
Abstract
Background:
The purpose of this study is to analyze quality-of-life (QoL) metrics in men treated with focal cryoablation (FC) compared with active surveillance (AS) for localized prostate cancer over a 4-year follow-up period. We further investigated the effect of prostate size and minimum tumor temperature on QoL outcomes.
Methods:
An Institutional Review Board-approved database was reviewed for patients who underwent FC or AS. QoL questionnaire responses were collected and scores were analyzed for differences between FC and AS, between prostate volume <50 cc and ≥50 cc, and “cold” (<−78°C) and “warm” (≥−78°C) tumor temperatures.
Results:
One hundred forty-eight AS and 60 FC patients were included. Compared with AS, no significant difference existed in urinary function (UF) measured by Expanded Prostate Cancer Index Composite (EPIC) (p = 0.593) and International Prostate Symptom Score (IPSS) (p = 0.241), bowel habits (p = 0.370), or anxiety (p = 0.672) across time post-FC. FC had significantly worse sexual function (SF) compared with AS measured by EPIC (p < 0.0001) and International Index of Erectile Function (IIEF) (p < 0.0001). Patients with prostate volume <50 cc did not demonstrate differences between AS and FC in UF on EPIC (p = 0.459) or IPSS (p = 0.628), but FC patients had worse SF on EPIC (p < 0.001) and IIEF (p < 0.001). FC patients with a prostate volume ≥50 cc had better UF measured by IPSS (p < 0.05) and similar SF on EPIC (p = 0.162) and IIEF (p = 0.771) compared with AS. UF over time measured by EPIC (0.825) and IPSS (p = 0.658) was the same between AS, “warm,” and “cold” FC groups. AS had significantly better SF than the “warm” and “cold” FC groups on EPIC (p < 0.001) and IIEF (p < 0.05).
Conclusions:
No differences were found in anxiety, urinary, or bowel function between AS and FC. Despite differences in SF, patients with larger prostates had no difference in SF and improved UF compared with AS. Future studies with larger cohorts are needed.
Introduction
Majority of patients with prostate cancer (PCa) receive a diagnosis of low- to intermediate-risk disease. 1 Active surveillance (AS) was developed as a conservative management strategy for these patients, with intent to avoid or delay treatment-related adverse effects by monitoring patients PCa for disease progression. 2,3 Despite adequate disease control and excellent quality-of-life (QoL) outcomes in patients who pursue AS, it is underutilized, possibly because of the psychologic burden of living with untreated PCa. 3 –5
Focal cryoablation (FC) has gained traction recently as a middle ground between AS and radical treatment. 6 Cryoablation involves controlled freezing of the prostate gland. 7 During the freezing process, protein denaturation, disruption of blood supply, and eventual apoptosis occurs. 7 The purpose of using this therapy focally is to treat the index lesion. 6,8,9 Although clinically insignificant tumors may coexist elsewhere, the index tumor is hypothesized to drive the biology of the disease and destruction of this tumor mitigates disease progression. 9 Destroying the index lesion rather than the whole gland spares the contralateral neurovascular bundle, potentially preserving genitourinary function. 6,8,9 Because FC eliminates disease, it may be preferable to AS. It is, therefore, important to understand QoL outcomes after FC and consider factors compromising outcomes as it may allow for improved patient selection.
During cryoablation, nerve damage may result from the lethal temperatures the prostate is exposed to; the extent of damage is temperature dependent. 10 –12 In addition, because tissue temperatures of the prostate gland are based on the cryoprobe radius, patients with small prostates may be at higher risk for nerve damage. 13,14 Therefore, we analyzed QoL metrics in men treated with FC compared with patients who deferred definitive treatment with AS. We further investigated the effect of prostate size and minimum tumor temperature on QoL outcomes.
Methods
Database maintenance
An IRB-approved prospectively maintained PCa database was reviewed. This database includes reports of patient-reported QoL surveys, including Expanded Prostate Cancer Index Composite (EPIC), International Prostate Symptom Score (IPSS), International Index of Erectile Function (IIEF) Questionnaire, and the Memorial Anxiety Scale for Prostate Cancer. 15 –18 Informed consent was received, and survey sets were mailed out after consent every 3 months for the first year and every 6 months for 4 years thereafter.
Study population
Patients were included in analysis if they were on AS or received FC as primary treatment, completed at least one survey within 4 years after treatment, and had low- to intermediate-risk PCa based on D'Amico risk criteria. Patients who had a history of a BPH procedure before treatment, AS patients who went on to receive definitive therapy, or FC patients who received hormone or salvage treatment before response were excluded. Tumor characteristics and demographics were recorded.
FC protocol
Patients were offered FC if they had a prostate-specific antigen (PSA) <10 ng/mL, unilateral disease, and lack of extracapsular extension. A single surgeon performed all cryoablation procedures using Galil Cryotherapy Surgical System (Galil Medical, Inc., Arden Hills, MN). Details on transrectal ultrasound (TRUS) cryoablation were previously outlined. 19 The prostate gland dimensions, volume, location of the urethra, peripheral zone, and distance to capsule were recorded through TRUS. Each cryoprobe was transperineally inserted into the prostate 10 mm apart, within 5 mm from the capsule, using a brachy-style grid. Prostate tissue was cooled to −40°C. The ice ball was monitored throughout on TRUS. A double freeze–thaw cycle was performed. Temperatures were monitored with thermal sensors. 7 Minimum temperature recorded out of cryoprobes was termed “minimum tumor temperature” for subsequent analysis.
AS protocol
Patients with Gleason group (GG) 1 or 2, clinical stage T1 or T2, and no evidence of extracapsular extension on multiparametric magnetic resonance imaging (mpMRI) were considered for AS (3). Men with GG 3 and significant comorbidities, shorter life expectancy, or favorable disease characteristics were also offered AS. 3
Patients on AS received PSA testing every 3 months and an annual mpMRI scan. 3 Patients warranted biopsy if they had a rise in PSA, unfavorable genomics, or disease progression on mpMRI. If confirmation biopsy was performed, upgrade of GG or increased volume of positive cores from the original tumor were indications for treatment. Patient preference was an additional indication for treatment. 3
Patient cohort design and statistical analysis
FC QoL scores were compared with AS scores. In the next portion of our analysis, patients were divided into two cohorts based on prostate volume—those with a prostate volume <50 cc and patients with a prostate volume ≥50 cc. QoL scores were then compared within each prostate volume cohort between FC and AS. The final portion of analysis divided the FC group into categories based on minimum tumor temperature achieved during ablation; these are noted as “cold” and “warm.” Tumor temperatures were compared against each other and AS. The “cold” group was defined as temperatures below −78°C and the “warm” cohort had temperatures of −78°C or above.
Patient characteristics were summarized using descriptive statistics. FC and AS cohorts were compared using the chi-square test or Fisher's exact test, as deemed appropriate, for categorical variables and the two-sample t-test or Mann–Whitney U test for continuous data.
Timing of the surveys was rounded to the nearest year and compared across time (12, 24, 36, and 48 months) using mixed-effects repeated measures analysis of covariance (RMANCOVA) models, adjusting for differences found between the groups in the univariate analyses and of clinical relevance. A group × time interaction effect was examined to determine the rate of change over time between AS and FC groups. p < 0.05 was considered statistically significant. Analyses were performed using SAS version 9.4 (SAS Institute, Inc., Cary, NC).
Results
Between 2014 and 2021, 148 AS (prostate volume <50 = 87, prostate volume ≥50 = 61) and 60 FC (prostate volume <50 = 39, prostate volume ≥50 = 21, “warm” = 27, “cold” = 33) patients met the inclusion criteria, with median follow-up of 78 months. Groups were comparable in age (66 vs 67 years, p = 0.082). Majority AS patients had low-risk PCa (82%), whereas majority FC patients had intermediate-risk disease (60%) (p < 0.001). Baseline tumor characteristics and demographics are found in Table 1.
Demographic Characteristics of Patients Who Underwent Focal Cryoablation Compared with Those Who Pursued Active Surveillance
IQR = interquartile range; PDE-5 = phosphodiesterase-5; PSA = prostate-specific antigen.
No difference was found in baseline prostate volume between AS or FC patients (44 cc vs 41 cc; p = 0.212). Urinary medication (p = 0.079) and phosphodiesterase-5 (PDE-5) inhibitor use (p = 0.527) at baseline was nearly equivalent in the two cohorts.
Effect of FC vs AS on QoL
There was not a significant difference in urinary function (UF) across time between the AS and FC groups as measured by both EPIC (p = 0.593) and IPSS (p = 0.241) (Fig. 1A, E). Significantly more FC patients used urinary medications post-treatment compared with AS (55% vs 24%; p < 0.001).
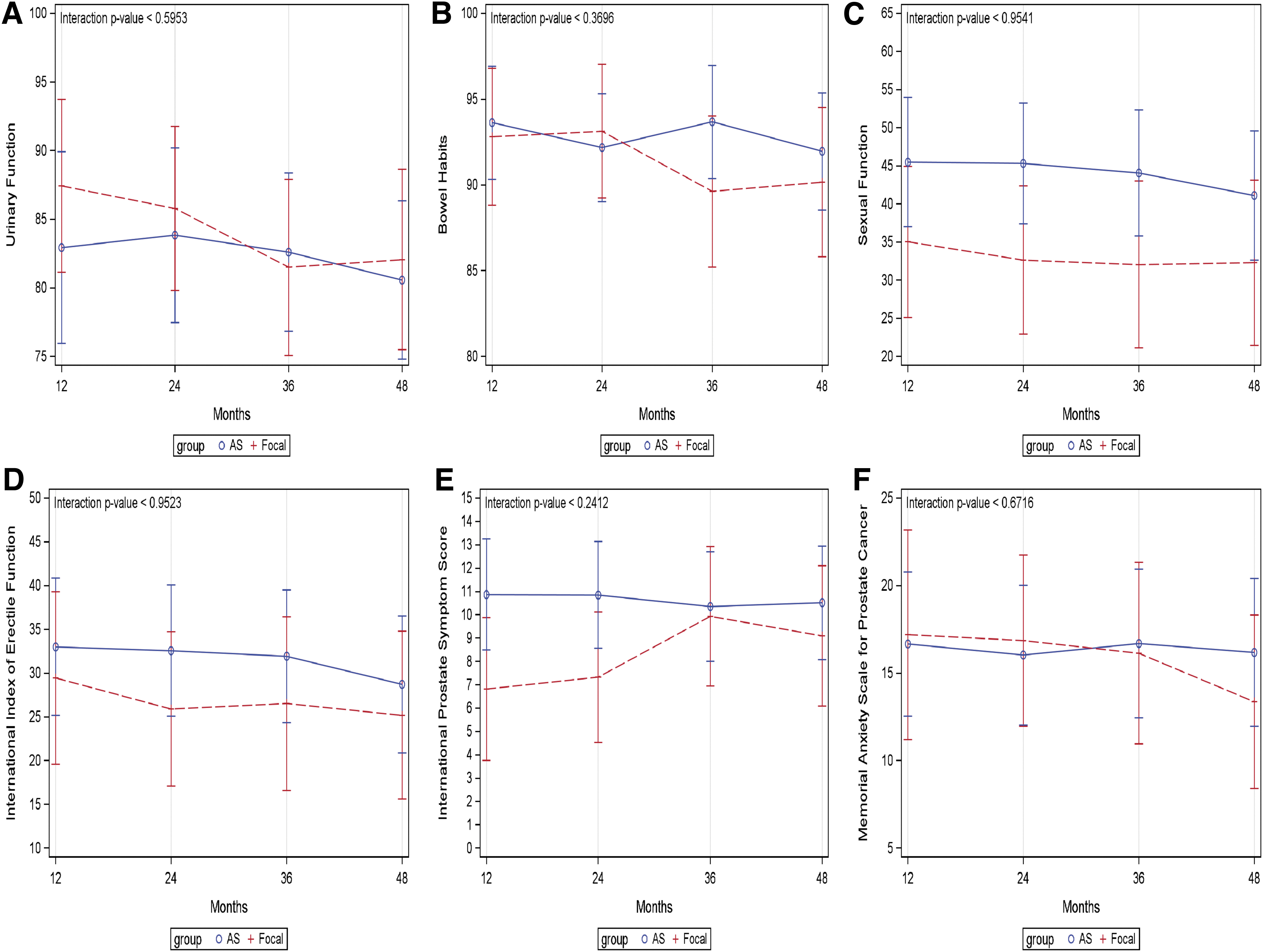
PCa patient-reported QoL 4-year progression after AS vs FC measured by
No significant difference existed across time between FC and AS groups with respect to bowel habits (BH) (p = 0.370) (Fig. 1B). Likewise, anxiety scores did not significantly change across time (p = 0.672) (Fig. 1F).
Sexual function (SF) did not significantly differ over time on EPIC (p < 0.954) or IIEF (p < 0.952) (Fig. 1C, D). However, patients post-FC reported significantly lower overall SF scores relative to AS quantified by EPIC (33 vs 44; p < 0.001) and IIEF (27 vs 32; p < 0.001). On IIEF subdomain scores, AS reported better erectile function (16 vs 10; p < 0.001), intercourse satisfaction (6.5 vs 3.8; p < 0.001), orgasmic function (6.5 vs 4.7; p < 0.005), and overall satisfaction (5.9 vs 4.6; p < 0.05) compared with FC. Yet, there was no difference in sexual desire (6.5 vs 5.8; p = 0.083). PDE-5 inhibitor use post-treatment did not differ among both cohorts (30% vs 32%; p = 0.804).
Effect of prostate volume on FC QoL
Patients with a prostate volume <50 cc who underwent AS or FC did not demonstrate differences in UF on EPIC (87 vs 85, p = 0.459) or IPSS (8.8 vs 9.4, p = 0.628), whereas differences were found in UF when comparing the two treatments in those with prostate volume ≥50 cc (Fig. 2A, E). Compared with AS, the FC group exhibited significantly less urinary symptoms on IPSS (12 vs 7, p < 0.05) although no significant difference was seen in EPIC (82 vs 87, p = 0.119). Regardless of prostate volume, significantly less AS patients took urinary medications than FC patients in those with a prostate <50 cc (18% vs 49%, p < 0.001) and those with a prostate volume ≥50 cc (33% vs 67%, p = 0.007).
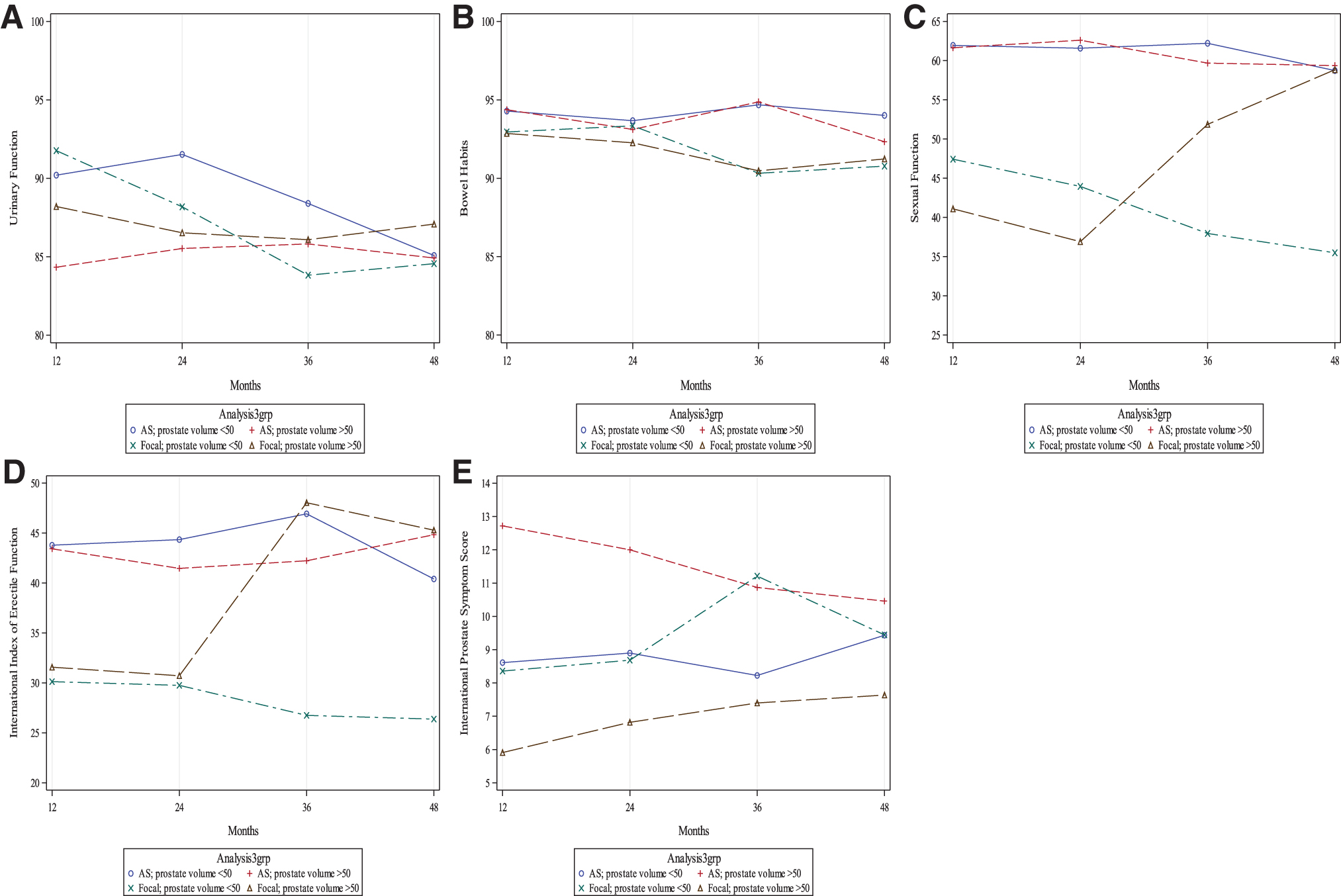
PCa patient-reported QoL 4-year progression after AS vs FC in patients with a prostate volume ≥50 cc compared with patients with a prostate volume <50 cc measured by
In patients with a prostate volume <50 cc, compared with AS, FC patients had significantly worse SF overall measured by EPIC (54 vs 35; p < 0.001) and IIEF (42 vs 27; p < 0.001) (Fig. 2C, D). However, in both EPIC and IIEF, this change over time was not significant (p = 0.645; p = 0.724). When compared with AS, IIEF subdomain scores in FC patients showed significantly worse erectile function (p < 0.001), intercourse satisfaction (p < 0.001), orgasmic function (p < 0.009), and overall satisfaction (p < 0.006).
No difference was found in sexual desire between both groups (p = 0.199). PDE-5 inhibitor use was similar among the two groups (30% vs 28%; p = 0.878). In contrast, men with prostate volume ≥50 cc did not demonstrate significant differences in SF between the AS or FC groups on EPIC (53 vs 43; p = 0.162) or IIEF (39 vs 38; p = 0.771). No difference was observed in IIEF subdomain in erectile function (p = 0.671), intercourse satisfaction (p = 0.701), orgasmic satisfaction (p = 0.425), sexual desire (p = 0.531), or overall satisfaction (p = 0.813). In addition, there was no difference in PDE-5 inhibitor use (34% vs 33%; p = 0.927).
Effect of FC on minimum tumor temperature
There was no statistically significant difference in UF measured by EPIC (p = 0.825) and IPSS (p = 0.658) or BH (p = 0.898) among the AS, “warm,” and “cold” groups when measured over entire time course or yearly intervals (Fig. 3A, B, E). Urinary medication use was significantly different among the AS, “warm,” and “cold” cohorts (24%, 48% vs 61%, p < 0.001). SF was also significantly different among the groups as measured by EPIC (54 vs 44 vs 32; p < 0.001) and IIEF (41 vs 32 vs 30; p < 0.05) (Fig. 3C, D).

PCa patient-reported QoL 4-year progression after AS vs “cold” or “warm” FC measured by
Conversely, no significant difference was observed in the progression of SF over time in either cohort for EPIC (p = 0.981) or IIEF (p = 0.997). In all IIEF subdomains, erectile function (16 vs 11 vs 10; p = 0.005), intercourse satisfaction (6.5 vs 3.6 vs 4.0; p = 0.004), orgasmic function (6.5 vs 5.5 vs 4.0; p = 0.003), sexual desire (6.5 vs 6.5 vs 5.2; p = 0.024), and overall satisfaction (5.9 vs 4.7 vs 4.6; p = 0.022), the AS group had significantly better scores compared with the “warm” and “cold” groups. There was no difference in PDE-5 inhibitor use among groups (p = 0.802).
Discussion
FC serves as a middle ground between AS and radical therapy by selectively targeting the index lesion while attempting to preserve functional outcomes. 6,8,9 In this study, we demonstrate over a 4-year follow-up period, no significant differences in UF, BH, or anxiety scores between men treated with FC compared with AS. Unsurprisingly, patients treated with FC had worse SF compared with AS. However, SF scores did not differ among AS and FC in men with large prostates and scores were slightly improved in men treated with FC with “warm” temperatures compared with “cold” temperatures. Men with large prostate glands had significantly less urinary symptoms on IPSS compared with AS patients suggesting a favorable role in FC in men with large prostate glands.
Interestingly, FC patients had better UF compared with AS over the first 24 months after treatment. This finding was significant in FC patients compared with AS patients with prostate glands ≥50 cc as measured by IPSS. These findings may indicate a dual role for FC in BPH and PCa management. Previously, Wang et al analyzed 21 patients with severe BPH who were treated with cryoablation for symptom management. 20 As was found in our study, cryoablation offered this cohort short-term improvement of urinary symptoms. In addition, Wang et al identified a significant improvement in urinary flow rate compared with pretreatment values. 20 The initial improvement of urinary symptoms after cryoablation may be caused by destruction of the alpha receptors in the prostate. 21 Furthermore, cryoablation decreases prostate size after involution of the treated area, which may further relieve symptoms. 21
Men with large prostate volumes also demonstrated no significant differences in SF between the two treatments. Although FC patients had lower SF scores compared with AS initially, these scores progressed to scores similar to AS over time. In contrast, FC patients with small prostate volumes demonstrated overall lower SF scores than AS, which persisted throughout the follow-up period. This may be because of the initial injury of the neurovascular bundles, a complication of cryoablation. 7 Previous studies identified the nerve damage to be transient, as axonal regeneration can occur. 10 –12
If the neural sheath is not irreversibly damaged, both sensation and motor function may return over several years. The extent of which this nerve damage occurs is temperature dependent. This may indicate why patients treated with “warmer” temperatures demonstrated slightly improved SF than those treated with “colder” temperatures. 7,10 –12 Furthermore, neurovascular bundles in men with large prostate glands may be less likely to be exposed to the lethal temperatures the neoplastic cells are exposed to compared with those with smaller prostate glands. 13
To our knowledge, this is the first study examining anxiety in FC patients compared with AS. Anxiety is an important consideration in patients choosing AS, as repeat PSA, biopsies, and mpMRI tests, required by the protocol, have been proven to provoke anxiety. 3 –5 Although no significant difference existed in anxiety scores among the two groups, AS patients' scores maintained high scores throughout whereas FC patients' scores trended downward. Although FC patients may have no difference in anxiety scores from patients who defer treatment, over time FC patients' anxiety may progress to lower levels than AS.
Our study reports on QoL outcomes using validated measurements over a 4-year follow-up period. Nevertheless, several limitations need to be considered. Because of the retrospective nature of our study, baseline scores were not sufficiently available to include. However, AS patients serve as the control, thus FC scores were compared with AS. In addition, as a result of the retrospective nature of this study, not all patients completed all survey sets and thus surveys that were filled out early on by respondents may not represent long follow-up.
Furthermore, this study is not devoid of selection bias. There is a significant imbalance in baseline tumor risk between the two cohorts; however, a previous study found tumor risk does not significantly confound the association between PCa treatment and QoL outcomes. 22 Although our study was a single-center study and thus sample size was a limitation, all procedures were performed by the same surgeon. Supplementary high-powered prospective and randomized studies are necessary to further explore QoL in patients opting for FC or AS.
Conclusions
This study provides insight on QoL in patients who undergo FC compared with AS. We find no difference in UF, BH, or anxiety scores over the 4-year follow-up period. Despite differences in SF between the two cohorts, patients with larger prostates had no difference in SF and improved UF compared with AS. Although future studies with larger cohorts are needed, these findings may facilitate counseling in patients deciding between these two therapies.
Footnotes
Authors' Contributions
A.M., J.S., and A.K. contributed to conception and design. A.M. and J.S. contributed to data collection. A.M. and M.A. contributed to data analysis and interpretation. A.M., J.S., M.A., P.J., A.C., and A.K. contributed to article writing. A.M., J.S., M.A., P.J., A.C., and A.K. contributed to final approval of article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.