
Abstract
Objectives:
To compare the safety and effectiveness of a novel flexible vacuum-assisted ureteral access sheath (FV-UAS) and traditional ureteral access sheath (UAS) in simulating retrograde intrarenal surgery (RIRS).
Materials and Methods:
A manometric model was established in porcine kidneys to observe the change in intrarenal pressure (IRP) in the FV-UAS and traditional UAS groups at different irrigation fluid velocities of 30, 50, 80, and 100 mL/min. Establish a kidney stone model (with 0.2 g, dry, ≤5 mm stones) to simulate RIRS. A total of 20 porcine kidneys were randomly numbered from 1 to 20 (FV-UAS group, 1 − 10; traditional UAS group, 11 − 20). The stone volume clearance rate and operation time were compared between the two groups. (“
Results:
FV-UAS can follow flexible ureteroscopy (f-URS) to cross the ureteropelvic junction (UPJ) and into the renal pelvis and calices. FV-UAS can actively make IRP <10 cmH2O by adjusting the negative values at different irrigation fluid velocities. The mean residual stone volume of the FV-UAS vs traditional UAS groups was 33.7 vs 92.5 mm3 (p = 0.017). The mean stone volume clearance rates of the FV-UAS vs traditional UAS groups were 98.5% and 95.9%, respectively (p = 0.017). Seven cases achieved complete stone-free status in the FV-UAS group. All patients had residual fragments postoperatively in the traditional UAS group.
Conclusions:
FV-UAS can follow f-URS to cross the UPJ and into the renal pelvis and calices, avoiding the interference of UPJ in controlling IRP. FV-UAS can actively control the IRP to be reduced to the desired range by adjusting the negative value under any irrigation fluid velocity. FV-UAS close to the stone can achieve complete stone-free status in RIRS.
Introduction
Retrograde intrarenal surgery (RIRS) is one of the main treatment for renal stones. 1,2 There are two difficult problems in controlling intrarenal pressure (IRP) and residual fragments (RFs) in RIRS. 3,4 The pyelovenous backflow occurs above 40 mm Hg. 5 It may cause infection during the pyelovenous backflow. 6 A study with a follow-up of 2 years showed that the self-elimination time for patients with RFs <1 and 1 to 3 mm were 9 and 13.9 months, respectively, whereas 18.1% and 28.6% of the patients had an increase in stone size. 7 To date, there is no clear way to completely remove these RFs, and only self-elimination by the patient. It takes a long time and can cause renal colic and hematuria and increase the stone size of RFs in the self-elimination process. 8 –11
The application of ureteral access sheath (UAS) improves the surgical field of vision, reduces IRP, and shortens the operating time. 12 –14 Generally, the UAS is placed below the ureteropelvic junction (UPJ) in the RIRS. 15 This causes the irrigation fluid in the kidney to pass through the UPJ to enter the UAS. The UPJ is relatively narrow and is a functional valve between the renal pelvis and proximal ureter, which has a certain impact on IRP control. 15
The purpose of this article is to describe a novel UAS, flexible vacuum-assisted ureteral access sheath (FV-UAS), which can follow flexible ureteroscopy (f-URS) to cross the UPJ and into the renal pelvis and calices. By establishing a manometric model and stone model in porcine kidneys to simulate RIRS, we compared the difference in IRP and stone volume clearance between FV-UAS and traditional UAS.
Materials and Methods
Flexible vacuum-assisted ureteral access sheath
The FV-UAS (Fig. 1A, B) is a novel UAS that has good flexibility and deformability at the tip, which can passively bend (bend >90°) with the bending of f-URS and can connect to a vacuum suction device. The FV-UAS is reinforced with wire springs to ensure that the lumen does not collapse when it bends.
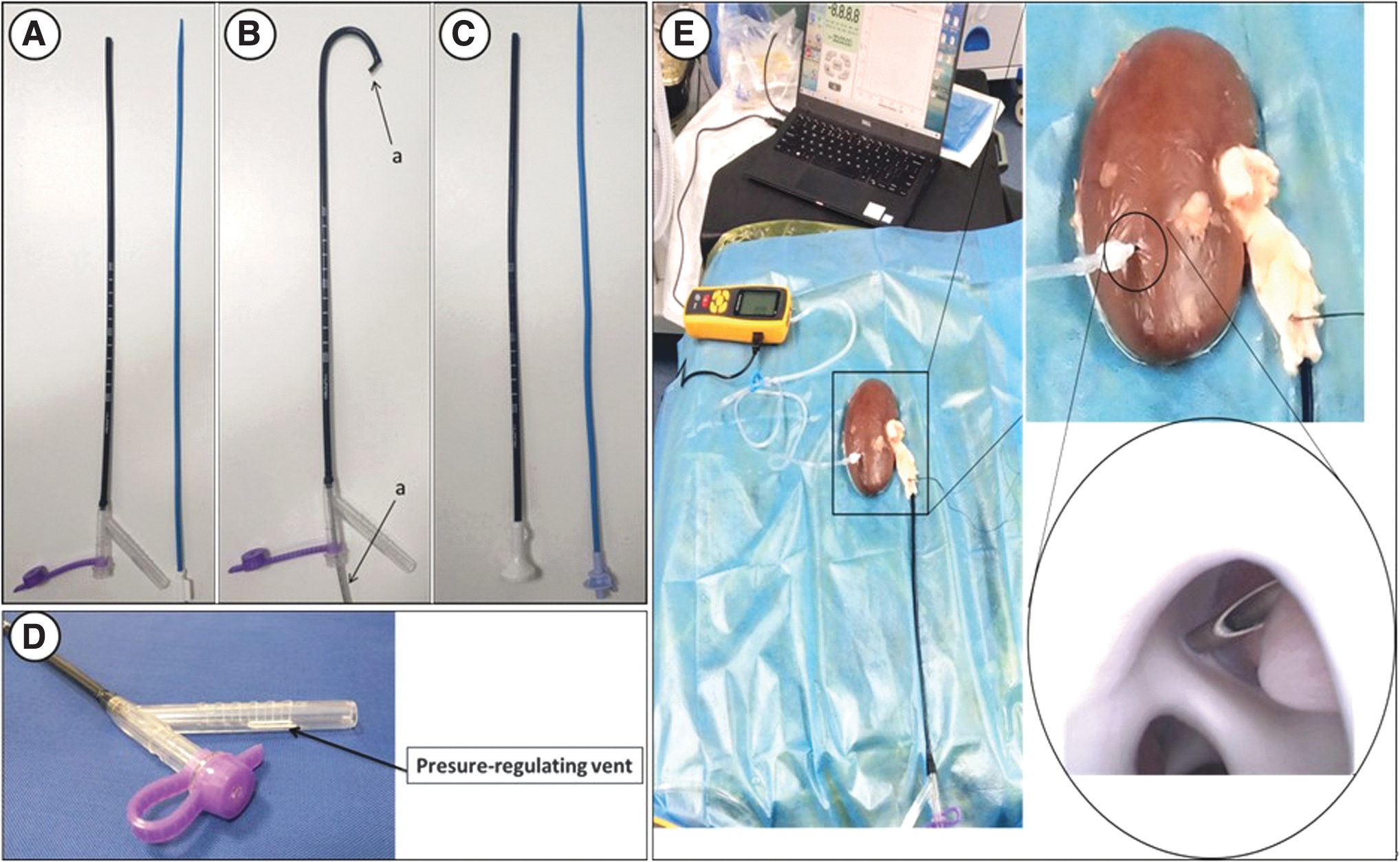
FV-UAS and manometric model:
Establish manometric model
All experimental procedures were conducted in conformity following the institutional guidelines for the care and use of laboratory animals at Nanchang University, Nanchang, China. This study was approved by the Ethical Committee of the Jiangxi Provincial People's Hospital Affiliated of Nanchang University (2021-080).
The pressure sensor (GM522, BENETECH, China) was placed in the renal calix by renal puncture and adjusted to the zero. 16 The FV-UAS (12/14F, 46 cm; ZHANGJIAGANG, Jiang Su, China) and the tip of the f-URS (7326071; Richard Wolf GmbH, Knittlingen, Germany) were located in the renal pelvis and connected to a vacuum suction device (YB-DX23B; SMAF, Shanghai, China). Traditional UAS (12/14F, 46 cm; ZHANGJIAGANG) was placed under the UPJ (no vacuum suction device was connected). The irrigation fluid velocity was 30, 50, 80, and 100 mL/min. The negative value and IRP were recorded under vacuum-assisted in the FV-UAS group and the IRP was recorded in the traditional UAS group.
Establish stone model in porcine kidney and simulate RIRS
A specimen of human kidney stones (stone size ≤5 mm), air-dried naturally at room temperature (25°C), was randomly mixed and weighed (0.2 g). The stones were entered into the collection system of porcine kidney. Twenty porcine kidney stone models were established and randomly numbered (number 1 − 10 for FV-UAS and number 11 − 20 for traditional UAS). The UAS was inserted through the ureter and fixed with a silk thread. This model has been used by scholars to simulate RIRS. 17
An f-URS (7326071; Richard Wolf GmbH) was inserted through the UAS. The FV-UAS (12/14F, 46 cm; ZHANGJIAGANG) was inserted as close to the stone as possible under the direct vision of f-URS. The traditional UAS (12/14F, 46 cm; ZHANGJIAGANG) was placed under the UPJ. Stone fragmentation was accomplished using a holmium-YAG laser (Moses Laser; Lumenis Ltd., Yokneam, Israel, frequency: 20 − 40 Hz, energy: 0.6 − 1.2 J). The FV-UAS group was connected to a vacuum suction device (YB-DX23B; SMAF), and the operation was completed when no stone was in the visual field. The basket is used to capture stones in traditional UAS groups; the operation ends when the basket cannot capture stones anymore. 9
The stone clearance efficiency was reflected in the stone volume clearance rate (“
Statistical methods
Data were processed using SPSS 22.0. Student's t-test was applied that were expressed as the mean ± standard deviation (SD). Two-sided p < 0.05 was considered statistically significant.
Results
The irrigation fluid velocity was 30, 50, 80, and 100 mL/min. At that time, the IRP of the traditional UAS group was 26–27, 47–48, 82–83, and 98–99 cmH2O, respectively. Meanwhile, the IRP of the FV-UAS group under different negative vacuum-assisted conditions was 7–8, 6–7, 6–7, and 9–10 cmH2O; negative values were 21–22, 52–53, 89–90, and 124–125 cmH2O, respectively (Table 1) (Fig. 2).

The changes of IRP: The IRP can be maintained at a lower level (<10 cmH2O) by adjusting negative value at any irrigation fluid velocities (irrigation fluid velocity: a: 30 mL/min. b: 50 mL/min. c: 80 mL/min. d: 100 mL/min). IRP = intrarenal pressure. Color images are available online.
The Values of Intrarenal Pressure at Different Irrigation Fluid Velocities
FV-UAS = flexible vacuum-assisted ureteral access sheath; IRP = intrarenal pressure; UAS = ureteral access sheath.
The mean (SD) preoperative stone volumes was 2210.1 (14.7) mm3 vs 2233.7 (11.7) mm3 (p = 0.226) in the FV-UAS group vs traditional UAS group; the mean (SD) operative time was 44.2 (7.7) minutes vs 39.7 minutes (6.5) (p = 0.178), and the mean (SD) residual stone volume was 33.7 (17.4) mm3 vs 92.5 (14.0) mm3 (p = 0.017), and the mean (SD) stone volume clearance rates were 98.5 (2.5) % vs 95.9 (2.0)% (p = 0.017). Seven cases achieved complete stone-free status in the FV-UAS group. All patients had RFs postoperatively in the traditional UAS group (Table 2).
The Data of Simulated Retrograde Intrarenal Surgery
SD = standard deviation; SFR = stone-free rate.
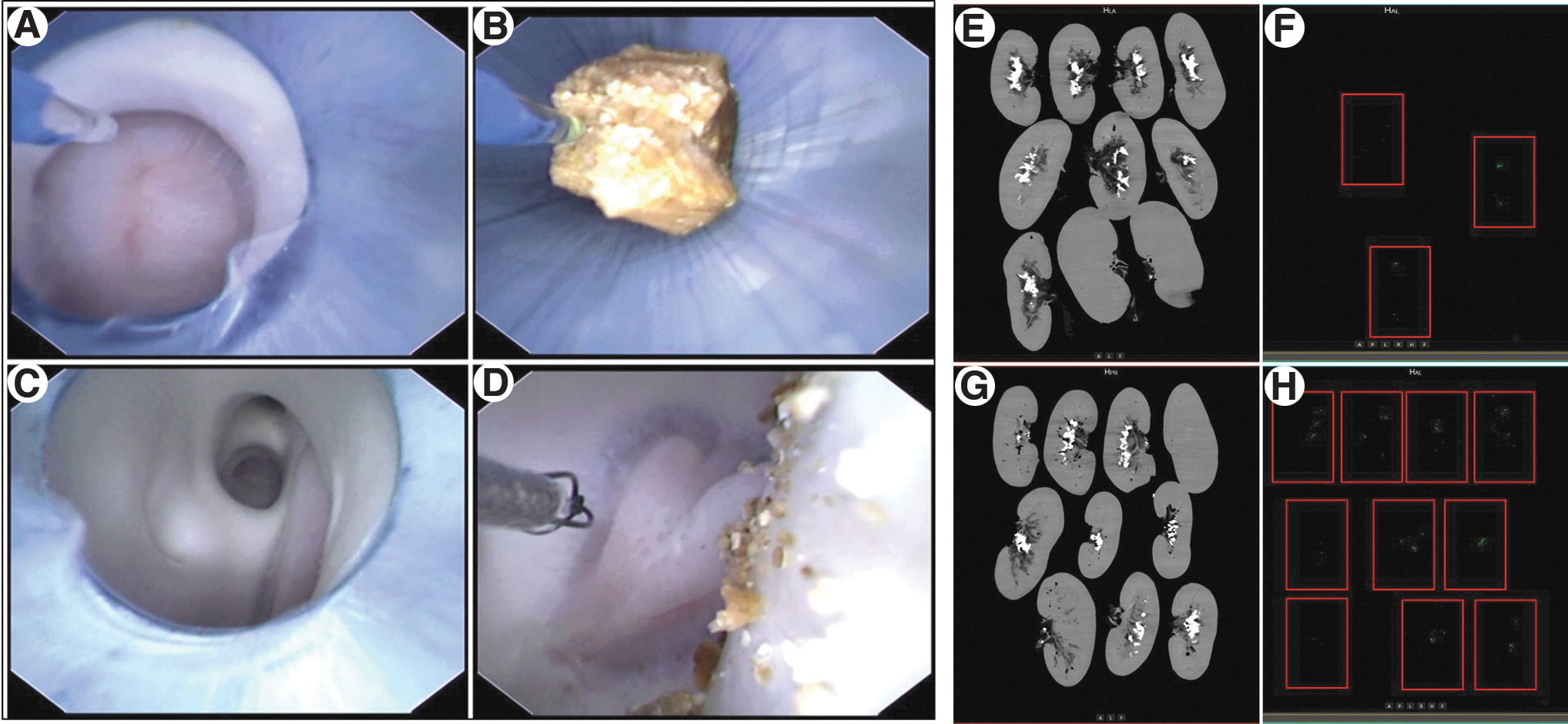
FV-UAS can follow f-URS to cross the UPJ and enter the renal pelvis and calices (Fig. 3A). Without using a basket, the stones can also flow out of the body with irrigation fluid when f-URS is withdrawn (Fig. 3B). Seven cases achieved complete stone-free status in the FV-UAS group (Fig. 3F). All cases had RFs that the basket could not capture postoperatively in the traditional UAS group (Fig. 3D, H). There is an edited surgical video for supplemental clarification (Supplementary Video S1).
Simulates RIRS:
Discussion
It is difficult to control IRP in RIRS when using traditional UAS. It is difficult for traditional UAS to cross the UPJ and enter the renal pelvis and calices; hence, some scholars place the UAS below the UPJ. 15 As a result, the irrigation fluid in the kidney needs to pass through the UPJ to enter the UAS. The UPJ is relatively narrow and acts as a functional valve between the renal pelvis and proximal ureter, obstructing the control of IRP. 15 It may cause the mucous membrane to block UAS opening when the UAS is placed below the UPJ and is used. In traditional surgery, the IRP is reduced by decreasing the irrigation fluid velocity; in the meantime, the decrease in velocity worsens the field of vision. 18 Some UAS for siphon and suction are designed applying the principle of active suction, but this problem of mucous membrane to block UAS opening still exists. 18 –21
FV-UAS reduced the IRP in our experiment. The FV-UAS can follow the f-URS to cross the UPJ and enter the renal pelvis and calices, avoiding the impact of UPJ on the control of IRP. The IRP can be maintained at a lower level (<10 cmH2O) by increasing the negative value at any irrigation fluid velocity. There is no mucosa blocking the FV-UAS opening when using vacuum-assisted because the FV-UAS is located in a renal collection system with a larger space.
The production of dust and RFs in the RIRS is inevitable. A study showed that the residual rates of RFs <3, <2, and <1 mm were 10% to 15%, 16.1%, and 86%, respectively, in RIRS. 22 It takes a long time and may cause renal colic and hematuria and increase the stone size of RFs in the self-elimination process. 8,9 To date, there is no clear way to remove these RFs completely. Hein and colleagues presented the extraction of adhesive stone using a biocompatible adhesive, and its ability to extract fragments was 1 mm. 17,23,24
The application of FV-UAS can achieve complete stone-free status. Stones of ≤1 mm can follow the irrigation fluid to drain from the gap between the f-URS and FV-UAS in our experiment. The stones of size 2 to 4 mm can flow out of the body with irrigation fluid when f-URS is withdrawn (Fig. 3B). If the suction channel is blocked with the generated fragments, our approach is to use a laser for stone fragmentation inside the flexible UAS or use an f-URS to push the fragments away. Finally, seven cases were completely stone free in the FV-UAS group (Fig. 3F). All cases had RFs that the basket could not capture postoperatively in the traditional UAS group (Fig. 3D, H). We thought of it as a vacuum cleaner; the dust cannot be removed when the vacuum cleaner is placed far from dust, to suck more dust, the vacuum cleaner must be moved closer to the dust. The FV-UAS is called a vacuum cleaner in the kidney. Vacuum-assisted treatment has been reported to improve the stone-free status. 20,21
High-velocity irrigation fluids can carry more stone fragments from the body. We introduce the concept of drag force (FD) to understand the effect of irrigation fluid velocity on stones. The drag force is one of the forces that water acts on the sediment particles.
25
Drag force formula:
The FV-UAS has limitations that must be connected to a vacuum suction device to achieve the function of actively controlling the IRP. FV-UAS cannot reach the lower calices of the small infundibulum-pelvic angle with the assistance of f-URS. We suggest using a basket to grab the stones and place them in the upper calices or middle calices before stone fragmentation when FV-UAS cannot reach the calices. The maximum band of the flexible UAS was related to the f-URS. The maximum band with the help of f-URS (7326071; Richard Wolf GmbH) was approximately 145°. The ultimate curvature of f-URS will be limited when the FV-UAS at the end of f-URS is on the same level (Fig. 1B). Restore the ultimate curvature of f-URS by extending f-URS forward or withdrawing FV-UAS.
The study has some limitations, such as in vitro model research. Therefore, it is necessary to further confirm the role of FV-UAS in clinical settings.
Conclusion
Our preliminary experience shows that FV-UAS can follow f-URS to cross the UPJ and into the renal pelvis and calices, avoiding the interference of UPJ in controlling IRP. The FV-UAS can actively control the IRP to be reduced to the desired range by adjusting the negative value under any irrigation fluid velocity. FV-UAS close to the stone can achieve complete stone-free status in RIRS. We call the FV-UAS a vacuum cleaner in the kidney. However, further clinical studies and comparisons with available techniques are required.
Footnotes
Authors' Contributions
Conception and design by J.C. and R.K. Surgeon: R.K. Acquisition of data by Y.C., C.L., L.L., L.Z., and L.G. Analysis and interpretation of data by Y.C. and C.L. Drafting of the article and statistical analysis by Y.C., C.L., and L.G. Critical revision by J.C., R.K., and L.K.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was funded by Health Commission of Jiangxi Province (202210011 to J.C.).
Supplementary Material
Supplementary Video S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.