TF was defined as: operative time (OT) <60 minutes, hemoglobin loss (HbL) ≤2 units, and no Clavien‐Dindo grade 2+ complications (CD2). PF was defined as: TF achievement, ≥50% IPSS reduction, and no ejaculatory dysfunction (EJD).
Results: A cohort of 176 patients was enrolled. Rolling average plots of TF and PF (Fig. 1) showed 50% TF success is seen after 5 cases, 70% is exceeded after 50 cases, and 50% PF success seen after 38 cases. Logistic regression (LR) analysis showed increased TF success after cases 40‐50 [OR = 3.3 (P = 0.064)] and PF success after cases 40‐50 [OR = 7.1 (P = 0.008)]. Analysis of variance and post‐hoc testing showed significant difference between case groups for OT (P = 0.042) and HbL (P = 0.011). LR showed significant reduction EJD incidence: cases 20‐30 [OR = 0.21 (P = 0.019)], 30‐40 [OR = 0.15 (P = 0.009)], 40‐50 [OR = 0.16 (P = 0.011)]. CD2 complication rate was not affected by experience, and neither was %IPSS change as 94% of patients showed ≥50% improvement after 3 months.
Conclusions: Robotic‐assistance and automation in Aquablation provided a quick learning curve which showed consistently low complication rates and high clinical improvement success independent of surgeon experience. Standardizing hemostasis methods, reducing OT through staff training, and improved veru‐protection zone planning in early cases can lead to more homogenous results and quicker learning.
Factors Informing Selection and Evaluation for Endourological Society Fellowships
K Gupta, JA Khusid, D Lundon, B Gallante, AS Sadiq, W Atallah, M Gupta
Icahn School of Medicine at Mount Sinai
Introduction & Objective: Endourology Society (ES) fellowships are highly sought after and competitive, yet there have been no studies evaluating the attributes or benchmarks used for fellow selection. The goal of this study was to survey program directors across North America to identify the most important factors in selecting fellowship candidates and evaluating fellows during their training.
Methods: A survey was constructed using REDCAP software and distributed via email to program directors of fellowships registered with the ES. Fellowships in the ES include Endourology‐Stone Disease (ESD) programs, robotic‐laparoscopic surgery programs (MIS), and combination programs. The survey used a Likert scale ranging from 1 (not important) to 5 (extremely important) to rank the criteria for selecting and evaluating fellows. The survey captured program demographics such as geographic region, program type, and program duration.
Results: Of the 52 ES program directors, 34 (65%) responded. The respondents represented 8 (23.5%) ESD programs, 7 (20.6%) MIS programs, and 19 (55.9%) combination programs; of which 15 (44.1%) were one‐year programs and 19 (55.9%) were two‐year programs. Overall, the top 5 factors for candidate selection were perceived fit of the applicant within the program, perceived level of applicant interest, initial interview, personal emails from applicants' advocates, and personal phone calls from applicants' advocates. Advocacy on behalf of the applicant appeared to be especially important for two‐year fellowships. Overall, the top 5 factors for the evaluation of fellows in training were patient interactions, professionalism, attitude/demeanor, operative skills, and interactions with ancillary staff. Research productivity was of greater importance for the evaluation of two‐year fellows.
Conclusions: Our findings suggest that applicants for ES fellowships should focus on the initial interview and recruiting supportive mentors to advocate for their applications, particularly for two‐year programs. Furthermore, though program directors value both clinical skills and research productivity in evaluating fellows, research productivity was of greater importance for two‐year programs. Further research into applicant perspectives on the fellowship application process is warranted.
Evaluation of uroLogical tEAching in bRitish medical school Nationally: the LEARN multicentre cross‐sectional study
A Ng, V Vinson, A Asif, C Lam, A Light, K Jayaraajan, WA Cambridge, MG Matthews, KD Clement, M Kulkarni, NR Bhatt, S Khadhouri, V Kasivisvanathan
Leicester Medical School, University of Leicester, Leicester
Introduction & Objective: The percentage of medical schools mandating urology rotations in the USA has decreased from 99% in 1956 to 17% in 2009, whereas 65% of medical school directors stated in 2008 that it was possible for their students to have graduated without a clinical rotation in urology. LEARN aims to evaluate the current status of UK undergraduate urology teaching.
Methods: LEARN is a UK‐wide multicentre cross‐sectional study of undergraduate urology teaching. Year 2‐5 medical students and postgraduate‐year 1 doctors (PGY1) from all medical schools in the UK were invited to complete a survey between the 3rd October 2020 and 20th December 2020. The objectives of this study are to evaluate the quantity and types of urology teaching of all UK medical schools against the British Association of Urological Surgeons' undergraduate syllabus and the mandated urological skills requirements set out by the UK General Medical Council. Students' and PGY1s' perceptions of urology as a career were also evaluated.
Results: 7,594 (91%) eligible responses out of the 8,346 responses from all 39 eligible medical schools were analysed. Amongst 1,253 PGY1s, 21% (259/1253) have graduated without any clinical attachment in urology. Andrology teaching is severely underrepresented. 13.1% (164/1253) have never performed a male genital examination on either a model or a patient. 44% (554/1253), 52% (657/1253) and 59% (745/1253) of PGY1s have never had any teaching on erectile dysfunction, male infertility or male urinary incontinence, respectively. In contrast, general urology such as urinary tract infections, acute kidney injury, and haematuria are well‐represented in the curriculum. Only 53% (658/1253) and 17% (212/1253) of PGY1s believed they had sufficient urology teaching in their medical course and have considered a career in urology, respectively.
Conclusions: LEARN is the largest evaluation of the undergraduate urology curriculum to date worldwide. While most urology topics were found to be well‐represented in the curriculum, LEARN has identified weaknesses in the curriculum, such as clinical exposure and andrology. The LEARN study will provide crucial evidence in reforming the urology curriculum to ensure competent and adequate urology knowledge in training doctors regardless of their future career choice.
Three‐dimensional printing models of horseshoe kidney and duplicated pelvicalyceal collecting system for flexible ureteroscopy training: a pilot study
UJ Pereira‐Sobrinho, LA Favorito, J Albero, ML Becalli, FJ Sampaio
State University of Rio de Janeiro
Introduction & Objective: Horseshoe kidney is the most common renal fusion anomaly, with prevalence of 0.25% in general the population. Ureteral anomalies of number are also frequent, particularly ureteral duplications, which have incidence of around 1/150 live births. The incidence of nephrolithiasis in horseshoe kidney patients is approximately 20%. The anatomical properties of anomalous kidneys present substantial obstacles to endourologic procedures, especially because of the position of the renal calyces. Flexible ureteroscopy is a common procedure nowadays, and most training programs use virtual reality simulators. In this study, we demonstrate a new option for endourological training, using three‐dimensional (3D) printing models of kidneys with congenital anomalies (horseshoe and duplicated pelvicalyceal collecting system).
Methods: The study was approved and performed according to the ethical standards of the hospital's institutional committee on experimentation with human beings (IRB: 1.171.286, CAAE: 70623417.7.0000.5259). Usable data of two patients with horseshoe kidneys and two patients with complete ureteral duplication were obtained from computed tomography (CT) scans as Digital Imaging and Communications in Medicine (DICOM) format from a public health unit. These DICOM images were processed with the Simplify3D® software and were printed using a Flashforge Dreamer® 2018 printer. The models were made of polylactic acid (PLA) and acrylonitrile butadiene styrene (ABS) with diameter of 1.75 millimeter. The navigation was obtained by the same observer with a digital flexible ureteroscope (3.3 x 670 mm, model DR030670, Endomaster®). The 3D printed kidney has low manufacturing cost (about US$ 100), and it is relatively quick to make (average of 22 hours).
Results: The digital flexible ureteroscope could be inserted into all casts and the entire collecting system (including the lower pole, as well as perpendicular minor calices) could be examined in horseshoe kidneys and ureteral duplications without difficulties.
Conclusions: Recently, the use of 3D silicone models of the collecting system (cavities) obtained from polyester resin endocasts was proposed for flexible ureteroscopy surgical training. Nevertheless it is very laborious and the molds obtained are not as perfect as the 3D printed kidney models. The use of 3D printed kidney models before endourological procedures for pre‐surgical training is feasible and can be done with low‐cost materials. The surgeon can train before proposing the appropriate surgical procedure to the patient using the 3D printed kidney and collecting system cavities.
The impact of surgery on the intimate and social relationships of prostate cancer patients: a qualitative meta‐synthesis
O Eymech, O Brunckhorst, K Ahmed, P Dasgupta, C James
King's college London
Introduction & Objective: Radical prostatectomy is associated with high curative outcomes. Despite the high survival rates, side‐effects associated with surgery such as sexual dysfunction and urinary incontinence have a significant impact on the patient's social wellbeing and interactions with others. This review aims to collate and analyse all available qualitative research addressing the impact of surgery on relationships with partner, friends, family and wider societal interactions.
Methods: This review was registered prospectively with PROSPERO (CRD42021227846) and conducted according to the PRISMA and ENTREQ reporting guidelines. Two authors independently searched Medline (via PubMed), CINAHL, PsycINFO and Embase (via OVID SP) from inception up to 29th of January 2021. Qualitative research addressing the impact of prostatectomy on the previously defined social wellbeing constructs were included. Risk of bias was assessed using the critical appraisal skills checklist for qualitative studies. A qualitative meta‐synthesis approach as described by Thomas and Harden was used to inductively generate codes, descriptive themes and overarching analytical themes to go beyond the context of the findings of primary studies.
Results: 22 full‐text articles were included describing the experiences of 382 radical prostatectomy patients. 87 codes, seven descriptive themes and two analytical themes were generated. The first analytical theme was ‘Pathway to Conversion’ which described how men's social behaviour changed throughout their post‐operative journey in order to adapt to a new normality. The descriptive themes under this analytical theme were 'Shaking the Foundation', 'Reminiscing over the Past' and 'Rediscovering Relationships'. ‘A Man on My Own’ is the second analytical theme which described how men felt alone and unsupported as they sought isolation throughout their treatment journey as a result of the stigma, shame and embarrassment associated with their changed body image. The descriptive themes generated under this analytical theme were 'The Social Stigma', 'Nobody Understands', 'Alleviating Burden' and 'Seeking Belonging'.
Conclusions: Radical prostatectomy has a significant impact on the social wellbeing of patients. This impact is important to be highlighted to patients in pre‐operative counselling. Post‐operatively, psychosocial interventions should aim to improve social relationships through targeting self‐esteem and body image. Further research should focus on underrepresented ethnic minorities, single men, the elderly and homosexual individuals.
Ureteroscopy (URS) video consensus: a simple and effective way to improve awareness of patients undergoing URS
F Esperto, F Prata, A Civitella, P Tuzzolo, L Romei, V Crimi, F Tedesco, N Deanesi, T Bach, Y Tanidir, R Scarpa, R Papalia
Dept. of Urology, Campus Biomedico University of Rome, Rome, Italy
Introduction & Objective: In the age of information technology, new platforms are consulted by patients (pts) to acquire their own consciousness about medical treatments. The European Association of Urology Patient Information (EAU PI) delivers high quality video‐content about surgical procedures with a language easy to understand for patients. Aim of our study was to assess the level of understanding and feasibility of video consensus administration in pts scheduled for ureterorenoscopy (URS)
Methods: The EAU PI video content about URS was translated in Italian and implemented with possible complication explanation at the end of it. From Aug 2020 to Jan 2021 all pts who underwent URS for stone disease at our institution were prospectively enrolled. A print‐based traditional consensus was administered and, after that, a video information about URS showing potential complications. Later, pts received a preformed Likert 10 scale questionnaire to evaluate: 1)comprehension; 2)contents; 3)satisfaction; 4)simplicity; 5)details; scoring from 1 to 10. Descriptive and variance analysis was performed through SPSS v25 with an alpha value of significance set at 0.05, comparing the different types of consensus
Results: 50 pts were included in our study and 50 questionnaires were evaluated. 44% (22) of pts were female and 56% (28) were male, 24% (12) were aged 29–39 years, 30% (15) 40–59 years, and 46% (23) were >59 years. Mean score ± standard deviation (SD) for different domains analysed was the following: mean comprehension score ± (SD) was 6.78 ± (0.679) in standard consensus group versus 8.38 ± (0.725) in the video consensus group, p* = 0.0001. Mean contents score ± (SD) was 6.52 ± (0.5) in standard consensus group versus 8.6 ± (0.728) in the video consensus group, p* = 0.0001. Mean satisfaction score ± (SD) was 6.38 ± (0.49) in standard consensus group versus 9 ± (0.7) in the video consensus group, p* = 0.0001. Mean simplicity score ± (SD) was 6.16 ± (0.37) in standard consensus group versus 8.28 ± (0.701) in the video consensus group, p* = 0.0001. Mean details score ± (SD) was 6.38 ± (0.49) in standard consensus group versus 8.72 ± (0.784) in the video consensus group, p* = 0.0001
*U Mann‐Whitney test for independent samples
Conclusions: All the domains analysed showed a higher statistically significant appreciation for video consent compared to traditional informed consent. Overall satisfaction, with a mean score of 9 out of 10, showed to our advice the way to chase for the future. Video consent represents a simple and comprehensive tool for pts and can improve their awareness and satisfaction
Robotic Retroperitoneal Lymph Node Dissection For Stage I Non‐Seminomatous Germ Cell Tumor
A Beksac, KN Meilika, AA Elbakry, KE Okhawere, O Ige, J Sfakianos, KK Badani
Introduction & Objective: In this video, we present a case of robotic retroperitoneal lymph node dissection (RPLND) for a stage I non‐seminomatous germ cell tumor. Our patient is a 27 year old male, who underwent left inguinal orchiectomy for a 1.9 cm testicular mass. Pathology revealed pT2, non‐ seminoma with lymphovascular invasion. Postoperative αFP and βHcG were within normal limits. Postoperative cross sectional imaging did not reveal any metastatic lesions. Patient was counseled regarding surveillance, chemotherapy, radiotherapy and retroperitoneal lymph node dissection and he elected to undergo robotic RPLND.
Methods: The patient was positioned in a supine position. DaVinci Xi system was used for surgery. Robotic 8 mm ports have been placed in a linear configuration below the umbilicus. A single 12 mm assistant trocar was used between the left arm and the camera port. From left to right instruments are as follows: Maryland bipolar forceps, camera, monopolar scissors, and prograsp forceps. As the initial step the small bowels are mobilized and the bowels were lifted up using the prograsp forceps. Dissection started from the iliac bifurcation towards the proximal. Duodenum was identified and carefully dissected to visualize the renal vein. Afterwards lymph nodes were dissected from the distal towards the proximal. Interaortocaval lymph nodes and paraaortic lymph nodes were dissected according to the standard template. During dissection titanium and vek clips have been used. Nerve sparing has been performed.
Results: Surgical time was 120 minutes. Patient was discharged at postoperative day 1 without complications. Pathology revealed 20 lymph nodes, all negative for malignancy.
Conclusions: This video demonstrates a stepwise technique to perform unilateral template robotic retroperitoneal lymph node dissection for testicular cancer.
Withdrawn
Mayhem in the Retroperitoneum: Eroded IVC Filters
AM Asghar, D Strauss, RA Lee, H Hirsch, E Choi, DD Eun
Introduction & Objective: Inferior Vena Cava (IVC) filters are a common preventative tool for pulmonary embolism in high‐risk patients. Erosion of a filter limb is a known entity, yet usually benign. In rare cases, endovascular filter extraction is indicated, especially if there is a risk of embolization, bowel involvement, or ureteral obstruction. We present a representative case of robotic extraction of an eroded IVC filter with concern for ureteral and bowel involvement from our small case series.
Methods: We report the case of a 43‐year‐old female with a history of brain vascular malformation, deep venous thrombus, and stroke. An OptEase (Cordis, Santa Clara, CA) IVC filter was placed 11 years prior to presentation. She presented with an incidental finding of IVC filter erosion on abdominal ultrasound and confirmed with computed tomography (CT). Although no hydronephrosis was seen, the ureteral course deviated significantly and appeared adherent to the filter. Vascular surgery team ruled out endovascular extraction but consulted urology for minimal invasive IVC filter removal based on our prior experience. Using a transperitoneal robotic approach with the patient in a modified flank position, IVC was dissected with minimal ureteral mobilization. Intravenous heparin was administered, IVC was clamped proximally we were able to successfully remove the eroded and embedded IVC filter piece by piece with minimal ureteral mobilization. The anterior fibrotic IVC wall was excised, requiring reconstruction using 8.0 x 1.6 cm ePTFE synthetic patch graft. The proximal clamp was removed first to flush the IVC of clot and/or air embolus before synching down the knot on the graft. Color flow doppler confirmed patent reconstructed IVC with excellent flow.
Results: Our console time was 245 minutes with 300mL blood loss. The IVC was clamped for 132 minutes. The patient was discharged post‐operative day 5 after a 2‐unit blood transfusion and optimized oral anticoagulation. Foley catheter and Blake drain were removed prior to discharge. She had no major (Clavien >2) 30 day post‐operative complications. Follow up CT scan at 12 months showed a patent IVC with no residual struts or ureteral involvement.
Conclusions: In this representative case, we demonstrate that robotic approach to extraction of an eroded IVC filter, especially when concern for ureteral involvement is safe, feasible, and effective. At our institution, multidisciplinary approach by using robotic assisted surgery to manage a variety of pathologies in the retroperitoneum has resulted in excellent outcomes.
Laparoscopic retroperitoneal lymphadenectomy in supine position: technical aspects
C Conde Redondo, V Pascual, M Bedate Nuñez, F Castroviejo Royo, F Natal Alvarez, A Zamora Horcajada, L Cuellar Martin, A Herranz Arriero
Introduction & Objective: Laparoscopic Lumboaortic Lymphadenectomy (LALA) is a technique common to Gynecology and Urology. In this video we present the supine approach.
The indications are:
UROLOGICAL: Salvage lymphadenectomy (LDNS), targeting metastases for patients with lymph node recurrence after primary treatment of prostate cancer (PCa) (included in the European guidelines as a treatment option for this patient population) Stage I non‐seminomatous germ cell testicular tumor. Stage II non‐seminomatous germ cell testicular tumor with negative tumor markers. Post chemotherapy residual mass with negative markers. Stage IIb testicular tumor with negative markers after an initial short course of chemotherapy, independent of the evolution of the lesions on imaging studies GYNECOLOGICAL: Endometrial cancer in patients with invasion of the lymphovascular space, deep myometrial invasion, cervical involvement, or high‐grade tumors
Methods: !We placed the patient in a forced Trendelemburg position, with antithromboembolism prophylaxis We begin surgery by identifying the right ureter and open the retroperitoneum longitudinally on the axis of the great vessels and fix it to the wall with points referenced from the outside. From the junction of the right ureter we ascend over the external iliac and the aorta. It is important to know in advance the existence of renal polar arteries to avoid injuring them Next we release the iliac vein and lift all the lymphatic tissue limited by the ureter externally, the psoas posteriorly and the renal vein superiorly. We perform lymphadenectomy releasing the cava, the interaortocave space and the anterior aspect of the aorta We started the liberation of the paraaortic space by identifying the left limits, ureter, psoas and lateral aspect of the aorta. We release the anterior aspect of the aorta until we identify the inferior mesenteric artery that we keep We liberate the left aortics lymphadenopathies above and below the mesenteric, having the ureter as a lateral limit We check the integrity of the mesenteric We ascend until we identify the gonadal vein that is sectioned, and we are careful not to injure the lumbar vein that usually comes out behind the left renal vein. We continue the dissection cranially until the renal vein We finish the dissection checking the integrity of the structures and the limits. Finally we put the specimen in the bag.
Results: Surgical time 150 minutes, bleeding 100 ml, number of nodes obtained 20.
Conclusions: The supine decubitus approach allows easy access to the retroperitoneum, avoiding decolation, providing a very intuitive laparoscopic field. It is an affordable technique in experienced hands.
New technologies in robot‐assisted kidney transplantation: improving surgical performances, expanding the indication
A Piana, A Territo, A Gallioli, M Fontana, P Diana, JM Gaya, O Rodriguez Faba, J Huguet, P Gavrilov, A Mercade', J Subiela, L Guirado, C Facundo, A Bellin, D Amparore, J Palou, F Porpiglia, A Breda
Introduction & Objective: Robot‐assisted kidney transplantation (RAKT) has been shown promising results in grafts coming from living donation. However, this technique has two main limitations. First, grafts coming from cadaveric donors, usually reserved to patients with advanced systemic disease who often present iliac artery plaques, are excluded from RAKT because of the lack of intraoperative haptic feedback. For this reason, we introduced 3D imaging reconstruction in RAKT through the augmented reality (AR) in order to intraoperatively guide the surgeon, showing where to put the clamps and perform arteriotomy in the recipient iliac artery. Second, the regional hypothermia during rewarming time is guaranteed by intermittent ice slush insertion in the abdominal cavity, which may be suboptimal and increase the risk of ileus. To overcome this limit, we developed and tested a cold ischemia device (CID) with the aim to maintain a low and constant graft temperature while avoiding ice slush introduction.
Methods: These two projects were conducted according to IDEAL model for surgical innovation. In the first project, iliac artery anatomy together with plaques was represented in a 3D printed model. Firstly, this model was used in open kidney transplantation (OKT) setting in order to test the accuracy of the 3D reconstruction, comparing it with intraoperative tactile feedback. Subsequently, we employed this technology in the AR setting, in two cases without plaques. Finally, we tested AR in a patient with plaques. In the second project, the cooling device was developed and tested in an ex‐vivo setting to assess its cooling performances. In phase 2a, the device was used in an in‐vivo porcine model to evaluate the feasibility to perform both a complete OKT and RAKT. In phase 2b, CID was employed in 4 patients undergoing OKT or RAKT from living donors. Graft temperature was monitored using a thermal probe.
Results: The 3D‐AR enabled to clamp the artery in the correct position and to find the right place to perform arteriotomy. Phase 2 demonstrated that both OKT and RAKT can be performed with the support of CID in a clinical setting, without any modification in our standard technique or perceived lengthening of the operative time. Graft temperature never exceeded 20°C. No complications related to the use of both these devices were recorded.
Conclusions: These new tools were designed to overcome RAKT's main limitations, optimizing the graft cooling system and including patients with atheromatic vascular disease, paving the way to expand the indications of RAKT.
Robotic Approach to Adrenal Mass with IVC Invasion: Managing a Difficult Case and Troubleshooting Failure of Equipment
M Billah, F Sheckley, S Ahsanuddin, J Cadwell, R Sawhney, R Harrison, M Ahmed
Introduction & Objective: Robotic‐Assisted Laparoscopic Surgery is now the mainstay approach to many urologic cases, including radical adrenalectomy. Robotic‐assisted surgery provides numerous benefits but can also pose unique challenges. This video aims to demonstrate managing a difficult robotic adrenalectomy case and troubleshooting failure of equipment.
Methods: The patient is a 48‐year‐old female presenting with abdominal pain and found to have an incidental finding of 6.5 cm right adrenal mass with MRI confirmation with very close proximity to the IVC. We evaluated the injury that happened intraoperatively, assessed how we were able to troubleshoot the issue without converting, and analyzed the factors used during dealing with this challenging case.
Results: The video outlines the process in which we were able to manage an intraoperative issue in which the vessel loop malfunctioned and failed to clamp the inferior vena cava after resection of the adrenal tumor from the IVC. The major bleeding vessel was controlled, and homeostasis regained without conversion. Full resection of the tumor continued with IVC repair taking robotically. The patient recovered well and was discharged home on postop day 4. The final pathology demonstrated leiomyosarcoma.
Conclusions: An experienced robotic surgeon with a deep understanding of the technology can manage even the most challenging intraoperative complications without the need to open. Robotic technology made it possible to control severe bleeding after the vessel loop malfunctioned and allowed IVC repair to be completed robotically.
Intracorporeal and Extracorporeal Robot‐Assisted Kidney Auto‐Transplantation: Experience of the ERUS RAKT Working Group
A Breda, P Diana, I Giron‐Nanne, A Territo, A Gallioli, A Piana, JM Gaya, L Desender, B Van Parys, J Palou, N Doumerc, K Decaestecker
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
Introduction & Objective: Kidney auto‐transplantation is a useful technique to be reserved for cases where kidney function is compromised by a complex anatomical configuration, such as long ureteric strictures and renal vascular anomalies not suitable for in situ reconstruction. Robotic‐assisted kidney auto‐transplantation (RAKAT) presents a novel, minimally invasive and highly accurate approach.
Methods: We retrospectively analyzed patients undergoing standard (eRAKAT) and totally intracorporeal RAKAT (iRAKAT) in a total of 3 institutions. eRAKAT consisted in a bench surgery for graft preparation after the robotic nephrectomy and was followed by graft transplantation. iRAKAT consisted in a nephrectomy phase followed by intracorporeal reperfusion and transplantation.
Results: Between 01/2017 and 02/2021, 29 patients underwent RAKAT. 15 and 14 were eRAKAT and iRAKAT, respectively. Median age was 42 (39‐50.5) and 37.5 (25.8‐55.4) for the eRAKAT and iRAKAT, respectively. In the eRAKAT and iRAKAT groups, 10, 4 and 1 patients and 10, 4, and 0 patients presented with 1, 2 and 3 arteries, respectively and 13 and 2 patients and 14 and 0 patients presented with 1 and 2 veins, respectively. Pre‐op median serum creatinine and GFR were for the eRAKAT group 0.79 mg/dL (0.71‐0.86) and 90 (78.4‐109.1) and for the iRAKAT group 0.83 (0.76‐1.05) and 84 (67‐99), respectively. None required conversion to open surgery. For the standard group, median operative time was 360 min (339‐397). eRAKAT median warm ischemia, cold ischemia and rewarming ischemia times were 3 (2‐4), 156 (131‐194), 44 (43‐49.5) min respectively. For the iRAKAT group, median operative time was 307 min (292.5‐467.7). Median warm ischemia, cold ischemia and rewarming ischemia times were 3 (2.8‐3), 27.5 (20‐55.1), 46.5 (24.2‐58.2) min respectively. 3 patients developed classified as Clavien‐Dindo >2 in the eRAKAT group and 1 patient for the iRAKAT, none led to graft loss. At 90 days follow‐up, serum creatinine and GFR were 0.78 (0.71‐0.82) and 85.5 (81.7‐109.4), and 0.91 (0.8‐1.1) and 81 (69‐87.5) for the eRAKAT and iRAKAT group respectively.
Conclusions: eRAKAT and iRAKAT represents a promising minimally‐invasive technique in selected cases with acceptable ischemia time and operative outcomes. The eRAKAT technique leads to the advantages of a better graft vascular management and reconstruction. The iRAKAT technique despite the higher technical difficulty, leads to shorter cold ischemia times. Comparative studies are needed to characterize and define the indications for the two approaches.
Introduction & Objective: Here we present a video showcasing robotic assisted laparoscopic retroperitoneal lymph node dissection for metastatic mixed germ cell testicular carcinoma. We propose this minimally invasive method as an emerging technique to reduce morbidity associated with open retroperitoneal lymph node dissection.
Methods: A 51‐year‐old male presented to our department with two months of right hemiscrotal swelling, subjective shaking and chills, a 15‐pound weight loss over six weeks, and intermittent throbbing right testicular pain. CT abdomen/pelvis revealed a right testicular mass measuring 7.5 x 5.0 x 4.0 cm and a mildly prominent retroperitoneal lymph node measuring 0.08 cm. Patient underwent right sided orchiectomy and presented for robotic assisted retroperitoneal lymph node dissection approximately five weeks later.
Results: Total operative time was 170:47 min. Patient was discharged home on post‐operative day two. At follow up appointment two weeks after procedure, patient had experienced no complications, had returned to work, and was referred to medical oncology for further recommendations.
Conclusions: Robotic assisted laparoscopic retroperitoneal lymph node dissection was found to be a safe and effective treatment option for metastatic mixed germ cell testicular carcinoma and may be considered for appropriate patients to minimize the morbidity traditionally associated with open retroperitoneal lymph node dissection.
Robotic Partial Adrenalectomy in a Pediatric Patient
AA Elbakry, D Zekan, M Ost, O AL‐Omar
Introduction & Objective: This is a demonstration of technique for robotic approach for partial adrenalectomy in a pediatric patient.
Methods: A 7‐year‐old female patient who presented with an incidental finding of right adrenal mass measuring 2.5 cm on US imaging. she had no history of hypertension and examination revealed normal BP. Laboratory workup was done and revealed normal levels of serum aldosterone, metanephrines and plasma renin activity. The mass was stable in size after 10 months follow up, however patient's family opted for surgical resection. patient was placed in flank position. We used 4 8 mm robotic ports and a 5 mm assistant port. We started by reflection of the colon and dissection the undersurface of the liver from the IVC and upper surface of the adrenal mass. The posterior peritoneum was incised to expose the plane between the IVC and the adrenal mass. adrenal mass was carefully dissected from the kidney, posterior abdominal wall and the IVC. The right adrenal vein was identified, controlled and divided. The mass was excised with preservation of the normal part of the adrenal gland.
Results: Total operative time was 2 hours and 50 minutes. Estimated blood loss was less than 5 milliliters. The patient was discharged home in less than 24 hours. Pathological examination revealed ganglioneuroma.
Conclusions: Robotic approach for adrenalectomy in pediatric patients is a safe and feasible technique.
Step‐wise Surgery Guidance for Laparoscopic Left Adrenalectomy
H Yang, S Hung, L Chang, K Chiu
Introduction & Objective: Laparoscopic adrenalectomy was first introduced in 1992 by Gagner et al. and has readily become the standard surgical procedure for most adrenal diseases. The benefits of this procedure include a shorter hospital stay, faster recovery, decreased medical costs, and improved patient satisfaction. Performing laparoscopic surgery is technically demanding and the surgeon must be familiar with both the critical steps and regional anatomies of the operation to ensure an excellent outcome and patient safety. In this video, we demonstrate the surgical anatomies, a step‐wise tutorial, pitfalls and trouble‐shooting for laparoscopic left adrenalectomy through the case of a patient.
Methods: A 28‐year‐old male was diagnosed a left supra‐renal tumor during a Focused Assessment with Sonography in Trauma (FAST) during a trauma evaluation. A pre‐operative Computed Tomography (CT) scan, laboratory data, surgical video clips as well as pathology, along with searches in the available literature are included in the video.
Results: During adrenal surgery, venous variation is common in cases of a large tumor or pheochromocytoma. Bleeding is the most common cause of conversion from laparoscopy to open surgery, whether the bleeder is venous or arterial. Direct but gentle compression of the bleeder allows the surgeon to inspect the bleeder carefully in order to determine further management.
Conclusions: Through this video, we demonstrate the critical steps and landmarks encountered during a laparoscopic left adrenalectomy, along with the common pitfalls and trouble‐shooting encountered.
Utilization of Indocyanine Green for Performance of Robotic Nephroureterectomy in Patient with Prior Ileal Conduit
A Denisenko, M Ferretti, J Baber, N Patel
Introduction & Objective: Upper Tract Urothelial Carcinoma may occur in approximately 5% of patients after radical cystectomy for bladder cancer (Meissner et. al.,2007). Minimally invasive surgery has been described for nephroureterectomy after prior cystectomy (Romero et. al. 2006) Alterred anatomy and prior adhesions make this a challenging case. Indocyanine Green is a diagnostic agent that can be used with Da Vinci Robot Firefly technology to outline structures. Here we demonstrate both intravascular and intra‐conduit utilization of ICG to facilitate nephroureterectomy after ileal conduit.
Methods: We present a 72 year old male with a prior history of radical cystectomy and ileal conduit being managed by outside urologist. Patient developed right hydronephrosis on outside imaging. He was thought to have a ureterointestinal anastamotic stricture and a nephroureteral stent was placed. He was referred to our institution for ureteral reimplant. Further workup revealed an upper tract urothelial cancer. A robotic right nephroureterectomy was elected.
Results: Patient tolerated procedure well. Operative time was 3 hours. Length of stay was 10 days due to post‐operative ileus. Estimated blood loss was 50mL. Pathology found to be 5.5cm high grade T1 lesion with negative margins. No readmissions or 90 day complications seen.
Conclusions: Robot assisted laparoscopic radical nephroureterectomy may be safely performed in patients with prior ileal conduit. Indocyanine green may help facilitate the robotic approach in these complex cases. Long term data and more cases needed to determine if robotic approach offers any advantages over standard.
The Utility of Indocyanine Green Fluorescence in Robotic‐Assisted Adrenalectomy for Functional and Non‐functional Tumors ‐ An Initial Experience in Taiwan
P Liu, Y Lin, Y Ou, C Hsu, M Tung
Introduction & Objective: Robotic‐assisted technique had been widely used for adrenalectomy due to requirement of angled instruments for dissection and limited operative field. Indocyanine green (ICG) dye had been used for minimally invasive surgery in recent years. We aimed to present Taiwan's first experience of application of ICG fluorescence in robotic‐assisted adrenalectomy for functional and non‐functional tumors. We evaluated the ICG presentation in different functional adrenal tumors.
Methods: There were 8 cases of robotic‐assisted adrenalectomy with applications of ICG fluorescence reviewed retrospectively. Perioperative data were collected. The operative techniques of robotic‐assisted adrenalectomy with successful ICG fluorescence performed from December 2017 to December 2019 were demonstrated via video.
Results: There were a total 8 patients receiving robotic‐assisted adrenalectomy under ICG fluorescence guidance. 3 cases presented with hypertension and hypokalemia were diagnosed with Conn's syndrome. 5 cases were non‐functional tumors. The mean operation time was 94.3 minutes (range, 70‐170 minutes). The mean hospital stay was 4.12 days (range, 3‐6 days). The pathological finding of 7 cases was: Adrenocortical adenoma. 1 case was adrenal lymphangioma. No perioperative complications were noted.
Conclusions: ICG fluorescence offers the advantages of real‐time intraoperative imaging, the adrenal tumor location and margin can be clearly identified during operation and further reduce operative time. The applications of ICG fluorescence in robotic‐assisted adrenalectomy are safe and feasible in all functional and non‐functional tumors.
Robotic Reconstruction of Uretero‐Ileal Anastamotic Stricture with VY Plasty
H Flynn, A Navaratnam, J Nielsen, S Davies
Introduction & Objective: N/A
Methods: N/A
Results: N/A
Conclusions: N/A
Robotic Partial Adrenalectomy for Syndromic Pheochromocytoma
A Woloshuk, J Farrow, CD Bahler, CP Sundaram
Introduction & Objective: Pheochromocytomas are rare catecholamine producing neoplasms of the adrenal medulla. Most cases are sporadic, but up to 40% of patients have the disease as part of a familial disorder – von Hippel‐Lindau syndrome, multiple endocrine neoplasia type 2 (MEN2), and neurofibromatosis type 1, are more likely to occur in younger patients and be bilateral. Presentation of pheochromocytomas include signs of catecholamine excess, but can also be found on screening of at‐risk individuals with serum metanephrines or cross‐sectional imaging.
The resection of pheochromocytomas is a high‐risk surgical procedure due to the potential for catecholamine surge, hemodynamic instability, and tumor seeding. In patients with syndromic pheochromocytoma, recent studies suggest that partial adrenalectomy does not decrease survival compared to bilateral adrenalectomy while avoiding the morbidity associated with lifelong glucocorticoid replacement.
Methods: A 23‐year‐old male with medullary thyroid cancer status post total thyroidectomy and known MEN2a was found to have elevated metanephrines on biochemical screening. Abdominal CT demonstrated 1.6 cm right and 1.0 cm left adrenal nodules – PET was negative for metastasis. A right partial adrenalectomy was performed robotically following appropriate alpha blockade (doxazosin). Intraoperative ultrasound was used to delineate tumor margins.
Results: Enucleation of the tumor was performed with a total operative time of 131 minutes and estimated blood loss of 20 mL. Vital signs remained stable throughout the procedure. Pathology revealed pheochromocytoma with negative margins. The patient did well postoperatively and was discharged on post‐operative day 1. Follow up appointment demonstrated stable blood pressure. Plasma metanephrines were within normal limits. Genetic testing revealed C634R mutation of the RET proto‐oncogene.
Conclusions: In patients with familial pheochromocytoma, partial adrenalectomy can be used to postpone or avoid glucocorticoid deficiency without impacting survival. In this case, we present a 23‐year‐old male with MEN2a who underwent robotic assisted partial adrenalectomy. This technique represents an attractive alternative for patients who might otherwise require bilateral adrenalectomy and lifelong glucocorticoid supplementation.
Video Session 10: Robotic Surgery: Bladder & Miscellaneous
V10: Robotic Surgery: Bladder & Miscellaneous
I Seo, IY Kim
Robot assisted laparoscopic vesico‐vaginal fistula repair with omental interposition : A prospective evaluation of Our experience
A Kumar, S Kumar, S Yadav, Y Prashanth, K Saurav
Introduction & Objective: The vesicovaginal fistula(VVF) causes lot of morbidity to the women and is a very debilitating condition . The Robot assisted Laparoscopic VVF repair is technically challenging, especially in trigonal fistula. We prospectively evaluated our experience of Robot assisted laparoscopic VVF repair with omental interpositionin trigonal and supratrigonal VVF.
Methods: In this prospective study, all consecutive patients with trigonal and supratrigonal VVF , from Oct 2019 to Feb 2020, requiring Robot assisted laparoscopic VVF repair with omental interposition(using da‐Vinci Xi Robotic system )were included. The patients with post radiotherapy and VVF with malignancy were excluded from the study. The various clinical data were recorded and analyzed. We are presenting video of one such case.
Results: A total of 9 patients were included in the study. The mean age was 37.1 years . The fistula was post open abdominal hysterectomy in 5(55.5%) and post lower segment caesarean section(LSCS) in 4(44.4%) patients. The mean fistula size was 2.5 cm. The fistula location was trigonal in 3(33.3%) and supratrigonal in 6(66.6%) patients. The mean operating time and mean estimated blood loss were 109.3 min and 67.3 ml respectively. Three(33.3%) patients required simultaneous modified Lich Gregoir ureteric reimplantation There was no open conversion and intraoperative complications. The mean catheterization time , mean hospital stay and mean convalescence were 10.9 days ,4.1 days and 1.9 weeks respectively. At mean follow up of 6 weeks , postoperative complications were mainly clavien 1 ‐2 in only 1(11.1%) patients . None of the patients showed recurrence of VVF or voiding symptoms .
Conclusions: Robot assisted laparoscopic VVF repair with omental interpositionin trigonal and supratrigonal VVF is feasible, safe with excellent efficacy, even in previously failed VVF repair. However, it is a technically challenging procedure and should be done by surgeons of significant expertise.
Perioperative outcomes of Robot assisted Lap Radical Prostatectomy in Locally Advanced High Risk Prostate Cancer: A prospective evaluation
A Kumar, S Kumar, S Yadav, Y Prashanth, K Saurav
Introduction & Objective: The management of locally advanced high risk prostate cancer is challenging. The various guidelines have suggested radical prostatectomy , as one of the options , in a multimodality approach. We prospectively evaluated the feasibility, safety and perioperative outcomes of Robot assisted laparoscopic radical prostatectomy(RARP), as a multimodality approach, in locally advanced high risk prostate cancer.
Methods: All consecutive patients undergoing RARP (using da‐Vinci Xi Robotic system)in locally advanced high risk prostate cancer, as a multimodality approach, by a single surgeon , between Oct 2019 and Feb 2020, at our institution were included. The various clinical data were recorded and analyzed. We are presenting video of one such case.
Results: A total of 21 patients with locally advanced and high risk prostate cancer were included. The mean age was 64.1 years with mean serum PSA of 13.9. The mean operating time and mean estimated blood loss were 147.8 min and 137.1 ml respectively. There was no open conversion. The intraoperative complications were seen in only 1(4.7% ) patients , as Clavien 1‐2. The mean catheterization time was 10.1 days. The postoperative complications were seen as Clavien 1‐2 in 2(9.4%) patients. In histopathology,19.1% and 80.9% patients had pT2 and
Conclusions: Robot assisted Laparoscopic radical prostatectomy in patients with locally advanced high‐risk prostate cancer can be offered as first intervention, followed by adjuvant treatment, as multimodality approach. It is feasible, safe with acceptable perioperative morbidity. However, it is a technically challenging procedure and should be done by surgeons of significant surgical expertise.
Robotic cystectomy and neobladder / ileal loop operation due to invasive bladder tumor
OB Argun, MB Tuna, T Doganca, I Tufek, C Obek, AR Kural
Introduction & Objective: To share our surgical technique and early results in the patient, where we performed robotic cystectomy + neobladder / ileal loop operation due to invasive bladder tumor.
Methods: Patients were positioned in supine and 30 degrees steep Trendelenburg position. Da‐Vinci Si system was used in all cases. Following cystectomy and lymphadenectomy, the left ureter was passed under the mesosigmoid to the right side. We firstly locate the most mobile loop of the ileum that reaches the urethra without tension. Following the determination of the ileocecal region, the distal ileum segment is isolated with a laparoscopic stapler for utilizing a tension free urethroileal anastomosis. First 20 F size hole is created at the antimesenteric part of the ileum. The anastomosis is performed with a 3/0 barbed suture material using Van Velthoven technique. Urethral bites need to be shallow as it can compromise postoperative urinary continence. Afterwards, approximately 40 cm ileum segment was separated with the help of stapler. Before performing the anastomosis of small bowel, blood supply of the ileal segment is controlled with ICG and using the firefly mode of the Da‐Vinci system. For small bowel anastomosis the intestinal lumps are lined up and intracorporeal side to side anastomosis is formed with a 2 60 mm laparoscopic stapler. Distal 10 cm and Proximal 30 cm of ileum is detubulurised using monopolar cautery. Approximately 30 cm part was detubulirised. The posterior plate was then reconstructed using a 3/0 absorbable suture in a running fashion. The neobladder was then folded asymmetrically. then the anterior wall were closed using V‐loc. Meanwhile, a 22 F 3‐way Foley catheter was placed into the neobladder from the urethra. The isolated loop was consequently opened according to Studer, leaving a 10 cm afferent segment. The ureters were conjoined using the Wallace technique with a 4/0 absorbable suture. Single‐J stents were placed over guide wire and the ends were advanced through the wall of the reservoir. Both ureters were then anastomosed to the afferent limb using a 3/0 barbed absorbable suture. Following the completion of the uretreroileal anastomosis the anterior Wall of the neobladder is closed with a running suture technique.
Results: A total of 8 patients underwent robotic ileal diversion (5 intracorporeal neobladder, 3 ileal conduit). No patient required a reversal. There was no bleeding that required blood transfusion. Postoperative prolonged ileus was observed in two patients, urosepsis in 1 patient, and left ureter incomplete stenosis in 2 patients.
Conclusions: Using Da‐Vinci Si® system, robotic cystectomy and ileal diversion can be performed with minimal morbidity and low blood loss.
Results of our series on oligometastatic prostate cancer. A case of robotic lymph node recurrence rescue surgery
A PÉREZ‐LANZAC, J ACEBAL LÚCIA, A Allona Almagro
Introduction & Objective: Oligometastatic prostate cancer (PC) is considered to be at 5 or less metastatic sites in bone based on bone scan (Tc‐99) and occasionally visceral findings. In recent years, a multidisciplinary approach has open up new alternatives of treatment to these patients1.
Methods: We present the surgery of a patient with lymph node recurrence after a Da Vinci robot‐assisted laparoscopic radical prostatectomy (PRLR). Eight patients underwent PRLR for their primary and presented PC recurrence from October 2003 to December 2019. All of them were diagnosed with oligometastasis by a PET‐CT Ga68 PSMA.
Results: We selected a 70‐years‐old patient who presented a biochemical recurrence 7 months after radical prostate surgery. An uptake in the left ilio‐obturator chain on the PET‐CT Ga68 PSMA was detected. A superextended ilio‐obturator bilateral limphadenectomy was completed within 140 minutes, blood loss was 300 ml and hospital stay was 3 days. There were no intraoperative or postoperative complications. Of the total series, 3 (37.5%) patients were under observation, 2 (25%) were treated with radiotherapy and 3 (37.5%) with salvage surgery. Five (62.5%) patients completed a second rescue treatment. Of them, 3 (60%) received a surgical approach and 2 (40%) radiotherapy. There were no deaths due to cancer. At the end of the follow‐up all patients were alive and the median overall survival (OS) was 62.56 (6.47 – 196.6) months.
Conclusions: Salvage surgery for oligometastatic PC was feasible and without complications. A multidisciplinary approach was associated with prolonged OS and allowed patients to delay systemic treatments.
1. Mosillo C, Iacovelli R, Ciccarese C, Fantinel E, Bimbatti D, Brunelli M, Bisogno I, Kinspergher S, Buttigliero C, Tucci M, Caffo O, Tortora G. De novo metastatic castration sensitive prostate cancer: State of art and future perspectives. Cancer Treat Rev 2018;70:67‐74.
Robot‐assisted Laparoscopic Radical Cystectomy in a Rural Hospital Setting
M Ferretti, J Baber, N Patel, J Dungca, E Spencer, B Protyniak
Introduction & Objective: Some authors have argued for procedures such as radical cystectomy to only be performed in “Centers of Excellence”. However, local performance of these procedures may also have advantages for overall patient care. Patients in rural settings do not always have resources or desire to travel to larger cities where centers of excellence are often located. Local urologists are often the ones providing follow up care when patients do travel for procedures and performing the procedure locally permits more continuity in the patient's care. Finally, wide dissemination of procedures and skill sets prevents against the medical system becoming too “fragile” in the event of unforeseen circumstances where centers of excellence are not as accessible. Using a team approach, we have implemented a robot assisted laparoscopic radical cystectomy program at our institution.
Methods: Robotic team was created at our institution for performance of the new procedure. Robot assisted radical cystectomy was performed in 10 consecutive patients.
Results: Robot‐assisted Laparoscopic Radical Cystectomy and Intracorporeal Urinary Diversion was performed in 10 patients with success. Patients age ranged from 51‐85 years old. Our 90 day readmission rate was 30% (3/10). Our 90 day complication rate 30% (3/10) : colitis(2/10) and blood transfusion(1/10). No Clavien Grade 3 or higher complications were observed. Our average Lymph node yield was 14 (range: 7‐28). Our average Length of Stay: 6 days (Range 4‐10). Our average Estimated Blood Loos was 270mL (range: 100‐500mL). Finally, our 90 day mortality rate is 0% (0/10).
Conclusions: Our results suggest that a robotic assisted laparoscopic radical cystectomy program may be safely implemented in rural hospital settings using a team‐based approach. Longer term follow up and further study needed to determine if results are equivocal to major centers
Robotic Simple Cystectomy for Benign Disease
M Ferretti, J Dungca, J Baber, B Protyniak, N Patel
Introduction & Objective: Robotic simple cystectomy for benign disease is performed as part of urinary diversion. This procedure may be indicated in patients with radiation cystitis, interstitial cystitis, neurogenic bladder or total incontinence refractory to more conservative measures. A modified simple cystectomy technique has been described by several groups including Neulander, et. al and Rowley et. al. We have adopted a similar modified version at our institution. Proposed benefits include shorter operative time, less blood loss and easier learning curve.
Methods: We perform a robot assisted simple cystectomy with intracorporeal urinary diversion. The bladder is dissected off the abdominal wall and transected in the midline. It is then removed in piecemeal fashion and removed with endocatch bag.
Results: Our patient tolerated procedure well with minimal blood loss and an operative time of 3 hours. She was sent home on POD7 with no complications at 90 days follow up.
Conclusions: Modified version of the robot simple cystectomy may be safely adopted. Further study will be needed to determine if this technique results in proposed advantages of shorter operative time, less blood loss and easier adoption.
Robotic Radical Cystectomy with Intracorporeal Urinary Diversion in a Male using the daVinci Single Port System
M Billah, R Sawhney, M Zhang, S Ahsanuddin, M Ahmed
Introduction & Objective: Utilization of the new daVinci single‐port (SP) system has slowly begun to increase within the field of urology. From radical prostatectomies, partial nephrectomies, and lymph node dissections to now radical cystectomies with intracorporeal urinary diversion, urologists are adapting the SP system to more complex procedures. This video illustrates the technique for radical cystectomy with intracorporeal urinary diversion in male patients and describes perioperative outcomes. The technique in females has been demonstrated in a separate abstract. A learning curve was involved in switching over to the SP system with an overall smooth transition.
Methods: This cohort study obtained IRB approval and utilized a prospective robotic cystectomy database. We review our single institution experience with robotic radical cystectomy with intracorporeal urinary diversion done in four patients. The included video reviews pertinent steps to performing a robotic radical cystectomy with intracorporeal urinary diversity using the SP system in a male patient.
Results: Radical cystectomies with intracorporeal urinary diversion were performed on four patients in a span of two months (perioperative data in Table 1). All cases were completed successfully without conversion to open. The average operative time was 247 minutes with a mean estimated blood loss of 225 ccs. The average length of stay was 5.5 days with no post‐operative complications within 30 days of each procedure.
Conclusions: Robotic assisted radical cystectomy with intracorporeal urinary diversion is safe and feasible using the new SP system. The SP system offers improved cosmesis over standard approaches, but limited data exists regarding perioperative outcomes such as time and pain reduction. Further study is necessary to determine if the approach will lead to reduced morbidity or improved perioperative outcomes.
Use of Indocyanine Green and Near‐Infrared Imaging Assists with Intraoperative Localization of the Ureter and Margins during Robotic Bladder Diverticulectomy
B Desroches, N Gopal, R Munver
Introduction & Objective: Intraoperative retrograde ureteral instillation of indocyanine green (ICG) in combination with near‐infrared fluorescence (NIRF) imaging (FireFlyÔ, Intuitive Surgical, Inc.) is increasingly being used during robotic urological surgery. We demonstrate the benefit of ICG use for ureteral identification and delineation of the margins of a large bladder diverticulum that closely abutted the left ureter during robotic bladder diverticulectomy.
Methods: A 60‐year‐old male was referred for management of a symptomatic large bladder diverticulum that resulted in urinary retention. On cross sectional imaging, the diverticulum was to the left, lateral, and posterior, in relation to the bladder. The diverticulum was in close proximity to the distal left ureter and the diverticulum neck was close to the left ureteral orifice. Cystoscopy with retrograde instillation of ICG into the left ureter and left indwelling ureteral stent placement were performed prior to initiation of the robotic portion of the surgical procedure. A four‐arm robotic transperitoneal approach was used with four 8 mm robotic trocars and one 12 mm assistant trocar. After peritoneal incision, the ureter was illuminated using NIRF. Ureteral dissection was performed as the ureter was mobilized off the bladder diverticulum. The dissection was carried to the level of the neck of the diverticulum. A flexible cystoscope was inserted transurethrally to guide the cystotomy and to prevent injury to the left ureteral orifice. The diverticulum was excised with the assistance of NIRF. Cystorrhaphy was performed in two layers with absorbable suture and a watertight closure was confirmed.
Results: In the accompanying video, the bladder diverticulum was adherent to the left distal ureter, requiring intermittent use of NIRF to precisely mobilize the ureter and prevent inadvertent transection. The bladder diverticulum was successfully dissected and transected at its neck without violation of the left ureter as confirmed with NIRF. The robotic operative time was 1 h 52 min, and total operative time was 2 h 48 min which included cystoscopy as well as umbilical hernia repair. Estimated blood loss was 50 cc and the patient was discharged on the first postoperative day. The urethral catheter was removed after 9 days and the ureteral stent was removed 7 days later.
Conclusions: Intraoperative identification of the ureter and diverticulum margins during robotic bladder diverticulectomy can be facilitated with use of ICG and NIRF. This case adds to the growing literature demonstrating the utility of ICG in the armamentarium of the robotic urological surgeon.
Robotic‐Assisted Diverticulectomy of Urinary Bladder for a Very Uncommon Case of Hutch Diverticulum with Obstructive Uropathy
C Yang, Y Lin, Y Ou, L Huang, C Hsu, M Tung
Introduction & Objective: When the ureteral ostium is included in the bladder diverticulum, it is called Hutch diverticulum. Hutch diverticulum is rarely seen in adult and usually been diagnosed at the first 10 years in childhood as a characteristics of congenital disease. This paper is to describe a case with adult Hutch diverticulum, performed by robotic‐assisted diverticulectomy of urinary bladder.
Methods: A 27‐year‐old man had been bothered by frequent urinary tract infection, and had not been through any congenital urinary tract medical histories ever. Under ultrasound of kidneys, right hydronephrosis was seen. Thereafter, intravenous pyelography was done, and a diverticulum could be observed seated superolateral to the right ureterovesical junction (UVJ), near right ureteral orifice, and contrast retention in that diverticulum was obviously evident. The computed tomography revealed the diverticulum clearly seen with ostium included in the bladder diverticulum. Robotic‐assisted diverticulectomy on his Hutch diverticulum was performed. Before the surgery, right ureteroscopy was performed and right ureteral stent was placed inside across the diverticulum ostinum. Then, he was placed steep Trendelenburg position about 30 degrees, one camera port, two working ports (8 mm) and 1 assistant port (12 mm) were settled. The approach was planned with transperitoneal way. At first, 300 milliliter saline was instilled to bulge the diverticulum out. After identified the diverticulum and right ureter, they were both carefully dissected. The transection was made on the diverticulum neck. In the end, the cutting defect on the right ureter was carefully sutured.
Results: The whole operation went on for 140 minutes, and blood loss was measured 20 milliliter. The incised Hutch diverticulum was about 3 cm in width and weighted 5 g. After discharge, we arranged ultrasound of bladder and kidneys and intravenous pyelography at follow‐ups. Right hydronephrosis was relieved. Intact bladder storage function and fully recovery of the right ureter were seen within one year after surgery.
Conclusions: Robotic‐assisted diverticulectomy to Hutch diverticulum is a safe and efficient reconstructive surgical method.
Robot‐assisted radical cystectomy with intracorporeal modified J‐pouch neobladder in female patient
P Li, Y Yang, L Tsai, C Huang
Introduction & Objective: Radical cystectomy with pelvic lymph node dissection and urinary diversion is considered to be a stander treatment of muscle‐invasive bladder cancer. It is one of the most challenge urologic surgical procedures, especially in female. Robot‐assisted radical cystectomy (RARC) with intracorporeal urinary diversion has been shown to have promising functional and oncologic outcomes. In this video, we demonstrate step‐by‐step the technique in our institute to perform a totally intracorporeal ileal neobladder.
Methods: The video present a 66 year‐old continent and neurologically healthy women affected by muscle‐invasive bladder cancer, who underwent Robot‐assisted radical cystectomy with pelvic lymph node dissection and intracoporeal orthotopic neobladder under the Davinci Si Robotic, four arms system. We took down total 65cm ileum; 20cm from ilealcecal valve to anastomosis urethra, 40cm to reconstruct J pouch, and 5cm to anatomosis bil. ureter.
Results: No intraoperative complications occurred. Ttotal operation time was 7hr44mins. Lymph node dissection area: para‐aortic area, inter‐cava area, right renal artery area. One artery and one vein was found. Blood loss was less than 50ml. No ureter stent placed. Follow‐up neobladder volume can reach 250‐300ml after 6months.
Conclusions: RARC with pure intracorporeal ileal neobladder minimize the invasion to patient and avoid re‐docking time. It is a safe and effective procedure with satisfactory outcomes for patient and urologist.
Robotic Bladder Diverticulectomy In a Pediatric Patient
AA Elbakry, O AL‐Omar
Introduction & Objective: This is a video demonstrating robotic approach for bladder diverticulectomy in a pediatric patient.
Methods: A 4 y.o. boy presented complaining of recurrent UTI, weak urinary stream and chronic constipation. diagnostic work up included a VCUG, which revealed a large narrow neck diverticulum at the right posterolateral wall of the bladder. We started with cystoscopy to better characterize the diverticulum. A ureteral stent was placed to facilitate ureter identification during dissection. Bladder was filled with sterile water, peritoneum was incised distal the vas deferens and the a hitch stitch was placed for upward retraction of the bladder. Diverticulum wall was identified and released from surrounding fat. Careful dissection of the diverticulum neck was performed. The diverticulum neck was sharply excised. Bladder wall opening was closed in 2 layers in interrupted fashion. Peritoneal window was closed. Ureteral stent was removed.
Results: Estimated blood loss was 2 ml. Hospital stay was less than 24 hours. Urethral catheter was removed after 7 days. Post voiding residual volume was 4 cc at 6 weeks follow up. The prophylactic antibiotic was discontinued at 6 weeks postoperatively.
Conclusions: Robotic approach is feasable for bladder diverticulum excision in pediatric patients.
Robotic assisted laparoscopic partial cystectomy using the Da‐Vinci Single‐Port Robotic System
MS Tonzi, A Singh
Introduction & Objective: To report the initial case of an extraperitoneal, trans‐vesicle robotic assisted laparoscopic partial cystectomy including en‐bloc excision of a bladder diverticulum with urothelial carcinoma using the da Vinci Single Port robotic system.
Methods: A 64‐year‐old male with a history of urothelial carcinoma was found to have recurrence of his disease inside of a narrow neck bladder diverticulum on surveillance cystoscopy. Remaining bladder was evaluated with random biopsies and there was no evidence of urothelial carcinoma in the rest of the bladder. The da Vinci Single Port robotic system was used to perform an extraperitoneal, trans‐vesicle partial cystectomy with en‐bloc resection. The bladder was entered extra‐peritoneally, and the robotic port was docked directly within the bladder using a small Gelport. The diverticulum containing the tumor was excised en‐bloc from within the bladder circumferentially and the defect closed.
Results: The patient tolerated the procedure uneventfully. The total operative time was 112 minutes. The patient was discharged on postoperative day one. At follow up, cystography demonstrated no contrast extravasation and his urethral catheter was removed on post‐operative day eight. Final pathology revealed negative surgical margins.
Conclusions: This is the initial report of a trans vesicle robotic assisted en‐bloc partial cystectomy for a recurrent urothelial carcinoma in a bladder diverticulum using the da Vinci Single Port robotic system. This provides an alternative to traditional minimally invasive approaches not amenable to trans‐urethral resection.
Robotic assisted laparoscopic bladder diverticulectomy with urethrolysis
MS Tonzi, H Okafor
Introduction & Objective: Here we present a robotic assisted laparoscopic bladder diverticulectomy and urethrolysis in a patient with urinary obstruction and dysfunctional voiding following a Birch colposuspension for female stress urinary incontinence.
Methods: DKS is a 64 yo female with a history of incomplete bladder emptying and dysfunctional voiding that began following a Burch colposuspension she received for female stress urinary incontinence. CT scan revealed a large mouth bladder diverticulum, which was confirmed by office cystoscopy. Urodynamics demonstrated incomplete bladder emptying with elevated voiding pressures. Patient was scheduled a robotic assisted diverticulectomy with urethrolysis. Details of the procedure will be highlighted in the accompanying video.
Results: A robotic assisted laparoscopic bladder diverticulectomy and urethrolysis was successfully performed. The patient was discharged on POD 1. At her 2 week follow up appointment her catheter was removed and cystogram demonstrated no extravasation. At her 3 month follow up appointment she voided with a normal bell shaped curve on uroflowmetry with minimal PVR. She reported no stress urinary incontinence.
Conclusions: Robotic assisted laparoscopic bladder diverticulectomy and urethrolysis is a safe approach in managing patients with bladder outlet obstruction and voiding dysfunction following an outlet procedure for female stress urinary incontinence. Moreover, this procedure can be performed without sacrificing urinary continence achieved at the original procedure.
Moderated Poster SessionModerated Poster Session 23: Robotics/Laparoscopy I
Single Port Robotic Ureterolysis for Ureteral Obstruction From Idiopathic Retroperitoneal Fibrosis
S Crivellaro, GR Hale, L Morgantini
University of Illinois at Chicago
Introduction & Objective: Idiopathic Retroperitoneal Fibrosis (RPF) is a rare, chronic, and progressive disorder with an unknown but estimated annual incidence of 1.3/100k people. RPF can cause ureteral obstruction and impair renal function, requiring medical therapy and renal decompression – sometimes in the form of ureterolysis. Ureterolysis has been described with open, laparoscopic, and multiport robotic techniques. In continuing to apply new surgical techniques and technology to treat this uncommon disease, this report seeks to assess the safety and feasibility of a single port robotic platform for a small consecutive series of patients who underwent single port robotic ureterolysis (SPU) to treat ureteral obstruction caused by RPF.
Methods: Between November 2019 and February 2021, data were collected on all cases of ureterolysis using the SP. Patient demographic, pre, peri‐, and post operative data were retrospectively collected for key outcomes
Results: During study interval, 7 cases (5 patients) of SPU were performed. 2 cases (1 patient) with concurrent pyeloplasty were excluded from this analysis. Average follow‐up was 238 days (7‐442). Table 1 displays perioperative data. 3 of 4 (75%) patients were discharged same day of surgery; average length of stay was 0.6 days. There were no intraoperative complications, re‐admissions, or required additional interventions. All patients are symptom free. No patients are currently on medication. 4 out of 5 (80%) cases and 3 of 4 (75%) patients are stent free and with radiographic evidence of stable/improved hydronephrosis. The case and patient with stent in place had SPU performed recently, thus without adequate length of follow up and has stent in place per protocol with scheduled assessment and follow up imaging.
Conclusions: Single port robotic ureterolysis is feasible, safe and opens the door to same day surgery for definitive treatment of this condition. The functional outcomes during our follow up period are encouraging. As we continue to develop and apply new technology and methods to treat this disease, single port robotic ureterolysis should be included in future studies and comparisons to delineate its role.
Withdrawn
Robotic Salvage Partial Nephrectomy: A Viable Approach for the Management of Local Tumor Recurrence Following Failed Nephron Sparing Surgery for Renal Tumors
C Griffin, F Zahwa, R Madi
Augusta University Health
Introduction & Objective: To assess the feasibility and report outcomes of salvage robotic partial nephrectomy in patients with suspected local recurrence of renal cell carcinoma following prior nephron‐sparing surgery or ablative procedure.
Methods: In this single‐center retrospective study, a chart review was conducted on all patients who underwent robotic partial nephrectomy (n = 225) performed by a single surgeon (RM). Of these patients, eight underwent salvage robotic partial nephrectomy for suspected local recurrence of renal cancer. Patient and tumor characteristics, perioperative outcomes, tumor pathology, and oncologic outcomes were recorded.
Results: The median patient age was 58 (52‐59), and the median body mass index was 33.2 (28.4 – 41.5) kg/m2. The median salvage tumor size was 2.1 (1.2 – 3.5) cm and the median preoperative and postoperative creatinine levels were 1.10 (0.82 – 1.62) mg/dL and 1.32 (1.01 – 1.94) mg/dL, respectively. The median preoperative and postoperative hematocrits were 43.2% (38.7 – 47.6) and 36.7% (33.6 – 39.2), respectively. Only one patient demonstrated a postoperative complication, which was a pseudoaneurysm; no other complications were noted. Six of eight patients in our series were confirmed to have a viable malignant tumor in the surgical specimen. One patient had evidence of tumor recurrence following salvage robotic partial nephrectomy with a median follow‐up time of 21 (2‐37) months.
Conclusions: Our preliminary experience with salvage robotic partial nephrectomy demonstrates a feasible and safe alternative to radical nephrectomy in patients with suspected local recurrence of renal cell carcinoma. Additionally, preoperative renal biopsy may offer some utility in assuring the necessity and timing of surgery.
Perioperative Outcomes of Robotic Transvesical Single‐Port Simple Prostatectomy versus Holmium Laser Enucleation of the Prostate
D Aguilar Palacios, J Kaouk, HC Wright, M Abou Zeinab, S De
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
Introduction & Objective: Promising perioperative outcomes with a robotic transvesical single‐port simple prostatectomy (TV‐SPP) technique for the management of large prostatic adenoma were recently reported. Herein, we aimed to compare perioperative outcomes between TV‐SPP and holmium laser enucleation of the prostate (HOLEP) for large prostates.
Methods: A retrospective review of all TV‐SPP cases (2019‐2021) was performed. Relevant preoperative characteristics and perioperative outcomes of TV‐SPP patients were compared with a similar cohort of HOLEP patients with prostate glands >80gms. The percent of prostate adenoma removed was estimated by the prostate specimen weight normalized by the preoperative prostatic volume.
Results: A total of 22 TV‐SPP and 38 HOLEP patients were included for analysis. Median (IQR) preoperative prostatic volume were 168 cm3 (117‐221) and 133 cm3 (101‐158) for TV‐SPP and HOLEP (p < 0.01), respectively. There was no difference in age, BMI, comorbidities or indication for surgery (all p > 0.05), and urinary retention or bothersome symptoms non‐responsive to medical management accounted for the vast majority of cases (>80%). Both techniques removed the same percent of prostate adenoma [median (IQR) for TV‐SPP 56% (39‐69) and 51% (37‐65) for HOLEP, p = 0.65]. There was no difference in estimated blood loss [median (IQR) for TV‐SPP 150ml (69‐250) and 100ml (50‐113) for HOLEP, p = 0.08] or blood transfusion rates [5% for both groups, p‐0.52]. None of the TV‐SPP patients required continues bladder irrigation (CBI) postoperatively, while all HOLEP patients were placed on CBI per protocol (p < 0.01). Median (IQR) days with catheter was 8 days (7‐10) for TV‐SPP and 1 day (1‐1) for HOLEP (p < 0.01). Trial of void was successful in most patients at first attempt ( >95%, p = 0.52). Mild and transient de novo incontinence was noted on 1 and 7 patients from the TV‐SPP and HOLEP (p < 0.01) group, respectively. Median (IQR) for length of stay was 1day (1‐1) for both groups (p = 0.8). Overall, there was no difference in the complication rates (p = 0.18), and there were no Clavien grade ≥3 complications.
Conclusions: Our data suggest that TV‐SPP and HOLEP have similar and favorable perioperative outcomes for the management of large prostatic adenomas. Circumferential trigonization of the bladder neck with the urethra during TV‐SPP virtually eliminates the risk of major hematuria and need for CBI postoperatively, although longer catheterization time was maintained in our initial cases.
Perioperative and Postoperative Outcomes of Single vs Multi‐Port Robotic‐Assisted Partial Nephrectomy
G Yankelevich, S Santarelli, D Kim, DC Edwards, Z Taylor, M Ahn
Medical University of South Carolina
Introduction & Objective: The research surrounding single‐port robotic‐assisted partial nephrectomies (SP‐RAPN) is limited. This study focuses on the perioperative and postoperative outcomes of SP versus multi‐port (MP) RAPN at our institution. Furthermore, there are few studies utilizing Patient Scar Assessment Scale (PSAS) scores to measure patient scar cosmesis after single‐site surgeries. To our knowledge, this is the first study that uses PSAS scores in comparing MP and SP‐RAPN.
Methods: Retrospectively queried a multi‐hospital database for patients who underwent SP or MP‐RAPN. Patient demographics, comorbidities, ASA status, and clinicopathologic disease characteristics were compared via Microsoft Excel® and Stata/MP 15.1 (StataCorp LP) using two‐sided tests with a significance level of 5%. Preoperative and postoperative hematocrit, total operating time (TOT), warm ischemia time (WIT), estimated blood loss (EBL), surgical margins, and morphine milligram equivalents (MME) were analyzed in the same fashion. Scar healing with subjective PSAS scores were recorded.
Results: 41 patients underwent RAPN between March 2018 and October 2020: 15 patients underwent SP and 26 underwent MP PN. Evaluation of perioperative parameters showed no significant difference in EBL, conversion from robotic approach, or positive surgical margins (Table 1). The SP approach was longer in both TOT and WIT, however this was skewed significantly by one case. Most of the patients who underwent SP‐RAPN used less than 24 daily MME (Figure 1). The MP‐RAPN cohort had a much broader usage of narcotics with much higher daily MME. There was no statistically significant difference between the cohorts, with both platforms yielding mean PSAS scores less than 12 out of 60 points possible.
Conclusions: SP‐RAPN is a safe and reasonable alternative to MP‐RAPN. There is no difference in surgical outcomes of the two techniques in regard to surgical margins, complication rates, bleeding, or length of hospital stay. PSAS scores indicate equivalent scar healing from both platforms.
Robotic Retroperitoneal Partial Nephrectomy in pT1b/> tumors – pushing the boundaries of robotic retroperitoneal surgery
S Sarkar, D Sri, J Oakley, M Malki, NJ Barber, M Hussain
Frimley Park Hospital
Introduction & Objective: Retroperitoneal renal surgery has demonstrated better quality of recovery compared to transperitoneal routes. As the boundaries of what is achievable robotically continue to be pushed, we present the findings of retroperitoneal RAPN at our high volume tertiary referral centre, exploring its feasibility and safety in T1b and higher stage renal tumours.
Methods: A prospective database of almost 800 RAPNs (2009 – 2020) was reviewed and 147 RAPNs for T1b/ > RCC were performed at our centre. Of these, 137 cases were performed via the retroperitoneal route. In our practice, we utilise a 4 port approach to retroperitoneal RAPN. Patient, tumour and operative characteristics were assessed and both oncological outcomes and trifecta and pentafecta achievements were determined.
Results: From 147 cases, 25 RAPNs were performed for imperative reasons, whilst the remainder were elective. Mean BMI+/‐ s.d amongst our cohort was 29.3 +/‐ 6.2. Median tumour size was 4.5cm (range 1.4cm – 10.5cm) and 73% of cases were stratified as intermediate/high risk using R.E.N.A.L nephrometry scoring. Thirteen patients had tumours in a hilar location, and 24% were anterior tumours. Median blood loss was 50mls, with an open conversion rate of 3%. Median warm ischaemic time (WIT) was 24mins, positive surgical margins were found in 4.7% and our post‐operative Clavien 3/ > complication rate was 3%. We had a 2 day median length of stay with a 30 day readmission rate of <5%. A third of patients had T3a/ > disease on definitive histology. Over a median 15 month follow up period (range 1 – 113 months), 7% of patients developed recurrences and our cohort demonstrated a 97% 5 year cancer specific survival. Trifecta was achieved in 59% of cases and pentafecta in 50%. R.E.N.A.L score (p = 0.001) and operative time (p = 0.001) were found to statistically significantly influence achievement of trifecta and in addition to these two factors, intraoperative blood loss (p = 0.027) influenced pentafecta achievement.
Conclusions: We demonstrate the retroperitoneal approach in RAPN is technically feasible and oncologically safe irrespective of location and complexity even in the challenging group of T1b/ > RCCs. In the hands of high volume centres that are skilled in the retroperitoneal approach the benefits of retroperitoneal surgery can be extended even to this challenging cohort of patients.
Perioperative Outcome in Robot‐Assisted Partial Nephrectomy with Surgical Navigation System for Highly Complex Tumors
J Mutaguchi, S Kobayashi, B Cho, K Lee, K Monji, E Kashiwagi, A Takeuchi, M Shiota, J Inokuchi, M Eto
Graduate School of Medical Sciences, Kyushu University Department of Urology
Introduction & Objective: Robot‐assisted partial nephrectomy(RAPN) is a widely accepted standard treatment for small renal tumors. Although the cases of RAPN increase, RAPN for highly complex tumor (HCT) are still challenging task even in expert surgeons. To establish a computer aided diagnosis system for RAPN, we have developed surgical navigation (SN) synchronized a endoscopic movement with 3‐dimensional virtual reality models. In this study, we evaluate the perioperative outcome of RAPN with SN for patients with HCT.
Methods: We retrospectively analyzed clinical outcomes for 157 patients who underwent RAPN with SN in our hospital between September 2016 and July 2019. We defined HCT as clinical T1b (cT1b) tumor, hilar tumor, and completely endophytic tumor. Patients with any one of the HCT were classified into HCT group (n = 72), and all other patients were classified into the non‐HCT group (n = 85). Demographic and tumor characteristics (age, sex, BMI, R.E.N.A.L nephrometry score (RNS), tumor site) and clinical outcomes (warm ischemia time (WIT), console time, trifecta and pentafecta achievement) were analyzed. Trifecta defined as WIT of less than 25 minutes, no complications and negative surgical margins. Pentafecta defined as trifecta plus greater than 90% preservation of estimated glomerular filtration rate postoperatively and no chronic kidney disease upstaging at 12 months. Multivariable logistic regression analysis were used to evaluate the predictive factor for prolonging WIT among HCT.
Results: There were no significant difference in baseline characteristics. HCT group had higher RNS (P < 0.01) and were larger in tumor size (38.0 vs 25.0 cm; P < 0.001). In perioperative outcome, HCT group had longer WIT (17.5 vs 13.0 min; p < 0.001) and longer console time (107.5 vs 96.0 min; p = 0.013) than non‐HCT group. There were no significant differences in the trifecta and pentafecta achievement between the two groups. Multivariate analysis found that only cT1b tumor was the independent factor associated with prolonging WIT among the HCT (OR: 4.24; p = 0.001).
Conclusions: RAPN with SN may contribute to acceptable perioperative outcome for patients with HCT. cT1b tumor should be paid attention due to prolonging WIT among HCT.
Oncologic Outcomes of Dehydrated Human Amnion/Chorion Membrane After Nerve‐Sparing Robotic‐Assisted Radical Prostatectomy: A Propensity Score Matched Analysis
J Noël, S Reddy, M Sandri, S Bhat, M Moschovas, T Rogers, V Patel
Global Robotics Institute
Introduction & Objective: To determine if patients undergoing placement of dehydrated human amnion/chorion membrane (dHACM) on the neurovascular bundle (NVB) during nerve‐sparing (NS) robot‐assisted radical prostatectomy (RARP) impacts on medium term oncological outcomes, as compared to a propensity score matched cohort.
Methods: From 2013 – 2019, we used dHACM in NS RALP in 635 patients. We excluded less than 12 months follow up and no data on current cancer status (n = 64 & n = 36 respectively), benign prostatic hyperplasia (n = 5), and unilateral NS (n = 1). From 2683 patients who did not undergo dHACM placement at RARP, we excluded those without data on cancer (n = 216) and without pre operative ISUP grade (n = 2). 529 patients who underwent NS RARP with dHACM (amnio group) were matched to 2465 patients who did not have dHACM at NS RARP (non amnio group) with a 1:1 propensity score and a minimum follow up of 36 months.
Results: Matching resulted in the analysis of 443:443 patients. For both groups, bilateral full NS was performed in 73% and partial NS 27%. Kaplan‐Meier cumulative incidence functions (CIFs) (Figure 1) for BCR showed no evidence that amnio group was better than non amnio group (p = 0.133). Sub‐analysis of PSM comparison to BCR is shown in the Kaplan‐Meier (CIFs) (Figure 2). Patients without PSM and with dHACM had significantly lower BCR rates compared to patients without PSM and without dHACM (HR = 0.56, 95% CI 0.34‐ 0.90, p = 0.02). Patients with PSM and with dHACM, had insignificantly higher BCR rates compared to patients with PSM and without dHACM (HR = 3.06, 95% CI 0.84 − 11.06, p = 0.09). The overall difference in BCR between all patients without and with PSM was statistically significant (HR 5.46,95% CI 1.40‐21.18, p = 0.014).
Conclusions: The data suggests that using dHACM does not appear to adversely increase BCR in patients with or without PSMs. Long term outcomes of dHACM on cancer recurrence and specific mortality after RARP will be undertaken.
Robot‐Assisted Partial Nephrectomy: A Single‐Center Matched‐Pair Analysis of the Retroperitoneal versus the Transperitoneal Approach
A Eraky, C Hamann, N Harke, M Tropmann‐Frick, K Juenemann, D Osmonov
University Hospital Schleswig‐Holstein, Campus Kiel, Department of Urology and Pediatric Urology, Kiel, Germany
Introduction & Objective: Robot‐assisted partial nephrectomy is a minimally invasive treatment option for localized kidney tumors. It can be performed either via the more routinely used transperitoneal approach or the retroperitoneal approach. Assessment and comparison of the retroperitoneal (RRPN) perioperative variables and the transperitoneal (TRPN) robot‐assisted partial nephrectomy using a matched‐pair analysis.
Methods: A retrospective review was carried out for 224 patients who underwent robot‐assisted partial nephrectomy between 2014 and 2019; 63 patients and 161 Patients underwent retroperitoneal and transperitoneal approaches, respectively. A matched‐pair analysis was performed on 51 pairs of patients.
The matching criteria used were age, Charlson comorbidity index, BMI (Body Mass Index), the grade of renal insufficiency, tumor diameter, and PAUDA score.
Results: In the group with retroperitoneal access, the time to reach the renal hilum (p < 0.001), the overall complication rate (p = 0.008), and the major complication rate (p = 0.01) were significantly lower compared to the transperitoneal group. The operative time was 143 vs. 150 minutes (p = 0.63), in RRPN vs. TRPN, respectively. Warm ischemia time was 10 minutes in RRPN vs. 12 minutes in TRPN (p = 0.07). Early unclamping was used in 71% in RRPN vs. 48% in TRPN (p = 0.02). The length of hospital stay was six days in both groups (p = 0.11). The cases' complexity, the rate of positive surgical margins, and postoperative kidney function were comparable in both groups (p > 0.05).
Conclusions: The advantages of RRPN lie in the shorter time to reach the renal hilum and the lower complication rates; the comparability with the other parameters proves the safety and feasibility of the retroperitoneal access for localized kidney tumors.
The retroperitoneal approach should be part of the robot surgical training to enable surgeons to master both techniques to treat localized renal tumors. Further studies are needed to identify objective selection criteria for the optimal choice of surgical access.
Robotic Approach for Distal Ureteral Reconstruction in Post‐Radiation ureteral stricture
AA Elbakry, K Aldabek, T Trump, K Mitchell, MW Salkini
Department of Urology, West Virginia University Hospital
Introduction & Objective: We are aiming to evaluate the role of robotic surgery in ureteral reconstruction following pelvic radiation.
Methods: We retrospectively identified all patients who underwent robotic reconstruction of the distal ureter in the last 10 years. Data collection included demographic data, preoperative baseline clinical data, operative data (operative time, EBL, conversion to open, surgical technique) and postoperative outcomes (early postoperative complications, hospital stay, 30‐days readmission, postoperative and delta eGFR, and reintervention rate). Analysis was done using IBM SPSS v24. Independent sample t test and Mann‐Whitney U test were used for continuous variables and Chi Square and Fisher's Exact tests were used for categorical variables.
Results: A total of 31 cases of robotic distal ureteral reconstruction were identified. Patients were categorized into 2 groups. Group 1 includes radiation naive patients and group 2 was formed by patents with history of pelvic radiation. The two groups were similar regarding baseline demographic data. Initial presentation was similar in both groups with evaluation for hydronephrosis being the most common presentation. Operative time, EBL, conversion to open, and length of stay were similar in both groups. There was no difference regarding early complications, 30‐days readmissions, and the duration of foley catheter or ureteral stent. Majority of patients in both groups reported symptoms improvement (100% in group 1 and 93.3% in group 2. Delta eGFR showed decrease eGFR in group 2 by 12 ml/min and improvement in group 1 by 3.1 ml/min, with no significant difference. One patient (6.7%) in group 2 required reintervention and underwent nephrectomy, while no patients in group 1 required reintervention.
Conclusions: Robotic surgery is a feasible approach for post‐radiation distal ureteral reconstruction with a high success rate and relatively similar outcome to radiation naive patients. More studies with a larger number of patients are needed to fully evaluate the role of robotic surgery in post‐radiation settings as an alternative for classic open surgery.
Robotic‐assisted radical prostatectomy in young adults: age‐stratified oncological and functional outcomes
S Bhat, M Covas Moschovas, J Noël, S Reddy, T Rogers, V Patel
Global robotics institute
Introduction & Objective: There is a scarcity of information on the outcomes of robotic‐assisted prostatectomy (RALP) in young men. To compare the age‐stratified functional and oncological outcomes of RALP in men aged ≤55 years.
Methods: Among 10,997 patients in our RALP series, 2,243 were ≤55 years old. These men were divided into 3 age‐stratified groups (group 1: ≤45 years, group 2: 46‐50 years, group 3: 51‐55 years old).
Results: Age‐stratified groups were compared for clinical, oncological, and trifecta outcomes. Kaplan‐Meier curves and Cox regression models were used to identify survival estimations and their predictors.
Results and Limitation: Overall, 33% and 22% of men had non‐organ confined (≥pT3) and Gleason ≥4 + 3 prostate cancer at final pathology, respectively. Younger patients had a higher incidence of low‐risk disease and better erectile function at presentation. Organ‐confined and Gleason 3 + 3 cancer rates for men ≤45 and 51‐55 years were 82% vs. 74% and 41% vs. 30%, respectively (p < 0.05). Biochemical recurrence‐free survival was similar among age‐stratified groups. Bilateral full nerve‐sparing (NS) rate was significantly higher in younger patients (74% in group 1 vs. 56% in group 3, p < 0.001). One‐year trifecta rates were 79.8%, 71.6%, and 63.9% regardless of baseline SHIM and NS for increasing age groups, respectively (p < 0.001). Age, comorbidity score, and extent of NS were independent predictors of functional recovery. This study is limited by its retrospective design.
Conclusions: At RALP, one third of patients ≤55 years have locally advanced or high‐risk prostate cancer. Age ≤45 years is associated with higher incidence of favorable tumor characteristics, which gives the surgeon increased ability to perform bilateral full NS, resulting in better functional recovery. Even in this young age group the influence of age is seen reflected by increase in the grade of disease and decrease in potency.
Hospital Ownership, Geographic Region, Patient Age and Insurance Status Appear to Influence Patient Selection for Robotic‐Assisted Ureteral Reimplantation: A Population‐Based Analysis
JT Kurtzman, AS Ha, R Kosber, R Blum, S Brandes
Columbia University Irving Medical Center
Introduction & Objective: Robotic‐assisted ureteral reimplantation (RAUR) has gained traction among pediatric urologists. However, less is known about its use among adults in the community. While prior studies have suggested several advantages of a robotic approach, none have addressed national trends in its utilization nor factors associated with patient selection. This is the first population‐based study in the literature to evaluate these issues.
Methods: The United States National Inpatient Sample was queried to identify all adult patients who underwent elective, non‐transplant related, ureteral reimplant (ICD‐9: 56.74), with or without a robotic assistance (ICD‐9: 17.42) from 2010‐2015. Survey‐weighted logistic regression via backwards selection Akaike Information Criterion was used to identify patient and hospital‐level factors associated with robotic surgery. Adjusted regression models were used to explore the association of robotic surgery with outcomes including: inpatient red blood cell (pRBC) transfusion, length of stay (LOS), and total hospital charges.
Results: A weighted total of 9,845 cases were identified, of which 1,793 (18.2%) were performed robotically. There were significantly increased odds of robotic surgical selection across consecutive years from 2010‐2015 and among patients operated on at private for‐profit hospitals, but significantly decreased odds among older patients, those with Medicaid and those operated on in Southern and Western states (Figure 1, all p < 0.05). When compared to open and laparoscopic approaches, RAUR was associated with reduced LOS (IRR: 0.57; p < 0.001) and decreased odds of pRBC transfusion (OR: 0.35; p < 0.001). There was no difference in the mean ratio of total hospital charges (Ratio: 0.88; p = 0.12).
Conclusions: Open ureteral reimplantation remains the most common surgical method used in the United States. Rates of RAUR have gradually increased with time, yet seem to be underutilized, despite improved perioperative morbidity and equal cost. Older age, Medicaid insurance and care at a non‐private hospital, negatively influences surgical selection for a robotic approach. This suggests a potential issue of unequal access to care or patient selection bias.
Racial Comparison of Patients Undergoing Minimally Invasive Partial Nephrectomy for Renal Masses at a Large Volume Tertiary Center
KG Sands, R Bhatt, J Vetter, A Paradis, AK Chow, S Bhayani, RS Figenshau, R Venkatesh
Washington University School of Medicine
Introduction & Objective: African American (AA) race has been identified to have a higher incidence of chronic kidney disease (CKD) and worse renal cancer survival compared to Caucasian Americans (CA) irrespective of tumor size, pathological type, and surgical procedure. We aimed to compare the outcomes between CA and AA patients undergoing minimally invasive partial nephrectomy at our high‐volume center.
Methods: We queried our partial nephrectomy data repository from 2007‐2017. We identified 981 cases of partial nephrectomy (robotic n = 943 and laparoscopic n = 38) of which there were 852 CA and 129 AA patients. We compared age, gender, body mass index (BMI), operative time, estimated blood loss (EBL), nephrometry score, tumor size, pre and post‐operative estimated glomerular filtration rate (GFR), length of stay, Charlson Comorbidity Index (CCI), tumor characteristics and 30‐day complication rate. We then estimated the overall and disease‐specific survival.
Results: Age, BMI, operative time, EBL, nephrometry score, tumor size, CCI, length of stay, and gender were not statistically different. The mean preoperative GFR was higher in the AA cohort (91.4 mL/min/1.73m2 vs 86.1 mL/min/1.73m2, p = 0.007); however, at 1‐year there was no mean difference (76.8 mL/min/1.73m2 vs 74.5 mL/min/1.73m2, p = 0.428). There was a higher percentage of Fuhrman Grade 3/4 in AA (33.3% vs 22.5%, p = 0.044). The AA cohort had a 2.66x higher incidence of papillary renal cell carcinoma (RCC) (34.9% vs 13.1%, p < 0.001) and unclassified RCC (3.9% vs. 0.4%, p = 0.001). There was no difference in tumor stage (p = 0.260) or incidence of benign histology (15.3% vs 11.6%, p = 0.278). There were no differences in thirty‐day complications (p = 0.330). Median follow‐up was 43.2 months. Using Kaplan‐Meier curves, there was no observed difference in overall survival (p = 0.752) or disease‐free survival (p = 0.403).
Conclusions: Our cohort of AA and CA patients with intermediate follow up showed no worse outcomes for CKD or survival when undergoing laparoscopic or robotic partial nephrectomy. For low stage renal cancer, there was no difference in overall survival and disease‐free survival at a median follow up of 43.2 months among AA patients, despite having higher grade tumors and a higher percentage of unclassified RCC. Our cohort of AA patients did have a higher incidence of papillary RCC. The equivalent overall and disease‐free survival could be due to the earlier discovery of lower stage renal masses incidentally identified on imaging studies performed equally for other reasons in both AA and CA patients.
Contemporary pure laparoscopic vs robotic assisted laparoscopic radical nephrectomy: Cost and peri‐operative Outcomes at a high‐volume tertiary center
KG Sands, RS Figenshau, J Vetter, A Paradis, A Pierce, AK Chow, S Bhayani, K Du, E Kim, R Venkatesh
Washington University School of Medicine
Introduction & Objective: The proportion of robotic procedures continues to rise although there is no distinct Current Procedural Terminology (CPT) code. The literature reinforces that robotic procedures take longer and are more costly. We compared cost and peri‐operative outcomes of laparoscopic radical nephrectomy (LRN) and robotic assisted radical nephrectomy (RARN) at our high‐volume center.
Methods: We retrospectively reviewed our 2012‐2015 data repository for patients undergoing RARN and LRN for a renal mass. Peri‐operative and oncologic outcomes were compared. We performed a multivariate analysis of operative time, estimated blood loss, length of stay, overall and major 90‐day complication rate while controlling for demographic data, Charlson Comorbidity Index (CCI), tumor size, and surgeon factors. We compared fixed, variable and distinct procedural costs.
Results: We identified 99 LRN and 95 RARN cases. There was no difference in demographic data, tumor size, preoperative renal function, and malignant histology. LRN had more comorbidities (49.5% vs 27.3% CCI 2+, p = 0.018). Mean preoperative GFR was higher in the robotic cohort (84.8 vs 75.1, p = 0.48). Mean operative time was 32.7 minutes longer (p = 0.002) and estimated blood loss 145ml higher (p = 0.007) for the RARN cohort. Mean length of stay was 0.9 days longer for RARN patients. Major and all 90‐day complication rates were no different. RARN mean procedural cost was higher by $464 when controlling for operative time (p < 0.001). Fixed costs were not statistically different. RARN variable costs were estimated to be $2,310 higher (p = 0.045).
Conclusions: Even with cost‐conscious experienced renal surgeons, RARN is associated with a longer procedure, higher supply costs, and higher hospitalization costs. There were fewer 30‐day readmissions for the RARN cohort with no difference in PSM and complications. With fewer LRN in the US each year, discussion to address cost is warranted. Without better outcomes for robotic surgery, a distinct CPT code is unlikely to happen.
Standardizing robotic partial nephrectomy results in similar patient outcomes across the tumor complexity spectrum
KE Okhawere, A Beksac, R Patel, TG Korn, M Ahsan, KN Meilika, KK Badani
Icahn School of Medicine at Mount Sinai
Introduction & Objective: Results for robotic partial nephrectomy (RPN) should remain reproducible and optimal, despite tumor complexity. This study compares perioperative and postoperative outcomes of patients with varying renal tumor complexities that underwent a standardized approach to robotic partial nephrectomy.
Methods: This is a retrospective single center study of 386 patients who have undergone robotic assisted partial nephrectomy via transperitoneal approach for kidney cancer using first assistant sparing technique (FAST) between May 2011 and September 2019. Baseline clinical data, perioperative, and postoperative outcomes were compared across tumor complexity ‐ low tumor complexity (4‐6), moderate tumor complexity (7‐9), and high tumor complexity (10‐12). Tumor complexity was defined using the R.E.N.A.L nephrometry score. Baseline clinical data, perioperative, and postoperative outcomes were compared using Kruskal Wallis test, Chi‐Square test of Independence and Fisher's exacts test.
Results: Of the 386 patients, 52.07% had low tumor complexities (n = 201), 41.97% had moderate tumor complexities (n = 162), and 5.96% had high tumor complexities (n = 23). Patients with high tumor complexity had significantly longer operative time (149 min vs. 143 min moderate complexity vs. 130 min low complexity, p = 0.023), longer ischemia time (12 min vs. 12 min intermediate vs. 10 min low complexity, p = 0.001), and significant reduction in eGFR (ΔeGFR) (‐12.95 mL/min/1.73m2 vs. ‐5.78 mL/min/1.73m2 intermediate vs. ‐0.96 mL/min/1.73m2 low complexity, p = 0.002). EBL, blood transfusion rate, postoperative complication rate, surgical complication rate, major complication rate, length of hospital stay, positive surgical margins, and trifecta achievement were not significantly different across complexities.
Conclusions: Regardless of tumor complexity, clinical and functional outcome among low, intermediate, and high complexity tumors were relatively similar. A standardized and reproducible technique is feasible through a robotic surgical platform. As surgical treatment advances to include management of higher complexity tumors, optimal patient outcome and renal functional preservation following partial nephrectomy is critical.
Comparing Partial Nephrectomy modalities in the Age of Robotics: Contemporary results from the US National Inpatient Sample
D Mikhail, M Nayan, M Kim, L Richstone, A Feldman
Lenox Hill/Northwell Health
Introduction & Objective: Robotic surgery has become the primary modality for many urological procedures in the US. Despite this, costs continue to be a barrier in other health systems. We sought to evaluate whether increases in utilization trends has lead to decreased overall costs and improved outcomes that are significant compared to laparoscopic and open partial nephrectomy.
Methods: We conducted a retrospective observational cohort study using the US National Inpatient Sample (NIS) discharge database from 2018 to compare open (OPN), laparoscopic (LPN) and robotic (RPN) partial nephrectomies. We controlled for comorbidities using the Elixhauser comorbidity index. Our primary objectives were to compare total charges, length of stay and transfusion rates between the 3 modalities and between LPN/RPN. We further compared our results to historical values (2013 NIS database). Statistical analysis was performed with appropriate survey weighting using Stata 16.
Results: A total of 4560 discharges representing 22800 partial nephrectomies were identified in the 2018 NIS database. Of these, 5890(26%) were OPN, 2990 (13%) were LPN and 13910 (61%) were RPN. Mean age was slightly lower for OPN (57.2 vs. 59.1/59.6, p = 0.002). Males made up 60% of our total sample, but there was no difference in sex distribution between modalities (p = 0.28). Mean Elixhauser score was higher for OPN (3.06 vs. 2.77/2.66, p = 0.002) as was proportion with score = >3 (57% vs. 49%/48%; p = 0.001), however, LPN and RPN were not significantly different. Those receiving RPN were more likely to have private insurance (50% vs. 46% LPN/44% OPN, p = 0.02). Mean LOS was higher for OPN than LPN/RPN (5.2 vs. 2.7/2.4, p < 0.01). Transfusion rates were also higher for OPN than LPN/RPN (7.5% vs. 2.3%/1.55%, p = < 0.001). Interestingly, total charges were lowest for RPN in 2018 compared to LPN/OPN ($71,277 vs. $75,228/$86,682, p = 0.0045). Although RPN/LPN costs were not statistically different (p = 0.168), this is a significant change from the 2013 data where RPN was less frequent (48% vs. 61%) and still the most expensive ($60,101 vs. $58,453/$59432). Controlling for Elixhauser score, age and sex – RPN remained significantly less costly in the 2018 data.
Conclusions: Robotic approach has taken over as the most commonly performed in the US for partial nephrectomy. With the urologic communities increasing experience, cost comparison to other modalities for partial nephrectomy is becoming significantly cheaper and is trending towards the most cost efficient of the three modalities, even compared to laparoscopy.
Robotic Partial Nephrectomy for Solitary Kidney Tumors –Expanding the Indication to T2 And T3 Disease?
A Beksac, S Kim, KE Okhawere, M Abou Zeinab, R Harrison, L Lenfant, ZR Schwen, MD Stifelman, DD Eun, R Abaza, KK Badani, J Kaouk
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
Introduction & Objective: We retrospectively compare oncological and renal functional outcomes between robotic and open partial nephrectomy (PN) in patients with a T2‐T3 renal mass and a solitary kidney.
Methods: From a multi‐institutional series which includes 86 open and 3949 robotic partial nephrectomies, we retrospectively identified 45 that underwent an open Partial and 120 that underwent a RPN in a solitary kidney. Of this cohort, 28 RPN and 15 OPN patients were confirmed to have a pT2 or pT3 renal cancer. Surgeries were performed between January 2012 and July 2019. Patients with familial renal cell carcinoma, prior ipsilateral PN or multiple ipsilateral synchronous tumors were excluded from analysis. Baseline demographics, clinical and tumor characteristics, perioperative and postoperative outcomes were compared using Chi‐square, Fisher's exact, Mann‐Whitney U, and student's t tests.
Results: Demographic data is presented in Table 1 and there were no significant differences. Peri‐operative and post‐operative data is presented in Table 2. Cold ischemia was utilized more in open group (92.9% vs. 10.7%, p < 0.001) and OPN group had longer ischemia time (48.9 min vs. 23.1 min, p < 0.001). Length of stay was longer in the OPN group (5 vs. 3 days, p = 0.001). Positive margin (20% OPN vs 14.3% RPN; p = 0.677). At a mean follow up of 19 months local recurrence rates (1 OPN vs 2 RPN, p = 1.000) were comparable, de novo CKD rate (46.7% OPN vs. 32.1% RPN, p = 0.348) and GFR preservation (75.2%% in OPN vs. 83.6% RPN, p = 0.368) were favorable in the RPN but this difference did not reach statistical significance.
Conclusions: With good case selection and experienced hands, robotic approach offers a reasonable alternative to open surgery in patients with T2 and T3 tumors and a solitary kidney.
The Outcome of Robotic Ureteral Reimplantation
MW Salkini
West Virginia University
Introduction & Objective: Ureteroneocystostomy, occasionally with creation of Boari flap, is the best option to substitute for the loss of the distal ureter in both benign and malignant conditions. The procedure is usually performed through a large midline or Gibson incision. Utilizing the robotic da Vinci® surgical system made it feasible to achieve the objectives of the procedure with minimally invasive approach. Our aim is to report our experience with robotic assisted ureteral substitution with and without creation of Boari flap.
Methods: We utilized de Vinci® robotic surgical system between September 2009 and February 2021 to reconstruct 37 distal ureteral units in 31 patients (6 patients needed bilateral ureteral reimplantation). 17 benign and 20 malignant conditions needed ureteral substitution. We prospectively collected the data with our institutional IRB approval. The distal ureter was excised with bladder cuff in cases of TCC involving the distal ureter. The proximal ureteral end was spatulated and re implanted to the bladder either directly or after developing Boari flap to enable tension free, leak proof anastomosis. Negative margin was insured in all the malignant cases.
Results: The average patient age was 63 years (ranging from 25‐80). We had 17 male and 14 female patients. All cases were completed robotically except one that needed to be converted to open due to adhesion. The patients were followed for an average of 35 months (ranging from 3 months to 84 months). All the ureters (%100) with benign strictures were patent after reimplantation during the time of follow up. However, 4 ureters (%21) who had lower ureteral TCC developed ureterovesical anastomosis stricture. All strictures occurred in patient with high grade TCC on the initial and final pathology after nephroureterectomy with excision of the flap. None of the 6 patient who had hx of radiation developed stricture. The distal ureter was excised with bladder cuff in cases of TCC involving the distal ureter.
Conclusions: Robotic reconstruction of the lower ureter with Boari flap is feasible and has an acceptable oncologic outcome. High grade TCC of the lower ureter is predictor of recurrence at the anastomosis. Longer follow up is needed especially in cases of malignancy.
Robotic Inferior vena cava (IVC) Tumor thrombectomy: single center series of 11 cases
N Pokala
University of Missouri
Introduction & Objective: Propagation of renal cell carcinoma (RCC) into the IVC occurs in 4‐10% of cases. While technically challenging, complete surgical resection of the tumor and thrombus offers a potential cure. Historically, the procedure was performed via the open approach. In recent years, a few small series have been published which highlight the feasibility and safety of robotic‐assisted laparoscopic (RAL) IVC tumor thrombectomy for RCC. In this study, we present our experience with RAL IVC tumor thrombectomy in 11 patients.
Methods: From 2015‐20 a single surgeon at the University of Missouri performed 11 RAL IVC tumor thrombectomies. Patients were reviewed retrospectively, data were collected on demographicss, tumor characteristics, surgical technique, complications, post‐operative course, follow‐up and outcomes.
Results: All patients were Caucasian (9 male). Median age was 64 years, median BMI was 27 Kg/m2 and median Charlson Comorbidity Index was 3.. Mean tumor size was 8.6 cm, mean IVC thrombus length was 4.5 cm and 1 tumor was left sided. By the Mayo classification system, 1 thrombus was level I, 6 were level II and 4 were level III. 5 patients had limited metastatic disease prior to surgery. 3 tumors were embolized preoperatively. 2 patients were Jehovah's witnesses and underwent intraoperative normovolemic hemodilution for planned autotransfusion. 10 patients underwent successful RAL IVC tumor thrombectomy without conversion. 1 case was converted to open radical nephrectomy only due to failure to progress in the setting of severe fibrosis and extensive desmoplastic reaction. For level III thrombi that extended to the hepatic veins, both supra‐hepatic IVC control and Pringle maneuver using liver mobilization techniques were preformed robotically. All cases were completed without intraoperative embolic event. Median operative time was 7.1 hours (range 5.5‐12) and median EBL was 900cc (range 400 to 5000). 5 patients received intraoperative blood transfusions. Median hospital stay was 5 days (range 4 to 14). Postoperative complications included 1 Clavien‐Dindo grade II (DVT), 3 grade IIIa (pneumothorax), 2 grade IVa (post op MI and sepsis), and 1 grade V. Thirty‐day mortality rate was 9%.
Conclusions: We present our single‐center 11 patient series of RAL IVC tumor thrombectomy performed on level I through III tumor thrombi. In our study, 1 case was converted to open and 1 death occurred within the 30‐day postoperative period due to progression of the thrombus and renal failure. The robotic approach to IVC tumor thrombectomy is feasible and safe, including the use of robotic liver‐mobilization techniques for level III thrombi extending to the hepatic veins.
Automatic 3D augmented reality Robot Assisted Partial Nephrectomy with Indocyanine green guidance for a more precise and safety procedure
F Porpiglia, D Amparore, F Piramide, E Checcucci, P Verri, P Alessio, A Pecoraro, S De Cillis, A Piana, G Volpi, M Sica, P Piazzolla, A Bellin, M Manfredi, E Vezzetti, C Fiori
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
Introduction & Objective: In the actual scenario of nephron sparing “precision” surgery, the availability of hyper‐accuracy 3D models (HA3DTM) revealed to be useful thanks to their spatial visualization.
In the last years, a step further was represented by the advent of Augmented Reality (AR) technology, in which the superimposition of 3D virtual images allowed an intraoperative surgical navigation.
In this study, with the aim to automatize the 3D virtual and endoscopic images co‐registration, we developed a dedicated software based on computer vision algorithms.
Methods: This is a feasibility study of our new dedicated software, named “IGNITE” (Indocyanine GreeN automatIc augmenTed rEality), able to automatically anchor the HA3D™ model with the endoscopic vision of the real organ with the use of computer vision algorithms. These tools need clear landmarks to correctly identify the target organ. In order to overcome the colors similarity of the operative field and to provide a more depictable shape of the organ we decided to use indocyanine. In this way the kidney appears as a bright green organ surrounded by a dark operative field (fig 1).
We enrolled patients with renal mass scheduled for AR robot‐assisted partial nephrectomy. All patients underwent a four‐phase contrast‐enhanced CT, in order to create the HA3D models, visualized as AR images inside the robotic console. Perioperative and postoperative data were collected and analyzed.
Results: Ten cases were enrolled in this pilot experience. Mean lesions size was 46.6 (+16.3) mm. Median PADUA score was 9 (IQR 8‐10). Mean operative and ischemia time were 88.9 (±42.7) and 20.5 (3.5) min, respectively.
In all the cases the automatic tracking was successful without manual assistance, allowing to perform enucleoresection of the renal mass with no damages of the tumor's pseudocapsule and avoiding positive surgical margins. Moreover, no intra‐ or postoperative complications ( >2 according to Clavien‐Dindo) were recorded.
Conclusions: Present findings suggest that the new evolution of our AR platform based on computer vision algorithm allows an effective automatic AR RAPN leading to a correct identification of the tumor without risk of complications or positive surgical margins.
Transitioning to the Extraperitoneal Single‐Port Robotic Kidney Transplantation
J Kaouk, M Abou Zeinab, A Beksac, Y Lin, A Aminsharifi, ZR Schwen, A Wee, M Eltemamy
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
Introduction & Objective: Robotic kidney transplantation (RKT) is a new therapeutic alternative to the standard open approach. The single port robotic approach has the potential to decrease surgical morbidity and allows for an extraperitoneal approach compared to the current robotic practice that is limited to the transperitoneal space. We present our initial experience of 7 patients who underwent SP RKT.
Methods: Seven patients with end stage renal disease (ESRD) underwent SP RKT. Both transperitoneal (cases 1‐3) and extraperitoneal (cases 4‐7) approaches were used.
All robotic transplant cases were completed successfully through a single periumbilical incision without the need of any additional ports. Intracorporeal ice was implemented in the last 3 cases.
We prospectively collected the perioperative data and postoperative kidney function by frequent serum creatinine measurement, and protocol biopsies at 3‐6 months and 1 year after transplantation.
Results: The mean age at transplantation was 55 years, mean BMI was 30 kg/m2 and four patients were males. Three patients had preemptive RKT, three were previously on intermittent hemodialysis and one patient was on peritoneal dialysis. Median (IQR) total operative and vascular anastomosis times were 372 (365,444) and 53 minutes (46, 56) respectively. All patients had good urine output during the first 24 hours and progressive improvement of graft function. None of them had delayed graft function requiring dialysis. Median (IQR) hospital stay was 2 days (2, 3) and median pain score at discharge was 2. Median creatinine level at 2 weeks, 1 month and 1 year were 1.5, 1.3, and 1.1 mg/dL respectively. All patients up to 1 year follow up had no acute rejection on protocol biopsies.
Conclusions: RKT using the single‐port platform is feasible and can be safely performed using the extraperitoneal approach. This approach provides patients with less surgical morbidity and successful graft functional outcomes.
Transvesical Single‐Port Radical Prostatectomy: Our Initial Series
J Kaouk, M Abou Zeinab, A Beksac, ZR Schwen
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
Introduction & Objective: Transvesical robot assisted radical prostatectomy (RARP) is an alternative approach for transperitoneal and extraperitoneal techniques in the treatment of localized low‐intermediate risk prostate cancer. We present the perioperative and postoperative outcomes of our initial 17 patients who underwent transvesical RARP using the single port robot platform, da Vinci SP (Intuitive Surgical, Sunnyvale, CA, USA).
Methods: From November 2020 to February 2021, done by a single surgeon, seventeen patients underwent SP radical prostatectomy through a transvesical approach.
Selection criteria were patients with intermediate National Comprehensive Cancer Network (NCCN) risk, pathology Gleason 6 with significant family history of prostate cancer or Gleason 4 + 3 with extensive previous abdominal surgeries.
Using a single 3 cm suprapubic midline incision, the bladder was incised, and the surgery was performed without the use of any additional ports.
Results: All cases were successfully completed without any conversion, intraoperative or postoperative complications. Median total operative time was 197 minutes and median estimated blood loss was 150 mL. Most of the patients (11/17) were discharged few hours after the surgery with a median postoperative hospital stay of 4.5 hours. Average pain score at discharge was 2.4 and none of the patients required opioids medications. Median Foley catheter stay was 5 days. Upon follow up, thirteen patients (76%) had immediate continence and all patients (100%) had complete urine control within 14 days after catheter removal, with a median of 2 days.
Conclusions: We demonstrated the feasibility of single‐port robotic transvesical radical prostatectomy using the novel SP robotic platform. In our initial experience, this approach allows for promising results such as single incision, no additional ports, minimal opioid use, same day discharge and immediate urine control.
Moderated Poster Session 24: Robotics/Laparoscopy II
Suprapubic robot‐assisted transumbilical two‐port laparoscopic adrenalectomy for huge pheochromocytoma and paraganglioma with report of 5 cases
Z Guoxi, G Xu, X Zou, Y Yuan, X Rihai, G Wu
Introduction & Objective: To summarize the experience of suprapubic robot‐assisted transumbilical two‐port laparoscopic adrenalectomy for huge pheochromocytoma and paraganglioma and to evaluate its safety and feasibility.
Methods: A retrospective analysis was performed on the clinical data of 5 patients who underwent suprapubic robot‐assisted transumbilical two‐port laparoscopic adrenalectomy for huge pheochromocytoma and paraganglioma. The five patients included 4 males and 1 females. The median age was 45.5years, and the median body mass index(BMI) was 23.4 kg/m2. The median systolic blood pressure was 142 mmHg, the median diastolic blood pressure was 106 mmHg, and the median heart rate was 98 bpm. There were 3 patients with hypertension, including 1 patient with cerebral infarction. The other 2 patients had no specific symptoms and the tumors were found during physical examination. There were 3 cases of tumor located in right adrenal region, one case located in left adrenal region and one case located in left renal hilum. The median diameter of the tumor was 6.5 cm. The median 24 h urinary dopamine was 896.4μg/24h, the median 24 h urinary noradrenaline was 450.7μg/24h, and the median 24 h urinary adrenaline was 66.5μg/24h, which were all increased. The index including operation time, blood loss and hospitalization time was recorded.
Results: All the 5 procedures were completed successfully. The median operative time was 115 min. The median estimated blood loss was 90 ml. All patients recovered well after surgery. Twenty‐four hours after the surgery, the median visual analogue scale(VAS) score of pain was 2. All patients resumed ambulation on 1 ∼ 2 days postoperatively. The drainages were removed on 2 ∼ 3 days postoperatively. The median postoperative hospital stay was 4 days. The pathological results included 3 cases of pheochromocytoma and 2 cases of paraganglioma. All patients were followed up postoperatively without tumor recurrence in a median follow‐up period of 5 months. The incision healed well. Umbilical scar was obscured due to umbilical folds, and suprapubic incision was not obvious due to pubic hair. The level of 24 h urinary catecholamine returned to normal. Among the 3 patients with hypertension, 2 patients recovered after surgery, and 1 patient still needed to be treated with antihypertensive drugs, but the dosage was reduced and blood pressure was well controlled.
Conclusions: Suprapubic robot‐assisted transumbilical two‐port laparoscopic adrenalectomy for huge pheochromocytoma and paraganglioma is safe and feasible with good cosmetic result, which is worthy of clinical application.
L Quanliang, Z Guoxi, X Zou, Y Yuan, X Rihai, G Wu
Introduction & Objective: To describe our experience with the robotic assistant transvaginal hybrid natural orifice transluminal endoscopic surgery nephrectomy (RA‐HTV‐NOTES‐N), and to evaluate its clinical value.
Methods: Retrospective analysis of the clinical data of 10 female patients who were underwent RA‐HTV‐NOTES‐N in our center. The median age 55years, median body mass index 21.9 kg/m2, and preoperative diagnosis are non‐functional kidneys. The lesions are located in 5 cases on the left and 5 cases on the right. 10 cases were performed by the same group of surgeons. General anesthesia, the patients were positioned in lithotomy with ipsilateral lumbar at 70° angle to the floor. The camera port was placed transvaginal via the posterior fornix, the robotic arm 1 and arm 2 were located on the upper and lower edges of the umbilical cord of the anterior midline respectively, and the assistant trocar was located at anterior midline of the pubic area or the scar of ligation. The ureter was identified above its cross over the iliac vessels and ligated using Hem‐o‐lock clips, after the hilum was identified, the Hem‐o‐lock applier was used to control the artery, and then the vein. The intact specimen was removed through an extended incision at the posterior vaginal fornix. The female sexual function and quality of life were assessed before and 3 months after the surgery by Female Sexual Function Index (FSFI) questionnaire and the MOS 36‐item Short‐Form Health Survey (SF‐36), respectively.
Results: RA‐HTV‐NOTES‐N was successfully completed in 10 patients. 1 case postoperative pathology indicated pyelocaliceal urothelial carcinoma, was performed laparoscopic ureterectomy and sleeve cystectomy in the second stage. The median operative time was 140 min and estimated blood loss was 320 ml. The median visual analogue score of 48 hours after operation was 2.5points. Postoperative complications occurred in 3 cases (2 Clavien‐Dindo grade 1, 1 Clavien‐Dindo grade2), no severe complications and no death case. The median follow‐up of 8 (range 6 to 12) months showed that umbilicus scar was hidden. The incision in the vagina healed well. No infection in the abdominal or pelvic cavity or celiocele occurred. The umbilicus scar is not obvious after surgery, 3 months after surgery, the median PSAQ score was 39 (31 ∼ 58), the median FSFI score was 29.1VS preoperative 28.54 (P > 0.05), and the quality of life index was significantly higher.
Conclusions: The early clinical experience shows that RA‐HTV‐NOTES‐N is feasible, safe and effective with good cosmetic outcome. It is worth applying in clinical practice, but requires multi‐center large sample size and long‐term follow‐up to evaluate its clinical application value in further.
Clipless and Athermal Pedicle Control with Selective Suturing Technique Proceeding with Neurovascular Bundle Preservation during Robot Assisted Radical Prostatectomy
MB Tuna, T Doganca, I Tufek, C Obek, AR Kural
Acibadem Maslak Hospital, Department of Urology
Introduction & Objective: During robot assisted radical prostatectomy, pedicle control can be accomplished by surgical clips and/or using different energy sources. Migration of surgical clips can cause bladder neck contracture and bladder stone formation. On the other hand; using different energy sources during pedicle division may cause thermal injury of the nerves which are critical for recovery of potency. In order to obviate this situation; we describe clipless and athermal pedicle control with selective suturing technique proceeding with neurovascular bundle preservation during robot assisted radical prostatectomy.
Methods: Robot assisted radical prostatectomy (RARP) is performed via transperitoneal route in antegrade fashion. After bladder neck incision, prostatic pedicle is divided. First right prostatic pedicle is selectively freed and cut. Bleeding is controlled by a running V‐Loc suture. Then neurovascular bundle is gently separated from the prostatic capsule starting at the basis and proceeding towards the apex. The same procedure is performed for the left prostatic pedicle. Following prostatectomy superficial bleeders are meticulously controlled by separate 5‐0 polyfilament sutures.
Results: Between March 2018 and May 2019 this technique was performed in 29 patients. Bilateral nerve sparing procedure was carried out in all cases. Mean preoperative PSA was 8.1 ± 2.1 ng/ml, mean patient age was 60.8 ± 6.5 and mean follow‐up was 13.6 ± 9.9 months. Mean console time, intraoperative blood loss and prostatectomy specimen weight were 201 ± 45 min, 237 ± 97 ml. and 59 ± 29 gr., respectively. Complications were assessed according to the Clavien‐Dindo classification. Clavien Grade 2, 3a and 3b complications were encountered in 1, 2 and 1 patients, respectively. Surgical margins were positive in 5 patients (17.2%). At post‐operative first month 28 of 29 patients were continent. Potency rate was 66% with PDE5 inhibitors.
Conclusions: Clipless control of pedicles during RARP(Robot assisted radical prostatectomy) seems to be feasible without compromising intraoperative blood loss.
A 10 year experience with retroperitoneal robotic‐assisted laparoscopic pyeloplasty
D Whiting, L Whitehurst, D Tsang, M Hussain, NJ Barber, M Malki
Frimley Park Hospital
Introduction & Objective: Robotic‐assisted laparoscopic pyeloplasty (RALP) can be performed using either a transperitoneal or retroperitoneal approach. The retroperitoneal approach is rarely reported on in the literature. Although it requires the surgeon to work in a smaller space, unlike the transperitoneal approach mobilisation of the colon is not required and it allows quick access to the PUJ. We report our 10 year experience of retroperitoneal‐RALP (R‐RALP).
Methods: A prospective database of 160 patients undergoing RALP between February 2010 and November 2019 in a single institution was analysed. The retroperitoneal approach was preferentially used with the transperitoneal approach only performed in cases where the renal pelvis was not particularly dilated. The procedures were performed by 3 consultant urologists and 5 supervised trainees. Data was recorded on demographics, operative details, complications and success rate. Success was determined as symptomatic improvement and/or an unobstructed renogram.
Results: Mean age was 45.3 ± 17.4 years. 74 (46.3%) patients were male. 152 cases (95.0%) were performed using a retroperitoneal approach and 8 (5.0%) transperitoneal. Mean operating time was 139.4 ± 45.6 minutes. 100 (62.5%) patients were found to have a crossing or accessory vessel(s). Mean estimated blood loss was 10.0 ± 26.8ml. A surgical drain was placed in 57 (71.3%) of the first 80 cases and 15 (18.8%) of the second 80 cases. Median drain duration was 1 day (range 1‐5). Median hospital stay was 1 night (range 1‐27). One (0.6%) case was converted to open pyeloplasty due to dense inflammatory tissue and one (0.6%) to robotic‐assisted nephrectomy due to severe adhesions around the PUJ. There were no blood transfusions. There were 6 major ( >grade 2 Clavien‐Dindo) post‐operative complications in 4 patients (2.5%). Two (1.3%) grade 3a complications: urine leak and pain after stent removal requiring nephrostomy. Three (1.9%) grade 3b complications: migrated stent requiring ureteroscopy, perirenal haematoma requiring open evacuation and stent re‐insertion. One (0.6%) grade 4 complication requiring ventilatory support on intensive care. 18 patients received follow‐up at an alternative hospital, 5 patients are awaiting follow‐up and 12 were lost to follow‐up. Of the remaining cases median length of follow‐up was 12 months (range 3‐36) and 92.7% (n = 115) were successful.
Conclusions: R‐RALP is a safe and effective treatment for PUJ obstruction allowing predictably rapid discharge from hospital without the need for a routine surgical drain.
Application of holographic image and navigation in robotic assisted laparoscopic radical prostatectomy
g Zhu
Beijing United Family Hospital and Clinics, Urology Beijing, People's Republic of China
Introduction & Objective: To evaluate the clinical value of the holographic image and navigation in robotic assisted laparoscopic radical prostatectomy (RARP) .
Methods: From Sept. 2020 to Dec. 2020, 5 patients diagnosed with prostate cancer in Beijing United Family Hospital were involved in this study. The mean age was 57 years(38~69 years). Before the operation, the engineers established the holographic image based on the enhanced MRI images. The holographic images were used in pre‐surgery planning. During the operation, the navigation was achieved by real time fusing holographic images with the robotic surgery endoscopic views. Some important structure such as prostate, bladder neck and the tumor could be observed and monitored in real time. The No.1 patient has high‐risk prostate cancer, underwent RARP+ extended pelvic lymph node dissection; The No.2 patient has low‐risk prostate cancer, underwent RARP, and the right side neurovascular bundle (NVB) was preserved; The No.3 patient has low‐risk prostate cancer, underwent RARP, and the bilateral side NVB was preserved; The No.4 patient has low‐risk prostate cancer, underwent RARP, and the right side NVB was preserved; The No.5 patient has high‐risk prostate cancer, underwent RARP+ extended pelvic lymph node dissection, and the bilateral side NVB was preserved.
Results: All the 5 cases surgeries were uneventful, no case was converted to open surgery, the mean operation time was 161.7min (160~250min), the mean blood loss was 426.7 ml(60~1000 ml). The pathological results were pT3bN0S1 cM0, pT2aN0S0 cM0, pT2aN0S0 cM0, pT2aN0S0 cM0 and pT3aN1S1 cM0, respectively. There was no over Clavien Dindo Ⅱ perioperative complications. The urinary continence rate at 2‐week post‐operation when catheter removal was 75%. The PSA level and erectile function will be monitored in the follow‐ up.
Conclusions: Holographic image navigation is with great clinical value in RARP, in particularly the tumor control, NVB preservation, urinary continence recovery, and reduction of surgery related complication.
Robotic Non Transecting Secondary Pyeloplasty Techniques for Recurrent Ureteropelvic Junction Obstruction
M Lee, Z Lee, AM Asghar, RA Lee, D Strauss, MD Stifelman, LC Zhao, DD Eun, N Krishnan
Lewis Katz School of Medicine at Temple University
Introduction & Objective: Management of patients with recurrent ureteropelvic junction obstruction (UPJO) after prior failed pyeloplasty is challenging. We described outcomes of three robotic non transecting pyeloplasty techniques that may be utilized for surgical management of patients in this setting.
Methods: We retrospectively reviewed our Collaborative of Reconstructive Robotic Ureteral Surgery (CORRUS) database for all consecutive patients between 04/2012—09/2019 who underwent a secondary pyeloplasty for management of a recurrent UPJO after prior failed pyeloplasty. The techniques used for secondary pyeloplasty included transecting (dismembered) and non transecting pyeloplasty (YV plasty, buccal mucosa graft ureteroplasty onlay or Heineke‐Mikulicz). Postoperatively, patients were assessed for surgical success which we defined as the absence of flank pain and obstruction on imaging. Perioperative variables between transecting and non transecting pyeloplasty were compared using nonparametric independent sample median tests and chi‐square tests; p < 0.05 was considered statistically significant.
Results: Overall, 28 patients met inclusion criteria (Table 1). There was no difference in median operative time (p = 0.26) and estimated blood loss (p > 0.99) between both groups. Near infrared fluorescence with indocyanine green was utilized more frequently in the non transecting group (85.7% versus 50.0%, p = 0.04). The non transecting group had a longer median stricture length (2.8 versus 1.1 centimeters, p = 0.04). There was no difference in surgical success rates between both groups (85.7% versus 85.7%, p > 0.99).
Conclusions: Non transecting pyeloplasty techniques including YV plasty, buccal mucosa graft ureteroplasty onlay and Heineke‐Mikulicz pyeloplasty may be safely and effectively utilized in patients with recurrent UPJO after prior failed pyeloplasty. Non transecting pyeloplasty techniques may preserve the fragile ureteral blood supply and help avoid ureteral devascularization in this setting.
Outcomes of Robotic Simple Prostatectomy After Prior Prostate Surgery
M Lee, CU Okoro, JY Lee, AM Asghar, D Strauss, Z Lee, DD Eun, N Krishnan
Lewis Katz School of Medicine at Temple University
Introduction & Objective: Surgical management of patients with enlarged prostates and lower urinary tract symptoms (LUTS) who failed prior prostate surgery may be challenging due to increased prostatic scarring and fibrosis. We compared outcomes of robotic simple prostatectomy (RASP) in patients with a history of prior prostate surgery versus patients without a history of prior prostate surgery.
Methods: We retrospectively reviewed outcomes of all consecutive patients who underwent RASP between 05/2013 and 01/2020. The indication for RASP included LUTS refractory to medical and/or surgical management, and a prostate volume ≥80 milliliters. Patients were grouped based on whether or not they underwent prior prostate surgery. Postoperatively, urinary function was assessed using the American Urological Association Symptom Score (AUASS) and Quality of Life (QOL) scores. Continuous and categorical variables were compared between both groups using independent t‐tests and chi‐square tests, respectively; p < 0.05 was considered significant.
Results: Overall, 177 patients met inclusion criteria (Table 1). Among the 26 (14.7%) patients who underwent prior prostate surgery, 20 (76.9%), 2 (7.7%), 1 (3.8%) and 3 (11.5%) patients underwent transurethral resection of the prostate, transurethral microwave therapy, water vapor thermal therapy or photoselective vaporization of the prostate, respectively. Mean prostate volume was significantly higher in the group that underwent prior prostate surgery (161.9 versus 150.0 milliliters, p = 0.02). There was no difference in mean estimated blood loss (p = 0.91), robotic console time (p = 0.46) or major 30‐day postoperative (Clavien >2) complications (p = 0.35) between both groups. With regards to urinary function, the mean improvement in AUASS (p = 0.79) and QOL scores (p = 0.98) were similar between both groups.
Conclusions: For management of patients with enlarged prostates and LUTS, RASP is associated with an improvement in urinary function outcomes and a low risk of postoperative complications. Perioperative outcomes of RASP are similar in patients who underwent prior prostate surgery versus those that did not undergo prior prostate surgery.
Time of ligation of dorsal venous complex during RALP: evaluation of oncological safety and peri‐operative outcomes in organ‐confined and locally advanced prostate cancer patients
L Sarchi, M Sighinolfi, E Morini, A Cassani, B Filippi, S Assumma, A Piro, M Ticonosco, R Ferrari, S Puliatti, G Bianchi, S Micali, BC Rocco
Azienda ospedaliero‐universitaria di Modena e Reggio Emilia, Modena, Italy
Introduction & Objective: Management of DVC during robotic radical prostatectomy (RALP) has been evaluated with regards to functional and oncologic outcomes. We aim to evaluate the impact of a prior (p‐DVC) vs delayed (d‐DVC) ligation of DVC on oncological and peri‐operative outcomes, focusing particularly on locally advanced diseases (≥pT3a)
Methods: We retrospectively assessed our prospectively collected database to search possible difference in positive surgical margin rate (PSM) between p‐DVC and d‐DVC. In 2018 146 RALP procedures for clinically organ confined or locally advanced PCa were performed. Mean age of patients was 63,6 yr. (DS 6,4), mean BMI 24,2 (DS 10,2), mean prostate volume was 47,7ml (DS 21, 8), mean PSA value was 9 ng/ml (DS 4,5). RALP were performed by 3 surgeons who already completed their LC process. 41 patients (28%) had a p‐DVC ligation whereas the remaining 105 (72%) had a d‐DVC one, according to surgeon's preference. In p‐DVC arm a single stitch was given prior to the beginning of apical dissection, before its resection; in d‐DVC arm the plexus was resected after apex dissection and then sutured. Primary endpoint was difference in PSM; estimated blood loss (EBL) was considered as a secondary endpoint with other peri‐operative outcomes (operative time, complication rate). Data were analyzed by means of SPSS‐12; parametric and non‐parametric tests to assess for differences were used (chi square, fisher exact test).
Results: Overall, a pT2 was found in 55,5% (81) and a ≥ pT3 in 44,5% patients (62); PSM rate was 11,1% (9) in pT2 and 50% (31) in pT3 cases. Baseline and tumor characteristics were overlapping between groups. A trend toward a lower rate of PSM in p‐DVC arm (19,5%, 8/41) compared to d‐DVC arm (32%, 34/105) was evident but did not reach statistical significance (p = 0.236). The time of ligation did not affect PSM rate at the apex (p = 0,13). When considering separately pT3 diseases, we failed to find a statistically significant difference between the approaches with regard to PSM rate (p = 0,125). EBL was significantly lower in p‐DVC (145 mL, DS 84) compared to d‐DVC (216 mL, DS 144), p = 0,02. Operative time and complication rates were similar.
Conclusions: Prior and delayed ligation of the DVC related to apical dissection are substantially safe and lead to similar post‐operative outcomes; this occurrence is seemingly applying also to locally advanced disease. Lower blood loss amount was reported in the p‐DVC group.
Utility of an Ultra Mini Doppler Ultrasound Probe Platform for Real‐Time Mapping for Nerve Spare during Robot Assisted Radical Prostatectomy
M Yao, D Mitchell, SS Kommu, BA Eddy
East Kent Urology Department, Kent and Canterbury Hospital, East Kent Hospitals University NHS Foundation Trust
Introduction & Objective: Nerve sparing during Robot Assisted Radical Prostatectomy (RARP) is a key step in aiding achievement of optimal outcomes for continence and erectile function in selected patients. The technique is often performed based on the surgeon's subjective perception of locale of the neurovascular bundle. Herein, we report our initial experience with a ultra mini transducer to permit real‐time doppler ultrasound aided nerve sparing during da Vinci™ RARP. We previously presented our experience using a larger probe [WCE 2017]. We found, at the time, that the probe was bulky and hampered the technique of real‐time ultrasound mapping.
Methods: An Ultra Mini Transducer (Hitachi Aloka Medical, Ltd., Japan) was deployed via a 10ml port following initial dissection of the anterior prostate and ligation of the dorsal vein complex. The transducer head was gripped with the robotic Prograsp™ instrument via a purpose built clip such that scanning ensued without obscuring views from the optics. The flat face of the linear transducer was manipulated with its flexible platform to permit real‐time visualization of the neurovascular bundles. Blood flow mapping using eFLOW mode offered fine spatial resolution and increased sensitivity. The transducer also permitted Real‐time Tissue Elastography (RTE) providing information on tissue stiffness during the surgical procedure. The neurovascular bundle was dissected with the aid of real‐time imaging sent via TilePro.
Results: 5 cases were successfully and safely completed with no discernible increase in the standard operative time. Follow‐up revealed preservation of erectile function upon review with no complications.
Conclusions: Real‐time doppler ultrasound aided nerve sparing with tandem use of an ultra mini transducer, aids in the optimal identification of the neurovascular bundles during RARP. Large scale multi‐centred studies with this and similar concept platforms could improve the precision with which nerve spare is conducted at the time of RARP.
Does Type of Robotic Platform Make a Difference in the Final Cost of Robotic‐Assisted Radical Prostatectomy?
M Covas Moschovas, TA Helman, S Bhat, T Rogers, M Sandri, S Reddy, J Noël, V Patel
Global Robotics Institute
Introduction & Objective: Continued advancement in robotic technology with the new da Vinci® Single Port (SP) platform has promising implications for urologic surgery. There have been descriptions of multiple urologic procedures performed with this console since its FDA approval in November 2018. Every new technology has its inherent challenges in terms of costs, and in the current global economic crisis, new equipment needs to be evaluated for economic feasibility. This study evaluates the difference of robot‐assisted radical prostatectomy (RARP) costs in patients with similar preoperative characteristics operated on using the da Vinci® SP and Xi robotic platforms.
Methods: We performed a retrospective analysis on 71 consecutive patients with prostate cancer who underwent RARP with the SP robot between June 2019 and April 2020. Propensity score (PS) matching was performed to compare patients with similar preoperative characteristics reducing bias and potential confounders. After PS matching, 71 patients were selected from a cohort of 875 who underwent RARP with the Xi robot in the same period with a single surgeon using the same surgical technique. We divided the total expense per surgery into the cost of disposable materials, robotic instruments (initial purchasing cost divided by the number of “lives”), and operative room costs. Only variable costs are included in this study, as fixed costs do not vary between procedures and are the same for both cohorts. Fixed costs include anesthesia, pathology, surgeon, and hospitalization fees.
Results: The median total cost for SP RARP was $5,586 ($5,360 ‐ $5,982) USD and $4,875 ($4,661 ‐ $5,093) USD with the XI for a median cost difference of $707 ($584 ‐ $832) (P < 0.001). The median cost of disposables for the SP was $1,877 ($1,588 ‐ $2,193) USD and for the Xi $1,527 ($1,407 ‐ $1,781) USD, P < 0.001. Non‐disposable instruments cost per case (fixed cost) was $1,610 and $1,270 USD for the SP and Xi, respectively.
Conclusions: The cost of radical prostatectomy in the SP cohort is higher than the Xi cohort. The greater price was primarily due to the increased cost of instruments and disposable materials. However, we believe that it is possible to minimize the SP surgery price with operative time reduction and increased outpatient procedures with early discharge protocols. In our experience, the lack of GelPOINT and space maker are also crucial factors to decrease the SP total cost.
Primary Results of in‐vivo Needle‐Based Confocal Laser Endomicroscopy in Human Prostate: A Safety and Feasibility Study
LA van Riel, A Swaan, CK Mannaerts, D Savci‐Heijink, TG van Leeuwen, TM de Reijke, M de Bruin, J Freund
Department of Urology, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, the Netherlands
Introduction & Objective: Contemporary prostate imaging and biopsy techniques used for prostate cancer detection can be improved by introducing optical imaging techniques, such as confocal laser endomicroscopy (CLE). CLE allows in vivo, high‐resolution, real‐time visualization and analysis of prostate tissue. This study aims to demonstrate the safety and feasibility of clinical in‐vivo needle‐based forward‐looking CLE (nCLE) imaging of the prostate.
Methods: For this feasibility study, two patients with a suspicion of prostate cancer underwent transperineal nCLE during ultrasound guided transperineal template mapping biopsies. After intravenous administration of fluorescein, nCLE imaging was performed with a forward‐looking probe (outer diameter 0.9mm) in two trajectories during a manual push‐forward and pull‐back motion. A biopsy was taken in a co‐registered parallel adjacent trajectory to the CLE trajectory for histopathologic comparison. Peri‐ and postprocedural adverse events, CLE device malfunction and procedural failures were recorded. nCLE image quality assessment and image interpretation were performed by an experienced CLE rater, blinded to any additional information.
Results: In both patients, no peri‐ and post‐procedural adverse events were reported following nCLE. No CLE device malfunction nor procedural failures were reported. Within 1.5 minutes after intravenous administration of fluorescein, nCLE image quality was sufficient for interpretation for at least 14 minutes, yielding more than 5000 CLE frames per patient. The pull‐back CLE recordings and most of the push‐forward recordings only visualized erythrocytes, being classified as non‐representative. During the push‐forward recordings, prostate tissue was scarcely visualized in single frames, insufficient for histopathologic correlation. Prostate carcinoma was identified by biopsy in one patient (Gleason score 4 + 3 = 7, >50%), while the biopsy from the other patient showed no malignancy.
Conclusions: nCLE imaging of in‐vivo prostate tissue with a forward‐looking CLE probe is safe without device malfunctions or procedural failures. nCLE is technically feasible, but the acquired CLE datasets are non‐representative. The non‐representative nature of the CLE images is possibly caused by bleeding artefacts, movement artefacts and a lack of contact time with the tissue of interest. A sideward‐looking CLE probe with an automated rotary pullback system might overcome these problems.
Preliminary results of in vivo focal transperineal laser ablation treatment of the prostate: correlation of mpMRI and CEUS imaging to histology in radical prostatectomy specimen
LA van Riel, R van kollenburg, TM de reijke, D Savci‐Heijink, MR Engelbrecht, HP Beerlage, TG van Leeuwen, M de Bruin, JR Oddens
Department of Urology, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, the Netherlands
Introduction & Objective: As an alternative for standard radical therapy of localized prostate cancer (PCa) focal ablative techniques are an option. Soractelite™ transperineal laser ablation (TPLA) using the Echolaser device, with four independent laser sources, is such a novel minimal invasive treatment. In order to evaluate the histological ablative efficacy in correlation with CEUS and mpMRI we conducted a study in patients planned for radical prostatectomy (RP). We correlated the ablation zone on RP specimens to CEUS imaging and MRI following TPLA. Moreover, safety and feasibility of TPLA using a (multi)fiber setup in men with localized PCa will be studied.
Methods: This is a prospective, multicenter and interventional phase I/II pilot study using Soractelite™ with an ablate‐and‐resect design that aims to include 15 patients, which has been approved by the Ethical Committee. In 3 patients TPLA procedures, using a single fiber delivering 1800J at 3W, were performed under continuous ultrasound guidance approximately 4 weeks before RP. Imaging (grayscale US, CEUS and mpMRI) was performed prior to TPLA and RP. The RP specimen was divided into whole‐mount H&E‐stained slides and these were digitized. The ablation zone was delineated on imaging and histology, and segmented into 3D models.
Results: Three office‐based TPLA procedures were successfully performed under ultrasound guidance using local anesthesia. Patients were discharged the same day. Qualitative analysis shows a clear delineation of the ablation zone on T2‐weighted, DCE and CEUS imaging. The 3D shape of the ablation zone on CEUS and MRI seems to be ellipsoid and this closely matches the shape of the delineated area of avital tissue on histopathology. Quantitative data, regarding 3D segmentation of T2‐weighted, DCE, CEUS and histopathology, is currently being analyzed to be presented.
Conclusions: These preliminary results show that TPLA is a feasible office‐based minimal invasive focal treatment of PCa and it can be performed safely under local anesthesia. Enrollment is still ongoing investigating multiple laser fiber configurations. The ablation zone is clearly visible on CEUS imaging and on MRI T2‐weighted and DCE imaging. The 3D reconstruction closely matches the ablation zone seen on histopathology.
Effect of intraoperative use of electrosurgery on urinary incontinence after robot‐assisted radical prostatectomy
A Sawada, A Hamada, T Inoue, O Ogawa
Department of Urology, Kyoto University Graduate school of Medicine
Introduction & Objective: One of the serious complications after robot‐assisted radical prostatectomy (RARP) is urinary incontinence. Recently, athermal RARP, which uses minimal electrosurgery (ES) devices, is reported to have a positive effect on early recovery from urinary continence. However, which component of RARP should be avoided using ES and how much to use remain unclear. To address these research gaps, the study aims to examine how ES generates heat and causes thermal denaturation in the tissues and the relationship between using ES and recovery from postoperative urinary continence.
Methods: 1) A piece of raw bovine liver was prepared, and an electrosurgical knife was used. Thermography was utilized to observe heat spread, and the degree of thermal denaturation was evaluated macroscopically and microscopically. 2) 64 RARP cases performed at our facility between January 2017 and March 2018 were divided into two groups, namely, individuals who recovered from urinary continence within one month and those after more than three months. Operative video clips were examined in detail to determine whether differences exist in the use of ES during RARP.
Results: 1) Tissue temperature was highest (120.0°C), and thermal denaturation (TD) was most widespread (5.0 × 4.3 mm) in the 1‐second coagulation mode, whereas TD was minimal (3.6 × 1.2 mm) in the 1‐second cut mode. In the bipolar application for 1 second, the temperature of the tissue was lowest (89.0°C), whereas TD was wider than that in the cut mode (4.9 × 4.1 mm). And a short duration per application resulted in less thermal damage. TD was 3.7 × 3.3 mm and 6.5 × 5.7 mm for the 0.3 and 3‐second coagulation mode, respectively. 2) The duration of monopolar application around the bladder neck and seminal vesicle was significantly short in early continence recovery group. Conversely, no significant differences were noted between the two groups regarding the use of monopolar and bipolar modes use around the endopelvic fascia, neurovascular bundle (NVB), and prostatic apex.
Conclusions: The results of the study suggest that using electrosurgery around the bladder neck and seminal vesicles mainly affected urinary continence. In addition, when the duration of one application of electrosurgery is shortened to 0.3 s or less, the recovery of urinary continence may not be adversely affected.
Robot‐Assisted Radical Cystectomy : Results from a Korean Multicenter Study
T No, J Tae, Y Choi, J Shim, S Kang, S Kim
Introduction & Objective: To evaluate the perioperative and oncological outcomes of robot‐assisted radical cystectomy(RARC) in Korea
Methods: From April 2007 to May 2019, a total of 730 bladder cancer patients were treated with RARC in 11 tertiary referral hospitals located in Korea. Demographics, perioperative outcomes and oncological outcomes were evaluated.
Results: Among the 730 RARC cases, 504(74.0%) were extracorporeal urinary diversions while 177(26.0%) were totally intracorporeal urinary diversions. 275(37.7%), 391(53.6%) and 26(3.6%) patients each received an ileal conduit, orthotopic neobladder and ureterocutaneostomy, respectively. The positive surgical margin rate was 3.0%. The mean lymph node yield for the standard and extended pelvic lymph node dissection (PLND) was 16.9 and 21.3, respectively. The mean estimated blood loss and intraoperative blood transfusion rate were 516mL and 15.5%, respectively. Readmission rate was 38.4% with gastrointestinal(15.1%) and infection(14.5%) complications being the most common type. The 5‐year overall survival and 3‐year recurrence‐free survival rates were 79.4% and 65.2%, respectively.
Conclusions: Results of RARC in Korea show comparable perioperative and oncological outcomes to current literature and also to historical open radical cystectomy data. Large prospective data is required to draw any definitive conclusions.
Withdrawn
Evaluation of robotic versus open approaches for Unilateral ureteral reimplantation in pediatric patients
AA Elbakry, K Aldabek, O AL‐Omar
Pediatric Urology, Department of Urology, West Virginia Uninversity Hospital
Introduction & Objective: We are aiming to evaluate if robotic ureteral reimplantation is a feasible and safe alternative to the conventional open approach in unilateral vesicoureteral reflux in pediatric population.
Methods: We retrospectively identified all pediatric patients who underwent robotic unilateral ureteral reimplantation, and a similar non‐concurrnet cohort of patients who underwent open ureteral reimplantion was also identified. A total of 33 patients met the inclusion criteria and were included in the analysis. Patients were divided into two groups: group 1 (robotic approach) and group 2 (open approach). Patients' demographics, perioperative data, and outcomes were collected and reviewed. Univariable analysis was done using independent sample t test and Mann‐Whitney U test for continuous data and Fisher Exact test for categorical data.
Results: A total of 17 patient underwent robotic approach and 16 patients underwent open approach. There was no difference between the two groups regarding demographic data (age and gender). There was no difference in the laterality, incidence of duplicated system or reflux grade. Group 1 had statistically higher percentage of constipation (94.2% vs 56% in group 2) and dysfunctional voiding (82% vs 37% in group 2) (P = 0.01). Both groups were similar regarding operative time and total length of detrusor tunnel. All patients in both groups were discharged after 24‐48 hours. No reported early postoperative complications in both groups. One patient in group 2 required readmission within 30 days for urinary tract infection. A total of 13 patients in group 1 underwent follow‐up voiding cystourethrogram (VCUG) that showed success rate of 100% with new development of contralateral Grade 1 VUR in 2 patients. In group 2, only 2 patients underwent follow‐up VCUG for febrile UTI and it showed newly developed contralateral VUR.
Conclusions: Our results suggests that robotic approach for ureteral reimplantation as a management for vesicoureteral reflux in pediatric population is a safe and feasible alternative to open approach. Future studies with larger number are warranted.
Intermediate Length Follow‐up of Single Port Laparoscopic Renal Cryoablation
HE Moreland, TC Peak, LJ Smith, MB Rothberg, JW Pike, LT O'Connor, DB Rukstalis
University of South Carolina School of Medicine
Introduction & Objective: Renal cryoablation has become established as a safe and efficacious therapy for small renal lesions when performed laparoscopically and percutaneously. The laparoscopic approach is associated with improved efficacy relative to percutaneous ablation but with higher risk of surgical toxicity. We have developed a minimally invasive retroperitoneal technique with a single port gel device that reduces toxicity while maintaining oncologic efficacy. We report the intermediate length follow‐up of a continuous, prospective database.
Methods: 54 patients were placed into standard lateral decubitus position with a 2‐3 cm incision made beneath the 12th rib. The retroperitoneal space was developed with balloon dissection and a GelPOINT Mini (Applied Medical) inserted. A percutaneous biopsy was performed under US guidance prior to placement of cryoprobes into the mass. All procedures were performed as outpatient under IV anesthesia without narcotics. Patient demographics, tumor characteristics, oncologic follow‐up, and disease‐free (DFS), disease‐specific (DSS), and overall survival (OS) data were evaluated.
Results: A total of 54 patients, with a median follow‐up of 23 months (range, 1–45), were identified. Median tumor size was 3.4 cm (1.5–7.2), ASA score was 3, CCI was 5 (2‐9), RENAL score was 7 (4–10), and 61% carcinoma on biopsy. 35 (64.8%) patients had posteriorly located masses. Four (8.5%) patients had a solitary kidney. An average of 2.6 cryoprobes were used. Two cases were performed as salvage following previous partial nephrectomy (PN). There were three perioperative adverse events (Clavien 1‐2) without evidence of acute renal or bowel injury. There were four instances of disease recurrence, occurring at 18, 18, 30, and 34 months. At the median follow‐up of 23 months, OS was 96.3%, DSS was 100%, and DFS was 96.3%. There were three deaths during a follow‐up period of 36 months, one from renal cell carcinoma at 34 months. At 36 months, OS was 90.9%, DSS was 90.9%, and DFS was 90%.
Conclusions: A single port retroperitoneal dissection for renal ablation is safe and effective as initial therapy for small masses of any location. The procedure can be performed as salvage following a prior PN or ablation and is feasible in masses located anteriorly or posteriorly. This approach is associated with minimal surgical toxicity, without measurable renal dysfunction. The OS and DSS at 23 months are highly favorable relative to established ablative approaches. This retroperitoneal approach should be considered for all patients undergoing excision of a small renal mass.
The Application of Suprapubic Robotic‐assisted Transumbilical Two‐port Laparoscopy in Urology
X Zou, X Tianpeng, Z Guoxi, L Quanliang, Y Yuan, X Rihai
Introduction & Objective: To evaluate the value of suprapubic robotic‐assisted trans umbilical two‐port laparoscopy (SRA‐TTL) in urology.
Methods: 25 patients underwent SRA‐TTL including 14 males and 11 females. The age ranged from 13 to 75, with an average age of 48.4. The body mass index (BMI) ranged from 17.9 to 31.1 kg/m2 with an average of 22.3 kg/m2. There were 11 cases of left side and 14 cases of right side, including 4 cases of adrenal tumor, 9 cases of renal carcinoma, 2 cases of renal hamartoma, 1 case of renal pelvis carcinoma, 8 cases of non‐functional kidney, and 1 case of ureteropelvic junction stenosis. All cases were performed with Da Vinci (XI) Surgical Robot. Under general anesthesia, the patients were placed in the lateral position with the affected side elevated by 70°. Two 8‐mm trocars were inserted at the medial margins of umbilicus and placed bipolar separating forceps and electric scissors respectively. An 8‐mm trocar was inserted in the suprapubic pubes covering area of affected side and placed laparoscope. A 12‐mm auxiliary trocar was inserted above the pubic symphysis and another 12‐mm auxiliary trocar was inserted in the epigastrium of affected side if necessary. The surgical procedures were performed according to the method of standard laparoscopic surgeries. The specimens were placed inside a homemade bag and removed outside by extending the suprapubic incision.
Results: All the 25 cases were successfully completed, including 4 cases of adrenal tumor resection, 8 cases of radical nephrectomy, 8 cases of partial nephrectomy, 3 cases of simple nephrectomy, 8 cases of upper urinary tract resection and 1 case of renal pelvis dissociation molding. The mean operative time was 159min. The mean estimated blood loss was 415ml. Three patients received blood transfusion. No case transferred to open surgery. One patient was injured in the great vessels during the operation and the vessels were repaired under laparoscopy with blood transfusion. The Visual pain score (VAS) 48 hours after surgery was 1 ∼ 4 points, and the postoperative hospital stay was 3 ∼ 19d. There was no major postoperative complication occurred. All the 25 patients were followed up for 1 to 11 months, with an average follow‐up of 7.0 months. No tumor recurrence or metastasis occurred in the tumor patients. The umbilical scar was basically invisible and the suprapubic scar was concealed due to pubic hair covering and skin wrinkles. No incisional hernia is formed.
Conclusions: Suprapubic robotic‐assisted transumbilical two‐port laparoscopic surgery fully combines the advantages of Da Vinci's surgical robot system and suprapubic single‐port laparoscopic technology, which is safe, feasible and worthy of clinical selection.
Suprapubic‐assisted transumbilical laparoendoscopic single‐site surgery for treatment of middle and upper ureteral stricture
L Li, G Wu, Z Zhong, X Hui, X Zou, Z Guoxi
Introduction & Objective: To investigate the application value of suprapubic‐assisted transumbilical laparoendoscopic single‐site (SA‐LESS) surgery in the treatment of middle and upper ureteral stricture.
Methods: From June 2016 to January 2020, 34 patients with middle and upper ureteral stricture underwent laparoscopic surgery in our hospital. Among them, 16 patients underwent SA‐LESS for ureteral stricture resection and anastomosis (Group A), and 18 patients underwent standard three‐port laparoscopy surgery(Group B). Another 14 patients (Group C) who underwent open ureteral stricture resection and anastomosis in our hospital from January 2015 to January 2017 were selected as control group. The clinical data of all patients were collected, including the causes of ureteral stricture, length of stricture, renal function, operative time, intraoperative blood loss, postoperative hospital stay, postoperative cosmetic effect, postoperative urinary leakage, restenosis and other complications.
Results: All the patients in group A and group B were successfully operated without additional working channels and no transfer to open surgery. All the 14 patients in group C were successfully operated. The operative time of the three groups was (113.23 ± 16.42)min, (108.54 ± 18.18)min and (115.9 ± 15.4)min, respectively, and there was no statistically significant difference(P = 0.073). The intraoperative blood loss in the three groups was (101.46 ± 11.01)ml, (99.85 ± 10.93)ml and (150.5 ± 20.4)ml, respectively. The blood loss in group A and group B was less than that in group C(P < 0.05). The postoperative 24h VAS scores of the three groups were 2.4 (1‐4), 2.8 (1‐4) and 3.8 (2‐5), respectively. The pain scores of group A and group B were lower than those of group C. The Patient Scar Evaluation Questionnaire (PSAQ) scores of the three groups were 31.08 ± 2.06, 33.63 ± 2.52 and 38.69 ± 2.59, respectively. The cosmetic scores of group A and group B were better than those of group C. There were no statistical differences in postoperative hospital stay, postoperative urinary leakage and restenosis among the three groups.
Conclusions: Suprapubic‐assisted transumbilical laparoendoscopic single‐site ureteral stricture resection and anastomosis is safe and feasible for the treatment of middle and upper ureteral stricture. It has the advantages of mild postoperative pain and good cosmetic effect, which is worthy of clinical application.
Single‐Port Transvesical versus Multiport Robotic Simple Prostatectomy: A Comparison of Perioperative Outcomes
M Abou Zeinab, A Beksac, J Ulchaker, J Kaouk
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
Introduction & Objective: Single‐port transvesical robotic simple prostatectomy (SP‐TVSP) is an alternative approach for multiport transperitoneal technique (MP‐TPSP) in treatment of large volume prostatic hyperplasia. We sought to compare the perioperative and postoperative outcomes between SP‐TVSP and MP‐TPSP.
Single‐port transvesical robotic simple prostatectomy (SP‐TVSP) is an alternative approach for multiport transperitoneal technique (MP‐TPSP) in treatment of large volume prostatic hyperplasia. We sought to compare the perioperative and postoperative outcomes between SP‐TVSP and MP‐TPSP.
Methods: From a single institution, data of 25 patients who underwent SP‐TVSP and 21 patients who underwent MP‐TPSP were retrospectively collected. All surgeries were performed by a single surgeon. SP‐TVSP was performed through a small suprapubic incision using the single port robot platform, da Vinci SP (Intuitive Surgical, Sunnyvale, CA, USA). MP‐TPSP was performed through the standard W configuration incisions using the da Vinci Si or Xi.
Results: There was no significant differences in demographic data. Median (IQR) preoperative prostatic volume was 181 vs 169 cc for SP‐TVSP and MP‐TPSP respectively (p = 0.67). The majority of the patients (85%) presented with acute urinary retention or bothersome symptoms nonresponsive to medical management necessitating surgery. No difference detected in median estimated blood loss (150 cc for both approaches, p = 0.276). All patients in multiport group had a Jackson‐Pratt (JP) drain inserted at the end of the procedure while none had a JP drain in the single‐port group (p < 0.001). Median (IQR) hospital stay was 0 days (0, 1) compared to 1 day (0,2) in SP‐TVSP and MP‐TPSP groups respectively (p = 0.019). Pain score at discharge was less in the SP‐TVSP arm (p = 0.045), and patients required less opioids after discharge (36% SP‐TVSP vs 100% MP‐TPSP, p < 0.001). Complications rate, postoperative postvoid residue, international prostate symptom score (IPSS) and continence rate were comparable between the two groups.
Conclusions: The SP‐TVSP approach, with direct bladder access, avoiding the intraabdominal cavity and avoiding the bivalving of the bladder resulted in a less invasive alternative to the multiport approach with equal effective outcomes.
Automated machine learning segmentation and measurement of urinary stones on CT scan
K Lembrikova, R Babajide, JB Ziemba, Y Fan, GE Tasian
Introduction & Objective: Treatment decisions for patients presenting with urinary stones depend on multiple factors including stone size, location, and renal anatomy. Current methods depend on manual measurement of these parameters by humans, which introduces inter‐ and intra‐observer variation, is laborious, and time‐consuming. The objective of this study is to evaluate the performance of a machine learning algorithm to quickly and accurately automate measurement of stone features and renal anatomy.
Methods: A sample of 95 CT scans from patients who underwent assessment and imaging for suspected kidney stones were included in the study. Two raters manually measured kidney stones in 3 orthogonal dimensions, renal pelvis width, and ureter diameter from 46 scans. A two‐way random intraclass correlation (ICC) score was calculated to quantify intrarater agreement. The remaining 49 scans were used to train a deep learning model to segment kidney stones from the surrounding kidney. Times for manual and machine calculations were recorded.
Results: The sample included 19 scans with kidney stones, 17 with ureteral stones, and 10 with both. Median time to measure stones in 3 dimensions was longer manually than with the machine algorithm (16.1 vs. 2.1 seconds). Intrarater reliability was poor for pelvis width (0.44, 95% CI 0.21 – 0.62) and ureter diameter (0.40, 95% CI 0.16 – 0.59), and good for stone size (0.79, 95% CI 0.75 – 0.83). The algorithm identified all stones present (100% sensitivity) with no false positive stones (100% sensitivity). Analyzing at the individual voxel level, the sensitivity of the algorithm for stone detection fell to 58%, while the specificity remained at 100%, using manual measurements as ground truth. Although the algorithm reliably captured the centers of stones, the total area of kidney stones identified by the machine was smaller than that identified by human raters (1,019.4 vs. 1,256.3 mm3).
Conclusions: Manual measurements of kidney stones and anatomy on CT are limited by the time required and poor reproducibility. The more rapid and accurate measurements provided by the machine learning algorithm has a high probability to transform clinical care as it enhances and standardizes assessment across patients, institutions, and providers.
Comparison of Different Methods to Assess Kidney Volume Loss Following Partial Nephrectomy
A Beksac, KE Okhawere, C Dominy, TG Korn, KN Meilika, KK Badani
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
Introduction & Objective: A significant factor used to predict kidney function following partial nephrectomy (PN) is parenchymal kidney volume loss. Other methods of estimating kidney functionality after PN include: tissue segmentation (TS) tools, ellipsoid formula (EF), and surgeon assessment of volume preservation (SAVP). The purpose of this study was to analyze correlation of these methods with actual kidney volume loss in order to identify the best predictor of volume loss following PN.
Methods: 61 patients undergoing robotic PN for renal cell carcinoma were analyzed between January 2019 and October 2019. The aforementioned methods were used to predict volume loss after the procedure. TS analysis was achieved using venous phase of axial cross‐sectional imaging and marking regions of interest around the tumor to calculate tumor volume preoperatively. The EF method used dimensions from pathology of the specimen to calculate volume. SAVP was performed by the surgeon estimating percentage loss of overall kidney volume during the PN. Finally, the actual volume was calculated by measuring water displacement caused by the resected specimen in a specimen cup post‐surgery. Volumes were reported in medians and interquartile ranges. Spearman correlation was used to identify associations between estimated volumes predicted by each method with actual volume loss.
Results: The median estimated actual specimen volume was 14.50 ml. The median volume estimated by TS was 10.18 ml, the median surgeon assessment of volume preservation was 90.00%, and the median volume predicted by EF was 10.66 ml. Actual specimen volume had a significant, positive correlation with volume predicted by TS (rs = 0.88, p < 0.001) and by EF (rs = 0.69, p < 0.001) . Actual volume showed a significant negative correlation with SAVP (rs = ‐0.63, p < 0.001).
Conclusions: There were significant associations between the different volume assessment methods with actual specimen volume, with the TS method having the strongest positive association. Further studies must look to long‐term functional data to be able to identify each method's association with kidney functional outcome.
Comparison of renal functional outcomes between warm and cold ischemia following minimally invasive partial nephrectomy
R Matsumoto, T Abe, S Yamada, J Furumido, H Kikuchi, T Osawa, N Shinohara
Department of Renal and Genitourinary surgery, Graduate School of Medicine, Hokkaido University
Introduction & Objective: Recently, minimally invasive partial nephrectomy (MIPN) has been introduced for the treatment of varying levels of clinical T1 renal tumors. Although the most common method of renal hilar clamping in MIPN is the warm ischemia (WI) technique, the limiting time for preserving the renal function has generally been reported as 20‐25 minutes. If a longer ischemia time is expected considering the surgeon's skill and tumor characteristics, the cold ischemia (CI) technique may be selected as the alternative method. However, to our knowledge, few studies have compared the renal functional outcomes following the aforementioned ischemic techniques in MIPN. In this study, we compared the functional outcomes of MIPN performed with the CI and WI techniques.
Methods: From August 2004 to December 2019, a total of 284 patients with clinical T1 renal tumors underwent MIPN (laparoscopic, n = 222; robotic‐assisted, n = 62) at our institution. Fifty‐seven patients were excluded because of insufficient data, conversion to open surgery or radical nephrectomy, bilateral tumor, or zero ischemia. Finally, 125 patients who underwent MIPN by the CI and 102 patients by the WI technique were included. MIPN with CI was performed using ice slush as previously reported. [Abe T et al., J Endourol, 2012]. Pre‐ and postoperative renal function was evaluated based on the estimated glomerular filtration rate (eGFR) and 99mTc‐mercaptoacetyltriglycine scintigraphy. A multivariate linear regression model was used to test the association between the percentage change in split renal function (SRF) and clinical factors.
Results: The median renal nephrectomy scores in the CI and WI groups were 6 and 7, respectively, and the median tumor size was 2.3 cm in both groups. The ischemia time in the CI group, including the initial 12‐15 minutes of hypothermia, was longer than that in the WI group (CI group, 50 minutes [IQR, 43–61]; WI group, 20 minutes [IQR, 16‐24]; p value <0.001). However, there was no significant difference between the two groups in the reduction in eGFR (CI group, 7.49 ± 1.49 mL/min/1.73 m2; WI group, 7.95 ± 1.63 mL/min/1.73 m2; p value = 0.679) and SRF (CI group, 9.59 ± 1.07 %; WI group, 8.39 ± 1.18 %; p value = 0.139) at 6 months after the surgery. Multiple regression analysis demonstrated a significant correlation between the ischemia time and the decrease in SRF in both groups.
Conclusions: The decline in renal function after MIPN did not differ between the CI and WI techniques, regardless of prolongation in the ischemia time. Furthermore, the CI technique could be useful in cases where the ischemia time is expected to be longer.
Oncologic outcomes following partial nephrectomy versus percutaneous cryoablation: A propensity score matched analysis
NA Pickersgill, J Palka, J Vetter, G Henning, E Kim, H Kim, R Venkatesh, RS Figenshau
Washington University School of Medicine
Introduction & Objective: While partial nephrectomy (PN) is the preferred treatment modality for small renal masses, percutaneous cryoablation (PCA) has emerged as an acceptable alternative with favorable outcomes. However, there is a deficit of long‐term, high‐quality data comparing the two techniques. We reviewed long‐term oncologic outcomes following PN and PCA for renal masses utilizing a propensity score matching method.
Methods: A total of 940 patients with renal masses treated with PCA or PN between 2005 and 2016 were identified within our prospectively maintained institutional database. Demographic and clinical variables and oncologic outcomes were assessed. Two hundred and thirty‐three patients who underwent PN were propensity‐score matched 1:1 to 233 patients who underwent PCA. Patients were matched based on demographics, Charlson Comorbidity Index (CCI), and tumor characteristics, with exact matching performed for nephrometry score. Disease‐free survival (DFS) and overall survival (OS) were estimated using the Kaplan‐Meier method.
Results: There were no statistically significant differences in sex, body mass index, tumor size, or nephrometry score between the two cohorts. Mean patient age was 65.3 ± 9.5 years in the PN and 68.1 ± 10.5 years in the PCA cohort (P = 0.002). Twelve percent of patients undergoing PN and 20.6% of patients undergoing PCA had CCI ≥4 (P = 0.045). Median follow‐up was 48.0 months for PN and 47.9 months for PCA. Five‐year DFS was 96.7% and 78.5% for PN and PCA, respectively.
Conclusions: We report one of the largest propensity score matched analyses to date comparing long‐term oncologic outcomes of PN and PCA. In our institutional experience, PCA has acceptable oncologic outcomes compared with PN when accounting for patient and tumor characteristics. A shared decision‐making approach should be taken when choosing a treatment strategy.
In vitro assessment of new ureteral biodegradable drug eluting stent design to adjuvant therapy in Upper tract urothelial carcinoma
F Soria, JE de La Cruz, M Soto, S Aznar, J Cenis Anadon, A Budia Alba, F Sanchez Margallo
Methods: Three groups are used that are different in the concentration of Mitomycin used for coating, as well as in the formulation of the polymeric matrix that delivers the MMC in a controlled manner. The stents are formulated for release within 6‐12 hours post‐stenting. Group I‐ 20mg MMC; Group II‐40 mg MMC; Group III‐70 mg MMC without excipients. Twenty‐nine 3 cm long fragments of the biodegradable BraidStent biodegradable ureteral stent coated with a polymeric matrix followed by a dip coating technique for coating with MMC are used. After coating stabilisation, all study samples are introduced into individual tubes containing 5 ml of artificial urine with orbital shaking at 36°C. The artificial urine is exchanged in the test tubes. The artificial urine is changed at follow‐up times: 6, 12, 24, 24, 48, 72, 96, 120 hours. Mitomycin C release kinetics is evaluated at each follow‐up by HPLC‐DAD.
Results: 203 samples were analysed by HPLC‐DAD. MMC is released in all groups between the first 6 and 12h of immersion in artificial urine. The mean MMC concentration detected in Groups I, II and III is 6.39, 10.64 and 52.22 mg/L respectively. No significant alterations in the urinary pH of the samples were detected during the study.
Conclusions: The present in vitro study confirms the adequate release of Mitomycin C in urine through a drug eluting stent, with better results with increasing concentration of MMC. The polymeric matrix used allows the delivery and release of Mitomycin after contact with artificial urine. However, the dose released is lower than that described for clinical application. Further experimental studies are needed to increase the dose and assess the effectiveness and safety of the released MMC.
The impact of diabetes on the prognosis of upper tract urothelial carcinoma after radical nephroureterectomy: a systematic review
X Gao, L Zhou, W Wang, H Li, K Wang
Department of Urology, Institute of Urology (Laboratory of Reconstructive Urology), West China Hospital, Sichuan University, Chengdu, Sichuan, P.R. China
Introduction & Objective: To date, several studies have shown that diabetes is related to the prognosis of upper tract urothelial carcinoma (UTUC) after radical nephroureterectomy (RNU), but this conclusion is still controversial. Here, we performed a meta‐analysis to explore the association between diabetes and UTUC prognosis.
Methods: In November 2020, we searched PubMed, Web of Science and the Cochrane Library to find relevant studies that evaluated the effect of diabetes on the prognosis of UTUC. The Newcastle Ottawa Scale was used to assess the quality of the literature. Review Manager 5.3 was used to pool cancer‐specific survival (CSS), overall survival (OS), recurrence‐free survival (RFS) and intravesical recurrence (IVR).
Results: A total of 10 studies with 11,303 patients were included in this meta‐analysis. Our pooled results showed that diabetes did not affect the survival outcome of UTUC, including CSS (HR 1.34; p = 0.08), OS (HR 1.24; p = 0.17), and RFS (HR 1.20; p = 0.17). However, diabetes increased the risk of IVR in UTUC (HR 1.26; p = 0.0002).
Conclusions: Although diabetes has no significant impact on the survival outcome of UTUC after RNU, it increases the risk of IVR. Therefore, bladder adjuvant chemotherapy after surgery may be necessary for UTUC patients with diabetes.
Is minimally invasive partial nephrectomy safe in case of cT2 renal masses? Comparative analysis after 10 years of follow‐up
D Amparore, A Pecoraro, F Piramide, E Checcucci, P Alessio, S De Cillis, G Volpi, A Piana, P Verri, M Sica, S Piscitello, M Burgio, B Carbonaro, D Zamengo, M Cossu, M Manfredi, C Fiori, F Porpiglia
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
Introduction & Objective: Nowadays the role of partial nephrectomy (PN) in the management of cT2 kidney tumors is controversial. In this study we aimed to compare oncologic and functional outcomes of minimally invasive radical nephrectomy (RN) and PN in cT2 renal masses.
Methods: Patients with cT2 renal masses underwent minimally‐invasive PN or RN performed by a highly experienced single surgeon from 2009 to 2019 were considered. Demographic, perioperative and functional variables were compared. Cumulative incidence plot and competing risks regression (CRR) models were used to test differences in 5‐year‐CSM (Cancer Specific Mortality) and 5‐year‐ OCM (Other Causes Mortality) rates. Kaplan‐Meier and Cox regression model was used to test differences in 5‐year progression free survival (PFS) rates (figure 2).
Results: Overall, 52 PN vs 64 RN patients were identified. Relative to RN, PN patients recorded higher rates of complications (25% vs 7.8%, p = 0.02) but lower upstaging rate (≥pT3a 64.1% vs 19.2%, p < 0.0001). Functional outcomes were in favor of PN (all p < 0.001). No differences were recorded between 5‐year CSM and OCM according to nephrectomy type (figure 1). At CRR models, older age and upstaging were independent predictors of 5‐year OCM and CSM, respectively (all p < 0.01). For PN vs RN the 5‐years PFS was 92.2% vs 72.8% (p = 0.02). Only upstaging, high grade tumors and presence of positive surgical margins were identified as independent predictors of 5 years PFS (all p < 0.01).
Conclusions: In experienced hands the treatment of cT2 renal neoplasms with minimally‐invasive PN is feasible, providing perioperative and oncological safety profiles comparable to RN, with advantages in terms of functional outcomes even for large tumors.
Predicting Renal Function after Radical Nephrectomy in Search for an Indication for Partial Nephrectomy
J Na, J Kim, S Alip, W Han
Yonsei University College of Medicine
Introduction & Objective: When considering surgical treatment for patients with renal cell carcinoma(RCC) of high complexity the choice between partial or radical nephrectomy is often at debate. In this study, we analyzed the predictive factors for renal function preservation or deterioration after radical nephrectomy to establish a standard when partial nephrectomy is most likely to benefit RCC patients.
Methods: Patients who underwent radical nephrectomy for T1a RCC in our institute from Dec, 2005 to Dec, 2015 with a follow‐up serum creatinine more than 1 year after surgery were included in this study. Those with metastatic disease, bilateral renal tumors, a CKD class 5, history of kidney transplantation were excluded. Renal function preservation(RFP) was defined as higher than 80% maintenance of estimated glomerular filtration rate (eGFR) compared to eGFR at 1 year after nephrectomy. Renal function deterioration(RFD) was defined as 50% or more decline of estimated glomerular filtration rate (eGFR) compared to eGFR at 1 year after nephrectomy.
Results: Among 457 patients followed for 83.9 ± 35.0 months included in this study there were 93 (20.4%) patients who had failed to preserve renal function (RFP‐failure) and 18 patients who had RFD during follow‐up. Age, BMI, preoperative eGFR, history of hypertension, diabetes, ASA classification were factors predicting RFP. These factors were entered in to multivariable analysis and age (OR 1.026, 95%CI 1.003 ∼ 1.051) and ASA classification remained as significant factors predicting RFP‐failure after radical nephrectomy. (Table1, Fig1) Age, preoperative eGFR, history of hypertension, diabetes, ASA class greater than 2 were significant factors predicting RFD. These factors were entered in to multivariable analysis and preoperative eGFR lower than 45 ml/min/1.73 m2 (OR 6.05, 95%CI 1.69 ∼ 21.7), diabetes (OR 2.73, 95%CI 1.003 ∼ 7.43) remained as significant factors predicting RFD after radical nephrectomy. (Table2, Fig2)
Conclusions: Patients with RCC who have a higher ASA classification and who are elder are less likely to preserve renal function and those who have a history of diabetes or with an eGFR lower than 45 ml/min/1.73 m2 are at increased risk for RFD during follow‐up after radical nephrectomy. For these patients, even if the tumor is complex, further consideration should be given to partial nephrectomy.
Analysis of risk factors predicting oncological outcome of the heterogenous T3aN0M0 kidney cancer
J Na, J Kim, J Kim, S Alip, W Han
Yonsei University College of Medicine
Introduction & Objective: The prognosis of T3a kidney cancer is heterogenous and there has been controversy whether factors such as tumor size, location of fat invasion, and presence of renal vein invasion impact oncological outcomes. In this study we analyzed the risk factors predicting oncological outcome of T3aN0M0 kidney cancer
Methods: Patients who underwent radical nephrectomy for T3aN0M0 kidney cancer from Jan, 2006 to Dec, 2015 were included in the study. Data on age, gender, tumor size, location of fat invasion, renal vein invasion and thrombosis, surgical margin, histologic grade, presence of necrosis, lymphovascular invasion and cause of death, recurrence on follow‐up were collected.
Results: 153 patients were included in the study. Location of extra‐renal fat invasion (EFI) was not a significant factor predicting cancer specific‐survival(CSS) or recurrence free survival(RFS). Presence of renal vein involvement (RVI) did not predict worse outcome compared to EFI. Coexisting EFI and RVI was associated with worse RFS (HR 2.05 (1.14 ∼ 3.70), p = 0.017), but not for CSS. Tumor size larger than 5cm was associated with worse CSS (HR 4.52 (1.38 ∼ 11.20), p = 0.01) and RFS (HR 4.52 (1.91 ∼ 10.72), p = 0.001). Tumor size and coexisting EFI and RVI were entered into multivariate regression analysis along with gender and Fuhrman grade which were also significant factors on univariate analysis. On multivariate analysis tumor size >5cm was a significant factor associated with CSS (HR 5.45 (1.26 ∼ 23.6), p = 0.023) and RFS (HR 4.69 (1.63 ∼ 13.45), p = 0.004). High Fuhrman grade was associated with worse RFS (HR 2.98 (1.05 ∼ 8.46), p = 0.04) and coexistence of EFI and RVI was not a significant factor. The 5 year CSS and RFS for tumors smaller than 5cm were 95.9% and 91.5%, while those for tumors larger than 5cm were 79.3% and 60.2%.
Conclusions: Among the factors known to be associated with oncological outcome of T3aN0M0 kidney cancer, location of EFI was not a significant factor and coexistence of EFI and RVI may be associated with worse RFS but was not a significant factor on multivariate analysis. Only tumor size was a significant factor associated with CSS and RFS on multivariate analysis.
Comparing perioperative outcomes between transperitoneal and retroperitoneal approaches in patient with obesity after robotic assisted partial nephrectomy
KE Okhawere, R Patel, A Beksac, KN Meilika, TG Korn, A perez, S Kuppa, R Harrison, R Abaza, DD Eun, A Bhandari, AK Hemal, J Porter, M Stifelman, KK Badani
Icahn School of Medicine at Mount Sinai
Introduction & Objective: Robotic partial nephrectomy (RPN) in obese patients can be complicated by the presence of significant abdominal and/or retroperitoneal fat. The retroperitoneal approach can be further complicated due to the limited working space in obese patients. To assess differences in perioperative outcomes, we performed a comparative analysis of obese patients who received RPN via a transperitoneal or retroperitoneal approach.
Methods: Using a multi‐institutional database, we analyzed 589 obese patients with a body mass index (BMI) >30 kg/m2 that had renal masses excised via RPN (434 transperitoneal, 155 retroperitoneal). To adjust for age, gender, BMI, CCI, baseline eGFR, tumor size, and tumor complexity, we utilized a 1:1 propensity score match. During the estimation of the propensity score, a missing indicator method was used. After propensity score matching, Mann Whitney U test, Chi‐square test and Fishers exact test were performed to compare perioperative outcomes between the two groups (154 transperitoneal, 154 retroperitoneal).
Results: After propensity matching, baseline, clinical and tumor characteristics were similar between the two groups. When comparing transperitoneal and retroperitoneal approaches, ischemia time (16 min vs. 17 min, p = 0.257), operative time (170 vs. 164 min, p = 0.401), estimated blood loss (100 ml vs, 100 ml, p = 0.836), length of stay (1 day vs. 1 day, p = 0.797) and perioperative complication rate (9.74% vs. 7.14%, p = 0.411) were found to be similar between the two groups. There was also no difference observed in positive surgical margin rate as (3.9 vs. 3.25%, p = 0.759).
Conclusions: Obese patients, regardless of surgical approach, experienced similar perioperative outcomes. Both transperitoneal and retroperitoneal approaches remain a safe and viable option for robotic partial nephrectomy in obese patients.
Prevalence of benign renal masses after partial or radical nephrectomy in Caucasian Americans versus African Americans
SP Argade, J Vetter, J Palka, KG Sands
Washington University School of Medicine
Introduction & Objective: Differentiating between benign and malignant renal masses can be challenging using noninvasive techniques. A substantial number of excised renal masses have benign pathology. Little is known about racial disparities in benign renal masses. This study sets out to compare the prevalence of benign renal masses in Caucasian Americans (CA) and African Americans (AA) after surgical excision.
Methods: We retrospectively reviewed all laparoscopic and robotic partial and radical nephrectomies performed at this institution between 2007‐2017 on patients self‐identifying as CA and AA. We compared baseline patient characteristics of each group including age, sex, BMI, and Charlson Comorbidity Index (CCI), baseline tumor characteristics including RENAL Nephrometry score and tumor size, surgical modality, and surgical technique. Finally, surgical pathology with regards to histology and pathological cell type were compared.
Results: We identified 1154 patients in the CA group and 171 patients in the AA group. There was no significant difference in age, BMI, and CCI between groups, but there were more women in the AA group (p = 0.03). Average RENAL Nephrometry scores were 7.7 and 7.5 (p = 0.33) and average tumor size was 3.7 and 3.4 cm (p = 0.18) for the CA and AA groups, respectively. Similar proportions of patients underwent laparoscopic vs. robotic procedure (p = 0.09) and partial vs. radical nephrectomy (p = 0.96). Pathologic analysis showed similar proportion of benign renal masses overall (12.4% CA vs. 9.4% AA, p = 0.25). However, there was a significantly higher proportion of angiomyolipoma (AML) (3.0% CA vs. 5.3% AA, p < 0.001), and lower proportion of oncocytoma (8.6% CA vs. 4.1% AA, p < 0.001) in AA patients (Table 1).
Conclusions: Analysis of CA vs. AA patients undergoing renal mass excision shared similar baseline patient, tumor, and surgical characteristics, but statistically significant differences in pathology. While similar proportions of patients in both groups were found to have benign renal masses, AML appears to be more prevalent and oncocytoma less prevalent in AA patients.
Defining Patient Selection for Surveillance of Renal masses: Results from a MUSIC consensus panel
A Patel, B Lane, M Butaney, A Johnson, J Qi, C Rogers, f Urological Surgery Improvement Collaborative
Henry Ford Health System
Introduction & Objective: The Michigan Urological Surgery Improvement Collaborative ‐ Kidney mass: Identifying and Defining Necessary Evaluation and therapY (MUSIC‐KIDNEY) has previously shown variability in patients selected for surveillance(AS). We established a consensus panel (CP) to help define appropriate candidates for AS.
Methods: A CP was organized within MUSIC using a modified Delphi method to define areas of consensus regarding AS. Participants indicated level of agreement with statements relating to patient(pt) selection for AS via an online tool. Factors not achieving agreement were iteratively developed between the 3 rounds of questionnaires. Level of agreement necessary to achieve consensus was set at 80%. Using the Rand appropriateness method a combination of factors including life expectancy (LE), tumor size, renal function, tumor complexity and perioperative risk were assessed.
Results: Twenty‐six MUSIC urologists (69% fellowship trained, 73% practicing in the community) formed the CP. 54% of statements achieved consensus on pt selection factors. Pt factors that achieved consensus for appropriateness of selection included life expectancy(LE), age, comorbidity, and renal function, with LE ranking 1st, the primary driver. Combination of LE with tumor size revealed all tumors <3cm and pts with LE <1year appropriate for AS (Figure 1). Addition of increasing tumor complexity, perioperative risk or declining renal function, appropriateness of AS increased. There were several pt scenarios in which it was unclear whether AS or intervention was more appropriate, and findings from biopsy were of great value to reaching a verdict in these situations (Figure 1). Tumor factors with low consensus(< 20%) for AS were cT3a, infiltrative masses, symptomatic masses, biopsy tumor grade 4 and variant histology (Figure 1).
Conclusions: A CP following a modified Delphi approach helped define areas of agreement regarding appropriate candidates for surveillance of renal masses. LE appears to be a strong factor in selection for surveillance. Consideration of tumor characteristics and biopsy may also improve the appropriateness of each management decision. Development and use of a LE calculator could aid clinicians and pts in the decision to pursue surveillance.
Risk factors for postoperative ileus after robot‐assisted radical cystectomy with intracorporeal urinary diversion
K Zennami, M Sumitomo, K Takahara, T Nukaya, M Takenaka, K Fukaya, M Ichino, N Fukami, H Sasaki, M Kusaka, R Shiroki
Introduction & Objective: Postoperative ileus (POI) is a common complication following radical cystectomy (RC) with intestinal urinary diversion. POI and delay of bowel recovery severely impair patient's quality of life and prolong length of hospital stay (LOS). Recently, robot‐assisted radical cystectomy (RARC) with intracorporeal urinary diversion (ICUD) has gained popularity and is rapidly expanding. However, predictors of POI following ICUD remains uncertain. In this study, we evaluated the risk factors of POI in patients who underwent RARC with ICUD.
Methods: We retrospectively analyzed 70 bladder cancer patients who received RARC with ICUD at Fujita Health University during 2011–2020. Baseline characteristics, perioperative and pathological outcomes were compared between the no POI and POI cohorts. The logistic regression analysis was used to identify the risk factors of POI.
Results: 20 (28.6%) of 70 patients developed POI. The POI cohort was associated with significantly higher rate of previous abdominal/pelvic surgery (p = 0.04) (Table 1), longer intestinal tract reconstruction time (p = 0.04), longer LOS (p < 0.001), longer time to first mobilization (p < 0.001), and longer time to water intake (p = 0.01). Significantly delayed bowel recovery (time to flatus, stool, and solid intake; all p < 0.001) were observed in the POI cohort (Table 2). Logistic regression analysis identified previous abdominal/pelvic surgery (p = 0.03) and time to first mobilization (p = 0.02) as independent predictor of POI (Table 3). There was no significant association between the type of previous abdominal/pelvic surgery and POI.
Conclusions: Early mobilization after surgery may help bowel recovery and prevention of subsequent ileus following ICUD. Since intestinal reconstruction time seems to affect POI, standardized and simplified ICUD technique should be performed.
hTERT, hTR and TERT promoter mutations as markers for urological cancers detection: a systematic review
A Morozov, N Potoldykova, M Enikeev, A Glukhov, A Shpikina, E Goryacheva, M Taratkin, B Malavaud, D Enikeev
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia
Introduction & Objective: There is a number of original studies addressing a role of telomerase and its subunits in urological cancers detection and follow‐up, but their application is still not clear. To contribute to the reappraisal of telomere biology in urology, we conducted a systematic analysis of biomarkers applications in bladder cancer (BCa), renal‐cell carcinoma (RCC) and prostate cancer (PCa).
Methods: We performed a systematic literature search using 2 databases (Medline and Scopus) over the past 20 years following PRISMA guidelines. The detailed search strategy and review protocol has been published in Prospero (ID 178460). The scope of the review according to PICO process is as follows:
P – patients with BCa, RCC or PCa
I – detection of hTERT (human telomerase reverse transcriptase mRNA) / hTR (human telomerase RNA) and TERT promoter mutations in urine OR in tissue
C – urine cytology OR histology
O – sensitivity and specificity of hTERT/hTR/TERT promoter mutations
Primary outcomes were sensitivity and specificity of the biomarkers. Secondary outcomes were the biomarkers predictive values for tumor characteristics.
Results: The final sample included 17 articles related to BCa, 9 related to RCC, and 12 – to PCa.
Regarding bladder cancer, hTERT in urine showed high sensitivity (mean values: 55‐96%), and specificity (69‐100%): it correlated with BCa grade and/or stage. hTR sensitivity ranged from 77% to 92%. With adapted cut‐off, it demonstrated 72‐89% specificity. TERT promoter mutation rate was up to 80% both in tissue and urine, resulting in 62‐92% sensitivity for primary tumors and 42% for relapse. Specificity ranged from 73% to 96%, no correlations with stage were observed.
In prostate cancer, hTERT in tissue, prostate secretion and serum showed high sensitivity (97.9%, 36% and 79.2‐97.5%, respectively) and specificity values (70%, 66%, 60‐100%). hTR showed very high sensitivity (88% in serum and 100% in tissue) although specificity values were highly variable depending on the series and techniques (0 – 96.5%).
In RCC, hTERT sensitivity on tissue ranged from 90 to 97%, specificity from 25 to 58%. There was an association of hTERT expression with tumor stage and grade.
Conclusions: hTERT showed high accuracy in genitourinary cancers, while the value of hTR was more controversial. hTERT and TERT promotor mutations may have predictive value for BCa and RCC staging and grading, while no such relationship was observed in PCa.
Real world experience of metastatic urothelial carcinoma treated with immune check point inhibitors
H Hsiang‐Chen, L Jian‐Ri
Taichung Veterans General Hospital, Division of Urology, Department of Surgery, Taichung
Introduction & Objective: Immune checkpoint inhibitors (ICIs) have become important tools for the treatment of metastatic urothelial carcinoma (mUC). Herein we presented our single institute experience using ICIs in mUC patients.
Methods: Between January 2015 and October 2020, 74 mUC patients treated with atezolizumab and pembrolizumab were included in this retrospective study. The study was reviewed and approved by the Institute of Review Board. Among them, 53 patients received atezolizumab and the other 21 received pembrolizumab.
Results: Ten patients (10/62, 16.12%) received carboplatin chemotherapy and the other 52 received cisplatin based chemotherapy. The basic characteristics were listed at table 1. The median age was 67 years old. The median treatment cycles of ICIs and chemotherapy were 6 and 4 respectively. The median ICIs and chemotherapy duration of treatment were 7.24 and 7.79 months respectively. The median progression free survival was 10.94 months and the overall survival was 28.44 months. ICIs response and chemotherapy duration were associated with decreased death risk (HR = 0.22, 95% CI = 0.08‐0.62, p = 0.004 and HR = 0.91, 95% CI = 0.86‐0.91, p = 0.003 respectively). Liver metastases and serum white blood cell count(WBC) before ICIs treatment were associated with increased risk of death (HR = 11.95, 95% CI = 3.22‐44.34, p < 0.001 and HR = 1.0001, 95% CI = 1.0001‐1.0002, p = 0.036 respectively, table 2). For further analysis of association of ICIs responses, only ICIs treatment duration was associated with better response (OR = 1.08, 95% CI = 1.01‐1.16, p = 0.025). However, high Neutrophil/Lymphocyte ratio (NLR) was associated with poor ICIs treatment response (OR = 0.97, 95% CI = 0.95‐0.996, p = 0.018).
Conclusions: Our real world data showed ICIs was effective in the treatment of mUC patients. Chemotherapy also had an impact on the patient survival. Serum WBC or NLR may account for an indicator as poor outcome or poor responders for ICIs treatment.
Establishment of Prognostic Nomogram and OS‐Calculator for Patients with Stage III and IV Renal Cell Carcinoma
l Hao, K Wang
Introduction & Objective: The study aimed to establish a nomogram and counterpart OS‐Calculator that contains variables that are readily accessible to predict overall survival (OS) for patients with stage III and IV renal cell carcinoma.
Methods: Patients with stage III and IV RCC were selected from the SEER database (n = 14147) from 2010 to 2015. Results from multivariate Cox regression served as a basis for the development of the nomogram. The predictive performance of the nomogram was determined by Harrell's concordance index (C‐index), receiver operating characteristic (ROC) curves, and calibration plots. Then the generalized linear model (GLM) was used to regress the total score of nomogram and OS, upon which OS‐Calculator was built.
Results: Independent prognostic factors were identified including age, marital status, race, pathological type, grade of differentiation, tumor size, node involvement, metastasis, surgery, radiation therapy and chemotherapy. C‐indexes were calculated of 0.811 (95% CI: 0.807 to 0.815) and 0.810 (95% CI: 0.800 to 0.820) for the training and validation cohorts respectively, which were statistically higher than that of TNM staging system. Area under the curve (AUCs) were calculated of 0.864 and 0.871 for 1‐year and 3‐year prediction respectively. The calibration plot show great agreement with actual survival rates. The nomogram total scores and OS was ideally explained by GLM model in 1‐year (R2, 0.991) and 3‐year (R2, 0.992) prediction. The OS‐Calculators based on GLM model were therefore available at https://drlihaoz.github.io/OS-Calculator-RCC/Calc/index.html
Conclusions: We developed a new nomogram and its counterpart OS‐Calculators that can accurately make survival predictions for patients with stage III and IV RCC.
Withdrawn
Incidence of benign tumors at partial nephrectomy for solitary renal mass presumed to be renal cell carcinoma: our experience of 195 cases
R Baio, U Di Mauro, O Intilla, G Molisso, A Pane, R Sanseverino
Introduction & Objective: In contemporary practice, a significant proportion of renal tumors are incidentally detected on imaging studies due to the improvements in technology and its more intensive use. This has resulted in smaller lesions being detected. Some recent series have revealed that up to 27% of small enhancing renal masses are benign at surgery. This challenges the appropriateness of surgery for all suspicious lesions, given the morbidity associated with such an intervention. The objective of this study was to determine the incidence of benign pathologic findings at partial nephrectomy for a solitary renal lesion.
Methods: A total of 195 patients who each underwent one partial nephrectomy for a solitary renal lesion with the intent to cure Renal Cell Carcinoma (RCC) were included in the final retrospective analysis. A benign neoplasm was found in 30 of these patients, including 19 males and 11 females, with 15 cases on the left side and 15 cases on the right side. Their age was between 29,9 to 79 years (average: 60,9 years). The tumor size was between 1,5 cm to 7 cm (average: 3 cm). Of the 30 cases, 9 were located in the middle of kidney, 15 in the upper pole and 6 in the lower pole.
Results: All the operations were successful. In only three cases of these 30 partial nephrectomies, conversion to open surgery was required. The blood loss ranged from 150 to 1800 mL (mean: 523 mL) while the operation time ranged from 75 to 330 min (mean: 186 min). The pathological results were renal oncocytoma in 26 cases, AngioMyoLipomas (AML) in 2 cases and cysts in the remaining two cases.
Conclusions: Historically, urologists have counseled patients that more than 90% of solid renal masses prove to be RCC at nephrectomy. However, contemporary reports have indicated that up to 27% of renal masses are benign at surgery; therefore, we retrospectively reviewed all partial nephrectomies for a solitary renal mass performed at our institution. We excluded patients with a known genetic predisposition to RCC or those who underwent resection of more than one lesion. We found that 15,4% of partial nephrectomies performed for a suspected solitary Renal Cell Carcinoma (RCC) revealed benign pathologic features (30 of 195). In view of these results, when surgery is elected, not only must one counsel the patient about the perioperative risks but a discussion must also take place about the dual therapeutic and diagnostic role of partial nephrectomy. The patient must be well informed that the odds of the final pathologic examination revealing a benign result are considerable.
High Risk Disease And Poor Followup: The Role Of Renal Mass Biopsy In A Cohort Of Veterans
K Anishchenko, S Antoine, R Lenzmeier, S Kim, GL Lloyd
Department of Urology, Rocky Mountain Regional Veterans Hospital
Introduction & Objective: Renal mass biopsy (RMB) is increasingly used in the clinical management of renal masses, especially for masses ≤4 cm (T1a). In this study, we sought to review utility of this procedure for identification and management of small renal cell carcinoma (RCC) in the setting of the unique and comorbid population of our Veterans Affairs Hospital.
Methods: From 136 renal mass biopsies performed between 06/2015 and 11/2020, 89 patients with T1a lesions were identified in this Quality Improvement analysis. Mass size, biopsy pathology, treatment, and imaging compliance were retrospectively analyzed. Surveillance compliance was compared to National Comprehensive Cancer Network (NCCN) guidelines for each treatment modality, which were recommended initially and reviewed at each patient visit.
Results: The median age of our cohort at time of RMB was 66 years old. Biopsy of T1a renal masses yielded diagnostic results in 96.5% with a complication rate of 2%: one retroperitoneal bleed treated with observation and one hemorrhage requiring embolization (Clavien Grades 1 and 3). Findings of unexpectedly aggressive lesions (Fuhrman Grade 4, Type 2 papillary RCC or sarcomatoid features) were identified by biopsy in 8 (9%), with 28 (31.5%) identified as benign or indolent neoplastic processes including oncocytoma. 57 (64%) patients were treated with cryoablation or surgery and 32 (36%) patients elected active surveillance (AS) for their renal masses. 16 patients in the AS group (50%) had a neoplastic RMB finding (oncocytoma or RCC), while 52 patients in treatment group (91.2%) had a neoplastic result. At the second follow‐up, compliance with NCCN‐recommended imaging was 50% for surveillance, 47% among those undergoing cryoablation and 47% among those undergoing partial or radical nephrectomy.
Conclusions: In this cohort, we found a significant incidence of high‐risk lesions on RMB and saw poor compliance with follow‐up imaging despite vigorous attempts to adhere to NCCN guidelines. Follow‐up was incomplete or absent in a high percentage of patients at all time points. More aggressive biopsy protocols with high consideration of treatment may be appropriate to limit risk in those lost to follow‐up. Given that 9% of our small renal masses were highly aggressive, a significant percentage may be at especially high risk in an active surveillance setting.
Initial Management of Indeterminate Renal Masses in a Statewide Collaborative:a MUSIC‐KIDNEY analysis
M Butaney, A Patel, B Lane, J Qi, A Johnson, C Rogers, f Urological Surgery Improvement Collaborative
Henry Ford Health System
Introduction & Objective: The widespread use of imaging has led to the increasing detection of incidental renal lesions. Although some may be accurately classified as suspicious (renal cell carcinoma) and others as benign (Bosniak I‐IIF cysts or angiomyolipomas), other lesions are best initially characterized as ‘indeterminate’. For example, when they cannot be determined to be enhancing without additional imaging sequences. Optimal management is not well understood. We assess the use of follow up imaging in the management of indeterminate renal lesions(IRL).
Methods: The Michigan Urological Surgery Improvement Collaborative—Kidney mass: Identifying and Defining Necessary Evaluation and therapY (MUSIC‐KIDNEY) commenced data collection in September 2017 by recording clinical, radiographic, pathologic, and follow‐up data at 13 diverse practices. At initial evaluation, data was recorded regarding the radiologist interpretation of each imaging study (suspicious, indeterminate, benign) as well as the clinician's assessment. Patients with complete data were assessed at 120 days after initial evaluation as to whether observation or treatment was performed.
Results: 19.6% (472/2413) patients(pts) were recorded as having an IRL at their initial imaging study, of which 36% had non‐contrast imaging. 23.9% (113/472) of pts with IRL underwent subsequent imaging(SI), of which 59.3% (67/113) were re‐classified as solid enhancing lesions, 20.4% as benign lesions, with only 20.4% IRL remaining. Of these 113 pts with repeat imaging, 17 underwent biopsy (15 malignant, 1 benign, 1 indeterminate) and 10 of 15 pts with cancer on biopsy underwent treatment, while the remaining selected surveillance. Pts with initial IRL reclassified to suspicious were less likely to have benign histology at pre‐treatment biopsy (8.7% vs. 9.7%) or surgery (6.1% vs. 10.5%) compared with lesions initially characterized as suspicious, but these did not reach statistical significance.
Conclusions: Until now, outcomes of indeterminate renal masses have been poorly understood. About 80% of patients with indeterminate renal lesions can be reclassified with subsequent dedicated imaging. Patients with benign renal lesions, including Bosniak I‐IIF cysts, T1a AMLs, and other non‐enhancing lesions or pseudotumors can be reassured and should not undergo intervention. Initial contrast axial imaging, the addition of further imaging and consideration of biopsy more fully characterizes an indeterminate renal lesion, often affecting subsequent management.
Endoscopic exploration directly impacts clinical decision making in the management of patients with suspected upper tract urothelial carcinoma following radical cystectomy
J Aumatell, P Diana, J Huguet, J Subiela, A Piana, JM Gaya, O Rodriguez Faba, A Territo, A Gallioli, J Palou, A Breda
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
Introduction & Objective: To assess whether use of endoscopic exploration (EE) as a routine diagnostic tool in patients with clinical suspicion of upper tract urothelial carcinoma (UTUC) following radical cystectomy (RC) significantly impacts management decision‐making and to describe the oncological outcomes of patients with UTUC after RC.
Methods: We performed a retrospective review of medical records of patients with suspicion of UTUC after RC between 2000 and 2019. Patient demographics, clinicopathological features, treatments, and outcomes were analyzed.
Results: We identified 60 patients with suspicion of UTUC. After diagnostic work‐up, 16 were submitted to radical nephroureterectomy (RNU) and 44 underwent diagnostic EE. After EE, a further 18/44 (40.9%) were submitted to RNU, while no evidence of tumor was found in 12 (27.3%) and the remaining 12 (27.3%) underwent endoscopic treatment (ET). Thus, in 24/44 (54.5%) patients the primary treatment strategy, i.e., RNU, was altered. Twenty‐nine (85.3%) of the 34 patients who underwent RNU had high‐grade (HG) tumors and 16 (47%) had muscle‐invasive disease. In the ET group, 6 (50%) had HG tumors and 10 (83.4%) had tumors less than 2 cm. The 5‐year estimated recurrence‐free survival and cancer‐specific survival were, respectively, 58.4% and 45.6% in the RNU group and 25% and 80.8% in the ET group.
Conclusions: Endoscopic exploration significantly impacts clinical decision‐making in patients with suspicion of UTUC after RC, resulting in a change in treatment strategy in approximately half of the patients. UTUC following RC has a poor prognosis and although RNU is the gold standard, ET could be considered in a selected group of patients.
Management of primary upper urinary tract carcinoma in situ diagnosed by ureteroscopic biopsy: is bacillus Calmette‐Guerin an alternative to nephroureterectomy?
S Fontanet‐Soler, A Territo, A Piana, A Gallioli, P Diana, J Huguet, JM Gaya, P Gavrilov, J Palou, A Breda
Department of Urology, Fundació Puigvert, Barcelona, Spain
Introduction & Objective:Carcinoma in situ in upper urinary tract (UT‐CIS) has an incidence of 5‐10%, which difficults to study its natural evolution and optimal treatment. Radical nephroureterectomy (RNU) still represents the gold standard treatment for UTUC, however attempts to treat conservatively UT‐CIS, especially in imperative cases, have been carried out since the 80s. The aim of this study is to compare the outcome of patients treated in our center who underwent RNU or conservative treatment with distal ureterectomy (DU) or bacillus Calmette‐Guérin (BCG) instillations for UT‐CIS.
Methods: We realized a retrospective study including patients with diagnosis of UT‐CIS between 1990‐2018. Diagnosis was confirmed histopathologically by performing ureteroscopy (URS) with multiple biopsies in patients with positive urinary cytology, negative CT urogram and negative bladder biopsies. After the histological confirmation of the diagnosis, all patients received some kind of treatment: RNU, DU or BCG instillations. BCG was administered either using nephrostomy tube, single‐J (S‐J) or double‐J (D‐J) ureteral stent. Clinicopathological features and outcomes were compared between the different groups of treatment.
Results: A total of 27 patients and 29 renal units (RU) were included in the study. Twenty (74.1%) patients had previous history of non‐muscle‐invasive bladder cancer. Sixteen patient (17 RU) (58,6%) received BCG treatment. The modalities of BCG administration included nephrostomy tube (4 patients), S‐J (5 patients) and D‐J (7 patients). Complete response and recurrence was detected in 10 and 7 RU. Treatment for recurrence was RNU. We detected 3 cases of disease progression, 2 patients died because of their cancer and one from other causes. Eight (27.5%) RU underwent RNU. In four of those patients contralateral recurrence was detected and caused exitus in one case due to disease progression. Recurrence treatments were DU (2) and BCG (2).
Four (13.7%) RU underwent DU: one patient developed a recurrence and was successfully treated with BCG perfusion and one case died due to cancer progression. No differences were found in cancer‐specific survival (p = 0.776), recurrence‐free survival (p = 0.841), progression‐free survival ( p = 0.451), or overall survival (p = 0.701) between the RNU and BCG groups.
Conclusions: Although RNU remains the gold standard treatment for UT‐CIS, our results confirm that BCG instillations are also effective. Histological confirmation of UT‐CIS is mandatory before any treatment.
Pre‐Nephroureterectomy Diagnosis of Low‐Grade Urothelial Carcinoma Does Not Predict Low Grade Disease On Final Pathology
M Hout, B GOLIJANIN, C Tucci, F Kazal, TK O'Rourke, DW Sobel, G Pareek, D Golijanin
The Warren Alpert Medical School of Brown University
Introduction & Objective: Upper tract urothelial carcinoma (UTUC) treatment depends on stage and grade of the disease. The gold standard of treatment is radical nephroureterectomy. In recent years UTUC treatment trends for low grade (LG) disease have shifted more towards minimally invasive and endoscopic approaches. Due to the potentially aggressive nature of UTUC, there is a risk of undertreatment especially if high grade (HG) disease is not confirmed on endoscopic biopsies. We sought to explore the risk of upgrading of UTUC, pathological, and long‐term outcomes.
Methods: A retrospective analysis of nephroureterectomy for UTUC cases performed at our hospital system from 1/1/2006 – 12/31/2020 was completed. Clinicopathologic features of patients were collected. Pre‐operative pathology and diagnostic methods were analyzed, and descriptive statistics were summarized. Paired, nominal data of pre‐operative and post‐operative grading were compared using McNemar's test. All analyses were completed using SPSS Version 26 (IBM Corp, Armonk NY).
Results: 97 patients were included. 68/97 (70%) of patients were diagnosed with UTUC pre‐operatively via endoscopic biopsy. 11 (11%) were diagnosed visually by endoscopy and 14 (14%) were diagnosed by cross sectional imaging. Of the 68 patients with biopsies, 37 (54%) were LG and 31 (46%) were HG. Of all patients with preop LG UTUC 25/37 (68%) were upgraded to HG UTUC (p < .0001) on final pathology. A total of 56/68 (84%) patients had HG UTUC on final pathology. Of patients with upgraded final pathology (n = 25), 16 (64%) were cT1, 8 (32%) cT2, and 1 (4%) was cT3 and were changed to 10 (40%) pTa, 7 (28%) pT1, 2 (8%) pT2, 5 (20%) pT3, and 1 (4%) pT4. Of upgraded patients with LG and HG on final pathology 2 (16%) and 11 (44%) ultimately passed away, respectively. Type of endoscopic biopsy device was not associated with a difference in LG biopsy upgrading.
Conclusions: Management of LG UTUC on endoscopic biopsies carries significant risk due to potential of undergrading. Caution is highly advised when selecting patients for minimally invasive or endoscopic management even if adequate pathology specimen has been harvested and results in LG disease. A prenephroureterectomy diagnosis of LG UTUC is a poor predictor of final pathology.
Moderated Poster Session 26: Clinical Oncology I
Laser versus Electrical E‐Bloc resection of bladder tumors for treatment of non‐muscle invasive bladder cancer; critical appraisal through a randomized trial
A Elshal, M Bahy, M Laymon, A Hashem, A Mosbah, A Nabeeh
Mansoura Urology and Nephrology Center
Introduction & Objective: Laser En‐bloc resection of bladder tumors (ERBT) has been reported as a safer procedure with less residual tumor and better specimen quality when compared to conventional resection. In this trial, we tested the non‐inferiority of electrical versus laser ERBT invasive bladder cancer (NMIBC).
Methods: Between June 2019 and December 2020, 106 patients with cystoscpic visual criteria of NMIBC were randomly allocated to laser and electrical enbloc resection. The primary endpoint was to assess the need of conversion to conventional TURBT. Operative parameters, quality of specimen, perioperative complications and completeness of resection as indicated by residual tumors in restaging TUR (2‐6 weeks after ERBT) Trial ID NCT04029948
Results: Patients` and tumor`s baseline characteristics were comparable in both groups. More resection time was reported during laser ERBT, P = 0.04. Technical failure with conversion to conventional resection was in 2 cases during electrical ERBT and none during Laser ERBT, P = 0.146 Detrusor muscle was sampled in 59.3% and 53.8% (p = 0.574) in Laser ERBT and electrical ERBT, respectively. Lamina propria invasion was 85.1%% and 84% in Laser ERBT and electrical ERBT, respectively (p = 0.111). Intraoperative complications were reported in 17.3% after electrical ERBT in the form of obturator kick, bladder perforation and with no complications reported in the laser group (P = 0.002). Table 1 There was no statistical difference between laser and electrosurgical ERBT regarding urethral catheter duration and hospital stay with P value 0.2 & 0.9 in the 2 groups respectively. Residual tumors at second look were detected in 6.5% and 2.6% Laser ERBT and electrical ERBT, respectively(P = 0.391)
Conclusions: Laser ERBT seems to be safer procedure for bladder tumor resection with longer resection time when compared to electrical ERBT
Clinical Significance of Preoperative Thrombocytosis in Patient with urothelial carcinoma from renal calyx to distal ureter
P Song, Y Kim, J Choi, Y Ko, K Moon, H Jung
Yeungnam University Medical Center
Introduction & Objective: In urothelial carcinoma (UC) of the bladder, preoperative thrombocytosis (PTC) has been identified as a predictor for oncologic outcome and survival after radical cystectomy. The aim of this study was to investigate the influence of an elevated platelet count in patients undergoing radical nephroureterectomy with bladder cuff excision (NUx) for UC from renal calyx to distal ureter on the oncological prognosis. Furthermore, the correlations of PTC with pathological parameters and perioperative blood transfusion (PBT) rates were analyzed.
Methods: A retrospective analysis of 101 patients undergoing NUx for UC between 2005 and 2019 was performed. For the cohort PTC was defined as a platelet count >450 G/. Chi‐square test was used to analyze the association of PTC with categorical variables including tumor stage, grade and PBT parameters. Cox regression analyses were used to investigate the association of PTC with outcome.
Results: The median age of patients at the moment of each operation was 68 years, 20.8% were female and 73.2% were male. The median PPC in the cohort was 271 G/l. PTC was detected in 29.67% of the patients. The median follow‐up was 49 months. The cancer specific survival adapted to PTC (thrombocytes: <450 G/l vs. >450 G/l) was 98.4% vs. 92.5% after 1 years and 92.1% vs. 12.2% after 5 years, respectively. PTC was significantly associated with muscle invasion, periureteral fat invasion and lymphovascular invasion (p < 0.001). PTC was also significantly associated with a higher rate of PBT (62.94% vs. 58.83%; p < 0.001). In the multivariate analysis PTC was significantly related to poor oncological survival (Hazard Ratio = 6.052; p = 0.008).
Conclusions: In this study, PTC was significantly associated with impaired oncological outcomes of patients undergoing NUx for UC. It represents an independent prognostic factor in oncological outcomes after NUx. PTC is also significantly correlated to an increased rate of PBT, which can be explained through tumor associated alterations of hemostasis.
Rate of Proliferation as Prognostic Marker in UTUC
C Malm, G Jaremko, M Brehmer
Karolinska Institutet. Stockholm South General Hospital
Introduction & Objective: Prognostic markers complementing tumor stage and grade for risk stratification and prediction of survival in UTUC are needed. We investigated rate of proliferation as predictor of invasiveness and disease‐specific survival (DSS). It can be analyzed in both barbotage and radical nephroureterectomy (rNU) specimens and is relatively inexpensive, objective and easy to secure peroperatively.
Methods: We included consecutive patients treated with rNU in two different hospitals in Stockholm between 2005‐2012 (n = 43) and 2005‐2013 (n = 72) respectively. All rNU specimens were re‐assessed by a single uropathologist. Rate of proliferation, measured as proportion of cells in S‐phase of the cell cycle, was analyzed using spectrophotometry flow cytometry, determining ploidy and rate of proliferation from paraffin‐embedded tissue blocks from the rNU specimens, 2011‐2014. The associations between S‐phase fraction and tumor grade (WHO 1999 and 2004), stage, overall survival (OS) and DSS were calculated.
Test of significance was performed using t‐test or Kruskal Wallis. Follow‐up time, OS and DSS were calculated. Receiver operating characteristics (ROC) and area under the curve (AUC) with 95 % confidence intervals were calculated for rate of proliferation in relation to stage and DSS, respectively. Patients with missing data in the reference standard (rNU specimen histopathology) were excluded. Patients with missing or indeterminate data in the index test were excluded in the analysis of that test (rate of proliferation), leaving 96 patients in the analysis of rate of proliferation.
Results: Proliferation rate was statistically significant different between stages (superficial or invasive), grades, ploidy and between patients that died of UTUC and those that did not. Risk of dying in UTUC increased with 17 % with every percent increase in rate of proliferation. Regarding both proliferation and DSS, CIS behaved more similar to superficial than high grade or invasive tumors.
Conclusions: AUC indicated that rate of proliferation was a good test both for predicting invasiveness and DSS and may be used as an add‐on test in conjunction with grading of barbotages and pathological anatomic diagnosis of biopsy or rNU specimens for risk stratification in UTUC.
Ureteroscopy Vs Radical Nephroureterectomy for low grade upper tract urothelial carcinoma
AY Lazarovich, AY Shvero, D Zillberman, E Fridman, M Laufer, Z Dotan, J Ramon, H Winkler, N Kleinmann
Sheba Tel‐Hashomer Medical Center
Introduction & Objective: In cases of upper tract urothelial carcinoma (UTUC) radical nephroureterectomy (RNU) is considered the standard treatment. However, in selective cases, Ureteroscopy (URS) with laser ablation is an appropriate alternative. Our goal is to compare the urological and oncological outcomes between URS treatment and RNU for low‐grade UTUC.
Methods: Medical records of patients who underwent URS treatment between 2014‐2018 and patients who underwent RNU between 1992‐2018 for low‐grade UTUC were reviewed. Data collected included: demographic data, clinical data, imaging, surgical and pathological findings, urological and oncological follow‐up (local recurrence, local progression, metastases, synchronous/metachronous bladder urothelial carcinoma). Univariate survival analysis, Wilcoxon (Breslow) was performed.
Results: This cohort included 59 patients, among them 42 (52% men) underwent URS and 17 underwent RNU (70.6% men). The mean tumor size (largest lesion) in the URS group was 17.5 mm versus 22.8 mm in the RNU group (p = 0.11). The median follow‐up in the URS group was 18 months (range 3‐60) versus 39 months (range 2‐264) in the RNU group. The mean creatinine elevation was lower after URS comparing to RNU, 0.05 and 0.37 respectively (p = 0.029). The mean decrease of glomerular filtration rate (GFR) was smaller in the URS group versus RNU: 1.93 and 18.1 respectively (p = 0.008). Local recurrence occurred in 64% of the cases in the URS group. No local recurrence was detected in the RNU group. New‐onset bladder urothelial carcinoma developed in 16.67% and 23.5% of the patients in the URS and RNU group, respectively. During the study period 1 patient in the RNU group developed metastatic progression, none of the patients in the URS group developed metastases. In a‐parametric survival analysis, no difference was found between the groups in time to metastatic progression (p = 0.42) and developing bladder urothelial carcinoma (p = 0.064). None of the patients has died from the disease during the study period.
Conclusions: URS is an attractive alternative to RNU in low‐grade UTUC, with no significant difference in oncological outcomes and with a significant advantage in preserving renal function.
Nephron sparing surgery in extreme cases of upper tract urothelial carcinoma
AY Lazarovich, AY Shvero, D Zillberman, M Laufer, Z Dotan, H Winkler, N Kleinmann
Sheba Tel‐Hashomer Medical Center
Introduction & Objective: Nephron sparing surgery for upper tract urothelial carcinoma (UTUC) is appropriate for size limited unifocal tumors. The objective of this study was to evaluate the surgical and oncological outcomes of endoscopic treatments for UTUC in extreme cases, who were referred to radical surgery in other institutions.
Methods: Medical records of patients who underwent endoscopic treatment for UTUC between 2013‐2019 were reviewed. We included low‐grade UTUC who were referred to radical nephroureterectomy (RNU) for tumors larger than 2 cm or in difficult to reach anatomic locations. We also included a subgroup of patients with imperative indications: single kidney, bilateral tumors, or advanced renal failure, who would have been dialysis‐dependent after RNU and were therefore treated endoscopically. We compared the oncologic outcomes of these cases with “standard” cases.
Results: Our cohort included 61 patients with low‐grade UTUC. The extreme cases group included 26 patients: 16 had high volume disease and 2 had difficult anatomic locations of the tumor. In addition, we included 4 patients with a tumor in a single kidney, 3 with bilateral tumors and one patient with chronic renal failure. The median tumor size in the extreme cases group was 15 mm (5‐40). The standard cases group included 35 patients, with a median tumor size of 15 mm (8‐20). The median follow‐up time was 16 months in both groups (3‐67). The local recurrence rate was 81% and 60% in the extreme and standard groups, respectively (p = 0.208). The mean time for recurrence was 6.3 and 9.4 months in the extreme and standard group, respectively. Histologic progression to high‐grade disease occurred in 1 patient in each group. There were no cases of local or metastatic progression or mortality from the disease.
Conclusions: Endoscopic treatment for low‐grade UTUC is feasible and safe also in extreme cases of low‐grade UTUC who were referred to RNU.
Skeletal muscle mass effects on estimated‐GFR decremant after donor nephrectomy
J Na, N Hong, M Yoon, Y Rhee, W Han
Yonsei University College of Medicine
Introduction & Objective: Estimated glomerular filtration rate(eGFR) based on serum creatinine is commonly used to follow the renal function of patients after nephrectomy. Although it is well known that skeletal muscle mass influences the level of serum creatinine, the effect of skeletal muscle mass on decreased renal function after acute nephron loss is not known. In this study we aimed to evaluate the effect of skeletal muscle mass on eGFR calculated by serum creatinine and cystatin C.
Methods: From our kidney donor database, 601 donors were randomly selected in even distribution across age and sex. Skeletal muscle area(SMA), skeletal muscle density(SMD) was extracted from the L3 level slice on predonation CT scan. Skeletal muscle index(SMI) was calculated by correcting SMA for height: SMA/height2. The association between the skeletal parameters and predonation eGFR derived from multiple methods, and with decreased eGFR ratio – calculated from serum creatinine and cystatin C ‐ at 6 month postdonation compared to predonation were analyzed by linear regression analysis.
Results: Among the selected donors skeletal muscle parameters were extracted from 592 donors. The skeletal muscle parameters were significantly different according to sex: SMA cm2 168.0 ± 23.1 vs 109.4 ± 13.8, SMD(Hounsfield Units, HU) 45.2 ± 5.2 vs 39.5 ± 6.0, and SMI cm2/m2 57.0 ± 7.2 vs 43.1 ± 5.1 (all p < 0.001). All skeletal parameters were significantly associated with age, sex and BMI. There was a significant correlation between predonation creatinine based eGFR and SMA and also SMI. No correlation was seen between skeletal muscle parameters and cystatin based eGFR or DTPA measured GFR (Table1). SMA and SMI had negative correlation with the %change of creatinine based eGFR at 6month post donation in male donors but not in female donors (Table2). The association of %change of cystatin C based eGFR with all skeletal muscle parameters were not significant. (Figure1)
Conclusions: Male kidney donors with high SMA or SMI are more likely to have decreased creatinine based eGFR after donation. However as this is not seen in cystatin C based eGFR this phenomenon is more likely associated with skeletal muscle mass rather than a reflection of true decrease in GFR. Cystatin C based eGFR may reflect postdonation GFR more accurately in muscular male donors.
The use of ureteral access sheath does not modify the pattern of disease recurrence during conservative management of upper tract urothelial carcinoma
E Ventimiglia, C Corsini, P Dioni, O Traxer, F Montorsi, A Salonia, L Villa, S Proietti
Division of Experimental Oncology/Unit of Urology; URI; IRCCS Ospedale San Raffaele
Introduction & Objective: The use of ureteral access sheath (UAS) during ureteroscopy for conservative management of upper tract urothelial carcinoma (UTUC) has been advocated as beneficial in order to prevent cancer recurrence both in the bladder and the upper urinary tract. However, there is no clear evidence at this regard. We aimed at assessing whether the use of UAS in this setting is able to prevent UTUC recurrence during follow‐up ureteroscopy.
Methods: Data from 102 consecutive ureteroscopies performed for UTUC at a single academic center between 2015 and 2020 were included in this analysis. Two experienced endo‐urologists performed all the procedures. Ureteroscopies were performed using a digital flexible ureterorenoscope (Flex XC, Karl‐Storz). Tumor Ho:YAG laser ablation was performed in every case whenever feasible (VersaPulse PowerSuite 100W, Lumenis) using 1J and 10 Hz. The use of 10/12 UAS (ReTrace, Porges‐Coloplast) was attempted whenever there was no evidence of disease in the ureter according to surgeon's preference. Multivariable logistic regression models tested the association between use of UAS and cancer recurrence at follow‐up ureteroscopy both in the upper tract and the bladder, accounting for possible differences in terms of age, tumor size and grade.
Results: Ureteral access sheath was used in 21 (21%) cases. There were not significant differences in terms of patients and tumor characteristics between cases performed with and without UAS (all p > 0.05). During follow‐up ureteroscopies, evidence for upper tract and bladder recurrence were found in 52/77 (68%) and 18/77 (23%) cases, respectively. The use of UAS was not associated with a decreased probability of cancer recurrence in the upper tract (OR, 1.22 [95% CIs: 0.44‐3.43], p > 0.05) and in the bladder (OR 1.76 [0.87‐1.56], p > 0.05) after accounting for tumor size, grade, and patient age.
Conclusions: The use of UAS does not seem to prevent the UTUC recurrence during endoscopic follow‐up. Both upper urinary tract and bladder recurrence pattern are not modified by the use of UAS.
How long should you wait in‐between follow‐up ureteroscopies during conservative management of upper‐tract urothelial carcinoma?
E Ventimiglia, F Montorsi, A Salonia, O Traxer, L Villa
Division of Experimental Oncology/Unit of Urology; URI; IRCCS Ospedale San Raffaele
Introduction & Objective: Flexible ureteroscopy is the main player during conservative management of upper tract urothelial carcinoma (UTUC). However, it is not clear what should be the proper endoscopic follow‐up strategy in patients with UTUC, especially in terms of timing between two consecutive endoscopic procedures. We aimed at the determining the best follow‐up strategy, defined as the one which minimize the risk of cancer progression.
Methods: Data from 140 consecutive ureteroscopies (n = 36 patients) performed for UTUC at a single academic center between 2015 and 2020 were included in this analysis. Two experienced endo‐urologists performed all the procedures. Ureteroscopies were performed using a digital flexible ureterorenoscope (Flex XC, Karl‐Storz). Tumor Ho:YAG laser ablation was performed in any case whenever feasible (VersaPulse PowerSuite 100W, Lumenis) using 1J and 10 Hz. Patients with high grade UTUC at initial diagnostic biopsy and managed conservatively due to imperative indications were included in the analysis. For each patient, we estimated the average interval between two consecutive ureteroscopic procedures (fURSint) until last follow‐up date. Multivariable Cox regression analysis estimated the association between fURSint and risk of cancer progression, accounting for patient age, tumor size and grade. Moreover, we analysed the graphical association (LOWESS curve) between fURSint and the multivariable adjusted probability of progression‐free survival, in order to identify possible non‐linear trends for both low‐ and high‐grade UTUC.
Results: Median (IQR) patient age and follow‐up time were respectively 70 (66‐79) years and 14 (6‐31) months. Median (IQR) fURSint was 3.4 (2‐5.6) months. Disease progression occurred in 11 (31%) patients and was classified as systemic in 4 (11%). At multivariable Cox regression analysis, longer fURSint was associated to reduced progression‐free survival (HR [95% CIs] 0.32 [0.19‐0.54]). A longer fURSint was more detrimental in men with high‐grade UTUC, especially when it was longer than 3 months (Figure 1).
Conclusions: A long fURSint should be avoided in men under endoscopic follow‐up for conservative management of UTUC. In men with high‐grade UTUC and imperative indications for endoscopic follow‐up, fURSint longer than 3 months is associated to poor prognosis.
Withdrawn
Comprehensive analysis of early outcomes in radical nephrectomy with Inferior Venacava thrombectomy ‐ a seven year single center experience
M Thangarasu, S Jayaprakash, T Ganesan, B Venugopal, N Ragavan, A Balakrishnan, D Raghavan, N Jain
Apollo Main Hospitals, Chennai, Tamil Nadu, India
Introduction & Objective: Renal cell carcinoma( RCC) accounts to 2‐3 % of all malignancies, among which 3‐4% of RCC has tumour thrombus extension into Inferior Vena Cava (IVC) and 1 % has extension of tumour thrombus into right atrium. We present a 7 year, single institution experience during which we have managed 36 cases of RCC with IVC thrombus with radical nephrectomy along with IVC thrombectomy.
Methods: We did a retrospective analysis of all patients who underwent radical nephrectomy along with IVC thrombectomy by a dedicated urology , vascular surgery and cardiothoracic surgery team, from the year 2013 to 2020. Mayo's classification was used to classify level of IVC thrombus. We collected demographic data, presenting symptoms , intra‐operative and perioperative details, histopathology, complications and overall survival status.
Results: Total number of patients included in the study were 36, out of which 30 (83.3%) of them were males. Mean age of patients were 55.2 +/‐8.8 years. The mean size of renal tumour was 10+/‐ 3.5 cms, 9.7 +/‐ 3.5 cms, 10+/‐ 5.9 cms and 9.5+/‐2.1 cms (p = 0.998) and the mean operating time was 2.8 +/‐0.3 hours, 4.6 +/‐ 2.1hours, 4.4+/‐ 1.1hours and 10.2+/‐2.6 hours (p = 0.0001) for level 1,2,3, and 4 tumours respectively. There was a significant difference in the amount of blood loss between the different levels, (p = 0.043) but post‐hoc analysis showed, there was no significant difference between level 3 and 4 tumours (p = 0.656). Histopathology revealed Clear cell variants in 25 patients( 69%). The overall mean survival time was 66 months with 95% Confidence interval of 53‐78 months. Kaplan‐Meier survival analysis and Log rank test showed there was a significant difference in survival,(p = 0.002) between different levels of thrombus. The mean Body mass index was very low in patients who died (19+/‐1.3) which was significant. The hospital stay was more in level 3 and 4 patients, but were not statistically significant (p = 0.112). The death rate was 11%, 16%, 66% in level 2,3 and 4 tumours respectively which was not statistically significant (p = 0.094). Overall mortality rate was 16.6% in this study.
Conclusions: RCC with IVC thrombus needs radical nephrectomy with IVC thrombectomy, which is a technically demanding procedure, needing multi‐speciality collaboration and a well equipped critical care unit is a necessity to improve morbidity and mortality. There was a significant difference in survival between different levels of thrombus with high mortality in level 4 tumours. The tumor size doesn't have an influence on the progression of tumour thrombus into IVC. Further prospective randomised trial to study the disease free survival are required in patients who receive chemotherapy.
Utility of cognitive targeted transrectal ultrasound biopsy for prostate cancer detection in financially constrained hospitals
M Thangarasu, S Jayaprakash, A Balakrishnan, A Sivaraman
Apollo Main Hospitals, Chennai, Tamil Nadu, India
Introduction & Objective: To evaluate the impact of cognitive targeted transrectal ultrasound prostate biopsy using MpMRI data in diagnosing clinically significant prostate cancer, in biopsy naive men in resource constrained countries.
Methods: In this single institutional prospective study, data of 115 biopsy naïve men were analysed from September 2018 to March 2020. MpMRI Cognitive Target Biopsy[MpMRI CTB] followed by Standard Biopsy [SB] were done in the patients with 3,4 and 5 PIRADS scores, in the same sitting by two different Urologists. Diagnostic yield of biopsy cores, complications, and stage migration of Gleason's grades was analyzed.
Results: Out of 115 patients, 34.57% had abnormal DRE, and the median serum PSA was 10.6 [4.5 – 20] ng/ml. Total MRI suspicious lesions were 249. Out of 1840 SB cores, 540 cores were positive for cancer [29.37%], and out of 498 MpMRI CTB cores, 184 were positive for cancer [36.78%]. [P < 0.0001]. HPE revealed 88%, 92%, and 100% clinically significant cancers in PIRADS 3,4 and 5 lesions. Cancer detection yield is better when SB and MPMRI CTB are combined, than either of the modality when used alone,[P‐< 0.0001]. Clavien‐Dindo grade 1 and grade 4a complication was seen in 72 [62.6%] and five [4%] patients.
Conclusions: By addition of pre‐biopsy MPMRI in biopsy‐naive men with suspected prostate cancer and equivocal DRE, more people with clinically significant prostate cancer can be detected than when compared with SB alone. Combining SB with MpMRI CTB has a superior diagnosing ability when compared with either of the biopsy modality when used alone. MpMRI CTB can be used in resource constrained hospitals till fusion biopsy is available without a drastic compromise on quality yield of diagnosis.
Dioscin promotes prostate cancer cell apoptosis and inhibits cell invasion by increasing SHP1 phosphorylation and suppressing subsequent MAPK signaling pathway
S He, Y Wei, J Yang
Introduction & Objective: Dioscin has anti‐oxidant effect and has shown anti‐cancer ability in many solid tumors, including prostate cancer (PCa). However, the role and mechanism of dioscin in are rarely analyzed and have not yet been fully elucidated. Protein tyrosine phosphatase SHP1 containing an oxidation‐sensitive domain, has been confirmed as a target for anticancer treatment. Herein, whether dioscin activates SHP1 to inhibit PCa and its potential subsequent signaling pathway were studied.
Methods: Two cell lines, one androgen‐sensitive (LNCaP) and one androgen‐independent (LNCaP‐C81), were used in vitro and in vivo studies. Western blot was used to detect phosphorylation of mitogen‐activated protein kinases (MAPKs), Caspase‐3 and Bad. The anticancer effects and possible mechanisms of dioscin were analyzed after the cells given two drug administration, interleukin‐6 (IL‐6) and dihydrotestosterone (DHT), respectively.
Results: Our results showed IL‐6 or DHT significantly inhibited p‐SHP1(Y536), and phosphorylation of subsequent proteins, p‐Erk1/2(Thr202/Tyr204), p‐P38(Tyr182) or p‐P38(Tyr180). While dioscin could inhibit cell growth and invasion by increasing the expression of p‐SHP1(Y536) and inhibiting phosphorylation of MAPK signaling pathway. Further study of in vivo confirmed these results and found dioscin promoted Caspase‐3 and Bad‐related cell apoptosis.
Conclusions: Our study suggests that dioscin may have potential anticancer effects on advanced PCa. These anticancer effect by dioscin may be due to its effect on increase of SHP1 phosphorylation and inhibiting subsequent MAPK signaling pathway.
Oncological and Functional Outcomes after Salvage Prostate Cryotherapy for the Management of Primary Brachytherapy versus Cryotherapy Failures: A Propensity Score Matched Comparison
H Orabi, A El‐Shafei, A Aminsharifi, L Gerber, Y Wu, T Polascik
Duke University Medical Center, Department of Urology
Introduction & Objective: To compare the outcome of prostate cryotherapy as a salvage modality for treatment of primary brachytherapy versus cryotherapy failure for localized prostate cancer.
Methods: Following IRB approval, we queried the Cryo‐On‐Line Database (COLD) registry and the Duke prostate cancer database for men treated with salvage cryotherapy (SC) following treatment failure of primary brachytherapy (group A = 113) vs primary cryotherapy (group B = 81). Biochemical recurrence (BCR) using Phoenix criteria was the primary endpoint assessed at 2‐ & 5‐years post SC. Secondary endpoints assessed functional outcomes including 12‐month urinary incontinence, rate of effective intercourse; recto‐urethral fistula and urinary retention. We estimated the association between treatment and biochemical progression‐free survival (BPFS) using inverse probability weighted (IPTW) Cox proportional hazards regression. Propensity score analysis, adjusting for Gleason, risk, and PSA, was implemented to account for non‐random assignment of primary treatment. To test for differences in the secondary functional outcomes between treatment modalities, we used Pearson's χ2 test or Fishers exact test, corrected for IPTW.
Results: 194 unweighted subjects were included who had complete data for the primary analysis. There was no statistical difference in 2‐year BCR (HR 0.9; 95% CI, 0.5–1.7) or 5‐year BCR (HR: 0.86; 95% CI, 0.5‐1.5) between the 2 groups (Figure 1). There was no statistical difference between the 2 groups regarding the adverse functional outcomes, although the incidence of incontinence and urinary retention was higher in group A than in group B.
Conclusions: Salvage cryotherapy after failed primary cryoablation and failed primary brachytherapy has similar oncological and functional outcomes, except salvage cryotherapy after primary cryotherapy had a lower rate of retention and incontinence. This information should be considered when selecting primary in‐situ organ‐preserving therapy for prostate cancer. Additional work with larger numbers of patients is needed to further validate these results with longer follow‐up.
A matched analysis of salvage robot assisted radical prostatectomy following focal ablation vs radical robotic assisted radical prostatectomy
S Bhat, M Covas Moschovas, J Noël, S Reddy, T Rogers, V Patel
Global robotics institute
Introduction & Objective: Focal therapy for prostate cancer has gained popularity given its relative noninvasiveness. We evaluated the impact of focal therapy on functional and oncological outcomes following RARP
Methods: 53 patients who had prostatectomy following the failure of focal ablation were selected as the primary group. The patients who had whole gland ablation and external beam therapy were excluded. They were then compared to a matched control sample of the ratio of 1:1 with the RARP cohort. Age, PSA, PSA density, BMI, SHIM, AUA, Charlson Comorbidity Index, Prostate weight, Preoperative Gleason score, and history of Smoking were used to perform matching. The oncological and functional outcomes between these groups were compared.
Results: No difference in EBL and OR time was noted between the focal and control group. More full NS and partial NS were performed in the control group compared to the focal group (p < 0.001). The focal therapy group had a higher incidence of positive surgical margin (35.8% vs 15.1%, p = 0.04). Also, the focal therapy group had higher incidence of GS > = 8 ( 28.3% vs 17%, p = 0.07) and positive lymph node status ( 73.5% vs 9.4%, p = 0.02). The primary RALP group had a higher incidence of lymphocele drainage post‐surgery (15.1 vs 0, p = 0.006).
Fig 1 shows CIF comparing the continence, potency, and biochemical recurrence in 1:1.
Conclusions: Salvage robotic‐assisted radical prostatectomy after focal therapy failure is feasible however, surgery following focal therapy causes nonfocal damage resulting in poorer functional outcomes. Focal therapy may also delay more definitive care leading to more advanced disease at RALP.
Management of upper tract urothelial carcinoma (UTUC) in patients with urinary diversion ‐ the 14Fr antegrade supermini approach
T Reid, S huq, E Edison, N de Luyk, R Vitale, C Allen, S Choong, R Hubbard
Department of Urology, University College London Hospital
Introduction & Objective: Upper tract urothelial carcinoma (UTUC) represents around 5% of urothelial cancers, with a rising incidence in the last decade. Improved percutaneous access using smaller tracts has led to an increased reliance on antegrade intervention in patients with complex urinary tract anatomy. We report on our experience of antegrade management of UTUC via 14Fr supermini percutaneous access (SMP).
Methods: Retrospective data collection was performed between 2016 and 2021. Patient factors, such as significant comorbidity and complex urinary tract anatomy, were identified and operative steps have been detailed. Length of stay (LoS), post‐operative biochemical parameters and complications have been summarised. Tumour characteristics and requirement for subsequent intervention have been addressed.
Results: Five patients underwent 14Fr antegrade SMP for UTUC (six procedures in total). All patients had urinary diversion due to previous lower tract urothelial carcinoma. Mean BMI was 26.01 and mean ASA 2.2. All patients had nephrostomies for drainage. 80 % of patients were discharged on postoperative day one or two. Average drop in haemoglobin was 13.17 g/L and all patients had preservation of renal function. Tumours were multifocal in 83.3 % and 40 % were low‐grade. Two patients continued with long‐term endoscopic management. Of the three patients who subsequently had radical nephroureterectomies, two had upstaging of their tumours.
Conclusions: Antegrade 14Fr SMP is an effective procedure for managing UTUC in patients with urinary diversion, allowing short LoS and low incidence of complications. It should be considered as an option for patients where retrograde access may not be possible.
Prevention of Bladder Recurrence with Intraoperative Gemcitabine Instillation Following Bladder Closure During Radical Nephroureterectomy
M Said, H Warner, V Packiam, CR Tracy, P Gellhaus
Introduction & Objective: Bladder recurrence (BR) after nephroureterectomy (RNU) common. Prophylactic instillation of intravesical mitomycin can reduce recurrence. Recently, gemcitabine has been shown to be safer and more effective at reducing tumors recurrence after TURBT. Extrapolating from the TURBT findings, we sought to evaluate the efficacy and safety of single, intraoperative gemcitabine instillation following bladder cuff closure during RNU.
Methods: We retrospectively reviewed all patients undergoing RNU (2016‐2020) and received 2 g gemcitabine IVC immediately following bladder cuff closure or received non‐gemcitabine chemotherapy (40 mg mitomycin C or 50 mg adriamycin) at the beginning of the procedure. The procedure was predominantly performed with the da Vinci Xi robot. Recurrence rates were evaluated using the Kaplan‐Meier curves and log‐rank test.
Results: At the time of RNU 22 patients received gemcitabine IVC and 29 patients received non‐gemcitabine chemotherapy. Over a median follow up of 12 months, 18% (4/22) of patients receiving gemcitabine chemotherapy and 38% (11/29) of patients receiving non‐gemcitabine chemotherapy experienced intravesical recurrence. Using the log‐rank test, estimated recurrence free survival did not differ between patient cohorts (p = 0.75). No adverse events potentially related to gemcitabine chemotherapy were noted within 30 days postoperatively.
Conclusions: Gemcitabine instilled immediately following bladder cuff closure appeared safe and without significant changes in bladder recurrence‐free survival compared to non‐gemcitabine chemotherapy.
Irreversible Electroporation for the Treatment of Small Renal Masses: 5‐Year Outcomes
JC Dai, TN Morgan, RL Steinberg, BA Johnson, A Garbens, H Kominsky, JA Cadeddu
UT Southwestern
Introduction & Objective: Irreversible electroporation (IRE) is a nonthermal ablative technology that applies high voltage, short pulse electrical current to create cellular membrane nanopores and ultimately resulting in apoptosis. This is thought to overcome thermal limitations of other ablative technologies. We report 5‐year oncologic outcomes of percutaneous IRE for small renal masses.
Results: IRE was used to treat 48 tumors in 47 patients. 22/48 tumors (45.8%) were biopsy‐confirmed renal cell carcinoma (RCC). No complications ≥ Clavien Grade III occurred and 36 patients (76.6%) were discharged the same day. Initial treatment success rate was 91.7% (n = 44/48); 3 treatment failures were managed with salvage radiofrequency ablation and 1 with robotic partial nephrectomy. Median follow up was 50.4‐months (IQR 29.0‐65.5). For biopsy‐confirmed RCC patients, 5‐year local recurrence‐free survival was 81.4%, 5‐year metastasis‐free survival was 93.3%, and 5‐year overall survival was 92.3% (Table 1). For all patients, local‐recurrence free survival, metastasis‐free survival, and overall survival at 5 years was 81.0%, 97.1%, and 90.6%, respectively. 81.4% in biopsy‐confirmed RCC patients (Table 1) and 81.0% in all patients. 5‐year metastasis‐free survival was 93.3% and 97.1%, respectively. 5‐year cancer‐specific survival was 100% for both biopsy‐confirmed RCC and all patient groups.
Conclusions: IRE has low morbidity, but suboptimal intermediate‐term oncologic outcomes compared to conventional thermal ablation techniques for small, low complexity tumors. Use of IRE should be restricted to select cases.
A systematic review of the use of non‐HPV biomarkers in penile squamous cell carcinoma
JA Bowie, S Singh, C O'Hanlon, O Brunckhorst, A Muneer, K Ahmed
King's College London
Introduction & Objective: The presence of lymph node metastasis (LNM) is the most important prognostic indicator for patients with penile squamous cell carcinoma (SCC). However, predicting which patients would benefit most from prophylactic lymphadenectomy is challenging. The use of Human Papilloma Virus (HPV) and its surrogate biomarker, P16INK4A, has been researched extensively, but there are other, lesser known biomarkers available which show promise in predicting outcomes. The aim of this systematic review is to provide an overview of the biomarkers p53, Ki‐67 and SCCAg in predicting LNM and cancer‐specific survival (CSS) in penile SCC.
Methods: MEDLINE, EMBASE, Cochrane Library, Scopus and ClinicalTrials.gov were searched from inception until 15 October 2020. Eligible studies were identified by 3 independent reviewers. Outcome measures included the presence of penile LNM and CSS. Extracted data was synthesised narratively following the Synthesis without Meta‐analysis reporting guidelines, with GRADE criteria utilised to evaluate the quality of the evidence. The Newcastle‐Ottawa Quality Assessment Scale for Cohort Studies was used to assess risk of bias, resulting in an AHRQ rating of ‘good’, ‘fair’, or ‘poor’. Due to the paucity of studies in the field, those with an AHRQ rating of ‘poor’ were included in this review.
Results: 999 articles were screened, with 20 selected for inclusion. Studies reporting the use of p53 to predict LNM and CSS were rated as having the highest quality of evidence using the GRADE criteria. The majority of papers identified showed a significant relationship between p53 expression and either LNM or CSS, with calculations of relative risk for LNM ranging from 1.04 – 266.4, and hazard ratios for CSS ranging from 3.20 – 15.28. All biomarker and outcome combinations had at least one study showing a significant effect on predicting the outcome. However, studies were heterogeneous: there was extensive variation in thresholds used to define overexpression of biomarkers, differences in end points used to define cancer‐specific survival, and many studies only used univariate statistical analysis.
Conclusions: A good basis of evidence exists for the relationship between p53 expression and LNM in penile SCC, suggesting this may be a useful adjunct as a predictive marker in this cohort. This has the potential to aid decision making for early inguinal lymphadenectomy in the difficult to treat clinically node negative subgroup. There is contradictory and unreliable evidence for the prognostic value of Ki‐67 and SCCAg in penile SCC for LNM and CSS. Larger, prospective studies are required with more rigorous methods and reporting to improve the evidence base.
Salvage Peri‐Rectal Mass Resection of Locally Recurrent Prostate Cancer after Radical Prostatectomy Delays the Need for Systemic Intervention
E Huang, K Liang, LM Huynh, W Zhang, TE Ahlering
University of California, Irvine
Introduction & Objective: Previously, we published an initial case series on salvage pelvic mass resections (sPMR) as a novel intervention following radical prostatectomy (RP) for local recurrent prostate cancer (PCa). In our experience, approximately 31% of our biochemical recurrences (BCR) occur in the extranodal peri‐rectal site. Common secondary treatments, such as radiation and hormonal therapy can negatively affect patients' quality of life (QOL). This case study update continues to show sPMR of local recurrent prostate cancer as an efficacious secondary intervention to delay the need for systemic treatments by slowing PSA progression.
Methods: Following RP, 87 patients underwent 68 Gallium PSMA/PET CT scan, of which 20 (31.25%) demonstrated radiographic evidence of localized prostate bed recurrence. Subsequently, a digital rectal exam was performed to confirm the presence of the pelvic mass recurrence. Of these patients, eight patients (40%) underwent open or laparoscopic trans‐anal excision of the tumor, performed by either a urologic surgeon or colorectal surgeon. Primary outcome evaluated was PSA progression, and secondary outcome evaluated was need for secondary intervention.
Results: All surgeries were completed outpatient without complications, and patients were discharged with <24 hour hospitalization with <1 week recovery time. Overall, PSA decreased by mean of 80.2% at 19.23(±10.59) mos following sPMR. Of the eight patients undergoing sPMR, 2/8 (25%) patients have undetectable PSA's at 24 and 6 months post‐sPMR. 4/8 (50%) patients have a slow rise in PSA, with no secondary treatment. 2/8 (25%) patients have a delayed rise in PSA with secondary treatment: one underwent a second sPMR after 30 months, and another began hormonal therapy 4 months post‐sPMR.
Conclusions: This updated feasibility case series confirms the utility of PSMA/PET scan imaging and subsequent intervention of dissection of pelvic mass recurrence by delaying PSA progression. sPMR continues to show that it can delay, and in some cases eliminate, the need for systemic intervention post‐radical prostatectomy. Further follow‐up is needed to confirm how long systemic treatments can be delayed.
Documentation of Nephrometry Scores for cT1 Renal Masses Correlates with Avoidance of Radical Nephrectomy Across the MUSIC‐KIDNEY Statewide QI Collaborative
S Perkins, A Patel, M Butaney, A Johnson, J Qi, C Rogers, B Lane, f Urological Surgery Improvement Collaborative
Henry Ford Health System
Introduction & Objective: Tumor complexity (TC) assessment with nephrometry scoring has been shown to help with identification of case complexity and contribute to preoperative planning. Our objective was to assess documentation of TC and its association with performance of radical nephrectomy (RN) for tumors
Methods: The Michigan Urological Surgery Improvement Collaborative ‐ Kidney mass: Identifying and Defining Necessary Evaluation and therapY (MUSICKIDNEY) program commenced data collection in September 2017. Data abstractors recorded clinical, radiographic, pathologic, and short‐term follow‐up data for patients with newly‐diagnosed T1 RM at 13 diverse practices with 45 physicians treating cT1RM. An educational session was conducted in Nov 2018 regarding documentation of Nephrometry scoring (RENAL Score) by the Urologist in clinic (rather than solely relying on radiology reports). Correlation coefficient was calculated for the rates of nephrometry documentation for cT1RM and percent of RN performed by urologists (with volume >10 cases).
Results: A total of 1527 patients with cT1RM were seen by 32 urologists and documentation of TC was performed in 40% (IQR 10.1‐44.4%). Overall, management of cT1RM was 52% surveillance, 31% PN/TA, and 15% RN and 2.5% other. Of the 637 surgical patients, RN rates for T1b were 65% (154/236) and for T1a were 18% (74/401) (p < 0.001). Rates of RN for cT1aRM ranged from 4%‐45% among 19 urologists. 42% of RN for cT1aRM had no documentation of TC. The lowest 5 surgeons documented TC for only 4.4% and performed RN for 25%, while the top 5 surgeons documented TC for 74% and performed RN on only 15%. At surgeon level, the correlation coefficient between rates of RENAL documentation and the rates of RN was ‐0.24 (Figure 1).
Conclusions: TC assessment with nephrometry scoring throughout our collaborative is an ongoing focus for QI, particularly as it appears to correlate with reduced rates of RN for cT1aRM. There are surely multiple factors that impact the decision to perform a RN for a cT1aRM, and we hope to be gaining traction regionally to help spare every kidney possible. Both improving documentation of TC and reducing RN for cT1aRM are QI goals we aim to address with ongoing initiatives.
Effect of Surgical Approach on Risk of Post‐Operative Renal Failure in Radical Nephrectomy and Nephroureterectomy: a validated risk model and propensity score matching
AA Nasrallah, C Gharios, M Itani, D Bacha, H Tamim, A El Hajj
Department of Surgery, Division of Urology. American University of Beirut Medical Center
Introduction & Objective: Radical nephrectomy (RN) and nephroureterectomy (RNU) and the gold‐standard surgical management for advanced‐stage kidney cancers. Post‐operative renal failure (PORF) is a significant morbidity associated with these procedures, and is a potent risk factor development of chronic kidney insufficiency and mortality. The authors aim to construct and validate a risk prediction model for PORF, and assess the influence of open versus minimally‐invasive surgery (MIS).
Methods: Patients were identified using the American College of Surgeons National Surgical Quality Improvement Program database (ACS‐NSQIP) from years 2005‐2014; exclusion criteria were transplant donor/recipient status, disseminated cancer, and acute preoperative renal injury or need for dialysis. Multivariate logistic regression was performed, model performance and calibration were tested by a ROC analysis and the Hosmer‐Lemeshow goodness of fit test, and validation with an independent cohort was performed. Propensity score matching (PSM) was performed between open and MIS groups.
Results: A total of 14,519 patients were included, of which 296 (2.0%) developed PORF. Multivariate logistic regression produced a 9‐factor model (Table 1) and included: age, gender, diabetes, hypertension, BMI, creatinine, hematocrit, platelet count, and surgical approach. Model ROC analysis (Figure 1) yielded a C‐Statistic of 0.79 (95% CI: 0.77, 0.82) and calibration R2 was 0.99. Validation with the independent cohort showed a C‐statistic of 0.79 (95% CI: 0.76, 0.81). The adjusted odds ratio for Open vs MIS was 2.24, 1.96, and 2.00 in the original cohort, validation cohort, and PSM analysis respectively.
Conclusions: The authors propose a robust and validated risk‐prediction model for PORF in RN/RNU patients, and demonstrate the significant effect of open versus minimally‐invasive surgery on the risk of PORF incidence. These findings can aid in optimization of perioperative management of high‐risk patients, to avoid the short‐ and long‐term consequences of PORF.
Radiofrequency and hyperthermia appear to have limited effect on bladder cancer cell viability and membrane permeability in vitro
JW van Hattum, IS Brummelhuis, EM Scutigliani, A Lev, JR Oddens, R Zweije, J Crezee, PM Krawczyk, E Oosterwijk, TM de Reijke, JA Witjes
Department of Urology, Amsterdam University Medical Centers, University of Amsterdam
Introduction & Objective: Chemohyperthemia (CHT), intravesical chemotherapy instillations at ±43°C, can be offered to patients with non‐muscle invasive bladder cancer (NMIBC). Radiofrequency (RF) or conductive heating (CO‐HT) can be used to achieve the desired temperature and RF is suggested to have advantages over CO‐HT due to additional non‐thermic effects. This study investigated the effect of RF and CO‐HT at 37°C and 43°C on bladder cancer cell viability and cell membrane permeability in vitro.
Methods: 3 NMIBC cells lines (T24, J82, RT4) and 1 benign smooth muscle cell line (hbSMC) were treated with or without IC50 mitomycin‐c (MMC) or epirubicin (EPI) for 1 hour while exposed to RF at 37°, RF at 42‐45°C (RF‐HT), CO‐HT at 43°C or control at 37°C (NT). A clinically applied antenna induced RF at 915MHz using 58Watt while the temperature was controlled with a thermostatic water bath. Viability was assessed 48 hours post‐treatment with a MTT assay. Membrane permeabilization in T24 cells was assessed by adding fluorescent propidium iodide (PI) to abovementioned treatment conditions and quantifying fluorescent intensity with flow cytometry. Additionally, fluorescence intensity caused by EPI was measured to assess EPI uptake. One‐way ANOVA was used to determine statistical significance.
Results: MMC and EPI decreased overall cell viability (figure 1). The combination of RF‐HT and EPI further decreased cell viability with 21% in T24 (p = 0.03) and 13% in J82 (p = 0.11). Single modality treatment of RF, CO‐HT and RF‐HT did not influence cell viability. CO‐HT alone and with MMC or EPI increased fluorescent intensity 1.48, 1.48 and 2.73‐fold compared with NT, MMC and EPI at 37°C, respectively. RF‐HT combined with EPI increased fluorescence 1.57‐fold compared to EPI at 37°C. Additional analyses showed increased intracellular EPI uptake after CO‐HT and RF‐HT compared to EPI at 37°C.
Conclusions: RF‐HT may further decrease cell viability when combined with EPI, possibly by increasing cell membrane permeability and increased EPI uptake. The difference between the limited treatment efficacy of CHT in vitro compared to greater reported clinical efficacy may be attributed to a possible immune response after CHT in vivo as opposed to direct cytotoxicity.
Clinical value of patient‐specific three‐dimensional printing of kidney before partial nephrectomy: Qualitative and quantitative assessments
R Nayyar, K Sharma, c Das, P Singh, B Nayak, A Seth
AIIMS
Introduction & Objective: To determine the role of patient‐specific 3D model of kidney before partial nephrectomy in complex renal tumours.
Methods: 13 3D models were printed for tumors having RENAL nephrometry score of ≥8. The DICOM data from triple phase CT abdomen (done within 2‐30 days of surgery) was converted to stereolithography (STL) data format and fed into a multijet multimaterial colour 3D printer to recreate high fidelity interactive real‐like model showing renal parenchyma, tumour, arteries and veins. The parenchyma was kept translucent to allow appreciation of internal expanse of the tumour and its relation with sinus vasculature and pelvicalyceal system. Options of cutting the model before surgery or using the sterilized model on‐table during surgery were available. All the surgeries were done by experienced surgeons. A questionnaire regarding realistic resemblance of model to actual surgical findings, impact on surgery and overall judgment of its usefulness was filled by the surgeon with each answer numbered 1 to 10 on a Likert scale.
Results: Mean RENAL score was 9.15 (8 to 11), tumor size was 44 (Range: 30 to 58) mm and warm ischemia time was 24.25 (Range: 15 to 35) minutes. Models were rated high (9.07 ± 0.86) for realistic resemblance domain (Table 1) and were rated better than CECT (8.38 ± 1.19) and intra‐operative ultrasound (8.07 ± 1.26) for orientation regarding resection margins. A further marginal improvement to 8.2 ± 0.84 was noted against ultrasound where surgeon did a dry cut pre‐operatively. Use of super‐selective arterial approach in 4; precise awareness about dissection of a major vessel in 4; retroperitoneoscopic approach in 1, and; surgical margin awareness in 3 were directly attributed to the model. Overall utility of having a model printed was rated high (8.23 ± 1.3).
Conclusions: The 3D print models of complex renal tumors have high realistic resemblance to actual patient's anatomy. They were rated better than pre‐operative CECT or intra‐operative ultrasound for orientation regarding surgical resection margins. It may also help change or modify the surgical plan in a subset of patients with a potential to improve overall outcomes in these complex cases.
Does Taping the Patient to the OR Table During Minimally Invasive Surgery Increase the Risk of Pressure Related Complications?
M Keheila, JD Belle, L Burke, AS Amasyali, M Hajiha, DD Baldwin, G Martin, B Yi
Loma Linda University, School of Medicine
Introduction & Objective: Rhabdomyolysis and neuropraxia are potential complications of positioning for minimally invasive surgical procedures. Patients in the modified lateral decubitus position utilized for laparoscopic renal surgery are routinely secured to the bed with tape to allow tilting to near supine and lateral decubitus positions. The effect of this taping upon effective patient weight and subsequent risk of rhabdomyolysis and neuropraxia has not been determined. The purpose of this study is to determine the effect of taping upon effective patient weight and subjective comfort.
Methods: A prospective, randomized study employed 30 subjects (14 male, 16 female) positioned in 45‐degree modified right lateral decubitus position and secured to the bed using 3” cloth tape in a manner identical to laparoscopic and robotic renal surgery in our institution. Subjects were positioned in modified lateral decubitus (45 degrees) with and without tape, supine (0 degrees) with tape, and right lateral decubitus (90 degrees) with tape (in reference to the floor; Figure 1). An XSENSOR Bluetooth high‐accuracy pressure sensor was used to record contact pressures under the upper body. In addition, subjects rated their breathing and overall comfort on a Likert scale (1‐10; 10 most comfortable). Data analysis was performed using ANOVA and Mann‐Whitney U‐tests. Significance was set at p < 0.05.
Results: After taping, the average baseline pressure (0.41 psi) of all subjects increased by 12.3%, 12.2%, and 9.5%, in the 0, 45, and 90 degree positions respectively. Taping increased the pressure more in patients with BMI >25 (0.50 psi) compared to those with BMI <25 (0.44 psi; p = 0.011). The angle of tilt (0, 45 or 90) did not significantly alter the pressure following taping. Taping had no effect upon overall comfort score, but significantly decreased breathing comfort (9.3 vs. 9.9; p < 0.05).
Conclusions: This study demonstrates that taping substantially increases the patient's effective weight and may subsequently increase the risk of rhabdomyolysis and neuropraxia. Future studies should develop taping strategies that do not increase the effective patient weight or alternative methods for securing the patient to the bed.
Black Light Illumination Improves Speed and Accuracy of Foot Pedal Activation Without Compromising Dark Adaptation
M Keheila, JD Belle, H You, J Maldonado, A Krause, AS Amasyali, M Hajiha, D BALDWIN, DD Baldwin, G Martin
Loma Linda University, Department of Urology
Introduction & Objective: A prior study has shown that foot pedal activation during endoscopic surgery frequently occurs in a dimly lit operating room (OR), resulting in the potential for incorrect pedal activation. This may increase radiation exposure, cause tissue injury, or rarely result in patient burns and OR fires. This study compares speed, accuracy, low‐light visual adaptation, and surgeon preference for foot pedal activation in 4 different lighting conditions.
Methods: During a simulated percutaneous nephrolithotomy (PCNL), pedals for C‐arm, laser, and ultrasonic lithotripter (USL) were randomized to 3 different positions. Twenty participants (urology attendings, residents, and medical students) activated pedals in a randomized order in 4 settings: a dark OR with black light illumination, a dark OR with glowstick illumination, a dark OR with no illumination, and an OR with overhead illumination (Fig 1). Endpoints included pedal activation time, number of attempted, incomplete, and incorrect activations, dark adaptation, and surgeon preference. ANOVA was used for analysis with p < 0.05 considered significant.
Results: Combined mean pedal activation in the glowstick (6.77 s) and black light (5.34 s) arms were faster than the no illumination arm (8.47 s, p < 0.05). In addition, individual pedal activations for the C‐arm, laser, and USL were with glowstick and black light illumination (p < 0.05 for all). The black light resulted in a decrease in attempted (0.30 vs. 3.45, p < 0.05), incomplete (1.25 vs. 7.75, p < 0.05), and incorrect activations (0.35 vs. 1.25, p < 0.05) compared to the dark setting, while demonstrating no difference compared to having room lights on. Dark adaptation was significantly improved with black light illumination compared to having the room lights on (134.5 vs. 140.5 luminance units, p < 0.05). 100% of participants preferred illuminated pedals compared to the dark OR, with 90% preferring the black light.
Conclusions: During a simulated PCNL, black light foot pedal illumination significantly improved accuracy and efficiency of instrument activation compared to the conventional dark OR, while also maintaining the surgeon's dark adaptation.
Withdrawn
Influence of Radiation's Risks Education on Urology Residents Practice in Urological Surgeries with Radiation
BO Manzo, Y Gomez, S Hector, MS Gonzalez, FC Vicentini, C Morales, E Tejeda, J Valero, J Sanchez Núñez
Introduction & Objective: To assess health risks knowledge about radiation exposure and compliance with safety radiation measures in Latin American urology residents.
Methods: A survey link was sent to urology residents in nineteen hospitals of Argentina, Brazil, Chile, Mexico, and Peru. We evaluated radiation protection practices, the protective equipment availability, and general knowledge about radiation risks. We compared the results between those residents who have received formal, informal, and no education on occupational radiation safety. For the comparison of parameters, we used the chi‐squared test. A P value <0.05 was indicative of statistical significance.
Results: A total of 174 urology residents completed the survey. Forty (23%) had answered to they have received formal education (presentations, classes, or academic sessions), 78 (44.9%) informal (during medical rounds or in surgery room), and 56 (32.1%) no education about radiation risks.
One hundred and thirty residents (74.7%) consider they did not receive enough radiation risks and preventive measures information. Most of the residents reported participating in 4‐5 procedures per week requiring fluoroscopy. One hundred percent of residents reported using lead aprons, 69% thyroid protectors, and 8% lined glasses in surgery. Sixty‐three residents (36.2%) were aware of the fluoroscopy screening time used in each procedure. Seventy‐seven residents (44.2%) recognized shielding and distance from the radiation source as protective measures. One hundred and five residents (60.3%) received dosimeters in their hospitals, but only thirty‐nine residents (37.1%) wore it in most procedures. Seventy‐one residents (40.8%) identified that urologist's lower extremities are exposed to more ionizing radiation when an X‐ray source is below the patient. There were differences between groups with prior formal, prior informal and no education regarding awareness of fluoroscopy time used in procedures (p = 0.007), regular dosimeter use (p = 0.0026), use of all protective equipment available (p = 0.0001), capacity of recognition of all three radiation protection principles (p = 0.0001), recognition cataracts risk in radiation exposure (p = 0.0001) and knowledge of X‐ray physics (p = 0.0001).
Conclusions: Residents that received formal education on radiation showed better radiation safety practices and knowledge regarding risks and measures to decrease radiation exposure. Latin American urology residents showed a significant lack of protective radiation practices and a lack of knowledge regarding the radiation risks.
Utilitzation of Surgical Skills Assessment Tool by Urologists At Health System Level – Trends in Implementation and Score Distribution
D Mikhail, S Pettit, J Sarcona, A Tabibzadeh, S Bolourani, D Thompson, A Antonacci, L Richstone
Lenox Hill/Northwell Health
Introduction & Objective: Surgical metrics in healthcare continue to be evaluated to score surgeons and hospitals. CSATS (Crowd Sourced Assessment of Technical Skills) is a validated robotic surgical skills metric currently utilized for surgeon feedback and quality improvement. Since 2018, CSATS, which reports a GEARS (Global Evaluative Assessment of Robotic Skills) score, has been available in our health system. We evaluated urologists utilization trends, scores and comparison to national quartile rankings.
Methods: Robotic surgery data was extracted for all urologists in our health system utilizing the da Vinci robot since 2014. CSATS data was submitted by 14 adult urologists over the past 2 years (2018‐19). Surgeons with <5 robotic cases over this period were excluded, leaving 12 surgeons. Total robotics cases, annual robotic surgery and CSATS utilization rates were evaluated for correlation with outcomes of GEARS scores, percentiles and length of stay (LOS). Two most common procedures, radical prostatectomy (RALP) and partial nephrectomy (RPN), were sub‐analyzed. Spearman's correlation coefficient was used to find significant relationships between volumes and scores.
Results: Our 12 surgeons performed 1587 robotic cases over the past 6 years, with 48% (n = 766) over the past 2 years. Of these, 299 (39%) were submitted to CSATS, with utilization increasing from 26% to 48% in 2018 and 2019. There was no significant difference in scores or percentiles between both years. Surgeon's CSATS utilization, median 48% (IQR 25‐55%), and LOS did not correlate with any outcomes. Total and 2‐year robotic volumes were significantly correlated with CSATS percentiles (R = 0.59, p = 0.045) and quartiles (R = 0.74, p = 0.006), however this relationship was not found with GEARS score (R = 52, p = 0.08). Evaluating RALPs (n = 427) and RPN (n = 106), surgical volume in these procedures correlated very highly with GEARS score (r = 0.8‐0.87, p < 0.01), percentiles (r = 0.8‐0.89, p < 0.01) and surgeon quartiles (r = 0.83‐0.91, p < 0.01).
Conclusions: Our institutional experience with a voluntary technical skills assessment tool (CSATS) showed that utilization is increasing among urologists, however utilization rate did not effect scores or length of stay. Surgeon robotic experience appropriately correlates with GEARS scores, percentiles and quartile rankings – an effect that is even more pronounced in common procedures (RALP and RPN). At our institution, we've validated CSATS relationship to experience, however, further analysis is needed to correlate scores with perioperative outcomes and complications.
Hygienic Keyboards: Designed to Reduce Infections, But May Increase Mistakes and Medical Errors
P Stokes, R Belay, JD Belle, M Keheila, AS Amasyali, M Hajiha, D Baldwin, DD Baldwin, A Assidon
Loma Linda University, Department of Urology
Introduction & Objective: Normally, an important goal for health care institutions is to reduce hospital‐acquired infections. This has become even more pervasive in the COVID‐19 era. One technique suggested to reduce transmission of infection is the use of a novel flat computer keyboard which is easier to sterilize. In an attempt to reduce infections, our institution replaced conventional keyboards with a flat “hygienic” keyboard covered by silicone. Although these keyboards are easily cleaned, lack of tactile feedback from conventional keys could make typing more difficult, potentially increasing errors. Medical errors cost $20 billion and are responsible for 100,000 deaths per year in the United States. The purpose of this study is to compare accuracy, speed and error correction rates between this flat keyboard and a conventional keyboard.
Methods: Using a prospective randomized protocol, 40 participants (physicians, nurses and medical students) performed a typing test on both a flat and conventional keyboard following a practice test. Results recorded were words per minute (WPM), accuracy, and error correction rates. Accuracy was defined by the percentage of correctly typed characters. The impact of the two different keyboards on clinical documentation was determined by measuring the number of typed words for every patient admitted to the urology service for 30 days. The one month data for word count, accuracy and speed were then extrapolated to a one year interval to project differences between keyboards.
Results: Subjects typed significantly faster using the conventional keyboard compared to the flat keyboard (58 v 50 WPM; p < 0.001). Accuracy was significantly higher using the conventional compared to the flat keyboard (94.5 v 90%; p = 0.024). The percent error correction was similar (52% vs. 52%; p = 0.31). During the one‐month study period, the urology service typed an average of 526 (43‐9480) words for 67 patients, a total of 35,242 words. Applying word and error rates to a one‐year period, using the conventional keyboard would save 17.7 hours and prevent 19,032 errors compared to the flat keyboard.
Conclusions: Although “hygienic” flat keyboards may prevent the spread of infection including COVID‐19, this study demonstrates that they are also associated with a 16% reduction in typing speed and a 5% increase in error rate.
Could 3D virtual models reduce positive surgical margins rate after robot‐assisted radical prostatectomy? A prospective comparative study
E Checcucci, A Pecoraro, S De Cillis, D Amparore, F Piramide, A Piana, G Volpi, P Alessio, M Sica, S Granato, S Piscitello, B Carbonaro, G Cattaneo, M Manfredi, C Fiori, F Porpiglia
Department of Urology, AOU San Luigi Gonzaga ‐ University of Turin
Introduction & Objective: Positive surgical margins (PSM) after radical prostatectomy represent a worrying circumstance for both surgeons and patients, leading to a higher rate of biochemical recurrence (BCR). The aim of this study was to investigate the role of 3D model during robot assisted radical prostatectomy (RARP) in reducing the PSM rate.
Methods: We prospectively enrolled patients with localised prostate cancer (cT1–3, cN0, cM0) undergoing preoperative mpMRI and subsequent RARP at our Centre from January 2016 to January 2020. Thanks to the support of bioengineers, starting from mpMRI bidimensional images, hyper accuracy 3D (HA3DTM) prostate models were realized. The first surgeon had the opportunity to use the models during the intervention in a cognitive or augmented reality setting. Demographic and perioperative variables were collected. The nerve sparing (NS) approach according to Pasadena classification and the PSMr were evaluated both in 3D and non‐3D groups. Modelling relied on multivariable logistic regression (MLR) models predicting the presence of PSM in the overall population and in 4 specific subgroups of patients: extra capsular extension patients, D'Amico high risk category, positive DRE, cT3 patients.
Results: 757 patients were enrolled. 3D technology was used in 160 patients during the procedure. In particular, both 3D cognitive (n = 56, 35%) and 3D augmented reality (n = 104, 65%) procedure were performed. No differences were observed in terms of preoperative and demographic mcharacteristics and complications rates between 3D and non‐3D groups. 3D patients were treated more often with full NS approach (20.6 vs. 12.7%, p < 0.05) and, had lower PSM rates (25 vs. 35.3%, p = 0.01), compared to their non‐3D counterpart. A subgroup analysis according to the type of NS showed no difference in terms of PSM rates between the two groups (33% vs. 36.8%, 22.9% vs. 32.1% and 22.7% vs.37.4% for respectively full, intermediate and standard NS approach, p > 0.05). Finally, at MLR, the availability of 3D technology (OR: 0.5, CI:0.3‐0.8, p = 0.005) and the absence of extracapsular extension (ECE, OR: 0.6, CI:0.4‐0.9, p = 0.004) at mpMRI were independent predictors of lower rates of PSM.
Conclusions: The use of 3D models during RARP allows to decrease the PSM rates. Moreover, it grants a more conservative NS approach, without compromising the PSM rate. However, the low sample size does not allow to identify a specific subgroup of patients in whom the advantage of 3D technology is maximized.
Thirty‐Year Trends in the Surgical Management of Urolithiasis in the United States
R Alam, JS Winoker, A Alam, BR Matlaga
Johns Hopkins University School of Medicine
Introduction & Objective: Over the past 30 years, the field of endourology has seen an explosion of technological advancements that has significantly changed the management of stone disease. We sought to determine if the constant refinement and increased familiarity with endoscopic procedures has led to a concomitant shift in treatment practices for both upper and lower urinary tract calculi.
Methods: In this population‐based cohort study, we used data from TriNetX, a large health research network with real‐time updates of electronic medical records (EMR) from 49 health care organizations in the United States. Due to the dependence on EMR, data from participating institutions prior to the implementation of an electronic record system are not included. Patients with upper tract stones who underwent shock wave lithotripsy (SWL), retrograde intrarenal surgery (RIRS), percutaneous nephrolithotomy (PCNL), or open surgery were identified based on Current Procedural Terminology (CPT) codes. Similarly, patients with lower tract stones who underwent cystolitholapaxy or cystolithotomy were separately identified and analyzed.
Results: SWL was the primary mode of treatment for patients with upper tract stones until 2000, after which RIRS saw a dramatic increase that has persisted through 2020 (Figure 1). During this time, PCNL has remained relatively stable, representing about 10% of upper tract stone procedures. For patients with lower tract stones, cystolitholapaxy has always been favored over cystolithotomy, and the gap continues to increase over time (Figure 2).
Conclusions: RIRS has gained considerable popularity at the expense of SWL for the management of upper tract calculi. However, the use of PCNL has been largely unaffected by this shift in practice patterns. The relative stability of PCNL may be a reflection of its surgical invasiveness when compared to SWL and RIRS, or may be due to less overlap in clinical indication with its less invasive counterparts, among other reasons. Minimally invasive approaches have always been and continue to be favored for the treatment of lower tract calculi.
Development of a Customizable Dual‐modality Kidney Phantom Model
BA Johnson, JC Gahan, J Vargas, P Le, M Shahedi, J Dormer, S Shahub, M Pfefferle, B Judson, Y Alshara, Q Li, B Fei
UT Southwestern
Introduction & Objective: We sought to develop a robust, cost‐effective, hyper‐realistic kidney phantom model that is compatible with both computed tomography (CT) and ultrasound (US). This phantom models can be utilized to simulate US‐guided and CT‐guided percutaneous of renal treatment such as lesion biopsy or collecting system access.
Methods: An anonymous contrast‐enhanced CT scan of a healthy patient was used as the source. Segmentation was performed to delineate renal anatomy. Injection molds of the renal parenchyma and collecting system were 3D‐printed. The material used to model each kidney component can be adjusted to suite the desire of the imaging modality (table 1). The process can be seen in figure 1. The entire phantom is placed in agar to represent the retroperitoneum.
Results: A kidney phantom was made utilizing this method. The cortex was made with bovine gelatin + povidone‐iodine, and the renal pelvis was made with agar + cellulose. A small cortical renal mass was simulated by injecting plain agar. The imaging results can be seen in figure 2. This phantom mimics a contrast enhanced renal parenchyma with a hypodense renal pelvis on CT. On ultrasound, this simulates US contrast in injected into the collecting system. Not including the cost of the imaging software or the 3D printer, these phantoms can be made for ∼$20 each.
Conclusions: We present a robust and cost‐effective kidney phantom model that allows for extremely customizable echogenicity and density to simulate realistic imaging characterizes on US and CT. This approach can be utilized for simulation training, or in novel medical device development.
A Novel Cost Effective Platform for Remote Live Surgical Mentoring and Review ‐ Advanced Mentoring in a High Volume Robotic Urological Training Centre
M Yao, J Mackinlay, A Barker, M Thomas, EH streeter, BA Eddy, SS kommu
East Kent Urology Department, Kent and Canterbury Hospital, East Kent Hospitals University NHS Foundation Trust
Introduction & Objective: With the near exponential uptake of Robotic Surgical Procedures and evolving trends in the need for optimal skills acquisition and delivery, there remains an ever expanding need to develop advanced tools to meet the demands. Our aim was to develop and assess the feasibility of an Intrinsic Streaming Platform for Remote Live Surgical Mentoring and Review. The platform was developed to serve a pentad of roles (1) To enable the Senior Surgeon to Mentor in a real‐time two way feedback system to facilitate optimal surgical outcomes for the patient (2) To enable the Junior Surgeon or Robotic Fellow to dial in and liaise with the Senior Surgeon at the time of surgery for guidance in case of difficulty (3) To enable Remote Teleconsultation for patient after care and followup (4) To enable video conference capabilities to facilitate Local, Regional and International dialogue during cases with ability to log into multiple sites and (5) Herein, we present our experience.
Methods: The platform was set up with the aid of the NHS Information Technology and Unified Communications Team. The schematic consisted of Large Screen Monitors coupled with both web based and hard wired platforms for direct visualisation of the Robotic Surgeon's Console View on a real‐time basis. The entire platform was achieved by connections using the daVinci Slave Screen, Robot Console, patient cart, Coax P2P, with a LAN directed connection and communications interface coupled with an Antrika Encoder.
Results: One hundred and twenty live cases were successfully tested with image transfer and two way communications between console surgeon and senior mentor with consent from patients. Futhermore, all five facets of the pentad of aims were successfully carried out with excellent feedback.
Conclusions: The Intrinsic Streaming Platform for Remote Live Surgical Mentoring and Review proved to be a workable and welcome tool for engagement of surgeon‐mentor, surgeon‐fellow, surgeon‐patient and interhospital interface and for optimal interaction in a high volume robotic fellowship training centre. Similar platforms could be set up in other robotic training centres.
Simulation models and training curricula for training in endoscopic enucleation of the prostate: A systematic review
K Pagonis, A Peteinaris, A Vagionis, C Adamou, D Liourdi, T Tokas, A Natsos, M Obaidat, G ortner, E Liatsikos, P Kallidonis
Department of Urology, University of Patras, Greece
Introduction & Objective: Transurethral surgeries are some of the most common everyday urological procedures. Nevertheless, endourology demands a set of skills that need training and operational experience. The introduction of laser for the enucleation of the prostate and the techniques of its use created a new educational field. In this review we investigated the current literature to find out if simulators, phantoms and other training models that could be used as a tool of teaching urologists alone, or within the boundaries of a course or a curriculum.
Methods: A systematic review was performed according to PRISMA statement and the recommendations of the European Association of Urology Guidelines office for conducting systematic reviews. 7 out of 51 studies met our inclusion criteria and are presented in the current review.
Results: It was found that VirtaMed UroSimTM HoLEP Simulator had excellent scores for face, content and construct validity and the majority of the participants in three of the studies agreed that it could be used for training. In addition, this simulator offers the opportunity for morcellation training. The Kansai University model for HOLEP does not support morcellation simulation, but it is believed to be more realistic and has also excellent face, content and construct validity scores. The CyberSim (Quanta System, Solbiate Olona VA, Italy) has not been evaluated, but it seems that it can be used for training without tutoring.
Conclusions: Simulators and courses or curricula based on a simulator‐based training could be a valuable learning tool for any surgeon and there is no doubt that they should be a part of a urologist's technical education.
How many cases are necessary to overcome the learning curve for retrograde intra‐renal surgery?
D Kim, S Jeon, S Lee, C Lee, S Chang, S Lee
Department of Urology, School of Medicine, Kyung Hee University
Introduction & Objective: Retrograde intra‐renal surgery (RIRS) has become one of the preferred treatment options for renal stones. Technique of RIRS may be challenging, which needs adequate training to achieve optimal results. However, the learning curve for RIRS has not been well established. The aim of this study is to estimate the minimum number of cases for a surgeon to perform RIRS consistently.
Methods: From January 2014 to May 2017, 279 patients received RIRS at Kyung Hee University Medical Center. All cases were performed by single surgeon. We retrospectively reviewed their medical records and included patients if the main stone had a maximal diameter between 10 and 30mm. All patients checked non‐enhanced CT at one month after surgery. According to the previous report, procedures were divided into 4 groups: first fifty procedures (Group 1), second fifty procedures (Group 2), third fifty procedures (Group 3), and fourth fifty procedures (Group 4). We excluded patients who did not follow our schedule or do not check postoperative CT yet. Success of treatment was defined as complete stone free or the presence of residual stone size less than 3mm.
Results: There was no difference in mean age, male to female ratio, and body mass index. Furthermore, mean stone sized showed no significant difference between the groups: 13.51 ± 5.43 vs. 14.11 ± 4.95 vs. 14.65 ± 7.05 vs. 14.81 ± 6.92 (p = 0.932, Group 1, 2, 3, and 4, respectively). However, as the case accumulates, mean operative time significantly decreased from 87.30 ± 41.66, 79.82 ± 44.61, 67.22 ± 36.67, and 56.43 ± 35.33 (p = 0.025). Success rate of Group 1 was only 62.2%. On the other hands, success rate of Group 2, 3 and 4 revealed 89.3%, 80.6%, and 90.5%, which was significantly higher than that of Group 1.
Conclusions: As the case accumulates, mean operative time decreases. And to achieve the stone free after RIRS, it seems that 50 cases is a reasonable estimative for experience needed.
On the Rocks: Can Urologists Identify Stone Composition Based on Endoscopic Images Alone? A Worldwide Survey of Urologists
JH Randall, BB Whiles, RV Carrera, JA Thompson, DA Duchene, DA Neff, WR Molina
University of Kansas
Introduction & Objective: At over $2 billion annually, nephrolithiasis is the second most expensive urologic disease in the United States. Medical prevention relies heavily on laboratory identification of a stone's chemical composition. We identified an opportunity for cost reduction by sending fewer stones for analysis, particularly in cases where composition is readily determined intraoperatively; however, it remains unclear if urologists can reliably determine this. Our objective was to assess urologists' ability to identify stone composition based on a single, static endoscopic image.
Methods: We captured intraoperative images depicting physical appearance of stones and determined the composition by chemical analysis. We built a survey with images of 10 different stones, representing 6 stone types: calcium oxalate (CaOx) monohydrate, CaOx dihydrate, calcium phosphate (CaP), cystine, struvite, and uric acid. The survey was distributed to members of the Endourological Society and the South Central Section of the American Urological Association. We asked respondents to predict stone composition based on a single image. An exact binomial test with Bonferroni correction assessed respondents' accuracy. We used linear regression to determine if years of experience, fellowship training, or self‐perceived ability to identify stone types improved accuracy.
Results: In total, 366 respondents completed the survey. Most were from academic institutions (69%), were fellowship‐trained endourologists (57%), and practiced outside of the United States (66%). The majority successfully identified the two images of CaOx monohydrate stones, with success rates of 70% and 63%. For CaOx dihydrate stones (2 images), success rates were 56% and 51%. CaP stones (2 images) were frequently misidentified, with success rates of 23% (brushite) and 10% (apatite). The apatite stone was commonly misclassified as CaOx monohydrate (52%). Additional success rates were: 75% and 38% for struvite (2 images), 42% for uric acid (1 image), and 14% for cystine (1 image). Fellowship training and self‐perceived ability improved accuracy by 4% (p = 0.01) and 16% (p < 0.001) respectively.
Conclusions: Certain stone types, especially CaOx, can be identified by a single static image, potentially reducing unnecessary laboratory costs. Since we only used single images, real‐world intraoperative identification could be greater than we predict. Further studies using endoscopic videos during lithotripsy rather than images alone are warranted.
Withdrawn
Analysis of hand/instrument motion during ureteroscopy: Development of an enhanced simulation platform to aid in resident training
S Koo, K Fok, N Seo, B Alsaikhan, B Carrillo, MA Farcas
University of Toronto
Introduction & Objective: Hand/instrument motion‐tracking in surgical simulation can provide valuable data to improve psychomotor skills, and can also serve as a more formative evaluative tool.1‐2 Although motion analysis has been well studied within laparoscopic surgery, it has been very poorly studied in endoscopic surgery.3 There are essentially no studies looking at surgeon hand/instrument motion tracking for flexible ureteroscopy (fURS), a surgical procedure that requires a significant amount of hand dexterity.4‐5 In this study we aimed to develop a ureteroscopic surgery simulation platform that incorporates motion tracking capabilities.
Methods: Using the PolhemusTM system we designed a motion tracking platform for a benchtop ureteroscopy simulator. This system was designed to capture specific instrument/surgeon hand motions determined to be important during fURS. Motion data were captured for a specific defined task performed on the simulator. Using this data, motion analysis metrics for fURS were established. 25 volunteers were tested on this new platform and motion analysis parameters were recorded and analyzed.
Results: Using motion tracking software we analyzed three key motions during fURS: scope in‐out motion, scope rotation, and scope tip flexion/extension. The target task was visualization of one upper, one inter‐, and one lower pole calyx on a benchtop surgical simulator of the left kidney. Participants were asked to pause for 10 seconds when visualizing each papilla to help discriminate the motion data. 25 participants were tested (5 novices, 13 residents, 7 urologists). While scope in‐out motion and scope tip flexion were significantly different between participants of different expertise level, the most discriminatory metric which differentiated experts from novices was scope rotation (Figure 1).
Conclusions: We were able to successfully create a flexible ureteroscopy simulation platform that captures instrument motion. Preliminary data suggests scope rotation is the most discriminatory motion parameter in fURS that discriminates between novice and expert surgeons.
Withdrawn
Survivin(BIRC5)Regulates Bladder Fibrosis in Partial Bladder Outlet Obstruction Rat Model
X Di, X Jin, L Xiang, X Gao, L Peng, W Wang, K Xiao, Y Liu, G Chen, D Luo, H Li, K Wang
Department of Urology, Institute of Urology (Laboratory of Reconstructive Urology), West China Hospitgal, Sichuan University
Introduction & Objective: Bladder fibrosis is a disease triggered by bladder outlet obstruction or inflammatory stimulus, which is highly associated with overactive bladder symptoms caused by decompensation of bladder function. However, the accurate mechanism of bladder fibrosis has not been fully understood. In this study, we aim at using bioinformatics to identify potential hub genes involving in bladder fibrosis.
Methods: The pBOO rat model(3 weeks) was constructed and Microarray analysis was performed. Hub genes were sheltered through protein‐protein interaction (PPI) network. Then, differentially expressed genes(DEGs)were identified, and gene ontology (GO) enrichment analysis, Kyoto Encyclopedia of Genes and Genomes (KEGG) enrichment analysis were conducted. Finally, the expression of hub gene was validated by immunohistochemistry(IHC)and immunoblotting analysis.
Results: We identified 20 hub genes which were associated with fibrosis process. Survivin (BIRC5) engaged in the whole pathological development of bladder fibrosis (proliferation, inflammation and extracellular matrix deposition). For further validation, immunohistochemistry(IHC)and immunoblotting analysis revealed a moderate increase of survivin in fibrosis bladder.
Conclusions: Survivin was found out as a potential hub gene in proliferation, inflammation and extracellular matrix deposition process, and that might be important in fibrosis. However, more molecular research are required to verify the function and mechanism of survivin in fibrosis.
Contemporary pain management practices of transurethral therapies for benign prostate hypertrophy: Results of a global survey
MS Lee, M Assmus, DK Agarwal, T Large, AE Krambeck
Northwestern University Feinberg School of Medicine
Introduction & Objective: As demonstrated by the AUA guidelines for surgical management of benign prostate hypertrophy, today's urologist has more tools at his/her disposable than ever before. However, multiple studies have demonstrated 24.0%‐50% of urologists prescribe opioids after transurethral resection of prostate or laser prostatectomy, which seems unexpectedly high. However, to our knowledge, no one has attempted to quantify the rates of opioid prescription for contemporary BPH therapies. Therefore, we performed a global survey of the 3500 members of the Endourology Society to determine postoperative pain management practices of all contemporary BPH therapies.
Methods: Each surgeon answered demographic information (age, gender, academic vs. non‐academic, fellowship‐trained), what BPH therapies they performed >10 cases/year, and finally what medications they used for pain management. Categories of BPH therapies included: ablation, enucleation, resect/vaporization, and MISTs. Subcategories included are shown in Table 2. Statistical analyses were performed using chi‐square tests to test if any associations existed between opioid‐prescribing behavior and surgeon demographics. Significance was set at p < 0.05.
Results: 175 surgeons from 45 countries responded to this global survey. Overall 23.4% of surgeons prescribed opioids. Rates of acetaminophen and NSAID‐use ranged from 55.9%‐86.8% and 56.6%‐89.5%, respectively (Table 1). On univariate analysis, no demographic variables were associated with opioid prescribing. Patients undergoing MISTs were more likely to receive postoperative opioids (OR = 2.34, 95%CI:1.04‐5.26, p = 0.0370). Tramadol was the most commonly prescribed opioid, 64.9% (n = 48/74).
Conclusions: In this global survey, 23.4% of surgeons prescribed opioids consistent with prior studies. We did not identify any demographic variables associated with opioid prescriptions, but patients undergoing MISTs were more likely to receive opioids.
Effectiveness of the RIRS navigation training module using 3D‐printing
G Jung, H Jung, J Han, S Jeong, H Yoon, J Park, S Cho
SMG‐SNU Boramae Medical Center
Introduction & Objective: This study aims to evaluate the feasibility of the newly‐developed 3D printed handy module for training of RIRS navigation in a group of urologists who were not fully exposed to RIRS as an operator and evaluate whether this new module can overcome the limitations of the existing modules.
Methods: Two specialists with sufficient clinical experience of RIRS provided the orientation training over a 10‐minutes to all trainees. One of the best Computed Tomography (CT) images was selected. The 3D printing simulator is manufactured through 5 processes. There were a total of 16 points per kidney. One navigation time started from the moment when endoscope entered into the ureter of the model. All 16 points were checked when the scope approached the inner side of the calyces where laser emission and stone fragmentation were available in clinical situations. After navigation was completed, the navigation time was measured and recorded. The goal was to perform ten times navigation for each side, starting from the right or left side at random. After the experiment, all trainees were asked to fill out a questionnaire.
Results: All 17 trainees were included. The training period average time was 3.05 ± 1.80 years. The eleven trainees (64.7%) had the experience of assisting RIRS less than 100 cases, and six trainees (35.3%) between 100 and 500. A total of 308 trials were performed; 154 trials per side. The average navigation times of the whole trials were 153.4 ± 92.6 sec, 149.5 ± 85.3 sec, and 157.2 ± 99.5 sec in the right side and left sides. There were no significant differences in the navigation times between the right and the left sides (P = 0.498).
The averages of the maximum and minimum navigation times were 354.3 ± 177.2 sec and 80.1 ± 25.6 sec. The mean navigation times of the first and the last trials of all trainees significantly decreased from 251.4 ± 108.0 sec to 93.9 ± 33.2 sec (P < .001). The change of navigation time did not show any significant differences between the RL and LR groups (P = 0.283). The average of reduction in navigation time was 201.3 ± 133.3 sec. The maximum and minimum reduction of navigation times were 400 sec and 45 sec.
Almost all trainees were satisfied with the training.
Conclusions: The newly‐developed 3D printing navigation training module seems to be adequate to improve RIRS skills for beginners.
Developing a Synchronous Hand/Instrument Motion‐Tracking and Video Capture Tool: Objective Assessment for Flexible Ureteroscopy Training
MA Farcas, J Trac, B Carrillo
Department of Urology at St. Michael's Hospital
Introduction & Objective: Hand/instrument motion‐tracking in surgical simulation provides valuable data to improve psychomotor skills, and can serve as a formative evaluation tool. Motion analysis has been well studied in laparoscopic surgery, but poorly studied in endoscopic surgery. There are essentially no studies looking at motion‐tracking for flexible ureteroscopy (fURS), a surgical procedure that requires significant hand dexterity. Our goal was to design a synchronized motion‐tracking and video capture system for fURS. The aim is to collect metrics for use in objective surgical skills assessments and to provide detailed trainee feedback to improve training.
Methods: Position (x, y, z) and orientation (roll, pitch, yaw) of the ureteroscope handle and tip, position of the lever (used to manipulate the tip), and movement (insertion, roll) at the insertion point was collected using a combination of sensors including a motion‐tracking platform (PolhemusTM), off‐the‐shelf inertial measurement units (IMUs) and optical sensors. Video data of the subject's hands was collected with a Raspberry Pi camera. Video data of the endoscopic view was collected from the video tower with an off‐the‐shelf USB video grabber. All components were controlled with custom Python software on a Raspberry Pi 4, and synchronized to its system clock.
Results: A prototype was assembled with the PolhemusTM standard sensor, IMUs and Raspberry Pi. A 10 minute trial demonstrated successful, synchronized data collection of the position and orientation of the instrument handle and lever, and video data of the subject's hands. Static position accuracy of the system was 0.7 mm, 1.8 mm and 1.0 mm in the x, y and z axes, respectively. Average CPU utilization went from an 8% baseline to 33% during data collection.
Conclusions: We have been able to successfully build a data collection system capable of gathering synchronized motion‐tracking and video data in fURS. The data pool can be utilized by surgeons and engineers to improve and standardize objective assessment and simulation training for endoscopic surgery. Our next steps include integration of optical sensors for insertion point tracking, a sensor for instrument tip tracking, and a USB video grabber to capture the endoscopic view.
Beyond Efficiency: Surface Electromyography Enables Additional Insights into the Quality of Surgical Motion of Expert Urologists
P Xu, D Haik, P Jiang, A Peta, Z Okhunov, A Brevik, S Tapiero, J Emmanuel, R Soangra, J Landman, RV Clayman
Introduction & Objective: The advent of laparoscopic and robotic surgery has required urologists to hone multiple skillsets that involve complex movements. Surface electromyography (EMG) accurately records aspects of complex movements. Our objective was to use EMG to capture the differences of surgical movement between expert urologists and trainees while performing laparoscopic and robotic surgical tasks.
Methods: Based on surgical experience, 26 participants were divided into three groups: novice trainees (no surgical training; n = 10), intermediate trainees (resident; n = 11), and experts (faculty; n = 5). With 12 surface EMG electrodes affixed to the upper extremities, participants performed 2 tasks: laparoscopic peg transfer (LPT) and robotic suturing (RS) (Figure 1). Performance EMG data were computed based on muscular activation and workload. These variables were compared across groups using ANOVA statistical analysis; significance was defined as p < 0.05 and differences were confirmed with posthoc Tukey analysis.
Results: Novices took longer to complete the LPT and RS tasks (Table 1). There was no significant difference across skill level for both tasks in muscle contraction range, root mean square (variability in linear motion), and average work per second. Experts had higher muscle contraction frequency compared to both novices and intermediate trainees in RS (P = < 0.01). Intermediate trainees had higher muscle contraction frequency compared to novices in LPT (p = 0.03). Experts had lower cumulative workload in RS compared to novices (p = 0.04).
Conclusions: Contrary to open surgery where speed is often regarded as a primary indicator of skill, among a range of personnel there were minimal differences in efficiency in task completion. Instead, experts in robotic surgery were distinguished by a higher muscle contraction frequency indicating a more concentrated effort expended on fine muscle control and microadjustments.
Video SessionVideo Session 11: Robotic Surgery: Prostate
V11: Robotic Surgery: Prostate
C Schwentner
Techniques to Reduce Robotic Prostatectomy Cost and Operative Time
M Billah, S Ahsanuddin, J Cadwell, R Sawhney, R Harrison, M Ahmed
Introduction & Objective: Intuitive introduced Single Port Robotic Assisted Laparoscopic Surgery in 2018. This new technology was a major step forward for single site minimally invasive surgery. It enables multiple instruments with fully wristed motions. The robotic prostatectomy has gained popularity as a minimally invasive surgical technique for the management of prostate cancer due to benefits such as decreased blood loss and patient recovery time. Robotic prostatectomy has been associated with additional cost and time on the operative table. We sought to determine if and how cost and operative time in robotic prostatectomy could be minimized through observation of high‐volume surgeons at our institution and present our data in a video format.
Methods: Surgeon specific data provided by the robotic surgery platform at our institution was examined to determine each surgeon`s operative speed, cost per operation, length of stay, and readmission rates following robotic prostatectomy. After determination of high performance in these areas, surgical technique was examined to analyze factors that contributed to the specific surgeon`s high performance.
Results: Surgeon specific data is displayed in Figure 1. An observational analysis determined one particular surgeon as an outlier in terms of operative speed and cost while still maintaining excellent outcomes based on length of stay and 30‐day readmission rate. Observation of this surgeon`s techniques revealed several time and cost‐saving maneuvers. Firstly, multipurpose instruments are utilized to save time and money; for example, the Maryland bipolar forceps are used throughout the case as an electrocautery instrument, grasper, retractor, and needle driver. Specific surgical techniques that reduce operative time were observed, such as forgoing a dorsal vein complex stitch. Additional maneuvers are highlighted in the video.
Conclusions: The techniques documented in our study could benefit the healthcare system by reducing operative costs as well as benefitting patients by reducing time on the operative table while maintaining quality of outcomes, especially as we make the transition to single port robotic surgery.
Robot‐assisted Radical Prostatectomy After Focal Therapy
A Garayev, F Atuğ
Introduction & Objective: HIFU is a treatment option for localized prostate cancer. Salvage radical prostatectomy is a treatment option for selected patients when local recurrence occurs following HIFU treatment. In this case report we aimed to describe robot‐assisted radical prostatectomy approach for patient with recurrence after HIFU treatment.
Methods: A 65‐year old male patient underwent TRUS biopsy due to elevated PSA level (7,1ng/ml) in 2015. Biopsy result revealed a prostatic adenocarcinoma with Gleason 3 + 3 pattern. After initial diagnosis patient underwent HIFU treatment. At postoperative 12month of treatment PSA level increased to 11.4 ng/ml suggesting of biochemical recurrence with residual disease. Prostate MP‐MRI showed residual disease at the right lobe of prostate. After discussing the treatment choices salvage RARP was planned.
Results: Console time and estimated blood loss was 175min and 150ml, respectively. No immediate or late postoperative complications were noted. Final pathology revealed ISUP Grade 2 disease at the right lobe involving prostatic capsule with negative surgical margins. At postoperative 3month of follow‐up the patient is fully continent and potent with PDE5i.
Conclusions: Salvage RARP is the safe and acceptable surgical approach after HIFU treatment with residual disease. This information may help clinicians with treatment selection and counselling of patients regarding to failed HİFU treatment.
Salvage Retzius‐Sparing Robotic Radical Prostatectomy: Step by step description
R Madi
Introduction & Objective: To Show the steps of salvage Robotic Radical Prostatectomy, and report on feasibility, safety, and continence outcomes using the Retzius‐sparing approach in the salvage setting (sRS‐RARP).
Methods: A total of 26 patients underwent robotic salvage prostatectomy at our institution from January 2012 to May 2020 by a single surgeon (RM). Twenty patients underwent sRS‐RARP and 6 underwent the standard approach (sRARP).
Results: Patients had comparable preoperative characteristics with no significant difference in age, race, prostate‐specific antigen level, and Gleason score. Most patients underwent primary external beam radiation therapy (69.2%). Median time to biochemical failure was 7.9 years (IQR 6.1‐13.4). sRS‐RARP required less console time (141.5 vs 199.5.0 minutes, P = .008) and less blood loss (50.0 mL vs 100.0 mL, P = .045) compared to sRARP. Postoperative course was uneventful with a median hospital stay of 1 day. Median catheterization time was 14.0 days (IQR 11.5‐17). Patients undergoing sRS‐RARP had better immediate (25.0% vs 0.0%, P < .001), 3 month (80.0% vs 0%, P < .001), and 12 month continence rates (100% vs 44%, P = .0384) compared to sRARP patients. Likewise, median time to continence was significantly shorter for sRS‐RARP patients (90.0 vs 270.0 days, P = .0095). Biochemical recurrence rate was 20.0% in the sRS‐RARP group and 33.3% in the sRARP group (P = .60).
Conclusions: Early experience suggests that sRS‐RARP is feasible, oncologically safe, and may offer improved continence compared to the sRARP approach.
Radio‐guided Surgery Experience During Robotic Radical Prostatectomy
MB Tuna, T Doganca, OB Argun, I Tufek, C Obek, L Guner, K Guven, AR Kural
Introduction & Objective: In this video, we share our experience of two patients who underwent radio‐guided surgery.
Methods: First case: 58‐year‐old patient with a PSA value of 9.5 ng/ml had undergone prostate biopsy for PIRADS 5 lesion detected in mpMRI. Gleason 9 (4 + 5) adenocancer reported.
Suspicious lymph nodes were detected in the left obturator fossa and anterior of the bladder with Ga68 PSMA PET. These lymph nodes were labeled with Tc99m macro aggregated albumin (MAA). During the surgery, after their excision of these nodes, they were checked with gamma probe and confirmed for radionuclide presence Frozen examination of these nodes showed adenocarcinoma metastasis.
Second case: 69‐year‐old patient with a PSA value of 24 ng/ml underwent prostate biopsy for a PIRADS 5 lesion at mpMRI. A Gleason 7 (4 + 3) adenocancer was detected. A pathological lymph node was detected in the right obturator fossa with Ga68 PSMA PET scan. This lymph node was labeled with MAA. Excised lymph node checked with gamma probe and confirmed for radionuclide presence . Likewise, frozen section analysis of the excised lymph node confirmed metastasis.
Results: Robot‐assisted radical prostatectomy and lymph node dissection is an essential step for the treatment of prostate cancer. Lymph node dissection in high‐risk patients are recommended in guidelines. Appropriate staging and survival advantage may provided with appropriate lymph node dissection. Today, Ga68 PSMA PET is frequently used for lymph node staging. In order to find and remove suspicious lymph nodes, marking can be done with Tc99m at the preoperative period, especially for the nodes that are not in standard dissection template.
Conclusions: Radio‐guided surgery can ease excision of metastatic lymph nodes located outside the standard lymphadenomectomy templates.
Retrograde paraaortocaval lypmphadenectomy during robotic radical prostatectomy in a patient followed by neoadjuvant chemo‐hormonal treatment
T Doganca, MB Tuna, OB Argun, I Tufek, S Keskin, C Obek, AR Kural
Introduction & Objective: This video presents a retrograde paraaortocaval lymphadenectomy procedure performed after super extended lymphadenectomy and robotic radical prostatectomy in a patient with very high risk prostate cancer.
Methods: The patient was a 67 years old gentleman with a PSA of 28 ng/ml. Prostate biopsy revealed Gleason 9 (4 + 5) prostate cancer in 12 of 12 cores. Ga68 PSMA PET showed multiple lymph only metastasis of paraaortocaval region up to the renal hilum. The patient received 6 cycles of chemohormonotherapy prior to the surgical treatment. After completion of radical prostatectomy and super extended lymphadenectomy an additional suprapubic camera port was inserted in the midline for retrograde access. Robotic crane was turned 180 degrees facing cranial. Lymphadenectomy template was extended up to the level of renal pedicle. First posterior peritoneum was opened from caecum to Treitz ligament , and right ureter was identified. Posterior peritoneum was lifted up on both sides via externally placed stay sutures. Upper limit of the lymphadenectomy template was identified. Caval and paracaval lymph nodes were excised with blunt and sharp dissection and using Weck clips. Great attention was paid to occlude large lymphatic vessels with Weck clips. Next step was identification of left ureter through mesosigmoideum. Left common iliac lymph nodes were removed below the mesenteric artery. Interaortocaval lymph nodes were excised with blunt and sharp dissection. Large lymphatic vessels were occluded with Weck clips. During interaortocaval lymph node dissection extra care must be paid no‐t to damage lumbar branches. Right renal artery was identified and preserved precisely. Then aortic and paraaortic lymph node dissection was started. During paraaortic lymph node dissection inferior mesenteric artery was identified and preserved carefully. Again, Weck clips were used to occlude large lymphatic vessels. After completion of paraaortocaval and interaortocaval lymph node dissection, surgical field was controlled carefully for potential bleeding.
Results: Estimated blood loss was 250 ml. and the operation time was 300 minutes. The drain was removed on postoperative second day and the patient was discharged on postoperative fifth day. On final histopathology, there was T3B N1 prostate cancer. Six out of 68 lymph nodes were positive for metastasis. Three of positive lymphs were in the paraaortocaval region.
Conclusions: At postoperative 12 month follow‐up, the patient is still on antiandrogen treatment and has a nadir PSA level.
Tips and Tricks of Super extended lymphadenectomy during robotic radical prostatectomy
T Doganca, MB Tuna, OB Argun, I Tufek, S Keskin, C Obek, AR Kural
Introduction & Objective: In this video, we present some tips and tricks for succesful and safe results in robotic surgery.
Methods: We present our recommendation as follows: Anatomical structures and landmarks should always be considered. When dissecting the peritoneum on the ureter, the use of thermal energy should be avoided. In paraaortic lymphadenectomy, the clip should be placed at the upper limit whenever possible. Attention should be paid to the mesosigmoid plan in the detection of the left ureter. In the left side lymphadenectomy, the left ureter should always be considered. IMA is the dissection limit and care should be taken not to damage it. Dissection of presacral lymph nodes may facilitate external iliac lymphadenectomy. On the right side, the 4th robotic arm can assist retraction. Robotic arm movements' parallel to the obturator nerve should be applied in Fossa Marseille dissection. We prefer to fix the peritoneal surface of the bladder to the suprapubic anterior abdominal wall to prevent the development of lymphocele.
Results: Taking care of anatomic structures and using some simple techniques during robotic surgery may provide more successful and safer results.
Conclusions: It is possible to perform safer and effective robotic surgery by paying attention to the above mentioned.
Surgical Tips of robot‐assisted radical prostatectomy in very high‐risk prostate cancer
J Park, H Park, H Lee, H Shin
Introduction & Objective: The role of radical prostatectomy (RP) in high‐risk prostate cancer (PC) is getting more important than the past because significant proportions of low risk PC is managed by active surveillance. In this video, we present 4 cases of very high‐risk PC patients, which were successfully treated with robot‐assisted RP (RARP).
Methods: A63 year‐old (patient 1) and 69 year‐old male (patient 2) were referred for elevated PSA (16.9 and 19.6 ng/ml, respectively). Both patients were identified as Gleason score 8 after prostatic biopsy. After stage work up, the patients were diagnosed with cT3aN0M0 (patient 1) and cT4N0M0 (patient 2). Preoperative digital rectal exam (DRE) and MRI of patient 1 revealed the established extraprostatic extension at left side of prostate, while patient 2 showed invasion of left seminal vesicle and gross bladder involvement. The other patients, a 57‐year‐old (patient 3) and 51‐year‐old male (patient 4) were referred for elevated PSA (117 and 49.1 ng/ml, respectively). Both patients were identified as Gleason score 9 after prostatic biopsy. After staging work up, the multiple retroperitoneal lymphadenopahty (D2 stage) was identified in both patients. Patient 3 was managed with primary androgen deprivation therapy (ADT), but after 4 year of ADT, PSA began to rise continuously and follow up imaging studies showed progression of primary tumor despite disappearance of previously noted multiple lymphadenopathy. Patient 4 were initially managed by neoadjuvant ADT due to DRE finding of prostate fixed to rectum. After 6 months of ADT, PSA level decreased to 0.3 ng/ml and prostate was movable on DRE, while previously noted retroperitoneal lymphadenopathy disappeared on follow up imaging studies. The four patients underwent RARP (patient 1, 2, 4: preplanned RARP and patient 3: salvage RARP) with lymph node dissection. In all patients, meticulous posterior dissection with appropriate blunt and sharp dissection was performed to prevent rectal injury.
Results: Surgery was performed safely without serious complication. All patients recovered uneventfully, and their PSA reached undetectable level at post‐operative 6 months
Conclusions: Though RARP is challenging in very high‐risk PC patients, it can be done safely without complication in experienced surgeon. In these challenging cases, it is important to check if the prostate is fixed to the rectum by the preoperative DRE. Meticulous posterior dissection is crucial to prevent rectal injury, and sharp dissection is recommended at severe adhesion sites.
Robotic‐assisted Radical Prostatectomy Utilizing the DaVinci SP System in a Patient with Previous Kidney Transplant
JA Ivey, R Pak
Mayo Clinic Florida
Introduction & Objective: We present what is to our knowledge the first reported case of robotic assisted radical prostatectomy in a patient with previous kidney transplant utilizing the DaVinci SP system. Prior literature discusses altering port placement with multiport robotic prostatectomy in a patient with previous kidney transplant in order to prevent robotic arms from clashing with and/or injuring the transplant kidney. Our hypothesis is that the SP system would simplify this process by the fact that the system only requires one port placement which is easily altered.
Methods: The Davinci SP system was utilized for robotic prostatectomy in a patient with previous kidney transplant to the left lower quadrant of the abdomen. Our single port trocar was placed through a 2.5cm incision through the Gelpoint Mini device. The port was placed 4cm cephalad to the umbilicus and 3 cm laterally to the patient's right side in order to minimize contact of the robot with the transplanted kidney. An additional 12mm Airseal assistant port was placed 8cm lateral to the SP trocar on the right hemiabdomen, making the case an “SP‐plus‐one” set‐up. The robotic prostatectomy was carried out in standard fasion, including a posterior approach to dissect out the seminal vesicles and posterior prostate, followed by an anterior approach within the space of Retzius. The bladder was dropped in standard fashion on the right‐hand side, but on the left‐hand side the bladder was not dissected off lateral to the medial umbilical ligament, in order to prevent damage to the transplant kidney transplant ureter. The SP system was easily maneuvered past the partially dropped bladder in transplant kidney to gain access to the prostate. The remaining portions of the case were carried out in a standard fashion.
Results: There were no apparent postoperative complications. Estimated blood loss was 100 mL. The patient's hospital stay was slightly prolonged due to an ileus which resolved on POD 3 when he was discharged. His creatinine and urine output remained at preoperative baseline during his hospital stay. His Foley catheter was removed on POD 7 with no apparent complication. Pathology revealed Gleason 3 + 4 = 7 in 5% of the prostate, confined to the gland.
Conclusions: The DaVinci SP system is safe to use for RALP in patients with prior kidney transplantation, and facilitates avoidance of the transplanted kidney. The SP system makes altering port placement simple and easy. The SP system's compact nature minimizes contact of robotic arms with surrounding structures.
Tips and tricks in salvage ralp post focal therapy failure for prostate cancer
S Bhat, M Covas Moschovas, S Reddy, J Noël, T Rogers, V Patel
Global robotics institute
Introduction & Objective: Salvage robot‐assisted laparoscopic prostatectomy (sRALP) is a technically demanding after focal therapy (FT) due to collateral fibrosis and anatomical disruptions of the anatomical landmarks. Some of the more popular focal therapies include cryotherapy, high intensity focused ultrasound (HIFU), and focal laser ablation (FLA). The failure rate of partial gland ablation ranges between 35%‐42% with about 14% in‐field recurrence(1,2). In this video, we present the challenges associated with sRALP following FT and describe key points in their management.
Methods: Between 2008 and 2018, 53 patients underwent sRALP by a single experienced surgeon in our institution. 7 patients had two FTs All procedures were performed using a transperitoneal six‐port technique. Difficulties caused by focal therapies at were identified and key points in their management are presented here.
Results: Case 1‐ Bilateral pelvic side‐wall fibrosis were common after HIFU ablation. The endopelvic fascia is relatively preserved at the prostate base whereas there is more fibrosis at the apex. Non‐focal collateral fibrosis can make nerve sparing challenging. Case 2‐ Apical dissection around the sphincter was typically difficult in brachytherapy patients because transperineal route used to place brachytherapy seeds. Ipsilateral fibrosis and contralateral recurrence may prevent full nerve preservation on the contralateral side. Case 3‐ Patient had fibrosis posteriorly resulting in severe perirectal fibrosis and adhesions. Serosal surture may be required. Case 4‐ Focal laser ablation can lead to anatomical disruptions. The patient developed posterior urethral diverticulum making sRALP challenging. We go behind the posterior urethral diverticulum by lifting the median lobe. Posterior dissection is then carried on behind the diverticulum to include it along with the prostate. Similar to regular RALP, sRALP following FT leads to poorer functional outcomes when come primary RALP.
Conclusions: sRALP should be performed by experienced surgeons due to severe collateral fibrosis, contralateral recurrence, anatomical disruptions etc irrespective of modality used for focal therapy. The surgeon should be familiar with challenges specific to different FTs and its routes. Despite the targeted nature of FT, significant non‐focal collateral damage contralateral recurrence, anatomical disruptions lead to poorer functional outcomes post salvage RALP.
Withdrawn
Nerve spare RALP with amniotic membrane: medium term outcomes
J Noël, S Reddy, S Bhat, M Moschovas, T Rogers, V Patel
Introduction & Objective: We present our results from patients undergoing nerve‐sparing (NS) robot‐assisted laparoscopic prostatectomy (RALP), 40 years after the discovery of the neurovascular bundle (NVB) by Walsh and Donker in 1981. Our objective in this cohort was to optimise NS by placing amniotic or dehydrated human amnion/chorion membrane (dHACM) on the NVB during surgery. According to previous studies, dHACM is a source of neurotrophic factors and cytokines. Our objective is to update the urological community on the functional and oncological outcomes of our cohort. We will demonstrate our video on the technique of NVB preservation and placement of the membrane during RALP.
Methods: We performed a transperitoneal multi‐port da Vinci robotic prostatectomy. We preserve the NVB by releasing their fascial plane from the prostate apex posteriorly. This is followed by an anterior release of the plane at a similar level, followed by a retrograde release of the NVB. This technique of placing dHACM on the spared NVB was utilised in 2013 – 2019 for 635 patients. In order to inform the urological community of oncological and functional outcomes, we excluded patients with less than 12 months follow up (n = 64), cancer status not captured (n = 36), benign prostatic hyperplasia (n = 5), and unilateral NS (n = 1). 529 (83% or 529/635) patients were included in this study who underwent a partial or full bilateral NS.
Results: 529 patients were followed‐up for median (IQR) of 42 months (25 89). Demographics include median (IQR) age 57 years (52‐62), median preop SHIM score was 24 (21‐15), and AUASS was 5 (2‐11). Full NS was performed in 74% (391/529) and partial NS in 26% (138/529) of this cohort. Pathological stage was pT2 = 399 (75%), pT3a = 107 (20%), pT3b = 19 (4%) and pT4 = 4 (1%) with N1 = 3 (0.6%). Our PSM = 86 (16%) with overall BCR was seen in 52 (10%) patients. Overall post operatively, 434 (82%) were sexual active. Median time to potency in 64 days and time to continence was 42 days. Full vs partial NS: median post op SHIM score 18 (13‐20) vs 15 (6‐20), median time to potency 64 (32‐184) days vs 64 (31‐244) days, and median time to continence 42 (21‐83) days vs 43 (30‐91) days. Age = 55years (n = 322): median post op SHIM score 18 (12‐20) vs 15 (10‐20), median time to potency 49 days (31‐157) vs 91 (32‐ 235) days, and median time to continence 42 (28‐ 70) days vs 42 (25‐91) days.
Conclusions: In our series the application of amniotic membrane/dHACM has satisfactory outcomes. A limitation is non‐respondent rates (4 ‐ 23%) depending on the outcome. Future direction is to compare these against a propensity score matched group to assess the impact of amniotic membrane grafts on the oncological outcomes after RALP.
RALP: Anatomy & Planes by Fellows for Fellows
J Noël, T Rogers, S Reddy, S Bhat, M Moschovas, V Patel
Introduction & Objective: The Robotic Assisted Laparoscopic Radical Prostatectomy (RALP) operation has a learning curve that, like all surgery, depends on the recognition of anatomy and planes. In this video, we present common landmarks along with a detailed narrative of each prostatectomy step. This should aid in Fellows' and Trainees' education in prostatectomy, and will allow them to discuss topics of RALP with their trainers, to enhance the learning and teaching experience.
Methods: All procedures in this video were an anterior transperitoneal multiport system approach to RALP, from a high volume centre. The video demonstrates the experience of the Senior author and the Fellow performing steps, with anatomy and plane recognition. A combination of surgical videos are presented to support the objective.
Results: First step of the bladder drop is to recognise that obliterated umbilical artery and inferior epigastric artery which should be coagulated and avoided respectively. Bladder neck dissection is performed with non‐sparing technique, and during seminal vesicle elevation, an appreciation of denonvillier's fascia and the layers is demonstrated. Athermal retrograde nerve spare is shown with anterior structures of the pelvic fascia after. After apical dissection, pelvic lymphadenectomy is shown and our rational for the right side to begin supervised training is discussed. Rocco reconstruction, the bladder neck reconstruction and vesicourethral anastomosis with a 3‐0 Quill concludes this training video.
Conclusions: RALP can be taught by peers and further aid in the distribution of knowledge on this varied and complex procedure, where anatomy recognition is a key step to optimising functional outcome. The novice surgeon should be familiar with the steps in order to enhance the training experience. We recommend a detailed series of each step and challenges with surgical plane recognition should be studied.
Robotic Assisted Laparoscopic Prostatectomy with the Da Vinci Xi® and SynchroSeal™ Instrument: A Single Surgeon Experience
ZR Leopold, P Romeo, HV Patel, A Srivastava, J Sterling, IY Kim
Introduction & Objective: Robot assisted laparoscopic prostatectomy (RALP) has become the gold‐standard treatment of organ confined prostate cancer. The ideal outcome includes maximizing the removal of malignancy while minimizing the common adverse effects of prostatectomy – erectile dysfunction and urinary incontinence. Since adoption of the da Vinci® robot, many accessories have been developed to optimize the surgical experience. Herein, we describe our experience with a novel accessory, SynchroSeal™, to perform a RALP and pelvic lymph node dissection.
Methods: All procedures were performed with the da Vinci Xi® system. The patient is placed in the supine position and the abdomen, perineum, and genitalia are sterile prepped in the standard fashion. A Varess needle is placed lateral to the left rectus abdominus at the level of the umbilicus for insufflation to 20 mmHg. A 12 mm camera port is placed superior to the umbilicus. Three 8 mm robotic ports and a 12 mm assistant port are placed over the right lower quadrant. Lastly, a 5 mm suction port is placed in the right upper quadrant. After bladder takedown, exposure of the endopelvic fascia, and mobilization of the periprostatic fat pad, the bladder neck was dissected posteriorly to the level of the seminal vesicles. The bladder neck was transected followed by dissection and removal of the seminal vesicles with bipolar cautery. The rectum was then sharply dissected away from the prostate allowing entrance into the intrafascial plane anteriorly. This plane is followed laterally and cephalad to the vascular pedicle. The pedicle is sharply excised after placement of Hem‐O‐Lock® clips. After, the dorsal venous complex was controlled using the SynchroSeal™ instrument, the urethra was sharply excised and all remaining attachment to the prostate were removed. The specimen was removed in an Endo Catch™ bag. Any remaining bleeding was controlled with 4‐0 Vicryl®. A pelvic lymph node dissection was carried out bilaterally. Finally, the urethral anastomosis was completed in the standard fashion.
Results: We have conducted a handful of RALPs using the da Vinci® robot with the SynchroSeal™ accessory. We have found this instrument to allow for excellent electrocautery, particularly during ligation of the dorsal venous complex, an aspect of this procedure notorious for difficult hemostasis. This system allows for minimal blood loss of often 10 mL or less.
Conclusions: In this video, we describe our experience performing a RALP with the da Vinci® SynchroSeal™ attachment. Our technique is easily reproducible and may offer several benefits including efficient and robust hemostasis.
Robotic Simple Prostatectomy Through the Posterior Transvesical Approach
AC Harbin, S Shekar, G Reyes
Introduction & Objective: Surgical options are limited in patients with benign prostatic hyperplasia (BPH) and gland size larger than 80‐100ml. Robotic simple prostatectomy (RSC) is emerging as a viable surgical option in such patients. However, the lack of standardization of surgical approach can lead to a variety of surgical outcomes. We present our experience with the posterior transvesical approach to RSC.
Methods: We retrospectively reviewed our series of patients undergoing RSC by a single surgeon (AH) at multiple institutions. Pre‐ and post‐operative functional outcomes were obtained using the international prostate symptom score (IPSS), sexual health inventory in men (SHIM) and post void residual (PVR).
Results: A total of 343 patients underwent RSC between September 2015 and February 2021. Demographic and perioperative data can be found in Table 1. Functional outcomes can be found in Table 2. The IPSS was significant improved (p < 0.001) and SHIM was not significant different (p = 0.08) at a median follow up of 7.6 months. Sixteen patients (4.6%) experienced Clavien >2 complications, and the rate of de novo urinary incontinence was 1.5% (urge = 2, stress = 3).
Conclusions: RSC through a posterior transvesical approach should be considered a viable, reproducible approach for symptomatic patients with large gland BPH.
Video Session 12: Single Port Robotic Surgery I
V12: Single Port Robotic Surgery I
S Crivellaro, K Kim, R Meherazin
Single‐Port Transvesical Robotic Radical Prostatectomy: Description of Technique
A Beksac, M Abou Zeinab, ZR Schwen, A Aminsharifi, J Kaouk
Introduction & Objective: We sought to describe our surgical technique for single port (SP) transvesical robotic radical prostatectomy using the da Vinci SP® surgical system (Intuitive Surgical, Sunnyvale, CA, USA).
Methods: Seventeen patients underwent SP radical prostatectomy through a transvesical approach. Patient selection criteria was localized intermediate risk prostate cancer with less than 7% lymph node metastasis rate. Through a 3 cm suprapubic midline incision the bladder was entered and a GelPOINT mini (Applied Medical, Rancho Santa Margarita, CA, USA) was inserted into the bladder. Floating docking technique was used. Through the gel port, the dedicated 25 mm multichannel port and a 12 mm assistant port were introduced. The surgical steps for transvesical radical prostatectomy were performed in the following order. 1) Posterior bladder neck dissection, 2) Vas deferens and seminal vesicle dissection, 3) Posterior dissection, 4) Anterior bladder neck and prostate dissection, 5) Pedicle and neurovascular bundle dissection, 6) Posterior Reconstruction and Urethrovesical Anostomosis, 7) removal of prostate through a single incision and bladder closure.
Results: Mean patients' age was 62.2 years and the mean preoperative prostate‐specific antigen (PSA) was 5.8 ng/ml. Single port robotic transvesical radical prostatectomy was performed successfully in 17 patients successfully without the need for additional port placement or open conversions. Average operative time was 197 minutes. Mean estimated blood loss was 150 mL. Three patients had focal positive surgical margins. Mean length of stay was 4.5 hours (outpatient setting). Median time with a Foley catheter after surgery was 4.5 days. 13 patients (76.5%) had immediate continence (0‐1 pad) after foley removal. No perioperative or postoperative complications were recorded.
Conclusions: We demonstrated the feasibility of single‐port robotic transvesical radical prostatectomy using a novel SP robotic platform. This approach provides additional advantages including single incision, no additional ports, minimal opioid use, immediate continence, and same day discharge without intraoperative and oncological outcomes compromise.
Single Port Robotic Radical Cystectomy with Intracorporeal Creation of Neobladder: Description of Technique and Perioperative Outcomes
M Billah, F Sheckley, R Sawhney, N Gopal, M Stifelman, D Ali, S Ahsanuddin, G Lovallo, M Ahmed
Introduction & Objective: The FDA approved the use of the DaVinci single port robotic system in 2018. The literature reports its use with radical cystectomy with an intracorporeal ileal conduit. However, there has been no publication of single port radical cystectomy with intracorporeal creation of neobladder to our knowledge. This study describes the technique in both male and female patients and illustrates preliminary outcomes. A learning curve was involved but the overall transition from multiport to single port was smooth.
Methods: This is an IRB approved prospective cohort study on robotic radical cystectomy. We identified five patients who underwent a single‐port radical cystectomy with intracorporeal neobladder creation. We performed surgery by duplicating the institutional steps of the multiport approach.
Results: The video presented shows the possibility to perform an entire radical cystectomy procedure was performed without the need to intervene with open laparotomy using a single 25 mm abdominal incision and the vaginal orifice. Through these two accesses, it was Single‐port radical cystectomies with intracorporeal neobladder were successfully performed in all five patients. The mean operative time was 311 minutes, with an average blood loss of 120 ccs. The average length of hospital stay was five days. There were no intraoperative or immediate postoperative complications.
Conclusions: This study demonstrates the feasibility of single‐port radical cystectomy with intracorporeal neobladder creation in both sexes. More extensive, multi‐institutional studies comparing single‐port and multiport radical cystectomy are needed to determine this approach's benefits.
Withdrawn
Use of Remotely Operated Suction Irrigation (ROSI) during Single‐Port Robotic Surgery
M Billah, S Ahsanuddin, J Cadwell, MD Stifelman, R Sawhney, R Harrison, M Ahmed
Introduction & Objective: The da Vinci Single‐Port robotic system was approved by the Food and Drug Administration for use in urologic procedures in 2018 and since, its implementation has become widespread. Given the new technology, surgeons have made adaptations to previous methods utilized with multiport surgery. In particular, use of rigid suction has largely been abandoned in favor of remotely operated suction irrigation (ROSI) with a flexible suction tip. The objective of this video is to demonstrate the use of ROSI across various urologic procedures.
Methods: We reviewed cases performed by a single surgeon at a single institution. Surgical procedures included radical prostatectomy, retroperitoneal partial nephrectomy, transabdominal partial nephrectomy, pyeloplasty, retroperitoneal lymph node dissection and inguinal lymph node dissection.
Results: The video demonstrates effective and reproducible use of the ROSI system across various urologic procedures. The ROSI system offers key advantages over rigid suction when utilizing the single‐port robotic system. It enables truly single incision surgery by removing the plus one port required for rigid suction. The flexible tip allows the device to easily fit through the gel port alongside the single‐port trocar. The device can be operated by either the surgeon or the bedside assistant.
Conclusions: There are certain challenges and concerns that surgeons should be aware of when working with the ROSI system. The manipulation of the ROSI device requires use of one arm and thus, its location and use must be carefully planned. The ROSI system can become clogged or malfunction requiring troubleshooting by knowledgeable and experienced staff. Despite its potential issues, the ROSI system is a safe and effective tool when used during single‐port robotic surgery and has many advantages over rigid suction. Its use can be extended across several urologic procedures including, but not limited to, partial nephrectomies, radical prostatectomies, and lymph node dissections.
Technical details comparing the da Vinci SP and da Vinci Xi approach to radical prostatectomy
M Covas Moschovas, S Bhat, T Rogers, S Reddy, J Noël, C Chew, E Mazzone, A Mottrie, V Patel
Global Robotics Institute
Introduction & Objective: Different groups have described the da Vinci SP approach to radical prostatectomy since the FDA clearance in 2019. However, the comparison between the SP robot and the previous multiport versions, such as the Xi, is still unclear. This video describes a side‐by‐side technique comparison between the da Vinci SP and Xi approach to radical prostatectomy (RP).
Methods: We performed a side‐by‐side video compilation illustrating the differences between the SP and Xi techniques in key points of a robotic‐assisted radical prostatectomy. The video was divided into ten different steps since the trocar placement until the anastomosis.
Results: The trocar placement is the first difference between both robots. While in the Xi we use six ports, in our SP technique, only two ports are placed. We illustrated the relocation pedal application during the SP access to different surgical sites. During the bladder dropping, the necessary traction is performed with the Prograsp in the Xi and with the Cadiere in the SP. We use the same technique concept to approach the bladder neck and seminal vesicles (SV). However, with the SP console, we do not have the same traction provided by the Xi instruments. The posterior prostate dissection is another difference because, with the Xi, we use the 30 degrees lens toggled (looking up), while with the SP, we perform the necessary deflection between the Denonvilliers layers. Also, the lateral prostate dissection and apical access are performed with the same technique in both robots. After the urethra division, the posterior reconstruction and anastomosis are performed with barbed suture. Finally, another difference is noted in the suturing step because the SP has less angulation and amplitude due to the lack of wrist‐like articulations founded in the Xi.
Conclusions: In our experience, we maintained the assistant trocar in the SP approach to avoid modifying or adapting our established technique performed with the multiport console. The surgical technique concept is the same with both consoles. However, the SP has a new learning curve in terms of port placement, multiple scope deflections, relocation pedal applications, lower traction strength, and different suturing angles.
Single Port Robot‐assisted Laparoscopic Radical Prostatectomy (SP‐RALP) A Side‐by‐Side Comparison of Extraperitoneal and Transperitoneal approaches
KN Meilika, A Beksac, KE Okhawere, O Ige, TG Korn, KK Badani
The Icahn School of Medicine at Mount Sinai
Introduction & Objective: in this side by side video we are comparing and contrasting the surgical steps of extraperitoneal and transperitoneal approaches to single port robot‐assisted laparoscopic radical prostatectomy (SP‐RALP).
Methods: We are presenting the extraperitoneal and transperitoneal approaches of single port robot‐assisted laparoscopic radical prostatectomy (SP‐RALP), The extraperitoneal approach is demonstrated in a 70‐year‐old gentleman with no significant past medical or surgical history. PSA was 5 ng/mL, trans‐rectal ultrasound (TRUS) guided biopsy demonstrated prostatic adenocarcinoma in 1 out of 12 cores with Gleason grade: 4 + 3 = 7. Prostate MRI showed a prostate size of 65 cc and 1x1 cm PI‐RADS 4 lesion in the basal part of left lobe. The transperitoneal approach is demonstrated in a 72‐year‐old gentleman with no significant past medical or surgical history. PSA was 13 ng/mL, and trans‐rectal ultrasound (TRUS) guided biopsy demonstrated prostatic adenocarcinoma in 4 out of 12 cores with Gleason grade: 4 + 4 = 8. Prostate MRI showed a prostate size of 180 cc and 2x1 cm PI‐RADS 4 lesion on the mid left lobe.
Results: The surgical and pathological characteristics of the 2 patients are shown in this table Below
Conclusions: The extraperitoneal and transperitoneal approaches to single port robot‐assisted laparoscopic radical prostatectomy (SP‐RALP) are technically feasible and reproducible with good post‐operative clinical course. A larger sample size is required to validate the extraperitoneal approach, which may have a unique application for single port robotic surgery.
Extraperitoneal Single Port Robot‐assisted Laparoscopic Radical Prostatectomy (SP‐RALP) After Prior Bilateral Laparoscopic Inguinal Hernia Repair
KN Meilika, KE Okhawere, A Beksac, O Ige, TG Korn, KK Badani
Introduction & Objective: In this video we are demonstrating the surgical steps of extraperitoneal approach of single port robot‐assisted laparoscopic radical prostatectomy (SP‐RALP) after prior bilateral laparoscopic inguinal hernia repair
Methods: We are presenting the extraperitoneal approach of single port robot‐assisted laparoscopic radical prostatectomy (SP‐RALP) in a 70‐year‐old gentleman with no significant past medical history, and a past surgical history of bilateral laparoscopic inguinal hernia repair. PSA was 6 ng/mL, trans‐rectal ultrasound guided (TRUS) biopsy demonstrated prostatic adenocarcinoma in 9 out of 12 cores with Gleason Grade: 3 + 4 = 7. the prostate MRI showed a prostate size of 60 cc and three PI‐RADS 4lesions.
Results: The operative time was 140 minutes, the estimated blood loss (EBL) was 112 mL, and patient was discharged next day, the catheter was removed on post‐operative day 6 and final pathology was adenocarcinoma of the prostate Gleason grade: 4 + 4 = 8, negative surgical margins and negative lymph nodes.
Conclusions: The extraperitoneal approach to single port robot‐assisted laparoscopic radical prostatectomy (SP‐RALP) is technically feasible even in challenging situations like fibrosis after prior pelvic surgeries. larger series and experience are required to validate this technique
Pure Single Port Redo Robot‐Assisted Laparoscopic Inguinal Lymph Node Dissection for Penile Cancer
KN Meilika, A Beksac, KE Okhawere, O Ige, TG Korn, KK Badani
Introduction & Objective: In this video, we are demonstrating the surgical steps of pure single port redo Robot‐assisted laparoscopic inguinal lymph node dissection for recurrent squamous cell carcinoma of the penis.
Methods: This is the surgical steps of pure single port redo‐robotic inguinal lymph node dissection in a 71‐year‐old active male smoker with a medical history of coronary heart disease, diabetes, hypertension and past surgical history of partial penectomy for squamous cell carcinoma of the glans followed by Left robot‐assisted laparoscopic inguinal lymph node dissection. Current surveillance images showed enlarged left inguinal lymph nodes as the solitary site of disease and no other evidence of disease.
Results: The operative time was 125 minutes, the estimated blood loss (EBL) was 20 ml, the patient was discharged the next day, and the final pathology was metastatic squamous cell carcinoma (SCC) in two excised lymph nodes.
Conclusions: The pure single port robot‐assisted laparoscopic inguinal lymph node dissection is technically feasible and reproducible even in challenging situations like fibrosis after prior surgeries with minimal post‐operative skin scaring. More research is required to validate this technique.
Single Port Simple Prostatectomy
S Talamini, S Crivellaro
Introduction & Objective: The surgical management of large gland benign prostatic hyperplasia (BPH) can pose significant challenges. In the large gland, guidelines suggest the use of innovative approaches including robotic simple prostatectomy, traditionally performed using a multiport robotic platform. The daVinci Single Port robot offers a less invasive approach to the simple prostatectomy. We present our experience using the Single Port robotic assisted simple prostatectomy (SP RASP) and demonstrate our surgical approach.
Methods: Our patient is an 85yo male with a long history of urinary retention, and was catheter dependent. He failed medicotherapy and was interested in definitive surgical management. The transvesical approach was facilitated using cystoscopic guidance with CO2 insufflation. A suprapubic incision, three finger breadths above the pubic bone was carried down until the bladder was encountered, and a mucosal diverticulum was created. 0‐Vicryl stay stitches were placed before opening the mucosa. The light from the cystoscope is visible through the diverticulum and guides the dissection. The gland was enucleated in an avascular plane, and the peripheral zone of the prostate, urethra, and bladder neck were reapproximated using a barbed V‐loc suture and Ethibond suture.
Results: Our experience with the first 16 cases performed at our institution reveals a significant decrease in mean postoperative IPSS (25.5 vs 6.4, p‐value <0.01), PVR (200 vs 44.6, p‐value 0.048), PSA (11 vs 0.6, p‐value 0.5), and no patients developed stress urinary incontinence. One patient developed de novo urge urinary incontinence. The patient highlighted in the video was discharged on postoperative day (POD) 0, his catheter removed POD 5, and his post void residual was 45ml on follow up.
Conclusions: The SP platform provides a less invasive approach than the traditional multiport RASP. As the peritoneum is not entered during the dissection, and a single small cystotomy is made, patients may be discharged on the same day as their surgery. We suspect that postoperative continence rates are improved over other treatment modalities for large gland BPH due to the bladder neck reconstruction, though a larger cohort will be needed to further evaluate this. Though SP RASP is within the initial learning curve at our institution, early results demonstrate the role for this modality in the treatment of large gland BPH.
Single‐Port Robotic Transvesical Total Prostatectomy
MJ Zuberek, O Feldman‐Schultz, S Crivellaro
Introduction & Objective: 20 years after the launch of a Multiport (MP) surgical robot, Intuitive Surgical (Sunnyvale, CA.) has recently introduced a new Single‐Port Robotic Platform (SP) for urologic procedures. Due to the innovative design of the camera system, instruments, and single robotic trocar this system can be now used in a more confined space. In this video we describe a novel technique for transvesical total prostatectomy. We postulate that this technique can be used as a treatment option for patients with benign prostatic hyperplasia (BPH) and low risk prostate cancer on active surveillance (AS) in order to treat the LUTS and help better manage the AS.
Methods: 77 yo male patient with ASA II, and no previous surgical history was recruited for this procedure. He was diagnosed with prostate cancer via biopsy with a pathologic stage of T1c. Pre‐biopsy PSA was 4.2 ng/ml. Biopsy revealed Gleason 6 with a low volume disease. Patient elected to proceed with AS. During his time on AS his LUTS became severe and refractory to medical therapy and he developed severe ED. PVR at that time was 150 cc. The patient was offered continual AS, additional medical therapy, or surgical intervention. patient elected to proceed with surgical intervention.
Results: The patient was admitted on the outpatient basis to the University of Illinois Hospital and Health Sciences System. A mini Gelpoint was introduced in a 3 cm transvesical incision. The SP was docked with a floating technique. The total prostatectomy was performed dissecting the “intrafascial” nerve sparing plan from 12 o' clock to 5 and 7 o'clock, entering the same plane at 6 o'clock, transecting the vases and seminal vesicles to the apex and transecting the pedicles on both sides. The anterior part of the prostate and the urethra were finally dissected. The anastomosis was performed with 2 running barbed sutures. There were no complications. The patient was discharged the same day and the catheter removed in 7 days. Final pathology revealed 80gm prostate with Gleason 6 adenocarcinoma and negative margins. 3 mo follow up demonstrated IPSS score of 5, PSA of 0.1 ng/ml, and PVR of 20 cc. The patient reports no stress urinary incontinence.
Conclusions: Transvesical SP total Prostatectomy is a viable, minimally invasive surgical technique for patients with bothersome LUTS refractory to medical therapy and low grade, localized prostate cancer in AS.
SP Extraperitoneal Radical Prostatectomy: Technique and Lessons on the Brink of 200 Cases
ZR Schwen, A Beksac, L Lenfant, A Aminsharifi, M Abou Zeinab, J Kaouk
Introduction & Objective: Enthusiasm for the robotic extraperitoneal radical prostatectomy (RERP) has been renewed with the introduction of the Da Vinci Single Port (SP) robotic platform. Our initial experience has revealed many advantages including easy extraperitoneal access, no need for steep Trendelenburg, and no assistant ports. Additionally, perioperative morbidity is reduced with high rates of same day discharge and reduced opioids.
Methods: After 185 cases, we describe our modified technique since we began the SP RERP in 2018. Primary outcome includes successful completion of the case extraperitoneally, without any steep Trendelenburg or conversions to a transperitoneal or open approach. Secondary outcomes of the study include same‐day discharge rate and opioid‐free recovery.
In the supine position, a 3cm infra‐umbilical incision is made. The anterior rectus fascia is incised and a kidney‐shaped balloon dilator is placed into the space of Retzius to develop the extraperitoneal space. Using an Alexis wound retractor and GelPOINT (Applied Medical, Rancho Santa Margarita, CA, USA), the “floating dock” technique is employed, through which the SP cannula, a 12mm Airseal, and a Remotely Operated Suction Irrigation (ROSI) suction tubing (Vascular Technology, Nashua, NH, USA) are placed. The SP is side‐docked in a camera‐up orientation. No assistant port is placed.
Surgical steps for the SP RERP replicate those of a standard multiport approach. Notable technical highlights include use of the robotic clip applier, which obviates the need for an assistant port in addition to use of the urethral catheter for an additional method of suctioning the prostate bed prior to the anastomosis. Following completion of the anastomosis, the specimen is placed in a specimen retrieval bag and the SP is undocked. Prior to closure of the fascia, the peritoneum is fenestrated to prevent accumulation of lymphatic fluid in the extraperitoneal space, which has eliminated our rate of symptomatic lymphoceles. No drain is placed.
Results: All 185 cases underwent successful completion of the SP RERP without any conversions to transperitoneal or open access, steep Trendelenburg, or assistant ports. We report a 94% same‐day discharge rate, corresponding to a median hospital stay of 4.8 hours (IQR 1.9‐70.5). Notably, only 51 patients (27.5%) required opioids post‐operatively corresponding to a 72.5% opioid‐free rate.
Conclusions: Our growing experience with the SP RERP confirms our initial observations demonstrating the advantages of avoiding steep Trendelenburg, staying extraperitoneally, and avoiding assistant ports to further minimize the morbidity of the radical prostatectomy.
Introduction & Objective: Laparoscopic simple prostatectomy using a multiport robotic‐assisted surgery for enlarged prostate have been frequently performed and shown to be safe and effective. Amongst its other advantages, the novel single‐port robotic surgical technology allows the surgeon to operate completely transvesically, avoiding the adverse effects of insufflating and entering the peritoneum.
Methods: Sixteen patients underwent TV SP simple prostatectomy from January 2019 to October 2020. A video was recorded for one of the procedures, which represents the general concept of the technique. A 2.5 cm suprapubic incision was made and developed through the rectus fascia, splitting the rectus muscles in the midline. The bladder was then distended, and stay sutures were used to maintain access to the dome of the bladder. A cystotomy was made and a small Alexis® wound protector and GelSeal® cap were placed tranvesically. The single port trocar and a 12 mm port was placed through the cap. The SP DaVinci® robot was then utilized to perform the simple prostatectomy tranvesically. Perioperative data and outcomes were collected in an IRB approved prospective database and analyzed.
Results: All 16 procedures were performed through a 25 mm single incision without the need to open and without any intraoperative or 30‐day postoperative complications. The average prostatic volume on ultrasound was 145 grams. Average operative time for these procedures was 122 minutes with 38.3 mL estimaged blood loss. All patients were discharged home on post‐operative day 1. Average Foley catheter duration was 5 days.
Conclusions: A SP robotic‐assisted laparoscopic surgery via the TV approach is a novel technique that can be used for a benign prostatomegaly safely and effectively. Its advantages to the multiport robotic approach need to be further studied, as prospective data and analysis comparing the two approaches are ongoing.
Video Session 13: Robotic Surgery: Kidney I
V13: Robotic Surgery: Kidney I
A Kumar, RB Nadler, F Porpiglia
Robotic approach to Vena Cava recurrence of Renal cell cancer after prior radical Nephrectomy
N Pokala
Introduction & Objective: Recurrence of Renal cell cancer in the Inferior vena cava (IVC) is rare after a prior radical nephrectomy. This patient presented with a IVC recurrence 3 years after a right radical nephrectomy for renal cell cancer. This video demostrates the first case of IVC recurrence that was managed with the robotic approach and also demostrates the technical modifications required for managing these pateints.
Methods: A 59 year old gentleman was referred to our institution with renal cell cancer recurrence in the Inferior vena cava three years after a right radical nephrectomy. Pateint was healthy with controlled hypertension. The previous laparoscopuic radical nephrectomy was performed for a pT3a Fuhrman grade 2 RCC. The renal vein was positive for tumor at the first radical nephrectomy. The pateint was followed witha Ct scan for a year and was then lost to follow‐up. he presented 3 years later with a CT suggestive of an level 2 subhepatic IVC thrombus and asingle pulmonary nodule.
Risks and benefits were discussed and the patient was recommended a robotic IVC thrombectomy
Results: Standard right radical nephrectomy postion and ports placed. The right renal artery was not dissected in the inter‐aortocaval grooove, but the procedure was identical to the standard roobtioc IVC thrombectomy. Eeven afetr succesful contorl of the IVC we noted increased bleeding from the tumor thrombus itself as an arterio‐venous fistula had developed at the previous staple site for the hilum. The bleeding stiopped on controlling the right renal artery. Total console time ws 290 minutes. Pateint developed a pneumothorax needing a chest tube. lenght of stay was 4 days.
Lung lesions was biopsied which confirmed a single metastasis. He was started on Nivolumab and the lung lesions almost disappeared and no new lesions were noted at one year follow‐up
Conclusions: Inferior Vena cava recurrence after a radical nephrectomy is rare. This video demostrates that a robotic approach is fasible and safe in thsi situation. Complete control of the bleeding may not be feasible due to the presence of an arteriovenous fistula and the conrol of the right renal aretery is recommended even in the presence of a prior radical nephrectomy.
Robotic Pringle Manoeuvre and Suprahepatic Inferior Vena Cava Control for Retrohepatic Level 3B IVC Thrombi from RCC
N Pokala
Introduction & Objective: Robotic techniques for the management of advanced Renal cell cancer is evolving and more complex thrombi can be safely tackled robotically. Retrohepatic thrombi at or above the level of the hepatic veins are challenging because the IVC needs to be controlled above the liver and also requires control and clamping of the hepatic artery nd portal vein. This video demonstrates the technique for performing this robotically.
Methods: Two male patients in presented with right renal masses and level 3b Inferior vena caval thrombi. The metastatic work‐up was negative and both patients were healthy. Risk benefits and alternatives were discussed andbpatients underwent robotic right nephrectmies and thrombectomy successfully. One of the patients was a Jehovah's witness who did not consent for blood transfusion but consented for normovolemic hemodilution.
The suprahepatic IVC control and a Pringle manoeuvre were performed in the steep reverse Trendlenberg with a standard liver resection port configuration. The patient was then placed in the modified lareral position for the control and extraction of the thrombus from the IVC and the right radical Nephrectomy.
Results: The video demonstrates that suprahepatic IVC control and pringle can be easily achieved. Both patients underwent sucessful operations. The mean operative time was over 10 hours. One of the patients required excision of the IVC segment and closure just below the hepatic veins and just above the left renal vein. This patient developed post‐operative lower limb edema and had a prologed hospital stay. At recent 9 months follow‐up both patients were cancer free.
Conclusions: Robotic Suprahepatic Inferior vena cava control and Pringle manoeuvre are feasible and safe robotically and Level 3b thrombi can be tackled robotically and safely in experienced hands.
Introduction & Objective: The risk of recurrent disease after partial nephrectomy is increased by high risk disease characteristics at the time of initial resection. Surveillance imaging after partial nephrectomy is of the utmost importance since this is the mechanism by which the majority of recurrences are detected. Traditionally, local recurrences have been treated via an open surgical approach. However, we propose treating local or peri‐renal recurrences via a robotic surgical approach.
Methods: This is a descriptive case report demonstrating an example of our institution's experience performing robotic re‐do partial nephrectomies. The specific steps and materials for completing this procedure were described in one patient who is a 75‐year‐old gentleman with history of a 3.3cm right renal mass. The patient originally underwent a robotic partial nephrectomy with final pathology of pT1aNxMx clear cell renal cell carcinoma (ccRCC) with negative margins.
Results: The patient had no evidence of disease recurrence until 27 months postoperatively, at which time a 1.4cm right peri‐renal mass was detected. A biopsy was obtained and confirmed recurrent ccRCC. Patient opted for a robotic re‐do partial nephrectomy. He was positioned in the usual left lateral position. After access to the abdominal cavity was obtained with the DaVinci Xi robotic surgical system, the colonic attachments were taken down. This portion of the procedure required an extended duration of time secondary to adhesions from prior surgery. This was followed by Kocherization of the duodenum and incision into Gerotas fascia with exposure of the medial aspect of the kidney. Intraoperative ultrasound (US) clearly identified the boundaries of the recurrent mass. The fat was incised circumferentially down to the renal parenchyma with a wide margin. This mass extended toward the old Hem‐o‐lock clips from the prior renorrhaphy. The base of the tumor was excised off the underlying renal parenchyma. Pathology confirmed the presence of recurrent ccRCC. There was noted to be an area just under the excision site concerning for possible residual disease, so a second deeper margin was obtained. US was repeated followed by ablation of the excision site with the argon beam. The patient tolerated the procedure well with an estimated blood loss of 20mL and an operative time of 3 hours and 8 minutes. Only ∼1 hour was spent on excision of the mass itself. The patient was discharged home on postoperative day number one. Final pathology was consistent with recurrent clear cell RCC with a negative deep surgical margin.
Conclusions: Robotic re‐do partial nephrectomy is a safe and feasible option for patients with peri‐renal recurrence.
Robot‐Assisted Laparoscopic Nephroureterectomy in a Horseshoe Kidney: Use of Indocyanine Green and Near‐Infrared Imaging Assists with Intraoperative Assessment of Vascularity
B Desroches, N Velázquez, R Munver
Introduction & Objective: Nephroureterectomy in a horseshoe kidney presents challenges due to malrotation of the kidney, anomalous vasculature, and difficulty in mobilization of the fused renal moieties. In precisely separating the right and left renal moieties, hemostasis is dependent on controlling the vascular supply to the isthmus. We present a technique for robot‐assisted laparoscopic (RAL) left nephroureterectomy in a 74‐year‐old male with high grade multifocal left upper tract urothelial carcinoma (HG UTUC) in a horseshoe kidney. Preoperative CT imaging demonstrated aberrant renal vasculature. Indocyanine green (ICG) and near‐infrared fluorescence (NIRF) imaging (FireFlyTM, Intuitive Surgical, Inc.) was utilized to delineate the renal vasculature and aid in precise division of the isthmus for maximal parenchymal preservation.
Methods: A four‐arm robotic transperitoneal approach was used with four 8 mm robotic trocars and one 12 mm assistant trocar. After mobilization of the colon, intraoperative ultrasound aided in localizing the renal hilum and isthmus below the investing tissues. Further dissection revealed the anterior location of the renal pelvis, proximal ureter, and anomalous vascular anatomy. The gonadal vein, main renal vessels, and accessory renal vessels were ligated and transected individually. The adrenal was left in situ. The lower portion of the left renal moiety was exposed and the isthmus was identified. Intravenous injection of ICG and use of NIRF revealed fluorescence pertaining to the vascularized parenchyma of the right moiety, and absence of fluorescence in the ischemic left moiety. NIRF confirmed the absence of additional anomalous renal vessels, while clearly delineating the interface between vascularized and devascularized tissue in the isthmus. The isthmus was sharply transected with robotic scissors, and the vascularized parenchyma was oversewn using a sliding clip technique, with excellent hemostasis. The distal ureterectomy, extravesical bladder cuff excision, and cystorrhaphy were then completed.
Results: The operative time was 2 hours 48 minutes with an estimated blood loss of 70 cc. The patient was discharged on the first postoperative day. The urethral catheter was removed after 6 days. Pathology revealed extensive pTa HG UTUC of the left renal pelvis and ureter, absence of lymphovascular invasion, and negative surgical margins.
Conclusions: RAL nephroureterectomy in a horseshoe kidney can be facilitated with judicious use of ICG and NIRF to aid in delineation of renal vasculature, confirmation of renal moiety devascularization, and in precise transection of the isthmus.
Robotic Radical Nephrectomy For Recurrent Renal Tumors
KN Meilika, KE Okhawere, A Beksac, O Ige, TG Korn, KK Badani
Introduction & Objective: Radical nephrectomy for recurrent renal tumors is a challenging procedure, in this video, we are presenting 2 cases of robotic radical nephrectomy for recurrent renal tumors.
Methods: We are demonstrating the robotic approach for recurrent renal cell carcinoma in 2 patients with prior partial nephrectomy: The first case is an example of right robotic radical nephrectomy 1 year after right robotic partial nephrectomy for 2.5 cm endophytic clear cell renal cell carcinoma. We are presenting both the initial partial nephrectomy and the subsequent radical nephrectomy. The second case is a right robotic radical nephrectomy 2 years after a right open partial nephrectomy Importantly, this case demonstrates the extreme difficulty in dealing with hilar fibrosis and bleeding.
Results: We have performed 17 salvage radical procedures. The Outcome data is seen in the Table below:
Conclusions: This video demonstrates examples of complex re‐do renal surgery. The robotic approach is a safe and reasonable option in this complex setting.
Robotic Metastectomy for Recurrent Renal Tumors
KN Meilika, A Beksac, KE Okhawere, O Ige, TG Korn, KK Badani
Introduction & Objective: Metastectomy of isolated lesions is appropriate in selected patients, this is supported by retrospective studies that showed long disease‐free intervals and median overall survival rates of 35% to 50%. In this video, we are presenting 2 cases of robotic metastectomy for solitary recurrent renal tumors.
Methods: The robotic approach is demonstrated through 2 case examples: The first case is an example of robotic excision of solitary 2 cm recurrent nodule close to the left adrenal gland, 1 year after robotic left radical nephrectomy for clear cell renal cell carcinoma. The second case is a robotic excision of 2 lesions, 1 cm left recurrent renal mass and a 3 cm retroperitoneal mass, 5 years after open left partial nephrectomy for chromophobe cell renal cell carcinoma. These 2 lesions are the only sites of metastasis, so the decision was made for repeat robotic partial nephrectomy and excision of retroperitoneal enlarged lymph nodes.
Results: Both patients went home next day without complications. The first case pathology was clear cell carcinoma with negative margins. Second case was recurrent chromophobe RCC with negative margins. Both patients remain without disease on follow up.
Conclusions: Robotic metastectomy for recurrent renal tumors is a safe and reproducible approach as it provides clear identification of planes and meticulous dissection of retroperitoneal fibrosis and scaring from previous surgery. Intraoperative ultrasound is crucial for tumor identification.
Selective Clamping for Robotic Partial Nephrectomy Using Indocyanine Green
J Dungca, J Baber, M Ferretti, N Patel
Introduction & Objective: Robotic partial nephrectomy is our preferred approach for small renal masses. When feasible, we have elected use of selective clamping technique to reduce overall kidney ischemia time and assist in renal preservation. Utilization of Indocyanine Green permits safe selective clamping technique.
Methods: We present a 61 year old male found to have a 3cm anterior renal mass incidentally. Patient has a history of diabetes and hypertension so renal preservation was desired. We performed a robotic partial nephrectomy with selective clamping of anterior arterial branch. Partial ischemia of the renal bed was confirmed using ICG. Patient tolerated procedure well.
Results: Patient tolerated the procedure well. There was a warm ischemia time of 18 minutes. At 1 year follow up there are no complications and no evidence of recurrence. The patient's GFR remains normal.
Conclusions: Use of indocyanine green is helpful as part of selective clamping for partial nephrectomy to improve feasibility. Further comparative studies may be warranted to determine if improved overall outcomes with selective clamping and partial nephrectomy
Robotic Retroperitoneal Radical Nephrectomy
M Said, RL Steinberg, CR Tracy, P Gellhaus
Introduction & Objective: A robotic approach to renal surgery has been shown to be safe and effective and is typically performed in a transperitoneal fashion. Retroperitoneal surgery avoids entry into the peritoneal cavity, obviating the need for lysis of intra‐abdominal adhesions and mobilization of visceral organs. Additionally, it can be considered in the super morbidly obese, those with end stage renal disease utilizing peritoneal dialysis and is a necessary tool for failed retroperitoneal partial nephrectomy. This video demonstrates a step‐by‐step technique for performing a robotic retroperitoneal radical nephrectomy. We present a sample case and share our institutional outcomes.
Methods: A 63‐year‐old male presented with a right 7.5 cm enhancing renal mass. He recently underwent an emergent right hemi‐colectomy for bowel hemorrhage and recovered. He underwent a robotic‐assisted laparoscopic right retroperitoneal radical nephrectomy, with the steps of the procedure presented here.
We prospectively gathered demographic data, as well as perioperative and oncologic outcomes from the robotic retroperitoneal radical nephrectomy cases performed at our institution.
Results: Five cases were reviewed. All patients had prior significant open intra‐abdominal surgery. Four patients had renal cell carcinoma, while one had a non‐functioning hydronephrotic kidney. The mean age was 61.4 years and mean BMI was 36.2. Mean operative time was 225 minutes (range: 186‐280) and median estimated blood loss was 60 mL (range: 30–350). For all patients cancer margins were negative. Median length of stay was 3 days (range: 2‐6).
Conclusions: Robotic retroperitoneal radical nephrectomy is feasible and safe. This approach allows the surgeon to avoid the peritoneal cavity while achieving good perioperative results, without compromising oncologic outcomes.
Robotic Radical Nephrectomy and Left‐Sided Level II Caval Thrombectomy: A New Combined Technique
JH Zhang, M Abou Zeinab, ZR Schwen, A Beksac, A Aminsharifi, M Eltemamy, J Kaouk
Introduction & Objective: Robot‐assisted laparoscopic IVC thrombectomy (RAL‐IVCTE) is challenging for left sided tumors due to the need for full IVC control and access to the contralateral hilum. Here, we combined our robotic approach for radical nephrectomy with an open approach to thrombectomy via a supra umbilical incision used also to extract the specimen.
Methods: A 69‐year‐old female was diagnosed with an 8.9cm left renal neoplasm with level II IVC tumor thrombus. She was placed in the left‐side‐up flank position with port placement illustrated in the video. The Da Vinci SI was docked. The descending colon was mobilized and the left gonadal vein was identified and followed to the hilum where an engorged renal vein with caval thrombus was identified. The left renal vein was fully dissected along its course anterior to aorta. The left renal artery was dissected posterior to vein and stapled. The inferior, lateral, and superior attachments of the kidney were taken to include the left adrenal with the specimen. The kidney was left detached with exception of the renal vein. The robot was undocked and the patient was swiftly shifted into supine. A small supra‐umbilical incision was made. The ascending colon and duodenum were mobilized medially. The right renal vein and IVC were identified and fully dissected to the level of hepatic veins. The infrarenal IVC was clamped caudal to the mobile tumor thrombus obliquely to exclude the takeoff of the right renal vein. Due to this oblique clamping method, the right renal artery and vein were left patent during thrombectomy. The IVC was opened longitudinally at the left renal vein takeoff and the thrombus was evacuated. The IVC was closed with 4‐0 prolene. Suprarenal and infrarenal clamps were removed sequentially and the left kidney with adrenal was delivered off the field.
Results: Operative time was 405 minutes. IVC clamp time was 14 minutes. Estimated blood loss was 500cc. Recovery course was uncomplicated. Return of bowel function was demonstrated on post‐operative day 2 with discharge on post‐operative day 4 with minimal pain. Pathology showed clear cell renal cell carcinoma with negative margins.
Conclusions: IVC thrombus associated with large left‐sided tumors require bilateral retroperitoneal access. With a preplanned combined technique, the surgeon may take advantage of robotic visualization for dissection of the large mass and hilum while utilizing a small supra‐umbilical incision for IVC thrombectomy and large specimen retrieval.
Robot assisted laparoscopic partial nephrectomy in Horseshoe kidney: Anatomical challenges and techniques
S SINGH, P Ahluwalia, S Prakash Ojha, G Gautam
Introduction & Objective: Nephron sparing surgery, specifically robotic assisted laparoscopic partial nephrectomy, has become a widely accepted treatment choice for small renal masses. Renal fusion abnormalities, such as horseshoe kidney, are uncommon congenital findings with a frequency of approximately 1 in 200 in the general population. Horseshoe kidney change the position and orientation of the kidney and complicate the treatment of renal disorders. This video demonstrates our technique for the management of a complex cT1b renal mass in a horseshoe kidney.
Methods: A 34‐year‐old gentleman with a history of gross painless hematuria was discovered to have horseshoe kidney on a CT urogram with evidence of 5x5 cm ill‐defined homogeneously enhancing mass in lower pole of left moiety, causing mild distortion of lower pole calyx. This mass was assigned a 9A on the nephrometry scoring scale. CT angiography was done preoperatively to assess the vascular supply and relations to the tumor. Patient was placed in the trendelenburg position with low lithotomy. Preoperative left ureteric catheterisation was done and the da Vinci Xi surgical system was docked. Intestine mobilized by incising peritoneum starting at root of mesentery to expose aorta and kidney. Main renal vessels and accessory vessels dissected free. Intraoperative ultrasound was used and margins of the tumor scored using diathermy. Only the lower accessory artery which was supplying the tumor was selectively clamped with bulldog. 5mg Indo Cyanin Green dye was given IV, and tumor checked under near infra‐red fluorescence. Mass was excised up to normal appearing parenchyma. Pelvicalyceal system closure was done using 4/0 PDS and confirmed by instilling methylene blue via ureteric catheter. Renorrhaphy was done in two layers which was hemostatic at the conclusion of the procedure.
Results: The patient had uneventful course postoperatively. His serum creatinine preoperatively was 1.3, and at the time of his discharge on postoperative day 3, it had returned to baseline. Final pathology showed papillary renal cell carcinoma type 1, Fuhrman nuclear grade 3 and 4.2cm in maximal dimension. The surgical margin was negative for malignancy. The patient is currently under 2 year follow‐up with no recurrence.
Conclusions: Robotic assisted laparoscopic partial nephrectomy can be a valuable addition to the urologist's armamentarium for the treatment of complex renal masses identified in horseshoe kidneys.
Robot‐assisted radical nephrectomy with inferior vena cava tumor thrombectomy: Technique and initial outcomes
S Singh, P Ahluwalia, S Prakash Ojha, G Gautam
Introduction & Objective: Renal tumors involving the inferior vena cava (IVC) appear to be a limitation to the application of laparoscopy. Laparoscopic management had only been reported in a limited fashion for short tumor thrombi not requiring cross‐clamping of the IVC. The first robotic nephrectomy for renal cancer with IVC tumor thrombus was performed in 2008 with the first series reported in 2011, including for larger tumor thrombi requiring IVC cross‐clamping for thrombus extraction. We herein describe our technique in a patient undergoing robot‐assisted radical nephrectomy (RARN) with inferior vena cava (IVC) tumor thrombectomy.
Methods: Our index case is a 46 years old gentleman with history of gross hematuria one month back. MRI abdomen revealed a 9.6 x 6.7 cm mass in upper and mid pole of right kidney with Level II IVC thrombus. Patient was counseled and was offered robotic radical nephrectomy with IVC thrombectomy. Vascular control was obtained with complete cross‐clamping of the vena cava with robotic bulldog clamps. The tumor thrombus was retrieved along with the IVC cuff as it was seen adherent to IVC wall. The specimen was extracted through a pfannensteil incision.
Results: Patient successfully underwent right robotic radical nephrectomy with IVC thrombectomy without open conversion. Console time was 270 minutes with estimated blood loss of 300 ml. No Drain was placed and foley catheter was removed on POD 1. Patient was discharged on POD 3. Histopathology was suggestive of conventional clear cell carcinoma with negative surgical margins. Follow up at 3 months showed no evidence of recurrence.
Conclusions: Robotic nephrectomy in the setting of inferior vena cava tumor thrombus is feasible and can be performed safely in selected patients. Despite the complex and critical nature of these procedures, favorable outcomes and reproducibility can be expected with adequate robotic experience.
En Bloc Resection of Locally Advanced Recurrent Renal Cell Carcinoma After Partial Nephrectomy
A Beksac, KN Meilika, AA Elbakry, KE Okhawere, O Ige, KK Badani
Introduction & Objective: In this video, we present en bloc resection of recurrent locally advanced renal cell carcinoma. Our patient is a 78 year old female who underwent left robotic partial nephrectomy for pT1a clear cell carcinoma with negative surgical margins. Postoperative 4 month imaging revealed a 1.6 cm new enhancing mass inseparable from the descending colon. Patient underwent laparoscopic segmental colon resection for the new tumor. Pathology consistent with metastatic clear cell renal cell carcinoma. 3 months after descending colon resection, cross sectional imaging was performed. Imaging revealed a 1.2 cm left kidney lower pole recurrent mass. Patient was scheduled for robotic left radical nephrectomy and possible segmental descending colon resection.
Methods: The patient was positioned in the full flank position. Pneumoperitoneum was established using a small cutdown incision. Ports were placed in a linear fashion since a DaVinci Xi system was used. Surgery started with standard laparoscopy. Colon was dissected medially by incising the white line of Toldt. However, left colon was stuck to the kidney. Therefore, dissection continued toward the posterior of the kidney. Psoas major was visualized and then dissection moved to the anterior side. Since the colon was stuck to the kidney, a trans mesenteric dissection was done to identify the ureter and the gonadal vein. This plane was developed further towards the proximal. Once the renal hilum was identified, the robot was docked. Renal artery and renal vein were dissected carefully. Gonadal vein was clipped using weck clips. A 30 mm vascular stapler was used for renal artery and 45 mm stapler used for renal vein. The kidney was dissected away from the aorta to the medial side and the spleen to the proximal side. After the nephrectomy was completed, the robot was undocked. Through an extraction incision, the colon is removed and EndoGIA staplers were used for colon resection and re‐anostomosis. Loop colostomy was not done.
Results: Surgical time was 210 minutes. Estimated blood loss 100 ml. Patient was discharged at postoperative day 5 without complications. Pathology revealed pT3a clear cell carcinoma with renal sinus fat invasion. Surgical margins were negative.
Conclusions: This video demonstrates a combination of standard laparoscopy and robot assisted laparoscopy in minimally invasive management of a locally advanced recurrent renal mass.
Robotic Excision of Local Recurrence Post Laparoscopic Radical Nephrectomy
KN Meilika, KE Okhawere, MP Wilson, TG Korn, KK Badani
Introduction & Objective: In this video, we are presenting the surgical steps of transperitoneal robotic excision of the locally recurrent renal tumor after prior laparoscopic right radical nephrectomy.
Methods: The steps were demonstrated in a 40‐year‐old patient, one year after laparoscopic right radical nephrectomy for T3aNo chromophobe renal cell carcinoma (due to sinus fat invasion). The Contrast CT demonstrated a solitary 3x2 cm retroperitoneal mass with no evidence of distant metastasis.
Results: The operative time was 125 minutes, blood loss was 75 ml, and the hospital stay was 23 hours. The pathology of the excised mass was chromophobe renal cell carcinoma with negative margins
Conclusions: Robotic excision of locally recurrent solitary renal tumors is a feasible approach. The utilization of intraoperative ultrasound is an invaluable tool for accurate delineation of the tumor margins and extension. Long‐term oncological outcomes should be evaluated.
Robotic‐assisted laparoscopic heminephrectomy for T3a renal mass in a solitary kidney
J Elyaguov, G Lovallo, M Stifelman, M Ahmed
Introduction & Objective: We review our technique for robotic heminephrectomy in a complex renal mass of a solitary kidney, with a focus on avoiding tense reapproximation of renal parenchyma, vascular compromise, and obstruction of renal pelvis/ureter. We also highlight the technique's safety and reproducibility from preliminary cohort results of complex T3a mass excisions.
Methods: A 64‐year‐old male with a history of right radical nephrectomy for right renal cell carcinoma (RCC) presented with a large left renal mass. CT imaging showed a complex posterior renal mass, at least 8cm and crossing the axial renal midline indicating a high RENAL nephrometry score of 11p. A multi‐port robotic transperitoneal approach was performed. Once the descending colon was mobilized, an intra‐operative ultrasound was used to demarcate healthy versus malignant tissue, and the parenchyma was scored for resection. A clamp was used over the renal artery and the large mass was subsequently resected entirely. Deep tissue margin reflected benign tissue. The pelvi‐calyceal disruptions and excision bed were oversewn with monocryl sutures. The kidney was then repositioned in normal anatomic lie and Gerota's fascia was reapproximated anteriorly with barbed suture and clips, instead of reapproximating the renal parenchyma. The tumor was removed, and a Foley catheter and drain were placed.
Results: There were no peri‐ or post‐operative complications. Operative time was 87min, ischemia time was 23min, estimated blood loss was 100ml. The length of stay was 2 days, whereby the Foley catheter was successfully removed on post operative day 1 and the drain on post operative day 2. Final pathology was T3a clear cell RCC that involved 3 closely adjacent tumors, invading perinephric adipose tissue and free of margins.
Conclusions: Robotic‐assisted heminephrectomy of a T3a renal mass in a solitary kidney without reapproximation of renal parenchyma is feasible and safe, preventing potential hilar and ureteral obstruction and compromise. Preliminary results of our cohort study demonstrate similar successful results for this procedure type.
Moderated Poster SessionModerated Poster Session 28: Robotics/Laparoscopy III
Long Term Comparative Outcomes of Robotic Partial Nephrectomy and Cryoablation in Patients with Solitary Kidneys: A Single Center Analysis
A Beksac, D Corrigan, M Abou Zeinab, ZR Schwen, A Aminsharifi, J Kaouk
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
Introduction & Objective: Patients with solitary kidneys are prone to postoperative acute kidney injury (AKI) following partial nephrectomy (PN). Cryoablation (CA) is a viable alternative to partial nephrectomy (PN) in treating small renal masses of patients with solitary kidneys. In this study, we compared the functional and oncological outcomes of CA and PN in patients with solitary kidney.
Methods: From a single institution, 74 patients with a solitary kidney who underwent small renal mass treatment were selected. 31 patients underwent PN and 43 patients underwent CA. Functional and oncological outcomes were compared between the two groups, with a median follow up of 59.4 months. AKI is defined according to RIFLE (Risk, Injury, and Failure; and Loss; and End‐stage kidney disease) criteria. Linear and logistic regression models were used for functional outcomes analysis, whereas oncological outcomes were analyzed using the Kaplan‐Meier method.
Results: At baseline, the PN group had lower median age (59 years vs 68, p < 0.001) and larger median tumor size (2.80 cm vs 2.0, p = 0.003). AKI at discharge was more common in the PN group (58% vs 2.8%, p < 0.001). eGFR preservation at discharge was higher in the CA group (100% vs 71%, p < 0.001). However, eGFR preservation was similar at one year (92% vs. 88.7%, p = 0.177) and last follow up (84% vs. 83%, p = 0.443). Recurrence rate was higher in the CA group (26.3% vs 3.2%, p = 0.009). Majority of recurrences were treated with repeat ablation (55.4%). Lower recurrence free survival (RFS) rate was seen in the CA group (p = 0.027), however, overall survival (OS) was comparable between the two groups (p = 0.16).
Conclusions: CA is shown to decrease the perioperative AKI compared to PN. However, long term functional outcome is similar. Oncologically, CA has significantly higher recurrence rate and repeat treatment rate.
Tumor Size Accurately Predicts Functional Outcomes following Radical Nephrectomy
A Beksac, KE Okhawere, D Ranti, KN Meilika, TG Korn, KK Badani
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
Introduction & Objective: Existing literature has shown that functional outcomes after partial nephrectomy are well correlated with renal parenchymal volume loss. Despite this, the impact of pre‐surgical kidney and tumor volume has yet to be established. We sought to analyze the association between volume loss and functional outcome following radical nephrectomy (RN).
Methods: We identified patients for our institutional database undergoing RN for a T2‐4 renal mass between January 2014 and June 2018. Patients with data establishing baseline measures of eGFR, ipsilateral and contralateral volume and postoperative eGFR up to 12 months postoperatively were included. Ipsilateral kidney volume was measured as tumor volume and functional volume separately. Functional outcome was measured as percentage change in eGFR between pre‐surgical baseline and 12 months follow‐up. Unadjusted and adjusted linear regression models were evaluated to understand the relationship between functional outcomes and covariate inputs.
Results: 55 total patients were included in the study. Median age was 67 years old, median baseline eGFR was 71.00, ipsilateral functional volume was 149.39, and 12‐month percentage change in eGFR was ‐27.79%. In the unadjusted models, CCI (β = 5.01 95% CI: 0.51, 9.51), tumor size (β = ‐2.95 95% CI: 0.51, 9.51), baseline GFR (β = ‐0.64 95% CI: ‐0.91, ‐0.36) were significantly associated with percentage change in eGFR at 12 months. In the adjusted models, tumor size (β = ‐2.07 95% CI: ‐4.00, ‐0.13) and baseline eGFR (β = ‐0.55 95% CI: ‐0.51, ‐0.18) remained significant predictors percentage change in eGFR at 12 months after controlling for CCI and ipsilateral volume. Ipsilateral volume and CCI were not statistically significant.
Conclusions: Baseline kidney function and tumor size independently predicted functional kidney outcomes after RN. However, tumor volume was not a predictive factor. Studies with larger sample size would be useful to further validate these findings.
Robot Assisted Radical Prostatectomy Following Kidney Transplantation
M Shahait, A Sandberg, RW dobbs, J walker, J Kim, P Mucksavage, D Lee
King Hussein Cancer Center
Introduction & Objective: Management of prostate cancer in kidney transplant recipients poses a unique surgical challenge because of the risk of direct or indirect injury to the transplanted kidney that may occur as a result of its anatomical proximity to surgical or radiation fields. Prior reports have consisted of small case series of relatively few patients. Herein, we report the largest single center study of the perioperative, functional, and oncological outcomes of RARP in kidney transplant recipients.
Methods: Between January 2014‐2019, 14 kidney transplant recipients with prostate cancer underwent RARP at a single center. Clinical and pathological features, perioperative and postoperative complications were retrospectively evaluated. Continence was defined as by patient utilization of zero urinary pads postoperatively.
Results: The median (IQR) age at RARP was 60.2 (57.8‐61.3) years, the interval between kidney transplant and RARP was 8.1 ± 7.5 years. The median (IQR) PSA was 6.9 (4‐8.6); 10 of 14 patients had intermediate or high‐risk prostate cancer. The median ASA score was 3, the mean (SD) operative time was 129.7 (26.3) minutes, and mean (SD) blood loss was 110 (44.6) ml. All cases were completed robotically, no intra‐operative or post‐operative complications were encountered, there was no graft loss or injury to transplanted ureter, and the mean length of stay was 1 (0.26) day. Final pathology demonstrated that 42.8% (6/14) of the patients had non‐organ confined disease (pT3a/T3b). 50% (7/14) of the patients were upgraded to higher risk Gleason 7 (3 + 4) disease or above on final surgical pathology.3 of 14 patients developed biochemical recurrence, 2 of them were treated with Hormone treatment only, and 1 patient received concomitant hormonal treatment and radiotherapy. Post‐RARP continence rate at 3 months, and 12 months were 45.5% (5/11) and 87.5% (7/8), respectively.
Conclusions: RARP following kidney transplantation represents a safe and feasible operation which does not appear to compromise oncological or transplant outcomes.
Robotic Radical Cystectomy Is Not Associated With Increased Incidence of Local Pelvic Recurrence
R Madi
Augusta University Health
Introduction & Objective: Robotic radical cystectomy (RRC) might be associated with an increased incidence of local pelvic recurrence and peritoneal seeding. We performed an institutional study evaluating the incidence and type of cancer recurrence following RRC.
Methods: Between January 2012 and July 2019, 100 consecutive robotic radical cystectomies (RRC) were performed by a single surgeon RM. Pre‐and Peri‐operative characteristics were analyzed. Early and late, local and distant recurrences were studied, with the assumption that early local recurrences might suggest technical causative factors.
Results: Median age was 63 ( IQR: 57‐75). Male to female ratio is 2 to 1. Median BMI was 27.7 ( IQR: 24‐32). 70% of patients were white, 27% were black, 2% were Hispanic, and 2% were Asians. Indications for cystectomy were refractory CIS in 6%, T disease in 26%, T2 disease in 52%, T3 disease in 5%, and T4 disease in 11%. Console time was 249 minutes ( IQR: 205‐318). 70% of patients underwent ileal conduit, 30% underwent neobladder. 85% of patients underwent extended PLND and median blood loss was 150 ml, no patient required transfusion. Final pathology showed T0, Ta, CIS, T1, T2, T3, and T4 diseases in 2%, 5%, 10%, 10%, 21%, 36%, and 16% respectively. Median hospital stay was 6 days and 34% of patients had 30 days complications. 50% of patients had more than 36 months follow‐up and overall, 24% of patients had cancer recurrences. Only 3 patients had recurrence within 3 months. Patient 1 had PT1, N1 disease with recurrences in common iliac lymph nodes and was treated by chemotherapy and is in complete remission. Patient 2 had pT3b N1 SCC with 3 months CT scans showing extensive pelvic and systemic recurrences and expired 6 months after surgery. Patient 3 had pT3a, N1 disease and had recurrence in the aorto‐caval LN, received chemo‐and immune therapy and has no evidence of disease.
Conclusions: Our experience with robotic radical cystectomy did not show an increased incidence of early or local recurrence that could be attributed to the surgical approach. We believe that adherence to oncological principles is achievable with robotic approach
The prevalence of orgasmic dysfunction after robot‐assisted radical prostatectomy
M Honda, R Shimizu, S Teraoka, Y Kimura, T Yumioka, H Iwamoto, S Morizane, K Hikita, A Takenaka
Department of Urology, Tottori University Faculty of Medicine
Introduction & Objective: In the literature, among the sexual problems that may arise after radical prostatectomy (RP), erectile dysfunction has received the most attention. However, orgasmic dysfunction such as orgasm‐associated urinary incontinence (climacturia), orgasm‐associated pain (dysorgasmia), anorgasmia, and altered perception of orgasm also occur in this context. The cause of orgasmic dysfunction is not well understood, and it remains unclear how many and which patients with RP, especially robot‐assisted radical prostatectomy (RARP), are affected. Therefore, this study aimed to evaluate the incidence and extent of orgasmic dysfunction in patients after RARP and identify the factors that could help predict the patients at risk.
Methods: The ethics committee of our institution approved this study. Between October 2010 and November 2019, we performed a single‐centre, cross‐sectional, questionnaire‐based investigation of patients who underwent RARP (n = 523). Of the 523 patients, men who received neoadjuvant therapy (n = 54), adjuvant therapy (n = 46), or died from other causes (n = 6) were excluded, leaving 417 subjects eligible for investigation. All patients were treated at our institution between 3 and 111 months prior to the start of the study. Six questions on sexual activity, orgasmic function, altered perception of orgasms, dysorgasmia, and climacturia were developed. Questionnaires were mailed in February 2020 including a letter inviting patients to participate in the study. The primary outcome measure was the prevalence rate of orgasmic dysfunction. The predictive factors were identified through logistic regression analyses.–
Results: Overall, 259 questionnaires were available for analyses. Among sexually active patients (n = 145), 33 (22.8%) reported anorgasmia, 83 (57.2%) reported decreased orgasm intensity after versus before RARP. Twenty‐two (15.1%) patients reported dysorgasmia; among these patients, pain was experienced almost always or always in 13.6%, sometimes in 13.6%, and a few times in 72.8% of cases. Climacturia was reported by 44 patients (30.3%). UI (odds ratio, 3.13; 95% confidence interval, 1.20–8.15) increased the risk of climacturia after RARP.
Conclusions: These results indicate that orgasmic dysfunction after RARP is relatively common and should be considered by clinicians and researchers. It remains difficult to predict which patients are at risk before surgery. However, urinary incontinence can help identify the patients who are at risk after RARP.
Comparison of Surgical Outcomes Between Single‐Port and Multiport Robotic‐Assisted Prostatectomy, Cystectomy, and Partial Nephrectomy: A High‐ Volume Tertiary Center Experience
NA Pickersgill, J Gross, N Barashi, R Bhatt, J Vetter, J Palka, G Henning, RS Figenshau
Washington University School of Medicine
Introduction & Objective: The landscape of surgical management of urologic cancers has evolved over the years with the widespread adoption of minimally invasive approaches. The recent introduction of the da Vinci single‐port surgical system marks yet another technological advance in robotic‐assisted radical prostatectomy (RARP), radical cystectomy (RARC), and partial nephrectomy (RAPN). As the use of the single‐port (SP) platform continues to increase, it is important to compare perioperative outcomes with the widely used multiport (MP) platforms. We report our experience with SP and MP RARP, RARC, and RAPN at a high‐volume tertiary care center.
Methods: We identified consecutive patients undergoing SP‐RARP (N = 69), SP‐RAPN (N = 18), and SP‐RARC (N = 14) between November 2019 and November 2020 performed by two experienced surgeons at our institution. These patients were matched 1:1 to concurrent consecutive patients undergoing MP‐RARP, MP‐RAPN, and MP‐RARC. Patient characteristics and perioperative outcomes were assessed.
Results: SP‐RARP had shorter mean operative time than MP‐RARP (P = 0.02). There were no differences in mean estimated blood loss (EBL), postoperative narcotic requirement, complication rate, or length of stay (LOS) between SP‐RARP and MP‐RARP. SP‐RARP had a higher positive margin rate ( >3 mm) and lower lymph node (LN) yield than MP‐RARP (P = 0.02), however both metrics improved with increasing experience performing SP‐RARP. There were no significant differences in operative time, EBL, postoperative narcotic requirement, complication rate, LOS, or positive margin rate between SP‐RAPN and MP‐RAPN or between SP‐RARC and MP‐RARC.
Conclusions: SP and MP platforms feature similar safety profiles for commonly performed urologic cancer operations. Following an initial learning curve, SP perioperative outcomes quickly approach equivalence to those of the MP platform. Randomized trials with long‐term follow‐up are needed to better evaluate functional and oncologic outcomes of this novel technology.
Oncological Outcomes of Laparoscopic and Open Radical Nephroureterectomy for Advanced Upper Tract Urothelial Carcinoma
J Correia, A Rocha, G Mendes, B Teixeira, A Fraga, M Silva‐Ramos
Department of Urology, Centro Hospitalar Universitário do Porto
Introduction & Objective: Laparoscopic radical nephroureterectomy (LNU) is increasingly being used instead of open radical nephroureterectomy (ONU) for the treatment of upper tract urothelial carcinoma (UTUC) due to better perioperative outcomes of minimally invasive surgery, but its oncological safety remains controversial. In particular, for advanced UTUC (T3/T4 and/or N+ disease) international guidelines still consider ONU as the current gold standard. Our objective was to compare the oncological outcomes of ONU with those of LNU.
Methods: We performed a retrospective analysis of all 48 patients submitted to radical nephroureterectomy for advanced UTUC (≥pT3 and/or pN+) between 2006 and 2019 in our center.
Bladder tumor‐free survival (BTFS), metastasis‐free survival (MFS) and cancer‐specific survival (CSS) were compared between groups. Recurrence‐free probabilities were estimated using Kaplan‐Meier analyses. A multivariable Cox regression model was used to evaluate the association of surgical approach and outcomes. A p value <0,05 was considered statistically significant.
Results: 26 LNU and 22 ONU were followed for a median of 16.5 months [IQR 6.5‐41.3]. Clinical and pathological characteristics were similar between groups. LNU was associated with better MFS (HR = 0.369; 95% CI: 0.163‐0.834; p = 0.017) and CSS (HR = 0.318; 95%CI: 0.129‐0.787; p = 0.013) than ONU. 5‐year MFS (59% vs 35%, log‐rank p = 0.011) and CSS (68% vs 42%, log‐rank p = 0.008) were significantly higher for LNU. Median time to cancer death for ONU was 12 months (95% CI: incalculable – 25.1), and was not reached for LNU. There was no significant difference in BTFS between groups (HR = 0.631; 95% CI: 0.180‐2.212; p = 0.472), with similar 5‐year BTFS rates (77% vs 81%, log‐rank p = 0.469, for LNU vs ONU). On multivariable Cox regression model, surgical approach remained an independent predictor of CSS (HR = 0.367; 95% CI: 0.142‐0.950; p = 0.039), and with a tendency to better MFS (HR = 0.424; 95%CI: 0.179‐1.005; p = 0.051).
Conclusions: In our population of advanced UTUC, there was no evidence that laparoscopic radical nephroureterectomy resulted in inferior oncological outcomes than those of open radical nephroureterectomy. Longer follow‐up of well‐controlled randomized trials is needed to confirm LNU as an effective oncological therapeutic alternative in this setting.
A Matched Analysis of Conventional Multi‐Port versus SP Single‐Site Robotic Partial Nephrectomy
J Na, S Alip, N Son, J Kim, W Jang, Y Lee, KH Rha, W Han
Yonsei University College of Medicine
Introduction & Objective: A purpose built single‐site robotic SP platform has recently been introduced and our institute is currently using this novel platform conducting truly single‐site robotic partial nephrectomy. In this study we aimed to compare its initial results with the conventional multi‐port robotic partial nephrectomy.
Methods: Patients who underwent single‐site robotic partial nephrectomy (SP group) were matched to those who underwent multi‐port robotic partial nephrectomy (MP group) during the same period by the same surgeon from Dec, 2018 to Apr, 2020. Patients were matched 1:3 according to RENAL nephrometry score, horizontal location of tumor(anterior/posterior), and vertical location of tumor(upper/mid/lower), sex and BMI.
Results: There were 21 patients in the SP group, and 62 matched patients in the MP group. The SP group had a longer overall operation time, console time, and warm ischemic time compared to the MP group. None of the patients included in the study had a complication greater than Clavien‐Dindo system grade 1, and all were recurrence free at a mean follow‐up of 12.5 (SD 5.8) months. Mean changes in eGFR showed no statistically significant differences in both groups at one week, three months, six months, and one year post‐operatively.
Conclusions: True single‐site robotic partial nephrectomy using the SP platform can be safely performed without an increase of major perioperative complication rates. Although there was an increase in operative time, especially ischemic time, the oncological and functional outcomes were equivalent to the conventional multi‐port robotic approach. This maybe attributed to the precise enucleoresection made possible by the articulating instruments of the SP platform.
Withdrawn
Robotic Assisted Kidney Transplantation – Point of technique with our experience of median follow up of 43 months (3.6 years)
AP Patil, A Ganpule, AK Parikh, A Singh, R Sabnis, M Desai
Muljibhai Patel Urological Hospital Nadiad
Introduction & Objective:: Kidney transplantation is the best renal replacement therapy for End‐Stage Renal Disease(ESRD) patients. Robotic approach(RAKT) may have upper edge of magnification enabling precise suturing and decreasing wound morbidity especially in obese patients. The data on this newer approach is just emerging. We intend to present the medium‐term follow‐up of a single centre experience of this approach.
Methods: We position the patient in Trendelenburg position with ports placed in inverted fan‐shaped fashion. We prefer Pfannenstiel incision for engraftment as it is cheap and allows quick access in case of catastrophe. After meticulous bench preparation, we engraft the kidney in an indigenous prepared graft jacket with tacking sutures for proper graft orientation. We perform vascular anastomoses after confirming the ureter is placed caudally. In case the kidney is anastomosed topsy‐turvy with ureter placed cranially, it can be anastomosed with native ureter. The kidney is properly retroperitonealized which is possible due to adequate peritoneal flap dissection. We present our experience of 29 patients of RAKT with median follow‐up of 43 months.
Results: Mean age our experience was 41.1 ± 12.7 years with BMI of 25.8 ± 4.6 kg/m2. We had 4 right sided donor kidneys with rest being left sided. Mean warm and cold ischemia time was 4.9 ± 1.3 and 114.4 ± 20.6 minutes. Mean operative time was 292.1 ± 57.0 minutes. Two patients had intra‐operative complication of topsy‐turvy kidney and graft surface bleeding. Mean creatinine at 1 year and current creatinine was 1.3 ± 0.4 and 1.9 ± 1.8 mg/dl. Three patients had graft loss with two being on maintenance dialysis and one had death due to lymphoproliferative disease.
Conclusions: RAKT is a safe and feasible option especially for obese ESRD patients with good medium follow‐up outcomes.
Robotic Ureteral Reconstruction for Recurrent Strictures After Prior Failed Management: A Multi‐Institutional Experience
M Lee, Z Lee, AM Asghar, RA Lee, D Strauss, R Reddy, MJ Metro, LC Zhao, MD Stifelman, DD Eun, N Krishnan
Lewis Katz School of Medicine at Temple University
Introduction & Objective: Surgical repair of recurrent ureteral strictures after prior failed intervention is technically challenging. We described our multi‐institutional experience with robotic ureteral reconstruction (RUR) in patients who failed prior endoscopic and/or surgical management.
Methods: We retrospectively reviewed our Collaborative of Reconstructive Robotic Ureteral Surgery (CORRUS) database for all consecutive patients who underwent RUR between 05/2012—01/2020 for a recurrent ureteral stricture after having undergone a prior failed endoscopic and/or surgical repair. The method for repair was determined by the primary surgeon based on clinical history and intraoperative findings. Postoperatively, patients were assessed for surgical success defined as the absence of flank pain and obstruction on imaging.
Results: Overall, 105 patients met inclusion criteria (Table 1). Median stricture length was 2 (IQR 1‐3) centimeters. Strictures were located at the ureteropelvic junction (UPJ) (41.0%), proximal (14.3%), middle (9.5%) or distal (35.2%) ureter. There were 9 (8.6%) radiation‐induced strictures. Prior failed management included endoscopic intervention (49.5%), surgical repair (25.7%) or both (24.8%). Median operative time was 187.5 (IQR 143.8‐279.3) minutes and estimated blood loss was 50 (IQR 40‐100) milliliters. RUR techniques included ureteroureterostomy (3.4%), ureterocalycostomy (5.2%), pyeloplasty (69.0%) or buccal mucosa graft ureteroplasty (22.4%) for UPJ and proximal strictures; ureteroureterostomy (20.0%) or buccal mucosa graft ureteroplasty (80.0%) for middle strictures; ureteroureterostomy (8.1%), side‐to‐side reimplant (18.9%), end‐to‐end reimplant (70.3%) or appendiceal bypass (2.7%) for distal strictures. Adjunctive techniques such as a downward nephropexy, psoas hitch or Boari flap were utilized in 7 (6.7%), 10 (9.5%) and 8 (7.6%) cases, respectively. Major (Clavien >2) postoperative complications occurred in 2 (1.9%) patients. At a median follow‐up of 15.1 (IQR 5.0‐30.4) months, 95 (90.5%) cases were surgically successful.
Conclusions: RUR may be performed with excellent intermediate‐term outcomes for patients with recurrent strictures after prior failed endoscopic and/or surgical management.
Comparison between Tisseel an PuraStat as a hemostatic material in robot assisted and laparoscopic partial nephrectomies
A Femic, M Häggman, S Ladjevardi
Department of Urology, Akademiska University Hospital
Introduction & Objective: Partial nephrectomy (PN) has become the standard surgical treatment for T1a (< 4cm) and for T1b tumors whenever feasible. Laparoscopic PN (LPN) was introduced as an alternative to open PN for the surgical treatment of small renal masses in 1993. Robotic assisted PN (RPN) was introduced in 2004. However, bleeding is the most common postoperative complication of open PN, LPN or RPN. Major bleeding can often be life‐threatening and requires immediate invasive management. To prevent postoperative bleeding some biologic fibrin sealants have increasingly been used. In our study we have compared two different hemostatic materials: Tisseel fibrin sealant produced by Baxter Laboraories, Inc and PuraStat hemostatic matrix produced by 3‐D Matrix Medical Technology. The aim of this study was to evaluate bleeding complication rates in patient received Tisseel versus PuraStat.
Methods: All patients with kidney tumours (T1a or T1b) who underwent LPN and RPN between 2008 and 2020 were included. Totally 148 were considered to be suitable for this study. The research is designed as a retrospective database study. Postoperative bleeding ratio was compared between the groups received Tisseel and PuraStat. The number of patient who needed blood transfusion, major bleeding ratio (Clavien‐Dindo 3 or 4) and the lenght of hospitalization were compared.
Results: Seventy‐six patients were included in Tisseel and 72 in PuraStat group. Median age was 63 and 61 years respectively. Mean Body Mass Index (BMI) was 28 in both groups. There was no significant difference in the median tumour size (32,5 mm) in Tisseel group and (29,1 mm) in PuraStat group. All patients in the PuraStat group were operated with RPN. In the Tisseel group 21 patients were operated with RPN and 55 with LPN. Sixteen percent of patients in the Tisseel group needed blood transfusion due to postoperative bleeding, compared to 12,5% in the PuraStat group. Major bleeding which required intervention occurred in 3 patients in each group. All those patients were treated by percutaneous endovascular embolization except one in Tisseel group who needed reoperation. There was no significant difference in the lenght of hospitalization due to postoperative bleeding.
Conclusions: Both materials was successfully applied during LPN and RPN. Our experience is that PuraStat appears to be more suitable than Tisseel, since it does not need thawing or other preparation before application. However, the results from our study did not show significant difference in postoperative bleeding complication ratio in compared groups.
Same Day Discharge for Robotic‐assisted Radical Prostatectomy: Recommendations from a Referral Center
S Reddy, R Perera, S Bhat, TA Helman, T Rogers, M Moschovas, J Noël, V Patel
AdventHealth Global Robotics Institute
Introduction & Objective: Due to the COVID‐19 global pandemic, in July 2020 we developed a same day discharge (SDD) protocol for robotic assisted laparoscopic prostatectomy (RALP) that balanced safety concerns with benefits of early discharge. In this study we present our experience and protocol.
Methods: We performed a prospective analysis of patients undergoing RALP who were selected for SDD in a high‐volume prostate cancer referral center. The criteria for discharge included uncomplicated surgery, stable postoperative hemoglobin, ambulation, tolerance of clear liquids without nausea or vomiting, pain control with oral medication, and patient/family comfort with SDD. We excluded patients older than 70 years, having concomitant general surgery operations, significant comorbidities (e.g. cardiopulmonary disease), and challenging procedures (e.g. salvage procedure, large prostates). We analyzed patient demographics, clinicopathologic factors, and operative outcomes and evaluated rates of SDD and factors associated with SDD failure (SDF).
Results: From July 13, 2020 to January 1, 2021, 101 patients undergoing RALP were selected for SDD. Eighty patients (79%) met criteria , 73 (72%) were successful SDD, and 28 (28%) were SDF. All the SDF were discharged on postoperative day 1. Preoperative demographics were similar between the two groups with a median age of 63 (57‐67) years and median BMI of 27 (25‐30) kg/m2. Intraoperative characteristics were not statistically different with a median operative time of 92 (81‐107) vs 103 (91‐111) minutes for SDD and SDF respectively (P = 0.51). The readmission in the SDD group was due to dizziness from hematoma and ileus from urine leak in the SDF cohort (P = 0.69). Of the 28 SDF patients, the most common reasons for staying were anesthesia‐related factors of nausea (35%) and drowsiness (7%), followed by patient/caregiver preference (25%), pain (14%), labile blood pressure (7%), arrhythmia (7%), and dizziness (7%).
Conclusions: SDD for patients undergoing RALP can be safely incorporated into a clinical care pathway without increasing readmission rates. Coordinated care with anesthesia and nursing teams is an integral part of developing a SDD program, as is preoperative counseling to manage expectations. Future aims will be to investigate anesthesia factors leading to nausea and to expand selection to more patients.
Introduction & Objective: The 3‐5 Shielded Trocar Technique (3‐5 STT) is a simple modification of the standard 3 mm laparoscopic trocar placement in an infant or child. This technique reduces the risk of significant injury when placing a 3 mm trocar's cutting tip into the peritoneal cavity.
The inner lumen of the 5 mm umbilical trocar is used to shield the 3 mm obturator from injuring vital structures when applying an axial force to the trocar. The technique eliminates placement of a traction suture, penetrating towel clamp or grasping the abdominal wall with the surgeon's opposite hand.
Methods: A retrospective study of pediatric patients undergoing laparoscopic orchiopexy over a 3.75 year period (5/17 to 2/21) using the 3‐5 Shielded Trocar Technique. Description of the technique: 1) Point the 5 mm umbilical trocar camera port at the proposed 3 mm working trocar entry site 5 cm lateral from the umbilicus. 2) Infiltrate the 3 mm trocar site with 0.25% Marcaine. 3) Under direct vision make a small skin incision and peritonotomy with a 11 blade scalpel. 4) Pass a fine tip straight mosquito clamp into the peritonotomy and stretch. 5) Pass the 3 mm trocar through the stab wound until the tip is just visible. 6) Point the tip of the 3 mm trocar towards the umbilicus and parallel to the abdominal wall. 7) Align the 5 mm trocar's lumen with the 3 mm trocar's cutting tip and engage the 5 mm trocar. 8) Push the 3 mm trocar (piston) into the lumen of the 5 mm trocar (cylinder) creating a tube within a tube.
Results: Average age of the patient undergoing laparoscopic orchiopexy: 16.1 months (9‐22 months). Average wt. 10.9 kg (7.26‐15.3 kg). Number of patients in the study N = 13. Number of times the 3‐5 STT was used N = 26. Testicle locations: non‐palpable undescended testicle N = 13; descended testicle N = 10; retractile testicle N = 2; atrophic descended testicle N = 1.
Conclusions: All 26 working 3 mm trocar sites were placed using the 3‐5 STT without an injury to the abdominal wall, contents of the peritoneal cavity or retroperitoneum. This small retrospective series of 13 patients (5 infants, 8 children) demonstrates the 3‐5 Shielded Trocar Technique's simplicity and safety.
Can Retroperitoneal Robot Assisted Partial Nephrectomy (RRAPN) be the default approach?
D Sri, M Malki, S Sarkar, H Niraghallaigh, G Pydisetty, J Oakley, M Hussain, NJ Barber
Introduction & Objective: Although retroperitoneal surgery has demonstrated a better quality of recovery compared to transperitoneal routes, Retroperitoneal Robot Assisted Partial Nephrectomy (RRAPN) remains proportionally infrequent. As the boundaries of what is achievable robotically continue to be pushed, we present our experience at a high volume tertiary referral centre that specialises in retroperitoneal surgery, exploring its feasibility and safety in the management of small renal masses.
Methods: A prospective database of 784 RAPNs (2009 – 2020) was reviewed and 721 RRAPNs (92%) were performed at our centre. In our practice, we utilise a 4 port approach to RRAPN. Patient, tumour and operative characteristics were assessed and both oncological outcomes and trifecta and pentafecta achievements were determined.
Results: From 784 cases, 112 RAPNs were performed for imperative reasons, whilst the remainder were elective. Mean BMI+/‐ s.d amongst our cohort was 28.6 +/‐ 5.7. Mean tumour size was 3.1cm (range 0.8cm – 10.5cm) and 47% of cases were stratified as intermediate/high risk using R.E.N.A.L nephrometry scoring. Forty six patients had lesions in a hilar location, and 30% were anterior. Median blood loss was 30mls, with an open conversion rate of 0.9% and transfusion rate of 1.6%. Median warm ischaemic time (WIT) was 21mins, positive surgical margins were found in 4% and our post‐operative Clavien 3/ > complication rate was 2.6%. We had a 1 day median length of stay with a 30 day readmission rate of 2%. Of 631 patients (80%) with a definitive histological diagnosis of cancer, 23% had T1b/ > disease. Over a mean 15 month follow up period (range 1 – 125 months), 2% of patients developed recurrences and our cohort demonstrated a 99% 5 year cancer specific survival. Trifecta was achieved in 67% of cases and pentafecta in 47%. Age (p = 0.05), operative time (p = 0.008), pT1b tumours (p = 0.03), R.E.N.A.L score and blood loss (p = 0.001) were found to statistically significantly influence achievement of trifecta.
Conclusions: We demonstrate the retroperitoneal approach in RAPN is technically feasible and oncologically safe irrespective of lesion location and complexity. In the hands of high volume centres that are skilled in the retroperitoneal approach the benefits of retroperitoneal surgery can be extended even to challenging cohorts of patients without compromising their oncological or functional outcomes.
Salvage Pelvic Lymph Node Dissection of Locally Recurrent Prostate Cancer after Radical Prostatectomy Can Delay the Need for Systemic Interventions
E Huang, K Liang, LM Huynh, W Zhang, TE Ahlering
University of California, Irvine
Introduction & Objective: With the advent of the 68‐Ga PSMA PET/CT scan, recurrences following radical prostatectomy (RP) can be localized to pelvic lymph nodes, soft pelvic tissue, and/or distant metastases. In our experience, 55% of patients with a biochemical recurrence (BCR) following surgery recur locally in the pelvic lymph nodes (PLN). Standard therapies such as radiation and/or hormonal therapy are known to negatively affect patients' quality of life (QOL) and, in this regard, the present study introduces salvage pelvic lymph node dissections (sPLND) of local recurrence as a potential treatment for local recurrences
Methods: Following RP, 87 patients underwent 68 Gallium PSMA/PET CT scan, of which 64 scans were positive, with 35 (40.2%) demonstrating radiographic evidence of localized recurrence in the PLN. Amongst the PLN positive group, 15 patients proceeded with sPLND by a single surgeon. The primary outcome evaluated was PSA kinetics, and secondary outcome evaluated was need for secondary treatment.
Results: All surgeries were completed outpatient without complication. Patients were discharged with <24 hours hospitalization with <1 week recovery time. Of the 15 patients who underwent sPLND, 6 (40.0%) patients had a stable rise in PSA with no secondary intervention at mean follow‐up time of 2.3 (±0.8) years following sPLND. 4 (26.7%) patients experienced a stable rise in PSA with secondary intervention, and 5 (33.3%) patients experienced BCR immediately, with immediate hormonal therapy as a secondary intervention. In 10/15 (33.33%) of the patients, PSA decreased by an average of 58% following sPLND. 6/15 (40.0%) patients did not require secondary systemic interventions such as radiation and hormonal therapy thus far (Table 1).
Conclusions: This case series explores the utility of PSMA/PET scan imaging and subsequent dissection of pelvic lymph node recurrences, demonstrating its potential to slow PSA progression and delay or eliminate the need for secondary intervention. Future studies with additional patients and greater follow‐up are required to evaluate PSA progression and secondary intervention post‐sPLND further.
Revo‐i versus da Vinci in retzius‐sparing robot‐assisted radical prostatectomy: a propensity score analysis of surgical and oncologic outcomes
P Koukourikis, S Alip, J Kim, KH Rha, W Han, J Na
Introduction & Objective: The Revo‐i is a new robotic surgical system developed by Meerecompany (Seongnam, Republic of Korea) and was granted license for commercial use by the Korean FDA in 2017. It has been seeking to gain entry into the robot market, to allow for more competitive pricing without sacrificing efficiency and quality. The aim of this study is to compare surgical and oncologic outcomes between matched cohorts of localized PCa using the Revo‐i and the da Vinci Si robots in retzius‐sparing robot‐assisted radical prostatectomy (rs‐RARP).
Methods: Patients who underwent rs‐RARP using the Revo‐i between 2016 and 2020 were compared with a matched cohort from a prospectively maintained database of patients who underwent rs‐RARP using the da Vinci systems by the same surgeon during the same period. Propensity score matching was performed using ten preoperative variables. A subset analysis of the surgical outcomes were performed between the initial cases (n = 20) and later cases (n = 13) of Revo‐i after improvements at the robot's software from the surgeon's feedback.
Results: Overall, 33 patients underwent rs‐RARP using the Revo‐i were matched 1:1 to 33 patients operated with the da Vinci Si system. All Revo‐i cases were completed without conversion to open or da Vinci surgery and no intraoperative complications. The Revo‐i cohort had longer console time, anastomosis time and operative time (p < 0.001). The estimated blood loss (EBL) was similar between the cohorts (p = 0.1). Both groups had similar rates of Clavien‐Dindo complications (p = 0.3), with no major complications for the Revo‐i group. In terms of oncologic outcomes, positive surgical margin and BCR (at six months) rates were similar between the cohorts (p > 0.05). The subset analysis showed a shorter console time and operative time for the later cases group (p < 0.001), with no differences in EBL, complication rates and margin positivity rates (p > 0.05).
Conclusions: Rs‐RARP performed with the Revo‐i when compared to the da Vinci resulted in similar EBL, complications, margin positivity, and BCR rates. The longer console and operative time were significantly improved after the initial learning curve of the surgeon with this new system and software improvement. Future controlled trials with Revo‐i accessing the long‐term outcomes are needed.
Withdrawn
Withdrawn
Comparative analysis of trifecta outcomes in robot‐assisted partial nephrectomy(RAPN) for cT1a versus cT1b plus renal tumors: Is RAPN for cT1b plus renal tumors feasible?
S SINGH, S khanna, D Darlington, S Patil, A Tamhankar, P Ahluwalia, G Gautam
AIIMS, Rishikesh
Introduction & Objective: Robotic assistance is being increasingly utilized for nephron sparing surgery for complex renal masses. We evaluated the outcomes of robot assisted partial nephrectomy (RAPN) for cT1a versus cT1b+ renal masses by a comparative analysis of trifecta outcomes between these two groups of patients.
Methods: We utilized our prospectively maintained database to identify patients undergoing RAPN for cT1a (Group 1, n = 41) and cT1b+ (Group 2, n = 37) renal masses from April,2016 to March,2020. Tumor complexity was investigated according to RENAL and PADUA nephrometry score.”Trifecta” was defined as achievement of negative surgical margin, no postoperative complications and warm ischemia time of ≤20 minutes. The demographic, perioperative, oncological and trifecta data were analyzed using appropriate statistical methods.
Results: Out of 78 patients, trifecta was achieved in 30 (38.4%) patients. There was no statistically significant difference between cT1a and cT1b plus tumors (p = 0.152) for trifecta achievement. We found a statistically significant difference between the two groups in terms of RENAL scores (p = 0.0005), PADUA score (p = 0.0002) and robotic console time (133.8 ± 42.8 Vs 170 ± 54.8 minutes for cT1a versus cT1b+, respectively)(p = 0.002), as shown in Table1. On multivariate analysis, warm ischemia time (p = 0.069), blood loss (p = 0.345), pelvi‐calyceal system (PCS) repair (p = 0.691), postoperative length of hospital stay (p = 0.026) and GFR reduction (p = 0.152) were not statistically different. There was no statistically significant difference in intraoperative or postoperative complications (p = 0.9317). None of the patients in both groups had positive surgical margins. Although recurrences were observed in two patients (5.4%) of the cT1b+ group, there was no statistical difference in the recurrence‐free survival at 12 and 24 months.
Conclusions: Our study shows that RAPN can be safely done for cT1b+ renal tumours. The rate of trifecta after RAPN was comparable between T1a and T1b+ renal masses. These findings reinforce the view that RAPN should be considered a viable option for cT1b+ lesions, whenever technically feasible with excellent long term outcomes.
Single Port Robotic Kidney Autotransplantation: Minimizing an Invasive Surgery
ZR Schwen, A Beksac, L Lenfant, A Aminsharifi, S Kim, A Wee, M Eltemamy, MJ Noble, J Kaouk
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
Introduction & Objective: Kidney autotransplantation (KAT) remains a viable option for select patients for renal salvage, however the open approach has been marred by significant morbidity and a high complication rate, owning to the high incisional burden for both the nephrectomy and the transplant portion of the case. Minimally invasive KAT approaches have attempted to reduce the morbidity, though this requires multiple sets of ports as well as repositioning the patient. We present our initial series of single‐port (SP) robotic KAT, ideal for multi‐quadrant surgeries, to evaluate the feasibility and safety of the novel approach.
Methods: Technical steps were designed using a cadaveric model and data was collected into an IRB‐approved database. Three consecutive patients underwent a SP KAT using the DaVinci SP. Indications included complex proximal ureteral stricture, severe metabolic stone disease, and chronic visceral pain due to a recurrent proximal ureteral stricture. Patient clinicopathologic variables and perioperative outcomes were recorded.
Results: Patient preoperative characteristics are summarized in Table 1. All SP KATs were successfully performed without repositioning or conversion to open. Operative times ranged from 507 to 547 mins with a warm and cold ischemia time between 4 to 10 mins and 86 to 182 mins, respectively. Patient #1 with severe stone diseases additionally underwent a Boari flap to permit stone passage. Preoperative outcomes are summarized in Table 2. At a median of 5 months follow‐up, postoperative GFRs were stable, ranging from +11.5% to ‐17.6%, there were no reported complications, and the grafts were draining well following stent removal. Notably, the patient who had chronic visceral pain had complete resolution of her pain postoperatively.
Conclusions: We demonstrated the safety and feasibility of the SP KAT, which aims to further reduce the perioperative morbidity of KAT. Furthermore, we showed that the SP KAT, which involves a dual multi‐quadrant surgery, can be performed through a single, small incision without requiring patient repositioning
Moderated Poster Session 29: Robotics/Laparoscopy IV
Prospective randomized evaluation of organ retrieval site for hernia development following robot assisted laparoscopic radical prostatectomy
OB Argun, MB Tuna, T Doganca, I Tufek, C Obek, AR Kural
Acibadem Mehmet Ali Aydınlar University School of Medicine Urology Department
Introduction & Objective: Minimally invasive techniques are gradually being used for surgical treatment of prostate cancer. However, the incisional hernia development after these techniques are yet to be evaluated. In this study, we compared 3 different organ retrieval site for the risk of incisional hernia development following robot assisted laparoscopic radical prostatectomy.
Methods: Between January 2018 and May 2019, 149 patients were enrolled for the study. In the first, second and third group, organs were retrieved through supraumbilical, right abdominal (through the assistant port) and Pfannenstiel incisions respectively. Patients were grouped according to the penultimate number of the social security numbers. In the postoperative period, the area where the organ was removed was evaluated by ultrasonography. Valsalva maneuver was applied during the ultrasonographic examination.
Results: We observed hernia in 20 patients. The frequency of hernia development for operations with different incision locations are as follows: Supraumbilical 9/49, Assistant port 10/49, Pfannenstiel: 1/51
Conclusions: Hernia development is significantly associated with incision location, we see that it is lower for pfannenstiel incision compared to supraumbilical and assistant port incision. We did not observe any other factor associated with hernia development.
Robotic Partial Nephrectomy for Hilar Tumors: Improving Outcomes to Replicate the Results of Non‐Hilar Tumors
A Beksac, M Abou Zeinab, ZR Schwen, A Aminsharifi, J Kaouk
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
Introduction & Objective: Hilar tumors pose a technical challenge during robotic partial nephrectomy (RPN). We sought to analyze the outcomes of RPN in patients with hilar renal masses with a focus on renal volume preservation, and compare results to non‐hilar tumors.
Methods: From a single institution series, we have analyzed the data of 191 consecutive patients (38 hilar vs. 153 non‐hilar) with available preoperative and postoperative CT scans for review. All patients underwent RPN for a localized renal mass. Preoperative and postoperative volumetric analyses were performed using a semi‐automated tissue segmentation tool. Univariate analysis was performed using Chi‐square test, Fischer's exact, and Wilcoxon rank‐sum tests. Perioperative and functional outcomes were assessed using linear mixed models and logistic regression models. Oncological outcomes were analyzed using the Kaplan‐Meier method.
Results: Median follow up was 24.2 months. Tumor volume (53.6 vs. 38.4, p = 0.014) and mean RENAL score (9.0 vs. 7.1, p < 0.001) were higher in the hilar group. Hilar group had longer warm ischemia time (24.4 vs. 20.5 minutes, p = 0.031). Ipsilateral volume preservation (79.6% vs. 76.8%, p = 0.126), Acute kidney injury (AKI) rate (18% vs. 15.8%, p = 0.749), eGFR preservation at one year (87.2% vs. 86.8%, p = 0.476), and eGFR preservation at last follow up (88% vs. 89%, p = 0.738) were comparable. Positive surgical margin rate (7.5% vs. 2.9%, p = 0.325), recurrence rate (2% vs. 5.3%, p = 0.254), 3‐year predicted RFS (p = 0.39), 3‐year predicted OS (p = 0.86), and trifecta achievement rate (72.2% vs. 80%, p = 0.349) were comparable.
Conclusions: With robotic surgical experience and optimal renal parenchymal volume preservation, RPN yields comparable results between patients with hilar and non‐hilar renal masses.
Redo Robotic Partial Nephrectomy for Recurrent Renal Masses: A Multi‐Institutional Analysis
A Beksac, U Carbonara, M Abou Zeinab, S Hemal, M Meagher, A Tafuri, G Tuderti, A Antonelli, R Autorino, G Simone, IH Derweesh, J Kaouk
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
Introduction & Objective: Recurrent renal masses pose a great challenge in performing robotic partial nephrectomy (RPN). We sought to analyze the outcomes of redo RPN in patients with a recurrent renal mass.
Methods: From a multi‐institutional dataset, we have analyzed the data of 72 patients who underwent RPN for a recurrent renal mass between 2010 and 2020. Patients with familial renal cell carcinoma and multiple renal tumors were excluded. Major complication defined by Clavien grade >2. Median follow up was 28.5 months. Baseline demographics, clinical and tumor characteristics, perioperative and postoperative outcomes are reported.
Results: Our cohort consisted of patients with history of ipsilateral cryoablation, laparoscopic, open and robotic surgeries. Median RENAL score was 8. In our study, 20% had hilar tumors and 9.7% had a solitary kidney. Partial nephrectomy was completed successfully in all cases. Two cases (2.8%) were converted to open surgery. None of the cases were converted to radical nephrectomy intraoperatively. One patient underwent radical nephrectomy postoperatively due to bleeding. Transfusion rate was 5.9% and major complication rate was 8.3%. Median length of stay was 3 days. Acute kidney injury was 35.1% at discharge, however eGFR preservation was 90.8% at one year follow up. Positive surgical margin rate was 9.5%. Recurrence was seen in 14 patients (15.2%), however only one patient had local recurrence (1.4%).
Conclusions: In experienced hands, RPN is an effective approach to treat recurrent renal masses with promising perioperative and functional outcome. However, distant recurrence was more common and patients should be monitored accordingly.
Is one Layer Mass Closure Enough in Robotic Partial Nephrectomy
A Dahman, MW Salkini
West Virginia University
Introduction & Objective: Warm ischemia time (WIT) has been a concern in robotic partial nephrectomy (RPN). Multiple maneuvers have been tried to reduce WIT, like clampless RPN, early unclamping, cooling and using of Laser. The first layer suturing to close the collecting system is time consuming and is considered by many an essential step in renorrhaphy as there has been always concern about urine leak after RPN. We mass closed the renal parenchyma without dedicated closure of the collecting system to speed the renorrhaphy and reduce warm ischemia time. We report our own experience in omitting the closure of the collecting system.
Methods: A total of 375 RPN performed at our institute. We did not specifically close the collecting system in the last 225 cases to speed the renorrhaphy. We left Jackson Pratt at the endo of the procedure whenever we open the collecting system. To detect any urine leak, we sent the drainage fluid for analysis (checked the Cr).
Results: The average patients age was 67 years (28 ‐79). The average WIT was 14 min (5‐19) which was significantly shorter that the earlier cases where we closed the collecting system separately as it was 19 min (14‐ 34) (P < 0.05). Average blood loss was 195 ml (50‐400) and that was less than before adopting the technique 225 ml (100‐1200) P < 0.02. The average JP output in the first 24 hrs after surgery was 40 (10‐200). The change of the creatinine was 0.3(0‐0.8), compared to 0.5 (0.2‐2) in the earlier cases (P < 0.05). Only 10 patients needed transfusion (4 %) and one needed intervention to stop delayed bleeding (0.4 %) after 3 weeks of surgery. Of note, one patient developed asymptomatic aneurism 12 months after surgery and that was embolized (0.4%). None of the patients experienced urine leak or as per the creatinine of the drainage fluid. No transfusion needed in any of the patients. WIT was maintained below 22 min in all the cases.
Conclusions: Omitting the closure of the collecting system speed the renorrhaphy and decreases WIT and creatinine changes after surgery. Minimal adverse event were encountered due to adoption of this technique.
Assessment of GEARS scores and perioperative outcomes for Robotic Prostatectomy among high volume surgeons
D Mikhail, S Pettit, F Cascio, A Antonacci, L Richstone
Lenox Hill/Northwell Health
Introduction & Objective: Surgical metrics in healthcare continue to be evaluated to score surgeons and hospitals. CSATS (Crowd Sourced Assessment of Technical Skills) is a validated robotic surgical skills metric providing 5‐category GEARS scores (Global Evaluative Assessment of Robotic Skills) currently utilized for surgeon feedback and quality improvement. We reviewed perioperative outcomes associated with GEARS scores for RALPs at our institution.
Methods: Robotic surgery data was extracted for all urologists in our health system over a 2 year period between 2018‐19. We selected high volume surgeons ( >10 RALPs per year) and reviewed their GEARS scores, perioperative metrics and outcomes. We identified 6 surgeons at our institution. We compared their average GEARS domains/scores, percentiles and quartiles and looked for correlation with perioperative outcomes including operative time, transfusion rates, 30 day readmissions and length of stay. Spearman's correlation coefficient was used to find significant relationships.
Results: Our 6 highest‐volume surgeons performed 287 RALPs over the 2 year period (mean 47, range 18‐97). Of these, 161 (56%) were submitted to CSATS. Average GEARS score was 20.12 (+/‐ 0.17). Three surgeons scored average the 3rd quartile while the other 3 were in the 2nd quartile. Median operative time was 213 minutes (+/‐ 54 min) and was correlated with the average percentile/quartile (p < 0.05). Average LOS was 1.99 +/‐ 1.3 days and was correlated with the surgeons' ‘robotic control domain’ (p < 0.05). Readmission rates approached correlation with GEARS score (p = 0.06). ICU admission (0.6%) and transfusion rates (1%) were both low and not correlated with any scores.
Conclusions: Our institutional experience with a voluntary technical skills assessment tool (CSATS) showed that utilization is increasing among high volume urologists, with 56% of cases being scored for RALPs. At this volume and in robotic prostatectomies, we don't see a significant measurable correlation with hospital metrics such as LOS, ICU admission, transfusion rates or complication rates. We hope to look at more procedures over a larger volume as we do see trends with readmission rates and expect significant correlations with higher power.
Neurovascular structure‐adjacent frozen‐section examination (NeuroSAFE) Robotic Assisted Laparoscopic Radical Prostatectomy: Outcomes from 500 consecutive cases in the UK
J Noël, N Spencer, S Lodhia, S Karim, S Taneja, D Moghanchizadeh, A Nayak, A Tamhankar, R Swamy, S Agarwal, A Narula, T Lane, J Adshead, N Vasdev
Global Robotics Institute
Introduction & Objective: : To report the United Kingdom's largest single centre experience of robotically assisted laparoscopic radical prostatectomies (RALP), using the neurovascular structure‐adjacent frozen‐section (NeuroSAFE) technique. We describe its' efficacy on histopathological and functional outcomes, to aid units in their early stages of adoption of this technique.
Methods: We prospectively collected data from November 2012 – December 2019 on 520 patients who underwent RALP with NeuroSAFE at our Institution. Exclusion criteria was pre‐operative indication to perform an extra‐fascial nerve spare or wide local excision prostatectomy, including salvage RALP. Our Institution's database was analysed for false positive frozen section (FS) margins as confirmed on paraffin histopathological analysis; console and FS report time; functional outcomes of potency, continence, surgical margins and biochemical recurrence (BCR).
Results: The median (range) of operative console time of our NeuroSAFE RALPs was 145 (90–300) minutes. The mean time of FS processing to report was 35 minutes. In our cohort, positive FS was seen in 30.7% (160/520) of patients, with a confirmatory paraffin analysis in 91.8% of cases (147/160). The neurovascular bundles (NVBs) that underwent secondary resection, contained tumour in 26.8% (43/160) of cases. 77.5% T2, 22.3% T3 cancer was found on final prostate specimen analysis. Biochemical recurrence (BCR) was 6.7% (35/520), of which FS was positive in 40% (14/35) of those cases. Bilateral nerve spare (NS) RALP was statistically significant for potency, over wide excision due to positive FS. There was insufficient evidence of a statistically significant association of urinary incontinence and positive surgical margin rates according to NS or NVB resection
Conclusions: Our mid to long term results of NeuroSAFE RALP describes acceptable functional outcomes. NeuroSAFE enables intra operative confirmation of the oncologic safety of a NS procedure. Patients with a positive FS on NeuroSAFE can be converted to a negative surgical margin (NSM) by wide resection of the NVB. This spared 1 in 4 men from positive margins posterolaterally in our series. No other technique has been externally validated to offer intraoperative ‘real time’ feedback on the oncologic safety of NS RALP. Limitations are the absence of a matched contemporary cohort of NS RALP without NeuroSAFE in our centre; three surgeons with variable NVB preservation techniques and three Uro‐pathologists
Surgical quality of robotic vs laparoscopic radical nephroureterectomy for upper tract urothelial carcinoma: a multicenter propensity score matched pair analysis (ROBUUST collaborative group)
A Veccia, U Carbonara, R Meherazin, DD Eun, ML Gonzalgo, V Margulis, R Uzzo, J Porter, CP Sundaram, F Abdollah, A Mottrie, A Minervini, KH Rha, G Cacciamani, G Simone, M Ferro, Z Wu, H Djaladat, I Derweesh, R Autorino
Division of Urology, Virginia Commonwealth University Health System, Richmond, VA, USA; b Urology Unit, ASST Spedali Civili Hospital, Brescia, Italy, Department of Medical and Surgical Specialties, Radiological Science, and Public Health, University of Brescia, Italy
Introduction & Objective: To evaluate the predictors of surgical quality (bladder cuff excision‐lymph‐node dissection‐no complications‐negative surgical margins) of robotic (RRNU) vs laparoscopic radical nephroureterectomy (LRNU) within a large multicenter study (ROBUUST collaborative group).
Methods: The ROBUUST includes data of 17 centers worldwide regarding patients who underwent either RRNU or LRNU between 2015 and 2019. Any T any N non‐metastatic patients were assessed. To account for any possible confounder, a 2:1 nearest‐neighbor propensity‐score matching with a 0.001 caliper, was performed weighting data by age, gender, race/ethnicity, BMI, tumor size and hydronephrosis. An univariable and a multivariable logistic regression model including ASA ≥3, multifocal tumor, pre‐operative biopsy, neoadjuvant chemotherapy, estimated blood loss, intraoperative complications and surgical approach to evaluate the predictors of surgical quality
Results: After propensity score matching, one‐hundred and eighty‐five patients in the RRNU and 91 in the LRNU were assessed. No relevant statistically significant difference at baseline and in clinical staging was found. RRNU showed higher rate of bladder cuff excision (81.9% vs 63.7%; p < 0.001) compared to LRNU, whereas LRNU had higher rate of overall complications (42.9% vs 24.9%; p = 0.003). Shorter length of stay was found for RRNU patients (3.5 days vs 5 days; p < 0.001). At multivariable analysis, LRNU was not associated to surgical quality (OR: 0.09; 95%CI: 0.02, 0.45; p = 0.003).
Conclusions: Within a large multi‐institutional dataset worldwide, RRNU showed to present better surgical outcomes in terms of complications and length of stay compared to LRNU. In addition, laparoscopic approach seems to provide poorer surgical quality in terms of bladder cuff excision, lymph‐node dissection, no complications and negative surgical margins.
Endophytic Tumor Resection via Robotic Assisted Partial Nephrectomy: Comparison of Retroperitoneal and Transperitoneal Approaches
KE Okhawere, A Beksac, A Rambhia, KN Meilika, TG Korn, JY Lee, G Wayne, DD Eun, A Bhandari, J Porter, M Stifelman, KK Badani
Icahn School of Medicine at Mount Sinai
Introduction & Objective: Resection of endophytic tumors presents a challenging scenario during robotic partial nephrectomy (RPN). Similar long term survival outcomes have been reported in the literature between retroperitoneal approach and transperitoneal approach RPN. As a result, with the goal of identifying an optimal surgical approach for RPN for endophytic tumors, we performed comparison of these two surgical approaches.
Methods: Data was obtained from our Multi‐institutional database of patients who underwent RPN for a completely endophytic renal mass using a transperitoneal or retroperitoneal approach. Exclusion criteria included patients who had missing data on surgical approach, solitary kidney, prior ipsilateral surgery, multiple tumors, and horseshoe kidney. Overall, 100 patient were included in the analysis. We compared baseline characteristics, perioperative and postoperative outcomes between transperitoneal and retroperitoneal approach using Mann Whitney U test, Chi‐square test and Fishers exact test.
Results: Of the 100 patients, 63 had transperitoneal RPN and 37 had retroperitoneal RPN. There was no significant difference in age (p = 0.322), gender (p = 0.907), body mass index (p = 0.467), Charlson comorbidity index (p = 0.834), tumor size (p = 0.977), RENAL nephrometry score (p = 0.857), and baseline estimated glomerular filtration rate (p = 0.619). Similarly, there was no difference in perioperative outcomes between the two approaches ‐ ischemia time (15 min vs. 18 min, p = 0.112), operative time (156 vs. 155 min, p = 0.752), estimated blood loss (100 ml vs, 50 ml, p = 0.115), length of stay (1 day vs. 1 day, p = 0.114) and perioperative complication rate (12% vs. 11%, p = 1.000). Positive surgical margin rate was similar between the two groups (3.1 vs. 2.7%, p = 1.000). Last follow‐up eGFR (p = 0.324) and de novo CKD occurrence (p = 0.706) was not significantly different between the two approaches.
Conclusions: Transperitoneal and retroperitoneal RPN yielded similar perioperative and functional outcomes in patients with endophytic tumors.
Robotic surgical management of recurrent kidney tumors: operative and oncologic outcomes in a single center experience
J Daza, TG Korn, KE Okhawere, KN Meilika, A Beksac, KK Badani
Icahn School of Medicine at Mount Sinai
Introduction & Objective: Approximately 4% of partial nephrectomy (PN) report local recurrences after surgery, necessitating a repeat partial or radical nephrectomy. Thus, a salvage PN (sRPN) is desirable when it would not interfere with oncological outcomes. In this study, we descriptively compare our center experience in the management of recurrent kidney tumors using a robotic radical and partial nephrectomy.
Methods: 78 patients with recurrence after a previous history of renal malignancy were identified. We compared baseline characteristics, surgical and pathological outcomes among those who had salvage robotic radical nephrectomy (sRRN) (n = 17, 21.52%) and sRPN (n = 62, 78.48%). Continuous variables were reported with medians and interquartile ranges while categorical variables were reported with frequency and percentages.
Results: Operative time between the sRRN and sRPN groups were similar (133 min vs 135 min). The median estimated blood loss for sRRN was 68 ml, compared to 100ml in sRPN. The median Ischemia time for sRPN was 12 minutes. One sRRN case was converted to open radical nephrectomy. In the sRRN group, no intraoperative complication was reported, while sSPN reported 3 cases. No major complications were reported in sRRN whereas sRPN had one complication. Median length of stay was 2 days for sRRN and 1 day for sRPN. Among the patients who underwent sRRN, the two most prevalent stages were pT1a (40%) and pT3a (26.67%). Whereas the two most prevalent stages in sRPN patients were pT1a (84.44%) and pT1b (13.33%). One recurrence was reported after sRRN (16.67%) while two were described after sRPN (6.67%).
Conclusions: sRPN may have similar oncological and perioperative outcomes as sRRN, Hence, sRRN and sRPN are safe and feasible procedures in patients with metachronous kidney tumors. We consider sRPN beneficial to patients with risk of local reoccurrences because of the critical need to preserve renal function and the likelihood of subsequent recurrence.
Factors Affecting Robotic and Laparoscopic Partial Converted to Radical Nephrectomy: A Retrospective Multi‐Institutional Study in the Michigan Urologic Surgery Improvement Collaborative (MUSIC)
M Rudoff, C Rogers, J Qi, A Johnson, M Mirza, B Lane, D Wenzler
Michigan State University College of Human Medicine
Introduction & Objective: Robot‐assisted partial nephrectomy (RPN) has become a common approach for surgical management of T1a renal masses. Previous studies are primarily from tertiary referral centers. We sought to identify factors affecting conversion of robotic and laparoscopic partial nephrectomy (LPN) in a multi‐institutional setting and to assess if patients with masses amenable to RPN or LPN would have a change in outcome compared to tertiary referral centers.
Methods: We retrospectively identified 324 patients who underwent attempted RPN or LPN between 2016 – 2019 at multiple centers, all of which are part of the Michigan Urologic Surgery Improvement Collaborative (MUSIC) database. Patient characteristics such as body mass index (BMI), Charlson comorbidity index, age, pre‐operative creatinine, and presence of chronic kidney disease (CKD) were collected. Data regarding the tumor, such as R.E.N.L. score, tumor size, reasons for conversion and final pathology results were also examined. These data and perioperative outcome were then compared between converted and non‐converted cases.
Results: The overall conversion rate was 4.6% (15 of 324 cases, 13 robotic, 2 laparoscopic). Patient age, BMI, Charlson comorbidity index, pre‐operative creatinine, and presence of chronic kidney disease did not significantly impact the rate of conversion. Tumor location was the main reason for conversion, accounting for 11/15 (73.3%) of conversions. Difficult dissection, blood loss, and tumor invading critical structures were also reasons for conversion. Increasing tumor size (4.6 vs 2.7cm, p < 0.01) was an independent factor for conversion. R.E.N.A.L. score was only reported in 75 cases. In reported cases, increasing R.E.N.L score was associated with increased rate of conversion. When the surgeons were surveyed of reasons for conversion, tumor location and characteristics was the most common reason cited (65%, 11/17), followed by proximity to the renal hilum (24%, 4/17), followed by blood loss (12%, 2/17). Converted cases final pathology revealed fat invasion 33% (5/15), Gerota fascia invasion 6.7% (1/15), renal vein invasion 13.3% (2/5), and direct extension to adrenal 6.7% (1/15).
Conclusions: In a multi‐institutional setting, the rate of robotic or laparoscopic partial converted to radical nephrectomy was 4.6%. This is consistent with the average rate of conversion at tertiary referral centers in previously reported literature. In our study, increasing tumor size and tumor complexity using R.E.N.L. score were the main predictors of conversion.
Impact of Multiple Renal Vessels on Graft Function in Laparoscopic Live Donor Nephrectomy
S Jayaprakash, M Thangarasu, N Jain
Apollo Main Hospitals, Chennai, Tamil Nadu, India
Introduction & Objective: Laparoscopic live donor nephrectomy (LLDN) in patients with multiple renal vessels(MRV) is technically challenging and concerns regarding prolonged operative times, ischemia time, and increased risk of complications still persists. Our objective is to assess the impact of multiple renal arteries and veins on graft function in laparoscopic kidney transplantation and comparison of the same with single renal arteries and veins in terms of early recipient outcomes, donor morbidities and graft function. There are no studies till now in South India.
Methods: A prospective, non‐randomized cohort study was conducted including all live laparoscopic donor renal transplants done by the Department of Nephrology and the Department of Urology, Apollo Hospital, Chennai between October 2018 and April 2020. A total of 117 consecutive live donor nephrectomies were performed and they were divided into Group 1(n = 41) multiple renal vessels and Group 2(n = 76) single renal vessels. They were compared in terms of donor and recipient outcomes.
Results: Laparoscopic donor nephrectomy was done successfully in 116 patients, one patient in group 1 needed conversion to open. Among Group 1, 10/41 (24.3%) had multiple veins and 9/41(21.9%) had early branching of arteries. Slow graft function was seen in 3 patients in each Group 1 (7.3%) and Group 2(3.9%), No Delayed graft function was seen in either groups. Graft failure was seen in one patient of Group 2, overall graft survival at 1 year was 100% in group 1 and 98% in group 2. No deaths were seen in either group. On comparison of outcomes between Group 1 and 2 only warm ischemia time was prolonged in group 1 (statistically significant), creatinine values at day 1, day 3, 1 month, 1 year, total operative time and complications (one urological complication – ureteral stenosis in group 1, no vascular complications) were statistically insignificant.
Conclusions: Laparoscopic live donor nephrectomy is a safe procedure for the donor, even with vascular multiplicity (including multiple veins) and should be considered to become the standard of care in living kidney donor transplantation regardless the number of renal vessels.
Robotic approach and other factors associated with early discharge following simple prostatectomy: a New York statewide analysis, 2009‐2017
KT Ravivarapu, EB Garden, O Omidele, A Small, O Al‐Alao, MA Palese
Icahn School of Medicine at Mount Sinai
Introduction & Objective: We sought to identify patient, provider, and facility factors associated with early discharge following simple prostatectomy (SP) for benign prostatic hyperplasia (BPH).
Methods: Using the New York State Statewide Planning and Research Cooperative System database, we analyzed all patients who underwent SP for BPH from 2009 to 2017 using ICD‐9 codes 60.3/60.4. Early discharge was defined as length of stay (LOS) <25th percentile (≤3 days). Multivariate logistic regression was performed to identify predictive factors associated with early discharge following SP, controlling for patient, provider, and facility‐level variables .
Results: Of 2907 patients included in the analysis, the average age was 70.8 +/‐ 8.2. From 2009‐2017, the rate of early discharge following SP increased from 32.5% to 42.7% of cases. Over this period, the rate of robotic approach increased from 2.6% to 16.8%. In multivariate analysis, early discharge following SP correlated with patients aged 45‐65 years (Ref: >65 years, OR 1.805, 95% CI 1.462‐2.228, p < 0.001), high hospital SP volume (Ref: low hospital SP volume, OR 1.330, 95% CI 1.030‐1.716, p = 0.029), surgeons with 16‐30 years of experience prior to surgery (Ref: 31+ years, OR 1.694, 95% CI 1.288‐2.229, p < 0.001), surgeons with 15 years of experience (Ref: 31+ years, OR 1.309, 95% CI 1.031‐1.663, p = 0.027), high surgeon SP volume (Ref: low surgeon SP volume, OR 1.527, 95% CI 1.152‐2.024, p = 0.003), and robotic approach (Ref: open SP, OR 3.266, 95% CI 2.339‐4.561, p < 0.001). Negative predictors of early discharge included Charlson Comorbidity Index 1‐2 (Ref: 0, OR 0.735, 95% CI 0.593‐0.911, p = 0.005), Medicaid insurance (Ref: self payor, OR 0.474, 95% CI 0.232‐0.969, p = 0.041), and teaching hospital status (Ref: non‐teaching, OR 0.647, 95% CI 0.489‐0.954, p = 0.002) (Table 1).
Conclusions: Early discharge after SP was associated with patient‐level factors like younger age and lower medical comorbidity index score, provider‐level factors such as newer graduates, high volume surgeons and robotic approach, as well as facility‐level factors such as high SP volume and non‐teaching status. The strongest driver of early discharge was use of a robotic approach, which increased substantially during the study period.
Laparoscopic partial nephrectomy with Thulium Laser enucleation of the tumour: perioperative and functional outcomes
M Maltagliati, L Berti, C Buizza, L Rivolta, A Calori, M Sighinolfi, S Micali, BC Rocco, G Bozzini
ASST Valle Olona
Introduction & Objective: To evaluate the technical feasibility, safety and functional outcomes of Thulium laser enucleation of RCC (Renal Cell Carcinoma) during Laparoscopic partial nephrectomy.
Methods: We evaluated consecutive patients with American Society of Anaesthesiologists (ASA) scores 1‐2 who underwent Thulium laser enucleation of RCC (ThuLER) during laparoscopic partial nephrectomy with controlled hypotension performed by a single surgeon from December 2019 to December 2020 (Group 1). Operative data, complications, Hb drop, serum creatinine and estimated glomerular filtration rates were compared with an homogenous group who performed a conventional enucleation of the mass (Group 2). Differences between groups were evaluated by the Chi‐square test and the Student's t test.
Results: 25 pts were in Group 1 and 27 in Group 2. No significant differences in mean intraoperative procedure duration and complication rate were found. The mean tumor diameter was 3.23 (1.5‐5.5). The mean PADUA score was 7.2 (5‐9). On the other hand, blood loss was found in favour for Group 1. 223 ml (range: 30‐500 ml in group 1) and 301 ml (range: 100‐850 ml in group 2); p = 0.045, 123 min vs 108 min and 8 % versus 11.1 %; p = 0.234, respectively about procedure lengths and complication rate. The renal vessels were not clamped, resulting in a warm ischemia time (WIT) of 0 minutes in all cases. All lesions in both groups were renal‐cell carcinoma stage pT1a. In all cases, base margins had negative results for tumor.
Conclusions: ThuLER during laparoscopic partial nephrectomy with controlled hypotension for RCC patients in ASA 1‐2 patients was feasible with no significant higher procedure length and less intraoperative blood loss and postoperative complications compared to conventional standard enucleation. The benefits of Thulium laser features seem to be promising.
Comparison of Bladder Neck Contracture Formation between Robotic Intracorporeal versus Extracorporeal Neobladder Construction
R Bhatt, J Vetter, KG Sands, A Zafar, AK Chow, E Kim
Washington University School of Medicine
Introduction & Objective: Robot assisted radical cystectomy (RARC) has become more accessible to surgeons world‐wide and descriptions of intracorporeal urinary diversion techniques such as orthotopic neobladder construction have increased. In this study, we aim to compare the rate of bladder neck contracture (BNC) formation between RARC with intracorporeal versus extracorporeal neobladder creation.
Methods: We retrospectively analyzed our database for patients who underwent RARC with an orthotopic neobladder as their urinary diversion (both intracorporeal and extracorporeal) between 2012‐2019. BNC was defined by the need for an additional surgical procedure (e.g. dilation, urethrotomy). Patients who underwent RARC with intracorporeal neobladder (n = 8) were compared to patients who underwent RARC with extracorporeal neobladder (n = 11) across patient characteristics and postoperative BNC formation rates. Kaplan‐Meier curves were generated for freedom from BNC based on neobladder approach and compared with the log‐rank test.
Results: For patients who received an extracorporeal neobladder, 73% (8/11) developed a BNC. In comparison, none of the patients in the intracorporeal group experienced BNC. Kaplan‐Meier survival analysis demonstrates the extracorporeal group's median probability of freedom from BNC as 1.3 years, while the intracorporeal group is free of BNC (p = 0.025).
Conclusions: RARC with intracorporeal neobladder creation demonstrated a significantly reduced BNC rate in contrast to RARC with extracorporeal neobladder construction. Longer term follow‐up is needed to assess the durability of this difference in BNC rates.
Comparison of Decipher Score in patients with both biopsy and prostatectomy tissue specimens
S Reddy, R Perera, J Noël, M Moschovas, S Bhat, R Pokhrel, M Sandri, T Rogers, V Patel
Global Robotics Institute
Introduction & Objective: The Decipher score (DS) utilizes a 22 RNA panel to discriminate prostate cancer metastasis and cancer‐specific mortality. The aim of this study is to assess the concordance of scores in a group of patients who had DS run on both prostate biopsy (PB) and prostatectomy specimen (PS).
Methods: We evaluated 57 patients with DS on their PB and PS from 2017–2020. DS was evaluated continuously in 0.1 increments (score range: 0‐1). We evaluated the concordance and predictive ability of PB and PS DS for adverse pathological features of extracapsular extension (ECE), seminal vesicle invasion (SVI), lymph node invasion (LNI), persistent PSA (PSA >0.1ng/ml at first postop PSA) and biochemical recurrence (BCR) using exact logistic regression and Pearson's coefficient correlation matrix.
Results: In our study, the median age of cohort was 69 years (IQR 65‐71) with a median follow up of 36 months (IQR 33‐38). Median preoperative PSA was 7.2 ng/ml (IQR 5 ‐ 9.7) and clinical T stage for T1c n = 33 (56%), T2a n = 23 (39%) and T2c n = 2 (3%). The median ISUP on PB was 3 (IQR 3 ‐ 4) and on PS was 3 (IQR 3 ‐ 5). The median DS on biopsy specimens was 0.68 (IQR 0.44 ‐ 0.79) and on the PS was 0.58 (IQR 0.44 ‐ 0.79). The concordance between BS and PS on Lin's concordance was 0.44 (95%CI 0.23 ‐ 0.65). Table 1 illustrates DS scores association with adverse pathologic features. No statistically significant association was found with PB and PS scores with ECE, LNI, PSM, SVI, or BCR. DS on PB had an OR of 2.01 (per 0.1 increase in DS) for persistent PSA (p = 0.008, 95%CI 1.16‐4.08), and PS had an OR of 2.15 (p = 0.0042, 95%CI 1.24‐4.43) for persistent PSA.
Conclusions: To our knowledge, this is the first study to compare the predictive ability of DS in PB and PS of the same patients for ECE, SVI, LNI, and BCR. We identified moderate concordance between the DS on PB and PS. There was statistically significant association of both PB and PS scores with persistent PSA but not with other parameters. Our sample size and event number were limited and future studies with more power may investigate these associations further.
Single‐Port robotic assisted kidney surgery: 2 years of experience with a novel platform
MJ Zuberek, L Morgantini, A Ganesh, C Dennis, R Trippel, J Huang, S Francavilla, M Abern, S Crivellaro
University of Illinois Hospital and Clinics
Introduction & Objective: 20 years after the launch of a Multiport (MP) surgical robot, Intuitive Surgical (Sunnyvale, CA.) has recently introduced a new Single‐Port Robotic Platform (SP) for urologic procedures. Initial reports provided a non‐inferiority confirmation of the platform. In this investigation we provide more than 2 years of data to support the feasibility and safety of the surgical management of multiple renal pathologies with the SP platform.
Methods: A retrospective chart review was performed on renal surgeries performed between December 2018 and February 2021 on 60 consecutive patients with clinically localized renal masses, infected cysts, or non functional kidneys. These procedures were performed by two experienced robotic surgeons in either transperitoneal (77%) or retroperitoneal (33%) approach.
Results: The mean operative time was 196.67 ± 39.69min. Mean estimated blood loss was 118 ± 161.76 ml. The mean warm ischemia time was 14.40 ± 15.40min. Length of stay average was 1.78 ± 2.07 days. Average RENAL nephrometry score for this population was 6.54 ± 2.3. There were a total of 5 intraoperative complications, 2 of which necessitated conversion to an open procedure.11 patients (18.3%) experienced postoperative complications highest being Clavien‐Dindo 3b. 14% of cases had positive surgical margins. However, at a mean length of follow up 4.21 ± 4.31 months, only 1 patient had recurrence and metastases present. Table 1 presents the breakdown of the study population.
Conclusions: In this extended cohort of 60 patients undergoing renal SP interventions we observed satisfactory patient outcomes that were at least comparable with previously published MP data. We believe that SP renal surgery has earned its place as a technique in the robotic landscape of urology and should be considered as an option for experienced surgeons.
Single‐Port robotic assisted retroperitoneal vs transperitoneal partial nephrectomy : a retrospective analysis
MJ Zuberek, L Morgantini, A Ganesh, C Dennis, R Trippel, J Huang, S Francavilla, M Abern, S Crivellaro
University of Illinois Hospital and Clinics
Introduction & Objective: 20 years after the launch of a Multiport (MP) surgical robot, Intuitive Surgical (Sunnyvale, CA.) has introduced a Single‐Port Robotic Platform (SP) for urologic procedures. Initial reports provided a non‐inferiority confirmation. Retroperitoneal (RP) robotic multiport kidney surgery has been previously described and validated. In this investigation we aim to compare the operative results of the RP vs transperitoneal(TP) approach with SP robotic partial nephrectomy (PN).
Methods: A retrospective chart review was performed on SP PN performed between December 2018 and February 2021 on 38 patients with clinically localized renal masses. These procedures were performed by two experienced robotic surgeons in either TP or RP approach.
Results: The RENAL score was lower in patients undergoing RP than TP surgery ( 5.11 vs 6 p = 0.041). Length of stay approached statistical significance, but not clinical (1.18 vs.1.55 p = 0.087). Notable parameters favoring RP over TP were operative time (165 min. vs 209 min. p = 0.008) and blood loss (79 ml vs 166 ml p = 0.050). The lack of difference in ischemia time for TP vs RP (24.05 min. vs 21.27 min. p = 0.312) is compensating the difference in the RENAL score. Complication rate was similar in both groups as the presence of positive surgical margins.
Conclusions: SP robotic TP and RP PN follow the previous surgical validation parameters established for robotic surgery. Length of stay is approaching a statistically significant difference in favor of RP and combined with decreased operative time and blood loss might make this approach more suitable for SP use in PN. Further prospective randomized studies are required to confirm these findings.
A novel risk index for cardiovascular adverse events following Partial Nephrectomy
AA Nasrallah, H Dakik, NF Abou Heidar, J Najdi, O Nasrallah, M Mansour, H Tamim, A El Hajj
Department of Surgery, Division of Urology. American University of Beirut Medical Center
Introduction & Objective: Partial Nephrectomy (PN) is the gold‐standard treatment for small localized renal masses. Its merits include preservation of renal functionality and relatively low complication rates. The rise of PN has seen a parallel increase in robotic‐assisted approaches. However, it is associated with a non‐trivial risk of cardiovascular morbidity and mortality in certain high‐risk patients. We aim to develop a PN‐specific risk index, and compare its performance to the Revised Cardiac Risk Index (RCRI) and AUB‐HAS2 index.
Methods: The American College of Surgeons – National Surgical Quality Improvement Program (ACS‐NSQIP) was used for identification of PN patients, and the outcome was defined as incidence of myocardial infarction, stroke, or mortality within 30 days of operation. A multivariate logistic regression analysis was conducted and resulted in a 6‐factor risk index. Performance and calibration were tested by a ROC analysis and the Hosmer‐Lemeshow test for goodness of fit, and compared to the RCRI and AUB‐HAS2 indices.
Results: From a cohort of 4,795 patients, 52 (1.1%) suffered from cardiovascular events. The final model included: Age ≥75 years, ASA class >2, Anemia, surgical Approach, Creatinine >1.5 mg/dL, and history of Heart disease; resulting in the PN‐A4CH index (Table 1). To note, open surgery was associated with an odds ratio of 2.8 (P < 0.001). ROC analysis showed a C‐Statistic of 0.81, calibration R2 was 0.99, and sensitivity was 85%. The RCRI index and AUB‐HAS2 indices provided C‐Statistics of 0.59 and 0.68 respectively (Figure 1).
Conclusions: The PN‐A4CH index showed good predictive ability, high calibration, and surpassed universal risk indices. The effect of surgical approach was well noted as open surgery was associated with increased odds of cardiovascular adverse events in comparison to minimally‐invasive approaches. The index would enable improved patient selection and optimization of perioperative management.
Results of a late clamping early declamping retroperitoneoscopic robotic assisted partial nephrectomy in a single surgeon series
W Khoder, S Astheimer, J Michaelis, M Grabbert, P Pohlmann, C Gratzke
Urology Department, Freiburg University
Introduction & Objective: The acceptable warm ischemia time (WIT) remains a matter of debate. Robotic‐assisted Retroperitoneoscopic partial nephrectomy (RPRPN) is an emerging promising approach, however associated with some challenges especially for some tumor locations. We present the results of late clamping early declamping RARPN for tumors in different renal positions to shorten WIT in a single surgeon series.
Methods: Beside 12mm assistant port, a robotic four‐arm retroperitoneal approach was performed. Hilar dissection of the renal artery follows. Gerota's fascia was entered some distance away from the tumour. Fat and Gerota's fascia were preserved on the tumor for accurate pathologic staging and to aid in retraction. Excision of the tumor was performed using cold cut scissors and Mirland forceps. After resection of tumor from all sides till depth in renal parenchyma, a bulldog clamp was applied, before cutting the deep tumor connection. A 4‐0 monocryl suture with an anchoring Hem‐o‐lok clip was used to oversaw renal parenchymal vessels and open renal calyces in tumor bed. The bulldog clamp is removed and the defect in the renal cortex was closed with 2/0 vicryl Sutures using sliding‐clip renorrhaphy.
Results: 239 consecutive patients underwent late clamping early declamping RPRPN. Tumor location was anterior (24%), posterior(72%), upper pole (33%), lower pole (26%), middle kidney (51%), peripheral (83%), central/hilar (17%). Median tumor size 3,8cm (2.8‐6.9). Median BMI 27.86 kg/m^2 (17.64‐48.47), median age 60.4years (25‐88), men versus females (60.67%vs.39.33%), right versus left kidney (48.17% vs 51.22%), ASA‐classification was grade I(4.57%), II(56.4%) and III (37.8%). median operation time (skin to skin) was 136min, median blood loss 175ml (100‐1000) with median WIT of 11 Minutes. There were no encountered conversions. The drains were removed in the 3rd postoperative day. Clavien‐Dindo classification of the postoperative complications only in 43 (17,9%) Patients, Grade I 19patients(44,2%), Grade II 10 patients(23,3%), Grade IIIa 7patients(16,3%), Grade IIIb 4 (9.3%), Grade IV 2(4,6%). CT/MRI at 3 months postoperatively documented complete healing of the defects with good ipsilateral renal function.
Conclusions: RARPN is feasible for all tumor locations in the kidney. The late clamping early declamping technique helps to shorten WIT to a significant level minimizing the effects of technical challenges of this approach.
Intraoperative Mannitol Administration During Laparoscopic Donor Nephrectomy and Impact on Long‐Term Graft Function
J Farrow, G Gryzinski, CD Bahler, CP Sundaram
Indiana University Health
Introduction & Objective: End‐Stage Renal Disease frequently results in dialysis, and at best, transplantation. Laparoscopic donor nephrectomy was introduced in 1995 and has been a valuable source of high‐quality organs. Improving long‐term graft function of recipients through judicious intra‐operative medical management remains an essential goal. Infusion of mannitol prior to hilar clamping during donor nephrectomy has been utilized by some surgeons based on its proposed cytoprotective properties – theoretically improving renal profusion, free‐radical savaging, and diuresis. However, there is a paucity of large long‐term studies evaluating its use. In this study, we aimed to explore the long‐term effects of mannitol administration on graft function as measured by creatinine.
Methods: A single‐center retrospective analysis of a contemporary cohort of donor nephrectomies was performed. Eighty donors (sample determined using a power 0.8 to detect a 20% difference in creatinine) were identified and then matched to recipients using Indiana University's Organ Transplant Tracking Record database. Patients were balanced by sex and stratified by intra‐operative administration of mannitol (yes vs no). Creatinine was recorded at fixed intervals per routine nephrology follow‐up. Statistical analysis was performed using SPSS.
Results: Basic demographics are presented in Table 1. The only significant difference in baseline clinical factors was diuretic administration, which was more frequently co‐administered with mannitol. Creatinine means by time can be seen in Figure 1. Multiple means comparisons were made using ANOVA and did not reveal any differences in creatinine up to 3 years of follow‐up (p > 0.05).
Conclusions: Mannitol administration did not statistical affect post‐transplant creatinine up to the three‐years follow‐up. On post‐hoc analysis, elimination of cases where diuretics were co‐administered did not change these results. Study limited by retrospective design and potential for unmeasured confounding. We did not control for kidney volume which can also influence creatinine trend. Future studies are warranted assuming larger sample size and potentially more restrictive definitions of creatinine change.
Propensity Score Matched Analysis of Single Port Versus Multiport Partial Nephrectomy
R Harrison, M Billah, T Lulla, C Caviasco, H Koster, R Sanchez De La Rosa, F Sheckley, A Sanders, G Lovallo, M Ahmed, MD Stifelman
Hackensack Meridian Hackensack University Medical Center
Introduction & Objective: In this study we compare perioperative and follow‐up outcomes between single port (SP) partial nephrectomy (PN) and multiport (MP) partial nephrectomy cases utilizing propensity score matching.
Methods: A retrospective chart review was performed of patients who underwent SP‐PN at our institution between 1/1/2019 and 10/1/2020. These patients were matched to MP patients from our prospective renal cancer database (1:1) on age (< 65, ≥65), sex, BMI, prior abdominal surgery, and nephrometry score using the optimal matching method. Categorical variables were compared using McNemar's test or Bowker's test of symmetry while continuous variables were compared using paired t‐tests or the Wilcoxon signed‐rank test.
Results: In all, 96 patients were included in the analysis after propensity score matching (48 MP and SP). Demographic characteristics are presented in Table 1 and show no significant differences, except pre‐op GFR category, in which the SP group had a greater percentage of patients with normal pre‐op renal function (87.5% vs 66.7%, p = 0.0352) and surgical approach, with SP cases being more likely to have been retroperitoneal. Outcome data is presented in Table 2. We found statistically significant differences only in regards to opioid use (measured in total morphine equivalents (TME)), with SP patients having lower median POD 1 (4.6 vs 9.8 TME, p = 0.0209) and cumulative opioid use (11.2 vs 18.4 TME, p = 0.0357).
Conclusions: Our early experience with SP‐PN shows similar outcomes when compared to MP‐PN regarding key metrics such as operative time, estimated blood loss, intraoperative complications and post‐op length of stay. These findings suggest SP‐PN is safe, reproducible and potentially offers better pain control, as evidenced by lower POD 1 and cumulative admission opioid use. Finally, SP may be more suitable for a retroperitoneal technique as evidenced by the increased use of this approach in SP patients. Further multi‐institutional studies are on the way to collaborate these findings.
Single‐center comparison hybrid vs robotic approach to nephrectomy and IVC thrombectomy
R Harrison, M Billah, R Sawhney, J Zaifman, M Wilderman, G Lovallo, M Ahmed, MD Stifelman
Hackensack Meridian Hackensack University Medical Center
Introduction & Objective: Radical nephrectomy (RN) with Inferior Vena Cava thrombectomy (IVC‐T) presents a serious challenge for even the most experienced urologist. Although continual advances make a fully‐ robotic approach more feasible, standard of care remains an open approach. For several years, surgeons at our institution have utilized a hybrid approach to this demanding surgery: the urologist performs the RN robotically while a vascular surgeon performs an open IVC‐T via a relatively small subcostal incision. This hybrid approach offers several potential benefits over a traditional open approach, namely a smaller incision with less chance of entering the thoracic cavity. The relative safety and efficacy of this approach have not been extensively investigated to date. Thus, the primary objective of this study was to compare perioperative outcomes in patients undergoing RN with either robotic or hybrid IVC‐T for level I‐II IVC tumor thrombus.
Methods: A retrospective chart review was performed of patients who underwent RN with IVC‐T at our institution from 2015 to 2021. End points included operative time, estimated blood loss, and intra‐ and post‐operative complications. Categorical variables were compared using chi‐ squared or Fisher's exact tests, continuous variables were compared using Mann‐Whitney U test.
Results: 14 patients were identified who had undergone RN with IVC‐T: 5 robotic, 9 hybrid. Table 1 summarizes the cohort's demographic characteristics‐ no significant differences were found. Outcome data is presented in Table 2. The hybrid approach was found to have significantly higher estimated blood loss (800 vs 50 mL, p = 0.029), was more likely to receive intraoperative transfusion (66.7% vs 0.0%, p = 0.028), and a longer hospital stay (4.0 vs 2.0 days, p = 0.001).
Conclusions: The hybrid approach is generally reserved for more difficult cases than could be handled robotically, which may help explain our findings. Ultimately more cases are needed before drawing conclusions about the role of this approach.
Moderated Poster Session 30: Prostate Cancer
Post Radical Prostatectomy Radiation Therapy with Androgen Deprivation Therapy Does Not Improve 10‐Year Overall and Prostate Cancer Specific Mortality Compared to Androgen Deprivation Therapy Alone
TE Ahlering, LM Huynh, E Huang, H Su
University of California, Irvine
Introduction & Objective: Salvage radiation therapy (sRT) has been shown to reliably reduce biochemical recurrence (BCR) following radical prostatectomy (RP); however, direct comparison of patients receiving concurrent sRT and androgen deprivation therapy (ADT) versus ADT monotherapy has not been published. We aim to compare 10‐yr overall survival (OS) and prostate‐cancer specific survival (PCSS) between sRT+ADT and ADT monotherapy.
Methods: Single surgeon retrospective cohort analysis (n = 1865) of prospective data of 406 BCRs after RP (adjuvant therapy or PSA >0.2 ng/dl, x2). Patients were managed with concurrent sRT+ADT (n = 87), ADT alone (n = 158), and active surveillance only (AS, n = 138). 10‐yr Kaplan‐Meier and Cox regression for OS and PCSS were measured. Ad hoc analysis was conducted combining AS (candidates for sRT) to the sRT+ADT group.
Results: Median (IQR) follow‐up was 7.3 (3.9‐10.7) years. Between sRT+ADT and ADT, OS (82.2% vs 73.2%, p = 0.09) and PCSS (82.5% vs 86.8%, p = 0.39) were not different in 10‐yr Kaplan‐Meier analysis. After adjusting for age, Gleason grade, stage, and preoperative PSA in Cox regression, OS and PCSS was not significantly different.
Ad hoc analysis of 138 (38%) BCR patients with DT >12months managed with only AS demonstrated OS and PCSS of 92% and 100% respectively. Further, when the sRT+ADT was combined with AS, OS/PCSS improved significantly compared to ADT monotherapy in Kaplan‐Meier analysis (p < 0.005).
Conclusions: The findings suggest that adding sRT to ADT did not improve OS/PCSS compared to ADT monotherapy. The absence of PCSM in AS patients, all of whom were candidates for sRT suggests the reason. The ad hoc introduction of the AS group resulted in statistically significantly lower PCSM in the RT/ADT group.
Active surveillance of post‐radical prostatectomy biochemical recurrence: Long term assessment of outcomes
TE Ahlering, E Huang, LM Huynh, H Su
University of California, Irvine
Introduction & Objective: Biochemical recurrence (BCR) following radical prostatectomy (RP) is an unreliable predictor of distant metastatic progression or prostate cancer death, consequently resulting in potential complications and expenses of overtreatment. Further, little has been published regarding the management decisions and outcomes for active surveillance (AS) patients. Herein, we characterize our long term experience with AS following post‐RP BCR without radiation and/or androgen deprivation therapy.
Methods: From June 2002 and September 2019, 1865 men underwent RP, of which 406 experienced BCR. Of these, 138 (34%) were observed without treatment intervention. BCR was defined by PSA >0.2 ng/dl, x2. PSAs were checked every 1‐3 months and entered into a PSADT graph (Figure 1). Men were considered to be formally in AS after 3+ years of increasing DT following surgery. Men with decreasing DT were treated and censored.
Results: Table 1 depicts the demographics of the AS patients, with a median follow‐up was 7.3 years (IQR: 4.6‐10.6) post‐RP. Of patients on AS, the average age was 63.7 +/‐ 7.2 years and 86%, 48%, 40%, 51% and 14% were GG 1 through 5, respectively. The current DT of AS patients averages 20 months, with 0% PCSM. Only 10% of patients with decreasing DT began treatment after an average of 4 years following BCR.
Conclusions: Of 406 patients experiencing post‐RP BCR, 34% of patients are effectively managed with AS, with 0% PCSM across all GG. Presently 69 (50%) AS men have been under observation for 7.3 to 18 years. These findings suggest that a significant portion of patients display a benign recurrence, characterized by an increasing DT following BCR and can be managed safely with observation alone.
Post‐radical prostatectomy prostate‐specific antigen doubling‐time kinetics: Observations of increasing versus decreasing doubling times
TE Ahlering, LM Huynh, E Huang, D Skarecky
University of California, Irvine
Introduction & Objective: Biochemical recurrence (BCR) following radical prostatectomy (RP) is an unreliable predictor of distant metastatic progression or prostate cancer (PC) death, consequently resulting in overtreatment. Further, little has been published about active surveillance (AS) specific management recommendations. Herein, we validate the practicality of using the kinetics (change) of PSA doubling time (PSADT) to direct continued observation versus intervention.
Methods: In a retrospective cohort analysis of 406 men with BCR (defined as adjuvant therapy or PSA >0.2 ng/dl, x2), 284 men were monitored post RP with PSADT graphs for all patients, and the PSADT was characterized as increasing vs decreasing. Receiver‐operator characteristic (ROC) curves were generated to assess the sensitivity/specificity/positive predictive value/negative predictive value of PSADT progression on treatment and prostate cancer specific mortality at 10 years post‐RARP, respectively.
Results: The median follow‐up was 7.6 (IQR: 4.6‐10.6) years. Of 284 men, 109 (38%) and 175 (62%) were in the no treatment versus treatment groups, respectively. 87% of men receiving treatment had a decreasing PSADT and 100% men with PCSM had a decreasing PSADT. ROC analysis showed 0.870 sensitivity and 1.0 specificity when predicting secondary treatment (AUC = 0.935) and 0.857 sensitivity and 0.50 specificity when predicting PCSM (AUC = 0.679).
Conclusions: A decreasing PSADT is a sensitive and specific metric for predicting the need for secondary intervention. We also found all men who died of PC had a decreasing PSADT. Lastly an increasing DT predicts a benign course without need for treatment. The current findings suggest that the kinetics of PSADT, increasing versus decreasing, is an accurate metric for the need of treatment. A direct comparison between PSADT kinetics and PSADT is needed.
Robotic Transversus Abdominis Plane Block is Clinically Equivalent to Ultrasound Guided Transversus Abdominis Plane Block and Local Anesthetic Injection:A Single Blind Randomized Clinical Trial in Robotic Prostatectomy Patients
DC Rosen, JS Winoker, G Mullen, E Moshier, A Sim, P Pathak, V Wagaskar, A Reddy, MA Palese, KK Badani, P Wiklund, A Tewari, R Mehrazin
Icahn Mount Sinai School of Medicine, Urology
Introduction & Objective: Regional anesthetic is a longstanding component of postoperative analgesia and has been advanced with the use of ultrasound guided Transversus Abdominis Plane (UTAP) blocks and robotically administered intracorporeal TAP blocks (RTAP). We report the first prospective, single‐blind, randomized clinical trial of administration of regional anesthetic comparing RTAP to UTAP to Local direct injection (Local) in Robotic Prostatectomy patients.
Methods: We randomized, in a 2:2:1 fashion, 114 blinded patients undergoing multiport robotic prostatectomy to RTAP:UTAP:Local, with the study powered to demonstrate non‐inferiority of RTAP to UTAP. We compared time to deliver the block as well as OR time, postoperative pain scores using the visual analog scale (VAS) by a blinded recorder, as well as intraoperative and postoperative analgesia required, which was given on an as needed basis.
Results: There was no significant difference in patient characteristics (Table I), or in ΔVAS between RTAP and UTAP or Local (ΔVAS at all time points p > 0.05) (Table II). UTAP had less effective analgesia than Local at 12 (ΔVAS = 1.52, 95% CI [0.08, 2.96] p < 0.05) and 24hrs postop (ΔVAS = 1.53, 95% CI [0.08, 2.97], p < 0.05). RTAP and Local were faster than UTAP (time to perform block 2.5 vs. 2.5 vs. 6.25 min, p < .001; mean OR time 240 vs. 214 vs. 248 min, p = .0469). There was no difference in postoperative narcotic, acetaminophen, ketorolac, or ondansetron requirements among the groups (p > 0.05). No patient required an extended length of stay due to pain control or had a trial related adverse event. No difference in outcomes was seen in patients with BMI >30.
Conclusions: RTAP is a clinically equivalent form of regional anesthesia to UTAP. Both RTAP and Local are significantly more efficient than UTAP with shorter time spent in the operating room and equivalent postoperative pain control, need for narcotic medications, and length of stay.
The value of PSA density per lesion in combination of PI‐RADS for improving the accuracy of prostate cancer detection
M Shahait, A Sandberg, A Achkar, D Lee, MC Strother, M Rosen, D Lee
King Hussein Cancer Center
Introduction & Objective: PSA production from the benign parenchyma is fixed at 0.3 ng/cc. However, the PSA production from the tumor cells varies according to the grade of the tumor. The use of PSA density (PSA‐D) assumes that all the cells equally is responsible for excess PSA production. Recently, there has been a heightened interest in calculating tumor‐related PSA to improve the prognostication value of the PSA.
Methods: We identified 152 men who underwent MRI/US‐guided fusion biopsy. Prostate size and lesion volume were calculated from MRI images using 3‐D reconstruction software. PSA density per dominant lesion (PSADL) was calculated as following: PSADL = (Observed PSA – PSA from benign tissue)/ Lesion volume. PSA from benign tissue = (epithelial fraction (0.1)) x (PSA/cm3 epithelial tissue (0.3)) x (volume of benign prostate tissue). The NPVs of PI‐RADS lesions for detecting clinically significant tumor (CSt), Gleason score ≥7 were calculated. PSADL cutoff was determined using ROC curve.
Results: Of the 152 patients, 91 (59.9%) and 33 (21.7%) patients were PIRADS 4 and 5 , respectively. A CSt was detected in 46.9% of all men, 42.2% with men with log PSADL <0.76, and 59.4 % of men with log PSADL . For CSt, the NPV of PIRADS 1‐3 was 82.1%. 90.5% with a PSAD <0.15, 91% with log PSADL of <0.76, 90.1% with PSAD <0.15 and with a PSADL <0.76. For PIRADS 4 lesions 41.8% were negative on biopsy with a PPV of 63.9%. The NPV of PIRADS 4 lesion was 41.8% , 58.2% with PSAD <0.15, 71.4% with log PSADL (p = 0.014), 76.9% with both PSAD <0.15 and PSADL of <0.76.
Conclusions: PSA density per lesion improve the NPV of PI‐RADS 4 lesions compared to PSAD in detecting CSt. As a such, using PSA density per lesion to stratify PI‐RADS 4 lesions might help in reducing unnecessary biopsies. If validated in an external cohort, future research is needed to determine the clinical value of PSA density per lesion in the management algorithm of patients with elevated PSA and equivocal mp‐MRI findings.
Is Retzius‐Sparing Robotic Radical Prostatectomy Oncologically Safe for High Risk Prostate Cancer Patients?
R Madi, N Hakam
Augusta University Health
Introduction & Objective: Retzius‐Sparing Robotic Radical Prostatectomy (RSRRP) has been gradually gaining popularity in the USA because of improved continence outcome over conventional approach. Most of published series however exclude early experience and high risk patients. We performed a comparative analysis between 52 consecutive high risk patients who underwent regular robotic radical prostatectomy (RRRP) to 60 consecutives patients who underwent RSRRP
Methods: Between May 2015 and may 2019 we analyzed our robotic prostatectomy database and identified 52 high‐ risk patients who underwent regular consecutive RRP and 60 patients who underwent consecutive Retzius‐sparing RRP. All surgeries were performed by a single surgeon (RM). Patients are labeled high risk if they have PSA higher than 20, Gleason Score (GS) of 8 or higher, or clinical T2c or higher. Pre‐operative and post–operative characteristics were analyzed and compared between both group
Results: Median age was 62.4 (IQR: 57‐68), median BMI was 29 (IQR: 25.6‐32), and median PSA was 11.35 (IQR: 6.2‐23). 25% of patients have a family history of prostate cancer. There was no difference in median PSA or Gleason score between both groups (G.S 8). 52% of patients had nerve sparing in the RSRRP while only 28% underwent nerve sparing in the regular approach ( p = 0.034). Bladder neck sparing was performed in 78% of the RSRRRP versus 42% (p = 0.0002). Console time was shorter in the Retzius group ( 140 minutes versus 180; p < 0.0001) . Positive margins were higher in the Retzius sparing group ( 48% versus 28% ; p = 0.047). The positive margin was mostly apical in both groups. On the other hand, 53% of the RSRRP were pT3 disease versus 8% in the regular approach (p < 0.001). Pelvic lymph nodes were involved in 23% of the RSRRP versus 5% in the regular group ( p < 0.001). Median first post‐operative PSA was 0.01 (IQR: 0.01‐0.045) in the RSRRP versus 0.1 ( IQR: 0‐0.1).
Conclusions: In comparison to the regular approach, Retzius‐sparing robotic radical prostatectomy appears to have higher incidence of positive surgical margins in comparison to the regular approach. However, this may be due to a more advanced pathologic stage in the Retzius group. Interestingly, median PSA after surgery appears to be lower in the Retzius‐sparing group.
Advanced Reconstruction of Vesicourethral Support (ARVUS) during robot‐assisted radical prostatectomy : Early recovery of urinary continence and predictive factors
S Teraoka, Y Kimura, T Yumioka, N Yamaguchi, B Kawamoto, H Iwamoto, S Morizane, K Hikita, M Honda, A Takenaka
Department of Urology, Tottori University Faculty of Medicine
Introduction & Objective: We investigated the effect of Advanced Reconstruction of Vesicourethral Support (ARVUS) on postoperative urinary incontinence in robot‐assisted radical prostatectomy (RARP) using propensity score matching (PSM).
Methods: From October 2010 to October 2020, 588 patients who underwent RARP in our department were included in the study. After May 2019, ARVUS was performed in principle in nerve non‐preserving cases. Cystography was performed at the time of urethral catheter removal to measure the distance from the suprapubic margin to the bladder neck and the posterior urethral bladder angle. Urinary incontinence was measured on the day after catheter removal, and evaluated 1 and 3 months after surgery using question 1 of the ICIQ‐SF. Factors influencing the amount of urinary incontinence on the day after catheter removal were also examined using multivariate analysis.
Results: There were 118 validly analyzed cases after PSM, of which 59 were in the ARVUS group (mean age 68.9 ± 5.6 years) and 59 were in the non‐ARVUS group (mean age 68.6 ± 5.2 years). In the ARVUS group the distance from the suprapubic margin to the bladder neck during cystography was significantly shorter (p < 0.001) and the posterior urethral bladder angle was significantly smaller (p < 0.001). Although there was no obvious significant difference in the amount of urinary incontinence on the day after catheter removal, the percentage of patients with urinary incontinence of 500 ml or less on the same day was significantly higher in the ARVUS group (p = 0.011). There was no significant difference in the percentage of patients with ICIQ‐SF question 1 below 1 at 1 and 3 months after surgery between the two groups (p = 0.489 and p = 0.360, respectively). In univariate analysis, the distance from the suprapubic rim to the bladder neck, the posterior urethral bladder angle and the ARVUS technique were significantly different (p < 0.001 p = 0.015, and p = 0.041, respectively. In the multivariate analysis, distance from the suprapubic rim to the bladder neck was a predictor of urinary incontinence below 500 ml on the day after catheter removal (p = 0.003).
Conclusions: In patients who underwent ARVUS, the effectiveness of early postoperative urinary incontinence was confirmed. The distance from the suprapubic margin to the bladder neck on cystography was significantly shorter in the ARVUS group, suggesting that it may be a predictor of early postoperative urinary retention.
Can direction of tumour growth predict prostate cancer grade?
D Papadopoulis, N Chari, D Ellis, U Ukwu, K Charitopoulos, I Donkov, S Bishara, S Mukherjee
London North West University Healthcare NHS Trust
Introduction & Objective: Multi‐parametric MRI (mp‐MRI) scan is now increasingly being used as a screening tool for the diagnosis of prostate cancer and prediction of its grade. The aim of this study was to determine if the maximum diameter of prostate cancer lesions in different planes on mp‐MRI prostate can be used to distinguish between prostate cancer, grade group (GG) >2, and GG >3 on transperineal targeted biopsy and create a predictive model based on the proposed and established parameters.
Methods: Patients who had a discrete lesion and underwent targeted transperineal biopsy, following mp‐MRI between January 2019 and November 2020 were included. For each lesion, the maximum transverse (x), antero‐posterior (y) and cranio‐caudal (z) dimension were measured from T2W images, along with lesion volume and minimum ADC value. In addition, age of the patient, prostate size, PSA, PSA density and the target and non‐target prostate biopsy grade group were recorded. The parameters were assessed against the presence of prostate cancer, GG >2 and GG >3 on target biopsy by binary logistic regression, using univariate and multivariate evaluation.
Results: In total, 193 lesions from 148 patients (mean age 65.2 years, median PSA 8.26 ng/ml, mean prostate volume 50.8 ml) were evaluated. Increased lesion volume, PSA, PIRADS score and decreased ADC were associated with higher GG (p < 0.001). The ratio of cranio‐caudal to anterior‐posterior dimension of the lesion increased from 1.20 (95% CI 1.14‐1.25) for GG ≤3 to 1.43 (95% CI 1.28‐1.57) for GG >3 (p = 0.0022). Multivariate binary regression using only diameters demonstrated that cranio‐caudal dimension was independently associated with target lesion GG >2 (p = 0.0182) and GG >3 (p = 0.0011).
Univariate evaluation of all parameters demonstrated that ADC was the strongest determination of lesion cancer (p = 0.0000, AUC 0.79) and GG >2 (p = 0.0000, AUC 0.79) but lesion z was the strongest determination of lesion GG >3 (p = 0.000 AUC = 0.81). The best multivariate models had an AUC of 0.84 for cancer, 0.88 for GG >2 and 0.89 for GG >3.
Conclusions: Higher grade prostate cancer has a propensity to grow in the cranio‐caudal direction and this can be incorporated into MRI based multivariate predictive models of biopsy disease grade.
Association Between Oncotype DX Genomic Prostate Score and Final Tumor Pathology Report After Radical Prostatectomy
S Bhat, M Covas Moschovas, C Chew, M Sandri, T Rogers, P Dell'Oglio, S Roof, S Reddy, M Sighinolfi, BC Rocco, V Patel, J Noël
Introduction & Objective: The Oncotype DX assay is a clinically validated 17‐gene‐based genomic assay that provides a genomic prostate score (GPS – scale 0‐100) measuring the heterogeneous nature of prostate tumors. The test is performed on prostate tissue collected from the biopsy. With a lack of data measuring the association between the GPS and tumor pathology after radical prostatectomy (RP), our study aims to compare this genetic test with different parameters of the final pathology.
Methods: We reviewed the 749 patients who underwent both the Oncotype DX assay and RP at a referral prostate cancer center between 2015 and 2019. Multivariable logistic regression analyses were performed to assess the association between the GPS and extraprostatic extension (EPE), positive surgical margins (PSM), and seminal vesicle invasion (SVI). Covariates were represented by age, clinical stage, PSA level, Gleason score, and time between the genomic assay and surgery. Odds ratios were determined per GPS quartile as well as per 20‐unit change in the GPS as previously done by validation studies of the GPS. Our primary endpoint was the presence of high‐risk features on final pathology.
Results: The median time between the Oncotype DX assay and surgery was 179 (141‐226) days. The median age, GPS, and PSA levels were 63 (58‐68) years old, 29 (21‐39), and 5.7ng/mL (4.6‐7.7), respectively. From our multivariable analysis, GPS was an independent predictor of EPE (OR: 1.7, 95% CI 1.4 to 2.3) and SVI (OR: 2.1, 95% CI 1.3 to 3.4). Additionally, when grouped into quartiles by GPS, the percentage of cases with EPE and SVI, had increasing rates in consecutively higher GPS quartiles. The area under the curve (AUC) in ROC curves from multivariate models predicting EPE and SVI revealed incremental gains in those including the GPS compared to those that did not.
Conclusions: We provided evidence that Oncotype DX GPS is significantly associated with the adverse pathology after RP. Specifically, as the GPS increases, the risk of EPE and SVI also increase. Therefore, based on the GPS genetic test scores of each patient, these findings may help clinicians improve preoperative patient counseling and develop surgical strategies in patients with higher chances of EPE or unfavorable pathological features.
Erectile function recovery prediction using a pre and post‐operative nomogram after Robot‐Assisted Laparoscopic Prostatectomy
S Bhat, M Covas Moschovas, J Noël, S Reddy, T Rogers, V Patel
Global robotics institute
Introduction & Objective: In this study we propose a preoperative and post‐operative nomogram to predict post‐operative potency recovery following robot assisted laparoscopic prostatectomy (RALP).
Methods: Patients from 1st January 2008 to 31st December 2016 (development set, n = 6502) were selected to develop the nomograms, and patients from 1st January 2016 to 1st January 2019 (validation set, n = 2706) were used for validation. Patients in both datasets had a minimum of 6 months of follow‐up. Starting from a set of candidate prognostic variables, the variable selection was performed by estimating the importance of predictors in a multivariable setting using survival random forests. Then, Multivariable Cox regression models were fitted on the development cohort (n = 6502) to predict EF recovery after RALP using as prognostic factors the covariates selected. Two nomograms were drawn using the regression coefficients of the pre‐ and post‐operative Cox models.
Results: Within the validation cohort, the median age of surgery and preoperative PSA were 64 and 5.9 ng/ml, respectively. 15.6% (n = 1011) , 42.1 % (n = 2727) and 42.3 % (n = 2747) patients harboured high, intermediate and low risk cap as per D Amico score. Preoperatively, 3052 (46.9 %) had no ED (SHIM ≥22), 1453 (22.4%) had mild ED and 1997 (30.7 %) had Moderate to Severe ED (SHIM ≤16).
Starting from the estimated coefficients of the pre‐ and post‐operative Cox models, two nomograms were drawn (Fig 1a and 1b). The discrimination ability of the pre‐operative model was evaluated on the development cohort using the ROC curves estimated at 3, 6, 12, and 24 months. The AUC at these time points was 0.726, 0.734, 0.754, and 0.778, respectively (Fig 2a). The AUCs of the post‐operative model at 3, 6, 12, and 24 months were 0.746, 0.756 and 0.777, and 0.801, respectively (Fig 2b).
Pre‐ and post‐operative predictive models were externally validated using a set of 2706 patients. The AUCs of the pre‐operative model at 3, 6, 12, and 24 months were 0.789, 0.772, 0.768, and 0.778, respectively. (Fig. 2c). The ROC curves of the post‐operative model at 3, 6, 12, and 24 months with AUCs of 0.807, 0.797, 0.793, and 0.798, respectively.( Fig 2d). Along with age and pre‐operative sexual function, NS technique determines the potency outcomes justifying better AUC for post‐operative model vs the pre‐operative model.
Conclusions: The above nomograms help us to predict with good accuracy the probability of potency recovery. This is a novel tool for the care giver to predict realistic expectation of potency outcomes to the patients, while preoperative and immediate post‐operative counselling.
Modelling of potency outcomes following robot assisted laparoscopic radical prostatectomy using cumulative incidence function for competing factors
S Bhat, M Covas Moschovas, S Reddy, J Noël, T Rogers, V Patel
Global robotics institute
Introduction & Objective: Potency rates reported in the literature vary from 54% to 90% at 12 months and 63% to 94% at 24 months respectively. Currently, there is no definitive way of predicting potency post RALP. We aimed to predict patients who have optimal potency outcomes following RALP using CIFs to study the covariate effects
Methods: Analysis of 7268 patents that underwent RALP in our institution by a single surgeon from 2008 to 2018. Cox regress on model used to identify covariates affecting potency Cumulative incidence functions (CIFs) were used to compare the probability and time to potency between the different grades of NS
Results: Age preoperative SHIM and the NS with potency were selected as covariates based on Cox regression model predicting potency. Patients with SHIM score >22 had a better chance of potency vs patient with SHIM <17 (OR ‐ 1 69, CI‐1.47 ‐1.79) Grade 1 NS had better potency vs Grade 4 NS (OR‐3.1, CI‐ 2. 51‐ 3. 83). Older patients >65 years had poorer rates of potency compared to patents <55 years (OR‐ 0 68, CI‐ 0.61‐ 0.75). On CIFs of the time to potency, the overall probability of achieving potency at 24 months in Grade 1 NS is 72%(95%CI‐71%‐74%) and at 36 months is 74% (95%CI 73%‐ 76%) in Grade 2 NS. The probability of achieving potency at 24 months is 48% ( 95% CI 46%‐ 50%) and at 36 months is 50.2% ( 95%CI 48.4%‐ 52.2%) Patients with no Pre‐op ED (SHIM >22) with Grade 1 NS had a probability of potency recovery at 24 months is 83% (95%CI 82.3% ‐ 85.5%) and at 36 months is 85.8% (95%CI 84.27% 87.33%). In patients less than 55 years with grade 1 NS the probability of potency recovery at 24 months is 58.5% (95%CI 82.81%‐ 87.05 %) and at 36 months is 87.5% (95%CI 85.38%‐ 89.44%)
Fig 1 shows CIFs of different subset of patients divided by age, SHIM and NS. In patients >65 years the grade2,3,4 NS curves are closer to each other compared to grade1 NS indicating grades of partial may not be as effective as compared to their younger counterparts but a grade 1 NS leads to good potency outcomes.
Conclusions: Preoperative EF age and the NS are the most influential for potency recovery in the order of significance following RALP. Young patents with good preoperative sexual function and grade 1 NS have earlier and better potency outcomes compared to counterparts. However, in older patients a full nerve preservation ( grade 1NS) yields best results but the benefit of other grades of nerve sparing is not so apparent.
Withdrawn
Increased cardiovascular risk after androgen deprivation therapies among newly diagnosed prostate cancer patients
H Hsiang‐Chen, L Jian‐Ri
Taichung Veterans General Hospital, Division of Urology, Department of Surgery, Taichung
Introduction & Objective: To investigate and compare the risk of cardiovascular disease (CVD) associated with different androgen deprivation therapies (ADT) and radical prostatectomy in newly diagnosed prostate cancer patients.
Methods: We retrospectively reviewed patients who had been newly diagnosed (ICD9‐CM code 185) with prostate cancer and receiving androgen deprivation therapies in National Health Insurance Research Database (NHIRD) from 2005 to 2009. There were comparisons of clinical characteristics with chi‐squared test and adjusted hazard ratio in survival risk between groups in different ADT.
Results: 2565 patients with newly diagnosed prostate cancer were included in the analysis with control group. 1088 patients were treated with injected hormone treatment, 286 with orchiedectomy, 812 with oral hormone treatment and 379 with radical prostatectomy. The exclusion criteria were patient under 18 year‐old or age unknown, patients with diagnosis of CVD before prostate cancer and patients without treatment or with multiple combined ADTs. Diabetes, hyperlipidemia, CVD and Charlson comorbidity index (CCI) were significantly worsen (p < 0.001) compared with control group in clinical characteristics. The risk of CVD associated with prostate cancer compared with control group was significant higher in all treatment group, injected hormone treatment with hazard ratio (HR) = 2.94 (95% Confidence Interval [CI] 2.51‐3.45, p < 0.001), orchiedectomy with HR = 3.43 (CI = 2.69‐4.36, p < 0.001), oral hormone treatment with HR = 2.87 (CI = 2.42‐3.39, p < 0.001) and radical prostatectomy with HR = 1.93 (CI = 1.5‐2.48, p < 0.001). When compared with group in radical prostatectomy, other treatment group still had higher risk in CVD associated with prostate cancer, injected hormone treatment with HR = 1.53 (CI = 1.19‐1.96, p < 0.001), orchiedectomy with HR = 1.78 (CI = 1.3‐ 2.43, p < 0.001) and oral hormone treatment with HR = 1.49 (CI = 1.15‐1.93, p < 0.001).
Conclusions: In our study, patients with newly diagnosed prostate cancer under ADT treatment or radical prostatectomy had higher risk of CVD compared with control group. However, patients treated with ADTs had higher risk of CVD compared with radical prostatectomy group.
Anal sphincter length and power are associated with early continent after radical prostatectomy
H Hsiang‐Chen, L Jian‐Ri
Taichung Veterans General Hospital, Division of Urology, Department of Surgery, Taichung
Introduction & Objective: Urinary incontinence is a common complication after radical prostatectomy (RP). Loss of the prostate support and urethral incompetence were the major causes. Pelvic floor muscles play an important role in the post RP continence. Several studies showed the association of predicted value of pelvic floor muscle or urethral length. Herein we prospectively collected post‐RP patients to understand the risk factor of post‐RP incontinence.
Methods: Between January 2019 and October 2020, patients who received robotic or laparoscopic RP were included in this study. The protocol was reviewed and approved by the Institute of Review Board. Patients were follow‐up at post‐RP 1‐month, 3‐month, 6 ‐month and 12‐month at most or continence reached. At each visit, patients were asked about the continence status. The definition of continence was pad free or a safety pad daily. Patients received digital rectal examination (DRE) to measure the functional anal sphincter length by the same surgeon. Additional anal sphincter strength was measured through manometry and scaled by the modified Oxford scale (MOS). The patient basic demography and MRI pelvic floor parameters were also recorded. Variants analysis were then performed.
Results: Total 86 patients included. The baseline were listed as table 1. The 1‐month and 3‐month continent rate was 46.51% and 81.4% respectively. Patients overall continent rate at 12‐month was 93.02%. Variants analysis showed the longer anal sphincter length increased the 1‐month and 3‐month continence (OR = 2.05, 95% CI = 1.17‐3.61, p = 0.012; OR = 2.84, 95% CI = 1.33‐6.08, p = 0.007 respectively). The anal sphincter length was cut off as 3.7cm by receiver operating characteristic (ROC) curve (figure 1).
Conclusions: Anal sphincter length by DRE could act as an predictor of post‐RP continence.
Fear of Recurrence and PSA Anxiety in Prostate Cancer
C James, O Brunckhorst, K Ahmed, P Dasgupta, O Eymech
Faculty of Life science and Medicine
Introduction & Objective: Prostate cancer (PCa) diagnosis is recognised to have profound mental health sequelae. Similarly associated mental wellbeing problems are increasingly being appreciated. Two important related problems include fear of cancer recurrence (FCR) and PSA anxiety. However, their prevalence and severity are poorly understood, and predisposing characteristics not known. Therefore, this review aims to measure the prevalence, severity, impacts and progression of FCR and PSA anxiety while identifying subgroups at risk of developing high levels.
Methods: A systematic literature search of MEDLINE, EMBASE and Psychinfo databases was conducted up to 25/02/21 by two independent reviewers. Observational studies measuring FCR and PSA anxiety levels in PCa patients and which utilised validated tools were included. Outcome measures were extracted and included prevalence of significant levels, mean scores of outcomes, and significant correlations between FCR/PSA anxiety scores and patient characteristics, as well as to other functional outcomes. Study risk of bias assessment was performed using the Joanna Briggs institute checklist, with low quality studies excluded from the review. A priori protocol was registered on the Prospero database (CRD42020225154).
Results: Post de duplication 918 results underwent screening with a final 27 included. A variety of measures were used , with the MAXPC‐FOR and MAXPC‐PSA subscale most commonly seen. Prevalence of high FCR ranged from 4‐45% (median = 16.5%) in 8 studies. Longitudinal studies found peak FCR and PSA anxiety at diagnosis with a small decrease after, with levels staying moderate to low 10 years post diagnosis. PSA Anxiety was found to be moderate with a median prevalence of 15%. Importantly, there were significant associations between both outcomes and more mental health symptoms and worse quality of life. Few studies compared between treatment groups, however where analysed active surveillance patients had higher FCR and PSA anxiety compared to radical prostatectomy. Studies were of a good quality of evidence with 10 deemed a low risk of bias and 17 a moderate risk.
Conclusions: FCR and PSA anxiety levels in prostate cancer patients are of a moderate level. However, importantly when either problem is present, they appear to be associated with poorer QOL and mental health. The only predictive characteristics are younger age and experiencing physical symptoms. Clinicians should refer patients promptly with these reported issues and their quality of life is found to be significantly worse. Further research is required to evaluate which treatment groups and other patient factors are associated with these symptoms.
Accompanying the prostate cancer patient pathway: evaluation of novel clinical decision support software
T Horn, M Henkel, F Leboutte, P Trotsenko, S Dugas, S Sutter, G Ficht, C Engesser, M Matthias, J Ebbing, H Seifert, B Stieltjes, C Wetterauer
Research and Analytic Services, University Hospital Basel
Introduction & Objective: Physicians spend more than half of their workday interacting with health information systems to care for their patients. Effective data management that provides physicians with comprehensive patient information from various information systems is required to ensure the future quality of clinical decision making.
We evaluated the impact of a novel, CE‐certified clinical decision support tool on physician's effectiveness and satisfaction in the clinical decision‐making process.
Methods: Using pre‐therapeutic prostate cancer management as a use case, we compared physician's expenditure of time, data quality, and user satisfaction in the decision‐ making process comparing the current standard with the novel solution (AI‐Pathway Companion Prostate Cancer, Siemens Healthcare GmbH, Erlangen, Germany). Ten urologists from our department conducted the diagnostic work‐up to the treatment decision for a total of 10 patients using both approaches.
Results: A significant reduction in the physician's expenditure of time for the decision making process by ‐59.9 % (p < 0,001) was found using the novel system. System usage showed a high positive effect on evaluated data quality parameters completeness (Cohen's d of 2.36), format (6.15), understandability (2.64), as well as user satisfaction (4.94).
Conclusions: The novel system demonstrated that effective data management can improve physician's effectiveness and satisfaction in the clinical decision‐making process. Further development is needed to map more complex patient pathways, such as the follow‐up treatment of prostate cancer.
Urology Questionnaire for patients referred with high PSA
F Kapasi, J Spicer
East Sussex NHS Trust
Introduction & Objective: In NHS, suspected prostate cancer patients are referred with 2‐week wait target. A thorough clinical examination and diagnostic and treatment pathways are discussed with the patient. Use of these booklets helps patients in understanding their condition and asking for relevant questions at the time of consultation and subsequently during their care pathway.
Methods:The utilisation of the information booklet distributed to patients for raised PSA and prostatic enlargement
• Every patient who is visiting the hospital with a raised PSA is given a booklet ‘Understanding PSA’ after a full consultation, clinical examination, and ‘How prostate cancer is diagnosed’ booklet is also distributed to explain the procedure with the pros and cons and different methods of prostate biopsy.
• Another booklet that is distributed is about ‘Enlarged prostate’ and it gives information about various drugs that are used for an enlarged prostate and surgical outcome and side‐effects of prostate surgery.
Results:
• 20 people took the survey, 25 questionnaires distributed. 80% response rate.
• 100% of patients found it acceptable for this material being distributed at time of initial consultation for evaluating and understanding their clinical problem.
The vast majority of patients read 75% or more of the booklets.
Did you find this information useful?
• Yes. One thing positive about prostate cancer is the level of information available. Good, clear, concise information and with an honest approach towards advising the patient.
• Yes, I found the booklet very informative and helpful for me to understand my condition.
• Yes, it was helpful – however some of the information was a little disturbing + painted a rather “black” picture.
Conclusions: Using the booklets gives patients helpful and meaningful information in streamlining their diagnosis and treatment.
Baseline preoperative Comorbidity Illness Burden and Hypertension in Predicting Overall Cause Mortality in Men with Prostate Cancer
E Choi, LM Huynh, FM El‐Khatib, R Carillo Ceja, M Towe, E Huang, FA Yafi, TE Ahlering
Introduction & Objective: The Charlson Comorbidity Index (CCI) has been utilized to predict mortality in men with prostate cancer (PCa). However, since the creation of the CCI, hypertension (HTN) has been excluded from the score. In this study, we analyze both HTN and CCI and their relationship to mortality in men with PCa.
Methods: 931 men with localized PCa were treated with robot‐assisted radical prostatectomy (RARP) between December 2009 and September 2019. A modified Charlson Comorbidity Index (mCCI) stripped of the age‐weighted domain was used to assess comorbid disease burden. HTN was assessed as a categorical variable. mCCI's and HTN's associations with Other‐Cause Mortality (OCM) and Prostate‐Cancer Specific Mortality (PCSM) were assessed with Pearson's correlation coefficients. Covariates of comorbid disease, age, OCM, and PCSM were identified using two‐tailed, Student t‐tests or Fisher's exact tests. If found to be significantly associated with OCM or PCSM, significant covariates of mCCI or HTN were adjusted with logistic regression models.
Results: HTN was positively correlated with OCM (r = 0.437, p = 0.012) while mCCI was not significantly associated with either OCM (p = 0.41) or PCSM (p = 0.32). Men with HTN were significantly older (65.0 vs 62.0, p < 0.001), had lower Sexual Health Inventory for Men (SHIM) scores (17.6 vs 20.0, p < 0.001), higher body mass index (BMI) (28.2 vs 26.6, p < 0.001), greater prostate volume (56.5 vs 52.8, p = 0.015), and lower pre‐operative total testosterone levels (348.2 vs 379.2, p = 0.006).
After adjusting for significant covariates as well as mCCI, men with HTN were 11 times more likely to die from non‐prostate cancer causes (OR: 11.4, p = 0.047). mCCI was not found to be an independent predictor of OCM (OR: 1.1, p = 0.892).
Conclusions: HTN is a key factor towards OCM for men who survive PCa and should be closely followed in this population. CCI scores do not accurately depict the burden of comorbid disease in men with PCa and may benefit from a revision to account for HTN.
Baseline preoperative Comorbidity Illness Burden and calculated Free Testosterone association with Sexual Function in Prostate Cancer
E Choi, LM Huynh, FM El‐Khatib, R Carillo Ceja, M Towe, E Huang, FA Yafi, TE Ahlering
Introduction & Objective: In men with prostate cancer (PCa), comorbid disease exacerbates poor sexual function. Our group had previously found that calculated free testosterone (cFT), rather than total testosterone (TT), was significantly associated with sexual function in men ≥60‐years of age. In this study, we seek to determine whether this effect is consistent with or independent of differing comorbid burden between younger and older men with PCa.
Methods: 733 men's baseline sexual function, cFT, and comorbidities were assessed prior to surgery, March 2010 ‐ September 2019. Patients were stratified by age (< 60 or ≥60‐years) and covariates of age, cFT, sexual function, and comorbid disease were identified using two‐tailed, Student t‐tests. Preoperative sexual function was assessed as a continuous variable via the International Index of Erectile Function (IIEF‐5). A modified Charlson Comorbidity Index (mCCI) stripped of the age‐weighted domain assessed comorbid disease burden. Hypertension (HTN), which is not included in CCI, was assessed as a separate categorical variable. Two linear regression models assessed whether cFT was predictive of sexual function after stratifying for age and significant covariates.
Results: Men over 60 years of age had significantly higher mCCI score and prostate weight, but lower cFT. Additionally, a higher proportion of these men also had high‐risk (GGG 4‐5) and high‐volume (p‐stage T3/T4) disease (Table 1).
After adjusting for covariates in linear regression, cFT (B: 0.34, 95% CI: 0.07 – 0.61, p = 0.014), mCCI (B: ‐1.84, 95% CI: ‐2.61 – ‐1.07, p < 0.001), and HTN (B: ‐2.19, 95% CI: ‐3.58 – ‐0.80, p = 0.002) were independent predictors of preoperative IIEF‐5 scores for men above the age of 60 years. GGG 4‐5 was also a significant covariate of preoperative IIEF‐5 scores for men above 60 years of age (B: ‐0.69, 95% CI: ‐1.30 – ‐0.07, p = 0.030).
Conclusions: Low cFT, increased mCCI, and HTN were independent predictors of reduced preoperative sexual function in older men (≥60‐years) with PCa as compared to men less than 60 years.
Active surveillance of prostate cancer. Persuasion strategy in doctor‐patient communication
T Osipenko, V Fedorovskaya, M Taratkin, A Morozov, E Bezrukov, G Akopyan, E Shpot, W Imo, D Enikeev
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia
Introduction & Objective: Active surveillance (AS) is regarded as the preferred treatment method of localized prostate cancer. Despite this fact, men might still wary of AS out of anxiety to live with untreated cancer. We sought to determine whether the appropriate verbal presentation of AS can influence patients to postpone radical treatment. The objective of the study was to estimate the persuasion potential of the communicative tactics supporting AS in term of decision‐making process during urological diagnostic consultations.
Methods: We enrolled 4 urologists and 30 patients with low‐risk prostate cancer: men with a Gleason score of 6 and a PSA level of less than 10 ng/mL. 30 diagnostic consultations in Russian were recorded at Sechenov University, and transcribed according to the GAT 2 transcription system. Study corpus was formed as a part of GIP Project (Germanistische Institutspartnerschaft) of the University of Hamburg and Sechenov University, supported by the DAAD (German Academic Exchange Service). Transcripts were analyzed using conversation analysis approach.
Results: Strategy verbalization is carried out by seven basic communicative tactics: stress relief (93%), AS presentation (93%), readiness for treatment method's changes (77%), appeal to foreign colleagues' experience (53%), demonstration of doctor's authority/ medical facility status (40%), demonstration of negative surgery consequences (33%), and increasing of patient status (27%). The success of the persuasion strategy is associated with the combined use of collegial and paternalistic models of doctor‐patient relationship. Patient‐centeredness is reflected in giving the patient the opportunity to choose the favorable method. Paternalism was shown 1) in a thorough AS characterization without mentioning other types of methods (53%); however, if the patient demonstrated any doubts, the oncologist was ready to describe alternative treatment options; 2) in explicit expression of a competent doctor's personal opinion which served as the decisive argument for patient's decision making (47%). Corpus analysis showed the efficiency of persuasion strategy in 80% of cases. Patient's consent to participate in AS was the criteria of strategy's efficiency.
Conclusions: The pilot study revealed a number of communicative tactics used to verbalize the strategy aimed to persuade of AS efficiency. Implementation of tactics allows the oncologist to warn and reduce cancer‐specific anxiety, avoiding overtreatment and reduction of the quality of life.
Longitudinal Urinary Bother and Symptoms following Radical Prostatectomy with Membranous Urethral Length Preservation
R Carillo Ceja, LM Huynh, H Su, E Huang, D Skarecky, TE Ahlering
Introduction & Objective: Our group previously published that maximization of membranous urethral length (MUL) during radical prostatectomy (RP) yields a significant improvement in continence recovery rates following RP. The present study seeks to further investigate the role of MUL preservation in improving urinary bother (QoL), American Urological Association Symptom Score (AUASS), and continence status following RP.
Methods: A retrospective analysis was conducted on RP patients from November 2004 to November 2018. Inclusion criteria consisted of RP as primary intervention, pad‐free status at time of surgery, minimum 2‐year follow‐up, and outcome data availability at pre‐op, 3 months, and one other time point. Primary outcomes were urinary symptoms measured by AUASS and QoL. Secondary outcomes were continence rates through pad‐free status. Age‐stratification was conducted to investigate its confounding effect. While primary analysis used t‐test and chi‐squared, ad‐hoc paired difference analysis was also performed.
Results: No differences in mean AUASS and QoL were observed for the overall sample. However, mean differences were greater for patients older than 65 years during paired difference analysis after the technique change (Figure 1A‐B). Sample continence rates were reported as 34%, 72%, and 92% prior to the technique change and increased to 52% (p < 0.001), 95% (p < 0.001), and 96% (p = 0.011) at 30‐day, 9‐month and greater than 15‐month follow‐up points, respectively (Table 1).
Conclusions: This technique change significantly improved QoL and AUASS for those over the age of 65, those at highest risk for adverse symptoms as supported by their higher pre‐ and post‐operative mean AUASS and QoL scores. Men under 65 did not show this substantial benefit. Time to continence improved for all patients. The results support the implementation of MUL maximization. However, further trials are encouraged.
Real time urethral and ureteral assessment during radical cystectomy using ex vivo optical imaging
F Esperto, F Prata, A Civitella, P Tuzzolo, V Crimi, L Romei, L Cacciatore, F Tedesco, C Taffon, A Crescenzi, R Scarpa, R Papalia
Dept. of Urology, Campus Biomedico University of Rome, Rome, Italy
Introduction & Objective: Histopathological examination of urethral and ureteral specimens using hematoxylin and eosin (H&E) is the gold standard for cancer detection. It is time‐consuming and does not provide a rapid evaluation of fresh tissue. Novel optical technologies are rapidly evolving in the fiedl of evaluation of biologic tissue specimens. Fluorescent confocal microscopy (FCM) is an ex vivo technique that has been widely used for ex vivo imaging in research studies, but there is limited evidence on the feasibility of its use in routine surgical practice. The aim of our study was to assess the feasibility and the reproducibility of FCM real‐time assessment of urethral and ureteral margins during open radical cystectomy (ORC)
Methods: Ethical Committee approval has been obtained. This is a prospective, comparative study evaluating FCM, frozen sections and H&E for urethral and ureteral tissues interpretation during ORC. From September 2020 to December 2020, 15 urethral and 29 ureteral surgical specimens from 15 consecutive patients who underwent radical cystectomy for bladder cancer (one with solitary kidney) were collected at our institution. Each specimen was intraoperatively stained with acridine orange for histopathological analysis using FCM (VivaScope; MAVIG, Munich, Germany), analysed as frozen section and sent for traditional H&E examination. One expert uro‐pathologist analysed all specimens to assess cancer infiltration. Diagnostic accuracy, sensitivity and specificity of FCM and frozen sections were assessed comparing with traditional H&E examination diagnoses for urethral and ureteral margins respectively
Results: FCM (figure 1) and frozen section specimens analysis showed the same sensitivity, specificity and diagnostic accuracy for both ureteral and urethral margins. A 100% sensitivity, specificity and diagnostic accuracy was showed for urethral margins; 87.5% sensitivity, 80.9% specificity and 82.7% diagnostic accuracy for ureteral margins when compared to H&E final examination diagnoses
Conclusions: FCM resulted to be a safe, feasible and reproducible method for the intraoperative assessment of urethral and ureteral surgical margins during ORC. Unlike frozen sections, FCM can generate optical sections of biologicspecimens allowing real‐time microscopic evaluation of fresh unfixed tissue, requiring minimal tissue preparation and preserving specimens from any damage, distortion or loss
Moderated Poster Session 31: Clinical Oncology II
Pelvic nodal spread for metastatic melanoma: technique and benefits of robotic approach
BC Rocco, M Sighinolfi, L Sarchi, S Assumma, G Bozzini, A Cassani, E Morini, F Turri, C De Carne, S Micali
Azienda ospedaliero‐universitaria di Modena e Reggio Emilia, Modena, Italy
Introduction & Objective: Nodal metastasis negatively affect melanoma prognosis. Despite the absence of prospective randomized studies surgical dissection is the gold standard. In case of positive sentinel biopsy, the earlier intervention is performed the higher is OS. In high‐risk patients, a simultaneous approach to inguinal and pelvic region can be recommended. We report a case series of patients with inferior limb melanoma elected to pelvic nodal dissection (PND). The aim is to report tips and tricks of Robotic PND, periop and oncological outcomes.
Methods: 4 patients with inferior limb melanoma were elected to robotic PND. Mean age 71 yr. (2 males, 2 females), 2 patients were ASA II, 2 ASA III (oral anticoagulants drugs). 2 had a prior inguinal nodal dissection, the others had a concomitant inguinal open dissection before the pelvic approach. PND is performed homolateral to the melanoma lesion and included external iliac, internal iliac, common iliac and obturator nodes. Trocar placement is the one used for robotic pelvic surgery, pelvic CT scan aids to pre‐plan the intervention according to the burden and site of the spread. The procedure starts dissecting the peritoneum over the ureter and proceeds caudally splitting it over the common and external iliac artery. The exposure of the Marseille's triangle allows a better mobilization of nodes, in the case of melanomatous location, often appear of bluish color and weak consistency. A soft and gentle nodes handling is suggested to reduce manipulation and prevent intraop injury. In case of bulky disease with strict proximity to vessels mimicking infiltration energy‐free and blunt gentle dissection makes the debridement affordable.
Results: Mean console time was 40 (± 25) min. Mean number of retrieved nodes was 13,2 (SD 5,6). Mean hospital stay was 7.7 (SD 7.8). None of the patients had a Clavien >1 related to PND or to inguinal open approach. Pelvic nodal metastasis was found in 2 patients. 3 had an adjuvant treatment with nivolumab, 1 dabrafenib; all treatments were started immediately after hospital leave. At 12 months follow‐up 3 patients were progression free, 1 has a metastatic disease (liver).
Conclusions: Robotic approach to PND for melanoma of the low leg may represent a novel indication for urologist. Robotics may be a key point to approach to nodal disease for melanoma patients: the precise dissection enables the management of bulky diseases, reduced invasiveness and LOS allows a fast recovery and eligibility to adjuvant treatment, possibly enhancing overall oncological outcomes.
Comparative Evaluation of Oncologic Outcomes According to the Anatomic Location of Surgical Margin Positivity After Partial Nephrectomy
A Beksac, S Kim, U Carbonara, M Meagher, A Tafuri, M Abou Zeinab, L Lenfant, A Antonelli, R Autorino, IH Derweesh, J Kaouk
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
Introduction & Objective: We sought to assess if the anatomical location of positive surgical margins (PSM) can affect the oncological outcomes following partial nephrectomy (PN).
Methods: From a multi‐institutional dataset, we performed a retrospective analysis of 115 patients who were found to have PSM following PN. Surgeries were performed between January 2010 to May 2020. Patients with benign pathology, less than 6 months follow up, baseline metastatic disease, bilateral tumors, familial renal cell carcinoma, and pathological node positive disease were excluded from analysis. Patients with PSM were stratified into two groups according to the anatomical location (parenchymal invasion, sinus fat invasion). Due to uneven sample size a 1:2 matched pair analysis was performed (by cT stage) to limit confounding effect of stage on recurrence. Demographics, clinical and tumor characteristics, and poncological outcomes were compared using Chi‐square, Fisher's exact, Mann‐Whitney U, and student's t tests. Kaplan‐Meier analysis performed to analyze recurrence free survival (RFS).
Results: Overall 84 patients were included in analysis (56 parenchymal vs. 28 sinus). Median follow‐up was 25 months (IQR 11‐41). Baseline characteristics were comparable between the two groups. Pathological tumor size was comparable. In the parenchymal group, more patients had multifocal PSM, whereas more patients had pT3a upstaging in the sinus group. Local recurrence rate was higher in the sinus group (17.9% vs. 10.9%, p = 0.377), however this association did not reach statistical significance. Distant recurrence rate was comparable as well (5.5% vs. 7.1%, p = 0.76). Kaplan‐Meier analysis did not show any difference in terms of RFS (p = 0.68)
Conclusions: At 25 months follow up, the location of positive surgical margin did not alter distance recurrence rates following PN.
Withdrawn
Perioperative and short‐term functional outcomes of robot‐assisted versus open partial nephrectomy : a single‐center retrospective study
K Takahara, K Fukaya, T Nukaya, M Takenaka, K Zennami, M Ichino, H Sasaki, M Sumitomo, R Shiroki
Introduction & Objective: This study aimed to compare the perioperative and short‐term functional outcomes between robot‐assisted partial nephrectomy (RAPN) and open partial nephrectomy (OPN) in Japanese patients.
Methods: We retrospectively analyzed 242 patients who underwent either RAPN or OPN between 2007 and 2017 at our hospital. Propensity score matching was carried out between the two groups at a ratio of 1:1. Perioperative outcomes and postoperative estimated glomerular filtration rates (eGFR) were compared at one and three years of follow‐up.
Results: After propensity score matching, we evaluated 39 patients from each group. The ischemia duration of the RAPN group was significantly shorter than that of the OPN group (18 vs. 24, p < 0.001). Moreover, the estimated blood loss (EBL) was significantly lower in the RAPN group than in the OPN group (50 vs. 174, p < 0.001). However, there were no significant differences in the postoperative eGFR between the two groups at one or three years of follow‐up (OPN 54.8 vs. RAPN 61.2, p = 0.109, and OPN 54.8 vs. RAPN 55.5, p = 0.262, respectively).
Conclusions: RAPN resulted in shorter ischemia durations and lower rates of EBL than did OPN; however, no differences in short‐term renal function were observed between RAPN and OPN in our propensity‐score matched Japanese cohort.
Robotic versus laparoscopic living donor nephrectomy: A prospective study
M Thai, Q Chau, L Dinh, K Hoang, K Thai, D Vu, T Tran, X Ngo, H Tiong, T Nguyen
University of Medicine and Pharmacy at Ho Chi Minh City, Cho Ray hospital
Introduction & Objective: Robotic‐assisted laparoscopic donor nephrectomy (RALDN) reportedly facilitate better hilar dissection but had associated concerns regarding longer graft retrieval and ischemia times. The aim of this study is to assess safety and efficacy of an initially introduced RALDN when compared to the routine retroperitoneal laparoscopic living donor nephrectomy (RLLDN) at a single institution transplant program.
Methods: Data were collected prospectively from 64 consecutive living kidney donors (12 for RALDN subgroup and 52 RLLDN subgroup) at our hospital from May 2018 to August 2019. All donors were approved by our Government Hospital Renal Transplantation Council according to Amsterdam Guidelines. Patient demographics, radiology findings, surgery results and complications were recorded. Primary endpoints were peri‐operative parameters, postoperative outcomes and complications. The surgeons were experienced retroperitoneoscopic using three ports and robotic surgeons using the Da Vinci Si System with three arm robotic ports.
Results: For the entire group, mean age ± SD was 51.7 ± 8.9 years, and 58% were females. Mean BMI was 22.5 ± 2.3 (15.6 ‐ 27.3). There were 54 (84%) left kidneys. Preoperatively, there were no significant differences between the two patient groups including age, gender, BMI, kidney side, hilar anatomy and ASA status. For perioperative outcomes, there was no significant differences (P > 0.05) comparing RALDN and RLLDN respectively for warm ischemic time (4.75 ± 1.54vs. 4.75 ± 1.38 minutes), operative time (233 ± 46 vs. 216 ± 41 minutes), hemoglobin (g/L) drop (9 ± 5.6 vs. 8.6 ± 7.2), postoperative complications (All Clavien) (16.7% vs. 9.6%), the donor blood creatinine at one month (1.1 ± 0.2 vs. 1.2 ± 0.3 mg/dL), and the recipient blood creatinine at one month (1.2 ± 0.3 vs. 1.4 ± 0.4 mg/dL). There were no open conversions or delayed graft functions in both groups.
Conclusions: This study showed that RALDN can be safely introduced into living donor program experienced in laparoscopic donor nephrectomy. This allows the program to utilize the operative advantages including better optics and instrument dexterity of the platform in all or selected cases.
Animal model assessment of new ureteral biodegradable Mitomycin‐eluting stent to adjuvant therapy in Upper tract urothelial carcinoma. Safety study
F Soria, JE de La Cruz, M Soto, S Aznar, J Cenis Anadon, J Caballero Romeu, A Serrano, F Sanchez Margallo
Results: Mitomycin C is fully released during the first 6 hours after ureteral stent placement in the animal model (< 10 mg/L). There is no difference between baseline and urinary pH values within the first 42 hours. The ureteral stents were safety and completely degraded between 4 and 6 weeks and no obstructive fragments were evident at weekly follow‐ups.
miR‐223‐5p targeting ERG inhibits the biological behavior of prostate cancer
Y Gao, Y Wei
Introduction & Objective: Accumulating studies foundmicroRNAs (miRNAs) possess suppressive effects and/or oncogenic functions in different types of human cancers. Recent emerging evidences support a novel concept that the lagging strand of miRNA duplex involves in the origination and development of certain cancers. Ectopic expression of miR‐223‐5p, the lagging strand of miR‐223 duplex, has been reported acting as anti‐tumor miRNA in many cancers. How miR‐223‐5p influencing prostate cancer (PCa) remains obscure and worth of experimental investigation.
Methods: The expressions of miR‐223‐5p and ERG in common PCa cell lines (DU145, PC3 and LNCaP) were detected and compared to RWPE‐1, respectively. Next, luciferase reporter assay was performed to verify whether miR‐223‐5p could specifically target and regulate ERG. Further discovery ERG's role in the PCa oncogenesis was also conducted by up or down regulating miR‐223‐3p expression.
Results: miR‐223‐5p was significantly down‐regulated in DU145 when compared to RWPE‐1, while it was only up‐regulated in LNCaP. Similarly, ERG expression remarkably decreased in both PC‐3 and DU145 than that in RWPE‐1, but significantly increasing in LNCaP. Luciferase assay demonstrated slightly decreased ERG expression after miR‐223‐5p‐mimics but significantly increased ERG expression after miR‐223‐5p‐inhibtor. Using gene interference, we further confirmed that both ERG mRNA and protein expressions were decreased in all PCa lines transfected ERG siRNA, but increasing in both DU145 and LNCaP cells with miR‐223‐5p antisense oligonucleotides. MTT assay, Transwell invasion and migration assay supported the function of ERG in PCa oncogenesis.
Conclusions: We revealed tumor suppressive abilities of miR‐223‐5p in PCa by targeting ERG gene. It could serve as a fundamental supplement and extension of our previous study about miR‐223‐3p in PCa, revealing the coordinative regulation between miR‐223‐5p and miR‐223‐3p in PCa cell biological behaviors. Exploration of miR‐233‐duplex orientated pathway networks may help us develop novel potential therapeutic options for PCa.
The myth of the “July Effect” in urology: a study of oncology and BPH surgeries in the ACS‐NSQIP database
EB Garden, KT Ravivarapu, O Omidele, AC Small, O Al‐Alao, MA Palese
Icahn School of Medicine at Mount Sinai
Introduction & Objective: Some theorize that patients receiving care early in the academic year are at increased risk of complications due to the recent transition of trainees to their new positions; this phenomenon is termed the “July Effect.” Here, we evaluate for the presence of the “July Effect” in urology among common oncology and benign prostatic hyperplasia (BPH) surgeries.
Methods: The American College of Surgeons National Surgical Quality Improvement Program (ACS‐NSQIP) database was used to identify all patients who underwent oncology (i.e. radical and partial nephrectomy, radical cystectomy, radical prostatectomy) and BPH surgery (i.e. transurethral resection of the prostate, Greenlight laser vaporization, holmium laser enucleation of the prostate) from 2015‐2019. Patients were grouped by admission quarter 1 (Q1, July–September) and quarter 4 (Q4, April–June); those admitted during Q2 or Q3, and those with missing data were excluded. Baseline characteristics, operative data and postoperative outcomes were compared between groups. Comorbidity burden was estimated using a modified Charlson Comorbidity Index (mCCI) score. Multivariable regression assessed for predictors of operative time, length of stay (LOS), 30‐day Clavien‐Dindo complications and readmission.
Results: 29,466 patients who underwent BPH procedures (32.5%) and 61,030 who underwent oncology procedures (67.5%) were studied. Compared to Q4, Q1 BPH patients were older with higher mCCI score. Q1 oncology patients were older and more commonly white with similar mCCI scores. Group comparisons revealed no differences in operative time, complications, or readmissions between patients admitted during Q1 or Q4 (all p > 0.05) (Table 1). While BPH patients had similar LOS in Q1 and Q4, Q4 oncology patients had slightly shorter LOS than in Q1 (3.05 vs. 3.17 days, p = 0.020). On regression, Q1 admission conferred no risk of prolonged operation, complications, or readmission for either group, but did correlate with longer LOS (+0.12 days [95% CI: 0.02, 0.22], p = 0.017).
Conclusions: We did not observe a “July Effect” among common urologic surgeries. Patients undergoing surgery in the Q1 are not subjected to increased risk of postoperative complications or readmissions. Oncology patients may have a slightly prolonged LOS.
Bilateral Renal Cell Carcinoma: Neoadjuvant Tyrosine Kinase Inhibitor helps preserve Renal function prior to Robotic Partial Nephrectomy
J Zeng, AA Lwin, A Wong, K Batai, BR Lee
University of Arizona College of Medicine
Introduction & Objective: Tyrosine kinase inhibitors (TKI) have the theoretical advantage of downsizing renal cell carcinoma (RCC) to facilitate nephron‐sparing surgery while preserving renal function with concomitant oncologic efficacy. In this study, our objective was to report oncological and functional outcomes of patients with bilateral renal masses in the contemporary era of TKIs.
Methods: After Institutional Review Board approval, 521 RCC patients were treated at the Department of Urology at the University of Arizona between 2010 – 2020. Patients who presented with bilateral renal masses were reviewed retrospectively. Surgical approach, percent decrease in size following TKI, change in renal function, time interval between surgeries, and recurrence rates were reviewed.
Results: A subset of 35 renal units were included in the analysis. The TKI cohort (n = 6) between 2017‐2019, was compared to the naïve treatment cohort (n = 29), during 2010 ‐ 2019. In TKI group, 66.7% of tumors were downsized sufficiently to allow partial nephrectomy. Average tumor size was 6.18 cm and 5.55 cm in TKI and no‐TKI group, respectively. In TKI group, there was an average of 49.2% decrease in tumor size. Compared to 18.6% creatinine rise postoperatively in no‐TKI group, patients with TKI use had a greater rise in creatinine, of 19.7%. However, no statistical difference was noted (p = 0.93). Both groups have no recurrence at the most recent follow‐up, with median of 22 months (1‐91) and 10 months (1‐36).
Conclusions: TKI plays a greater role in preserving renal function, GFR, while maintaining oncological efficacy. Downsizing of tumors with TKI by 49% allows nephron‐sparing surgery to be performed to minimize renal failure and risk of dialysis. Prospective studies are required to validate the oncologic efficacy and persistent benefit.
Neoadjuvant chemotherapy combined with immunotherapy followed by radical cystectomy
C Chang, C Lin, C Huang, K Chen, P Hsiao, C Tsai, Y Yang
Introduction & Objective: RC alone for MIBC is insufficient and it is associated with a high rate of cancer‐specific mortality. Neoadjuvant chemotherapy (NAC) in muscle‐invasive bladder cancer (MIBC) improves survival at radical cystectomy (RC). Both NAC and Immunotherapy gives benefit to response rate in studies, combined use of NAC and immunotherapy maybe has synergistic effect in response rate and survival. We share our experience of chemotherapy combined with immunotherapy followed by radical cystectomy.
Methods: Patients with MIBC eligible for neoadjuvant chemotherapy and planned for RC between January 2017 and March 2020 was included. Patient characteristics, Clinical course, drugs, and pathologic response were evaluated. Meanwhile the safety of combination of chemotherapy and immunotherapy in patients with MIBC prior to RC will be mentioned.
Results: 12 patients have been enrolled. All of the NAC was Gemcitabine and platinum‐based drugs. six patients received the combination of Durvalumab, five Nivolumab, and one Pembrolizumab. Pathologic downstage was observed in 9(75%) patients, and 6 of them was ypT0N0. However, 3 patients had no response to the neoadjuvant therapy according to the pathologic results. The medium fallow time was 157 days. And the average time from the end of neoadjuvant therapy to surgery was 24.4 days. The combination has not resulted in any add toxicity or mortality so far.
Conclusions: Neoadjuvant chemotherapy combined with immunotherapy is safe and effective treatment for MIBC according to the current study. We need more time and data to confirm whether this therapy gives more benefit to the overall survival or progression free survival for the patients. Further enrollment and evaluation is ongoing.
Real‐life practice of enbloc resection of bladder cancer among IEA and ESUT members: a survey
G bonfante, M Sighinolfi, T Calcagnile, M Ticonosco, L Sarchi, A Cassani, S Assumma, S Puliatti, G Bozzini, A gozen, J Rassweiler, BC Rocco, S Micali
Azienda ospedaliero‐universitaria di Modena e Reggio Emilia, Modena, Italy
Introduction & Objective: Enbloc resection (ERBT) is considered an oncologically noninferior technique for trans‐urethral resection of bladder cancer. ERBT seems to provide a properly oriented specimen for an adequate assessment of muscle layer and lateral margins status. Recently, an International Collaborative Consensus statement on ERBT has been drafted, to standardize various technical aspects and indications. The aim of the study is to assess with a survey the use of ERBT in the daily surgical practice.
Methods: We developed an 18‐items survey investigating subjective opinions on the following issues: feasibility, indications, personal experience and techniques, possible advantages‐disadvantages, complications and pathological issues, assessment of histological specimens. The survey was designed by 2 urologists according to most of the Cherries Guidelines, uploaded on Google Form and distributed in March 2020 via e‐mail to IEA and ESUT members. Data were collected on an Excel database and a descriptive analysis was performed.
Results: 118 urologists completed the survey. Age between 30 and 49 yr. with >10 yr. of clinical practice. 66% started performing lower urinary tract endoscopy more than 10 years ago, 54% are working in high‐volume hospitals (≥200 TURBT/year). ERBT is performed by 81% of surgeons, while 19% consider it less safe than TURBT for the higher rate of bleeding loss and bladder perforation. All the urologists agree to carry out ERBT in case of exophytic lesions, 60% use it for flat lesions too. 2 cm is considered the ideal cut‐off for ERBT for 40% of surveyed urologists, 3 cm is the ideal cut‐off for 41% whereas 19% consider ERBT feasible also for lesions ≥3 cm. Tumour extraction is made by flushing (73%), grasper (43%), endobag (11%) and resectoscope loop (9%). The major advantages for 53% are the higher rate of muscle layer presence and the possibility of more exhaustive pathological report. 51% consider the presence of lateral margins relevant, in 39% of the cases the pathologist does not provide data on lateral mucosa status. 41% of urologists have started ERBT from ≤3 years, only 1 managed major complication (Clavien‐Dindo ≥3). The source of energy is monopolar current in 87%, bipolar current (40%), only 38% use laser energy (Thulium‐YAG laser).
Conclusions: The survey showed that ERBT penetration in endourological community is high and the procedure is considered feasible by most of the surveyed urologists. Guidance from guidelines and consensus statements ‐ together with an appropriate training – would allow ERBT and its indications to further spread.
Intravesical hyperthermic chemotherapy with Mitomycin C in intermediate‐high risk non muscle invasive bladder cancer: Our early results
S Pethe, R Nayyar, P Singh, B Nayak, A Seth
AIIMS
Introduction & Objective: Hyperthermic intravesical chemotherapy (HIVEC) is an upcoming treatment option with limited data regarding its efficacy as first line option against standard intravesical Mitomycin C or BCG. We present our early experience and results with use of HIVEC with mitomycin‐C (MMC) for patients with intermediate and high risk non‐muscle invasive bladder cancer (NMIBC).
Methods: From June 2018 to December 2020, 35 newly diagnosed intermediate and high risk cases of NMIBC, received adjuvant HIVEC treatment with Mitomycin C using Combat BRS™ system. All cases were diagnosed after restage resection of tumor and had also received standard peri‐operative instillation of Mitomycin C. The treatment regimen included an induction cycle of once a week session for six weeks and a subsequent maintenance regimen of once a month session for 12 months. Each session consisted of intravesical instillation of a solution of 40 mg MMC in 40 ml distilled water and continuously recirculated at temperature of 43.0°C, for a contact time 1 hour. Patients were followed up with check cystoscopy every 3 months.
Results: 28 patients had intermediate risk while 7 patients had high risk disease. All cases tolerated the treatment sessions well and have completed induction phase. 24 patients have completed 1 year maintenance regimen as well. Mean follow‐up is 19.7 months (Range‐ 3 to 30 months). 4 patients with intermediate risk disease (14%) and 2 with high risk disease (28%) had tumor recurrence at mean follow up of 9 months and 5 months respectively. 9 out of 35 patients continued to show a non‐healing ulcerative lesion at resection sites which were histologically necrosis only. None of the patients in the intermediate arm had disease progression. 10 cases developed dysuria, suprapubic pain or febrile UTI. All were Clavien Dindo 1 adverse events.
Conclusions: The recirculant hyperthermic MMC using Combat's HIVEC system is safe and effective and is capable of achieving good success rates in adjuvant settings. Long term follow up is essential to determine the efficacy of this treatment modality. Non‐healing ulcers during check cystoscopy is a clinical concern with such therapy and needs to be addressed with focussed studies.
Trends in 30‐Day Complications in Robotic‐Assisted Laparoscopic Prostatectomy (RALP)
S Marthi, DW Sobel, TK O'Rourke, C Tucci, G Pareek
Warren Alpert Medical School of Brown University
Introduction & Objective: There has been a sharp increase in the number of urologic robotic‐assisted procedures in recent years, but few studies have examined longitudinal trends in complication rates. This study assesses whether national 30‐day complication rates for robotic‐assisted laparoscopic prostatectomy (RALP) have decreased as surgeons perform higher volumes of these procedures.
Methods: We identified 40,993 patients who underwent RALP in the NSQIP database from 2012‐2017. One‐way ANOVAs were performed for each patient characteristic and complication to evaluate any population variation between years. We conducted binary regressions to evaluate the contribution of year as predictor of each outcome. Multivariate regressions were performed to evaluate whether significant trends could be better explained by demographics, comorbidities, or increases in rates of pelvic lymph node dissection (PLND) during RALP.
Results: Population characteristics by year are summarized in Table 1. Univariate analyses revealed that over time organ infection (OR 1.17, 95% CI 1.09‐1.27 [p < .001]) and urinary tract infection (UTI) (OR 1.11, 95% CI 1.06‐1.16 [p < .001]) rates increased while length of stay (p = .001) and operative time (p < .001) decreased. Year of surgery remained a significant predictor of organ infection and UTI when assessed alongside PLND, comorbidity, and demographics on multivariate analysis. Other factors, including weight and PLND, were found to help predict both organ infection and UTI (Table 2).
Conclusions: While length of stay and operative time have decreased as the robotic experience has matured, the risk of post‐operative infections following RALP have paradoxically increased in recent years. Further study into recent changes in robotic surgery is needed to better understand the reasons for and mechanisms behind these trends.
Perioperative Serum Cytokine Levels in Patients Treated with Robot‐Assisted Laparoscopic Partial Nephrectomy
A Koizumi, S Narita, S Kashima, R Yamamoto, T Nara, M Huang, K Numakura, M Saito, S Satoh, T Habuchi
Department of Urology Akita University School of Medicine
Introduction & Objective: We assessed the impact of the perioperative serum levels of six inflammatory cytokines on clinical outcomes in patients with renal cell carcinoma (RCC) treated with robot‐assisted laparoscopic partial nephrectomy (RAPN).
Methods: We included 138 patients who underwent RAPN for localized RCC between 2013 and 2020. We measured six inflammatory cytokines (interleukin [IL]‐10, IL‐6, IL‐8, IL‐1b, IL‐12p70, and tumor necrosis factor [TNF]‐a) using the BD Cytometric Bead Array Human Inflammatory Kit (BD, Tokyo, Japan), along with white blood cell count (WBC) and C‐reactive protein (CRP) level. Measurements were performed before the operation (pre‐OP), immediately after the operation (post‐OP), and at postoperative Day 1 (POD1). We statistically investigated the relationship between clinical outcomes and the levels of inflammatory mediators.
Results: The median age and body mass index were 64 years and 24. 5 kg/m2, respectively. The median tumor diameter was 30 mm; 116 (84.1%) and 22 (15.9%) patients had cT1a and cT1b disease, respectively. The median R.E.N.A.L. nephrometry score was 7. The levels of WBC, CRP, and IL‐10 at post‐OP and POD1 were significantly higher than those measured at pre‐OP (each, p < 0.05). The levels of IL‐6 and IL‐8 at post‐OP were significantly higher than those detected at pre‐OP (each, p < 0.05). The univariate analysis showed that the surgical approach, operative time, R.E.N.A.L. nephrometry score, and clinical stage were significantly associated with higher levels of IL‐6 and IL‐10 at POD1. The multivariate analysis showed that the retroperitoneal approach was an independent risk factor for a high IL‐10 level at POD1 (p = 0.031). Regarding the impact of cytokine levels on postoperative renal function, the patients with worse renal function had a significantly higher IL‐6 level at POD1 than those with better renal function (53. 3 pg/mL vs. 40. 4 pg/mL, respectively; p = 0.038). The multivariate analysis showed that a high IL‐6 level at POD1 was an independent risk factor for deterioration of renal function at 1 month (p = 0.039). There were no relationships between serum cytokine levels and oncological outcomes.
Conclusions: In RAPN, the retroperitoneal approach was linked to a risk for increased postoperative serum levels of inflammatory cytokines. The serum level of IL‐6 at POD1 was associated with postoperative renal deterioration in patients with RCC treated with RAPN.
Renal biopsies performed before versus during ablation of T1 renal tumors: implications for prevention of overtreatment and follow‐up
C Widdershoven, B Aarts, PJ Zondervan, E Klompenhouwer, OM van Delden, W Prevoo, A Montauban van Swijndregt, M Henderickx, J van Moorselaar, A Bex, B Lagerveld
Introduction & Objective: To compare the effect of different strategies in renal mass biopsy (RMB) performed either before or during the ablation procedure on the rate of malignant, benign or non‐diagnostic tumors.
Methods: A retrospective multi‐center study was conducted in patients with a T1 renal mass treated with cryo‐, radio frequency‐ or microwave ablation between January 2007 and July 2019 in three hospitals of the Kidney Cancer Network Amsterdam. In addition, a search in the PALGA pathology database was performed to identify patients that were planned for ablation but were not treated because of a benign or non‐diagnostic pathology result. Patient and tumor characteristics and information on malignant, benign, and non‐diagnostic biopsy results were collected to establish rates of overtreatment and number of ablations avoided in case of benign or non‐diagnostic histology. The Chi‐squared test was used to analyze difference between the groups.
Results: RMB was performed in 714 patients, of whom 231 patients received biopsy before planned ablation, and 483 patients at the time of ablation. Pathology results before ablation were malignant in 63% (145/231), benign in 20% (46/231) and non‐diagnostic in 17% (40/231). Pathology results at the time of ablation were malignant in 67.5% (326/483), benign in 16.8% (81/483) and non‐diagnostic in 15.7% (76/483), leading to a total of 32.5% of ablation of benign or non‐diagnostic lesions. Of the patients with a benign biopsy obtained before ablation, 80.4% (37/46) chose not to undergo ablation. Patients with inconclusive biopsy before planned ablation chose an informed individualized approach including ablation, repeated biopsy, or no intervention in 56%, 34% and 10%.
Conclusions: Renal biopsy performed before the ablation procedure leads to a higher diagnostic rate and a lower treatment rate of benign tumors as compared to performing a biopsy during the ablation procedure. It is therefore recommended to perform a biopsy before the ablation as it reduces overtreatment and increases the diagnostic yield.
Withdrawn
Withdrawn
Withdrawn
The position of urine cytology within the diagnostic process for upper tract urothelial carcinoma
N Hendriks, GM Kamphuis, HP Beerlage, BM Schout, RC Pelger, KS Doherty, J Baard
Amsterdam UMC
Introduction & Objective: The value of cytology within the diagnostic process for patients with upper tract urothelial carcinoma (UTUC) seems limited. Until 2017, urine cytology was adopted in the EAU guidelines on UTUC as a strong recommendation in the diagnostic process but has been removed in the subsequent editions. However, cytology is still mentioned in the risk stratification upon which choice of treatment should be based. We evaluated the value of cytology in the diagnostic process in our cohort of patients treated for UTUC.
Methods: We evaluated the cytology samples of 174 adult patients with histopathological confirmed non‐metastatic UTUC (2010‐2020) and compared them with the biopsy specimen (patients treated by either kidney sparing surgery or radical nephroureterectomy (RNU)) and the RNU specimen.
Results: Bladder cytology was suspect for malignancy in 48.9% and in 55.4% for selective cytology. In the majority of patients a low grade bladder cytology outcome was confirmed by a biopsy specimen (87.5%). In case of high grade bladder cytology, this percentage was only 50% which is similar toselective cytology. Selective cytology was more accurate in case of low grade cytology (91.7%) when compared to the biopsy specimen. When no malignant cells were found in bladder or selective cytology, biopsies turned out to be high grade in respectively 56.5% and 12.0% (figure 1). Results of cytology grade in relation to grade in RNU specimen (figure 2) were not considerably better when compared to biopsies (figure 1).
When histopathological examination of RNU specimen was compared to biopsies 27.8% of low grade biopsies proved to be high grade in the RNU specimen.
Conclusions: The value of urine cytology within the diagnostic process of UTUC is limited. Sensitivity is low, as approximately half of all histopathologic confirmed UTUC is negative for malignancy in bladder and selective cytology. With respect to tumor grading, cytology results do not correspond well with either biopsies nor RNU specimen results.
Ablative Therapies versus Partial Nephrectomy for Small Renal Masses – A systematic review and meta‐analysis of observational studies
V Vinson, A Abul, F Osman, H Ng, K Wang, Y Yuan, J Cartledge, T Wah
School of Medicine, Faculty of Medicine and Health, University of Leeds, Leeds Department of Targeted Intervention, Division of Surgery and Interventional Science, University College London, London
Introduction & Objective: Ablative therapy (AT) has shown similar oncological durability to partial nephrectomy (PN) when managing small renal masses (SRMs), however, high‐quality primary studies and systematic reviews are limited. This review aims to compare oncological outcomes in patients undergoing AT vs PN for solitary T1a or T1b SRMs.
Methods: Medline, EMBASE, Cochrane CENTRAL and conference proceedings were searched on the 15th July 2020 for comparative studies respective to our research question. The Cochrane RoB 2.0, ROBINS‐I tool and the GRADE approach were used to assess any risk of biases and certainty of evidence in the included studies. The review is registered on PROSPERO (CRD42020199099).
Results: 1,748 records were retrieved. 32 observational studies and 1 RCT integrating 74,946 patients were included. Serious confounding bias were found in included studies as patients undergoing AT patients are significantly older than PN patients (MD 5.70, 95% CI 3.83‐ 7.58). In T1a patients, AT patients have significantly worse overall survival (HR 1.64, 95% CI 1.39‐1.95). Local recurrence‐free survival is similar with PN in patients with longer than five‐years follow‐up (HR 1.54, 95%CI 0.88‐2.71) (Table). AT Patients also have similar cancer‐specific survival (CSS), metastatic‐free, disease‐free survival; significantly fewer post‐operative complications (RR 0.72, 95%CI 0.55‐0.94; Figure) and smaller decline in estimated glomerular filtration rate post‐operatively (MD: ‐7.42, 95%CI ‐13.1‐ ‐1.70) than those undergoing PN. In T1b patients, while CSS was found to be similar between the two groups of treatments, evidence are contradicting for other oncological outcomes.
Conclusions: In T1a patients, long‐term oncological durability is similar in AT and PN. AT patients have significantly fewer complications and better renal function preservation than those undergoing PN. Overall survival is better following PN compared to AT. post‐operatively. This review is however limited by poor certainty of evidence; long‐term high‐quality studies are needed to confirm the potential benefits of AT, especially in T1b patients.
Leveraging Natural Language Processing to Identify Incidental Renal Masses
J James, A Rai, L Richstone
The Smith Institute for Urology
Introduction & Objective: With the rise in the usage of radiological imaging, there has been an increase in incidental findings of renal masses. However, often the urologist is rather inconsistently referred these cases depending on the ordering provider and location of the imaging. Natural language processing is the field of computer science, linguistics and artificial intelligence that enables the use of algorithms to interpret natural language text. Using this method, we aimed to identify potentially worrisome renal masses through imaging performed at our institution to aid in the automation of patient follow up.
Methods: We retrospectively screened computed tomography studies for complex renal masses from a four‐week period at a single tertiary academic center. We created a search algorithm leveraging Boolean expressions utilizing Nuance mPower Clinical Analytics, a natural language processing program. The goal of the search algorithm was to search every computed tomography radiology read performed at our institution and select for those studies with concerning renal masses. Radiology reports were then grouped by patient to avoid duplication.
Results: A total of 1735 patients were screened for renal masses. Of the 1735 patients, 49 patients were found to have complex renal masses. Using the algorithm, the program identified 52 patients potentially having complex renal masses. 41 patients out of the 52 patients had relevant renal masses and 11 patients did not. The program did not capture 8 patients with complex renal masses. The sensitivity, specificity, positive predictive value, and negative predicative value of the search query were 84% (41/49), 99% (1675/1686), 79% (41/52), and 99% (1675/1683), respectively.
Conclusions: As the rate of imaging and incidental findings arise, leveraging natural language processing may be a useful adjunct in quickly identifying multiple urologic conditions. Our data demonstrates that this algorithm is able to capture patients with incidental findings of complex renal masses quickly and effectively.
Moderated Poster Session 32: Inflammation
Gut microbiota and metabolites acetic acid were involved in the association between renal calcium oxalate stones and diabetes
K Wang, Q Jiang, X Jin, Y Liu, Y Ma, L Zhou, H Li
West China Hospital, Sichuan University
Introduction & Objective: Renal calcium oxalate (CaOx) stones is one of the most common urological diseases. Gut microbiota was associated with many metabolic diseases, like diabetes. Many studies showed that diabetes was a risk factor for renal stones. We aimed to study the role of gut microbiota in renal CaOx stones and diabetes and the underlying mechanisms.
Methods: We recruited 20 diabetes patients, 20 renal CaOx stones patients, 20 diabetes+renal CaOx stones patients and 20 controls, and analyzed gut microbiota by 16S rRNA sequencing analysis. Then we provided vinegar for renal CaOx stone model rats and renal CaOx stone+diabetes model rats by gavage to verify the effect of acetic acid on the formation of renal stones. Finally, we exposed HK‐2 cells to high glucose medium and sodium acetate, and examined the expression of tight junction protein (Occludin) and the adhesion of calcium oxalate crystals.
Results: The relative abundance of Bacteroides, Faecalibacterium and Prevotella were the highest in the gut microbiota of healthy controls group, followed by diabetes patients, renal CaOx stones patients, and diabetes+renal CaOx stones patients. These bacteria could produce acetic acid. Supplementation of vinegar reduced renal CaOx crystals, and increased blood acetic acid level in renal CaOx stones model rats and renal CaOx stone+diabetes model rats. The expression of Occludin in kidney also decreased in these two kinds of model rats and increased in vinegar‐gavaged rats. In vitro, after sodium acetate treatment, the number of crystal adhesion in HK‐2 cells decreased, and the expression of Occludin in mRNA and protein level also increased. These changes persisted in the high‐glucose environment.
Conclusions: Gut microbiota and its metabolites (acetic acid) played an important role in the formation of renal CaOx stones. Acetic acid could reduce renal CaOx stones by regulating the expression of tight junction protein in kidney and the adhesion of CaOx crystals.
Identifying Predictors of Sepsis Post‐Ureteroscopy in a US‐Based Population: Results from the Endourological Society TOWER Collaborative
N Bhojani, R Paranjpe, B Cutone, S Bhattacharya, BH Chew
University of Montreal Hospital Center (CHUM)
Introduction & Objective: Ureteroscopy (URS) is the most frequently performed procedure for the management of stone disease. A potential complication is sepsis which can lead to significant patient morbidity and mortality. The objective of the current study was to evaluate the incidence of sepsis post‐URS as well as identify clinical and demographic predictors from a large database.
Methods: A retrospective analysis was conducted using the IBM MarketScan commercial database. Patients were included if they had an index URS procedure between Jan 2015 and Oct 2018, developed sepsis within 30 days of URS and were ≥18‐years. Patients with a sepsis or URS event 6‐months prior to the index date were excluded from the study. A multinomial logistic regression was conducted to identify various clinical and demographic predictors of sepsis post‐URS. The demographic predictors included gender, age, region, while the clinical predictors included the Elixhauser comorbidity score, and comorbidities such as diabetes, hyperlipidemia, obesity, and ischemic heart disease. The analysis was performed using Instant Health Data software.
Results: The patient cohort consisted of 81,980 patients. Of these, 4.88% developed sepsis and 1.24% developed severe sepsis. The overall incidence of developing sepsis was 4.91%. Males (OR = 0.33; p‐value <0.0001), patients with hyperlipidemia (OR = 0.76; p‐value <0.0001) and obesity (OR = 0.9; p‐value = 0.03) had a significantly lower likelihood of developing sepsis post‐URS. Diabetic patients (OR = 1.55; p‐value <0.0001), older patients (age 55‐64 versus 18‐34; OR = 1.39; p‐value <0.0001) and patients with a higher Elixhauser comorbidity score (OR = 1.10; p‐value <0.0001) had a significantly higher likelihood of developing sepsis post‐URS.
Conclusions: The current study demonstrated a 4.91% incidence of sepsis post‐URS in a large commercial database of patients in the USA. Male gender, hyperlipidemia and obesity were protective against sepsis while diabetes, older patients and higher Elixhauser comorbidity score were associated with higher rates of sepsis. These results can help identify patients at a higher risk of sepsis post‐URS. Furthermore, appropriate targeted counseling and monitoring can help reduce sepsis associated morbidity and mortality thereby improving outcomes.
What is the Cost of Sepsis after Ureteroscopy? Results from the Endourological Society TOWER Collaborative
N Bhojani, R Paranjpe, B Cutone, S Rojanasarot, BH Chew
University of Montreal Hospital Center (CHUM)
Introduction & Objective: Sepsis is a serious and potentially fatal complication post‐ureteroscopy (URS) among patients with stone disease. To our knowledge, no study has provided data on healthcare utilization and costs of a septic event following URS. The objective of the current study was to evaluate healthcare utilization including real‐world outcomes and costs associated with sepsis post‐URS.
Methods: A retrospective claims data analysis was conducted using the IBM MarketScan commercial database. Patients were included if they had an index URS procedure between Jan 2015 and Oct 2018, developed sepsis within 30 days of URS and were ≥18‐years. Patients with a sepsis or URS event 6‐months prior to the index date were excluded from the study. Descriptive analysis measuring health care utilization including Emergency Department (ED), inpatient stays, Intensive Care Unit (ICU), and medical costs adjusted to 2020 USD, were performed. The health care utilization and cost measures were associated with sepsis as the primary diagnosis and were measured within 1 month of the event. The analysis was performed using Instant Health Data software.
Results: The URS cohort comprised 81,980 patients in the USA. Of these, 1.24% developed severe sepsis and 4.88% developed sepsis with an overall incidence of 4.91%. Among the sepsis cohort, 83.3% of patients developed sepsis on the day of their URS. The mean time to a sepsis diagnosis was 1.81 (±5.19) days. Further, 44.72% of septic patients were aged 55‐64 years, 71.66% were female, and their mean Elixhauser comorbidity score was 1.96 (±2.15). In septic patients, 84.39% required inpatient care and their mean length of stay was 6.25 (±11.61) days. Also, 27.22% of these patients were admitted to the ICU, and 1.91% had an ED visit. The average 1‐month medical cost associated with a diagnosis of sepsis post‐URS was $26,093 (±39,263).
Conclusions: Of patients who developed sepsis post‐URS the vast majority required inpatient hospital care with an average length of stay of more than 6 days. Patients with sepsis had substantial healthcare utilization and costs (avg = $26,093 USD) reflecting that sepsis post URS is both a significant clinical and economic event.
The Endourologic Disease Group for Excellence (EDGE) Prospective Randomized Trial of 2 weeks vs 3 months of post‐operative antibiotics after percutaneous nephrolithotomy in complex patients with infection‐related kidney stones
BH Chew, AE Krambeck, NL Miller, R Hsi, KB Scotland, R Paterson, VK Wong, M Semins, D Lange
University of British Columbia
Introduction & Objective: Struvite infection kidney stones are associated with bacterial infection. Although accounting for only 15% of all stones, they cause disproportionate mortality (up to 67%). Treatment of struvite stones involve complete surgical stone removal followed by antibiotic therapy to eliminate the bacterial infection to reduce stone recurrence. Currently, the optimal duration of antibiotic therapy to prevent stone recurrence is unknown. We sought to determine if there is a difference in outcome between 2 weeks or 3 months of antibiotics post percutaneous nephrolithotomy (PCNL).
Methods: This was a multi‐center, prospective randomized trial evaluating patients with struvite stones undergoing PCNL. Inclusion criteria additionally included stone free status after surgery, defined as having no residual fragments on CT 2mm or larger. Patients were randomized to 2 weeks or 3 months of post‐operative oral antibiotics (nitrofurantoin or culture specific antibiotic). Surveillance imaging and urine culture was performed at 3, 6, and 12‐months post‐PCNL to determine the recurrence of stones and urine colonization or infection. The study was powered to 80% with 18 patients in each group.
Results: A total of 38 patients (51.7 ± 17.7y) were enrolled and randomized to either 2 weeks (n = 20) or 3 months (n = 18) of antibiotic therapy post‐PCNL. BMI was similar between groups (31.9 ± 9.7 vs 31.7 ± 11.8 kg/m2) as was stone surface area (426 ± 194 vs 683 ± 856mm2, p = 0.32), respectively. At 3, 6, and 12 month follow‐up, positive urine cultures were 40% vs 33.3%, 30% vs 50%, and 30% vs 38.9% between 2 wk and 3 mo groups, respectively (p = ns). At 3, 6, and 12 month follow‐up, stone free rates were 62.5% vs 61.5%, 61.5% vs 55.6%, 66.7% vs 50% (p = ns), between 2wk and 3 mo groups, respectively. No patients in either cohort were admitted to hospital for or sepsis or febrile episodes.
Conclusions: There is no difference in stone recurrence, re‐infection or recurrent urinary tract infections comparing 2 weeks versus 3 months of post‐operative antibiotics among patients with struvite kidney stones undergoing PCNL. For patients with complete clearance of struvite stones following PCNL, 2 weeks of post‐operative oral antibiotics is sufficient to prevent recurrent infections and stones. This patient population is at high risk of recurrence for both infections and stones.
Proteomic analysis of stone matrix: A window to the pathogenesis of urolithiasis
Q Wang, Y Yang, F Sun, S Wang
Department of Urology, Guizhou Provincial People's Hospital, Guizhou University, Guiyang, Guizhou, 550000, China
Introduction & Objective: Proteins are the most abundant component of kidney stone matrix and they can reflect the process of stone formation. Many studies have explored the proteomics of urinary stones and crystals. We aim to make a comprehensive presentation of the proteins in kidney stone and to identify reliable and new biomolecules for nephrolithiasis research.
Methods: A systematic review of studies focusing on the proteomics of urinary stones and crystals was conducted in November 2020. ClusterProfiler R package was used to transform the proteins to corresponding genes and Ensembl ID. We took intersection of the proteomic results from each study to find out the 20 most frequently identified stone matrix proteins. Biological information of the top 20 proteins was obtained from Human Protein Altas. Gene Ontology (GO) and Kyoto Encyclopedia of Genes and Genome (KEGG) analysis were conducted to explore the biological function of the top 20 proteins. In addition, we performed immunohistochemistry to detect the expression of three matrix proteins (S100A8, S100A9 and osteopontin) in renal tissue from kidney stone patients.
Results: Nineteen relevant studies were included for analysis. After removing the duplications, a total of 1409 proteins were identified in stone matrix. S100A8, S100A9, uromodulin, albumin, osteopontin, lactotransferrin, vitamin K‐dependent protein Z, prothrombin, hemoglobin subunit beta, myeloperoxidase, mannan‐binding lectin serine protease 2, lysozyme C, complement C3, serum amyloid P‐component, cathepsin G, vitronectin, apolipoprotein A‐1, eosinophil cationic protein, fibrinogen alpha chain, and apolipoprotein D were the 20 most common proteins in stone matrix. GO and KEGG analysis revealed that they were mainly engaged in inflammation and immune response. Immunohistochemistry showed that the expression of S100A8, S100A9, and osteopontin was increased in renal tissue from kidney stone patients.
Conclusions: Proteins in kidney stone matrix mainly play a role in inflammation and immune response. Studies exploring the immune response in nephrolithiasis are expected in the future.
Withdrawn
The Optilume Drug Coated Balloon for recurrent anterior urethral strictures: 3‐year results for the ROBUST I study
O Kayes, S Elliott, R Virasoro, J DeLong, R Estrella, M Pichardo, R Rodriguez‐Lay, G Espino
St James's University Hospital
Introduction & Objective: Mechanical dilation and direct visualization internal urethrotomy (DVIU) are the most widely utilized treatments for urethral stricture disease, but recurrence rates are high after re‐treatment. This study investigates the safety and efficacy of the Optilume® paclitaxel‐coated balloon for the treatment of recurrent anterior strictures.
Methods: Ethics committee approval was gained prior to enrollment commencing. Men with recurrent bulbar strictures ≤2cm with 1‐4 prior endoscopic treatments were treated with the Optilume® drug‐coated balloon. Patients have been followed at 3 months, 6 months, and annually through 3 years. The primary safety endpoint was serious urinary adverse events. The primary efficacy endpoint was the proportion of subjects with ≥50% improvement in International Prostate Symptom Score (IPSS) at 3 years. Subjects receiving secondary treatment were treated as failures for this endpoint. Secondary outcomes included quality of life, freedom from repeat intervention, erectile function, flow rate, and post‐void residual urine volume.
Results: A total of 53 subjects were enrolled and treated; 43 were evaluable at the 3‐year follow‐up for the primary endpoint. 43% of men had undergone ≥2 previous dilations, with a mean of 1.7 prior dilations. There were no serious adverse events related to treatment at 3 years. Success was achieved in 29/43 (67%), which is consistent with 2‐year results. IPSS improved from a mean of 25.2 at baseline to 5.5 at 3 years (p < 0.001). Freedom from repeat intervention of the study stricture was 33/43 (77%). Quality of life, flow rate, and post‐void residual urine volumes improved significantly from baseline. There was no impact on erectile function.
Conclusions: Subjects with recurrent bulbar strictures treated with Optilume® paclitaxel‐coated balloon exhibited significant improvement in symptomatic and functional outcomes through 3 years post treatment. The rate of success is consistent with reported 2‐year outcomes. Long term follow up will continue through 5 years in the ROBUST I study, and a randomized study is ongoing.
The effect of urinary infection and antibiotics on calcium urolithiasis: A potential novel pathogenic role for zinc
J Bjazevic, KF Al, JP Burton, H Razvi
Western University
Introduction & Objective: Recent evidence suggests that the formation of calcium‐based stone disease may be impacted by both urinary bacteria and antibiotics. Zinc (Zn) may play an integral role in this process given that it serves as both an early nidus for the mineralization of urinary stones and is involved in host immune system function and bacterial pathogenesis. We aimed to further investigate the role of urinary bacteria and antibiotics on the pathogenesis of urolithiasis, potentially through modulating Zn transporters as part of the immune response.
Methods: Wild‐type Drosophila melanogaster (DM) flies were reared under standard conditions with either a standard or lithogenic diet containing 0.1% sodium oxalate, and then treated with a combination of either a non‐urease producing E. coli strain (UTI89), ciprofloxacin (0.2 μg/mL) or TMP‐SMX (30/10 μg/mL) for 7 or 14 days. Stone burden was assessed through measured pixel intensity of CaOx crystals in dissected Malpighian tubules. To assess Zn transporter gene expression, DM flies were homogenized, and total RNA was isolated and converted to cDNA and sequenced on an Illumina NextSeq. Quantitative PCT was then performed for each known DM Zn transporter gene [ZnT35C (CG3994), ZnT63C (CG17723), ZnT41F (CG11163)], using ®–tubulin as an internal control.
Results: Increased CaOx stone formation at day 7 was observed in the DM flies treated with E. coli UTI89 (p = 0.005), ciprofloxacin (p < 0.001), and TMP‐SMX (p = 0.003). Preliminary results demonstrated a trend towards increased expression of the Zn transporter gene ZnT41F in DM flies treated with UTI89. However, co‐treatment with both E. coli UTI89 and either antibiotic reduced the expression of ZnT41F to baseline levels.
Conclusions: These findings suggest that non‐urease producing E. coli, and the antibiotics ciprofloxacin and TMP‐SMX impact CaOx stone formation, and that modulation of Zn transport proteins may be involved in this process. Further investigation is required to confirm these results and delineate the exact mechanism involved.
Impact of Peri‐operative Antibiotic Choice on Infectious Complications After PCNL‐ A Prospective Randomized Trial
HC Wright, N Kachroo, RK Jain, O Mohammed, DC Fedrigon, A Zampini, S De, MJ Noble, M Monga, W Isac, S Sivalingam
Cleveland Clinic‐ Glickman Urological & Kidney Institute
Introduction & Objective: The American Urological Association guidelines recommend peri‐procedural antibiotics for percutaneous nephrolithotomy (PCNL), yet it is not clear which is superior. Given the risk of infectious complications after PCNL, we prospectively compared two common antibiotics: ciprofloxacin (cipro) versus cefazolin, on PCNL outcomes, focusing on the presence of systemic inflammatory response syndrome (SIRS) criteria. We hypothesized that the use of cipro will result in less infectious complications due to its broader spectrum for urinary bacterial coverage.
Methods: Adult patients undergoing PCNL were randomized to receive either cipro or cefazolin perioperatively. All had negative pre‐operative urine cultures. Demographic and peri‐operative data were collected, including SIRS criteria, intra‐operative urine culture, duration of hospitalization, and need for intensive care. SIRS is defined by ≥2 of the following: body temperature <96.8 °F or >100.4 °F, heart rate >90 bpm, respiratory rate >20 per minute, WBC count <4000 or >12,000 cells/mm3. Wilcoxon‐Mann‐Whitney was used to compare continuous variables and a Chi‐square test or Fisher's exact test was used to compare categorical variables. All statistical analysis was performed using SPSS version 26 (IBM).
Results: One hundred twenty‐two patients were enrolled and randomized (69 Cefazolin, 53 cipro). Mean age was higher in the cipro group (61 vs. 57, p = 0.02). All other pre‐operative characteristics were similar (p > 0.05). Intra and post‐operative findings were similar, with no difference between groups (p > 0.05), including the number of patients meeting SIRS criteria. There were 3 positive intra‐operative urine cultures in the cefazolin group, versus none in the cipro group, although this was not significant (p = 0.26). One patient required intensive care in the cipro group, versus none in the cefazolin group. There were no Clavien‐Dindo ≥3 complications, and no adverse reactions to either antibiotic.
Conclusions: Despite the relatively broader coverage for urinary tract pathogens with Cipro, this prospective trial did not show superiority over cefazolin. Accordingly, we reject our hypothesis as this data shows cefazolin and cipro appear to have equal effects on post PCNL SIRS outcomes, allowing for more options with perioperative antibiotic prophylaxis.
Withdrawn
Urosepsi and Mortality, which aspects affect which outcomes
M Maltagliati, L Berti, U Besana, C Gastaldi, L Rivolta, C Buizza, M Sighinolfi, BC Rocco, S Micali, G Bozzini
ASST Valle Olona
Introduction & Objective: Urosepsis is a drammatical situation caused by the infection of the urinary tract. Urosepsis is not that uncommon and can lead to critical conditions including death. We analyzed the risk factors for mortality in patients with urosepsis.
Methods: We treated 115 patients with Urosepsis from January 2015 to June 2019 in our hospital. We classified the patients into two groups, Group 1 including patients who died within 30 days of hospitalization, and Group 2 patients that remained alive. We evaluated the data including: age, sex, underlying disease, source of bacteremia, bacterial cultures, performance status (PS), laboratory date, vital signs, duration of hospital, eventual surgical treatment. The Fisher's exact test was used to compare the two Groups. Multivariate logistic regression was used to examine the factors for mortality of urosepsis.
Results: The causes of urosepsis were complicated pyelonephritis in 77.4%, non‐obstructed pyelonephritis in 10.4%, emphysematous pyelonephritis in 5.2%, prostatitis in 3.5%, and cystitis with dysuria in 3.5%. Seven patients (6.1%) died within 30 days of hospitalization; complicated pyelonephritis (6), emphysematous pyelonephritis (1). The median age of the dead patients was 87 years (range, 83‐95 years). Group 1 is significantly older than the Group 2 (p = 0.003). There were no significant differences in mortality with regard to sex or underlying disease. All dead patients had significantly worse PS (p = 0.0001). Among patients evaluated with urinary culture, the most common micro‐organism isolated was Escherichia coli, which was positive in 75 patients (65.2%). 62.6% patients had positive‐blood culture (E.coli was the most common). Pseudomonas aeruginosa in urine was significantly more present in Group 1 (p = 0.0049) where fever was significantly higher(p = 0.017). Nephrostomy and Ureteral stents placement were done in 41 patients. There were no significant differences in mortality with regard to kinds of drainage. Multivariate analysis demonstrated that the risk factor for mortality was the age (p = 0.006).
Conclusions: Urosepsis remains a fatal disease. The older patients, especially with worse performance status and P. Aeruginosa infection are more at risk for death.
Withdrawn
Preoperative Predictors of Positive Stone Culture
JA Khusid, BT Edelblute, D Lundon, AS Sadiq, WM Atallah, M Gupta
Icahn School of Medicine at Mount Sinai
Introduction & Objective: Positive kidney and ureteral stone cultures are associated with infectious postop complications, however culture results are not available until 24 hours or more after surgery. We sought to determine which preop factors may predict stone culture positivity.
Methods: Our high‐volume kidney stone center maintains an endourology database which we retrospectively reviewed to identify adult patients from 2015 onwards in whom a kidney or ureteral stone culture was performed. We collected data on patient demographics, comorbidities, preop urine cultures, radiographic findings, and stone culture results.
Tests for associations were conducted using Chi‐square or Fisher exact tests for categorical variables, and Students t tests or Wilcoxon Ran‐Sum tests for continuous variables. Strength and direction of associations between covariates and status of stone culture were assessed using odds ratios and 95% confidence intervals.
Results: Complete data were available for 133 patients, of whom 34 (25.6%) had positive stone cultures. Of these, 116 patients (87.2%) underwent percutaneous nephrolithotomy (PCNL) and the remaining underwent ureteroscopy (URS). Factors associated with stone culture positivity were history of diabetes (DM), history of hypertension (HTN), history of recurrent urinary tract infection (UTI), UTI within the past year, preexisting ureteral stent or nephrotomy tube, positive preop urine culture (UCx), and presence of a staghorn calculus (Table 1). The most common organisms identified within stone cultures were Enterococcus, Escherichia, and Candida species (Table 2).
Conclusions: Patients with DM, HTN, positive preop UCx, recurrent UTIs, UTI within the past year, pre‐existing tube, or staghorn calculus who are undergoing PCNL or URS are at higher risk for positive stone cultures and should be monitored postop for signs and symptoms of impending sepsis. If sepsis develops, broad spectrum antibiotics including antifungals should be considered given the wide diversity of infectious species within stone cultures.
Kidney stones prevalence in Inflammatory Bowel Disease patients: An initial cohort report
V Dall'Aqua, L Macedo, A Lopes Neto
Introduction & Objective: Nephrolithiasis is a worldwide health problem because its high elevated prevalence in general population (1‐15%). Inflammatory bowel disease patients, in whom fluids, minerals and metabolites absorption, reabsorption and excretion are modified, this prevalence seems even worse (7‐15%). In order to establish the urinary lithiasis prevalence in this specific group we conduct the present data review.
Methods: A transversal, retrospective and descriptive study is reported. Medical records from inflammatory bowel disease patients registered in ABC Medical School Gastroenterology Division was reviewed from January 2013 and January 2018 and the collected data was included in analysis. Image study (CT scan or urinary sonography) was required to patient selection. Age, gender, basis disease and kidney stone presence was described.
Results: Sixty patients were included. In this group, 45% (27) was male and the majority (65%) had between 30 and 60 years‐old. Crohn's Disease was the base disease in 43% (26) patients, whilst Ulcerative Colitis was present in 57% (34). Kidney stone disease was identified in 13 (22%) patients, more frequently associated with Ulcerative Colitis (62%).
Conclusions: Kidney stones in inflammatory bowel disease patients seems to show a higher prevalence than in general population. Females had higher involvement and economically active population is the most affected group. Both disease, Crohn's Disease and Ulcerative Colitis, showed urinary lithiasis but a slightly predominance was noted in the second group. Further large cohort studies are necessary to prove these finds. We started an specific Clinics in our institution to study kidney stones epidemiology, physiopathology and risk factors in this population and, in a close future, more strong data will be available.
Increased Prevalence of Urinary Tract Infections and Catheter‐Associated Urinary Tract Infections in Disorders Characterized by Iron Dysregulation
PR Patton, A Selva, B Prol, Z Chen, V Bird
Urologic Integrated Care
Introduction & Objective: Urinary tract infection (UTI) accounts for up to 40% of all healthcare‐associated infections and its prevalence varies among different populations. Bacteria require iron‐rich environments for optimal survival. Escherichia coli (E. coli), the most common pathogen responsible for UTI, has been shown to thrive in iron‐rich environments. Our aim was to explore the prevalence of UTI and catheter‐associated urinary tract infection (CAUTI) in a cohort of patients with iron‐sequestering disorders compared to other populations.
Methods: The University of Florida Health Informatics for Integrating Biology and the Bedside (i2b2) system was queried for the purpose of retrospective analysis of UTI and CAUTI associated with E. coli sepsis. International Classification Codes (ICD‐9 and ICD‐10) were used to obtain our target diagnoses of interest, subjects with the classically iron‐wasting diseases: sickle cell anemia (SS), thalassemia (T), and hemochromatosis (H). Control groups included the general population (GP) and subjects with Crohn's disease (CD) and ulcerative colitis (UC). Univariate analysis was performed. We used SASv.9.4 for our analysis. P‐values were calculated in comparison with the GP.
Results: A total of 1.1 million patients from 2012‐2018 were included in our data query. UTI prevalence in GP, CD and UC was 4.8%, 12.8% and 12.5%, respectively (p < 0.0001 for CD and UC). CAUTI prevalence in GP, CD, and UC was 0.1%, 0.4%, and 0.6%, respectively (p < 0.0001 for CD and UC). In comparison, UTI prevalence in SS, T, and H was 21.1%, 14.8% and 14.9%, respectively (p < 0.0001 for SS, T, and H). CAUTI prevalence in SS and H was 0.9 and 0.7%, respectively (p < 0.0001 for SS and H). The prevalence of E. coli sepsis in SS, H, T, UC, and CD was 1.3%, 0.4%, 0.3%, 0.4%, 0.3%, respectively, and 0.05% in GP (p < 0.0004 for T; p < 0.0001 for SS, H, UC, and CD).
Conclusions: Both iron‐sequestering and iron‐deficient disorders have a significantly higher prevalence of UTI and CAUTI when compared to the GP. In particular, our data suggest that individuals with SS represent a vulnerable group susceptible to all: UTI, CAUTI, urosepsis, and E. coli‐related septicemia. Iron imbalance is a novel risk factor for the development of UTI and related infections. Efforts aimed at prevention of UTI should be pursued in these high‐risk groups and further research should be directed towards this phenomenon.
Withdrawn
Patient Predictors of 30 Day Post‐Operative Infectious Complications for Percutaneous Nephrolithotomy
V Kommidi, A Garbens, H Trivedi, BA Johnson, M Pearle, JA Antonelli
UT Southwestern
Introduction & Objective: Positive pre‐operative urine culture results or sepsis and risk of infectious complications after percutaneous nephrolithotomy (PCNL) have not been thoroughly studied. Therefore, we sought to investigate the relationship between pre‐operative presence of urinary tract infection (UTI) and sepsis and risk of 30‐day infectious complications following PCNL.
Methods: We performed a retrospective cohort study examining all patients who underwent PCNL between 2015 and 2019 at a high volume academic stone center. All patients received a 7‐10 day course of empiric or culture‐based antibiotics prior to surgery. Data on patient demographics, including presence of urinary tract infection (UTI) or sepsis at time of initial consultation with urology at our institution were recorded. Peri‐operative and post‐operative variables were collected and analyzed. Primary outcome was development of 30‐day post‐operative infectious complication (afebrile/febrile urinary tract infection (UTI) or sepsis). Chi‐squared tests, two‐tailed independent t‐tests, and multivariate logistic regression were used to isolate predisposing factors for infectious complications.
Results: In total, 525 patients with 603 renal units underwent PCNL procedures between 2015 and 2019. From these procedures, 34 (5.6%) were diagnosed with UTI with or without fever and 11 (1.8%) developed sepsis within 30 days of operation. On univariate analysis, positive urine culture at initial consultation with urology (p < 0.001), female gender (p = 0.024), race (p = 0.009), and American Society of Anesthesiology (ASA) classification scores (p = 0.020) were all associated with increased rates of post‐operative infection. Presence of a nephrostomy tube or ureteric stent prior to PCNL was not a predictor of infectious complications (p = 0.13). On multivariate logistic regression, risk factors for developing post‐operative UTI without signs of sepsis included UTI at initial urology consultation (OR: 3.9, CI: 1.7 – 9.0, p = 0.002) and ASA >2 (OR: 2.5, 95% CI: 1.1 – 5.8, p = 0.031). Risk factors for developing post‐operative sepsis included sepsis at initial urology consultation (OR: 23.2, CI: 1.8 – 296.0, p = 0.016) and African American race (OR: 8.7, CI: 1.5 – 50.0, p = 0.016).
Conclusions: Presence of UTI and sepsis from urinary source at time of initial urology consultation significantly increases risk of post‐operative infectious complications. Further studies expanding on our results are warranted.
Withdrawn
Fighting uropathogen adhesion on stents with internal and external metal‐based coatings
B Domingues, IM Aroso, E Lima, A A. Barros, R L. Reis, R Bessa
University of Minho
Introduction & Objective: The adhesion of uropathogen on stents can lead to symptomatic infections and promote encrustation, which may affect the indwelling time of the devices. Over the years, metal‐based approaches demonstrated efficacy impairing biofilm formation on stents, with emphasis for zinc‐ and silver‐based strategies, due to their intrinsic antimicrobial properties and biocompatibility. As the urine has in‐stent and out‐of‐stent flows, the biofilm formation can occur inside or outside the stent. Unlike most strategies that only have exterior coatings, in order to provide more efficient antimicrobial properties, we developed internal and external metal‐based coatings on polyurethane stents.
Methods: We performed a modification on the inner and out surfaces of polyurethane stents (7F Tecoflex, Nordson Medical), starting by surface activation with tin(II) chloride dihydrate (≥98%, Sigma‐Aldrich), followed by a electroless plating of metals, namely, zinc and silver, separately. X‐ray diffraction (XRD), contact‐angle, scanning electron microscope (SEM), and energy‐dispersive X‐ray spectroscopy (EDS) analyses were performed to properly characterize the modified surfaces. Biocompatibility assays were carried out following international standard ISO10993‐5, using L929 mouse fibroblast (ATCC NCTC clone 929:CCL 1) and G/G mouse uroepithelial (DSMZ ACC 224). To evaluate antimicrobial effects of coatings, the modified stents were incubated, separately, with Escherichia coli ATCC 25922 and Staphylococcus aureus ATCC 700698 (Methicillin‐resistant strain), following an established biofilm formation protocol.
Results: We designed a protocol able to modify stents, both internally and externally (Fig. 1), as proved by SEM, XRD, contact‐angle, and EDS analyses. Both coatings were efficient against uropathogens, exhibited antibacterial activity by lowering the adherence of both strains, up to two orders of magnitude without compromise L929 and G/G cells viability.
Conclusions: The development of inner and out metal‐based coatings bestows appropriate antimicrobial properties to ureteral stents, conferring advantages comparing with the standard stents on the market.
Drosophila melanogaster grown in cystine containing agar demonstrates cystine in malpighian tubules and absence of dose dependent survival
RI Carey, DL Carey, MS Carey
Florida State University College of Medicine
Introduction & Objective: The common fruit fly, Drosophila melanogaster (Dm), has Malpighian tubules (Mt) that are very similar to the human ureter. Although Dm has served as a model for calcium oxalate kidney stone research, a PubMed literature search revealed no published papers about a cystine stone model in Dm. It has been established that Dm grown in agar containing varying amounts of ethylene glycol will show a dose dependent survival curve associated with Dm death caused by calcium oxalate crystal obstruction of the Mt. In our study we evaluated the dose dependent survival of Dm grown in agar containing varying amounts of cystine and we developed a protocol for dissection, chemical staining, and microscopic analysis to identify cystine stones in the Mt of Dm.
Methods: Wild type Oregon R type fruit flies were grown on standard agar and in cystine concentrations of 0.03%, 0.1%, 1%, and 3%. Survival was assessed every 3 days. Dissection was performed under 15X light microscopy. Cystine stone formation was assessed under 400X to 1000X phase contrast microscopy. 10% sodium nitroprusside solution was used for colorimetric identification of the cystine stones. Dm were anesthetized with FlyNapTM triethylamine for 4 minutes and sexed under 15x magnification
Results: Sexed, uni‐gender vials of Dm containing 50 flies each showed at most a 0.8% difference (98.6% lowest to 99.4% highest) in the number of surviving flies per group of vials over the span of 100 fold concentration differences (0.03% to 3%) for cystine. Survival curves were assessed for 60 days and there was no dose dependent alteration of survival. Phase contrast microscopy revealed the presence of hexagonal cystine crystals in the Mt. This finding was confirmed by the presence of sodium nitroprusside and Ellman's reagent, which selectively turned these stones red, distinguishing them from the larger, coffin‐shaped calcium oxalate stones that can be incidental findings.
Conclusions: There was no dose dependent survival difference with varying concentrations of cystine in the agar over 60 days. Cystine crystals can be positively identified under phase‐contrast microscopy in properly dissected and prepared Mt. Although present in the Mt, the cystine stones are small and do not grow to a sufficient size to cause fatal obstruction. Our study demonstrates a reproducible protocol that demonstrates Dm readily ingest and concentrate cystine in their Mt,. Despite concentration of cystine in the Mt, stone formation large enough to cause obstruction of the Mt is inhibited.
Prevalence of bacteriuria among pregnant women and changes in antibiotic resistance patterns: a six‐year study
EC Cotton, BK Somani, K Saeed, R Geraghty, S Umranikar
University of Southampton
Introduction & Objective: Asymptomatic bacteriuria (ASB) during pregnancy is a major risk factor for development of urinary tract infections and pyelonephritis, which can lead to maternal and foetal consequences. Current European guidelines recommend screening for ASB in pregnancy and treating with appropriate antibiotics. This study aimed determine both the prevalence of ASB during pregnancy, the most common causing pathogens and their resistance patterns.
Methods: A retrospective analysis was performed using microbiology laboratory data from urine sample culture of pregnant women collected at our University hospital over a 6‐year period from 2014‐2019. Identification and susceptibility testing were performed using standard microbiology procedures based on British Society of Antimicrobial Chemotherapy (BSAC) and European Committee on Antimicrobial Susceptibility Testing (EUCAST).
Results: From 1522 positive urine specimens over a 6‐year period, the most common isolates were Escherichia coli and Coliform (lactose fermenters) (n = 1171, 76.9%), followed by Enterococcus faecalis and other enterococci (n = 191, 12.5%). In 2019, the resistance of E.Coli was 56.8%, 25.3% and 4.7% for amoxicillin, trimethoprim and gentamycin respectively, with an increase in resistance of 8% and 3.3% for trimethoprim and gentamycin respectively over this 6‐year period. The resistance rates for nitrofurantoin was 1% and 5.5% for E.Coli and Group B streptococcus respectively.
Conclusions: Antimicrobial resistance (AMR) is a global issue and treatment of ASB can be challenging during pregnancy. Our study shows the trends of AMR in this vulnerable group and will help confirm treatment effectiveness and direct guideline recommendations locally and nationally.
Coeval xanthogranulomatous pyelonephritis and renal replacement lipomatosis
S SINGH, A UPADHAYA, A Mittal, T ADITYA NARAIN, S kumar, V Kumar Panwar, S Navriya
AIIMS
Introduction & Objective: Xanthogranulomatous pyelonephritis (XGP) and renal replacement lipomatosis ( (RRL) have comparative etiopathogenic, clinical and radiological highlights. We show an instance of XGP that was at first emulating as RRL, but later found to be co‐existent with RRL in same kidney and look at the similitudes and the contrasts between them.
Methods: A 40 year old female without any comorbidities presented with chief complaints of right flank pain for past 6months. There was associated history of mild dysuria for past 1month without any pyuria or haematuria. At presentation patient had haemoglobin of 9.3 g/dl with total leucocyte counts of 13400. Serum urea and creatinine of patient was 33 mg/dl and 0.62 mg/dl, respectively. Urine culture shows growth of mixed organism. A contrast enhanced computed tomography (CECT) abdomen done outside showed right kidney replaced by mixed fatty and soft tissue densities mass of 12x9x11cms with pockets of air. Also,25x 30mm stag horn calculi in right renal pelvis with no contrast in the collecting system was seen. CT scan images raised a clinical suspicious of coexistent RRL, showing an ill‐defined adipose mass filling up the right renal fossa. Pre‐operatively a provisional diagnosis of XGP coexistent with RRL was made. DTPA (Diethylenetriamine pentaacetate) scan showed no peak in right kidney with differential function of 9% and GFR 4.53 ml/min. The patient underwent open right simple nephrectomy with primary repair of iatrogenic duodenal injury. Severe adhesions present around the right kidney were carefully ligated and cut.
Results: Gross specimen cut section showed proliferative fatty tissues ceaseless to renal sinus and perirenal fat, encompassing atrophic renal parenchyma. Microscopic findings showed thyrodization of tubules, numerous necrotising granulomas containing histiocytes and lymphocytes with plasma cells neutrophils and mixed inflammatory infiltrate . The histopathology additionally demonstrated xanthoma cells foci with expansion of large mature adipose cells and inflammatory cell infiltration. No malignant cells were identified. All the highlights were reminiscent of xanthogranulomatous pyelonephritis with RRL. Post operative period was uneventful.
Conclusions: Xanthogranulomatous pyelonephritis is an uncommon condition and with concurrent renal replacement lipomatosis is as yet an uncommon element. Differential diagnosis can be reached by explicit imaging combined with operative and pathological findings.
Video SessionVideo Session 14: Robotic Surgery: Ureter and Lower Tract
V14: Robotic Surgery: Ureter and Lower Tract
MA Palese, S Nathan, S Kang
The Outcome of Ureteroneocystostomy Utilizing da Vinci®
A Dahman, MW Salkini
Introduction & Objective: Ureteroneocystostomy, occasionally with creation of Boari flap, is the best option to substitute for the loss of the distal ureter in both benign and malignant conditions. The procedure is usually performed through a large midline or Gibson incision. Utilizing the robotic da Vinci® surgical system made it feasible to achieve the objectives of the procedure with minimally invasive approach. Our aim is to report our experience with robotic assisted ureteral substitution with and without creation of Boari flap.
Methods: We utilized de Vinci® robotic surgical system between September 2009 and February 2021 to reconstruct 37 distal ureteral units in 31 patients (6 patients needed bilateral ureteral reimplantation). 17 benign and 20 malignant conditions needed ureteral substitution. We prospectively collected the data with our institutional IRB approval. The distal ureter was excised with bladder cuff in cases of TCC involving the distal ureter. The proximal ureteral end was spatulated and re implanted to the bladder either directly or after developing Boari flap to enable tension free, leak proof anastomosis. Negative margin was insured in all the malignant cases.
Results: The average patient age was 63 years (ranging from 25‐80). We had 17 male and 14 female patients. All cases were completed robotically except one that needed to be converted to open due to adhesion. The patients were followed for an average of 35 months (ranging from 3 months to 84 months). All the ureters (%100) with benign strictures were patent after reimplantation during the time of follow up. However, 4 ureters (%21) who had lower ureteral TCC developed ureterovesical anastomosis stricture. All strictures occurred in patient with high grade TCC on the initial and final pathology after nephroureterectomy with excision of the flap. None of the 6 patient who had hx of radiation developed stricture. The distal ureter was excised with bladder cuff in cases of TCC involving the distal ureter.
Conclusions: Robotic reconstruction of the lower ureter with Boari flap is feasible and has an acceptable oncologic outcome. High grade TCC of the lower ureter is predictor of recurrence at the anastomosis. Longer follow up is needed especially in cases of malignancy.
Repair of Entero‐Conduit Fistula Using Robot‐Assisted Laparoscopy
AM Asghar, D Strauss, DD Eun
Introduction & Objective: We present a case highlighting surgical management of an entero‐conduit fistula (ECF), with robot‐assisted laparoscopy (RAL). The patient is a 71‐year‐old male with a history of non‐invasive high‐grade urothelial carcinoma (UC) of the left distal ureter who underwent a RAL distal ureterectomy and ureteroneocystostomy and subsequent left RAL completion nephroureterectomy and eventual RAL radical cystoprostatectomy (RC) and intracorporeal ileal conduit (IC) diversion due to recurrence despite an induction course of intravesical BCG. Most recently, he developed metastatic disease to his right lung and underwent robot‐assisted right lobectomy. Currently, the patient is disease‐free. Nearly two years after RC, he presented with food particles and air per his urostomy. He also had a positive poppy seed test. Initially, pouchoscopy identified a pinpoint ECF tract at the proximal end of the IC. A 6‐month trial of conservative management was unsuccessful with multiple episodes of pyelonephritis of his solitary right kidney requiring prophylactic antibiotics. Here, we demonstrate our approach to RAL ECF repair.
Methods: We began with pouchoscopy, which revealed a larger ECF, able to be cannulated by a 5 Fr open‐ended catheter. Injection of contrast highlighted the ECF. A simultaneous pouchogram revealed reflux to the solitary right kidney. Access was obtained using a 5mm optical trocar without difficulty. We noted no significant intra‐abdominal adhesions despite his past surgeries. Four 8mm robotic ports and a 5mm assistant port were used as outlined in the video. The ureteral anastomosis was easily identified and further dissection revealed the ECF in proximity to the bowel‐bowel anastomosis staple line. We upsized the left 8mm robotic port to 12mm to use a 45mm robotic stapler. The ECF tract was stapled and oversewn using 4‐0 silk sutures. Omentopexy and interposition flap was performed by mobilizing the omentum and fixating it in between the bowel and IC using 4‐0 silk sutures to prevent recurrence.
Results: Operative console time was 98 minutes with 25mL of blood loss. He was discharged on the same day. The red rubber catheter, which was secured to the IC, was removed at his 2‐week post‐operative visit. He remains symptom‐free at this time.
Conclusions: First‐line treatment of ECF is conservative management, with surgical repair reserved for rare failure. This case shows the feasibility of RAL ECF repair and revisions for urinary diversion‐related complications. Additionally, it highlights a potential benefit of RAL given minimal adhesion development despite multiple prior major intra‐abdominal surgeries done using the robotic approach.
Introduction & Objective: Robot‐assisted simple prostatectomy (RSP) is a minimally invasive surgical approach for treatment of patients with large volume benign prostate hyperplasia. In this report we aimed to describe the feasibility of Retzius‐sparing RSP technique.
Methods: A 62‐year‐old male presented to Urology Department with a 1‐year history of lower urinary tract symptoms (LUTS). He was on medical treatment regimen with alpha‐blocker drugs. The general assessment including medication and surgical history was unremarkable. The blood PSA level was 2.3ng/mL. Urinary ultrasound and prostate multi‐parametric MRI imaging confirmed the presence of 125cc of benign prostate enlargement. After completing assessments, it was planned to perform a retzius‐sparing robot‐assisted simple prostatectomy.
Results: Consol time and estimated blood was 115mins and 100ml, respectively. No immediate or late complications was noted. The operation was performed with retzius sparing approach. Complete bladder neck trigonization was achieved for better epithelial healing. The drainage catheter and Foley removed at postoperative day 1 and 3, respectively. Final pathology revealed benign prostate hyperplasia.
Conclusions: Robot‐assisted simple prostatectomy is becoming widely used surgical approach for enlarged benign prostate. Complete bladder neck approximation to the urethral edge significantly decreases postoperative dysuria and macroscopic hematuria.
Use of a Bioregenerative Amniotic Membrane Allograft Wrap During Robot‐Assisted Ureterolysis
B Desroches, N Velázquez, R Munver
Introduction & Objective: Omental wrap is commonly performed following ureterolysis to prevent recurrence of periureteral adhesions and fibrosis. We present the case of a 37‐year‐old female with a surgical history of two caesarean sections and laparotomy for the treatment of endometriosis. She subsequently developed right flank pain due to right distal ureteral extrinsic compression requiring a chronic indwelling ureteral stent. Robot‐assisted ureterolysis was subsequently performed. We describe a novel use of a bioregenerative amniotic membrane allograft (CLARIXTM, Amniox Medical, Inc.) to promote ureteral tissue healing and as an adhesion barrier to prevent recurrence of fibrosis.
Methods: The patient's indwelling ureteral stent was removed prior to surgery. Surgery began with right retrograde pyelography which demonstrated a long narrow area of the right distal ureter. A flexible ureteroscope could not be advanced through the ureteral narrowing. A four‐arm robotic transperitoneal approach was used with an additional 12 mm assistant trocar. Lysis of adhesions was performed and revealed inadequate omental tissue. Adhesions of the intestines, appendix, and right ovary encased the right ureter, and appendectomy and right oophorectomy were performed. Robot‐assisted ureterolysis was performed as extensive retroperitoneal fibrosis was noted distal to the right common iliac vessels extending to the level of the bladder. Following ureterolysis, ureteral patency was confirmed as a flexible ureteroscope successfully passed the area of the ureteral narrowing, with the absence of intraluminal obstruction. Vascularity of the ureter was confirmed with intravenous injection of indocyanine green (ICG) and use of near‐infrared fluorescence imaging (FireFlyTM, Intuitive Surgical, Inc.). An indwelling ureteral stent was placed. Omental wrap could not be performed due to the absence of adequate omental tissue. As a result, bioregenerative amniotic membrane allograft wrap of the distal ureter was performed and was secured with 3‐0 monofilament suture.
Results: The operative time was 3 hours 28 minutes and estimated blood loss was 50 cc. The patient was discharged on the first postoperative day and the ureteral stent was removed at 4 weeks. Imaging with renal ultrasound and nuclear medicine renal scan was performed at 10 weeks. The patient had complete symptom resolution.
Conclusions: Cryopreserved human amniotic membrane/umbilical cord tissue assists with healing and minimizes inflammation and fibrosis recurrence. Bioregenerative amniotic membrane allograft wrap after ureterolysis is a reasonable option when omental wrap is not feasible.
Robotic‐Assisted Vesico‐Vaginal Fistula Repair with Omental Flap Interposition
CU Okoro, CJ Rutledge, DD Eun, N Krishnan
Introduction & Objective: We present a case of a 56 year old female with a history of endometrial adenocarcinoma who underwent a total abdominal hysterectomy and bilateral salpingo‐oophorectomy. One month postoperatively she began having urinary frequency, nocturnal enuresis and persistent daytime mixed urinary incontinence requiring significant pad usage. A cystoscopy identified a defect along the base of the bladder proximal to the trigone and a CT urogram confirmed evidence of a vesico‐vaginal fistula (VVF). She was referred to us and elected to undergo a robotic VVF repair. We describe our approach for robotic assisted VVF repair with omental flap interposition and highlight the key aspects of our surgical technique.
Methods: Endoscopic cannulation of the fistula was performed prior to robotic repair. The patient was then placed in steep Trendelenburg and three working robotic ports and an assistant port were used. There were significant post‐surgical adhesions requiring an extensive lysis of adhesions to completely vacate the deep pelvis. Coordinated vaginal retraction with an EEA sizer allowed for adequate dissection of the vesico‐vaginal junction. The fistula was identified through a trans‐vesical approach. The vagina and posterior bladder were mobilized distal to the location of the fistula. The bladder and vagina were then each closed in a single layer. An omental flap was interposed between the bladder and vagina.
Results: Estimated blood loss was 50 cc, total console time was 166 minutes. No complications were encountered. The patient was discharged on post‐operative day 1 and her catheter removed on postoperative day 6. She remains dry at 4.5 month follow up.
Conclusions: Vesico‐vaginal fistulas represent a significantly morbid condition commonly presenting with persistent urinary incontinence. It can result as a complication following gynecologic surgery for benign or malignant conditions, as was the case with this patient. In the post‐surgical setting, and depending on the timing of repair, there can be significant adhesions and inflammation making repair challenging. The robotic platform allows for superior visualization and maneuverability within the deep pelvis, with robotic VVF repair yielding excellent peri‐operative outcomes. We describe the principles for a successful robotic VVF repair with omental flap interposition.
Tips and Tricks for Robotic Ureteral Reimplantation for Pediatric Age Group
AA Elbakry, M Ost, O AL‐Omar
Introduction & Objective: This is a video demonstrating our technical tips and tricks for robotic ureteral reimplantation in male and female pediatric patients for management of vesicoureteral reflux.
Methods: For female robotic ureteral reimplantation, we have a stepwise approach for ureter identification that starts with ureter identification and dissection distal to uterine vessels. In some cases, additional step for proximal ureteral dissection with broad ligament window is required to better identify and isolate the ureter. Better exposure of the ureter can be achieved by complete medial mobilization of the broad ligament with division of the round ligament and the uterine vessels. In male patients, ureter is identified and dissected proximal to the vas deferens. Next, we create the detrusor tunnel in an inverted Y fashion. Detrusorrhaphy starts with an inverted V stitch proximally and an anchoring stitch distally. Then, the tunnel is closed in interrupted fashion with inclusion of the ureter adventitia in the stitches to prevent ureteral slippage out of the tunnel.
Results: We demonstrated our technique with tips and tricks for robotic ureteral reimplantation in male and female pediatric patients with vesicoureteral reflux.
Conclusions: Robotic ureteral reimplantation is feasable in male and female pediatric patients.
Robot‐Assisted Vesico‐Vaginal Fistula Repair
H Hsiang‐Chen, C Kun‐Yuan
Introduction & Objective: Vesico‐vaginal fistula (VVF) is an abnormal opening between the bladder and the vagina, and that classically results in continuous urinary incontinence after a recent pelvic operation. VVFs are the most distressing complications of gynecologic and obstetric procedures. Although the incidence of VVFs has become rare in the industrialized world, they still commonly occur in developing countries. The diagnosis can be established by methylene blue test, tampon test and Cystoscopy. The method of closure depends on the surgeon's training and experience. The main complication of VVF surgery is recurrent fistula formation.
Methods: A 51‐year‐old male, a case of uterine myoma and post abdominal total hysterectomy (ATH) 4 months ago, with chief complaint of continuous urine incontinence for months. VV fistula was told at other hospital and then she went to our hospital for second option. The cystoscopy was performed and showed an at least 1 centimeter hole at the junction of posterior wall and trigone of the bladder. Due to high riding fistula pattern and patient's asking, robotic approach but not tran‐vaginal approach was informed and arranged.
Results: During the operation, the patient was put in trendelenburg position. There are five ports for the surgery. An 8 millimeter camera port was inserted at supraumbilical site, another three 8 millimeter port were used as robotic working arm, and one 12 millimeter trocar was inserted as assisted port. In the beginning, adhesionlysis was performed due to previous ATH procedure. After exposure the fistula site, we made a circle maker as incision guiding then fistulectomy was performed. The vaginal and bladder defect were closed with a 3‐0 V‐Loc suture by continuous method. Then take down a distal omentum by Endo‐GIA as an omental flap for interposition between the bladder and vaginal incisions. The patient recovery smoothly in the post‐operative period. A following up cyctourethrogram on post‐operation‐day 3 reported there was no leakage sign from the bladder.
Conclusions: Robotic‐assisted vesico‐vaginal fistula repair is a feasible option for selected patient. The advantages of the robotic technique include threedimensional visualization and more degrees of wristed instrumentation. The interposition of flaps or grafts is considered to be a protective factor.
Robot‐Assisted Repair of Complex Benign Distal Ureteroenteric Strictures Following Radical Cystectomy
V Maxon, A Goh
Introduction & Objective: This video aims to provide a step‐by‐step approach for robot‐assisted repair of complex benign distal ureteroenteric strictures (UES) following radical cystectomy (RC).
Methods: We demonstrate the feasibility and safety of robotic repair through two clinical scenarios after different forms of diversion and open primary surgery. The cases demonstrate increasing complexity and advanced reconstruction including appendiceal interposition. UES repair is performed in the setting of an open Indiana pouch and a repeat repair after RC and ileal conduit (IC). The patients were placed in the modified lateral position with right side up. Port placement was directed at the right lower quadrant. The steps of the operation consist of extensive lysis of adhesions, mobilization of the diversion and ureter, identification of the UES, excision of ureteral scar tissue and spatulation, assessment of ureteral perfusion using indocyanine green (ICG) fluorescence and the creation of a tension‐free and watertight anastomosis.
Results: Both cases were completed successfully without the need for open conversion. There were no intraoperative complications. Operative times ranged from 180‐273 minutes. Estimated blood loss ranged from 10‐50ml. All patients were discharged on postoperative day 1. No major complications occurred within 90 days of discharge. Renal function remained stable in both patients at 6 weeks postoperatively. Patients were followed with functional renal imaging at 3 months postoperatively.
Conclusions: Robot‐assisted repair of UES is feasible and safe, even in the setting of extensive prior open abdominal surgery. This is the ideal approach for UES repair because it requires less mobilization of surrounding structures, allows for intraoperative ureteral assessment with ICG fluorescence and can successfully create a tension‐free and watertight anastomosis. Our patients recovered quickly and without complications.
Indocyanine Green Angiography for Use in Robotic Spermatic Cord Denervation
AM Makedon, JC Morrison, GL Lloyd
Introduction & Objective: Chronic orchialgia continues to be a challenge for urologists to treat and for patients to live with. Currently, conservative treatment (rest, anti‐inflammatory drugs, physical therapy, antidepressants) is the first line therapy for men struggling with chronic orchialgia. However, when these approaches fail, alternative therapies are required. Before resorting to orchiectomy, microsurgical spermatic cord denervation (MSCD) has been shown to significantly decrease pain with few side effects for the correctly‐selected patient. Accurate microsurgical technique and especially avoidance of arterial injury is critical, especially for novice surgeons as well as in cases with aberrant anatomy. In this video presentation, we describe the novel use of indocyanine green (ICG) angiography in correlation with Doppler during robotic MSCD for the purpose of arterial localization and verification of preservation.
Methods: Robotic MSCD was performed in 10 cases of chronic orchialgia following failed conservative treatment and after a successful anesthetic cord block in the office. The procedure consists of a few distinct steps: division of the cremasteric muscle, isolation of the vas deferens and division of the central adipose tissue. ICG was injected twice in each procedure: to identify the testicular artery during central dissection and to confirm preservation of the artery at conclusion. Micro‐doppler was used adjunctly to confirm findings
Results: In all 10 patients, ICG angiography successfully identified the location and course of the testicular artery, including in cases of aberrant and reoperative anatomy. Doppler assessment confirmed this.
Conclusions: ICG angiography during robotic MSCD is a novel technique to clarify spermatic cord arterial anatomy and is especially useful in the setting of prior surgery and developmental abnormality. This technique is a valuable adjunct to this procedure for novice surgeons, as well as producing visual documentation of successful arterial preservation, without adding significant time or complication
Robotic Techniques in the Management of Ureteral Anomalies
J Natarajan, J Farrow, CP Sundaram
Introduction & Objective: Ectopic ureter is a rare, congenital disorder that can lead to complications of recurrent urinary tract infections (UTI), hydronephrosis, and incontinence. Robotic surgery is increasingly used in the treatment of this ureteral anomaly when compared to open and laparoscopic approaches. We show how the Da Vinci Surgical Robot can successfully assist in surgeries for left and right sided ectopic ureters.
Methods: Two patients were treated for complications of ectopic ureter using the Da Vinci Surgical System at a single academic institution. The first patient was a 63‐year‐old female who was incidentally found to have upper pole hydronephrosis of the left kidney. A pyelogram confirmed a distal obstruction of the upper pole ureter, while demonstrating a normal lower pole ureter. Since balloon dilation did not resolve the ureteral stricture, she underwent a ureteroureterostomy where the upper pole moiety was anastomosed to the ipsilateral ureter using a running suture. Prior to stitching the front plate of the ureter, the patency of the ureter was assessed using a feeding tube, and a JJ stent was placed to ensure proper urine flow. The second patient was an 18‐year‐old female who presented with recurrent UTIs and pyelonephritis. A voiding cystourethrogram and ultrasound confirmed reflux into the right upper pole. This required a heminephrectomy of the upper pole and removal of the ectopic ureter. The initial portion of the surgery involved stapling the distal part of the ectopic ureter laparoscopically. After this was done, the heminephrectomy of the upper pole was done using the Da Vinci Robot. Important structures include: normal ureter and hydroureter.
Results: Both patients underwent successful robotic surgery with no post‐operative complications. The post‐operative CT scans show unobstructed urine outflow to the bladder after the surgeries. Any signs of hydronephrosis or renal dilation were resolved.
Conclusions: Ureteral anomalies may be appropriately treated using robotic approaches on both the left and right sides.
Robotic Excision of a Large Mullerian Duct Cyst
A Srinivasan, P Kerr, C Kosarek, T Dafashy, L Alzweri, j sonstein
Introduction & Objective: Mullerian Duct Cysts are exceedingly rare, with a reported prevalence of 1‐5%, and management is often described in case reports. Various methods include robotic, laparoscopic, open and percutaneous drainage of cysts. We describe our approach to the management of a large, symptomatic Mullerian Duct cyst using the minimally invasive Da Vinci Xi robot.
Methods: A 38 year old man was referred for constipation, obstructive lower urinary tract symptoms (LUTS) and acute urinary retention (AUR). Digital rectal exam noted a small, 15 cc prostate with a large palpable mass cranial to the prostate. An MRI noted a 15 cm mass between the rectum and prostate with no enhancement noted, and aspiration of the mass confirmed a Mullerian Duct cyst. After thorough discussion of treatment options and informed consent, the patient was taken to the operating room for robotic excision of the cyst.
Cystoscopy was performed, and bilateral open ended catheters were placed without difficulty and plugged into an Edelman catheter. The anatomy was distorted secondary to mass effect. After obtaining pneumoperitoneum, the cyst was visualized in the pelvis. Adhesions were taken down sharply. We dissected a flap of peritoneum off the cyst posteriorly. This was noted to be very adherent and fibrotic. At this point, the cyst was entered and 600cc of dark fluid was irrigated from the cyst. We continued our dissection laterally. The anterior rectum was densely adherent to the posterior aspect of the cyst and this was dissected free in an athermic sharp fashion. The cyst was densely adherent and fibrotic, and in close proximity to the left ureter. We used the firefly, and Indocyanine Green was injected through the bilateral ureteral stents to visualize the right ureter. The cyst was completely excised, and the remaining tissue was marsupialized. The cyst was placed into a small endocatch bag. The remaining cyst wall was oversewn using 2‐0 Vicryl. The pelvis was irrigated, the robot was undocked, and the specimen was removed from our midline camera port after slightly extending our incision cranially.
Results: The final pathology of the cyst was noted to be consistent with a Mullerian Duct cyst and at one month follow up, the patient reported significant improvement in constipation, voiding and ejaculation. His International Prostate Symptom Score (IPSS) was now 0, 0 (improved from 13, 4 originally) and he had stopped taking tamsulosin.
Conclusions: Mullerian Duct cysts are rare entities that often appear in the literature as case reports and though various techniques have been described to manage these symptomatic cysts, we describe our successful, minimally invasive, robotic approach.
Video Session 15: Single Port Robotic Surgery II
V15: Single Port Robotic Surgery II
Z Xiaofeng, R Madi, A Singh
Single Port Donor Nephrectomy Via Modified Pfannenstiel Incision: Initial Preclinical Experience
A Beksac, ZR Schwen, L Lenfant, M Abou Zeinab, A Aminsharifi, M Eltemamy, J Kaouk
Introduction & Objective: We describe the surgical technique for single port (SP) transperitoneal donor nephrectomy through a modified Pfannenstiel incision using the da Vinci SP surgical system (Intuitive Surgical, Sunnyvale, CA, USA) on a cadaver.
Methods: The SP surgical system was used to perform transperitoneal donor nephrectomy in a male cadaver. Through A 3 cm modified Pfannenstiel incision was made 4.5 cm from the midline. Through the incision GelPOINT mini (Applied Medical, Rancho Santa Margarita, CA, USA) system was inserted transperitoneally and floating docking technique was used. Through the gel port, the dedicated 25 mm multichannel port and a 12 mm assistant port were introduced. The surgical steps for donor nephrectomy were performed in the following order. 1) Mobilization of the colon, 2) Identification of psoas muscle, ureter and the gonadal vein, 3) hilum dissection, 4) perirenal dissection, 5) ligation of the renal artery and renal vein, 6) removal of kidney by the enlarging incision.
Results: Transperitoneal SP donor nephrectomy was successfully completed without apparent complications. No additional ports were needed and total operative time was 64 minutes.
Conclusions: We demonstrated the feasibility of single‐port transperitoneal donor nephrectomy via modified Pfannenstiel incision, using the novel SP robotic platform. Further assessment is necessary in a clinical setting.
Robotic Assisted Single Port Radical Nephroureterectomy Using the Intuitive SP Surgical System: Our Early Experience
AK Chow, BG Patel, G Henning, M Wahba, KG Sands, RS Figenshau
Introduction & Objective: There has been an Increasing interest in the utilization of the Intuitive single port surgical system for all facets of urologic oncology. In this video, we demonstrate a step‐by‐step approach for a robotic assisted radical nephroureterectomy using the Intuitive Da Vinci SP Surgical System.
Methods: The patient is a 59 year old female who presented with left flank pain and gross hematuria. CT urogram reveals a large filling defect in the left renal pelvis consistent with upper tract urothelial carcinoma. The SP port is placed along the left midclavicular line just lateral and superior to the umbilicus. In this case, we did utilize an additional 12 mm AirSeal assistant port. This incision can be made close to the SP port so that both incisions can be connected for a single incision extraction. The surgery follow the standard steps of a multi‐arm radical nephroureterectomy. The colon is medialized to reveal the underlying gerota's fascia. The proximal ureter is identified and ligated with a weck clip to eliminate antegrade seeding during manipulation of the kidney. The renal hilum is ligated in an en‐bloc fashion with an endo GIA stapler. The superior aspect of the kidney is dissected from its splenic attachments. The kidney is further mobilized laterally. The SP robotic port can be targeted down into the pelvis to dissect the ureter distally. The ureter is completely excised with a sufficient bladder cuff. The bladder defect is closed with a running 3‐0 v loc suture The specimen was placed in an entrapment sac. The robotic trocar site was extended to the assistant AirSeal incision to extract the specimen .
Results: At our institution, we have successfully completed two SP radical nephroureterectomies. Estimated blood loss is minimal, ranging from 50 – 100 cc. Operative time range from 249 – 354 minutes. Pathology of both specimens revealed high grade papillary urothelial carcinoma, both with negative margins.
Conclusions: The SP surgical system is a safe and effective platform for radical nephroureterectomy. It provides multi‐quadrant access without the need for repositioning, redocking, and negates clashing of instruments in the pelvis. An additional AirSeal port when placed in close proximity to the SP robotic trocar port allows for a single site incision after specimen extraction.
Robotic Assisted Single Port Retroperitoneal Off‐Clamp Partial Nephrectomy Using the Intuitive SP Surgical System: Our Early Experience
AK Chow, G Henning, B Patel, KG Sands, E Kim, RS Figenshau
Introduction & Objective: In this video, we present our surgical technique and experience for a single port retroperitoneal off‐clamp partial nephrectomy utilizing the Intuitive Da Vinci Single port surgical system
Methods: The patient is a 75 year old male with a 3 cm mass located in the posterior lower pole of the left kidney. Calculated Nephrometry score is 5p, notable for a close proximity to the collecting system. An incision is made just caudal to the tip of the 12th rib. Retroperitoneal access is obtained in the standard fashion using a dilating balloon. A GelPort is utilized with our SP robotic trocar to allow sufficient length for deployment of the SP robotic arms. An 8 mm air seal assist port was placed lateral and caudal to the Gel port. Upon entry into the retroperitoneum, the psoas is identified and used as our posterior reference point. The plane between the para‐renal fat and psoas sheath is divided. It is important to maintain this plane so that the retroperitoneal fat is lifted anteriorly as to directly approach the renal artery. The renal artery is sufficiently skeletonized to allow placement of a vascular clamp if robust bleeding is encountered during the off‐clamp tumor resection. Gerota's fascia and the peri‐renal fat is cleaned off of the renal parenchyma. The margin of the tumor is marked with cautery. We continue a combination of meticulous cautery and sharp excision circumferentially around the tumor. The collecting system and sinus fat is encountered indicating sufficient depth of excision The collecting system is closed in a running fashion with a 2‐0 v‐loc suture. The renorrpahy is completed with a series of 0‐ vicryl sutures using the sliding clip technique. The specimen was placed in an entrapment sac and extracted through the gel port incision.
Results: At our institution, we have successfully completed three single port retroperitoneal partial nephrectomies using our off‐clamp technique. Estimate blood loss ranges from 50 – 150 cc. There is a learning curve as demonstrated by our operative time of 249 ‐331 minutes. Change in post‐surgical serum creatinine was + .01 to + .18 at short term follow‐up. All three cases had papillary renal cell carcinoma with negative margin.
Conclusions: The SP surgical system is a safe and effective platform for retroperitoneal off‐clamp partial nephrectomy. Our off‐clamp technique has shown excellent oncological outcomes. We do acknowledge a learning curve with the SP surgical system as demonstrated by our operative time.
Tips and Tricks for a True Single‐Site Surgery with the da Vinci SP platform: How to Increase Working Range of Assistant Instruments
J Na, J Kim, S Alip, W Han
Introduction & Objective: The da Vinci SP platform is gaining popularity in the urologic society. Although the da Vinci SP platform has been developed for single‐site surgery many surgeons prefer to place an additional assistant port. This owes to the limited working space of the bedside assistant when assisting through the same incision with the multichannel robotic port.
The ROSI (Remotely Operative Suction Irrigation) system has been introduced as a useful alternativehowever, it is not yet available globally and requires additional devices. Thus, we introduce the following tips and tricks to increase the working range of the bedside assistant using rigid instruments during a true single‐site surgery with the SP platform.
Methods: Thus, we introduce the following tips and tricks to increase the working range of the bedside assistant using rigid instruments during a true single‐site surgery with the SP platform.
Results:
(1) Remove the robotic instrument in the #2 channel opposite to the camera if possible. This will improve access to central area of the visible field.
(2) In order to increase the working range on the left side, raise up the robotic instrument on the left.
(3) When the robotic instrument needs to keep its position and method (2) is not possible, rotate the SP robot clockwise.
(4) Utilizing the robotic joints will further improve downward accessibility. Bow down the SP port and raise up the robotic camera and instruments.
Conclusions: Utilizing these methods increases the working range of assistant instruments in all directions.
This allows a safe and feasible single‐site surgery using the da Vinci SP platform with adequate assistance from the bedside.
Feasibility of Anterior Port Placement for Retroperitoneal Single‐Site SP Renal Surgery; a Cadaver Pilot Study
J Na, S Alip, J Kim, W Han
Introduction & Objective: The da Vinci SP (Intuitive Surgical, Sunnyvale, CA) which is a “purpose‐designed” single‐port robotic platform is emerging as a new surgical approach and has been reported to be applied to various urologic surgeries. Feasibility of the SP system for retroperitoneal renal surgery such as partial nephrectomy has been reported. However, for patients with a small body habitus it is difficult to secure the distance needed for the SP platform. In such patients placing an anterior port may help to widen the distance from the port site to the kidney. A cadaver pilot study was conducted to test the application of an anterior port site for single‐site renal surgery using the SP platform.
Methods: The cadaver was placed in semi‐lateral position. A transverse anterior incision was made 2cm caudal and medial from the ASIS. GelPOINT advanced access platform (Applied Medical) placed through incision and SP system was docked.
Results: The study was done in the following order. (1) Retroperitoneal lateral and posterior dissection of the kidney. (2) Renal artery dissection by posterior approach. (3) Simulation of posterior renal tumor resection. (4) Renorraphy. (5) Ureter dissection. (6) Anterior dissecton of renal vein and artery. (7) Dissection of kidney upper pole. (8) Renal vessel ligation using titanium clip and laparoscopic staplers. (9) Ureter ligation.
Conclusions: Anterior port placement using the SP surgical system for retroperitoneal renal surgery such as partial nephrectomy or donor nephrectomy was feasible in this cadaver study.
Single Port Robotic Assisted Laparoscopic Retroperitoneal Partial Nephrectomy
M Billah, S Ahsanuddin, J Cadwell, F Sheckley, M Ahmed
Introduction & Objective: Intuitive introduced Single Port Robotic Assisted Laparoscopic Surgery in 2018 and it is already approved for urologic kidney and prostate cases. This new technology was a major step forward for single site minimally invasive surgery. It enables multiple instruments with fully wristed motions as opposed to previous technologies which did not allow for wrist movements. Instruments are introduced through a 25mm cannula. This technology can enable truly single port surgery. This video aims to demonstrate single port surgery with a truly single incision by placing the assistant port in the same incision as the robotic port. This video highlights tips and tricks for single port robotic retroperitoneal surgery.
Methods: 74 year old female presented with 1.4cm left upper renal mass. A review of our single port data was done using our prospective renal database. Data points including intraoperative and perioperative outcomes were noted.
Results: Patient underwent single port retroperitoneal partial nephrectomy. A single 35 mm incision was made in left flank. The 25mm robotic cannula and 12mm assistant port were placed in the gel mini port. Our early data included nine patients and when compared against an age matched cohort, there were no significant perioperative differences in outcome.
Conclusions: The single port is a new technology that hopes to enable quicker recovery and less pain for patients. As with all new technologies, there is an associated learning curve. As opposed to previous single port technologies, the new DaVinci Single Port system is easy to use and accessible. It brings the complexity of single port surgery within reach of all surgeons. With time and increasing case load, single port robotic surgery can be as safe and as effective as multiport robotic surgery.
Single‐Port Robotic Kidney Transplantation via Extraperitoneal Approach
M Eltemamy, Y Lin, A Aminsharifi, A Beksac, ZR Schwen, M Abou Zeinab, D Goldfarb, A Wee, J Kaouk
Introduction & Objective: The surgical technique for robotic kidney transplantation (KTx) has been developed for the past decade. Recent robotic KTx series showed comparable outcomes to traditional open KTx regarding the graft function and complication. However, the previous series were multi‐port robotic surgery with an intraperitoneal approach. In this video, we present the technique of a novel single‐port robotic KTx with an extraperitoneal approach.
Methods: We use the Da Vinci Robotic SP system to perform the single‐port robotic KTx. The extraperitoneal route was made through a 5 cm midline infra‐umbilical incision. A Gelpoint port was used for docking the robot. Meticulous preparation of the kidney is crucial on the bench to prevent bleeding after reperfusion. A ureteral stent was placed on the bench table. The external iliac vessels were carefully dissection and vascular anastomosis was performed with 6‐O Gortex sutures on CV‐6 needles. After reperfusion of the kidney, ureteral implantation was performed with 4‐O Vicryl sutures.
Results: Seven procedures have been performed since January 2020. The median time for venous and arterial anastomosis was 28 (24‐26) and 23 (15‐29) minutes, respectively. Ureteral anastomosis time was 35 (12‐48) minutes. The length of stay was 2 (2‐5) days. On postoperative day 2, the pain scale was 0 for all the patients. All 7 cases were completed successfully without any major complication or conversion. There was no delayed graft function after the surgery either. The creatine level was less than 2.5 mg/dL for all the patients at 14 days after the surgery.
Conclusions: Robotic single‐port KTx via extraperitoneal approach is a safe and feasible procedure. In this series, the anastomosis time was longer than traditional KTx, however, no impact on the graft function was observed. Shorter length of stay and less pain were noted.
Single Port Robotic‐assisted Laparoscopic Transmesenteric Dismembered Pyeloplasty
D Cao, D Simon, AK Chow
Introduction & Objective: We present the case of a 15‐year‐old male who underwent single port robot‐assisted laparoscopic transmesenteric dismembered pyeloplasty for ureteropelvic junction obstruction. The patient is non‐verbal at baseline and presented with pain to an outside hospital ER. A non‐contrast CT scan revealed severe left hydronephrosis without evidence of stone, suggestive of ureteropelvic junction obstruction. Subsequent ultrasound and renal Lasix scan confirmed obstruction of the left renal unit. He was referred by his pediatric urologist for minimally invasive management. We aim to demonstrate our technique with the daVinci SP system with the “air dock” technique allowing for true single incision laparoscopic transmesenteric dismembered pyeloplasty.
Methods: The procedure was performed using the daVinci SP single port robotic system and GelPOINT Mini access platform. A single 3cm transverse paramedian incision was made at the level of the left 12th rib. The GelPOINT Mini was placed into the peritoneum but not placed flush against the skin. A 5mm Airseal port was placed through the GelPOINT Mini and pneumoperitoneum was established. The daVinci SP trochar was inserted through the GelPOINT and the arms were docked under direct vision. A 16Fr foley was placed through the GelPOINT for surgeon directed suction. The surgeon was then able to deploy the arms through the incision into the abdomen. The dilated renal pelvis and ureter were identified immediately underneath mesentery. Incision was made through an avascular segment of the mesentery and the ureteropelvic junction was dissected free. The ureter was dismembered from the renal pelvis and spatulated laterally. The ureter was anastomosed to the renal pelvis, excluding the intrinsic stenotic segment. A ureteral stent was placed prior to completing the anastomosis.
Results: The patient tolerated the procedure well and without complications. Though he is non‐verbal, he did not express any signs of pain on postoperative day one. His foley catheter was removed and he passed his void trial. He was discharged that evening. At the 6‐week followup, the stent was removed. He was doing well without any evidence of pain.
Conclusions: This surgical case reports demonstrates true single port transmesenteric dismembered pyeloplasty in a pediatric patient. By utilizing the airdock configuration with the GelPOINT, there was sufficient room to work with the daVinci SP surgical system. The accompanying video demonstrates our setup and surgical technique.
Use of Remotely Operated Suction Irrigation (ROSI) during Single Port Urologic Robotic Surgery: Creating a Truly Single Incision for Minimally Invasive Surgery
N Gopal, M Billah, C Cumarasamy, C Wright, M Stifelman, M Ahmed
Introduction & Objective: With the advent of Da Vinci SP (single port), complex urological operations are being performed with robotic arms introduced through a single incision. However, because it is difficult to introduce the rigid suction tip into the single incision without impairing mobility of the other robotic arms, surgeons have been making a separate 5 mm incision for introduction of suction during single port surgeries. Here we demonstrate use of ROSI (remotely operated suction irrigator), which has a flexible tip that can be introduced into the single incision and be controlled by the surgeon during the operation. As we will illustrate, with the use of ROSI during single port prostatectomy and cystectomy, one can minimize the need for a separate 5 mm assistant port for suctioning without sacrificing the quality of the procedure.
Methods: A GelPOINT access platform is placed into the respective surgical site (i.e., retropubic space for radical prostatectomy; bladder for simple prostatectomy; and peritoneal cavity for cystectomy). A single port trocar and 12 mm assistant port are placed through the access platform. The ROSI is placed into the 12 mm assistant port. The assistant controls the suction with a suction pedal, although one has the option of continuous suction. The surgeon can move the ROSI around the surgical field easily given its flexible tip.
Results: As the accompanying video illustrates, the ROSI can be placed within the periphery of the surgeon's view for suction of smoke; actively manipulated when suctioning urine or blood; and can be placed in the area of dissection if one is suspecting probable bleeding. With the ROSI, we perform radical and simple prostatectomies with a single incision. With a radical cystectomy, a 5 mm assistant port is required to help manipulate bowel, but as we place a JP drain anyway postoperatively, the incision is used as the JP site postoperatively.
Conclusions: Here we demonstrate a case series in single port urological surgery using a suction tip through a single incision to minimize the number of incisions required without sacrificing the quality of the procedures. With the aid of ROSI, we truly can achieve single incision minimally invasive surgery.
Single Port Robotic‐Assisted Removal of an Eroded Inflatable Penile Prosthesis Reservoir and Repair of an Associated Bladder Fistula
DP Simon, S Brockman, A Beer, AK Chow
Introduction & Objective: We present the case of a 73‐year‐old man who underwent single port robotic removal of a retained Inflatable Penile Prosthesis (IPP) reservoir with intravesical erosion and repair of an associated bladder fistula. The patient had a 3‐piece IPP placed in 2014 for erectile dysfunction after radical prostatectomy for prostate cancer. He underwent device explant two years later for infection, at which time the IPP reservoir was “drained and retained”. He developed re‐infection one year later and was again taken to the operating room; however, surgery was aborted due to vascular injuries. He presented to us for evaluation of dysuria and gross hematuria six years after initial IPP placement. Work‐up with CT imaging and cystoscopy demonstrated intravesical erosion of the retained reservoir. We aim to describe our technique for single port removal of the eroded penile prosthesis reservoir and repair of an associated bladder fistula.
Methods: Procedures were performed using the da Vinci SP single port robotic system. The SP robot port was placed through a 3 cm incision superior to the umbilicus, and an additional 12 mm assistant port was placed in the Right Lower Quadrant (RLQ). The peritoneum was incised anteriorly lateral to the medial umbilical ligament, and the space of Retzius was developed by sharp and blunt dissection through densely adherent tissue planes. The pseudocapsule surrounding the eroded reservoir was incised, and the exposed reservoir was removed. Two fistulous tracts identified between the pseudocapsule and bladder were circumferentially excised, and the resultant bladder wall defect was repaired in a single layer with running 3‐0 V‐Loc suture. A drain was placed alongside the bladder repair and externalized through the RLQ assistant port.
Results: The patient tolerated these procedures well and without complications. He was admitted for routine postoperative observation overnight after surgery. On postoperative day one, the drain was removed, and the patient was discharged home with the Foley catheter remaining in place. At 2‐week follow‐up, the patient was recovering well and a cystogram was obtained showing no leaks, and the Foley catheter was removed.
Conclusions: This surgical case report demonstrates the feasibility and safety of performing removal of an eroded IPP reservoir through a minimally invasive approach with the da Vinci SP surgical system. The accompanying video provides a step‐by‐step demonstration of our technique.
Minimally Invasive Lymphocele Drainage using the da Vinci® Single Port Platform: Step‐by‐Step Technique
S Reddy, M Moschovas, S Bhat, J Noël, R Perera, TA Helman, T Rogers, V Patel
Introduction & Objective: Some reports in the literature describe lymphocele formation in up to half of patients following pelvic lymph node dissection (PLND) in robotic‐assisted radical prostatectomy (RARP), with 1‐ 2% requiring intervention. Several treatment modalities for symptomatic lymphoceles are available, including percutaneous drainage, sclerosing agents, and surgical marsupialization, typically performed by laparoscopy or with a multiport robotic platform. The advantage of surgical approach is permanent excision of the lymphocele capsule and fewer days with pelvic drains compared to percutaneous drainage. This study aims to describe and illustrate, for the first time, the step‐by‐step surgical management of symptomatic lymphoceles using a less invasive robotic platform, the da Vinci® Single Port (SP).
Methods: We describe the outcomes of three patients who underwent lymphocelectomy and marsupialization with the da Vinci® SP for symptomatic lymphoceles following RARP and PLND with the da Vinci® Xi.
Results: Operative time for the case was 84 minutes. The blood loss was 25 ml. No intra‐ or post‐operative complications were reported. The patient had his drain removed in under 24 hours after surgery. The mean follow‐up period was 7.7 months. There were no complications or lymphocele recurrence.
Conclusions: Da Vinci® SP lymphocelectomy is safe and feasible with satisfactory outcomes. The SP enables definitive treatment of the lymphocele sac, reducing the number of days with abdominal drains and allows further decrease in surgical invasiveness with fewer incisions and better cosmesis.
Single Port Robotic Kidney Autotransplantation: Description of the Technique
ZR Schwen, A Beksac, M Abou Zeinab, MJ Noble, A Wee, M Eltemamy, J Kaouk
Department of Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
Introduction & Objective: Kidney autotransplantation (KAT) remains a viable option for renal salvage, however the open approach has been marred by significant morbidity due to the high incisional burden. We present our initial series of single‐port (SP) robotic KAT, ideal for multi‐quadrant surgeries, to evaluate the feasibility and safety of the novel approach.
Methods: Inclusion indications for three consecutive patients included complex proximal ureteral stricture, recurrent nephrolithiasis due to metabolic stone disease, and chronic visceral pain. The primary outcome of this study was feasibility in the form of successful completion of the autotransplant defined as no conversions to open and preservation of renal function at follow‐up.
Patients are placed in the supine position, bumped to 45 degrees. Through a midline 5cm periumbilical incision, the SP is docked in the camera‐up orientation in addition to the robotic scissors (right), Maryland bipolar (down), and cadiere grasper (left). A “floating‐dock” access is used through a GelPOINT and wound retractor including a 12mm Airseal and ROSI flexible suction tubing.
The nephrectomy portion of the KAT is similar to a donor nephrectomy: maximizing the length of the renal vessels and ureter and release of all attachments prior to ligating the hilum. The autograft is quickly delivered through the wound retractor after stapling the hilum and is prepared on the back bench in an ice bath. The SP robotic arms are re‐directed towards the ipsilateral pelvis and the external iliac vessels are cleared of fat and adventitia in preparation for the anastomoses. Next, the kidney is re‐introduced through the wound retractor.
With the kidney oriented medially, the vascular anastomoses are performed in a side‐to‐side fashion using a 6‐0 Gore‐Tex suture, starting with the external iliac vein. The external iliac arteriotomy is created with an aortic punch. The kidney is then flipped laterally and the ureteroneocystostomy is performed over a double‐J ureteral stent. For those with severe stone disease, a Boari flap and pyelovesicostomy is performed. Lastly, the peritoneum is closed overtop the kidney to extraperitonealize the graft.
Results: There were no abortions or conversions to open. Estimated blood loss ranged from 50‐100 mLs and the median hospital length of stay was 2 days. At a median of 5 months follow‐up, postoperative GFRs were stable, ranging from +11.5% to ‐17.6%, and there were no reported complications.
Conclusions: We show the safety and feasibility of the SP KAT, which aims to further reduce the morbidity of KAT. Furthermore, we showed that the SP KAT can be performed through a single incision without patient repositioning.
Video Session 16: Robotic Surgery: Kidney II
V16: Robotic Surgery: Kidney II
S Jackman, J Bell, R Autorino
Robot assisted Laparoscopic transperitoneal “No clamp”‐ Zero Ischemia time partial nephrectomy in clinical T1a renal tumors
A Kumar, Y Prashanth, S Kumar, S Yadav, K Saurav
Introduction & Objective: The role of warm ischemia time(WIT) as modifiable predictor of postoperative renal function , has led to development of techniques to minimise WIT. The role of clampless robot assisted laparoscopic partial nephrectomy(RPN) in renal tumors is still not established . We prospectively evaluated the feasibility, safety , efficacy and Trifecta outcomes of RPN in clinical T1a renal tumors.
Methods: All consecutive patients undergoing clampless RPN(using da‐Vinci robotic system) for a clinical T1a predominantly exophytic renal tumors and normal contralateral kidney by a single surgeon between Oct 2019 and January 2020 at our institution were included. The various clinical data were recorded and analyzed. We are presenting video of one such case.
Results: A total of 7 patients were included in the study. The mean age was 56.5 years with mean preoperative serum creatinine and estimated glomerular filtration rate ( GFR) were 0.67 mg/dl and 72.7 ml/min/1.73 m2 respectively. The mean tumor size was 3.1 cm. The tumor was superior polar in 3(42.8%)patients, mesorenal 2(28.5%) patients and inferior polar in 2(28.5%) patients. The tumor growth pattern was cortical in 5 (71.4%) patients and corticomedullar in 2(28.6%) patients. The mean operating time and estimated blood loss were 81.3 min and 103 ml respectively . There was no conversion to open . The positive surgical margins were nil. In histopathology , renal cell carcinoma was found in all patients. The intraoperative and postoperative complications were seen in nil and 1 patient respectively and mainly Clavien 1 ‐ 2 only. The mean estimated GFR at 1 month (70.9) was not significantly lesser than preoperative value( p = 0.54).
Conclusions: Robot assisted Laparoscopic Clampless partial nephrectomy for small predominantly exophytic renal masses (T1a), is feasible, effective with preservation of renal function , acceptable complications and optimal Trifecta outcomes. However, it is a technically challenging procedure and should be done by surgeons of significant surgical expertise
Retroperitoneal Robotic Partial Nephrectomy For a Hilar Renal Mass
A Beksac, KN Meilika, AA Elbakry, KE Okhawere, O Ige, KK Badani
Introduction & Objective: In this video, we present a challenging case of retroperitoneal robotic partial nephrectomy for a posterior and hilar renal mass. The patient is a 66 year old female with an incidental 1.7 cm posterior and hilar renal mass.
Methods: The patient was positioned in the full flank position. Initial incision was made 2 cm below the 12th rib on the mid axillary line. Spacemaker balloon system was used to create space in the retroperitoneum. Four 8 mm trocars have been used in a straight line. A 12 mm assistant trocar was used. As initial step pararenal and perirenal fat have been dissected to visualize the hilum and the renal mass. In this case the renal mass is small and deep into the hilum. Using the TilePro feature, intraoperative ultrasound has been used to verify the tumor's size, edges and depth. Two bulldog clamps have been used for warm ischemia. After tumor resection, first layer renorrhaphy was performed using 3.0 barbed polyglyconate suture. After the first layer, renal artery was unclamped and defect was visualized for arterial bleeders. After excluding arterial bleeding, 0 polyglactin sutures have been used for the second layer.
Results: Surgery was completed in 90 minutes, with an estimated blood loss of 25 mL. Warm ischemia time was 9 minutes. Drain was removed at day 1 and patient was discharged without complications. Pathology revealed oncocytoma with negative surgical margins.
Conclusions: This video demonstrates a stepwise technique for retroperitoneal robotic partial nephrectomy for a challenging hilar renal mass.
Re‐do Robotic Pyeloplasty for Recurrent Ureteropelvic Junction Obstruction: A Case Series Review with Intraoperative Tips and Tricks for Success
BB Whiles, DA Duchene
Introduction & Objective: Ureteropelvic junction (UPJ) obstruction in adults accounts for approximately 1000 hospitalization in the US each year. Despite the high rates of success for pyeloplasty in both adults and children, 5% of patients will develop secondary or recurrent UPJ obstruction. Although various approaches and outcomes have been described for the management of recurrent UPJ obstruction to include outcomes after re‐do pyeloplasty, little information in the literature exists regarding how these re‐do procedures may differ intraoperatively from primary UPJ repair procedures.
Methods: A retrospective chart review was completed to identify all patients who underwent pyeloplasty at our tertiary care academic medical center between 01/2019‐01/2021. Prior pyeloplasty procedures were identified to determine which patients underwent a re‐do pyeloplasty. Patient demographics were obtained via chart review. Intraoperative video footage was reviewed to identify learning points for re‐do robotic pyeloplasty procedures.
Results: A total of 43 patients underwent robotic assisted laparoscopic pyeloplasty by a single, fellowship trained robotic surgeon. Of these cases, 6 (14.0%) were re‐do pyeloplasty cases for patients that had previously undergone a pyeloplasty at an outside institution before referral to our center. Average patient age at the time of initial pyeloplasty was 27.3 years (range 17‐42 years) and 34 years (range 21‐66) at the time of re‐do pyeloplasty. Time from initial surgery to re‐do procedure was 12.2 years (range 1‐24). Right sided UPJ obstructions were seen in 5 of 6 patients undergoing re‐do pyeloplasty, and 50% of patients were female. Maneuvers utilized to aid in successful re‐do procedure included nephropexy in 2 patients, lower pole vessel transection in 2 patients, vessel transposition in 1 patient, and adhesiolysis in 1 patient. No patients required Heineke‐Mikulicz stricturoplasty, spiral flap, or buccal graft. Total operative time was 245 min +/‐ 59.6 min (Mean +/‐ SD). No patients have had recurrence of their UPJ obstruction during short‐term follow up, with follow up ranging between 1 and 16 months.
Conclusions: Re‐do robotic surgical cases can be challenging, even in experienced hands. However, using a few intraoperative maneuvers, re‐do pyeloplasty via a robotic approach can be safely and easily completed.
A Standardized Technique for All Robotic Kidney Surgery
KN Meilika, MP Wilson, KE Okhawere, TG Korn, KK Badani
Introduction & Objective: This Multiview video is demonstrating our standardized approach for all robotic kidney surgery. We have standardized the patient positioning, port placement, and robot docking of the DaVinci Xi system in an effort to optimize efficiency and reduce unnecessary steps for all renal surgery (Partial and radical nephrectomy +/‐ IVC thrombectomy, nephroureterectomy, simple nephrectomy, and ureteral reconstruction including pyeloplasty). For Partial nephrectomy, the same applies to all tumor locations (anterior/posterior/upper polar/lower polar).
Methods: We start by identifying the lateral border of the ipsilateral rectus muscle, this line represents the linear configuration of the 4 ports of the DaVinci Xi system during this transperitoneal approach. There is a single 12 mm assistant port, and a possible 5mm liver retractor in right side cases if necessary. After Veress needle placement, we start by opening pressure of 2 mmHg, we insufflated to 15 mmHg to ensure that there is enough room to prevent injury during blind entry of the 1st (camera) port, then the 0° scope is introduced through the 1st port to observe the anatomy and find the best site to place the 5 mm port for the liver retraction, the 12 mm assistant port placed making a triangle configuration between the 5 mm port (liver retractor) and the uppermost port of DaVinci Xi system. Staying with the concept of the linear configuration of the 4 ports of the DaVinci xi system and depending on observed anatomy the lowermost port is then placed; the last port is then placed halfway between the lowermost port and the camera port which allows maximal side to side working space. The final tip in system docking is to put the bottom of the arm at the level of the canula top which maximizes the up and down working space, then the arms are separated to prevent clashing.
Results: We have safely used this approach in more than 500 various robotic kidney procedures. The most common was robotic partial nephrectomy and utilized for any tumor location. A standardized approach resulted in significant improvement in operative room time efficiency and surgical team efficiency.
Conclusions: This approach has improved the operative room time efficiency, improved the surgical team efficiency, minimized the variability for all robotic renal procedures.
Robotic Partial Nephrectomy For Large Angiomyolipoma “12 cm” with zero ischemia time
A Mohamed, A Mansour, N Younes, A Al ansari
Introduction & Objective: Angiomyolipoma (AML) is the most frequent benign tumor of the kidney, composed of vascular, smooth muscle and fat elements , They are relatively uncommon in the general population, occurring in 0.3%–2.1% of people . Women are more frequently affected than men, with a female‐to‐male ratio of 11 : 4. The lesions may present as sporadic cases 80 % of cases or in association with tuberous sclerosis complex (TSC) 20 % of cases . Small AML less than 4 cm is usually asymptomatic and the diagnosis of is often incidental, When Lesions greater than 4 cm in diameter are often symptomatic and manifest with a clinical picture characterized by lumbar pain, anemia and hematuria. Retroperitoneal hemorrhage and/or bleeding into the renal collecting system are the major complications of AML.
Methods:Case Presentation:
51 years old male patient with no chronic co morbidities, complain of left loin pain for 6 months, no urinary symptoms, review of the other systems within normal
No skin lesions
No family history of renal tumors
Examination:
General examination and local examination within normal Labs Within normal
Radiological investigation:
US followed by CT with contrast which showed left renal mass suggesting AML around 12 cm
Pt offered all aspects of management including angioembolization but he requested surgical excision
Robotic Left partial nephrectomy with zero ischemia time was done
Histopathology came later as AML confirming the diagnosis
Results: Video Presentation
Conclusions:Discussion :
This presentation highlight the different approach in management of AML , The therapeutic strategy of AML varies from case to case, Selective embolization of the feeding artery and surgical removal of the lesion are the pillars of AML management . Alternatively, it is possible to follow the clinical course for small size AML with periodic surveillance of the lesion, Nephrectomy can be opted for in more severe cases, In case the above mentioned alternatives cannot be performed, a medical approach with agents such as sirolimus, an inhibitor of the mammalian target of rapamycin (mTOR) can be chosen.
Giant renal AMLs like our case are exceedingly uncommon. Review of literature reveals few cases of giant renal AMLs like this, all of which required radical nephrectomy for definitive treatment, In our case we choose to perform Partial nephrectomy and preserve the kidney.
Horseshoe Kidney Robotic Assisted Laparoscopic Pyeloplasty: A Case Series
D Au, A Zganjar, DA Duchene
University of Kansas
Introduction & Objective: Horseshoe kidneys are uncommon with an estimated incidence of approximately 1 in 500 persons. Horseshoe kidneys are characterized by arrested developmental ascent and are therefore located lower in the abdomen or pelvis. They are also typically malrotated with ureters passing over the isthmus or anterior to renal parenchyma and have widely variant renal vasculature. As many as 33% will have associated ureteropelvic junction obstruction. Various approaches to horseshoe kidney pyeloplasty have been used over the decades, more recently minimally invasive robotic approaches have been utilized. Owing to the unique anatomy of horseshoe kidneys there are several technical and anatomic considerations that should be considered and which we aim to demonstrate in this video
Methods: Using a da Vinci robotic surgical system, we performed robotic assisted laparoscopic dismembered pyeloplasty on two patients with horseshoe kidneys and left ureteropelvic junction obstruction. We recorded this case series to demonstrate technical considerations, anatomy, and technique for performing robotic assisted laparoscopic pyeloplasty for horseshoe kidneys with ureteropelvic junction obstruction.
Results: Robotic assisted laparoscopic pyeloplasty is a safe and effective approach to the challenging anatomy ureteropelvic junction obstruction in horseshoe kidneys pose. Robotic ports should be placed inferior and medially compared to orthotopic pyeloplasty.
Conclusions: Ureteropelvic junction obstructions are common in horseshoe kidneys and these can initially present in adulthood. Horseshoe kidneys differ from orthotopic kidneys in abdominal location, orientation, and vasculature. Horseshoe kidneys can be approached trans‐mesenteric or by reflecting colon and mesentery medially. Ureteropelvic junction obstructions in horseshoe kidneys are typically high inserting with ureter stretched anteriorly over renal parenchyma. The goal of reconstruction is to re‐anastomose the ureter to the most dependent portion of the renal pelvis. Crossing vessels are usually not an etiology of obstruction. Symphysiotomy (division of isthmus) is generally not recommended due to increased risk of infection, fistulas, leakages, and bleeding.
Introduction & Objective: Pelvic kidneys are uncommon with an estimated incidence of approximately 1 in 3,000 persons. Pelvic kidneys are characterized by arrested renal developmental ascent in the pelvis. Pelvic kidneys are typically malrotated with high renal pelvis ureteral insertion and have widely variant renal vasculature. As many as 37% will have associated ureteropelvic junction obstruction. Various approaches to pelvic kidney pyeloplasty have been taken over the decades and more recently minimally invasive robotic approaches have been utilized. Owing to the unique anatomy of pelvic kidneys there are several technical and anatomic considerations that should be considered which we aim to demonstrate in this video.
Methods: Using a da Vinci robotic surgical system, we performed robotic assisted laparoscopic dismembered pyeloplasty on a patient with a left pelvic kidney with ureteropelvic junction obstruction. We recorded this case to demonstrate technical considerations, anatomy, and technique for performing robotic assisted laparoscopic pyeloplasty in pelvic kidneys with ureteropelvic junction obstruction.
Results: Robotic assisted laparoscopic pyeloplasty is a safe and effective approach to the challenging anatomy pelvic kidney ureteropelvic junction obstructions pose. Patients can either be placed in lateral decubitus position or a lithotomy position depending on orientation of the pelvic kidney.
Conclusions: While pelvic kidneys are uncommon overall, ureteropelvic junction obstructions are common in pelvic kidneys and these can initially present symptomatically in adulthood. Although often compared to horseshoe kidneys, the approach to a pelvic kidney is significantly different than that of a horseshoe kidney. Pelvic kidneys differ in both port placement as well as in the increased technical difficulty of attaining adequate operative exposure. Crossing vessels are often an etiology of obstruction in pelvic kidneys and these vessels may be critical to surrounding structures. Due to the high risk of injuring major adjacent vasculature or aberrant pelvic kidney blood supply, careful pre‐operative radiographic studies to delineate vascular anatomy are recommended. Ureteropelvic junction obstructions in pelvic kidneys are typically associated with high ureteral insertion and repair should be aimed at reconstructing the ureteropelvic junction at the most dependent portion of the renal pelvis.
Partial renal allograft nephrectomy with reconstruction of intrarenal urinary tract
RN Trushkin, AE Lubennikov, TK Isaev, DF Kantimerov, L Artuhina, A Gubko
Introduction & Objective: Kidney transplantation has emerged as the gold standard for patients with chronic renal failure. Patients who have undergone renal transplantation are at twofold increased risk of developing malignancy compared with general population. Even if incidence of renal cell carcinoma in allogenic kidney transplant is low (0.19‐0.5%) it is a complicated clinical case for urologists.
Present management of solid renal masses in an allograft kidney transplant is the same as the management of a native kidney and includes partial nephrectomy, radical nephrectomy, percutaneous radiofrequency ablation, and percutaneous cryoablation.
We would like to introduce an interesting clinical case of a massive intra‐sinus (10.3 х 8.3 cm) tumor of the allograft kidney. An incidental allograft kidney tumor has been revealed in a young female patient (33 y). We performed partial nephrectomy and reconstructed the intrarenal part of the urinary tract.
Methods: We performed a laparoscopic partial nephrectomy with reconstruction of intrarenal urinary tract and reimplantation of ureter. Partial nephrectomy of the tumor was accompanied with clipping lower calyx and followed by anastomosis of infundibulum and renal papilla. Due to the large size of the tumor the ureter was cut off and re‐implanted into the urinary bladder.
Results: Postoperative period was unremarkable. On POD2 a CT‐excretory urography was held. Drainages were removed on POD5. Creatinine level was 174 mcmol/l before the surgery and 130 mcmol/l on the discharge day. The patient went home after 10 days at hospital.
Conclusions: reconstruction of intrarenal urinary tract can give a chance to save the kidney even if the tumor size is considerable and renal score points out a high complexity of partial nephrectomy. Moreover, it can also be performed in allograft kidney patients.
Robotic anatrophic nephrolithotomy with intracorporeal renal hypothermia
W Hu, Y Lin, Y Ou, J Sheu, M Tung
Introduction & Objective: We aimed to demonstrate the technique and timing for achieving cold ischemia during robotic anatrophic nephrolithotomy.
Methods: We present a 59‐year‐old female with a 2.3 cm left lower pole partial staghorn stone complicated with recurrent pyelonephritis. She elected to undergo a robotic anatrophic nephrolithotomy after the infection was controlled. We planned to access with aids of a robotic ultrasound probe and intracorporeal renal hypothermia. We conducted with trans‐peritoneal 5‐arm approach. (A 12‐mm trocar for camera, two 8‐mm trocars for robotic arms and two 5‐mm trocars for assistant.)
We used the 8‐mm trocar to facilitate introduction of ice slush. Sterile iced saline slush was created in a slush machine and 20‐ml syringes were modified by cutting off the nozzle end to make a wider opening. We introduced the ice slush once the kidney has been completely mobilized and calculi has been identified via ultrasound probe. In addition to 20‐milliliter syringe, we utilized the obturator for insertion of ice through the 8‐milimeter trocar. Moreover, we placed a gauze cradling around the kidney to protect the surrounding bowel from the cold injury. Finally, the incision was made laterally and longitudinally through full thickness of cortex and the stone was extracted.
Results: The cold ischemia time was 25 minutes and the coldest renal temperature was 24.1 degrees Celsius. The post‐operative estimated glomerular filtration rate (eGFR) was 119.8 ml/min/1.73 m2 3 days after the surgery compared to 131.2 ml/min/1.73 m2 of pre‐operative eGFR. She stayed in the hospital for 7 days without any complication.
Conclusions: Robotic anatrophic nephrolithotomy with intracorporeal renal hypothermia using ice slush is technically feasible and may maintain postoperative renal function.
Our technique is cost‐effective and simple. It is highly reproducible without commercial instruments.
Robotic Assisted Ureteroplasty with Buccal Mucosa Graft for a 3cm Mid‐Ureteral Stricture
DT Lybbert, BF Schwartz
Introduction & Objective: Patients with long, mid‐ureteral stricture disease can be difficult to manage for the surgeon and the symptoms and treatment can often be painful and frustrating for the patients. Recently, there have been few reports of using buccal mucosa grafting as a way an option for treatment of patients that have either failed more conventional treatment or been unable to tolerate ongoing ureteral stent exchanges.
Methods: This is a case report of a 72 year old male with a 3cm mid‐ureteral stricture who had not tolerated indwelling ureteral stents and who sought out alternative therapy. After discussing with the patient, he agreed to undergo a relatively novel procedure of using buccal mucosa grafting in a ureteroplasty in the hopes of relieving his pain and resolving his ureteral obstruction. Pre‐operative and post‐operative imaging, as well as video recorded during the case was used to compile this video to demonstrate our approach to robatoic assisted laparoscopic ureteroplasty with buccal mucosa graft.
Results: The patient had limited options for treatment of his ureteral stricture, but was successully treated with a buccal mucosa graft ureteroplasty. The procedure was tolerated well and follow up since the then has demonstrated lasting symptomatic relief and radiographic evidence of being stricture free for the past year.
Conclusions: Options for complex ureteral stricture disease are limited and the course of treatment can be frustrating for patients. Ureteroplasty with buccal mucosa grafting is a somewhat new approach to complex ureteral stricture disease that has shown to be a viable option for patients with long mid‐ureteral strictures.
Robotic‐assisted laparoscopic calyceal diverticulectomy and nephrolithotomy
A Ludvigson, P Motamedinia, JJ Su, R Ho, K Hotchkiss, D Singh
Introduction & Objective: Percutaneous treatment of stones within calyceal diverticulae is not always possible, because the thin overlying parenchyma of the diverticulum can increase the risk of postoperative urine leak, and the position of the diverticulum is not always amenable to percutaneous access. However, surgical excision can result in recurrence or urine leak as well if precautions are not taken. We present our technique for robotic‐assisted laparoscopic calyceal diverticulectomy, with simultaenous extraction of a large kidney stone.
Methods: Our patient, a 44‐year‐old female, underwent robotic‐assisted laparoscopic calyceal diverticulectomy of the left kidney. The procedure was recorded with her consent and the relevant operative techniques were highlighted.
Results: After exposing the renal capsule, ultrasonography was used to identify the calyceal diverticulum and the large stone within it. The roof of the diverticulum was excised and the contents, mucoid and purulent material, were aspirated out. The stone was extracted intact. Argon beam electrocautery was used to fulgurate the entire surface of the diverticulum to promote scarring and contracture. Next, the ostium of the diverticulum was closed using Vicryl suture. Finally, the diverticular cavity was filled with perinephric and colonic fat, to minimize the chances of recurrence. The area was copiously irrigated with antibiotic solution. It was not necessary to clamp the hilum at any point during the case. A drain was placed, and then discontinued on post‐operative day 1 with low output and a creatinine level consistent with serum. The patient was discharged home on post operative day 1, and continues to recover well in the outpatient setting.
Conclusions: The laparoscopic approach is ideally suited to treat calyceal diverticulae of the kidney. Multiple techniques can be used in tandem to prevent recurrence of the diverticulum after it is excised. The minimally‐invasive nature of the procedure hastens patient recovery and return to normal function.
Introduction & Objective: Here we present a patient with recurrent proximal ureteral stricture initially managed by balloon dilation. A robotic assisted buccal augmented ureteroplasty was performed.
Methods: CW is a 47 year‐old male with long history of urolithiasis, and symptomatic proximal right ureteral stricture. He was initially diagnosed following a work‐up for bilateral urolithiasis. Subsequent balloon dilation of his stricture failed to provide resolution. A ureteral stent was placed and he was referred to our clinic to discuss possible ureteroplasty. His ureteral stent was removed and a Right nephrostomy tube was placed preoperatively. He was scheduled for a robotic assisted buccal augmented ureteroplasty. Details of the procedure will be highlighted in the accompanying video.
Results: A robotic assisted buccal augmented ureteroplasty was successfully performed. The procedure went routinely, and the patient was discharged on post op day 1. His right ureteral stent was removed at his 6‐week follow up, and he reported continued resolution of his right flank pain at the 3 month follow up appointment.
Conclusions: Buccal augmented robotic ureteroplasty is a safe, and feasible technique in the management of upper ureteral stricture disease.
Ureteral side‐to‐side anastomosis for transecting injury of completely duplicated collecting system
RA Lee, AM Asghar, D Strauss, MJ Metro, DD Eun
Introduction & Objective: Iatrogenic injuries commonly occur at the distal ureter. The gold standard for distal ureteral injury is ureteroneocystotomy, however new techniques such as side‐to‐side (StS) anastomosis have demonstrated safe and comparable outcomes. In a duplicated collecting system, two ipsilateral ureters may drain the kidney into the bladder independently or as a single common ureter which may complicate preoperative planning for ureteral reconstruction. Currently limited literature exists regarding iatrogenic distal ureteral injuries to duplicated collecting systems.
Methods: 51 year old female with a history of left robot assisted hysterectomy which was complicated by flank pain post operatively. Imaging work up revealed a duplicated left collecting system with left hydronephrosis concerning for ureteral injury and obstruction. After failed ureteral stent placement patient underwent percutaneous nephrostomy drainage of both left renal moieties.
Patient was evaluated and scheduled for a robotic ureterolysis and reconstruction, and ultimately underwent a robotic assisted side‐to‐side anastomosis and ureteroneocystotomy as described in our video.
Results: Total console time was 241 minutes with an estimated blood loss of 150 mL. There were no intraoperative complications. Patient was discharged with ureteral stent and foley on post operative day one. On follow up, patient with no clinical or radiographic evidence of left ureteral obstruction.
Conclusions: We demonstrate that robot‐assisted StS ureteral anastomosis with an intravesical non‐refluxing ureteroneocystotomy in a duplicated collecting system is a safe and effective option. This technique allows maximal preservation of ureteral perfusion and reimplantation of one ureter. ICG helps facilitate ureteral dissection and assess ureteral blood supply intraoperatively to aid in successful reconstruction.
Combined Robotic and Endoscopic Pyelolithotomy in a Pelvic Kidney
A Higgins, A Nourian, J Cohn, J Friedlander
Introduction & Objective: Ectopic kidneys are rare congenital anomalies, and may be susceptible to higher rates of nephrolithiasis, reflux, and ureteropelvic junction obstruction due to their orientation. Treatment of nephrolithiasis in patients with pelvic kidneys remains challenging due to the complex anatomy and surrounding structures. We describe the treatment of a patient with an ectopic left kidney who presented with a large kidney stone burden.
Methods: A 35‐year‐old male presenting with abdominal pain was found to have a 3.1 cm staghorn calculus with mild hydronephrosis in a left pelvic kidney, as well as additional left lower pole renal stones measuring 1.3 cm and 0.7 cm (Figure 1). Computed tomography angiography was obtained preoperatively and demonstrated that the ectopic kidney was anterior to the bifurcation of the iliac vessels with overlying bowel, making a percutaneous approach challenging, however, the anterior orientation of the renal pelvis appeared amenable to combined robotic‐assisted and endoscopic pyelolithotomy.
Results: The kidney was accessed via a traditional pelvic surgery robotic port set up. The renal pelvis was sharply incised to deliver the staghorn calculus in one specimen. A flexible cystoscope was introduced via a laparoscopic trocar and guided into the incised renal pelvis and lower pole to remove remaining stones via a combination of basket extraction and aspiration via the laparoscopic suction‐irrigator (Figure 2). A ureteral stent was then advanced through the pyelotomy, down the ureter, and into the bladder via a guidewire before watertight closure of the renal pelvis and reapproximation of the peri‐renal fat and peritoneum. The patient was discharged on postoperative day one following removal of his foley catheter and Jackson‐Pratt drain, and he underwent stent removal 6 weeks postoperatively.
Conclusions: Combined robotic‐assisted and endoscopic pyelolithotomy can be a safe and effective approach for pelvic kidney stones that may not be amenable to a single or traditional treatment modality.